SPECIAL DIAGNOSTIC STUDIES IN BLUNT TRAUMA OLEH : Prof.DR.Dr Abdul Rasyid SpRad (K),Ph.D Dr.Evo Elidar Sp.Rad
|
|
|
- Peter Casey
- 5 years ago
- Views:
Transcription
1 SPECIAL DIAGNOSTIC STUDIES IN BLUNT TRAUMA OLEH : Prof.DR.Dr Abdul Rasyid SpRad (K),Ph.D Dr.Evo Elidar Sp.Rad
2

3

4
5 Trauma Emergency Room layout Ideally the trauma emergency room is centrally located to provide quick access to the CT scanner, angiography suite, OR and ICU


6
7 Approach to trauma patient Primary survey (ABC s) Resuscitation and primary imaging Secondary survey (physical and imaging) Definitive Care
8 Imaging on admission Lateral C-spine radiograph before endotracheal intubation Chest AP +/- lateral Abdominal US CT once hemodynamically stable MRI has a limited role in imaging of acutely injured trauma patient
9 Imaging on admission Lateral C-spine: R/O C-spine fracture CXR: R/O pneumothorax/wide mediastinum US: R/O hemoperitoneum CT (+ IV/oral contrast): R/O organspecific injuries MRI: limited role
10

11

12 Stiell IG, et al. Lancet. 2001;357:
13
14
15
16

17

18


19
20 BLUNT ABDOMINAL TRAUMA Common injury patterns (1) In patients undergoing laparotomy for blunt trauma, most frequently injured organs are spleen (40-55%), liver (35-45%), and small bowel (5-10%). (ATLS, 2001) Duodenum: Classically, frontal-impact MVC with unrestrained driver; or direct blow to abdomen. Bloody gastric aspirate, retroperitoneal air on XR or CT Confirmed with upper GI series or double contrast CT Small bowel injury: Generally from sudden deceleration with subsequent tearing near fixed points of attachment. Often associated with seat belt sign, lumbar distraction fracture (Chance fracture) DPL superior to FAST or CT for diagnosis.
21 Common injury patterns (2) Pancreas: Direct epigastric blow compressing pancreas against vertebral column. Early normal serum amylase does NOT exclude major pancreatic trauma. CT with PO/IV contrast NOT particularly sensitive in immediate post-injury period. Diaphragm: Most commonly, 5-10 cm rupture involving posterolateral hemidiaphragm. Noted on CXR: blurred or elevated hemidiaphragm, hemothorax, GT in chest Genitourinary: Anterior injuries (below UG diaphragm): usually from straddle impact. Posterior injuries (above UG diaphragm): in patient with multisystem injuries and pelvic fractures.
22 Common injury patterns (3) Solid organ injury Laceration to liver, spleen, or kidney Injury to one of these three + hemodynamic instability: considered indication for urgent laparotomy Isolated solid organ injury in hemodynamically stable patient: can often be managed nonoperatively. Pelvic fractures: Suggest major force applied to patient. Usually auto-ped, MVC, or motorcycle Significant association with intraperitoneal and retroperitoneal organs and vascular structures.
23 Diagnostic Peritoneal Lavage 98% sensitive for intraperitoneal bleeding (ATLS) Open or closed (Seldinger); usually infraumbilical, but may be supraumbilical in pelvic frxs or advanced pregnancy. Free aspiration of blood, GI contents, or bile in demodynamically abnormal pt: indication for laparotomy If gross blood (> 10 ml) or GI contents not aspirated, perform lavage with 1000 ml warmed LR. Allow to mix, compress abdomen and logross paient, the sent to lab. + test: >100,000 RBC/mm3, >500 WBC/mm3, Gram stain with bacteria. Alters subsequent examination of patient Has been somewhat superceded by FAST in common use; now generally performed in unstable patients with intermediate FAST exams, or with suspicion for small bowel injury.
24 FAST: Strengths and Limitations Strengths Rapid (~2 mins) Portable Inexpensive Technically simple, easy to train (studies show competence can be achieved after ~30 studies) Can be performed serially Useful for guiding triage decisions in trauma patients Limitations Does not typically identify source of bleeding, or detect injuries that do not cause hemoperitoneum Requires extensive training to assess parenchyma reliably Limited in detecting <250 cc intraperitoneal fluid Particularly poor at detecting bowel and mesentery damage (44% sensitivity) Difficult to assess retroperitoneum Limited by habitus in obese patients
25 FAST: Accuracy For identifying hemoperitoneum in blunt abdominal trauma: Sensitivity 76-90% Specificity % The larger the hemoperitoneum, the higher the sensitivity. So sensitivity increases for clinically significant hemoperitoneum. How much fluid can FAST detect? 250 cc total 100 cc in Morison s pouch
26 HEMOPERITONEUM
27 Does FAST replace CT? Only at the extremes. Unstable patient, (+) FAST OR Stable patient, low force injury, (-) FAST consider observing patient. CT is far more sensitive than FAST for detecting and characterizing abdominal injury in trauma. The gold standard for characterizing intraparenchymal injury. Death begins with a CT. Never send an unstable patient to CT. FAST, however, can be performed during resuscitation.
28 Computed Tomography Only at the extremes. Unstable patient, (+) FAST OR Stable patient, low force injury, (-) FAST consider observing patient. CT is far more sensitive than FAST for detecting and characterizing abdominal injury in trauma. The gold standard for characterizing intraparenchymal injury. Death begins with a CT. Never send an unstable patient to CT. FAST, however, can be performed during resuscitation.
29 Computed Tomography EAST level I recommendations (2001): CT is recommended for evaluation of hemodynamically stable patients with equivocal findings on physical examination, associated neurologic injury, or multiple extra-abdominal injuries. CT is the diagnostic modality of choice for nonoperative management of solid visceral injuries
30 EAST Algorithm: Unstable Eastern Association for the Surgery of Trauma,2001
31 EAST Algorithm: Stable Eastern Association for the Surgery of Trauma, 2001


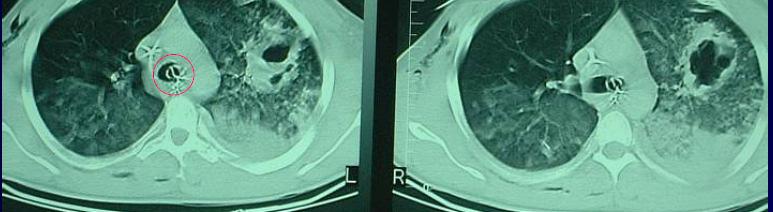
32 SPLEEN INJURY U S G S U B C A P H E M
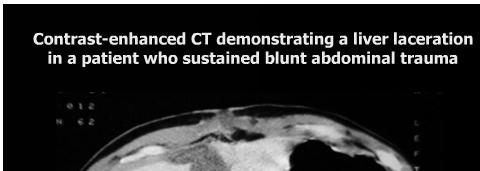
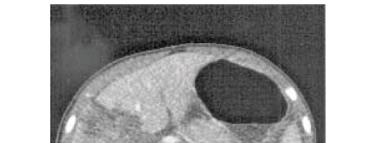
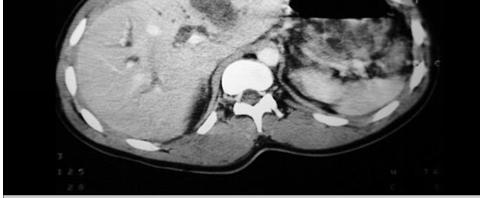
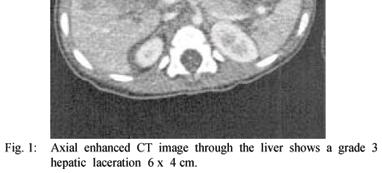
33 LIVER LACERATION






34 SUBCAPSULAR HEM RENAL CONTUSION RENAL LACERATION WITHOUT INVOLVEMENT THE COLLECTING SYSTEM RENAL LACERATION INVOLVING COLLECTING SYSTEM


35 US COMPARISON CT Images in a 54-year-old woman admitted to the hospital after MVC : US does not demonstrate any injury of the R-kidney CT demonstrates a large laceration of the R-kidney that is sorrounded by extensuve hematoma

36 US COMPARISON CT Images in a 22 year-old man admitted to the hospital Afeter a motor vehicle accident US demonstrates a norma;-appearing sp;een CT scan depicts an extensive splenic laceration, Hemoperitoneum is seen in the perisplenic and perihepatic
37
Pediatric Abdomen Trauma
 Pediatric Abdomen Trauma Susan D. John, MD, FACR Pediatric Trauma Trauma is leading cause of death and disability in children and adolescents Causes and effects vary between age groups Blunt trauma predominates
Pediatric Abdomen Trauma Susan D. John, MD, FACR Pediatric Trauma Trauma is leading cause of death and disability in children and adolescents Causes and effects vary between age groups Blunt trauma predominates
2 Blunt Abdominal Trauma
 2 Blunt Abdominal Trauma Ricardo Ferrada, Diego Rivera, and Paula Ferrada Pearls and Pitfalls Patients suffering a high-energy trauma have solid viscera rupture in the abdomen and/or aortic rupture in
2 Blunt Abdominal Trauma Ricardo Ferrada, Diego Rivera, and Paula Ferrada Pearls and Pitfalls Patients suffering a high-energy trauma have solid viscera rupture in the abdomen and/or aortic rupture in
2. Blunt abdominal Trauma
 Abdominal Trauma 1. Evaluation and management depends on: a. Mechanism (Blunt versus Penetrating) b. Injury complex in addition to abdomen c. Haemodynamic stability assessment: i. Classically patient s
Abdominal Trauma 1. Evaluation and management depends on: a. Mechanism (Blunt versus Penetrating) b. Injury complex in addition to abdomen c. Haemodynamic stability assessment: i. Classically patient s
MANAGEMENT OF SOLID ORGAN INJURIES
 MANAGEMENT OF SOLID ORGAN INJURIES Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Director of Surgical Critical Care, Harborview Medical Center Introduction Solid organ injury
MANAGEMENT OF SOLID ORGAN INJURIES Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Director of Surgical Critical Care, Harborview Medical Center Introduction Solid organ injury
Evaluation of Children with Blunt Abdominal Trauma. James F. Holmes, MD, MPH UC Davis School of Medicine
 Evaluation of Children with Blunt Abdominal Trauma James F. Holmes, MD, MPH UC Davis School of Medicine Objectives Epidemiology of intra-abdominal injury (IAI) Physical examination findings with IAI Laboratory
Evaluation of Children with Blunt Abdominal Trauma James F. Holmes, MD, MPH UC Davis School of Medicine Objectives Epidemiology of intra-abdominal injury (IAI) Physical examination findings with IAI Laboratory
Imaging in the Trauma Patient
 Imaging in the Trauma Patient David A. Spain, MD Department of Surgery Stanford University Pan Scan Instead of Clinical Exam? 1 Granted, some patients don t need CT scan Platinum Package Stanford Special
Imaging in the Trauma Patient David A. Spain, MD Department of Surgery Stanford University Pan Scan Instead of Clinical Exam? 1 Granted, some patients don t need CT scan Platinum Package Stanford Special
Abdominal Trauma. Nat Krairojananan M.D., FRCST Department of Trauma and Emergency Medicine Phramongkutklao Hospital
 Abdominal Trauma Nat Krairojananan M.D., FRCST Department of Trauma and Emergency Medicine Phramongkutklao Hospital overview Quick review abdominal anatomy Review of mechanism of injury Review of investigation
Abdominal Trauma Nat Krairojananan M.D., FRCST Department of Trauma and Emergency Medicine Phramongkutklao Hospital overview Quick review abdominal anatomy Review of mechanism of injury Review of investigation
Pan Scan Instead of Clinical Exam? David A. Spain, MD
 Pan Scan Instead of Clinical Exam? David A. Spain, MD Granted, some patients don t t need CT scan Platinum Package Stanford Special CT Scan Head Neck Chest Abdomen Pelvis Takes about 20 minutes to do
Pan Scan Instead of Clinical Exam? David A. Spain, MD Granted, some patients don t t need CT scan Platinum Package Stanford Special CT Scan Head Neck Chest Abdomen Pelvis Takes about 20 minutes to do
Which Blunt Trauma Patients Should Be Studied by Abdominal CT?
 MDCT of Bowel and Mesenteric Injury: How Findings Influence Management 4 th Nordic Trauma Radiology Course 2006 4 th Nordic Trauma Radiology Course 2006 Stuart E. Mirvis, M.D., FACR Department of Radiology
MDCT of Bowel and Mesenteric Injury: How Findings Influence Management 4 th Nordic Trauma Radiology Course 2006 4 th Nordic Trauma Radiology Course 2006 Stuart E. Mirvis, M.D., FACR Department of Radiology
Role of Focused Assessment with Sonography for Trauma (FAST) and in abdominal trauma: Radiologist s perspective
 and in abdominal trauma: Radiologist s perspective") Original Research Article Role of Focused Assessment with Sonography for Trauma (FAST) and CT scan in abdominal trauma: Radiologist s perspective Nirav Patel 1*, Niket Domadia 2, Konark Sarvaiya 1, Anil
Original Research Article Role of Focused Assessment with Sonography for Trauma (FAST) and CT scan in abdominal trauma: Radiologist s perspective Nirav Patel 1*, Niket Domadia 2, Konark Sarvaiya 1, Anil
SSRG International Journal of Medical Science (SSRG-IJMS) volume 1 Issue 2 December 2014
 volume 1 Issue 2 December 2014") Blunt Abdominal Trauma: Making Decision of Management with Conventional and Ultrasonography Evaluation Dr.Naveen K G 1, Dr. Ravi N 2, Dr. Nagaraj B R 3 1(senior resident-department of radiology, Bangalore
Blunt Abdominal Trauma: Making Decision of Management with Conventional and Ultrasonography Evaluation Dr.Naveen K G 1, Dr. Ravi N 2, Dr. Nagaraj B R 3 1(senior resident-department of radiology, Bangalore
MISSED FINDINGS IN EMERGENCY RADIOLOGY: CASE BASE SESSION 5 th Nordic Trauma Radiology Course Oslo, Norway
 MISSED FINDINGS IN EMERGENCY RADIOLOGY: CASE BASE SESSION 5 th Nordic Trauma Radiology Course Oslo, Norway K.SHANMUGANATHAN M.D. EASILY MISSED FINDINGS IN EMERGENCY RADIOLOGY OBJECTIVES Commonly missed
MISSED FINDINGS IN EMERGENCY RADIOLOGY: CASE BASE SESSION 5 th Nordic Trauma Radiology Course Oslo, Norway K.SHANMUGANATHAN M.D. EASILY MISSED FINDINGS IN EMERGENCY RADIOLOGY OBJECTIVES Commonly missed
George M Wadie, MD Director Division of Pediatric Surgery Sacred Heart Medical Center. Springfield, OR Adjunct Assistant Professor of Surgery Oregon
 George M Wadie, MD Director Division of Pediatric Surgery Sacred Heart Medical Center. Springfield, OR Adjunct Assistant Professor of Surgery Oregon Health and Sciences University. Portland, OR Outline
George M Wadie, MD Director Division of Pediatric Surgery Sacred Heart Medical Center. Springfield, OR Adjunct Assistant Professor of Surgery Oregon Health and Sciences University. Portland, OR Outline
PROTOCOLS. Lap-belt syndrome. Principal investigator. Background
 Lap-belt syndrome Principal investigator Claude Cyr, MD, Centre hospitalier universitaire de Sherbrooke, 3001 12 e Avenue Nord, Sherbrooke QC J1H 5N4; tel.: (819) 346-1110, ext. 14634; fax: (819) 564-5398;
Lap-belt syndrome Principal investigator Claude Cyr, MD, Centre hospitalier universitaire de Sherbrooke, 3001 12 e Avenue Nord, Sherbrooke QC J1H 5N4; tel.: (819) 346-1110, ext. 14634; fax: (819) 564-5398;
Sasha Dubrovsky, MSc MD FRCPC Pediatric Emergency Medicine Montreal Children s Hospital - MUHC October 2010
