Supportive Care for the Person with Chronic Kidney Disease. Dr. J. Kappel May 2014
|
|
|
- Clifton Gilbert
- 6 years ago
- Views:
Transcription
1 Supportive Care for the Person with Chronic Kidney Disease Dr. J. Kappel May 2014
2 Objectives 1 To develop an understanding of renal replacement therapy (RRT) and comprehensive conservative management and why they are chosen 2
3 Objectives 2 To provide a framework for appropriate care for those people with chronic kidney disease (CKD) who chose not to initiate RRT or for those who chose to terminate RRT. 3
4 Objectives 1 To develop an understanding of renal replacement therapy (RRT) and comprehensive conservative management and why they are chosen 4
5 Chronic Kidney Disease - Stages Stage 1 Description Kidney Damage with Normal or GFR GFR (ml/min/1.73 m 2 ) >90 2 Mild GFR Moderate GFR Severe GFR Kidney Failure <15 or Dialysis 5 Adapted from Am J Kidney Dis 2002; 39 (2, Suppl. 1): S46-S75
6 When do you initiate RRT? Uremic symptoms Pruritus, restless legs, altered appetite Weight loss Uncontrolled hyperkalemia, acidosis, pulmonary edema Signs - pericardial friction rub, neuropathy, encephalopathy Numbers - CrCl 6 mls/min in absence of anything else CMAJ February
7 Incident ESRD Patients by Age 800 R P M P Source: CORR Annual Report
8 Primary Diagnosis of Incident ESRD Patients 60 R P M P Diabetes RVD GN PCKD Source: CORR Annual Report
9 Dialysis Treatment for ESRD Peritoneal Dialysis Hemodialysis In Hospital In Satellite unit At home Transplantation Comprehensive Conservative Management 9

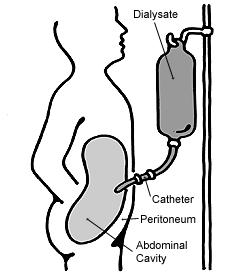
10 Peritoneal Dialysis 10


11 Hemodialysis 11
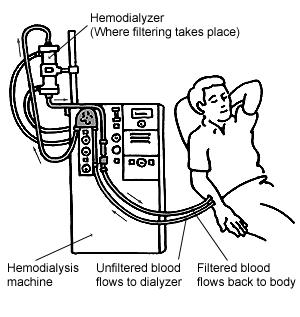

12 Hemodialysis 12

13 Transplantation 13
14 Comprehensive Conservative Management Interdisciplinary care model Provide excellent symptom control Strengthen psychosocial and spiritual support Focus on quality of life for patient and family Allow for a smooth transition to palliative and hospice care 14
15 Process for Choosing Treatment CCM vs RRT 1 Transplant Dialysis 2 Home Hospital/Clinic 3 HD PD 4 Conventional Nocturnal CAPD 5 5 Short Daily CPD Adapted from: Golper et al Seminars in Dialysis Vol 26, No 2l 15
16 Factors to consider Patient Factors Values and preferences Prognosis Physical factors: abdominal surgeries, peripheral vascular disease, other comorbid conditions Support system System Factors Capacity Knowledge Financial Potential to harm Collaborative decision between patient, family and healthcare team 16
17 Potential Medical, Emotional and Social Harms Related to Dialysis Medical Complications of vascular/peritoneal access Infections/sepsis Acceleration of renal failure Dialysis trial Worsening of pre-existing vascular disease including dementia Functional decline in frail and vulnerable people Pain with needles Prolonged immobilization Dialysis related muscle cramps, fatigue, headache, chronic low back pain Generally feeling unwell Adapted from: Should an Elderly Patient with Stage V CKD and Dementia be started on Dialysis? Irene Ying, Zoe Levitt, Sarbjit Vanita Jassal 17
18 Potential Medical, Emotional and Social Harms Related to Dialysis Emotional and Social Time and cost commuting to dialysis center Limited to no employment opportunities Social and cultural isolation Movement from place of residence Inability or reduced ability to travel for leisure Medicalization of death Adapted from: Should an Elderly Patient with Stage V CKD and Dementia be started on Dialysis? Irene Ying, Zoe Levitt, Sarbjit Vanita Jassal 18
19 Prognosis in ESRD Most patients and physicians tend to overestimate survival Many patients and health care providers are reluctant to discuss prognosis Lack of confidence in predicting prognosis Fear of abolishing hope Discomfort with such discussions Estimating prognosis is vital to decision making about starting and stopping dialysis Needs to be part of the discussion when deciding about options 19
20 Prognosis in ESRD Trajectory of illness Mortality risk factors 20
21 Trajectory of Illness Models exist for chronic lung disease, heart failure, stroke and diabetes Acute declines are common among dialysis patients hospitalized for: Acute MI Limb amputation Sepsis from hemodialysis lines Hip fractures Functional status declines, risk of death increases Burden of therapy outweighs benefits in many cases 21
22 Trajectory of Illness Advance Care Planning in CKD/ESRD: An Evolving Process Jean L. Holley 22
23 Low serum albumin Mortality Risk Factors Consistent and strong predictor of death Poor functional status Highly predictive of early death Comorbid conditions ischemic heart disease, cancer, peripheral vascular disease, dementia and diabetes Modified Charlson Comorbidity Index Composite score of age and multiple comorbid conditions The risk of a 40-year old on dialysis dying from a myocardial infarction is about 100 times greater than the risk for a person the same age with normal renal function 23

24 Patient age Mortality Risk Factors O Hare et al 24

25 Mortality Risk Factors Tamara KI
26 Mortality Risk Factors Answering NO to the surprise question Would you be surprised if this patient died within the next 12 months? 26
27 Online calculators Prognosis in ESRD Exact prognosis for an individual may be unclear These prognostic tools can aid in advance care planning Do the patients want this information Canadian study in CKD clinic: 97% wanted this information, but mostly Caucasian US study: 51% wanted this information, more ethnically diverse 27
28 Prognosis 28
29 Should an Elderly Patient with Stage V CKD and Dementia be started on Dialysis? Irene Ying, Zoe Levitt, Sarbjit Vanita Jassal 29
30 Objectives 1 To develop an understanding of renal replacement therapy (RRT) and comprehensive conservative management and why they are chosen 30
31 Objectives 2 To provide a framework for appropriate care for those people with chronic kidney disease (CKD) who chose not to initiate RRT or for those who chose to terminate RRT. 31
32 Those who choose not to initiate RRT Can live for months and even years after making this decision Interdisciplinary care includes: Diet Anemia management Blood pressure control Symptom control Psychological/spiritual support Death from renal failure is NOT PAINFUL 32
33 Those who choose to stop RRT The option of withdrawing from dialysis is an appropriate topic to be discussed by nephrologists/health care providers whenever a patient or family member mentions it and when patients suffer irreversible, profound neurologic impairment. About 20 25% of patients per year choose to stop dialysis The burden of therapy now outweighs any expectation of benefit and we are simply prolonging death 33
34 Framework for Appropriate Care Interdisciplinary team care Identifying patients with poor prognosis either before RRT or during the course of RRT and thus in need of supportive care Advance care planning Symptom assessment and management Care of the dying patient Bereavement processes for families and staff 34
35 Clinical Practice Guideline Renal Physicians Association Shared Decision Making in the Appropriate Initiation of and Withdrawal from Dialysis Kidney End-of-Life Coalition 35
36 Once dialysis is stopped Death can occur fairly quickly or the patient may live for several weeks depending on the amount of residual renal function. Average life span is about 7 days. Range 1 49 days. Certain subsets of the population seem to have especially short survival: Patients who are admitted to hospital or inpatient hospice unit. Patients who are bed bound with altered level of consciousness. Patients with edema have shorter survival, suggesting that volume status affects prognosis. 36
37 Symptom Burden Extensive Severe Significantly impacts quality of life Patients often underreport their symptoms 37
38 Symptom Burden Modified Edmonton Symptom Assessment System 10 visual analogue scales with a superimposed 0 10 scale for pain, activity, nausea, pruritus, depression, anxiety, drowsiness, appetite, wellbeing and shortness of breath 38
39 39

40 Symptom assessment 40
41 Symptom Control - Pain Most common problem in all May be due to their primary disease PCKD Or to concurrent comorbidity diabetes, PVD Or to disease from their renal failure calciphylaxis, renal bone disease 41
42 Symptom Control - Pain Use of analgesics By mouth if possible By the clock given regularly By the ladder (next slide) For the individual No standard doses Attention to detail 42
43 WHO Analgesic Ladder Modified for safety in CKD patients Step 3: Severe Pain (7-10) Hydromorphone, Methadone, Fentanyl, Oxycodone + Nonopioid analgesics + Adjuvants Step 2: Moderate Pain (5-6) Hydromorphone, Oxycodone, Tramadol + Nonopioid analgesics + Adjuvants Step 1: Mild Pain (1-4) Acetaminophen + Adjuvants 43
44 WHO Analgesic Ladder Modified for safety in CKD patients Step 3: Severe Pain (7-10) Hydromorphone, Methadone, Fentanyl, Oxycodone + Nonopioid analgesics + Adjuvants Step 2: Moderate Pain (5-6) Hydromorphone, Oxycodone, Tramadol + Nonopioid analgesics + Adjuvants Step 1: Mild Pain (1-4) Acetaminophen + Adjuvants NSAIDs: Higher risk of bleeding but can be used 44
45 WHO Analgesic Ladder Modified for safety in CKD patients Step 3: Severe Pain (7-10) Hydromorphone, Methadone, Fentanyl, Oxycodone + Nonopioid analgesics + Adjuvants Step 1: Mild Pain (1-4) Acetaminophen + Adjuvants Step 2: Moderate Pain (5-6) Hydromorphone, Oxycodone, Tramadol + Nonopioid analgesics + Adjuvants Codeine: metabolites accumulate, constipation Tramadol: mg bid Morphine not well tolerated, constipation, myoclonic jerks Demerol causes seizures Hydromorphone needs dose titration Oxycodone well tolerated by some, possible abuse by others 45
46 WHO Analgesic Ladder Modified for safety in CKD patients Step 3: Severe Pain (7-10) Hydromorphone, Methadone, Fentanyl, Oxycodone + Nonopioid analgesics + Adjuvants Step 2: Moderate Pain (5-6) Hydromorphone, Oxycodone, Tramadol + Nonopioid analgesics + Adjuvants Methadone not removed by dialysis, use as in other patients, well tolerated Fentanyl very helpful Step 1: Mild Pain (1-4) Acetaminophen + Adjuvants 46
47 Adjuvant Drugs: Neuropathic Pain TCAs Amitriptyline, Nortriptyline Sedation, dry mouth, constipation, urinary retention, fatigue, postural hypotension Can alter seizure threshold mg qhs Anticonvulsants Carbamazepine Interaction with warfarin Well tolerated 200 mg od increasing to maximum dose of 1600 mg Valproic acid GI irritation, weight gain 200 mg increasing to a maximum dose of 1000 mg 47
48 Adjuvant Drugs: Neuropathic Pain Anticonvulsants Gabapentin Drowsiness, ataxia Titrate slowly, up to 600 mg/day generally tolerated Clonazepam Sedation mg qhs 48
49 Adjuvant Drugs- MSK Pain Corticosteroids Benzodiazepines for muscle spasms Baclofen for muscle spasm not recommended as CNS side effects common Quinine sulphate for muscle cramps 49
50 Symptom Control - Pruritus Multiple etiologies: Hyperphosphatemia, increased calciumphosphate deposition in skin, dry skin, inadequate dialysis, anemia, iron deficiency Management: Review of diet with particular attention to phosphate. If a patient has decided to stop dialysis, there are no diet restrictions control pruritus with drugs (next slide). Use emollients such as oatmeal moisturizer, mineral oil or Uremol cream 50
51 Symptom Control - Pruritus Management: Phosphate binders such as Amphogel or Basaljel. Oral anti-histamines of your choice Capsaicin cream bid-qid Photo therapy with UVB ultraviolet light three times weekly Narcan can be useful Cholestyramine 1 pkg bid but can interfere with the absorption of other drugs Thalidomide 100 mg at hs 51
52 Symptom Control Restless Legs Unclear as to whether this is related to uremic neuropathy or to other associated comorbid conditions. Anemia, iron deficiency may be implicated Management: TCAs, lithium, neuroleptics and caffeine aggravates RLS Treat anemia and iron deficiency Trial of benzodiazepines: Clonazepam mg qhs Dopaminergic agents: Sinemet 25/100 mg od tid Gabapentin mg od Tachyphylaxis occurs and therefore after 3-4 months the drugs may need to be rotated. 52
53 Symptom Control- Shortness of Breath Etiology Salt and water excess Further decline in renal function Advancing cardiac disease Management: Salt and water restriction Diuretics Lasix 120 mg po/iv q4-6h Nitro patch Oxygen Scopolamine patch Opioids Benzodiazepines 53
54 Symptom Control - Anorexia Multiple etiologies: Advancing renal failure, inadequate dialysis, anemia, depression, dry mouth, constipation, diabetic gastro paresis Management: Oral moisturizers Anemia treatment Anti-emetic Anti-depressants with appetite stimulating properties Trial of zinc 50 mg bid po Trial of appetite stimulants: Megace, Nabilone, Prednisone 54
55 Symptom Control Nausea/Vomiting Etiology Uremia Fluid-electrolyte abnormalities Hypotension Comorbid conditions Medication side effects Management: Treat hypotension If due to gastroparesis, use Maxeran 5-10 mg ½ hour prior to meals Use standard anti-emetics Gravol, Stemetil Haloperidol mg po/sc tid Ondansetron in usual doses 55
56 Symptom Control - Constipation Etiology is usually the renal diet which restricts fruits, vegetables and high fibre foods (ie bran) together with the fluid restriction, physical inactivity and medications such as Amphogel Management: Stool softeners Lactulose, Mag citrate, Lax-a-Day 56
57 Etiology Symptom Control - Insomnia Anemia Sleep apnea RLS Management Treat anemia Diagnose and treat sleep apnea/rls Avoid caffeine, smoking, alcohol and napping in the daytime Sleep aides Zoplicone usual dose Any benzodiazepine 57
58 Symptom Control - Tiredness Etiology Anemia Iron deficiency Depression Insomnia Poor nutrition Medications Management: Treat anemia and iron deficiency Treat insomnia Encourage exercise Trial of anti-depressants 58
59 Framework for Appropriate Care Interdisciplinary team care Identifying patients with poor prognosis either before RRT or during the course of RRT and thus in need of supportive care Advance care planning Symptom assessment and management Care of the dying patient Bereavement processes for families and staff 59
60 Objectives 2 To provide a framework for appropriate care for those people with chronic kidney disease (CKD) who chose not to initiate RRT or for those who chose to terminate RRT. 60

61 Questions? 61
62 Resources
BACKGROUND Measuring renal function :
 A GUIDE TO USE OF COMMON PALLIATIVE CARE DRUGS IN RENAL IMPAIRMENT These guidelines bring together information and recommendations from the Palliative Care formulary (PCF5 ) BACKGROUND Measuring renal
A GUIDE TO USE OF COMMON PALLIATIVE CARE DRUGS IN RENAL IMPAIRMENT These guidelines bring together information and recommendations from the Palliative Care formulary (PCF5 ) BACKGROUND Measuring renal
Regional Renal Training
 Regional Renal Training Palliative and End of Life Care Dr Clare Kendall North Bristol NHS Trust Advanced Kidney Disease Dialysis/Transplant Conservative Management Deteriorating despite dialysis/failing
Regional Renal Training Palliative and End of Life Care Dr Clare Kendall North Bristol NHS Trust Advanced Kidney Disease Dialysis/Transplant Conservative Management Deteriorating despite dialysis/failing
Overview of Essentials of Pain Management. Updated 11/2016
 0 Overview of Essentials of Pain Management Updated 11/2016 1 Overview of Essentials of Pain Management 1. Assess pain intensity on a 0 10 scale in which 0 = no pain at all and 10 = the worst pain imaginable.
0 Overview of Essentials of Pain Management Updated 11/2016 1 Overview of Essentials of Pain Management 1. Assess pain intensity on a 0 10 scale in which 0 = no pain at all and 10 = the worst pain imaginable.
Palliative and Hospice Care of the Terminally Ill Introduction
 Palliative and Hospice Care of the Terminally Ill Introduction There has been an increase in life expectancy for men and women of all races to 77.6 years Leading causes of death in older patients are chronic
Palliative and Hospice Care of the Terminally Ill Introduction There has been an increase in life expectancy for men and women of all races to 77.6 years Leading causes of death in older patients are chronic
Pain Management in Older Adults. Mary Shelkey, PhD, ARNP
 Pain Management in Older Adults Mary Shelkey, PhD, ARNP Cause of Death/ Demographic and Social Trends Early 1900s Current Medicine's Focus Comfort Cure Cause of Death Infectious Diseases/ Communicable
Pain Management in Older Adults Mary Shelkey, PhD, ARNP Cause of Death/ Demographic and Social Trends Early 1900s Current Medicine's Focus Comfort Cure Cause of Death Infectious Diseases/ Communicable
Pain Management Management in Hepatic Hepatic and and Renal Dysfunction
 Pain Management in Hepatic and Renal Dysfunction Review the pharmacologic basis for medications used in pain management Identify pain medications which hshould ldbe avoided in patients with hepatic dysfunction
Pain Management in Hepatic and Renal Dysfunction Review the pharmacologic basis for medications used in pain management Identify pain medications which hshould ldbe avoided in patients with hepatic dysfunction
CARE OF THE DYING PATIENT WITH ESKD ELIZABETH JOSLAND - RSC CNC
 CARE OF THE DYING PATIENT WITH ESKD ELIZABETH JOSLAND - RSC CNC OBJECTIVES UNDERSTANDING OF: POTENTIAL COMPLEXITIES OF ESKD PATIENTS IMPORTANCE OF COMMUNICATION CONSIDERATIONS AT END-OF-LIFE END-OF-LIFE
CARE OF THE DYING PATIENT WITH ESKD ELIZABETH JOSLAND - RSC CNC OBJECTIVES UNDERSTANDING OF: POTENTIAL COMPLEXITIES OF ESKD PATIENTS IMPORTANCE OF COMMUNICATION CONSIDERATIONS AT END-OF-LIFE END-OF-LIFE
Road Blocks in Non-Cancer Palliative Care Obstacles observed from outpatient non-cancer palliative practice.
 Road Blocks in Non-Cancer Palliative Care Obstacles observed from outpatient non-cancer palliative practice. 25th Annual Palliative Education and Research Days, West Edmonton Mall. Edmonton. 2014 Amanda
Road Blocks in Non-Cancer Palliative Care Obstacles observed from outpatient non-cancer palliative practice. 25th Annual Palliative Education and Research Days, West Edmonton Mall. Edmonton. 2014 Amanda
END STAGE RENAL DISEASE AND THE DISCONTINUATION OF DIALYSIS
 END STAGE RENAL DISEASE AND THE DISCONTINUATION OF DIALYSIS Dr. Nicki Apostle December 8, 2014 Disclosures: I listen to Taylor Swift (Don t lie so do you) CASE STUDY: Mrs. S 83 yo F from LTC referred to
END STAGE RENAL DISEASE AND THE DISCONTINUATION OF DIALYSIS Dr. Nicki Apostle December 8, 2014 Disclosures: I listen to Taylor Swift (Don t lie so do you) CASE STUDY: Mrs. S 83 yo F from LTC referred to
Renal Palliative Care Last Days of Life
 Renal Palliative Care Last Days of Life Introduction This guideline is an aid to clinical decision-making and good practice for patients with stage 4-5 chronic kidney disease (egfr
Renal Palliative Care Last Days of Life Introduction This guideline is an aid to clinical decision-making and good practice for patients with stage 4-5 chronic kidney disease (egfr
NEUROPATHIC CANCER PAIN STANDARDS AND GUIDELINES
 NEUROPATHIC CANCER PAIN STANDARDS AND GUIDELINES GENERAL PRINCIPLES Neuropathic pain may be relieved in the majority of patients by multimodal management A careful history and examination are essential.
NEUROPATHIC CANCER PAIN STANDARDS AND GUIDELINES GENERAL PRINCIPLES Neuropathic pain may be relieved in the majority of patients by multimodal management A careful history and examination are essential.
Symptom Management Challenges at End-of-Life
 Symptom Management Challenges at End-of-Life Amanda Lovell, PharmD, BCGP Clinical Pharmacist- Inpatient Units Optum Hospice Pharmacy Services February 15, 2018 Hospice Pharmacy Services Objectives Identify
Symptom Management Challenges at End-of-Life Amanda Lovell, PharmD, BCGP Clinical Pharmacist- Inpatient Units Optum Hospice Pharmacy Services February 15, 2018 Hospice Pharmacy Services Objectives Identify
Palliative Prescribing - Pain
 Palliative Prescribing - Pain LAURA BARNFIELD 21/2/17 Aims To understand the classes of painkillers available in palliative care To gain confidence in counselling regarding opiates To gain confidence prescribing
Palliative Prescribing - Pain LAURA BARNFIELD 21/2/17 Aims To understand the classes of painkillers available in palliative care To gain confidence in counselling regarding opiates To gain confidence prescribing
Pain Assessment & Management. For General Nursing Orientation
 Pain Assessment & Management For General Nursing Orientation April 2012 Overview Definition of pain Barriers to effective pain management Types of pain Objective pain assessment Approaches to management
Pain Assessment & Management For General Nursing Orientation April 2012 Overview Definition of pain Barriers to effective pain management Types of pain Objective pain assessment Approaches to management
The pain of it all. Rod MacLeod MNZM. Hibiscus Hospice, Auckland and University of Auckland
 The pain of it all Rod MacLeod MNZM Hibiscus Hospice, Auckland and University of Auckland Definition of PAIN An unpleasant sensory and emotional experience which we primarily associate with tissue damage
The pain of it all Rod MacLeod MNZM Hibiscus Hospice, Auckland and University of Auckland Definition of PAIN An unpleasant sensory and emotional experience which we primarily associate with tissue damage
Non Malignant Pain: Symptom Management
 Non Malignant Pain: Symptom Management Renal Care Symposium July 2018 Anica Vasic Pain Management Unit St George Hospital Definitions Prevalence Assessment Treatment Medications Newer agents: tapentadol,
Non Malignant Pain: Symptom Management Renal Care Symposium July 2018 Anica Vasic Pain Management Unit St George Hospital Definitions Prevalence Assessment Treatment Medications Newer agents: tapentadol,
Pain management in Paediatric Palliative Care. Dr Jane Nakawesi 14 th August 2017
 Pain management in Paediatric Palliative Care Dr Jane Nakawesi 14 th August 2017 Content Management of pain in children Non pharmacological Pharmacological Exit level outcomes The participants will: Know
Pain management in Paediatric Palliative Care Dr Jane Nakawesi 14 th August 2017 Content Management of pain in children Non pharmacological Pharmacological Exit level outcomes The participants will: Know
GUIDELINES ON THE MANAGEMENT OF PAIN DUE TO CANCER IN ADULTS
 GUIDELINES ON THE MANAGEMENT OF PAIN DUE TO CANCER IN ADULTS Bristol Palliative Care Collaborative Contact Numbers: Hospital Specialist Palliative Care Teams: North Bristol 0117 4146392 UH Bristol 0117
GUIDELINES ON THE MANAGEMENT OF PAIN DUE TO CANCER IN ADULTS Bristol Palliative Care Collaborative Contact Numbers: Hospital Specialist Palliative Care Teams: North Bristol 0117 4146392 UH Bristol 0117
End of Life Care in Renal Disease. Tara Collidge Consultant, Glasgow Renal Unit
 End of Life Care in Renal Disease Tara Collidge Consultant, Glasgow Renal Unit Aim to cover.. Background of end stage renal failure population Registry data (SRR) Our unit outcomes How to know when someone
End of Life Care in Renal Disease Tara Collidge Consultant, Glasgow Renal Unit Aim to cover.. Background of end stage renal failure population Registry data (SRR) Our unit outcomes How to know when someone
Palliative Care for Primary Care Providers QUYNH BUI, MD MPH DECEMBER 2015
 Palliative Care for Primary Care Providers QUYNH BUI, MD MPH DECEMBER 2015 Objectives Define palliative care and primary palliative care Describe the rationale for providing primary palliative care in
Palliative Care for Primary Care Providers QUYNH BUI, MD MPH DECEMBER 2015 Objectives Define palliative care and primary palliative care Describe the rationale for providing primary palliative care in
Pain and Chronic Kidney Disease
 Pain and Chronic Kidney Disease Frank Brennan Palliative Care Physician Department of Nephrology, St George Hospital Renal Supportive Care Symposium St George Hospital August 21 2015 Epidemiology Effect
Pain and Chronic Kidney Disease Frank Brennan Palliative Care Physician Department of Nephrology, St George Hospital Renal Supportive Care Symposium St George Hospital August 21 2015 Epidemiology Effect
Care of the dying in End Stage Kidney Disease (ESKD) - Conservative. Elizabeth Josland Renal Supportive Care CNC St George Hospital
 - Conservative. Elizabeth Josland Renal Supportive Care CNC St George Hospital") Care of the dying in End Stage Kidney Disease (ESKD) - Conservative Elizabeth Josland Renal Supportive Care CNC St George Hospital Introduction What does conservative management look like? How does the
Care of the dying in End Stage Kidney Disease (ESKD) - Conservative Elizabeth Josland Renal Supportive Care CNC St George Hospital Introduction What does conservative management look like? How does the
HMFP Comprehensive Headache Center Department of Anesthesia, Critical Care and Pain Medicine Beth Israel Deaconess Medical Center Instructor in
 HMFP Comprehensive Headache Center Department of Anesthesia, Critical Care and Pain Medicine Beth Israel Deaconess Medical Center Instructor in Anesthesia and Neurology Harvard Medical School Limited time
HMFP Comprehensive Headache Center Department of Anesthesia, Critical Care and Pain Medicine Beth Israel Deaconess Medical Center Instructor in Anesthesia and Neurology Harvard Medical School Limited time
Conservative Management of Uraemia
 Conservative Management of Uraemia Information for Health Professionals Renal Department The York Hospital and Scarborough Hospital Tel: 01904 725370 For more information, please contact: The Renal Specialist
Conservative Management of Uraemia Information for Health Professionals Renal Department The York Hospital and Scarborough Hospital Tel: 01904 725370 For more information, please contact: The Renal Specialist
PAIN. TREATMENT TABLES Analgesics. NON-OPIOID ANALGESICS Generic Name Trade Names (Examples) Duration Initial Dose
 Duration Initial Dose") NON-OPIOID SHORT-ACTING LONG-ACTING **** O PAIN TREATMENT TABLES Analgesics NON-OPIOID ANALGESICS Generic Name Trade Names (Examples) Duration Initial Dose Tramadol 50 mg Ultram Every 4 hours 1-2 tabs,
NON-OPIOID SHORT-ACTING LONG-ACTING **** O PAIN TREATMENT TABLES Analgesics NON-OPIOID ANALGESICS Generic Name Trade Names (Examples) Duration Initial Dose Tramadol 50 mg Ultram Every 4 hours 1-2 tabs,
Knock Out Opioid Abuse in New Jersey:
 Knock Out Opioid Abuse in New Jersey: A Resource for Safer Prescribing GUIDELINE FOR PRESCRIBING OPIOIDS FOR CHRONIC PAIN IMPROVING PRACTICE THROUGH RECOMMENDATIONS CDC s Guideline for Prescribing Opioids
Knock Out Opioid Abuse in New Jersey: A Resource for Safer Prescribing GUIDELINE FOR PRESCRIBING OPIOIDS FOR CHRONIC PAIN IMPROVING PRACTICE THROUGH RECOMMENDATIONS CDC s Guideline for Prescribing Opioids
Managing Care at End of Life:
 Managing Care at End of Life: Physical Suffering Pain & Dyspnea Verna Sellers, MD, MPH, AGSF Medical Director Centra PACE Lynchburg, Virginia 1 Speaker Disclosures: Dr. Sellers has disclosed that she has
Managing Care at End of Life: Physical Suffering Pain & Dyspnea Verna Sellers, MD, MPH, AGSF Medical Director Centra PACE Lynchburg, Virginia 1 Speaker Disclosures: Dr. Sellers has disclosed that she has
Hospice and Palliative Medicine
 Hospice and Palliative Medicine Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the
Hospice and Palliative Medicine Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the
THE CONSERVATIVE CARE PATHWAY
 THE CONSERVATIVE CARE PATHWAY Dr. Gaylene Hargrove Sept. 19, 2015 Island Health Renal Program End of Life Conference Learning Objectives Describe and discuss what defines conservative care. Identify key
THE CONSERVATIVE CARE PATHWAY Dr. Gaylene Hargrove Sept. 19, 2015 Island Health Renal Program End of Life Conference Learning Objectives Describe and discuss what defines conservative care. Identify key
Pain. Christine Illingworth. Community Nurse St Luke s Hospice 17/5/17
 Pain Christine Illingworth Community Nurse St Luke s Hospice 17/5/17 What is pain? Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damage Pain is whatever
Pain Christine Illingworth Community Nurse St Luke s Hospice 17/5/17 What is pain? Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damage Pain is whatever
Conservative Care Pathway: A Client-Centred Approach
 2016 Conservative Care Pathway: A Client-Centred Approach Abbotsford Kidney Care Clinic October 7, 2016 Bobbi Preston, MSW, RCSW Jane Valcourt, RN Susan Cooper, MD, FRCP Goals of Session 1. Introduce the
2016 Conservative Care Pathway: A Client-Centred Approach Abbotsford Kidney Care Clinic October 7, 2016 Bobbi Preston, MSW, RCSW Jane Valcourt, RN Susan Cooper, MD, FRCP Goals of Session 1. Introduce the
Oxford Kidney Unit A guide to conservative kidney management. Information for Healthcare Professionals
 Oxford Kidney Unit A guide to conservative kidney management Information for Healthcare Professionals What is conservative kidney management? Some people with advanced kidney disease (chronic kidney disease
Oxford Kidney Unit A guide to conservative kidney management Information for Healthcare Professionals What is conservative kidney management? Some people with advanced kidney disease (chronic kidney disease
3/27/2013. Objectives. Psychopharmacology at the End of Life Nicole Thurston, MD
 Psychopharmacology at the End of Life Nicole Thurston, MD Psychiatrist Mountain States Tumor Institute Objectives Describe 2 common psychiatric symptoms that can present at or near end of life. Review
Psychopharmacology at the End of Life Nicole Thurston, MD Psychiatrist Mountain States Tumor Institute Objectives Describe 2 common psychiatric symptoms that can present at or near end of life. Review
Pain Management Strategies Webinar/Teleconference
 Pain Management Strategies Webinar/Teleconference Barry K. Baines, MD April 16, 2009 Objectives Describe the principles of pain management. Identify considerations in the use of opioids. Describe the benefits
Pain Management Strategies Webinar/Teleconference Barry K. Baines, MD April 16, 2009 Objectives Describe the principles of pain management. Identify considerations in the use of opioids. Describe the benefits
Learning Objectives. Delirium. Delirium. Delirium. Terminal Restlessness 3/28/2016
 Terminal Restlessness Dr. Christopher Churchill St. Cloud VA Health Care System EC&R Service Line Director & Medical Director Hospice & Palliative Care March 31, 2016 Learning Objectives Different Terminology
Terminal Restlessness Dr. Christopher Churchill St. Cloud VA Health Care System EC&R Service Line Director & Medical Director Hospice & Palliative Care March 31, 2016 Learning Objectives Different Terminology
PALLIATIVE CARE IN THE END STAGE RENAL DISEASE (ESRD) POPULATION:
 POPULATION:") PALLIATIVE CARE IN THE END STAGE RENAL DISEASE (ESRD) POPULATION: BEYOND THE BASICS AND INTO THE FUTURE Daniel Sturgill MD and Alexandria Bear MD 20 April 2018 CONFLICTS OF INTEREST We have no financial
PALLIATIVE CARE IN THE END STAGE RENAL DISEASE (ESRD) POPULATION: BEYOND THE BASICS AND INTO THE FUTURE Daniel Sturgill MD and Alexandria Bear MD 20 April 2018 CONFLICTS OF INTEREST We have no financial
Disclosures. Management of Chronic, Non- Terminal Pain. Learning Objectives. Outline. Drug Schedules. Applicable State Laws
 Disclosures Management of Chronic, Non- Terminal Pain No financial disclosures or conflicts of interest to report Michael A. Smith, PharmD, BCPS Clinical Assistant Professor, University of Michigan College
Disclosures Management of Chronic, Non- Terminal Pain No financial disclosures or conflicts of interest to report Michael A. Smith, PharmD, BCPS Clinical Assistant Professor, University of Michigan College
The World Health Organization has developed and has widely accepted an algorithm for treatment of cancer pain. This is described as the three-step lad
 Hello. My name is Cynthia Abarado. I m an Advanced Practice Nurse at the Department of Genitourinary Medical Oncology at The University of Texas MD Anderson Cancer Center. I am going to present to you
Hello. My name is Cynthia Abarado. I m an Advanced Practice Nurse at the Department of Genitourinary Medical Oncology at The University of Texas MD Anderson Cancer Center. I am going to present to you
Mitigating Risks While Optimizing the Benefits of Pharmacologic Agents to Manage Pain in the Elderly
 Mitigating Risks While Optimizing the Benefits of Pharmacologic Agents to Manage Pain in the Elderly Mary Lynn McPherson, PharmD, MDE, MA, BCPS, CPE Professor and Executive Director, Advanced Post-Graduate
Mitigating Risks While Optimizing the Benefits of Pharmacologic Agents to Manage Pain in the Elderly Mary Lynn McPherson, PharmD, MDE, MA, BCPS, CPE Professor and Executive Director, Advanced Post-Graduate
IF I M NOT TREATING WITH OPIOIDS, THEN WHAT AM I SUPPOSED TO USE?
 NON-OPIOID TREATMENT OPTIONS FOR CHRONIC PAIN Alison Knutson, PharmD, BCACP Medication Management Pharmacist Park Nicollet Creekside Clinic Dr. Knutson indicated no potential conflict of interest to this
NON-OPIOID TREATMENT OPTIONS FOR CHRONIC PAIN Alison Knutson, PharmD, BCACP Medication Management Pharmacist Park Nicollet Creekside Clinic Dr. Knutson indicated no potential conflict of interest to this
Decision-making around commencing dialysis
 Decision-making around commencing dialysis A.M.Anutra Chittinandana, MD. Bhumibol Aduyadej Hospital Mr.H Mr. H was an 86-year-old man with diabetic and ischemic nephropathy, otherwise well. He was followed
Decision-making around commencing dialysis A.M.Anutra Chittinandana, MD. Bhumibol Aduyadej Hospital Mr.H Mr. H was an 86-year-old man with diabetic and ischemic nephropathy, otherwise well. He was followed
DISCLAIMER: ECHO Nevada emphasizes patient privacy and asks participants to not share ANY Protected Health Information during ECHO clinics.
 DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
PALLIATIVE TREATMENT BY DR. KHRONGKAMOL SIHABAN MEDICAL ONCOLOGIST
 PALLIATIVE TREATMENT BY DR. KHRONGKAMOL SIHABAN MEDICAL ONCOLOGIST TREATMENT IN ONCOLOGY Main treatment : surgery Neoadjuvant treatment : RT, CMT Adjuvant treatment : Tx micrometastatic disease -CMT,Targeted
PALLIATIVE TREATMENT BY DR. KHRONGKAMOL SIHABAN MEDICAL ONCOLOGIST TREATMENT IN ONCOLOGY Main treatment : surgery Neoadjuvant treatment : RT, CMT Adjuvant treatment : Tx micrometastatic disease -CMT,Targeted
End-Stage Renal Disease. Anna Vinnikova, M.D. Associate Professor of Medicine Division of Nephrology
 End-Stage Renal Disease Anna Vinnikova, M.D. Associate Professor of Medicine Division of Nephrology ESRD : Life with renal replacement therapy CASE: 18 month old male with HUS develops ESRD PD complicated
End-Stage Renal Disease Anna Vinnikova, M.D. Associate Professor of Medicine Division of Nephrology ESRD : Life with renal replacement therapy CASE: 18 month old male with HUS develops ESRD PD complicated
Analgesics: Management of Pain In the Elderly Handout Package
 Analgesics: Management of Pain In the Elderly Handout Package Analgesics: Management of Pain in the Elderly Each patient or resident and their pain problem is unique. A complete assessment should be performed
Analgesics: Management of Pain In the Elderly Handout Package Analgesics: Management of Pain in the Elderly Each patient or resident and their pain problem is unique. A complete assessment should be performed
Medications for the Treatment of Neuropathic Pain
 Medications for the Treatment of Neuropathic Pain February 23, 2011 Jinny Tavee, MD Associate Professor Neurological Institute Cleveland Clinic Foundation Neuropathic Pain Pain, paresthesias, and sensory
Medications for the Treatment of Neuropathic Pain February 23, 2011 Jinny Tavee, MD Associate Professor Neurological Institute Cleveland Clinic Foundation Neuropathic Pain Pain, paresthesias, and sensory
Index. Surg Clin N Am 85 (2005) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Surg Clin N Am 85 (2005) 393 398 Index Note: Page numbers of article titles are in boldface type. A Acetaminophen, for chronic pain, in surgical patients, 219 a2 Adrenergic agonists, for neuropathic pain,
Surg Clin N Am 85 (2005) 393 398 Index Note: Page numbers of article titles are in boldface type. A Acetaminophen, for chronic pain, in surgical patients, 219 a2 Adrenergic agonists, for neuropathic pain,
CLINICAL GUIDELINES FOR END OF LIFE CARE MEDICATIONS IN LONG TERM CARE HOMES
 CLINICAL GUIDELINES F END OF LIFE CARE MEDICATIONS IN LONG TERM CARE HOMES OPENING STATEMENT: Insert Facility Name is committed to providing effective end-of-life symptom management to all residents. Symptom
CLINICAL GUIDELINES F END OF LIFE CARE MEDICATIONS IN LONG TERM CARE HOMES OPENING STATEMENT: Insert Facility Name is committed to providing effective end-of-life symptom management to all residents. Symptom
Agonists: morphine, fentanyl Agonists-Antagonists: nalbuphine Antagonists: naloxone
 Opioid Definition All drugs, natural or synthetic, that bind to opiate receptors Agonists: morphine, fentanyl Agonists-Antagonists: nalbuphine Antagonists: naloxone Opioid agonists increase pain threshold
Opioid Definition All drugs, natural or synthetic, that bind to opiate receptors Agonists: morphine, fentanyl Agonists-Antagonists: nalbuphine Antagonists: naloxone Opioid agonists increase pain threshold
4/10/2018. Preparing for Death. Describe a Recent Death You Have Observed. The Nurse, Dying and Death
 Preparing for Death Core Curriculum FINAL HOURS CARLA JOLLEY MN, ARNP, AOCN, ACHPN WHIDBEYHEALTH PALLIATIVE CARE JOLLEC@WHIDBEYHEALTH.ORG Everyone dies Advance care planning Recognizing the transition
Preparing for Death Core Curriculum FINAL HOURS CARLA JOLLEY MN, ARNP, AOCN, ACHPN WHIDBEYHEALTH PALLIATIVE CARE JOLLEC@WHIDBEYHEALTH.ORG Everyone dies Advance care planning Recognizing the transition
Enhanced Community Palliative Support Services. Lynne Ghasemi St Luke s Hospice
 Enhanced Community Palliative Support Services Lynne Ghasemi St Luke s Hospice Learning Outcomes Define the different types of pain Describe the process of pain assessment Discuss pharmacological management
Enhanced Community Palliative Support Services Lynne Ghasemi St Luke s Hospice Learning Outcomes Define the different types of pain Describe the process of pain assessment Discuss pharmacological management
PATIENTS WHO WITHDRAW FROM DIALYSIS. Dr Katalin Urban Palliative Care Specialist Greenwich Hospital
 PATIENTS WHO WITHDRAW FROM DIALYSIS Dr Katalin Urban Palliative Care Specialist Greenwich Hospital Registrar project for FRACP Title: Patients who withdraw from dialysis in a Sydney centre with Palliative
PATIENTS WHO WITHDRAW FROM DIALYSIS Dr Katalin Urban Palliative Care Specialist Greenwich Hospital Registrar project for FRACP Title: Patients who withdraw from dialysis in a Sydney centre with Palliative
What Matters to you? Responding to patient symptoms with practical tools: The development of the BCPRA symptoms management protocols
 What Matters to you? Responding to patient symptoms with practical tools: The development of the BCPRA symptoms management protocols Learning objectives 1. Review the process leading to the development
What Matters to you? Responding to patient symptoms with practical tools: The development of the BCPRA symptoms management protocols Learning objectives 1. Review the process leading to the development
GUIDELINES AND AUDIT IMPLEMENTATION NETWORK
 GUIDELINES AND AUDIT IMPLEMENTATION NETWORK General Palliative Care Guidelines The Management of Pain at the End Of Life November 2010 Aim To provide a user friendly, evidence based guide for the management
GUIDELINES AND AUDIT IMPLEMENTATION NETWORK General Palliative Care Guidelines The Management of Pain at the End Of Life November 2010 Aim To provide a user friendly, evidence based guide for the management
Renal Care and Liver Disease: Disease Trajectory and Hospice Eligibility
 Renal Care and Liver Disease: Disease Trajectory and Hospice Eligibility Terri L. Maxwell PhD, APRN VP, Strategic Initiatives Weatherbee Resources/HEN Course Materials & Disclosure Course materials including
Renal Care and Liver Disease: Disease Trajectory and Hospice Eligibility Terri L. Maxwell PhD, APRN VP, Strategic Initiatives Weatherbee Resources/HEN Course Materials & Disclosure Course materials including
Care in the Last Days of Life
 Care in the Last Days of Life Introduction This guideline is an aid to clinical decision making and good practice in person-centred care for patients who are deteriorating and at risk of dying. The patient
Care in the Last Days of Life Introduction This guideline is an aid to clinical decision making and good practice in person-centred care for patients who are deteriorating and at risk of dying. The patient
Delirium. Assessment and Management
 Delirium Assessment and Management Goals and Objectives Participants will: 1. be able to recognize and diagnose the syndrome of delirium. 2. understand the causes of delirium. 3. become knowledgeable about
Delirium Assessment and Management Goals and Objectives Participants will: 1. be able to recognize and diagnose the syndrome of delirium. 2. understand the causes of delirium. 3. become knowledgeable about
Palliative Medicine in Critical Care Not Just Hospice. Robin. Truth or Myth 6/11/2015. Francine Arneson, MD Palliative Medicine
 Palliative Medicine in Critical Care Not Just Hospice Francine Arneson, MD Palliative Medicine Robin 45 year old female married, husband in Afghanistan. 4 children ages 17-24. Mother has been providing
Palliative Medicine in Critical Care Not Just Hospice Francine Arneson, MD Palliative Medicine Robin 45 year old female married, husband in Afghanistan. 4 children ages 17-24. Mother has been providing
Treating patients with end-stage liver disease: Are we ready? Dr. Mino R. Mitri, M.D., C.M., M.Ed., FRCPC
 Treating patients with end-stage liver disease: Are we ready? Dr. Mino R. Mitri, M.D., C.M., M.Ed., FRCPC mino.mitri@ubc.ca No Conflict of Interest 157 patients 157 patients 6 transplanted Criteria Liver
Treating patients with end-stage liver disease: Are we ready? Dr. Mino R. Mitri, M.D., C.M., M.Ed., FRCPC mino.mitri@ubc.ca No Conflict of Interest 157 patients 157 patients 6 transplanted Criteria Liver
PAIN MANAGEMENT 101. By: Vicki McCulloch RN, NP & DeAnna Looper RN, CHPN, CHPCA
 PAIN MANAGEMENT 101 By: Vicki McCulloch RN, NP & DeAnna Looper RN, CHPN, CHPCA Objectives Identify a step-wise approach to pain management. Identify the WHO Pain Ladder. Identify non-pharmacological pain
PAIN MANAGEMENT 101 By: Vicki McCulloch RN, NP & DeAnna Looper RN, CHPN, CHPCA Objectives Identify a step-wise approach to pain management. Identify the WHO Pain Ladder. Identify non-pharmacological pain
Course Handouts & Post Test
 End Stage Liver Disease (ESLD) End Stage Renal Disease (ESRD) Disease Trajectory and Hospice Eligibility Terri Maxwell PhD, APRN VP, Strategic Initiatives Weatherbee Resources Inc. & Hospice Education
End Stage Liver Disease (ESLD) End Stage Renal Disease (ESRD) Disease Trajectory and Hospice Eligibility Terri Maxwell PhD, APRN VP, Strategic Initiatives Weatherbee Resources Inc. & Hospice Education
Three triggers that suggest that patients could benefit from a hospice palliative care approach
 Why is it important to identify people nearing the end of life? About 1% of the population dies each year. Although some deaths are unexpected, many more in fact can be predicted. This is inherently difficult,
Why is it important to identify people nearing the end of life? About 1% of the population dies each year. Although some deaths are unexpected, many more in fact can be predicted. This is inherently difficult,
Pain control in Cancer patients. Dr Ali Shoeibi, Assistant Professor of Neurology
 Pain control in Cancer patients Dr Ali Shoeibi, Assistant Professor of Neurology More than two thirds of patients with advanced cancer experience cancer pain Almost all pain can be controlled to some extent
Pain control in Cancer patients Dr Ali Shoeibi, Assistant Professor of Neurology More than two thirds of patients with advanced cancer experience cancer pain Almost all pain can be controlled to some extent
Geri-PARDY! (2015 Beers Criteria) Pharmacology Edition
 Pharmacology Edition") Geri-PARDY! Pharmacology Edition (2015 Beers Criteria) Aurelio Muyot, MD, AGSF, FACP Assistant Professor College of Osteopathic Medicine Touro University Nevada Objectives Review the 2015 Beers Criteria
Geri-PARDY! Pharmacology Edition (2015 Beers Criteria) Aurelio Muyot, MD, AGSF, FACP Assistant Professor College of Osteopathic Medicine Touro University Nevada Objectives Review the 2015 Beers Criteria
Foundations of Palliative Care Series
 Foundations of Palliative Care Series Developed by: Tim Sakaluk MD, Ingrid See CPL, Tammy Dyson SW, Sharon Salomons SCP!!!!!! This course was developed in collaboration with the UBC Learning Circle to
Foundations of Palliative Care Series Developed by: Tim Sakaluk MD, Ingrid See CPL, Tammy Dyson SW, Sharon Salomons SCP!!!!!! This course was developed in collaboration with the UBC Learning Circle to
6/6/2018. Nalbuphine: Analgesic with a Niche. Mellar P Davis MD FCCP FAAHPM. Summary of Advantages. Summary of Advantages
 Nalbuphine: Analgesic with a Niche Mellar P Davis MD FCCP FAAHPM 1 Summary of Advantages Safe in renal failure- fecal excretion Analgesia equal to morphine with fewer side effects Reduced constipation
Nalbuphine: Analgesic with a Niche Mellar P Davis MD FCCP FAAHPM 1 Summary of Advantages Safe in renal failure- fecal excretion Analgesia equal to morphine with fewer side effects Reduced constipation
Psychology of Pain DR. ARNEL BANAGA SALGADO,
 Psychology of Pain DR. ARNEL BANAGA SALGADO, Doctor of Psychology (USA) FPM (Ph.D.) Psychology (India) Doctor of Education (Phl) Master of Arts in Nursing (Phl) Master of Arts in Teaching Psychology (PNU)
Psychology of Pain DR. ARNEL BANAGA SALGADO, Doctor of Psychology (USA) FPM (Ph.D.) Psychology (India) Doctor of Education (Phl) Master of Arts in Nursing (Phl) Master of Arts in Teaching Psychology (PNU)
Pain management. Coleman Palliative Care Conference: February 2016 Josh Baru MD Stacie Levine MD
 Pain management Coleman Palliative Care Conference: February 2016 Josh Baru MD Stacie Levine MD Case #1 61 yo man with history of Stage 3 colon cancer, s/p resection and adjuvant chemotherapy with FOLFOX
Pain management Coleman Palliative Care Conference: February 2016 Josh Baru MD Stacie Levine MD Case #1 61 yo man with history of Stage 3 colon cancer, s/p resection and adjuvant chemotherapy with FOLFOX
NYSPFP Kickoff. Reducing Adverse Drug Events from Opioids. April 6, 2017
 NYSPFP Kickoff Reducing Adverse Drug Events from Opioids April 6, 2017 I have no financial relationships with drug companies, durable medical equipment companies or other for profit entities related to
NYSPFP Kickoff Reducing Adverse Drug Events from Opioids April 6, 2017 I have no financial relationships with drug companies, durable medical equipment companies or other for profit entities related to
Analgesia in patients with impaired renal function Formulary Guidance
 Analgesia in patients with impaired renal function Formulary Guidance Approved by Trust D&TC: January 2010 Revised March 2017 Contents Paragraph Page 1 Aim 4 2 Introduction 4 3 Assessment of renal function
Analgesia in patients with impaired renal function Formulary Guidance Approved by Trust D&TC: January 2010 Revised March 2017 Contents Paragraph Page 1 Aim 4 2 Introduction 4 3 Assessment of renal function
E-Learning Module N: Pharmacological Review
 E-Learning Module N: Pharmacological Review This Module requires the learner to have read Chapter 13 of the Fundamentals Program Guide and the other required readings associated with the topic. Revised:
E-Learning Module N: Pharmacological Review This Module requires the learner to have read Chapter 13 of the Fundamentals Program Guide and the other required readings associated with the topic. Revised:
Objectives. Symptom Management in the Frail Elderly Population. Disclosures. Symptom Management: Pain 12/05/2014
 Objectives Symptom Management in the Frail Elderly Population Dr. Katie Marchington, MD, CCFP Palliative Care Physician Toronto Western Hospital Kensington Hospice To reflect on why we should identify
Objectives Symptom Management in the Frail Elderly Population Dr. Katie Marchington, MD, CCFP Palliative Care Physician Toronto Western Hospital Kensington Hospice To reflect on why we should identify
OPIOID- INDUCED NEUROTOXICITY*
 OPIOID- INDUCED NEUROTOXICITY* Sriram Yennu MD, MS, FAAHPM Palliative Care, Rehabilitation and Integrative Medicine U.T. M.D. Anderson Cancer Center *Slide Deck courtesy Dept PRIM MDACC PATIENT #1: MRS
OPIOID- INDUCED NEUROTOXICITY* Sriram Yennu MD, MS, FAAHPM Palliative Care, Rehabilitation and Integrative Medicine U.T. M.D. Anderson Cancer Center *Slide Deck courtesy Dept PRIM MDACC PATIENT #1: MRS
Optimizing Your Quality of Life During Cancer Treatment: Pain & Side Effect Management
 Optimizing Your Quality of Life During Cancer Treatment: Pain & Side Effect Management Eric Roeland, MD GI Oncology Palliative Medicine Pancreatic Cancer Patient Tool Belt Chemotherapy Surgery Pain & Symptom
Optimizing Your Quality of Life During Cancer Treatment: Pain & Side Effect Management Eric Roeland, MD GI Oncology Palliative Medicine Pancreatic Cancer Patient Tool Belt Chemotherapy Surgery Pain & Symptom
Waterloo Wellington (WW) Symptom Management Guideline for the End of Life (EOL) Medication Order Set for Long Term Care (LTC)
 Symptom Management Guideline for the End of Life (EOL) Medication Order Set for Long Term Care (LTC)") Waterloo Wellington (WW) Symptom Management Guideline for the End of Life (EOL) Medication Order Set for Long Term Care (LTC) May 2018 THE WATERLOO WELLINGTON SYMPTOM MANAGEMENT GUIDELINE FOR THE END OF
Waterloo Wellington (WW) Symptom Management Guideline for the End of Life (EOL) Medication Order Set for Long Term Care (LTC) May 2018 THE WATERLOO WELLINGTON SYMPTOM MANAGEMENT GUIDELINE FOR THE END OF
Chronic Kidney Disease. Basics of CKD Terms Diagnosis Management
 Chronic Kidney Disease Basics of CKD Terms Diagnosis Management Review the prevalence of chronic kidney disease (CKD) Review how CKD develops Review populations at risk for CKD Review CKD diagnosis Objectives
Chronic Kidney Disease Basics of CKD Terms Diagnosis Management Review the prevalence of chronic kidney disease (CKD) Review how CKD develops Review populations at risk for CKD Review CKD diagnosis Objectives
Canadian Guideline for Opioids for Chronic Non-Cancer Pain. Speaker Disclosure. Objectives. Canadian Guideline for Opioids for Chronic Non-Cancer Pain
 Canadian Guideline for Opioids for Chronic Non-Cancer Pain John Fraser Community Hospital Program New Glasgow November 1, 2017 This speaker has been asked to disclose to the audience any involvement with
Canadian Guideline for Opioids for Chronic Non-Cancer Pain John Fraser Community Hospital Program New Glasgow November 1, 2017 This speaker has been asked to disclose to the audience any involvement with
Acute Pain Management in the Hospital Setting. Alexandra Phan, PharmD PGY-1 Pharmacy Practice Resident Medical Center Hospital Odessa, TX
 Acute Pain Management in the Hospital Setting Alexandra Phan, PharmD PGY-1 Pharmacy Practice Resident Medical Center Hospital Odessa, TX 2 What is Pain? An unpleasant sensory and emotional experience associated
Acute Pain Management in the Hospital Setting Alexandra Phan, PharmD PGY-1 Pharmacy Practice Resident Medical Center Hospital Odessa, TX 2 What is Pain? An unpleasant sensory and emotional experience associated
Neuropathic Pain Treatment Guidelines
 Neuropathic Pain Treatment Guidelines Background Pain is an unpleasant sensory and emotional experience that can have a significant impact on a person s quality of life, general health, psychological health,
Neuropathic Pain Treatment Guidelines Background Pain is an unpleasant sensory and emotional experience that can have a significant impact on a person s quality of life, general health, psychological health,
9/30/2017. Case Study: Complete Pain Assessment and Multimodal Approach to Pain Management. Program Objectives. Impact of Poorly Managed Pain
 Case Study: Complete Pain Assessment and Multimodal Approach to Pain Management MARY BETH PARTYKA MSN ADULT NURSE PRACTITIONER ADVOCATE CHRIST MEDICAL CENTER ADULT PAIN SERVICE Program Objectives Identify
Case Study: Complete Pain Assessment and Multimodal Approach to Pain Management MARY BETH PARTYKA MSN ADULT NURSE PRACTITIONER ADVOCATE CHRIST MEDICAL CENTER ADULT PAIN SERVICE Program Objectives Identify
Supportive Care. End of Life Phase
 Supportive Care End of Life Phase Guidelines for Health Care Professionals In the care of patients with established renal failure who are in the last days of life References: Chambers E J (2004) End of
Supportive Care End of Life Phase Guidelines for Health Care Professionals In the care of patients with established renal failure who are in the last days of life References: Chambers E J (2004) End of
Palliative Care in Chronic Kidney Disease: Past Successes, Remaining Challenges. Sara Davison BC Nephrology Days, Vancouver, BC Nov 6, 2009
 Palliative Care in Chronic Kidney Disease: Past Successes, Remaining Challenges Sara Davison BC Nephrology Days, Vancouver, BC Nov 6, 2009 Objectives Highlight the relevance of palliative/supportive care
Palliative Care in Chronic Kidney Disease: Past Successes, Remaining Challenges Sara Davison BC Nephrology Days, Vancouver, BC Nov 6, 2009 Objectives Highlight the relevance of palliative/supportive care
Mid Essex Locality Guideline for Management of Adult Acute and Chronic Non-Cancer Pain in Primary care
 Guideline for Management of Adult Acute and Chronic Non-Cancer Pain in Primary care If possible patients should be assessed using a simple visual analogue scale VAS to determine the most appropriate stage
Guideline for Management of Adult Acute and Chronic Non-Cancer Pain in Primary care If possible patients should be assessed using a simple visual analogue scale VAS to determine the most appropriate stage
Dementia Medications Acetylcholinesterase Inhibitors (AChEIs) and Glutamate (NMDA) Receptor Antagonist
 and Glutamate (NMDA) Receptor Antagonist") Dementia Medications Acetylcholinesterase Inhibitors (AChEIs) and Glutamate (NMDA) Receptor Antagonist Medication Dosage Indication for Use Aricept (donepezil) Exelon (rivastigmine) 5mg 23mg* ODT 5mg Solution
Dementia Medications Acetylcholinesterase Inhibitors (AChEIs) and Glutamate (NMDA) Receptor Antagonist Medication Dosage Indication for Use Aricept (donepezil) Exelon (rivastigmine) 5mg 23mg* ODT 5mg Solution
Renal Supportive Care an overview. Frank Brennan, Palliative Care Physician.
 Renal Supportive Care an overview. Frank Brennan, Palliative Care Physician. 2014 Renal Palliative Care Caring for adult patients with ESKD an overview Frank Brennan Palliative Care Consultant Department
Renal Supportive Care an overview. Frank Brennan, Palliative Care Physician. 2014 Renal Palliative Care Caring for adult patients with ESKD an overview Frank Brennan Palliative Care Consultant Department
Nociceptive Pain. Pathophysiologic Pain. Types of Pain. At Presentation. At Presentation. Nonpharmacologic Therapy. Modulation
 Learning Objectives Effective, Safe Analgesia An Approach to Appropriate Outpatient Chronic Pain Treatment By the end of this presentation, participants will be able to: Identify multiple factors that
Learning Objectives Effective, Safe Analgesia An Approach to Appropriate Outpatient Chronic Pain Treatment By the end of this presentation, participants will be able to: Identify multiple factors that
Geriatric Pharmacology
 Geriatric Pharmacology Janice Scheufler R.Ph.,PharmD, FASCP Clinical Pharmacist Hospice of the Western Reserve Objectives List three risk factors for adverse drug events in the elderly Discuss two physiological
Geriatric Pharmacology Janice Scheufler R.Ph.,PharmD, FASCP Clinical Pharmacist Hospice of the Western Reserve Objectives List three risk factors for adverse drug events in the elderly Discuss two physiological
What s New 2003? What new treatments? What have you discontinued? More information please!
 What s New 2003? What new treatments? What have you discontinued? More information please! 1 What s New 2003? Submissions = 137 UK = 52 (38%) Doctors = 60% Nurses = 25% Pharmacists = 15% 2 What s New?
What s New 2003? What new treatments? What have you discontinued? More information please! 1 What s New 2003? Submissions = 137 UK = 52 (38%) Doctors = 60% Nurses = 25% Pharmacists = 15% 2 What s New?
Palliative Medicine Overview. Francine Arneson, MD Palliative Medicine
 Palliative Medicine Overview Francine Arneson, MD Palliative Medicine Palliative Medicine: Definition Palliative care: An approach that improves the quality of life of patients and their families facing
Palliative Medicine Overview Francine Arneson, MD Palliative Medicine Palliative Medicine: Definition Palliative care: An approach that improves the quality of life of patients and their families facing
Nausea and Vomiting in Palliative Care
 Nausea and Vomiting in Palliative Care Definitions Nausea - an unpleasant feeling of the need to vomit Vomiting - the expulsion of gastric contents through the mouth, caused by forceful and sustained contraction
Nausea and Vomiting in Palliative Care Definitions Nausea - an unpleasant feeling of the need to vomit Vomiting - the expulsion of gastric contents through the mouth, caused by forceful and sustained contraction
HOPE. Considerations. Considerations ISING. Safe Opioid Prescribing Guidelines for ACUTE Non-Malignant Pain
 Due to the high level of prescription drug use and abuse in Lake County, these guidelines have been developed to standardize prescribing habits and limit risk of unintended harm when prescribing opioid
Due to the high level of prescription drug use and abuse in Lake County, these guidelines have been developed to standardize prescribing habits and limit risk of unintended harm when prescribing opioid
Non-opioid and adjuvant pain management
 Non-opioid and adjuvant pain management ALLISON JORDAN, MD, HMDC MEDICAL DIRECTOR OF PALLIATIVE CARE SERVICES CHRISTIAN AND ALTON MEMORIAL HOSPITALS ASSOCIATE MEDICAL DIRECTOR, BJC HOSPICE ASSISTANT PROFESSOR
Non-opioid and adjuvant pain management ALLISON JORDAN, MD, HMDC MEDICAL DIRECTOR OF PALLIATIVE CARE SERVICES CHRISTIAN AND ALTON MEMORIAL HOSPITALS ASSOCIATE MEDICAL DIRECTOR, BJC HOSPICE ASSISTANT PROFESSOR
Pharm-D candidate (KSU)
") Topic review & case presentation Noor Naif Al-Hakami Pharm-D candidate (KSU) 2014 According to The National Kidney Foundation Kidney Disease Outcome Quality Initiative (KDOQI): Kidney damage for more than
Topic review & case presentation Noor Naif Al-Hakami Pharm-D candidate (KSU) 2014 According to The National Kidney Foundation Kidney Disease Outcome Quality Initiative (KDOQI): Kidney damage for more than
Symptom Management Pocket Guides: DELIRIUM
 Symptom Management Pocket Guides: DELIRIUM August 2010 DELIRIUM Page Considerations. 1 Assessment 2 Diagnosis. 3 Non-Pharmacological treatment 3 Pharmacological treatment. 5 Mild Delirium... 6 Moderate
Symptom Management Pocket Guides: DELIRIUM August 2010 DELIRIUM Page Considerations. 1 Assessment 2 Diagnosis. 3 Non-Pharmacological treatment 3 Pharmacological treatment. 5 Mild Delirium... 6 Moderate
SUMMARY OF ARIZONA OPIOID PRESCRIBING GUIDELINES FOR THE TREATMENT OF CHRONIC NON-TERMINAL PAIN (CNTP)
") 9 SUMMARY OF ARIZONA OPIOID PRESCRIBING GUIDELINES FOR THE TREATMENT OF CHRONIC NON-TERMINAL PAIN (CNTP) SUMMARY OF ARIZONA OPIOID PRESCRIBING GUIDELINES FOR THE TREATMENT OF ACUTE PAIN NONOPIOID TREATMENTS
9 SUMMARY OF ARIZONA OPIOID PRESCRIBING GUIDELINES FOR THE TREATMENT OF CHRONIC NON-TERMINAL PAIN (CNTP) SUMMARY OF ARIZONA OPIOID PRESCRIBING GUIDELINES FOR THE TREATMENT OF ACUTE PAIN NONOPIOID TREATMENTS
Pain Management Dilemmas. Five Pain Dilemmas. Barriers: Meet Loretta. Daniel Johnson, MD, FAAHPM
 Pain Management Dilemmas Daniel Johnson, MD, FAAHPM Kaiser Permanente University of Colorado Five Pain Dilemmas 1. Barriers to Pain Management 2. Selecting and Titrating Opioids 3. Managing PCAs 4. Using
Pain Management Dilemmas Daniel Johnson, MD, FAAHPM Kaiser Permanente University of Colorado Five Pain Dilemmas 1. Barriers to Pain Management 2. Selecting and Titrating Opioids 3. Managing PCAs 4. Using
In our patients the cause of seizures can be broadly divided into structural and systemic causes.
 Guidelines for the management of Seizures Amalgamation and update of previous policies 7 (Seizure guidelines, ND, 2015) and 9 (Status epilepticus, KJ, 2011) Seizures can occur in up to 15% of the Palliative
Guidelines for the management of Seizures Amalgamation and update of previous policies 7 (Seizure guidelines, ND, 2015) and 9 (Status epilepticus, KJ, 2011) Seizures can occur in up to 15% of the Palliative
Pain Management in the Elderly. Martha Watson, MS, APRN, GCNS Christie Bowser, RN-BC, RN
 Pain Management in the Elderly Martha Watson, MS, APRN, GCNS Christie Bowser, RN-BC, RN Objectives So How Much Do You Really Know? www.geriatricpain.org Geriatric Pain Knowledge Assessment The Geriatric
Pain Management in the Elderly Martha Watson, MS, APRN, GCNS Christie Bowser, RN-BC, RN Objectives So How Much Do You Really Know? www.geriatricpain.org Geriatric Pain Knowledge Assessment The Geriatric
CHAMP: Bedside Teaching TREATING PAIN. Stacie Levine MD. What is the approach to treating pain in the aging adult patient?
 CHAMP: Bedside Teaching TREATING PAIN Stacie Levine MD Teaching Trigger: An older adult patient is identified as having pain. Clinical Question: What is the approach to treating pain in the aging adult
CHAMP: Bedside Teaching TREATING PAIN Stacie Levine MD Teaching Trigger: An older adult patient is identified as having pain. Clinical Question: What is the approach to treating pain in the aging adult
Measure #403: Adult Kidney Disease: Referral to Hospice National Quality Strategy Domain: Patient and Caregiver-Centered Experience and Outcomes
 Measure #403: Adult Kidney Disease: Referral to Hospice National Quality Strategy Domain: Patient and Caregiver-Centered Experience and Outcomes 2017 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE
Measure #403: Adult Kidney Disease: Referral to Hospice National Quality Strategy Domain: Patient and Caregiver-Centered Experience and Outcomes 2017 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE