Optimization of antibodies, selection, protocols and controls Breast tumours
|
|
|
- Meryl Walters
- 6 years ago
- Views:
Transcription
1 Optimization of antibodies, selection, protocols and controls Breast tumours Søren Nielsen Project coordinator & Scheme Manager NordiQC Aalborg University Hospital, Denmark
2 Breast panel: GCDFP-15 Mammaglobin Gata 3 Smooth MHCM ASMA (p63) E-cadherin p120 ER PR HER-2 Is it primary breast? Is it invasive? Is it lobular or ductal? Which teraphy?
3 Breast panel: GCDFP-15 Mammaglobin Gata 3 Smooth MHCM ASMA (p63) E-cadherin p120 ER PR HER-2 Is it primary breast? Is it invasive? Is it lobular or ductal? Which teraphy?
4 Generel App laboratories in total > 70 countries Breast HER-2 ISH
5 Focus: Appropriate technical quality; signal-to-noise, morphology etc Appropriate analytical sensitivity and specificity indicated by concordance of ER status in the included tumours to reference



6 Uterine cervix Tonsil Breast carc. high Breast carc. low Breast carc. negative

7
8 strogen receptor; ass rate influenced by participation New participants Old participants Run B10, % (n=61) 71% (n=134) Run B15, % (n=54) 86% (n=208) Run B19, % (n=86) 73% (n=259)


9 Estrogen receptor; Pass rate influenced by protocol harmonization 2003 B B15 Titre range / average titre 1: / 1:125 1: / 1:90 HIER by in-house buffer 88% 6% HIER by high ph 70% 94% Polymer/multimer kit 56% 93% Fully automated system 6% 59%


10



11 HIER alk. ph 2- & 3-step kits Carefully calib. Uterine cervix; all epithelial cells Tonsil; scattered T-cells




 Insufficient")



12 Estrogen receptor; 85% Weak / False negative 10% False positive 5% Impaired morphology, etc Suf. Ins. Too low titre (EP1, SP1 conc.) Insufficient HIER, Clone 1D5 Clone 6F11 by HIER at high ph, 3-step pol. (not observed on VMS) Clone 1D5 at high titre, Biotin-based kits, HIER in pressure cooker


13 Breast panel: Estrogen Receptor Basic protocol settings for an optimal staining result (NQC) Retrieval Titre Detection RTU Detection mab 1D5 HIER High 1: & 3-step Dako 2- & 3-step mab 6F11* HIER Ci, High 1: & 3-step Leica 3-step rmab EP1 HIER High 1: & 3-step Dako 2- & 3-step rmab SP1 HIER High 1: & 3-step Ventana 2- & 3-step * Efficient HIER, high conc., 3-step pol. & low stringent washing can give aberrant nuclear staining Not seen on Ventana stainer, rarely on Autostainer and most commonly on Bond stainer. Use uterine cervix and tonsil to verify level of sensitivity and specificity;
14 Focus: Appropriate technical quality; signal-to-noise, morphology etc Appropriate analytical sensitivity and specificity indicated by concordance of PR status in the included tumours to reference



15 Uterine cervix Can vary. Tonsil Breast carc. high Breast carc. low Breast carc. negative
16


17




18 HIER alk. ph 2- & 3-step kits Carefully calib. Uterine cervix all columnar epith. cells, and majority of basal squam. epith. cells (can be neg. in some pts).




")


")
19 Progesterone receptor; 75% Weak / False negative 20% False positive 5% Impaired morphology, etc Tonsil Suf. Ins. Too low titre (16, PgR636) Insufficient HIER Clone SP2 and 1E2. 1E2 mainly by off-label protocol (ext. sensitivity) Clone 1A6, Biotin-based kits, HIER in pressure cooker
 1:100-800 2- & 3-step Dako 3-step mab PGR1294 HIER (High) 1:250 5.")
20 IHC Protocols and controls for Breast tumours Breast panel: Progesterone Receptor Basic protocol settings for an optimal staining result (NQC) Retrieval Titre Detection RTU Detection mab 16 HIER High 1: & 3-step Leica 3-step mab PGR636* HIER (High) 1: & 3-step Dako 3-step mab PGR1294 HIER (High) 1: & 3-step Dako 2-step rmab 1E2** HIER High - - Ventana 2-step * mab clone PGR636 has shown to be less successful on Ventana BenchMark Ultra ** rmab clone 1E2, RTU might provide aberrant false pos. result by 3-step protocols, reduced HIER and prolonged Ab incubation time compared to Ventana guidelines Use uterine cervix and tonsil to verify level of sensitivity and specificity;

21 Focus: Appropriate technical quality; signal-to-noise, morphology etc Appropriate analytical sensitivity and specificity indicated by concordance to FISH status and IHC level established by reference data in all the included tumours.


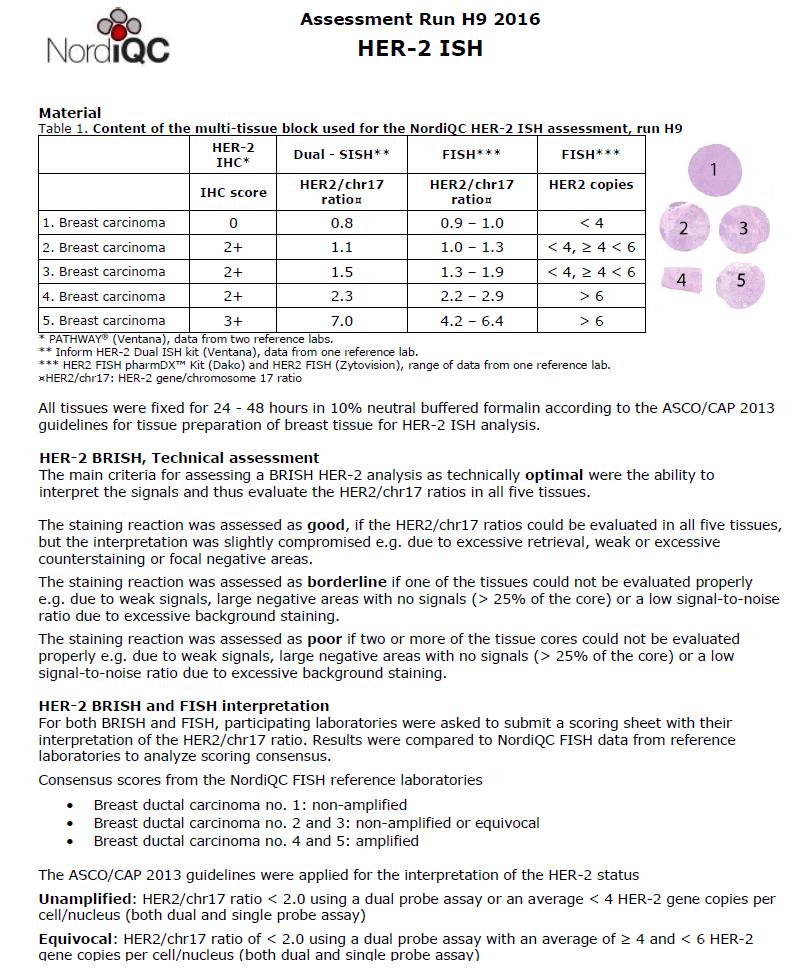
22 Material processed according to ASCO/CAP


23 > CK Optimal Ampl. 3+ Ampl. 2+ Unampl. 2+ Unampl. 0 Poor 10-20% HER2+ found in 2+ cat. Ampl. 3+ Ampl. 1+ Unampl. 1+ Unampl. 0 23


24 > CK Optimal Ampl. 3+ Ampl. 2+ Unampl. 2+ Unampl. 0 Poor Ampl. 3+ Ampl. 2+ Unampl. 3+ Unampl. 1 24

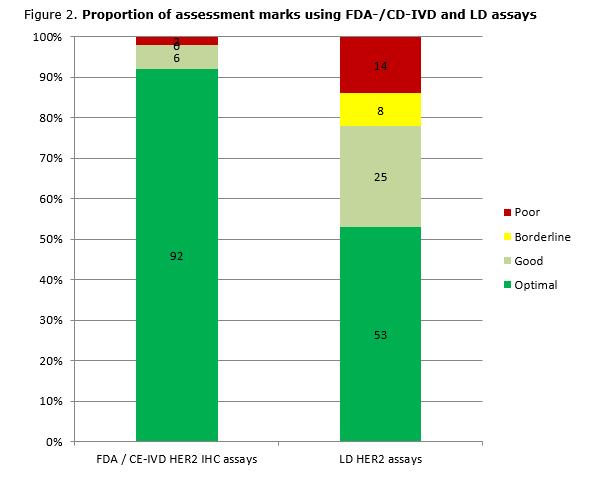
25 App 90 % of insuff. results are FN and seen both by FDA / CE-IVD kits and laboratory developed assays. FP results have virtually only been seen by laboratory developed assays. 25
 and/or too short incubation of primary & secondary Ab (<30M) Oracle, Leica: No single or combination of causes have been identified Laboratory developed")
26 Typical causes for insufficient results in the NordiQC HER2 IHC breast module: FDA / CE-IVD HER2 IHC kits: PATHWAY, Ventana: Too short HIER (<24M) and/or too short incubation of primary Ab (<12M) HercepTest, Dako: Too short HIER (<40M) and/or too short incubation of primary & secondary Ab (<30M) Oracle, Leica: No single or combination of causes have been identified Laboratory developed assays: Inappropriate titre of primary Ab, less successful primary Ab, insufficient HIER, etc.. 26

27 Control material for HER2 IHC: performace control / consistency Histology: 3+ tumour Cell lines: tumour 2+ Applicable for DIA & ref data comparing run-to-run


28 Control material for HER2 IHC: performace control / consistency Histocyte cell lines HER2: Horizon cell lines HER2 0,99 0,99 0,99 0,87 0,66 0,85 0,13 0,15 0,24 0,30 0,15 0,34 Pathway Oracle Herceptest Pathway Oracle HercepTest
29


30 CK7 ISH: ISH: Optimal Ampl. 3+ Ampl. 2+ Unampl. 2+ Unampl. 0 ISH: Good Increased need for additional ISH Ampl. 3+ Ampl. 2+ Unampl. 2+ Unampl
31 31

32 5% didn t return slides for BRISH due to technical errors. 32



33 Technically optimal results in the NordiQC HER2 ISH breast module: INFORM HER2 Dual ISH, Ventana ZytoDot 2C, ZytoVision HER2 black chr17 red HER2 green chr17 red U A 33
34 Typical causes for insufficient results in the NordiQC HER2 ISH breast module: FDA / CE-IVD HER2 BRISH (CISH/DDISH/etc) kits: INFORM HER2 Dual ISH, Ventana: Excessive proteolysis (>16M), HIER in CC1. DuoCISH pharmdx, Dako: Insufficient proteolysis, inappropriate handling of chromogen. ZytoDot 2C, ZytoVision: Excessive proteolysis. In 90% of insufficient results, no single or combination of causes could be identified 34



35 Technically insufficient results in the NordiQC HER2 ISH breast module: INFORM HER2 Dual ISH, Ventana HER2 black chr17 red Excessive protelysis U Neg areas >25% Silver precip. U 35

36 90% of ins. results used approriate protocol. 36


37 What is faint? Visible at 40X? What is weak? Visible at 10X? Up to 20-40% HER2 IHC tests are reflexed to ISH due to expanded criteria for 2+ (internal data)

38 From a technical point of view, it might be critical to change from a robust and relatively simple IHC assay to a less robust and complex test and simultanously more expensive test 38

39 HER2 Gene-Protein-Assay (Roche): HER2 IHC + DDISH no EQA data yet. 39


40 Slightly higher concordance regarding interpretation for FISH
41 Conclusions: 1. Pass rates for ER, PR and HER2 IHC are improved. Robust clones, high quality IHC systems. 2. CE-IVD labelled RTU assays / systems have shown superior performance compared to laboratory developed assays. 3. HER2 BRISH (DDISH/SISH/CISH) results have not been improved.
42 Breast panel: GCDFP-15 Mammaglobin Gata 3 Smooth MHCM ASMA (p63) E-cadherin p120 ER PR HER-2 Is it primary breast? Is it invasive? Is it lobular or ductal? Which teraphy?

43 IHC Protocols and controls for Breast tumours GCDFP15 / Mammaglobin reaction pattern A moderate to strong, distinct cytoplasmic staining reaction in scattered ductal epithelial cells and in apocrine metaplastic cells. Breast Skin Tonsil A moderate to strong, distinct cytoplasmic staining reaction of the majority of the epithelial cells of the eccrine sweat glands No staining reaction should be seen.


44 IHC Protocols and controls for Breast tumours GCDFP15 / Mammaglobin reaction pattern Antigen diffusion Carc. 4 Carc. 4 44


45 IHC Protocols and controls for Breast tumours Local diffusion


46 IHC Protocols and controls for Breast tumours GCDFP15 / Mammaglobin reaction pattern Carc. 1 - Mammaglobin Carc. 2 - Mammaglobin 46


47 IHC Protocols and controls for Breast tumours GCDFP15 / Mammaglobin reaction pattern Tandem application Carc. 3 - Mammaglobin Carc. 3 - GCDFP15 47

48 IHC Protocols and controls for Breast tumours Ins.: Omission of HIER and/or too low conc. RTU > Conc. (difficult to calibrate what is best control )

49 IHC Protocols and controls for Breast tumours



50 IHC Protocols and controls for Breast tumours Ins.: Too low/high conc. HIER and calibration mandatory for optimal results 50

51 IHC Protocols and controls for Breast tumours Breast panel: GCDFP15 & Mammaglobin Basic protocol settings for an optimal staining result (NQC) Retrieval Titre Detection RTU Detection mab 23A3 HIER High 1: step Dako 2- & 3-step mab D6 HIER High 1: step - - rmab EP1582Y HIER High 1: step Ventana 2- & 3-step mab HIER High 1: & 3-step Dako 2-step mab 31A5 HIER High - - Ventana 2-step rmab clone EP1582Y can show positive staining reaction in smooth muscle cells

52 IHC Protocols and controls for Breast tumours GATA3 reaction pattern ICAPCs Tonsil Kidney App. An at least weak nuclear staining reaction of the majority of T-cells in the T-zones in the tonsil. An at least moderate, distinct nuclear staining reaction of virtually all epithelial cells in collecting ducts and podocytes in glomeruli in the kidney. No staining reaction in epithelial cells should be seen.
. But also seen in other neoplasias Lobular carc. Urothelial carc. Leiomyosarcoma")
53 IHC Protocols and controls for Breast tumours Breast panel: GATA3 Basic protocol settings for an optimal staining result (NQC) Retrieval Titre Detection RTU Detection mab L HIER TE 1: & 3-step Ventana 2- & 3-step GATA3: Highly sensitive for Breast carcinomas (& Urothelial carcinoma). But also seen in other neoplasias Lobular carc. Urothelial carc. Leiomyosarcoma
54 Breast panel: GCDFP-15 Mammaglobin Gata 3 Smooth MHCM ASMA (p63) E-cadherin p120 ER PR HER-2 Is it primary breast? Is it invasive? Is it lobular or ductal? Which teraphy?

55 IHC Protocols and controls for Breast tumours SMH reaction pattern ICAPCs A weak to moderate, distinct cytoplasmic staining reaction in the follicular dendritic network of germinal centres. No staining should be seen in epithelial cells. Tonsil Appendix Breast A moderate to strong, distinct cytoplasmic staining reaction of all smooth muscle cells in muscularis propria and vessels. No staining in epithelium. A moderate to strong cytoplasmic staining reaction must be seen in myoepithelium. No staining reaction should be seen in luminal epithelial cells.

56 IHC Protocols and controls for Breast tumours mab clone SMMS-1 HIER in alk. ph HIER in alk. ph + proteolysis Insufficient HIER provided a too low sensitivity 56



57 IHC Protocols and controls for Breast tumours p63 / SMH p63 / SMH 57
58 IHC Protocols and controls for Breast tumours Breast panel: SMH Basic protocol settings for an optimal staining result (NQC) Retrieval Titre Detection RTU Detection mab SMMS1 HIER High 1: & 3-step Ventana 3-step rmab EPR5336 HIER High 1: step - -

59 IHC Protocols and controls for Breast tumours ASMA reaction pattern ICAPCs A moderate to strong, distinct cytoplasmic staining of the majority of the perisinusoidal cells in the liver. No staining should be seen in hepatocytes. Liver Appendix Tonsil A strong, distinct cytoplasmic staining of all the smooth muscle cells in the muscularis propria, lamina muscularis mucosae and myofibroblasts lining the crypts. A moderate to strong cytoplasmic staining must be seen in smooth muscle cells e.g. vessels No staining should be seen in lymphocytes and epithelial cells.

60 IHC Protocols and controls for Breast tumours
61 IHC Protocols and controls for Breast tumours

62 IHC Protocols and controls for Breast tumours


63 IHC Protocols and controls for Breast tumours



64 IHC Protocols and controls for Breast tumours AS Bond Ultra Protocol for clone depending on IHC stainer platform mab clone 1A4 (Dako*) Dako AS48 Leica Bond III VMS Ultra Titre 1: * / RTU 1: * 1: * Retrieval HIER TRS High HIER ER 2 None Detection 2- or 3-step 3-step 3-step

65 IHC Protocols and controls for Breast tumours Breast panel: ASMA Ventana BenchMark Basic protocol settings for an optimal staining result (NQC) Retrieval Titre Detection RTU Detection rmab EP188 P2 4M + CC1M 1:200 3-step OP + AMP - - ASMA: Left: EP188, VMS platform, combined retrieval OptiView + AMP Right: 1A4 Dako platform HIER EnVision FLEX


66 IHC Protocols and controls for Breast tumours
67 Breast panel: GCDFP-15 Mammaglobin Gata 3 Smooth MHCM ASMA (p63) E-cadherin p120 ER PR HER-2 Is it primary breast? Is it invasive? Is it lobular or ductal? Which teraphy?

68 IHC Protocols and controls for Breast tumours ECAD reaction pattern ICAPCs Liver Colon Tonsil An at least weak to moderate membranous staining reaction of virtually all the hepatocytes. A moderate to strong, distinct membranous staining reaction of virtually all the columnar epithelial cells in the colon / appendix. A moderate to strong, distinct membranous staining reaction of virtually all squamous epithelial cells. No staining reaction of the vast majority of lymphocytes.




