Minimally Invasive Gynecologic Surgery: Laparoscopic Treatment of the Pelvic Mass
|
|
|
- Elaine Jennings
- 5 years ago
- Views:
Transcription

1 Minimally Invasive Gynecologic Surgery: Laparoscopic Treatment of the Pelvic Mass R. Wendel Naumann, M.D. Director, Minimally Invasive Surgery in Gyn Oncology Carolinas Medical Center Charlotte, NC 1 Conflicts of Interest I have no conflicts of interest relevant to this talk Other relationships - Alexion - consulting - Merck - consulting/research - Novocure - consulting - Biodesix - consulting - Genentech - consulting/speaker s bureau - Clovis - consulting - Janssen - consulting 2
2 Objectives Ovarian cancer screening Risk reducing surgery What masses are appropriate for laparoscopy Risk of spillage Which masses can be safely removed with stroma sparing techniques versus oophorectomy Techniques for removal Laparoscopic bags Hand assisted ports 3 Life is short, the art long, opportunity fleeting, experiment treacherous, judgment difficult.!! -Hippocrates! 4



3 Ovarian Cancer and Age Percent! Rate per 100,000! 60!!!! 45!!!! 30!!!! 15!!!! 0! Yancik R, A J Obstet Gynecol 154:638, 1986" 5 5! United Kingdom Collaborative Trial of Ovarian Cancer Screening (UKCTOCS) Goal was to develop an acceptable Screening algorithm with minimal surgical complications - NORMAL risk women Trial run from April 2001 through September 2005 Very large trial - 1,243,282 screened - 202,638 randomized Randomized to three arms - Control Group - Ultrasound only - Multimodal Screening Jacobs IJ, Lancet 387:945,

4 Patterns of Ca-125 Skates SJ, J Clin Oncol 21:206s, Stage Migration from Multimodal Screening Jacobs IJ, Lancet 387:945,

5 Multimodal Screening Mortality Compared to Control Mortality reduction: 0 7 years 8% (-27, 43) Mortality reduction: 7 14 years 28% ( -3, 49) 16% reduction Jacobs IJ, Lancet 387:945, Based on the FDA s review of available clinical data from ovarian cancer screening trials and recommendations from healthcare professional societies and the U.S. Preventive Services Task Force, available data do not demonstrate that currently available ovarian cancer screening tests are accurate and reliable in screening asymptomatic women for early ovarian cancer. 10
6 Model versus prediction Start age = 61, 9 screens, 14 years follow-up Actual Mortality Difference = 11% Predicted Mortality Difference = 10% Naumann RW, unpublished" 11 Screening model Markov model based on stage shift seen in UKCTOCS trial Model accurately predicted mortality from ovarian cancer Adjusted for different stages seen in screening Looked at screening starting at age 50 - Overall 5% reduction in ovarian cancer mortality could prevent 51 deaths per 100,000 women screened for 20 yr - Not cost effective Screening costs alone would be greater than $650,000/life yr Naumann RW, unpublished" 12
:1462, 2011\"")
7 The Origin of Ovarian Cancer 13 Reactive Oxygen Species are Indispensable in Ovulation" Ovulation involves ROS LH stimulation is proinflammatory ROS may activate EGFR inhibition of EGFRspecific phosphatases MAPK phosphorylation and activation of MEK signaling Shkolnik K, PNAS 108(4):1462, 2011" 14

:5284, 2008\" 15 Is the Fallopian Tube to Blame?")
8 Mechanism for Transformation" Genotoxic stress increases risk with DNA repair deficiency also explains tumor heterogeneity" Precursor in fallopian tube" Tubal (retrograde flow)" Ovulatory cycles increases genotoxic stress" Levanon K, J Clin Oncol 26(3):5284, 2008" 15 Is the Fallopian Tube to Blame?" Kurman RJ, Am J Surg Path 34(3):433, 2010" 16

9 Progression to High Grade (Type II) Ovarian Cancer" Karst AM, Gynecol Oncol 123:5, 2011" 17 Salpingectomy: Post Reproduction" Most effective tubal sterilization 1,5 No negative impact on ovarian function 2 Can reduce incidence of: Serous cancer 3 Surgery for tubal disease 8% after TL 4 1. Peterson et al, AJOG, 1996 (US Collab. Review of Sterilization) Seidhoff et al, JMIG, 2013 Lessard-Anderson et al, SGO, 2013 Morse et al, AJOG, 2002 Bartz, et al, Rev Obstet Gynecol,
 Hysterectomy and BSO (n = 37,348) Tubal ligation (n = 81,658) Unilateral Salpingectomy (n = 472,263) Bilateral")
10 Swedish Cancer Registry Data Compared 251,000 women after Gyn procedures to 5.5 million women between 1973 and Included women after Hysterectomy (n = 98,026) Hysterectomy and BSO (n = 37,348) Tubal ligation (n = 81,658) Unilateral Salpingectomy (n = 472,263) Bilateral Salpingectomy (n = 70,566) - Did not include women hysterectomy and salpingectomy (n = 2,646) Registry captures 99% of cancers and 95% cause of death Falconer H, JNCI 107(2): dju410, 2015" 22 RR of Ovarian Cancer Swedish Cancer Registry Data Falconer H, JNCI 107(2): dju410, 2015" 23



11 SGO Statement" 24! BRCA1 Carriers" Surgery is recommended at age 35 for BRCA1 but there is some risk before! Finch APM, J Clin Oncol, 32:1, 2014! 25!


12 BRCA2 Carriers" Surgery is recommended at age 40 for BRCA2 but cancers are much later! Finch APM, J Clin Oncol, 32:1, 2014! 26! Surgery for Risk Reduction" Skeletonize the ovarian vessels for complete removal" open the retroperitoneal space!!" Inspect peritoneal surfaces and biopsy anything suspicious" Peritoneal washings" Identify patient as high risk to pathology" step section of entire fallopian tube " Remove the adnexa in a bag to preserve epithelium" There is a chance of finding cancer at the time of surgery - particularly in older women with BRCA1" May still be at risk for peritoneal cancer (RR = )" 27!

13 Management of a Pelvic Mass 33 ACOG/SGO Referral Guidelines 34

14 ACOG/SGO Referral Guidelines Updates in Orange" 35 When do you Refer a Patient to a Gynecologic Oncologist? When the risk of malignancy exceeds the 5-10% range When you do not feel confident that you can remove the mass without abdominal spillage if there is any risk of malignancy When you are likely to encounter difficult surgical conditions that might make you open Multiple medical problems Multiple previous surgeries 36
15 Work-up for a Pelvic Mass ACOG/SGO Referral Guidelines Evaluation of Pelvic Mass - Obtain Ca-125 and CEA - Other tumor markers when appropriate AFP, bhcg, inhibin Transvaginal ultrasound is the most cost effect test in evaluation of pelvic mass Routine CT scan or MRI NOT indicated except in the cases where malignancy is being evaluated 37 ACOG/SGO Referral Guidelines for a Pelvic Mass Premenopausal Ca-125 > 200 Markedly elevated! Ascites! Evidence of abdominal or distant metastasis! Family history of breast or ovarian cancer (1st degree relative)! Postmenopausal Same as Premenopausal with ANY elevation of Ca-125! Nodular or fixed mass! Perimenarchal with elevated tumor markers! ACOG Practice Bulletin, Number 83, July 2007! Gynecol Oncol 78(3):S5, 2000! 38
 Premenopausal with Cancer! 44% (263/597) Postmenopausal with Cancer! Sensitivity! PPV! NPV!")

16 Validation of ACOG Guidelines at a Single Institution" Reviewed 837 patients at Mayo Clinic! 20% (48/240) Premenopausal with Cancer! 44% (263/597) Postmenopausal with Cancer! Sensitivity! PPV! NPV! Premenopausal! Early 77%! - 56%! Late - 92%! 40%! 92%! Postmenopausal! Early 93%! - 80%! Late - 98%! 60%! 93%! Dearking AC, Obstet Gynecol 110:841, 2007! 40 U/S Morphology Index! DePriest PD, Gynecol Oncol 55(2):174, 1994! 41
:174, 1994!")
17 Kentucky Morphology Index High Risk MI 5 42 U/S Morphology Index Statistical Performance of the Morphology Index Score Using a Value of 5 as Indicative of Malignancy! Sensitivity! 0.89! Specificity! 0.73! Positive predictive value! 0.46! Negative predictive value! 0.96! DePriest PD, Gynecol Oncol 55(2):174, 1994! 43
18 Observation can be justified in an asymptomatic woman with a normal Ca-125 in the absence of transvaginal ultrasound findings suspicious for cancer. ACOG Practice Bulletin #174 November, 2016" 44 Proportion of Borderline and Ovarian Malignancy presenting as Simple (Unilocular) Cysts Borderline! Ovarian Ca! Total! Exacoustos! /33 0/82 3/115 Fruscella! /113 0/0 4/113 Valentin! /1 0/27 0/28 Gramellini! /5 0/15 0/20 Valentin! /5 0/19 0/24 Hata! /9 0/42 0/51 Jokubkiene! /6 0/21 0/27 Granberg! /39 Valentin! /186 6/764 7/417 TOTAL! 12/358 (3.4%) 6/970 (0.6%) 18/1367 (1.3%) Valentin L, Ultrasound Obstet Gynecol 41:80, 2013" 45


