Renal sympathetic denervation as a potential treatment for hypertension
|
|
|
- Austen Ellis
- 5 years ago
- Views:
Transcription





1 Renal sympathetic denervation as a potential treatment for hypertension (Why we must keep going) Dr Andrew SP Sharp Consultant Cardiologist and Honorary Senior Lecturer Royal Devon and Exeter Hospital and Exeter Medical School
2 Conflicts of Interest Consultant: Medtronic, Philips Volcano Research Funding: Medtronic
3 Let s get this out of the way
4 Let s get this out of the way Renal Denervation may not work.at all Particularly with radiofrequency technology, which has design strengths but also limitations in current iterations
5 Now. I will detail why we require more research in this area
6 Why bother?
7 The procedure doesn t work you ve had years to prove it. Move on! Trial design and technology used are key to proving whether a technology works or not Trials of catheter intervention for acute stroke failed until the right trial design deployed the right technology Now a Class 1A indication a year later
8 Background 1.1 billion hypertensives worldwide Fewer than half at recommended target Drug-based strategies are currently not getting >500 million people to target This represents a failure of current therapeutic strategies 30% Untreated 35% Treated and controlled 35% Treated but uncontrolled*
9 Why are drugs not getting patients to target? Compliance Physician treatment inertia Side effects from drugs Drug Resistance Patients not diagnosed

10 Who on earth would want their kidneys ablated?

11 People (%) 8% of adults would rather die two years early than take drugs forever Number of Weeks Willing to Trade Hutchins et al. Circ Cardiovasc Qual Outcomes. 2015;8:00-00.
12 Case Study from Exeter 42 yr old diabetic male Elevated BMI (35) Taking: Indapamide 2.5, Spironolactone 25, Ramipril 10, Amlodipine 10 BP: Office: 188/98 DABP 188/94, NABP 177/88

13 Home BPs before RDN

14 ABP before RDN

15 ABP before RDN

16 Original Technique

17 1 wk post RDN Post procedure home BPs

18 Post procedure ABP at 1 year

19 Post procedure ABP
20 Ambulatory BP response Fall of Day ABP of 42/14 Fall of Night ABP of 38/11 Drugs at time of 1 year ABP were: Indapamide 2.5, Ramipril 10, Amlod 10, Eplerenone 25 (switched due to S/E) Three year follow-up BP controlled on four agents

21 ECG before RDN

22 ECG at 1 year regression of LVH and strain pattern
23 What this case tells us: There is no doubt that blood pressure has fallen Dramatically How and why?

24 What is the sympathetic nervous system? Fight or flight Conserves salt and water Tightens Arteries Increases blood pressure Elevates heart rate Increases alertness Designed to help you run away from this About 30% of the SNS involves the kidneys
25 The effects are mostly bad for CV health

26 The aim of RDN M Leon, TCT 2013

27 How can we disrupt the SNS? M Leon, TCT 2013
28 Doesn t it damage the wall? Heat the adventitia to 80 degrees Blood flow cools the near field Enough energy to permanently disrupt the nerves Not enough to cause significant lasting damage to the renal arterial wall

29 Virmani, TCT 2013
30 How do we know that RDN really does persistently reduce sympathetic activity?

31 Peroneal nerve sympathetic firing can be quantified and is reduce by RDN Schlaich M et al. NEJM. 2009;36(9):
:s167. Schlaich et al. J Htn. 2009;27(suppl 4):s154.")
32 Kidney norepinephrine spillover is reduced by RDN Esler et al. J Htn. 2009;27(suppl 4):s167. Schlaich et al. J Htn. 2009;27(suppl 4):s154.
33 How will the kidney function without sympathetic control? Transplanted kidneys: Lack innervation Effectively maintain fluid and electrolyte balance Supports that sympathetic component of control represents overdrive system, rather than foundation of basic renal function Blaufox et al. N Engl J Med. 1969;280(2):62 66.
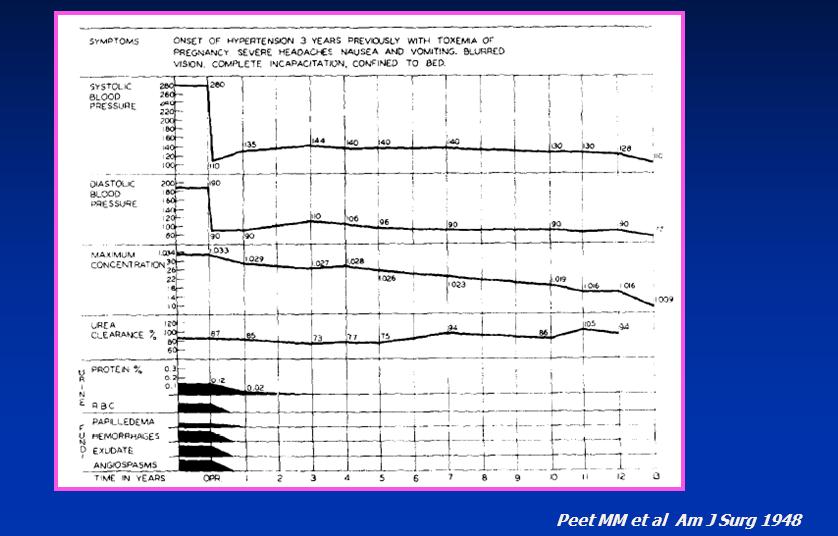
34 We have known that the process of sympathectomy markedly reduces blood pressure for a long-time



35 Sympathectomy: An Early Surgical Precedent Dr. Reginald H. Smithwick 1952
36
37 % Survivals Surgical Sympathectomy in Essential Hypertension Provided Beneficial Effect on Survival Medical 2 Medical Time in Years Survival rate of normal population Age 43 Sympathectomy 2 Sympathectomy 1 Surgical n=1266 Medical n=467 However, surgical sympathectomy was associated with significant morbidity 2 Sources: 1. Adapted from Smithwick RH, Thompson JE. JAMA. 1953;152: Gewirtz JR, Bisognano JD. Cardiol J. 2011;18:

38 Catheter based, selective sympathectomy is the endpoint of an 80 year research programme M Leon, TCT 2013
39 Observational studies


40 UK Renal Denervation Affiliation - results
41 UK Renal Denervation Affiliation Investigator-led Initiative 18 of 21 UK centers with RDN experience All performed 5+ RDN cases at time of conception All cases performed for treatment-resistant hypertension

42 UK Renal Denervation Affiliation Birmingham Heartlands Birmingham QE Bournemouth Bristol Dundee Exeter Glasgow Hastings Hull Kent and Canterbury London Barts London Brompton London Imperial London St Georges London St Thomas Sheffield Southampton Wycombe


43 Pre-procedural BP data


44 Follow-up Office BP data

45 ABP follow-up
46 Do we harm the kidneys? Anatomically, there are few cases of renal artery stenosis (>10,000 cases done worldwide) What about physiologically?
47 Change in GFR over time
48 4ml/min/yr in GLOBAL Renal function declines year on year in hypertension RDN effect? Bakris. Am J Kid Disease


49 What about other trial data?
50 HTN-2 Randomised trial RDN (n = 52) Control (n = 54) p-value Baseline systolic BP (mmhg) 178 ± ± Baseline diastolic BP (mmhg) 97 ± ± Number anti-htn medications 5.2 ± ± * n = 42 for RDN and n = 43 for Control. Wilcoxon rank-sum test for two independent samples used for between-group comparisons of UACR. n = 39 for RDN and n = 42 for Control. Expanded results presented at the American College of Cardiology Annual Meeting 2012 (Esler, M.)

51 mm Hg Office SBP through 30 Months* 6m Primary Endpoint Control Crossover Randomization 6m post procedure 12m post procedure 18m post procedure 24m post procedure 6m post randomization 12m post randomization 18m post randomization 24m post randomization 30m post randomization Esler M, ASH 2013

52 Enlightn 1 results (176/96 starting BP)

53 Then came Symplicity HTN-3

54 Symplicity HTN-3 Substantial BP falls Occurred in BOTH groups Difference between groups 2.4mmHg only
55 So what happened in HTN-3? Well, the technology might not work The alternative explanations are The RDN BP lowering effect is much less powerful than that observed in open label studies The study design masked the measured clinical benefit The study procedure was not conducted properly
56 The crucial issue of renal nerve anatomy and catheter design

57 We thought that most of the nerves were within range of a 3mm burn depth

58 s distal ease the sful Distribution of nerves proximal renal artery vs distal egies can th ers y. ry Superior Inferior Nerves more frequently make a close approach in the distal segment Distribution of renal nerves around renal artery ahfoud F. Sakakura et al. JACC 2014

59 Can we reliably get the nerves? Distal Proximal Prior concept uniform radial distribution Distal Proximal Current concept nonuniform radial distribution Sakakura K et al. JACC :
60 Therefore With a proximal ablation strategy, the technique is relying on randomly hitting where nerves dip down towards the vessel This was the recommended ablation strategy at the time A distal ablation strategy should ensure more reliable denervation


61 Has a distal ablation strategy been demonstrated to be more effective? IVY study. Melder et al. TCT Note: Each animal served as its own control in this study
62 Are there any signals within HTN-3 to support this?
63 Ablation attempts and change in BP in HTN-3 MORE ABLATIONS = MORE BP REDUCTION OFFICE 24 hr ambulatory SBP
64 Were there other technical issues in the HTN-3 trial? The trial was a sham-controlled RCT of Renal denervation versus placebo The recommended RDN technique is to ablate the four points of a compass in a retrograde spiral fashion Four quadrant ablation Animal data suggests we need to get >70% of the nerves to produce a BP lowering effect We therefore need all four quadrants to be ablated
65 What proportion of patients had the recommended (and required) four quadrant ablation in the HTN- 3 trials? 5%
66 Four-quadrant ablations in HTN-3 Procedural Variability Correlation with # of ablations Correlation with 4-quadrant ablation pattern Cross-section of artery Inferior Anterior Superior Posterior
67 Four quadrant ablations Procedural Variability Operators performed their 1 st procedure within the trial Correlation with # of ablations Correlation with 4-quadrant ablation pattern >50% cases were performed by operators with a cumulative experience of 2 procedures by the end of the trial Cross-section of artery Inferior Anterior Superior Posterior
68 Patients With Medication Changes (%) Medication changes Medication Changes During Trial Medication changes were permitted between procedure and primary endpoint assessment in cases of hypertensive urgency ~40% (n = 211) of trial subjects required medication changes between baseline and primary efficacy endpoint assessment: 69% of first medication changes were medically necessary 121 patients had a med change due to an adverse event 80 patients had a med change due to a drug side-effect What proportion of patients with hypertension under your care meet such a criteria during 6 month follow-up? ~69% were changes in drugs at maximally-tolerated dose % RDN 40% N = 139 N = 72 Control Drug changes during the trial
69 Current state of play We know: Surgical sympathectomy reduces blood pressure RDN appears to perform selective sympathectomy in animals if correct technique and technology is deployed Blood pressure fell after RDN in >5000 (observational) published cases Early serious side effects (<3 yrs) appear few
70 Current state of play We don t know: The true magnitude of effect in a real-world population (is it real and meaningful?) Long-term outcomes (>7 years) Whether any BP reduction from RDN has same magnitude of effect as seen with BP reduction with drugs
71 RCTs currently active

72 SPYRAL research programme Medtronic dominate the field This is their flagship research programme Two centres in the UK, 22 globally

73 SPYRAL RDN catheter Four electrode RFA catheter Monitor tracks impedance and temp changes during delivery Delivers simultaneously for 60 seconds

74 A lot of thought has gone into these trials
75 Trial 1: SPYRAL OFF Office BP Diastolic >90 ABP on no drugs
76 SPYRAL OFF Uncontaminated RDN Week 1: Four week washout if on drugs If BP >180 exit trial and re-start drugs Week 4: final screen Week 6: RDN treatment or sham Week 18: Begin drug-titration schedule (ARB/CCB/Diuretic) One year unblinded
77 Trial 2: SPYRAL ON Age BP on office despite between 1 and 3 drugs (A-B-C-D) BP on ABPM DOT with urine testing to confirm compliance RDN:Sham in 1:1 ratio

78 Trials 3&4: RADIANCE ON/OFF Sham-controlled trial programme Similar concept to SPYRAL Instead of RF energy, uses ultrasound to denervate Delivered percutaneously via catheter approach Reliably reaches 6mm depth so appears well designed for task
79 Conclusions Hundreds of millions of patients with hypertension have uncontrolled blood pressure A 2mmHg reduction in systolic BP would be expected to reduce the risk of the stroke by 10% Some people would, unfortunately and literally, rather die than take pills New methods of BP control are required
80 Conclusions Proving efficacy when the primary endpoint is as variable as BP is extremely challenging I often get asked whether I believe in renal denervation Its not a religion! We must know whether RDN reduces BP before we give up on it through sound scientific research Those trials are now active in the SW of England
81 If you have interested patients... me on Ask your patient to register via my research website:

82
The Future of Renal Denervation
 The Future of Renal Denervation Ron Waksman, MD, FACC, FSCAI Professor of Medicine, (Cardiology) Georgetown University Director, Cardiovascular Research Advanced Education MedStar Heart Institute, Washington
The Future of Renal Denervation Ron Waksman, MD, FACC, FSCAI Professor of Medicine, (Cardiology) Georgetown University Director, Cardiovascular Research Advanced Education MedStar Heart Institute, Washington
Catheter-Based Renal Denervation (RDN)
") Hypertension lecture 3: Catheter-Based Renal Denervation (RDN) Adapted from slides prepared by Dr IOEBRAHIM, UNITAS HOSPITAL and others Hypertension Epidemiology 30% Untreated 35% Treated & Controlled
Hypertension lecture 3: Catheter-Based Renal Denervation (RDN) Adapted from slides prepared by Dr IOEBRAHIM, UNITAS HOSPITAL and others Hypertension Epidemiology 30% Untreated 35% Treated & Controlled
RISE, FALL AND RESURRECTION OF RENAL DENERVATION. Michael A. Weber, MD State University of New York Downstate College of Medicine
 RISE, FALL AND RESURRECTION OF RENAL DENERVATION Michael A. Weber, MD State University of New York Downstate College of Medicine Michael Weber, Disclosures Research/Trial Commitments and Consulting: Boston
RISE, FALL AND RESURRECTION OF RENAL DENERVATION Michael A. Weber, MD State University of New York Downstate College of Medicine Michael Weber, Disclosures Research/Trial Commitments and Consulting: Boston
Catheter-Based Renal Sympathetic Denervation in the Management of Resistant Hypertension
 Catheter-Based Renal Sympathetic Denervation in the Management of Resistant Hypertension Henry Krum, Markus Schlaich, Paul Sobotka, Rob Whitbourn, Jerzy Sadowski, Krzysztof Bartus, Boguslaw Kapelak, Horst
Catheter-Based Renal Sympathetic Denervation in the Management of Resistant Hypertension Henry Krum, Markus Schlaich, Paul Sobotka, Rob Whitbourn, Jerzy Sadowski, Krzysztof Bartus, Boguslaw Kapelak, Horst
Renal denervation for treatment of resistant hypertension
 Renal denervation for treatment of resistant hypertension Dr U. Nqebelele Division of Nephrology Department of Internal Medicine Charlotte Maxeke Johannesburg Academic Hospital Thomas Willis: 1621-1675
Renal denervation for treatment of resistant hypertension Dr U. Nqebelele Division of Nephrology Department of Internal Medicine Charlotte Maxeke Johannesburg Academic Hospital Thomas Willis: 1621-1675
Disclosures for Dr. Bhatt
 Renal Denervation Deepak L. Bhatt, MD, MPH, FACC, FAHA, FSCAI, FESC Executive Director of Interventional Cardiovascular Programs, BWH Heart & Vascular Center Professor of Medicine, Harvard Medical School
Renal Denervation Deepak L. Bhatt, MD, MPH, FACC, FAHA, FSCAI, FESC Executive Director of Interventional Cardiovascular Programs, BWH Heart & Vascular Center Professor of Medicine, Harvard Medical School
Stephen G. Worthley 1, Gerard T. Wilkins 2, Mark W. Webster 3,Joseph K. Montarello 1, Paul T. Antonis 4, Robert J. Whitbourn 5, Roderic J.
 Six Month Results of First-in-Human Sympathetic Renal Artery Denervation Using a Next Generation Multi-Electrode Renal Artery Denervation System in Patients with Drug-Resistant Hypertension Stephen G.
Six Month Results of First-in-Human Sympathetic Renal Artery Denervation Using a Next Generation Multi-Electrode Renal Artery Denervation System in Patients with Drug-Resistant Hypertension Stephen G.
Renal Denervation For Hypertension: Status Update
 Samuel N. Steerman, Presenter MD, FACS, name RPVI EVMS Assistant Professor of Surgery Sentara Vascular Specialists Renal Denervation For Hypertension: Status Update Disclosures Disclosures Speaker s Panel
Samuel N. Steerman, Presenter MD, FACS, name RPVI EVMS Assistant Professor of Surgery Sentara Vascular Specialists Renal Denervation For Hypertension: Status Update Disclosures Disclosures Speaker s Panel
Renal Denervation. by Walead Latif, DO, MBA, CPE Assistant Clinical Professor Rutgers Medical School
 Renal Denervation by Walead Latif, DO, MBA, CPE Assistant Clinical Professor Rutgers Medical School Disclosure Information ACOI Annual Meeting I have the following financial relationships to disclose:
Renal Denervation by Walead Latif, DO, MBA, CPE Assistant Clinical Professor Rutgers Medical School Disclosure Information ACOI Annual Meeting I have the following financial relationships to disclose:
Preliminary Results of RETREAT
 LINC 2015 Leipzig, Germany, Jan 27-30, 2015 Preliminary Results of RETREAT (Renal Denervation with Ultrasound After Failed Radiofrequency Denervation) Horst Sievert, Jan Philipp Kulow, Stefan Bertog, Predrag
LINC 2015 Leipzig, Germany, Jan 27-30, 2015 Preliminary Results of RETREAT (Renal Denervation with Ultrasound After Failed Radiofrequency Denervation) Horst Sievert, Jan Philipp Kulow, Stefan Bertog, Predrag
Renal Sympathetic Denervation Beyond Hypertension: Therapy for Arrhythmias and for Autonomic Nervous System Dysfunction?
 Renal Sympathetic Denervation Beyond Hypertension: Therapy for Arrhythmias and for Autonomic Nervous System Dysfunction? Vivek Y. Reddy, MD Helmsley Trust Professor of Medicine Director, Cardiac Arrhythmia
Renal Sympathetic Denervation Beyond Hypertension: Therapy for Arrhythmias and for Autonomic Nervous System Dysfunction? Vivek Y. Reddy, MD Helmsley Trust Professor of Medicine Director, Cardiac Arrhythmia
With an unrestricted educational grant from. The Interventional Treatment of Resistant Hypertension
 With an unrestricted educational grant from The Interventional Treatment of Resistant Hypertension Felix Mahfoud Interventional Cardiology University Hospital Homburg/Saar Germany Dr. Mahfoud graduated
With an unrestricted educational grant from The Interventional Treatment of Resistant Hypertension Felix Mahfoud Interventional Cardiology University Hospital Homburg/Saar Germany Dr. Mahfoud graduated
Renal Sympathetic Denervation for HTN
 Renal Sympathetic Denervation for HTN Se-Young Yim Department of CardioVascular Center Samsung Medical Center Worldwide Prevalence of Hypertension Is Increasing In 2000, 972 million (26%), of the adult
Renal Sympathetic Denervation for HTN Se-Young Yim Department of CardioVascular Center Samsung Medical Center Worldwide Prevalence of Hypertension Is Increasing In 2000, 972 million (26%), of the adult
Devices and Long-Term Outcomes of Renal Denervation for Hypertension
 18th ANGIOPLASTY SUMMIT-TCTAP 2013 Seoul, Korea, April 23-26, 2013 Devices and Long-Term Outcomes of Renal Denervation for Hypertension Horst Sievert, Ilona Hofmann, Laura Vaskelyte, Stefan Bertog, Simon
18th ANGIOPLASTY SUMMIT-TCTAP 2013 Seoul, Korea, April 23-26, 2013 Devices and Long-Term Outcomes of Renal Denervation for Hypertension Horst Sievert, Ilona Hofmann, Laura Vaskelyte, Stefan Bertog, Simon
Catheter-Based Renal Denervation Reduces Total Body and Renal Noradrenaline Spillover and Blood Pressure in Resistant Hypertension
 Catheter-Based Renal Denervation Reduces Total Body and Renal Noradrenaline Spillover and Blood Pressure in Resistant Hypertension Murray Esler, Markus Schlaich, Paul Sobotka, Rob Whitbourn, Jerzy Sadowski,
Catheter-Based Renal Denervation Reduces Total Body and Renal Noradrenaline Spillover and Blood Pressure in Resistant Hypertension Murray Esler, Markus Schlaich, Paul Sobotka, Rob Whitbourn, Jerzy Sadowski,
Transcatheter Perivascular Alcohol- Mediated Renal Denervation