69 IHC Protocols and controls for Breast tumours mab clones HECD-1 & NCH-38 most successful HIER 2 or 3-step mul/pol. mab clone 36 aberrant nuclear staining reaction rmab clone EP700y inferior signal-to-noise


70 IHC Protocols and controls for Breast tumours E-Cadherin Liver CSQI: Hepatocytes


71 IHC Protocols and controls for Breast tumours Lobular breast carcinoma mab clone HECD-1 or NCH-38 mab clone 36 Technical? Biology?

72 IHC Protocols and controls for Breast tumours mab 36B5 mab 36 Clone 36 reacts with cytoplasmic component Nuclear localization might occur due to B-Cat mutation (has to be confirmed and no data on breast tumours).







73 IHC Protocols and controls for Breast tumours NCH-38 vs EP700Y Colon - Kidney NCH-38 Colon - Kidney EP700Y Titre A Colon Kidney EP700Y Titre B

74 IHC Protocols and controls for Breast tumours ICAPCs Liver An at least weak to moderate membranous staining reaction of virtually all the hepatocytes. A moderate to strong pre-dominantly membranous staining reaction must be seen all epithelial cells of bile ducts. p120 Catenin Tonsil An at least weak to moderate membranous staining reaction of germinal centre macrophages and the follicular dendritic network. 74

75 IHC Protocols and controls for Breast tumours Ductal carc. p120 Catenin Lobular carc. 75
76 IHC Protocols and controls for Breast tumours Breast panel: E-Cadherin (& p120) Basic protocol settings for an optimal staining result (NQC) E-CAD Retrieval Titre Detection RTU Detection mab NCH-38 HIER High 1: & 3-step Dako 2- & 3-step mab HECD-1 HIER High 1: & 3-step - - mab 36B5 HIER High 1:50 2- & 3-step - - mab ECH-6 HIER High 1:100 2-step - - mab 36 HIER High - - Ventana 2-step* * Short incubation time 8-16 min. and 2-step multimer p120 Retrieval Titre Detection RTU Detection mab MRQ-5 HIER high 1: & 3-step - -
Breast cancer: Antibody selection, protocol optimzation controls and EQA
 Breast cancer: Antibody selection, protocol optimzation controls and EQA Workshop in Diagnostic Immunohistochemistry Oud St. Jan/ Old St. John Brugge (Bruges), Belgium June 13th 15nd 2018 Rasmus Røge,
Breast cancer: Antibody selection, protocol optimzation controls and EQA Workshop in Diagnostic Immunohistochemistry Oud St. Jan/ Old St. John Brugge (Bruges), Belgium June 13th 15nd 2018 Rasmus Røge,
External Quality Assessment of Breast Marker Analysis. NordiQC data
 External Quality Assessment of Breast Marker Analysis NordiQC data Søren Nielsen Scheme Manager NordiQC Aalborg University Hospital, Denmark Aalborg 12.06 2015 Markers assessed in NordiQC Predictive markers
External Quality Assessment of Breast Marker Analysis NordiQC data Søren Nielsen Scheme Manager NordiQC Aalborg University Hospital, Denmark Aalborg 12.06 2015 Markers assessed in NordiQC Predictive markers
SMH (Myosin, smooth muscle heavy chain)
") Material The slide to be stained for SMH comprised: Assessment Run 50 2017 SMH (Myosin, smooth muscle heavy chain) 1.Tonsil, 2. Esophagus, 3. Breast hyperplasia, 4. Breast ductal carcinoma in situ (DCIS),
Material The slide to be stained for SMH comprised: Assessment Run 50 2017 SMH (Myosin, smooth muscle heavy chain) 1.Tonsil, 2. Esophagus, 3. Breast hyperplasia, 4. Breast ductal carcinoma in situ (DCIS),
Assessment Run GATA3
 Assessment Run 44 2015 GATA3 Material The slide to be stained for GATA3 comprised: 1. Tonsil 2. Kidney, 3. Urothelial carcinoma, 4. Breast ductal carcinoma, 5. Colon adenocarcinoma All tissues were fixed
Assessment Run 44 2015 GATA3 Material The slide to be stained for GATA3 comprised: 1. Tonsil 2. Kidney, 3. Urothelial carcinoma, 4. Breast ductal carcinoma, 5. Colon adenocarcinoma All tissues were fixed
Assessment Run B HER-2 IHC. HER-2/chr17 ratio**
 Assessment Run B2 20 HER-2 IHC Material The slide to be stained for HER-2 comprised the following 5 tissues: IHC HER-2 Score* (0, +, 2+,3+) FISH HER-2/chr7 ratio**. Breast ductal carcinoma 0..3 2. Breast
Assessment Run B2 20 HER-2 IHC Material The slide to be stained for HER-2 comprised the following 5 tissues: IHC HER-2 Score* (0, +, 2+,3+) FISH HER-2/chr7 ratio**. Breast ductal carcinoma 0..3 2. Breast
Carcinoembryonic antigen (CEA)
") Assessment Run 37 2013 Carcinoembryonic antigen (CEA) Material The slide to be stained for CEA comprised: 1. Appendix, 2. Liver, 3-4. Colon adenocarcinoma, 5. Urothelial carcinoma All tissues were fixed
Assessment Run 37 2013 Carcinoembryonic antigen (CEA) Material The slide to be stained for CEA comprised: 1. Appendix, 2. Liver, 3-4. Colon adenocarcinoma, 5. Urothelial carcinoma All tissues were fixed
Assessment Run B HER2 IHC
 Assessment Run B26 208 HER2 IHC Material The slide to be stained for HER2 comprised the following 5 materials: IHC: HER2 Score* (0, +, 2+, 3+) FISH: HER2 gene/chr 7 ratio**. Breast carcinoma, no. 2+..3
Assessment Run B26 208 HER2 IHC Material The slide to be stained for HER2 comprised the following 5 materials: IHC: HER2 Score* (0, +, 2+, 3+) FISH: HER2 gene/chr 7 ratio**. Breast carcinoma, no. 2+..3
Estrogen receptor (ER)
") Assessment Run B7 204 Estrogen receptor (ER) Material The slide to be stained for ER comprised: No. Tissue ER-positivity* ER-intensity*. Uterine cervix 80-90% Moderate to strong 2. Breast carcinoma 0%
Assessment Run B7 204 Estrogen receptor (ER) Material The slide to be stained for ER comprised: No. Tissue ER-positivity* ER-intensity*. Uterine cervix 80-90% Moderate to strong 2. Breast carcinoma 0%
Assessment Run
 Assessment Run 50 2017 S100 Material The slide to be stained for S100 comprised: 1. Appendix, 2. Tonsil, 3. Schwannoma, 4-5. Malignant melanoma, 6. Colon adenocarcinoma. All tissues were fixed in 10% neutral
Assessment Run 50 2017 S100 Material The slide to be stained for S100 comprised: 1. Appendix, 2. Tonsil, 3. Schwannoma, 4-5. Malignant melanoma, 6. Colon adenocarcinoma. All tissues were fixed in 10% neutral
Estrogen receptor (ER)
") Material The slide to be stained for ER comprised: Assessment Run B26 2018 Estrogen receptor (ER) No. Tissue ER-positivity* ER-intensity* 1. Uterine cervix 80-90% Moderate to strong 2. Tonsil 1-5% Weak
Material The slide to be stained for ER comprised: Assessment Run B26 2018 Estrogen receptor (ER) No. Tissue ER-positivity* ER-intensity* 1. Uterine cervix 80-90% Moderate to strong 2. Tonsil 1-5% Weak
Assessment Run B HER2 IHC
 Assessment Run B24 2017 HER2 IHC Material The slide to be stained for HER2 comprised the following 5 materials: IHC: HER2 Score* (0, 1+, 2+, 3+) FISH: HER2 gene/chr 17 ratio** 1. Breast carcinoma, no.
Assessment Run B24 2017 HER2 IHC Material The slide to be stained for HER2 comprised the following 5 materials: IHC: HER2 Score* (0, 1+, 2+, 3+) FISH: HER2 gene/chr 17 ratio** 1. Breast carcinoma, no.
Assessment Run C1 2017
 Assessment Run C1 2017 PD-L1 The first assessment in this new NordiQC Companion module C1 focused on the accuracy of the PD-L1 IHC assays performed by the participating laboratories to identify patients
Assessment Run C1 2017 PD-L1 The first assessment in this new NordiQC Companion module C1 focused on the accuracy of the PD-L1 IHC assays performed by the participating laboratories to identify patients
Cytokeratin 19 (CK19)
") Assessment Run 34 202 Cytokeratin 9 (CK9) Material The slide to be stained for CK9 comprised:. Thyroid gland, 2. Appendix, 3. Esophagus, 4. Papillary thyroid carcinoma, 5 & 6. Pancreatic neuroendocrine
Assessment Run 34 202 Cytokeratin 9 (CK9) Material The slide to be stained for CK9 comprised:. Thyroid gland, 2. Appendix, 3. Esophagus, 4. Papillary thyroid carcinoma, 5 & 6. Pancreatic neuroendocrine
Estrogen receptor (ER)
") Material The slide to be stained for ER comprised: Assessment B25 208 Estrogen receptor (ER) No. Tissue ER-positivity* ER-intensity*. Uterine cervix 80-90% Moderate to strong 2. Tonsil < 2-5% Weak to strong
Material The slide to be stained for ER comprised: Assessment B25 208 Estrogen receptor (ER) No. Tissue ER-positivity* ER-intensity*. Uterine cervix 80-90% Moderate to strong 2. Tonsil < 2-5% Weak to strong
Assessment Run NKX3.1 (NKX3.1)
") Assessment Run 49 2017 NKX3.1 (NKX3.1) Material The slide to be stained for NKX3.1 comprised: 1. Testis 2. Appendix 3-4. Prostate adenocarcinoma 5. Prostate hyperplasia All tissues were fixed in 10% neutral
Assessment Run 49 2017 NKX3.1 (NKX3.1) Material The slide to be stained for NKX3.1 comprised: 1. Testis 2. Appendix 3-4. Prostate adenocarcinoma 5. Prostate hyperplasia All tissues were fixed in 10% neutral
Assessment Run C3 2018
 Assessment Run C3 2018 PD-L1 Amended version May 14 th 2018 The third assessment in NordiQC Companion module C3 focused on the accuracy of the PD-L1 IHC assays performed by the participating laboratories
Assessment Run C3 2018 PD-L1 Amended version May 14 th 2018 The third assessment in NordiQC Companion module C3 focused on the accuracy of the PD-L1 IHC assays performed by the participating laboratories
Thyroid transcription factor-1 (TTF1) Assessment run
 Assessment run") Thyroid transcription factor- (TTF) Assessment run 39 203 The slide to be stained for TTF comprised:. Thyroid gland, 2. Liver, 3. Normal lung, 4. Lung adenocarcinoma 5. Colon adenocarcinoma, 6 & 7. Lung
Thyroid transcription factor- (TTF) Assessment run 39 203 The slide to be stained for TTF comprised:. Thyroid gland, 2. Liver, 3. Normal lung, 4. Lung adenocarcinoma 5. Colon adenocarcinoma, 6 & 7. Lung
NordiQC External Quality Assurance in Immunohistochemistry
 NordiQC External Quality Assurance in Immunohistochemistry Mogens Vyberg Professor of Clinical Pathology Director of NordiQC Aalborg University Hospital, Aalborg, Denmark AALBORG (~ 200.000 inhabitants)
NordiQC External Quality Assurance in Immunohistochemistry Mogens Vyberg Professor of Clinical Pathology Director of NordiQC Aalborg University Hospital, Aalborg, Denmark AALBORG (~ 200.000 inhabitants)
Lung Anaplastic Lymphoma Kinase (lu-alk)
") Assessment Run 5 207 Lung Anaplastic Lymphoma Kinase (lu-alk) Material The slide to be stained for lu-alk comprised:. Appendix, 2. Tonsil, 3. Merkel cell carcinoma, 4. Anaplastic large cell lymphoma with
Assessment Run 5 207 Lung Anaplastic Lymphoma Kinase (lu-alk) Material The slide to be stained for lu-alk comprised:. Appendix, 2. Tonsil, 3. Merkel cell carcinoma, 4. Anaplastic large cell lymphoma with
Quality Assurance in Immunohistochemistry: Experiences from NordiQC
 Nordic immunohistochemical Quality Control 2 Quality Assurance in Immunohistochemistry: Experiences from NordiQC Prof. Mogens Vyberg NordiQC Institute of Pathology Aalborg University Hospital Aalborg,
Nordic immunohistochemical Quality Control 2 Quality Assurance in Immunohistochemistry: Experiences from NordiQC Prof. Mogens Vyberg NordiQC Institute of Pathology Aalborg University Hospital Aalborg,
10 years of NordiQC Why are 30% of labs still getting it wrong?
 Mogens Vyberg & Søren Nielsen NordiQC Institute of Pathology Aalborg University Hospital Aalborg, Denmark May 29th 2015 10 years of NordiQC Why are 30% of labs still getting it wrong? Nothing to declare
Mogens Vyberg & Søren Nielsen NordiQC Institute of Pathology Aalborg University Hospital Aalborg, Denmark May 29th 2015 10 years of NordiQC Why are 30% of labs still getting it wrong? Nothing to declare
The impact of proficiency testing on lab immunoassays
 The impact of proficiency testing on lab immunoassays Mogens Vyberg Professor of Clinical Pathology Director of NordiQC Aalborg University Hospital, Aalborg, Denmark Nordic Immunohistochemical Quality
The impact of proficiency testing on lab immunoassays Mogens Vyberg Professor of Clinical Pathology Director of NordiQC Aalborg University Hospital, Aalborg, Denmark Nordic Immunohistochemical Quality
Epithelial cell-cell adhesion molecule (Ep-CAM)
") Assessment Run 3 011 Epithelial cell-cell adhesion molecule (Ep-CAM) Material The slide to be stained for Ep-CAM comprised: 1. Appendix,. Kidney, 3. Adrenal gland, 4. Lung carcinoid, 5 & 6. Renal clear
Assessment Run 3 011 Epithelial cell-cell adhesion molecule (Ep-CAM) Material The slide to be stained for Ep-CAM comprised: 1. Appendix,. Kidney, 3. Adrenal gland, 4. Lung carcinoid, 5 & 6. Renal clear
Assessment Run CK19
 Assessment Run 29 200 CK9 The slide to be stained for CK9 comprised:. Appendix, 2. Thyroid gland, 3. Pancreas, 4. Ductal breast carcinoma, 5. Esophagus, 6. Papillary thyroid carcinoma. All tissues were
Assessment Run 29 200 CK9 The slide to be stained for CK9 comprised:. Appendix, 2. Thyroid gland, 3. Pancreas, 4. Ductal breast carcinoma, 5. Esophagus, 6. Papillary thyroid carcinoma. All tissues were
Sal-like protein 4 (SALL4)
") Assessment Run 43 205 Sal-like protein 4 (SALL4) The slide to be stained for SALL4 comprised:. Appendix, 2. Testis, 3. Renal clear cell carcinoma, 4. Seminoma, 5. Intratubular germ cell neoplasia (IGCN),
Assessment Run 43 205 Sal-like protein 4 (SALL4) The slide to be stained for SALL4 comprised:. Appendix, 2. Testis, 3. Renal clear cell carcinoma, 4. Seminoma, 5. Intratubular germ cell neoplasia (IGCN),
Breast cancer: IHC classification. Mogens Vyberg Professor of Clinical Pathology Director of NordiQC Aalborg University Hospital, Aalborg, Denmark
 Breast cancer: IHC classification Mogens Vyberg Professor of Clinical Pathology Director of NordiQC Aalborg University Hospital, Aalborg, Denmark http://upload.wikimedia.org/wikipedia/commons/1/1a/breast.svg
Breast cancer: IHC classification Mogens Vyberg Professor of Clinical Pathology Director of NordiQC Aalborg University Hospital, Aalborg, Denmark http://upload.wikimedia.org/wikipedia/commons/1/1a/breast.svg
HER2 ISH (BRISH or FISH)
") Assessment Run H14 2018 HER2 ISH (BRISH or FISH) Material Table 1. Content of the multi-block used for the NordiQC HER2 ISH assessment, run H14 HER2 IHC* IHC score Dual - SISH** FISH*** FISH*** HER2/chr17
Assessment Run H14 2018 HER2 ISH (BRISH or FISH) Material Table 1. Content of the multi-block used for the NordiQC HER2 ISH assessment, run H14 HER2 IHC* IHC score Dual - SISH** FISH*** FISH*** HER2/chr17
NordiQC - update
 NordiQC - update 00-0 EQUALIS Uppsala 0 Tomas Seidal NordiQC participants NordiQC participants n:30 S DK N 6 F Ice Bel 54 NL 4 Ger 6 Aust USA 0 It 8 Argent 8.. 96% participation in S,DK & N ~ 60% in Finland
NordiQC - update 00-0 EQUALIS Uppsala 0 Tomas Seidal NordiQC participants NordiQC participants n:30 S DK N 6 F Ice Bel 54 NL 4 Ger 6 Aust USA 0 It 8 Argent 8.. 96% participation in S,DK & N ~ 60% in Finland
Nordic Immunohistochemical Quality Control
 Nordic Immunohistochemical Quality Control Immunohistochemistry in the classifiation of neoplasias of the alimentary tract & External Quality Assurance of Immunohistochemistry for GI cancer markers Mogens
Nordic Immunohistochemical Quality Control Immunohistochemistry in the classifiation of neoplasias of the alimentary tract & External Quality Assurance of Immunohistochemistry for GI cancer markers Mogens
External Quality Assessment of melanocytic marker analyses NordiQC experience
 External Quality Assessment of melanocytic marker analyses NordiQC experience Jan Klos MD, Department of Pathology Stavanger University Hospital Norway 1 Content 18 Runs = 2112 submissions between 2001-2014
External Quality Assessment of melanocytic marker analyses NordiQC experience Jan Klos MD, Department of Pathology Stavanger University Hospital Norway 1 Content 18 Runs = 2112 submissions between 2001-2014
Immunohistochemical principles The technical test approach. Pre-analytical parametres
 Immunohistochemical principles The technical test approach Pre-analytical parametres Søren Nielsen Global Pathology Manager Agilent Technologies (Former Scheme Manager, NordiQC) 2 IHC project coordinator
Immunohistochemical principles The technical test approach Pre-analytical parametres Søren Nielsen Global Pathology Manager Agilent Technologies (Former Scheme Manager, NordiQC) 2 IHC project coordinator
Assessment Run B HER-2
 Assessment Run B1 2006 HER-2 The slide to be stained for HER-2 comprised: 1. Cell line JIMT-1 (Amplified)* 2. Cell line MDA-453 (Amplified) 3. Cell line MCF-7 (Not amplified) 4. Cell line BT474 (Amplified)
Assessment Run B1 2006 HER-2 The slide to be stained for HER-2 comprised: 1. Cell line JIMT-1 (Amplified)* 2. Cell line MDA-453 (Amplified) 3. Cell line MCF-7 (Not amplified) 4. Cell line BT474 (Amplified)
The unkown primary tumour: IHC Classification, antibody selection, protocol optimization, controls and EQA (part I)
") The unkown primary tumour: IHC Classification, antibody selection, protocol optimization, Mogens Vyberg Professor of Clinical Pathology Director of NordiQC Aalborg University Hospital, Aalborg, Denmark
The unkown primary tumour: IHC Classification, antibody selection, protocol optimization, Mogens Vyberg Professor of Clinical Pathology Director of NordiQC Aalborg University Hospital, Aalborg, Denmark
The unknown primary tumour: IHC classification part I, the primary panel - Antibody selection, protocol optimization, controls and EQA
 The unknown primary tumour: IHC classification part I, Mogens Vyberg Professor of Clinical Pathology Director of NordiQC Aalborg University Hospital, Aalborg, Denmark the primary panel - Antibody selection,
The unknown primary tumour: IHC classification part I, Mogens Vyberg Professor of Clinical Pathology Director of NordiQC Aalborg University Hospital, Aalborg, Denmark the primary panel - Antibody selection,
Product Introduction. Product Codes: HCL029, HCL030 and HCL031. Issue
 Product Introduction Product Codes: HCL029, HCL030 and HCL031 Issue 1. 180510 Contents Introduction to Estrogen Receptor 2 ER immunohistochemistry 3 Quality control 5 Cell lines as controls 6 Estrogen
Product Introduction Product Codes: HCL029, HCL030 and HCL031 Issue 1. 180510 Contents Introduction to Estrogen Receptor 2 ER immunohistochemistry 3 Quality control 5 Cell lines as controls 6 Estrogen
IHC Stainer platforms. Overview, pros and cons
 IHC Stainer platforms Overview, pros and cons Bart De Wiest Quality manager IHC OLV Hospital, Aalst, Belgium Donald Van Hecke Lab & Quality manager AZ St-Lucas, Brugge, Belgium Goal of this lecture: to
IHC Stainer platforms Overview, pros and cons Bart De Wiest Quality manager IHC OLV Hospital, Aalst, Belgium Donald Van Hecke Lab & Quality manager AZ St-Lucas, Brugge, Belgium Goal of this lecture: to
Immunohistochemical classification of lung carcinomas and mesotheliomas. Prof. Mogens Vyberg NordiQC Institute of Pathology Aalborg, Denmark
 Immunohistochemical classification of lung carcinomas and mesotheliomas Prof. Mogens Vyberg NordiQC Institute of Pathology Aalborg, Denmark Endobronchial ultrasound guided transbronchial needle biopsy
Immunohistochemical classification of lung carcinomas and mesotheliomas Prof. Mogens Vyberg NordiQC Institute of Pathology Aalborg, Denmark Endobronchial ultrasound guided transbronchial needle biopsy
Diagnostic IHC in lung and pleura pathology
 Diagnostic IHC in lung and pleura pathology Mogens Vyberg Professor of Clinical Pathology Director of NordiQC Aalborg University Hospital, Aalborg, Denmark WHO 2004 and Web Malignant mesothelioma Epithelioid
Diagnostic IHC in lung and pleura pathology Mogens Vyberg Professor of Clinical Pathology Director of NordiQC Aalborg University Hospital, Aalborg, Denmark WHO 2004 and Web Malignant mesothelioma Epithelioid
Image analysis in IHC overview, considerations and applications
 Image analysis in IHC overview, considerations and applications Rasmus Røge, MD, Institute of Pathology, Aalborg University Hospital NordiQC workshop September 2016 Aalborg, Denmark Outline Theory Image
Image analysis in IHC overview, considerations and applications Rasmus Røge, MD, Institute of Pathology, Aalborg University Hospital NordiQC workshop September 2016 Aalborg, Denmark Outline Theory Image
Immunohistochemistry. Potential and challenges To be or not to be
 Immunohistochemistry Potential and challenges To be or not to be Søren Nielsen Scheme Manager NordiQC Aalborg University Hospital, Denmark Vårmöte 19.05.2016 Karlstad Overview IHC project coordinator at
Immunohistochemistry Potential and challenges To be or not to be Søren Nielsen Scheme Manager NordiQC Aalborg University Hospital, Denmark Vårmöte 19.05.2016 Karlstad Overview IHC project coordinator at
DOUBLE STAINS. Toll-Free: Direct:
 DOUBLE STAINS CD61 + CD71 DAB Brown: CD61 Alk. Phos. Red: CD71 Bone Marrow DAB Brown: Megakaryocytes Alk. Phos. Red: Erythroid Precursors 400x CD61 (2f2) 0.1 ml concentrate............. 161M-14 0.5 ml
DOUBLE STAINS CD61 + CD71 DAB Brown: CD61 Alk. Phos. Red: CD71 Bone Marrow DAB Brown: Megakaryocytes Alk. Phos. Red: Erythroid Precursors 400x CD61 (2f2) 0.1 ml concentrate............. 161M-14 0.5 ml
The unkown primary tumour: IHC Classification, antibody selection, protocol optimization, controls and EQA (part II)
") The unkown primary tumour: IHC Classification, antibody selection, protocol optimization, Mogens Vyberg Professor of Clinical Pathology Director of NordiQC Aalborg University Hospital, Aalborg, Denmark
The unkown primary tumour: IHC Classification, antibody selection, protocol optimization, Mogens Vyberg Professor of Clinical Pathology Director of NordiQC Aalborg University Hospital, Aalborg, Denmark
Single and Multiplex Immunohistochemistry
 Single and Multiplex Immunohistochemistry Steve Westra, BS Reagent Product Specialist Leica Biosystems IHC Theory Polyclonal vs Monoclonal Polyclonal reagents Detect a multitude of epitopes Batch to batch
Single and Multiplex Immunohistochemistry Steve Westra, BS Reagent Product Specialist Leica Biosystems IHC Theory Polyclonal vs Monoclonal Polyclonal reagents Detect a multitude of epitopes Batch to batch
Product Introduction
 Product Introduction Product Codes: HCL026, HCL027 and HCL028 Contents Introduction to HER2 2 HER2 immunohistochemistry 3 Cell lines as controls 5 HER2 Analyte Control DR IHC 7 HER2 Analyte Control DR
Product Introduction Product Codes: HCL026, HCL027 and HCL028 Contents Introduction to HER2 2 HER2 immunohistochemistry 3 Cell lines as controls 5 HER2 Analyte Control DR IHC 7 HER2 Analyte Control DR
Breast cancer diagnostic solutions Deliver diagnostic confidence
 Breast cancer diagnostic solutions Deliver diagnostic confidence 2 Breast cancer diagnostic solutions Roche Tissue Diagnostics is committed to improving outcomes in breast cancer Breast cancer...the most
Breast cancer diagnostic solutions Deliver diagnostic confidence 2 Breast cancer diagnostic solutions Roche Tissue Diagnostics is committed to improving outcomes in breast cancer Breast cancer...the most
HistoCyte Laboratories Ltd
 HistoCyte Laboratories Ltd Progesterone Receptor: The neglected breast receptor! Dr Ian Milton & Colin Tristram November 2018 UKNEQAS Autumn meeting Introduction Progesterone is an important prognostic
HistoCyte Laboratories Ltd Progesterone Receptor: The neglected breast receptor! Dr Ian Milton & Colin Tristram November 2018 UKNEQAS Autumn meeting Introduction Progesterone is an important prognostic
The Panel Approach to Diagnostics. Lauren Hopson International Product Specialist Cell Marque Corporation
 The Panel Approach to Diagnostics Lauren Hopson International Product Specialist Cell Marque Corporation Cell Marque Rocklin, California About Cell Marque: IVD primary antibody manufacturer Distributors
The Panel Approach to Diagnostics Lauren Hopson International Product Specialist Cell Marque Corporation Cell Marque Rocklin, California About Cell Marque: IVD primary antibody manufacturer Distributors
Immunocytochemistry. Run 119/48. Improving Immunocytochemistry for Over 25 Years Results - Summary Graphs - Pass Rates Best Methods - Selected Images
 g Run 119/48 Immunocytochemistry Modules General Pathology: TTF-1& p63 2-11 Breast Pathology: PR 12-19 Breast Pathology: HER2 IHC 2-26 Immunocytochemistry Improving Immunocytochemistry for Over 25 Years
g Run 119/48 Immunocytochemistry Modules General Pathology: TTF-1& p63 2-11 Breast Pathology: PR 12-19 Breast Pathology: HER2 IHC 2-26 Immunocytochemistry Improving Immunocytochemistry for Over 25 Years
PD-L1 Analyte Control DR
 Quality in Control PD-L1 Analyte Control DR PD-L1_PI_v2 Product Codes: HCL019, HCL020 and HCL021 Contents PD-L1 Analyte Control DR 2 What is PD-L1? 3 The Role of PD-L1 in Cancer 3 PD-L1 Assessment 4 PD-L1
Quality in Control PD-L1 Analyte Control DR PD-L1_PI_v2 Product Codes: HCL019, HCL020 and HCL021 Contents PD-L1 Analyte Control DR 2 What is PD-L1? 3 The Role of PD-L1 in Cancer 3 PD-L1 Assessment 4 PD-L1
Immunohistochemical classification of the unknown primary tumour (UPT) Part I. Prof. Mogens Vyberg NordiQC Institute of Pathology Aalborg, Denmark
 Part I. Prof. Mogens Vyberg NordiQC Institute of Pathology Aalborg, Denmark") Immunohistochemical classification of the unknown primary tumour (UPT) Part I Prof. Mogens Vyberg NordiQC Institute of Pathology Aalborg, Denmark Tumours of unknown origin: Histology Brain tumour - biopsy
Immunohistochemical classification of the unknown primary tumour (UPT) Part I Prof. Mogens Vyberg NordiQC Institute of Pathology Aalborg, Denmark Tumours of unknown origin: Histology Brain tumour - biopsy
Immunohistochemical classification of breast tumours
 Immunohistochemical classification of breast tumours Workshop in Diagnostic Immunohistochemistry September 19 th - 21 th 2018 Anne-Vibeke Lænkholm Department of Surgical Pathology, Zealand University Hospital,
Immunohistochemical classification of breast tumours Workshop in Diagnostic Immunohistochemistry September 19 th - 21 th 2018 Anne-Vibeke Lænkholm Department of Surgical Pathology, Zealand University Hospital,
HPV/p16 Analyte Control
 HPV/p16 Analyte Control Utility review and ring study results Colin Tristram, Director 2017 HPV/p16 Analyte Control Collaboration: Dr Max Robinson at Newcastle University a leading pathologist in head
HPV/p16 Analyte Control Utility review and ring study results Colin Tristram, Director 2017 HPV/p16 Analyte Control Collaboration: Dr Max Robinson at Newcastle University a leading pathologist in head
What kind of material should we use for ICC in our daily routine. Torill Sauer Department of Pathology, Akershus University Hospital
 What kind of material should we use for ICC in our daily routine Torill Sauer Department of Pathology, Akershus University Hospital Diversity of preparing cytological material Cell block Direct smears
What kind of material should we use for ICC in our daily routine Torill Sauer Department of Pathology, Akershus University Hospital Diversity of preparing cytological material Cell block Direct smears
IDH1 R132H/ATRX Immunohistochemical validation
 IDH1 R132H/ATRX Immunohistochemical validation CIQC/DSM 2016 12 June 2016 0835-0905 Stephen Yip, M.D., Ph.D., FRCPC University of British Columbia Disclosure Statement I have nothing to disclose I will
IDH1 R132H/ATRX Immunohistochemical validation CIQC/DSM 2016 12 June 2016 0835-0905 Stephen Yip, M.D., Ph.D., FRCPC University of British Columbia Disclosure Statement I have nothing to disclose I will
Immunotherapy in NSCLC Pathologist role
 Immunotherapy in NSCLC Pathologist role Pimpin Incharoen, M.D. Assistant Professor, Thoracic Pathology Department of Pathology, Ramathibodi Hospital Genetic alterations in NSCLC Khono et al, Trans Lung
Immunotherapy in NSCLC Pathologist role Pimpin Incharoen, M.D. Assistant Professor, Thoracic Pathology Department of Pathology, Ramathibodi Hospital Genetic alterations in NSCLC Khono et al, Trans Lung
Assessment performed on Tuesday, July 29, 2014, at Lions Gate Hospital, North Vancouver
 Assessors report for ciqc Run 37: BRAF V600E (April 2014) Assessors: B Gilks, R Wolber, K Ung, P Tavassoli, J Garratt and J Won (recorder) Assessment performed on Tuesday, July 29, 2014, at Lions Gate
Assessors report for ciqc Run 37: BRAF V600E (April 2014) Assessors: B Gilks, R Wolber, K Ung, P Tavassoli, J Garratt and J Won (recorder) Assessment performed on Tuesday, July 29, 2014, at Lions Gate
Classification of the unknown primary tumour: the primary IHC panel
 CIQC/CAP-ACP SEMINAR 2013: DIAGNOSTIC IHC AND MOLECULAR PATHOLOGY Classification of the unknown primary tumour: the primary IHC panel Aalborg University Hospital Denmark Tumours of unknown origin: Histology
CIQC/CAP-ACP SEMINAR 2013: DIAGNOSTIC IHC AND MOLECULAR PATHOLOGY Classification of the unknown primary tumour: the primary IHC panel Aalborg University Hospital Denmark Tumours of unknown origin: Histology
Present Role of Immunohistochemistry in the. Subtypes. Beppe Viale European Institute of Oncology University of Milan Milan-Italy
 Present Role of Immunohistochemistry in the Classification of Molecular Subtypes Beppe Viale European Institute of Oncology University of Milan Milan-Italy We know it is many diseases Breast cancer is
Present Role of Immunohistochemistry in the Classification of Molecular Subtypes Beppe Viale European Institute of Oncology University of Milan Milan-Italy We know it is many diseases Breast cancer is
# Best Practices for IHC Detection and Interpretation of ER, PR, and HER2 Protein Overexpression in Breast Cancer
 #1034 - Best Practices for IHC Detection and Interpretation of ER, PR, and HER2 Protein Overexpression in Breast Cancer Richard W. Cartun, MS, PhD Andrew Ricci, Jr, MD Department of Pathology Hartford
#1034 - Best Practices for IHC Detection and Interpretation of ER, PR, and HER2 Protein Overexpression in Breast Cancer Richard W. Cartun, MS, PhD Andrew Ricci, Jr, MD Department of Pathology Hartford
Recent advances in breast cancers
 Recent advances in breast cancers Breast cancer is a hetrogenous disease due to distinct genetic alterations. Similar morphological subtypes show variation in clinical behaviour especially in response
Recent advances in breast cancers Breast cancer is a hetrogenous disease due to distinct genetic alterations. Similar morphological subtypes show variation in clinical behaviour especially in response
Milestones in Her 2 Testing
 Human Epidermal Growth Factor Receptor 2 (HER2) Testing - Validation, Application and Correlation Her2 is encoded by the C-erbB2 gene and is one of four oncoproteins belonging to the Human Epidermal Growth
Human Epidermal Growth Factor Receptor 2 (HER2) Testing - Validation, Application and Correlation Her2 is encoded by the C-erbB2 gene and is one of four oncoproteins belonging to the Human Epidermal Growth
Quality Control/Quality Assurance in Diagnostic Immunohistochemistry
 CIHRT Exhibit P- Page Quality Control/Quality Assurance in Diagnostic Immunohistochemistry Emina Torlakovic, MD, PhD College of Medicine University of Saskatchewan Emina Emilia Torlakovic, MD, PhD Associate
CIHRT Exhibit P- Page Quality Control/Quality Assurance in Diagnostic Immunohistochemistry Emina Torlakovic, MD, PhD College of Medicine University of Saskatchewan Emina Emilia Torlakovic, MD, PhD Associate
COMPUTER-AIDED HER-2/neu EVALUATION IN EXTERNAL QUALITY ASSURANCE (EQA) OF BREAST CANCER SCREENING PROGRAMME
 OF BREAST CANCER SCREENING PROGRAMME") COMPUTER-AIDED HER-2/neu EVALUATION IN EXTERNAL QUALITY ASSURANCE (EQA) OF BREAST CANCER SCREENING PROGRAMME Maria Lunardi MD Anatomic Pathology Fracastoro Hospital San Bonifacio, Verona -Italy HER2-neu
COMPUTER-AIDED HER-2/neu EVALUATION IN EXTERNAL QUALITY ASSURANCE (EQA) OF BREAST CANCER SCREENING PROGRAMME Maria Lunardi MD Anatomic Pathology Fracastoro Hospital San Bonifacio, Verona -Italy HER2-neu
Results you can trust
 PRODUCT I NF OR MAT ION pharmdx Results you can trust The first and only FDA-approved PD-L1 test to assess the magnitude of treatment effect on progression-free survival in melanoma patients from OPDIVO
PRODUCT I NF OR MAT ION pharmdx Results you can trust The first and only FDA-approved PD-L1 test to assess the magnitude of treatment effect on progression-free survival in melanoma patients from OPDIVO
Instant Quality FISH. The name says it all.
 COMPANION DIAGNOSTICS Instant Quality FISH Instant Quality FISH. The name says it all. IQ: Instant Quality every time. Breast carcinoma stained with : Triple filter showing Blue DAPI colors nuclei, FITC
COMPANION DIAGNOSTICS Instant Quality FISH Instant Quality FISH. The name says it all. IQ: Instant Quality every time. Breast carcinoma stained with : Triple filter showing Blue DAPI colors nuclei, FITC
Epithelia will be discussed according to the following scheme: Type Number of layers Shape Line drawing. Squamous Cuboidal Columnar
 Epithelia Epithelia will be discussed according to the following scheme: Type Number of layers Shape Line drawing Simple Squamous Cuboidal Columnar Covering and Lining epithelium Pseudostratified Stratified
Epithelia Epithelia will be discussed according to the following scheme: Type Number of layers Shape Line drawing Simple Squamous Cuboidal Columnar Covering and Lining epithelium Pseudostratified Stratified
HER2 CISH pharmdx TM Kit Interpretation Guide Breast Cancer
 P A T H O L O G Y HER2 CISH pharmdx TM Kit Interpretation Guide Breast Cancer FROM CERTAINTY COMES TRUST For in vitro diagnostic use HER2 CISH pharmdx Kit HER2 CISH pharmdx Kit is intended for dual-color
P A T H O L O G Y HER2 CISH pharmdx TM Kit Interpretation Guide Breast Cancer FROM CERTAINTY COMES TRUST For in vitro diagnostic use HER2 CISH pharmdx Kit HER2 CISH pharmdx Kit is intended for dual-color
Workflow. Connecting the Pieces For Total Patient Care
 Workflow Connecting the Pieces For Total Patient Care Biocare provides a full line of IHC and molecular pathology products for cancer and infectious disease diagnosis. From a full range of equipment: including
Workflow Connecting the Pieces For Total Patient Care Biocare provides a full line of IHC and molecular pathology products for cancer and infectious disease diagnosis. From a full range of equipment: including
Supplementary Online Content
 Supplementary Online Content Rimm DL, Han G, Taube JM, et al. A prospective, multi-institutional, pathologistbased assessment of 4 immunohistochemistry assays for PD-L1 expression in non small cell lung
Supplementary Online Content Rimm DL, Han G, Taube JM, et al. A prospective, multi-institutional, pathologistbased assessment of 4 immunohistochemistry assays for PD-L1 expression in non small cell lung
Predictive markers for treatment with Immune checkpoint inhibitors - PD-L1 et al -
 Predictive markers for treatment with Immune checkpoint inhibitors - PD-L1 et al - Lukas Bubendorf Pathology Improved overall survival as a result of combination therapy Predictive biomarkers for the treatment
Predictive markers for treatment with Immune checkpoint inhibitors - PD-L1 et al - Lukas Bubendorf Pathology Improved overall survival as a result of combination therapy Predictive biomarkers for the treatment
Immunohistochemical Expression of Hormone Receptors and The Histological Characteristics of Biochemically Hormone Receptor Negative Breast Cancers
 Breast Cancer Vol. 14 No. 1 January 2007 Original Article Immunohistochemical Expression of Hormone Receptors and The Histological Characteristics of Biochemically Hormone Receptor Negative Breast Cancers
Breast Cancer Vol. 14 No. 1 January 2007 Original Article Immunohistochemical Expression of Hormone Receptors and The Histological Characteristics of Biochemically Hormone Receptor Negative Breast Cancers
Protocols for Zytomed Systems antibodies on fully automated IHC staining systems date of issue: September 20, 2012
 Protocols for Zytomed Systems antibodies on fully automated IHC staining systems date of issue: September 20, 2012 These protocols were provided by customers. Under no circumstances shall Zytomed Systems
Protocols for Zytomed Systems antibodies on fully automated IHC staining systems date of issue: September 20, 2012 These protocols were provided by customers. Under no circumstances shall Zytomed Systems
Dr. dr. Primariadewi R, SpPA(K)
") Curriculum Vitae Dr. dr. Primariadewi R, SpPA(K) Education : Medical Doctor from UKRIDA Doctoral Degree from Faculty of Medicine University of Indonesia Pathologist Specialist and Consultant from Faculty
Curriculum Vitae Dr. dr. Primariadewi R, SpPA(K) Education : Medical Doctor from UKRIDA Doctoral Degree from Faculty of Medicine University of Indonesia Pathologist Specialist and Consultant from Faculty
Immunohistochemistry and Bladder Tumours
 Immunohistochemistry and Bladder Tumours Dr. Andrew J. Evans MD PhD FRCPC Consultant in Genitourinary Pathology University Health Network Toronto, ON Objec ves Review markers of urothelial differen a on
Immunohistochemistry and Bladder Tumours Dr. Andrew J. Evans MD PhD FRCPC Consultant in Genitourinary Pathology University Health Network Toronto, ON Objec ves Review markers of urothelial differen a on
Urinary Bladder: WHO Classification and AJCC Staging Update 2017
 Urinary Bladder: WHO Classification and AJCC Staging Update 2017 Houston Society of Clinical Pathologists 58 th Annual Spring Symposium Houston, TX April 8, 2017 Jesse K. McKenney, MD Classification
Urinary Bladder: WHO Classification and AJCC Staging Update 2017 Houston Society of Clinical Pathologists 58 th Annual Spring Symposium Houston, TX April 8, 2017 Jesse K. McKenney, MD Classification
Review and Updates of Immunohistochemistry in Selected Salivary Gland and Head and Neck Tumors
 Review and Updates of Immunohistochemistry in Selected Salivary Gland and Head and Neck Tumors. Monophasic tumors : myoepithelioma, acinic cell carcinoma, and salivary duct carcinoma. Biphasic tumors includes
Review and Updates of Immunohistochemistry in Selected Salivary Gland and Head and Neck Tumors. Monophasic tumors : myoepithelioma, acinic cell carcinoma, and salivary duct carcinoma. Biphasic tumors includes
Assessment performed on Friday, September 18, 2015, at Vancouver General Hospital
 Assessors report for ciqc Run 49: ATRX (June 2015) Assessors: S Yip and J Won (recorder) Assessment performed on Friday, September 18, 2015, at Vancouver General Hospital Background The combined application
Assessors report for ciqc Run 49: ATRX (June 2015) Assessors: S Yip and J Won (recorder) Assessment performed on Friday, September 18, 2015, at Vancouver General Hospital Background The combined application
4/12/2018. MUSC Pathology Symposium Kiawah Island April 18, Jesse K. McKenney, MD
 MUSC Pathology Symposium Kiawah Island April 18, 2018 Jesse K. McKenney, MD 1 Urothelial Carcinoma with Alternative Differentiation 2 Urothelial Carcinoma with Alternative Differentiation Recognition as
MUSC Pathology Symposium Kiawah Island April 18, 2018 Jesse K. McKenney, MD 1 Urothelial Carcinoma with Alternative Differentiation 2 Urothelial Carcinoma with Alternative Differentiation Recognition as
EQA for PD-L1 IHC staining: is it a conundrum? Keith Miller
 EQA for PD-L1 IHC staining: is it a conundrum? Keith Miller Director UK National External Quality Assessment Scheme for Immunohistochemistry & In-situ Hybridisation The dangers of using laboratory developed
EQA for PD-L1 IHC staining: is it a conundrum? Keith Miller Director UK National External Quality Assessment Scheme for Immunohistochemistry & In-situ Hybridisation The dangers of using laboratory developed
Mammaglobin vs GCDFP-15 An Immunohistologic Validation Survey for Sensitivity and Specificity
 Anatomic Pathology / MAMMAGLOBIN IN BREAST CARCINOMA Mammaglobin vs GCDFP-15 An Immunohistologic Validation Survey for Sensitivity and Specificity Rohit Bhargava, MD, 1 Sushil Beriwal, MD, 2 and David
Anatomic Pathology / MAMMAGLOBIN IN BREAST CARCINOMA Mammaglobin vs GCDFP-15 An Immunohistologic Validation Survey for Sensitivity and Specificity Rohit Bhargava, MD, 1 Sushil Beriwal, MD, 2 and David
VENTANA PD-L1 (SP142) Assay Guiding immunotherapy
 Assay Guiding immunotherapy") VENTANA PD-L1 (SP142) Assay Guiding immunotherapy Hiker s path: VENTANA PD-L1 (SP142) Assay on urothelial carcinoma tissue Location: Point Conception, CA VENTANA PD-L1 (SP142) Assay Identify patients most
VENTANA PD-L1 (SP142) Assay Guiding immunotherapy Hiker s path: VENTANA PD-L1 (SP142) Assay on urothelial carcinoma tissue Location: Point Conception, CA VENTANA PD-L1 (SP142) Assay Identify patients most
Aspects of quality in breast pathology. Andrew Lee Nottingham University Hospitals
 Aspects of quality in breast pathology Andrew Lee Nottingham University Hospitals British breast pathology EQA: performance issues Ian Ellis Friday 8.30 am National breast screening pathology audit 2015
Aspects of quality in breast pathology Andrew Lee Nottingham University Hospitals British breast pathology EQA: performance issues Ian Ellis Friday 8.30 am National breast screening pathology audit 2015
The Challenges of Implementing a PD-L1 Proficiency Testing Program in Australia
 VASCULAR CELL OPEN ACCESS ORIGINAL RESEARCH The Challenges of Implementing a PD-L1 Proficiency Testing Program in Australia Pagliuso Julia, Parry Suzanne, Haffajee Zenobia, Badrick Tony, Miller Keith,
VASCULAR CELL OPEN ACCESS ORIGINAL RESEARCH The Challenges of Implementing a PD-L1 Proficiency Testing Program in Australia Pagliuso Julia, Parry Suzanne, Haffajee Zenobia, Badrick Tony, Miller Keith,
In Situ Hybridization: Market Strategies and Forecasts, US,
 In Situ Hybridization: Market Strategies and Forecasts, US, 2018-2024 Table of Contents In Situ Hybridization: Executive Summary The study is designed to give a comprehensive overview of the In Situ Hybridization
In Situ Hybridization: Market Strategies and Forecasts, US, 2018-2024 Table of Contents In Situ Hybridization: Executive Summary The study is designed to give a comprehensive overview of the In Situ Hybridization
Immunocytochemistry. Run 113/42. Improving Immunocytochemistry for Over 25 Years Results - Summary Graphs - Pass Rates Best Methods - Selected Images
 g Run 113/42 Articles / Reports Scheme Updates: May 216 2 Immunocytochemistry Modules General Pathology: SMA & CK 5/6 3-13 Breast Pathology: ER 14-2 Breast Pathology: HER2 IHC 21-26 Immunocytochemistry
g Run 113/42 Articles / Reports Scheme Updates: May 216 2 Immunocytochemistry Modules General Pathology: SMA & CK 5/6 3-13 Breast Pathology: ER 14-2 Breast Pathology: HER2 IHC 21-26 Immunocytochemistry
Vernieuwing en diagnostiek bij NSCLC: Immunotherapy: PD-L1 analyse: waar staan we
 9e avondsymposium: "Nieuwe ontwikkelingen in de behandeling van NSCLC" 9 november 2016, UMCG Vernieuwing en diagnostiek bij NSCLC: Immunotherapy: PD-L1 analyse: waar staan we Wim Timens Professor and Chair
9e avondsymposium: "Nieuwe ontwikkelingen in de behandeling van NSCLC" 9 november 2016, UMCG Vernieuwing en diagnostiek bij NSCLC: Immunotherapy: PD-L1 analyse: waar staan we Wim Timens Professor and Chair
Histological Type. Morphological and Molecular Typing of breast Cancer. Nottingham Tenovus Primary Breast Cancer Study. Survival (%) Ian Ellis
 Ian Ellis") Morphological and Molecular Typing of breast Cancer Ian Ellis Molecular Medical Sciences, University of Nottingham Department of Histopathology, Nottingham University Hospitals NHS Trust Histological Type
Morphological and Molecular Typing of breast Cancer Ian Ellis Molecular Medical Sciences, University of Nottingham Department of Histopathology, Nottingham University Hospitals NHS Trust Histological Type
Coordinate Expression of Cytokeratins 7 and 20 in Prostate Adenocarcinoma and Bladder Urothelial Carcinoma
 Anatomic Pathology / CYTOKERATINS 7 AND 20 IN PROSTATE AND BLADDER CARCINOMAS Coordinate Expression of Cytokeratins 7 and 20 in Prostate Adenocarcinoma and Bladder Urothelial Carcinoma Nader H. Bassily,
Anatomic Pathology / CYTOKERATINS 7 AND 20 IN PROSTATE AND BLADDER CARCINOMAS Coordinate Expression of Cytokeratins 7 and 20 in Prostate Adenocarcinoma and Bladder Urothelial Carcinoma Nader H. Bassily,
ONCO TEAM DIAGNOSTIC
 ONCO TEAM DIAGNOSTIC ONCO TEAM SPECIALISTS The team at ONCO TEAM has 23 specialists: o 11 general pathology seniors: - 8 PhD (1 PhD on lung tumors pathology) o 3 general pathology specialists; o 2 dermopathology
ONCO TEAM DIAGNOSTIC ONCO TEAM SPECIALISTS The team at ONCO TEAM has 23 specialists: o 11 general pathology seniors: - 8 PhD (1 PhD on lung tumors pathology) o 3 general pathology specialists; o 2 dermopathology
NSCLC. Harmonization study 1. Lung cancer and other malignancies -PD-L1 assay, QuIP EQA
 Lung cancer and other malignancies -PD-L1 assay, QuIP EQA Korinna Jöhrens Institute for pathology Carl Gustav Cars Universitätsklinikum Dresden, Germany Medical consultant QuIP 11.05.2018 NSCLC Harmonization
Lung cancer and other malignancies -PD-L1 assay, QuIP EQA Korinna Jöhrens Institute for pathology Carl Gustav Cars Universitätsklinikum Dresden, Germany Medical consultant QuIP 11.05.2018 NSCLC Harmonization
Optimal algorithm for HER2 testing
 Optimal algorithm for HER2 testing The revised definition of IHC 2+ (equivocal) is invasive breast cancer with Weak to moderate complete membrane staining observed in >10% of tumor cells. (see Figure 1
Optimal algorithm for HER2 testing The revised definition of IHC 2+ (equivocal) is invasive breast cancer with Weak to moderate complete membrane staining observed in >10% of tumor cells. (see Figure 1
FISH mcgh Karyotyping ISH RT-PCR. Expression arrays RNA. Tissue microarrays Protein arrays MS. Protein IHC
 Classification of Breast Cancer in the Molecular Era Susan J. Done University Health Network, Toronto Why classify? Prognosis Prediction of response to therapy Pathogenesis Invasive breast cancer can have
Classification of Breast Cancer in the Molecular Era Susan J. Done University Health Network, Toronto Why classify? Prognosis Prediction of response to therapy Pathogenesis Invasive breast cancer can have
Interpretation Manual - Gastric or Gastroesophageal Junction Adenocarcinoma. PD-L1 IHC 22C3 pharmdx is FDA-approved for in vitro diagnostic use
 Interpretation Manual - Gastric or Gastroesophageal Junction Adenocarcinoma PD-L1 IHC 22C3 pharmdx is FDA-approved for in vitro diagnostic use For countries outside of the United States, see the local
Interpretation Manual - Gastric or Gastroesophageal Junction Adenocarcinoma PD-L1 IHC 22C3 pharmdx is FDA-approved for in vitro diagnostic use For countries outside of the United States, see the local
Applications of IHC. Determination of the primary site in metastatic tumors of unknown origin
 Applications of IHC Determination of the primary site in metastatic tumors of unknown origin Classification of tumors that appear 'undifferentiated' by standard light microscopy Precise classification
Applications of IHC Determination of the primary site in metastatic tumors of unknown origin Classification of tumors that appear 'undifferentiated' by standard light microscopy Precise classification
Supplemental Data Table 1 Characteristics of the MHH BC cohort number percent cases histology IDBC ILBC others 6 3 pt status pt1
 Supplemental Data Table 1 Characteristics of the MHH BC cohort number percent cases 183 100 histology IDBC 128 70 ILBC 49 27 others 6 3 pt status pt1 98 54 pt2 56 31 pt3 14 8 pt4 14 8 ptx 1 1 pn status
Supplemental Data Table 1 Characteristics of the MHH BC cohort number percent cases 183 100 histology IDBC 128 70 ILBC 49 27 others 6 3 pt status pt1 98 54 pt2 56 31 pt3 14 8 pt4 14 8 ptx 1 1 pn status
Cluster designation 5 staining of normal and non-lymphoid neoplastic skin*
 J Cutan Pathol 2005: 32: 50 54 Copyright # Blackwell Munksgaard 2005 Blackwell Munksgaard. Printed in Denmark Journal of Cutaneous Pathology Cluster designation 5 staining of normal and non-lymphoid neoplastic
J Cutan Pathol 2005: 32: 50 54 Copyright # Blackwell Munksgaard 2005 Blackwell Munksgaard. Printed in Denmark Journal of Cutaneous Pathology Cluster designation 5 staining of normal and non-lymphoid neoplastic
Thermo Scientific UltraVision Quanto for Immunohistochemistry The New Generation Micro-Polymer Detection System
 Thermo Scientific for Immunohistochemistry The New Generation Micro-Polymer Detection System highest sensitivity sharp crisp clear shorter incubation times UltraVision Quanto the new Micro-Polymer System
Thermo Scientific for Immunohistochemistry The New Generation Micro-Polymer Detection System highest sensitivity sharp crisp clear shorter incubation times UltraVision Quanto the new Micro-Polymer System
A National Quality Assurance program for breast immunohistochemistry: an Italian perspective
 PATHOLOGICA 208;0:83-9 Original article A National Quality Assurance program for breast immunohistochemistry: an Italian perspective E. GUADAGNO, G. DE ROSA *, O. NAPPI 2 Department of Advanced Biomedical
PATHOLOGICA 208;0:83-9 Original article A National Quality Assurance program for breast immunohistochemistry: an Italian perspective E. GUADAGNO, G. DE ROSA *, O. NAPPI 2 Department of Advanced Biomedical
Assessment of Breast Cancer with Borderline HER2 Status Using MIP Microarray
 Assessment of Breast Cancer with Borderline HER2 Status Using MIP Microarray Hui Chen, Aysegul A Sahin, Xinyan Lu, Lei Huo, Rajesh R Singh, Ronald Abraham, Shumaila Virani, Bal Mukund Mishra, Russell Broaddus,
Assessment of Breast Cancer with Borderline HER2 Status Using MIP Microarray Hui Chen, Aysegul A Sahin, Xinyan Lu, Lei Huo, Rajesh R Singh, Ronald Abraham, Shumaila Virani, Bal Mukund Mishra, Russell Broaddus,