 Sasha Dubrovsky, MSc MD FRCPC Pediatric Emergency Medicine Montreal Children s Hospital - MUHC October 2010 Learning objectives 1. Discuss diagnostic goals in pediatric trauma Diagnose All vs. Severe Injuries
Sasha Dubrovsky, MSc MD FRCPC Pediatric Emergency Medicine Montreal Children s Hospital - MUHC October 2010 Learning objectives 1. Discuss diagnostic goals in pediatric trauma Diagnose All vs. Severe Injuries
CT IMAGING OF BLUNT SPLENIC INJURY: A PICTORIAL ESSAY
 CT IMAGING OF BLUNT SPLENIC INJURY: A PICTORIAL ESSAY Radhiana H, Azian AA, Ahmad Razali MR, Amran AR, Azlin S, S Kamariah CM Department of Radiology International Islamic University Malaysia Kuantan,
CT IMAGING OF BLUNT SPLENIC INJURY: A PICTORIAL ESSAY Radhiana H, Azian AA, Ahmad Razali MR, Amran AR, Azlin S, S Kamariah CM Department of Radiology International Islamic University Malaysia Kuantan,
FAST Focused Assessment with Sonography in Trauma
 FAST Focused Assessment with Sonography in Trauma Wilma Rodriguez Mojica,MD,FACR Professor of Radiology UPR School of Medicine Ultrasound Section - Radiological Sciences Department OBJECTIVES Understand
FAST Focused Assessment with Sonography in Trauma Wilma Rodriguez Mojica,MD,FACR Professor of Radiology UPR School of Medicine Ultrasound Section - Radiological Sciences Department OBJECTIVES Understand
LIVER INJURIES PROFF. S.FLORET
 LIVER INJURIES PROFF. S.FLORET Abdominal injuries For anatomical consideration: Abdomen can be divided in four areas Intra thoracic abdomen True abdomen Pelvic abdomen Retroperitoneal abdomen ETIOLOGY
LIVER INJURIES PROFF. S.FLORET Abdominal injuries For anatomical consideration: Abdomen can be divided in four areas Intra thoracic abdomen True abdomen Pelvic abdomen Retroperitoneal abdomen ETIOLOGY
Muscle spasm Diminished bowel sounds Nausea/vomiting
 3 4 5 6 7 8 9 0 Chapter 8: Abdomen and Genitalia Injuries Abdominal Injuries Abdomen is major body cavity extending from to pelvis. Contains organs that make up digestive, urinary, and genitourinary systems.
3 4 5 6 7 8 9 0 Chapter 8: Abdomen and Genitalia Injuries Abdominal Injuries Abdomen is major body cavity extending from to pelvis. Contains organs that make up digestive, urinary, and genitourinary systems.
A Z OF ABDOMINAL RADIOLOGY
 Z OF BDOMINL RDIOLOGY bdominal trauma to Z of bdominal Radiology Clinical characteristics general discussion, followed by organ-specific summaries, is given below. bdominal trauma is managed as part of
Z OF BDOMINL RDIOLOGY bdominal trauma to Z of bdominal Radiology Clinical characteristics general discussion, followed by organ-specific summaries, is given below. bdominal trauma is managed as part of
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines
 Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Blunt Abdominal Trauma Evaluation and Management Guideline PEDIATRIC Practice Management Guideline Contact: Trauma Center
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Blunt Abdominal Trauma Evaluation and Management Guideline PEDIATRIC Practice Management Guideline Contact: Trauma Center
The Role of the FAST exam in the EDRU
 The Role of the FAST exam in the EDRU A. Robb McLean, MD, MHCM Vice Chair of Clinical Operations, Department of Emergency Medicine Joint Trauma Conference June 20, 2017 Disclosures Goals Describe the performance,
The Role of the FAST exam in the EDRU A. Robb McLean, MD, MHCM Vice Chair of Clinical Operations, Department of Emergency Medicine Joint Trauma Conference June 20, 2017 Disclosures Goals Describe the performance,
Laparotomy for Abdominal Injury in Traffic Accidents
 Qasim O. Al-Qasabi, FRCS; Mohammed K. Alam, MS, FRCS (Ed); Arun K. Tyagi, FRCS; Abdulla Al-Kraida, FRCS; Mohammed I. Al-Sebayel, FRCS From the Departments of Surgery, Riyadh Central Hospital (Drs. Al-Qasabi,
Qasim O. Al-Qasabi, FRCS; Mohammed K. Alam, MS, FRCS (Ed); Arun K. Tyagi, FRCS; Abdulla Al-Kraida, FRCS; Mohammed I. Al-Sebayel, FRCS From the Departments of Surgery, Riyadh Central Hospital (Drs. Al-Qasabi,
Extended FAST Exam. Goal of Trauma Care. Golden Hour of Trauma
 Extended FAST Exam Goal of Trauma Care Golden Hour of Trauma Best INITIAL screening modality in trauma efast 2014 LLSA Article (ACEP Policy Statement) Level B Recommendation: In hemodynamically unstable
Extended FAST Exam Goal of Trauma Care Golden Hour of Trauma Best INITIAL screening modality in trauma efast 2014 LLSA Article (ACEP Policy Statement) Level B Recommendation: In hemodynamically unstable
Initial Pelvic Fracture Management. Patrick M Reilly MD FACS February 27, 2010
 Initial Pelvic Fracture Management Patrick M Reilly MD FACS February 27, 2010 John Pryor MD Field Triage* * Step One : Physiology * Step Two : Anatomy * Step Three : Mechanism * Step Four : Co-Morbid Conditions
Initial Pelvic Fracture Management Patrick M Reilly MD FACS February 27, 2010 John Pryor MD Field Triage* * Step One : Physiology * Step Two : Anatomy * Step Three : Mechanism * Step Four : Co-Morbid Conditions
Abdominal Ultrasonography
 Abdominal Ultrasonography David A. Masneri, DO, FACEP, FAAEM Assistant Professor of Emergency Medicine Assistant Director, Emergency Medicine Residency Medical Director, Operational Medicine Division Center
Abdominal Ultrasonography David A. Masneri, DO, FACEP, FAAEM Assistant Professor of Emergency Medicine Assistant Director, Emergency Medicine Residency Medical Director, Operational Medicine Division Center
ABDOMINAL TRAUMA Lecture Prof. Zbigniew Wlodarczyk
 ABDOMINAL TRAUMA Lecture Prof. Zbigniew Wlodarczyk Epidemiology 2% of all traumas (4% amongst hospitalized patients) 75% M 25% F Average age 35 years 80% close 20% penetrating 40% liver and spleen, 10%
ABDOMINAL TRAUMA Lecture Prof. Zbigniew Wlodarczyk Epidemiology 2% of all traumas (4% amongst hospitalized patients) 75% M 25% F Average age 35 years 80% close 20% penetrating 40% liver and spleen, 10%
Genitourinary Trauma Introduction GU Trauma overlooked
 Genitourinary Trauma Introduction GU Trauma overlooked 10-20% of all injured patients Long term morbidity Impotence Incontinence Life-threatening injuries first Urethral Injury Plan Bladder Injury Kidney
Genitourinary Trauma Introduction GU Trauma overlooked 10-20% of all injured patients Long term morbidity Impotence Incontinence Life-threatening injuries first Urethral Injury Plan Bladder Injury Kidney
Penetrating abdominal trauma clinical view. Ari Leppäniemi, MD Department of Abdominal Surgery Meilahti hospital University of Helsinki Finland
 Penetrating abdominal trauma clinical view Ari Leppäniemi, MD Department of Abdominal Surgery Meilahti hospital University of Helsinki Finland Meilahti hospital - one of Helsinki University hospitals -
Penetrating abdominal trauma clinical view Ari Leppäniemi, MD Department of Abdominal Surgery Meilahti hospital University of Helsinki Finland Meilahti hospital - one of Helsinki University hospitals -
Management of Pelvic Fracture
 Management of Pelvis Fracture with Hemodynamic Instability James W. Davis MD Professor of Clinical Surgery, UCSF/Fresno Chief of Trauma Management of Pelvic Fracture How NOT to do it The basics Evaluation
Management of Pelvis Fracture with Hemodynamic Instability James W. Davis MD Professor of Clinical Surgery, UCSF/Fresno Chief of Trauma Management of Pelvic Fracture How NOT to do it The basics Evaluation
Abdomen and Genitalia Injuries. Chapter 28
 Abdomen and Genitalia Injuries Chapter 28 Hollow Organs in the Abdominal Cavity Signs of Peritonitis Abdominal pain Tenderness Muscle spasm Diminished bowel sounds Nausea/vomiting Distention Solid Organs
Abdomen and Genitalia Injuries Chapter 28 Hollow Organs in the Abdominal Cavity Signs of Peritonitis Abdominal pain Tenderness Muscle spasm Diminished bowel sounds Nausea/vomiting Distention Solid Organs
Diagnosis & Management of Kidney Trauma. LAU - Urology Residency Program LOP Urology Residents Meeting
 Diagnosis & Management of Kidney Trauma LAU - Urology Residency Program LOP Urology Residents Meeting Outline Introduction Investigation Staging Treatment Introduction The kidneys are the most common genitourinary
Diagnosis & Management of Kidney Trauma LAU - Urology Residency Program LOP Urology Residents Meeting Outline Introduction Investigation Staging Treatment Introduction The kidneys are the most common genitourinary
Imaging in abdominal trauma
 Imaging in abdominal trauma Dilyana Baleva Medical University Varna Landesklinikum Mistelbach-Gänserndorf Learning objectives Definition, demographics and etiology Imaging modalities and protocols Common
Imaging in abdominal trauma Dilyana Baleva Medical University Varna Landesklinikum Mistelbach-Gänserndorf Learning objectives Definition, demographics and etiology Imaging modalities and protocols Common
Case Conference. Discussion. Indications of Trauma Blue. Trauma Protocol In SKH. Trauma Blue VS. Trauma Red. Supervisor:VS 楊毓錚 Presenter:R1 周光緯
 Case Conference Supervisor:VS 楊毓錚 Presenter:R1 周光緯 Discussion 2010.7.14 2/81 Trauma Protocol In SKH Indications of Trauma Blue Trauma Blue VS. Trauma Red 3/81 Severe trauma mechanism : 1. Trauma to multiple
Case Conference Supervisor:VS 楊毓錚 Presenter:R1 周光緯 Discussion 2010.7.14 2/81 Trauma Protocol In SKH Indications of Trauma Blue Trauma Blue VS. Trauma Red 3/81 Severe trauma mechanism : 1. Trauma to multiple
PRACTICE GUIDELINE TITLE: NON-OPERATIVE MANAGEMENT OF LIVER / SPLENIC INJURIES
 PRACTICE GUIDELINE Effective Date: 6-18-04 Manual Reference: Deaconess Trauma Services TITLE: N-OPERATIVE MANAGEMENT OF LIVER / SPLENIC INJURIES PURPOSE: To define when non-operative management of liver
PRACTICE GUIDELINE Effective Date: 6-18-04 Manual Reference: Deaconess Trauma Services TITLE: N-OPERATIVE MANAGEMENT OF LIVER / SPLENIC INJURIES PURPOSE: To define when non-operative management of liver
Still is there a Role of Diagnostic Peritoneal Lavage in the Management of Blunt Abdominal Trauma?
 Still is there a Role of Diagnostic Peritoneal Lavage in the Management of Blunt Abdominal Trauma? KHAWAR AWAIS BUTT 1, NABEEL AHMED 2, MEHMOOD ALAM 3, SOMER MASOOD 4 1 Department of Surgery, Avicenna
Still is there a Role of Diagnostic Peritoneal Lavage in the Management of Blunt Abdominal Trauma? KHAWAR AWAIS BUTT 1, NABEEL AHMED 2, MEHMOOD ALAM 3, SOMER MASOOD 4 1 Department of Surgery, Avicenna
Blunt Abdominal Trauma79
 Blunt Abdominal Trauma79 Carlo L. Rosen, Eric L. Legome, and Richard E. Wolfe KEY POINTS Intraperitoneal bleeding is an immediately lifethreatening injury after blunt trauma. Management of intraperitoneal
Blunt Abdominal Trauma79 Carlo L. Rosen, Eric L. Legome, and Richard E. Wolfe KEY POINTS Intraperitoneal bleeding is an immediately lifethreatening injury after blunt trauma. Management of intraperitoneal
The FAST Exam! Dr. David Easton MD FRCPC Critical Care and Emergency Medicine University of Manitoba Canada
 The FAST Exam! Dr. David Easton MD FRCPC Critical Care and Emergency Medicine University of Manitoba Canada Dr. David Easton MD FRCPC Assistant Professor Section of Critical Care and Emergency Medicine
The FAST Exam! Dr. David Easton MD FRCPC Critical Care and Emergency Medicine University of Manitoba Canada Dr. David Easton MD FRCPC Assistant Professor Section of Critical Care and Emergency Medicine
SAS Journal of Surgery ISSN SAS J. Surg., Volume-2; Issue-1 (Jan-Feb, 2016); p Available online at
; p Available online at") SAS Journal of Surgery ISSN 2454-5104 SAS J. Surg., Volume-2; Issue-1 (Jan-Feb, 2016); p-53-59 Available online at http://sassociety.com/sasjs/ Original Research Article Clinical Study, Evaluation and
SAS Journal of Surgery ISSN 2454-5104 SAS J. Surg., Volume-2; Issue-1 (Jan-Feb, 2016); p-53-59 Available online at http://sassociety.com/sasjs/ Original Research Article Clinical Study, Evaluation and
Radiological Investigations of Abdominal Trauma
 76 77 Investigations of Abdominal Trauma Introduction: Trauma to abdominal organs is a common cause of patient morbidity and mortality among trauma patients. Causes of abdominal trauma include blunt injuries,
76 77 Investigations of Abdominal Trauma Introduction: Trauma to abdominal organs is a common cause of patient morbidity and mortality among trauma patients. Causes of abdominal trauma include blunt injuries,
Trauma Workshop! Skills Centre, St George Hospital! Saturday 15 March 2014!
 Trauma Workshop Skills Centre, St George Hospital Saturday 15 March 2014 VMO facilitators: Dr Ricardo Hamilton (Campbelltown Hospital) Dr Mary Langcake (St George Hospital) Dr Anthony Chambers (St George
Trauma Workshop Skills Centre, St George Hospital Saturday 15 March 2014 VMO facilitators: Dr Ricardo Hamilton (Campbelltown Hospital) Dr Mary Langcake (St George Hospital) Dr Anthony Chambers (St George
A Review on the Role of Laparoscopy in Abdominal Trauma
 10.5005/jp-journals-10007-1109 ORIGINAL ARTICLE WJOLS A Review on the Role of Laparoscopy in Abdominal Trauma Aryan Ahmed Specialist General Surgeon, ATLS Instructor, Department of General Surgery, Hamad
10.5005/jp-journals-10007-1109 ORIGINAL ARTICLE WJOLS A Review on the Role of Laparoscopy in Abdominal Trauma Aryan Ahmed Specialist General Surgeon, ATLS Instructor, Department of General Surgery, Hamad
ABDOMINAL TRAUMA MODULE
 INTRODUCTION ABDOMINAL TRAUMA MODULE Blunt abdominal trauma most commonly occurs in the setting of motor vehicle accidents, pedestrian related trauma, direct blows and falls. 1 In these situations, blunt
INTRODUCTION ABDOMINAL TRAUMA MODULE Blunt abdominal trauma most commonly occurs in the setting of motor vehicle accidents, pedestrian related trauma, direct blows and falls. 1 In these situations, blunt
The Focused Assessment with Sonography for Trauma, (FAST) procedure.
