The Royal Marsden. Surgery for Gastric and GE Junction Cancer: primary palliative when and where? William Allum
|
|
|
- Harold Barber
- 5 years ago
- Views:
Transcription


1 The Royal Marsden Surgery for Gastric and GE Junction Cancer: primary palliative when and where? William Allum
2 The Royal Marsden William Allum Conflict of Interest None


3 Any surgeon can cure Surgeon - dependent No surgeon can cure EMR D2 GASTRECTOMY H N SN. WEDGE P EMR, endoscopic mucousal resection.

4 4 Algorithm of Standard Treatment Neoadjuvant Chemotherapy
5 The Royal Marsden Subtypes of gastric cancer Type Features Diffuse, signet ring cancer Intestinal type, distal gastric cancer Proximal, non-diffuse cardia / junctional cancer CDH-1 mutation Lepidic growth Peritoneal metastasis Correa hypothesis chronic inflammation H.Pylori associated Obesity / GORD related H. pylori protective Poorest prognosis HER2 strongest expression
6 The Royal Marsden R0 Resection A surgical procedure in which there is no evidence of macroscopic residual tumour in the tumour bed, lymph nodes and/or distant sites with microscopic negative resection margins Hermanek P, Wittekind C. Pathol Res Pract. 1994;190(2):
7 Japanese Rules End Results of Surgical Resection Cumulative Survival Rate, % Years Absolute curative 78.7±1.7%; n=2706 Relative curative 39.6±3.7%; n=823 Relative non-curative 16.5±4.8%; n=281 Absolute non-curative 1.4±0.9%; n= Maruyama Jpn J Surg 11:
8 Indication and Division Lines for Distal Subtotal and Total Gastrectomy Distal subtotal gastrectomy >2cm from cardia >5cm from cardia Total gastrectomy Early cancer or well-circumscribed advanced cancer Infiltrative advanced cancer <5cm 3cm When the proximal distance from the cardia is less than the required length, total gastrectomy is indicated Total gastrectomy is always indicated in diffuse carcinoma (Borrmann type 4) regardless of its size



9 Total Gastrectomy and Lymph Node Dissection 4d 4sb D1 D1+ D2 4sa a 8a p 11d 10 Japanese Gastric Cancer Association, 2011 Gastric Cancer 14:



10 Distal Gastrectomy and Lymph Node Dissection 4d 4sb D1 D1+ D a 8a p Japanese Gastric Cancer Association, 2011 Gastric Cancer 14:
11 11 The Royal Marsden Western Trials UK MRC D1 vsd2 (1996, 1999) 5 year survival D1 35% D2 33% Operative mortality D1 6.5% D2 13% Dutch Gastric Cancer trial (2010) operative mortality D1 4% D2 10% 15 year survival D1 21% D2 29% (NS) gastric cancer deaths D1 48 D2 37 (p 0.01) Italian trial (2014) operative mortality D1 3.0% D2 2.2% 5 year survival D1 66.5% D2 64.2% pt2-4 / N0 D1 38% D2 59%
12 The Royal Marsden European Guidelines Surgery GUIDELINE GASTRIC RESECTION LYMPHADENECTOMY SIGN (2006) German S3 (2011) R0 (proximal, distal circumferential margins) R0 (proximal, distal circumferential margins) 5cm intestinal 8cm diffuse D2 > 25 lymph nodes D2 > 25 lymph nodes > 16 nodes for TNM No pancreatectomy / splenectomy UK (2011) R0 D2 for stage II & III if fit St Gallen (2012/2018) ESMO (2016) ct1 diffuse resect R0 T1a T1b - III > 15 nodes for TNM D2 without pancreatectomy or splenectomy D1 alpha / beta D2
13 The Royal Marsden Surgery in ST03 Radicality of Resection ECX (n=533) ECX+B (n=530) p-value Extent of resection R0 315 (74%) 301 (75%) R1 108 (26%) 100 (25%) No resection Unavailable (84%) underwent surgical resection Operative mortality 2.7% Operative morbidity 52% Respiratory 24%, Sepsis 18%, Wound healing 10%
14 The Royal Marsden Lymph node resection status ECX ECX+B Total Number of nodes n % n % n % Median (IQR) 24 (17-33) 25 (18-34) 24 (17-34) Range Take home message >15 nodes 82% >25 nodes 49% None < Unknown 4 <1 3 <1 7 <1 TOTAL Acknowledgment: Bill Allum for help with these slides
15 Post-operative survival by Resection Status
16 Left thoraco-abdominal approach versus abdominal transhiatal approach in Siewert type II and III (JCOG 9502) Gastric carcinoma, oesophageal invasion ( 3 cm) T2-4, N0-2, M0 Preoperative randomisation of institution, macroscopic type, clinical T Abdominal (AT) Total gastrectomy, D2 + left upper paraaortic dissection Thoraco-abdominal (LT) Total gastrectomy, D2 + left upper paraaortic + mediastinal dissection Observation if curative resection AT, abdominal transhiatal; LT, left thoraco-abdominal. Sasako et al. Lancet Oncol. 2006;7(8):
17 JCOG 9502 Overall Survival Proportion Surviving AT: Abdominal (n=82) LT: Thoraco-abddominal (n=85) Years After Randomization Sasako et al. Lancet Oncol. 2006;7(8):
18 D2 lymphadenectomy alone or with para-aortic nodal dissection for gastric cancer (JCOG 9501) Adenocarcinoma T2b/T3/T4, N0/N1/N2, Curative operation, Lavage cytology (-) Intraoperative Randomisation 523 patients enrolled between July 1995 and April Institutions Survival analysis performed April 2006 Group A (standard) D2 Group B (Extended) D2 + PAND Observation Endpoints 1. Overall survival 2. Recurrence-free survival, morbidity/mortality PAND, para-aortic nodal dissection. Sasako M, et al. N Eng J Med. 2008;359(5):
19 JCOG 9501 Overall Survival 1.00 Overall Survival, % year Survival 5-year Survival D2 (n=263) 76.4% 69.2% D2 + PAND (n=259*) 76.4% 70.3% D2 D2 + PAND HR=1.03 ( ) one-sided P= HR, hazard ratio. *One case was ineligible because of changed histologic diagnosis. Sasako M, et al. N Engl J Med. 2008;359(5): Years
20 JCOG 0110 Splenectomy or Not Adenocarcinoma in upper 1/3 T2/T3/T4, N0/N1/N2, Not greater curve, Curative operation, Lavage cytology (-) Intraoperative randomisation Group A (Splenectomy) Total gastrectomy, D2 Group B (Spleen preserve) Total gastrectomy, D2 Observation (S-1 adjuvant for Stage II/III) Endpoints 1. Overall survival Sano T, et al. J Clin Oncol. 2010;28(15 Suppl):abstract Morbidity, operation time, blood loss
21 The Royal Marsden Extended Lymphadenectomy T3/4 cancers Mixed or diffuse histology Upper third of the stomach De Manzoni G, et al. Ann Surg Oncol. 2011;18(8):
22 Extended Lymphadenectomy 1.0 Probability of Survival pn 0 pn 1 pn 2 pn 3 M1a Time After Operation, months Roviello F, et al. Eur J Surg Oncol. 2010;36(5):
23 The Royal Marsden Splenectomy or Not (JCOG 0110) Similar operative mortality with or without splenectomy Greater postoperative morbidity with splenectomy Greater intraoperative blood loss with splenectomy Overall Survival Sano T, et al. Annals of Surgery. 2017: 265(2): Relapse free survival
24 The Royal Marsden Minimally Invasive Surgery Shorter inpatient stay Less blood loss Quicker return to GI function? Anastomotic leak rates Intraluminal bleeding
25 The Royal Marsden Minimally Invasive Surgery KLASS 01 Trial Laparoscopic Distal Gastrectomy in early disease Morbidity 14.8%, Mortality 0% Survival LADG 95.8% vs ODG 95.9%.
26 The Royal Marsden Minimally Invasive Surgery Advanced Disease KLASS 02 LADG vs Open feasible D2 dissection Complications LADG 16.4% ODG 24.3%. KLASS 06 Lap Total Gastrectomy

27 27 The Royal Marsden Nutritional aspects of Enhanced Recovery Robotic vs Laparoscopy Obesity and Type of Gastrectomy No difference estimated blood loss, retrieved lymph nodes, complication rates, open conversion, length of stay Lymph node dissection Lower blood loss for robotic after D2 but not <D2 Cost Robotic more expensive 250% Park et al. EJSO 42 (2016) Kim et al Ann Surg 2016; 263:103-9
28 OESOPHAGO-GASTRIC JUNCTIONAL ADENOCARCINOMA
29 The Royal Marsden TNM-8 Oesphagogastric Junction Oesophagus and Gastric Carcinomas A tumourthe epicenter of which is within 2 cm of the oesophagogastricjunctionand also extends into the oesophagusis classified and staged using the oesophagealscheme. Cancers involving the oesophagogastricjunction (OGJ) whose epicenteris within the proximal 2 cm of the cardia(siewerttypes I/II) are to be staged as oesophageal Cancers whose epicenteris more than 2 cm distal from the OGJ will be staged using the Stomach Cancer TNM and Stage even if the OGJ is involved.



30 OESOPHAGO-GASTRIC JUNCTIONAL ADENOCARCINOMA Type I Type II Type III The problem of large tumours Accuracy of preoperative endoscopy and imaging techniques Location of the epicenter of the tumour vs. length of esophageal or gastric involvement
31 The Royal Marsden Operation Selection Surgical Approach Margins Lymphadenectomy
32 EORTC Consensus St Gallen 2012 / 2018 Type I Oesophago-gastrectomy Type II Oesophago-gastrectomy or Extended Total Gastrectomy Type I & II Mediastinal Lymphadenectomy 2 field Type III - Extended Total Gastrectomy
33 The Royal Marsden Dutch Trial Trans Hiatal Oesophagectomy vs Trans Thoracic Oesophagectomy 220 patients with mid and lower oesophageal ACA THO Lower morbidity TTO More nodes More respiratory complications Hulscher et ln Engl J Med 2002;347:

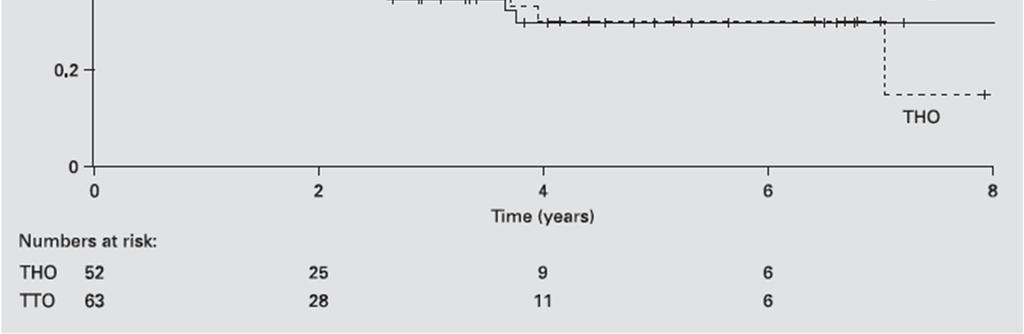
34 Dutch Trial THO vs TTO
35 Dutch Trial THO vs TTO
36 The Royal Marsden Minimally Invasive Oesophagectomy 101 open; 65 MIO; 9 Conversion pt1a & pt1b. N0 Intraoperative Morbidity Medium Term MIO Less blood loss Gastroparesis Less pain OPEN Shorter time Respiratory More fatigued Nafteux et al 2011 Eur J Cardio Surgery 40: 1455
37 The Royal Marsden Minimally Invasive Oesophagectomy MIRO trial Major Complications Respiratory Complications Survival 3 yr OE (n=104) 67 (64.4%) 31 (30.1%) 54.8% HMIE (n=103) 37 (35.9%) 18 (17.7%) 67.0% TIME trial Respiratory Complications Survival 3 yr OE (n=56) 19 (34%) 40.4% HMIE (n=59) 7 (12%) 50.5% Biere et al Lancet 2012; 379: Straatman et al Ann Surg 2017; 266: Mariette et al ESMO 2017
38 The Royal Marsden Operation Selection Surgical Approach Margins Lymphadenectomy
39 Resection Margin and Survival Longitudinal Barbour et al. Ann Surg 246: 1-8
40 The Royal Marsden Circumferential resection margin (CRM) size correlates with overall survival Prospective database, single institution study, N = 229 CRM n Median Survival (95% CI) Probability of survival Kaplan-Meier curves of OS by margin size: --- >2.0mm mm --- <1mm --- 0mm Positive yrs ( ) <1mm yrs ( ) mm yrs (2.0 no upper CI) 2.0mm 105 Not reached Time (years) CRM size is a significant prognostic factor for overall survival 40.6% of patients in this study had a CRM <1mm Post operative chemoradiation did not alter survival in patients with CRM <1mm BUT smaller CRM may just reflect a larger tumour Landau et al., ESMO 2010 (Abstract 711PD)
41 41 The Royal Marsden Nutritional aspects of Enhanced Recovery CRM in Neoadjuvant Trials CS S CF ECX CXRT S OEO2 25% 28% OEO5 41% 33% CROSS 8% 30% Radical Surgery 13% -2/62
42 The Royal Marsden Operation Selection Surgical Approach Margins Lymphadenectomy



43

44 Risk of Systemic Disease and Number of Nodes Involved Peyre et al 2008 Peyre et al 2008 Ann Surg 248:
45
46 The Royal Marsden INCURABLE DISEASE Palliative Intent Quality of life vsquantity of life Patient Wishes Resection vs Chemotherapy? Subtotal vs Total Gastrectomy?
47 The Royal Marsden Palliative Resection Dutch D1 vsd2 trial 295 / 996 (29%) incurable T + H + P + N4 + macroscopically irresectable liver metastasis peritoneal metastasis distant lymph nodes Hartgrink et al Br J Surg 2002, 89:1438
48 The Royal Marsden Dutch Gastric Cancer Trial (D1 D2) Palliative Resection Patients 996 palliative resections 285 (26%) Survival benefit of Surgery: Survival probability no resection resection P = patients < 70 and 1 metastatic site H + P + N4 + liver metastasis peritoneal metastasis distant lymph nodes Years since surgery Numbers at risk: no resection: resection: Hartgrink Br J Surg 2002
49 The Royal Marsden Palliative Surgery Selection ASA I & II Non R0 resection Single site solid organ metastasis Localised peritoneal disease without signet ring cancer (Robb et al 2012) 49

50 The Royal Marsden Lancet Oncology 2016!!
51 The Royal Marsden

52 The Royal Marsden 23 trials including 870 patients Median survival 22 months 5-y-surv. all 23,9 % synchronous 22,6 % metachronous 30,0 %



53 OLIGOMETASTATIC DISEASE Yoshida, Kodera et al Gastric Cancer 2016
54 54 Surgery Quality Assurance


55 55 Clinical pathways EURECCA Upper GI 13 countries affiliated to EURECCA upper GI group Data source Registry National audit National society National audit
56
57 Fontana et al Gastric Cancer 2016



58 Thank you for your attention
The Royal Marsden. Surgery for Gastric and GE Junction Cancer: primary palliative when and where? William Allum Consultant Surgeon
 The Royal Marsden Surgery for Gastric and GE Junction Cancer: primary palliative when and where? William Allum Consultant Surgeon Any surgeon can cure Surgeon - dependent No surgeon can cure EMR D2 GASTRECTOMY
The Royal Marsden Surgery for Gastric and GE Junction Cancer: primary palliative when and where? William Allum Consultant Surgeon Any surgeon can cure Surgeon - dependent No surgeon can cure EMR D2 GASTRECTOMY
Approaches to Surgical Treatment of Gastric Cancer. Byrne Lee, MD FACS Chief, Mixed Tumor Surgery Service
 Approaches to Surgical Treatment of Gastric Cancer Byrne Lee, MD FACS Chief, Mixed Tumor Surgery Service Disclosures I do not have anything to disclose Outline Background Diagnosis Histology Staging Surgery
Approaches to Surgical Treatment of Gastric Cancer Byrne Lee, MD FACS Chief, Mixed Tumor Surgery Service Disclosures I do not have anything to disclose Outline Background Diagnosis Histology Staging Surgery
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only.
 The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
B Breast cancer, managing risk of lobular, in hereditary diffuse gastric cancer, 51
 Index Note: Page numbers of article titles are in boldface type. A Adenocarcinoma, gastric. See also Gastric cancer. D2 nodal dissection for 57 70 Adjuvant therapy, for gastric cancer, impact of D2 dissection
Index Note: Page numbers of article titles are in boldface type. A Adenocarcinoma, gastric. See also Gastric cancer. D2 nodal dissection for 57 70 Adjuvant therapy, for gastric cancer, impact of D2 dissection
Surgery for Gastric and Oesophageal Cancer
 Surgery for Gastric and Oesophageal Cancer Trends in cancer mortality, England and Wales SMR base 1980 Oesophago-Gastric Cancer The National Problem 5 th commonest malignancy 4 th commonest cause of death
Surgery for Gastric and Oesophageal Cancer Trends in cancer mortality, England and Wales SMR base 1980 Oesophago-Gastric Cancer The National Problem 5 th commonest malignancy 4 th commonest cause of death
Conventional Gastrectomy for Gastric Cancer. Franklin Wright UCHSC Department of Surgery Grand Rounds January 14, 2008
 Conventional Gastrectomy for Gastric Cancer Franklin Wright UCHSC Department of Surgery Grand Rounds January 14, 2008 Overview Gastric Adenocarcinoma Conventional vs Radical Lymphadenectomy Non-randomized
Conventional Gastrectomy for Gastric Cancer Franklin Wright UCHSC Department of Surgery Grand Rounds January 14, 2008 Overview Gastric Adenocarcinoma Conventional vs Radical Lymphadenectomy Non-randomized
Esophageal cancer: Biology, natural history, staging and therapeutic options
 EGEUS 2nd Meeting Esophageal cancer: Biology, natural history, staging and therapeutic options Michael Bau Mortensen MD, Ph.D. Associate Professor of Surgery Centre for Surgical Ultrasound, Upper GI Section,
EGEUS 2nd Meeting Esophageal cancer: Biology, natural history, staging and therapeutic options Michael Bau Mortensen MD, Ph.D. Associate Professor of Surgery Centre for Surgical Ultrasound, Upper GI Section,
Epidemiology, aetiology and the patient pathway in oesophageal and pancreatic cancers
 Epidemiology, aetiology and the patient pathway in oesophageal and pancreatic cancers Dr Ian Chau Consultant Medical Oncologist Women's cancers Breast cancer introduction 3 What profession are you in?
Epidemiology, aetiology and the patient pathway in oesophageal and pancreatic cancers Dr Ian Chau Consultant Medical Oncologist Women's cancers Breast cancer introduction 3 What profession are you in?
MINIMALLY INVASIVE ESOPHAGECTOMY FOR CANCER: where do we stand?
 MINIMALLY INVASIVE ESOPHAGECTOMY FOR CANCER: where do we stand? Ph Nafteux, MD Copenhagen, Nov 3rd 2011 Department of Thoracic Surgery, University Hospitals Leuven, Belgium W. Coosemans, H. Decaluwé, Ph.
MINIMALLY INVASIVE ESOPHAGECTOMY FOR CANCER: where do we stand? Ph Nafteux, MD Copenhagen, Nov 3rd 2011 Department of Thoracic Surgery, University Hospitals Leuven, Belgium W. Coosemans, H. Decaluwé, Ph.
Michael A. Choti, MD, FACS Department of Surgery Johns Hopkins Medicine, Baltimore, MD
 Michael A. Choti, MD, FACS Department of Surgery Johns Hopkins Medicine, Baltimore, MD Surgical Therapy of Gastric Cancer CLINICAL QUESTIONS 1. How much of the stomach should be removed? 2. How many lymph
Michael A. Choti, MD, FACS Department of Surgery Johns Hopkins Medicine, Baltimore, MD Surgical Therapy of Gastric Cancer CLINICAL QUESTIONS 1. How much of the stomach should be removed? 2. How many lymph
سرطان المعدة. Gastric Cancer حمود حامد
 سرطان المعدة Gastric Cancer ا أ لستاذ الدك تور حمود حامد عميد كلية الطب البشري بجامعة دمشق Epidemiology second leading cause of cancer death and fourth most common cancer worldwide Overall declining Histologic
سرطان المعدة Gastric Cancer ا أ لستاذ الدك تور حمود حامد عميد كلية الطب البشري بجامعة دمشق Epidemiology second leading cause of cancer death and fourth most common cancer worldwide Overall declining Histologic
Research Article Survival Benefit of Adjuvant Radiation Therapy for Gastric Cancer following Gastrectomy and Extended Lymphadenectomy
 International Surgical Oncology Volume 2012, Article ID 307670, 7 pages doi:10.1155/2012/307670 Research Article Survival Benefit of Adjuvant Radiation Therapy for Gastric Cancer following Gastrectomy
International Surgical Oncology Volume 2012, Article ID 307670, 7 pages doi:10.1155/2012/307670 Research Article Survival Benefit of Adjuvant Radiation Therapy for Gastric Cancer following Gastrectomy
Surgical Treatment of Gastric Cancer
 SMGr up Surgical Treatment of Gastric Cancer Igor Correia de Farias 1 *, Maria Luiza Leite de Medeiros 2, Wilson Luiz da Costa Júnior 1, Heber Salvador de Castro Ribeiro 1, Alessandro Landskron Diniz 1,
SMGr up Surgical Treatment of Gastric Cancer Igor Correia de Farias 1 *, Maria Luiza Leite de Medeiros 2, Wilson Luiz da Costa Júnior 1, Heber Salvador de Castro Ribeiro 1, Alessandro Landskron Diniz 1,
Satisfactory surgical outcome of T2 gastric cancer after modified D2 lymphadenectomy
 Original Article Satisfactory surgical outcome of T2 gastric cancer after modified D2 lymphadenectomy Shupeng Zhang 1, Liangliang Wu 2, Xiaona Wang 2, Xuewei Ding 2, Han Liang 2 1 Department of General
Original Article Satisfactory surgical outcome of T2 gastric cancer after modified D2 lymphadenectomy Shupeng Zhang 1, Liangliang Wu 2, Xiaona Wang 2, Xuewei Ding 2, Han Liang 2 1 Department of General
Newly Diagnosed Cases Cancer Related Death NCI 2006 Data
 Multi-Disciplinary Management of Esophageal Cancer: Surgical and Medical Steps Forward Alarming Thoracic Twin Towers 200000 150000 UCSF UCD Thoracic Oncology Conference November 21, 2009 100000 50000 0
Multi-Disciplinary Management of Esophageal Cancer: Surgical and Medical Steps Forward Alarming Thoracic Twin Towers 200000 150000 UCSF UCD Thoracic Oncology Conference November 21, 2009 100000 50000 0
Gastric Cancer: Surgery and Regional Therapy. Epidemiology. Risk factors
 Gastric Cancer: Surgery and Regional Therapy Timothy J. Kennedy, MD Montefiore Medical Center Assistant Professor of Surgery Upper Gastrointestinal and Pancreas Surgery December 15, 2012 1 Epidemiology
Gastric Cancer: Surgery and Regional Therapy Timothy J. Kennedy, MD Montefiore Medical Center Assistant Professor of Surgery Upper Gastrointestinal and Pancreas Surgery December 15, 2012 1 Epidemiology
Advances in gastric cancer: How to approach localised disease?
 Advances in gastric cancer: How to approach localised disease? Andrés Cervantes Professor of Medicine Classical approach to localised gastric cancer Surgical resection Pathology assessment and estimation
