Sasha Dubrovsky, MSc MD FRCPC Pediatric Emergency Medicine Montreal Children s Hospital - MUHC October 2010
|
|
|
- Emerald Wilson
- 5 years ago
- Views:
Transcription


1 Sasha Dubrovsky, MSc MD FRCPC Pediatric Emergency Medicine Montreal Children s Hospital - MUHC October 2010
2 Learning objectives 1. Discuss diagnostic goals in pediatric trauma Diagnose All vs. Severe Injuries Risks vs. benefit of CT Scan 2. Recognize which blunt torso trauma patients are at high risk for injuries 3. Role of bedside U/S in pediatric trauma
3 Trauma # 1 killer children > 1 years old 20% ED visits trauma related Predominant mechanism BLUNT MVC Auto vs. Pedestrian Bicycle-related Fall
4 Major Trauma Head Most common injury Responsible for 80% trauma deaths Thorax Account for ~15% trauma related deaths Abdomen Common cause of initially missed fatal injuries
5 Pediatric ED s Trauma Paradigm: Assess all trauma patients Minor Major Diagnose and manage Clinically apparent injuries Occult injuries Do no harm Both at risk of occult injury Ex. CT radiation Ex. Missed serious injuries
6 Overview Case Radiation Risks of computer tomography Common injuries Intra-abdominal Injury (IAI) Role of screening tests Pediatric Bedside Ultrasound

7 Computed tomography Imaging gold standard Cost Sedation and transport considerations Severe injuries less common than in adults Most injuries managed conservatively Radiation Risks
8 Radiation imparts an increased lifetime risk of cancer MORTALITY 1 per 1000 pediatric CT 1 per 3000 adult CT
9 1/550 1/1000 Brenner et al. NEJM 2001 Lifetime attributable cancer mortality risk as a function of age for a single typical CT examination
10 ALARA As Low As Reasonably Achievable Principle Limiting number of CT scans ordered (Physician) Size-based adjustments of scanning parameters (Radiology Department)
11
12 Who should get CT? Is there a way to stratify those at higher risk of serious injury and need for intervention? Ex: Head Injury CATCH, PECARN, Canadian CT Ex: C-Spine NEXUS, Canadian c/spine
13 Who should get CT? How to select out those blunt trauma patients at highest risk of severe injury to the abdomen?
14 Intra-Abdominal Injuries (IAI) Seen in 10-30% pediatric multisystem traumas Common cause of initially unrecognized fatal injuries Mechanism MVC (especially lateral impact MVC, seat belt use, ejected) Pedestrian Falls (especially >10 feet) Abuse/Assault
15 Intra Abdominal Injury Most common injuries Liver Spleen Kidney Less common include Hollow viscus Pancreas Bladder
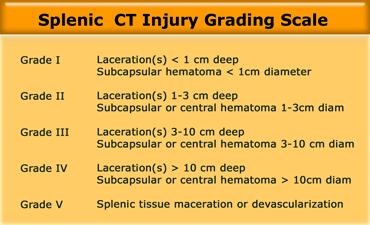

16 Spleen


17 Stable Patient with IAI: Non-operative Management American Pediatric Surgical Association Guideline 2000
18 Non-operative Management McVay et al Throw out the grade book for stable patients Admit x 24 hours NPO and bedrest Serial exam Serial 6, 12, 24 hours (HCT>0.21) Clinic in 1 month with U/S
19 Regardless of conservative strategy, >95% managed successfully with no intervention Of those who fail, become apparent clinically Mainly high grade injuries (Grades 4+) Clear discharge instruction Ex. Delayed Splenic Bleed rate 0.33%-1.4% (Davies et al 2009, Zarzour et al. 2009)
20 So what to do Risk vs. benefit Trauma center philosophy Identify ALL Then need to scan ALL Identify Severe Need to identify strategy to identify those at high risk
21 Risk Stratification based on investigations To dip or not to dip? That is the question

22 Risk Stratification via investigations Taylor et al children with CT Abdomen Hematuria in 68% Hematuria risk (1.6 fold) of any IAI liver (33%) spleen (37%) renal (27%) However, only Symptomatic Hematuria at risk
23 Risk Stratification via investigations Holmes et al Prospective observational study, age < patients enrolled, trauma team activation Goal: identify elements of physical exam and laboratory data predictive of IAI Identification of children with intra-abdominal injuries after blunt trauma. Annals of Emergency Medicine 2002, 39:
24 Imaging or Look inside in 664/1095 (64%) 36% not investigated NO apparent cases of missed IAI (1 week phone f/u + rechecked registry at end of study)
25 10% intra-abdominal injury Mean age 8.4 ± 4.8 years 73% had free fluid Organs injured: Liver 41% Spleen 38% GI tract 23% Urinary tract 15% Multiple Injury 22%
26 85% patients with IAI had physical exam findings suggestive Abdominal tenderness BP Femur Fracture GCS 13 ( unreliable exam )
27 15% OCCULT intra-abdominal injury

28
29
30
31 Validation Study: Holmes et al Pediatric Validation Study 1119 patients, 14% IAI 68% Positive rule 20% IAI 32% Negative rule 2% IAI Sensitivity 95% 7/8 missed observation alone 1/8 Non-therapeutic laparotomy (seatbelt)

32

33 Focused Assessment with Sonography in Trauma (aka FAST)

")
34 FAST Morison s Pouch (RUQ)


35 FAST Left Upper Quadrant



36 FAST Pelvic
37 Adult FAST SOAP RCT Trial by Melinker et al Decreased time to operative care (57 vs 166 min) Shorter hospital lengths of stay (6 vs 10 days) Less likely to have CT Torso Lower hospital charges Fewer complication rates
38 Pediatric FAST No clear role Conservative management for most FAST less sensitive Not well studied
39 Why is literature so confusing? U/S Performer: Trauma Team Leader (TTL) vs. Radiology Diverse training/experience U/S Goal: Free fluid: Population: Outcome: Free fluid vs. Parenchymal vs. both Absent in up to 30% pediatric IAI Severe trauma vs. All trauma CT vs. Clinical Course
40 FAST Performer When looking for free fluid Radiology = TTL (surgical or ED)
41 U/S Goal Free fluid vs. parenchymal Radiology based studies Ex. Richards et al Liver Injury CT Grade Sensitivity Free Fluid Sensitivity Free Fluid ± Parenchymal 1 17 % 26 % 2 74 % 80 % 3 97 % 97 % % 100 % % 100 %

42 Free Fluid Emery et al Observational study in children Outcome: any IAI on CT Sensitivity 45%, Specificity 88%, NPV 81% Most of false negative low grade
43 Population Holmes et al Normotensive Sensitivity 82%, Specificity 95%, NPV 97% BP 100% Sensitivity Hypotensive (n=13) Sensitivity 100%, Specificity 100%, NPV 100% 98% (n=187) negative FAST conservatively managed 2 GI tract injury \ 2 liver ( LFTs )
44 Outcome Soudack et al (radiology) 313 pediatric patients Outcome: + CT/OR or Normal follow-up Sensitivity 93% specificity 97% PPV 95% NPV 96% 65% FAST negative No IAI \ nor late complications Since introduction of FAST, use of CT
45 FAST by Pediatric TTL Thourani et al patients <15 years old by PGY 3 + Sensitivity 80% Specificity 100% NPV 96% 2 false negative 2 yo Trace fluid no IAI 11 yo Pedestrian with repeat FAST + and splenic injury
46 FAST by pediatric TTL Patrick et al children with BAT Sensitivity 71% Specificity 100% NPV 93% Sensitivity 100% for Significant free fluid
47 Meta-analysis Pediatric FAST Holmes et al studies, all cohort, 3838 children U/S Protocol FAST FAST FAST (free fluid) (free fluid) (free fluid and solid organs) Outcome of interest Hemoperitoneum Any IAI Any IAI Sensitivity 80% 66% 82% Specificity 96% 93% 97% Likelihood ratio % Likelihood ratio
48

49
50 Physical Exam with FAST Suthers et al Prospective observational study <17 yo 180 children screened 120 had FAST/ P/E / CT Mean age 10, ISS 13, mostly blunt trauma Sensitivity Specificity PPV NPV Physical Exam 81% 73% 47% 93% FAST 70% 100% 100% 92% P/E + FAST 100% 75% 54% 100%
51 LFTs and FAST Sola et al (Jackson Memorial, Miami) Retrospective review 400 patients Mean age 9, Mean ISS 16 Any injury on CT (including injuries with no free fluid) FAST alone: FN=67, >2/3 low grade liver/spleen If take out low grade, FAST sensitivity >80% Sensitivity Specificity PPV NPV FAST 50% 91% 68% 83% FAST + LFTs 88% 98% 94% 96%
52 Serial FAST Blackbourne et al Serial FAST within 24 hours by TTL (on-call residents) Mean age 39 [1-90], mean time to 2 nd FAST 4 hours Outcome: clinical course Sensitivity Specificity PPV NPV Initial U/S 31% 99.8% 95% 92% Second U/S 72% 99.8% 98% 97%
53 Serial FAST Blackbourne et al % FAST negative had CT/OR 2/501 (0.4%) Neg-Neg OR (hollow-viscus) 10/26 (35 %) Neg-Pos OR

54 Advanced trauma application Pneumothorax Bedside u/s more sensitive than supine CXR Sensitivity 98% vs. 75%
55 Bedside Ultrasound Clear role in pediatric BAT screens for those at high risk severe IAI (i.e. high grade injury)
56 Proposed Algorithm
57 Potential Algorithm FAST + Serial FAST +
58 Summary Occult abdominal injuries up to 10% Most injuries managed conservatively CT-SCAN ALL NOT INDICATED select those at high risk of severe injuries Serial Exams Serial Bedside U/S CXR Screening HCT, LFT, U/A