 Transcatheter Perivascular Alcohol- Mediated Renal Denervation Wojtek Wojakowski, MD, PhD Medical University of Silesia American Heart of Poland Katowice, Poland I, Wojciech Wojakowski DO NOT have a financial
Transcatheter Perivascular Alcohol- Mediated Renal Denervation Wojtek Wojakowski, MD, PhD Medical University of Silesia American Heart of Poland Katowice, Poland I, Wojciech Wojakowski DO NOT have a financial
Hypertension Guidelines Michael A. Weber, MD Division of Cardiovascular Medicine State University of New York Downstate Medical Center
 Hypertension Guidelines 2016 Michael A. Weber, MD Division of Cardiovascular Medicine State University of New York Downstate Medical Center Speaker Disclosures I disclose that I am a Consultant for: Ablative
Hypertension Guidelines 2016 Michael A. Weber, MD Division of Cardiovascular Medicine State University of New York Downstate Medical Center Speaker Disclosures I disclose that I am a Consultant for: Ablative
Update on renal denervation: Latest data
 LINC 2018 Update on renal denervation: Latest data Felix Mahfoud Saarland University Hospital, Germany Potential Conflicts of Interest I have the following potential conflicts of interest to report: Research
LINC 2018 Update on renal denervation: Latest data Felix Mahfoud Saarland University Hospital, Germany Potential Conflicts of Interest I have the following potential conflicts of interest to report: Research
Hypertension: the Heart Vs the Kidney. George Moturi Physician/Nephrologist Aga Khan Hospital Nairobi
 Hypertension: the Heart Vs the Kidney George Moturi Physician/Nephrologist Aga Khan Hospital Nairobi 24 th Feb, 2017 Travel facilitation from Novartis Disclaimer Systolic blood pressure (SBP) of at least
Hypertension: the Heart Vs the Kidney George Moturi Physician/Nephrologist Aga Khan Hospital Nairobi 24 th Feb, 2017 Travel facilitation from Novartis Disclaimer Systolic blood pressure (SBP) of at least
noradrenaline spillover and systemic blood pressure in patients with resistant hypertension
 Effects of renal sympathetic denervation on noradrenaline spillover and systemic blood pressure in patients with resistant hypertension Markus Schlaich Neurovascular Hypertension & Kidney Disease Laboratory
Effects of renal sympathetic denervation on noradrenaline spillover and systemic blood pressure in patients with resistant hypertension Markus Schlaich Neurovascular Hypertension & Kidney Disease Laboratory
Byeong-Keuk Kim, MD, PhD. Division of Cardiology, Severance Cardiovascular Hospital Yonsei University College of Medicine, Seoul, Korea
 Byeong-Keuk Kim, MD, PhD Division of Cardiology, Severance Cardiovascular Hospital Yonsei University College of Medicine, Seoul, Korea BP change (mmhg) from Baseline to 6 Months (mmhg) Catheter-based renal
Byeong-Keuk Kim, MD, PhD Division of Cardiology, Severance Cardiovascular Hospital Yonsei University College of Medicine, Seoul, Korea BP change (mmhg) from Baseline to 6 Months (mmhg) Catheter-based renal
Renal Denervation. Henry Krum MBBS PhD FRACP. Centre of Cardiovascular Research & Monash University/Alfred Hospital;
 Renal Denervation Henry Krum MBBS PhD FRACP Centre of Cardiovascular Research & Education in Therapeutics, Monash University/Alfred Hospital; Alfred Heart Centre, The Alfred Hospital, Melbourne Australia
Renal Denervation Henry Krum MBBS PhD FRACP Centre of Cardiovascular Research & Education in Therapeutics, Monash University/Alfred Hospital; Alfred Heart Centre, The Alfred Hospital, Melbourne Australia
Renal Denervation: The Case for Cardiology
 Renal Denervation: The Case for Cardiology John C. Gurley, MD University of Kentucky Presenter Disclosure Information John C Gurley, MD Renal Denervation: The Case for Cardiology FINANCIAL DISCLOSURE:
Renal Denervation: The Case for Cardiology John C. Gurley, MD University of Kentucky Presenter Disclosure Information John C Gurley, MD Renal Denervation: The Case for Cardiology FINANCIAL DISCLOSURE:
EnligHTN I, First-in-Human Multicenter Study of a Multi-Electrode Renal Denervation Catheter in Patients with Drug-Resistant Hypertension
 EnligHTN I, First-in-Human Multicenter Study of a Multi-Electrode Renal Denervation Catheter in Patients with Drug-Resistant Hypertension Vasilios Papademetriou, MD 1 Prof. Stephen Worthley, MD 2 Costas
EnligHTN I, First-in-Human Multicenter Study of a Multi-Electrode Renal Denervation Catheter in Patients with Drug-Resistant Hypertension Vasilios Papademetriou, MD 1 Prof. Stephen Worthley, MD 2 Costas
Ambulatory Blood Pressure Measurement. Objectives of the Presentation. Methods of Measuring BP: Pros and Cons
 Ambulatory Blood Pressure Measurement William B. White, MD Professor of Medicine and Chief, Hypertension and Clinical Pharmacology Calhoun Cardiology Center University of Connecticut School of Medicine
Ambulatory Blood Pressure Measurement William B. White, MD Professor of Medicine and Chief, Hypertension and Clinical Pharmacology Calhoun Cardiology Center University of Connecticut School of Medicine
Autumn Meeting Birmingham. Renal Denervation
 Autumn Meeting Birmingham Renal Denervation Andreas Baumbach, MD, FRCP, FESC Consultant Cardiologist, hon. Reader in Cardiology Bristol Heart Institute University Hospitals Bristol Renal Denervation BACKGROUND
Autumn Meeting Birmingham Renal Denervation Andreas Baumbach, MD, FRCP, FESC Consultant Cardiologist, hon. Reader in Cardiology Bristol Heart Institute University Hospitals Bristol Renal Denervation BACKGROUND
Optimal blood pressure targets in chronic kidney disease
 Optimal blood pressure targets in chronic kidney disease Pr. Michel Burnier Service of Nephrology and Hypertension University Hospital Lausanne Switzerland Evidence-Based Guideline for the Management
Optimal blood pressure targets in chronic kidney disease Pr. Michel Burnier Service of Nephrology and Hypertension University Hospital Lausanne Switzerland Evidence-Based Guideline for the Management
MINNEAPOLIS September 12, 2012 Medtronic, Inc. (NYSE: MDT) today announced findings
 today announced findings") NEWS RELEASE Contacts: Wendy Dougherty Jeff Warren Public Relations Investor Relations 707-541-3004 763-505-2696 FOR IMMEDIATE RELEASE HEALTH-ECONOMIC ANALYSIS SUGGESTS MEDTRONIC SYMPLICITY RENAL DENERVATION
NEWS RELEASE Contacts: Wendy Dougherty Jeff Warren Public Relations Investor Relations 707-541-3004 763-505-2696 FOR IMMEDIATE RELEASE HEALTH-ECONOMIC ANALYSIS SUGGESTS MEDTRONIC SYMPLICITY RENAL DENERVATION
MP Radiofrequency Ablation of the Renal Sympathetic Nerves as a Treatment for Resistant Hypertension
 Medical Policy Radiofrequency Ablation of the Renal Sympathetic Nerves as a Treatment for Resistant Hypertension BCBSA Ref. Policy: 7.01.136 Last Review: 09/19/2018 Effective Date: 09/19/2018 Section:
Medical Policy Radiofrequency Ablation of the Renal Sympathetic Nerves as a Treatment for Resistant Hypertension BCBSA Ref. Policy: 7.01.136 Last Review: 09/19/2018 Effective Date: 09/19/2018 Section:
Treating Hypertension With a Catheter..Wait What? David P. Lee, M.D. 22 June 2013 Stanford University
 Treating Hypertension With a Catheter..Wait What? David P. Lee, M.D. 22 June 2013 Stanford University COI Medtronic: Research Grant, Consultant Boston Scientific: Research Grant, MAB Worldwide Prevalence
Treating Hypertension With a Catheter..Wait What? David P. Lee, M.D. 22 June 2013 Stanford University COI Medtronic: Research Grant, Consultant Boston Scientific: Research Grant, MAB Worldwide Prevalence