19 Unilateral Cysts in Post-Menopausal Women UK screened 15,106 women > 50 yo - 18% developed unilateral cysts Ovarian Cancer - 0.8% developed cancer - All had changes in cyst at the time of diagnosis F/U not standard - Some recommend stopping f/u after 1 year if no solid components and 2 years with solid components (no data - long term f/u unknown) Modesitt SC Obstet Gynecol 102(3):594, 2003" 46 Management of Ovarian Torsion If fertility preservation is the goal reduction of torsion with cystectomy should be performed In most cases, the residual ovary will regain perfusion and remain viable Despite evidence of necrosis and ischemia at the time of surgical exploration, ovarian function will be preserved in 90% of cases Ovarian fixation is controversial, but may be considered, especially if torsion is recurrent 47

20 New Tumor Markers 48 Markers to Predict Ovarian Cancer FDA Approved for triage prior to surgery" ACOG Practice bulletin #174, November, 2016" 49

21 Ca-125 Antigen derived from coelomic and mullerian epithelium Normal < 35 U/ml Expressed in 80% of non-mucinous epithelial cancers less often expressed in clear cell or mucinous cancer Only 50% of patients with stage I ovarian cancer will have an elevated level FDA approved from treatment monitoring but not preoperative evaluation or screening often false positive elevation 50 Tumor Markers for Pelvic Mass Moore RG, Gynecol Oncol 108:402, 2007! 51


22 HE4 Antigen derived from Human Epididymis Protein Product of the WFDC2 (HE4) gene which is over expressed in ovarian cancer 93% serous 100% endometrioid 50% clear cell Normal 150 pm FDA approval for monitoring cancer treatment FDA approved algorithm for pre-operative evaluation or screening in 2011 Dapkin R, Cancer Res 65:2162, 2005! 53 Logistic Regression Algorithm Pooled data from two Pilot Studies CA 125II derived using Abbott ARCHITECT CA 125II measured directly on WIHRI samples, but imputed for Boston samples Final algorithm 54


23 Stratification of Patients with Pelvic Mass using a Logistic Regression Algorithm Post-menopausal women only 55 Stratification of Patients with Pelvic Mass using a Logistic Regression Algorithm Pre-Menopausal Women 56

24 OVA-1 OVA-1 - Qualitative assay of 5 tumor markers Approved for pre-operative diagnosis - over 18 years - pelvic mass prior to surgery when malignancy is not suspected - cost ~$650 NOT to be used as a screening test 57 Components of OVA-1 58


25 Scoring Algorithm value from 0-10 Cutoff value - Premenopausal less than 5 = low risk 5 or greater = high risk - Postmenopausal less than 4.4 = low risk 4.4 or greater = high risk 59 Ova1 Score and Risk of Malignancy Risk Malignancy! Bristow R, Gynecol Oncol 128(2):252, 2013" Ova1 Score! 61
26 OVA-1 Sensitivity Subjects! n! OVA-1! Ca-125 (II)! All Cancers! 161! 92%! 69%! All Ov Ca! 96! 99%! 82%! Early EOC! 41! 98%! 66%! Premenopausal EOC! 14! 93%! 36%! Ueland et al, 13th Annual International Gynecologic Cancer Society meeting (October, 2010, Prague)" 62 Ova-1 Assessment by Menopausal Status Premenopausal! Postmenopausal! Preop! Preop + Ova-1! Preop! Preop + Ova-1! Sensitivity! 60%! 89%! 81%! 98%! Specificity! 83%! 40%! 74%! 28%! NPV! 90%! 94%! 85%! 96%! PPV! 46%! 26%! 69%! 49%! NPV = negative predictive value, PPV = positive predictive value" OVA1 Product Insert" 63
27 Ova500 Trial 494 pts from 27 centers 92% sensitivity - 94% in premenopausal women - 91% in stage I/II Identified 78/84 women with early ovarian cancer - NPV = 98% - 51% specificity Bristow R, Gynecol Oncol 128(2):252, 2013! 64 Overa Second generation test - Replaced 2 markers with HE4 and FSH Performance (testing OV500 sample) - NPP = 97.7% - Sensitivity = 93.5% - Specificity Alone = 69.1% (277/401) With clinical impression = 64.8% (260/401) - PPV Alone = 40.4% (84/208) With clinical impression = 37.9% (86/277) Reduces False (+) by ~ 1/3 67
28 Laparoscopic Management 68 When Should you approach a mass laparoscopically? Anytime you can remove the mass without excessive risk of spillage or laparotomy MUST carefully document the lack or presence of spillage Should be confident that you will not need a laparotomy If the risk of malignancy is low (pre referral guidelines) You can get the patient in to see a gyn oncologist quickly if the mass is malignant 69

29 Laparoscopy with Ovarian Mass DON Ts Don t rupture mass Don t remove mass without a bag Don t leave a piece of the ovary Don t open if Gynecologic Oncology not available 70 Predictors of Clinical Outcome in the Management of Laparoscopic Masses n = 396! Overall Rate of Rupture = 25%! Conversion Rate = 25%! Havrilesky LJ, Obstet Gynecol 102(2):243, 2003! 71
30 Randomized Trials of Laparotomy vs. Laparoscopy for Pelvic Masses n! OR Time (min)! Scope Open! Rupture*! Scope Open! Fanfani! 2004! 100! 72! 87! 6%! 2%! Yuen! 1997! 102! 59! 52! 27%! 30%! Deckardt! 1994! 192! 97! 116! Not# Reported! *Rupture rate for Fanfani excluded endometrosis! 72 Germ Cell Tumors" All germ cell tumors will require treatment except" Stage IA Dysgerminoma" 30% recurrence rate but salvage rate very high" Stage IA grade 1 Immature Teratoma" Rupture does not change number of cycles of chemotherapy given" The tumors CAN be confused with epithelial tumors!!! (especially in the middle of the night)" BE CONSERVATIVE IN YOUNG WOMEN!" 73

31 Effect of Surgical Rupture on Prognosis in Stage I Ovarian Cancer # Study! n! % Ruptured! Comments! Findings! Sevelda, P# 1989! Dembo, A# 1990! de la Cuesta, RS# 1994! 60! N.S.! All staged# Treated with WART! 100! 24%! Not staged# Rupture rate higher for Gr2/3! 56! 35%! Not staged# Only 35% ruptured got chemo! No difference from rupture! Adhesions, not rupture, appear to increase RR! Increase in RR with rupture! Kodama, S# 1997! Mizuno, M# 2003! 181! 25%! Incompletely staged in 75%! Rupture significant in univaraiate but not multivariate analysis! 214! 35%! Most not staged/ Difference inicr only in mucinous and endometrioid! Ruptured tumors intermediate between I A/B and IC! Bakkum-Gamez, JN# 2009! 161! 24%! All staged# No multivariate analysis! Univariant higher RR with rupture! Stage I A/B not different from ICR! FIGO Staging System for Ovarian Cancer 76
!")
32 Summary of Risk: Meta-Analysis! IC3 is worse than IC1! HR 1.47 ( )! IC1 is worse than IA! HR 2.41 ( )! IC1 is no different that IA if patients are completely staged and receive chemotherapy! HR 1.49 ( )! Kim, Eur J Surg Oncol 2013; 39: " 77 78
33 Survival in Stage I Granulosa Cell Tumor with and without Rupture" Non-ruptured (n = 127)! Ruptured (n = 42)! P = in Multivariate analysis! Bjorkholm E, Gynecol Oncol 11:261, 1981! 79 Tumor Rupture No convincing evidence that tumor rupture changes prognosis in epithelial and germ cell tumors May change stage May change treatment recommendation for chemotherapy in low grade malignancies New bulletin states emphatically that risk is higher May change outcome in granulosa cell tumors No conclusive evidence that the risk of rupture is significantly higher with laparoscopy surgical morbidity is definitely lower 80
34 Atypically Proliferating Tumor of Uncertain Malignant Potential (Borderline Tumors) 81 Overview of Conservative Surgery Ovarian Borderline Tumors Patients! 2496! Recurrence! 140! 5.6%! Death! 5! 0.2%! Fertility! Desire! 222! Conceive! 132! 59%! Swanton A, Eupean J Obstet Gynecol Repro Bio 135:3, 2007! 83


35 Risk of Recurrence of Borderline Tumors by Approach and Surgery Poncelet C, Ann Surg Oncol 13(4):565, 2006! 84 Take Home Message for Borderline Ovarian Tumors Recurrence rate is higher after cystectomy compared to oophorectomy - risk of rupture higher with cystectomy risk of recurrence higher after rupture - Most recurrences are borderline - Surgery should be guided by size of tumor appearance of contralateral ovary patient wishes Staging surgery may be prognostic but does not appear to be therapeutic - Omentectomy optimal - Nodal Dissection not necessary 85
36 Conservative Management of Ovarian Cancer 86 Data on Conservative Therapy for Early Ovarian Cancer (<40 yo) Stage IA! Total# n! Conservative Surgery! n! %! Grade 1! 39! 24! 62%! Grade 2! 13! 8! 61%! Grade 3! 7! 4! 57%! Stage IB! 5! 1! 20%! Stage IC! 35! 19! 54%! 99! 56! 56%! Colombo H, Gynecol Oncol 55(3 pt 2):S47, 1994! 87
37 Recurrence after Conservative Therapy for Early Ovarian Cancer Surgery! Conservative! Radical! #! %! #! %! Sage IA! 8%! 9%! Grade 1! 1/24! 0/15! Grade 2! 1/8! 1/5! Grade 3! 1/4! 1/3! Stage IB! 0/1! 1/4! Stage IC! 0/19! 2/16! Total! 3/56! 5%! 5/43! 12%! Colombo H, Gynecol Oncol 55(3 pt 2):S47, 1994! 88 Data on Conservative Therapy for Early Ovarian Cancer Reproductive Status! No. Pts! No attempt at conception! 39! Attempt at conception! 17! Problem-free! 17! Failure! 0! Colombo H, Gynecol Oncol 55(3 pt 2):S47, 1994! 89
38 NCCN Guidelines for Ovarian Cancer In stage I disease minimally invasive surgery can be considered should be performed by experienced gyn oncologists Adequate para-aortic nodal sampling required For patients with apparent early stage disease (germ cell, LMP, sex cord stromal tumors, and early ovarian cancer) can be treated by USO and comprehensive surgical staging Primary invasive mucinous tumors of the ovary are uncommon, thus the upper and lower GI tract should be examined to r/o an occult GI primary with ovarian metastases Appendectomy should be performed in all mucinous tumors and considered in all patients with epithelial malignancies due to the frequent occult involvement of the appendix 90 Removal of the Mass By three methods we may learn wisdom: First, by reflection, which is noblest; Second, by imitation, which is easiest; and third by experience, which is the bitterest. -Confucius 98


