Resident Teaching Conference 10/16/09 Rondi Kauffmann Resident presenter William Nealon Faculty presenter
|
|
|
- Ophelia Harper
- 5 years ago
- Views:
Transcription


1 Resident Teaching Conference 10/16/09 Rondi Kauffmann Resident presenter William Nealon Faculty presenter
2 KC 59 year old male Referred to Surgery clinic for incidentally discovered 5cm x 3cm pancreatic cyst
3 HPI: Pancreatic cyst incidentally discovered Denies nausea, emesis or abdominal pain No weight loss, fever, chills No jaundice, normal bowel movements No history of pancreatitis ROS: negative
4 PMH Htn Pulmonary nodule Dyslipidemia Heart murmur Diverticulosis PSH Tonsillectomy vasectomy FH Lung cancer father Htn mother, sister, brother Meds Benicar Vitamin B Zocor Omeprazole Aspirin SH Married Retired Smoked 1.5 ppd X years, quit 1993 Heavy etoh drinker 15 years ago, but now only drinks 6 pack every other week
5 Physical Exam P: 76 BP: 176/92 RR: 18 bpm Temp: 98.1 General: A&O, no jaundice, no lymphadenopathy Abdomen: soft, nontender, no masses, normal rectal exam
6 Labs LDL 150 Cholesterol 208 Triglycerides 132 HDL 32 Total protein 7.5 Albumin 4.4 Total bilirubin 0.7 Alk phos 67 ALT 37 AST 35 Amylase 13 Lipase 19 Ca
7
8
9
10
11 EUS with biopsy Body with normal echotexture Pancreatic duct measures 1.1 mm in diameter Large, well circumscribed, anechoic lesion measuring 2.5 cm x 4.7 cm arising from body No septations Normal pancreatic duct without stricture or stone
12 FNA Pathology: mixed lymphoid population, granular debris, negative for malignancy CEA: Cyst fluid amylase <10
13 Treatment Central pancreatectomy, omental pedicle flap, serosal patch Final pathology: pancreatic lymphoepithelial cyst, negative for malignancy
14 RR 63 year old male Referred to Surgery clinic with abdominal fullness and pain
15 HPI: 3 months duration of symptoms Weight loss of 32 lbs. in 10 weeks No fever, chills, nausea, melena, steatorrhea, jaundice ROS negative except for HPI
16 PMH Type 2 diabetes Thyroid cyst Hypertriglyceridemia PSH Tonsillectomy/adenoidectomy Cystoscopy EGD/colonoscopy 2008 FH Type 2 diabetes father Meds Protonix Captopril Synthroid Crestor Tylenol Naproxen MVI Echinacea Garlic Lantus Humalog
17 Physical Exam P: 120 BP 154/95 RR 18 bpm temp 98.1 General: A&O, no jaundice, no wasting Abdomen: soft, mild tenderness, no masses
18 Labs Total protein 7.1 Albumin 4.3 Total bilirubin 1.8 Alk phos 120 ALT 20 AST 20 CEA Ca , 245
19
20

21
22 EUS with FNA and cyst aspiration Large loculated cystic lesion arising from neck of pancreas Contained septations 2.5 x 3.0 cm Difficulty passing the scope into duodenum
23 Cytopathology Cyst FNA: Degenerated cells with amorphous debris, not diagnostic of malignancy No mucin Cyst amylase 1209 Cyst CEA >50,000 Pancreas neck FNA: adenocarcinoma Duodenal bulb biopsy: involved by moderate to poorly differentiated adenocarcinoma
24 PET Intense uptake corresponding to masses in right colon and pancreas Three low density lesions within the liver Multiple mesenteric lymph nodes with moderate FDG uptake Mild to moderate uptake in left supraclavicular lymph nodes
25 A 40 year old man with no co morbidities presents with diffuse abdominal pain and distention and a 2 day history of nausea and vomiting. He is afebrile and hemodynamically normal, but is anuric and serum creatinine is 3.0 mg/dl. A CT scan confirms necrotizing pancreatitis with a large peripancreatic phlegmon. There is no evidence of cholelithiasis or cholecystitis. He has had no prior episodes of pancreatitis. The next step in management should be A. Total parenteral nutrition (TPN) B. Bowel rest, fluid resuscitation C. Surgical pancreatic debridement D. Fine needle aspiration of peripancreatic fluid E. Prophylactic antifungal agents
26 A 39 year old woman is admitted with gallstone pancreatitis and epigastric pain. Pertinent data include amylase, 2000 U/L; bilirubin, 1.2 mg/dl; and WBC count 15,000. After 2 days of medical management, her epigastric pain resolves. Her amylase is 340 U/L and her bilirubin and WBC count have normalized. Laparoscopic cholecystectomy should be attempted A. After ERCP and sphincterotomy B. Prior to discharge C. Once her amylase is normal D. 4 6 weeks later to allow for a cooling down period E. Only if the patient develops recurrent pancreatitis

27
28
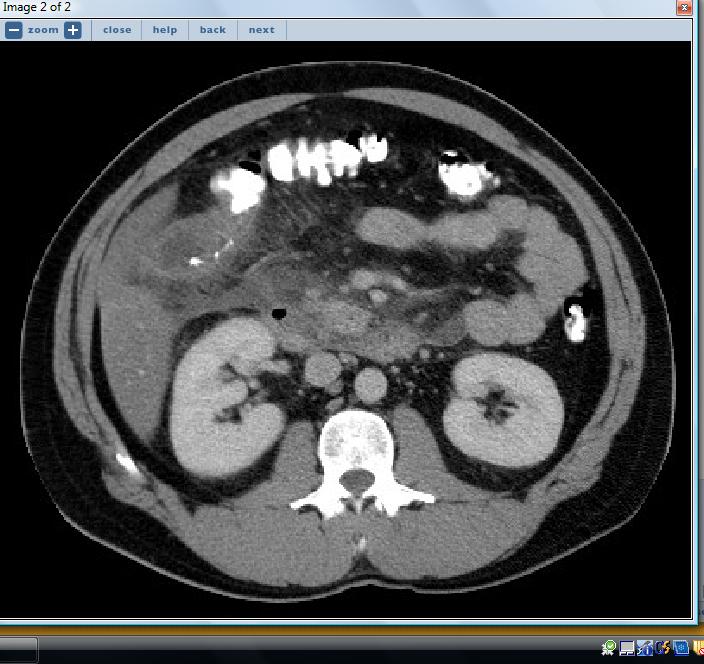
29 A 35 year old male is admitted with acute pancreatitis secondary to hypertriglyceridemia. Oral intake is discontinued, and he is hydrated with IV fluids. He has minimal upper abdominal tenderness. 72 hours after admission, he has worsening leukocytosis and elevated amylase with RUQ rebound tenderness. The CT scan shown is obtained. The most appropriate management would be A. Laparotomy B. Nasogastric tube decompression and broad spectrum antibiotics C. Somatostatin therapy D. Repeat CT scan in 48 to 72 hours E. Percutaneous drainage.