What We've Learned from Simplicity HTN-1,2, and Registries
 ANGIOPLASTY SUMMIT-TCTAP 2012 Seoul, Korea, April 24-27, 2012 What We've Learned from Simplicity HTN-1,2, and Registries Horst Sievert, Ann-Kathrin Ziegler, Benjamin Kaltenbach, Ilona Hofmann, Undine Pittl
ANGIOPLASTY SUMMIT-TCTAP 2012 Seoul, Korea, April 24-27, 2012 What We've Learned from Simplicity HTN-1,2, and Registries Horst Sievert, Ann-Kathrin Ziegler, Benjamin Kaltenbach, Ilona Hofmann, Undine Pittl
Catheter Based Denervation for Heart Failure
 Catheter Based Denervation for Heart Failure David E. Kandzari, MD, FACC, FSCAI Chief Scientific Officer Director, Interventional Cardiology Piedmont Heart Institute Atlanta, Georgia david.kandzari@piedmont.org
Catheter Based Denervation for Heart Failure David E. Kandzari, MD, FACC, FSCAI Chief Scientific Officer Director, Interventional Cardiology Piedmont Heart Institute Atlanta, Georgia david.kandzari@piedmont.org
Renal Artery Denervation New Concepts in Hypertension Treatment
 Renal Artery Denervation New Concepts in Hypertension Treatment Istanbul Course of Interventional Cardiology J. Weil Medizinische Klinik II Kardiologie, Angiologie und internistische Intensivmedizin Universitätsklinikum,
Renal Artery Denervation New Concepts in Hypertension Treatment Istanbul Course of Interventional Cardiology J. Weil Medizinische Klinik II Kardiologie, Angiologie und internistische Intensivmedizin Universitätsklinikum,
Hypertension Management Controversies in the Elderly Patient
 Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Management of Hypertension and Consequences of non-compliance. Colin Edwards
 Management of Hypertension and Consequences of non-compliance Colin Edwards CARDIOLOGIST AHG May 2016 Outline 1. Consequences of poorly controlled hypertension 2. BP targets and anti-hypertensive drugs
Management of Hypertension and Consequences of non-compliance Colin Edwards CARDIOLOGIST AHG May 2016 Outline 1. Consequences of poorly controlled hypertension 2. BP targets and anti-hypertensive drugs
Renal denervation: Current evidence and remaining uncertainties
 Renal denervation: Current evidence and remaining uncertainties Michel Azizi Georges Pompidou European Hospital Hypertension Unit ESH excellence Center Paris Descartes University Clinical Investigation
Renal denervation: Current evidence and remaining uncertainties Michel Azizi Georges Pompidou European Hospital Hypertension Unit ESH excellence Center Paris Descartes University Clinical Investigation
Christopher Valentine, MD
 Resistant Hypertension Christopher Valentine, MD Program Director, Nephrology Fellowship Program Department of Internal Medicine Division of Nephrology The Ohio State University Wexner Medical Center Disclosures
Resistant Hypertension Christopher Valentine, MD Program Director, Nephrology Fellowship Program Department of Internal Medicine Division of Nephrology The Ohio State University Wexner Medical Center Disclosures
Difficult-to-Control & Resistant Hypertension. Anthony Viera, MD, MPH, FAHA Professor and Chair
 Difficult-to-Control & Resistant Hypertension Anthony Viera, MD, MPH, FAHA Professor and Chair Objectives Define resistant hypertension Discuss evaluation strategy for patient with HTN that appears difficult
Difficult-to-Control & Resistant Hypertension Anthony Viera, MD, MPH, FAHA Professor and Chair Objectives Define resistant hypertension Discuss evaluation strategy for patient with HTN that appears difficult
THE BLOOD PRESSURE PROCEDURE
 THE BLOOD PRESSURE PROCEDURE An innovative procedure that could help lower your blood pressure. THIS BOOKLET IS DESIGNED TO HELP YOU LEARN MORE ABOUT THE BLOOD PRESSURE PROCEDURE CALLED RDN CONTENTS 4
THE BLOOD PRESSURE PROCEDURE An innovative procedure that could help lower your blood pressure. THIS BOOKLET IS DESIGNED TO HELP YOU LEARN MORE ABOUT THE BLOOD PRESSURE PROCEDURE CALLED RDN CONTENTS 4
The Global SYMPLICITY Registry: Safety and Effectiveness of Renal Artery Denervation In Real World Patients With Uncontrolled Hypertension
 The Global SYMPLICITY Registry: Safety and Effectiveness of Renal Artery Denervation In Real World Patients With Uncontrolled Hypertension Michael Böhm, MD on behalf of the GSR Investigators March 30,
The Global SYMPLICITY Registry: Safety and Effectiveness of Renal Artery Denervation In Real World Patients With Uncontrolled Hypertension Michael Böhm, MD on behalf of the GSR Investigators March 30,
Real World Experience with Renal Denervation Therapy
 JCR 2013 Real World Experience with Renal Denervation Therapy Seung-Hyuk Choi Division of Cardiology Samsung Medical Center Seoul, Korea Hypertension A Major Public Health Burden Astonishing prevalence
JCR 2013 Real World Experience with Renal Denervation Therapy Seung-Hyuk Choi Division of Cardiology Samsung Medical Center Seoul, Korea Hypertension A Major Public Health Burden Astonishing prevalence
Hypertension AN OVERVIEW
 AN OVERVIEW Hypertension Your doctor has determined that you have high blood pressure, or hypertension. Although high blood pressure is never really cured, it can be controlled by early detection, lifestyle
AN OVERVIEW Hypertension Your doctor has determined that you have high blood pressure, or hypertension. Although high blood pressure is never really cured, it can be controlled by early detection, lifestyle
Percutaneous Renal Denervation: A New Promise in the Treatment of RHT?
 BAD KROZINGEN Prof. T. Zeller, MD Bad Krozingen, Germany Percutaneous Renal Denervation: A New Promise in the Treatment of RHT? Potential conflicts of interest Speaker s name: Thomas Zeller X I have the
BAD KROZINGEN Prof. T. Zeller, MD Bad Krozingen, Germany Percutaneous Renal Denervation: A New Promise in the Treatment of RHT? Potential conflicts of interest Speaker s name: Thomas Zeller X I have the
Renal Sympathetic Denervation Using an Irrigated Radiofrequency Ablation Catheter for the Management of Drug-Resistant Hypertension
 JACC: CARDIOVASCULAR INTERVENTIONS VOL. 5, NO. 7, 2012 2012 BY THE AMERICAN COLLEGE OF CARDIOLOGY FOUNDATION ISSN 1936-8798/$36.00 PUBLISHED BY ELSEVIER INC. http://dx.doi.org/10.1016/j.jcin.2012.01.027
JACC: CARDIOVASCULAR INTERVENTIONS VOL. 5, NO. 7, 2012 2012 BY THE AMERICAN COLLEGE OF CARDIOLOGY FOUNDATION ISSN 1936-8798/$36.00 PUBLISHED BY ELSEVIER INC. http://dx.doi.org/10.1016/j.jcin.2012.01.027
Management of Resistant Hypertension in Diabetes
 Management of Resistant Hypertension in Diabetes Soon Hee Lee, M.D., Ph.D. Divisoin of Endocrinology & Metabolism, Department of Internal Medicine, Busan Paik Hospital, College of Medicine, Inje University,
Management of Resistant Hypertension in Diabetes Soon Hee Lee, M.D., Ph.D. Divisoin of Endocrinology & Metabolism, Department of Internal Medicine, Busan Paik Hospital, College of Medicine, Inje University,
SPYRAL HTN ON MED. Disclosure
 Renal Denervation in the Presence of Antihypertensive Medications: Six-month Results from the Randomized, Blinded, Sham-controlled SPYRAL HTN-ON MED Trial Dr. David E. Kandzari Piedmont Heart Institute,
Renal Denervation in the Presence of Antihypertensive Medications: Six-month Results from the Randomized, Blinded, Sham-controlled SPYRAL HTN-ON MED Trial Dr. David E. Kandzari Piedmont Heart Institute,
Renal Denervation for Resistant Hypertension