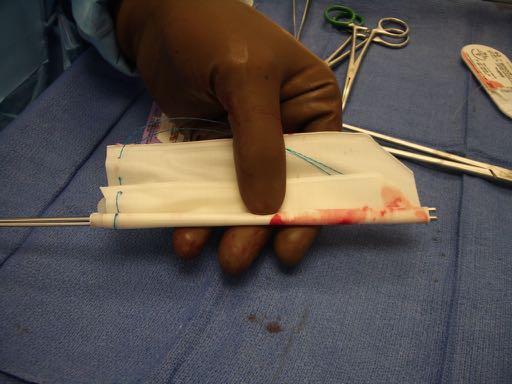

39 Spleen Bags 99 Spleen Bag Introducer 100


40 Anchor Bag cm Complex Mass in a Postmenopausal Woman!



41 18 cm Complex Pelvic Mass 104 Large Containment Bag 105


42 106 Large Pelvic Mass in a 28 YO Woman 107





43 Large Pelvic Mass in a 28 YO Woman 108 Hand Assisted Access 109

44 Port Placement for Very Large Mass 8 cm Hand Assist Port! 110


45 After Right Salpingo-oophorectomy 112 Post-op 113

46 There is nothing like a challenge to bring out the best in man. - Sir Sean Connery 120 Ginormous Mass 121
47 Can you just aspirate a simple cyst? Can be done if very low risk - Especially if high risk surgery Recurrence rate - Nikolaou % premenpausal 25% postmenopausal - Garcia-Tejedor % Minimally invasive excision preferrable 122 Ginormous Mass!
Adnexal Masses in Menopausal Women Surgery or Surveillance?
 Adnexal Masses in Menopausal Women Surgery or Surveillance? FREDTALK IDEASWORTHSPREADING Disclosure I am a member of Vermillion s Speakers Bureau I am NOT a paid consultant for Vermillion Inc. nor do I
Adnexal Masses in Menopausal Women Surgery or Surveillance? FREDTALK IDEASWORTHSPREADING Disclosure I am a member of Vermillion s Speakers Bureau I am NOT a paid consultant for Vermillion Inc. nor do I
SCREENING FOR OVARIAN CANCER DR MACİT ARVAS
 SCREENING FOR OVARIAN CANCER DR MACİT ARVAS Ovarian cancer is the leading cause of death from gynecologic malignancy In 2008, ovarian cancer was the seventh common cancer in women worldwide There were
SCREENING FOR OVARIAN CANCER DR MACİT ARVAS Ovarian cancer is the leading cause of death from gynecologic malignancy In 2008, ovarian cancer was the seventh common cancer in women worldwide There were
Adnexal Masses in Menopausal Women
 Adnexal Masses in Menopausal Women Surgery or Surveillance? Disclosure Frederick R. Ueland, MD Professor and Director Division of Gynecologic Oncology University of Kentucky I have no financial disclosures
Adnexal Masses in Menopausal Women Surgery or Surveillance? Disclosure Frederick R. Ueland, MD Professor and Director Division of Gynecologic Oncology University of Kentucky I have no financial disclosures
OVARIAN CARCINOMA Immune Therapy. Antibodies to CA-125 (Ovarex) Vaccine therapy
 Vaccine therapy") OVARIAN CARCINOMA Immune Therapy Antibodies to CA-125 (Ovarex) Vaccine therapy OVARIAN CARCINOMA Targeted Therapy Bevacizumab (Avastin): GOG- 218 Anti-VEGF, angiogenesis inhibitor TLK 286 (Telcyta): Glutathione
OVARIAN CARCINOMA Immune Therapy Antibodies to CA-125 (Ovarex) Vaccine therapy OVARIAN CARCINOMA Targeted Therapy Bevacizumab (Avastin): GOG- 218 Anti-VEGF, angiogenesis inhibitor TLK 286 (Telcyta): Glutathione
Is It Time To Implement Ovarian Cancer Screening?
 Is It Time To Implement Ovarian Cancer Screening? Prof Dr Samet Topuz Istanbul Medıcal Faculty Department Of Obstetrics and Gynecology ESGO Prevention in Gynaecological Malignancies September 08 2016 Antalya
Is It Time To Implement Ovarian Cancer Screening? Prof Dr Samet Topuz Istanbul Medıcal Faculty Department Of Obstetrics and Gynecology ESGO Prevention in Gynaecological Malignancies September 08 2016 Antalya
OVARIAN CANCER Updates in Screening, Early Detection and Prevention
 UW MEDICINE SUSAN PATRICIA TECK MEMORIAL LECTURE October 2017 OVARIAN CANCER Updates in Screening, Early Detection and Prevention BARBARA GOFF, MD Seattle Gynecologic Society March 2018 OVARIAN CANCER
UW MEDICINE SUSAN PATRICIA TECK MEMORIAL LECTURE October 2017 OVARIAN CANCER Updates in Screening, Early Detection and Prevention BARBARA GOFF, MD Seattle Gynecologic Society March 2018 OVARIAN CANCER
Unexpected Gynecologic Findings at Laparotomy. Susan A. Davidson, MD University of Colorado, Denver School of Medicine
 Unexpected Gynecologic Findings at Laparotomy Susan A. Davidson, MD University of Colorado, Denver School of Medicine Adnexal Mass: Gyn Etiologies Uterine Leiomyomas Pregnancy Malignancy Tubal Pregnancy
Unexpected Gynecologic Findings at Laparotomy Susan A. Davidson, MD University of Colorado, Denver School of Medicine Adnexal Mass: Gyn Etiologies Uterine Leiomyomas Pregnancy Malignancy Tubal Pregnancy
Triage of Ovarian Masses. Andreas Obermair Brisbane
 Triage of Ovarian Masses Andreas Obermair Brisbane Why Triage? In ovarian cancer, best outcomes for patients can be achieved when patients are treated in tertiary centres by a multidisciplinary team led
Triage of Ovarian Masses Andreas Obermair Brisbane Why Triage? In ovarian cancer, best outcomes for patients can be achieved when patients are treated in tertiary centres by a multidisciplinary team led
Inherited Ovarian Cancer Diagnosis and Prevention
 Inherited Ovarian Cancer Diagnosis and Prevention Dr. Jacob Korach - Deputy director Gynecologic Oncology (past chair - Israeli Society of Gynecologic Oncology) Prof. Eitan Friedman - Head, Oncogenetics
Inherited Ovarian Cancer Diagnosis and Prevention Dr. Jacob Korach - Deputy director Gynecologic Oncology (past chair - Israeli Society of Gynecologic Oncology) Prof. Eitan Friedman - Head, Oncogenetics
Chapter 2: Initial treatment for endometrial cancer (including histologic variant type)
") Chapter 2: Initial treatment for endometrial cancer (including histologic variant type) CQ01 Which surgical techniques for hysterectomy are recommended for patients considered to be stage I preoperatively?
Chapter 2: Initial treatment for endometrial cancer (including histologic variant type) CQ01 Which surgical techniques for hysterectomy are recommended for patients considered to be stage I preoperatively?
Borderline Ovarian Tumours. Andreas Obermair Brisbane
 Borderline Ovarian Tumours Andreas Obermair Brisbane Definition First described in 1929 Cellular features of malignancy Cellular atypia Mitotic activity No stromal invasion An entity per se??? (or precursor
Borderline Ovarian Tumours Andreas Obermair Brisbane Definition First described in 1929 Cellular features of malignancy Cellular atypia Mitotic activity No stromal invasion An entity per se??? (or precursor
BSO, HRT, and ERT. No relevant financial disclosures
 BSO, HRT, and ERT Jubilee Brown, MD Professor & Associate Director, Gynecologic Oncology Levine Cancer Institute at the Carolinas HealthCare System Charlotte, North Carolina No relevant financial disclosures
BSO, HRT, and ERT Jubilee Brown, MD Professor & Associate Director, Gynecologic Oncology Levine Cancer Institute at the Carolinas HealthCare System Charlotte, North Carolina No relevant financial disclosures
Ovarian, Peritoneal, and Fallopian Tube Epithelial Cancer (OPT)
") Ovarian, Peritoneal, and Fallopian Tube Epithelial Cancer (OPT) ACOG District II 2 Learning Objectives At the end of this clinical presentation, obstetrician gynecologists and other women s health care
Ovarian, Peritoneal, and Fallopian Tube Epithelial Cancer (OPT) ACOG District II 2 Learning Objectives At the end of this clinical presentation, obstetrician gynecologists and other women s health care
Partners: Introductions: Dr. Carolyn Johnston Deanna Cosens & Ann Garvin. Ovarian Cancer and Primary Care July 16, :00 9:00am EST 7/16/2014
 Welcome To The Webinar Technical Support Ovarian Cancer and Primary Care July 16, 2014 8:00 9:00am EST In order to hear the presentation please call 1 (626) 544-0058, access code 167-314-644, followed
Welcome To The Webinar Technical Support Ovarian Cancer and Primary Care July 16, 2014 8:00 9:00am EST In order to hear the presentation please call 1 (626) 544-0058, access code 167-314-644, followed
IOTA and Models for Screening for Ovarian Cancer
 IOTA and Models for Screening for Ovarian Cancer Hennie Botha MARCH 2017 T H IG PY R O C F O SP EA KE R Silent Killer to Whispering Disease Listening to your body.. new, persistent, and increases in severity
IOTA and Models for Screening for Ovarian Cancer Hennie Botha MARCH 2017 T H IG PY R O C F O SP EA KE R Silent Killer to Whispering Disease Listening to your body.. new, persistent, and increases in severity
NATIONAL CLINICAL GUIDELINE INVESTIGATION AND MANAGEMENT OVARIAN CYSTS IN POSTMENOPAUSAL WOMEN
 NATIONAL CLINICAL GUIDELINE INVESTIGATION AND MANAGEMENT OF OVARIAN CYSTS IN POSTMENOPAUSAL WOMEN Institute of Obstetricians and Gynaecologists, Royal College of Physicians of Ireland and the Clinical