30
31 A 35 year old male has epigastric pain and emesis. Four week previously, he was discharged after an admission for uncomplicated acute pancreatitis. He has been receiving corticosteroids since a renal transplant 4 years ago. Pertinent data include: WBC 11,000; amylase 1000; and normal creatinine. The CT scan shown is obtained. The most appropriate management is A. Open debridement B. Cystgastrostomy C. Roux en Y cystjejunostomy D. Enteral feeding distal to the ligament of Treitz E. CT guided percutanous drainage
32 Pseudocysts Develop in 5 10% of patients with acute pancreatitis and 50% of patients with chronic pancreatitis Suspect if patient does not recover with one week of medical therapy, or when symptoms return after period of improvement
33 Pseudocysts Acute fluid collection Irregular in shape Frequently resolve Debridement reserved for necrotizing pancreatitis with infection or abscess Follow with serial CT Treatment: expectant management Pseudocyst Require 6 12 weeks to mature Caused by disruption of pancreatic duct Usually seen in setting of chronic pancreatitis May cause obstruction of gastric outlet or biliary tree
34 Complications of Pseudocysts Obstruction Infection Pain Hemosuccus pancreaticus
35 Treatment of Pseudocysts Open Laparoscopic Endoscopic

36
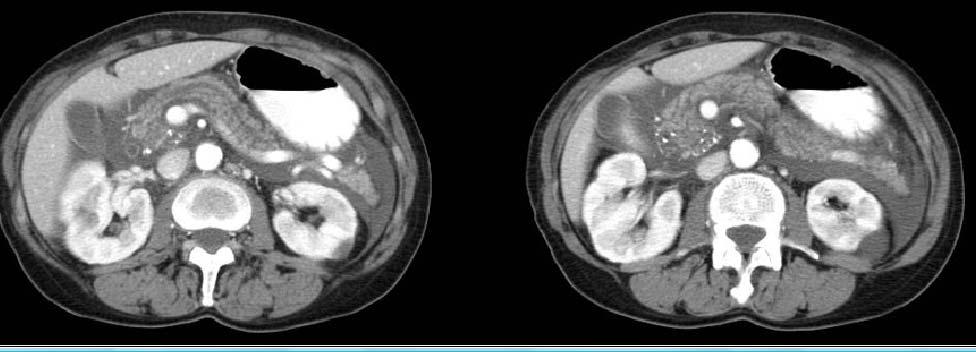
37 A 42 year old previously healthy man arrives in the Emergency Department with a 12 hour history of excruciating epigastric pain. He is afebrile and not jaundiced. Pulse is 115/min, blood pressure 90/60, and WBC count is 16,400. The CT scan show is obtained. Immediate management should include A. Peritoneal dialysis B. Exploratory laparotomy C. Needle aspiration D. Fluid resuscitation E. ERCP
38
39 Four weeks later, the patient returns to the Emergency Department with abdominal fullness. Vital signs are normal. The CT scan show is obtained. Treatment now should be A. ERCP B. Surgical decompression C. Percutaneous aspiration D. 14 day course of antibiotics E. Repeat CT scan in 30 days
40 Treatment of pseudocysts MUST send biopsy of cyst wall to exclude malignancy
Case Scenario 1. Discharge Summary
 Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
Disclosures. Extra-hepatic Biliary Disease and the Pancreas. Objectives. Pancreatitis 10/3/2018. No relevant financial disclosures to report
 Extra-hepatic Biliary Disease and the Pancreas Disclosures No relevant financial disclosures to report Jeffrey Coughenour MD FACS Clinical Associate Professor of Surgery and Emergency Medicine Division
Extra-hepatic Biliary Disease and the Pancreas Disclosures No relevant financial disclosures to report Jeffrey Coughenour MD FACS Clinical Associate Professor of Surgery and Emergency Medicine Division
PANCREATIC PSEUDOCYSTS. Madhuri Rao MD PGY-5 Kings County Hospital Center
 PANCREATIC PSEUDOCYSTS Madhuri Rao MD PGY-5 Kings County Hospital Center 34 yo M Case Presentation PMH: Chronic pancreatitis (ETOH related) PSH: Nil Meds: Nil NKDA www.downstatesurgery.org Symptoms o Chronic
PANCREATIC PSEUDOCYSTS Madhuri Rao MD PGY-5 Kings County Hospital Center 34 yo M Case Presentation PMH: Chronic pancreatitis (ETOH related) PSH: Nil Meds: Nil NKDA www.downstatesurgery.org Symptoms o Chronic
Management of Gallbladder Disease
 Management of Gallbladder Disease Steven B. Johnson, MD, FACS, FCCM Professor and Chairman, Department of Surgery Program Director, Phoenix Integrated Surgical Residency University of Arizona College of
Management of Gallbladder Disease Steven B. Johnson, MD, FACS, FCCM Professor and Chairman, Department of Surgery Program Director, Phoenix Integrated Surgical Residency University of Arizona College of
Morning Report. Allison Haden, MD October 1, 2002
 Morning Report Allison Haden, MD October 1, 2002 68 yo WM with N/V and abdominal pain Became ill about 2 weeks ago, per pt. intermittent nausea: worse w/eating vomiting within 30min of eating, nonbilious,
Morning Report Allison Haden, MD October 1, 2002 68 yo WM with N/V and abdominal pain Became ill about 2 weeks ago, per pt. intermittent nausea: worse w/eating vomiting within 30min of eating, nonbilious,
Case Discussion Splenic Abscess
 Case Discussion Splenic Abscess Personal Data Gender: male Birth Date: 1928/Mar/06th Allergy: Mefenamic Smoking: 0.5 PPD for 55 years Alcohol: negative (?) 4 Months Ago Abdominal pain: epigastric area
Case Discussion Splenic Abscess Personal Data Gender: male Birth Date: 1928/Mar/06th Allergy: Mefenamic Smoking: 0.5 PPD for 55 years Alcohol: negative (?) 4 Months Ago Abdominal pain: epigastric area
GASTROENTEROLOGY ESSENTIALS
 GASTROENTEROLOGY ESSENTIALS Practical Gastroenterology 8/25/2018 Jahnavi Koppala, MBBS Abdullah Abdussalam, MD A 48-year-old male was evaluated for noncardiac chest pain. Treatment with PPI twice daily
GASTROENTEROLOGY ESSENTIALS Practical Gastroenterology 8/25/2018 Jahnavi Koppala, MBBS Abdullah Abdussalam, MD A 48-year-old male was evaluated for noncardiac chest pain. Treatment with PPI twice daily
Lutheran Medical Center. Daniel H. Hunt, M.D. June 10 th, 2005
 Lutheran Medical Center Daniel H. Hunt, M.D. June 10 th, 2005 History xx y.o. pt with primary CBD stones s/p ERCP xx months earlier for attempted stone extraction resulting in post ERCP pancreatitis. Patient
Lutheran Medical Center Daniel H. Hunt, M.D. June 10 th, 2005 History xx y.o. pt with primary CBD stones s/p ERCP xx months earlier for attempted stone extraction resulting in post ERCP pancreatitis. Patient
ACG Clinical Guideline: Management of Acute Pancreatitis
 ACG Clinical Guideline: Management of Acute Pancreatitis Scott Tenner, MD, MPH, FACG 1, John Baillie, MB, ChB, FRCP, FACG 2, John DeWitt, MD, FACG 3 and Santhi Swaroop Vege, MD, FACG 4 1 State University
ACG Clinical Guideline: Management of Acute Pancreatitis Scott Tenner, MD, MPH, FACG 1, John Baillie, MB, ChB, FRCP, FACG 2, John DeWitt, MD, FACG 3 and Santhi Swaroop Vege, MD, FACG 4 1 State University
Background. RUQ Ultrasound Normal, Recommend Clinical Correlation. Sohail R. Shah, MD, MSHA, FACS, FAAP Texas Children s Hosptial
 RUQ Ultrasound Normal, Recommend Clinical Correlation Sohail R. Shah, MD, MSHA, FACS, FAAP Texas Children s Hosptial Background Incidence of pediatric gallbladder disease continues to rise U.S. Pediatric
RUQ Ultrasound Normal, Recommend Clinical Correlation Sohail R. Shah, MD, MSHA, FACS, FAAP Texas Children s Hosptial Background Incidence of pediatric gallbladder disease continues to rise U.S. Pediatric
Acute Pancreatitis:
 American College of Gastroenterology 2014 Acute Pancreatitis Scott Tenner, MD, MPH, FACG Clinical Professor of Medicine State University of New York Health Sciences Center Director, Brooklyn Gastroenterology
American College of Gastroenterology 2014 Acute Pancreatitis Scott Tenner, MD, MPH, FACG Clinical Professor of Medicine State University of New York Health Sciences Center Director, Brooklyn Gastroenterology
Case 1. Intro to Gallbladder & Pancreas Pathology. Case 1 DIAGNOSIS??? Acute Cholecystitis. Acute Cholecystitis. Helen Remotti M.D.