 procedure.") The Focused Assessment with Sonography for Trauma, (FAST) procedure. ROBERT H. WRIGLEY Professor Veterinary Diagnostic Imaging University of Sydney Veterinary Teaching Hospital Professor Emeritus Colorado
The Focused Assessment with Sonography for Trauma, (FAST) procedure. ROBERT H. WRIGLEY Professor Veterinary Diagnostic Imaging University of Sydney Veterinary Teaching Hospital Professor Emeritus Colorado
We have reviewed this material in accordance with U.S. Copyright Law and have tried to maximize your ability to
 Author(s): Patrick Carter, Daniel Wachter, Rockefeller Oteng, Carl Seger, 2009-2010. License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution
Author(s): Patrick Carter, Daniel Wachter, Rockefeller Oteng, Carl Seger, 2009-2010. License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution
MEDICAL MANAGEMENT OF ABDOMINAL TRAUMA. LUIS H. TELLO MV, MS, DVM, COS Portland Hospital Classic International Medical Advisor Banfield Pet Hospital
 MEDICAL MANAGEMENT OF ABDOMINAL TRAUMA LUIS H. TELLO MV, MS, DVM, COS Portland Hospital Classic International Medical Advisor Banfield Pet Hospital ABDOMINAL TRAUMA 70-80% of multiple trauma patients 55%
MEDICAL MANAGEMENT OF ABDOMINAL TRAUMA LUIS H. TELLO MV, MS, DVM, COS Portland Hospital Classic International Medical Advisor Banfield Pet Hospital ABDOMINAL TRAUMA 70-80% of multiple trauma patients 55%
The Trauma Pan Scan A SYSTEMATIC APPROACH TO NOT KILLING THE PATIENT
 The Trauma Pan Scan A SYSTEMATIC APPROACH TO NOT KILLING THE PATIENT On-call duty Trauma patient Questions by ER doctors Questions by consultants What to do when you don t have time to think?! Questions
The Trauma Pan Scan A SYSTEMATIC APPROACH TO NOT KILLING THE PATIENT On-call duty Trauma patient Questions by ER doctors Questions by consultants What to do when you don t have time to think?! Questions
A PROSPECTIVE STUDY OF CONSERVATIVE MANAGEMENT IN CASES OF HEMOPERITONEUM IN SOLID ORGAN INJURIES AT TERTIARY CARE HOSPITAL IN WESTERN INDIA
 RESEARCH ARTICLE A PROSPECTIVE STUDY OF CONSERVATIVE MANAGEMENT IN CASES OF HEMOPERITONEUM IN SOLID ORGAN INJURIES AT TERTIARY CARE HOSPITAL IN WESTERN INDIA Chintan Patel 1, Isha Patel 2, Divyang Dave
RESEARCH ARTICLE A PROSPECTIVE STUDY OF CONSERVATIVE MANAGEMENT IN CASES OF HEMOPERITONEUM IN SOLID ORGAN INJURIES AT TERTIARY CARE HOSPITAL IN WESTERN INDIA Chintan Patel 1, Isha Patel 2, Divyang Dave
Pediatric Trauma Karim Rafaat, MD
 Pediatric Trauma Karim Rafaat, MD Goals Time is short I m going to presume you know your basic ATLS (that s that whole ABCD thing, by the way) Discuss each general trauma susceptible region Focus on: Epidemiology
Pediatric Trauma Karim Rafaat, MD Goals Time is short I m going to presume you know your basic ATLS (that s that whole ABCD thing, by the way) Discuss each general trauma susceptible region Focus on: Epidemiology
Emergency CT of blunt abdominal trauma: experience from a large urban hospital in Southern China
 Review Article Emergency CT of blunt abdominal trauma: experience from a large urban hospital in Southern China Jingshan Gong, Dongdong Mei, Minjie Yang, Jianmin Xu, Yangyang Zhou Department of Radiology,
Review Article Emergency CT of blunt abdominal trauma: experience from a large urban hospital in Southern China Jingshan Gong, Dongdong Mei, Minjie Yang, Jianmin Xu, Yangyang Zhou Department of Radiology,
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines
 Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Splenic Injury Evaluation and Management Guideline ADULT Practice Management Guideline Contact: Trauma Center Medical
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Splenic Injury Evaluation and Management Guideline ADULT Practice Management Guideline Contact: Trauma Center Medical
Selective Nonoperative Management of Penetrating Abdominal Trauma. Kings County Hospital Center Verena Liu, MD 10/13/2011
 Selective Nonoperative Management of Penetrating Abdominal Trauma Kings County Hospital Center Verena Liu, MD 10/13/2011 Case Presentation 28M admitted on 8/27/2011 s/p GSW to right upper quadrant and
Selective Nonoperative Management of Penetrating Abdominal Trauma Kings County Hospital Center Verena Liu, MD 10/13/2011 Case Presentation 28M admitted on 8/27/2011 s/p GSW to right upper quadrant and
Conservative Versus Delayed Laparoscopic Exploration for Blunt Abdominal Trauma
 Med. J. Cairo Univ., Vol. 80, No. 1, September: 575-584, 2012 www.medicaljournalofcairouniversity.com Conservative Versus Delayed Laparoscopic Exploration for Blunt Abdominal Trauma TAMER M. NABIL, M.D.*;
Med. J. Cairo Univ., Vol. 80, No. 1, September: 575-584, 2012 www.medicaljournalofcairouniversity.com Conservative Versus Delayed Laparoscopic Exploration for Blunt Abdominal Trauma TAMER M. NABIL, M.D.*;
Enter modality here Enter modality here, enter none if none. Principal Modality (2): Case Report # [] Date accepted: April 2015
![Enter modality here Enter modality here, enter none if none. Principal Modality (2): Case Report # [] Date accepted: April 2015](/thumbs/83/87309292.jpg "Enter modality here Enter modality here, enter none if none. Principal Modality (2): Case Report # [] Date accepted: April 2015") Radiological Category: Enter category here Principal Modality (1): Principal Modality (2): Enter modality here Enter modality here, enter none if none Case Report # [] Submitted by: Varun Rachakonda, M.D.
Radiological Category: Enter category here Principal Modality (1): Principal Modality (2): Enter modality here Enter modality here, enter none if none Case Report # [] Submitted by: Varun Rachakonda, M.D.
