Complex Acute Surgical Pain Management. Thomas Baribeault MSN, CRNA
|
|
|
- Prudence Robinson
- 5 years ago
- Views:
Transcription
1 Complex Acute Surgical Pain Management Thomas Baribeault MSN, CRNA
2 Introduction Anatomy and pathophysiology of acute surgical pain Pharmacology Chronic pain patient Opioid tolerant patient
3 Introduction Over 50% of surgical patients report poor postoperative pain control 1:15 surgical patients develop opioid addiction or dependence Poorly managed acute surgical pain delays healing, increases complication rates, prolongs hospital stay, increases cost, and risk of chronic post-surgical pain Chronic pain is more prevalent than all forms of cancer
4 Anatomy Physiology Peripheral Nerves (first order neurons) A Beta Touch and pressure Low threshold Interneuron A Delta First/Fast Pain response High threshold
5 Anatomy Physiology Peripheral Nerves (first order neurons) C Slow/long pain response High threshold Mechano/thermal/chemo responsive 15% silent respond only to inflammation Soma Dorsal Root Ganglion can still cause depolarization even if nerve is blocked in periphery
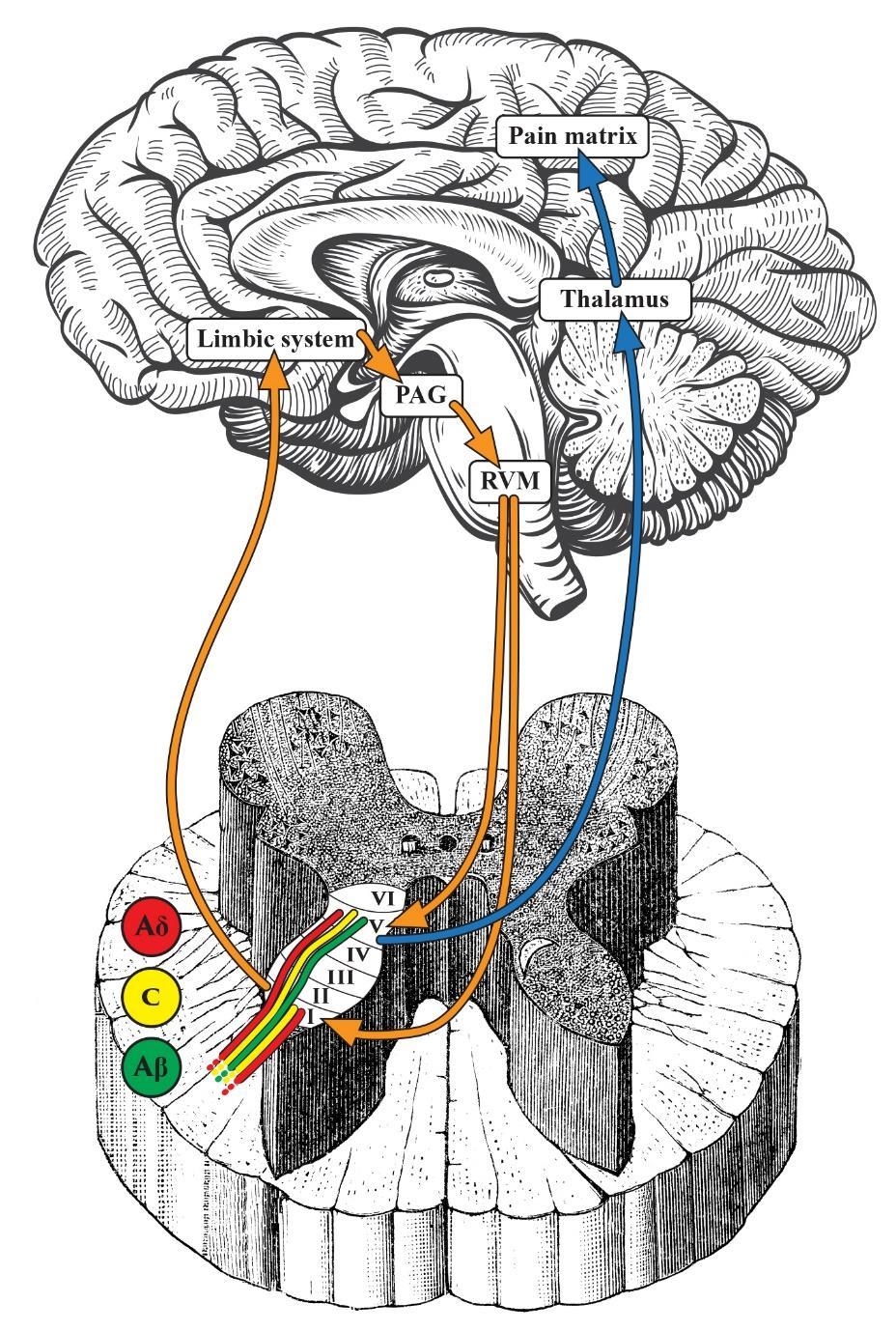
6 Anatomy Physiology Spinal Nerves (second order neurons) Peripheral nerves synapse with the spinal nerves at the Rexed Lamina of the spinal cord Each peripheral nerve ascends and descends to synapse at the Rexed Lamina of 4-5 dermatomes
7 Anatomy Physiology Rexed Lamina I A Delta and C fibers Nociceptive specific cells Rexed Lamina V A Beta, A Delta, and C fibers Wide Dynamic Range neurons Others II,III,IV,VI
8 Anatomy Physiology Ascending fibers Spinothalamic tract Spinal nerves cross to contralateral side Primary ascending tract Thalamus Others Spinoreticular Spinomesencephalic
9 Anatomy Physiology Brain (third order neurons) Thalamus Periaqueductal Grey Rostral Ventromedial Medulla Descending spinal fibers Pain matrix
10 Anatomy Physiology
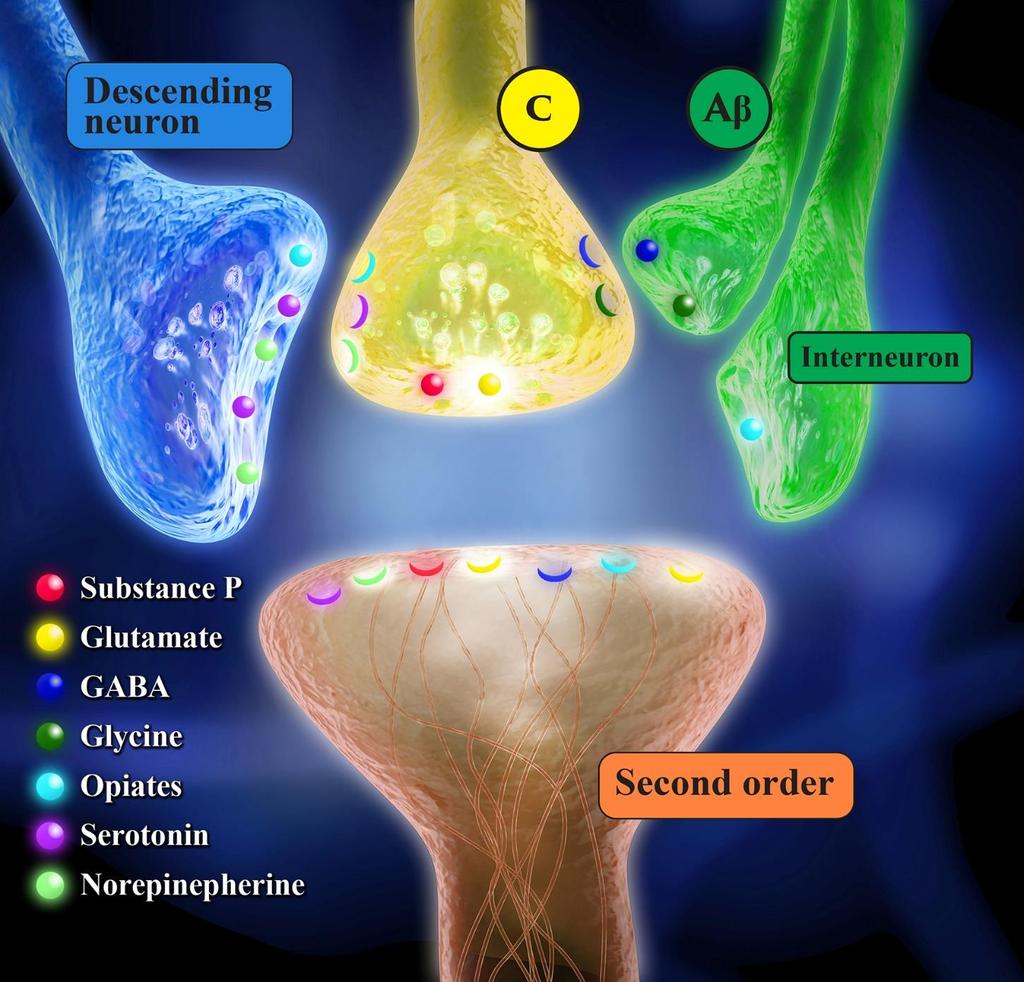
11 Anatomy Physiology Neurotransmitters Glutamate Primary pain neurotransmitter Binds to AMPA, NMDA, KA» Ionic channels 8 mglur Substance P Binds to NK1 receptor Enhances depolarization Others CGRP, CCK, etc
12 Anatomy Physiology Pain inhibition A Beta inhibition Activates interneurons Release Gaba and Glycine Inhibits first and second order neurons PAG Release endorphins, dynorphins, enkephalins Endogenous opioid substances RVM Activates descending inhibitory nerve fibers Release serotonin, norepinephrine
13 Anatomy Physiology
14 Hyperalgesia Peripheral Sensitization (Primary Hyperalgesia) Tissue damage causes release of inflammatory mediators Sensitizing soup Bradykinin, Substance P, Histamine, Leukotrienes, etc
15 Hyperalgesia Peripheral Sensitization (Primary Hyperalgesia) C Fibers Activation of silent fibers High threshold become low threshold Produce stronger stimulus with same stimulation Continue firing after stimulation has stopped Lose mechano/thermos/chemo specificity Nerve memory Repeat exposure within 21 days leads to more severe changes Can lead to permanent changes in nerve function
16 Hyperalgesia
17 Hyperalgesia
18 Hyperalgesia Inflammatory Induced Central Sensitization Prostaglandin E2 in CSF Mechanism not understood Interaction of COX 2 and NMDA receptor
19 Hyperalgesia Central Sensitization (Secondary hyperalgesia) Wind Up Peripherally sensitized C fibers release excess glutamate into synaptic cleft Mg plug blocking Ca channel is lost Body creates more AMPA receptors Starts in minutes
20 Hyperalgesia
21 Hyperalgesia
22 Hyperalgesia Allodynia Death of the interneuron A Beta fibers lose inhibitory effect Touch and pressure becomes painful
23 Hyperalgesia
24 Pharmacology Peripheral Sensitization Steroids NSAIDS Local Anesthetics Cannabinoids
25 Pharmacology Steroids Dexamethasone Dose 4-10 mg Mechanism Inhibits prostaglandins, leukotrienes and histamine Considerations Increases glucose diabetics/non same % Does not inhibit healing
26 Pharmacology NSAIDS Cox 1 vs Cox 2 inhibition Cox 1 Gastric ulcer Platelet dysfunction Renal dysfunction Cox 2 Renal dysfunction Reduces pain, fever, and inflammation Contraindications renal failure, gi bleed, thrombotic event, CABG, age >60, thrombocytopenia
27 Pharmacology NSAIDS Non-selective cox inhibitors Ibuprofen PO, IV, TD Naproxen PO Diclofenac PO, IV, TD Toradol PO, IV Cox 2 inhibitor Celecoxib PO Parecoxib IV (Non-US)
28 Pharmacology NSAIDS Surgical considerations No difference in analgesia, different toxicity profiles Renal function, age, hydration Platelet dysfunction/bleeding concerns Cox 2 inhibitor given pre-op, inflammatory benefit
29 Pharmacology Acetaminophen Dose 1G 15 mg/kg Mechanism Unknown No anti-inflammatory effect Considerations Liver dysfunction PO vs IV/Cost vs Efficacy Statistically significant reduction in pain
30 Pharmacology Lidocaine Dose 1.5 mg/kg 2-3 mg/kg/hr Mechanism Systemic analgesia 2, 8, 48 hours Blocks prostaglandin release Considerations Safety 2-3 mcg/ml plasma concentration
31 Pharmacology Cannabinoids THC vs CBD 2x anti-inflammatory effect dexamethasone Analgesic effect at the C1 and C2 receptors
32 Pharmacology Central Sensitization Glutamate Ketamine, N2O, Mg, Gabapentin/Pregabalin Substance P Dexmedetomidine, Clonidine, Tizanidine Serotonin/Norepinephrine Duloxetine, Tramadol, Tapentadol
33 Pharmacology Ketamine Dose mg/kg mg/kg 2-10 mcg/kg/min 1:1 morphine PCA Mechanism Blocks NMDA glutamate receptor
34 Pharmacology Ketamine Considerations Caution cardiovascular disease, increased ICP, and catecholamine depression Hallucinations/disassociation Reverse and prevent OIH/OT Bronchodilator Treatment for depression, suicidal ideation, and PTSD
35 Pharmacology N2O Dose 50% ET = 15 mg morphine Mechanism Blocks NMDA receptor Considerations Caution in pulmonary hypertension, B12 anemia, and respiratory disease Can reverse hyperalgesia
36 Pharmacology Magnesium Dose mg/kg 10 mg/kg/hr infusion Mechanism Prevents loss of Mg plug from NMDA receptor Considerations Analgesia not dose dependent Caution in renal failure Prolongs NMB Prevent post-operative shivering