 Cholecystitis acute chronic Gallbladder tumors Adenomyoma (benign) Adenocarcinoma Pancreatitis acute chronic Pancreatic tumors Intro to Gallbladder & Pancreas Pathology Helen Remotti M.D. Case 1 70 year
Cholecystitis acute chronic Gallbladder tumors Adenomyoma (benign) Adenocarcinoma Pancreatitis acute chronic Pancreatic tumors Intro to Gallbladder & Pancreas Pathology Helen Remotti M.D. Case 1 70 year
Correspondence should be addressed to Justin Cochrane;
 Case Reports in Gastrointestinal Medicine Volume 2015, Article ID 794282, 4 pages http://dx.doi.org/10.1155/2015/794282 Case Report Acute on Chronic Pancreatitis Causing a Highway to the Colon with Subsequent
Case Reports in Gastrointestinal Medicine Volume 2015, Article ID 794282, 4 pages http://dx.doi.org/10.1155/2015/794282 Case Report Acute on Chronic Pancreatitis Causing a Highway to the Colon with Subsequent
Abdominal Pain. Luke Donnelly, MD Emergency Medicine
 Abdominal Pain Luke Donnelly, MD Emergency Medicine Objectives Approach to abdominal pain Evaluation Critical diagnoses and treatments Abdominal Pain Most Common ER Complaint Broad Differential Can often
Abdominal Pain Luke Donnelly, MD Emergency Medicine Objectives Approach to abdominal pain Evaluation Critical diagnoses and treatments Abdominal Pain Most Common ER Complaint Broad Differential Can often
Emergency Surgery Course Graz, March ACUTE PANCREATITIS. Carlos Mesquita Coimbra
 ACUTE PANCREATITIS Carlos Mesquita Coimbra ESSENTIALS (1) AP occurs when digestive enzymes become activated while still in the pancreas, causing inflammation repeated bouts of AP can lead to chronic pancreatitis
ACUTE PANCREATITIS Carlos Mesquita Coimbra ESSENTIALS (1) AP occurs when digestive enzymes become activated while still in the pancreas, causing inflammation repeated bouts of AP can lead to chronic pancreatitis
The role of endoscopy in the diagnosis and treatment of cystic pancreatic neoplasms
 The role of endoscopy in the diagnosis and treatment of cystic pancreatic neoplasms CYSTIC LESIONS AND FLUID COLLECTIONS OF THE PANCREAS Their pathology ranges from pseudocysts and pancreatic necrosis
The role of endoscopy in the diagnosis and treatment of cystic pancreatic neoplasms CYSTIC LESIONS AND FLUID COLLECTIONS OF THE PANCREAS Their pathology ranges from pseudocysts and pancreatic necrosis
Severe necrotizing pancreatitis. ICU Fellowship Training Radboudumc
 Severe necrotizing pancreatitis ICU Fellowship Training Radboudumc Acute pancreatitis Patients with acute pancreatitis van Dijk SM. Gut 2017;66:2024-2032 Diagnosis Revised Atlanta classification Abdominal
Severe necrotizing pancreatitis ICU Fellowship Training Radboudumc Acute pancreatitis Patients with acute pancreatitis van Dijk SM. Gut 2017;66:2024-2032 Diagnosis Revised Atlanta classification Abdominal
Management of biliary injury after laparoscopic cholecystectomy N. Dayes Kings County Hospital Center & Long Island College Hospital 8/19/2010
 Management of biliary injury after laparoscopic cholecystectomy N. Dayes Kings County Hospital Center & Long Island College Hospital 8/19/2010 Case Presentation 30 y.o. woman with 2 weeks of RUQ abdominal
Management of biliary injury after laparoscopic cholecystectomy N. Dayes Kings County Hospital Center & Long Island College Hospital 8/19/2010 Case Presentation 30 y.o. woman with 2 weeks of RUQ abdominal
Afternoon Session Cases
 Afternoon Session Cases Case 1 19 year old woman Presented with abdominal pain to community hospital Mild incr WBC a14, 000, Hg normal, lipase 100 (normal to 75) US 5.2 x 3.7 x 4 cm mass in porta hepatis
Afternoon Session Cases Case 1 19 year old woman Presented with abdominal pain to community hospital Mild incr WBC a14, 000, Hg normal, lipase 100 (normal to 75) US 5.2 x 3.7 x 4 cm mass in porta hepatis
Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds
 Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds Imaging in jaundice and 2ww pathway Image protocol Staging Limitations Pancreatic cancer 1.2.4 Refer people using a suspected
Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds Imaging in jaundice and 2ww pathway Image protocol Staging Limitations Pancreatic cancer 1.2.4 Refer people using a suspected
LOKUN! I got stomach ache!
 LOKUN! I got stomach ache! Mr L is a 67year old Chinese gentleman who is a non smoker, social drinker. He has a medical history significant for Hypertension, Hyperlipidemia, Type 2 Diabetes Mellitus, Chronic
LOKUN! I got stomach ache! Mr L is a 67year old Chinese gentleman who is a non smoker, social drinker. He has a medical history significant for Hypertension, Hyperlipidemia, Type 2 Diabetes Mellitus, Chronic
Acute Abdomen. Nirav Patel MD, FACS Banner University Medical Center - Phoenix
 Acute Abdomen Nirav Patel MD, FACS Banner University Medical Center - Phoenix ? Diffuse periumbilical with localization to RLQ + Nausea, anorexia, fevers - Diarrhea, emesis Exacerbated by movement, bumps
Acute Abdomen Nirav Patel MD, FACS Banner University Medical Center - Phoenix ? Diffuse periumbilical with localization to RLQ + Nausea, anorexia, fevers - Diarrhea, emesis Exacerbated by movement, bumps
Cystic Disease of the Liver Work Up and Management. Louis Ferrari MD, PGY 3 6/9/16 SUNY Downstate Medical Center
 Cystic Disease of the Liver Work Up and Management Louis Ferrari MD, PGY 3 6/9/16 SUNY Downstate Medical Center The Case 73F presents to clinic after diagnostic laparoscopy at OSH. Known liver mass for
Cystic Disease of the Liver Work Up and Management Louis Ferrari MD, PGY 3 6/9/16 SUNY Downstate Medical Center The Case 73F presents to clinic after diagnostic laparoscopy at OSH. Known liver mass for
Cystic liver lesion and eosinophilia
 November, 2005 Cystic liver lesion and eosinophilia Jakob Begun, Harvard medical School Year III Patient Presentation 55 year old Cape Verde female presented to her PCP with 6 month history of variable
November, 2005 Cystic liver lesion and eosinophilia Jakob Begun, Harvard medical School Year III Patient Presentation 55 year old Cape Verde female presented to her PCP with 6 month history of variable
PANCREATIC PSEUDOCYST DRAINAGE: ENDOSCOPIC APPROACHES & THE NURSING ROLE. PRESENTED BY: Susan DePasquale, CGRN, MSN
 PANCREATIC PSEUDOCYST DRAINAGE: ENDOSCOPIC APPROACHES & THE NURSING ROLE PRESENTED BY: Susan DePasquale, CGRN, MSN Pancreatic Fluid Collection (PFC) A result of pancreatic duct (PD) and side branch disruption,
PANCREATIC PSEUDOCYST DRAINAGE: ENDOSCOPIC APPROACHES & THE NURSING ROLE PRESENTED BY: Susan DePasquale, CGRN, MSN Pancreatic Fluid Collection (PFC) A result of pancreatic duct (PD) and side branch disruption,
Clinical Radiological Pathological Conference
 Clinical Radiological Pathological Conference CASE 1: A 59-year-old female Housekeeper Live in Phuket, Thailand Progressive dyspnea for 1 year Present illness 1 year PTA : She developed dyspnea on exertion
Clinical Radiological Pathological Conference CASE 1: A 59-year-old female Housekeeper Live in Phuket, Thailand Progressive dyspnea for 1 year Present illness 1 year PTA : She developed dyspnea on exertion
Documentation Dissection
 History of Present Illness: Documentation Dissection The patient is a 50-year-old male c/o symptoms for past 4 months 1, severe 2 bloating and stomach cramps, some nausea, vomiting, diarrhea. In last 3
History of Present Illness: Documentation Dissection The patient is a 50-year-old male c/o symptoms for past 4 months 1, severe 2 bloating and stomach cramps, some nausea, vomiting, diarrhea. In last 3
Perforation of a Duodenal Diverticulum. Elective Student S. C.
