CML UPDATE 2018 DAVID S. SNYDER, M.D. MARCH
|
|
|
- Beverly Pierce
- 6 years ago
- Views:
Transcription
1 CML UPDATE 2018 DAVID S. SNYDER, M.D. MARCH 15, 2018 Click to edit Master Presentation Date
2 DISCLOSURES I have nothing to disclose

3
4 Loss in expectation of life of patients with chronic myeloid leukemia in Sweden, over year of diagnosis, by age at diagnosis and sex. Hannah Bower et al. JCO 2016;34: by American Society of Clinical Oncology
5 Number of Cases As Result of Treatment Success the Prevalence of CML Is Increasing Steadily Incidence 4,700 per year Age-matched mortality ratio vs normal population = x greater steady state number of CML patients in US by Accounts for increased US population to 410 million in CML = chronic myelogenous leukemia. Huang et al, Year
6 WORKUP NCCN Guidelines Version Chronic Myeloid Leukemia CLINICAL PRESENTATION ADDITIONAL EVALUATION NCCN Guidelines Index Table of Contents Discussion H&P, including spleen size by palpation (cm below costal margin) CBC with differential Chemistry profile Bone marrow a aspirate and biopsy for morphologic and cytogenetic evaluation Quantitative RT-PCR (qpcr) using International Scale (IS) for BCR- ABL1 (blood) Hepatitis panel (hepatitis B surface antigen [HBsAg], hepatitis B surface antibody [HBsAb], hepatitis B core antibody [anti-hbc], IgM anti-hbc, IgG anti-hbc) Ph positive or BCR- ABL1 positive Ph negative and BCR- ABL1 negative Chronic phase CML Advanced phase CML Accelerated phase b Blast phase b Evaluate for diseases other than CML (See NCCN Guidelines for Myeloproliferative Neoplasms) Determine risk score (See Risk Calculation Table CML-A) Additional testing Flow cytometry to determine cell lineage Mutational analysis HLA testing, if considering allogeneic HCT (See CML-6) See Primary Treatment (CML-2) See Primary Treatment (CML-4) Note: All recommendations are category 2A unless otherwise indicated. Clinical Trials: NCCN believes that the best management of any patient with cancer is in a clinical trial. Participation in clinical trials is a Bone especially marrow encouraged. evaluation should be done for the initial workup, to provide morphologic review, and also to detect other chromosomal abnormalities in addition to Ph Version chromosome , 01/24/18 FISH National can Comprehensive be used Cancer if cytogenetic Network, Inc. 2018, evaluation All rights reserved. is The not NCCN possible. Guidelines and this illustration may not be reproduced in any form without the express written permission b of NCCN See Definitions. of Accelerated Phase and Blast Phase (CML-B). CML-1
7 NCCN Guidelines Version Chronic Myeloid Leukemia NCCN Guidelines Index Table of Contents Discussion CLINICAL PRESENTATION TREATMENT Advanced phase CML Treatment Considerations Evaluate for allogeneic HCT Disease progression to advanced phase while on TKI therapy has worse prognosis than presenting with advanced phase CML. Treatment options are based on patient comorbidities and age. Selection of TKI is based on prior therapy and/or BCR-ABL mutation profile. CNS involvement has been described in blast phase CML. Lumbar puncture and CNS prophylaxis is recommended for lymphoid blast phase. Accelerated phase b Blast phase b Lymphoid Myeloid Clinical trial or TKI (CML-F) or Omacetaxine i (CML-F) Clinical trial or ALL-type induction chemotherapy + TKI (CML-F) (See NCCN Guidelines for Acute Lymphoblastic Leukemia) or TKI (CML-F) + steroids Clinical trial or AML-type induction chemotherapy + TKI (CML-F) (See NCCN Guidelines for Acute Myeloid Leukemia) or TKI (CML-F) Note: All recommendations are category 2A unless otherwise indicated. Clinical Trials: NCCN believes that the best management of any patient with cancer is in a clinical trial. Participation in clinical trials is b See especially Definitions encouraged. of Accelerated Phase and Blast Phase (CML-B). Version i Omacetaxine , 01/24/18 is a National treatment Comprehensive option Cancer for Network, patients Inc. 2018, with All rights disease reserved. progression The NCCN Guidelines to accelerated and this illustration phase may not be CML. reproduced Omacetaxine any form without is the not express a treatment written option for patients who present with permission of NCCN accelerated. phase CML. CML-4



8 Why? Risk score calculation Predicts treatment response High and Intermediate Sokal risk NCCN guidelines suggest risk-based approach to TKI choice Predicts treatment free remission success Low Sokal risk Independent predictor of relapse with cessation Baseline Bcr-Abl transcript 60 months 73% ( 95 %CI: 60 months 47% ( 95 %CI: 34-62) Clarifies determination of early molecular response Patient-specific kinetics of transcript reduction P= Mahon et al, 2011.

9
10 Loss of CCyR (%) Value of MMR in Prolonging Remission Response at 12 months n Loss of CCyR CCyR without MMR 95 24% CCyR plus MMR 32 3% P=0.04 Hughes et al, 2010; Cortes et al, 2005; Marin et al, Months Since Start of Imatinib Therapy

11 % With MMR 11 3-Mo BCR-ABL Predicts MMR, PFS Similarly for Imatinib and Nilotinib Nilotinib (300 mg BID) Imatinib (400 mg QD) % > 1% 10% > 10% n = 120 n = 41 n = 89 n = 133 n = 24 n = 88 By 1 Year 76% 71% By 2 Years 89% 78% 67% 52% 3-y PFS 95.6% 95.3% 98.5% 96.5% % 31% 4% 2% % 20% 83.8% 82.9% Time Since Randomization (Months) Note: greater numbers of early responders with frontline nilotinib Hochhaus A, et al. Haematologica. 2012;97(s1). Abstract 584.
12 Estimated 5-year (A, B) overall survival (OS) and (C, D) progression-free survival (PFS) by molecular response at 3 months for both treatment arms. Jorge E. Cortes et al. JCO 2016;34: by American Society of Clinical Oncology

13 Summary >10% at 3 months is a poor risk category Not all patients with a BCR-ABL1 value >10% at 3 months have a high ongoing risk of treatment failure any reduction below 10% by 6 months may improve outcome the rate of reduction over the first 3 months is an important factor for outcome and could be considered in therapeutic decisions
14 NCCN Guidelines Version Chronic Myeloid Leukemia NCCN Guidelines Index Table of Contents Discussion RESPONSE MILESTONES c,e BCR-ABL1 (IS) 3 months 6 months 12 months >12 months >10% f YELLOW RED >1% 10% GREEN YELLOW RED >0.1% 1% GREEN YELLOW 0.1% GREEN RED YELLOW CLINICAL CONSIDERATIONS Evaluate patient compliance and drug interactions Mutational analysis Evaluate patient compliance and drug interactions Mutational analysis SECOND-LINE AND SUBSEQUENT TREATMENT OPTIONS Switch to alternate TKI (CML-5) and Evaluate for HCT (CML-6) Switch to alternate TKI (CML-5) or Continue same TKI (CML-F) g or Dose escalation of imatinib (to a max of 800 mg) and Evaluate for HCT (CML-6) GREEN Monitor response (CML-F) and side effects Continue same TKI (CML-F) h csee Monitoring Response to TKI Therapy and Mutational Analysis (CML-C). e See Criteria for Hematologic, Cytogenetic, and Molecular Response and Relapse (CML-D). f Patients Note: All with recommendations BCR-ABL1 are only category slightly 2A >10% unless at otherwise 3 months indicated. and/or with a steep decline from baseline, may achieve <10% at 6 months and have generally favorable outcomes. Clinical Trials: Therefore, NCCN believes it is important that the best to management interpret the of value any patient 3 with months cancer in this in a context, clinical trial. before Participation making drastic in clinical changes trials is to the treatment strategy. g Achievement especially encouraged. of response milestones must be interpreted within the clinical context. Patients with more than 50% reduction compared to baseline or minimally above Version the , 10% 01/24/18 cutoff can National continue Comprehensive the Cancer same Network, dose Inc. 2018, of dasatinib, All rights reserved. nilotinib, The NCCN or Guidelines bosutinib and this for illustration another may not 3be months. reproduced in any form without the express written permission h of NCCN. Discontinuation of TKI with careful monitoring is feasible in selected patients. See Discontinuation of TKI Therapy(CML-E). CML-3
15 NCCN Guidelines Version Chronic Myeloid Leukemia NCCN Guidelines Index Table of Contents Discussion MONITORING RESPONSE TO TKI THERAPY AND MUTATIONAL ANALYSIS Test Bone marrow cytogeneti cs 1 Quantitative RT- PCR (qpcr) using IS BCR-ABL kinase domain mutation analysis Recommendation At diagnosis Failure to reach response milestones Any sign of loss of response (defined as hematologic or cytogenetic relapse) At diagnosis Every 3 months after initiating treatment. After BCR-ABL1 (IS) 1% (>0.1% 1%) has been achieved, every 3 months for 2 years and every 3 6 months thereafter If there is 1-log increase in BCR-ABL1 transcript levels with MMR, qpcr should be repeated in 1 3 months Chronic phase Failure to reach response milestones Any sign of loss of response (defined as hematologic or cytogenetic relapse) 1-log increase in BCR-ABL1 transcript levels and loss of MMR Disease progression to accelerated or blast phase Note: All recommendations are category 2A unless otherwise indicated. Clinical Trials: NCCN believes that the best management of any patient with cancer is in a clinical trial. Participation in clinical trials is especially encouraged. Version , 01/24/18 National Comprehensive Cancer Network, Inc. 2018, All rights reserved. The NCCN Guidelines and this illustration may not be reproduced in any form without the express written permission of NCCN. 1 FISH has been inadequately studied for monitoring response to treatment. CML-C