PONGSASIT SINGHATAS, M.D. Department of Surgery Faculty of Medicine, Ramathibodi Hospital Mahidol University
 PONGSASIT SINGHATAS, M.D. Department of Surgery Faculty of Medicine, Ramathibodi Hospital Mahidol University Patient survive Low morbidity GOOD JUDGMENT COMES FROM EXPERIENCE EXPERIENCE COMES FROM BAD
PONGSASIT SINGHATAS, M.D. Department of Surgery Faculty of Medicine, Ramathibodi Hospital Mahidol University Patient survive Low morbidity GOOD JUDGMENT COMES FROM EXPERIENCE EXPERIENCE COMES FROM BAD
Pancreatico-Duodenal Trauma: Drain, Debride, Divert, Despair BACKGROUND EPIDEMIOLOGY 9/11/2018
 Pancreatico-Duodenal Trauma: Drain, Debride, Divert, Despair Rochelle A. Dicker, M.D. Professor of Surgery and Anesthesia UCLA BACKGROUND Lancet 1827: Travers, B Rupture of the Pancreas British Journal
Pancreatico-Duodenal Trauma: Drain, Debride, Divert, Despair Rochelle A. Dicker, M.D. Professor of Surgery and Anesthesia UCLA BACKGROUND Lancet 1827: Travers, B Rupture of the Pancreas British Journal
If your patient is stable, perform a complete assessment using inspection, auscultation, percussion, and pal- By Cynthia Blank-Reid, RN, CEN, MSN
 Abdominal trauma: Dealing with the damage Hidden in the abdomen, life-threatening injuries can elude detection. Find out how to evaluate your patient s condition and prevent further harm. By Cynthia Blank-Reid,
Abdominal trauma: Dealing with the damage Hidden in the abdomen, life-threatening injuries can elude detection. Find out how to evaluate your patient s condition and prevent further harm. By Cynthia Blank-Reid,
A Severely Injured Pediatric Trauma Patient: Case Presentation and Discussion
 A Severely Injured Pediatric Trauma Patient: Case Presentation and Discussion Christopher Butts PhD, DO Surgical Critical Care Fellow Cooper University Hospital H&P 10 year old female presents as a trauma
A Severely Injured Pediatric Trauma Patient: Case Presentation and Discussion Christopher Butts PhD, DO Surgical Critical Care Fellow Cooper University Hospital H&P 10 year old female presents as a trauma
Objectives. Review ATLS from the pediatric perspective Convince you that children aren t simply little. Impress you with my Power Point mastery
 Pediatric Trauma Objectives Review ATLS from the pediatric perspective Convince you that children aren t simply little adults (especially when it comes to trauma) Impress you with my Power Point mastery
Pediatric Trauma Objectives Review ATLS from the pediatric perspective Convince you that children aren t simply little adults (especially when it comes to trauma) Impress you with my Power Point mastery
Canadian Undergraduate Urology Curriculum (CanUUC): Genitourinary Trauma. Last reviewed June 2014
: Genitourinary Trauma. Last reviewed June 2014") Canadian Undergraduate Urology Curriculum (CanUUC): Genitourinary Trauma Last reviewed June 2014 Session Objectives 1. Recognize hematuria as the cardinal symptom of urinary tract trauma. 1. Outline the
Canadian Undergraduate Urology Curriculum (CanUUC): Genitourinary Trauma Last reviewed June 2014 Session Objectives 1. Recognize hematuria as the cardinal symptom of urinary tract trauma. 1. Outline the
I have no financial disclosures.
 In the Belly of the Whale: Surviving Thoracoabdominal Trauma Debra Esernio Jenssen, MD, FAAP I have no financial disclosures. Objectives Review epidemiology of abusive chest and abdominal trauma. Identify
In the Belly of the Whale: Surviving Thoracoabdominal Trauma Debra Esernio Jenssen, MD, FAAP I have no financial disclosures. Objectives Review epidemiology of abusive chest and abdominal trauma. Identify
A prospective evaluation of the predictive value of serum amylase levels in the assessment of patients with blunt abdominal trauma
 A prospective evaluation of the predictive value of serum amylase levels in the assessment of patients with blunt abdominal trauma I E Donkin, R Jones, C Aldous, D L Clarke Department of General Surgery,
A prospective evaluation of the predictive value of serum amylase levels in the assessment of patients with blunt abdominal trauma I E Donkin, R Jones, C Aldous, D L Clarke Department of General Surgery,
SPINE EVALUATION AND CLEARANCE Basic Principles
 SPINE EVALUATION AND CLEARANCE Basic Principles General 1. Entire spine is immobilized during primary survey. 2. Radiographic clearance of the spine is not required before emergent surgical procedures.
SPINE EVALUATION AND CLEARANCE Basic Principles General 1. Entire spine is immobilized during primary survey. 2. Radiographic clearance of the spine is not required before emergent surgical procedures.
Renal Trauma: Management Options
 Renal Trauma: Management Options Immediate surgical repair Nephrectomy Conservative management Alonso RC et al. Kidney in Danger: CT Findings of Blunt and Penetrating Renal Trauma. RadioGraphics 2009;
Renal Trauma: Management Options Immediate surgical repair Nephrectomy Conservative management Alonso RC et al. Kidney in Danger: CT Findings of Blunt and Penetrating Renal Trauma. RadioGraphics 2009;
Urogenital Injuries The role of radiology
 Urogenital Injuries The role of radiology NORDTER 7 th Nordic Trauma Radiology Course Helsinki, Finland May 21-24, 2012 Johann Baptist Dormagen, MD, PhD Oslo University Hospital, Norway Kidney injuries
Urogenital Injuries The role of radiology NORDTER 7 th Nordic Trauma Radiology Course Helsinki, Finland May 21-24, 2012 Johann Baptist Dormagen, MD, PhD Oslo University Hospital, Norway Kidney injuries
Interventional Radiology for Solid Organ Trauma. Case Study 8/17/2017. Diagnosis? Case Study (cont d)
") Interventional Radiology for Solid Organ Trauma Jamie Gallivan RN, BSN Interventional Radiology Case Study 6 y/o boy fell out of 2 nd story window onto concrete Hemodynamically stable at scene Arrival
Interventional Radiology for Solid Organ Trauma Jamie Gallivan RN, BSN Interventional Radiology Case Study 6 y/o boy fell out of 2 nd story window onto concrete Hemodynamically stable at scene Arrival
Little Kids in Big Crashes The Bio-mechanics of Kids in Car Crashes. Lisa Schwing, RN Trauma Program Manager Dayton Children s
 Little Kids in Big Crashes The Bio-mechanics of Kids in Car Crashes Lisa Schwing, RN Trauma Program Manager Dayton Children s Very Little Research There has been very little research on the forces a crash
Little Kids in Big Crashes The Bio-mechanics of Kids in Car Crashes Lisa Schwing, RN Trauma Program Manager Dayton Children s Very Little Research There has been very little research on the forces a crash
A Clinical Study of Blunt Injury Abdomen in a Tertiary Care Hospital
 Original Article Print ISSN: 2321-6379 Online ISSN: 2321-595X DOI: 10.17354/ijss/2017/167 A Clinical Study of Blunt Injury Abdomen in a Tertiary Care Hospital J Amuthan 1, A Vijay 2, C Pradeep 2, Heber
Original Article Print ISSN: 2321-6379 Online ISSN: 2321-595X DOI: 10.17354/ijss/2017/167 A Clinical Study of Blunt Injury Abdomen in a Tertiary Care Hospital J Amuthan 1, A Vijay 2, C Pradeep 2, Heber
ISPUB.COM. Traumatic Uretero-Pelvic Junction Disruption. G Kraushaar, S Harder, K Visvanathan INTRODUCTION CASE REPORT
 ISPUB.COM The Internet Journal of Radiology Volume 4 Number 1 Traumatic Uretero-Pelvic Junction Disruption G Kraushaar, S Harder, K Visvanathan Citation G Kraushaar, S Harder, K Visvanathan. Traumatic
ISPUB.COM The Internet Journal of Radiology Volume 4 Number 1 Traumatic Uretero-Pelvic Junction Disruption G Kraushaar, S Harder, K Visvanathan Citation G Kraushaar, S Harder, K Visvanathan. Traumatic
The ABC s of Chest Trauma
 The ABC s of Chest Trauma J Bradley Pickhardt MD, FACS Providence St Patrick Hospital What s the Problem? 2/3 of trauma patients have chest trauma Responsible for 25% of all trauma deaths Most injuries
The ABC s of Chest Trauma J Bradley Pickhardt MD, FACS Providence St Patrick Hospital What s the Problem? 2/3 of trauma patients have chest trauma Responsible for 25% of all trauma deaths Most injuries
Major Trauma Scenarios. Ballarat Health Services Emergency Medicine Training Hub
 Major Trauma Scenarios Ballarat Health Services Emergency Medicine Training Hub Trauma Scenario 1 You receive a phone call from the ambulance service. They have a 27 yr old male involved in a MCA, he is