 Perforation of a Duodenal Diverticulum 2008 4 Elective Student S. C. Case History An elderly male presented to the Emergency Department with abdominal pain. Chief Complaint: Worsening, diffuse abdominal
Perforation of a Duodenal Diverticulum 2008 4 Elective Student S. C. Case History An elderly male presented to the Emergency Department with abdominal pain. Chief Complaint: Worsening, diffuse abdominal
General Surgery PURPLE SERVICE MUHC-RVH Site
 Preamble HPB is a clinical teaching unit with several different vocations: It regroups all solid organ Transplantation as well as most advanced Hepatobiliary and Pancreatic clinical activities performed
Preamble HPB is a clinical teaching unit with several different vocations: It regroups all solid organ Transplantation as well as most advanced Hepatobiliary and Pancreatic clinical activities performed
Vesalius SCALpel : Biliary (see also: biliary/pancreatic folios) Physiology
 Physiology") Vesalius SCALpel : Biliary (see also: biliary/pancreatic folios) Physiology 95% of bile acids reabsorbed; colic and chenodeoxycolic primary bile acids cholecystokinin (CCK) major stimulus of gallbladder
Vesalius SCALpel : Biliary (see also: biliary/pancreatic folios) Physiology 95% of bile acids reabsorbed; colic and chenodeoxycolic primary bile acids cholecystokinin (CCK) major stimulus of gallbladder
Pathophysiology ACUTE PANCREATITIS
 Pancreatitis Pathophysiology ACUTE PANCREATITIS BILIARY OBSTRUCTION Duct obstruction in the bile duct, pancreatic duct, or both. Increasing pressure Unregulated activation of digestive enzymes. Inflammation
Pancreatitis Pathophysiology ACUTE PANCREATITIS BILIARY OBSTRUCTION Duct obstruction in the bile duct, pancreatic duct, or both. Increasing pressure Unregulated activation of digestive enzymes. Inflammation
BILIARY TRACT & PANCREAS, PART II
 CME Pretest BILIARY TRACT & PANCREAS, PART II VOLUME 41 1 2015 A pretest is mandatory to earn CME credit on the posttest. The pretest should be completed BEFORE reading the overview. Both tests must be
CME Pretest BILIARY TRACT & PANCREAS, PART II VOLUME 41 1 2015 A pretest is mandatory to earn CME credit on the posttest. The pretest should be completed BEFORE reading the overview. Both tests must be
Discharge Summary-Page 1
 Discharge Summary-Page 1 Admission diagnosis: 1. Gastritis. 2. Alcoholic cirrhosis, ascites, grade 1 esophageal varices. 3. Recent left knee arthroplasty. 4. Osteoporosis naqmq : 1. Three chest X-rays
Discharge Summary-Page 1 Admission diagnosis: 1. Gastritis. 2. Alcoholic cirrhosis, ascites, grade 1 esophageal varices. 3. Recent left knee arthroplasty. 4. Osteoporosis naqmq : 1. Three chest X-rays
JOHN M UECKER, MD, FACS COMPLEX PANCREATICODUODENAL INJURIES
 JOHN M UECKER, MD, FACS COMPLEX PANCREATICODUODENAL INJURIES THE PROBLEM DUODENAL / PANCREATIC INJURIES Difficult to diagnose Not very common Anatomic and physiologic challenges 90% rate of associated
JOHN M UECKER, MD, FACS COMPLEX PANCREATICODUODENAL INJURIES THE PROBLEM DUODENAL / PANCREATIC INJURIES Difficult to diagnose Not very common Anatomic and physiologic challenges 90% rate of associated
CLINICAL MANIFESTATIONS AND DIAGNOSIS OF ACUTE PANCREATITIS. Raed Abu Sham a, M.D
 CLINICAL MANIFESTATIONS AND DIAGNOSIS OF ACUTE PANCREATITIS Raed Abu Sham a, M.D ACUTE PANCREATITIS Acute inflammatory process of the pancreas that resolves both clinically and histologically. It is usually
CLINICAL MANIFESTATIONS AND DIAGNOSIS OF ACUTE PANCREATITIS Raed Abu Sham a, M.D ACUTE PANCREATITIS Acute inflammatory process of the pancreas that resolves both clinically and histologically. It is usually
The Bile Duct (and Pancreas) and the Physician
 and the Physician") The Bile Duct (and Pancreas) and the Physician Javaid Iqbal Consultant in Gastroenterology and Pancreato-biliary Medicine University Hospital South Manchester Not so common?! Two weeks 38 ERCP s 20 15
The Bile Duct (and Pancreas) and the Physician Javaid Iqbal Consultant in Gastroenterology and Pancreato-biliary Medicine University Hospital South Manchester Not so common?! Two weeks 38 ERCP s 20 15
Pancreatic Benign April 27, 2016
 Department of Surgery Pancreatic Benign April 27, 2016 James Choi Dr. Hernandez Objectives Medical Expert: 1. Anatomy and congenital anomalies of the pancreas and pancreatic duct (divisum, annular pancreas
Department of Surgery Pancreatic Benign April 27, 2016 James Choi Dr. Hernandez Objectives Medical Expert: 1. Anatomy and congenital anomalies of the pancreas and pancreatic duct (divisum, annular pancreas
MAKING CONNECTIONS. Los Angeles Medical Center
 MAKING CONNECTIONS Los Angeles Medical Center Resident: Chris Molloy, MD Fellow: Christian Coroian, MD, MBA Attending: Tina Hardley, MD Program/Dept(s): Los Angeles Medical Center CHIEF COMPLAINT & HPI
MAKING CONNECTIONS Los Angeles Medical Center Resident: Chris Molloy, MD Fellow: Christian Coroian, MD, MBA Attending: Tina Hardley, MD Program/Dept(s): Los Angeles Medical Center CHIEF COMPLAINT & HPI
Evolving Gallstone Ileus. SUNY Downstate Case Conference January 12, 2012
 Evolving Gallstone Ileus SUNY Downstate Case Conference January 12, 2012 Initial Presentation HPI: 90 yo F c 1wk h/o abdominal pain and N/V. Denied F/C. Passing flatus/bm. PMH: DM, HTN, CAD. PSH: C-sections
Evolving Gallstone Ileus SUNY Downstate Case Conference January 12, 2012 Initial Presentation HPI: 90 yo F c 1wk h/o abdominal pain and N/V. Denied F/C. Passing flatus/bm. PMH: DM, HTN, CAD. PSH: C-sections
Chapter 45 3/2/2017. Care of the Patient with a Gallbladder, Liver, Biliary Tract, or Exocrine Pancreatic Disorder
 Chapter 45 Care of the Patient with a Gallbladder, Liver, Biliary Tract, or Exocrine Pancreatic Disorder All items and derived items 2015, 2011, 2006 by Mosby, Inc., an imprint of Elsevier Inc. All rights
Chapter 45 Care of the Patient with a Gallbladder, Liver, Biliary Tract, or Exocrine Pancreatic Disorder All items and derived items 2015, 2011, 2006 by Mosby, Inc., an imprint of Elsevier Inc. All rights
Siddharth Gosavi, Vydehi Institute of Medical Sciences & Research Centre, India Under the guidance of Gillian Lieberman, MD
 Under the guidance of Gillian Lieberman, MD March 2016 RADIOLOGICAL HALLMARKS OF NECROTIZING PANCREATITIS Siddharth Gosavi, Vydehi Institute of Medical Sciences & Research Centre, India Under the guidance
Under the guidance of Gillian Lieberman, MD March 2016 RADIOLOGICAL HALLMARKS OF NECROTIZING PANCREATITIS Siddharth Gosavi, Vydehi Institute of Medical Sciences & Research Centre, India Under the guidance
Together, putting patients first
 The Role of a Gastroenterologist in the Diagnosis and Management of Pancreatic Cancer Sarah Jowett, Consultant Gastroenterologist Bradford Teaching Hospitals Trust Leeds Regional Study Day, 12 September
The Role of a Gastroenterologist in the Diagnosis and Management of Pancreatic Cancer Sarah Jowett, Consultant Gastroenterologist Bradford Teaching Hospitals Trust Leeds Regional Study Day, 12 September
Slide 1. Slide 2. Slide 3 Pancreatic Cancer- Case #1. Endoscopic management of GI malignancy. Endoscopic approaches in GI malignancy- Agenda
 Slide 1 A teaching hospital of Harvard Medical School Endoscopic management of GI malignancy Tyler Berzin MD, MS Center for Advanced Endoscopy Division of Gastroenterology Beth Israel Deaconess Medical
Slide 1 A teaching hospital of Harvard Medical School Endoscopic management of GI malignancy Tyler Berzin MD, MS Center for Advanced Endoscopy Division of Gastroenterology Beth Israel Deaconess Medical
12 Blueprints Q&A Step 2 Surgery
 12 Blueprints Q&A Step 2 Surgery 34. A 40-year-old female has been referred to you for a recent ER and hospital admission, from which she was given a diagnosis of acute diverticulitis. Treatment at that
12 Blueprints Q&A Step 2 Surgery 34. A 40-year-old female has been referred to you for a recent ER and hospital admission, from which she was given a diagnosis of acute diverticulitis. Treatment at that
ERCP / PTC Surgical Laparoscopic vs open Timing and order of approach
 Choledocholithiasis Which Approach and When? Lygia Stewart, MD University of California, San Francisco 2010 Naffziger Post-Graduate Course Clinical Manifestations of Choledocholithiasis Asymptomatic (no
Choledocholithiasis Which Approach and When? Lygia Stewart, MD University of California, San Francisco 2010 Naffziger Post-Graduate Course Clinical Manifestations of Choledocholithiasis Asymptomatic (no
Pancreas Case Scenario #1
 Pancreas Case Scenario #1 An 85 year old white female presented to her primary care physician with increasing abdominal pain. On 8/19 she had a CT scan of the abdomen and pelvis. This showed a 4.6 cm mass
Pancreas Case Scenario #1 An 85 year old white female presented to her primary care physician with increasing abdominal pain. On 8/19 she had a CT scan of the abdomen and pelvis. This showed a 4.6 cm mass
53 year old Female with Hypoglycemia. Colleen Flynn, MD April 5, 2012
 53 year old Female with Hypoglycemia Colleen Flynn, MD April 5, 2012 HPI 53 yo F referred to the endocrine clinic for hypoglycemia x 1 year. History of a non secreting metastatic neuroendocrine tumor diagnosed
53 year old Female with Hypoglycemia Colleen Flynn, MD April 5, 2012 HPI 53 yo F referred to the endocrine clinic for hypoglycemia x 1 year. History of a non secreting metastatic neuroendocrine tumor diagnosed
GALLBLADDER CANCER. Lidie M. Lajoie MD Downstate Surgery M&M July 21, 2011
 GALLBLADDER CANCER Lidie M. Lajoie MD Downstate Surgery M&M July 21, 2011 Agenda Case Presentation Epidemiology Pathogenesis & Pathology Staging Presentation & Diagnosis Stage-wise Management Outcomes/Prognosis
GALLBLADDER CANCER Lidie M. Lajoie MD Downstate Surgery M&M July 21, 2011 Agenda Case Presentation Epidemiology Pathogenesis & Pathology Staging Presentation & Diagnosis Stage-wise Management Outcomes/Prognosis
Management of Gastroenterology Emergencies Tim Gardner, MD Director, Pancreatic Disorders Section of Gastroenterology and Hepatology
 Management of Gastroenterology Emergencies Tim Gardner, MD Director, Pancreatic Disorders Section of Gastroenterology and Hepatology DHMC CREST Symposium November 7, 2008 There are no financial disclosures
Management of Gastroenterology Emergencies Tim Gardner, MD Director, Pancreatic Disorders Section of Gastroenterology and Hepatology DHMC CREST Symposium November 7, 2008 There are no financial disclosures
D DAVID PUBLISHING. Groove Pancreatitis: A Case Report. 1. Introduction. 2. Case Report
 Journal of Pharmacy and Pharmacology 6 (2018) 415-419 doi: 10.17265/2328-2150/2018.04.013 D DAVID PUBLISHING Luciana Leony Valente, Mariama Alves Dantas Fagundes, Camila Medrado Pereira Barbosa, Hélio
Journal of Pharmacy and Pharmacology 6 (2018) 415-419 doi: 10.17265/2328-2150/2018.04.013 D DAVID PUBLISHING Luciana Leony Valente, Mariama Alves Dantas Fagundes, Camila Medrado Pereira Barbosa, Hélio
CASE-BASED SMALL GROUP DISCUSSION MHD II
 MHD II, Session 11, Student Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION MHD II Session 11 April 11, 2016 STUDENT COPY MHD II, Session 11, Student Copy Page 2 CASE HISTORY 1 Chief complaint: Our baby
MHD II, Session 11, Student Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION MHD II Session 11 April 11, 2016 STUDENT COPY MHD II, Session 11, Student Copy Page 2 CASE HISTORY 1 Chief complaint: Our baby
16 April 2010 Resident Teaching Conference. Pancreatitis. W. H. Nealon, M.D., F.A.C.S. J.J. Smith, M.D., D.W.D.
 16 April 2010 Resident Teaching Conference Pancreatitis W. H. Nealon, M.D., F.A.C.S. J.J. Smith, M.D., D.W.D. Santorini Wirsung anatomy.med.umich.edu/.../ duodenum_ans.html Bud and ductology Ventral pancreatic
16 April 2010 Resident Teaching Conference Pancreatitis W. H. Nealon, M.D., F.A.C.S. J.J. Smith, M.D., D.W.D. Santorini Wirsung anatomy.med.umich.edu/.../ duodenum_ans.html Bud and ductology Ventral pancreatic
What to do and not do before seeking surgical consultation for a patient with suspected pancreatic cancer
 What to do and not do before seeking surgical consultation for a patient with suspected pancreatic cancer 9 Th Annual Symposium on Gastrointestinal Cancers, St. Louis University School of Medicine Carlos
What to do and not do before seeking surgical consultation for a patient with suspected pancreatic cancer 9 Th Annual Symposium on Gastrointestinal Cancers, St. Louis University School of Medicine Carlos
Unusual Pancreatic Neoplasms RTC 2/11/2011
 Unusual Pancreatic Neoplasms RTC 2/11/2011 Objectives Intraductal Papillary Mucinous Neoplasm (IPMN) Mucinous Cystic Neoplasm (MCN) Islet Cell Tumors Insulinoma Glucagonoma VIPoma Somatostatinoma Gastrinoma
Unusual Pancreatic Neoplasms RTC 2/11/2011 Objectives Intraductal Papillary Mucinous Neoplasm (IPMN) Mucinous Cystic Neoplasm (MCN) Islet Cell Tumors Insulinoma Glucagonoma VIPoma Somatostatinoma Gastrinoma
Case 1- B.N. 66 yr old F with PMHx of breast cancer s/ p mastectomy, HTN, DM presented with dysphagia to solids and liquids.
 Case 1- B.N 66 yr old F with PMHx of breast cancer s/ p mastectomy, HTN, DM presented with dysphagia to solids and liquids. Reports retching to clear esophagus. Case 1- B.N EGD: Stricture in the distal
Case 1- B.N 66 yr old F with PMHx of breast cancer s/ p mastectomy, HTN, DM presented with dysphagia to solids and liquids. Reports retching to clear esophagus. Case 1- B.N EGD: Stricture in the distal
Cholecystitis is defined as nonspecific inflammation of the gallbladder with or without cholelithiasis. Types: calculous and acalculous.