16
17 FIRST LINE THERAPY Click to edit Master Presentation Date
18
19 NCCN Guidelines Version Chronic Myeloid Leukemia NCCN Guidelines Index Table of Contents Discussion CLINICAL PRESENTATION PRIMARY TREATMENT Chronic phase CML Treatment Considerations: Patient comorbidities and drug toxicities Monitor response c Evaluate patient compliance and drug interactions Early toxicity monitoring Low-risk score (See Risk Calculation Table CML-A) Intermediate- or highrisk score (See Risk Calculation Table CML-A) First generation TKI (Imatinib or generic imatinib 400 mg QD) (category 1) or Second generation TKI (Bosutinib 400 mg QD [category 1] or Dasatinib 100 mg QD [category 1] or Nilotinib 300 mg BID [category 1]) or Clinical trial First generation TKI (Imatinib or generic imatinib 400 mg QD) or Second generation TKI (Bosutinib 400 mg QD [category 1] d or Dasatinib 100 mg QD [category 1] d or Nilotinib 300 mg BID [category 1] d ) or Clinical trial See Response Milestones and Treatment Options (CML-3) c See Response Milestones and Treatment Options (CML-3) c csee Monitoring Response to TKI Therapy and Mutational Analysis(CML-C). dlong-term follow-up data from the DASISION and ENESTnd trials and preliminary data from the BFORE trial suggest that patients with an intermediate- or high-risk Sokal or Hasford score may preferentially benefit from second generation TKI (dasatinib, nilotinib, or bosutinib). See Discussion for additional information. Note: All recommendations are category 2A unless otherwise indicated. Clinical Trials: NCCN believes that the best management of any patient with cancer is in a clinical trial. Participation in clinical trials is especially encouraged. Version , 01/24/18 National Comprehensive Cancer Network, Inc. 2018, All rights reserved. The NCCN Guidelines and this illustration may not be reproduced in any form without the express written permission of NCCN. CML-2
 IM400 ENEST/D ASISION TIDEL I (IM600) TIDEL II (IM600) SPIRIT FRANCE (IM600) ENESTnd (NIL) DASISION (DAS) >10% at 3 mos ---")
20 What Is the Standard? Comparative Results: Imatinib 400/600,Nilotinib, Dasatinib IRIS (IM400) IM400 ENEST/D ASISION TIDEL I (IM600) TIDEL II (IM600) SPIRIT FRANCE (IM600) ENESTnd (NIL) DASISION (DAS) >10% at 3 mos %/36% 24% 12% --- 9% 16% CCyR at 12mos 69% 65%/73% 88% 87% a 65% 80% 85% MMR at 12mos 40% 27%/28% 47% 64% 49% 55% 46% MMR at 24 mos 55% 44%/46% 73% 73% 53% 71% 64% MR4.5 at 12mos --- 4%/--- 18% b 19% 22% b 11% 5% MR4.5 at 24mos --- 9%/8% % 26% b 25% 17% OS at 3 yrs 92% 94%/93% % % 94% a Inferred from MR2.0; b MR4.0 rather than MR4.5. Druker et al, 2006; Kantarjian et al, 2010; Kantarjian, Shah et al, 2012; Hughes et al, 2008; Yeung et al, 2015; Preudhomme et al, 2010.

21 Second Generation TKIs Have Improved Response But Not Changed Overall Survival Over Imatinib Response Landmarks Complete cytogenetic response at 12 mos Major molecular response at 12 mos Major molecular response at 60 mos Complete molecular response at 60 mos Overall survival at 60 mos ENESTnd DASISION Imatinib Nilotinib Gain Imatinib Dasatinib Gain 65% 80% +15% 73% 85% +12% 27% 55% +28% 28% 46% +18% 60% 77% +17% 64% 76% +12% 31% 54% +23% 33% 42% +9% 91.7% 93.7% +2% 90% 91% +1% Δ Green Indicates Statistically Significant Difference Red Indicates Nonsignificant Difference Saglio et al, 2010; Kantarjian et al, 2010; Kantarjian, Shah et al, 2012; Larson et al, 2013; Hochhaus et al, 2013.

, % Bosutinib Imatinib P 12 mo 7.5 3.0 0.")
22 Molecular response (%) Molecular Response at 12 and 18 Months BFORE: First-line Bosutinib vs Imatinib in CML P= P= P= CML=chronic myeloid leukemia; ITT=intent-to-treat; mitt=modified intent-to-treat; MR=molecular response; MMR=major molecular response P= P= P= Month: MMR (ITT) MMR (mitt) MR 4 (mitt) MR 4.5 (mitt) MR 4 (ITT), % Bosutinib Imatinib P 12 mo < mo Bosutinib ITT: n=268 mitt: n= months 18 months P=0.02 Imatinib ITT: n=268 mitt: n= months 18 months P=0.11 MR 4.5 (ITT), % Bosutinib Imatinib P 12 mo mo

23 Published in: Neil P. Shah; JCO Ahead of Print DOI: /JCO Copyright 2017 American Society of Clinical Oncology
24 BCR-ABL Mutations: 3-Year Exploratory Analysis Dasatinib 100 mg QD (n=259) DASISION 4-Year Fol Imatinib 400 mg QD (n=260) Patients with mutations detected Clinically relevant on-treatment events, n a No MMR within 12 months No cccyr within 12 months 8 12 Loss of CCyR fold BCR-ABL increase with loss of MMR 2 1 Tested at discontinuation 12 months 3 2 Mutations detected (n) F317I/L (3) V299L (3) G250E (1) T315I (11) M244V (1) G250E (3) D276G (1) E355G (2) L387M (1) E450G (1) L248V (1) E255K/V (4) M351T (3) F359C/I/V (5) H396P (1) Y253H (1) Three additional patients in the imatinib arm (and no additional patients in the dasatinib arm) had mutations in the 4- year per-protocol analysis: G250E, M244V, and F317L/H396R Includes 7 patients with 2 mutations: 1 dasatinib patient (V299L/F317I) and 6 imatinib patients (M351T/F359V, E255V/E450G, L248V/E355G, E255K/M351T, E255V/Y253H, D276G/F359C) a Patients may have had multiple events.
25 RESISTANCE AND 2 ND /3 RD LINE THERAPY Click to edit Master Presentation Date

26 Second Generation TKIs, CML Chronic Phase, After Imatinib: Similar Benefits Months follow-up >24 Complete Hematologic Response Dasatinib Bosutinib Nilotinib Median of 24 >24 89% 86% 77% Major Cytogenetic Response 59% 54% 56% Complete Cytogenetic Response 44% 41% 41% 2-year Progression Free Survival 80% 79% 64% 2-year Overall Survival 91% 92% 87% Shah et al, 2010; Kantarjian, Giles et al, 2011; Cortes et al, 2011.
27 Mutations: When to Look Both the European LeukemiaNet (ELN) and National Comprehensive Cancer Network recommend ABL kinase domain mutational analysis under certain circumstances: Soverini et al, 2011; NCCN, Recommendations on When to Perform Mutational Analysis ELN At diagnosis - Only in advanced phase or blast crisis patients During first-line imatinib therapy - In case of failure - In case of an increase in BCR-ABL transcript levels leading to loss of major molecular response - In any other case of suboptimal response During second-line dasatinib or nilotinib therapy - In case of hematologic or cytogenetic failure NCCN BCR-ABL transcript levels >10% by qpcr IS or less than partial cytogenetic response at 3 months Less than complete cytogenetic response at 12 or 18 months Any sign of loss of response - Defined as hematologic or cytogenetic relapse or 1 log increase in BCR-ABL transcript levels and loss of major molecular response Disease progression to advanced phase

28 Iceberg Analogy #2: Resistance May Be More Complex Than We Think Old sequencing (Sanger sequencing): lower detection limit, 20% Y253H F359V New sequencing techniques, like ultra deep sequencing: lower detection limit, 1% T315I + Y253H T315I L248R Soverini et al 2013.
 are the")


:489-498.")
29 BCR-ABL1 Kinase Domain (KD) Mutations Choice of TKI Tyrosine-kinase After Resistance inhibitors (TKIs) are the mainstay of the treatment of CML BCR-ABL1 KD mutations are the most frequently identified mechanism of acquired TKI resistance 1 BCR-ABL1 mutation testing by conventional Sanger sequencing is recommended for patients with progression, failure and warning 2 1 Clin Cancer Res. 2006; 12(24): Blood. 2013;121(3): th American Society of Hematology Annual Meeting December 7-10, 2013 New Orleans, LA 1

 From compound mutations (>1")

30 Resistance to TKIs and Compound Mutations Hard to differentiate polyclonal mutations (2 different clones) From compound mutations (>1 mutation in the same clone) Zabriskie et al, That may be challenging to treat



31 CML BCR ABL1 Despite a common initiating genetic lesion, CML is a heterogeneous disease and a proportion of patients fail therapy We used next-generation sequencing to 1. Determine whether mutations in other genes are present at diagnosis in some patients that may cooperate with BCR-ABL1 to drive primary drug resistance or modify response 2. To assess additional genomic lesions at disease progression Susan Branford et al, ASH2017









32 % Frequency of relevant SNVs/indels/fusions in genes recurrently mutated in patients with additional variants % 47% 35% Diagnosis Acquired at BC Missense Fs/Stop/Splice Fusion Exon deletion % 20% 14% 6% 6% 4% 4% 4% 4% Susan Branford et al, ASH2017

33 Presence of mutation in genes associated with epigenetic regulation confer poor long-term TKI response. TaeHyung Kim et al. Blood 2017;129: by American Society of Hematology


34 Ponatinib After Second Generation TKI Failure In a cross-study comparison, ponatinib consistently achieved higher complete cytogenetic response rates after 2nd generation TKI failure Lipton et al, 2013.
35 Ponatinib Response Rates in 3rd- and 4th-Line CP-CML Imatinib-nilotinib Imatinib-dasatinib Imatinib-dasatinib-nilotinib Imatinib-nilotinib-dasatinib MCyR, % Patients I-N I-D I-D-N I-N-D CCyR, % Patients I-N I-D I-D-N I-N-D MMR, % Patients I-N I-D I-D-N I-N-D 100% 100% 100% 75% % 67 75% 50% 25% % % 33 50% 25% % 0% 0% n=33 n=52 n=68 n=46 n=33 n=52 n=68 n=46 n=33 n=52 n=68 n=46 Hochhaus et al, 2013; Kantarjian et al, 2013.
36 Omacetaxine Conclusions Omacetaxine is a first-in-class protein synthesis inhibitor with modest activity in highly pretreated CP-CML and accelerated phase patients, including those with the BCR-ABL T315I mutation Response duration appears to be modest Grade 3/4 myelosuppression is common Non-hematologic grade 3/4 toxicities are uncommon Omacetaxine was approved by the US FDA in October 2012 for the treatment of imatinib-resistant chronic and accelerated phase CML
37 EARLY AND LATE COMPLICATIONS Click to edit Master Presentation Date
?")
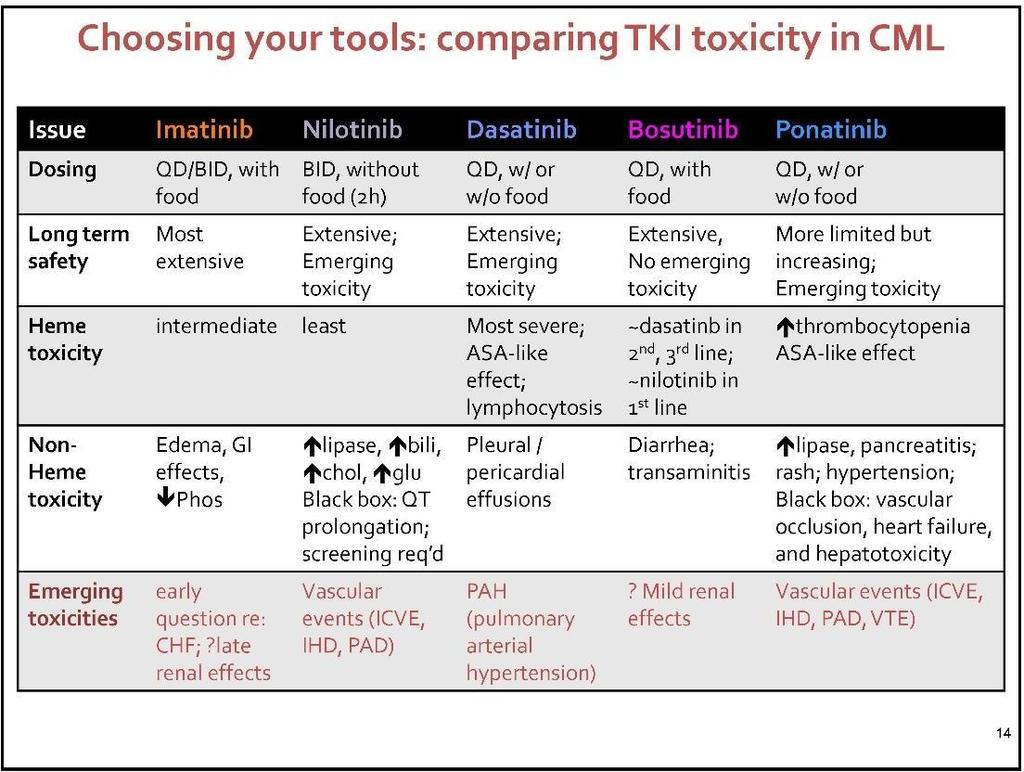
38 The Spectrum of CML TKI Toxicities Ponatinib Vascular adverse events Hypertension Pancreatic enzyme elevation Rash Nilotinib Vascular adverse events Hyperglycemia, Lipids Pancreatic enzyme elevation Indirect hyperbilirubinemia Imatinib Edema/fluid retention Myalgias Hypophosphatemia GI effects (diarrhea, nausea)?renal changes Myelosupression Transaminase Electrolyte Δ QT prolongation Dasatinib Bosutinib Diarrhea/nausea Transaminitis?Renal effects Pleural/pericardial effusion Pulmonary arterial hypertension Bleeding risk NCCN, 2016.
39
40 Ponatinib: Arterial and Venous Thrombotic Events (PACE Trial) Vascular occlusive events a Arterial occlusive events: 28% Venous thromboembolic events: 5% Cerebrovascular Cardiovascular Peripheral vascular AE 5% SAE 4% AE 14% SAE 11% AE 11% SAE 9% AE 11% SAE 8% Exposure-adjusted incidence over time (per 100 patient years): Total Years Total Years AE SAE 0-<1 1-<2 2-<3 3 a AE SAE 0-<1 1-<2 2-<3 3 a a Events occurring in patients with CP-CML; b Median follow-up 35.3 months, analysis for 3 years does not cover a fourth full year for all patients. Cortes et al, 2015.
41 Ponatinib Phase II Study (PACE) Multivariate Analysis: Arterial Thrombotic AEs Estimated Probability fit & 95% CI Dose Intensity (mg/day) Factors significantly associated with arterial thrombotic AEs: Older age (P<0.0001) History of diabetes (P=0.0003) History of ischemia (P=0.0087) Higher dose intensity to time of first event (P=0.0009) Each 15 mg/d reduction in dose intensity results in a predicted reduction of ~40% in the risk of an arterial thrombotic event Cortes, Kim et al, 2013.
42 Risk Mitigation Strategies 1. ASA 81 mg a day; statins? 2. Dose reduction: at start? After MMR? 3. Control traditional risk factors
43 ATE with TKI in CML-CP Multivariate Analysis Variables IR 95% CI For IR P value Age TKI Imatinib Nilotinib Ponatinib Dasatinib Male Race (white) Diabetes Coronary artery disease Hypertension Dyslipidemia
44 ATE with TKI in CML-CP Conclusion ATE occur relatively frequently during therapy with TKI Incidence increases with time of exposure Higher incidence with 2 nd and 3 rd generation TKI compared to imatinib (ponatinib > nilotinib/dasatinib > imatinib) Older age and history of diabetes increase risk Close monitoring and management of co-morbidities required during treatment Occurrence with all TKI suggests possible association with abl inhibition

45 Algorithm for determining the clinical management of low- and high-risk patients with CML treated with TKIs. Mary C. Barber et al. Hematology 2017;2017: by American Society of Hematology
46 TKI DISCONTINUATION AND TREATMENT FREE REMISSION (TFR) Click to edit Master Presentation Date
47 REASONS TO DISCONTINUE: 1. ONGOING TOXICITY- FATIGUE, ARTHRALGIAS, GI UPSET, ETC. 2. FINANCIAL TOXICITY 3. FEMALE PATIENT AND PREGNANCY Click to edit Master Presentation Date
. Grade 1-2 % Grade 3 % TOTAL % Musculoskeletal symptoms** 226 29.7 9 1.2 235 30.")
48 EURO-SKI: Adverse events musculoskeletal symptoms A TKI withdrawal syndrome consisting of new, mostly transient, musculoskeletal pain or discomfort has been described in EUROSKI patients and other cessation trials (Richter et al JCO 2014 Mori et al 2015, Am J Hematology 2015; Lee et al, Haematologica 2016). Grade 1-2 % Grade 3 % TOTAL % Musculoskeletal symptoms** ** musculoskeletal pain, bone and/or joint pain, arthralgia, muscle pain, myalgia, joint stiffness, lumbalgia, articular pain, muscular pain, neck pain, arthromyalgia, pain both arms, pain legs.
49 Paradise Lost, Regained? Cumulative incidence of regained MR4.5 in A-STIM retreated patients after loss of MMR 100 Percent Percent MR CMR With >500 patients reported and very large numbers under investigation, single case of transformation resulting from TFR trial Months Median time to regain deep molecular remission: 7.3 mo One patient with CML >15 yr experienced lymphoid blast crisis 8.5 mo from regained MMR after restarting imatinib Rousselot et al, 2014.

50
51 Cumulative incidence of molecular relapses At 60 months 61% ( 95% CI: 52-70) Cumulative incidence function, accounting for competing events (death in CMR without any relapse n = 1*) *1 case in CMR after 9 months of imatinib cessation (due to myocardial infarction)

52

53

54
55 Molecular Relapse-free Survival (%) Molecular Relapse-free Survival Molecular Relapse-free Survival in All Enrolled Patients (N = 84) Estimated survival 95% confidence band MRFS, % (95% CI) 60 49% (38.0, 59.4) Patients at risk Months Since Dasatinib Discontinuation Patients on first-line dasatinib (n = 37) 54 (38.0, 70.1) Patients on subsequent lines of dasatinib (n = 47) Resistant (n = 25) Intolerant (n = 18) 45 (30.2, 58.7) 44 (24.5, 63.5) 50 (26.9, 73.1) No patients lost CCyR or CHR; no transformation events or deaths were observed CI = confidence interval; CCyR = complete cytogenetic response; CHR = complete hematologic response; MMR = major molecular response; MRFS = molecular relapse-free survival. 55
56 Summary and Conclusions In patients with CML-CP in DMR discontinuing dasatinib, 48% of patients maintained TFR 1 year after discontinuation MMR rates at 1 year were similar for patients on first-line (54%) and subsequent lines of dasatinib (43%) 100% of evaluable patients who lost MMR quickly regained their response after therapy was reinitiated (median time to regain MMR was 1.9 months) Adverse events reported here were consistent with the known safety profile of dasatinib Only 9.5% of patients reported symptoms of dasatinib withdrawal, and most events resolved without concomitant therapy This largest dasatinib discontinuation trial to date strongly supports the feasibility of TFR in patients with CML-CP in DMR treated in the first line and beyond CML-CP = chronic-phase chronic myeloid leukemia; DMR = deep molecular response; MMR = major molecular response; TFR = treatment-free remission. 56

57

58
59 Conclusion EURO-SKI outlines important preconditions which can be employed as guidance for stopping criteria. Best cut-off was defined by 3.1 years for MR 4 duration and 5.8 years for total imatinib-treatment duration. Apart from the two cut-offs, an almost linear increase in TFR probability per additional year on treatment / in MR 4 for patients treated first-line with imatinib could be demonstrated and validated! MR 4 duration was most important (relative increase of probability of about 16% / year). Time on TKI without MR 4 was hardly important (relative increase of probability to stay in MMR about 0.86% / year).

60 Criteria to guide selection of patients suitable for a TFR attempt. Timothy P. Hughes, and David M. Ross Blood 2016;128: by American Society of Hematology

61

62
63 Survival without MMR loss Cumulative incidence of MMR loss MMR stability after nilotinib dose reduction and once daily dosing 2 patients lost MMR 4 and 6 months after nilotinib dose reduction QD Cumulative incidence of MMR loss by 12 months was 9.7% (95% CI: 88.%-99.3) Survival without MMR loss was 97.2% at 12 months Survival without MMR loss Cumulative incidence of MMR loss 100% 100% 80% 80% 60% 60% 40% 40% 20% At 12 months: 97.2% (5% CI: 93.3%-100%) 20% By 12 months: 9.7% (95% CI: 88.%-99.3) 0% Months since nilotinib dose reduction 0% Months since nilotinib dose reduction
64 Conclusion (2) New CML management proposal for clinical practice Lower dose TKI Full dose TKI Lower dose TKI No DMR: Lifelong low-dose therapy CML Optimal response Induction Optimal response Consolidation Long-lasting DMR: TFR attempt Stop TKI
65 FUTURE AND CURRENT STATE Click to edit Master Presentation Date

66
 SH2 Kinase SH2 BCR ABL001 Kinase INACTIVE ACTIVE Developed to gain greater BCR-ABL1")

67 4th Generation TKI ABL001 Allosterically Inhibits BCR-ABL1 Kinase Activity BCR SH3 SH3 t(9;22) SH2 Kinase SH2 BCR ABL001 Kinase INACTIVE ACTIVE Developed to gain greater BCR-ABL1 inhibition, with activity against BCR-ABL1 mutations conferring resistance to TKIs Potential to combine with TKIs for greater pharmacological control of BCR-ABL1 ABL001 Ottman et al, 2015.