59 Conclusion As pediatric trauma experts Need to diagnose severe injuries Need to ensure no harm Educate / Primary prevention
Evaluation of Children with Blunt Abdominal Trauma. James F. Holmes, MD, MPH UC Davis School of Medicine
 Evaluation of Children with Blunt Abdominal Trauma James F. Holmes, MD, MPH UC Davis School of Medicine Objectives Epidemiology of intra-abdominal injury (IAI) Physical examination findings with IAI Laboratory
Evaluation of Children with Blunt Abdominal Trauma James F. Holmes, MD, MPH UC Davis School of Medicine Objectives Epidemiology of intra-abdominal injury (IAI) Physical examination findings with IAI Laboratory
The Role of the FAST exam in the EDRU
 The Role of the FAST exam in the EDRU A. Robb McLean, MD, MHCM Vice Chair of Clinical Operations, Department of Emergency Medicine Joint Trauma Conference June 20, 2017 Disclosures Goals Describe the performance,
The Role of the FAST exam in the EDRU A. Robb McLean, MD, MHCM Vice Chair of Clinical Operations, Department of Emergency Medicine Joint Trauma Conference June 20, 2017 Disclosures Goals Describe the performance,
Imaging in the Trauma Patient
 Imaging in the Trauma Patient David A. Spain, MD Department of Surgery Stanford University Pan Scan Instead of Clinical Exam? 1 Granted, some patients don t need CT scan Platinum Package Stanford Special
Imaging in the Trauma Patient David A. Spain, MD Department of Surgery Stanford University Pan Scan Instead of Clinical Exam? 1 Granted, some patients don t need CT scan Platinum Package Stanford Special
PEDIATRIC BLUNT TRAUMA WHAT S DIFFERENT? NORDIC TRAUMA COURSE 2016
 PEDIATRIC BLUNT TRAUMA WHAT S DIFFERENT? NORDIC TRAUMA COURSE 2016 Ken F. Linnau, MD, MS Emergency Radiology Harborview Medical Center University of Washington Seattle, WA Thanks to Nupur Verma, MD University
PEDIATRIC BLUNT TRAUMA WHAT S DIFFERENT? NORDIC TRAUMA COURSE 2016 Ken F. Linnau, MD, MS Emergency Radiology Harborview Medical Center University of Washington Seattle, WA Thanks to Nupur Verma, MD University
George M Wadie, MD Director Division of Pediatric Surgery Sacred Heart Medical Center. Springfield, OR Adjunct Assistant Professor of Surgery Oregon
 George M Wadie, MD Director Division of Pediatric Surgery Sacred Heart Medical Center. Springfield, OR Adjunct Assistant Professor of Surgery Oregon Health and Sciences University. Portland, OR Outline
George M Wadie, MD Director Division of Pediatric Surgery Sacred Heart Medical Center. Springfield, OR Adjunct Assistant Professor of Surgery Oregon Health and Sciences University. Portland, OR Outline
2. Blunt abdominal Trauma
 Abdominal Trauma 1. Evaluation and management depends on: a. Mechanism (Blunt versus Penetrating) b. Injury complex in addition to abdomen c. Haemodynamic stability assessment: i. Classically patient s
Abdominal Trauma 1. Evaluation and management depends on: a. Mechanism (Blunt versus Penetrating) b. Injury complex in addition to abdomen c. Haemodynamic stability assessment: i. Classically patient s
Pediatric Abdomen Trauma
 Pediatric Abdomen Trauma Susan D. John, MD, FACR Pediatric Trauma Trauma is leading cause of death and disability in children and adolescents Causes and effects vary between age groups Blunt trauma predominates
Pediatric Abdomen Trauma Susan D. John, MD, FACR Pediatric Trauma Trauma is leading cause of death and disability in children and adolescents Causes and effects vary between age groups Blunt trauma predominates
Pediatric Blunt Abdominal Trauma: Solid Organs, Seatbelts, and Sieverts. 23 March. The Plan. Tucker Redfern Symposium Ramin Jamshidi, MD FACS
 Pediatric Blunt Abdominal Trauma: Solid Organs, Seatbelts, and Sieverts Tucker Redfern Symposium 2018 23 March 1965: Gemini 3 launch 2001: Mir scrapped The Plan Solid Organ Injuries Seat-Belt Trauma Abdominal
Pediatric Blunt Abdominal Trauma: Solid Organs, Seatbelts, and Sieverts Tucker Redfern Symposium 2018 23 March 1965: Gemini 3 launch 2001: Mir scrapped The Plan Solid Organ Injuries Seat-Belt Trauma Abdominal
SPECIAL DIAGNOSTIC STUDIES IN BLUNT TRAUMA OLEH : Prof.DR.Dr Abdul Rasyid SpRad (K),Ph.D Dr.Evo Elidar Sp.Rad
,Ph.D Dr.Evo Elidar Sp.Rad") SPECIAL DIAGNOSTIC STUDIES IN BLUNT TRAUMA OLEH : Prof.DR.Dr Abdul Rasyid SpRad (K),Ph.D Dr.Evo Elidar Sp.Rad Trauma Emergency Room layout Ideally the trauma emergency room is centrally located to provide
SPECIAL DIAGNOSTIC STUDIES IN BLUNT TRAUMA OLEH : Prof.DR.Dr Abdul Rasyid SpRad (K),Ph.D Dr.Evo Elidar Sp.Rad Trauma Emergency Room layout Ideally the trauma emergency room is centrally located to provide
Blunt abdominal trauma in children
 REVIEW C URRENT OPINION Blunt abdominal trauma in children Deborah Schonfeld and Lois K. Lee Purpose of review This review will examine the current evidence regarding pediatric blunt abdominal trauma and
REVIEW C URRENT OPINION Blunt abdominal trauma in children Deborah Schonfeld and Lois K. Lee Purpose of review This review will examine the current evidence regarding pediatric blunt abdominal trauma and
of Trauma Assembly 27 th Page 1
 Eastern Association for the Surgery of Trauma 27 th Annual Scientific Assembly Sunrise Session 08 To Scan or Not To Scan Thatt is the Question January 16, 2014 Waldorf Astoria Naples Naples, Floridaa Page
Eastern Association for the Surgery of Trauma 27 th Annual Scientific Assembly Sunrise Session 08 To Scan or Not To Scan Thatt is the Question January 16, 2014 Waldorf Astoria Naples Naples, Floridaa Page
Pan Scan Instead of Clinical Exam? David A. Spain, MD
 Pan Scan Instead of Clinical Exam? David A. Spain, MD Granted, some patients don t t need CT scan Platinum Package Stanford Special CT Scan Head Neck Chest Abdomen Pelvis Takes about 20 minutes to do
Pan Scan Instead of Clinical Exam? David A. Spain, MD Granted, some patients don t t need CT scan Platinum Package Stanford Special CT Scan Head Neck Chest Abdomen Pelvis Takes about 20 minutes to do
Study of management of blunt injuries to solid abdominal organs
 Original article: Study of management of blunt injuries to solid abdominal organs 1Dr. Jayant Jain, 2 Dr. S.P. Singh, 3 Dr. Arun Bhargava 1III year resident, Dept of General Surgery NIMS hospital and medical
Original article: Study of management of blunt injuries to solid abdominal organs 1Dr. Jayant Jain, 2 Dr. S.P. Singh, 3 Dr. Arun Bhargava 1III year resident, Dept of General Surgery NIMS hospital and medical
Thicker than Water. Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago
 Thicker than Water Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago I have no relevant financial relationships to disclose. Who is bleeding? How much and what kind
Thicker than Water Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago I have no relevant financial relationships to disclose. Who is bleeding? How much and what kind
Role of FAST or Abdominal Ultrasound to Limit CT Imaging in Evaluation of the Pediatric Abdominal Trauma Patient
 Curr Surg Rep (2014) 2:56 DOI 10.1007/s40137-014-0056-z PEDIATRIC TRAUMA SURGERY (AC FISCHER, SECTION EDITOR) Role of FAST or Abdominal Ultrasound to Limit CT Imaging in Evaluation of the Pediatric Abdominal
Curr Surg Rep (2014) 2:56 DOI 10.1007/s40137-014-0056-z PEDIATRIC TRAUMA SURGERY (AC FISCHER, SECTION EDITOR) Role of FAST or Abdominal Ultrasound to Limit CT Imaging in Evaluation of the Pediatric Abdominal
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines
 Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Blunt Abdominal Trauma Evaluation and Management Guideline PEDIATRIC Practice Management Guideline Contact: Trauma Center
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Blunt Abdominal Trauma Evaluation and Management Guideline PEDIATRIC Practice Management Guideline Contact: Trauma Center
NON-OPERATIVE MANAGEMENT OF PEDIATRIC SOLID ORGAN INJURY
 NON-OPERATIVE MANAGEMENT OF PEDIATRIC SOLID ORGAN INJURY JESSICA A. NAIDITCH, MD TRAUMA MEDICAL DIRECTOR, DELL CHILDREN S MEDICAL CENTER OF CENTRAL TEXAS ASSISTANT PROFESSOR OF SURGERY AND PERIOPERATIVE
NON-OPERATIVE MANAGEMENT OF PEDIATRIC SOLID ORGAN INJURY JESSICA A. NAIDITCH, MD TRAUMA MEDICAL DIRECTOR, DELL CHILDREN S MEDICAL CENTER OF CENTRAL TEXAS ASSISTANT PROFESSOR OF SURGERY AND PERIOPERATIVE