Advances in gastric cancer: How to approach localised disease? Andrés Cervantes Professor of Medicine Classical approach to localised gastric cancer Surgical resection Pathology assessment and estimation
Determining the Optimal Surgical Approach to Esophageal Cancer
 Determining the Optimal Surgical Approach to Esophageal Cancer Amit Bhargava, MD Attending Thoracic Surgeon Department of Cardiovascular and Thoracic Surgery Open Esophagectomy versus Minimally Invasive
Determining the Optimal Surgical Approach to Esophageal Cancer Amit Bhargava, MD Attending Thoracic Surgeon Department of Cardiovascular and Thoracic Surgery Open Esophagectomy versus Minimally Invasive
CLINICAL EFFECTIVENESS
 Re-audit of gastrointestinal tract specimens with respect to compliance with RCPath guidelines Dr Manisha Ram Dr Moina Kadri Background epidemiology and aetiology Over the past 20 years there has been
Re-audit of gastrointestinal tract specimens with respect to compliance with RCPath guidelines Dr Manisha Ram Dr Moina Kadri Background epidemiology and aetiology Over the past 20 years there has been
The Learning Curve for Minimally Invasive Esophagectomy
 The Learning Curve for Minimally Invasive Esophagectomy AATS Focus on Thoracic Surgery Mastering Surgical Innovation Las Vegas Nevada Oct. 27-28 2017 Scott J Swanson, M.D. Professor of Surgery Harvard
The Learning Curve for Minimally Invasive Esophagectomy AATS Focus on Thoracic Surgery Mastering Surgical Innovation Las Vegas Nevada Oct. 27-28 2017 Scott J Swanson, M.D. Professor of Surgery Harvard
Correspondence to: Jiankun Hu, MD, PhD. Department of Gastrointestinal Surgery; Institute of Gastric Cancer, State Key Laboratory of.
 Original Article Comparison of survival outcomes between transthoracic and transabdominal surgical approaches in patients with Siewert-II/III esophagogastric junction adenocarcinoma: a single-institution
Original Article Comparison of survival outcomes between transthoracic and transabdominal surgical approaches in patients with Siewert-II/III esophagogastric junction adenocarcinoma: a single-institution
Surgical Problems in Proximal GI Cancer Management Cardia Tumours Question #1: What are cardia tumours?
 Surgical Problems in Proximal GI Cancer Management Cardia Tumours Question #1: What are cardia tumours? Question #2: How are cardia tumours managed? Michael F. Humer December 3, 2005 Vancouver, BC Case
Surgical Problems in Proximal GI Cancer Management Cardia Tumours Question #1: What are cardia tumours? Question #2: How are cardia tumours managed? Michael F. Humer December 3, 2005 Vancouver, BC Case
COLON AND RECTAL CANCER
 COLON AND RECTAL CANCER Mark Sun, MD Clinical Associate Professor of Surgery University of Minnesota No disclosures Objectives 1) Understand the epidemiology, management, and prognosis of colon and rectal
COLON AND RECTAL CANCER Mark Sun, MD Clinical Associate Professor of Surgery University of Minnesota No disclosures Objectives 1) Understand the epidemiology, management, and prognosis of colon and rectal
Significance of the lymph nodes in the 7th station in rational dissection for metastasis of distal gastric cancer with different T categories
 Original Article Significance of the lymph nodes in the 7th station in rational dissection for metastasis of distal gastric cancer with different T categories Wu Song, Yulong He, Shaochuan Wang, Weiling
Original Article Significance of the lymph nodes in the 7th station in rational dissection for metastasis of distal gastric cancer with different T categories Wu Song, Yulong He, Shaochuan Wang, Weiling
Positive impact of adding No.14v lymph node to D2 dissection on survival for distal gastric cancer patients after surgery with curative intent
 Original Article Positive impact of adding No.14v lymph node to D2 dissection on survival for distal gastric cancer patients after surgery with curative intent Yuexiang Liang 1,2 *, Liangliang Wu 1 *,
Original Article Positive impact of adding No.14v lymph node to D2 dissection on survival for distal gastric cancer patients after surgery with curative intent Yuexiang Liang 1,2 *, Liangliang Wu 1 *,
Akiko Serizawa *, Kiyoaki Taniguchi, Takuji Yamada, Kunihiko Amano, Sho Kotake, Shunichi Ito and Masakazu Yamamoto
 Serizawa et al. Surgical Case Reports (2018) 4:88 https://doi.org/10.1186/s40792-018-0494-4 CASE REPORT Successful conversion surgery for unresectable gastric cancer with giant paraaortic lymph node metastasis
Serizawa et al. Surgical Case Reports (2018) 4:88 https://doi.org/10.1186/s40792-018-0494-4 CASE REPORT Successful conversion surgery for unresectable gastric cancer with giant paraaortic lymph node metastasis
intent treatment be in the elderly?
 Gastric cancer: How strong can curative intent treatment be in the elderly? Caio Max S. Rocha Lima, M.D. Professor of Medicine University of Miami & Sylvester Cancer Center Gastric cancer: epidemiology
Gastric cancer: How strong can curative intent treatment be in the elderly? Caio Max S. Rocha Lima, M.D. Professor of Medicine University of Miami & Sylvester Cancer Center Gastric cancer: epidemiology
Subtotal versus total gastrectomy for T3 adenocarcinoma of the antrum
 Gastric Cancer (2003) 6: 237 242 DOI 10.1007/s10120-003-0261-4 Original article 2003 by International and Japanese Gastric Cancer Associations Subtotal versus total gastrectomy for T3 adenocarcinoma of
Gastric Cancer (2003) 6: 237 242 DOI 10.1007/s10120-003-0261-4 Original article 2003 by International and Japanese Gastric Cancer Associations Subtotal versus total gastrectomy for T3 adenocarcinoma of
DATA REPORT. August 2014
 AUDIT DATA REPORT August 2014 Prepared for the Australian and New Zealand Gastric and Oesophageal Surgical Association by the Royal Australasian College of Surgeons 199 Ward St, North Adelaide, SA 5006
AUDIT DATA REPORT August 2014 Prepared for the Australian and New Zealand Gastric and Oesophageal Surgical Association by the Royal Australasian College of Surgeons 199 Ward St, North Adelaide, SA 5006
Treatment Strategy for Non-curative Resection of Early Gastric Cancer. Jun Haneg Lee. Sungkyunkwan University, Samsung Medical Center, Seoul Korea
 Treatment Strategy for Non-curative Resection of Early Gastric Cancer Jun Haneg Lee. Sungkyunkwan University, Samsung Medical Center, Seoul Korea Classic EMR/ESD data analysis style Endoscopic resection
Treatment Strategy for Non-curative Resection of Early Gastric Cancer Jun Haneg Lee. Sungkyunkwan University, Samsung Medical Center, Seoul Korea Classic EMR/ESD data analysis style Endoscopic resection
Perigastric lymph node metastases in gastric cancer: comparison of different staging systems
 Gastric Cancer (1999) 2: 201 205 Original article 1999 by International and Japanese Gastric Cancer Associations Perigastric lymph node metastases in gastric cancer: comparison of different staging systems
Gastric Cancer (1999) 2: 201 205 Original article 1999 by International and Japanese Gastric Cancer Associations Perigastric lymph node metastases in gastric cancer: comparison of different staging systems
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only.
 The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
A study on clinicopathological features and prognostic factors of patients with upper gastric cancer and middle and lower gastric cancer.
 Biomedical Research 2018; 29 (2): 365-370 ISSN 0970-938X www.biomedres.info A study on clinicopathological features and prognostic factors of patients with upper gastric cancer and middle and lower gastric
Biomedical Research 2018; 29 (2): 365-370 ISSN 0970-938X www.biomedres.info A study on clinicopathological features and prognostic factors of patients with upper gastric cancer and middle and lower gastric
Gastric Cancer Histopathology Reporting Proforma
 Gastric Cancer Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given name(s) Date of birth Sex Male Female Intersex/indeterminate