68 Mechanisms of persistence and approaches to targeting CML leukemia stem cells. Ravi Bhatia Hematology 2017;2017: by American Society of Hematology
69

70 Published in: Neil P. Shah; JCO Ahead of Print DOI: /JCO Copyright 2017 American Society of Clinical Oncology
DAVID S. SNYDER, M.D.
 CML UPDATE 2019 DAVID S. SNYDER, M.D. MARCH 21,2019 Click to edit Master Presentation Date Disclosures I do not have anything to disclose 2001 2016 Loss in expectation of life of patients with chronic
CML UPDATE 2019 DAVID S. SNYDER, M.D. MARCH 21,2019 Click to edit Master Presentation Date Disclosures I do not have anything to disclose 2001 2016 Loss in expectation of life of patients with chronic
Stopping TKI s in CML- Are we There Yet? Joseph O. Moore, MD Duke Cancer Institute
 Stopping TKI s in CML- Are we There Yet? Joseph O. Moore, MD Duke Cancer Institute Natural History of CML Accumulation of immature myeloid cells New cytogenetic changes Chronic Phase Accelerated Phase
Stopping TKI s in CML- Are we There Yet? Joseph O. Moore, MD Duke Cancer Institute Natural History of CML Accumulation of immature myeloid cells New cytogenetic changes Chronic Phase Accelerated Phase
CML: Living with a Chronic Disease
 CML: Living with a Chronic Disease Jorge Cortes, MD Chief, CML and AML Sections Department of Leukemia M. D. Anderson Cancer Center Houston, Texas Survival in Early Chronic Phase CML TKI Interferon Chemotherapy
CML: Living with a Chronic Disease Jorge Cortes, MD Chief, CML and AML Sections Department of Leukemia M. D. Anderson Cancer Center Houston, Texas Survival in Early Chronic Phase CML TKI Interferon Chemotherapy
The concept of TFR (Treatment Free Remission) in CML
 in CML") The concept of TFR (Treatment Free Remission) in CML Giuseppe Saglio University of Turin, Italy What can we expect today on long-term therapy with TKIs in CML? German CML study IV Relative and overall
The concept of TFR (Treatment Free Remission) in CML Giuseppe Saglio University of Turin, Italy What can we expect today on long-term therapy with TKIs in CML? German CML study IV Relative and overall
HOW I TREAT CML. 4. KONGRES HEMATOLOGOV IN TRANSFUZIOLOGOV SLOVENIJE Z MEDNARODNO UDELEŽBO Terme Olimia, Podčetrtek,
 HOW I TREAT CML 4. KONGRES HEMATOLOGOV IN TRANSFUZIOLOGOV SLOVENIJE Z MEDNARODNO UDELEŽBO Terme Olimia, Podčetrtek, 12. - 14. april, 2012 Gianantonio Rosti Dpt of Hematology and Oncological Sciences S.
HOW I TREAT CML 4. KONGRES HEMATOLOGOV IN TRANSFUZIOLOGOV SLOVENIJE Z MEDNARODNO UDELEŽBO Terme Olimia, Podčetrtek, 12. - 14. april, 2012 Gianantonio Rosti Dpt of Hematology and Oncological Sciences S.
Stopping treatment how much we understand about mechanisms to stop successfully today, and where are the limits? Andreas Hochhaus
 Stopping treatment how much we understand about mechanisms to stop successfully today, and where are the limits? Andreas Hochhaus Frankfurt I 27.5.2017 Aims of CML Therapy Leukemia cells >10 12 CHR 10
Stopping treatment how much we understand about mechanisms to stop successfully today, and where are the limits? Andreas Hochhaus Frankfurt I 27.5.2017 Aims of CML Therapy Leukemia cells >10 12 CHR 10
Does Generic Imatinib Change the Treatment Approach in CML?
 Does Generic Imatinib Change the Treatment Approach in CML? Jerald P. Radich, MD Fred Hutchinson Cancer Research Center/ Seattle Cancer Care Alliance NCCN.org For Clinicians NCCN.org/patients For Patients
Does Generic Imatinib Change the Treatment Approach in CML? Jerald P. Radich, MD Fred Hutchinson Cancer Research Center/ Seattle Cancer Care Alliance NCCN.org For Clinicians NCCN.org/patients For Patients
ELN Recommendations on treatment choice and response. Gianantonio Rosti, MD, Department of Hematology, University of Bologna, Italy
 ELN Recommendations on treatment choice and response Gianantonio Rosti, MD, Department of Hematology, University of Bologna, Italy ELN 2013 Response to Front-line Treatment Baseline 3 months 6 months OPTIMAL
ELN Recommendations on treatment choice and response Gianantonio Rosti, MD, Department of Hematology, University of Bologna, Italy ELN 2013 Response to Front-line Treatment Baseline 3 months 6 months OPTIMAL
Guidelines and real World: Management of CML in chronic and advanced phases. Carolina Pavlovsky. FUNDALEU May 2017 Frankfurt
 Guidelines and real World: Management of CML in chronic and advanced phases Carolina Pavlovsky. FUNDALEU 26-28 May 217 Frankfurt Some Issues in CML 217 First Line treatment: Imatinib vs 2nd generation
Guidelines and real World: Management of CML in chronic and advanced phases Carolina Pavlovsky. FUNDALEU 26-28 May 217 Frankfurt Some Issues in CML 217 First Line treatment: Imatinib vs 2nd generation
2 nd Generation TKI Frontline Therapy in CML
 2 nd Generation TKI Frontline Therapy in CML Elias Jabbour, M.D. April 212 New York Frontline Therapy of CML in 212 - imatinib 4 mg daily - nilotinib 3 mg BID - dasatinib 1 mg daily Second / third line
2 nd Generation TKI Frontline Therapy in CML Elias Jabbour, M.D. April 212 New York Frontline Therapy of CML in 212 - imatinib 4 mg daily - nilotinib 3 mg BID - dasatinib 1 mg daily Second / third line
Role of Second Generation Tyrosine Kinase Inhibitors in Newly Diagnosed CML. GIUSEPPE SAGLIO, MD University of Torino, Italy
 Role of Second Generation Tyrosine Kinase Inhibitors in Newly Diagnosed CML GIUSEPPE SAGLIO, MD University of Torino, Italy Outcome in 282 Patients Treated with Imatinib First Line in Hammersmith Hospital
Role of Second Generation Tyrosine Kinase Inhibitors in Newly Diagnosed CML GIUSEPPE SAGLIO, MD University of Torino, Italy Outcome in 282 Patients Treated with Imatinib First Line in Hammersmith Hospital
SESSION III: Chronic myeloid leukemia PONATINIB. Gianantonio Rosti, MD, Department of Hematology, University of Bologna, Italy
 SESSION III: Chronic myeloid leukemia PONATINIB Gianantonio Rosti, MD, Department of Hematology, University of Bologna, Italy Ponatinib A Pan-BCR-ABL Inhibitor Rationally designed inhibitor of BCR- ABL
SESSION III: Chronic myeloid leukemia PONATINIB Gianantonio Rosti, MD, Department of Hematology, University of Bologna, Italy Ponatinib A Pan-BCR-ABL Inhibitor Rationally designed inhibitor of BCR- ABL
The BCR-ABL1 fusion. Epidemiology. At the center of advances in hematology and molecular medicine
 At the center of advances in hematology and molecular medicine Philadelphia chromosome-positive chronic myeloid leukemia Robert E. Richard MD PhD rrichard@uw.edu robert.richard@va.gov Philadelphia chromosome
At the center of advances in hematology and molecular medicine Philadelphia chromosome-positive chronic myeloid leukemia Robert E. Richard MD PhD rrichard@uw.edu robert.richard@va.gov Philadelphia chromosome
Treatment free remission in CML: from the concept to practice. François-Xavier Mahon. Cancer Center Bordeaux Université Bordeaux, France
 Treatment free remission in CML: from the concept to practice François-Xavier Mahon Cancer Center Bordeaux Université Bordeaux, France CML is a model 1960 1970 1980 1990 2000 2010 Philadelphia chromosome
Treatment free remission in CML: from the concept to practice François-Xavier Mahon Cancer Center Bordeaux Université Bordeaux, France CML is a model 1960 1970 1980 1990 2000 2010 Philadelphia chromosome
IRIS 8-Year Update. Management of TKI Resistance Will KD mutations matter? Sustained CCyR on study. 37% Unacceptable Outcome 17% 53% 15%
 Management of TKI Resistance Will KD mutations matter? IRIS 8-Year Update 17% 53% 5% 15% 37% Unacceptable Outcome No CCyR Lost CCyR CCyR Other 3% 7% Safety Lost-regained CCyR Sustained CCyR on study Deininger
Management of TKI Resistance Will KD mutations matter? IRIS 8-Year Update 17% 53% 5% 15% 37% Unacceptable Outcome No CCyR Lost CCyR CCyR Other 3% 7% Safety Lost-regained CCyR Sustained CCyR on study Deininger
Stopping Treatment in CML and dose reduction in clinical practice: Can we do it safely? YES WE CAN!
 Stopping Treatment in CML and dose reduction in clinical practice: Can we do it safely? YES WE CAN! Dragana Milojković The Hammersmith Hospital, London, UK Leukemic burden Current Aim of TKI therapy Molecular
Stopping Treatment in CML and dose reduction in clinical practice: Can we do it safely? YES WE CAN! Dragana Milojković The Hammersmith Hospital, London, UK Leukemic burden Current Aim of TKI therapy Molecular
Welcome and Introductions
 Living with Chronic Myeloid Leukemia Welcome and Introductions Living with Chronic Myeloid Leukemia Living with Chronic Myeloid Leukemia (CML) Neil P. Shah, MD, PhD Edward S. Ageno Distinguished Professor
Living with Chronic Myeloid Leukemia Welcome and Introductions Living with Chronic Myeloid Leukemia Living with Chronic Myeloid Leukemia (CML) Neil P. Shah, MD, PhD Edward S. Ageno Distinguished Professor
CML: Yesterday, Today and Tomorrow. Jorge Cortes, MD Chief CML Section Department of Leukemia The University of Texas, M.D. Anderson Cancer Center
 CML: Yesterday, Today and Tomorrow Jorge Cortes, MD Chief CML Section Department of Leukemia The University of Texas, M.D. Anderson Cancer Center Five Years of Signal Transduction Inhibition The Beginning
CML: Yesterday, Today and Tomorrow Jorge Cortes, MD Chief CML Section Department of Leukemia The University of Texas, M.D. Anderson Cancer Center Five Years of Signal Transduction Inhibition The Beginning
Oxford Style Debate on STOPPING Treatment.
 Oxford Style Debate on STOPPING Treatment. This house believes that there are good reasons NOT to stop CML treatment. It should be done within clinical trials, OR only in expert centers where frequent,
Oxford Style Debate on STOPPING Treatment. This house believes that there are good reasons NOT to stop CML treatment. It should be done within clinical trials, OR only in expert centers where frequent,