 Cholecystitis is defined as nonspecific inflammation of the gallbladder with or without cholelithiasis. Types: calculous and acalculous. Anatomy of the gallbladder The gallbladder, a pear-shaped reservoir
Cholecystitis is defined as nonspecific inflammation of the gallbladder with or without cholelithiasis. Types: calculous and acalculous. Anatomy of the gallbladder The gallbladder, a pear-shaped reservoir
Appendix 5. EFSUMB Newsletter. Gastroenterological Ultrasound
 EFSUMB Newsletter 87 Examinations should encompass the full range of pathological conditions listed below A log book listing the types of examinations undertaken should be kept Training should usually
EFSUMB Newsletter 87 Examinations should encompass the full range of pathological conditions listed below A log book listing the types of examinations undertaken should be kept Training should usually
Jaundice. Agnieszka Dobrowolska- Zachwieja, MD, PhD
 Jaundice Agnieszka Dobrowolska- Zachwieja, MD, PhD Jaundice definition Jaundice, as in the French jaune, refers to the yellow discoloration of the skin. It arises from the abnormal accumulation of bilirubin
Jaundice Agnieszka Dobrowolska- Zachwieja, MD, PhD Jaundice definition Jaundice, as in the French jaune, refers to the yellow discoloration of the skin. It arises from the abnormal accumulation of bilirubin
How 5 Diseases Became One. Moez Tajdin R3 McGill University
 How 5 Diseases Became One Moez Tajdin R3 McGill University Conflicts of Interest None! Mr. M. ID: 65 M PMH Benign prostatic hyperplasia Prostate cancer Awaiting biopsy Skin rash Dyslipidemia Hypertension
How 5 Diseases Became One Moez Tajdin R3 McGill University Conflicts of Interest None! Mr. M. ID: 65 M PMH Benign prostatic hyperplasia Prostate cancer Awaiting biopsy Skin rash Dyslipidemia Hypertension
Frank Burton Memorial Update on Pancreato-biliary Cancers
 Frank Burton Memorial Update on Pancreato-biliary Cancers Diagnosis and management of pancreatic cancer: common dilemmas Moderators: Banke Agarwal, MD Paul Buse, MD Evaluation of patients with obstructive
Frank Burton Memorial Update on Pancreato-biliary Cancers Diagnosis and management of pancreatic cancer: common dilemmas Moderators: Banke Agarwal, MD Paul Buse, MD Evaluation of patients with obstructive
Chronic pancreatitis mimicking intraductal papillary mucinous neoplasm of the pancreas; Report of tow cases
 Jichi Medical University Journal Chronic pancreatitis mimicking intraductal papillary mucinous neoplasm of the pancreas; Report of tow cases Noritoshi Mizuta, Hiroshi Noda, Nao Kakizawa, Nobuyuki Toyama,
Jichi Medical University Journal Chronic pancreatitis mimicking intraductal papillary mucinous neoplasm of the pancreas; Report of tow cases Noritoshi Mizuta, Hiroshi Noda, Nao Kakizawa, Nobuyuki Toyama,
PANCREATIC CANCER GUIDELINES
 PANCREATIC CANCER GUIDELINES North-East London Cancer Network & Barts and the London HPB Centre PROTOCOL FOR MANAGEMENT OF PANCREATIC CANCER (SEPTEMBER 2010) I. PRE-REFERRAL GUIDELINES Screening 1. Offer
PANCREATIC CANCER GUIDELINES North-East London Cancer Network & Barts and the London HPB Centre PROTOCOL FOR MANAGEMENT OF PANCREATIC CANCER (SEPTEMBER 2010) I. PRE-REFERRAL GUIDELINES Screening 1. Offer
Surgical Management of Chronic Pancreatitis VERENA LIU, MD KINGS COUNTY HOSPITAL CENTER SURGERY GRAND ROUNDS 4/1/2013
 Surgical Management of Chronic Pancreatitis VERENA LIU, MD KINGS COUNTY HOSPITAL CENTER SURGERY GRAND ROUNDS 4/1/2013 Case Report 42F with h/o chronic pancreatitis due to alcohol use with chronic upper
Surgical Management of Chronic Pancreatitis VERENA LIU, MD KINGS COUNTY HOSPITAL CENTER SURGERY GRAND ROUNDS 4/1/2013 Case Report 42F with h/o chronic pancreatitis due to alcohol use with chronic upper
Case Report Spontaneous Intramural Duodenal Hematoma: Pancreatitis, Obstructive Jaundice, and Upper Intestinal Obstruction
 Case Reports in Surgery Volume 2016, Article ID 5321081, 4 pages http://dx.doi.org/10.1155/2016/5321081 Case Report Spontaneous Intramural Duodenal Hematoma: Pancreatitis, Obstructive Jaundice, and Upper
Case Reports in Surgery Volume 2016, Article ID 5321081, 4 pages http://dx.doi.org/10.1155/2016/5321081 Case Report Spontaneous Intramural Duodenal Hematoma: Pancreatitis, Obstructive Jaundice, and Upper
General Surgery Service
 General Surgery Service Patient Care Goals and Objectives Stomach/Duodenum and Bariatric assessed for a) Obesity surgery b) Treatment of i) Adenocarcinoma of the stomach ii) GIST iii) Carcinoid 2) Optimize
General Surgery Service Patient Care Goals and Objectives Stomach/Duodenum and Bariatric assessed for a) Obesity surgery b) Treatment of i) Adenocarcinoma of the stomach ii) GIST iii) Carcinoid 2) Optimize
Imaging Guided Biopsy. Edited & Presented by ; Hussien A.B ALI DINAR. Msc Lecturer,Reporting Sonographer
 Imaging Guided Biopsy Edited & Presented by ; Hussien A.B ALI DINAR. Msc Lecturer,Reporting Sonographer Objective By the End of this lessons you should : Define what biopsy Justify Aim to perform biopsy
Imaging Guided Biopsy Edited & Presented by ; Hussien A.B ALI DINAR. Msc Lecturer,Reporting Sonographer Objective By the End of this lessons you should : Define what biopsy Justify Aim to perform biopsy
Case Reports. Intraductal Papillary Cholangiocarcinoma: Case Report and Review of the Literature INTRODUCTION CASE REPORT
 Case Reports Kongkam K, Rerknimitr R 45 Case Report and Review of the Literature Pradermchai Kongkam, M.D. Rungsun Rerknimitr, M.D. ABSTRACT A case of papillary cholangiocarcinoma is presented. A 64-year-old
Case Reports Kongkam K, Rerknimitr R 45 Case Report and Review of the Literature Pradermchai Kongkam, M.D. Rungsun Rerknimitr, M.D. ABSTRACT A case of papillary cholangiocarcinoma is presented. A 64-year-old
Tata Memorial Centre s opinion is summarized as follows: 1. Given the type 1 stricture (as mentioned in the structured summary), assessment
, assessment") March 5 th 2016 Dear Ms. Malti Sinha, Thank you for reaching out to Tata Memorial Centre for an expert opinion in regard to assessing your treatment options. Navya Network is pleased to offer this online
March 5 th 2016 Dear Ms. Malti Sinha, Thank you for reaching out to Tata Memorial Centre for an expert opinion in regard to assessing your treatment options. Navya Network is pleased to offer this online
Cases from the Clinic Maryland ACP Meeting January 30, 2016
 Cases from the Clinic Maryland ACP Meeting January 30, 2016 Bimal Ashar, MD, FACP D. William Schlott, MD Associate Professor of Medicine Johns Hopkins University School of Medicine 1 CASE 1: GK 46-year-old
Cases from the Clinic Maryland ACP Meeting January 30, 2016 Bimal Ashar, MD, FACP D. William Schlott, MD Associate Professor of Medicine Johns Hopkins University School of Medicine 1 CASE 1: GK 46-year-old
Biliary tree dilation - and now what?
 Biliary tree dilation - and now what? Poster No.: C-1767 Congress: ECR 2012 Type: Educational Exhibit Authors: I. Ferreira, A. B. Ramos, S. Magalhães, M. Certo; Porto/PT Keywords: Pathology, Diagnostic
Biliary tree dilation - and now what? Poster No.: C-1767 Congress: ECR 2012 Type: Educational Exhibit Authors: I. Ferreira, A. B. Ramos, S. Magalhães, M. Certo; Porto/PT Keywords: Pathology, Diagnostic
amount (per occasion): If yes: frequency: N/A / occasionally/monthly/weekly/daily
: If yes: frequency: N/A / occasionally/monthly/weekly/daily") 1. Patient personal details Insurance number:.. Name:. Date of birth:... Gender: female / male Race: Asian-Indian / White / Black / N/A Admission date:.. Last day of treatment:. Date of interview: Institute:
1. Patient personal details Insurance number:.. Name:. Date of birth:... Gender: female / male Race: Asian-Indian / White / Black / N/A Admission date:.. Last day of treatment:. Date of interview: Institute:
Pain can produce unstable hemodynamics
 Pain can produce unstable hemodynamics 30-year-old male came to emergency department for severe epigastric pain for 6 hours as well as nausea and vomiting. 1)BP: 130/70mmHg 2)HR:
Pain can produce unstable hemodynamics 30-year-old male came to emergency department for severe epigastric pain for 6 hours as well as nausea and vomiting. 1)BP: 130/70mmHg 2)HR:
Management of Gallbladder Disease. Cory Buschmann, MD PGY-5 11/28/2017
 Management of Gallbladder Disease Cory Buschmann, MD PGY-5 11/28/2017 Financial disclosures None Content Scope of gallbladder diseases Evaluation H&P Labs Imaging Cholecystectomy vs cholecystostomy Ancillary
Management of Gallbladder Disease Cory Buschmann, MD PGY-5 11/28/2017 Financial disclosures None Content Scope of gallbladder diseases Evaluation H&P Labs Imaging Cholecystectomy vs cholecystostomy Ancillary
Chronic Pancreatitis. Ara Sahakian, M.D. Assistant Professor of Medicine USC core lecture
 Chronic Pancreatitis Ara Sahakian, M.D. Assistant Professor of Medicine USC core lecture What is Chronic Pancreatitis Progressive inflammatory disease Pancreatic parenchyma replaced w/fibrous tissue Destruction
Chronic Pancreatitis Ara Sahakian, M.D. Assistant Professor of Medicine USC core lecture What is Chronic Pancreatitis Progressive inflammatory disease Pancreatic parenchyma replaced w/fibrous tissue Destruction
Management of Pancreatic Fistulae
 Management of Pancreatic Fistulae Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre Fistula definition A Fistula is a permanent abnormal passageway between two organs (epithelial
Management of Pancreatic Fistulae Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre Fistula definition A Fistula is a permanent abnormal passageway between two organs (epithelial
Adv Pathophysiology Unit 9: GI Page 1 of 10
 Adv Pathophysiology Unit 9: GI Page 1 of 10 Learning objectives for this file: 1. Recognize positive physical and lab findings that point to the diagnosis 2. Appreciate the appearance of the affected organ
Adv Pathophysiology Unit 9: GI Page 1 of 10 Learning objectives for this file: 1. Recognize positive physical and lab findings that point to the diagnosis 2. Appreciate the appearance of the affected organ
The Pancreas. Basic Anatomy. Endocrine pancreas. Exocrine pancreas. Pancreas vasculature. Islets of Langerhans. Acinar cells Ductal System
 SGNA: Back to Basics Rogelio G. Silva, MD Assistant Clinical Professor of Medicine University of Illinois at Chicago Department of Medicine Division of Gastroenterology Advocate Christ Medical Center GI
SGNA: Back to Basics Rogelio G. Silva, MD Assistant Clinical Professor of Medicine University of Illinois at Chicago Department of Medicine Division of Gastroenterology Advocate Christ Medical Center GI
Disclosures. Overview. Case 1. Common Bile Duct Sizes 10/14/2016. General GI + Advanced Endoscopy: NAFLD/Stones/Pancreatitis
 Disclosures General GI + Advanced Endoscopy: NAFLD/Stones/Pancreatitis 123 Blank Blank, LLC Aldo Maspons, MD Assistant Professor Director of Endoscopy Department of Pediatrics Texas Tech University Health
Disclosures General GI + Advanced Endoscopy: NAFLD/Stones/Pancreatitis 123 Blank Blank, LLC Aldo Maspons, MD Assistant Professor Director of Endoscopy Department of Pediatrics Texas Tech University Health
Case Presentation: Mr. S
 Case Presentation: Mr. S History Seen as inpatient in May, but has significant prior history and is a poor historian 53 y.o. Male no PMH, has been out of contact with medicine for years aside from hernia
Case Presentation: Mr. S History Seen as inpatient in May, but has significant prior history and is a poor historian 53 y.o. Male no PMH, has been out of contact with medicine for years aside from hernia
concerned about his health and does not want to end up on medication, like his siblings
 Volume: 802 Questions Question: 1 A 45-year-old male comes to your office for his first annual checkup in the last 10 years. On first impression, he appears overweight but is otherwise healthy and has
Volume: 802 Questions Question: 1 A 45-year-old male comes to your office for his first annual checkup in the last 10 years. On first impression, he appears overweight but is otherwise healthy and has
Post-Operative Chylous Ascites. David Kashan, PGY-4 Richmond University Medical Center 7/30/15
 Post-Operative Chylous Ascites David Kashan, PGY-4 Richmond University Medical Center 7/30/15 HPI Patient is a 76 year old female p/w one day of worsening abdominal pain, +N/V, fevers and chills HPI PMHx:
Post-Operative Chylous Ascites David Kashan, PGY-4 Richmond University Medical Center 7/30/15 HPI Patient is a 76 year old female p/w one day of worsening abdominal pain, +N/V, fevers and chills HPI PMHx:
GASTRO-INTESTINAL TRACT INFECTIONS - ANTIMICROBIAL MANAGEMENT
 GASTRO-INTESTINAL TRACT INFECTIONS - ANTIMICROBIAL MANAGEMENT Name & Title Of Author: Dr Linda Jewes, Consultant Microbiologist Date Amended: December 2016 Approved by Committee/Group: Drugs & Therapeutics
GASTRO-INTESTINAL TRACT INFECTIONS - ANTIMICROBIAL MANAGEMENT Name & Title Of Author: Dr Linda Jewes, Consultant Microbiologist Date Amended: December 2016 Approved by Committee/Group: Drugs & Therapeutics
Case Presentation. PMH: HTN, BPH, strabismus PSH: appendectomy Medications: norvasc, tamsulosin NKDA SH/FH: negative
 Case Presentation 68yM referred for incidental finding of pancreatic head mass on CT scan for elevated PSA. No symptoms. Denied pruritus, jaundice, change in color of urine/stool, anorexia, or weight loss.
Case Presentation 68yM referred for incidental finding of pancreatic head mass on CT scan for elevated PSA. No symptoms. Denied pruritus, jaundice, change in color of urine/stool, anorexia, or weight loss.
Advanced Pathophysiology Unit 7: Renal-Urologic Page 1 of 6
 Advanced Pathophysiology Unit 7: Renal-Urologic Page 1 of 6 Learning Objectives for this File: 1. Understand how clinical presentation drives the diagnostic workup 2. Recognize how patient education is
Advanced Pathophysiology Unit 7: Renal-Urologic Page 1 of 6 Learning Objectives for this File: 1. Understand how clinical presentation drives the diagnostic workup 2. Recognize how patient education is
Comprehensive Study of Acute Pancreatitis (Diagnosis, Disease Course, and Clinical Management): A Retrospective and Prospective Study
: A Retrospective and Prospective Study") Original Article Print ISSN: 2321-6379 Online ISSN: 2321-595X DOI: 10.17354/ijss/2017/449 Comprehensive Study of Acute Pancreatitis (Diagnosis, Disease Course, and Clinical Management): A Retrospective
Original Article Print ISSN: 2321-6379 Online ISSN: 2321-595X DOI: 10.17354/ijss/2017/449 Comprehensive Study of Acute Pancreatitis (Diagnosis, Disease Course, and Clinical Management): A Retrospective
General'Surgery'Service'
 General'Surgery'Service' Patient Care Goals and Objectives 1)! Stomach/Duodenum and Bariatric 2)! Interpret the results of clinical evaluations (history, physical examination) performed on patients being
General'Surgery'Service' Patient Care Goals and Objectives 1)! Stomach/Duodenum and Bariatric 2)! Interpret the results of clinical evaluations (history, physical examination) performed on patients being
VS: BP 165/90, P 98, RR 18, T 37 C; waist circ 38 in, Wt 240 lbs (109 kg), Ht 5'8''
, Ht 5'8''") IMC Didactic Case-Diabetes Mellitus Chief Complaint "I was recently diagnosed with diabetes and would like to have my blood sugar tested. I think that my blood sugar is running low because I have the shakes
IMC Didactic Case-Diabetes Mellitus Chief Complaint "I was recently diagnosed with diabetes and would like to have my blood sugar tested. I think that my blood sugar is running low because I have the shakes
Surgical Management of Acute Pancreatitis
 Surgical Management of Acute Pancreatitis Steven J. Hughes, MD, FACS Cracchiolo Family Professor of Surgery and Chief, General Surgery Overview Biliary pancreatitis a cost effective algorithm Key concepts
Surgical Management of Acute Pancreatitis Steven J. Hughes, MD, FACS Cracchiolo Family Professor of Surgery and Chief, General Surgery Overview Biliary pancreatitis a cost effective algorithm Key concepts
7/11/2017. We re gonna help a lot of people today. Biliary/Pancreatic Endoscopy. AGS July 1-2, Kenneth M. Sigman, MD
 Biliary/Pancreatic Endoscopy AGS July 1-2, 2017 Kenneth M. Sigman, MD We re gonna help a lot of people today 1 2 3 4 Cannulation It all starts with cannulation Double Wire Cannulation Difficult cannulations
Biliary/Pancreatic Endoscopy AGS July 1-2, 2017 Kenneth M. Sigman, MD We re gonna help a lot of people today 1 2 3 4 Cannulation It all starts with cannulation Double Wire Cannulation Difficult cannulations
Management of Acute Pancreatitis
 Management of Acute Pancreatitis A Clinical Practice Guideline developed by the University of Toronto s Best Practice in Surgery JA Greenberg, M Bawazeer, J Hsu, J Marshall, JO Friedrich, A Nathens, N
Management of Acute Pancreatitis A Clinical Practice Guideline developed by the University of Toronto s Best Practice in Surgery JA Greenberg, M Bawazeer, J Hsu, J Marshall, JO Friedrich, A Nathens, N
Cholangiocarcinoma: Radiologic evaluation and interventions
 November 2014 Cholangiocarcinoma: Radiologic evaluation and interventions Colin Nevins, Harvard Medical School Year III Agenda Initial course and work-up Endoscopic retrograde cholangiopancreatography
November 2014 Cholangiocarcinoma: Radiologic evaluation and interventions Colin Nevins, Harvard Medical School Year III Agenda Initial course and work-up Endoscopic retrograde cholangiopancreatography
Rokitansky-Aschoff sinuses are epithelial invaginations in the gallbladder wall that from as a result of increased gallbladder pressures.
 Anatomy The complexity of the biliary tree can be broken down into much simpler segments. The intrahepatic ducts converge to form the right and left hepatic ducts which exit the liver and join to become
Anatomy The complexity of the biliary tree can be broken down into much simpler segments. The intrahepatic ducts converge to form the right and left hepatic ducts which exit the liver and join to become
MANAGEMENT OF PYOGENIC LIVER ABSCESS BOYOUNG SONG, M.D. SUNY DOWNSTATE SURGERY 11/7/13
 MANAGEMENT OF PYOGENIC LIVER ABSCESS BOYOUNG SONG, M.D. SUNY DOWNSTATE SURGERY 11/7/13 CASE THE PATIENT IS A 79 YEAR OLD MALE WITH 3 DAY HISTORY OF LOWER ABDOMINAL PAIN, NAUSEA WITHOUT VOMITING, CHILLS
MANAGEMENT OF PYOGENIC LIVER ABSCESS BOYOUNG SONG, M.D. SUNY DOWNSTATE SURGERY 11/7/13 CASE THE PATIENT IS A 79 YEAR OLD MALE WITH 3 DAY HISTORY OF LOWER ABDOMINAL PAIN, NAUSEA WITHOUT VOMITING, CHILLS
Aliu Sanni MD SUNY Downstate Medical Center August 16, 2012
 Aliu Sanni MD SUNY Downstate Medical Center August 16, 2012 Case Presentation 60yr old AAF with PMH of CAD s/p PCI 1983, CVA, GERD, HTN presented with retrosternal chest pain on 06/12 Associated dysphagia
Aliu Sanni MD SUNY Downstate Medical Center August 16, 2012 Case Presentation 60yr old AAF with PMH of CAD s/p PCI 1983, CVA, GERD, HTN presented with retrosternal chest pain on 06/12 Associated dysphagia
JMSCR Vol 04 Issue 08 Page August 2016
 www.jmscr.igmpublication.org Impact Factor 5.244 Index Copernicus Value: 83.27 ISSN (e)-2347-176x ISSN (p) 2455-0450 DOI: http://dx.doi.org/10.18535/jmscr/v4i8.08 Acute Pancreatitis with Normal Amylase
www.jmscr.igmpublication.org Impact Factor 5.244 Index Copernicus Value: 83.27 ISSN (e)-2347-176x ISSN (p) 2455-0450 DOI: http://dx.doi.org/10.18535/jmscr/v4i8.08 Acute Pancreatitis with Normal Amylase
Pancreatitis. Acute Pancreatitis
 Pancreatitis Pancreatitis is an inflammation of the pancreas. The pancreas is a large gland behind the stomach and close to the duodenum. The duodenum is the upper part of the small intestine. The pancreas
Pancreatitis Pancreatitis is an inflammation of the pancreas. The pancreas is a large gland behind the stomach and close to the duodenum. The duodenum is the upper part of the small intestine. The pancreas
A CASE REPORT OF SPONTANEOUS BILOMA - AN ENIGMATIC SURGICAL PROBLEM
 A CASE REPORT OF SPONTANEOUS BILOMA - AN ENIGMATIC SURGICAL PROBLEM *Sumanta Kumar Ghosh and Biswajit Mukherjee ESIC Medical College, Joka, Kolkata, India *Author for Correspondence ABSTRACT Occurrence
A CASE REPORT OF SPONTANEOUS BILOMA - AN ENIGMATIC SURGICAL PROBLEM *Sumanta Kumar Ghosh and Biswajit Mukherjee ESIC Medical College, Joka, Kolkata, India *Author for Correspondence ABSTRACT Occurrence
Non Operative Management of Perforated Duodenal Ulcers. Rabih Nemr M.D. Kings County Hospital Sept 2006
 Non Operative Management of Perforated Duodenal Ulcers Rabih Nemr M.D. Kings County Hospital Sept 2006 Case presentation 40 year old male presenting with abdominal pain: Epigastric Worsening over the last
Non Operative Management of Perforated Duodenal Ulcers Rabih Nemr M.D. Kings County Hospital Sept 2006 Case presentation 40 year old male presenting with abdominal pain: Epigastric Worsening over the last
A 34 year old woman with Vomiting and abdominal pain
 A 34 year old woman with Vomiting and abdominal pain The patient was a 34 y/o woman admitted because of epigastric pain developed from 2 months ago. It was a crampy pain without radiation that became better
A 34 year old woman with Vomiting and abdominal pain The patient was a 34 y/o woman admitted because of epigastric pain developed from 2 months ago. It was a crampy pain without radiation that became better