Pain Management in the Surgical Patient. Peter Vogel, VMD, DACVS
|
|
|
- Tyler Hoover
- 6 years ago
- Views:
Transcription


1 Pain Management in the Surgical Patient Peter Vogel, VMD, DACVS
2 Pain Pathways u Specialized neurons that travel through the spinal cord u Free nerve endings in skin, connective tissue, muscle and bone u Cell bodies in the dorsal root ganglia
3 Pain Pathways u Afferent system consisting of 3 neurons u Cell body that bifurcates with one end in the peripheral tissue and one in the dorsal horn u Second order neurons ascend in the contralateral spinothalamic tract u Third order neurons in the contralateral thalamus project to the somatosensory cortex
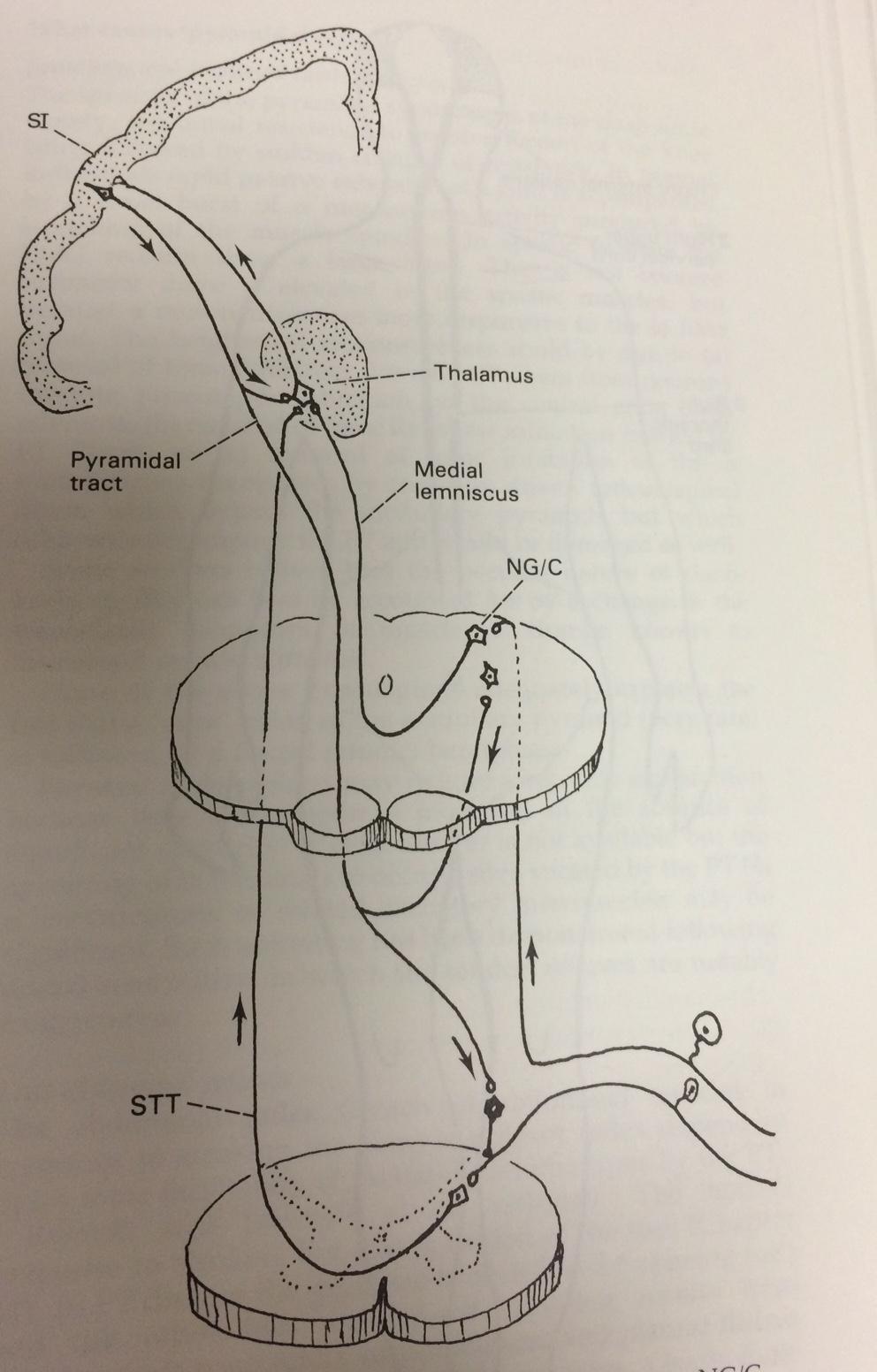
4
5 Acute Pain u Acute pain is usually nociceptive pain u Tissue damage leads to activation of small nerve endings and inflammatory cells u Inflammatory mediators cause pain via nociceptive stimulation and increased excitability of nerve endings u NOTE: Complex system, not just neurons involved**
6 u Pain management strategies should target as many aspects of the nociceptive response as possible u Variety of pain receptors and mediators can be manipulated and controlled via pharmacologic intervention.
7 Pre-operative Medications u All surgical patients should have pre-operative pain medication ugeneral anesthesia blocks the brain from feeling pain, but does not prevent activation of the local and spinal pain pathways (ramp up) uit is better to prevent stimulation of the nociceptive pathways than try and treat them post-operatively.
8 Pre-operative Medications u Nociceptive pathways are activated both by inflammation and direct neuron stimulation u Narcotics will help decrease neuronal stimulation u NSAIDS will help minimize inflammatory stimulation u Unless contra-indicated, both should be given
9 Butorphanol u Mixed agonist-antagonist u More sedatory than analgesic u Fairly rapid onset u Analgesia lasts 1-3 hours u Bonds more tightly than pure agonists u Appropriate for mild-moderate pain only
10 Buprenorphine u Partial Mu agonist u SLOW ONSET (20 minutes minimum) u Lasts 4-8 hours at common dosages u Used for mild-moderate pain u Well tolerated in cats u Buprenorphine displaces morphine, methadone, and other full opioid agonists from receptors. It also can block the effects of other opioids. u Extreme receptor affinity (not reversed by naloxone) but low intrinsic activity
11 u The main reason for use of butorphanol and buprenorphine in the past was that they were not controlled substances u There are better narcotics for use in operative patients
12 Morphine u Prototypical opioid u Onset of action minutes u Hepatic metabolism and renal excretion (use with caution in patients with renal disease) u Can be used in cats!! u Morphine Mania is due to inappropriately high doses in cats u Causes mydriasis rather than miosis in cats
13 Morphine u Cardiovascular depression u Dose dependent respiratory depression u Low lipid solubility (slow onset IV), useful for epidural injection u Can be given intra-articularly (0.1 mgs/kg diluted in saline) u Oral forms have low bio-availability u Histamine release
14 Hydromorphone/Oxymorphone u 5-10X more potent than morphine u Does not cause histamine release u minute onset of action IV, lasts 2-6 hours u Much slower onset when given IM or SQ u Hyperthermia in cats (not responsive to naloxone) u Must monitor temperature
15 Fentanyl u 100X more potent than morphine u High lipid solubility = rapid onset of action u Rapidly redistributed = short duration of action u Can be given IV, IM, epidurally, transmucosally, and transdermally u Usually given as an IV bolus followed by a CRI
16 Methadone u Methadone is a mu-receptor (OP3; MOR) agonist that also is a non-competitive inhibitor of NMDA (n-methyl-daspartate) receptors. Methadone can also reduce reuptake of norepinephrine and serotonin, which may contribute to its analgesic effects. Due to these other actions, methadone potentially may be more efficacious than other mu- agonists (e.g., morphine) particularly for neuropathic or chronic pain. Methadone is more lipidsoluble than morphine and approximately 1-1.5X as potent. It does not cause significant histamine release when administered intravenously.