Chronic myeloid leukemia (CML) Warunsuda Sripakdee, BCOP,BCP Prince of Songkla University
 Warunsuda Sripakdee, BCOP,BCP Prince of Songkla University") Chronic myeloid leukemia (CML) 1 Warunsuda Sripakdee, BCOP,BCP Prince of Songkla University Hematologic malignancies CML ALL AML 2 CML CD34+ results from an acquired mutation that affects hematopoietic
Chronic myeloid leukemia (CML) 1 Warunsuda Sripakdee, BCOP,BCP Prince of Songkla University Hematologic malignancies CML ALL AML 2 CML CD34+ results from an acquired mutation that affects hematopoietic
CML and Future Perspective. Hani Al-Hashmi, MD
 CML and Future Perspective Hani Al-Hashmi, MD Objectives Learning from CML history Outcome of interest to clinician Patient and community interest!! Learning from CML history Survival Probability (All
CML and Future Perspective Hani Al-Hashmi, MD Objectives Learning from CML history Outcome of interest to clinician Patient and community interest!! Learning from CML history Survival Probability (All
Contemporary and Future Approaches in CML. Emory Meeting; Sea Island August 2014 Hagop Kantarjian, M.D.
 Contemporary and Future Approaches in CML Emory Meeting; Sea Island August 2014 Hagop Kantarjian, M.D. 1 CML. Historical vs. Modern Perspective Parameter Historical Modern Course Fatal Indolent Prognosis
Contemporary and Future Approaches in CML Emory Meeting; Sea Island August 2014 Hagop Kantarjian, M.D. 1 CML. Historical vs. Modern Perspective Parameter Historical Modern Course Fatal Indolent Prognosis
A 34-year old women came because of abdominal discomfort. Vital sign was stable. Spleen tip was palpable.
 1 Case 1 A 34-year old women came because of abdominal discomfort. Vital sign was stable. Spleen tip was palpable. CBC and bone marrow aspiration and biopsy were done. Chromosome study showed she had t(9;22)
1 Case 1 A 34-year old women came because of abdominal discomfort. Vital sign was stable. Spleen tip was palpable. CBC and bone marrow aspiration and biopsy were done. Chromosome study showed she had t(9;22)
CML David L Porter, MD University of Pennsylvania Medical Center Abramson Cancer Center CML Current treatment options for CML
 1 CML 2012 LLS Jan 26, 2012 David L Porter, MD University of Pennsylvania Medical Center Abramson Cancer Center CML 2012 Current treatment options for CML patients Emerging therapies for CML treatment
1 CML 2012 LLS Jan 26, 2012 David L Porter, MD University of Pennsylvania Medical Center Abramson Cancer Center CML 2012 Current treatment options for CML patients Emerging therapies for CML treatment
2nd generation TKIs to first line therapy
 New Horizons 2011 Newly diagnosed CML moving 2nd generation TKIs to first line therapy Gianantonio Rosti Dept. Of Hematology and Oncology St. Orsola-Malpighi University Hospital Bologna (Italy) GIMEMA
New Horizons 2011 Newly diagnosed CML moving 2nd generation TKIs to first line therapy Gianantonio Rosti Dept. Of Hematology and Oncology St. Orsola-Malpighi University Hospital Bologna (Italy) GIMEMA
CML Clinical Case Scenario
 CML Clinical Case Scenario Neil Shah, MD, PhD Edward S. Ageno Distinguished Professor in Hematology/Oncology Leader, Hematopoietic Malignancies Program Helen Diller Family Comprehensive Cancer Center at
CML Clinical Case Scenario Neil Shah, MD, PhD Edward S. Ageno Distinguished Professor in Hematology/Oncology Leader, Hematopoietic Malignancies Program Helen Diller Family Comprehensive Cancer Center at
Starting & stopping therapy in Chronic Myeloid Leukemia: What more is needed? Richard A. Larson, MD University of Chicago March 2019
 Starting & stopping therapy in Chronic Myeloid Leukemia: What more is needed? Richard A. Larson, MD University of Chicago March 2019 Disclosures Richard A. Larson, MD Research funding to the University
Starting & stopping therapy in Chronic Myeloid Leukemia: What more is needed? Richard A. Larson, MD University of Chicago March 2019 Disclosures Richard A. Larson, MD Research funding to the University
10 YEARS EXPERIENCE OF TYROSINE KINASE INHIBITOR THERAPY FOR CML IN OXFORD
 10 YEARS EXPERIENCE OF TYROSINE KINASE INHIBITOR THERAPY FOR CML IN OXFORD Dalia Khan 1, Noemi Roy 1, Vasha Bari 1, Grant Vallance 1, Helene Dreau 1, Timothy Littlewood 1, Andrew Peniket 1, Paresh Vyas
10 YEARS EXPERIENCE OF TYROSINE KINASE INHIBITOR THERAPY FOR CML IN OXFORD Dalia Khan 1, Noemi Roy 1, Vasha Bari 1, Grant Vallance 1, Helene Dreau 1, Timothy Littlewood 1, Andrew Peniket 1, Paresh Vyas
Chronic Myeloid Leukemia A Disease of Young at Heart but Not of Body
 Chronic Myeloid Leukemia A Disease of Young at Heart but Not of Body Jeffrey H Lipton, PhD MD FRCPC Staff Physician, Princess Margaret Cancer Centre Professor of Medicine University of Toronto POGO November,
Chronic Myeloid Leukemia A Disease of Young at Heart but Not of Body Jeffrey H Lipton, PhD MD FRCPC Staff Physician, Princess Margaret Cancer Centre Professor of Medicine University of Toronto POGO November,
New drugs and trials. Andreas Hochhaus
 New drugs and trials. Andreas Hochhaus Hadera I Oct 2018 Introduction ABL001 is a potent, specific inhibitor of BCR-ABL1 with a distinct allosteric mechanism of action BCR-ABL1 Protein Binds a distinct
New drugs and trials. Andreas Hochhaus Hadera I Oct 2018 Introduction ABL001 is a potent, specific inhibitor of BCR-ABL1 with a distinct allosteric mechanism of action BCR-ABL1 Protein Binds a distinct
What is New in CML Jorge Cortes, MD Chief, CML and AML Sections Department of Leukemia MD Anderson Cancer Center Houston, Texas
 What is New in CML 2018 Jorge Cortes, MD Chief, CML and AML Sections Department of Leukemia MD Anderson Cancer Center Houston, Texas Final Results CML-IV Molecular Response with Imatinib 1538 pts newly
What is New in CML 2018 Jorge Cortes, MD Chief, CML and AML Sections Department of Leukemia MD Anderson Cancer Center Houston, Texas Final Results CML-IV Molecular Response with Imatinib 1538 pts newly
EUROPEAN LEUKEMIANET RECOMMENDATIONS FOR CHRONIC MYELOID LEUKEMIA
 EUROPEAN LEUKEMIANET RECOMMENDATIONS FOR CHRONIC MYELOID LEUKEMIA SAN DIEGO, 11 DECEMBER 2011 AMSTERDAM, 14 JUNE 2012 BALTIMORE, 20 SEPTEMBER 2012 ATLANTA, 6 DECEMBER 2012 ELN, CML Panel Jane Apperley
EUROPEAN LEUKEMIANET RECOMMENDATIONS FOR CHRONIC MYELOID LEUKEMIA SAN DIEGO, 11 DECEMBER 2011 AMSTERDAM, 14 JUNE 2012 BALTIMORE, 20 SEPTEMBER 2012 ATLANTA, 6 DECEMBER 2012 ELN, CML Panel Jane Apperley
BMS Satellite Symposium
 ICKSH 2018 BMS Satellite Symposium Emerging Trends in CML Management CHAIRMAN The Head of Catholic Hematology Hospital The Director of the Catholic Leukemia Research Institute at the Catholic University
ICKSH 2018 BMS Satellite Symposium Emerging Trends in CML Management CHAIRMAN The Head of Catholic Hematology Hospital The Director of the Catholic Leukemia Research Institute at the Catholic University
NEW DRUGS IN HEMATOLOGY Bologna, 9-11 May 2016 CHRONIC MYELOID LEUKEMIA STATUS OF THE ART OF TREATMENT.
 NEW DRUGS IN HEMATOLOGY Bologna, 9-11 May 2016 CHRONIC MYELOID LEUKEMIA STATUS OF THE ART OF TREATMENT Michele.baccarani@unibo.it Michele BACCARANI, MD Professor of Hematology at the Universities of Trieste,
NEW DRUGS IN HEMATOLOGY Bologna, 9-11 May 2016 CHRONIC MYELOID LEUKEMIA STATUS OF THE ART OF TREATMENT Michele.baccarani@unibo.it Michele BACCARANI, MD Professor of Hematology at the Universities of Trieste,
Dose reduction. What do we know and how we do it in clinical practice. Andreas Hochhaus
 Dose reduction. What do we know and how we do it in clinical practice. Andreas Hochhaus Hadera I Oct 2018 Front-line Randomized Trials in CML-CP Trial Drugs References IRIS IM 400 vs IFN/AraC TOPS IM
Dose reduction. What do we know and how we do it in clinical practice. Andreas Hochhaus Hadera I Oct 2018 Front-line Randomized Trials in CML-CP Trial Drugs References IRIS IM 400 vs IFN/AraC TOPS IM
New drugs in first-line therapy
 New drugs in first-line therapy Gianantonio Rosti Dept of Hematology and Oncology Seràgnoli, Bologna University (Italy) GIMEMA (Gruppo Italiano Malattie Ematologiche dell Adulto) CML WORKING PARTY IRIS
New drugs in first-line therapy Gianantonio Rosti Dept of Hematology and Oncology Seràgnoli, Bologna University (Italy) GIMEMA (Gruppo Italiano Malattie Ematologiche dell Adulto) CML WORKING PARTY IRIS
Accepted Manuscript. Improving Outcomes in Chronic Myeloid Leukemia Over Time in the Era of Tyrosine Kinase Inhibitors. Pradnya Chopade, Luke P.
 Accepted Manuscript Improving Outcomes in Chronic Myeloid Leukemia Over Time in the Era of Tyrosine Kinase Inhibitors Pradnya Chopade, Luke P. Akard PII: S2152-2650(18)30343-4 DOI: 10.1016/j.clml.2018.06.029
Accepted Manuscript Improving Outcomes in Chronic Myeloid Leukemia Over Time in the Era of Tyrosine Kinase Inhibitors Pradnya Chopade, Luke P. Akard PII: S2152-2650(18)30343-4 DOI: 10.1016/j.clml.2018.06.029
RESEARCH ARTICLE. Introduction. Methods Wiley Periodicals, Inc.
 BCR/ABL level at 6 months identifies good risk CML subgroup after failing early molecular response at 3 months following imatinib therapy for CML in chronic phase AJH Dennis (Dong Hwan) Kim, 1 * Nada Hamad,
BCR/ABL level at 6 months identifies good risk CML subgroup after failing early molecular response at 3 months following imatinib therapy for CML in chronic phase AJH Dennis (Dong Hwan) Kim, 1 * Nada Hamad,
Imatinib & Ponatinib. Two ends of the spectrum in 2016s reality
 Imatinib & Ponatinib Two ends of the spectrum in 2016s reality CML 2016 Benefits & risks Steve O Brien CML Horizons, May 2016 Disclosures Research funding, participation in company trial, speaker, consultant,
Imatinib & Ponatinib Two ends of the spectrum in 2016s reality CML 2016 Benefits & risks Steve O Brien CML Horizons, May 2016 Disclosures Research funding, participation in company trial, speaker, consultant,
I nuovi guariti? La malattia minima residua nella leucemia mieloide cronica. Fabrizio Pane
 I nuovi guariti? La malattia minima residua nella leucemia mieloide cronica Fabrizio Pane What could be the concept of Cure in CML? Sustained DMR with or without TKI therapy And 100% CML-related survival
I nuovi guariti? La malattia minima residua nella leucemia mieloide cronica Fabrizio Pane What could be the concept of Cure in CML? Sustained DMR with or without TKI therapy And 100% CML-related survival
How I treat high risck CML
 Torino, September 14, 2018 How I treat high risck CML Patrizia Pregno Hematology Dept. Citta della Salute e della Scienza Torino Disclosures Advisory Board: Novartis, Pfizer, Incyte Speaker Honoraria:
Torino, September 14, 2018 How I treat high risck CML Patrizia Pregno Hematology Dept. Citta della Salute e della Scienza Torino Disclosures Advisory Board: Novartis, Pfizer, Incyte Speaker Honoraria:
What is New in CML in Hagop Kantarjian, M.D. February 2011
 What is New in CML in 2011 Hagop Kantarjian, M.D. February 2011 1 CML. Historical vs. Modern Perspective Parameter Historical Modern Course Fatal Indolent Prognosis Poor Excellent 10-yr survival 10% 84-90%
What is New in CML in 2011 Hagop Kantarjian, M.D. February 2011 1 CML. Historical vs. Modern Perspective Parameter Historical Modern Course Fatal Indolent Prognosis Poor Excellent 10-yr survival 10% 84-90%
Low doses of tyrosine kinase inhibitors in CML
 CML Horizons Conference Warsaw 4-6 May 2018 Low doses of tyrosine kinase inhibitors in CML Delphine Rea, MD, PhD Pôle Hématologie Oncologie Radiothérapie INSERM UMR-1160 Centre Hospitalo-Universitaire
CML Horizons Conference Warsaw 4-6 May 2018 Low doses of tyrosine kinase inhibitors in CML Delphine Rea, MD, PhD Pôle Hématologie Oncologie Radiothérapie INSERM UMR-1160 Centre Hospitalo-Universitaire
Management of CML in blast crisis. Lymphoma Tumor Board November 27, 2015
 Management of CML in blast crisis Lymphoma Tumor Board November 27, 2015 Chronic Phase CML - 2. Peter Maslak, ASH Image Bank 2011; 2011-2455 Copyright 2011 American Society of Hematology. Copyright restrictions
Management of CML in blast crisis Lymphoma Tumor Board November 27, 2015 Chronic Phase CML - 2. Peter Maslak, ASH Image Bank 2011; 2011-2455 Copyright 2011 American Society of Hematology. Copyright restrictions
La terapia della LMC: è possibile guarire senza trapianto? Fabrizio Pane
 La terapia della LMC: è possibile guarire senza trapianto? Fabrizio Pane What could be the concept of Cure in CML? Sustained DMR with or without TKI therapy And 100% CML-related survival And QoL comparable
La terapia della LMC: è possibile guarire senza trapianto? Fabrizio Pane What could be the concept of Cure in CML? Sustained DMR with or without TKI therapy And 100% CML-related survival And QoL comparable
Chronic Myeloid Leukaemia
 Chronic Myeloid Leukaemia Molecular Response: What is really important? Jeff Szer The Royal Melbourne Hospital PROBABILITY, % PROBABILITY OF SURVIVAL AFTER MYELOABLATIVE TRANSPLANTS FOR CML IN CHRONIC
Chronic Myeloid Leukaemia Molecular Response: What is really important? Jeff Szer The Royal Melbourne Hospital PROBABILITY, % PROBABILITY OF SURVIVAL AFTER MYELOABLATIVE TRANSPLANTS FOR CML IN CHRONIC
What is the optimal management strategy for younger CP-CML patients with matched, related donors who fail to achieve CCyR
 What is the optimal management strategy for younger CP-CML patients with matched, related donors who fail to achieve CCyR after 18 months of imatinib? Second generation TKIs as a bridge to allogeneic SCT
What is the optimal management strategy for younger CP-CML patients with matched, related donors who fail to achieve CCyR after 18 months of imatinib? Second generation TKIs as a bridge to allogeneic SCT
1 Educational session salient points. Tim Hughes, Vivian Oehler and Rick Van Etten. Tim - Imatinib is a less toxic drug than what we are seeing with
 1 Educational session salient points. Tim Hughes, Vivian Oehler and Rick Van Etten. Tim - Imatinib is a less toxic drug than what we are seeing with both Nilotinib and Dasatinib. Nilotinib for the cardio
1 Educational session salient points. Tim Hughes, Vivian Oehler and Rick Van Etten. Tim - Imatinib is a less toxic drug than what we are seeing with both Nilotinib and Dasatinib. Nilotinib for the cardio
Contemporary and Future Approaches in Management of CML. Disclosures
 Winship Cancer Institute of Emory University Contemporary and Future Approaches in Management of CML Hagop Kantarjian, MD Chairman and Professor, Department of Leukemia University of Texas M. D. Anderson
Winship Cancer Institute of Emory University Contemporary and Future Approaches in Management of CML Hagop Kantarjian, MD Chairman and Professor, Department of Leukemia University of Texas M. D. Anderson
Blast Phase Chronic Myelogenous Leukemia
 Blast Phase Chronic Myelogenous Leukemia Benjamin Powers, MD; and Suman Kambhampati, MD The dramatic improvement in survival with tyrosine kinase inhibitors has not been demonstrated in the advanced blast
Blast Phase Chronic Myelogenous Leukemia Benjamin Powers, MD; and Suman Kambhampati, MD The dramatic improvement in survival with tyrosine kinase inhibitors has not been demonstrated in the advanced blast
MRD in CML (BCR-ABL1)
") MRD in CML (BCR-ABL1) Moleculaire Biologie en Cytometrie cursus Barbara Denys LAbo Hematologie UZ Gent 6 mei 2011 2008 Universitair Ziekenhuis Gent 1 Myeloproliferative Neoplasms o WHO classification 2008:
MRD in CML (BCR-ABL1) Moleculaire Biologie en Cytometrie cursus Barbara Denys LAbo Hematologie UZ Gent 6 mei 2011 2008 Universitair Ziekenhuis Gent 1 Myeloproliferative Neoplasms o WHO classification 2008:
Study Design and Endpoints
 Complete Molecular Response (CMR) Rate With Nilotinib in Patients With CML-CP Without CMR After 2 Years on Imatinib: Preliminary Results From the Randomized ENESTcmr Trial Timothy P. Hughes, Jeffrey H.
Complete Molecular Response (CMR) Rate With Nilotinib in Patients With CML-CP Without CMR After 2 Years on Imatinib: Preliminary Results From the Randomized ENESTcmr Trial Timothy P. Hughes, Jeffrey H.
MP BCR-ABL1 Testing in Chronic Myelogenous Leukemia and Acute Lymphoblastic Leukemia
 Medical Policy BCBSA Ref. Policy: 2.04.85 Last Review: 10/18/2018 Effective Date: 10/18/2018 Section: Medicine Related Policies 8.01.30 Hematopoietic Cell Transplantation for Chronic Myelogenous Leukemia
Medical Policy BCBSA Ref. Policy: 2.04.85 Last Review: 10/18/2018 Effective Date: 10/18/2018 Section: Medicine Related Policies 8.01.30 Hematopoietic Cell Transplantation for Chronic Myelogenous Leukemia
Milestones and Monitoring
 Curr Hematol Malig Rep (2015) 10:167 172 DOI 10.1007/s11899-015-0258-1 CHRONIC MYELOID LEUKEMIAS (E JABBOUR, SECTION EDITOR) Milestones and Monitoring Alessandro Morotti 1 & Carmen Fava 1 & Giuseppe Saglio
Curr Hematol Malig Rep (2015) 10:167 172 DOI 10.1007/s11899-015-0258-1 CHRONIC MYELOID LEUKEMIAS (E JABBOUR, SECTION EDITOR) Milestones and Monitoring Alessandro Morotti 1 & Carmen Fava 1 & Giuseppe Saglio
IS MUTATION ANALYSIS OF BCR-ABL OF ANY VALUE IN CLINICAL MANAGEMENT OF CML PATIENTS? David Marin, Imperial College London
 IS MUTATION ANALYSIS OF BCR-ABL OF ANY VALUE IN CLINICAL MANAGEMENT OF CML PATIENTS? David Marin, Imperial College London Tell me generals, are we politicians necessary? I have to admit defeat before starting
IS MUTATION ANALYSIS OF BCR-ABL OF ANY VALUE IN CLINICAL MANAGEMENT OF CML PATIENTS? David Marin, Imperial College London Tell me generals, are we politicians necessary? I have to admit defeat before starting
CML TREATMENT GUIDELINES
 CML TREATMENT GUIDELINES INITIAL INVESTIGATION Propose enrolment in the CML Registry of the CML-MPN Quebec Research Group. Medical history : Question for cardio-respiratory disorders, diabetes, pancreatitis,
CML TREATMENT GUIDELINES INITIAL INVESTIGATION Propose enrolment in the CML Registry of the CML-MPN Quebec Research Group. Medical history : Question for cardio-respiratory disorders, diabetes, pancreatitis,
AGGIORNAMENTI IN EMATOLOGIA Faenza, 7 Giugno 2018 LMC: ALGORITMI TERAPEUTICI ATTUALI E IL PROBLEMA DELLA RESISTENZA.
 AGGIORNAMENTI IN EMATOLOGIA Faenza, 7 Giugno 2018 LMC: ALGORITMI TERAPEUTICI ATTUALI E IL PROBLEMA DELLA RESISTENZA Michele.Baccarani@unibo.it EUROPEAN LEUKEMIANET 2013 (Blood 2013;122:885 892). RESPONSE
AGGIORNAMENTI IN EMATOLOGIA Faenza, 7 Giugno 2018 LMC: ALGORITMI TERAPEUTICI ATTUALI E IL PROBLEMA DELLA RESISTENZA Michele.Baccarani@unibo.it EUROPEAN LEUKEMIANET 2013 (Blood 2013;122:885 892). RESPONSE
NEW DRUGS IN HEMATOLOGY
 NEW DRUGS IN HEMATOLOGY BOLOGNA, 15-17 April 2013 TYROSINE KINASE INHIBITORS IN CHRONIC MYELOID LEUKEMIA MICHELE BACCARANI michele.baccarani@unibo.it Historic Development of CML Therapy Palliative Therapy
NEW DRUGS IN HEMATOLOGY BOLOGNA, 15-17 April 2013 TYROSINE KINASE INHIBITORS IN CHRONIC MYELOID LEUKEMIA MICHELE BACCARANI michele.baccarani@unibo.it Historic Development of CML Therapy Palliative Therapy
BCCA Protocol Summary for Treatment of Chronic Myeloid Leukemia and Ph+ Acute Lymphoblastic Leukemia Using PONAtinib
 BCCA Protocol Summary for Treatment of Chronic Myeloid Leukemia and Ph+ Acute Lymphoblastic Leukemia Using PONAtinib Protocol Code Tumour Group Contact Physician ULKCMLP Leukemia Dr. Donna Forrest ELIGIBILITY:
BCCA Protocol Summary for Treatment of Chronic Myeloid Leukemia and Ph+ Acute Lymphoblastic Leukemia Using PONAtinib Protocol Code Tumour Group Contact Physician ULKCMLP Leukemia Dr. Donna Forrest ELIGIBILITY:
Molecular monitoring of CML patients
 EHA, Education Session, CML Stockholm, 14 June 2013 Molecular monitoring of CML patients Martin C. Müller Medical Faculty Mannheim Ruprecht-Karls-University Heidelberg Mannheim, Germany Disclosures Research
EHA, Education Session, CML Stockholm, 14 June 2013 Molecular monitoring of CML patients Martin C. Müller Medical Faculty Mannheim Ruprecht-Karls-University Heidelberg Mannheim, Germany Disclosures Research
What Can We Expect from Imatinib? CML Case Presentation. Presenter Disclosure Information. CML Case Presentation (cont)? Session 2: 8:15 AM - 9:00 AM
? Session 2: 8:15 AM - 9:00 AM") Welcome to Master Class for Oncologists Session 2: 8:15 AM - 9: AM Miami, FL December 18, 29 Chronic Myelocytic Leukemia: Imatinib and Beyond Speaker: Daniel J. DeAngelo, MD, PhD Dana-Farber Cancer Institute
Welcome to Master Class for Oncologists Session 2: 8:15 AM - 9: AM Miami, FL December 18, 29 Chronic Myelocytic Leukemia: Imatinib and Beyond Speaker: Daniel J. DeAngelo, MD, PhD Dana-Farber Cancer Institute
9/26/2018. Learning Objectives
 ADVANCES IN CHRONIC MYELOID LEUKEMIA Alison Wakoff Loren, MD, MSCE Associate Professor of Medicine Director, Blood & Marrow Transplantation Vice Chair, Faculty Development Department of Medicine Perelman
ADVANCES IN CHRONIC MYELOID LEUKEMIA Alison Wakoff Loren, MD, MSCE Associate Professor of Medicine Director, Blood & Marrow Transplantation Vice Chair, Faculty Development Department of Medicine Perelman
Chronic Myelogenous Leukemia
 NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ) Chronic Myelogenous Leukemia Version 1.2015 NCCN.org Continue Version 1.2015, 08/28/14 National Comprehensive Cancer Network, Inc. 2014,
NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ) Chronic Myelogenous Leukemia Version 1.2015 NCCN.org Continue Version 1.2015, 08/28/14 National Comprehensive Cancer Network, Inc. 2014,
Discontinuation of Tyrosine Kinase Inhibitors in Chronic Myeloid Leukemia: What s Stopping us from Stopping?
 Discontinuation of Tyrosine Kinase Inhibitors in Chronic Myeloid Leukemia: What s Stopping us from Stopping? David Pham, PharmD PGY2 Hematology/Oncology Pharmacy Resident South Texas VA Health Care System
Discontinuation of Tyrosine Kinase Inhibitors in Chronic Myeloid Leukemia: What s Stopping us from Stopping? David Pham, PharmD PGY2 Hematology/Oncology Pharmacy Resident South Texas VA Health Care System
State of the Art Therapy and Monitoring of CML Hagop Kantarjian, M.D. Grand Rounds Hackensack, New Jersey. September 22, 2010
 State of the Art Therapy and Monitoring of CML - 2010 Hagop Kantarjian, M.D. Grand Rounds Hackensack, ew Jersey September 22, 2010 1 CML. Historical vs. Modern Perspective Parameter Historical Modern Course
State of the Art Therapy and Monitoring of CML - 2010 Hagop Kantarjian, M.D. Grand Rounds Hackensack, ew Jersey September 22, 2010 1 CML. Historical vs. Modern Perspective Parameter Historical Modern Course
CML Update 2016 Arthur 2016
 CML Update 2016 Chronic Myeloid Leukemia Splenomegaly CML (3 phase disease) Increased white cells Malignant proliferation of myeloid white cells Initially mature cells a) chronic phase of disease Evolution
CML Update 2016 Chronic Myeloid Leukemia Splenomegaly CML (3 phase disease) Increased white cells Malignant proliferation of myeloid white cells Initially mature cells a) chronic phase of disease Evolution
1794 Updating Long-Term Outcome of Intermittent Imatinib. (INTERIM) Treatment in Elderly Patients with Ph+-CML
 Treatment in Elderly Patients with Ph+-CML") 738 What Is the Most Cost-Effective Strategy for Treating Newly Diagnosed Chronic Phase Chronic Myeloid Leukaemia (CML) after Imatinib Loses Patent Exclusivity? https://ash.confex.com/ash/2014/webprogram/paper71699.html
738 What Is the Most Cost-Effective Strategy for Treating Newly Diagnosed Chronic Phase Chronic Myeloid Leukaemia (CML) after Imatinib Loses Patent Exclusivity? https://ash.confex.com/ash/2014/webprogram/paper71699.html
Practical Guidance for the Management of CML in 2016
 Practical Guidance for the Management of CML in 2016 Neil Shah, MD, PhD Edward S. Ageno Distinguished Professor in Hematology/Oncology Leader, Hematopoietic Malignancies Program Helen Diller Family Comprehensive
Practical Guidance for the Management of CML in 2016 Neil Shah, MD, PhD Edward S. Ageno Distinguished Professor in Hematology/Oncology Leader, Hematopoietic Malignancies Program Helen Diller Family Comprehensive
CML HORIZONS 101 AND CML 101
 CML HORIZONS 101 AND CML 101 by Pat Garcia-Gonzalez, USA May 1, 2015 Barcelona, Spain Goals of this Session Everything you ever wanted to know and were afraid of asking Help you navigate the conference
CML HORIZONS 101 AND CML 101 by Pat Garcia-Gonzalez, USA May 1, 2015 Barcelona, Spain Goals of this Session Everything you ever wanted to know and were afraid of asking Help you navigate the conference
Chronic Myelogenous Leukemia
 NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ) Chronic Myelogenous Leukemia Version 3.2014 NCCN.org Continue Version 3.2014, 01/15/14 National Comprehensive Cancer Network, Inc. 2014,
NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ) Chronic Myelogenous Leukemia Version 3.2014 NCCN.org Continue Version 3.2014, 01/15/14 National Comprehensive Cancer Network, Inc. 2014,
State of the Art Therapy and Monitoring of CML Hagop Kantarjian, M.D. Grand Rounds UT Southwestern. October 28, 2010
 State of the Art Therapy and Monitoring of CML - 2010 Hagop Kantarjian, M.D. Grand Rounds UT Southwestern October 28, 2010 1 CML. Historical vs. Modern Perspective Parameter Historical Modern Course Fatal
State of the Art Therapy and Monitoring of CML - 2010 Hagop Kantarjian, M.D. Grand Rounds UT Southwestern October 28, 2010 1 CML. Historical vs. Modern Perspective Parameter Historical Modern Course Fatal
C Longer follow up on IRIS data
 hronic Myeloid Leukemia Drs. Rena Buckstein, Mervat Mahrous & Eugenia Piliotis with input from Dr. J. Lipton (PMH) Updated August 2008* Updates: C Longer follow up on IRIS data Guidelines for monitoring
hronic Myeloid Leukemia Drs. Rena Buckstein, Mervat Mahrous & Eugenia Piliotis with input from Dr. J. Lipton (PMH) Updated August 2008* Updates: C Longer follow up on IRIS data Guidelines for monitoring
15 th Annual Miami Cancer Meeting
 15 th Annual Miami Cancer Meeting CLL and CML Mohamed A. Kharfan-Dabaja, MD, MBA, FACP Director, Blood and Marrow Transplantation and Cellular Therapies Mayo Clinic Jacksonville, FL 15 th Annual Miami
15 th Annual Miami Cancer Meeting CLL and CML Mohamed A. Kharfan-Dabaja, MD, MBA, FACP Director, Blood and Marrow Transplantation and Cellular Therapies Mayo Clinic Jacksonville, FL 15 th Annual Miami
Molecular Detection of BCR/ABL1 for the Diagnosis and Monitoring of CML
 Molecular Detection of BCR/ABL1 for the Diagnosis and Monitoring of CML Imran Mirza, MD, MS, FRCPC Pathology & Laboratory Medicine Institute Sheikh Khalifa Medical City, Abu Dhabi, UAE. imirza@skmc.ae
Molecular Detection of BCR/ABL1 for the Diagnosis and Monitoring of CML Imran Mirza, MD, MS, FRCPC Pathology & Laboratory Medicine Institute Sheikh Khalifa Medical City, Abu Dhabi, UAE. imirza@skmc.ae
History of CML Treatment
 History of CML Treatment Eduardo Olavarria No conflict of interest Lisbon, 20th March 2018 #EBMT18 www.ebmt.or What is CML? The mystery of chronic myeloid leukaemia Chronic myeloid leukaemia Often diagnosed
History of CML Treatment Eduardo Olavarria No conflict of interest Lisbon, 20th March 2018 #EBMT18 www.ebmt.or What is CML? The mystery of chronic myeloid leukaemia Chronic myeloid leukaemia Often diagnosed
Dati sulla sospensione della terapia
 Leucemia Mieloide Cronica Dati sulla sospensione della terapia Gianantonio Rosti, Bologna BCR-ABL Loading in CML Patients 100% 10% 1% MMR MR 4 MR 4.5 STIM study design N=100 Start Imatinib CMR Sustained
Leucemia Mieloide Cronica Dati sulla sospensione della terapia Gianantonio Rosti, Bologna BCR-ABL Loading in CML Patients 100% 10% 1% MMR MR 4 MR 4.5 STIM study design N=100 Start Imatinib CMR Sustained
Is there a best TKI for chronic phase CML?
 MANAGING TYPICAL AND ATYPICAL CHRONIC MYELOID LEUKEMIA Is there a best TKI for chronic phase CML? Richard A. Larson 1 1 Section of Hematology/Oncology, Department of Medicine, and Comprehensive Cancer
MANAGING TYPICAL AND ATYPICAL CHRONIC MYELOID LEUKEMIA Is there a best TKI for chronic phase CML? Richard A. Larson 1 1 Section of Hematology/Oncology, Department of Medicine, and Comprehensive Cancer
CML 301 SOME INTRODUCTION INTO CML, CML SCIENCE, DRUG DEVELOPMENT AND INFORMATION RESOURCES. by Sarunas Narbutas Jan Geissler.
 CML 301 SOME INTRODUCTION INTO CML, CML SCIENCE, DRUG DEVELOPMENT AND INFORMATION RESOURCES by Sarunas Narbutas Jan Geissler 4 May 2018 CML 101 / BASICS: UNDERSTANDING THE DISCUSSIONS IN CML SESSIONS What
CML 301 SOME INTRODUCTION INTO CML, CML SCIENCE, DRUG DEVELOPMENT AND INFORMATION RESOURCES by Sarunas Narbutas Jan Geissler 4 May 2018 CML 101 / BASICS: UNDERSTANDING THE DISCUSSIONS IN CML SESSIONS What
Which TKI? An embarrassment of riches for chronic myeloid leukemia patients
 CHRONIC MYELOID LEUKEMIA:REFINING/REDEFINING THE STATE OF THE ART Which TKI? An embarrassment of riches for chronic myeloid leukemia patients Timothy Hughes 1 and Deborah White 1 1 South Australian Health
CHRONIC MYELOID LEUKEMIA:REFINING/REDEFINING THE STATE OF THE ART Which TKI? An embarrassment of riches for chronic myeloid leukemia patients Timothy Hughes 1 and Deborah White 1 1 South Australian Health
Executive summary Overview
 Executive summary Overview In this appraisal, we have demonstrated that dasatinib is clinically more effective, as well as more cost effective, than imatinib, the current standard of care. In the pivotal
Executive summary Overview In this appraisal, we have demonstrated that dasatinib is clinically more effective, as well as more cost effective, than imatinib, the current standard of care. In the pivotal
CML: definition. CML epidemiology. CML diagnosis. CML: peripheralbloodsmear. Cytogenetic abnormality of CML