UC Irvine Western Journal of Emergency Medicine: Integrating Emergency Care with Population Health
 UC Irvine Western Journal of Emergency Medicine: Integrating Emergency Care with Population Health Title Analysis of Urobilinogen and Urine Bilirubin for Intra-Abdominal Injury in Blunt Trauma Patients
UC Irvine Western Journal of Emergency Medicine: Integrating Emergency Care with Population Health Title Analysis of Urobilinogen and Urine Bilirubin for Intra-Abdominal Injury in Blunt Trauma Patients
Use of CT in minor traumatic brain injury. Lisa Ayoub-Rodriguez, MD Bert Johansson, MD Michael Lee, MD
 Use of CT in minor traumatic brain injury Lisa Ayoub-Rodriguez, MD Bert Johansson, MD Michael Lee, MD No financial or other conflicts of interest Epidemiology of traumatic brain injury (TBI) Risks associated
Use of CT in minor traumatic brain injury Lisa Ayoub-Rodriguez, MD Bert Johansson, MD Michael Lee, MD No financial or other conflicts of interest Epidemiology of traumatic brain injury (TBI) Risks associated
Penetrating abdominal trauma clinical view. Ari Leppäniemi, MD Department of Abdominal Surgery Meilahti hospital University of Helsinki Finland
 Penetrating abdominal trauma clinical view Ari Leppäniemi, MD Department of Abdominal Surgery Meilahti hospital University of Helsinki Finland Meilahti hospital - one of Helsinki University hospitals -
Penetrating abdominal trauma clinical view Ari Leppäniemi, MD Department of Abdominal Surgery Meilahti hospital University of Helsinki Finland Meilahti hospital - one of Helsinki University hospitals -
Focused Assessment with Sonography in Trauma (FAST) UC Irvine School of Medicine
 UC Irvine School of Medicine") Focused Assessment with Sonography in Trauma (FAST) UC Irvine School of Medicine Purpose of FAST exam Quickly evaluate patient s status in emergency situations Blunt or penetrating trauma Visualize fluid
Focused Assessment with Sonography in Trauma (FAST) UC Irvine School of Medicine Purpose of FAST exam Quickly evaluate patient s status in emergency situations Blunt or penetrating trauma Visualize fluid
Selective Nonoperative Management of Penetrating Abdominal Trauma. Kings County Hospital Center Verena Liu, MD 10/13/2011
 Selective Nonoperative Management of Penetrating Abdominal Trauma Kings County Hospital Center Verena Liu, MD 10/13/2011 Case Presentation 28M admitted on 8/27/2011 s/p GSW to right upper quadrant and
Selective Nonoperative Management of Penetrating Abdominal Trauma Kings County Hospital Center Verena Liu, MD 10/13/2011 Case Presentation 28M admitted on 8/27/2011 s/p GSW to right upper quadrant and
Head injury in children
 Head injury in children Michael Kim, MD Department of Emergency Medicine University of Wisconsin- Madison #1 cause of death and disability Bimodal distribution 62,000 hospitalization 564,000 ED visits
Head injury in children Michael Kim, MD Department of Emergency Medicine University of Wisconsin- Madison #1 cause of death and disability Bimodal distribution 62,000 hospitalization 564,000 ED visits
The Utility of Sonography for the Triage of Blunt Abdominal Trauma Patients to Exploratory Laparotomy
 FAST for Triage of Blunt Abdominal Trauma Abdominal Imaging Original Research The Utility of Sonography for the Triage of Blunt Abdominal Trauma Patients to Exploratory Brett C. Lee 1 Eleanor L. Ormsby
FAST for Triage of Blunt Abdominal Trauma Abdominal Imaging Original Research The Utility of Sonography for the Triage of Blunt Abdominal Trauma Patients to Exploratory Brett C. Lee 1 Eleanor L. Ormsby
2 Blunt Abdominal Trauma
 2 Blunt Abdominal Trauma Ricardo Ferrada, Diego Rivera, and Paula Ferrada Pearls and Pitfalls Patients suffering a high-energy trauma have solid viscera rupture in the abdomen and/or aortic rupture in
2 Blunt Abdominal Trauma Ricardo Ferrada, Diego Rivera, and Paula Ferrada Pearls and Pitfalls Patients suffering a high-energy trauma have solid viscera rupture in the abdomen and/or aortic rupture in
Extended FAST Exam. Goal of Trauma Care. Golden Hour of Trauma
 Extended FAST Exam Goal of Trauma Care Golden Hour of Trauma Best INITIAL screening modality in trauma efast 2014 LLSA Article (ACEP Policy Statement) Level B Recommendation: In hemodynamically unstable
Extended FAST Exam Goal of Trauma Care Golden Hour of Trauma Best INITIAL screening modality in trauma efast 2014 LLSA Article (ACEP Policy Statement) Level B Recommendation: In hemodynamically unstable
Pediatric Solid Organ Injury
 Pediatric Solid Organ Injury Grand Rounds St. Charles Medical Center Bend, OR July 20, 2018 Disclosures Disclosure of relevant financial relationships in the past 12 months: I have had no relevant financial
Pediatric Solid Organ Injury Grand Rounds St. Charles Medical Center Bend, OR July 20, 2018 Disclosures Disclosure of relevant financial relationships in the past 12 months: I have had no relevant financial
TALK TRAUMA Clearing the C-Spine. David Ouellette
 TALK TRAUMA 2011 Clearing the C-Spine David Ouellette Case #1 - Mother / Daughter MVC 34 y/o female Dangerous mechanism CHI Mumbling incoherently Femur # - distracting injury ETOH - 22 9 y/o female Dangerous
TALK TRAUMA 2011 Clearing the C-Spine David Ouellette Case #1 - Mother / Daughter MVC 34 y/o female Dangerous mechanism CHI Mumbling incoherently Femur # - distracting injury ETOH - 22 9 y/o female Dangerous
Abdominal Trauma. Nat Krairojananan M.D., FRCST Department of Trauma and Emergency Medicine Phramongkutklao Hospital
 Abdominal Trauma Nat Krairojananan M.D., FRCST Department of Trauma and Emergency Medicine Phramongkutklao Hospital overview Quick review abdominal anatomy Review of mechanism of injury Review of investigation
Abdominal Trauma Nat Krairojananan M.D., FRCST Department of Trauma and Emergency Medicine Phramongkutklao Hospital overview Quick review abdominal anatomy Review of mechanism of injury Review of investigation
Guideline for the Management of Blunt Liver and Spleen Injuries
 Pediatric Trauma Practice Guideline Management of Blunt Liver and Spleen Guideline for the Management of Blunt Liver and Spleen Background: Children are more vulnerable to blunt abdominal injury than adults.
Pediatric Trauma Practice Guideline Management of Blunt Liver and Spleen Guideline for the Management of Blunt Liver and Spleen Background: Children are more vulnerable to blunt abdominal injury than adults.
Adult Trauma Advances in Pediatrics. (sometimes they are little adults) FAST examination. Who is bleeding? How much and what kind of TXA volume?
 FAST examination. Who is bleeding? How much and what kind of TXA volume?") Adult Trauma Advances in Pediatrics (sometimes they are little adults) Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago Alisa McQueen MD, FAAP, FACEP Associate
Adult Trauma Advances in Pediatrics (sometimes they are little adults) Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago Alisa McQueen MD, FAAP, FACEP Associate
Abdominal Ultrasonography
 Abdominal Ultrasonography David A. Masneri, DO, FACEP, FAAEM Assistant Professor of Emergency Medicine Assistant Director, Emergency Medicine Residency Medical Director, Operational Medicine Division Center
Abdominal Ultrasonography David A. Masneri, DO, FACEP, FAAEM Assistant Professor of Emergency Medicine Assistant Director, Emergency Medicine Residency Medical Director, Operational Medicine Division Center
MANAGEMENT OF SOLID ORGAN INJURIES
 MANAGEMENT OF SOLID ORGAN INJURIES Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Director of Surgical Critical Care, Harborview Medical Center Introduction Solid organ injury
MANAGEMENT OF SOLID ORGAN INJURIES Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Director of Surgical Critical Care, Harborview Medical Center Introduction Solid organ injury
Little Kids in Big Crashes The Bio-mechanics of Kids in Car Crashes. Lisa Schwing, RN Trauma Program Manager Dayton Children s
 Little Kids in Big Crashes The Bio-mechanics of Kids in Car Crashes Lisa Schwing, RN Trauma Program Manager Dayton Children s Very Little Research There has been very little research on the forces a crash
Little Kids in Big Crashes The Bio-mechanics of Kids in Car Crashes Lisa Schwing, RN Trauma Program Manager Dayton Children s Very Little Research There has been very little research on the forces a crash
Pediatric Trauma. Sept 2nd, Patrick Murphy Neil Merritt
 Pediatric Trauma Sept 2nd, 2015 Patrick Murphy Neil Merritt Objectives Objectives Medical Expert 1. Describe the types of pediatric injuries sustained with a given mode of trauma, and identify the most
Pediatric Trauma Sept 2nd, 2015 Patrick Murphy Neil Merritt Objectives Objectives Medical Expert 1. Describe the types of pediatric injuries sustained with a given mode of trauma, and identify the most
Ultrasound. FAST Focused Assessment with Sonography in Trauma
 Ultrasound FAST Focused Assessment with Sonography in Trauma Rohit Patel, MD University of Florida Health Director, Critical Care Ultrasound Surgical ICU Center for Intensive Care Gainesville, Florida
Ultrasound FAST Focused Assessment with Sonography in Trauma Rohit Patel, MD University of Florida Health Director, Critical Care Ultrasound Surgical ICU Center for Intensive Care Gainesville, Florida
Steven Aaron Ross, M.D. Pediatric Radiologist El Paso Imaging Consultants El Paso Children s Hospital
 Steven Aaron Ross, M.D. Pediatric Radiologist El Paso Imaging Consultants El Paso Children s Hospital I will prescribe regimens for the good of my patients according to my ability and my judgment and never
Steven Aaron Ross, M.D. Pediatric Radiologist El Paso Imaging Consultants El Paso Children s Hospital I will prescribe regimens for the good of my patients according to my ability and my judgment and never
SAS Journal of Surgery ISSN SAS J. Surg., Volume-2; Issue-1 (Jan-Feb, 2016); p Available online at
; p Available online at") SAS Journal of Surgery ISSN 2454-5104 SAS J. Surg., Volume-2; Issue-1 (Jan-Feb, 2016); p-53-59 Available online at http://sassociety.com/sasjs/ Original Research Article Clinical Study, Evaluation and
SAS Journal of Surgery ISSN 2454-5104 SAS J. Surg., Volume-2; Issue-1 (Jan-Feb, 2016); p-53-59 Available online at http://sassociety.com/sasjs/ Original Research Article Clinical Study, Evaluation and
Objectives. The Extended FAST Exam. Focused Assessment e With Sonography In. Trauma (FAST)
") Northern California Emergency Ultrasound Course Objectives The Extended FAST Exam Rimon Bengiamin, MD, RDMS UC SF Discuss the components of the EFAST exam Evaluate the utility of the EFAST Review how to
Northern California Emergency Ultrasound Course Objectives The Extended FAST Exam Rimon Bengiamin, MD, RDMS UC SF Discuss the components of the EFAST exam Evaluate the utility of the EFAST Review how to
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines
 Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Splenic Injury Evaluation and Management Guideline ADULT Practice Management Guideline Contact: Trauma Center Medical
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Splenic Injury Evaluation and Management Guideline ADULT Practice Management Guideline Contact: Trauma Center Medical
PRACTICE GUIDELINE TITLE: NON-OPERATIVE MANAGEMENT OF LIVER / SPLENIC INJURIES
 PRACTICE GUIDELINE Effective Date: 6-18-04 Manual Reference: Deaconess Trauma Services TITLE: N-OPERATIVE MANAGEMENT OF LIVER / SPLENIC INJURIES PURPOSE: To define when non-operative management of liver
PRACTICE GUIDELINE Effective Date: 6-18-04 Manual Reference: Deaconess Trauma Services TITLE: N-OPERATIVE MANAGEMENT OF LIVER / SPLENIC INJURIES PURPOSE: To define when non-operative management of liver
Bladder Trauma Data Collection Sheet
 Bladder Trauma Data Collection Sheet If there was no traumatic injury with PENETRATION of the bladder DO NOT proceed Date of injury: / / Time of injury: Date of hospital arrival: / / Time of hospital arrival:
Bladder Trauma Data Collection Sheet If there was no traumatic injury with PENETRATION of the bladder DO NOT proceed Date of injury: / / Time of injury: Date of hospital arrival: / / Time of hospital arrival:
MEDICAL MANAGEMENT OF ABDOMINAL TRAUMA. LUIS H. TELLO MV, MS, DVM, COS Portland Hospital Classic International Medical Advisor Banfield Pet Hospital
 MEDICAL MANAGEMENT OF ABDOMINAL TRAUMA LUIS H. TELLO MV, MS, DVM, COS Portland Hospital Classic International Medical Advisor Banfield Pet Hospital ABDOMINAL TRAUMA 70-80% of multiple trauma patients 55%
MEDICAL MANAGEMENT OF ABDOMINAL TRAUMA LUIS H. TELLO MV, MS, DVM, COS Portland Hospital Classic International Medical Advisor Banfield Pet Hospital ABDOMINAL TRAUMA 70-80% of multiple trauma patients 55%
CLINICAL MANAGEMENT GUIDELINE PAGE 1 NO REVISION NO. 1 EFFECTIVE DATE: 03/01/2015 SUPERSEDES: 9/26/12
 CLINICAL MANAGEMENT GUIDELINE PAGE 1 REVISION NO. 1 EFFECTIVE DATE: 03/01/2015 SUPERSEDES: 9/26/12 DEPARTMENT (DIVISION): Trauma TITLE: Management of Abdominal Solid Organ Injuries PURPOSE The vast majority
CLINICAL MANAGEMENT GUIDELINE PAGE 1 REVISION NO. 1 EFFECTIVE DATE: 03/01/2015 SUPERSEDES: 9/26/12 DEPARTMENT (DIVISION): Trauma TITLE: Management of Abdominal Solid Organ Injuries PURPOSE The vast majority
A prospective evaluation of the predictive value of serum amylase levels in the assessment of patients with blunt abdominal trauma
 A prospective evaluation of the predictive value of serum amylase levels in the assessment of patients with blunt abdominal trauma I E Donkin, R Jones, C Aldous, D L Clarke Department of General Surgery,
A prospective evaluation of the predictive value of serum amylase levels in the assessment of patients with blunt abdominal trauma I E Donkin, R Jones, C Aldous, D L Clarke Department of General Surgery,
A Severely Injured Pediatric Trauma Patient: Case Presentation and Discussion
 A Severely Injured Pediatric Trauma Patient: Case Presentation and Discussion Christopher Butts PhD, DO Surgical Critical Care Fellow Cooper University Hospital H&P 10 year old female presents as a trauma
A Severely Injured Pediatric Trauma Patient: Case Presentation and Discussion Christopher Butts PhD, DO Surgical Critical Care Fellow Cooper University Hospital H&P 10 year old female presents as a trauma
Free fluid accumulation following blunt abdominal trauma: potential for expansion of the FAST protocol
 Hong Kong Journal of Emergency Medicine Free fluid accumulation following blunt abdominal trauma: potential for expansion of the FAST protocol N Simpson, P Page, DM Taylor Objective: To determine sites
Hong Kong Journal of Emergency Medicine Free fluid accumulation following blunt abdominal trauma: potential for expansion of the FAST protocol N Simpson, P Page, DM Taylor Objective: To determine sites
Caudal Edge of the Liver in the Right Upper Quadrant (RUQ) View Is the Most Sensitive Area for Free Fluid on the FAST Exam
 View Is the Most Sensitive Area for Free Fluid on the FAST Exam") Original Research Caudal Edge of the Liver in the Right Upper Quadrant (RUQ) View Is the Most Sensitive Area for Free Fluid on the FAST Exam Viveta Lobo, MD* Michelle Hunter-Behrend, MD* Erin Cullnan,
Original Research Caudal Edge of the Liver in the Right Upper Quadrant (RUQ) View Is the Most Sensitive Area for Free Fluid on the FAST Exam Viveta Lobo, MD* Michelle Hunter-Behrend, MD* Erin Cullnan,
Muscle spasm Diminished bowel sounds Nausea/vomiting
 3 4 5 6 7 8 9 0 Chapter 8: Abdomen and Genitalia Injuries Abdominal Injuries Abdomen is major body cavity extending from to pelvis. Contains organs that make up digestive, urinary, and genitourinary systems.
3 4 5 6 7 8 9 0 Chapter 8: Abdomen and Genitalia Injuries Abdominal Injuries Abdomen is major body cavity extending from to pelvis. Contains organs that make up digestive, urinary, and genitourinary systems.
Major Trauma Scenarios. Ballarat Health Services Emergency Medicine Training Hub
 Major Trauma Scenarios Ballarat Health Services Emergency Medicine Training Hub Trauma Scenario 1 You receive a phone call from the ambulance service. They have a 27 yr old male involved in a MCA, he is
Major Trauma Scenarios Ballarat Health Services Emergency Medicine Training Hub Trauma Scenario 1 You receive a phone call from the ambulance service. They have a 27 yr old male involved in a MCA, he is
The FAST Exam! Dr. David Easton MD FRCPC Critical Care and Emergency Medicine University of Manitoba Canada
 The FAST Exam! Dr. David Easton MD FRCPC Critical Care and Emergency Medicine University of Manitoba Canada Dr. David Easton MD FRCPC Assistant Professor Section of Critical Care and Emergency Medicine
The FAST Exam! Dr. David Easton MD FRCPC Critical Care and Emergency Medicine University of Manitoba Canada Dr. David Easton MD FRCPC Assistant Professor Section of Critical Care and Emergency Medicine
Avoidable Imaging Learning Collaborative: 2008 Mild Traumatic Brain Injury Clinical Policy Success Story BWH Head and PE CTs with Clinical Decision
 Avoidable Imaging Learning Collaborative: 2008 Mild Traumatic Brain Injury Clinical Policy Success Story BWH Head and PE CTs with Clinical Decision Support Using the Canadian CT Head Rule to Reduce Unnecessary
Avoidable Imaging Learning Collaborative: 2008 Mild Traumatic Brain Injury Clinical Policy Success Story BWH Head and PE CTs with Clinical Decision Support Using the Canadian CT Head Rule to Reduce Unnecessary
Interventional Radiology for Solid Organ Trauma. Case Study 8/17/2017. Diagnosis? Case Study (cont d)
") Interventional Radiology for Solid Organ Trauma Jamie Gallivan RN, BSN Interventional Radiology Case Study 6 y/o boy fell out of 2 nd story window onto concrete Hemodynamically stable at scene Arrival
Interventional Radiology for Solid Organ Trauma Jamie Gallivan RN, BSN Interventional Radiology Case Study 6 y/o boy fell out of 2 nd story window onto concrete Hemodynamically stable at scene Arrival
Gastrointestinal Emergencies CEN REVIEW 2017 MARY RALEY, BSN, RN, CEN, TCRN, TNSCC
 Gastrointestinal Emergencies CEN REVIEW 2017 MARY RALEY, BSN, RN, CEN, TCRN, TNSCC Gastrointestinal Emergencies is 7% of the CEN A. Acute abdomen B. Bleeding C. Cholecystitis D. Cirrhosis E. Diverticulitis
Gastrointestinal Emergencies CEN REVIEW 2017 MARY RALEY, BSN, RN, CEN, TCRN, TNSCC Gastrointestinal Emergencies is 7% of the CEN A. Acute abdomen B. Bleeding C. Cholecystitis D. Cirrhosis E. Diverticulitis
Pediatric Trauma. July 27 th, Suzana Buac, PGY4. Dr. Neil Merritt
 Pediatric Trauma July 27 th, 2016. Suzana Buac, PGY4 Dr. Neil Merritt Case 5yoM fall from roof Fall from roof of home while father was shingling 5yoM fall from roof Fall from roof of home while father
Pediatric Trauma July 27 th, 2016. Suzana Buac, PGY4 Dr. Neil Merritt Case 5yoM fall from roof Fall from roof of home while father was shingling 5yoM fall from roof Fall from roof of home while father
FAST Focused Assessment with Sonography in Trauma
 FAST Focused Assessment with Sonography in Trauma Wilma Rodriguez Mojica,MD,FACR Professor of Radiology UPR School of Medicine Ultrasound Section - Radiological Sciences Department OBJECTIVES Understand
FAST Focused Assessment with Sonography in Trauma Wilma Rodriguez Mojica,MD,FACR Professor of Radiology UPR School of Medicine Ultrasound Section - Radiological Sciences Department OBJECTIVES Understand
Case Based Review (Whew!)
") Northern California Emergency Ultrasound Course Case Based Review (Whew!) Martine Sargent, MD Ultrasound Director, Assistant Professor UCSF Department of Emergency Medicine San Francisco General Hospital
Northern California Emergency Ultrasound Course Case Based Review (Whew!) Martine Sargent, MD Ultrasound Director, Assistant Professor UCSF Department of Emergency Medicine San Francisco General Hospital
CLINICAL INVESTIGATIONS
 808 Sokolove et al. d SEAT BELT SIGN AND ABDOMINAL INJURY IN CHILDREN CLINICAL INVESTIGATIONS Association between the Sign and Intraabdominal Injury in Children with Blunt Torso Trauma Peter E. Sokolove,
808 Sokolove et al. d SEAT BELT SIGN AND ABDOMINAL INJURY IN CHILDREN CLINICAL INVESTIGATIONS Association between the Sign and Intraabdominal Injury in Children with Blunt Torso Trauma Peter E. Sokolove,
Algorithms for managing the common trauma patient
 ALGORITHMS Algorithms for managing the common trauma patient J John, MB ChB Department of Urology, Frere Hospital, East London Hospital Complex, East London, South Africa Corresponding author: J John (jeffveenajohn@gmail.com)
ALGORITHMS Algorithms for managing the common trauma patient J John, MB ChB Department of Urology, Frere Hospital, East London Hospital Complex, East London, South Africa Corresponding author: J John (jeffveenajohn@gmail.com)
The Focused Assessment with Sonography for Trauma, (FAST) procedure.
 procedure.") The Focused Assessment with Sonography for Trauma, (FAST) procedure. ROBERT H. WRIGLEY Professor Veterinary Diagnostic Imaging University of Sydney Veterinary Teaching Hospital Professor Emeritus Colorado
The Focused Assessment with Sonography for Trauma, (FAST) procedure. ROBERT H. WRIGLEY Professor Veterinary Diagnostic Imaging University of Sydney Veterinary Teaching Hospital Professor Emeritus Colorado
Which Blunt Trauma Patients Should Be Studied by Abdominal CT?
 MDCT of Bowel and Mesenteric Injury: How Findings Influence Management 4 th Nordic Trauma Radiology Course 2006 4 th Nordic Trauma Radiology Course 2006 Stuart E. Mirvis, M.D., FACR Department of Radiology
MDCT of Bowel and Mesenteric Injury: How Findings Influence Management 4 th Nordic Trauma Radiology Course 2006 4 th Nordic Trauma Radiology Course 2006 Stuart E. Mirvis, M.D., FACR Department of Radiology
Dr. Mike Brzozowski Trauma Team Leader and Emergency. Sunnybrook Health Sciences Centre Toronto, Ontario
 Dr. Mike Brzozowski Trauma Team Leader and Emergency Physician i Sunnybrook Health Sciences Centre Toronto, Ontario Learning Objectives To better understand the controversies with respect to the rational
Dr. Mike Brzozowski Trauma Team Leader and Emergency Physician i Sunnybrook Health Sciences Centre Toronto, Ontario Learning Objectives To better understand the controversies with respect to the rational
17. Imaging and interventional radiology
 17. Imaging and interventional radiology These guidelines have been adapted from the Leeds Major Trauma Centre Imaging in Paediatric Major Trauma guidelines Written by Dr Annmarie Jeanes (Consultant Paediatric
17. Imaging and interventional radiology These guidelines have been adapted from the Leeds Major Trauma Centre Imaging in Paediatric Major Trauma guidelines Written by Dr Annmarie Jeanes (Consultant Paediatric
Identifying Children at Very Low Risk of Clinically Important Blunt Abdominal Injuries
 CLINICAL DECISION RULES/ORIGINAL RESEARCH Identifying Children at Very Low Risk of Clinically Important Blunt Abdominal Injuries James F. Holmes, MD, MPH; Kathleen Lillis, MD; David Monroe, MD; Dominic
CLINICAL DECISION RULES/ORIGINAL RESEARCH Identifying Children at Very Low Risk of Clinically Important Blunt Abdominal Injuries James F. Holmes, MD, MPH; Kathleen Lillis, MD; David Monroe, MD; Dominic
MISSED FINDINGS IN EMERGENCY RADIOLOGY: CASE BASE SESSION 5 th Nordic Trauma Radiology Course Oslo, Norway
 MISSED FINDINGS IN EMERGENCY RADIOLOGY: CASE BASE SESSION 5 th Nordic Trauma Radiology Course Oslo, Norway K.SHANMUGANATHAN M.D. EASILY MISSED FINDINGS IN EMERGENCY RADIOLOGY OBJECTIVES Commonly missed
MISSED FINDINGS IN EMERGENCY RADIOLOGY: CASE BASE SESSION 5 th Nordic Trauma Radiology Course Oslo, Norway K.SHANMUGANATHAN M.D. EASILY MISSED FINDINGS IN EMERGENCY RADIOLOGY OBJECTIVES Commonly missed
Pediatric Trauma: Pearls of Management
 Pediatric Trauma: Pearls of Management Judith R. Klein, MD Assistant Professor UCSF-SFGH SFGH Department of Emergency Medicine Pediatric Trauma: The Problem Leading cause of M/M age 1-241 50% of all pediatric
Pediatric Trauma: Pearls of Management Judith R. Klein, MD Assistant Professor UCSF-SFGH SFGH Department of Emergency Medicine Pediatric Trauma: The Problem Leading cause of M/M age 1-241 50% of all pediatric
Tummy Trauma: Evaluation and Management of the Injured Child Catherine J. Goodhue, CPNP Pediatric Nurse Practitioner Trauma Program/Division of
 Tummy Trauma: Evaluation and Management of the Injured Child Catherine J. Goodhue, CPNP Pediatric Nurse Practitioner Trauma Program/Division of Pediatric Surgery Objectives 1. Discuss common mechanisms
Tummy Trauma: Evaluation and Management of the Injured Child Catherine J. Goodhue, CPNP Pediatric Nurse Practitioner Trauma Program/Division of Pediatric Surgery Objectives 1. Discuss common mechanisms