NATIONAL CLINICAL GUIDELINE INVESTIGATION AND MANAGEMENT OF OVARIAN CYSTS IN POSTMENOPAUSAL WOMEN Institute of Obstetricians and Gynaecologists, Royal College of Physicians of Ireland and the Clinical
GYNECOLOGIC MALIGNANCIES: Ovarian Cancer
 GYNECOLOGIC MALIGNANCIES: Ovarian Cancer KRISTEN STARBUCK, MD ROSWELL PARK CANCER INSTITUTE DEPARTMENT OF SURGERY DIVISION OF GYNECOLOGIC ONCOLOGY APRIL 19 TH, 2018 Objectives Basic Cancer Statistics Discuss
GYNECOLOGIC MALIGNANCIES: Ovarian Cancer KRISTEN STARBUCK, MD ROSWELL PARK CANCER INSTITUTE DEPARTMENT OF SURGERY DIVISION OF GYNECOLOGIC ONCOLOGY APRIL 19 TH, 2018 Objectives Basic Cancer Statistics Discuss
Staging and Treatment Update for Gynecologic Malignancies
 Staging and Treatment Update for Gynecologic Malignancies Bunja Rungruang, MD Medical College of Georgia No disclosures 4 th most common new cases of cancer in women 5 th and 6 th leading cancer deaths
Staging and Treatment Update for Gynecologic Malignancies Bunja Rungruang, MD Medical College of Georgia No disclosures 4 th most common new cases of cancer in women 5 th and 6 th leading cancer deaths
Clinical guideline Published: 27 April 2011 nice.org.uk/guidance/cg122
 Ovarian cancer: recognition and initial management Clinical guideline Published: 27 April 2011 nice.org.uk/guidance/cg122 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Ovarian cancer: recognition and initial management Clinical guideline Published: 27 April 2011 nice.org.uk/guidance/cg122 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Key Recommendations. Gynecologic management of women with inherited risk of gynecologic cancer
 Gynecologic management of women with inherited risk of gynecologic cancer C. Bethan Powell MD Kaiser Permanente Northern California Gynecologic Oncology Program Lead, Kaiser Permanente Northern California
Gynecologic management of women with inherited risk of gynecologic cancer C. Bethan Powell MD Kaiser Permanente Northern California Gynecologic Oncology Program Lead, Kaiser Permanente Northern California
Practice of Medicine-1 Ovarian Cancer Clinical Correlation
 Practice of Medicine-1 Ovarian Cancer Clinical Correlation Amir A. Jazaeri, M.D. Assistant Professor, Division of Gynecologic Oncology American Cancer Society Female Cancers 2000 Statistics Reprinted by
Practice of Medicine-1 Ovarian Cancer Clinical Correlation Amir A. Jazaeri, M.D. Assistant Professor, Division of Gynecologic Oncology American Cancer Society Female Cancers 2000 Statistics Reprinted by
Gynecologic Oncologist. Surgery Chemotherapy Radiation Therapy Hormonal Therapy Immunotherapy. Cervical cancer
 Gynecologic Oncology Pre invasive vulvar, vaginal, & cervical disease Vulvar Cervical Endometrial Uterine Sarcoma Fallopian Tube Ovarian GTD Gynecologic Oncologist Surgery Chemotherapy Radiation Therapy
Gynecologic Oncology Pre invasive vulvar, vaginal, & cervical disease Vulvar Cervical Endometrial Uterine Sarcoma Fallopian Tube Ovarian GTD Gynecologic Oncologist Surgery Chemotherapy Radiation Therapy
This policy is applicable to Commercial Products only. For BlueCHiP for Medicare, see Related Policy section.
 Medical Coverage Policy Multimarker Serum Testing Related to Ovarian Cancer EFFECTIVE DATE: 10 01 2015 POLICY LAST UPDATED: 04 17 2018 OVERVIEW This policy documents the coverage determination for Multimarker
Medical Coverage Policy Multimarker Serum Testing Related to Ovarian Cancer EFFECTIVE DATE: 10 01 2015 POLICY LAST UPDATED: 04 17 2018 OVERVIEW This policy documents the coverage determination for Multimarker
3 cell types in the normal ovary
 Ovarian tumors 3 cell types in the normal ovary Surface (coelomic epithelium) the origin of the great majority of ovarian tumors (neoplasms) 90% of malignant ovarian tumors Totipotent germ cells Sex cord-stromal
Ovarian tumors 3 cell types in the normal ovary Surface (coelomic epithelium) the origin of the great majority of ovarian tumors (neoplasms) 90% of malignant ovarian tumors Totipotent germ cells Sex cord-stromal
Protocol. Multimarker Serum Testing Related to Ovarian Cancer
 Protocol Multimarker Serum Testing Related to Ovarian Cancer (20462) Medical Benefit Effective Date: 04/01/18 Next Review Date: 01/19 Preauthorization Yes Review Dates: 01/11, 01/12, 01/13, 01/14, 01/15,
Protocol Multimarker Serum Testing Related to Ovarian Cancer (20462) Medical Benefit Effective Date: 04/01/18 Next Review Date: 01/19 Preauthorization Yes Review Dates: 01/11, 01/12, 01/13, 01/14, 01/15,
EDUCATIONAL COMMENTARY CA 125. Learning Outcomes
 EDUCATIONAL COMMENTARY CA 125 Learning Outcomes Upon completion of this exercise, participants will be able to: discuss the use of CA 125 levels in monitoring patients undergoing treatment for ovarian
EDUCATIONAL COMMENTARY CA 125 Learning Outcomes Upon completion of this exercise, participants will be able to: discuss the use of CA 125 levels in monitoring patients undergoing treatment for ovarian
Ask the Experts Obstetrics & Gynecology
 1 Management of the Adnexal Mass James H. Liu, MD, and Kristine M. Zanotti, MD June 2011 Volume 117 Issue 6 Pages 1413 28 Click Here to Read the Full Article Questions written by: Rini Banerjee Ratan,
1 Management of the Adnexal Mass James H. Liu, MD, and Kristine M. Zanotti, MD June 2011 Volume 117 Issue 6 Pages 1413 28 Click Here to Read the Full Article Questions written by: Rini Banerjee Ratan,
IMMATURE TERATOMA: SURGICAL TREATMENT
 CARAVAGGIO 10-12 MAGGIO 2010 IMMATURE TERATOMA: SURGICAL TREATMENT G. Mangili, E. Garavaglia, C. Sigismondi R VIGANO Dipartimento Materno Infantile, UF Ginecologia Oncologica IRCCS San Raffaele Milano
CARAVAGGIO 10-12 MAGGIO 2010 IMMATURE TERATOMA: SURGICAL TREATMENT G. Mangili, E. Garavaglia, C. Sigismondi R VIGANO Dipartimento Materno Infantile, UF Ginecologia Oncologica IRCCS San Raffaele Milano
Mousa. Najat kayed &Renad Al-Awamleh. Nizar Alkhlaifat
 6 Mousa Najat kayed &Renad Al-Awamleh Nizar Alkhlaifat P a g e 1 This sheet written based on record 13 on website Cover slide( 95-117 ) No need to go back to slide FALLOPIAN TUBE PATHOLOGY In general fallopian
6 Mousa Najat kayed &Renad Al-Awamleh Nizar Alkhlaifat P a g e 1 This sheet written based on record 13 on website Cover slide( 95-117 ) No need to go back to slide FALLOPIAN TUBE PATHOLOGY In general fallopian
Because ovarian cancer is usually diagnosed
 OVARIAN CANCER Recent studies shed light on early detection of but it s not a green light for routine screening. Until promising avenues of research lead further, refer women who have an adnexal mass,
OVARIAN CANCER Recent studies shed light on early detection of but it s not a green light for routine screening. Until promising avenues of research lead further, refer women who have an adnexal mass,
LAPAROSCOPY and OVARIAN CANCER
 LAPAROSCOPY and OVARIAN CANCER J. DAUPLAT Clermont-Ferrand France UNIVERSITÉ D'AUVERGNE CLERMONT 1 1 - PROPHYLACTIC OOPHORECTOMY 2 - DIAGNOSIS 3 - EARLY STAGES : STAGING 4 - ADVANCED STAGES - ASSESSMENT
LAPAROSCOPY and OVARIAN CANCER J. DAUPLAT Clermont-Ferrand France UNIVERSITÉ D'AUVERGNE CLERMONT 1 1 - PROPHYLACTIC OOPHORECTOMY 2 - DIAGNOSIS 3 - EARLY STAGES : STAGING 4 - ADVANCED STAGES - ASSESSMENT
Gynecologic Cancers are many diseases. Speaker Disclosure: Gynecologic Cancer Care in the Age of Precision Medicine. Controversies in Women s Health
 Gynecologic Cancer Care in the Age of Precision Medicine Gynecologic Cancers in the Age of Precision Medicine Controversies in Women s Health Lee-may Chen, MD Department of Obstetrics, Gynecology & Reproductive
Gynecologic Cancer Care in the Age of Precision Medicine Gynecologic Cancers in the Age of Precision Medicine Controversies in Women s Health Lee-may Chen, MD Department of Obstetrics, Gynecology & Reproductive
Corporate Medical Policy
 Corporate Medical Policy Proteomics-based Testing Related to Ovarian Cancer File Name: Origination: Last CAP Review: Next CAP Review: Last Review: proteomics_based_testing_related_to_ovarian_cancer 7/2010
Corporate Medical Policy Proteomics-based Testing Related to Ovarian Cancer File Name: Origination: Last CAP Review: Next CAP Review: Last Review: proteomics_based_testing_related_to_ovarian_cancer 7/2010