 Renal Denervation for Resistant Hypertension James W. Choi MD FACC FSCAI Cardiology Consultants of Texas Director Interventional Cardiology Fellowship Baylor University Medical Center Baylor Heart & Vascular
Renal Denervation for Resistant Hypertension James W. Choi MD FACC FSCAI Cardiology Consultants of Texas Director Interventional Cardiology Fellowship Baylor University Medical Center Baylor Heart & Vascular
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
MANAGEMENT OF HYPERTENSION: TREATMENT THRESHOLDS AND MEDICATION SELECTION
 Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
DISCLOSURES OUTLINE OUTLINE 9/29/2014 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE
 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
Objectives. Describe results and implications of recent landmark hypertension trials
 Hypertension Update Daniel Schwartz, MD Assistant Professor of Medicine Associate Medical Director of Heart Transplantation Temple University School of Medicine Disclosures I currently have no relationships
Hypertension Update Daniel Schwartz, MD Assistant Professor of Medicine Associate Medical Director of Heart Transplantation Temple University School of Medicine Disclosures I currently have no relationships
Les techniques interventionnelles dans le traitement de l hypertension artérielle: faut-il y croire encore?
 Les techniques interventionnelles dans le traitement de l hypertension artérielle: faut-il y croire encore? Prof M Burnier Service de Néphrologie et Hypertension, CHUV, Lausanne Evian 2015 Approches non-médicamenteuses
Les techniques interventionnelles dans le traitement de l hypertension artérielle: faut-il y croire encore? Prof M Burnier Service de Néphrologie et Hypertension, CHUV, Lausanne Evian 2015 Approches non-médicamenteuses
Update in Hypertension
 Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
Christian Daugaard Peters, MD, PhD Department of Renal Medicine Aarhus University Hospital, Denmark Disclosures: None
 The effect of renal denervation on central blood pressure and arterial stiffness in treatment resistant essential hypertension: a substudy of a randomized sham-controlled double-blinded trial (the ReSET
The effect of renal denervation on central blood pressure and arterial stiffness in treatment resistant essential hypertension: a substudy of a randomized sham-controlled double-blinded trial (the ReSET
Dr Diana R Holdright. MD, FRCP, FESC, FACC, MBBS, DA, BSc. Consultant Cardiologist HYPERTENSION.
 Dr Diana R Holdright MD, FRCP, FESC, FACC, MBBS, DA, BSc. Consultant Cardiologist HYPERTENSION www.drholdright.co.uk Blood pressure is the pressure exerted on the walls of the arteries when the heart pumps;
Dr Diana R Holdright MD, FRCP, FESC, FACC, MBBS, DA, BSc. Consultant Cardiologist HYPERTENSION www.drholdright.co.uk Blood pressure is the pressure exerted on the walls of the arteries when the heart pumps;
Objectives. JNC 7 Is Nice But What s Up With JNC 8? Why Do We Care? Hypertension Background: Prevalence
 JNC 7 Is Nice But What s Up With JNC 8? 37 th Annual CAPA Conference October 4 th 2013 Ignacio de Artola, Jr. M.D. Assistant Professor of Clinical Family Medicine Medical Director, Primary Care Physician
JNC 7 Is Nice But What s Up With JNC 8? 37 th Annual CAPA Conference October 4 th 2013 Ignacio de Artola, Jr. M.D. Assistant Professor of Clinical Family Medicine Medical Director, Primary Care Physician
Prof. Andrzej Wiecek Department of Nephrology, Endocrinology and Metabolic Diseases Medical University of Silesia Katowice, Poland.
 What could be the role of renal denervation in chronic kidney disease? Andrzej Wiecek, Katowice, Poland Chairs: Peter J. Blankestijn, Utrecht, The Netherlands Jonathan Moss, Glasgow, UK Prof. Andrzej Wiecek
What could be the role of renal denervation in chronic kidney disease? Andrzej Wiecek, Katowice, Poland Chairs: Peter J. Blankestijn, Utrecht, The Netherlands Jonathan Moss, Glasgow, UK Prof. Andrzej Wiecek
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
RESISTANT HYPERTENSION
 RESISTANT HYPERTENSION John D. Bisognano, MD PhD Professor of Medicine / Cardiology President-Elect, American Society of Hypertension Director, Outpatient Cardiology University of Rochester RESISTANT HYPERTENSION
RESISTANT HYPERTENSION John D. Bisognano, MD PhD Professor of Medicine / Cardiology President-Elect, American Society of Hypertension Director, Outpatient Cardiology University of Rochester RESISTANT HYPERTENSION
Hypertension: What s new since JNC 7. Harold M. Szerlip, MD, FACP, FCCP, FASN, FNKF
 Hypertension: What s new since JNC 7 Harold M. Szerlip, MD, FACP, FCCP, FASN, FNKF Disclosures Spectral Diagnostics Site investigator Eli Lilly Site investigator ACP IM ITE writing committee NBME Step
Hypertension: What s new since JNC 7 Harold M. Szerlip, MD, FACP, FCCP, FASN, FNKF Disclosures Spectral Diagnostics Site investigator Eli Lilly Site investigator ACP IM ITE writing committee NBME Step
Patrick Kay, General and Interventional Cardiologist Auckland or healthpoint.co.nz
 Patrick Kay, General and Interventional Cardiologist Auckland ipatkay@hotmail.com or healthpoint.co.nz Rotorua 2015 Rotorua 2015 Graphical example of true mean and variation, and of regression to the
Patrick Kay, General and Interventional Cardiologist Auckland ipatkay@hotmail.com or healthpoint.co.nz Rotorua 2015 Rotorua 2015 Graphical example of true mean and variation, and of regression to the
Radiofrequency Ablation of the Renal Sympathetic Nerves as a Treatment for Resistant Hypertension
 Radiofrequency Ablation of the Renal Sympathetic Nerves as a Treatment for Resistant Hypertension Policy Number: 7.01.136 Last Review: 5/2018 Origination: 11/2015 Next Review: 11/2018 Policy Blue Cross
Radiofrequency Ablation of the Renal Sympathetic Nerves as a Treatment for Resistant Hypertension Policy Number: 7.01.136 Last Review: 5/2018 Origination: 11/2015 Next Review: 11/2018 Policy Blue Cross
Renal Denervation: Back to the Future?
 Renal Denervation: Back to the Future? RCP BHS Hypertension State of the Art 27 th June 2016 Adrian J.B. Brady MD, FRCP(Glasg), FRCPE, FBHS, FESC, FAHA Associate Professor, University of Glasgow Consultant
Renal Denervation: Back to the Future? RCP BHS Hypertension State of the Art 27 th June 2016 Adrian J.B. Brady MD, FRCP(Glasg), FRCPE, FBHS, FESC, FAHA Associate Professor, University of Glasgow Consultant
Colin Edwards. Cardiologist Auckland Heart Group Waitemata Health
 Colin Edwards Cardiologist Auckland Heart Group Waitemata Health August 2011 BP MEASUREMENTS measured seated mean of 2 or BP recordings at least 2 visits 2 x risk of developing true hypertension Size of
Colin Edwards Cardiologist Auckland Heart Group Waitemata Health August 2011 BP MEASUREMENTS measured seated mean of 2 or BP recordings at least 2 visits 2 x risk of developing true hypertension Size of
Managing HTN in the Elderly: How Low to Go
 Managing HTN in the Elderly: How Low to Go Laxmi S. Mehta, MD, FACC The Ohio State University Medical Center Assistant Professor of Clinical Internal Medicine Clinical Director of the Women s Cardiovascular
Managing HTN in the Elderly: How Low to Go Laxmi S. Mehta, MD, FACC The Ohio State University Medical Center Assistant Professor of Clinical Internal Medicine Clinical Director of the Women s Cardiovascular
Update on HTN and ABPM. Raj Padwal Division of General Internal Medicine University of Alberta