Major Trauma Scenarios Ballarat Health Services Emergency Medicine Training Hub Trauma Scenario 1 You receive a phone call from the ambulance service. They have a 27 yr old male involved in a MCA, he is
Intra- abdominal Solid Organ Injuries in Blunt Injury Abdomen in Tertiary Care Medical College Hospital, Madurai: A Prospective study
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 16, Issue 11 Ver. III (Nov. 2017), PP 46-50 www.iosrjournals.org Intra- abdominal Solid Organ Injuries
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 16, Issue 11 Ver. III (Nov. 2017), PP 46-50 www.iosrjournals.org Intra- abdominal Solid Organ Injuries
Medical - Clinical Research & Reviews
 Research Article Research Article Medical - Clinical Research & Reviews ISSN 2575-6087 Management of Kidney in Saiful Anwar General Hospital Malang Indonesia Besut Daryanto, I Made Udiyana Indradiputra,
Research Article Research Article Medical - Clinical Research & Reviews ISSN 2575-6087 Management of Kidney in Saiful Anwar General Hospital Malang Indonesia Besut Daryanto, I Made Udiyana Indradiputra,
Free fluid accumulation following blunt abdominal trauma: potential for expansion of the FAST protocol
 Hong Kong Journal of Emergency Medicine Free fluid accumulation following blunt abdominal trauma: potential for expansion of the FAST protocol N Simpson, P Page, DM Taylor Objective: To determine sites
Hong Kong Journal of Emergency Medicine Free fluid accumulation following blunt abdominal trauma: potential for expansion of the FAST protocol N Simpson, P Page, DM Taylor Objective: To determine sites
ISPUB.COM. S Gopalswamy, R Mohanraj, P Viswanathan, V Baskaran INTRODUCTION HYPOTHESIS MATERIAL AND METHODS RESULTS
 ISPUB.COM The Internet Journal of Surgery Volume 15 Number 2 Non-Operative Management of Solid Organ Injuries due to Blunt Abdominal Trauma (NOMAT): Seven-year experience in a Teaching District General
ISPUB.COM The Internet Journal of Surgery Volume 15 Number 2 Non-Operative Management of Solid Organ Injuries due to Blunt Abdominal Trauma (NOMAT): Seven-year experience in a Teaching District General
Study of management of blunt injuries to solid abdominal organs
 Original article: Study of management of blunt injuries to solid abdominal organs 1Dr. Jayant Jain, 2 Dr. S.P. Singh, 3 Dr. Arun Bhargava 1III year resident, Dept of General Surgery NIMS hospital and medical
Original article: Study of management of blunt injuries to solid abdominal organs 1Dr. Jayant Jain, 2 Dr. S.P. Singh, 3 Dr. Arun Bhargava 1III year resident, Dept of General Surgery NIMS hospital and medical
10/2/2018. Acute Management of Pelvic Injuries. Learning Objectives. 17 yo male ped struck by truck
 17 yo male ped struck by truck Acute Management of Pelvic Injuries David Volgas, MD CoxHealth University of Missouri HD unstable Open pelvic wound superior gluteal fold through rectum to scrotum Open rami
17 yo male ped struck by truck Acute Management of Pelvic Injuries David Volgas, MD CoxHealth University of Missouri HD unstable Open pelvic wound superior gluteal fold through rectum to scrotum Open rami
Gastrointestinal Emergencies CEN REVIEW 2017 MARY RALEY, BSN, RN, CEN, TCRN, TNSCC
 Gastrointestinal Emergencies CEN REVIEW 2017 MARY RALEY, BSN, RN, CEN, TCRN, TNSCC Gastrointestinal Emergencies is 7% of the CEN A. Acute abdomen B. Bleeding C. Cholecystitis D. Cirrhosis E. Diverticulitis
Gastrointestinal Emergencies CEN REVIEW 2017 MARY RALEY, BSN, RN, CEN, TCRN, TNSCC Gastrointestinal Emergencies is 7% of the CEN A. Acute abdomen B. Bleeding C. Cholecystitis D. Cirrhosis E. Diverticulitis
Blunt abdominal trauma: changing patterns in diagnostic and treatment strategies van der Vlies, C.H.
 UvA-DARE (Digital Academic Repository) Blunt abdominal trauma: changing patterns in diagnostic and treatment strategies van der Vlies, C.H. Link to publication Citation for published version (APA): van
UvA-DARE (Digital Academic Repository) Blunt abdominal trauma: changing patterns in diagnostic and treatment strategies van der Vlies, C.H. Link to publication Citation for published version (APA): van
IMAGING OF BLUNT ABDOMINAL TRAUMA, PART I
 IMAGING OF BLUNT ABDOMINAL TRAUMA, PART I QuickTime and a TIFF (Uncompressed) decompressor are needed to see this picture. Ruedi F. Thoeni, M. D. D University of California, San Francisco SCBT-MR Summer
IMAGING OF BLUNT ABDOMINAL TRAUMA, PART I QuickTime and a TIFF (Uncompressed) decompressor are needed to see this picture. Ruedi F. Thoeni, M. D. D University of California, San Francisco SCBT-MR Summer
Fall down stairs. Left rib fractures. John A Cieslak III, MD, PhD Charan Singh, MD
 Fall down stairs. Left rib fractures. John A Cieslak III, MD, PhD Charan Singh, MD ? Splenic lacerations, hemoperitoneum, and traumatic pseudoaneurysm formation. High attenuation extraluminal contrast
Fall down stairs. Left rib fractures. John A Cieslak III, MD, PhD Charan Singh, MD ? Splenic lacerations, hemoperitoneum, and traumatic pseudoaneurysm formation. High attenuation extraluminal contrast
vel 2 Level 2 3,034 c-spine evaluations with CSR Level 3 detected injury only 53% of the time. Level 3 False (-) rate 47%
 rate 47%") Objectives Blunt and Penetrating Neck Trauma Julie Mayglothling, MD, FACEP Virginia Commonwealth University Richmond, VA Summit to Sound, May 20 th, 2011 Blunt Neck Trauma Evaluation of the low mechanism,
Objectives Blunt and Penetrating Neck Trauma Julie Mayglothling, MD, FACEP Virginia Commonwealth University Richmond, VA Summit to Sound, May 20 th, 2011 Blunt Neck Trauma Evaluation of the low mechanism,
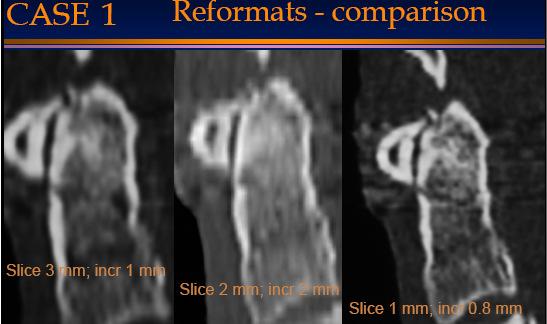
General Imaging. Imaging modalities. Incremental CT. Multislice CT Multislice CT [ MDCT ]
![General Imaging. Imaging modalities. Incremental CT. Multislice CT Multislice CT [ MDCT ]](/thumbs/76/74079340.jpg "General Imaging. Imaging modalities. Incremental CT. Multislice CT Multislice CT [ MDCT ]") General Imaging Imaging modalities Conventional X-rays Ultrasonography [ US ] Computed tomography [ CT ] Radionuclide imaging Magnetic resonance imaging [ MRI ] Angiography conventional, CT,MRI Interventional
General Imaging Imaging modalities Conventional X-rays Ultrasonography [ US ] Computed tomography [ CT ] Radionuclide imaging Magnetic resonance imaging [ MRI ] Angiography conventional, CT,MRI Interventional
Algorithms for managing the common trauma patient
 ALGORITHMS Algorithms for managing the common trauma patient J John, MB ChB Department of Urology, Frere Hospital, East London Hospital Complex, East London, South Africa Corresponding author: J John (jeffveenajohn@gmail.com)
ALGORITHMS Algorithms for managing the common trauma patient J John, MB ChB Department of Urology, Frere Hospital, East London Hospital Complex, East London, South Africa Corresponding author: J John (jeffveenajohn@gmail.com)
Office of the Chief Medical Examiner Persons Present
 Office of the Chief Medical Examiner CB # 7580 Chapel Hill, NC 27599-7580 Telephone 9199662253 REPORT OF AUTOPSY EXAMINATION DECEDENT Document Identifier B200901668 Autopsy Type ME Autopsy Name John Walter
Office of the Chief Medical Examiner CB # 7580 Chapel Hill, NC 27599-7580 Telephone 9199662253 REPORT OF AUTOPSY EXAMINATION DECEDENT Document Identifier B200901668 Autopsy Type ME Autopsy Name John Walter
Background Focused Assessment with Sonography in Trauma. Johann Baptist Dormagen, MD, PhD
 Focused Assessment with Sonography in Trauma Johann Baptist Dormagen, MD, PhD Unit of Abdominal and Oncologic Radiology Department of Radiology and Nuclear Medicine Oslo University Hospital, Norway 8 th
Focused Assessment with Sonography in Trauma Johann Baptist Dormagen, MD, PhD Unit of Abdominal and Oncologic Radiology Department of Radiology and Nuclear Medicine Oslo University Hospital, Norway 8 th
Guideline for the Management of Blunt Liver and Spleen Injuries
 Pediatric Trauma Practice Guideline Management of Blunt Liver and Spleen Guideline for the Management of Blunt Liver and Spleen Background: Children are more vulnerable to blunt abdominal injury than adults.
Pediatric Trauma Practice Guideline Management of Blunt Liver and Spleen Guideline for the Management of Blunt Liver and Spleen Background: Children are more vulnerable to blunt abdominal injury than adults.
Case Discussion Splenic Abscess
 Case Discussion Splenic Abscess Personal Data Gender: male Birth Date: 1928/Mar/06th Allergy: Mefenamic Smoking: 0.5 PPD for 55 years Alcohol: negative (?) 4 Months Ago Abdominal pain: epigastric area
Case Discussion Splenic Abscess Personal Data Gender: male Birth Date: 1928/Mar/06th Allergy: Mefenamic Smoking: 0.5 PPD for 55 years Alcohol: negative (?) 4 Months Ago Abdominal pain: epigastric area
Ultrasound in abdominal trauma: an
 Archives of Emergency Medicine, 1988, 5, 26-33 Ultrasound in abdominal trauma: an alternative to peritoneal lavage J. A. CHAMBERS & W. J. PILBROW Accident Unit, Countess of Chester Hospital, Chester, England
Archives of Emergency Medicine, 1988, 5, 26-33 Ultrasound in abdominal trauma: an alternative to peritoneal lavage J. A. CHAMBERS & W. J. PILBROW Accident Unit, Countess of Chester Hospital, Chester, England
A Pattern of Abdominal Organs Injuries in Blunt Trauma and Their Outcome
 ORIGINAL ARTICLE A Pattern of Abdominal Organs Injuries in Blunt Trauma and Their Outcome RIAZ AHMAD, YASEEN RAFI, RANA SOHAIL, MAHAM JAVED, MUSHAL NOOR, KHALID JAVAID ABID ABSTRACT Aim: To found out pattern
ORIGINAL ARTICLE A Pattern of Abdominal Organs Injuries in Blunt Trauma and Their Outcome RIAZ AHMAD, YASEEN RAFI, RANA SOHAIL, MAHAM JAVED, MUSHAL NOOR, KHALID JAVAID ABID ABSTRACT Aim: To found out pattern
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal injuries clinical presentation of, 23 24 Abdominal trauma evaluation for pediatric surgeon, 59 74 background of, 60 colon and
Index Note: Page numbers of article titles are in boldface type. A Abdominal injuries clinical presentation of, 23 24 Abdominal trauma evaluation for pediatric surgeon, 59 74 background of, 60 colon and
Role of CT in Evaluation of Blunt Abdominal Trauma
 International Journal of Medical Imaging 2015; 3(5): 89-93 Published online July 29, 2015 (http://www.sciencepublishinggroup.com/j/ijmi) doi: 10.11648/j.ijmi.20150305.11 ISSN: 2330-8303 (Print); ISSN:
International Journal of Medical Imaging 2015; 3(5): 89-93 Published online July 29, 2015 (http://www.sciencepublishinggroup.com/j/ijmi) doi: 10.11648/j.ijmi.20150305.11 ISSN: 2330-8303 (Print); ISSN:
Lab Monitor Images Dissection of the Abdominal Vasculature + Lower Digestive System
 Lab Monitor Images Dissection of the Abdominal Vasculature + Lower Digestive System Stomach & Duodenum Frontal (AP) View Nasogastric tube 2 1 3 4 Stomach Pylorus Duodenum 1 Duodenum 2 Duodenum 3 Duodenum
Lab Monitor Images Dissection of the Abdominal Vasculature + Lower Digestive System Stomach & Duodenum Frontal (AP) View Nasogastric tube 2 1 3 4 Stomach Pylorus Duodenum 1 Duodenum 2 Duodenum 3 Duodenum
TEVAR for trauma is here to stay: Advances in the Treatment of Blunt Thoracic Aortic Injury
 TEVAR for trauma is here to stay: Advances in the Treatment of Blunt Thoracic Aortic Injury Megan Brenner MD MS RPVI FACS Associate Professor of Surgery Division of Trauma/Surgical Critical Care, RA Cowley
TEVAR for trauma is here to stay: Advances in the Treatment of Blunt Thoracic Aortic Injury Megan Brenner MD MS RPVI FACS Associate Professor of Surgery Division of Trauma/Surgical Critical Care, RA Cowley
UBC Department of Urologic Sciences Lecture Series. Urological Trauma
 UBC Department of Urologic Sciences Lecture Series Urological Trauma Disclaimer: This is a lot of information to cover and we are unlikely to cover it all today These slides are to be utilized for your
UBC Department of Urologic Sciences Lecture Series Urological Trauma Disclaimer: This is a lot of information to cover and we are unlikely to cover it all today These slides are to be utilized for your
n Make tremendous difference in patients lives: n Diagnosing or excluding disease and injury n Evaluating response to therapy
 Imaging: Choosing the Appropriate Exam Rob Milman, MD Austin Radiological Association What is a Radiologist? A physician who specializes in diagnosing and treating disease and injury by using medical imaging
Imaging: Choosing the Appropriate Exam Rob Milman, MD Austin Radiological Association What is a Radiologist? A physician who specializes in diagnosing and treating disease and injury by using medical imaging
West Yorkshire Major Trauma Network Clinical Guidelines 2015
 WYMTN: Pelvic fracture with urogenital trauma KEY RECOMMENDATIONS 1. During the initial exploratory survey / secondary survey, a. The external urethral meatus and the transurethral bladder catheter (if
WYMTN: Pelvic fracture with urogenital trauma KEY RECOMMENDATIONS 1. During the initial exploratory survey / secondary survey, a. The external urethral meatus and the transurethral bladder catheter (if
Role of Imaging in the evaluation of Renal Trauma
 Role of Imaging in the evaluation of Renal Trauma M. H. Ather,M.A. Noor ( Department of Surgery, The Aga Khan University, Karachi. ) Trauma is the leading cause of morbidity and mortality among young adults
Role of Imaging in the evaluation of Renal Trauma M. H. Ather,M.A. Noor ( Department of Surgery, The Aga Khan University, Karachi. ) Trauma is the leading cause of morbidity and mortality among young adults
Abdominal Solid Organ Injury
 Abdominal Solid Organ Injury 9th Nordic Trauma Radiology Course Aarhus, Denmark May 23-26, 2016 K.SHANMUGANATHAN M.D. ABDOMINAL TRAUMA OBJECTIVES Splenic injury Late arterial / early p-v phase imaging
Abdominal Solid Organ Injury 9th Nordic Trauma Radiology Course Aarhus, Denmark May 23-26, 2016 K.SHANMUGANATHAN M.D. ABDOMINAL TRAUMA OBJECTIVES Splenic injury Late arterial / early p-v phase imaging