37 Pharmacology Gabapentin/Pregabalin Dose Gabapentin mg Pregabalin mg Mechanism Blocks pre-synaptic release of glutamate and substance P
38 Pharmacology Gabapentin/Pregabalin Considerations Post-operative sedation Pregabalin fast absorption, more consistent plasma levels Pregabalin rare side effects Angioedema, thrombocytopenia, rhabdomyolysis, increased pr interval
39 Pharmacology Dexmedetomidine Dose mcg/kg over 10 minutes mcg/kg/hr Mechanism Sedation Pain Blocks norepinephrine in the locus coeruleus Blocks substance P from binding to the NK1 receptor
40 Pharmacology Dexmedetomidine Considerations Caution tachy/bradycardia, hyper/hypotension Post-operative sedation Reduction in emergence delirium Prevents post-operative shivering
41 Pharmacology Clonidine Dose 2-3 mcg/kg IV 3-5 mcg/kg PO Mechanism Same as dexmedetomidine Considerations 12 hour half life Less specific for pain/sedation receptors than dexmedetomidine
42 Pharmacology Tizanidine Dose 2-4 mg PO Considerations Muscle relaxant with A2 agonist activity
43 Pharmacology Tramadol/Tapentadol Duloxetine mg SSRI/SSNI Cyclobenzaprine Muscle relaxant structurally similar to TCI
44 Chronic pain Chronic Post-surgical Pain Pain long after healing process is complete Poorly controlled pain is the best predictor Most common procedures Thoracotomy, sternotomy, breast surgery, amputation Mechanism not known Inflammatory changes to peripheral nerves Central sensitization of spinal nerves Chronic changes to Thalamus
45 Chronic pain Chronic Post-surgical Pain Risk factors Age Young > old Type and length of surgery > 3 hours Pre-operative opioid use Genetic factors
46 Chronic pain Chronic Post-surgical Pain Prediction Not successful Prevention Mixed results in studies Combination treatment best results Regional/Neuraxial Anti-inflammatories Central antagonism Non-opioid analgesics
47 Chronic pain Fibromyalgia Multiple conditions Similar symptoms Similar pathophysiology Widespread pain index >7, symptom severity score >5, >3 months Fibromyalgia-ness score Screening surgical patient predicts Amount of post-operative pain Opioid requirements
48 Chronic pain Fibromyalgia Symptoms Diffuse central hyperalgesia (Spine/Thalamus) Volume Knob concept Tender points With or without inflammatory process Allodynia Sensitivity to heat or cold Sensitivity to auditory/visual stimuli Sleep disruption Fatigue Memory or attention problems
49 Chronic pain Fibromyalgia Symptoms Poor exercise tolerance Depression Pain Lack of answers or effective treatment Treatment by healthcare workers
50 Chronic pain Fibromyalgia Treatment Anti-depressants TCA» Amitriptyline» Cyclobenzaprine SSRI/SSNI» Duloxetine» Milnacipran Gabapentinoid Gabapentin Pregabalin
51 Chronic pain Fibromyalgia Treatment Tizanidine Acetaminophen/Nsaids Mild success Tramadol/Tapentadol Serotonin/norepinephrine Aerobic exercise Cognitive behavioral therapy
52 Chronic pain Fibromyalgia Does not work Opioids Overactive release of bodies endogenous opioids
53 Chronic pain Fibromyalgia Surgery Pre-operative Honest conversation about expectations and pain Mistrust because of mistreatment by healthcare professionals Misdiagnosed Medical/nonmedical therapy not optimized May have been given erroneous information about condition
54 Chronic pain Fibromyalgia Surgery Pain management Opioids not effective for treatment of pain» If on opioid do not stop rebound phenomenon Regional or neuraxial technique Maximize central acting drugs» Glutamate Ketamine, N2O, Mg, Gabapentin/Pregabalin» Substance P Clonidine, Dexmedetomidine, Tizanidine» Serotonin/Norepinephrine Duloxetine, Tramadol
55 Chronic pain Fibromyalgia Surgery Pain management Acetaminophen Nsaids
56 Opioid tolerant Chronic opioid therapy Illicit opioid Opioid addiction therapy Methadone Buprenorphine Suboxone Subutex Naltrexone (Vivitrol)
57 Opioid Tolerant Opioids Benefit No ceiling effect, limited by side effects Disadvantage Sisyphus effect = hyperalgesia + tolerance Rates of long term use increase after 3 days 100% of long term opioid users develop dependence Addiction risk increases with use
58 Opioid Tolerant Diphenylpropulamines Methadone Broad spectrum Opioid Mu, Delta, Kappa, NMDA blocks opioid tolerance and hyperalgesia 6-8 hour alpha phase elimination 400% inter-patient variability Respiratory depression often outlasts analgesia DANGER Prolongs QT
59 Opioid Tolerant Partial Agonist Buprenorphine High affinity/partial agonist Mu receptors Less sedation, nausea, pruritus, respiratory depression and urinary retention Slow disassociation from Mu receptors Antagonist Kappa Suboxone Buprenorphine + Naloxone Subutex Buprenorphine
60 Opioid Tolerant Naltrexone (Vivitrol) Opioid Antagonist Can t be started until after withdrawal complete Monthly injection Least abuse potential and side effects
61 Opioid Tolerant Surgery Methadone Continue Buprenorphine and Naltrexone Minor Surgery Continue treatment Multi-modal therapy Major surgery Wean off vs. continue» How painful is surgery» Ability to treat that pain with non-opioids» 3 days buprenorphine» 28 days naltrexone
62 Opioid Tolerant Surgery Pre-operative Honest conversation about expectations and pain Mistrust because of mistreatment and judgment by healthcare professionals May not have been given appropriate instructions regarding therapy» Weaned and now at high risk for relapse» Not weaned and high risk for uncontrolled pain May have been given erroneous information
63 Opioid Tolerant Surgery Regional or neuraxial technique Maximize central acting drugs Glutamate Ketamine, N2O, Mg, Gabapentin/Pregabalin Substance P Clonidine, Dexmedetomidine, Tizanidine Serotonin/Norepinephrine Duloxetine, Tramadol Nsaids Acetaminophen
64 References Fishman S, Bonica J. Bonica's Management Of Pain. Philadelphia, Pa: Wolters Kluwer; Sinatra, R., Jahr, J. and Watkins-Pitchford, J. (2011). The essence of analgesia and analgesics. Cambridge: Cambridge University Press.
PAIN & ANALGESIA. often accompanied by clinical depression. fibromyalgia, chronic fatigue, etc. COX 1, COX 2, and COX 3 (a variant of COX 1)
") Pain - subjective experience associated with detection of tissue damage ( nociception ) acute - serves as a warning chronic - nociception gone bad often accompanied by clinical depression fibromyalgia,
Pain - subjective experience associated with detection of tissue damage ( nociception ) acute - serves as a warning chronic - nociception gone bad often accompanied by clinical depression fibromyalgia,
Pharmacology of Pain Transmission and Modulation
 Pharmacology of Pain Transmission and Modulation 2 Jürg Schliessbach and Konrad Maurer Nociceptive Nerve Fibers Pain is transmitted to the central nervous system via thinly myelinated Aδ and unmyelinated
Pharmacology of Pain Transmission and Modulation 2 Jürg Schliessbach and Konrad Maurer Nociceptive Nerve Fibers Pain is transmitted to the central nervous system via thinly myelinated Aδ and unmyelinated
Receptors and Neurotransmitters: It Sounds Greek to Me. Agenda. What We Know About Pain 9/7/2012
 Receptors and Neurotransmitters: It Sounds Greek to Me Cathy Carlson, PhD, RN Northern Illinois University Agenda We will be going through this lecture on basic pain physiology using analogies, mnemonics,
Receptors and Neurotransmitters: It Sounds Greek to Me Cathy Carlson, PhD, RN Northern Illinois University Agenda We will be going through this lecture on basic pain physiology using analogies, mnemonics,
Pain Pathways. Dr Sameer Gupta Consultant in Anaesthesia and Pain Management, NGH
 Pain Pathways Dr Sameer Gupta Consultant in Anaesthesia and Pain Management, NGH Objective To give you a simplistic and basic concepts of pain pathways to help understand the complex issue of pain Pain
Pain Pathways Dr Sameer Gupta Consultant in Anaesthesia and Pain Management, NGH Objective To give you a simplistic and basic concepts of pain pathways to help understand the complex issue of pain Pain
CHAPTER 4 PAIN AND ITS MANAGEMENT
 CHAPTER 4 PAIN AND ITS MANAGEMENT Pain Definition: An unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage. Types of Pain
CHAPTER 4 PAIN AND ITS MANAGEMENT Pain Definition: An unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage. Types of Pain
Learning Objectives. Perioperative goals. Acute Pain in the Chronic Pain Patient for Ambulatory Surgery 9/8/16
 Acute Pain in the Chronic Pain Patient for Ambulatory Surgery Danielle Ludwin, MD Associate Professor of Anesthesiology Division of Regional and Orthopedic Anesthesia Columbia University Medical Center
Acute Pain in the Chronic Pain Patient for Ambulatory Surgery Danielle Ludwin, MD Associate Professor of Anesthesiology Division of Regional and Orthopedic Anesthesia Columbia University Medical Center
Acute Postoperative Pain. David Radvinsky, MD March 24, 2016
 Acute Postoperative Pain David Radvinsky, MD March 24, 2016 Objectives 1. Discuss the multimodal approach to pain management and discuss the various classes of drugs based on receptor mechanism. 2. Give
Acute Postoperative Pain David Radvinsky, MD March 24, 2016 Objectives 1. Discuss the multimodal approach to pain management and discuss the various classes of drugs based on receptor mechanism. 2. Give
Spinal Cord Injury Pain. Michael Massey, DO CentraCare Health St Cloud, MN 11/07/2018
 Spinal Cord Injury Pain Michael Massey, DO CentraCare Health St Cloud, MN 11/07/2018 Objectives At the conclusion of this session, participants should be able to: 1. Understand the difference between nociceptive
Spinal Cord Injury Pain Michael Massey, DO CentraCare Health St Cloud, MN 11/07/2018 Objectives At the conclusion of this session, participants should be able to: 1. Understand the difference between nociceptive
The Fifth Vital Sign.
 Recognizing And Monitoring The Painful Patient Susan Clark, LVT, VTS(ECC) The Fifth Vital Sign. Pain control is part of the accepted standard of care in veterinary medicine. The ability to recognize the
Recognizing And Monitoring The Painful Patient Susan Clark, LVT, VTS(ECC) The Fifth Vital Sign. Pain control is part of the accepted standard of care in veterinary medicine. The ability to recognize the
AKA a painful lecture by Colleen Blanchfield, MD Full Circle Neuropsychiatric Wellness Center
 A lecture on PAIN AKA a painful lecture by Colleen Blanchfield, MD Full Circle Neuropsychiatric Wellness Center 1 Overview of the lecture Anatomy of the Pain Tract How a painful stimulus travels from the
A lecture on PAIN AKA a painful lecture by Colleen Blanchfield, MD Full Circle Neuropsychiatric Wellness Center 1 Overview of the lecture Anatomy of the Pain Tract How a painful stimulus travels from the
Acute Pain NETP: SEPTEMBER 2013 COHORT
 Acute Pain NETP: SEPTEMBER 2013 COHORT Pain & Suffering an unpleasant sensory & emotional experience associated with actual or potential tissue damage, or described in terms of such damage International
Acute Pain NETP: SEPTEMBER 2013 COHORT Pain & Suffering an unpleasant sensory & emotional experience associated with actual or potential tissue damage, or described in terms of such damage International
Proceedings of the World Small Animal Veterinary Association Sydney, Australia 2007
 Proceedings of the World Small Animal Sydney, Australia 2007 Hosted by: Next WSAVA Congress REDUCING THE PAIN FACTOR AN UPDATE ON PERI-OPERATIVE ANALGESIA Sandra Forysth, BVSc DipACVA Institute of Veterinary,
Proceedings of the World Small Animal Sydney, Australia 2007 Hosted by: Next WSAVA Congress REDUCING THE PAIN FACTOR AN UPDATE ON PERI-OPERATIVE ANALGESIA Sandra Forysth, BVSc DipACVA Institute of Veterinary,
NON-OPIOID ANALGESIA & THE IMPLICATIONS OF ANESTHETIC DRUGS IN THE PERI-ANESTHETIC ARENA AMANDA AFFLECK CRNA
 NON-OPIOID ANALGESIA & THE IMPLICATIONS OF ANESTHETIC DRUGS IN THE PERI-ANESTHETIC ARENA AMANDA AFFLECK CRNA OR, ANESTHESIA, WHY DO THEY DO THAT? OUTLINE Neurotransmission of pain Arachidonic Acid pathway
NON-OPIOID ANALGESIA & THE IMPLICATIONS OF ANESTHETIC DRUGS IN THE PERI-ANESTHETIC ARENA AMANDA AFFLECK CRNA OR, ANESTHESIA, WHY DO THEY DO THAT? OUTLINE Neurotransmission of pain Arachidonic Acid pathway
Review Normal Pain Anatomy and Physiology Pathological Pain Pathways? Targeted Treatments Future Developments 9/26/2011
 Jeremy A. Adler, MS, PA C Pacific Pain Medicine Consultants Encinitas, CA Consultant Pfizer Endo Pharmaceuticals Azur Pharma Janssen Pharmaceuticals St. Jude Medical As part of this presentation, off label
Jeremy A. Adler, MS, PA C Pacific Pain Medicine Consultants Encinitas, CA Consultant Pfizer Endo Pharmaceuticals Azur Pharma Janssen Pharmaceuticals St. Jude Medical As part of this presentation, off label
Chapter 16. Sense of Pain
 Chapter 16 Sense of Pain Pain Discomfort caused by tissue injury or noxious stimulation, and typically leading to evasive action important /// helps to protect us lost of pain in diabetes mellitus = diabetic
Chapter 16 Sense of Pain Pain Discomfort caused by tissue injury or noxious stimulation, and typically leading to evasive action important /// helps to protect us lost of pain in diabetes mellitus = diabetic
Acute Pain Management in the Opioid Tolerant Patient. Objectives. Opioids. The participant will be able to define opioid tolerance
 Acute Pain Management in the Opioid Tolerant Patient Kathleen M. Colfer, MSN, RN-BC Clinical Nurse Specialist Acute Pain Management Service Department of Anesthesiology Thomas Jefferson University Hospital
Acute Pain Management in the Opioid Tolerant Patient Kathleen M. Colfer, MSN, RN-BC Clinical Nurse Specialist Acute Pain Management Service Department of Anesthesiology Thomas Jefferson University Hospital
Management of Pain. Agenda: Definitions Pathophysiology Analgesics
 C. Brian Warriner, MD, FRCPC Professor and Past Chair UBC Department of Anesthesiology, Pharmacology and Therapeutics brian.warriner@vch.ca Agenda: Definitions Pathophysiology Analgesics Gases(N 2 O) Opiates
C. Brian Warriner, MD, FRCPC Professor and Past Chair UBC Department of Anesthesiology, Pharmacology and Therapeutics brian.warriner@vch.ca Agenda: Definitions Pathophysiology Analgesics Gases(N 2 O) Opiates
UCSF Pediatric Hospital Medicine Boot Camp Pain Session 6/21/14. Cynthia Kim and Stephen Wilson
 UCSF Pediatric Hospital Medicine Boot Camp Pain Session 6/21/14 Cynthia Kim and Stephen Wilson Rules Buzz first and player answers If answer correct, then the player asks teammates if they want to keep
UCSF Pediatric Hospital Medicine Boot Camp Pain Session 6/21/14 Cynthia Kim and Stephen Wilson Rules Buzz first and player answers If answer correct, then the player asks teammates if they want to keep
Lumbar Fusion. Reference Guide for PACU CLINICAL PATHWAY. All patient variances to the pathway are to be circled and addressed in the progress notes.
 Reference Guide for PACU Lumbar Fusion CLINICAL PATHWAY All patient variances to the pathway are to be circled and addressed in the progress notes. This Clinical Pathway is intended to assist in clinical
Reference Guide for PACU Lumbar Fusion CLINICAL PATHWAY All patient variances to the pathway are to be circled and addressed in the progress notes. This Clinical Pathway is intended to assist in clinical
CHAPTER 4 PAIN AND ITS MANAGEMENT
 CHAPTER 4 PAIN AND ITS MANAGEMENT Pain Definition: An unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage. Types of Pain
CHAPTER 4 PAIN AND ITS MANAGEMENT Pain Definition: An unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage. Types of Pain
Action Potentials and Synaptic Transmission. BIO 219 Napa Valley College Dr. Adam Ross
 Action Potentials and Synaptic Transmission BIO 219 Napa Valley College Dr. Adam Ross Review of action potentials Nodes of Ranvier Nucleus Dendrites Cell body In saltatory conduction, the nerve impulses
Action Potentials and Synaptic Transmission BIO 219 Napa Valley College Dr. Adam Ross Review of action potentials Nodes of Ranvier Nucleus Dendrites Cell body In saltatory conduction, the nerve impulses
San Francisco Chronicle, June 2001
 PAIN San Francisco Chronicle, June 2001 CONGENITAL INSENSITIVITY TO PAIN PAIN IS A SUBJECTIVE EXPERIENCE: It is not a stimulus MAJOR FEATURES OF THE PAIN EXPERIENCE: Sensory discriminative Affective (emotional)
PAIN San Francisco Chronicle, June 2001 CONGENITAL INSENSITIVITY TO PAIN PAIN IS A SUBJECTIVE EXPERIENCE: It is not a stimulus MAJOR FEATURES OF THE PAIN EXPERIENCE: Sensory discriminative Affective (emotional)
Prescription Pain Management. University of Hawai i Hilo Pre- Nursing Program NURS 203 General Pharmacology Danita 1 Narciso Pharm D
 Prescription Pain Management University of Hawai i Hilo Pre- Nursing Program NURS 203 General Pharmacology Danita 1 Narciso Pharm D 2 Objectives Understand how to preform a pain assessment Know which medications
Prescription Pain Management University of Hawai i Hilo Pre- Nursing Program NURS 203 General Pharmacology Danita 1 Narciso Pharm D 2 Objectives Understand how to preform a pain assessment Know which medications
Slide 1. Slide 2. Slide 3. Opioid (Narcotic) Analgesics and Antagonists. Lesson 6.1. Lesson 6.1. Opioid (Narcotic) Analgesics and Antagonists
 Analgesics and Antagonists. Lesson 6.1. Lesson 6.1. Opioid (Narcotic) Analgesics and Antagonists") Slide 1 Opioid (Narcotic) Analgesics and Antagonists Chapter 6 1 Slide 2 Lesson 6.1 Opioid (Narcotic) Analgesics and Antagonists 1. Explain the classification, mechanism of action, and pharmacokinetics
Slide 1 Opioid (Narcotic) Analgesics and Antagonists Chapter 6 1 Slide 2 Lesson 6.1 Opioid (Narcotic) Analgesics and Antagonists 1. Explain the classification, mechanism of action, and pharmacokinetics
PAIN IS A SUBJECTIVE EXPERIENCE: It is not a stimulus. MAJOR FEATURES OF THE PAIN EXPERIENCE: Sensory discriminative Affective (emotional) Cognitive
 Cognitive") PAIN PAIN IS A SUBJECTIVE EXPERIENCE: It is not a stimulus MAJOR FEATURES OF THE PAIN EXPERIENCE: Sensory discriminative Affective (emotional) Cognitive MEASUREMENT OF PAIN: A BIG PROBLEM Worst pain ever
PAIN PAIN IS A SUBJECTIVE EXPERIENCE: It is not a stimulus MAJOR FEATURES OF THE PAIN EXPERIENCE: Sensory discriminative Affective (emotional) Cognitive MEASUREMENT OF PAIN: A BIG PROBLEM Worst pain ever
Objectives. Opioid Free Anesthesia Surgery without opioids. Opioid Use In The United States
 Opioid Free Anesthesia Surgery without opioids 2 Objectives Review of pain physiology Evaluate need for continuing opioid substitution therapy Review Neuraxial and Periperal Regional Anesthesia Learn ways
Opioid Free Anesthesia Surgery without opioids 2 Objectives Review of pain physiology Evaluate need for continuing opioid substitution therapy Review Neuraxial and Periperal Regional Anesthesia Learn ways
3/1/2018. Disclosures. Objectives. Clinical advisory board member- Daiichi Sankyo
 Adjuvant pain medications in geriatrics Thomas B. Gregory, Pharm.D., BCPS, CPE, FASPE Clinical Pharmacy Specialist Pain Management CoxHealth Springfield, MO Disclosures Clinical advisory board member-
Adjuvant pain medications in geriatrics Thomas B. Gregory, Pharm.D., BCPS, CPE, FASPE Clinical Pharmacy Specialist Pain Management CoxHealth Springfield, MO Disclosures Clinical advisory board member-
Associate Professor Supranee Niruthisard Department of Anesthesiology Faculty of Medicine Chulalongkorn University January 21, 2008
 Associate Professor Supranee Niruthisard Department of Anesthesiology Faculty of Medicine Chulalongkorn University January 21, 2008 PAIN MECHANISMS Somatic Nociceptive Visceral Inflammatory response sensitizes
Associate Professor Supranee Niruthisard Department of Anesthesiology Faculty of Medicine Chulalongkorn University January 21, 2008 PAIN MECHANISMS Somatic Nociceptive Visceral Inflammatory response sensitizes
Somatosensory Physiology (Pain And Temperature) Richard M. Costanzo, Ph.D.
 Richard M. Costanzo, Ph.D.") Somatosensory Physiology (Pain And Temperature) Richard M. Costanzo, Ph.D. OBJECTIVES After studying the material of this lecture the student should be familiar with: 1. The relationship between nociception
Somatosensory Physiology (Pain And Temperature) Richard M. Costanzo, Ph.D. OBJECTIVES After studying the material of this lecture the student should be familiar with: 1. The relationship between nociception
POST OPERATIVE PAIN MANAGEMENT: PAIN AND COMPLICATIONS
 POST OPERATIVE PAIN MANAGEMENT: PAIN AND COMPLICATIONS November 9, 2018 Aimee LaMere, CNP Molly McNaughton, CNP Leslie Weide, MSW, LICSW, ACM Disclosures: Conflict of interest statement: We certify that,
POST OPERATIVE PAIN MANAGEMENT: PAIN AND COMPLICATIONS November 9, 2018 Aimee LaMere, CNP Molly McNaughton, CNP Leslie Weide, MSW, LICSW, ACM Disclosures: Conflict of interest statement: We certify that,
1 The Physiology of Pain
 1 The Physiology of Pain Rohit Juneja and Siân Jaggar Introduction Definitions Key Messages Pain is still underdiagnosed and undertreated. Pain is a subjective experience and may even be present in the
1 The Physiology of Pain Rohit Juneja and Siân Jaggar Introduction Definitions Key Messages Pain is still underdiagnosed and undertreated. Pain is a subjective experience and may even be present in the
Practical Management Of Osteoporosis
 Practical Management Of Osteoporosis CONFERENCE 2012 Education Centre, Bournemouth.19 November The following companies have given funding towards the cost of this meeting but have no input into the agenda
Practical Management Of Osteoporosis CONFERENCE 2012 Education Centre, Bournemouth.19 November The following companies have given funding towards the cost of this meeting but have no input into the agenda
PERIOPERATIVE PAIN MANAGEMENT: WHAT S UP WITH METHADONE?
 PERIOPERATIVE PAIN MANAGEMENT: WHAT S UP WITH METHADONE? Sandra Z Perkowski, VMD, PhD, DACVAA University of Pennsylvania, School of Veterinary Medicine, Philadelphia, PA Pre-emptive and multimodal use
PERIOPERATIVE PAIN MANAGEMENT: WHAT S UP WITH METHADONE? Sandra Z Perkowski, VMD, PhD, DACVAA University of Pennsylvania, School of Veterinary Medicine, Philadelphia, PA Pre-emptive and multimodal use
Neurobiology of Pain Adjuvant analgesia
 Neurobiology of Pain Adjuvant analgesia Jason Brooks Consultant Anaesthesia and Pain Management BCH March 2017 The Brief A broad overview of the abnormal and normal anatomy and physiology of pain pathways
Neurobiology of Pain Adjuvant analgesia Jason Brooks Consultant Anaesthesia and Pain Management BCH March 2017 The Brief A broad overview of the abnormal and normal anatomy and physiology of pain pathways
Acute pain management in opioid tolerant patients. Muhammad Laklouk
 Acute pain management in opioid tolerant patients Muhammad Laklouk General principles An adequate review and assessment Provision of effective analgesia (including attenuation of tolerance and hyperalgesia)
Acute pain management in opioid tolerant patients Muhammad Laklouk General principles An adequate review and assessment Provision of effective analgesia (including attenuation of tolerance and hyperalgesia)
Analgesics and Adjuvants for Pain Therapy
 Topics to be covered Analgesics and Adjuvants for Pain Therapy Chuthamanee C. Suthisisang BPharm, PhD Department of Pharmacology Faculty of Pharmacy Mahidol University Neurochemistry of pain Early pain
Topics to be covered Analgesics and Adjuvants for Pain Therapy Chuthamanee C. Suthisisang BPharm, PhD Department of Pharmacology Faculty of Pharmacy Mahidol University Neurochemistry of pain Early pain
Neuropathic Pain in Palliative Care
 Neuropathic Pain in Palliative Care Neuropathic Pain in Advanced Cancer Affects 40% of patients Multiple concurrent pains are common Often complex pathophysiology with mixed components Nocioceptive Neuropathic
Neuropathic Pain in Palliative Care Neuropathic Pain in Advanced Cancer Affects 40% of patients Multiple concurrent pains are common Often complex pathophysiology with mixed components Nocioceptive Neuropathic
Pathophysiology of Pain
 Pathophysiology of Pain Wound Inflammatory response Chemical mediators Activity in Pain Path PAIN http://neuroscience.uth.tmc.edu/s2/chapter08.html Chris Cohan, Ph.D. Dept. of Pathology/Anat Sci University
Pathophysiology of Pain Wound Inflammatory response Chemical mediators Activity in Pain Path PAIN http://neuroscience.uth.tmc.edu/s2/chapter08.html Chris Cohan, Ph.D. Dept. of Pathology/Anat Sci University
9/30/2017. Case Study: Complete Pain Assessment and Multimodal Approach to Pain Management. Program Objectives. Impact of Poorly Managed Pain
 Case Study: Complete Pain Assessment and Multimodal Approach to Pain Management MARY BETH PARTYKA MSN ADULT NURSE PRACTITIONER ADVOCATE CHRIST MEDICAL CENTER ADULT PAIN SERVICE Program Objectives Identify
Case Study: Complete Pain Assessment and Multimodal Approach to Pain Management MARY BETH PARTYKA MSN ADULT NURSE PRACTITIONER ADVOCATE CHRIST MEDICAL CENTER ADULT PAIN SERVICE Program Objectives Identify
Transition from acute to chronic pain
 A Feizerfan FRCA G Sheh BHB MBChB FAFRM(RACP) FFPMANZCA Matrix reference 3E00 Key points Physiology of pain involves activation and complex interactions of autonomic, peripheral and central nervous systems,
A Feizerfan FRCA G Sheh BHB MBChB FAFRM(RACP) FFPMANZCA Matrix reference 3E00 Key points Physiology of pain involves activation and complex interactions of autonomic, peripheral and central nervous systems,
Pain Management in the Surgical Patient. Peter Vogel, VMD, DACVS
 Pain Management in the Surgical Patient Peter Vogel, VMD, DACVS Pain Pathways u Specialized neurons that travel through the spinal cord u Free nerve endings in skin, connective tissue, muscle and bone
Pain Management in the Surgical Patient Peter Vogel, VMD, DACVS Pain Pathways u Specialized neurons that travel through the spinal cord u Free nerve endings in skin, connective tissue, muscle and bone
Anaesthesia and Pain Management for Endo Exo Femoral Prosthesis (EEFP) Bridging the Gap from Surgery to Rehabilitation
 Bridging the Gap from Surgery to Rehabilitation") Anaesthesia and Pain Management for Endo Exo Femoral Prosthesis (EEFP) Bridging the Gap from Surgery to Rehabilitation Dr Ajay Kumar Senior Lecturer Macquarie and Melbourne University Introduction Amputee
Anaesthesia and Pain Management for Endo Exo Femoral Prosthesis (EEFP) Bridging the Gap from Surgery to Rehabilitation Dr Ajay Kumar Senior Lecturer Macquarie and Melbourne University Introduction Amputee
Rational Polypharmacy
 Rational Polypharmacy Thomas B. Gregory, PharmD, BCPS, CPE, FASPE Disclosures Clinical advisory board: Daiichi Sankyo 1 Introduction Cox Health Ambulatory Pain Clinic Pharmacy Specialist Learning Objectives
Rational Polypharmacy Thomas B. Gregory, PharmD, BCPS, CPE, FASPE Disclosures Clinical advisory board: Daiichi Sankyo 1 Introduction Cox Health Ambulatory Pain Clinic Pharmacy Specialist Learning Objectives
A Pain Management Primer for Pharmacists. Jessica Geiger-Hayes, PharmD, BCPS, CPE Andrea Wetshtein, PharmD, BCPS, CPE
 A Pain Management Primer for Pharmacists Jessica Geiger-Hayes, PharmD, BCPS, CPE Andrea Wetshtein, PharmD, BCPS, CPE Objectives Discuss the differences between somatic, visceral, and neuropathic pain Design
A Pain Management Primer for Pharmacists Jessica Geiger-Hayes, PharmD, BCPS, CPE Andrea Wetshtein, PharmD, BCPS, CPE Objectives Discuss the differences between somatic, visceral, and neuropathic pain Design
Understanding pain and mental illness Impact on management principles
 Understanding pain and mental illness Impact on management principles Chris Alderman Consultant Psychopharmacologist Pain and mental illness - context PAIN MENTAL ILLNESS OTHER FACTORS (personality, history.
Understanding pain and mental illness Impact on management principles Chris Alderman Consultant Psychopharmacologist Pain and mental illness - context PAIN MENTAL ILLNESS OTHER FACTORS (personality, history.
POST-OP MULTIMODAL PAIN MANAGEMENT. Maripat Welz-Bosna Reading Hospital Medical Center Department of Medicine Hospitalist Services/Pain Management
 POST-OP MULTIMODAL PAIN MANAGEMENT Maripat Welz-Bosna Reading Hospital Medical Center Department of Medicine Hospitalist Services/Pain Management Objectives Understand the basic neurobiology of the pain
POST-OP MULTIMODAL PAIN MANAGEMENT Maripat Welz-Bosna Reading Hospital Medical Center Department of Medicine Hospitalist Services/Pain Management Objectives Understand the basic neurobiology of the pain
Analgesic Drugs PHL-358-PHARMACOLOGY AND THERAPEUTICS-I. Mr.D.Raju,M.pharm, Lecturer
 Analgesic Drugs PHL-358-PHARMACOLOGY AND THERAPEUTICS-I Mr.D.Raju,M.pharm, Lecturer Mechanisms of Pain and Nociception Nociception is the mechanism whereby noxious peripheral stimuli are transmitted to
Analgesic Drugs PHL-358-PHARMACOLOGY AND THERAPEUTICS-I Mr.D.Raju,M.pharm, Lecturer Mechanisms of Pain and Nociception Nociception is the mechanism whereby noxious peripheral stimuli are transmitted to
SOMATOSENSORY SYSTEMS AND PAIN
 SOMATOSENSORY SYSTEMS AND PAIN A 21 year old man presented with a stab wound of the right side of the neck (Panel A). Neurological examination revealed right hemiplegia and complete right-sided loss of
SOMATOSENSORY SYSTEMS AND PAIN A 21 year old man presented with a stab wound of the right side of the neck (Panel A). Neurological examination revealed right hemiplegia and complete right-sided loss of
The anatomy and physiology of pain
 The anatomy and physiology of pain Charlotte E Steeds Abstract Pain is an unpleasant experience that results from both physical and psychological responses to injury. A complex set of pathways transmits
The anatomy and physiology of pain Charlotte E Steeds Abstract Pain is an unpleasant experience that results from both physical and psychological responses to injury. A complex set of pathways transmits
Fibromyalgia: Current Trends and Concepts
 Fibromyalgia: Current Trends and Concepts Dr. Brian Kahan Fellow American Academy of Physical Medicine and Rehabilitation Diplomat American Academy of Pain Medicine American College of Rheumatology (ACR)
Fibromyalgia: Current Trends and Concepts Dr. Brian Kahan Fellow American Academy of Physical Medicine and Rehabilitation Diplomat American Academy of Pain Medicine American College of Rheumatology (ACR)
Non-opioid and adjuvant pain management
 Non-opioid and adjuvant pain management ALLISON JORDAN, MD, HMDC MEDICAL DIRECTOR OF PALLIATIVE CARE SERVICES CHRISTIAN AND ALTON MEMORIAL HOSPITALS ASSOCIATE MEDICAL DIRECTOR, BJC HOSPICE ASSISTANT PROFESSOR
Non-opioid and adjuvant pain management ALLISON JORDAN, MD, HMDC MEDICAL DIRECTOR OF PALLIATIVE CARE SERVICES CHRISTIAN AND ALTON MEMORIAL HOSPITALS ASSOCIATE MEDICAL DIRECTOR, BJC HOSPICE ASSISTANT PROFESSOR
niap Terms and Definitions
 Our topic today is about analgesics. niap General concept: pain brings patients to the Doctors at the same time. Fear from the pain can keep the patient from going to the Doctors at appropriate time. We
Our topic today is about analgesics. niap General concept: pain brings patients to the Doctors at the same time. Fear from the pain can keep the patient from going to the Doctors at appropriate time. We
Management of Chronic Pain in Children. Objectives: Common Myths about Pain. University of Texas Health Science Center at San Antonio, Texas
 Management of Chronic Pain in Children I have no disclosures. Glen Medellin, MD Cure sometimes, treat often, comfort always. Hippocrates Objectives: The number of children admitted with chronic pain has
Management of Chronic Pain in Children I have no disclosures. Glen Medellin, MD Cure sometimes, treat often, comfort always. Hippocrates Objectives: The number of children admitted with chronic pain has
PAIN. Physiology of pain relating to pain management
 PAIN Physiology of pain relating to pain management What is pain? An unpleasant sensory and emotional experience associated with actual or potential tissue damage. (Melzac and Wall) The generation of pain
PAIN Physiology of pain relating to pain management What is pain? An unpleasant sensory and emotional experience associated with actual or potential tissue damage. (Melzac and Wall) The generation of pain
Practical Pain Management Leah Centanni, MSN, FNP-C, Asst. Clinical Professor CANP Conference March 22, 2014
 Practical Pain Management Leah Centanni, MSN, FNP-C, Asst. Clinical Professor CANP Conference March 22, 2014 Overview Types of Pain Physical Examination of Pain Pharmacologic Approach in Pain Management
Practical Pain Management Leah Centanni, MSN, FNP-C, Asst. Clinical Professor CANP Conference March 22, 2014 Overview Types of Pain Physical Examination of Pain Pharmacologic Approach in Pain Management
CHAMP: Bedside Teaching TREATING PAIN. Stacie Levine MD. What is the approach to treating pain in the aging adult patient?
 CHAMP: Bedside Teaching TREATING PAIN Stacie Levine MD Teaching Trigger: An older adult patient is identified as having pain. Clinical Question: What is the approach to treating pain in the aging adult
CHAMP: Bedside Teaching TREATING PAIN Stacie Levine MD Teaching Trigger: An older adult patient is identified as having pain. Clinical Question: What is the approach to treating pain in the aging adult
@FeliciaJCox. Caring for the person with addiction in the acute pain setting. Felicia Cox FRCN MSc RN
 @FeliciaJCox Caring for the person with addiction in the acute pain setting Felicia Cox FRCN MSc RN Disclosures Editor - British Journal of Pain Associate Editor - Pain Clinical Updates (IASP PAIN Reports)
@FeliciaJCox Caring for the person with addiction in the acute pain setting Felicia Cox FRCN MSc RN Disclosures Editor - British Journal of Pain Associate Editor - Pain Clinical Updates (IASP PAIN Reports)
IF I M NOT TREATING WITH OPIOIDS, THEN WHAT AM I SUPPOSED TO USE?
 NON-OPIOID TREATMENT OPTIONS FOR CHRONIC PAIN Alison Knutson, PharmD, BCACP Medication Management Pharmacist Park Nicollet Creekside Clinic Dr. Knutson indicated no potential conflict of interest to this
NON-OPIOID TREATMENT OPTIONS FOR CHRONIC PAIN Alison Knutson, PharmD, BCACP Medication Management Pharmacist Park Nicollet Creekside Clinic Dr. Knutson indicated no potential conflict of interest to this
Inpatient Management of Trauma Related Pain
 Inpatient Management of Trauma Related Pain STOMP Summit September 9, 2016 Ann O Rourke, MD, MPH University of Wisconsin Department of Surgery 1 Our patient Small SDH Intubated Hemopneumothorax with multiple
Inpatient Management of Trauma Related Pain STOMP Summit September 9, 2016 Ann O Rourke, MD, MPH University of Wisconsin Department of Surgery 1 Our patient Small SDH Intubated Hemopneumothorax with multiple
Pathophysiology of Pain. Ramon Go MD Assistant Professor Anesthesiology and Pain medicine NYP-CUMC
 Pathophysiology of Pain Ramon Go MD Assistant Professor Anesthesiology and Pain medicine NYP-CUMC Learning Objectives Anatomic pathway of nociception Discuss the multiple target sites of pharmacological
Pathophysiology of Pain Ramon Go MD Assistant Professor Anesthesiology and Pain medicine NYP-CUMC Learning Objectives Anatomic pathway of nociception Discuss the multiple target sites of pharmacological
Multimodal analgesic therapy has gained widespread
 TOPICAL REVIEW Analgesia for Anesthetized Patients Kip A. Lemke, DVM, MSc, Dipl. ACVA, and Catherine M. Creighton, DVM Many perioperative pain management protocols for cats and dogs are overly complex,
TOPICAL REVIEW Analgesia for Anesthetized Patients Kip A. Lemke, DVM, MSc, Dipl. ACVA, and Catherine M. Creighton, DVM Many perioperative pain management protocols for cats and dogs are overly complex,
Screening - inclusion criteria
 A Date of data collection: B Time of data collection: C Ward where data is collected: 2 0 1 Y M M D D H H M M D Research assistant Code: Patient code (local): Room number: Screening - inclusion criteria
A Date of data collection: B Time of data collection: C Ward where data is collected: 2 0 1 Y M M D D H H M M D Research assistant Code: Patient code (local): Room number: Screening - inclusion criteria
2018 Learning Outcomes
 I. Pain Physiology and Anatomy (20%) A. Describe the basic anatomy of the nervous system. B. Describe the physiological mechanisms of neuronal function (eg- action potentials). C. Review the nociceptive
I. Pain Physiology and Anatomy (20%) A. Describe the basic anatomy of the nervous system. B. Describe the physiological mechanisms of neuronal function (eg- action potentials). C. Review the nociceptive
What do we want for pain medications?
 New Trends in Pain Pharmacotherapy Dr. Chi Wai Cheung MBBS(HK), FHKCA, FHKAM(Anaesthesiology), Dip Pain Mgt(HKCA) Clinical Assistant Professor Department of Anaesthesiology The University of Hong Kong
New Trends in Pain Pharmacotherapy Dr. Chi Wai Cheung MBBS(HK), FHKCA, FHKAM(Anaesthesiology), Dip Pain Mgt(HKCA) Clinical Assistant Professor Department of Anaesthesiology The University of Hong Kong
CANNABIS AND PAIN. Debra Kimless, M.D. Medical Director, ForwardGro MAOP Annual Meeting September 14, 2018
 CANNABIS AND PAIN Debra Kimless, M.D. Medical Director, ForwardGro MAOP Annual Meeting September 14, 2018 FDA APPROVAL: PREGABALIN, DULOXETINE, MILNACIPRAN FOR FIBROMYALGIA PREGABALIN, DULOXETINE FOR
CANNABIS AND PAIN Debra Kimless, M.D. Medical Director, ForwardGro MAOP Annual Meeting September 14, 2018 FDA APPROVAL: PREGABALIN, DULOXETINE, MILNACIPRAN FOR FIBROMYALGIA PREGABALIN, DULOXETINE FOR
Postoperative Pain Management. Nimmaanrat S, MD, FRCAT, MMed (Pain Mgt)
") Postoperative Pain Management Nimmaanrat S, MD, FRCAT, MMed (Pain Mgt) Topics to be Covered Definition Neurobiology Classification Multimodal analgesia Preventive analgesia Step down approach Measurement
Postoperative Pain Management Nimmaanrat S, MD, FRCAT, MMed (Pain Mgt) Topics to be Covered Definition Neurobiology Classification Multimodal analgesia Preventive analgesia Step down approach Measurement
Screening - inclusion criteria
 PAIN OUT Community research EU ROP EAN COMMISSION A Date of data collection: B Time of data collection: C Ward where data is collected: 2 0 1 Y M M D D H H M M D Research assistant Code: Room number: Screening
PAIN OUT Community research EU ROP EAN COMMISSION A Date of data collection: B Time of data collection: C Ward where data is collected: 2 0 1 Y M M D D H H M M D Research assistant Code: Room number: Screening
Last time we talked about the descending pathways of pain and the ALS. Today we will continue talking about these descending pathways.
 Last time we talked about the descending pathways of pain and the ALS. Today we will continue talking about these descending pathways. Each higher level will control the level under It. In controlling
Last time we talked about the descending pathways of pain and the ALS. Today we will continue talking about these descending pathways. Each higher level will control the level under It. In controlling
Acute Pain Management
 Acute Pain Management Dr Zamil Karim MBBS, FANZCA,FFPMANZCA, FIPP The journey to Acute pain management begins in the perioperative period. The evaluation and assessment occurs in the perioperative period
Acute Pain Management Dr Zamil Karim MBBS, FANZCA,FFPMANZCA, FIPP The journey to Acute pain management begins in the perioperative period. The evaluation and assessment occurs in the perioperative period
Narcotic Analgesics. Jacqueline Morgan March 22, 2017
 Narcotic Analgesics Jacqueline Morgan March 22, 2017 Pain Unpleasant sensory and emotional experience with actual or potential tissue damage Universal, complex, subjective experience Number one reason
Narcotic Analgesics Jacqueline Morgan March 22, 2017 Pain Unpleasant sensory and emotional experience with actual or potential tissue damage Universal, complex, subjective experience Number one reason
The WHY and HOW of Acute Pain Control
 The WHY and HOW of Acute Pain Control James S. Gaynor, DVM, MS, DACVAA, DAAPM Frisco, CO USA jgaynor@nopetpain.com www.peakvets.com Principles of Pain Management Pain control is good medicine Pre-emptive,
The WHY and HOW of Acute Pain Control James S. Gaynor, DVM, MS, DACVAA, DAAPM Frisco, CO USA jgaynor@nopetpain.com www.peakvets.com Principles of Pain Management Pain control is good medicine Pre-emptive,
SUMMARY OF ARIZONA OPIOID PRESCRIBING GUIDELINES FOR THE TREATMENT OF CHRONIC NON-TERMINAL PAIN (CNTP)
") 9 SUMMARY OF ARIZONA OPIOID PRESCRIBING GUIDELINES FOR THE TREATMENT OF CHRONIC NON-TERMINAL PAIN (CNTP) SUMMARY OF ARIZONA OPIOID PRESCRIBING GUIDELINES FOR THE TREATMENT OF ACUTE PAIN NONOPIOID TREATMENTS
9 SUMMARY OF ARIZONA OPIOID PRESCRIBING GUIDELINES FOR THE TREATMENT OF CHRONIC NON-TERMINAL PAIN (CNTP) SUMMARY OF ARIZONA OPIOID PRESCRIBING GUIDELINES FOR THE TREATMENT OF ACUTE PAIN NONOPIOID TREATMENTS
21 st June BDS BASHD Therapeutics Pain and Analgesia. BASHD Therapeutics Analgesics and Pain Management. Links to other BASHD content
 Volume of Prescribing by Dentists 2011 ( a reminder) BASHD Therapeutics Analgesics and Pain Management Analgesics account for 1 in 80 dental prescriptions made A lot more analgesics will be suggested for
Volume of Prescribing by Dentists 2011 ( a reminder) BASHD Therapeutics Analgesics and Pain Management Analgesics account for 1 in 80 dental prescriptions made A lot more analgesics will be suggested for
Pain Mechanisms. Prof Michael G Irwin MD, FRCA, FANZCA FHKAM Head Department of Anaesthesiology University of Hong Kong. The Somatosensory System
 ain Mechanisms rof Michael G Irwin MD, FRCA, FANZCA FHKAM Head Department of Anaesthesiology University of Hong Kong The Somatosensory System Frontal cortex Descending pathway eriaqueductal gray matter
ain Mechanisms rof Michael G Irwin MD, FRCA, FANZCA FHKAM Head Department of Anaesthesiology University of Hong Kong The Somatosensory System Frontal cortex Descending pathway eriaqueductal gray matter
If Not Opioids then LEAH EDMONDS CSHP OCTOBER 26, 2017
 If Not Opioids then what LEAH EDMONDS CSHP OCTOBER 26, 2017 Disclosure Nothing to disclose Objectives Identify various non-opioid options for the treatment of chronic non cancer pain Choose appropriate
If Not Opioids then what LEAH EDMONDS CSHP OCTOBER 26, 2017 Disclosure Nothing to disclose Objectives Identify various non-opioid options for the treatment of chronic non cancer pain Choose appropriate
THE OPIUM POPPY OPIOID PHARMACOLOGY 2/18/16. PCTH 300/305 Andrew Horne, PhD MEDC 309. Papaver somniferum. Poppy Seeds Opiates
 OPIOID PHARMACOLOGY PCTH 300/305 Andrew Horne, PhD andrew.horne@ubc.ca MEDC 309 THE OPIUM POPPY Papaver somniferum Sleep-bringing poppy Poppy Seeds Opiates Opium Poppy Straw 1 OPIATES VS. OPIOIDS Opiates:
OPIOID PHARMACOLOGY PCTH 300/305 Andrew Horne, PhD andrew.horne@ubc.ca MEDC 309 THE OPIUM POPPY Papaver somniferum Sleep-bringing poppy Poppy Seeds Opiates Opium Poppy Straw 1 OPIATES VS. OPIOIDS Opiates:
Karam Darwish. Dr. Munir. Munir Gharaibeh
 7 Karam Darwish Dr. Munir Munir Gharaibeh Opioid Analgesics Pain is an important symptom as it is usually the symptom that brings the patient to the hospital, and an Analgesic is a drug used to relieve
7 Karam Darwish Dr. Munir Munir Gharaibeh Opioid Analgesics Pain is an important symptom as it is usually the symptom that brings the patient to the hospital, and an Analgesic is a drug used to relieve
Steven Richeimer, M.D.
 Steven Richeimer, M.D. Associate Professor of Anesthesiology & Psychiatry Chief, Division of Pain Medicine Keck School of Medicine, USC Los Angeles, CA 323-442-6202 www.helpforpain.com Pain Light touch
Steven Richeimer, M.D. Associate Professor of Anesthesiology & Psychiatry Chief, Division of Pain Medicine Keck School of Medicine, USC Los Angeles, CA 323-442-6202 www.helpforpain.com Pain Light touch
SEEING KETAMINE IN A NEW LIGHT
 SEEING KETAMINE IN A NEW LIGHT BobbieJean Sweitzer, M.D., FACP Professor of Anesthesiology Director of Perioperative Medicine Northwestern University Bobbie.Sweitzer@northwestern.edu LEARNING OBJECTIVES
SEEING KETAMINE IN A NEW LIGHT BobbieJean Sweitzer, M.D., FACP Professor of Anesthesiology Director of Perioperative Medicine Northwestern University Bobbie.Sweitzer@northwestern.edu LEARNING OBJECTIVES
3/15/2018. Pain. Pain. Opioid Analgesics Addiction. Pain
 Pain Pain Well, I guess that explains the abdominal pains. Well, I guess that explains the abdominal pains. Pain is a component of virtually all clinical strategies, and management of pain is a primary
Pain Pain Well, I guess that explains the abdominal pains. Well, I guess that explains the abdominal pains. Pain is a component of virtually all clinical strategies, and management of pain is a primary
211MDS Pain theories
 211MDS Pain theories Definition In 1986, the International Association for the Study of Pain (IASP) defined pain as a sensory and emotional experience associated with real or potential injuries, or described
211MDS Pain theories Definition In 1986, the International Association for the Study of Pain (IASP) defined pain as a sensory and emotional experience associated with real or potential injuries, or described
Agonists: morphine, fentanyl Agonists-Antagonists: nalbuphine Antagonists: naloxone
 Opioid Definition All drugs, natural or synthetic, that bind to opiate receptors Agonists: morphine, fentanyl Agonists-Antagonists: nalbuphine Antagonists: naloxone Opioid agonists increase pain threshold
Opioid Definition All drugs, natural or synthetic, that bind to opiate receptors Agonists: morphine, fentanyl Agonists-Antagonists: nalbuphine Antagonists: naloxone Opioid agonists increase pain threshold
Introduction to some interesting research questions: Molecular biology of the primary afferent nociceptor
 Introduction to some interesting research questions: Molecular biology of the primary afferent nociceptor NOCICEPTORS ARE NOT IDENTICAL PEPTIDE SubP/CGRP Trk A NON-PEPTIDE IB4 P2X 3 c-ret Snider and McMahon
Introduction to some interesting research questions: Molecular biology of the primary afferent nociceptor NOCICEPTORS ARE NOT IDENTICAL PEPTIDE SubP/CGRP Trk A NON-PEPTIDE IB4 P2X 3 c-ret Snider and McMahon
Pain classifications slow and fast
 Pain classifications slow and fast Fast Pain Slow Pain Sharp, pricking (Aδ) fiber Short latency Well localized Short duration Dull, burning (C) fiber Slower onset Diffuse Long duration Less emotional Emotional,
Pain classifications slow and fast Fast Pain Slow Pain Sharp, pricking (Aδ) fiber Short latency Well localized Short duration Dull, burning (C) fiber Slower onset Diffuse Long duration Less emotional Emotional,
Presentation objectives. Overcoming Acute Pain Management Hurdles in the Tertiary Setting The High Risk Patient
 Overcoming Acute Pain Management Hurdles in the Tertiary Setting The High Risk Patient Ewan McNicol PharmD, MS Presentation objectives Outline principles for management of acute pain, with focus on perioperative
Overcoming Acute Pain Management Hurdles in the Tertiary Setting The High Risk Patient Ewan McNicol PharmD, MS Presentation objectives Outline principles for management of acute pain, with focus on perioperative
The Nervous System. Anatomy of a Neuron
 The Nervous System Chapter 38.1-38.5 Anatomy of a Neuron I. Dendrites II. Cell Body III. Axon Synaptic terminal 1 Neuron Connections dendrites cell body terminal cell body cell body terminals dendrites
The Nervous System Chapter 38.1-38.5 Anatomy of a Neuron I. Dendrites II. Cell Body III. Axon Synaptic terminal 1 Neuron Connections dendrites cell body terminal cell body cell body terminals dendrites
Treating Pain and Depression
 Treating Pain and Depression Without Getting Depressed Joseph P, Arpaia, MD www.jparpaiamd.com More than 50% of patients with chronic pain also have clinically significant depression. Interestingly that
Treating Pain and Depression Without Getting Depressed Joseph P, Arpaia, MD www.jparpaiamd.com More than 50% of patients with chronic pain also have clinically significant depression. Interestingly that
The Nervous System Mark Stanford, Ph.D.
 The Nervous System Functional Neuroanatomy and How Neurons Communicate Mark Stanford, Ph.D. Santa Clara Valley Health & Hospital System Addiction Medicine and Therapy Services The Nervous System In response
The Nervous System Functional Neuroanatomy and How Neurons Communicate Mark Stanford, Ph.D. Santa Clara Valley Health & Hospital System Addiction Medicine and Therapy Services The Nervous System In response
Intraspinal (Neuraxial) Analgesia Community Nurses Competency Test
 Analgesia Community Nurses Competency Test") Intraspinal (Neuraxial) Analgesia Community Nurses Competency Test 1 Intraspinal (Neuraxial) Analgesia for Community Nurses Competency Test 1) Name the two major classifications of pain. i. ii. 2) Neuropathic
Intraspinal (Neuraxial) Analgesia Community Nurses Competency Test 1 Intraspinal (Neuraxial) Analgesia for Community Nurses Competency Test 1) Name the two major classifications of pain. i. ii. 2) Neuropathic
BEYOND OPIOIDS: ADJUNCTS FOR TREATING PAIN
 BEYOND OPIOIDS: ADJUNCTS FOR TREATING PAIN Ronald Januchowski, D.O. 2017 Objectives By the end of the presentation, the learner should be able to: Summarize the risks of opiates when used for non-cancer
BEYOND OPIOIDS: ADJUNCTS FOR TREATING PAIN Ronald Januchowski, D.O. 2017 Objectives By the end of the presentation, the learner should be able to: Summarize the risks of opiates when used for non-cancer
Goals for sedation during mechanical ventilation
 New Uses of Old Medications Gina Riggi, PharmD, BCCCP, BCPS Clinical Pharmacist Trauma ICU Jackson Memorial Hospital Disclosure I do not have anything to disclose Objectives Describe the use of ketamine
New Uses of Old Medications Gina Riggi, PharmD, BCCCP, BCPS Clinical Pharmacist Trauma ICU Jackson Memorial Hospital Disclosure I do not have anything to disclose Objectives Describe the use of ketamine
MAT for Opioid Dependence. MAT and Pain Management. Epidemiology. Epidemiology. Factors Impacting Pain Perception 9/23/2014
 MAT for Opioid Dependence Methadone maintenance treatment (MMT) Buprenorphine/naloxone (suboxone) Buprenorhine/naloxone (BupNX) Buprenorphine SL Parenteral naltrexone (P-ntx) Oral naltrexone (ntx) MAT
MAT for Opioid Dependence Methadone maintenance treatment (MMT) Buprenorphine/naloxone (suboxone) Buprenorhine/naloxone (BupNX) Buprenorphine SL Parenteral naltrexone (P-ntx) Oral naltrexone (ntx) MAT
Update on Pain: Collaborative Care for the Complex Patient
 Update on Pain: Collaborative Care for the Complex Patient Nirmala R. Abraham, MD Medical Director Sycamore Pain Management Center Kettering Health Network Objectives Standardized approach to patient care
Update on Pain: Collaborative Care for the Complex Patient Nirmala R. Abraham, MD Medical Director Sycamore Pain Management Center Kettering Health Network Objectives Standardized approach to patient care
EEK 16. MPharm Programme PAIN & ANALGESIA. Dr Abdel Ennaceur. Slide 1 of 78 M14 Pain Lecture notes
 MPharm Programme PAIN & ANALGESIA Dr Abdel Ennaceur Slide 1 of 78 M14 Pain Lecture notes WEEK Terminology Tract: collection of axons in the CNS Nucleus:(nuclei, plural) collection of neuron cell bodies
MPharm Programme PAIN & ANALGESIA Dr Abdel Ennaceur Slide 1 of 78 M14 Pain Lecture notes WEEK Terminology Tract: collection of axons in the CNS Nucleus:(nuclei, plural) collection of neuron cell bodies
Hurts So Good! The Concept of Pain and Pain Management. The Concept of Pain. The Concept of Pain. Program Learning Objectives
 Program Learning Objectives Hurts So Good! Management of Dental Pain and Patient Care Considerations Thomas A. Viola, R.Ph., C.C.P. Fourth District Dental Society May 22, 2015 2015 Thomas A. Viola, R.Ph.
Program Learning Objectives Hurts So Good! Management of Dental Pain and Patient Care Considerations Thomas A. Viola, R.Ph., C.C.P. Fourth District Dental Society May 22, 2015 2015 Thomas A. Viola, R.Ph.
WITHDRAWING FROM BUPRENORPHINE THERAPY
 WITHDRAWING FROM BUPRENORPHINE THERAPY VARIOUS REASONS TO STOP BUPRENORPHINE pregnancy and lactation emergency surgery/elective surgery difficult to manage side effects of buprenorphine patients showing
WITHDRAWING FROM BUPRENORPHINE THERAPY VARIOUS REASONS TO STOP BUPRENORPHINE pregnancy and lactation emergency surgery/elective surgery difficult to manage side effects of buprenorphine patients showing
Cancer-induced bone pain
 Cancer-induced bone pain Common Prevalent in particular cancers: breast (73%), prostate (68%), thyroid (42%), lung (36%), renal (35%), colon (5%) Correlates with an increased morbidity Reduced performance
Cancer-induced bone pain Common Prevalent in particular cancers: breast (73%), prostate (68%), thyroid (42%), lung (36%), renal (35%), colon (5%) Correlates with an increased morbidity Reduced performance
Somatic Sensory System I. Background
 Somatic Sensory System I. Background A. Differences between somatic senses and other senses 1. Receptors are distributed throughout the body as opposed to being concentrated at small, specialized locations
Somatic Sensory System I. Background A. Differences between somatic senses and other senses 1. Receptors are distributed throughout the body as opposed to being concentrated at small, specialized locations
Basics of Pharmacology
 Basics of Pharmacology Pekka Rauhala Transmed 2013 What is pharmacology? Pharmacology may be defined as the study of the effects of drugs on the function of living systems Pharmacodynamics The mechanism(s)
Basics of Pharmacology Pekka Rauhala Transmed 2013 What is pharmacology? Pharmacology may be defined as the study of the effects of drugs on the function of living systems Pharmacodynamics The mechanism(s)