 Update on HTN and ABPM Raj Padwal Division of General Internal Medicine University of Alberta Disclosures Funding: CIHR, AIHS, HSF, UHF Research Collaboration: Novo Nordisk, CVRx Consulting: Vivus, Medtronic
Update on HTN and ABPM Raj Padwal Division of General Internal Medicine University of Alberta Disclosures Funding: CIHR, AIHS, HSF, UHF Research Collaboration: Novo Nordisk, CVRx Consulting: Vivus, Medtronic
Assessing Blood Pressure for Clinical Research: Pearls & Pitfalls
 Assessing Blood Pressure for Clinical Research: Pearls & Pitfalls Anthony J. Viera, MD, MPH, FAHA Department of Family Medicine Hypertension Research Program UNC School of Medicine Objectives Review limitations
Assessing Blood Pressure for Clinical Research: Pearls & Pitfalls Anthony J. Viera, MD, MPH, FAHA Department of Family Medicine Hypertension Research Program UNC School of Medicine Objectives Review limitations
Life After CORAL: What Did CORAL Prove? David Paul Slovut, MD, PhD Co-director TAVR, Dir of Advanced Intervention
 Life After CORAL: What Did CORAL Prove? David Paul Slovut, MD, PhD Co-director TAVR, Dir of Advanced Intervention No Relationships to Disclose The Need for Modern Renal Trials Increased rate of RAS diagnosis
Life After CORAL: What Did CORAL Prove? David Paul Slovut, MD, PhD Co-director TAVR, Dir of Advanced Intervention No Relationships to Disclose The Need for Modern Renal Trials Increased rate of RAS diagnosis
Treating Hypertension With a Catheter..Wait What? COI 5/3/2013. Worldwide Prevalence of Hypertension Is Increasing
 Treating Hypertension With a Catheter..Wait What? David P. Lee, M.D. 4 May 2013 Stanford University COI Medtronic: Research Grant, Consultant Boston Scientific: Research Grant, MAB Worldwide Prevalence
Treating Hypertension With a Catheter..Wait What? David P. Lee, M.D. 4 May 2013 Stanford University COI Medtronic: Research Grant, Consultant Boston Scientific: Research Grant, MAB Worldwide Prevalence
Preventing and Treating High Blood Pressure
 Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
High blood pressure (Hypertension)
") High blood pressure (Hypertension) Information for patients from the Department of Renal (Kidney) Medicine This leaflet is not meant to replace the information discussed between you and your doctor, but
High blood pressure (Hypertension) Information for patients from the Department of Renal (Kidney) Medicine This leaflet is not meant to replace the information discussed between you and your doctor, but
JNC 8 -Controversies. Sagren Naidoo Nephrologist CMJAH
 JNC 8 -Controversies Sagren Naidoo Nephrologist CMJAH Joint National Committee (JNC) Panel appointed by the National Heart, Lung, and Blood Institute (NHLBI) First guidelines (JNC-1) published in 1977
JNC 8 -Controversies Sagren Naidoo Nephrologist CMJAH Joint National Committee (JNC) Panel appointed by the National Heart, Lung, and Blood Institute (NHLBI) First guidelines (JNC-1) published in 1977
Hypertension 2015: Recent Evidence that Will Change Your Practice
 Hypertension 2015: Recent Evidence that Will Change Your Practice Gerald W. Smetana, M.D. Division of General Medicine Beth Israel Deaconess Medical Center Professor of Medicine Harvard Medical School
Hypertension 2015: Recent Evidence that Will Change Your Practice Gerald W. Smetana, M.D. Division of General Medicine Beth Israel Deaconess Medical Center Professor of Medicine Harvard Medical School
Slide notes: References:
 1 2 3 Cut-off values for the definition of hypertension are systolic blood pressure (SBP) 135 and/or diastolic blood pressure (DBP) 85 mmhg for home blood pressure monitoring (HBPM) and daytime ambulatory
1 2 3 Cut-off values for the definition of hypertension are systolic blood pressure (SBP) 135 and/or diastolic blood pressure (DBP) 85 mmhg for home blood pressure monitoring (HBPM) and daytime ambulatory
CATHETER-BASED RENAL DENERVATION INCREASES INSULIN SENSITIVITY AND IMPROVES GLUCOSE METABOLISM IN PATIENTS WITH RESISTANT HYPERTENSION
 CATHETER-BASED RENAL DENERVATION INCREASES INSULIN SENSITIVITY AND IMPROVES GLUCOSE METABOLISM IN PATIENTS WITH RESISTANT HYPERTENSION F. Mahfoud, Ch. Ukena, B. Cremers, I. Kindermann, M. Kindermann, P.
CATHETER-BASED RENAL DENERVATION INCREASES INSULIN SENSITIVITY AND IMPROVES GLUCOSE METABOLISM IN PATIENTS WITH RESISTANT HYPERTENSION F. Mahfoud, Ch. Ukena, B. Cremers, I. Kindermann, M. Kindermann, P.
Hypertension in 2015: SPRINT-ing ahead of JNC-8. MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic
 Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
Συμπεράσματα από τις νέες μελέτες για την αρτηριακή υπέρταση (SPRINT,PATHAY 2,HOPE 3)
") Συμπεράσματα από τις νέες μελέτες για την αρτηριακή υπέρταση (SPRINT,PATHAY 2,HOPE 3) Χάρης Γράσσος MD,FESC,PhD,EHS Διευθυντής Καρδιολόγος Γ.Ν.Α ΚΑΤ Visiting Professor University of Bolton U.K New England
Συμπεράσματα από τις νέες μελέτες για την αρτηριακή υπέρταση (SPRINT,PATHAY 2,HOPE 3) Χάρης Γράσσος MD,FESC,PhD,EHS Διευθυντής Καρδιολόγος Γ.Ν.Α ΚΑΤ Visiting Professor University of Bolton U.K New England
Treating Hypertension in 2018: What Makes the Most Sense Today?
 Treating Hypertension in 2018: What Makes the Most Sense Today? Daniel Blanchard, MD Professor of Medicine UC San Diego Cardiovascular Center La Jolla, California 1 2 Speaker Disclosures Consultant and/or
Treating Hypertension in 2018: What Makes the Most Sense Today? Daniel Blanchard, MD Professor of Medicine UC San Diego Cardiovascular Center La Jolla, California 1 2 Speaker Disclosures Consultant and/or
Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, Financial Disclosures
 Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, 2015 William C. Cushman, MD Professor, Preventive Medicine, Medicine, and Physiology University
Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, 2015 William C. Cushman, MD Professor, Preventive Medicine, Medicine, and Physiology University
Hypertension in Geriatrics. Dr. Allen Liu Consultant Nephrologist 10 September 2016
 Hypertension in Geriatrics Dr. Allen Liu Consultant Nephrologist 10 September 2016 Annual mortality (%) Cardiovascular Mortality Rates are Higher among Dialysis Patients 100 10 1 0.1 0.01 0.001 25-34
Hypertension in Geriatrics Dr. Allen Liu Consultant Nephrologist 10 September 2016 Annual mortality (%) Cardiovascular Mortality Rates are Higher among Dialysis Patients 100 10 1 0.1 0.01 0.001 25-34
HYPERTENSION: UPDATE 2018
 HYPERTENSION: UPDATE 2018 From the Cardiologist point of view Richard C Padgett, MD I have no disclosures HYPERTENSION ALWAYS THE ELEPHANT IN THE EXAM ROOM BUT SOMETIMES IT CHARGES HTN IN US ~78 million
HYPERTENSION: UPDATE 2018 From the Cardiologist point of view Richard C Padgett, MD I have no disclosures HYPERTENSION ALWAYS THE ELEPHANT IN THE EXAM ROOM BUT SOMETIMES IT CHARGES HTN IN US ~78 million
Modern Management of Hypertension
 Modern Management of Hypertension Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Hypertension Prevalence
Modern Management of Hypertension Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Hypertension Prevalence
Hypertension Update 2009
 Hypertension Update 2009 New Drugs, New Goals, New Approaches, New Lessons from Clinical Trials Timothy C Fagan, MD, FACP Professor Emeritus University of Arizona New Drugs Direct Renin Inhibitors Endothelin