Update on Sentinel Node Biopsy in Endometrial Cancer: Feasibility, Technique, Impact
 Update on Sentinel Node Biopsy in Endometrial Cancer: Feasibility, Technique, Impact Bjørn Hagen, MD, PhD St Olavs Hospital Trondheim University Hospital Trondheim, Norway Endometrial Cancer (EC) The most
Update on Sentinel Node Biopsy in Endometrial Cancer: Feasibility, Technique, Impact Bjørn Hagen, MD, PhD St Olavs Hospital Trondheim University Hospital Trondheim, Norway Endometrial Cancer (EC) The most
Biology Response Controversies and Advances
 Biology Response Controversies and Advances in BRCA related ovarian cancer Lessons learned and future directions Michael Friedlander The Prince of Wales Hospital and Royal Hospital for Women Sydney BREAST-CANCER
Biology Response Controversies and Advances in BRCA related ovarian cancer Lessons learned and future directions Michael Friedlander The Prince of Wales Hospital and Royal Hospital for Women Sydney BREAST-CANCER
David Nunns on behalf of the Gynae Guidelines Group Date:
 Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc) Borderline tumours of the ovary management and follow-up Author: Contact Name and Job Title Directorate & Speciality
Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc) Borderline tumours of the ovary management and follow-up Author: Contact Name and Job Title Directorate & Speciality
Ovarian Cancer Includes Epithelial, Fallopian Tube, Primary Peritoneal Cancer, and Ovarian Germ Cell Tumors
 Ovarian Cancer Includes Epithelial, Fallopian Tube, Primary Peritoneal Cancer, and Ovarian Germ Cell Tumors Overview Ovarian epithelial cancer, fallopian tube cancer, and primary peritoneal cancer are
Ovarian Cancer Includes Epithelial, Fallopian Tube, Primary Peritoneal Cancer, and Ovarian Germ Cell Tumors Overview Ovarian epithelial cancer, fallopian tube cancer, and primary peritoneal cancer are
ACR Appropriateness Criteria Ovarian Cancer Screening EVIDENCE TABLE
 1. Lutz AM, Willmann JK, Drescher CW, et al. Early diagnosis of ovarian carcinoma: is a solution in sight? Radiology. 2011; 259(2):329-345. Type To review serum biomarkers and imaging tests for the early
1. Lutz AM, Willmann JK, Drescher CW, et al. Early diagnosis of ovarian carcinoma: is a solution in sight? Radiology. 2011; 259(2):329-345. Type To review serum biomarkers and imaging tests for the early
Gynecologic Cancers are many diseases. Gynecologic Cancers in the Age of Precision Medicine Advances in Internal Medicine. Speaker Disclosure:
 Gynecologic Cancer Care in the Age of Precision Medicine Gynecologic Cancers in the Age of Precision Medicine Advances in Internal Medicine Lee-may Chen, MD Department of Obstetrics, Gynecology & Reproductive
Gynecologic Cancer Care in the Age of Precision Medicine Gynecologic Cancers in the Age of Precision Medicine Advances in Internal Medicine Lee-may Chen, MD Department of Obstetrics, Gynecology & Reproductive
3 Summary of clinical applications and limitations of measurements
 CA125 (serum) 1 Name and description of analyte 1.1 Name of analyte Cancer Antigen 125 (CA125) 1.2 Alternative names Mucin-16 1.3 NLMC code To follow 1.4 Description of analyte CA125 is an antigenic determinant
CA125 (serum) 1 Name and description of analyte 1.1 Name of analyte Cancer Antigen 125 (CA125) 1.2 Alternative names Mucin-16 1.3 NLMC code To follow 1.4 Description of analyte CA125 is an antigenic determinant
Diagnosi, inquadramento clinico e chirurgia
 Tumori germinali, stromali e forme rare : stato dell arte, novità e prospettive Caravaggio 10-12 giugno 2010 Giorgia Mangili IRCCS San Raffaele Milano Diagnosi, inquadramento clinico e chirurgia SEX-CORD
Tumori germinali, stromali e forme rare : stato dell arte, novità e prospettive Caravaggio 10-12 giugno 2010 Giorgia Mangili IRCCS San Raffaele Milano Diagnosi, inquadramento clinico e chirurgia SEX-CORD
Epithelial Ovarian Cancer 8/2/2013. Tu-be or Not Tu-be: Is the Fallopian Tube the Source of Ovarian Cancer?
 Tu-be or Not Tu-be: Is the Fallopian Tube the Source of Ovarian Cancer? Ann E. Smith Sehdev, MD Director, Center for Gynecologic Pathology Cascade Pathology, Portland, Oregon Ann E. Smith Sehdev has no
Tu-be or Not Tu-be: Is the Fallopian Tube the Source of Ovarian Cancer? Ann E. Smith Sehdev, MD Director, Center for Gynecologic Pathology Cascade Pathology, Portland, Oregon Ann E. Smith Sehdev has no
Screening and prevention of ovarian cancer
 Chapter 2 Screening and prevention of ovarian cancer Prevention of ovarian carcinoma Oral contraceptive pills Use of oral contraceptive pills (OCPs) has been associated with a significant reduction in
Chapter 2 Screening and prevention of ovarian cancer Prevention of ovarian carcinoma Oral contraceptive pills Use of oral contraceptive pills (OCPs) has been associated with a significant reduction in
POLICY PRODUCT VARIATIONS DESCRIPTION/BACKGROUND RATIONALE DEFINITIONS BENEFIT VARIATIONS DISCLAIMER CODING INFORMATION REFERENCES POLICY HISTORY
 Original Issue Date (Created): October 1, 2014 Most Recent Review Date (Revised): May 20, 2014 Effective Date: October 1, 2014 POLICY PRODUCT VARIATIONS DESCRIPTION/BACKGROUND RATIONALE DEFINITIONS BENEFIT
Original Issue Date (Created): October 1, 2014 Most Recent Review Date (Revised): May 20, 2014 Effective Date: October 1, 2014 POLICY PRODUCT VARIATIONS DESCRIPTION/BACKGROUND RATIONALE DEFINITIONS BENEFIT
CA125 in the diagnosis of ovarian cancer: the art in medicine
 CA125 in the diagnosis of ovarian cancer: the art in medicine Dr Marcia Hall Consultant Medical Oncology Mount Vernon Cancer Centre Hillingdon Hospital Wexham Park Hospital Epidemiology Ovarian cancer
CA125 in the diagnosis of ovarian cancer: the art in medicine Dr Marcia Hall Consultant Medical Oncology Mount Vernon Cancer Centre Hillingdon Hospital Wexham Park Hospital Epidemiology Ovarian cancer
Ovarian Tumors. Andrea Hayes-Jordan MD FACS, FAAP Section Chief, Pediatric Surgery/Surgical Onc. UT MD Anderson Cancer Center
 Ovarian Tumors Andrea Hayes-Jordan MD FACS, FAAP Section Chief, Pediatric Surgery/Surgical Onc. UT MD Anderson Cancer Center Case 13yo female with abdominal pain Ultrasound shows huge ovarian mass Surgeon
Ovarian Tumors Andrea Hayes-Jordan MD FACS, FAAP Section Chief, Pediatric Surgery/Surgical Onc. UT MD Anderson Cancer Center Case 13yo female with abdominal pain Ultrasound shows huge ovarian mass Surgeon
General history. Basic Data : Age :62y/o Date of admitted: Married status : Married
 General history Basic Data : Age :62y/o Date of admitted:940510 Married status : Married General history Chief Complain : bilateral ovarian cyst incidentally being found out during pap smear. Present Illness
General history Basic Data : Age :62y/o Date of admitted:940510 Married status : Married General history Chief Complain : bilateral ovarian cyst incidentally being found out during pap smear. Present Illness
Multimodal approach to predict ovarian malignancy prior to laparoscopy
 2017; 3(2): 149-153 ISSN Print: 2394-7500 ISSN Online: 2394-5869 Impact Factor: 5.2 IJAR 2017; 3(2): 149-153 www.allresearchjournal.com Received: 24-12-2016 Accepted: 25-01-2017 Dr. Juhi Bhatti Dr. Shriraj
2017; 3(2): 149-153 ISSN Print: 2394-7500 ISSN Online: 2394-5869 Impact Factor: 5.2 IJAR 2017; 3(2): 149-153 www.allresearchjournal.com Received: 24-12-2016 Accepted: 25-01-2017 Dr. Juhi Bhatti Dr. Shriraj
Pathology of Ovarian Tumours. Dr. Jyothi Ranganathan MD ( Path) AFMC Pune PDCC (Cytopathology) PGI Chandigarh
 AFMC Pune PDCC (Cytopathology) PGI Chandigarh") Pathology of Ovarian Tumours Dr. Jyothi Ranganathan MD ( Path) AFMC Pune PDCC (Cytopathology) PGI Chandigarh Outline Incidence Risk factors Classification Pathology of tumours Tumour markers Prevention
Pathology of Ovarian Tumours Dr. Jyothi Ranganathan MD ( Path) AFMC Pune PDCC (Cytopathology) PGI Chandigarh Outline Incidence Risk factors Classification Pathology of tumours Tumour markers Prevention
Both type I and type II tumors develop from extraovarian tissue that implants on the ovary. Both for LGSC and HGSC, the fallopian tube appears to be
 Recent studies have led to the development of a new paradigm for the pathogenesis and origin of EOC, based on a dualistic model of carcinogenesis that divides EOC into 2 broad categories designated types