UBC Department of Urologic Sciences Lecture Series. Urological Trauma
 UBC Department of Urologic Sciences Lecture Series Urological Trauma Disclaimer: This is a lot of information to cover and we are unlikely to cover it all today These slides are to be utilized for your
UBC Department of Urologic Sciences Lecture Series Urological Trauma Disclaimer: This is a lot of information to cover and we are unlikely to cover it all today These slides are to be utilized for your
Radiology of the abdomen Lecture -1-
 Radiology of the abdomen Lecture -1- Objectives To know radiology modalities used in abdomen imaging mainly GI tract. To know advantages and disadvantages of each modality. To know indications and contraindications
Radiology of the abdomen Lecture -1- Objectives To know radiology modalities used in abdomen imaging mainly GI tract. To know advantages and disadvantages of each modality. To know indications and contraindications
3/14/2014 USED TO BE SIMPLE.. TO IMMOBILIZE OR NOT TO IMMOBILIZE.THAT IS THE QUESTION THE PROBLEM OLD THINKING
 USED TO BE SIMPLE.. TO IMMOBILIZE OR NOT TO IMMOBILIZE.THAT IS THE QUESTION Immobilization following injury used to be a simple decision--but no one was thinking. Up to 5 million people per year receive
USED TO BE SIMPLE.. TO IMMOBILIZE OR NOT TO IMMOBILIZE.THAT IS THE QUESTION Immobilization following injury used to be a simple decision--but no one was thinking. Up to 5 million people per year receive
Imaging in abdominal trauma
 Imaging in abdominal trauma Dilyana Baleva Medical University Varna Landesklinikum Mistelbach-Gänserndorf Learning objectives Definition, demographics and etiology Imaging modalities and protocols Common
Imaging in abdominal trauma Dilyana Baleva Medical University Varna Landesklinikum Mistelbach-Gänserndorf Learning objectives Definition, demographics and etiology Imaging modalities and protocols Common
The Questionable Utility of Oral Contrast for the Patient with Abdominal Pain in the Emergency Department
 The Questionable Utility of Oral Contrast for the Patient with Abdominal Pain in the Emergency Department Jonathan Rakofsky, MD PGY3 Henry Ford Hospital Emergency Medicine Program December 2014 All patients
The Questionable Utility of Oral Contrast for the Patient with Abdominal Pain in the Emergency Department Jonathan Rakofsky, MD PGY3 Henry Ford Hospital Emergency Medicine Program December 2014 All patients
Initial Pelvic Fracture Management. Patrick M Reilly MD FACS February 27, 2010
 Initial Pelvic Fracture Management Patrick M Reilly MD FACS February 27, 2010 John Pryor MD Field Triage* * Step One : Physiology * Step Two : Anatomy * Step Three : Mechanism * Step Four : Co-Morbid Conditions
Initial Pelvic Fracture Management Patrick M Reilly MD FACS February 27, 2010 John Pryor MD Field Triage* * Step One : Physiology * Step Two : Anatomy * Step Three : Mechanism * Step Four : Co-Morbid Conditions
Objectives. Pediatric Trauma Update: Objectives: Topics
 Objectives Pediatric Trauma Update: 2013 Christopher Newton MD, FACS, FAAP Medical Director Trauma Services and Surgical Critical Care Children s Hospital Oakland Review recent trends and advancements
Objectives Pediatric Trauma Update: 2013 Christopher Newton MD, FACS, FAAP Medical Director Trauma Services and Surgical Critical Care Children s Hospital Oakland Review recent trends and advancements
The Value of Urinalysis in Detection of Abdominal Organ Injuries in Children with Hematuria Following Blunt Abdominal Trauma; A Diagnostic Study
 http:// ijp.mums.ac.ir Original Article (Pages: 6103-6110) The Value of Urinalysis in Detection of Abdominal Organ Injuries in Children with Hematuria Following Blunt Abdominal Trauma; A Diagnostic Study
http:// ijp.mums.ac.ir Original Article (Pages: 6103-6110) The Value of Urinalysis in Detection of Abdominal Organ Injuries in Children with Hematuria Following Blunt Abdominal Trauma; A Diagnostic Study
Radiological Investigations of Abdominal Trauma
 76 77 Investigations of Abdominal Trauma Introduction: Trauma to abdominal organs is a common cause of patient morbidity and mortality among trauma patients. Causes of abdominal trauma include blunt injuries,
76 77 Investigations of Abdominal Trauma Introduction: Trauma to abdominal organs is a common cause of patient morbidity and mortality among trauma patients. Causes of abdominal trauma include blunt injuries,
Focused abdominal sonography for trauma in the clinical evaluation of children with blunt abdominal trauma
 Ben-Ishay et al. World Journal of Emergency Surgery (2015)10:27 DOI 10.1186/s13017-015-0021-x WORLD JOURNAL OF EMERGENCY SURGERY RESEARCH ARTICLE Open Access Focused abdominal sonography for trauma in
Ben-Ishay et al. World Journal of Emergency Surgery (2015)10:27 DOI 10.1186/s13017-015-0021-x WORLD JOURNAL OF EMERGENCY SURGERY RESEARCH ARTICLE Open Access Focused abdominal sonography for trauma in
Cases from the Streets. Kelly Buchanan MD, ATC/L EMS Fellow December, 2011
 Cases from the Streets Kelly Buchanan MD, ATC/L EMS Fellow December, 2011 The Scene Car vs Light Pole, 35 mph, front right side damage 10 with no PCI + airbag deployment, starring on windshield Given the
Cases from the Streets Kelly Buchanan MD, ATC/L EMS Fellow December, 2011 The Scene Car vs Light Pole, 35 mph, front right side damage 10 with no PCI + airbag deployment, starring on windshield Given the
US Applications. Case Based Wrap-Up 1. Case 1 E-FAST. Case presentations E-FAST Abdominal. Pearls for each indication
 Case Based Wrap-Up 1 Stephanie J. Doniger MD RDMS FAAP FACEP Associate Director, Pediatric Emergency Ultrasound Stanford University Medical Center US Applications Case presentations E-FAST Abdominal Aorta
Case Based Wrap-Up 1 Stephanie J. Doniger MD RDMS FAAP FACEP Associate Director, Pediatric Emergency Ultrasound Stanford University Medical Center US Applications Case presentations E-FAST Abdominal Aorta
M Magray, M Shahdhar, M Wani, M Shafi, J Sheikh, H Wani
 ISPUB.COM The Internet Journal of Surgery Volume 30 Number 2 Studying The Role Of Computed Tomography In Selective Management Of Blunt Abdominal Trauma Patients In A Single Tertiary Care Centre In Northern
ISPUB.COM The Internet Journal of Surgery Volume 30 Number 2 Studying The Role Of Computed Tomography In Selective Management Of Blunt Abdominal Trauma Patients In A Single Tertiary Care Centre In Northern
Residents should not independently perform focused abdominal sonography for trauma after 10 training examinations
 Washington University School of Medicine Digital Commons@Becker Open Access Publications 2004 Residents should not independently perform focused abdominal sonography for trauma after 10 training examinations
Washington University School of Medicine Digital Commons@Becker Open Access Publications 2004 Residents should not independently perform focused abdominal sonography for trauma after 10 training examinations
Pediatric Trauma Cases
 Pediatric Trauma Cases QPEM 2018 Barbara Blackie, MD, MEd, FRCPC DISCLOSURE I do not have any relevant financial relationship with commercial interest to disclose. Learning Objectives -Manage interactive
Pediatric Trauma Cases QPEM 2018 Barbara Blackie, MD, MEd, FRCPC DISCLOSURE I do not have any relevant financial relationship with commercial interest to disclose. Learning Objectives -Manage interactive
Abdomen and Genitalia Injuries. Chapter 28
 Abdomen and Genitalia Injuries Chapter 28 Hollow Organs in the Abdominal Cavity Signs of Peritonitis Abdominal pain Tenderness Muscle spasm Diminished bowel sounds Nausea/vomiting Distention Solid Organs
Abdomen and Genitalia Injuries Chapter 28 Hollow Organs in the Abdominal Cavity Signs of Peritonitis Abdominal pain Tenderness Muscle spasm Diminished bowel sounds Nausea/vomiting Distention Solid Organs
PROTOCOLS. Lap-belt syndrome. Principal investigator. Background
 Lap-belt syndrome Principal investigator Claude Cyr, MD, Centre hospitalier universitaire de Sherbrooke, 3001 12 e Avenue Nord, Sherbrooke QC J1H 5N4; tel.: (819) 346-1110, ext. 14634; fax: (819) 564-5398;
Lap-belt syndrome Principal investigator Claude Cyr, MD, Centre hospitalier universitaire de Sherbrooke, 3001 12 e Avenue Nord, Sherbrooke QC J1H 5N4; tel.: (819) 346-1110, ext. 14634; fax: (819) 564-5398;
10/27/2014. An experience that causes physical, emotional, or psychological distress or harm.
 Ann Marie Szoke, DNP, CRNP Supervisor Advanced Practitioners St. Luke s University Hospital To review multiple traumatic events through case presentations Discuss the concept of the Hybrid Operating Room
Ann Marie Szoke, DNP, CRNP Supervisor Advanced Practitioners St. Luke s University Hospital To review multiple traumatic events through case presentations Discuss the concept of the Hybrid Operating Room
Does a Blush on CT following Blunt Abdominal Injury Necessitate an Invasive Intervention?
 Does a Blush on CT following Blunt Abdominal Injury Necessitate an Invasive Intervention? Ragavan V Siddharthan, MD, Martha-Conley Ingram, BS., Andrew Morris, MD, Curtis Travers, MPH, Courtney McCracken,
Does a Blush on CT following Blunt Abdominal Injury Necessitate an Invasive Intervention? Ragavan V Siddharthan, MD, Martha-Conley Ingram, BS., Andrew Morris, MD, Curtis Travers, MPH, Courtney McCracken,
Pediatric Aspects of Advanced Trauma Life Support: Transition from EMS to the Trauma Room PEDIATRIC TRAUMA DIRECTOR, HASBRO CHILDREN S HOSPITAL
 Pediatric Aspects of Advanced Trauma Life Support: Transition from EMS to the Trauma Room HALE WILLS, MD PEDIATRIC TRAUMA DIRECTOR, HASBRO CHILDREN S HOSPITAL Objectives 1. Identify the critical components
Pediatric Aspects of Advanced Trauma Life Support: Transition from EMS to the Trauma Room HALE WILLS, MD PEDIATRIC TRAUMA DIRECTOR, HASBRO CHILDREN S HOSPITAL Objectives 1. Identify the critical components
ASYMPTOMATIC MICROSCOPIC HEMATURIA IN WOMEN JOLYN HILL, MD ASSISTANT PROFESSOR, CLINICAL UROGYNECOLOGY FEBRUARY14, 2017
 ASYMPTOMATIC MICROSCOPIC HEMATURIA IN WOMEN JOLYN HILL, MD ASSISTANT PROFESSOR, CLINICAL UROGYNECOLOGY FEBRUARY14, 2017 DISCLOSURES No financial disclosures Urogynecologist via Ob/Gyn pathway ASYMPTOMATIC
ASYMPTOMATIC MICROSCOPIC HEMATURIA IN WOMEN JOLYN HILL, MD ASSISTANT PROFESSOR, CLINICAL UROGYNECOLOGY FEBRUARY14, 2017 DISCLOSURES No financial disclosures Urogynecologist via Ob/Gyn pathway ASYMPTOMATIC
Low-Dose CT: Clinical Studies & the Radiologist Perspective
 Low-Dose CT: Clinical Studies & the Radiologist Perspective RD-ASiR RD-MBIR SD-FBP RD=0.35 msv (80% dose reduction) Perry J. Pickhardt, MD UW School of Medicine & Public Health Low-Dose CT: Clinical Overview
Low-Dose CT: Clinical Studies & the Radiologist Perspective RD-ASiR RD-MBIR SD-FBP RD=0.35 msv (80% dose reduction) Perry J. Pickhardt, MD UW School of Medicine & Public Health Low-Dose CT: Clinical Overview
Genitourinary Trauma Introduction GU Trauma overlooked
 Genitourinary Trauma Introduction GU Trauma overlooked 10-20% of all injured patients Long term morbidity Impotence Incontinence Life-threatening injuries first Urethral Injury Plan Bladder Injury Kidney
Genitourinary Trauma Introduction GU Trauma overlooked 10-20% of all injured patients Long term morbidity Impotence Incontinence Life-threatening injuries first Urethral Injury Plan Bladder Injury Kidney
CEDR 2018 QCDR Measures for CMS 2018 MIPS Performance Year Reporting
 ACEP19 Emergency Department Utilization of CT for Minor Blunt Head Trauma for Aged 18 Years and Older Percentage of visits for aged 18 years and older who presented with a minor blunt head trauma who had
ACEP19 Emergency Department Utilization of CT for Minor Blunt Head Trauma for Aged 18 Years and Older Percentage of visits for aged 18 years and older who presented with a minor blunt head trauma who had
Review. 1. Peritonitis would MOST likely result following injury to the: A. liver. B. spleen. C. kidney. D. stomach.
 Chapter 28 Review Review 1. Peritonitis would MOST likely result following injury to the: A. liver. B. spleen. C. kidney. D. stomach. Review Answer: D Rationale: In general, solid organs bleed when injured
Chapter 28 Review Review 1. Peritonitis would MOST likely result following injury to the: A. liver. B. spleen. C. kidney. D. stomach. Review Answer: D Rationale: In general, solid organs bleed when injured
ORIGINAL ARTICLE. FAST as a predictor of clinical outcome in blunt abdominal trauma
 FAST as a predictor of clinical outcome in blunt abdominal trauma Benjamin M Terry, MD, MPH David Blehar, MD Romolo Gaspari, MD Department of Emergency Medicine, University of Massachusetts Medical School,
FAST as a predictor of clinical outcome in blunt abdominal trauma Benjamin M Terry, MD, MPH David Blehar, MD Romolo Gaspari, MD Department of Emergency Medicine, University of Massachusetts Medical School,
Focused Assessment Sonography of Trauma (FAST) Scanning Protocol
 Scanning Protocol") Focused Assessment Sonography of Trauma (FAST) Scanning Protocol Romolo Gaspari CHAPTER 3 GOAL OF THE FAST EXAM Demonstrate free fluid in abdomen, pleural space, or pericardial space. EMERGENCY ULTRASOUND
Focused Assessment Sonography of Trauma (FAST) Scanning Protocol Romolo Gaspari CHAPTER 3 GOAL OF THE FAST EXAM Demonstrate free fluid in abdomen, pleural space, or pericardial space. EMERGENCY ULTRASOUND
Alexander Y. Sheng, 1 Peregrine Dalziel, 2 Andrew S. Liteplo, 2 Peter Fagenholz, 3 and Vicki E. Noble Introduction
 Emergency Medicine International Volume 2013, Article ID 678380, 7 pages http://dx.doi.org/10.1155/2013/678380 Research Article Focused Assessment with Sonography in Trauma and Abdominal Computed Tomography
Emergency Medicine International Volume 2013, Article ID 678380, 7 pages http://dx.doi.org/10.1155/2013/678380 Research Article Focused Assessment with Sonography in Trauma and Abdominal Computed Tomography
Should This Article Change My Practice? Ran Goldman, MD BC Children s Hospital University of British Columbia
 Should This Article Change My Practice? Ran Goldman, MD BC Children s Hospital University of British Columbia Febrile Seizures Pulled Elbow Asthma Abdominal Trauma Looking Good Prolonged Febrile Seizures
Should This Article Change My Practice? Ran Goldman, MD BC Children s Hospital University of British Columbia Febrile Seizures Pulled Elbow Asthma Abdominal Trauma Looking Good Prolonged Febrile Seizures
Pediatric head trauma: the evidence regarding indications for emergent neuroimaging
 DOI 10.1007/s00247-008-0996-5 ALARA: BUILDING BRIDGES BETWEEN RADIOLOGY AND EMERGENCY MEDICINE Pediatric head trauma: the evidence regarding indications for emergent neuroimaging Nathan Kuppermann Received:
DOI 10.1007/s00247-008-0996-5 ALARA: BUILDING BRIDGES BETWEEN RADIOLOGY AND EMERGENCY MEDICINE Pediatric head trauma: the evidence regarding indications for emergent neuroimaging Nathan Kuppermann Received:
The utility of focused abdominal ultrasound in blunt abdominal trauma: a reappraisal
 The American Journal of Surgery 194 (2007) 728 733 Presentation The utility of focused abdominal ultrasound in blunt abdominal trauma: a reappraisal Thomas S. Helling, M.D., F.A.C.S.*, Jennifer Wilson,
The American Journal of Surgery 194 (2007) 728 733 Presentation The utility of focused abdominal ultrasound in blunt abdominal trauma: a reappraisal Thomas S. Helling, M.D., F.A.C.S.*, Jennifer Wilson,
Title: Post traumatic Diaphragmatic hernia in children: Diagnostic Dilemmas and lessons learned. Type: Original article
 Title: Post traumatic Diaphragmatic hernia in children: Diagnostic Dilemmas and lessons learned. Type: Original article Authors: Dr Vaibhav Pandey 1*, Dr. Pranay Panigrahi 2 Srivastav 4 & Dr Rakesh Kumar
Title: Post traumatic Diaphragmatic hernia in children: Diagnostic Dilemmas and lessons learned. Type: Original article Authors: Dr Vaibhav Pandey 1*, Dr. Pranay Panigrahi 2 Srivastav 4 & Dr Rakesh Kumar
Outcomes & Clinical Trials Update: Empyema & NEC
 Outcomes & Clinical Trials Update: Empyema & NEC American Pediatric Surgical Association Outcomes & Clinical Trials Committee Fizan Abdullah, Chair Saleem Islam, Vice Chair Gudrun Aspelund Catherine C.
Outcomes & Clinical Trials Update: Empyema & NEC American Pediatric Surgical Association Outcomes & Clinical Trials Committee Fizan Abdullah, Chair Saleem Islam, Vice Chair Gudrun Aspelund Catherine C.