 MolecularDiagnostic.be Third Scientific Meeting Molecular Diagnostics.be t(9;22) CML: definition Management of CML patients treated with TKI: the place of molecular monitoring Antwerp, December 13 th 11
MolecularDiagnostic.be Third Scientific Meeting Molecular Diagnostics.be t(9;22) CML: definition Management of CML patients treated with TKI: the place of molecular monitoring Antwerp, December 13 th 11
517 Spirit 2: An NCRI Randomised Study Comparing Dasatinib with Imatinib in Patients with Newly Diagnosed CML
 517 Spirit 2: An NCRI Randomised Study Comparing Dasatinib with Imatinib in Patients with Newly Diagnosed CML https://ash.confex.com/ash/2014/webprogram/paper66809.html Objective. SPIRIT 2 is the largest
517 Spirit 2: An NCRI Randomised Study Comparing Dasatinib with Imatinib in Patients with Newly Diagnosed CML https://ash.confex.com/ash/2014/webprogram/paper66809.html Objective. SPIRIT 2 is the largest
Hull and East Yorkshire and North Lincolnshire NHS Trusts Haematology Multidisciplinary Team Guideline and Pathway. Chronic Myeloid Leukaemia
 Hull and East Yorkshire and North Lincolnshire NHS Trusts Haematology Multidisciplinary Team Guideline and Pathway Chronic Myeloid Leukaemia 1 BACKGROUND The Hull and North Lincolnshire Haematology Multidisciplinary
Hull and East Yorkshire and North Lincolnshire NHS Trusts Haematology Multidisciplinary Team Guideline and Pathway Chronic Myeloid Leukaemia 1 BACKGROUND The Hull and North Lincolnshire Haematology Multidisciplinary
Juan Luis Steegmann Hospital de la Princesa. Madrid. JL Steegmann
 Juan Luis Steegmann Hospital de la Princesa. Madrid. Juan Luis Steegmann Hospital de la Princesa. Madrid No rush,at least in Chronic Phase Blast Phase*: SCT asap, after restablishing CP with TKI Accelerated
Juan Luis Steegmann Hospital de la Princesa. Madrid. Juan Luis Steegmann Hospital de la Princesa. Madrid No rush,at least in Chronic Phase Blast Phase*: SCT asap, after restablishing CP with TKI Accelerated
The speaker has no financial relationships with a commercial interest to disclose and no conflicts of interest to resolve.
 Hana Safah MD Professor of Medicine Tulane University School of Medicine Director of the SCT program, Tulane Medical Center The speaker has no financial relationships with a commercial interest to disclose
Hana Safah MD Professor of Medicine Tulane University School of Medicine Director of the SCT program, Tulane Medical Center The speaker has no financial relationships with a commercial interest to disclose
Imatinib dose intensification, combination therapies. Andreas Hochhaus Universitätsklinikum Jena, Germany
 Imatinib dose intensification, combination therapies Andreas Hochhaus Universitätsklinikum Jena, Germany Apperley JF. Lancet Oncol. 2007 High OCT-1 activity is associated with faster MMR in imatinib treated
Imatinib dose intensification, combination therapies Andreas Hochhaus Universitätsklinikum Jena, Germany Apperley JF. Lancet Oncol. 2007 High OCT-1 activity is associated with faster MMR in imatinib treated
Q&A and Technical Support Opening Remarks. Opening Remarks. Susan L. Buchanan, MS, PA-C Dana-Farber Cancer Institute
 Susan L. Buchanan, MS, PA-C Dana-Farber Cancer Institute Daniel J. DeAngelo, MD, PhD Dana-Farber Cancer Institute August 7, 2015 Moderated by Rose K. Joyce NCCN, Conferences and Meetings Department This
Susan L. Buchanan, MS, PA-C Dana-Farber Cancer Institute Daniel J. DeAngelo, MD, PhD Dana-Farber Cancer Institute August 7, 2015 Moderated by Rose K. Joyce NCCN, Conferences and Meetings Department This
Understanding Treatment-Free Remission and How It Impacts You
 Understanding Treatment-Free Remission and How It Impacts You Written by Michael J. Mauro, M.D. Leader, Myeloproliferative Disorders Program Memorial Sloan Kettering Cancer Center Professor of Medicine,
Understanding Treatment-Free Remission and How It Impacts You Written by Michael J. Mauro, M.D. Leader, Myeloproliferative Disorders Program Memorial Sloan Kettering Cancer Center Professor of Medicine,
Chronic Myeloid Leukemia, Version
 1108 NCCN Chronic Myeloid Leukemia, Version 1.2019 Clinical Practice Guidelines in Oncology Jerald P. Radich, MD; Michael Deininger, MD, PhD; Camille N. Abboud, MD; Jessica K. Altman, MD; Ellin Berman,
1108 NCCN Chronic Myeloid Leukemia, Version 1.2019 Clinical Practice Guidelines in Oncology Jerald P. Radich, MD; Michael Deininger, MD, PhD; Camille N. Abboud, MD; Jessica K. Altman, MD; Ellin Berman,
Chronic Myeloid Leukemia
 NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ) Version 1.2019 August 1, 2018 NCCN.org Continue Version 1.2019, 08/01/18 National Comprehensive Cancer Network, Inc. 2018, All rights reserved.
NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ) Version 1.2019 August 1, 2018 NCCN.org Continue Version 1.2019, 08/01/18 National Comprehensive Cancer Network, Inc. 2018, All rights reserved.
Post ASH Actualités LMC
 Post ASH 2014 - Actualités LMC Actualités de première ligne LMC PC ENESTnd (6 ans) Dasision (5 ans) EPIC Spirit France (5 ans) Spirit 2 UK (5 ans) ENESTnd: Mise à jour à 6 ans Design = 846 ults with wly
Post ASH 2014 - Actualités LMC Actualités de première ligne LMC PC ENESTnd (6 ans) Dasision (5 ans) EPIC Spirit France (5 ans) Spirit 2 UK (5 ans) ENESTnd: Mise à jour à 6 ans Design = 846 ults with wly
Diagnosis and Management of Chronic Myeloid Leukaemia
 Diagnosis and Management of Chronic Myeloid Leukaemia Dr Simon Watt Dr Katherine O Neill Dr Fiona Dignan Written July 2017 Prof Tim Somervaille Review July 2019 1 Table of Contents 1.0 Introduction 3 2.0
Diagnosis and Management of Chronic Myeloid Leukaemia Dr Simon Watt Dr Katherine O Neill Dr Fiona Dignan Written July 2017 Prof Tim Somervaille Review July 2019 1 Table of Contents 1.0 Introduction 3 2.0
pan-canadian Oncology Drug Review Final Clinical Guidance Report Bosutinib (Bosulif) for Chronic Myelogenous Leukemia April 21, 2015
 for Chronic Myelogenous Leukemia April 21, 2015") pan-canadian Oncology Drug Review Final Clinical Guidance Report Bosutinib (Bosulif) for Chronic Myelogenous Leukemia April 21, 2015 DISCLAIMER Not a Substitute for Professional Advice This report is primarily
pan-canadian Oncology Drug Review Final Clinical Guidance Report Bosutinib (Bosulif) for Chronic Myelogenous Leukemia April 21, 2015 DISCLAIMER Not a Substitute for Professional Advice This report is primarily
Venice Meeting Highlights: Key lessons. Conclusions Michele Baccarani Rüdiger Hehlmann
 Venice Meeting Highlights: Key lessons Conclusions Michele Baccarani Rüdiger Hehlmann CML therapy in the imatinib era CML prognosis has improved dramatically Cellular and molecular biology studies help
Venice Meeting Highlights: Key lessons Conclusions Michele Baccarani Rüdiger Hehlmann CML therapy in the imatinib era CML prognosis has improved dramatically Cellular and molecular biology studies help
A COMPARATIVE EFFECTIVENESS ANALYSIS OF PATIENTS NEWLY INITIATING TYROSINE KINASE INHIBITOR THERAPY FOR CHRONIC MYELOID LEUKEMIA.
 A COMPARATIVE EFFECTIVENESS ANALYSIS OF PATIENTS NEWLY INITIATING TYROSINE KINASE INHIBITOR THERAPY FOR CHRONIC MYELOID LEUKEMIA Melea Ward A dissertation submitted to the faculty of the University of
A COMPARATIVE EFFECTIVENESS ANALYSIS OF PATIENTS NEWLY INITIATING TYROSINE KINASE INHIBITOR THERAPY FOR CHRONIC MYELOID LEUKEMIA Melea Ward A dissertation submitted to the faculty of the University of
TREATMENT INTENT Disease modification- see European LeukemiaNet (ELN) 2013 guidelines for treatment goals.
 2013 guidelines for treatment goals.") BOSUTINIB INDICATION Licensed / NICE TA401 (BLUETEQ required) The treatment of adult patients with chronic, accelerated and blast phase Philadelphia chromosome positive chronic myeloid leukaemia (Ph+ CML)
BOSUTINIB INDICATION Licensed / NICE TA401 (BLUETEQ required) The treatment of adult patients with chronic, accelerated and blast phase Philadelphia chromosome positive chronic myeloid leukaemia (Ph+ CML)
When to change therapy? Andreas Hochhaus Universitätsklinikum Jena, Germany
 When to change therapy? Andreas Hochhaus Universitätsklinikum Jena, Germany Chromosome 22 Chromosome 9 e1 1b m-bcr M-bcr e1 e2 b1 b5 5 3 BCR ABL 5 3 1a a2 a3 μ -bcr e19 a11 e1a2 b2a2 b3a2 e19a2 p190 bcr-abl
When to change therapy? Andreas Hochhaus Universitätsklinikum Jena, Germany Chromosome 22 Chromosome 9 e1 1b m-bcr M-bcr e1 e2 b1 b5 5 3 BCR ABL 5 3 1a a2 a3 μ -bcr e19 a11 e1a2 b2a2 b3a2 e19a2 p190 bcr-abl
ESMO Updated Guidelines & Treatment Strategies in CML-CP: Maximizing Eligibility for TFR.
 ESMO Updated Guidelines & Treatment Strategies in CML-CP: Maximizing Eligibility for TFR. Pierre Laneuville, MD, FRCP(C) McGill University Health Center, Montreal. Korea, March 2018. Disclosures Activity
ESMO Updated Guidelines & Treatment Strategies in CML-CP: Maximizing Eligibility for TFR. Pierre Laneuville, MD, FRCP(C) McGill University Health Center, Montreal. Korea, March 2018. Disclosures Activity
Current Monitoring for CML: Goals and. Jorge Cortes, MD Chief, CML & AML Section Department of Leukemia MD Anderson Cancer Center
 Current Monitoring for CML: Goals and Principles Jorge Cortes, MD Chief, CML & AML Section Department of Leukemia MD Anderson Cancer Center Survival in Early Chronic Phase CML MDACC 2009 The Philadelphia
Current Monitoring for CML: Goals and Principles Jorge Cortes, MD Chief, CML & AML Section Department of Leukemia MD Anderson Cancer Center Survival in Early Chronic Phase CML MDACC 2009 The Philadelphia
Chronic Myeloid Leukemia
 NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ) Version 1.2018 July 26, 2017 NCCN.org Continue Version 1.2018, 07/26/17 National Comprehensive Cancer Network, Inc. 2017, All rights reserved.
NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ) Version 1.2018 July 26, 2017 NCCN.org Continue Version 1.2018, 07/26/17 National Comprehensive Cancer Network, Inc. 2017, All rights reserved.