Recent studies have led to the development of a new paradigm for the pathogenesis and origin of EOC, based on a dualistic model of carcinogenesis that divides EOC into 2 broad categories designated types
Disclosure. Objectives
 Charles A. Leath, III, MD, MSPH Associate Professor University of Alabama at Birmingham Disclosure I have no potential financial or other conflicts of interest. The view(s) expressed herein are those of
Charles A. Leath, III, MD, MSPH Associate Professor University of Alabama at Birmingham Disclosure I have no potential financial or other conflicts of interest. The view(s) expressed herein are those of
Is CA-125 the Leading Biomarker in Determining Early-Onset Ovarian Cancer Diagnosis in 2016?
 University of Rhode Island DigitalCommons@URI Senior Honors Projects Honors Program at the University of Rhode Island 2016 Is CA-125 the Leading Biomarker in Determining Early-Onset Ovarian Cancer Diagnosis
University of Rhode Island DigitalCommons@URI Senior Honors Projects Honors Program at the University of Rhode Island 2016 Is CA-125 the Leading Biomarker in Determining Early-Onset Ovarian Cancer Diagnosis
RESEARCH ARTICLE. Hariyono Winarto*, Bismarck Joel Laihad, Laila Nuranna. Abstract. Introduction
 DOI:http://dx.doi.org/10.7314/APJCP.2014.15.5.1949 RESEARCH ARTICLE Modification of Cutoff Values for HE4, CA125, the Risk of Malignancy Index, and the Risk of Malignancy Algorithm for Ovarian Cancer Detection
DOI:http://dx.doi.org/10.7314/APJCP.2014.15.5.1949 RESEARCH ARTICLE Modification of Cutoff Values for HE4, CA125, the Risk of Malignancy Index, and the Risk of Malignancy Algorithm for Ovarian Cancer Detection
MPH Quiz. 1. How many primaries are present based on this pathology report? 2. What rule is this based on?
 MPH Quiz Case 1 Surgical Pathology from hysterectomy performed July 11, 2007 Final Diagnosis: Uterus, resection: Endometrioid adenocarcinoma, Grade 1 involving most of endometrium, myometrial invasion
MPH Quiz Case 1 Surgical Pathology from hysterectomy performed July 11, 2007 Final Diagnosis: Uterus, resection: Endometrioid adenocarcinoma, Grade 1 involving most of endometrium, myometrial invasion
Joshua Cohen MD Gynecologic Oncology Fellow UCLA/Cedars-Sinai Medical Center
 Joshua Cohen MD Gynecologic Oncology Fellow UCLA/Cedars-Sinai Medical Center No conflicts of interest to disclose Educational Objectives Recognize challenges in current paradigms associated with biomarker
Joshua Cohen MD Gynecologic Oncology Fellow UCLA/Cedars-Sinai Medical Center No conflicts of interest to disclose Educational Objectives Recognize challenges in current paradigms associated with biomarker
Gynecologic Cancer Surveillance and Survivorship: Informing Practice and Policy
 Gynecologic Cancer Surveillance and Survivorship: Informing Practice and Policy Stephanie Yap, M.D. University Gynecologic Oncology Northside Cancer Institute Our Learning Objectives Review survival rates,
Gynecologic Cancer Surveillance and Survivorship: Informing Practice and Policy Stephanie Yap, M.D. University Gynecologic Oncology Northside Cancer Institute Our Learning Objectives Review survival rates,
Significance of Ovarian Endometriosis on the Prognosis of Ovarian Clear Cell Carcinoma
 ORIGINAL STUDY Significance of Ovarian Endometriosis on the Prognosis of Ovarian Clear Cell Carcinoma Jeong-Yeol Park, MD, PhD, Dae-Yeon Kim, MD, PhD, Dae-Shik Suh, MD, PhD, Jong-Hyeok Kim, MD, PhD, Yong-Man
ORIGINAL STUDY Significance of Ovarian Endometriosis on the Prognosis of Ovarian Clear Cell Carcinoma Jeong-Yeol Park, MD, PhD, Dae-Yeon Kim, MD, PhD, Dae-Shik Suh, MD, PhD, Jong-Hyeok Kim, MD, PhD, Yong-Man
Cancer arising from Endometriosis and Its Clinical implications
 Cancer arising from Endometriosis and Its Clinical implications 1) Nezhat F, Cohen C, Rahaman J, Gretz H, Cole P, Kalir T. Comparative immunohistochemical studies of bcl-2 and p53 proteins in benign
Cancer arising from Endometriosis and Its Clinical implications 1) Nezhat F, Cohen C, Rahaman J, Gretz H, Cole P, Kalir T. Comparative immunohistochemical studies of bcl-2 and p53 proteins in benign
Endometrial Cancer. Incidence. Types 3/25/2019
 Endometrial Cancer J. Anthony Rakowski DO, FACOOG MSU SCS Board Review Coarse Incidence 53,630 new cases yearly 8,590 deaths yearly 4 th most common malignancy in women worldwide Most common GYN malignancy
Endometrial Cancer J. Anthony Rakowski DO, FACOOG MSU SCS Board Review Coarse Incidence 53,630 new cases yearly 8,590 deaths yearly 4 th most common malignancy in women worldwide Most common GYN malignancy
Current Concept in Ovarian Carcinoma: Pathology Perspectives
 Current Concept in Ovarian Carcinoma: Pathology Perspectives Rouba Ali-Fehmi, MD Professor of Pathology The Karmanos Cancer Institute, Wayne State University School of Medicine Current Concept in Ovarian
Current Concept in Ovarian Carcinoma: Pathology Perspectives Rouba Ali-Fehmi, MD Professor of Pathology The Karmanos Cancer Institute, Wayne State University School of Medicine Current Concept in Ovarian
Epithelial Ovarian Cancer
 Epithelial Ovarian Cancer GYNE/ONC Practice Guideline Dr. Alex Hammond Dr. Ian Kerr Dr. Akira Sugimoto Dr. Stephen Welch Kay Faroni Christine Gawlik Kerri Thornton Approval Date: This guideline is a statement
Epithelial Ovarian Cancer GYNE/ONC Practice Guideline Dr. Alex Hammond Dr. Ian Kerr Dr. Akira Sugimoto Dr. Stephen Welch Kay Faroni Christine Gawlik Kerri Thornton Approval Date: This guideline is a statement
L/O/G/O. Ovarian Tumor. Xiaoyu Niu Obstetrics and Gynecology Department Sichuan University West China Second Hospital
 L/O/G/O Ovarian Tumor Xiaoyu Niu Obstetrics and Gynecology Department Sichuan University West China Second Hospital Essentials classification of ovarian tumor clinical manifestation of ovarian tumor metastatic
L/O/G/O Ovarian Tumor Xiaoyu Niu Obstetrics and Gynecology Department Sichuan University West China Second Hospital Essentials classification of ovarian tumor clinical manifestation of ovarian tumor metastatic
Institute of Pathology First Faculty of Medicine Charles University. Ovary
 Ovary Barrett esophagus ph in vagina between 3.8 and 4.5 ph of stomach varies from 1-2 (hydrochloric acid) up to 4-5 BE probably results from upward migration of columnar cells from gastroesophageal junction
Ovary Barrett esophagus ph in vagina between 3.8 and 4.5 ph of stomach varies from 1-2 (hydrochloric acid) up to 4-5 BE probably results from upward migration of columnar cells from gastroesophageal junction
See the latest estimates for new cases of ovarian cancer and deaths in the US and what research is currently being done.
 About Ovarian Cancer Overview and Types If you have been diagnosed with ovarian cancer or are worried about it, you likely have a lot of questions. Learning some basics is a good place to start. What Is
About Ovarian Cancer Overview and Types If you have been diagnosed with ovarian cancer or are worried about it, you likely have a lot of questions. Learning some basics is a good place to start. What Is
Newton Wellesley Hospital 2013
 Newton Wellesley Hospital 20 Standard 4.6 Assessment and Evaluation of Treatment Planning Endometrial Cancer Each year a physician member of the cancer committee conducts a study to ensure that diagnostic
Newton Wellesley Hospital 20 Standard 4.6 Assessment and Evaluation of Treatment Planning Endometrial Cancer Each year a physician member of the cancer committee conducts a study to ensure that diagnostic
Focus on... Ovarian cancer. HE4 & ROMA score
 Focus on... Ovarian cancer HE4 & ROMA score Ovarian cancer in the world* Accounting for around 4% of all cancers diagnosed in women The estimated World age-standardised incidence rate for the more developed
Focus on... Ovarian cancer HE4 & ROMA score Ovarian cancer in the world* Accounting for around 4% of all cancers diagnosed in women The estimated World age-standardised incidence rate for the more developed
Risk Reduction management for Ovarian Cancer in Women with BRCA1/2 Mutation
 Risk Reduction management for Ovarian Cancer in Women with BRCA1/2 Mutation Global Breast Cancer Conference 2018 2018. 4. 6 (Fri) Songdo, Incheon, Korea Hereditary Gynecologic Cancer Clinic Precision Medicine
Risk Reduction management for Ovarian Cancer in Women with BRCA1/2 Mutation Global Breast Cancer Conference 2018 2018. 4. 6 (Fri) Songdo, Incheon, Korea Hereditary Gynecologic Cancer Clinic Precision Medicine
RESEARCH ARTICLE. Usanee Chatchotikawong 1, Irene Ruengkhachorn 1 *, Chairat Leelaphatanadit 1, Nisarat Phithakwatchara 2. Abstract.
 RESEARCH ARTICLE 8-year Analysis of the Prevalence of Lymph Nodes Metastasis, Oncologic and Pregnancy Outcomes in Apparent Early-Stage Malignant Ovarian Germ Cell Tumors Usanee Chatchotikawong 1, Irene
RESEARCH ARTICLE 8-year Analysis of the Prevalence of Lymph Nodes Metastasis, Oncologic and Pregnancy Outcomes in Apparent Early-Stage Malignant Ovarian Germ Cell Tumors Usanee Chatchotikawong 1, Irene
Springer Healthcare. Understanding and Diagnosing Ovarian Cancer. Concise Reference: Krishnansu S Tewari, Bradley J Monk
 Concise Reference: Understanding and Diagnosing Ovarian Cancer Krishnansu S Tewari, Bradley J Monk Extracted from: The 21 st Century Handbook of Clinical Ovarian Cancer Published by Springer Healthcare
Concise Reference: Understanding and Diagnosing Ovarian Cancer Krishnansu S Tewari, Bradley J Monk Extracted from: The 21 st Century Handbook of Clinical Ovarian Cancer Published by Springer Healthcare
FERTILITY SPARING IN ENDOMETRIAL CANCER
 FERTILITY SPARING IN ENDOMETRIAL CANCER Prof. Dr. Bülent Özçelik Erciyes University Medical Faculty Department of Obstetrics and Gynecology Gynecologic Oncology Unit Endometrial Cancer Most frequent gynecologic
FERTILITY SPARING IN ENDOMETRIAL CANCER Prof. Dr. Bülent Özçelik Erciyes University Medical Faculty Department of Obstetrics and Gynecology Gynecologic Oncology Unit Endometrial Cancer Most frequent gynecologic
Port-Site Metastases After Robotic Surgery for Gynecologic Malignancy
 SCIENTIFIC PAPER Port-Site Metastases After Robotic Surgery for Gynecologic Malignancy Noah Rindos, MD, Christine L. Curry, MD, PhD, Rami Tabbarah, MD, Valena Wright, MD ABSTRACT Background and Objectives:
SCIENTIFIC PAPER Port-Site Metastases After Robotic Surgery for Gynecologic Malignancy Noah Rindos, MD, Christine L. Curry, MD, PhD, Rami Tabbarah, MD, Valena Wright, MD ABSTRACT Background and Objectives:
receive adjuvant chemotherapy
 Women with high h risk early stage endometrial cancer should receive adjuvant chemotherapy Michael Friedlander The Prince of Wales Cancer Centre and Royal Hospital for Women The Prince of Wales Cancer
Women with high h risk early stage endometrial cancer should receive adjuvant chemotherapy Michael Friedlander The Prince of Wales Cancer Centre and Royal Hospital for Women The Prince of Wales Cancer
Potentials for iatrogenic ovarian hyporresponse following
 Potentials for iatrogenic ovarian hyporresponse following endoscopic surgery Juan A Garcia-Velasco, MD IVI-Madrid, Rey Juan Carlos University Madrid, Spain Transition from 1980 s to 2007 Old aforism in
Potentials for iatrogenic ovarian hyporresponse following endoscopic surgery Juan A Garcia-Velasco, MD IVI-Madrid, Rey Juan Carlos University Madrid, Spain Transition from 1980 s to 2007 Old aforism in
Table E2. Studies from 1998 November 2008 That Focus on Performance of Imaging Modalities for Ovarian Lesion Detection and Characterization
 Table E2. Studies from 1998 November 2008 That Focus on Imaging Modalities for Ovarian Lesion Detection and Characterization No. of No. of Tumor Types and Sensitivity Specificity PPV NPV Accuracy False-Positive
Table E2. Studies from 1998 November 2008 That Focus on Imaging Modalities for Ovarian Lesion Detection and Characterization No. of No. of Tumor Types and Sensitivity Specificity PPV NPV Accuracy False-Positive
Recurrence of sex cord tumor with annular tubules in young patient with Peutz-Jeghers syndrome
 Slimane et al. 74 CASE REPORT PEER REVIEWED OPEN ACCESS Recurrence of sex cord tumor with annular tubules in young patient with Peutz-Jeghers syndrome Meher Slimane, Selma Gadria, Manel Hadidane, Houyem
Slimane et al. 74 CASE REPORT PEER REVIEWED OPEN ACCESS Recurrence of sex cord tumor with annular tubules in young patient with Peutz-Jeghers syndrome Meher Slimane, Selma Gadria, Manel Hadidane, Houyem
Hitting the High Points Gynecologic Oncology Review
 Hitting the High Points is designed to cover exam-based material, from preinvasive neoplasms of the female genital tract to the presentation, diagnosis and treatment, including surgery, chemotherapy, and
Hitting the High Points is designed to cover exam-based material, from preinvasive neoplasms of the female genital tract to the presentation, diagnosis and treatment, including surgery, chemotherapy, and
Low-grade serous neoplasia. Robert A. Soslow, MD
 Low-grade serous neoplasia Robert A. Soslow, MD soslowr@mskcc.org Outline Orientation Ovarian tumor overview Non serous borderline tumors Serous borderline tumors Clinical summary Morphologic description
Low-grade serous neoplasia Robert A. Soslow, MD soslowr@mskcc.org Outline Orientation Ovarian tumor overview Non serous borderline tumors Serous borderline tumors Clinical summary Morphologic description
Unilateral salpingo-oophorectomy as fertility-sparing surgery for borderline ovarian tumors
 Available online at www.sciencedirect.com Journal of the Chinese Medical Association 74 (2011) 250e254 Original Article Unilateral salpingo-oophorectomy as fertility-sparing surgery for borderline ovarian
Available online at www.sciencedirect.com Journal of the Chinese Medical Association 74 (2011) 250e254 Original Article Unilateral salpingo-oophorectomy as fertility-sparing surgery for borderline ovarian
Human epididymal protein 4 The role of HE4 in the management of patients presenting with pelvic mass Publication abstracts
 Human epididymal protein 4 The role of HE4 in the management of patients presenting with pelvic mass Publication abstracts Ovarian cancer is diagnosed annually in more than 200,000 women worldwide, with
Human epididymal protein 4 The role of HE4 in the management of patients presenting with pelvic mass Publication abstracts Ovarian cancer is diagnosed annually in more than 200,000 women worldwide, with
Surgery to Reduce the Risk of Ovarian Cancer. Information for Women at Increased Risk
 Surgery to Reduce the Risk of Ovarian Cancer Information for Women at Increased Risk Centre for Genetics Education NSW Health 2017 The Centre for Genetics Education NSW Health Level 5 2C Herbert St St
Surgery to Reduce the Risk of Ovarian Cancer Information for Women at Increased Risk Centre for Genetics Education NSW Health 2017 The Centre for Genetics Education NSW Health Level 5 2C Herbert St St
Please complete prior to the webinar. HOSPITAL REGISTRY WEBINAR FEMALE REPRODUCTIVE SYSTEM EXERCISES CASE 1: FEMALE REPRODUCTIVE
 Please complete prior to the webinar. HOSPITAL REGISTRY WEBINAR FEMALE REPRODUCTIVE SYSTEM EXERCISES PHYSICAL EXAMINATION CASE 1: FEMALE REPRODUCTIVE 3/5 Patient presents through the emergency room with
Please complete prior to the webinar. HOSPITAL REGISTRY WEBINAR FEMALE REPRODUCTIVE SYSTEM EXERCISES PHYSICAL EXAMINATION CASE 1: FEMALE REPRODUCTIVE 3/5 Patient presents through the emergency room with
Survival Analysis and Prognosis for Patients with Serous and Mucinous Borderline Ovarian Tumors: 14-Year Experience from a Tertiary Center in Iran
 ORIGINAL ARTICLE Survival Analysis and Prognosis for Patients with Serous and Mucinous Borderline Ovarian Tumors: 14-Year Experience from a Tertiary Center in Iran Katayoun Ziari, Ebrahim Soleymani, and
ORIGINAL ARTICLE Survival Analysis and Prognosis for Patients with Serous and Mucinous Borderline Ovarian Tumors: 14-Year Experience from a Tertiary Center in Iran Katayoun Ziari, Ebrahim Soleymani, and
OVARIAN CANCER STATISTICS
 bioprognos OncoOVARIAN Dx Non-invasive blood test useful to suggest a possible diagnosis in patients with suspected malignancy in the ovarians, reduce inappropriate diagnostic tests, days of hospitalization,
bioprognos OncoOVARIAN Dx Non-invasive blood test useful to suggest a possible diagnosis in patients with suspected malignancy in the ovarians, reduce inappropriate diagnostic tests, days of hospitalization,
International Society of Gynecological Pathologists Symposium 2007
 International Society of Gynecological Pathologists Symposium 2007 Anais Malpica, M.D. Department of Pathology The University of Texas M.D. Anderson Cancer Center Grading of Ovarian Cancer Histologic grade
International Society of Gynecological Pathologists Symposium 2007 Anais Malpica, M.D. Department of Pathology The University of Texas M.D. Anderson Cancer Center Grading of Ovarian Cancer Histologic grade
Key Recommendations. Gynecologic management of women with inherited risk of gynecologic cancer. HBOC related genes. I have nothing to disclose
 Gynecologic management of women with inherited risk of gynecologic cancer C. Bethan Powell MD Kaiser Permanente Northern California Gynecologic Oncology Program I have nothing to disclose Key Recommendations
Gynecologic management of women with inherited risk of gynecologic cancer C. Bethan Powell MD Kaiser Permanente Northern California Gynecologic Oncology Program I have nothing to disclose Key Recommendations
The Adnexal Mass. Handout NCUS 3/18/2017 Suzanne Dixon, MD
 The Adnexal Mass Handout NCUS 3/18/2017 Suzanne Dixon, MD Objectives: Pelvic mass differential Characteristics of the normal ovary Standard terminology for ovarian masses Benign vs. malignant features
The Adnexal Mass Handout NCUS 3/18/2017 Suzanne Dixon, MD Objectives: Pelvic mass differential Characteristics of the normal ovary Standard terminology for ovarian masses Benign vs. malignant features
Management of Endometrial Hyperplasia
 Management of Endometrial Hyperplasia I have nothing to disclose. Stefanie M. Ueda, M.D. Assistant Clinical Professor UCSF Division of Gynecologic Oncology Female Malignancies in the United States New
Management of Endometrial Hyperplasia I have nothing to disclose. Stefanie M. Ueda, M.D. Assistant Clinical Professor UCSF Division of Gynecologic Oncology Female Malignancies in the United States New
Clinical outcome of cystectomy compared with unilateral salpingo-oophorectomy as fertility-sparing treatment of borderline ovarian tumors
 REPRODUCTIVE SURGERY Clinical outcome of cystectomy compared with unilateral salpingo-oophorectomy as fertility-sparing treatment of borderline ovarian tumors Yoav Yinon, M.D., Mario E. Beiner, M.D., Walter
REPRODUCTIVE SURGERY Clinical outcome of cystectomy compared with unilateral salpingo-oophorectomy as fertility-sparing treatment of borderline ovarian tumors Yoav Yinon, M.D., Mario E. Beiner, M.D., Walter
Prospective study evaluating a strategy of surgery alone and surveillance in FIGO stage I malignant ovarian germ cell tumor (KGOG 3033)
") Prospective study evaluating a strategy of surgery alone and surveillance in FIGO stage I malignant ovarian germ cell tumor (KGOG 3033) Investigators/Collaborators: Jeong-Yeol Park, M.D., Ph.D. Department
Prospective study evaluating a strategy of surgery alone and surveillance in FIGO stage I malignant ovarian germ cell tumor (KGOG 3033) Investigators/Collaborators: Jeong-Yeol Park, M.D., Ph.D. Department
Gynaecological cancers. Mr Vivek Nama MD MRCOG Consultant Gynaecological Oncologist
 Gynaecological cancers Mr Vivek Nama MD MRCOG Consultant Gynaecological Oncologist Gynaecological cancers Why do we need 2 week wait? Early/timely diagnosis of cancer Possibly less invasive treatment and
Gynaecological cancers Mr Vivek Nama MD MRCOG Consultant Gynaecological Oncologist Gynaecological cancers Why do we need 2 week wait? Early/timely diagnosis of cancer Possibly less invasive treatment and
The Role of Imaging for Gynecologic Emergencies
 Objectives The Role of Imaging for Gynecologic Emergencies M. Jonathon Solnik, MD, FACOG FACS Associate Professor of Obstetrics & Gynaecology Head of Gynaecology & Minimally Invasive Surgery University
Objectives The Role of Imaging for Gynecologic Emergencies M. Jonathon Solnik, MD, FACOG FACS Associate Professor of Obstetrics & Gynaecology Head of Gynaecology & Minimally Invasive Surgery University
Screening for Ovarian Cancer: The Possible Improvement by 3D Ultrasound and 3D Power Doppler
 REVIEW ARTICLE DSJUOG Screening for Ovarian Cancer: The Possible Improvement by 3D Ultrasound and 3D Power Doppler 1 Asim Kurjak, 2 Ulrich Honemeyer, 1 Matija Prka 1 Department of Obstetrics and Gynecology,
REVIEW ARTICLE DSJUOG Screening for Ovarian Cancer: The Possible Improvement by 3D Ultrasound and 3D Power Doppler 1 Asim Kurjak, 2 Ulrich Honemeyer, 1 Matija Prka 1 Department of Obstetrics and Gynecology,
--- or not, and do we need to come up with newer strategies for ovarian cancer screening.
 My name is Dr. Karen Lu and I am a Professor of Gynecologic Oncology at the University of Texas MD Anderson Cancer Center. I also serve as Co-Medical Director for Clinical Cancer Genetics. I m going to
My name is Dr. Karen Lu and I am a Professor of Gynecologic Oncology at the University of Texas MD Anderson Cancer Center. I also serve as Co-Medical Director for Clinical Cancer Genetics. I m going to
Adjuvant Therapies in Endometrial Cancer. Emma Hudson
 Adjuvant Therapies in Endometrial Cancer Emma Hudson Endometrial Cancer Most common gynaecological cancer Incidence increasing in Western world 1-2% cancer deaths 75% patients postmenopausal 97% epithelial
Adjuvant Therapies in Endometrial Cancer Emma Hudson Endometrial Cancer Most common gynaecological cancer Incidence increasing in Western world 1-2% cancer deaths 75% patients postmenopausal 97% epithelial
surgical staging g in early endometrial cancer
 Risk adapted d approach to surgical staging g in early endometrial cancer Leon Massuger University Medical Centre St Radboud Nijmegen, The Netherlands Doing nodes Yes Yes Yes No No No 1957---------------------------
Risk adapted d approach to surgical staging g in early endometrial cancer Leon Massuger University Medical Centre St Radboud Nijmegen, The Netherlands Doing nodes Yes Yes Yes No No No 1957---------------------------
Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc)
") Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc) Author: Contact Name and Job Title Directorate & Speciality Assessment, referral and initial management of ultrasound
Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc) Author: Contact Name and Job Title Directorate & Speciality Assessment, referral and initial management of ultrasound
BRCA mutation carrier patient: How to manage?
 BRCA mutation carrier patient: How to manage? Clinical Case Presentation Katarzyna Sosińska-Mielcarek Department of Oncology and Radiotherapy University Clinical Center Gdansk, Poland esmo.org DISCLOSURE
BRCA mutation carrier patient: How to manage? Clinical Case Presentation Katarzyna Sosińska-Mielcarek Department of Oncology and Radiotherapy University Clinical Center Gdansk, Poland esmo.org DISCLOSURE
Squamous cell carcinoma arising in a dermoid cyst of the ovary: a case series
 DOI: 10.1111/j.1471-0528.2007.01478.x www.blackwellpublishing.com/bjog Gynaecological oncology Squamous cell carcinoma arising in a dermoid cyst of the ovary: a case series JL Hurwitz, a A Fenton, a WG
DOI: 10.1111/j.1471-0528.2007.01478.x www.blackwellpublishing.com/bjog Gynaecological oncology Squamous cell carcinoma arising in a dermoid cyst of the ovary: a case series JL Hurwitz, a A Fenton, a WG
CAN TV U/S REDUCE THE
 CAN TV U/S REDUCE THE NEED FOR SURGERY IN GYNECOLOGY? Steven R. Goldstein, M.D. Professor of Obstetrics & Gynecology New York University it School of fmedicine i Director of Gynecologic Ultrasound Co-Director
CAN TV U/S REDUCE THE NEED FOR SURGERY IN GYNECOLOGY? Steven R. Goldstein, M.D. Professor of Obstetrics & Gynecology New York University it School of fmedicine i Director of Gynecologic Ultrasound Co-Director
Laparoscopic Management of Early Stage Endometrial Cancer. B. Rabischong, M. Canis, G. Le Bouedec, C. Pomel, J.L Achard, J. Dauplat, G.
 Laparoscopic Management of Early Stage Endometrial Cancer B. Rabischong, M. Canis, G. Le Bouedec, C. Pomel, J.L Achard, J. Dauplat, G. Mage Early Stage of Endometrial Cancer most of cases diagnosed (clinical
Laparoscopic Management of Early Stage Endometrial Cancer B. Rabischong, M. Canis, G. Le Bouedec, C. Pomel, J.L Achard, J. Dauplat, G. Mage Early Stage of Endometrial Cancer most of cases diagnosed (clinical