Gastric Cancer Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given name(s) Date of birth Sex Male Female Intersex/indeterminate
Gastric Cancer in a Young Postpartum Female. Kings County Hospital Center SUNY Downstate Case Conference May 24, 2012
 Gastric Cancer in a Young Postpartum Female Kings County Hospital Center SUNY Downstate Case Conference May 24, 2012 Case HPI: 31 yo F, G5P3, 3 weeks s/p C-section, with gastric outlet obstruction. Pt
Gastric Cancer in a Young Postpartum Female Kings County Hospital Center SUNY Downstate Case Conference May 24, 2012 Case HPI: 31 yo F, G5P3, 3 weeks s/p C-section, with gastric outlet obstruction. Pt
COLON AND RECTAL CANCER
 No disclosures COLON AND RECTAL CANCER Mark Sun, MD Clinical Assistant Professor of Surgery University of Minnesota Colon and Rectal Cancer Statistics Overall Incidence 2016 134,490 new cases 8.0% of all
No disclosures COLON AND RECTAL CANCER Mark Sun, MD Clinical Assistant Professor of Surgery University of Minnesota Colon and Rectal Cancer Statistics Overall Incidence 2016 134,490 new cases 8.0% of all
Outcome after emergency surgery in patients with a free perforation caused by gastric cancer
 experimental and therapeutic medicine 1: 199-203, 2010 199 Outcome after emergency surgery in patients with a free perforation caused by gastric cancer Hironori Tsujimoto 1, Shuichi Hiraki 1, Naoko Sakamoto
experimental and therapeutic medicine 1: 199-203, 2010 199 Outcome after emergency surgery in patients with a free perforation caused by gastric cancer Hironori Tsujimoto 1, Shuichi Hiraki 1, Naoko Sakamoto
When to Integrate Surgery for Metatstatic Urothelial Cancers
 When to Integrate Surgery for Metatstatic Urothelial Cancers Wade J. Sexton, M.D. Senior Member and Professor Department of Genitourinary Oncology Moffitt Cancer Center Case Presentation #1 67 yo male
When to Integrate Surgery for Metatstatic Urothelial Cancers Wade J. Sexton, M.D. Senior Member and Professor Department of Genitourinary Oncology Moffitt Cancer Center Case Presentation #1 67 yo male
National Oesophago-Gastric Cancer Audit New Patient Registration sheet Patients with Oesophageal High Grade Glandular Dysplasia
 National Oesophago-Gastric Cancer Audit New Patient Registration sheet Patients with Oesophageal High Grade Glandular Dysplasia Patient Details Surname: NHS number: Forename: Postcode: Sex: Male Female
National Oesophago-Gastric Cancer Audit New Patient Registration sheet Patients with Oesophageal High Grade Glandular Dysplasia Patient Details Surname: NHS number: Forename: Postcode: Sex: Male Female
WHAT SHOULD WE DO WITH TUMOUR BUDDING IN EARLY COLORECTAL CANCER?
 CANCER STAGING TNM and prognosis in CRC WHAT SHOULD WE DO WITH TUMOUR BUDDING IN EARLY COLORECTAL CANCER? Alessandro Lugli, MD Institute of Pathology University of Bern Switzerland Maastricht, June 19
CANCER STAGING TNM and prognosis in CRC WHAT SHOULD WE DO WITH TUMOUR BUDDING IN EARLY COLORECTAL CANCER? Alessandro Lugli, MD Institute of Pathology University of Bern Switzerland Maastricht, June 19
Efficacy of prophylactic splenectomy for proximal advanced gastric cancer invading greater curvature
 Ohkura et al. World Journal of Surgical Oncology (2017) 15:106 DOI 10.1186/s12957-017-1173-9 RESEARCH Open Access Efficacy of prophylactic splenectomy for proximal advanced gastric cancer invading greater
Ohkura et al. World Journal of Surgical Oncology (2017) 15:106 DOI 10.1186/s12957-017-1173-9 RESEARCH Open Access Efficacy of prophylactic splenectomy for proximal advanced gastric cancer invading greater
Printed by Hadi Ranjkeshzadeh on 11/12/2010 4:40:23 PM. For personal use only. Not approved for distribution. Copyright 2010 National Comprehensive
 Discussion Categories of Evidence and Consensus Category 1: The recommendation is based on high-level evidence (e.g. randomized controlled trials) and there is uniform consensus. Category 2A: The recommendation
Discussion Categories of Evidence and Consensus Category 1: The recommendation is based on high-level evidence (e.g. randomized controlled trials) and there is uniform consensus. Category 2A: The recommendation
Xiang Hu*, Liang Cao*, Yi Yu. Introduction
 Original Article Prognostic prediction in gastric cancer patients without serosal invasion: comparative study between UICC 7 th edition and JCGS 13 th edition N-classification systems Xiang Hu*, Liang
Original Article Prognostic prediction in gastric cancer patients without serosal invasion: comparative study between UICC 7 th edition and JCGS 13 th edition N-classification systems Xiang Hu*, Liang
CASE DISCUSSION ON GASTRIC CANCER BASED ON ESMO GUIDELINES
 ESMO Preceptorship GI Tumours Singapore 20-22 nd October CASE DISCUSSION ON GASTRIC CANCER BASED ON ESMO GUIDELINES Professor. J-Y. Douillard MD PhD ESMO Chief Medical Officer CLINICAL PRACTICE GUIDELINES
ESMO Preceptorship GI Tumours Singapore 20-22 nd October CASE DISCUSSION ON GASTRIC CANCER BASED ON ESMO GUIDELINES Professor. J-Y. Douillard MD PhD ESMO Chief Medical Officer CLINICAL PRACTICE GUIDELINES
OESOPHAGO-GASTRIC CANCER 2016
 SOUTH EAST SCOTLAND CANCER NETWORK PROSPECTIVE CANCER AUDIT OESOPHAGO-GASTRIC CANCER 2016 COMPARATIVE AUDIT REPORT Mr Peter Lamb SCAN Lead Upper GI Cancer Clinician Dr Jonathan Fletcher, Consultant Physician,
SOUTH EAST SCOTLAND CANCER NETWORK PROSPECTIVE CANCER AUDIT OESOPHAGO-GASTRIC CANCER 2016 COMPARATIVE AUDIT REPORT Mr Peter Lamb SCAN Lead Upper GI Cancer Clinician Dr Jonathan Fletcher, Consultant Physician,
How many lymph nodes are enough? defining the extent of lymph node dissection in stage I III gastric cancer using the National Cancer Database
 Original Article How many lymph nodes are enough? defining the extent of lymph node dissection in stage I III gastric cancer using the National Cancer Database Karna Sura, Hong Ye, Charles C. Vu, John
Original Article How many lymph nodes are enough? defining the extent of lymph node dissection in stage I III gastric cancer using the National Cancer Database Karna Sura, Hong Ye, Charles C. Vu, John
Case Scenario 1. The patient has now completed his neoadjuvant chemoradiation and has been cleared for surgery.
 Case Scenario 1 July 10, 2010 A 67-year-old male with squamous cell carcinoma of the mid thoracic esophagus presents for surgical resection. The patient has completed preoperative chemoradiation. This
Case Scenario 1 July 10, 2010 A 67-year-old male with squamous cell carcinoma of the mid thoracic esophagus presents for surgical resection. The patient has completed preoperative chemoradiation. This
Surgical Management of Gastroesophageal Cancer in China
 Surgical Management of Gastroesophageal Cancer in China Yihong SUN, M.D., Ph.D., FRCS, Fudan University General Surgery Research Institute of Fudan University 01/14/2017; Detriot Disclosure I have no relevant
Surgical Management of Gastroesophageal Cancer in China Yihong SUN, M.D., Ph.D., FRCS, Fudan University General Surgery Research Institute of Fudan University 01/14/2017; Detriot Disclosure I have no relevant
Impact of infectious complications on gastric cancer recurrence
 Gastric Cancer (2015) 18:368 374 DOI 10.1007/s10120-014-0361-3 ORIGINAL ARTICLE Impact of infectious complications on gastric cancer recurrence Tsutomu Hayashi Takaki Yoshikawa Toru Aoyama Shinichi Hasegawa
Gastric Cancer (2015) 18:368 374 DOI 10.1007/s10120-014-0361-3 ORIGINAL ARTICLE Impact of infectious complications on gastric cancer recurrence Tsutomu Hayashi Takaki Yoshikawa Toru Aoyama Shinichi Hasegawa
Chirurgie beim oligo-metastatischen NSCLC
 24. Ärzte-Fortbildungskurs in Klinischer Onkologie 20.-22. Februar 2014, Kantonsspital St. Gallen Chirurgie beim oligo-metastatischen NSCLC Prof. Dr. med. Walter Weder Klinikdirektor Thoraxchirurgie, UniversitätsSpital
24. Ärzte-Fortbildungskurs in Klinischer Onkologie 20.-22. Februar 2014, Kantonsspital St. Gallen Chirurgie beim oligo-metastatischen NSCLC Prof. Dr. med. Walter Weder Klinikdirektor Thoraxchirurgie, UniversitätsSpital
Chapter 2: Initial treatment for endometrial cancer (including histologic variant type)
") Chapter 2: Initial treatment for endometrial cancer (including histologic variant type) CQ01 Which surgical techniques for hysterectomy are recommended for patients considered to be stage I preoperatively?
Chapter 2: Initial treatment for endometrial cancer (including histologic variant type) CQ01 Which surgical techniques for hysterectomy are recommended for patients considered to be stage I preoperatively?
Management of Esophageal Cancer: Evidence Based Review of Current Guidelines. Madhuri Rao, MD PGY-5 SUNY Downstate Medical Center
 Management of Esophageal Cancer: Evidence Based Review of Current Guidelines Madhuri Rao, MD PGY-5 SUNY Downstate Medical Center Case Presentation 68 y/o male PMH: NIDDM, HTN, hyperlipidemia, CAD s/p stents,
Management of Esophageal Cancer: Evidence Based Review of Current Guidelines Madhuri Rao, MD PGY-5 SUNY Downstate Medical Center Case Presentation 68 y/o male PMH: NIDDM, HTN, hyperlipidemia, CAD s/p stents,
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Adenocarcinoma, pancreatic ductal, laparoscopic distal pancreatectomy for, 61 Adrenal cortical carcinoma, laparoscopic adrenalectomy for, 114
Note: Page numbers of article titles are in boldface type. A Adenocarcinoma, pancreatic ductal, laparoscopic distal pancreatectomy for, 61 Adrenal cortical carcinoma, laparoscopic adrenalectomy for, 114
Utility of the Proximal Margin Frozen Section for Resection of Gastric Adenocarcinoma: A 7-Institution Study of the US Gastric Cancer Collaborative
 Ann Surg Oncol (2014) 21:4202 4210 DOI 10.1245/s10434-014-3834-z ORIGINAL ARTICLE GASTROINTESTINAL ONCOLOGY Utility of the Proximal Margin Frozen Section for Resection of Gastric Adenocarcinoma: A 7-Institution
Ann Surg Oncol (2014) 21:4202 4210 DOI 10.1245/s10434-014-3834-z ORIGINAL ARTICLE GASTROINTESTINAL ONCOLOGY Utility of the Proximal Margin Frozen Section for Resection of Gastric Adenocarcinoma: A 7-Institution
The detection rate of early gastric cancer has been increasing owing to advances in
 Focused Issue of This Month Sung Hoon Noh, MD, ph.d Department of Surgery, Yonsei University College of Medicine E - mail : sunghoonn@yuhs.ac J Korean Med Assoc 2010; 53(4): 306-310 Abstract The detection
Focused Issue of This Month Sung Hoon Noh, MD, ph.d Department of Surgery, Yonsei University College of Medicine E - mail : sunghoonn@yuhs.ac J Korean Med Assoc 2010; 53(4): 306-310 Abstract The detection
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal drainage, after hepatic resection, 159 160 Ablation, radiofrequency, for hepatocellular carcinoma, 160 161 Adenocarcinoma, pancreatic.
Index Note: Page numbers of article titles are in boldface type. A Abdominal drainage, after hepatic resection, 159 160 Ablation, radiofrequency, for hepatocellular carcinoma, 160 161 Adenocarcinoma, pancreatic.
Summary of the study protocol of the FLOT3-Study
 Summary of the study protocol of the FLOT3-Study EudraCT no. 2007-005143-17 Protocol Code: S396 Title A Prospective Multicenter Study With 5-FU, Leucovorin, Oxaliplatin and Docetaxel (FLOT) in Patients
Summary of the study protocol of the FLOT3-Study EudraCT no. 2007-005143-17 Protocol Code: S396 Title A Prospective Multicenter Study With 5-FU, Leucovorin, Oxaliplatin and Docetaxel (FLOT) in Patients
Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with pancreatic
 Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with pancreatic cancer Section AA Cancer Centre Referrals In the absence of metastatic
Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with pancreatic cancer Section AA Cancer Centre Referrals In the absence of metastatic
Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy
 Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy Authors: Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments 1.1 Cancer reporting: Biopsies
Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy Authors: Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments 1.1 Cancer reporting: Biopsies
Impact of upfront randomization for postoperative treatment on quality of surgery in the CRITICS gastric cancer trial
 Gastric Cancer (219) 22:369 376 https://doi.org/1.7/s112-18-875-1 ORIGINAL ARTICLE Impact of upfront randomization for postoperative treatment on quality of surgery in the CRITICS gastric cancer trial
Gastric Cancer (219) 22:369 376 https://doi.org/1.7/s112-18-875-1 ORIGINAL ARTICLE Impact of upfront randomization for postoperative treatment on quality of surgery in the CRITICS gastric cancer trial
Gastric Cancer Staging AJCC eighth edition. Duncan McLeod Westmead Hospital, NSW
 Gastric Cancer Staging AJCC eighth edition Duncan McLeod Westmead Hospital, NSW Summary of changes New clinical stage prognostic groups, ctnm Postneoadjuvant therapy pathologic stage groupings, yptnm -
Gastric Cancer Staging AJCC eighth edition Duncan McLeod Westmead Hospital, NSW Summary of changes New clinical stage prognostic groups, ctnm Postneoadjuvant therapy pathologic stage groupings, yptnm -
Clinical Study Impact of the Number of Dissected Lymph Nodes on Survival for Gastric Cancer after Distal Subtotal Gastrectomy
 Gastroenterology Research and Practice Volume 2011, Article ID 476014, 7 pages doi:10.1155/2011/476014 Clinical Study Impact of the Number of Dissected Lymph Nodes on Survival for Gastric Cancer after
Gastroenterology Research and Practice Volume 2011, Article ID 476014, 7 pages doi:10.1155/2011/476014 Clinical Study Impact of the Number of Dissected Lymph Nodes on Survival for Gastric Cancer after
Tumours of the Oesophagus & Gastro-Oesophageal Junction Histopathology Reporting Proforma
 Tumours of the Oesophagus & Gastro-Oesophageal Junction Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given
Tumours of the Oesophagus & Gastro-Oesophageal Junction Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given
Esophageal Cancer. Wesley A. Papenfuss MD FACS Surgical Oncology Aurora Cancer Care. David Demos MD Thoracic Surgery Aurora Cancer Care
 Esophageal Cancer Wesley A. Papenfuss MD FACS Surgical Oncology Aurora Cancer Care David Demos MD Thoracic Surgery Aurora Cancer Care No Disclosures Learning Objectives Review the classification scheme
Esophageal Cancer Wesley A. Papenfuss MD FACS Surgical Oncology Aurora Cancer Care David Demos MD Thoracic Surgery Aurora Cancer Care No Disclosures Learning Objectives Review the classification scheme
Surgical strategies in esophageal cancer
 Gastro-Conference Berlin 2005 October 1-2, 2005 Surgical strategies in esophageal cancer J. Rüdiger Siewert Department of Surgery, Klinikum rechts der Isar Technische Universität München Esophageal Cancer
Gastro-Conference Berlin 2005 October 1-2, 2005 Surgical strategies in esophageal cancer J. Rüdiger Siewert Department of Surgery, Klinikum rechts der Isar Technische Universität München Esophageal Cancer
How much colon should be resected?
 Colon Cancer Surgical Standard of Care and Operative Techniques Madhulika G. Varma MD Professor and Chief Section of Colorectal Surgery University of California, San Francisco How much colon should be
Colon Cancer Surgical Standard of Care and Operative Techniques Madhulika G. Varma MD Professor and Chief Section of Colorectal Surgery University of California, San Francisco How much colon should be
Resectable locally advanced oesophagogastric cancer
 Resectable locally advanced oesophagogastric cancer Clinical Case Discussion Florian Lordick University Cancer Center Leipzig University Clinic Leipzig Leipzig, Germany esmo.org DISCLOSURES Honoraria for
Resectable locally advanced oesophagogastric cancer Clinical Case Discussion Florian Lordick University Cancer Center Leipzig University Clinic Leipzig Leipzig, Germany esmo.org DISCLOSURES Honoraria for
How the ANZGOSA audit can benefit your practice: a look at GIST surgery from an Australian and NZ perspective. Aravind Suppiah; Sarah K.
 How the ANZGOSA audit can benefit your practice: a look at GIST surgery from an Australian and NZ perspective Aravind Suppiah; Sarah K. Thompson ANZGOSA database Commenced 2010; 1469 cases (2002 2014)
How the ANZGOSA audit can benefit your practice: a look at GIST surgery from an Australian and NZ perspective Aravind Suppiah; Sarah K. Thompson ANZGOSA database Commenced 2010; 1469 cases (2002 2014)
Case Scenario year-old white male presented to personal physician with dyspepsia with reflux.
 Case Scenario 1 57-year-old white male presented to personal physician with dyspepsia with reflux. 7/12 EGD: In the gastroesophageal junction we found an exophytic tumor. The tumor occupies approximately
Case Scenario 1 57-year-old white male presented to personal physician with dyspepsia with reflux. 7/12 EGD: In the gastroesophageal junction we found an exophytic tumor. The tumor occupies approximately
Minimally Invasive Esophagectomy- Valuable. Jayer Chung, MD University of Colorado Health Sciences Center December 11, 2006
 Minimally Invasive Esophagectomy- Valuable Jayer Chung, MD University of Colorado Health Sciences Center December 11, 2006 Overview Esophageal carcinoma What is minimally invasive esophagectomy (MIE)?
Minimally Invasive Esophagectomy- Valuable Jayer Chung, MD University of Colorado Health Sciences Center December 11, 2006 Overview Esophageal carcinoma What is minimally invasive esophagectomy (MIE)?
GASTRIC CANCER RANDOMIZED CONTROLLED TRIAL ON D2 LINPHADENECTOMY VS STANDARD D1 LINPHADENECTOMY
 GASTRIC CANCER RANDOMIZED CONTROLLED TRIAL ON D2 LINPHADENECTOMY VS STANDARD D1 LINPHADENECTOMY Maurizio Degiuli, MD Coordinator of the IGCSG (Italian Gastric Cancer Study Group) Antonio Ponti, MD MPH
GASTRIC CANCER RANDOMIZED CONTROLLED TRIAL ON D2 LINPHADENECTOMY VS STANDARD D1 LINPHADENECTOMY Maurizio Degiuli, MD Coordinator of the IGCSG (Italian Gastric Cancer Study Group) Antonio Ponti, MD MPH
Clinicopathological Characteristics and Outcome Indicators of Stage II Gastric Cancer According to the Japanese Classification of Gastric Cancer
 Clinicopathological Characteristics and Outcome Indicators of Stage II Gastric Cancer According to the Japanese Classification of Gastric Cancer HITOSHI OJIMA 1, KEN-ICHIRO ARAKI 1, TOSHIHIDE KATO 1, KAORI
Clinicopathological Characteristics and Outcome Indicators of Stage II Gastric Cancer According to the Japanese Classification of Gastric Cancer HITOSHI OJIMA 1, KEN-ICHIRO ARAKI 1, TOSHIHIDE KATO 1, KAORI
Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016. Background
 Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016 Background Mostly adenocarcinoma (scc possible, but treated like anal cancer) 39, 220 cases annually Primary treatment: surgery
Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016 Background Mostly adenocarcinoma (scc possible, but treated like anal cancer) 39, 220 cases annually Primary treatment: surgery
A Proposed Strategy for Treatment of Superficial Carcinoma. in the Thoracic Esophagus Based on an Analysis. of Lymph Node Metastasis
 Kitakanto Med J 2002 ; 52 : 189-193 189 A Proposed Strategy for Treatment of Superficial Carcinoma in the Thoracic Esophagus Based on an Analysis of Lymph Node Metastasis Susumu Kawate,' Susumu Ohwada,'
Kitakanto Med J 2002 ; 52 : 189-193 189 A Proposed Strategy for Treatment of Superficial Carcinoma in the Thoracic Esophagus Based on an Analysis of Lymph Node Metastasis Susumu Kawate,' Susumu Ohwada,'
Treatment of oligometastatic NSCLC
 Treatment of oligometastatic NSCLC Jarosław Kużdżał Department of Thoracic Surgery Jagiellonian University Collegium Medicum, John Paul II Hospital, Cracow New idea? 14 NSCLC patients with solitary extrathoracic
Treatment of oligometastatic NSCLC Jarosław Kużdżał Department of Thoracic Surgery Jagiellonian University Collegium Medicum, John Paul II Hospital, Cracow New idea? 14 NSCLC patients with solitary extrathoracic
MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER
 10 MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER Recommendations from the EAU Working Party on Muscle Invasive and Metastatic Bladder Cancer G. Jakse (chairman), F. Algaba, S. Fossa, A. Stenzl, C. Sternberg
10 MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER Recommendations from the EAU Working Party on Muscle Invasive and Metastatic Bladder Cancer G. Jakse (chairman), F. Algaba, S. Fossa, A. Stenzl, C. Sternberg
Outcomes of Abdominal Total Gastrectomy for Type II and III Gastroesophageal Junction Tumors: Single Center s Experience in Korea
 J Gastric Cancer 2012;12(1):36-42 http://dx.doi.org/10.5230/jgc.2012.12.1.36 Original Article Outcomes of Abdominal Total Gastrectomy for Type II and III Gastroesophageal Junction Tumors: Single Center
J Gastric Cancer 2012;12(1):36-42 http://dx.doi.org/10.5230/jgc.2012.12.1.36 Original Article Outcomes of Abdominal Total Gastrectomy for Type II and III Gastroesophageal Junction Tumors: Single Center
General introduction and outline of thesis
 General introduction and outline of thesis General introduction and outline of thesis 11 GENERAL INTRODUCTION AND OUTLINE OF THESIS The incidence of esophageal cancer is increasing in the western world.
General introduction and outline of thesis General introduction and outline of thesis 11 GENERAL INTRODUCTION AND OUTLINE OF THESIS The incidence of esophageal cancer is increasing in the western world.
The CROSS road in neoadjuvant therapy for esophageal cancer: long-term results of CROSS trial
 Editorial The CROSS road in neoadjuvant therapy for esophageal cancer: long-term results of CROSS trial Ian Wong, Simon Law Division of Esophageal and Upper Gastrointestinal Surgery, Department of Surgery,
Editorial The CROSS road in neoadjuvant therapy for esophageal cancer: long-term results of CROSS trial Ian Wong, Simon Law Division of Esophageal and Upper Gastrointestinal Surgery, Department of Surgery,
1. Epidemiology of Esophageal Cancer 2. Operative Strategies 3. Minimally Invasive Esophagectomy 4. Video
 Minimally Invasive Esophagectomy Guilherme M Campos, MD, FACS Assistant Professor of Surgery Director G.I. Motility Center Director Bariatric Surgery Program University of California San Francisco ESOPHAGEAL
Minimally Invasive Esophagectomy Guilherme M Campos, MD, FACS Assistant Professor of Surgery Director G.I. Motility Center Director Bariatric Surgery Program University of California San Francisco ESOPHAGEAL
위 ESD 후내시경소견 성균관대학교의과대학내과이준행
 위 ESD 후내시경소견 성균관대학교의과대학내과이준행 문제의식 위궤양, 조기위암, 진행위암의내시경소견은배운다. 위암수술후소견은가끔배운다. 위암내시경시술후소견은배운적이없다. 관찰과조직검사에대한가이드라인이없다. ESD 후정상내시경소견 성균관대학교의과대학내과이준행 처음의뢰되었을때의사진 ESD M/D, 18mm, LP, RM (-), L/V (-) 추적내시경소견 2
위 ESD 후내시경소견 성균관대학교의과대학내과이준행 문제의식 위궤양, 조기위암, 진행위암의내시경소견은배운다. 위암수술후소견은가끔배운다. 위암내시경시술후소견은배운적이없다. 관찰과조직검사에대한가이드라인이없다. ESD 후정상내시경소견 성균관대학교의과대학내과이준행 처음의뢰되었을때의사진 ESD M/D, 18mm, LP, RM (-), L/V (-) 추적내시경소견 2
GASTRIC CANCER. Joyce Au SUNY Downstate Grand Rounds July 11, 2013
 GASTRIC CANCER Joyce Au SUNY Downstate Grand Rounds July 11, 2013 xxm with gastric adenocarcinoma on biopsy of antral lesion on EGD at outside hospital PMH: residual schizophrenia, HTN PSH: exploratory
GASTRIC CANCER Joyce Au SUNY Downstate Grand Rounds July 11, 2013 xxm with gastric adenocarcinoma on biopsy of antral lesion on EGD at outside hospital PMH: residual schizophrenia, HTN PSH: exploratory
Determining the optimal number of lymph nodes harvested during esophagectomy
 Original Article Determining the optimal number of lymph nodes harvested during esophagectomy Khaldoun Almhanna, Jill Weber, Ravi Shridhar, Sarah Hoffe, Jonathan Strosberg, Kenneth Meredith Department
Original Article Determining the optimal number of lymph nodes harvested during esophagectomy Khaldoun Almhanna, Jill Weber, Ravi Shridhar, Sarah Hoffe, Jonathan Strosberg, Kenneth Meredith Department
Gastroesophag Gastroesopha eal Junction Adenocarcinoma: What is the best adjuvant regimen? Michael G. G. H addock Haddock M.D.
 Gastroesophageal Junction Adenocarcinoma: What is the best adjuvant regimen? Michael G. Haddock M.D. Mayo Clinic Rochester, MN Locally Advanced GE Junction ACA CT S CT or CT S CT/RT Proposition Chemoradiation
Gastroesophageal Junction Adenocarcinoma: What is the best adjuvant regimen? Michael G. Haddock M.D. Mayo Clinic Rochester, MN Locally Advanced GE Junction ACA CT S CT or CT S CT/RT Proposition Chemoradiation
Adjuvant Chemotherapy for Rectal Cancer: Are we making progress?
 Adjuvant Chemotherapy for Rectal Cancer: Are we making progress? Hagen Kennecke, MD, MHA, FRCPC Division Of Medical Oncology British Columbia Cancer Agency October 25, 2008 Objectives Review milestones
Adjuvant Chemotherapy for Rectal Cancer: Are we making progress? Hagen Kennecke, MD, MHA, FRCPC Division Of Medical Oncology British Columbia Cancer Agency October 25, 2008 Objectives Review milestones
Gastric linitis plastica: which role for surgical resection?
 Gastric Cancer (2012) 15:56 60 DOI 10.1007/s10120-011-0063-z ORIGINAL ARTICLE Gastric linitis plastica: which role for surgical resection? Corrado Pedrazzani Daniele Marrelli Fabio Pacelli Maria Di Cosmo
Gastric Cancer (2012) 15:56 60 DOI 10.1007/s10120-011-0063-z ORIGINAL ARTICLE Gastric linitis plastica: which role for surgical resection? Corrado Pedrazzani Daniele Marrelli Fabio Pacelli Maria Di Cosmo
Retrospectively analysis of the pathology and prognosis of 131 cases of adenocarcinoma of the esophagogastric junction (Siewert type II/III)
") Original Article Retrospectively analysis of the pathology and prognosis of 131 cases of adenocarcinoma of the esophagogastric junction (Siewert type II/III) Zifeng Yang*, Junjiang Wang*, Deqing Wu, Jiabin
Original Article Retrospectively analysis of the pathology and prognosis of 131 cases of adenocarcinoma of the esophagogastric junction (Siewert type II/III) Zifeng Yang*, Junjiang Wang*, Deqing Wu, Jiabin
Surgical Management of Pancreatic Cancer
 I Congresso de Oncologia D Or July 5-6, 2013 Surgical Management of Pancreatic Cancer Michael A. Choti, MD, MBA, FACS Department of Surgery Johns Hopkins University School of Medicine, Baltimore, MD Estimated
I Congresso de Oncologia D Or July 5-6, 2013 Surgical Management of Pancreatic Cancer Michael A. Choti, MD, MBA, FACS Department of Surgery Johns Hopkins University School of Medicine, Baltimore, MD Estimated
Risk factors for lymph node metastasis in histologically poorly differentiated type early gastric cancer
 498 Original article Risk factors for lymph node metastasis in histologically poorly differentiated type early gastric cancer Authors C. Kunisaki 1, M. Takahashi 2, Y. Nagahori 3, T. Fukushima 3, H. Makino
498 Original article Risk factors for lymph node metastasis in histologically poorly differentiated type early gastric cancer Authors C. Kunisaki 1, M. Takahashi 2, Y. Nagahori 3, T. Fukushima 3, H. Makino
SMALL BOWEL ADENOCARCINOMA. Dr. C. Jeske
 SMALL BOWEL ADENOCARCINOMA Dr. C. Jeske Case presentation 54 year old female. Presents with OJ and weight loss. Abdominal examination only reveals a palpable gallbladder. ERCP reveals a circumferential
SMALL BOWEL ADENOCARCINOMA Dr. C. Jeske Case presentation 54 year old female. Presents with OJ and weight loss. Abdominal examination only reveals a palpable gallbladder. ERCP reveals a circumferential
Extended multi-organ resection for ct4 gastric carcinoma: A retrospective analysis
 Original Article Extended multi-organ resection for ct4 gastric carcinoma: A retrospective analysis 1. Longbin Xiao, 2. Mingzhe Li, 3. Fengfeng Xu, Department of General Surgery I, 4. Huishao Ye, Department
Original Article Extended multi-organ resection for ct4 gastric carcinoma: A retrospective analysis 1. Longbin Xiao, 2. Mingzhe Li, 3. Fengfeng Xu, Department of General Surgery I, 4. Huishao Ye, Department
gastric cancer; lymph node dissection;
 Yonago Acta Medica 18;61:175 181 Original Article Therapeutic Value of Lymph Node Dissection Along the Superior Mesenteric Vein and the Posterior Surface of the Pancreatic Head in Gastric Cancer Located
Yonago Acta Medica 18;61:175 181 Original Article Therapeutic Value of Lymph Node Dissection Along the Superior Mesenteric Vein and the Posterior Surface of the Pancreatic Head in Gastric Cancer Located
Quiz Adenocarcinoma of the distal stomach has been increasing in the last 20 years. a. True b. False
 Quiz 1 1. Which of the following are risk factors for esophagus cancer. a. Obesity b. Gastroesophageal reflux c. Smoking and Alcohol d. All of the above 2. Adenocarcinoma of the distal stomach has been
Quiz 1 1. Which of the following are risk factors for esophagus cancer. a. Obesity b. Gastroesophageal reflux c. Smoking and Alcohol d. All of the above 2. Adenocarcinoma of the distal stomach has been
MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER
 MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER (Text update March 2008) A. Stenzl (chairman), N.C. Cowan, M. De Santis, G. Jakse, M. Kuczyk, A.S. Merseburger, M.J. Ribal, A. Sherif, J.A. Witjes Introduction
MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER (Text update March 2008) A. Stenzl (chairman), N.C. Cowan, M. De Santis, G. Jakse, M. Kuczyk, A.S. Merseburger, M.J. Ribal, A. Sherif, J.A. Witjes Introduction
ESD for EGC with undifferentiated histology
 ESD for EGC with undifferentiated histology Jun Haeng Lee, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea Biopsy: M/D adenocarcinoma ESD: SRC >>
ESD for EGC with undifferentiated histology Jun Haeng Lee, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea Biopsy: M/D adenocarcinoma ESD: SRC >>
Theoretical therapeutic impact of lymph node dissection on adenocarcinoma and squamous cell carcinoma
 Gastric Cancer (2016) 19:143 149 DOI 10.1007/s10120-014-0439-y ORIGINAL ARTICLE Theoretical therapeutic impact of lymph node dissection on adenocarcinoma and squamous cell carcinoma of the esophagogastric
Gastric Cancer (2016) 19:143 149 DOI 10.1007/s10120-014-0439-y ORIGINAL ARTICLE Theoretical therapeutic impact of lymph node dissection on adenocarcinoma and squamous cell carcinoma of the esophagogastric
Evidence tabel stadiering
 Evidence tabel stadiering Auteurs, T stage Syst Reviews Kwee, 2007 Systematic review Studies included up to aug 2006 Kelly, 2001 Systematic review Studies included from 1991-1996 steekproefgrootte) Included
Evidence tabel stadiering Auteurs, T stage Syst Reviews Kwee, 2007 Systematic review Studies included up to aug 2006 Kelly, 2001 Systematic review Studies included from 1991-1996 steekproefgrootte) Included
Is Hepatic Resection Needed in the Patients with Peritoneal Side T2 Gallbladder Cancer?
 Is Hepatic Resection Needed in the Patients with Peritoneal Side T2 Gallbladder Cancer? Lee H, Park JY, Youn S, Kwon W, Heo JS, Choi SH, Choi DW Department of Surgery, Samsung Medical Center Sungkyunkwan
Is Hepatic Resection Needed in the Patients with Peritoneal Side T2 Gallbladder Cancer? Lee H, Park JY, Youn S, Kwon W, Heo JS, Choi SH, Choi DW Department of Surgery, Samsung Medical Center Sungkyunkwan
Minimally Invasive Esophagectomy
 Minimally Invasive Esophagectomy M A R K B E R R Y, M D A S S O C I AT E P R O F E S S O R D E PA R T M E N T OF C A R D I O T H O R A C I C S U R G E R Y S TA N F O R D U N I V E R S I T Y S E P T E M
Minimally Invasive Esophagectomy M A R K B E R R Y, M D A S S O C I AT E P R O F E S S O R D E PA R T M E N T OF C A R D I O T H O R A C I C S U R G E R Y S TA N F O R D U N I V E R S I T Y S E P T E M