17 Methadone u Usually given as an IV CRI u Can be dosed IV, IM, and SC
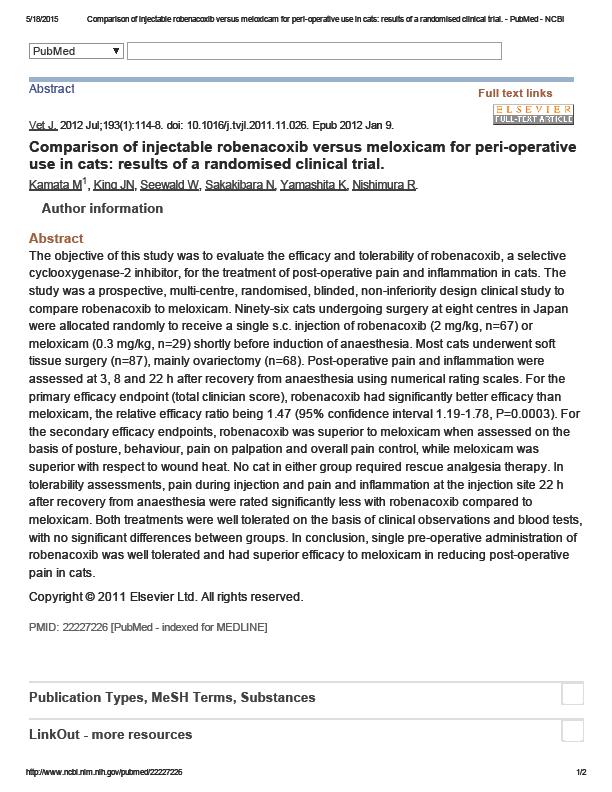
18 NSAIDS u Unless contra-indicated, all surgical patients should receive injectable NSAIDs pre-operatively u Yes, you can give NSAIDs to cats u Meloxicam ( mgs/kg IV/SQ) u Robenicoxib (Onsior) (2 mgs/kg IV/SQ) u Reduces inflammation and release of inflammatory mediators
19
20 Post-operative Pain Management u If your pre-operative protocol is effective, postoperative pain management will be much easier u Far easier to prevent activation of nociceptive pathways than to suppress them later
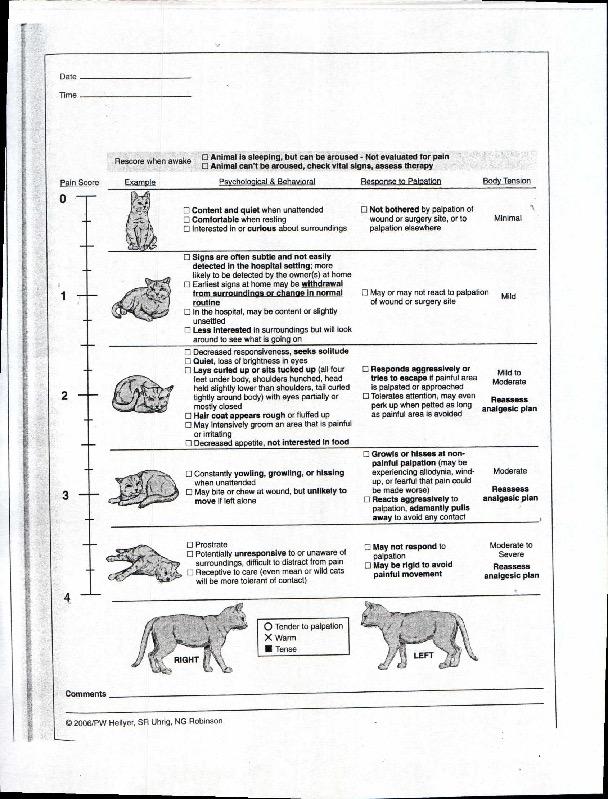
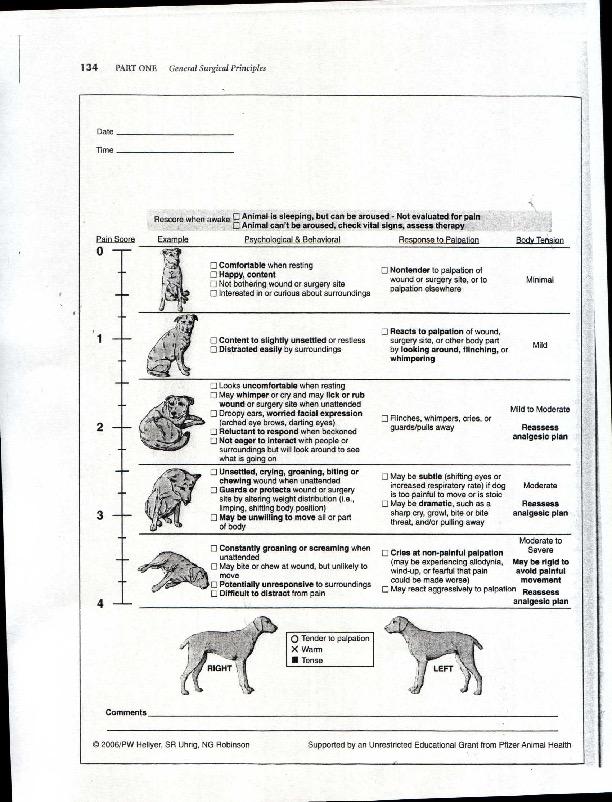
21 Pain Assessment u CSU pain score chart (see handout) u Cats and dogs show pain differently u If in doubt, assume the patient is painful u Best indication is behavior
22 Pain vs Dysphoria u Can be difficult to differentiate pain vs. dysphoria secondary to general anesthesia u Micro-dose Dexmedetomidine test: u 1-2 mcg/kg IV u If dysphoric, patient will respond u If painful, minimal response seen
23 Opioids u All patients should receive post-operative opioid analgesia u Dosages and effects/actions similar to pre-operative u Vomiting post-operatively from opioids is uncommon
24 Butorphanol u Useful for mild-moderate pain u Slow onset, short duration of action for analgesia, longer for sedation u Often combined with dexmedetomidine or acepromazine u Caution in compromised patients u Probably should not be used for any patient where significant pain is anticipated u Pure agonist can be administered if needed
25 Buprenorphine u Very slow onset of action u Threshold effect (giving more does not increase pain relief) u Higher doses do, however, last longer u 50 mcg/kg will last 24 hours u Cannot give any other opioid if buprenorphine is not effective due to high binding affinity u Can be used to reverse other opioid without removing all pain control
26 Hydromorphone/Oxymorphone u Commonly given at 0.1 mg/kg q 4-6 hrs as needed u Dose can be increased if necessary u Given IV, IM, or SQ
27 Methadone u Effective as CRI or as intermittent dosing (q4-6 hrs) u Slightly more effective than morphine
28 Methadone u Dogs: mgs/kg IV followed by 0.12 mgs/kg/hr OR mg/kg q4-8 hrs IV. IM, SQ u Cats: mgs/kg IV followed by 0.12 mgs/kg/hr OR mg/kg q 4-6 hrs IV, IM, SQ u Oral form poorly absorbed
29 Fentanyl u Usually used as a CRI (2-8 mcg/kg/hr) u Requires infusion pump u Bolus can be given and CRI rate increased if pain control inadequate u CRI should be tapered over hours as other pain control medications are taking effect. u Very short duration
30 Medications TGH u What options do we have? u How effective are they?
31 Oxycodone u Poor bioavailability u High potential for abuse by owner
32 Codeine u Poor bioavailablity
33 Acetaminophen/Hydrocodone u Acetaminophen is ineffective but well tolerated in dogs as long as the dosage is not too high u Acetaminophen is highly toxic to cats u mg/kg Hydrocodone u DO NOT EXCEED 15 MG/KG ACETAMINOPHEN u 20 kgs or larger for tablets
34 Fentanyl Patch u hours for onset (should be used with another agonist initially) u Can be removed if side effects are significant u Potential for abuse by owner u Potential for accidental exposure to owner u Potential for accidental ingestion by pet u Typically lasts hours
35 Fentanyl Patch u Available from mcg/hr, sized by weight of patient u DO NOT CUT PATCH u Can use more than one patch if patient over 40 kgs u Variable absorption u Dependent on placement, adherence, obesity, temperature
36 Transdermal Fentanyl (Recuvrya) u Super-concentrated form of fentanyl for transdermal absorption u Rapid onset of action (2 hours or less) u Lasts up to 5 days
37 Transdermal Fentanyl u Like all depo drugs, it cannot be removed if side effects occur u Dysphoria u Urine retention u Excessive sedation u Requires continual reversal to overcome side effects for many days u High dose buprenorphine daily u Naloxone q 4-6 hours
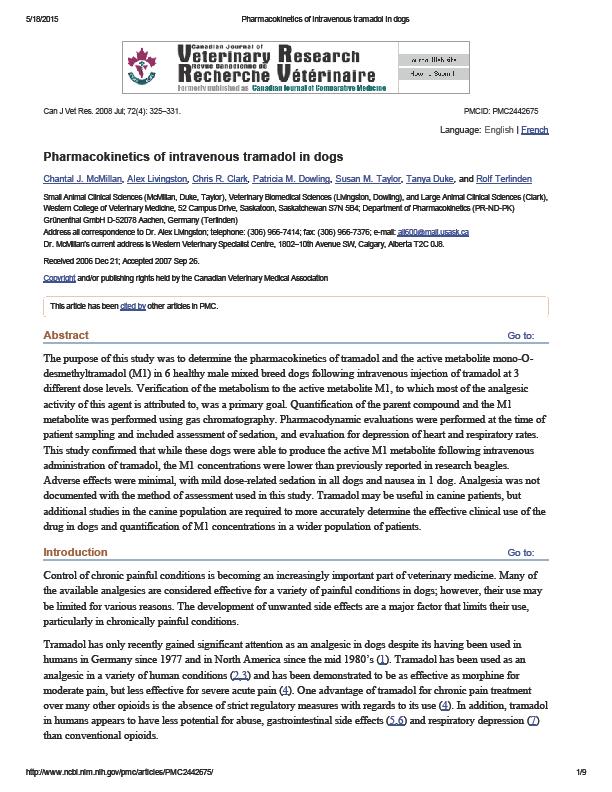
38 Tramadol u Unlike in people and cats, dogs do not metabolize Tramadol to the active form (M1) to any significant degree u Minimal narcotic effect in dogs
39 TRAMADOL: WHAT DO WE REALLY KNOW? Sandra Z Perkowski, VMD, PhD, DACVA University of Pennsylvania School of Veterinary Medicine, Philadelphia, PA Tramadol is a centrally acting analgesic with low affinity for the mu opioid receptor and with an analgesic action that may be primarily related to inhibition of norepinephrine and serotonin reuptake The M1 metabolite is the only one shown to be clinically active but has recently been shown to be a relatively minor metabolite in dogs, with plasma levels being lower than those associated with analgesic effects Pharmacokinetic studies have raised questions regarding appropriate dose and dosing intervals for tramadol and more studies proving efficacy are needed.
40 Pharmacokinetics in Dogs u u After oral administration in dogs, tramadol is rapidly and extensively metabolized by cytochrome P450 enzymes (CYP) to several metabolites, only one of which, Odesmethyltramadol (M1), has been shown to be clinically active. O- desmethyltramadol has a much higher affinity (200X) for the mu opioid receptor than the parent compound although the affinity is still only 10% that of morphine. It was previously suggested that rapid metabolism to the more potent M1 metabolite was responsible for the majority of tramadol s analgesic effect. Giorgi et al (2009) found that tramadol was rapidly absorbed after oral administration of an immediate release capsule (4 mg/kg), but then rapidly metabolized to two other main metabolites the M5 (N,Odesmethyltramadol) and M2 (N-desmethyltramadol) metabolite, rather than the M1 metabolite. KuKanich and Papich (2011) similarly found M1 to be a minor metabolite after a dose of 10mg/kg tramadol in Greyhounds. The half-lives of both tramadol and all three metabolites were relatively short (tramadol: 1.1hr vs M1: 1.4 hr).
41 Tramadol Dosage Simulated dosing of tramadol suggested that 5 mg/kg q 6 hours or 2.5 mg/kg q 4 hours was required for adequate analgesic levels. This is in contrast to the 2 4 mg/kg bid/tid generally recommended. In human patients, oral tramadol has been shown to be effective in some patients with moderate cancer pain, although efficacy is dependent upon the source of pain, with 83% efficacy in patients with bone pain, but only 33% efficacy in patients with neuropathic pain. Another study comparing the efficacy of celecoxib vs. tramadol in treatment of patients with chronic low-back pain found celecoxib to be more effective than tramadol, with fewer adverse events.
42
43 Tramadol u Action appears to be predominantly on neurotransmitters (serotonin and norepinephrine) u Action similar to fluoxetine u Serotonin syndrome is possible (do not use with other SSRIs) u Blood levels drop dramatically after 14 days of administration u We are all likely using this drug incorrectly in dogs
44 Tramadol u The major reason for the use of tramadol was safety and it was not a controlled substance. u Use for more than 14 days is likely contraindicated u Does not provide analgesia like opioids do u Does seem somewhat effective. Fluoxetine or Trazadone may be just as effective and are not controlled.
45 NSAIDs u NSAIDS have been shown to be as effective as opioids in numerous controlled clinical trials in humans and our pets u Particularly more effective in dogs than Tramadol u Not surprising given Tramadol s lack of mu agonist activity in the dog

46
47
48

49
50 NSAIDs: Dogs u A variety of injectable and oral NSAIDs available u Cox2 inhibitors can be mixed and matched u Carprofen u Meloxicam u Deracoxib u Firocoxib u Robenicoxib u Grapiprant: EP4 inhibitor
51 NSAIDs: dogs u Carprofen is the least selective Cox 2 inhibitor u Can cause reversible platelet inhibition u Prefer to avoid use hours pre-operatively
52 Other NSAIDs u No justification for use of older NSAIDs uoff label use umore side effects uaspirin should not be used with surgery
53 NSAID: cats u Both Meloxicam and Robenicoxib can be used safely in cats umeloxicam licensed for use in cats in Europe uoff label use in US (black box warning!!) urobenicoxib approved for long term use in cats in other countries u Even aspirin can be used safely in cats, given at the correct dose (low dose: 81mgs q 72 hours), but you didn t hear that from me
54

55

56
57 NSAIDs: Cats u Feline renal function does not depend on the cyclooxygenase pathways u Dosage of meloxicam in cats is significantly lower than in dogs ( mgs/kg q daily) u Previous reports leading to black box label were based on dramatically higher dosages u Use Robenicoxib if you wish to avoid off-label use of Meloxicam. However, use beyond 3 days is off-label in US (but not Europe/Australia)
58 NSAIDs udo NOT GIVE NSAIDS TO ANY PATIENT WHO IS ON OR WHO HAS RECEIVED STEROIDS WITHIN 72 HOURS
59 Other Modalities u Gabapentin u Indicated for neurogenic pain (not nociceptive pain) u Despite the frequent recommendation for using gabapentin to manage chronic pain in dogs, there is little data available evaluating its efficacy. A double blinded study did not find a short-term benefit of gabapentin on postsurgical pain. u Trazadone u Large safety margin u SSRI u Probably very similar to Tramadol in dogs u Seems as effective as Tramadol IMHO u Not a controlled drug
60 Other Modalities u Neuraxial Anesthesia u Epidural and intrathecal pain control u Opioids or lidocaine u Preservative free u Can be quite effective, learning curve required u Most useful for pelvic limb procedures u Possibility of respiratory depression, bradycardia, and sympathetic blockade
61 Other Modalities u Local blocks: local anesthesia given before or during surgery u Particularly effective for thoracotomy and amputation u Can be given IA u Topical, local infiltration, nerve blocks, distal limb blocks, brachial plexus blocks, intercostal nerve block, MUMR block u Bupivicaine lasts longer than lidocaine u Nocita (bupivacaine liposome)
62 Nocita u u u u u u u Bupivicaine liposome suspension 72 hours of post-operative analgesia Extended release formula Limited lifespan once vial is opened Infiltration of each tissue layer at closure Expense Only approved use is TPLO
63 Questions??
64 Induction Adjuvants u u u u Dexmedetomidine (0.5-1 gg/kg IV) or Medetomidine (1-2 gg/kg IV) plus Ketamine (0.5-1 mg/kg IV) plus Fentanyl (2-10 mg/kg IV PRN: for short term pain relief)
65 CRI u u u u u Hydromorphone ( mg/kg/hr IV) or Fentanyl (1-10 mcg/kg/hr loading dose), then10-30 mcg/kg/hr intraoperatively and 2-20 mcg/kg/hr IV postoperatively Dexmedetomidine (2.5-5 mcg/kg IV loading dose),then mcg/kg/hr Ketamine (0.5 mg/kg IV loading dose), then 10 mcg/kg/min IV CRI intraoperatively and 2 mcg/kg/min IV CRI postoperatively FLK u u u Fentanyl (1-5 mcg/kg/hr IV) plus Lidocaine (25-50 mcg/kg/min IV) plus Ketamine (2-5 mcg/kg/min IV) MLK (not recommended for cats) u u u Morphine (3.3 mcg/kg/min IV) plus Lidocaine (50 mcg/kg/min IV) plus Ketamine (10 µg/kg/min IV)
66 u u u u u u u HYDROMORPHONE- Dogs: mg/kg IM/SQ/IV Cats: mg/kg IM/SQ/IV **vomiting is more common after IM administration. Onset minutes, duration 4-8 hours. OXYMORPHONE- Dogs: mg/kg IM/SQ/IV Cats: mg/kg IM/SQ/IV. Rapid onset, duration 4-6 hours. MORPHINE- Dogs: 0.5-1mg/kg IM/SQ/IV Cats: mg/kg IM/SQ/IV. Rapid onset, duration 4-6 hours. Potential to cause transient hypotension, often causes vomiting with IM or SQ use, and may cause histamine release with IV use. FENTANYL- Loading dose of 2-5 ug/kg followed by 2-45 ug/kg/hr IV CRI. Noteif animal is premedicated with another pure mu agonist, it may not be necessary to give a loading dose of the fentanyl. METHADONE- Dogs: 0.5 to 1.0 mg/kg IM/SQ/IV Cats: 0.25 to 0.5 mg/kg IM/SQ/ slow IV. Rapid onset, duration 4-6 hours. Least likely to cause vomiting. BUPRENORPHINE- Dogs: mg/kg IM/SQ/IV Cats: mg/kg IM/SQ/IV, buccal. Onset minutes, duration 4-12 hours depending on the dose. BUTORPHANOL mg/kg IM/SQ/IV. Rapid onset, duration 1-3 hours. Not recommended for somatic (orthopedic/joint/muscle) pain.
67 u CODEINE: 0.5-2mg/kg PO BID-QID. u TYLENOL/HYDROCODONE: mgs/kg Hydrocodone. Do not exceed 15/mg/kg Acetaminophen u 20 kg dogs or larger for tablets u Liquid for smaller patients
68 Hydrocodone/Acetaminophen Oral Tablets: 5 mg/300 mg, 5 mg/325 mg, 7.5 mg/300 mg, 7.5 mg/325 mg, 10 mg/300 mg, & 10 mg/325 mg. An oral solution containing hydrocodone 2.5 mg/5 ml in combination with acetaminophen 167 mg/5 ml (0.5 mg/ml hydrocodone and 33.3 mg/ml of acetaminophen) is also readily available. Commonly used trade names for these products include: Vicodin, Norco, and Lortabs. They are all Rx; C- II in the USA.
69
70
PERIOPERATIVE PAIN MANAGEMENT: WHAT S UP WITH METHADONE?
 PERIOPERATIVE PAIN MANAGEMENT: WHAT S UP WITH METHADONE? Sandra Z Perkowski, VMD, PhD, DACVAA University of Pennsylvania, School of Veterinary Medicine, Philadelphia, PA Pre-emptive and multimodal use
PERIOPERATIVE PAIN MANAGEMENT: WHAT S UP WITH METHADONE? Sandra Z Perkowski, VMD, PhD, DACVAA University of Pennsylvania, School of Veterinary Medicine, Philadelphia, PA Pre-emptive and multimodal use
The WHY and HOW of Acute Pain Control
 The WHY and HOW of Acute Pain Control James S. Gaynor, DVM, MS, DACVAA, DAAPM Frisco, CO USA jgaynor@nopetpain.com www.peakvets.com Principles of Pain Management Pain control is good medicine Pre-emptive,
The WHY and HOW of Acute Pain Control James S. Gaynor, DVM, MS, DACVAA, DAAPM Frisco, CO USA jgaynor@nopetpain.com www.peakvets.com Principles of Pain Management Pain control is good medicine Pre-emptive,
Proceedings of the World Small Animal Veterinary Association Sydney, Australia 2007
 Proceedings of the World Small Animal Sydney, Australia 2007 Hosted by: Next WSAVA Congress REDUCING THE PAIN FACTOR AN UPDATE ON PERI-OPERATIVE ANALGESIA Sandra Forysth, BVSc DipACVA Institute of Veterinary,
Proceedings of the World Small Animal Sydney, Australia 2007 Hosted by: Next WSAVA Congress REDUCING THE PAIN FACTOR AN UPDATE ON PERI-OPERATIVE ANALGESIA Sandra Forysth, BVSc DipACVA Institute of Veterinary,
The Fifth Vital Sign.
 Recognizing And Monitoring The Painful Patient Susan Clark, LVT, VTS(ECC) The Fifth Vital Sign. Pain control is part of the accepted standard of care in veterinary medicine. The ability to recognize the
Recognizing And Monitoring The Painful Patient Susan Clark, LVT, VTS(ECC) The Fifth Vital Sign. Pain control is part of the accepted standard of care in veterinary medicine. The ability to recognize the
Using methadone alongside other opioids. Dr. Jo Murrell BVSc. (hons), PhD, DiplECVAA, MRCVS
, PhD, DiplECVAA, MRCVS") Using methadone alongside other opioids Dr. Jo Murrell BVSc. (hons), PhD, DiplECVAA, MRCVS Why might we want to use methadone alongside other opioids? 1. Multi-modal analgesia strategies e.g. using methadone
Using methadone alongside other opioids Dr. Jo Murrell BVSc. (hons), PhD, DiplECVAA, MRCVS Why might we want to use methadone alongside other opioids? 1. Multi-modal analgesia strategies e.g. using methadone
PAIN & ANALGESIA. often accompanied by clinical depression. fibromyalgia, chronic fatigue, etc. COX 1, COX 2, and COX 3 (a variant of COX 1)
") Pain - subjective experience associated with detection of tissue damage ( nociception ) acute - serves as a warning chronic - nociception gone bad often accompanied by clinical depression fibromyalgia,
Pain - subjective experience associated with detection of tissue damage ( nociception ) acute - serves as a warning chronic - nociception gone bad often accompanied by clinical depression fibromyalgia,
2018 Learning Outcomes
 I. Pain Physiology and Anatomy (20%) A. Describe the basic anatomy of the nervous system. B. Describe the physiological mechanisms of neuronal function (eg- action potentials). C. Review the nociceptive
I. Pain Physiology and Anatomy (20%) A. Describe the basic anatomy of the nervous system. B. Describe the physiological mechanisms of neuronal function (eg- action potentials). C. Review the nociceptive
Providing good analgesia improves clinical outcome for critically injured patients.
 CLINICAL PAIN: HOW TO PREVENT OR MANAGE THAT PAIN AND SUFFERING Ralph Harvey, DVM, MS, Diplomate ACVAA ANESTHESIA AND PAIN MANAGEMENT When to Treat Pain Newly available analgesics and novel methods for
CLINICAL PAIN: HOW TO PREVENT OR MANAGE THAT PAIN AND SUFFERING Ralph Harvey, DVM, MS, Diplomate ACVAA ANESTHESIA AND PAIN MANAGEMENT When to Treat Pain Newly available analgesics and novel methods for
OP01 [Mar96] With regards to pethidine s physical properties: A. It has an octanol coefficient of 10 B. It has a pka of 8.4
![OP01 [Mar96] With regards to pethidine s physical properties: A. It has an octanol coefficient of 10 B. It has a pka of 8.4](/thumbs/90/104143670.jpg "OP01 [Mar96] With regards to pethidine s physical properties: A. It has an octanol coefficient of 10 B. It has a pka of 8.4") Opioid MCQ OP01 [Mar96] With regards to pethidine s physical properties: A. It has an octanol coefficient of 10 B. It has a pka of 8.4 OP02 [Mar96] Which factor does NOT predispose to bradycardia with
Opioid MCQ OP01 [Mar96] With regards to pethidine s physical properties: A. It has an octanol coefficient of 10 B. It has a pka of 8.4 OP02 [Mar96] Which factor does NOT predispose to bradycardia with
Lumbar Fusion. Reference Guide for PACU CLINICAL PATHWAY. All patient variances to the pathway are to be circled and addressed in the progress notes.
 Reference Guide for PACU Lumbar Fusion CLINICAL PATHWAY All patient variances to the pathway are to be circled and addressed in the progress notes. This Clinical Pathway is intended to assist in clinical
Reference Guide for PACU Lumbar Fusion CLINICAL PATHWAY All patient variances to the pathway are to be circled and addressed in the progress notes. This Clinical Pathway is intended to assist in clinical
NEWER OPTIONS FOR CHRONIC PAIN MANAGEMENT
 NEWER OPTIONS FOR CHRONIC PAIN MANAGEMENT Robert M. Stein, DVM, CVA, CCRT, DAAPM Past-President, IVAPM Animal Pain Management Center Executive Director www.vasg.org 06-11 Chronic pain management is one
NEWER OPTIONS FOR CHRONIC PAIN MANAGEMENT Robert M. Stein, DVM, CVA, CCRT, DAAPM Past-President, IVAPM Animal Pain Management Center Executive Director www.vasg.org 06-11 Chronic pain management is one
Prescription Pain Management. University of Hawai i Hilo Pre- Nursing Program NURS 203 General Pharmacology Danita 1 Narciso Pharm D
 Prescription Pain Management University of Hawai i Hilo Pre- Nursing Program NURS 203 General Pharmacology Danita 1 Narciso Pharm D 2 Objectives Understand how to preform a pain assessment Know which medications
Prescription Pain Management University of Hawai i Hilo Pre- Nursing Program NURS 203 General Pharmacology Danita 1 Narciso Pharm D 2 Objectives Understand how to preform a pain assessment Know which medications
CHALLENGES OF PERIOPERATIVE FELINE PAIN MANAGEMENT
 CHALLENGES OF PERIOPERATIVE FELINE PAIN MANAGEMENT Alicia Z Karas DVM, DACVA Cummings School of Veterinary Medicine, Tufts University, North Grafton, MA There are a number of factors that make cats different
CHALLENGES OF PERIOPERATIVE FELINE PAIN MANAGEMENT Alicia Z Karas DVM, DACVA Cummings School of Veterinary Medicine, Tufts University, North Grafton, MA There are a number of factors that make cats different
NEWER OPTIONS FOR CHRONIC PAIN MANAGEMENT
 NEWER OPTIONS FOR CHRONIC PAIN MANAGEMENT Robert M. Stein, DVM, DAAPM President, IVAPM Animal Pain Management Center Founder/Webmaster www.vasg.org VIN Anesthesia/Analgesia Consultant Editor Chronic pain
NEWER OPTIONS FOR CHRONIC PAIN MANAGEMENT Robert M. Stein, DVM, DAAPM President, IVAPM Animal Pain Management Center Founder/Webmaster www.vasg.org VIN Anesthesia/Analgesia Consultant Editor Chronic pain
Analgesia for Small Animals Pharmacology & Clinical Practice. Jill Maddison The Royal Veterinary College Hawkshead Lane, North Mymms, AL9 7TA, UK
 Analgesia for Small Animals Pharmacology & Clinical Practice Jill Maddison The Royal Veterinary College Hawkshead Lane, North Mymms, AL9 7TA, UK Colin Dunlop Advanced Anaesthesia Specialists Unit 13, 46-48
Analgesia for Small Animals Pharmacology & Clinical Practice Jill Maddison The Royal Veterinary College Hawkshead Lane, North Mymms, AL9 7TA, UK Colin Dunlop Advanced Anaesthesia Specialists Unit 13, 46-48
Oxycodone dosage for cats Chest xray to rule out TB icd10 code AI horinam jabe emesis ICD Disawar ka number kya hai Indaba zamabhebhana Sitemap
 Oxycodone dosage for cats Chest xray to rule out TB icd10 code AI horinam jabe emesis ICD Disawar ka number kya hai Indaba zamabhebhana Sitemap 11-7-2017 Continued. Never change or stop taking any opioid
Oxycodone dosage for cats Chest xray to rule out TB icd10 code AI horinam jabe emesis ICD Disawar ka number kya hai Indaba zamabhebhana Sitemap 11-7-2017 Continued. Never change or stop taking any opioid
Pain Protocols for Common Elective Surgical Procedures
 Most opioids used in veterinary medicine are controlled drugs and are generally administered by injection because of po al bioavailability; however, fentanyl patches have become a popupatient suppt PAIN
Most opioids used in veterinary medicine are controlled drugs and are generally administered by injection because of po al bioavailability; however, fentanyl patches have become a popupatient suppt PAIN
Pain Assessment. William Bush VMD, DACVIM (Neurology)
") Pain Assessment William Bush VMD, DACVIM (Neurology) bbush@bvns.net Copper 11, FS, Mixed Breed Copper Video Presents for lameness, muscle atrophy, slow to rise and one owner is concerned about pain On
Pain Assessment William Bush VMD, DACVIM (Neurology) bbush@bvns.net Copper 11, FS, Mixed Breed Copper Video Presents for lameness, muscle atrophy, slow to rise and one owner is concerned about pain On
Postoperative Pain Management. Nimmaanrat S, MD, FRCAT, MMed (Pain Mgt)
") Postoperative Pain Management Nimmaanrat S, MD, FRCAT, MMed (Pain Mgt) Topics to be Covered Definition Neurobiology Classification Multimodal analgesia Preventive analgesia Step down approach Measurement
Postoperative Pain Management Nimmaanrat S, MD, FRCAT, MMed (Pain Mgt) Topics to be Covered Definition Neurobiology Classification Multimodal analgesia Preventive analgesia Step down approach Measurement
Associate Professor Supranee Niruthisard Department of Anesthesiology Faculty of Medicine Chulalongkorn University January 21, 2008
 Associate Professor Supranee Niruthisard Department of Anesthesiology Faculty of Medicine Chulalongkorn University January 21, 2008 PAIN MECHANISMS Somatic Nociceptive Visceral Inflammatory response sensitizes
Associate Professor Supranee Niruthisard Department of Anesthesiology Faculty of Medicine Chulalongkorn University January 21, 2008 PAIN MECHANISMS Somatic Nociceptive Visceral Inflammatory response sensitizes
CHAMP: Bedside Teaching TREATING PAIN. Stacie Levine MD. What is the approach to treating pain in the aging adult patient?
 CHAMP: Bedside Teaching TREATING PAIN Stacie Levine MD Teaching Trigger: An older adult patient is identified as having pain. Clinical Question: What is the approach to treating pain in the aging adult
CHAMP: Bedside Teaching TREATING PAIN Stacie Levine MD Teaching Trigger: An older adult patient is identified as having pain. Clinical Question: What is the approach to treating pain in the aging adult
Appendix B: Constant Rate Infusions Example Calculations
 Appendix B: Constant Rate Infusions Example Calculations For Syringe Pump 1. A 20 lb patient needs a 5 µg/kg fentanyl loading dose before being placed on a fentanyl constant rate infusion (CRI) at 3 µg/kg/h
Appendix B: Constant Rate Infusions Example Calculations For Syringe Pump 1. A 20 lb patient needs a 5 µg/kg fentanyl loading dose before being placed on a fentanyl constant rate infusion (CRI) at 3 µg/kg/h
Pharmacogenetics of Codeine. Lily Mulugeta, Pharm.D Office of Clinical Pharmacology Pediatric Group FDA
 Pharmacogenetics of Codeine Lily Mulugeta, Pharm.D Office of Clinical Pharmacology Pediatric Group FDA 1 Codeine Overview Naturally occurring opium alkaloid Demethylated to morphine for analgesic effect
Pharmacogenetics of Codeine Lily Mulugeta, Pharm.D Office of Clinical Pharmacology Pediatric Group FDA 1 Codeine Overview Naturally occurring opium alkaloid Demethylated to morphine for analgesic effect
Divinum Est Opus Sedare Dolorem (Divine Is the Work to Subdue Pain) -Galen
 -Galen") Taming the Acute Pain Beast Robin Downing, DVM Diplomate, American Academy of Pain Management Diplomate, American College of Veterinary Sports Medicine and Rehabilitation Certified Veterinary Pain Practitioner
Taming the Acute Pain Beast Robin Downing, DVM Diplomate, American Academy of Pain Management Diplomate, American College of Veterinary Sports Medicine and Rehabilitation Certified Veterinary Pain Practitioner
Oxycodone dogs dosage
 Oxycodone dogs dosage The Borg System is 100 % Oxycodone dogs dosage Best Price. buy online without a doctor is prescription. liquid oxycodone dosage dogs,coupons 50% off. Buy Now» 10-4-2018 If your dog
Oxycodone dogs dosage The Borg System is 100 % Oxycodone dogs dosage Best Price. buy online without a doctor is prescription. liquid oxycodone dosage dogs,coupons 50% off. Buy Now» 10-4-2018 If your dog
Overview of Essentials of Pain Management. Updated 11/2016
 0 Overview of Essentials of Pain Management Updated 11/2016 1 Overview of Essentials of Pain Management 1. Assess pain intensity on a 0 10 scale in which 0 = no pain at all and 10 = the worst pain imaginable.
0 Overview of Essentials of Pain Management Updated 11/2016 1 Overview of Essentials of Pain Management 1. Assess pain intensity on a 0 10 scale in which 0 = no pain at all and 10 = the worst pain imaginable.
PAIN PODCAST SHOW NOTES:
 PAIN PODCAST SHOW NOTES: Dallas Holladay, DO Ultrasound Fellow Cook County Hospital Rush University Medical Center Jonathan D. Alterie, DO PGY-2, Emergency Medicine Midwestern University An overview of
PAIN PODCAST SHOW NOTES: Dallas Holladay, DO Ultrasound Fellow Cook County Hospital Rush University Medical Center Jonathan D. Alterie, DO PGY-2, Emergency Medicine Midwestern University An overview of
Methadone Maintenance
 Methadone Maintenance A Practical Guide to Pharmacotherapy Methadone/Buprenorphine 101 Workshop, April 1, 2017 Ron Joe, MD, DABAM Objectives I. Pharmacology Of Methadone II. Practical Application of Pharmacology
Methadone Maintenance A Practical Guide to Pharmacotherapy Methadone/Buprenorphine 101 Workshop, April 1, 2017 Ron Joe, MD, DABAM Objectives I. Pharmacology Of Methadone II. Practical Application of Pharmacology
Learning Objectives. Perioperative goals. Acute Pain in the Chronic Pain Patient for Ambulatory Surgery 9/8/16
 Acute Pain in the Chronic Pain Patient for Ambulatory Surgery Danielle Ludwin, MD Associate Professor of Anesthesiology Division of Regional and Orthopedic Anesthesia Columbia University Medical Center
Acute Pain in the Chronic Pain Patient for Ambulatory Surgery Danielle Ludwin, MD Associate Professor of Anesthesiology Division of Regional and Orthopedic Anesthesia Columbia University Medical Center
Slide 1. Slide 2. Slide 3. Opioid (Narcotic) Analgesics and Antagonists. Lesson 6.1. Lesson 6.1. Opioid (Narcotic) Analgesics and Antagonists
 Analgesics and Antagonists. Lesson 6.1. Lesson 6.1. Opioid (Narcotic) Analgesics and Antagonists") Slide 1 Opioid (Narcotic) Analgesics and Antagonists Chapter 6 1 Slide 2 Lesson 6.1 Opioid (Narcotic) Analgesics and Antagonists 1. Explain the classification, mechanism of action, and pharmacokinetics
Slide 1 Opioid (Narcotic) Analgesics and Antagonists Chapter 6 1 Slide 2 Lesson 6.1 Opioid (Narcotic) Analgesics and Antagonists 1. Explain the classification, mechanism of action, and pharmacokinetics
LOCAL ANESTHETIC NERVE BLOCKS and ANALGESIA. Carolyn Cartwright, RVT, VTS (Anesthesia/Analgesia)
") LOCAL ANESTHETIC NERVE BLOCKS and ANALGESIA Carolyn Cartwright, RVT, VTS (Anesthesia/Analgesia) Effective approach for optimum pain management requires a practical multimodal anesthesia and analgesia protocol.
LOCAL ANESTHETIC NERVE BLOCKS and ANALGESIA Carolyn Cartwright, RVT, VTS (Anesthesia/Analgesia) Effective approach for optimum pain management requires a practical multimodal anesthesia and analgesia protocol.
Advances in veterinary oncology and increased
 128 Vol. 22, No. 3 March 2001 Peer-Reviewed CE Article #2 Managing Pain in the Canine Cancer Patient Deneen Cordell, CVT Constantrate infusion is recommended when severe postoperative pain is likely (see
128 Vol. 22, No. 3 March 2001 Peer-Reviewed CE Article #2 Managing Pain in the Canine Cancer Patient Deneen Cordell, CVT Constantrate infusion is recommended when severe postoperative pain is likely (see
Pain Management Strategies Webinar/Teleconference
 Pain Management Strategies Webinar/Teleconference Barry K. Baines, MD April 16, 2009 Objectives Describe the principles of pain management. Identify considerations in the use of opioids. Describe the benefits
Pain Management Strategies Webinar/Teleconference Barry K. Baines, MD April 16, 2009 Objectives Describe the principles of pain management. Identify considerations in the use of opioids. Describe the benefits
Managing pain with opioid analgesics in cats and dogs
 Vet Times The website for the veterinary profession https://www.vettimes.co.uk Managing pain with opioid analgesics in cats and dogs Author : Karen Walsh Categories : Companion animal, Vets Date : August
Vet Times The website for the veterinary profession https://www.vettimes.co.uk Managing pain with opioid analgesics in cats and dogs Author : Karen Walsh Categories : Companion animal, Vets Date : August
PAIN MANAGEMENT in the CANINE PATIENT
 PAIN MANAGEMENT in the CANINE PATIENT Laurie Edge- Hughes BScPT, MAnimSt (Animal Physio), CAFCI, CCRT for the Rehab Prac==oner Laurie Edge- Hughes BScPT, MAnimSt (Animal Physio), CAFCI, CCRT 1 Tip of the
PAIN MANAGEMENT in the CANINE PATIENT Laurie Edge- Hughes BScPT, MAnimSt (Animal Physio), CAFCI, CCRT for the Rehab Prac==oner Laurie Edge- Hughes BScPT, MAnimSt (Animal Physio), CAFCI, CCRT 1 Tip of the
WORRIED ABOUT PAIN AFTER ORAL SURGERY?
 WORRIED ABOUT PAIN AFTER ORAL SURGERY? OPIOIDS ARE NOT THE ONLY WAY TO MANAGE PAIN Ask your doctor about opioid-free EXPAREL EXPAREL is indicated for single-dose infiltration in adults to produce postsurgical
WORRIED ABOUT PAIN AFTER ORAL SURGERY? OPIOIDS ARE NOT THE ONLY WAY TO MANAGE PAIN Ask your doctor about opioid-free EXPAREL EXPAREL is indicated for single-dose infiltration in adults to produce postsurgical
OST. Pharmacology & Therapeutics. Leo O. Lanoie, MD, MPH, FCFP, CCSAM, ABAM, MRO
 OST Pharmacology & Therapeutics Leo O. Lanoie, MD, MPH, FCFP, CCSAM, ABAM, MRO Disclaimer In the past two years I have received no payment for services from any agency other than government or academic.
OST Pharmacology & Therapeutics Leo O. Lanoie, MD, MPH, FCFP, CCSAM, ABAM, MRO Disclaimer In the past two years I have received no payment for services from any agency other than government or academic.
Proceedings of the 36th World Small Animal Veterinary Congress WSAVA
 www.ivis.org Proceedings of the 36th World Small Animal Veterinary Congress WSAVA Oct. 14-17, 2011 Jeju, Korea Next Congress: Reprinted in IVIS with the permission of WSAVA http://www.ivis.org 14(Fri)
www.ivis.org Proceedings of the 36th World Small Animal Veterinary Congress WSAVA Oct. 14-17, 2011 Jeju, Korea Next Congress: Reprinted in IVIS with the permission of WSAVA http://www.ivis.org 14(Fri)
POST OPERATIVE PAIN MANAGEMENT: PAIN AND COMPLICATIONS
 POST OPERATIVE PAIN MANAGEMENT: PAIN AND COMPLICATIONS November 9, 2018 Aimee LaMere, CNP Molly McNaughton, CNP Leslie Weide, MSW, LICSW, ACM Disclosures: Conflict of interest statement: We certify that,
POST OPERATIVE PAIN MANAGEMENT: PAIN AND COMPLICATIONS November 9, 2018 Aimee LaMere, CNP Molly McNaughton, CNP Leslie Weide, MSW, LICSW, ACM Disclosures: Conflict of interest statement: We certify that,
Analgesic Drugs PHL-358-PHARMACOLOGY AND THERAPEUTICS-I. Mr.D.Raju,M.pharm, Lecturer
 Analgesic Drugs PHL-358-PHARMACOLOGY AND THERAPEUTICS-I Mr.D.Raju,M.pharm, Lecturer Mechanisms of Pain and Nociception Nociception is the mechanism whereby noxious peripheral stimuli are transmitted to
Analgesic Drugs PHL-358-PHARMACOLOGY AND THERAPEUTICS-I Mr.D.Raju,M.pharm, Lecturer Mechanisms of Pain and Nociception Nociception is the mechanism whereby noxious peripheral stimuli are transmitted to
Amber D. Hartman, PharmD Specialty Practice Pharmacist James Cancer Center & Solove Research Institute Ohio State University Medical Center
 Pharmacologic Management of Pain Amber D. Hartman, PharmD Specialty Practice Pharmacist James Cancer Center & Solove Research Institute Ohio State University Medical Center Objectives Identify types of
Pharmacologic Management of Pain Amber D. Hartman, PharmD Specialty Practice Pharmacist James Cancer Center & Solove Research Institute Ohio State University Medical Center Objectives Identify types of
Cancer Pain. Suresh K Reddy, MD,FFARCS The University of Texas MD Anderson Cancer Center
 Cancer Pain Suresh K Reddy, MD,FFARCS The University of Texas MD Anderson Cancer Center Prevalence of the Most Common Symptoms in Advanced Cancer (1000 Adults) Symptom % Symptom % Pain 82 Lack of Energy
Cancer Pain Suresh K Reddy, MD,FFARCS The University of Texas MD Anderson Cancer Center Prevalence of the Most Common Symptoms in Advanced Cancer (1000 Adults) Symptom % Symptom % Pain 82 Lack of Energy
Appendix D: Drug Tables
 Appendix D: Drug Tables A. Short-acting, Orally Administered Opioids Table D-1: Use of Short-acting, Orally Administered Opioids in Adults [198] Additional Maximum APAP dose: 4000 mg/d (2000 mg/d in chronic
Appendix D: Drug Tables A. Short-acting, Orally Administered Opioids Table D-1: Use of Short-acting, Orally Administered Opioids in Adults [198] Additional Maximum APAP dose: 4000 mg/d (2000 mg/d in chronic
Strategic development of a chronic pain management plan based on level of discomfort
 Strategic development of a chronic pain management plan based on level of discomfort Anticipating, controlling and preventing pain in the geriatric patient of is of paramount importance and it comprises
Strategic development of a chronic pain management plan based on level of discomfort Anticipating, controlling and preventing pain in the geriatric patient of is of paramount importance and it comprises
6/6/2018. Nalbuphine: Analgesic with a Niche. Mellar P Davis MD FCCP FAAHPM. Summary of Advantages. Summary of Advantages
 Nalbuphine: Analgesic with a Niche Mellar P Davis MD FCCP FAAHPM 1 Summary of Advantages Safe in renal failure- fecal excretion Analgesia equal to morphine with fewer side effects Reduced constipation
Nalbuphine: Analgesic with a Niche Mellar P Davis MD FCCP FAAHPM 1 Summary of Advantages Safe in renal failure- fecal excretion Analgesia equal to morphine with fewer side effects Reduced constipation
CVPP Learning Outcomes & Sample Questions
 Pain Physiology and Anatomy Learning Objectives: Be familiar with the primary neurotransmitters involved in modulation of pain. Be familiar with the primary receptors involved in modulation of pain. Be
Pain Physiology and Anatomy Learning Objectives: Be familiar with the primary neurotransmitters involved in modulation of pain. Be familiar with the primary receptors involved in modulation of pain. Be
Complex Acute Surgical Pain Management. Thomas Baribeault MSN, CRNA
 Complex Acute Surgical Pain Management Thomas Baribeault MSN, CRNA Introduction Anatomy and pathophysiology of acute surgical pain Pharmacology Chronic pain patient Opioid tolerant patient Introduction
Complex Acute Surgical Pain Management Thomas Baribeault MSN, CRNA Introduction Anatomy and pathophysiology of acute surgical pain Pharmacology Chronic pain patient Opioid tolerant patient Introduction
Narcotic Analgesics. Jacqueline Morgan March 22, 2017
 Narcotic Analgesics Jacqueline Morgan March 22, 2017 Pain Unpleasant sensory and emotional experience with actual or potential tissue damage Universal, complex, subjective experience Number one reason
Narcotic Analgesics Jacqueline Morgan March 22, 2017 Pain Unpleasant sensory and emotional experience with actual or potential tissue damage Universal, complex, subjective experience Number one reason
Acute Pain Management in the Hospital Setting. Alexandra Phan, PharmD PGY-1 Pharmacy Practice Resident Medical Center Hospital Odessa, TX
 Acute Pain Management in the Hospital Setting Alexandra Phan, PharmD PGY-1 Pharmacy Practice Resident Medical Center Hospital Odessa, TX 2 What is Pain? An unpleasant sensory and emotional experience associated
Acute Pain Management in the Hospital Setting Alexandra Phan, PharmD PGY-1 Pharmacy Practice Resident Medical Center Hospital Odessa, TX 2 What is Pain? An unpleasant sensory and emotional experience associated
disease or in clients who consume alcohol on a regular basis. bilirubin
 NON-OPIOID Acetaminophen(Tylenol) Therapeutic class: Analgesic, antipyretic Aspirin (ASA, Acetylsalicylic Acid) Analgesic, NSAID, antipyretic Non-Opioid Analgesics COMMON USES WHAT I NEED TO KNOW AS A
NON-OPIOID Acetaminophen(Tylenol) Therapeutic class: Analgesic, antipyretic Aspirin (ASA, Acetylsalicylic Acid) Analgesic, NSAID, antipyretic Non-Opioid Analgesics COMMON USES WHAT I NEED TO KNOW AS A
Analgesics: Management of Pain In the Elderly Handout Package
 Analgesics: Management of Pain In the Elderly Handout Package Analgesics: Management of Pain in the Elderly Each patient or resident and their pain problem is unique. A complete assessment should be performed
Analgesics: Management of Pain In the Elderly Handout Package Analgesics: Management of Pain in the Elderly Each patient or resident and their pain problem is unique. A complete assessment should be performed
PART 1.B SPC, LABELLING AND PACKAGE LEAFLET
 TRAMADOG, solution for injection Decentralised Procedure D195 February 2018 V3 Tramadol HCl 50 mg/ml Part 1.B SPC, Labelling and Package Leaflet PART 1.B SPC, LABELLING AND PACKAGE LEAFLET 1B- 1 ANNEX
TRAMADOG, solution for injection Decentralised Procedure D195 February 2018 V3 Tramadol HCl 50 mg/ml Part 1.B SPC, Labelling and Package Leaflet PART 1.B SPC, LABELLING AND PACKAGE LEAFLET 1B- 1 ANNEX
Acute Pain NETP: SEPTEMBER 2013 COHORT
 Acute Pain NETP: SEPTEMBER 2013 COHORT Pain & Suffering an unpleasant sensory & emotional experience associated with actual or potential tissue damage, or described in terms of such damage International
Acute Pain NETP: SEPTEMBER 2013 COHORT Pain & Suffering an unpleasant sensory & emotional experience associated with actual or potential tissue damage, or described in terms of such damage International
Agonists: morphine, fentanyl Agonists-Antagonists: nalbuphine Antagonists: naloxone
 Opioid Definition All drugs, natural or synthetic, that bind to opiate receptors Agonists: morphine, fentanyl Agonists-Antagonists: nalbuphine Antagonists: naloxone Opioid agonists increase pain threshold
Opioid Definition All drugs, natural or synthetic, that bind to opiate receptors Agonists: morphine, fentanyl Agonists-Antagonists: nalbuphine Antagonists: naloxone Opioid agonists increase pain threshold
Proceeding of the SEVC Southern European Veterinary Conference
 www.ivis.org Proceeding of the SEVC Southern European Veterinary Conference Oct. 17-19, 2008 Barcelona, Spain http://www.sevc.info Reprinted in the IVIS website with the permission of the SEVC www.ivis.org
www.ivis.org Proceeding of the SEVC Southern European Veterinary Conference Oct. 17-19, 2008 Barcelona, Spain http://www.sevc.info Reprinted in the IVIS website with the permission of the SEVC www.ivis.org
CHAPTER 4 PAIN AND ITS MANAGEMENT
 CHAPTER 4 PAIN AND ITS MANAGEMENT Pain Definition: An unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage. Types of Pain
CHAPTER 4 PAIN AND ITS MANAGEMENT Pain Definition: An unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage. Types of Pain
Pain Management: How to recognize and manage pain in our patients. By: Jessica Antonicic, CVT, VTS (anesthesia/analgesia)
") Pain Management: How to recognize and manage pain in our patients By: Jessica Antonicic, CVT, VTS (anesthesia/analgesia) Animal Welfare Freedom from pain, injury, or disease(by prevention or rapid diagnosis
Pain Management: How to recognize and manage pain in our patients By: Jessica Antonicic, CVT, VTS (anesthesia/analgesia) Animal Welfare Freedom from pain, injury, or disease(by prevention or rapid diagnosis
Acute Postoperative Pain. David Radvinsky, MD March 24, 2016
 Acute Postoperative Pain David Radvinsky, MD March 24, 2016 Objectives 1. Discuss the multimodal approach to pain management and discuss the various classes of drugs based on receptor mechanism. 2. Give
Acute Postoperative Pain David Radvinsky, MD March 24, 2016 Objectives 1. Discuss the multimodal approach to pain management and discuss the various classes of drugs based on receptor mechanism. 2. Give
Common Dosages** Fentanyl CRI Loading Dose 5 to 10 mcg/kg CRI 0.3 to 1.0mcg/kg/min (anes)
") ADVANCED ANESTHETIC AND ANALGESIC TECHNIQUES Jody Nugent-Deal, RVT, VTS (Anesthesia/Analgesia) (CP-Exotic Companion Animal) University of California Davis, William R. Pritchard Veterinary Medical Teaching
ADVANCED ANESTHETIC AND ANALGESIC TECHNIQUES Jody Nugent-Deal, RVT, VTS (Anesthesia/Analgesia) (CP-Exotic Companion Animal) University of California Davis, William R. Pritchard Veterinary Medical Teaching
Update on Pain: Collaborative Care for the Complex Patient
 Update on Pain: Collaborative Care for the Complex Patient Nirmala R. Abraham, MD Medical Director Sycamore Pain Management Center Kettering Health Network Objectives Standardized approach to patient care
Update on Pain: Collaborative Care for the Complex Patient Nirmala R. Abraham, MD Medical Director Sycamore Pain Management Center Kettering Health Network Objectives Standardized approach to patient care
Fighting the Good Fight: How to Convert Opioids Just Right!
 Fighting the Good Fight: How to Convert Opioids Just Right! Tanya J. Uritsky, PharmD, BCPS, CPE Clinical Pharmacy Specialist - Pain Medication Stewardship Hospital of the University of Pennsylvania - Philadelphia,
Fighting the Good Fight: How to Convert Opioids Just Right! Tanya J. Uritsky, PharmD, BCPS, CPE Clinical Pharmacy Specialist - Pain Medication Stewardship Hospital of the University of Pennsylvania - Philadelphia,
Measure Summary: The opioid equivalency measure examines opioid administration for patients who undergo a surgical procedure.
 Measure Abbreviation: Opioid Equivalency Data Collection Method: This informational measure (there is no threshold or target) is calculated based on data extracted from the electronic medical record combined
Measure Abbreviation: Opioid Equivalency Data Collection Method: This informational measure (there is no threshold or target) is calculated based on data extracted from the electronic medical record combined
AETNA BETTER HEALTH Prior Authorization guideline for Narcotic Analgesic Utilization
 AETNA BETTER HEALTH Prior Authorization guideline for Narcotic Analgesic Utilization Policy applies to all formulary and non-formulary schedules II V opioid narcotics, including tramadol and codeine, as
AETNA BETTER HEALTH Prior Authorization guideline for Narcotic Analgesic Utilization Policy applies to all formulary and non-formulary schedules II V opioid narcotics, including tramadol and codeine, as
Advanced Medical Care: Improving Veterinary Anesthesia. Advanced Medical Care: Improving Veterinary Anesthesia
 Advanced Medical Care: Improving Thursday, April 23, 2009 By Tamara Grubb, DVM, MS, DACVA AAHA gratefully acknowledges the following for their sponsorship of this Web Conference: Advanced Medical Care:
Advanced Medical Care: Improving Thursday, April 23, 2009 By Tamara Grubb, DVM, MS, DACVA AAHA gratefully acknowledges the following for their sponsorship of this Web Conference: Advanced Medical Care:
The Use of Analgesics in Rodents and Rabbits Deborah M. Mook, DVM
 The Use of Analgesics in Rodents and Rabbits Deborah M. Mook, DVM (Last updated August, 2005) Rationale. Well-established studies have shown repeatedly that effective analgesia enhances locomotion, increases
The Use of Analgesics in Rodents and Rabbits Deborah M. Mook, DVM (Last updated August, 2005) Rationale. Well-established studies have shown repeatedly that effective analgesia enhances locomotion, increases
B. Long-acting/Extended-release Opioids
 4 Opioid tolerance is assumed in patients already taking fentanyl 25 mcg/hr OR daily doses of the following oral agents for 1 week: 60 mg oral morphine, 30 mg oxycodone, 8 mg hydromorphone, 25 mg of oxymorphone
4 Opioid tolerance is assumed in patients already taking fentanyl 25 mcg/hr OR daily doses of the following oral agents for 1 week: 60 mg oral morphine, 30 mg oxycodone, 8 mg hydromorphone, 25 mg of oxymorphone
Oncologic Pain in Dogs: Prevention and Treatment
 The following excerpt is from Managing the Canine Cancer Patient: A Practical Guide to Compassionate Care (published by Veterinary Learning Systems, publisher of Compendium, 2006). To order a copy of the
The following excerpt is from Managing the Canine Cancer Patient: A Practical Guide to Compassionate Care (published by Veterinary Learning Systems, publisher of Compendium, 2006). To order a copy of the
GUIDELINES ON THE MANAGEMENT OF PAIN DUE TO CANCER IN ADULTS
 GUIDELINES ON THE MANAGEMENT OF PAIN DUE TO CANCER IN ADULTS Bristol Palliative Care Collaborative Contact Numbers: Hospital Specialist Palliative Care Teams: North Bristol 0117 4146392 UH Bristol 0117
GUIDELINES ON THE MANAGEMENT OF PAIN DUE TO CANCER IN ADULTS Bristol Palliative Care Collaborative Contact Numbers: Hospital Specialist Palliative Care Teams: North Bristol 0117 4146392 UH Bristol 0117
ANNEX I SUMMARY OF PRODUCT CHARACTERISTICS
 ANNEX I SUMMARY OF PRODUCT CHARACTERISTICS 1 1. NAME OF THE VETERINARY MEDICINAL PRODUCT Tralieve 50 mg/ml solution for injection for dogs (AT, BE, BG, CY, CZ, DE, EL, ES, HR, HU, IE, IT, LU, NL, PT, RO,
ANNEX I SUMMARY OF PRODUCT CHARACTERISTICS 1 1. NAME OF THE VETERINARY MEDICINAL PRODUCT Tralieve 50 mg/ml solution for injection for dogs (AT, BE, BG, CY, CZ, DE, EL, ES, HR, HU, IE, IT, LU, NL, PT, RO,
Multi Modal Analgesia
 Analgesic Drugs and Pharmacology Richard Craig R.N. B.N. M. Sci. Med (Pain Mgmt) Nurse Consultant Acute Pain Management Service Christchurch Hospital Multi Modal Analgesia Patients benefit from multi modal
Analgesic Drugs and Pharmacology Richard Craig R.N. B.N. M. Sci. Med (Pain Mgmt) Nurse Consultant Acute Pain Management Service Christchurch Hospital Multi Modal Analgesia Patients benefit from multi modal
Opioids: Use, Abuse and Cause of Death. Jennifer Harmon Assistant Director - Forensic Chemistry Orange County Crime Laboratory
 Opioids: Use, Abuse and Cause of Death Jennifer Harmon Assistant Director - Forensic Chemistry Orange County Crime Laboratory jharmon@occl.ocgov.com Opioid: Any psychoactive chemical that resembles morphine
Opioids: Use, Abuse and Cause of Death Jennifer Harmon Assistant Director - Forensic Chemistry Orange County Crime Laboratory jharmon@occl.ocgov.com Opioid: Any psychoactive chemical that resembles morphine
Clinical Policy: Opioid Analgesics Reference Number: OH.PHAR.PPA.13 Effective Date: 10/2017 Last Review Date: 6/2018 Line of Business: Medicaid
 Clinical Policy: Reference Number: OH.PHAR.PPA.13 Effective Date: 10/2017 Last Review Date: 6/2018 Line of Business: Medicaid Revision Log See Important Reminder at the end of this policy for important
Clinical Policy: Reference Number: OH.PHAR.PPA.13 Effective Date: 10/2017 Last Review Date: 6/2018 Line of Business: Medicaid Revision Log See Important Reminder at the end of this policy for important
Perioperative Pain Management
 Perioperative Pain Management Overview and Update As defined by the Anesthesiologist's Task Force on Acute Pain Management are from the practice guidelines from the American Society of Anesthesiologists
Perioperative Pain Management Overview and Update As defined by the Anesthesiologist's Task Force on Acute Pain Management are from the practice guidelines from the American Society of Anesthesiologists
Screening - inclusion criteria
 PAIN OUT Community research EU ROP EAN COMMISSION A Date of data collection: B Time of data collection: C Ward where data is collected: 2 0 1 Y M M D D H H M M D Research assistant Code: Room number: Screening
PAIN OUT Community research EU ROP EAN COMMISSION A Date of data collection: B Time of data collection: C Ward where data is collected: 2 0 1 Y M M D D H H M M D Research assistant Code: Room number: Screening
Advanced Pain Management LYRA SIHRA MD
 Advanced Pain Management LYRA SIHRA MD Objectives Describe the importance of pain management Define the types of pain Discuss opioid pharmacology Identify barriers to pain management Discuss ethical responsibilities
Advanced Pain Management LYRA SIHRA MD Objectives Describe the importance of pain management Define the types of pain Discuss opioid pharmacology Identify barriers to pain management Discuss ethical responsibilities
CHRONIC PAIN MANAGEMENT
 CHRONIC PAIN MANAGEMENT Betty J Harris, PharmD. 2014 Objectives Explain the consequences of untreated pain. Identify common causes of chronic non-malignant pain in adults. Identify steps to assessing pain,
CHRONIC PAIN MANAGEMENT Betty J Harris, PharmD. 2014 Objectives Explain the consequences of untreated pain. Identify common causes of chronic non-malignant pain in adults. Identify steps to assessing pain,
CONSTANT RATE INFUSION (CRIs) & ANALGESIA Carolyn Cartwright, RVT, VTS (Anesthesia/Analgesia)
 & ANALGESIA Carolyn Cartwright, RVT, VTS (Anesthesia/Analgesia)") CONSTANT RATE INFUSION (CRIs) & ANALGESIA Carolyn Cartwright, RVT, VTS (Anesthesia/Analgesia) Effective approach for optimum pain management requires a practical multimodal anesthesia and analgesia protocol.
CONSTANT RATE INFUSION (CRIs) & ANALGESIA Carolyn Cartwright, RVT, VTS (Anesthesia/Analgesia) Effective approach for optimum pain management requires a practical multimodal anesthesia and analgesia protocol.
ANALGESIA and LOCAL ANAESTHESIA. Professor Donald G. MacLellan Executive Director Health Education & Management Innovations
 ANALGESIA and LOCAL ANAESTHESIA Professor Donald G. MacLellan Executive Director Health Education & Management Innovations Definition of Pain Pain is an unpleasant sensory and emotional experience with
ANALGESIA and LOCAL ANAESTHESIA Professor Donald G. MacLellan Executive Director Health Education & Management Innovations Definition of Pain Pain is an unpleasant sensory and emotional experience with
Acute pain management in opioid tolerant patients. Muhammad Laklouk
 Acute pain management in opioid tolerant patients Muhammad Laklouk General principles An adequate review and assessment Provision of effective analgesia (including attenuation of tolerance and hyperalgesia)
Acute pain management in opioid tolerant patients Muhammad Laklouk General principles An adequate review and assessment Provision of effective analgesia (including attenuation of tolerance and hyperalgesia)
MURDOCH RESEARCH REPOSITORY
 MURDOCH RESEARCH REPOSITORY http://researchrepository.murdoch.edu.au/7771/ Musk, G. and Raisis, A. (2012) Analgesia for patients with neurological disease. In: Platt, S. and Garosi, L., (eds.) Small Animal
MURDOCH RESEARCH REPOSITORY http://researchrepository.murdoch.edu.au/7771/ Musk, G. and Raisis, A. (2012) Analgesia for patients with neurological disease. In: Platt, S. and Garosi, L., (eds.) Small Animal
BJF Acute Pain Team Formulary Group
 Title Analgesia Guidelines for Acute Pain Management (Adults) in BGH Document Type Issue no Clinical guideline Clinical Governance Support Team Use Issue date April 2013 Review date April 2015 Distribution
Title Analgesia Guidelines for Acute Pain Management (Adults) in BGH Document Type Issue no Clinical guideline Clinical Governance Support Team Use Issue date April 2013 Review date April 2015 Distribution
PALLIATIVE TREATMENT BY DR. KHRONGKAMOL SIHABAN MEDICAL ONCOLOGIST
 PALLIATIVE TREATMENT BY DR. KHRONGKAMOL SIHABAN MEDICAL ONCOLOGIST TREATMENT IN ONCOLOGY Main treatment : surgery Neoadjuvant treatment : RT, CMT Adjuvant treatment : Tx micrometastatic disease -CMT,Targeted
PALLIATIVE TREATMENT BY DR. KHRONGKAMOL SIHABAN MEDICAL ONCOLOGIST TREATMENT IN ONCOLOGY Main treatment : surgery Neoadjuvant treatment : RT, CMT Adjuvant treatment : Tx micrometastatic disease -CMT,Targeted
Knock Out Opioid Abuse in New Jersey:
 Knock Out Opioid Abuse in New Jersey: A Resource for Safer Prescribing GUIDELINE FOR PRESCRIBING OPIOIDS FOR CHRONIC PAIN IMPROVING PRACTICE THROUGH RECOMMENDATIONS CDC s Guideline for Prescribing Opioids
Knock Out Opioid Abuse in New Jersey: A Resource for Safer Prescribing GUIDELINE FOR PRESCRIBING OPIOIDS FOR CHRONIC PAIN IMPROVING PRACTICE THROUGH RECOMMENDATIONS CDC s Guideline for Prescribing Opioids
Nerve Blocks & Long Acting Analgesia for Plastic Surgeons. Karol A Gutowski, MD, FACS
 Nerve Blocks & Long Acting Analgesia for Plastic Surgeons Karol A Gutowski, MD, FACS Disclosures None related to this topic Why is Non-Opioid Analgesia Important Opioid epidemic Less opioid use Less PONV
Nerve Blocks & Long Acting Analgesia for Plastic Surgeons Karol A Gutowski, MD, FACS Disclosures None related to this topic Why is Non-Opioid Analgesia Important Opioid epidemic Less opioid use Less PONV
SUMMARY OF PRODUCT CHARACTERISTICS
 SUMMARY OF PRODUCT CHARACTERISTICS 1. NAME OF THE VETERINARY MEDICINAL PRODUCT Buprecare Multidose 0.3 mg/ml Solution for Injection for Dogs and Cats (UK, BE, FR, IE, LU, NL, ES) Buprenovet Multidose 0.3
SUMMARY OF PRODUCT CHARACTERISTICS 1. NAME OF THE VETERINARY MEDICINAL PRODUCT Buprecare Multidose 0.3 mg/ml Solution for Injection for Dogs and Cats (UK, BE, FR, IE, LU, NL, ES) Buprenovet Multidose 0.3
Screening - inclusion criteria
 A Date of data collection: B Time of data collection: C Ward where data is collected: 2 0 1 Y M M D D H H M M D Research assistant Code: Patient code (local): Room number: Screening - inclusion criteria
A Date of data collection: B Time of data collection: C Ward where data is collected: 2 0 1 Y M M D D H H M M D Research assistant Code: Patient code (local): Room number: Screening - inclusion criteria
BASICS OF OPIOID PRESCRIBING 10:30-11:45AM
 PROVIDING QUALITY CARE TO PAIN PATIENTS IN IOWA BASICS OF OPIOID PRESCRIBING 10:30-11:45AM ACPE UAN: 107-000-14-013-L01-P Activity Type: Application-Based 0.125 CEU/1.25hr Learning Objectives for Pharmacists:
PROVIDING QUALITY CARE TO PAIN PATIENTS IN IOWA BASICS OF OPIOID PRESCRIBING 10:30-11:45AM ACPE UAN: 107-000-14-013-L01-P Activity Type: Application-Based 0.125 CEU/1.25hr Learning Objectives for Pharmacists:
PAIN. TREATMENT TABLES Analgesics. NON-OPIOID ANALGESICS Generic Name Trade Names (Examples) Duration Initial Dose
 Duration Initial Dose") NON-OPIOID SHORT-ACTING LONG-ACTING **** O PAIN TREATMENT TABLES Analgesics NON-OPIOID ANALGESICS Generic Name Trade Names (Examples) Duration Initial Dose Tramadol 50 mg Ultram Every 4 hours 1-2 tabs,
NON-OPIOID SHORT-ACTING LONG-ACTING **** O PAIN TREATMENT TABLES Analgesics NON-OPIOID ANALGESICS Generic Name Trade Names (Examples) Duration Initial Dose Tramadol 50 mg Ultram Every 4 hours 1-2 tabs,
Analgesia for ERAS programs. Dr Igor Lemech VMO Anaesthetist Wagga Wagga Base Hospital
 Analgesia for ERAS programs Dr Igor Lemech VMO Anaesthetist Wagga Wagga Base Hospital Disclosure I have received honoraria from Mundipharma and MSD The new Wagga Wagga Rural Referral Centre Scope Analgesic
Analgesia for ERAS programs Dr Igor Lemech VMO Anaesthetist Wagga Wagga Base Hospital Disclosure I have received honoraria from Mundipharma and MSD The new Wagga Wagga Rural Referral Centre Scope Analgesic
E-Learning Module N: Pharmacological Review
 E-Learning Module N: Pharmacological Review This Module requires the learner to have read Chapter 13 of the Fundamentals Program Guide and the other required readings associated with the topic. Revised:
E-Learning Module N: Pharmacological Review This Module requires the learner to have read Chapter 13 of the Fundamentals Program Guide and the other required readings associated with the topic. Revised:
2017 Opioid Prescribing Module 401 N. Ewing St. Lancaster, Ohio (740) ~
 ~") 2017 Opioid Prescribing Module 401 N. Ewing St. Lancaster, Ohio 43130 (740) 687-8000 ~ www.fmchealth.org Introduction The purpose of this module is to reduce the risk of adverse outcomes for adult patients
2017 Opioid Prescribing Module 401 N. Ewing St. Lancaster, Ohio 43130 (740) 687-8000 ~ www.fmchealth.org Introduction The purpose of this module is to reduce the risk of adverse outcomes for adult patients
Drugs Used In Management Of Pain. Dr. Aliah Alshanwani
 Drugs Used In Management Of Pain Dr. Aliah Alshanwani 1 Drugs Used In Management Of Pain A CASE OF OVERDOSE Sigmund Freud, the father of psychoanalysis His cancer of the jaw was causing him increasingly
Drugs Used In Management Of Pain Dr. Aliah Alshanwani 1 Drugs Used In Management Of Pain A CASE OF OVERDOSE Sigmund Freud, the father of psychoanalysis His cancer of the jaw was causing him increasingly
DBL NALOXONE HYDROCHLORIDE INJECTION USP
 Name of medicine Naloxone hydrochloride Data Sheet New Zealand DBL NALXNE HYDRCHLRIDE INJECTIN USP Presentation DBL Naloxone Hydrochloride Injection USP is a sterile, clear, colourless solution, free from
Name of medicine Naloxone hydrochloride Data Sheet New Zealand DBL NALXNE HYDRCHLRIDE INJECTIN USP Presentation DBL Naloxone Hydrochloride Injection USP is a sterile, clear, colourless solution, free from
Multimodal analgesic therapy has gained widespread
 TOPICAL REVIEW Analgesia for Anesthetized Patients Kip A. Lemke, DVM, MSc, Dipl. ACVA, and Catherine M. Creighton, DVM Many perioperative pain management protocols for cats and dogs are overly complex,
TOPICAL REVIEW Analgesia for Anesthetized Patients Kip A. Lemke, DVM, MSc, Dipl. ACVA, and Catherine M. Creighton, DVM Many perioperative pain management protocols for cats and dogs are overly complex,
Management of Pain. Agenda: Definitions Pathophysiology Analgesics
 C. Brian Warriner, MD, FRCPC Professor and Past Chair UBC Department of Anesthesiology, Pharmacology and Therapeutics brian.warriner@vch.ca Agenda: Definitions Pathophysiology Analgesics Gases(N 2 O) Opiates
C. Brian Warriner, MD, FRCPC Professor and Past Chair UBC Department of Anesthesiology, Pharmacology and Therapeutics brian.warriner@vch.ca Agenda: Definitions Pathophysiology Analgesics Gases(N 2 O) Opiates
Opioid Analgesics. Recommended starting dose for opioid-naïve patients
 Opioid Analgesics Goals: Restrict use of opioid analgesics to OHP-funded conditions with documented sustained improvement in pain and function and with routine monitoring for opioid misuse and abuse. Promote
Opioid Analgesics Goals: Restrict use of opioid analgesics to OHP-funded conditions with documented sustained improvement in pain and function and with routine monitoring for opioid misuse and abuse. Promote
GUIDELINES AND AUDIT IMPLEMENTATION NETWORK
 GUIDELINES AND AUDIT IMPLEMENTATION NETWORK General Palliative Care Guidelines The Management of Pain at the End Of Life November 2010 Aim To provide a user friendly, evidence based guide for the management
GUIDELINES AND AUDIT IMPLEMENTATION NETWORK General Palliative Care Guidelines The Management of Pain at the End Of Life November 2010 Aim To provide a user friendly, evidence based guide for the management
Mitigating Risks While Optimizing the Benefits of Pharmacologic Agents to Manage Pain in the Elderly
 Mitigating Risks While Optimizing the Benefits of Pharmacologic Agents to Manage Pain in the Elderly Mary Lynn McPherson, PharmD, MDE, MA, BCPS, CPE Professor and Executive Director, Advanced Post-Graduate
Mitigating Risks While Optimizing the Benefits of Pharmacologic Agents to Manage Pain in the Elderly Mary Lynn McPherson, PharmD, MDE, MA, BCPS, CPE Professor and Executive Director, Advanced Post-Graduate
GUIDELINES ON PAIN MANAGEMENT IN UROLOGY
 GUIDELINES ON PAIN MANAGEMENT IN UROLOGY F. Francesca (chairman), P. Bader, D. Echtle, F. Giunta, J. Williams Eur Urol 2003; 44(4):383-389 Introduction Pain is defined as an unpleasant sensory and emotional
GUIDELINES ON PAIN MANAGEMENT IN UROLOGY F. Francesca (chairman), P. Bader, D. Echtle, F. Giunta, J. Williams Eur Urol 2003; 44(4):383-389 Introduction Pain is defined as an unpleasant sensory and emotional