Hypertension Update 2009 New Drugs, New Goals, New Approaches, New Lessons from Clinical Trials Timothy C Fagan, MD, FACP Professor Emeritus University of Arizona New Drugs Direct Renin Inhibitors Endothelin
Clinical Policy Title: Renal denervation
 Clinical Policy Title: Renal denervation Clinical Policy Number: 09.03.04 Effective Date: February 1, 2017 Initial Review Date: November 16, 2016 Most Recent Review Date: January 11, 2018 Next Review Date:
Clinical Policy Title: Renal denervation Clinical Policy Number: 09.03.04 Effective Date: February 1, 2017 Initial Review Date: November 16, 2016 Most Recent Review Date: January 11, 2018 Next Review Date:
When should you treat blood pressure in the young?
 ESC Stockholm - Dilemmas in Cardiovascular Disease Prevention in the Young: 30 th August 2010 When should you treat blood pressure in the young? Bryan Williams MD FRCP FAHA FESC Professor of Medicine Department
ESC Stockholm - Dilemmas in Cardiovascular Disease Prevention in the Young: 30 th August 2010 When should you treat blood pressure in the young? Bryan Williams MD FRCP FAHA FESC Professor of Medicine Department
Special Lecture 11/08/2013. Hypertension Dr. HN Mayrovitz
 Special Lecture 11/08/2013 Hypertension Dr. HN Mayrovitz Arterial Blood Pressure (ABP) Major Factors Summarized Sympathetic Hormones Arteriole MAP ~ Q x TPR + f (V / C) SV x HR Renal SBP Hypertension =
Special Lecture 11/08/2013 Hypertension Dr. HN Mayrovitz Arterial Blood Pressure (ABP) Major Factors Summarized Sympathetic Hormones Arteriole MAP ~ Q x TPR + f (V / C) SV x HR Renal SBP Hypertension =
BackBeat Cardiac Neuromodulation Therapy (CNT) for Immediate, Substantial and Sustained Lowering of Blood Pressure. Daniel Burkhoff MD PhD
 for Immediate, Substantial and Sustained Lowering of Blood Pressure. Daniel Burkhoff MD PhD") BackBeat Cardiac Neuromodulation Therapy (CNT) for Immediate, Substantial and Sustained Lowering of Blood Pressure Daniel Burkhoff MD PhD Director Heart Failure, Hemodynamics and Mechanical Support Research
BackBeat Cardiac Neuromodulation Therapy (CNT) for Immediate, Substantial and Sustained Lowering of Blood Pressure Daniel Burkhoff MD PhD Director Heart Failure, Hemodynamics and Mechanical Support Research
Brent M. Egan, MD Professor of Medicine USCSOM Greenville
 Contemporary Management of Uncontrolled and Treatment Resistant Hypertension Brent M. Egan, MD Professor of Medicine USCSOM Greenville Disclosures (past 3 years): Honoraria: BCBSSC, Medtronic Grant Support:
Contemporary Management of Uncontrolled and Treatment Resistant Hypertension Brent M. Egan, MD Professor of Medicine USCSOM Greenville Disclosures (past 3 years): Honoraria: BCBSSC, Medtronic Grant Support:
Importance of Ambulatory Blood Pressure Monitoring in Adolescents
 Importance of Ambulatory Blood Pressure Monitoring in Adolescents Josep Redon, MD, PhD, FAHA Internal Medicine Hospital Clinico Universitario de Valencia University of Valencia CIBERObn Instituto de Salud
Importance of Ambulatory Blood Pressure Monitoring in Adolescents Josep Redon, MD, PhD, FAHA Internal Medicine Hospital Clinico Universitario de Valencia University of Valencia CIBERObn Instituto de Salud
Φαρµακευτική θεραπεία υπερτασικών ασθενών. Δ. Τσιαχρής, Καρδιολόγος, Α Πανεπιστηµαική Καρδιολογική Κλινική
 Φαρµακευτική θεραπεία υπερτασικών ασθενών Δ. Τσιαχρής, Καρδιολόγος, Α Πανεπιστηµαική Καρδιολογική Κλινική A 42-Year-Old Female with True Severe Resistant Hypertension Female, 42 years old, smoker BMI:
Φαρµακευτική θεραπεία υπερτασικών ασθενών Δ. Τσιαχρής, Καρδιολόγος, Α Πανεπιστηµαική Καρδιολογική Κλινική A 42-Year-Old Female with True Severe Resistant Hypertension Female, 42 years old, smoker BMI:
Renal Sympathetic Denervation for Treatment of Resistant Hypertension: 18-Month Results from the Symplicity HTN-2 Randomized Controlled Trial
 Renal Sympathetic Denervation for Treatment of Resistant Hypertension: 18-Month Results from the Symplicity HTN-2 Randomized Controlled Trial Prof Murray Esler Baker IDI Heart and Diabetes Institute, Melbourne
Renal Sympathetic Denervation for Treatment of Resistant Hypertension: 18-Month Results from the Symplicity HTN-2 Randomized Controlled Trial Prof Murray Esler Baker IDI Heart and Diabetes Institute, Melbourne
A/Prof Gerard Wilkins. A/Proff of Medicine at Otago University Cardiac Services at Dunedin Hospital
 A/Prof Gerard Wilkins A/Proff of Medicine at Otago University Cardiac Services at Dunedin Hospital Hypertension Ambulatory BP Monitoring Gerard T Wilkins Assoc Professor of Medicine, Consultant Cardiologist,
A/Prof Gerard Wilkins A/Proff of Medicine at Otago University Cardiac Services at Dunedin Hospital Hypertension Ambulatory BP Monitoring Gerard T Wilkins Assoc Professor of Medicine, Consultant Cardiologist,
Radiofrequency Energy Provides Safe & Durable Blood Pressure Reduction: Complete 3 Year Results from Symplicity HTN-1
 Radiofrequency Energy Provides Safe & Durable Blood Pressure Reduction: Complete 3 Year Results from Symplicity HTN-1 Henry Krum MBBS PhD FRACP FESC for the Symplicity I Investigators CCRE Therapeutics,
Radiofrequency Energy Provides Safe & Durable Blood Pressure Reduction: Complete 3 Year Results from Symplicity HTN-1 Henry Krum MBBS PhD FRACP FESC for the Symplicity I Investigators CCRE Therapeutics,
Ejection Fraction in Patients With Chronic Heart Failure. Diastolic Heart Failure or Heart Failure with Preserved Ejection Fraction
 Diastolic Heart Failure or Heart Failure with Preserved Ejection Fraction Keith Miller MD Diastolic Heart Failure Risk Factors Common Risk Factors Aging Female gender Obesity Hypertension Diabetes mellitus
Diastolic Heart Failure or Heart Failure with Preserved Ejection Fraction Keith Miller MD Diastolic Heart Failure Risk Factors Common Risk Factors Aging Female gender Obesity Hypertension Diabetes mellitus
CKD & HT. Anne-Marie Angus
 CKD & HT Anne-Marie Angus Hypertension definitions Persisting BP >140/90 and HBPM >135/85 Stage 1 >140/90 (HBPM >135/85) Stage 2 >160/100 (HBPM >150/90) Severe >180/100 White coat HT Why treat? A major
CKD & HT Anne-Marie Angus Hypertension definitions Persisting BP >140/90 and HBPM >135/85 Stage 1 >140/90 (HBPM >135/85) Stage 2 >160/100 (HBPM >150/90) Severe >180/100 White coat HT Why treat? A major
Hypertension and Cardiovascular Disease
 Hypertension and Cardiovascular Disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
Hypertension and Cardiovascular Disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
Transcatheter Renal Denervation and Hong Kong Experience
 Transcatheter Renal Denervation and Hong Kong Experience Dr. Steven Li Siu-lung FACC, FESC, FRCP, FACP Director, Heart Centre, Union Hospital President, Hong Kong Society of Congenital and Structural Heart
Transcatheter Renal Denervation and Hong Kong Experience Dr. Steven Li Siu-lung FACC, FESC, FRCP, FACP Director, Heart Centre, Union Hospital President, Hong Kong Society of Congenital and Structural Heart
Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension
 Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension Prof. Massimo Volpe, MD, FAHA, FESC, Chair of Cardiology, Department of Clinical and Molecular Medicine
Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension Prof. Massimo Volpe, MD, FAHA, FESC, Chair of Cardiology, Department of Clinical and Molecular Medicine
Jared Moore, MD, FACP
 Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner