Acute Abdomen. Nirav Patel MD, FACS Banner University Medical Center - Phoenix
|
|
|
- Norman Bailey
- 5 years ago
- Views:
Transcription

1 Acute Abdomen Nirav Patel MD, FACS Banner University Medical Center - Phoenix
2 ? Diffuse periumbilical with localization to RLQ + Nausea, anorexia, fevers - Diarrhea, emesis Exacerbated by movement, bumps Lo grade fever TTP with rebound RLQ: McBurney s point, Rovsing s sign. WBC: 12, UA: + leuckocytes



3 enlarged appendix diameter = 12mm minimal peri-appediceal inflammatory change








4 Management Appendectomy: Open Laparoscopic
5
6 Non-operative management Several systematic reviews and metaanalyses compared the safety and efficacy of antibiotic treatment versus appendectomy for the primary treatment of uncomplicated, acute appendicitis: Patients treated with antibiotics had fewer major (4.9 versus 8.4 percent) or minor (2.2 versus 12.5 percent) complications compared with those who underwent surgery. Most patients assigned to the antibiotic-first approach were able to avoid appendectomy initially, although up to 53 percent of patients crossed over to surgery within the first 48 hours of antibiotic treatment. Patients in the antibiotic-first group had favorable clinical outcomes (including reduction in whitecell count avoidance of peritonitis and general symptom reduction As compared with the appendectomy group, patients in the antibiotic-first group had lower or similar pain scores required fewer doses of narcotics and had a quicker return to work As compared with the appendectomy group, the rate of perforation was not higher in the antibiotic-first group. After initial treatment success, 10 to 37 percent of the patients in the antibiotic-first group eventually required appendectomy for recurrent appendicitis or symptoms of abdominal pain (mean time to appendectomy, 4.2 to 7 months). A separate, observational study showed an overall recurrence rate of 13.8 percent in 159 patients treated initially with antibiotics then followed for two years Although high-risk patients (eg, older adults, immunocompromised, patients with medical comorbidities) could potentially benefit the most from nonsurgical treatment of appendicitis, they were excluded from all trials cited above. Thus, the efficacy of the antibiotic-first approach to management of appendicitis in this group of patients remains unknown.


7 Perforated Appendicitis Phlegmon: Antimicrobial therapy Abscess: perq drainage Interval Appendectomy
8 Interval Appendectomy Traditionally, an interval appendectomy has been recommended for these patients six to eight weeks after presentation for two primary reasons: To prevent recurrence of appendicitis [8,66]. To exclude neoplasms (such as carcinoid, adenocarcinoma, mucinous cystadenoma, and cystadenocarcinomas) especially in older adults who have higher incidences of appendiceal neoplasm. Patients (>50, appropriate family hx) should also have a colonoscopy to rule out cecal pathology. The need for interval appendectomy is debated: A malignant disease was detected in 1.2 percent of cases and an important benign disease in 0.7 percent. Recurrent appendicitis developed in 7.4 percent of cases (95% CI ).



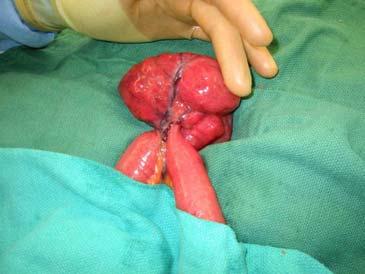
9 Fakeout! Mesenteric adenitis: gut flu Meckel s diverticulitis: Rules of 2 Tubo-ovarian pathology Infarcted appendiceal epiploicae
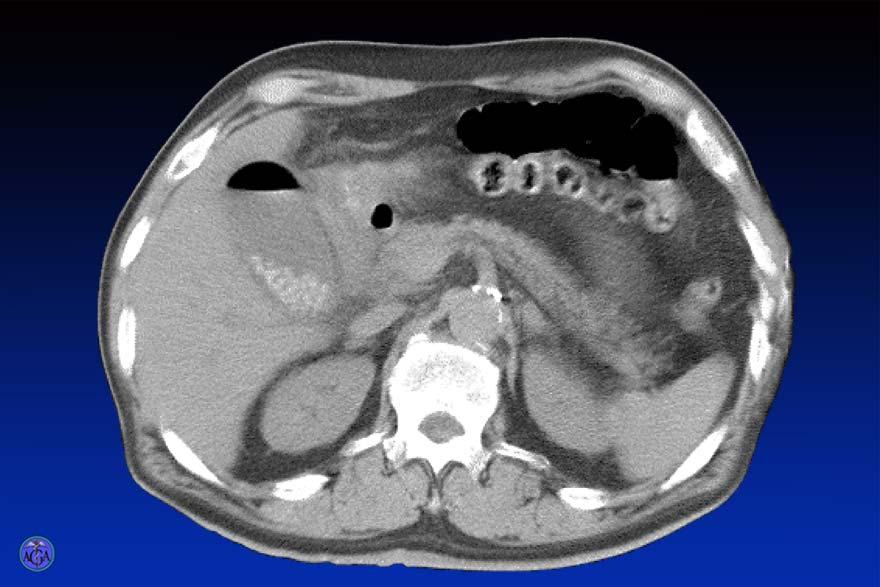
10 ? 70 y/o woman with abdominal pain. Crampy, waves, twisting + Nausea, emesis. Intolerance of po intake - flatus, BM: small PSHX includes hysterectomy, appy.
11 ? VS: Afebrile, normotensive PE: distended, tympanitic, hi pithched BS. Minimally TTP, no peritoneal signs WBC: WNL
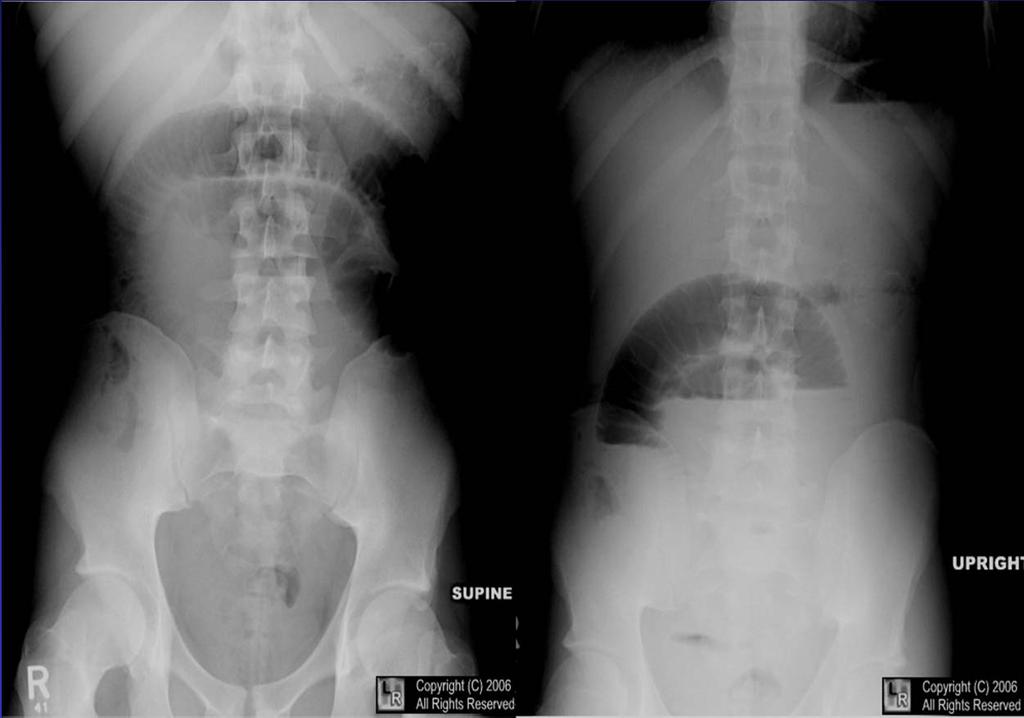

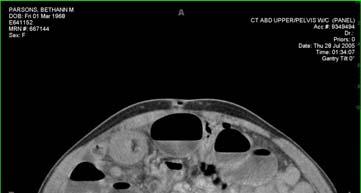
12 Imaging
13 Where is the obstruction? Proximal Breath: Bitter Abdomen (Inspection): Scaphoid Abdomen (Auscultation): Borborygmi Abdomen (Palpation): Variable Abdomen (Percussion): Dull Distal Breath: Feculent Abdomen (Inspection): Rotund Abdomen (Auscultation): Quiet Abdomen (Palpation): Achy Abdomen (Percussion): Tympanitic





14 - Adhesions SBO: Etiology -Hernia

15 - Malignancy SBO: Etiology - Iatrogenic

16 Management - Partial vs Complete - Uncomplicated vs Complicated Leukocytosis, acidosis, pneumatosis, free air
17 Partial Uncomplicated Non-operative management: NPO, IVF, +/- NG decompression 90-95% resolution w/in 72 hours.
18 Gastrointestinal Secretions Organ/ Fluid Plasma Salivary Stomach Duodenum Pancreas Liver Small Bowel Colon 0.9% NS Ringer s lactate Volume/ Day Na (meq/l) K (meq/l) Cl (meq/l) HCO 3 (meq/l) * Scant ** * Also 60 meq H + /L **14 meq/l converted to HCO 3- by the liver


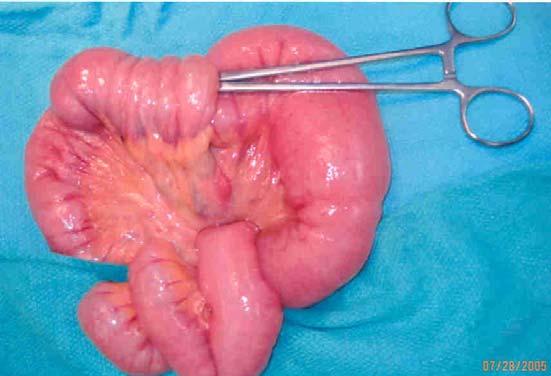
19 Refractory/Complete/ Complicated Operative intervention: Open Laparoscopic
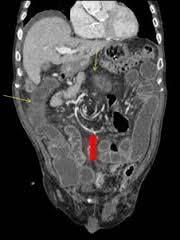
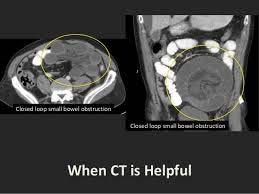
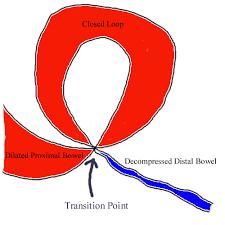
20 Whirl sign Refractory/Complete/ Complicated Portal Venous air Closed loop
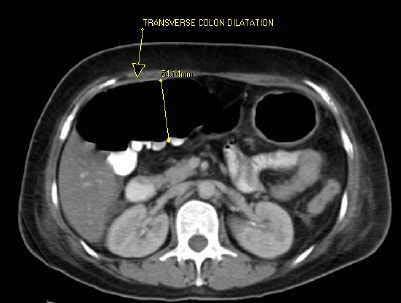
21 ? 65yo M sudden onset of AP at 6pm Sharp, diffuse Exacerbated by movement, deep breaths + nausea, denies emesis Hx of recent NSAID use for hip pain
22 ? Afebrile, hypotensive, tachycardic Distress Diffuse peritoneal findings




23 Imaging


24 Management IVF resuscitation, antimicrobial therapy, OR: Laparotomy Laparoscopy
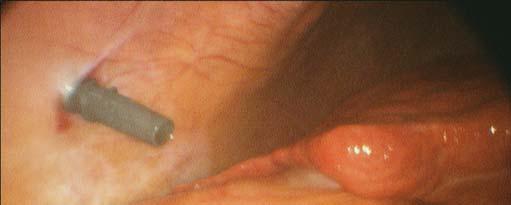
25 ? Elderly nursing home resident brought in for progressive abdominal distension, nausea, anorexia.? Flatus, No BMx 3days Relatively immobile, Multiple medications Afebrile, mild tachycardia Abd: significantly distended, tympanitic


26 Imaging


27 Management Endoscopic decompression Open vs Laparoscopic sigmoid ressection
28 ? 42yoF, awoken with epigastric discomfort Sharp, radiating around to her back on right + nausea, emesis Cheese pizza for dinner Lo grade temp, mildly tachycardic Moderate distress TTP epigastrium, RUQ, no peritoneal signs WBC, LFT :WNL Symptoms resolved with analgesia administration
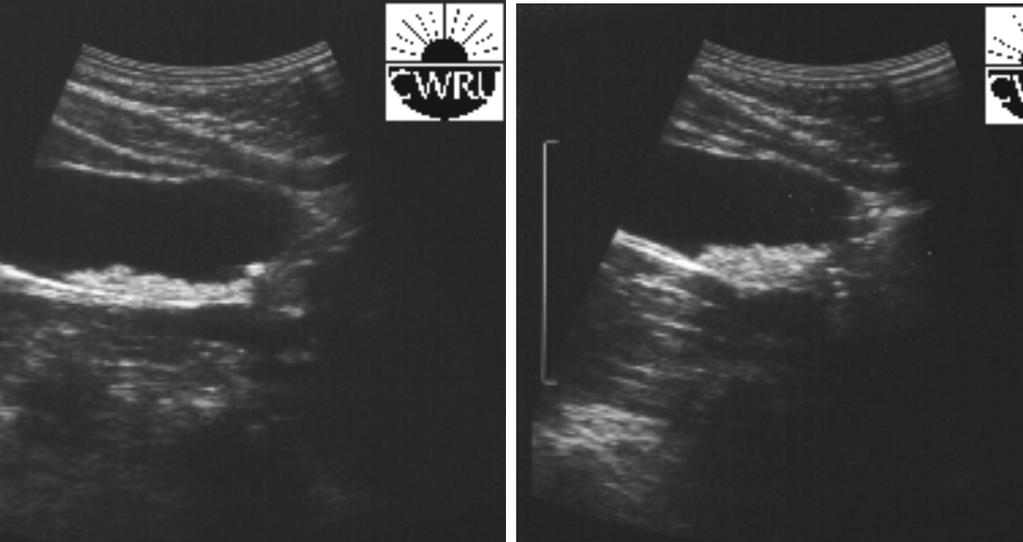

29 Imaging
30 Natural History Asymptomatic Stones 5yrs 10% symptomatic (2%/yr) 10yrs 15% symptomatic 15yrs 18% symptomatic ***90% who become symptomatic initially have just biliary colic Cholecystectomy not needed Symptomatic stones 50% develop recurrent sx 1-2%/yr develop complications of gallstone disease Gracie and Ransohoff. NEJM. 1982



31 Symptomatic Stones

32 Acute Calculous Cholecystitis Lab: WBC, LFT US: Wall thickening (>4mm), pericholecystic fluid, sonographic Murphy s HIDA scan: No filling of gallbladder Immidiate vs Interval Cholecystectomy PerQ Cholecystostomy tube placement
33 Biliary Pancreatitis Fold increase over normal Lipase Amylase Hours after onset Cholecystectomy during same hospitalization

34 Cholangitis Charcot s Triad: RUQ pain, Jaundice, Fever Reynold s Pentad: Hypotension, MS change Endoscopic, PerQ, Laparoscopic/Open decompression


35 Endoscopic
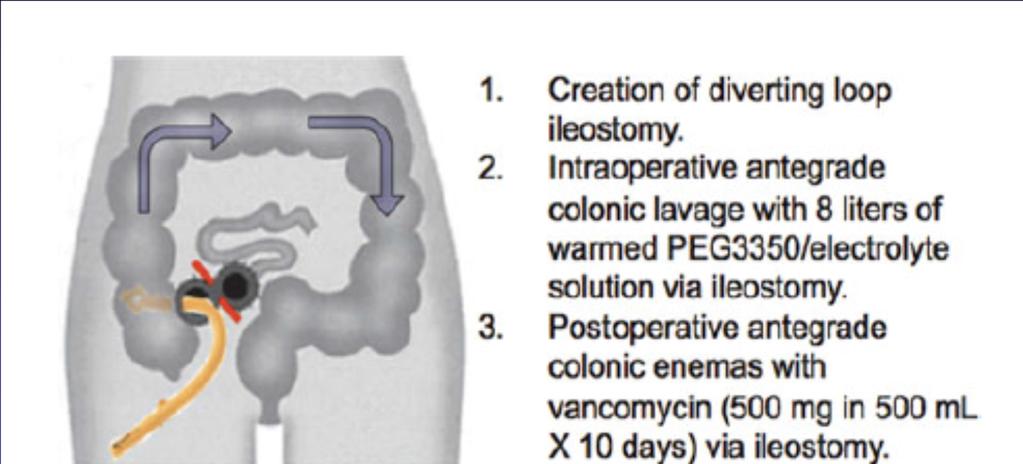
36 A 37 year-old woman is evaluated in the emergency department for the acute onset of pain after 2 weeks of bloody diarrhea.?pmh/meds On physical examination, she appears ill, febrile, hypotensive, tachycardic and tachypneic. Abdominal examination discloses absent bowel sounds, distention, and diffuse marked tenderness with mild palpation. Lab: WBC 19, Lactate 9. XRay



37
38
39
Management of Gallbladder Disease
 Management of Gallbladder Disease Steven B. Johnson, MD, FACS, FCCM Professor and Chairman, Department of Surgery Program Director, Phoenix Integrated Surgical Residency University of Arizona College of
Management of Gallbladder Disease Steven B. Johnson, MD, FACS, FCCM Professor and Chairman, Department of Surgery Program Director, Phoenix Integrated Surgical Residency University of Arizona College of
GENERAL SURGERY FOR SMART PEOPLE JOE NOLD MD, FACS WICHITA SURGICAL SPECIALISTS
 GENERAL SURGERY FOR SMART PEOPLE JOE NOLD MD, FACS WICHITA SURGICAL SPECIALISTS CONFLICTS/DECLARATIONS I have no financial conflicts or declarations I AM always willing to see a consult for you TEXT TOPICS
GENERAL SURGERY FOR SMART PEOPLE JOE NOLD MD, FACS WICHITA SURGICAL SPECIALISTS CONFLICTS/DECLARATIONS I have no financial conflicts or declarations I AM always willing to see a consult for you TEXT TOPICS
Abdominal Pain. Luke Donnelly, MD Emergency Medicine
 Abdominal Pain Luke Donnelly, MD Emergency Medicine Objectives Approach to abdominal pain Evaluation Critical diagnoses and treatments Abdominal Pain Most Common ER Complaint Broad Differential Can often
Abdominal Pain Luke Donnelly, MD Emergency Medicine Objectives Approach to abdominal pain Evaluation Critical diagnoses and treatments Abdominal Pain Most Common ER Complaint Broad Differential Can often
The Acute Abdomen New Mexico Nurse Practitioner Council Annual Conference, 2012
 The Acute Abdomen New Mexico Nurse Practitioner Council Annual Conference, 2012 Darra D. Kingsley, MD Associate Professor, Surgery, University of New Mexico School of Medicine Associate Chief of Staff,
The Acute Abdomen New Mexico Nurse Practitioner Council Annual Conference, 2012 Darra D. Kingsley, MD Associate Professor, Surgery, University of New Mexico School of Medicine Associate Chief of Staff,
Surgical Education Series
 Surgical Education Series The Acute Abdomen Ahmad kachooei, MD MPH Assistant Professor Division of General Surgery Department of Surgery University of Qom Outline Definitions What causes an acute abdomen
Surgical Education Series The Acute Abdomen Ahmad kachooei, MD MPH Assistant Professor Division of General Surgery Department of Surgery University of Qom Outline Definitions What causes an acute abdomen
General Surgery Service
 General Surgery Service Patient Care Goals and Objectives Stomach/Duodenum and Bariatric assessed for a) Obesity surgery b) Treatment of i) Adenocarcinoma of the stomach ii) GIST iii) Carcinoid 2) Optimize
General Surgery Service Patient Care Goals and Objectives Stomach/Duodenum and Bariatric assessed for a) Obesity surgery b) Treatment of i) Adenocarcinoma of the stomach ii) GIST iii) Carcinoid 2) Optimize
General'Surgery'Service'
 General'Surgery'Service' Patient Care Goals and Objectives 1)! Stomach/Duodenum and Bariatric 2)! Interpret the results of clinical evaluations (history, physical examination) performed on patients being
General'Surgery'Service' Patient Care Goals and Objectives 1)! Stomach/Duodenum and Bariatric 2)! Interpret the results of clinical evaluations (history, physical examination) performed on patients being
Management of Gallbladder Disease. Cory Buschmann, MD PGY-5 11/28/2017
 Management of Gallbladder Disease Cory Buschmann, MD PGY-5 11/28/2017 Financial disclosures None Content Scope of gallbladder diseases Evaluation H&P Labs Imaging Cholecystectomy vs cholecystostomy Ancillary
Management of Gallbladder Disease Cory Buschmann, MD PGY-5 11/28/2017 Financial disclosures None Content Scope of gallbladder diseases Evaluation H&P Labs Imaging Cholecystectomy vs cholecystostomy Ancillary
Always keep it in the differential
 Acute Appendicitis Lissa C. Sakata and Lindsey Perea 2 Always keep it in the differential Learning Objectives 1. The learner should be able to describe the etiology of acute appendicitis. 2. The learner
Acute Appendicitis Lissa C. Sakata and Lindsey Perea 2 Always keep it in the differential Learning Objectives 1. The learner should be able to describe the etiology of acute appendicitis. 2. The learner
Causes of abdominal pain Doctors in the ED spend lots of time and money diagnosing abdominal pain. They still often do not know the exact cause
 1 2 3 What's Going On in There? EMS and Abdominal Pain Kevin McFarlane BSN,RN,CEN,CPEN,EMT Southwest Emergency Education and Consulting What is going on in there Acute Abdomen Sudden onset of pain within
1 2 3 What's Going On in There? EMS and Abdominal Pain Kevin McFarlane BSN,RN,CEN,CPEN,EMT Southwest Emergency Education and Consulting What is going on in there Acute Abdomen Sudden onset of pain within
ACUTE ABDOMEN. Dr. M Asadi. Surgical Oncology Research Center MUMS. Assistant Professor of General Surgery
 ACUTE ABDOMEN Dr. M Asadi Assistant Professor of General Surgery Surgical Oncology Research Center MUMS Definition I. The term Acute Abdomen refers to signs & symptoms of abdominal pain and tenderness,
ACUTE ABDOMEN Dr. M Asadi Assistant Professor of General Surgery Surgical Oncology Research Center MUMS Definition I. The term Acute Abdomen refers to signs & symptoms of abdominal pain and tenderness,
Abdominal pain is a common complaint. Acute Surgical. The Basics
 Acute Surgical The Basics When a patient presents to the ED with acute abdominal pain, the emergency physician s role in taking a history, performing an exam, selecting the appropriate imaging modality,
Acute Surgical The Basics When a patient presents to the ED with acute abdominal pain, the emergency physician s role in taking a history, performing an exam, selecting the appropriate imaging modality,
Abdominal Assessment
 Abdominal Assessment Mary Marian, MS,RD,CSO University of AZ, Tucson, AZ Neha Parekh, MS,RD,LD,CNSC Cleveland Clinic, Cleveland, OH Objectives: 1. Outline the steps in performing an abdominal examination.
Abdominal Assessment Mary Marian, MS,RD,CSO University of AZ, Tucson, AZ Neha Parekh, MS,RD,LD,CNSC Cleveland Clinic, Cleveland, OH Objectives: 1. Outline the steps in performing an abdominal examination.
12 Blueprints Q&A Step 2 Surgery
 12 Blueprints Q&A Step 2 Surgery 34. A 40-year-old female has been referred to you for a recent ER and hospital admission, from which she was given a diagnosis of acute diverticulitis. Treatment at that
12 Blueprints Q&A Step 2 Surgery 34. A 40-year-old female has been referred to you for a recent ER and hospital admission, from which she was given a diagnosis of acute diverticulitis. Treatment at that
Resident Teaching Conference 10/16/09 Rondi Kauffmann Resident presenter William Nealon Faculty presenter
 Resident Teaching Conference 10/16/09 Rondi Kauffmann Resident presenter William Nealon Faculty presenter KC 59 year old male Referred to Surgery clinic for incidentally discovered 5cm x 3cm pancreatic
Resident Teaching Conference 10/16/09 Rondi Kauffmann Resident presenter William Nealon Faculty presenter KC 59 year old male Referred to Surgery clinic for incidentally discovered 5cm x 3cm pancreatic
An Approach to Abdominal Pain
 An Approach to Abdominal Pain objectives Should know the different types of abd pain Is acute or chronic? Hx taking skills with knowing the key questions Important abdominal pain signs A good differential
An Approach to Abdominal Pain objectives Should know the different types of abd pain Is acute or chronic? Hx taking skills with knowing the key questions Important abdominal pain signs A good differential
USMLE and COMLEX II. CE / CK Review. General Surgery. 1. Northwestern Medical Review
 USMLE and COMLEX II CE / CK Review General Surgery 1. Northwestern Medical Review Northwestern Medical Review www.northwesternmedicalreview.com Lansing, Michigan 2014-2015 Acute Abdomen 1. Your patient
USMLE and COMLEX II CE / CK Review General Surgery 1. Northwestern Medical Review Northwestern Medical Review www.northwesternmedicalreview.com Lansing, Michigan 2014-2015 Acute Abdomen 1. Your patient
Medical Management of Appendicitis: Are We There Yet? Monica E. Lopez, MD, FACS, FAAP
 Medical Management of Appendicitis: Are We There Yet? Monica E. Lopez, MD, FACS, FAAP Texas Children s Hospital Objectives Discuss the surgical and non-operative approaches to the treatment of appendicitis
Medical Management of Appendicitis: Are We There Yet? Monica E. Lopez, MD, FACS, FAAP Texas Children s Hospital Objectives Discuss the surgical and non-operative approaches to the treatment of appendicitis
Management of Small Bowel Obstruction: An Update. Case Presentation
 Management of Small Bowel Obstruction: An Update The Postgraduate Course in General Surgery March 20-23, 2011 Jonathan Carter, MD Assistant Professor of Surgery Case Presentation 67 year old otherwise
Management of Small Bowel Obstruction: An Update The Postgraduate Course in General Surgery March 20-23, 2011 Jonathan Carter, MD Assistant Professor of Surgery Case Presentation 67 year old otherwise
3/21/2011. Case Presentation. Management of Small Bowel Obstruction: An Update. CT abdomen and pelvis. Abdominal plain films
 Case Presentation 67 year old otherwise healthy woman presents to the ED with a chief complaint of abdominal pain, nausea and vomiting for five days. Management of Small Bowel Obstruction: An Update The
Case Presentation 67 year old otherwise healthy woman presents to the ED with a chief complaint of abdominal pain, nausea and vomiting for five days. Management of Small Bowel Obstruction: An Update The
A 34 year old woman with Vomiting and abdominal pain
 A 34 year old woman with Vomiting and abdominal pain The patient was a 34 y/o woman admitted because of epigastric pain developed from 2 months ago. It was a crampy pain without radiation that became better
A 34 year old woman with Vomiting and abdominal pain The patient was a 34 y/o woman admitted because of epigastric pain developed from 2 months ago. It was a crampy pain without radiation that became better
Pediatric Surgical Emergencies Veronica Victorian, PA-C
 Pediatric Surgical Emergencies Veronica Victorian, PA-C Texas Children s Hospital Division of Pediatric General Surgery Assistant Professor, Baylor College of Medicine Objectives 1. Define Pediatric Surgical
Pediatric Surgical Emergencies Veronica Victorian, PA-C Texas Children s Hospital Division of Pediatric General Surgery Assistant Professor, Baylor College of Medicine Objectives 1. Define Pediatric Surgical
3/22/2011. Inflammatory Bowel Disease. Inflammatory Bowel Disease Objectives: Appendicitis. Lemone and Burke Chapter 26
 Inflammatory Bowel Disease Lemone and Burke Chapter 26 Inflammatory Bowel Disease Objectives: Discuss etiology, patho and clinical manifestations of Appendicitis Peritonitis Ulcerative Colitis Crohn s
Inflammatory Bowel Disease Lemone and Burke Chapter 26 Inflammatory Bowel Disease Objectives: Discuss etiology, patho and clinical manifestations of Appendicitis Peritonitis Ulcerative Colitis Crohn s
Plain Radiographs in Non-Traumatic Abdominal Pain. Plain Radiographs in Non-Traumatic Abdominal Pain
 Jake Block, MD Associate Professor Associate Vice-Chairman for Clinical Operations Director, Musculoskeletal and Emergency Radiology Department of Radiology and Radiological Sciences Vanderbilt University
Jake Block, MD Associate Professor Associate Vice-Chairman for Clinical Operations Director, Musculoskeletal and Emergency Radiology Department of Radiology and Radiological Sciences Vanderbilt University
Case Discussion Splenic Abscess
 Case Discussion Splenic Abscess Personal Data Gender: male Birth Date: 1928/Mar/06th Allergy: Mefenamic Smoking: 0.5 PPD for 55 years Alcohol: negative (?) 4 Months Ago Abdominal pain: epigastric area
Case Discussion Splenic Abscess Personal Data Gender: male Birth Date: 1928/Mar/06th Allergy: Mefenamic Smoking: 0.5 PPD for 55 years Alcohol: negative (?) 4 Months Ago Abdominal pain: epigastric area
Surgical Management of IBD. Val Jefford Grand Rounds October 14, 2003
 Surgical Management of IBD Val Jefford Grand Rounds October 14, 2003 Introduction Important Features Clinical Presentation Evaluation Medical Treatment Surgical Treatment Cases Overview Introduction Two
Surgical Management of IBD Val Jefford Grand Rounds October 14, 2003 Introduction Important Features Clinical Presentation Evaluation Medical Treatment Surgical Treatment Cases Overview Introduction Two
9/21/15. Joshua Pruitt, MD, FAAEM Medical Director, LifeGuard Air Ambulance Iowa PA Society Fall CME Conference September 29, 2015
 Unless they prove otherwise. ~Every ED attending ever Joshua Pruitt, MD, FAAEM Medical Director, LifeGuard Air Ambulance Iowa PA Society Fall CME Conference September 29, 2015 AAA with rupture Mesenteric
Unless they prove otherwise. ~Every ED attending ever Joshua Pruitt, MD, FAAEM Medical Director, LifeGuard Air Ambulance Iowa PA Society Fall CME Conference September 29, 2015 AAA with rupture Mesenteric
Abdo Pain rules & regulations. Mark Hartnell 2010
 Abdo Pain rules & regulations Mark Hartnell 2010 Aims Simple rules which might help in patients with abdominal pain Talk about some myths and realities Discuss some practical how to s in day to day treatment
Abdo Pain rules & regulations Mark Hartnell 2010 Aims Simple rules which might help in patients with abdominal pain Talk about some myths and realities Discuss some practical how to s in day to day treatment
Christopher Lau Kings County Hospital SUNY Downstate Medical Center February 24, 2011
 Christopher Lau Kings County Hospital SUNY Downstate Medical Center February 24, 2011 37 year old male presented with 1 day history of abdominal pain Pain was diffuse but worst in the epigastric area No
Christopher Lau Kings County Hospital SUNY Downstate Medical Center February 24, 2011 37 year old male presented with 1 day history of abdominal pain Pain was diffuse but worst in the epigastric area No
Cholecystitis is defined as nonspecific inflammation of the gallbladder with or without cholelithiasis. Types: calculous and acalculous.
 Cholecystitis is defined as nonspecific inflammation of the gallbladder with or without cholelithiasis. Types: calculous and acalculous. Anatomy of the gallbladder The gallbladder, a pear-shaped reservoir
Cholecystitis is defined as nonspecific inflammation of the gallbladder with or without cholelithiasis. Types: calculous and acalculous. Anatomy of the gallbladder The gallbladder, a pear-shaped reservoir
Perforation of a Duodenal Diverticulum. Elective Student S. C.
 Perforation of a Duodenal Diverticulum 2008 4 Elective Student S. C. Case History An elderly male presented to the Emergency Department with abdominal pain. Chief Complaint: Worsening, diffuse abdominal
Perforation of a Duodenal Diverticulum 2008 4 Elective Student S. C. Case History An elderly male presented to the Emergency Department with abdominal pain. Chief Complaint: Worsening, diffuse abdominal
ACUTE ABDOMEN IN OLDER CHILDREN. Carlos J. Sivit M.D.
 ACUTE ABDOMEN IN OLDER CHILDREN Carlos J. Sivit M.D. ACUTE ABDOMEN Clinical condition characterized by severe abdominal pain developing over several hours ACUTE ABDOMINAL PAIN Common childhood complaint
ACUTE ABDOMEN IN OLDER CHILDREN Carlos J. Sivit M.D. ACUTE ABDOMEN Clinical condition characterized by severe abdominal pain developing over several hours ACUTE ABDOMINAL PAIN Common childhood complaint
A patient with an unusual congenital anomaly of the pancreaticobiliary tree
 A patient with an unusual congenital anomaly of the pancreaticobiliary tree Thomas Hocker, HMS IV BIDMC Core Radiology Case Presentation September 17, 2007 Review of Normal Pancreaticobiliary Tract Anatomy
A patient with an unusual congenital anomaly of the pancreaticobiliary tree Thomas Hocker, HMS IV BIDMC Core Radiology Case Presentation September 17, 2007 Review of Normal Pancreaticobiliary Tract Anatomy
Biliary Tract Disease NIKI TADAYON GENERAL & VASCULAR SURGEON SHOHADA TAJRISH HOSPITAL
 Biliary Tract Disease NIKI TADAYON GENERAL & VASCULAR SURGEON SHOHADA TAJRISH HOSPITAL Differential Diagnosis of RUQ pain Gallstone disease (and its related complications) Gastritis/duodenitis Peptic ulcer
Biliary Tract Disease NIKI TADAYON GENERAL & VASCULAR SURGEON SHOHADA TAJRISH HOSPITAL Differential Diagnosis of RUQ pain Gallstone disease (and its related complications) Gastritis/duodenitis Peptic ulcer
General Data. 王 X 村 78 y/o 男性
 General Data 王 X 村 78 y/o 男性 Chief Complaint Vomiting twice this early morning Fever up to 38.9ºC was noted Present Illness (1) Old CVA with left side weakness for more than 10 years and with bed ridden
General Data 王 X 村 78 y/o 男性 Chief Complaint Vomiting twice this early morning Fever up to 38.9ºC was noted Present Illness (1) Old CVA with left side weakness for more than 10 years and with bed ridden
Background. RUQ Ultrasound Normal, Recommend Clinical Correlation. Sohail R. Shah, MD, MSHA, FACS, FAAP Texas Children s Hosptial
 RUQ Ultrasound Normal, Recommend Clinical Correlation Sohail R. Shah, MD, MSHA, FACS, FAAP Texas Children s Hosptial Background Incidence of pediatric gallbladder disease continues to rise U.S. Pediatric
RUQ Ultrasound Normal, Recommend Clinical Correlation Sohail R. Shah, MD, MSHA, FACS, FAAP Texas Children s Hosptial Background Incidence of pediatric gallbladder disease continues to rise U.S. Pediatric
SASKATCHEWAN REGISTERED NURSES ASSOCIATION. RNs WITH ADDITIONAL AUTHORIZED PRACTICE CLINICAL DECISION TOOL AUGUST 2017
 DEFINITION Cholelithiasis Presence of gall stones in the biliary tract. Biliary Colic Right upper quadrant pain due to obstruction of a bile duct by a gallstone. Cholecystitis Inflammation of the gallbladder
DEFINITION Cholelithiasis Presence of gall stones in the biliary tract. Biliary Colic Right upper quadrant pain due to obstruction of a bile duct by a gallstone. Cholecystitis Inflammation of the gallbladder
From Inflammation to Ischemia May apply to all luminal structures Obstruction Small or large bowel Appendix Gall bladder Ureter Hydrostatic Pressure:
 The Acute Abdomen Surgical Issues for the Family Practitioner Rochelle A. Dicker, MD Assistant Professor of Surgery and Anesthesia UC San Francisco Visceral Pain Vague Deep Associated with nausea/vomiting
The Acute Abdomen Surgical Issues for the Family Practitioner Rochelle A. Dicker, MD Assistant Professor of Surgery and Anesthesia UC San Francisco Visceral Pain Vague Deep Associated with nausea/vomiting
Documentation Dissection
 History of Present Illness: Documentation Dissection The patient is a 50-year-old male c/o symptoms for past 4 months 1, severe 2 bloating and stomach cramps, some nausea, vomiting, diarrhea. In last 3
History of Present Illness: Documentation Dissection The patient is a 50-year-old male c/o symptoms for past 4 months 1, severe 2 bloating and stomach cramps, some nausea, vomiting, diarrhea. In last 3
Abdominal Examination Benchmarks
 Abdominal Examination Benchmarks Preparation and Positioning: Stand on the right side of the patient. The patient should be supine and double draped so only the abdomen is exposed o To relax the abdominal
Abdominal Examination Benchmarks Preparation and Positioning: Stand on the right side of the patient. The patient should be supine and double draped so only the abdomen is exposed o To relax the abdominal
Biliary Tree Ultrasound - In a nutshell. Pamela Parker Lead Sonographer
 Biliary Tree Ultrasound - In a nutshell Pamela Parker Lead Sonographer Aims Review what we know about the biliary system Common pathologies Pitfalls Reporting tips The Nutshell Background Biliary examinations
Biliary Tree Ultrasound - In a nutshell Pamela Parker Lead Sonographer Aims Review what we know about the biliary system Common pathologies Pitfalls Reporting tips The Nutshell Background Biliary examinations
Types of peritonitis and management. J olita Augus te, PGY-5 SUNY Downs tate Grand Rounds 11/3/2016
 Types of peritonitis and management J olita Augus te, PGY-5 SUNY Downs tate Grand Rounds 11/3/2016 Case Presentation xx year old patient presents to ED with complaints of one day of abdominal pain s ince
Types of peritonitis and management J olita Augus te, PGY-5 SUNY Downs tate Grand Rounds 11/3/2016 Case Presentation xx year old patient presents to ED with complaints of one day of abdominal pain s ince
Imaging Criteria (CT findings) Inflammatory changes localized to appendix +/- appendiceal dilation +/- contrast non-filling
 Inflammatory changes localized to appendix +/- appendiceal dilation +/- contrast non-filling") Table 1. Data Dictionaries for Grading System for EGS Conditions A. Acute Appendicitis I Description Acutely inflamed appendix, intact Gangrenous appendix, intact Perforated appendix with local contamination
Table 1. Data Dictionaries for Grading System for EGS Conditions A. Acute Appendicitis I Description Acutely inflamed appendix, intact Gangrenous appendix, intact Perforated appendix with local contamination
Introduction to Evidence Based Medicine:
 Introduction to Evidence Based Medicine: General Abdominal Examination o Inspection Cullen s sign and Grey Turner s sign are indications of intraperitoneal or retroperitoneal hemorrhage. Traditionally,
Introduction to Evidence Based Medicine: General Abdominal Examination o Inspection Cullen s sign and Grey Turner s sign are indications of intraperitoneal or retroperitoneal hemorrhage. Traditionally,
Non Operative Management of Perforated Duodenal Ulcers. Rabih Nemr M.D. Kings County Hospital Sept 2006
 Non Operative Management of Perforated Duodenal Ulcers Rabih Nemr M.D. Kings County Hospital Sept 2006 Case presentation 40 year old male presenting with abdominal pain: Epigastric Worsening over the last
Non Operative Management of Perforated Duodenal Ulcers Rabih Nemr M.D. Kings County Hospital Sept 2006 Case presentation 40 year old male presenting with abdominal pain: Epigastric Worsening over the last
Case 1. Intro to Gallbladder & Pancreas Pathology. Case 1 DIAGNOSIS??? Acute Cholecystitis. Acute Cholecystitis. Helen Remotti M.D.
 Cholecystitis acute chronic Gallbladder tumors Adenomyoma (benign) Adenocarcinoma Pancreatitis acute chronic Pancreatic tumors Intro to Gallbladder & Pancreas Pathology Helen Remotti M.D. Case 1 70 year
Cholecystitis acute chronic Gallbladder tumors Adenomyoma (benign) Adenocarcinoma Pancreatitis acute chronic Pancreatic tumors Intro to Gallbladder & Pancreas Pathology Helen Remotti M.D. Case 1 70 year
GENI Program: GI and Abdominal Chief Complaints. Kim Macfarlane Clinical Nurse Specialist, Critical Care February 2008
 GENI Program: GI and Abdominal Chief Complaints Kim Macfarlane Clinical Nurse Specialist, Critical Care February 2008 Dehydration Common acute and chronic problem Recognition is critically important to
GENI Program: GI and Abdominal Chief Complaints Kim Macfarlane Clinical Nurse Specialist, Critical Care February 2008 Dehydration Common acute and chronic problem Recognition is critically important to
UNDERSTANDING X-RAYS: ABDOMINAL IMAGING THE ABDOMEN
 UNDERSTANDING X-RAYS: ABDOMINAL IMAGING THE ABDOMEN Radiology Enterprises radiologyenterprises@gmail.com www.radiologyenterprises.com STOMACH AND SMALL BOWEL STOMACH AND SMALL BOWEL Swallowed air is a
UNDERSTANDING X-RAYS: ABDOMINAL IMAGING THE ABDOMEN Radiology Enterprises radiologyenterprises@gmail.com www.radiologyenterprises.com STOMACH AND SMALL BOWEL STOMACH AND SMALL BOWEL Swallowed air is a
LOKUN! I got stomach ache!
 LOKUN! I got stomach ache! Mr L is a 67year old Chinese gentleman who is a non smoker, social drinker. He has a medical history significant for Hypertension, Hyperlipidemia, Type 2 Diabetes Mellitus, Chronic
LOKUN! I got stomach ache! Mr L is a 67year old Chinese gentleman who is a non smoker, social drinker. He has a medical history significant for Hypertension, Hyperlipidemia, Type 2 Diabetes Mellitus, Chronic
Cholelithiasis & cholecystitis
 1 Cholelithiasis & cholecystitis Dr. Muhammad Shamim FCPS (Pak), FACS (USA), FICS (USA) Assistant Professor, Dept. of Surgery College of Medicine, Prince Sattam bin Abdulaziz University Email: surgeon.shamim@gmail.com
1 Cholelithiasis & cholecystitis Dr. Muhammad Shamim FCPS (Pak), FACS (USA), FICS (USA) Assistant Professor, Dept. of Surgery College of Medicine, Prince Sattam bin Abdulaziz University Email: surgeon.shamim@gmail.com
THE APPROACH TO THE PATIENT WITH ACUTE ABDOMINAL PAIN
 THE APPROACH TO THE PATIENT WITH ACUTE ABDOMINAL PAIN Nick D Ardenne Sheba Medical Center, Internal Medicine Department St. George s University of London MANAGEMENT IN THE ED ABCs of Resuscitation AIRWAY:
THE APPROACH TO THE PATIENT WITH ACUTE ABDOMINAL PAIN Nick D Ardenne Sheba Medical Center, Internal Medicine Department St. George s University of London MANAGEMENT IN THE ED ABCs of Resuscitation AIRWAY:
GASTRO-INTESTINAL TRACT INFECTIONS - ANTIMICROBIAL MANAGEMENT
 GASTRO-INTESTINAL TRACT INFECTIONS - ANTIMICROBIAL MANAGEMENT Name & Title Of Author: Dr Linda Jewes, Consultant Microbiologist Date Amended: December 2016 Approved by Committee/Group: Drugs & Therapeutics
GASTRO-INTESTINAL TRACT INFECTIONS - ANTIMICROBIAL MANAGEMENT Name & Title Of Author: Dr Linda Jewes, Consultant Microbiologist Date Amended: December 2016 Approved by Committee/Group: Drugs & Therapeutics
Chapter 32 Gastroenterology General Pathophysiology General Risk Factors for GI emergencies: Excessive Consumption Excessive Smoking Increased
 1 2 3 4 5 6 7 Chapter 32 Gastroenterology General Pathophysiology General Risk Factors for GI emergencies: Excessive Consumption Excessive Smoking Increased Ingestion of Caustic Substances Poor Bowel Habits
1 2 3 4 5 6 7 Chapter 32 Gastroenterology General Pathophysiology General Risk Factors for GI emergencies: Excessive Consumption Excessive Smoking Increased Ingestion of Caustic Substances Poor Bowel Habits
MANAGEMENT OF PYOGENIC LIVER ABSCESS BOYOUNG SONG, M.D. SUNY DOWNSTATE SURGERY 11/7/13
 MANAGEMENT OF PYOGENIC LIVER ABSCESS BOYOUNG SONG, M.D. SUNY DOWNSTATE SURGERY 11/7/13 CASE THE PATIENT IS A 79 YEAR OLD MALE WITH 3 DAY HISTORY OF LOWER ABDOMINAL PAIN, NAUSEA WITHOUT VOMITING, CHILLS
MANAGEMENT OF PYOGENIC LIVER ABSCESS BOYOUNG SONG, M.D. SUNY DOWNSTATE SURGERY 11/7/13 CASE THE PATIENT IS A 79 YEAR OLD MALE WITH 3 DAY HISTORY OF LOWER ABDOMINAL PAIN, NAUSEA WITHOUT VOMITING, CHILLS
Locally Advanced Colon Cancer. Feiran Lou MD. MS. Richmond University Medical Center Department of Surgery
 Locally Advanced Colon Cancer Feiran Lou MD. MS. Richmond University Medical Center Department of Surgery Case 34 yo man presented with severe RLQ abdominal pain X 24 hrs. No nausea/vomiting/fever. + flatus.
Locally Advanced Colon Cancer Feiran Lou MD. MS. Richmond University Medical Center Department of Surgery Case 34 yo man presented with severe RLQ abdominal pain X 24 hrs. No nausea/vomiting/fever. + flatus.
Nordic Forum - Trauma & Emergency Radiology. Bowel Obstruction: Imaging Update
 Nordic Forum - Trauma & Emergency Radiology Bowel Obstruction: Imaging Update Borut Marincek Institute of Diagnostic Radiology University Hospital Zurich, Switzerland Acute Abdomen Bowel Obstruction Bowel
Nordic Forum - Trauma & Emergency Radiology Bowel Obstruction: Imaging Update Borut Marincek Institute of Diagnostic Radiology University Hospital Zurich, Switzerland Acute Abdomen Bowel Obstruction Bowel
Chapter 14: Training in Radiology. DDSEP Chapter 1: Question 12
 DDSEP Chapter 1: Question 12 A 52-year-old white male presents for evaluation of sudden onset of abdominal pain and shoulder pain. His past medical history is notable for a history of coronary artery disease,
DDSEP Chapter 1: Question 12 A 52-year-old white male presents for evaluation of sudden onset of abdominal pain and shoulder pain. His past medical history is notable for a history of coronary artery disease,
Emergency Surgery Course Graz, March ACUTE PANCREATITIS. Carlos Mesquita Coimbra
 ACUTE PANCREATITIS Carlos Mesquita Coimbra ESSENTIALS (1) AP occurs when digestive enzymes become activated while still in the pancreas, causing inflammation repeated bouts of AP can lead to chronic pancreatitis
ACUTE PANCREATITIS Carlos Mesquita Coimbra ESSENTIALS (1) AP occurs when digestive enzymes become activated while still in the pancreas, causing inflammation repeated bouts of AP can lead to chronic pancreatitis
Evidence Process for Abdominal Pain Guideline Research 11/16/2017. Guideline Review using ADAPTE method and AGREE II instrument 11/16/2017
 Evidence Process for Abdominal Pain Guideline Research Guideline Review using ADAPTE method and AGREE II instrument Approximately 139 Potentially relevant guidelines identified in various resources* 59
Evidence Process for Abdominal Pain Guideline Research Guideline Review using ADAPTE method and AGREE II instrument Approximately 139 Potentially relevant guidelines identified in various resources* 59
The EM Educator Series
 The EM Educator Series The EM Educator Series: Why is my patient with gallbladder pathology so sick? Author: Alex Koyfman, MD (@EMHighAK) // Edited by: Brit Long, MD (@long_brit) and Manpreet Singh, MD
The EM Educator Series The EM Educator Series: Why is my patient with gallbladder pathology so sick? Author: Alex Koyfman, MD (@EMHighAK) // Edited by: Brit Long, MD (@long_brit) and Manpreet Singh, MD
DISCLAIMER. No Conflict of Interest
 DISCLAIMER No Conflict of Interest EXCLAIMER No Interest in Conflict GALLSTONES FAQs and FACTS John Dunn, FRACS Laparoscopy Auckland YOU GOTTA KNOW THIS STUFF HOW DO THEY FORM? Gallbladder Lithogenic
DISCLAIMER No Conflict of Interest EXCLAIMER No Interest in Conflict GALLSTONES FAQs and FACTS John Dunn, FRACS Laparoscopy Auckland YOU GOTTA KNOW THIS STUFF HOW DO THEY FORM? Gallbladder Lithogenic
8/29/2016 DIVERTICULAR DISEASE: WHAT EVERY NURSE PRACTITIONER SHOULD KNOW. LENORE LAMANNA Ed.D, ANP-C LEARNING OBJECTIVES
 DIVERTICULAR DISEASE: WHAT EVERY NURSE PRACTITIONER SHOULD KNOW LENORE LAMANNA Ed.D, ANP-C LEARNING OBJECTIVES Define Diverticular Disease Discuss Epidemiology and Pathophysiology of Diverticular disease
DIVERTICULAR DISEASE: WHAT EVERY NURSE PRACTITIONER SHOULD KNOW LENORE LAMANNA Ed.D, ANP-C LEARNING OBJECTIVES Define Diverticular Disease Discuss Epidemiology and Pathophysiology of Diverticular disease
GASTROINTESTINAL IMAGING STUDY GUIDE
 GASTROINTESTINAL IMAGING STUDY GUIDE Pharynx Diverticula Foreign bodies Trauma o Motility Disorders Esophagus Diverticula Trauma Esophagitis Barrett esophagus Rings, webs, and strictures Varices Benign
GASTROINTESTINAL IMAGING STUDY GUIDE Pharynx Diverticula Foreign bodies Trauma o Motility Disorders Esophagus Diverticula Trauma Esophagitis Barrett esophagus Rings, webs, and strictures Varices Benign
By Junaid Asghar M Med, FAFP Consultant Adult Emergency Medicine. King Faisal Specialist Hospital & Research Centre- Riyadh- KSA
 By Junaid Asghar M Med, FAFP Consultant Adult Emergency Medicine King Faisal Specialist Hospital & Research Centre- Riyadh- KSA Case No 1 A VIP patient brings his 21 years son in EM with the complaints
By Junaid Asghar M Med, FAFP Consultant Adult Emergency Medicine King Faisal Specialist Hospital & Research Centre- Riyadh- KSA Case No 1 A VIP patient brings his 21 years son in EM with the complaints
Biliary Tract Disease. Emmet Andrews Cork University Hospital 6 th September 2010
 Biliary Tract Disease Emmet Andrews Cork University Hospital 6 th September 2010 Overview Gallstones Biliary tract tumours Other conditions Acute acalculous cholecystitis Mirizzi s syndrome Primary Biliary
Biliary Tract Disease Emmet Andrews Cork University Hospital 6 th September 2010 Overview Gallstones Biliary tract tumours Other conditions Acute acalculous cholecystitis Mirizzi s syndrome Primary Biliary
Chapter 24 - Abdominal_Emergencies
 Introduction to Emergency Medical Care 1 OBJECTIVES 24.1 Define key terms introduced in this chapter. 13, 15, 18, 20 22 24.2 Describe the location, structure, and function of the organs in the abdominal
Introduction to Emergency Medical Care 1 OBJECTIVES 24.1 Define key terms introduced in this chapter. 13, 15, 18, 20 22 24.2 Describe the location, structure, and function of the organs in the abdominal
Gallstone ileus:diagnostic and therapeutic dilemma
 Saurabh et al. 1 CASE SERIES OPEN ACCESS Gallstone ileus:diagnostic and therapeutic dilemma Shireesh Saurabh, Andrew Camerota, Jeffrey Zavotsky ABSTRACT Introduction: Gallstone ileus is a rare complication
Saurabh et al. 1 CASE SERIES OPEN ACCESS Gallstone ileus:diagnostic and therapeutic dilemma Shireesh Saurabh, Andrew Camerota, Jeffrey Zavotsky ABSTRACT Introduction: Gallstone ileus is a rare complication
Hepatobiliary Ultrasound Rimon Bengiamin, MD, RDMS Assistant Clinical Professor Director of Emergency Ultrasound UCSF Fresno. Objectives. Why?
 Hepatobiliary Ultrasound Rimon Bengiamin, MD, RDMS Assistant Clinical Professor Director of Emergency Ultrasound UCSF Fresno Objectives Discuss the goals of point-of-care biliary ultrasound Review the
Hepatobiliary Ultrasound Rimon Bengiamin, MD, RDMS Assistant Clinical Professor Director of Emergency Ultrasound UCSF Fresno Objectives Discuss the goals of point-of-care biliary ultrasound Review the
Information for Consent Cholecystectomy (Laparoscopic/Open) 膽囊切除術 ( 腹腔鏡 / 開放性 )
 膽囊切除術 ( 腹腔鏡 / 開放性 )") Version 1.0 Page 1 of 3 Information for Consent Cholecystectomy (Laparoscopic/Open) 膽囊切除術 ( 腹腔鏡 / 開放性 ) Introduction Gallbladder is a sac connected to the biliary tree. It serves the function of concentration
Version 1.0 Page 1 of 3 Information for Consent Cholecystectomy (Laparoscopic/Open) 膽囊切除術 ( 腹腔鏡 / 開放性 ) Introduction Gallbladder is a sac connected to the biliary tree. It serves the function of concentration
GI Emergencies and the On-Call Call
 GI Emergencies and the On-Call Call Julie Yang, MD, FASGE Director of Therapeutic Endoscopy Assistant Professor of Medicine Montefiore Medical Center Albert Einstein College of Medicine Objectives Scenarios
GI Emergencies and the On-Call Call Julie Yang, MD, FASGE Director of Therapeutic Endoscopy Assistant Professor of Medicine Montefiore Medical Center Albert Einstein College of Medicine Objectives Scenarios
Vesalius SCALpel : Biliary (see also: biliary/pancreatic folios) Physiology
 Physiology") Vesalius SCALpel : Biliary (see also: biliary/pancreatic folios) Physiology 95% of bile acids reabsorbed; colic and chenodeoxycolic primary bile acids cholecystokinin (CCK) major stimulus of gallbladder
Vesalius SCALpel : Biliary (see also: biliary/pancreatic folios) Physiology 95% of bile acids reabsorbed; colic and chenodeoxycolic primary bile acids cholecystokinin (CCK) major stimulus of gallbladder
You are called to see another patient. Melissa Wong, MD Richmond University Medical Center 30 April 2015
 You are called to see another patient Melissa Wong, MD Richmond University Medical Center 30 April 2015 Case Presentation 51F, progressive abdominal pain x 1d +flatus, +BM Last colonoscopy 2013 (hyperplastic
You are called to see another patient Melissa Wong, MD Richmond University Medical Center 30 April 2015 Case Presentation 51F, progressive abdominal pain x 1d +flatus, +BM Last colonoscopy 2013 (hyperplastic
Correspondence should be addressed to Justin Cochrane;
 Case Reports in Gastrointestinal Medicine Volume 2015, Article ID 794282, 4 pages http://dx.doi.org/10.1155/2015/794282 Case Report Acute on Chronic Pancreatitis Causing a Highway to the Colon with Subsequent
Case Reports in Gastrointestinal Medicine Volume 2015, Article ID 794282, 4 pages http://dx.doi.org/10.1155/2015/794282 Case Report Acute on Chronic Pancreatitis Causing a Highway to the Colon with Subsequent
Lahey Clinic Internal Medicine Residency Program: Curriculum for Gastroenterology
 Lahey Clinic Internal Medicine Residency Program: Curriculum for Gastroenterology Faculty representative: David L. Burns, MD, CNSP Resident representative: Tom Castiglione, MD Revision date: March 6, 2006
Lahey Clinic Internal Medicine Residency Program: Curriculum for Gastroenterology Faculty representative: David L. Burns, MD, CNSP Resident representative: Tom Castiglione, MD Revision date: March 6, 2006
LOOKING FOR AIR IN ALL THE WRONG PLACES Richard M. Gore, MD North Shore University Health System University of Chicago Evanston, IL
 SIGNIFICANCE OF EXTRALUMINAL ABDOMINAL GAS: LOOKING FOR AIR IN ALL THE WRONG PLACES Richard M. Gore, MD North Shore University Health System University of Chicago Evanston, IL SCBT/MR 2012 October 26,
SIGNIFICANCE OF EXTRALUMINAL ABDOMINAL GAS: LOOKING FOR AIR IN ALL THE WRONG PLACES Richard M. Gore, MD North Shore University Health System University of Chicago Evanston, IL SCBT/MR 2012 October 26,
CLINICAL VIGNETTE 2016; 2:1
 CLINICAL VIGNETTE 2016; 2:1 Editor-in-Chief: Olufemi E. Idowu. Neurological surgery Division, Department of Surgery, LASUCOM/LASUTH, Ikeja, Lagos, Nigeria. MANAGEMENT OF APPENDICITIS Ibrahim NA, Njokanma
CLINICAL VIGNETTE 2016; 2:1 Editor-in-Chief: Olufemi E. Idowu. Neurological surgery Division, Department of Surgery, LASUCOM/LASUTH, Ikeja, Lagos, Nigeria. MANAGEMENT OF APPENDICITIS Ibrahim NA, Njokanma
Abdominal Imaging - 9 Topics in 90 min
 Abdominal Imaging 9 topics in 90 min Antonio C. Westphalen, MD PhD Departments of Radiology and Biomedical Imaging, and Urology Liver Biliary tree Gallbladder Pancreas Kidneys Small bowel Colon Abscess?
Abdominal Imaging 9 topics in 90 min Antonio C. Westphalen, MD PhD Departments of Radiology and Biomedical Imaging, and Urology Liver Biliary tree Gallbladder Pancreas Kidneys Small bowel Colon Abscess?
Appendicitis USG vs CT
 Appendicitis USG vs CT Dr Sateesh Kumar Kailasam MBBS Dip EM (RCGP, UK) MRCEM (UK) Group Head Maxcure Group of Hospitals National Treasurer Society for Emergency Medicine India (SEMI) My Talk includes
Appendicitis USG vs CT Dr Sateesh Kumar Kailasam MBBS Dip EM (RCGP, UK) MRCEM (UK) Group Head Maxcure Group of Hospitals National Treasurer Society for Emergency Medicine India (SEMI) My Talk includes
GI -A & P Review PUD. Peptic Ulcer Disease (PUD) Objectives: Identify different types Gastric Ulcer Duodenal Ulcer Stress Ulcer
 Objectives: Identify different types Gastric Ulcer Duodenal Ulcer Stress Ulcer") GI -A & P Review Lemone and Burke Chapters 21-26 Mouth Pharynx Esophagus Stomach Small Intestines Large Intestines Liver and Gallbladder Pancreas Peptic Ulcer Disease (PUD) Objectives: Identify different
GI -A & P Review Lemone and Burke Chapters 21-26 Mouth Pharynx Esophagus Stomach Small Intestines Large Intestines Liver and Gallbladder Pancreas Peptic Ulcer Disease (PUD) Objectives: Identify different
Adv Pathophysiology Unit 9: GI Page 1 of 10
 Adv Pathophysiology Unit 9: GI Page 1 of 10 Learning objectives for this file: 1. Recognize positive physical and lab findings that point to the diagnosis 2. Appreciate the appearance of the affected organ
Adv Pathophysiology Unit 9: GI Page 1 of 10 Learning objectives for this file: 1. Recognize positive physical and lab findings that point to the diagnosis 2. Appreciate the appearance of the affected organ
Common Pediatric Surgical Emergencies
 Common Pediatric Surgical Emergencies John Doski, Tate Nice San Antonio Pediatric Surgery Associates Division of Pediatric Surgery Departments of Surgery and Pediatrics Disclosure John Doski, MD has no
Common Pediatric Surgical Emergencies John Doski, Tate Nice San Antonio Pediatric Surgery Associates Division of Pediatric Surgery Departments of Surgery and Pediatrics Disclosure John Doski, MD has no
Abdominal & scrotal pain
 Abdominal & scrotal pain Junior Teach Emergency Department 1 Created by SR Bruijns 03/11/2010 Objectives Understanding of, and emergency management of Acute abdominal pain Undifferentiated abdominal pain
Abdominal & scrotal pain Junior Teach Emergency Department 1 Created by SR Bruijns 03/11/2010 Objectives Understanding of, and emergency management of Acute abdominal pain Undifferentiated abdominal pain
ADULT RETROGRADE INTUSSUSCEPTION Brian Tiu Richmond University Medical Center September 3, 2015
 ADULT RETROGRADE INTUSSUSCEPTION Brian Tiu Richmond University Medical Center September 3, 2015 CASE PRESENTATION 41 yo woman presented one day hx abdominal pain, worsening nausea/vomiting denied flatus/bm
ADULT RETROGRADE INTUSSUSCEPTION Brian Tiu Richmond University Medical Center September 3, 2015 CASE PRESENTATION 41 yo woman presented one day hx abdominal pain, worsening nausea/vomiting denied flatus/bm
OPEN ACCESS TEXTBOOK OF GENERAL SURGERY
 OPEN ACCESS TEXTBOOK OF GENERAL SURGERY MESENTERIC ISCHAEMIA P Zwanepoel INTRODUCTION Mesenteric ischaemia results from hypoperfusion of the gut, most commonly due to occlusion, thrombosis or vasospasm.
OPEN ACCESS TEXTBOOK OF GENERAL SURGERY MESENTERIC ISCHAEMIA P Zwanepoel INTRODUCTION Mesenteric ischaemia results from hypoperfusion of the gut, most commonly due to occlusion, thrombosis or vasospasm.
Emergency Surgery Board Department of General Surgery Rambam Health Care Campus
 Emergency Surgery Board Department of General Surgery Rambam Health Care Campus Surgical Complications of Peptic Ulcer Disease Case Presentation and Review of the Literature Case Presentation 40y male
Emergency Surgery Board Department of General Surgery Rambam Health Care Campus Surgical Complications of Peptic Ulcer Disease Case Presentation and Review of the Literature Case Presentation 40y male
Evaluation of Acute Abdominal Pain
 Evaluation of Acute Abdominal Pain Michael Ziegler, MD Pediatric Emergency Medicine Associates, LLC Pediatric Sedation Services, LLC Scottish Rite WellStar Healthcare Systems Objectives Review a systematic
Evaluation of Acute Abdominal Pain Michael Ziegler, MD Pediatric Emergency Medicine Associates, LLC Pediatric Sedation Services, LLC Scottish Rite WellStar Healthcare Systems Objectives Review a systematic
Subtotal cholecystectomy for complicated acute cholecystitis: a multicenter prospective observational study
 Study title Subtotal cholecystectomy for complicated acute cholecystitis: a multicenter prospective observational study Primary Investigator: Kazuhide Matsushima, MD Co-Primary investigator: Zachary Warriner,
Study title Subtotal cholecystectomy for complicated acute cholecystitis: a multicenter prospective observational study Primary Investigator: Kazuhide Matsushima, MD Co-Primary investigator: Zachary Warriner,
Acute Pancreatitis:
 American College of Gastroenterology 2014 Acute Pancreatitis Scott Tenner, MD, MPH, FACG Clinical Professor of Medicine State University of New York Health Sciences Center Director, Brooklyn Gastroenterology
American College of Gastroenterology 2014 Acute Pancreatitis Scott Tenner, MD, MPH, FACG Clinical Professor of Medicine State University of New York Health Sciences Center Director, Brooklyn Gastroenterology
GASTROENTEROLOGY ESSENTIALS
 GASTROENTEROLOGY ESSENTIALS Practical Gastroenterology 8/25/2018 Jahnavi Koppala, MBBS Abdullah Abdussalam, MD A 48-year-old male was evaluated for noncardiac chest pain. Treatment with PPI twice daily
GASTROENTEROLOGY ESSENTIALS Practical Gastroenterology 8/25/2018 Jahnavi Koppala, MBBS Abdullah Abdussalam, MD A 48-year-old male was evaluated for noncardiac chest pain. Treatment with PPI twice daily
Hepatobiliary Disease
 Hepatobiliary Disease 大林慈濟綜合醫院 魏昌國 一般外科 Cholelithiasis 膽道結石 Incidence (USA) 10% in adult 85% cholesterol stones 15% pigment stone Risk factors Cholesterol stones Age Female(2x, 25% versus 12% at age 60),
Hepatobiliary Disease 大林慈濟綜合醫院 魏昌國 一般外科 Cholelithiasis 膽道結石 Incidence (USA) 10% in adult 85% cholesterol stones 15% pigment stone Risk factors Cholesterol stones Age Female(2x, 25% versus 12% at age 60),
Disclosures. Extra-hepatic Biliary Disease and the Pancreas. Objectives. Pancreatitis 10/3/2018. No relevant financial disclosures to report
 Extra-hepatic Biliary Disease and the Pancreas Disclosures No relevant financial disclosures to report Jeffrey Coughenour MD FACS Clinical Associate Professor of Surgery and Emergency Medicine Division
Extra-hepatic Biliary Disease and the Pancreas Disclosures No relevant financial disclosures to report Jeffrey Coughenour MD FACS Clinical Associate Professor of Surgery and Emergency Medicine Division
X-ray Corner. Imaging of the Small Bowel. Pantongrag-Brown L. Case 1. A 63-year-old man presented with abdominal pain, nausea and vomiting.
 THAI J 42 Imaging of the Small Bowel GASTROENTEROL 2015 X-ray Corner Imaging of the Small Bowel Pantongrag-Brown L Small bowel is the longest tubular organ in the body, about 18-22 feet. It is anchored
THAI J 42 Imaging of the Small Bowel GASTROENTEROL 2015 X-ray Corner Imaging of the Small Bowel Pantongrag-Brown L Small bowel is the longest tubular organ in the body, about 18-22 feet. It is anchored
Case Study: #3: Gallbladder Carcinoma?
 Case Study: #3: Gallbladder Carcinoma? By: Megan Wyatt K. SON Wyatt 225 2B1 RDMS, RVT Patient: Male 85 YOA Caucasian Indication: Elevated Alkaline Phosphatase History Annual physical showed elevated alkaline
Case Study: #3: Gallbladder Carcinoma? By: Megan Wyatt K. SON Wyatt 225 2B1 RDMS, RVT Patient: Male 85 YOA Caucasian Indication: Elevated Alkaline Phosphatase History Annual physical showed elevated alkaline
Management of biliary injury after laparoscopic cholecystectomy N. Dayes Kings County Hospital Center & Long Island College Hospital 8/19/2010
 Management of biliary injury after laparoscopic cholecystectomy N. Dayes Kings County Hospital Center & Long Island College Hospital 8/19/2010 Case Presentation 30 y.o. woman with 2 weeks of RUQ abdominal
Management of biliary injury after laparoscopic cholecystectomy N. Dayes Kings County Hospital Center & Long Island College Hospital 8/19/2010 Case Presentation 30 y.o. woman with 2 weeks of RUQ abdominal
Postoperative Ultrasound Evaluation of Gastric Distension; A Pilot study
 Postoperative Ultrasound Evaluation of Gastric Distension; A Pilot study M Jaronczyk MD, W Boyan Jr. MD, M Goldfarb MD. FACS. MMC Dept of Surgery Nausea and vomiting are common complaints of postoperative
Postoperative Ultrasound Evaluation of Gastric Distension; A Pilot study M Jaronczyk MD, W Boyan Jr. MD, M Goldfarb MD. FACS. MMC Dept of Surgery Nausea and vomiting are common complaints of postoperative
Bowel obstruction and tumors
 Bowel obstruction and tumors Intestinal Obstruction Obstruction of the GI tract may occur at any level, but the small intestine is most often involved because of its relatively narrow lumen. Causes: Hernias
Bowel obstruction and tumors Intestinal Obstruction Obstruction of the GI tract may occur at any level, but the small intestine is most often involved because of its relatively narrow lumen. Causes: Hernias
US Applications. Case Based Wrap-Up 1. Case 1 E-FAST. Case presentations E-FAST Abdominal. Pearls for each indication
 Case Based Wrap-Up 1 Stephanie J. Doniger MD RDMS FAAP FACEP Associate Director, Pediatric Emergency Ultrasound Stanford University Medical Center US Applications Case presentations E-FAST Abdominal Aorta
Case Based Wrap-Up 1 Stephanie J. Doniger MD RDMS FAAP FACEP Associate Director, Pediatric Emergency Ultrasound Stanford University Medical Center US Applications Case presentations E-FAST Abdominal Aorta
GI -A & P Review Mouth Pharynx Esophagus Stomach Small Intestines Large Intestines Liver and Gallbladder Pancreas 8/11/2011
 Lemone and Burke Chapters 21,23-25 ATI M/S Unit 7 Objectives Review A&P Identify diagnostic exams Discuss etiology, pathophysiology, clinical manifestation, and collaborative management of: PUD Hernias
Lemone and Burke Chapters 21,23-25 ATI M/S Unit 7 Objectives Review A&P Identify diagnostic exams Discuss etiology, pathophysiology, clinical manifestation, and collaborative management of: PUD Hernias
REFERRAL GUIDELINES: GALLSTONES
 REFERRAL GUIDELINES: GALLSTONES Document Purpose To ensure patients with gallstones disease are managed appropriately in primary/ secondary care Oxford Radcliffe Hospital Surgical Department Surgical Registrar
REFERRAL GUIDELINES: GALLSTONES Document Purpose To ensure patients with gallstones disease are managed appropriately in primary/ secondary care Oxford Radcliffe Hospital Surgical Department Surgical Registrar
Safe Answers For The American Board of Surgery Certifying Exam & Recertifying Exam
 Safe Answers For The American Board of Surgery Certifying Exam & Recertifying Exam By Sarmad Aji, MD., FACS. A comprehensive review of the most commonly asked questions on the American Board of Surgery
Safe Answers For The American Board of Surgery Certifying Exam & Recertifying Exam By Sarmad Aji, MD., FACS. A comprehensive review of the most commonly asked questions on the American Board of Surgery