A 34 year old woman with Vomiting and abdominal pain
|
|
|
- Brenda Stone
- 5 years ago
- Views:
Transcription


1 A 34 year old woman with Vomiting and abdominal pain

2 The patient was a 34 y/o woman admitted because of epigastric pain developed from 2 months ago. It was a crampy pain without radiation that became better with vomiting. She didn t have any history of hematemesis, melena, jaundice, weight loss, headache and fever. No history of constipation, diarrhea and obstipation.

3 BP=120/70 PR=80 RR=14 T=37.2
4 No history of: PUD Renal disorders Chronic liver disease DM HTN Recent surgery (cesarean section 7 years ago)
5 Drug history: Negative Familial history: Negative
6 Head and Neck: No paleness No icter No lymphadenopathy JVP=Nl Thyroid=Nl
7 Chest: Lung=Bilateral clear Heart=Nl Abdomen: Skin=Nl Obese No distention Slightly tenderness in epigastr No rebound tenderness No organomegally Bowel sound= Nl Extremities: Nl
8 2 months ago was admitted for the first time at ER because of the same complaint. Some work up such as lab tests and abdominopelvic sonography was performed that were normal and she was discharged.
9 1 month ago because of abdominal pain, vomiting and rise in Cr was admitted in nephrology ward for rule out of the cause of ARF.

10 CBC: WBC=5600 Hb=12 MCV=87 Plt=121000
11 Urea:104 Cr=2.1(reduced to 1.3) Na=138 K=4 AST=45 ALT=40 ALKP=140 ESR=12
12 U/A: Ph=5 Pro=1+ WBC=2-4 RBC=1-2 Bact=Negative
13 HBS Ag=Negative ANA=Negative Anti ds DNA=26 C3=1.2 C4=0.16
14 Abdominopelvic Sonography: Nl
15 1 weeks ago the patient was admitted in surgery ward because of the same complaint for rule out of pancreatitis.
16 Abdominopelvic CT with IV and Oral contrast: Liver, spleen, pancreas are normal Enlarged gall bladder Both kidneys have normal size and paranchymal thickness No evidence of hydronephrosis Upper GI Endoscopy: Nl
17 Some lab tests (Amylase,Lipase) was performed for her that were normal and then she was discharged.

18 Disorders of the gut and peritoneum Mechanical obstruction Functional gastrointestinal disorders IBS Dyspepsia Gastroparesis Organic gastrointestinal disorders (Cholecystitis, Pancreatitis, PUD, Hepatitis, Crohn's disease, Mesenteric ischemia, Inflammatory intraperitoneal disease )
19 Infectious causes Gastroenteritis( Viral, Bacterial ) Nongastrointestinal infections( Otitis media)
20 CNS causes Migraine Increased intracranial pressure (Malignancy, Hemorrhage, Infarction, Abscess, Meningitis, Pseudotumor cerebri ) Seizure disorders Psychiatric disease (Psychogenic vomiting, Anxiety disorders, Depression, Anorexia nervosa, Bulimia nervosa ) Labyrinthine disorders(motion sickness, Labyrinthitis, Tumors, Meniere's disease )
21 Medications Cancer chemotherapy Analgesics Cardiovascular medications (Digoxin, Antiarrhythmics, Antihypertensives, β-blockers, Calcium channel antagonists ) Diuretics Oral antidiabetics Oral contraceptives Antibiotics/antivirals Gastrointestinal medications (Sulfasalazine, Azathioprine ) Antiasthmatics (Theophylline )) CNS medication(anticonvulsants, Antiparkinsonian )
22 Endocrinologic and metabolic causes Pregnancy Uremia Diabetic ketoacidosis Hyperparathyroidism Hypoparathyroidism Hyperthyroidism Addison's disease Acute intermittent porphyria
23 Postoperative nausea and vomiting Cyclic vomiting syndrome Miscellaneous causes Myocardial infarction Heart failure Starvation
24 CBC: WBC=8500 Hb=13 MCV=80 Plt=235000
25 BS:86 Urea:62 Cr:1.4 Na:144 K:4.3 Ca:4 Ast:123 Alt:113 Alkp:190 Bili (T=1.1, D=0.8) INR:1
26 U/A: PH=5 Pro=Negative RBC=0-1 WBC=0-1 Bact=Negative VBG: PH=7.40 PCO2=35 HCO3=24
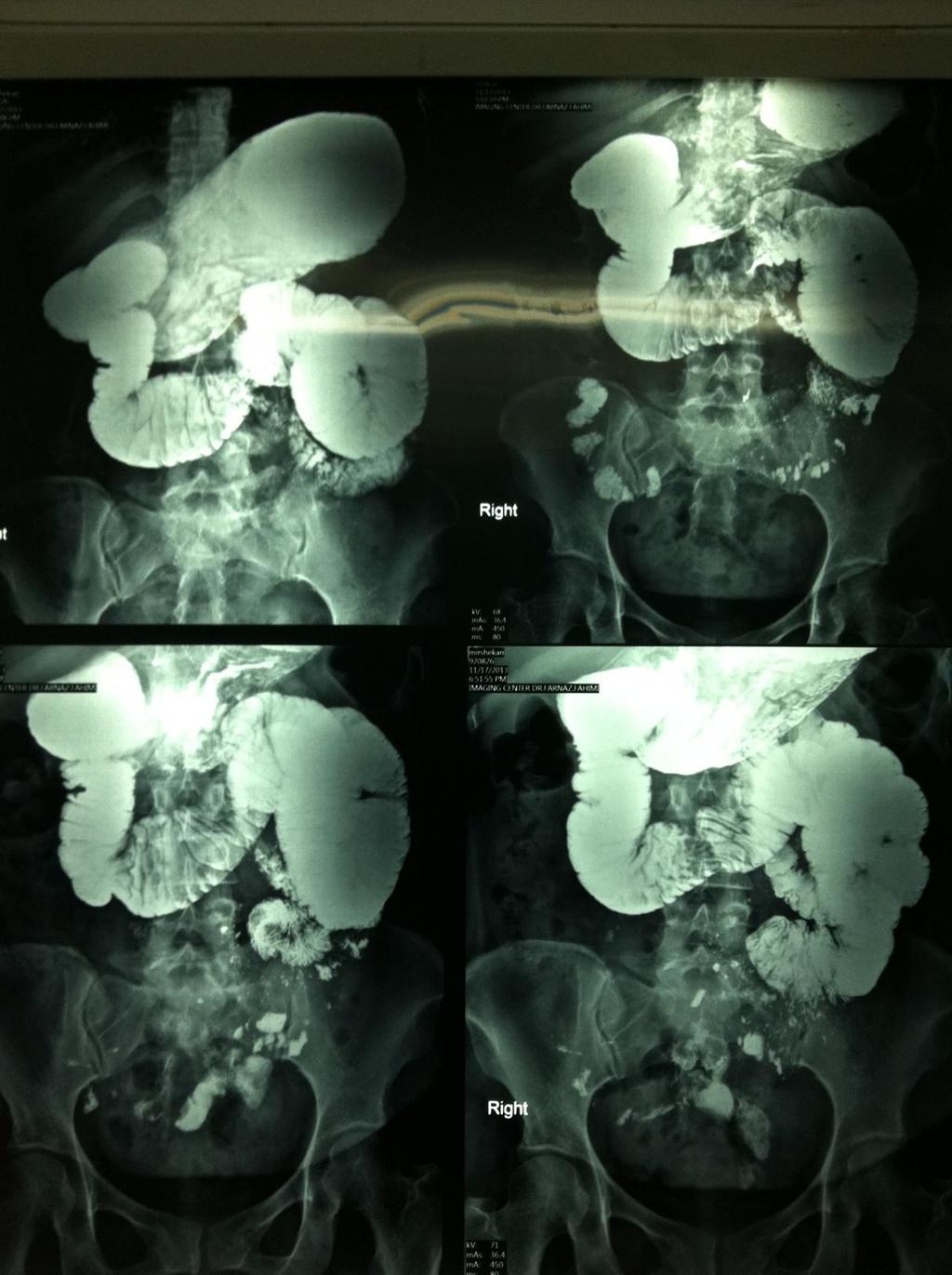
27 Abdominopelvic Sonography: Nl Bowel series: Dilation in stomach and duodenum and proximal of jejunum are evident in favor of obstruction Small passage of barium toward distal part of small bowel
28
29 Small bowel obstruction (SBO) occurs when the normal flow of intestinal contents is interrupted. The most frequent causes are postoperative adhesions and hernias, which cause extrinsic compression of the intestine. Less frequently, tumors or strictures of the small bowel can cause intrinsic blockage.

30 The most common symptoms of SBO are abdominal distention, vomiting, crampy abdominal pain, and inability to pass flatus. In proximal obstruction, nausea and vomiting can be relatively severe compared to distal obstruction, but distention of the abdomen is somewhat less since the proximal intestine acts as a reservoir as it dilates.
31 Adhesions Postoperative adhesions cause the majority of small bowel obstructions. Malignancy Malignant tumors are the second most common cause of SBO. Hernias the third leading cause of intestinal obstruction. Strictures Intraluminal stricture can be caused by a number of disorders including Crohn's disease, certain drugs such as entericcoated potassium chloride solutions and NSAIDs, radiation therapy, ischemia, and tumors.
32 Trauma Traumatic small bowel obstruction caused by intramural hematoma results in nausea, vomiting, and upper abdominal tenderness. Intussusception is rare in adults Gallstone ileus results from erosion and fistulization between the biliary and intestinal tracts. Bezoars Superior mesenteric artery syndrome The syndrome is characterized by compression of the third portion of the duodenum due to narrowing of the space between the superior mesenteric artery and aorta and is primarily attributed to loss of the intervening mesenteric fat pad.

33 The diagnosis of SBO can be made by history and physical examination in the majority of patients. While imaging is potentially helpful in establishing the diagnosis, in most cases a laparotomy will be needed to make a definitive diagnosis and for treatment if a patient does not respond to nonoperative management. Laboratory studies are generally not helpful in determining the presence of small bowel obstruction, but can help in the assessment of the degree of dehydration.

34 Plain abdominal radiography Multiple air-fluid levels with distended loops of small bowel. Small bowel series These studies are highly sensitive and are the gold standard for determining whether an obstruction is partial or complete. Computerized tomography More recently, CT has been replacing the small bowel series as the adjunctive study of choice since it can simultaneously provide information about the presence, level, severity, and cause of obstruction. Ultrasonography ultrasound may be appropriate for pregnant patients or as a bedside test for the critically ill.

35 INITIAL MANAGEMENT The primary goals in the initial management of patients with SBO are to determine: The degree of volume depletion and metabolic derangement. The severity, cause, extent and location of the obstruction. Whether nonoperative management can be considered The need for and timing of operative intervention
36 NONOPERATIVE MANAGEMENT can sometimes be successful in patients with partial SBO. IV fluid Nasogastric tube Water soluble contrast- Hypertonic water soluble contrast agents (eg, Gastrografin) can be used for both diagnostic and therapeutic purposes in the setting of partial small bowel obstruction.
37 OPERATIVE MANAGEMENT Approximately one-quarter of patients admitted for small bowel obstruction will require operation. Patients suspected of having complete or closed-loop obstruction with fever, leukocytosis, tachycardia, metabolic acidosis, continuous pain or peritonitis warrant prompt exploration.
38 Surgery consult was done and the patient referred for laparatomy.
39 Laparatomy was performed: A nodule and stricture was found in 30cm from treits ligament in jejunum that was resected.
40 Pathologic report: Pneumatosis cystoides Intestinalis
ACUTE ABDOMEN. Dr. M Asadi. Surgical Oncology Research Center MUMS. Assistant Professor of General Surgery
 ACUTE ABDOMEN Dr. M Asadi Assistant Professor of General Surgery Surgical Oncology Research Center MUMS Definition I. The term Acute Abdomen refers to signs & symptoms of abdominal pain and tenderness,
ACUTE ABDOMEN Dr. M Asadi Assistant Professor of General Surgery Surgical Oncology Research Center MUMS Definition I. The term Acute Abdomen refers to signs & symptoms of abdominal pain and tenderness,
Abdominal Pain. Luke Donnelly, MD Emergency Medicine
 Abdominal Pain Luke Donnelly, MD Emergency Medicine Objectives Approach to abdominal pain Evaluation Critical diagnoses and treatments Abdominal Pain Most Common ER Complaint Broad Differential Can often
Abdominal Pain Luke Donnelly, MD Emergency Medicine Objectives Approach to abdominal pain Evaluation Critical diagnoses and treatments Abdominal Pain Most Common ER Complaint Broad Differential Can often
An Approach to Abdominal Pain
 An Approach to Abdominal Pain objectives Should know the different types of abd pain Is acute or chronic? Hx taking skills with knowing the key questions Important abdominal pain signs A good differential
An Approach to Abdominal Pain objectives Should know the different types of abd pain Is acute or chronic? Hx taking skills with knowing the key questions Important abdominal pain signs A good differential
GASTROENTEROLOGY ESSENTIALS
 GASTROENTEROLOGY ESSENTIALS Practical Gastroenterology 8/25/2018 Jahnavi Koppala, MBBS Abdullah Abdussalam, MD A 48-year-old male was evaluated for noncardiac chest pain. Treatment with PPI twice daily
GASTROENTEROLOGY ESSENTIALS Practical Gastroenterology 8/25/2018 Jahnavi Koppala, MBBS Abdullah Abdussalam, MD A 48-year-old male was evaluated for noncardiac chest pain. Treatment with PPI twice daily
UNDERSTANDING X-RAYS: ABDOMINAL IMAGING THE ABDOMEN
 UNDERSTANDING X-RAYS: ABDOMINAL IMAGING THE ABDOMEN Radiology Enterprises radiologyenterprises@gmail.com www.radiologyenterprises.com STOMACH AND SMALL BOWEL STOMACH AND SMALL BOWEL Swallowed air is a
UNDERSTANDING X-RAYS: ABDOMINAL IMAGING THE ABDOMEN Radiology Enterprises radiologyenterprises@gmail.com www.radiologyenterprises.com STOMACH AND SMALL BOWEL STOMACH AND SMALL BOWEL Swallowed air is a
Abdominal Assessment
 Abdominal Assessment Mary Marian, MS,RD,CSO University of AZ, Tucson, AZ Neha Parekh, MS,RD,LD,CNSC Cleveland Clinic, Cleveland, OH Objectives: 1. Outline the steps in performing an abdominal examination.
Abdominal Assessment Mary Marian, MS,RD,CSO University of AZ, Tucson, AZ Neha Parekh, MS,RD,LD,CNSC Cleveland Clinic, Cleveland, OH Objectives: 1. Outline the steps in performing an abdominal examination.
General Data. 王 X 村 78 y/o 男性
 General Data 王 X 村 78 y/o 男性 Chief Complaint Vomiting twice this early morning Fever up to 38.9ºC was noted Present Illness (1) Old CVA with left side weakness for more than 10 years and with bed ridden
General Data 王 X 村 78 y/o 男性 Chief Complaint Vomiting twice this early morning Fever up to 38.9ºC was noted Present Illness (1) Old CVA with left side weakness for more than 10 years and with bed ridden
Vomiting Approach to diagnosis
 Vomiting Approach to diagnosis By Dr. Sahar El-Gharabawy Associate professor of internal medicine Hepato-gastroenterology Unit )SMH ) Mansoura University Definitions: Nausea: Feeling "sick to the stomach",
Vomiting Approach to diagnosis By Dr. Sahar El-Gharabawy Associate professor of internal medicine Hepato-gastroenterology Unit )SMH ) Mansoura University Definitions: Nausea: Feeling "sick to the stomach",
ADULT RETROGRADE INTUSSUSCEPTION Brian Tiu Richmond University Medical Center September 3, 2015
 ADULT RETROGRADE INTUSSUSCEPTION Brian Tiu Richmond University Medical Center September 3, 2015 CASE PRESENTATION 41 yo woman presented one day hx abdominal pain, worsening nausea/vomiting denied flatus/bm
ADULT RETROGRADE INTUSSUSCEPTION Brian Tiu Richmond University Medical Center September 3, 2015 CASE PRESENTATION 41 yo woman presented one day hx abdominal pain, worsening nausea/vomiting denied flatus/bm
Documentation Dissection
 History of Present Illness: Documentation Dissection The patient is a 50-year-old male c/o symptoms for past 4 months 1, severe 2 bloating and stomach cramps, some nausea, vomiting, diarrhea. In last 3
History of Present Illness: Documentation Dissection The patient is a 50-year-old male c/o symptoms for past 4 months 1, severe 2 bloating and stomach cramps, some nausea, vomiting, diarrhea. In last 3
A Case of Pneumatosis Cystoides Intestinalis Mimicking Intestinal Perforation
 Showa Univ J Med Sci 26 2, 169 173, June 2014 Case Report A Case of Pneumatosis Cystoides Intestinalis Mimicking Intestinal Perforation Takahiro UMEMOTO 1, Yoshikuni HARADA 1, Makiko SAKATA 1, Gaku KIGAWA
Showa Univ J Med Sci 26 2, 169 173, June 2014 Case Report A Case of Pneumatosis Cystoides Intestinalis Mimicking Intestinal Perforation Takahiro UMEMOTO 1, Yoshikuni HARADA 1, Makiko SAKATA 1, Gaku KIGAWA
VOMITING. Tan Lay Zye
 VOMITING Tan Lay Zye Vomiting is a common symptom. It is a complex reflex behavioural response involving forceful expulsion of the stomach contents through oral cavity. Contents Emetic reflex Causes of
VOMITING Tan Lay Zye Vomiting is a common symptom. It is a complex reflex behavioural response involving forceful expulsion of the stomach contents through oral cavity. Contents Emetic reflex Causes of
Perforation of a Duodenal Diverticulum. Elective Student S. C.
 Perforation of a Duodenal Diverticulum 2008 4 Elective Student S. C. Case History An elderly male presented to the Emergency Department with abdominal pain. Chief Complaint: Worsening, diffuse abdominal
Perforation of a Duodenal Diverticulum 2008 4 Elective Student S. C. Case History An elderly male presented to the Emergency Department with abdominal pain. Chief Complaint: Worsening, diffuse abdominal
12 Blueprints Q&A Step 2 Surgery
 12 Blueprints Q&A Step 2 Surgery 34. A 40-year-old female has been referred to you for a recent ER and hospital admission, from which she was given a diagnosis of acute diverticulitis. Treatment at that
12 Blueprints Q&A Step 2 Surgery 34. A 40-year-old female has been referred to you for a recent ER and hospital admission, from which she was given a diagnosis of acute diverticulitis. Treatment at that
Acute Abdomen. Nirav Patel MD, FACS Banner University Medical Center - Phoenix
 Acute Abdomen Nirav Patel MD, FACS Banner University Medical Center - Phoenix ? Diffuse periumbilical with localization to RLQ + Nausea, anorexia, fevers - Diarrhea, emesis Exacerbated by movement, bumps
Acute Abdomen Nirav Patel MD, FACS Banner University Medical Center - Phoenix ? Diffuse periumbilical with localization to RLQ + Nausea, anorexia, fevers - Diarrhea, emesis Exacerbated by movement, bumps
Cecal Volvulus: Case Presentation and Review of CT Findings
 August 2011 Cecal Volvulus: Case Presentation and Review of CT Findings Omar Pardesi, Harvard Medical School Year III Our Patient LD: History & Physical HPI: 28 y.o. female presents with diffuse abdominal
August 2011 Cecal Volvulus: Case Presentation and Review of CT Findings Omar Pardesi, Harvard Medical School Year III Our Patient LD: History & Physical HPI: 28 y.o. female presents with diffuse abdominal
Chapter 32 Gastroenterology General Pathophysiology General Risk Factors for GI emergencies: Excessive Consumption Excessive Smoking Increased
 1 2 3 4 5 6 7 Chapter 32 Gastroenterology General Pathophysiology General Risk Factors for GI emergencies: Excessive Consumption Excessive Smoking Increased Ingestion of Caustic Substances Poor Bowel Habits
1 2 3 4 5 6 7 Chapter 32 Gastroenterology General Pathophysiology General Risk Factors for GI emergencies: Excessive Consumption Excessive Smoking Increased Ingestion of Caustic Substances Poor Bowel Habits
Spleen indications of splenectomy complications OPSI
 Intestinal obstruction Differences between adynamic ileus and mechanical obstruction Aetiology Pathophysiology (Cluster contractions- bowel proximal to the obstruction dilate- wall of obstructed gut is
Intestinal obstruction Differences between adynamic ileus and mechanical obstruction Aetiology Pathophysiology (Cluster contractions- bowel proximal to the obstruction dilate- wall of obstructed gut is
Introduction and Definitions
 Bowel obstruction Introduction and Definitions Accounts for 5% of all acute surgical admissions Patients are often extremely ill requiring prompt assessment, resuscitation and intensive monitoring Obstruction
Bowel obstruction Introduction and Definitions Accounts for 5% of all acute surgical admissions Patients are often extremely ill requiring prompt assessment, resuscitation and intensive monitoring Obstruction
CLINICAL PRESENTATION AND RADIOLOGY QUIZ QUESTION
 Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 09/17/2011 Radiology Quiz of the Week # 38 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 09/17/2011 Radiology Quiz of the Week # 38 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
Management of Small Bowel Obstruction: An Update. Case Presentation
 Management of Small Bowel Obstruction: An Update The Postgraduate Course in General Surgery March 20-23, 2011 Jonathan Carter, MD Assistant Professor of Surgery Case Presentation 67 year old otherwise
Management of Small Bowel Obstruction: An Update The Postgraduate Course in General Surgery March 20-23, 2011 Jonathan Carter, MD Assistant Professor of Surgery Case Presentation 67 year old otherwise
3/21/2011. Case Presentation. Management of Small Bowel Obstruction: An Update. CT abdomen and pelvis. Abdominal plain films
 Case Presentation 67 year old otherwise healthy woman presents to the ED with a chief complaint of abdominal pain, nausea and vomiting for five days. Management of Small Bowel Obstruction: An Update The
Case Presentation 67 year old otherwise healthy woman presents to the ED with a chief complaint of abdominal pain, nausea and vomiting for five days. Management of Small Bowel Obstruction: An Update The
3/22/2011. Inflammatory Bowel Disease. Inflammatory Bowel Disease Objectives: Appendicitis. Lemone and Burke Chapter 26
 Inflammatory Bowel Disease Lemone and Burke Chapter 26 Inflammatory Bowel Disease Objectives: Discuss etiology, patho and clinical manifestations of Appendicitis Peritonitis Ulcerative Colitis Crohn s
Inflammatory Bowel Disease Lemone and Burke Chapter 26 Inflammatory Bowel Disease Objectives: Discuss etiology, patho and clinical manifestations of Appendicitis Peritonitis Ulcerative Colitis Crohn s
Case Cholecystoduodenal fistula with migrated gallstone leading to gastric outlet obstruction: Bouveret's syndrome
 Case 14613 Cholecystoduodenal fistula with migrated gallstone leading to gastric outlet obstruction: Bouveret's syndrome Eva De Backer 1, Filip Vanhoenacker 2, 3, 4, Adelard De Backer5 1: Ghent University,
Case 14613 Cholecystoduodenal fistula with migrated gallstone leading to gastric outlet obstruction: Bouveret's syndrome Eva De Backer 1, Filip Vanhoenacker 2, 3, 4, Adelard De Backer5 1: Ghent University,
Intestinal Obstruction Clinical Presentation & Causes
 Intestinal Obstruction Clinical Presentation & Causes V Chidambaram-Nathan Consultant Transplant and General Surgeon Sheffield Kidney Institute Northern General Hospital Intestinal Obstruction One of the
Intestinal Obstruction Clinical Presentation & Causes V Chidambaram-Nathan Consultant Transplant and General Surgeon Sheffield Kidney Institute Northern General Hospital Intestinal Obstruction One of the
Surgical Management of IBD. Val Jefford Grand Rounds October 14, 2003
 Surgical Management of IBD Val Jefford Grand Rounds October 14, 2003 Introduction Important Features Clinical Presentation Evaluation Medical Treatment Surgical Treatment Cases Overview Introduction Two
Surgical Management of IBD Val Jefford Grand Rounds October 14, 2003 Introduction Important Features Clinical Presentation Evaluation Medical Treatment Surgical Treatment Cases Overview Introduction Two
Nordic Forum - Trauma & Emergency Radiology. Bowel Obstruction: Imaging Update
 Nordic Forum - Trauma & Emergency Radiology Bowel Obstruction: Imaging Update Borut Marincek Institute of Diagnostic Radiology University Hospital Zurich, Switzerland Acute Abdomen Bowel Obstruction Bowel
Nordic Forum - Trauma & Emergency Radiology Bowel Obstruction: Imaging Update Borut Marincek Institute of Diagnostic Radiology University Hospital Zurich, Switzerland Acute Abdomen Bowel Obstruction Bowel
Resident Teaching Conference 10/16/09 Rondi Kauffmann Resident presenter William Nealon Faculty presenter
 Resident Teaching Conference 10/16/09 Rondi Kauffmann Resident presenter William Nealon Faculty presenter KC 59 year old male Referred to Surgery clinic for incidentally discovered 5cm x 3cm pancreatic
Resident Teaching Conference 10/16/09 Rondi Kauffmann Resident presenter William Nealon Faculty presenter KC 59 year old male Referred to Surgery clinic for incidentally discovered 5cm x 3cm pancreatic
Plain abdomen The standard films are supine & erect AP views (alternative to erect, lateral decubitus film is used in ill patients).
.") Plain abdomen The standard films are supine & erect AP views (alternative to erect, lateral decubitus film is used in ill patients). The stomach can be readily identified by its location, gastric rugae
Plain abdomen The standard films are supine & erect AP views (alternative to erect, lateral decubitus film is used in ill patients). The stomach can be readily identified by its location, gastric rugae
GENERAL SURGERY FOR SMART PEOPLE JOE NOLD MD, FACS WICHITA SURGICAL SPECIALISTS
 GENERAL SURGERY FOR SMART PEOPLE JOE NOLD MD, FACS WICHITA SURGICAL SPECIALISTS CONFLICTS/DECLARATIONS I have no financial conflicts or declarations I AM always willing to see a consult for you TEXT TOPICS
GENERAL SURGERY FOR SMART PEOPLE JOE NOLD MD, FACS WICHITA SURGICAL SPECIALISTS CONFLICTS/DECLARATIONS I have no financial conflicts or declarations I AM always willing to see a consult for you TEXT TOPICS
Gastrointestinal Tract Imaging. Objectives. Reference. VMB 960 April 6, Stomach Small Intestine Colon. Radiography & Ultrasound
 Gastrointestinal Tract Imaging VMB 960 April 6, 2009 Stomach Small Intestine Colon Objectives Radiography & Ultrasound Contrast Examination of the Small Intestine Reference Chapters 45 47 Pages 750 805
Gastrointestinal Tract Imaging VMB 960 April 6, 2009 Stomach Small Intestine Colon Objectives Radiography & Ultrasound Contrast Examination of the Small Intestine Reference Chapters 45 47 Pages 750 805
Adv Pathophysiology Unit 9: GI Page 1 of 10
 Adv Pathophysiology Unit 9: GI Page 1 of 10 Learning objectives for this file: 1. Recognize positive physical and lab findings that point to the diagnosis 2. Appreciate the appearance of the affected organ
Adv Pathophysiology Unit 9: GI Page 1 of 10 Learning objectives for this file: 1. Recognize positive physical and lab findings that point to the diagnosis 2. Appreciate the appearance of the affected organ
PMH: DM HTN Colon cancer s/p left hemicolectomy, chemo Now with mets to liver and peritoneum. Restarted on chemo 2/4/13 oxaliplatin, cepecitabine
 3.5.2013 75 y.o M with PMH of HTN, DM II with nephropathy, CKD stage III(b/l cr 1.5), colon cancer s/p hemicolectomy (8/2011) now with recurrence and mets to liver and peritoneum undergoing chemo at woodhull,
3.5.2013 75 y.o M with PMH of HTN, DM II with nephropathy, CKD stage III(b/l cr 1.5), colon cancer s/p hemicolectomy (8/2011) now with recurrence and mets to liver and peritoneum undergoing chemo at woodhull,
Chapter 34. Nursing Care of Patients with Lower Gastrointestinal Disorders
 Chapter 34 Nursing Care of Patients with Lower Gastrointestinal Disorders Lower Gastrointestinal System Small Intestines Large Intestines Rectum Anus Constipation Fecal Mass Held In Rectum Feces Become
Chapter 34 Nursing Care of Patients with Lower Gastrointestinal Disorders Lower Gastrointestinal System Small Intestines Large Intestines Rectum Anus Constipation Fecal Mass Held In Rectum Feces Become
LOOKING FOR AIR IN ALL THE WRONG PLACES Richard M. Gore, MD North Shore University Health System University of Chicago Evanston, IL
 SIGNIFICANCE OF EXTRALUMINAL ABDOMINAL GAS: LOOKING FOR AIR IN ALL THE WRONG PLACES Richard M. Gore, MD North Shore University Health System University of Chicago Evanston, IL SCBT/MR 2012 October 26,
SIGNIFICANCE OF EXTRALUMINAL ABDOMINAL GAS: LOOKING FOR AIR IN ALL THE WRONG PLACES Richard M. Gore, MD North Shore University Health System University of Chicago Evanston, IL SCBT/MR 2012 October 26,
Gastrointestinal Emergencies CEN REVIEW 2017 MARY RALEY, BSN, RN, CEN, TCRN, TNSCC
 Gastrointestinal Emergencies CEN REVIEW 2017 MARY RALEY, BSN, RN, CEN, TCRN, TNSCC Gastrointestinal Emergencies is 7% of the CEN A. Acute abdomen B. Bleeding C. Cholecystitis D. Cirrhosis E. Diverticulitis
Gastrointestinal Emergencies CEN REVIEW 2017 MARY RALEY, BSN, RN, CEN, TCRN, TNSCC Gastrointestinal Emergencies is 7% of the CEN A. Acute abdomen B. Bleeding C. Cholecystitis D. Cirrhosis E. Diverticulitis
Computed tomography (CT) imaging review of small bowel obstruction
 imaging review of small bowel obstruction") Computed tomography (CT) imaging review of small bowel obstruction Poster No.: C-1602 Congress: ECR 2010 Type: Educational Exhibit Topic: GI Tract - Small Bowel Authors: A. Vousough, D. S. Prasad ; Aberdeen/UK,
Computed tomography (CT) imaging review of small bowel obstruction Poster No.: C-1602 Congress: ECR 2010 Type: Educational Exhibit Topic: GI Tract - Small Bowel Authors: A. Vousough, D. S. Prasad ; Aberdeen/UK,
Evidence Process for Abdominal Pain Guideline Research 11/16/2017. Guideline Review using ADAPTE method and AGREE II instrument 11/16/2017
 Evidence Process for Abdominal Pain Guideline Research Guideline Review using ADAPTE method and AGREE II instrument Approximately 139 Potentially relevant guidelines identified in various resources* 59
Evidence Process for Abdominal Pain Guideline Research Guideline Review using ADAPTE method and AGREE II instrument Approximately 139 Potentially relevant guidelines identified in various resources* 59
Evolving Gallstone Ileus. SUNY Downstate Case Conference January 12, 2012
 Evolving Gallstone Ileus SUNY Downstate Case Conference January 12, 2012 Initial Presentation HPI: 90 yo F c 1wk h/o abdominal pain and N/V. Denied F/C. Passing flatus/bm. PMH: DM, HTN, CAD. PSH: C-sections
Evolving Gallstone Ileus SUNY Downstate Case Conference January 12, 2012 Initial Presentation HPI: 90 yo F c 1wk h/o abdominal pain and N/V. Denied F/C. Passing flatus/bm. PMH: DM, HTN, CAD. PSH: C-sections
CASE-BASED SMALL GROUP DISCUSSION MHD II
 MHD II, Session 11, Student Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION MHD II Session 11 April 11, 2016 STUDENT COPY MHD II, Session 11, Student Copy Page 2 CASE HISTORY 1 Chief complaint: Our baby
MHD II, Session 11, Student Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION MHD II Session 11 April 11, 2016 STUDENT COPY MHD II, Session 11, Student Copy Page 2 CASE HISTORY 1 Chief complaint: Our baby
Causes of abdominal pain Doctors in the ED spend lots of time and money diagnosing abdominal pain. They still often do not know the exact cause
 1 2 3 What's Going On in There? EMS and Abdominal Pain Kevin McFarlane BSN,RN,CEN,CPEN,EMT Southwest Emergency Education and Consulting What is going on in there Acute Abdomen Sudden onset of pain within
1 2 3 What's Going On in There? EMS and Abdominal Pain Kevin McFarlane BSN,RN,CEN,CPEN,EMT Southwest Emergency Education and Consulting What is going on in there Acute Abdomen Sudden onset of pain within
X-ray Corner. Imaging of the Small Bowel. Pantongrag-Brown L. Case 1. A 63-year-old man presented with abdominal pain, nausea and vomiting.
 THAI J 42 Imaging of the Small Bowel GASTROENTEROL 2015 X-ray Corner Imaging of the Small Bowel Pantongrag-Brown L Small bowel is the longest tubular organ in the body, about 18-22 feet. It is anchored
THAI J 42 Imaging of the Small Bowel GASTROENTEROL 2015 X-ray Corner Imaging of the Small Bowel Pantongrag-Brown L Small bowel is the longest tubular organ in the body, about 18-22 feet. It is anchored
Computed tomography (CT) imaging review of small bowel obstruction
 imaging review of small bowel obstruction") Computed tomography (CT) imaging review of small bowel obstruction Poster No.: C-1602 Congress: ECR 2010 Type: Educational Exhibit Topic: GI Tract Authors: A. Vousough, D. S. Prasad ; Aberdeen/UK, Leeds/UK
Computed tomography (CT) imaging review of small bowel obstruction Poster No.: C-1602 Congress: ECR 2010 Type: Educational Exhibit Topic: GI Tract Authors: A. Vousough, D. S. Prasad ; Aberdeen/UK, Leeds/UK
Gastroenterology. Certification Examination Blueprint. Purpose of the exam
 Gastroenterology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified gastroenterologist
Gastroenterology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified gastroenterologist
Chapter 14: Training in Radiology. DDSEP Chapter 1: Question 12
 DDSEP Chapter 1: Question 12 A 52-year-old white male presents for evaluation of sudden onset of abdominal pain and shoulder pain. His past medical history is notable for a history of coronary artery disease,
DDSEP Chapter 1: Question 12 A 52-year-old white male presents for evaluation of sudden onset of abdominal pain and shoulder pain. His past medical history is notable for a history of coronary artery disease,
Role of imaging in the evaluation of the acute abdomen
 Prof. András Palkó MD, PhD Role of imaging in the evaluation of the acute abdomen Faculty of General Medicine University of Szeged Hungary 1 Definition Sudden onset of severe symptoms requiring emergency
Prof. András Palkó MD, PhD Role of imaging in the evaluation of the acute abdomen Faculty of General Medicine University of Szeged Hungary 1 Definition Sudden onset of severe symptoms requiring emergency
LOKUN! I got stomach ache!
 LOKUN! I got stomach ache! Mr L is a 67year old Chinese gentleman who is a non smoker, social drinker. He has a medical history significant for Hypertension, Hyperlipidemia, Type 2 Diabetes Mellitus, Chronic
LOKUN! I got stomach ache! Mr L is a 67year old Chinese gentleman who is a non smoker, social drinker. He has a medical history significant for Hypertension, Hyperlipidemia, Type 2 Diabetes Mellitus, Chronic
Safe Answers For The American Board of Surgery Certifying Exam & Recertifying Exam
 Safe Answers For The American Board of Surgery Certifying Exam & Recertifying Exam By Sarmad Aji, MD., FACS. A comprehensive review of the most commonly asked questions on the American Board of Surgery
Safe Answers For The American Board of Surgery Certifying Exam & Recertifying Exam By Sarmad Aji, MD., FACS. A comprehensive review of the most commonly asked questions on the American Board of Surgery
BRONCHOGENIC CARCINOMA CHALLENGES IN EVALUATION
 BRONCHOGENIC CARCINOMA CHALLENGES IN EVALUATION GRAND ROUND WARD 7C DATE: 25 TH MARCH 2015 PRESENTER: DR E. SAYO FACILITATOR: DR J MECHA DEMOGRAPHIC DATA NAME : CM AGE: 69 YEARS ADDRESS : KIAMBU OCCUPATION:
BRONCHOGENIC CARCINOMA CHALLENGES IN EVALUATION GRAND ROUND WARD 7C DATE: 25 TH MARCH 2015 PRESENTER: DR E. SAYO FACILITATOR: DR J MECHA DEMOGRAPHIC DATA NAME : CM AGE: 69 YEARS ADDRESS : KIAMBU OCCUPATION:
Always keep it in the differential
 Acute Appendicitis Lissa C. Sakata and Lindsey Perea 2 Always keep it in the differential Learning Objectives 1. The learner should be able to describe the etiology of acute appendicitis. 2. The learner
Acute Appendicitis Lissa C. Sakata and Lindsey Perea 2 Always keep it in the differential Learning Objectives 1. The learner should be able to describe the etiology of acute appendicitis. 2. The learner
GENI Program: GI and Abdominal Chief Complaints. Kim Macfarlane Clinical Nurse Specialist, Critical Care February 2008
 GENI Program: GI and Abdominal Chief Complaints Kim Macfarlane Clinical Nurse Specialist, Critical Care February 2008 Dehydration Common acute and chronic problem Recognition is critically important to
GENI Program: GI and Abdominal Chief Complaints Kim Macfarlane Clinical Nurse Specialist, Critical Care February 2008 Dehydration Common acute and chronic problem Recognition is critically important to
What is Crohn's disease?
 What is Crohn's disease? Crohn's disease is a chronic inflammatory disorder that causes inflammation of the digestive tract. It can affect any area of the GI tract, from the mouth to the anus, but it most
What is Crohn's disease? Crohn's disease is a chronic inflammatory disorder that causes inflammation of the digestive tract. It can affect any area of the GI tract, from the mouth to the anus, but it most
Surgical Education Series
 Surgical Education Series The Acute Abdomen Ahmad kachooei, MD MPH Assistant Professor Division of General Surgery Department of Surgery University of Qom Outline Definitions What causes an acute abdomen
Surgical Education Series The Acute Abdomen Ahmad kachooei, MD MPH Assistant Professor Division of General Surgery Department of Surgery University of Qom Outline Definitions What causes an acute abdomen
ACUTE ABDOMEN IN OLDER CHILDREN. Carlos J. Sivit M.D.
 ACUTE ABDOMEN IN OLDER CHILDREN Carlos J. Sivit M.D. ACUTE ABDOMEN Clinical condition characterized by severe abdominal pain developing over several hours ACUTE ABDOMINAL PAIN Common childhood complaint
ACUTE ABDOMEN IN OLDER CHILDREN Carlos J. Sivit M.D. ACUTE ABDOMEN Clinical condition characterized by severe abdominal pain developing over several hours ACUTE ABDOMINAL PAIN Common childhood complaint
GASTROENTEROLOGY Maintenance of Certification (MOC) Examination Blueprint
 Examination Blueprint") GASTROENTEROLOGY Maintenance of Certification (MOC) Examination Blueprint ABIM invites diplomates to help develop the Gastroenterology MOC exam blueprint Based on feedback from physicians that MOC assessments
GASTROENTEROLOGY Maintenance of Certification (MOC) Examination Blueprint ABIM invites diplomates to help develop the Gastroenterology MOC exam blueprint Based on feedback from physicians that MOC assessments
Case Scenario 1. Discharge Summary
 Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
Emergency Surgery Board Department of General Surgery Rambam Health Care Campus
 Emergency Surgery Board Department of General Surgery Rambam Health Care Campus Surgical Complications of Peptic Ulcer Disease Case Presentation and Review of the Literature Case Presentation 40y male
Emergency Surgery Board Department of General Surgery Rambam Health Care Campus Surgical Complications of Peptic Ulcer Disease Case Presentation and Review of the Literature Case Presentation 40y male
Cases from the Clinic Maryland ACP Meeting January 30, 2016
 Cases from the Clinic Maryland ACP Meeting January 30, 2016 Bimal Ashar, MD, FACP D. William Schlott, MD Associate Professor of Medicine Johns Hopkins University School of Medicine 1 CASE 1: GK 46-year-old
Cases from the Clinic Maryland ACP Meeting January 30, 2016 Bimal Ashar, MD, FACP D. William Schlott, MD Associate Professor of Medicine Johns Hopkins University School of Medicine 1 CASE 1: GK 46-year-old
Case Discussion Splenic Abscess
 Case Discussion Splenic Abscess Personal Data Gender: male Birth Date: 1928/Mar/06th Allergy: Mefenamic Smoking: 0.5 PPD for 55 years Alcohol: negative (?) 4 Months Ago Abdominal pain: epigastric area
Case Discussion Splenic Abscess Personal Data Gender: male Birth Date: 1928/Mar/06th Allergy: Mefenamic Smoking: 0.5 PPD for 55 years Alcohol: negative (?) 4 Months Ago Abdominal pain: epigastric area
Case Report An Uncommon Cause of a Small-Bowel Obstruction
 Hindawi Case Reports in Gastrointestinal Medicine Volume 2017, Article ID 1628215, 4 pages https://doi.org/10.1155/2017/1628215 Case Report An Uncommon Cause of a Small-Bowel Obstruction Ali Zakaria, Bayan
Hindawi Case Reports in Gastrointestinal Medicine Volume 2017, Article ID 1628215, 4 pages https://doi.org/10.1155/2017/1628215 Case Report An Uncommon Cause of a Small-Bowel Obstruction Ali Zakaria, Bayan
: Abdominal Emergencies
 INTRODUCTION Abdominal complaints are very common in emergency medicine. The specific cause of the abdominal pain can very rarely be determined in the pre-hospital environment, however performing a good
INTRODUCTION Abdominal complaints are very common in emergency medicine. The specific cause of the abdominal pain can very rarely be determined in the pre-hospital environment, however performing a good
Appendix 5. EFSUMB Newsletter. Gastroenterological Ultrasound
 EFSUMB Newsletter 87 Examinations should encompass the full range of pathological conditions listed below A log book listing the types of examinations undertaken should be kept Training should usually
EFSUMB Newsletter 87 Examinations should encompass the full range of pathological conditions listed below A log book listing the types of examinations undertaken should be kept Training should usually
SASKATCHEWAN REGISTERED NURSES ASSOCIATION. RNs WITH ADDITIONAL AUTHORIZED PRACTICE CLINICAL DECISION TOOL AUGUST 2017
 DEFINITION Cholelithiasis Presence of gall stones in the biliary tract. Biliary Colic Right upper quadrant pain due to obstruction of a bile duct by a gallstone. Cholecystitis Inflammation of the gallbladder
DEFINITION Cholelithiasis Presence of gall stones in the biliary tract. Biliary Colic Right upper quadrant pain due to obstruction of a bile duct by a gallstone. Cholecystitis Inflammation of the gallbladder
Abdo Pain rules & regulations. Mark Hartnell 2010
 Abdo Pain rules & regulations Mark Hartnell 2010 Aims Simple rules which might help in patients with abdominal pain Talk about some myths and realities Discuss some practical how to s in day to day treatment
Abdo Pain rules & regulations Mark Hartnell 2010 Aims Simple rules which might help in patients with abdominal pain Talk about some myths and realities Discuss some practical how to s in day to day treatment
Correspondence should be addressed to Justin Cochrane;
 Case Reports in Gastrointestinal Medicine Volume 2015, Article ID 794282, 4 pages http://dx.doi.org/10.1155/2015/794282 Case Report Acute on Chronic Pancreatitis Causing a Highway to the Colon with Subsequent
Case Reports in Gastrointestinal Medicine Volume 2015, Article ID 794282, 4 pages http://dx.doi.org/10.1155/2015/794282 Case Report Acute on Chronic Pancreatitis Causing a Highway to the Colon with Subsequent
Nephrotic Syndrome. Sara Alsharhan PharmD candidate, KSU 2014
 Nephrotic Syndrome Sara Alsharhan PharmD candidate, KSU 2014 Outline Introduction Nephrotic syndrome classifications Signs and symptoms Diagnoses Management Complications Monitoring Case presentation Introduction
Nephrotic Syndrome Sara Alsharhan PharmD candidate, KSU 2014 Outline Introduction Nephrotic syndrome classifications Signs and symptoms Diagnoses Management Complications Monitoring Case presentation Introduction
Abdominal radiology 腹部放射線學
 Abdominal radiology 腹部放射線學 台北醫學大學 - 市立萬芳醫院 留偉順 laowilson@hotmail.com The Normal Abdominal Series Chest Supine abdomen Erect abdomen Left lateral decubitus abdomen Learning objectives Understanding normal
Abdominal radiology 腹部放射線學 台北醫學大學 - 市立萬芳醫院 留偉順 laowilson@hotmail.com The Normal Abdominal Series Chest Supine abdomen Erect abdomen Left lateral decubitus abdomen Learning objectives Understanding normal
Phillip A. Bilderback, MD, Ryan K. Smith, BA, and W. Scott Helton, MD, FACS
 gastrointestinal tract and abdomen INTESTINAL OBSTRUCTION Phillip A. Bilderback, MD, Ryan K. Smith, BA, and W. Scott Helton, MD, FACS Intestinal obstruction is a common medical problem and accounts for
gastrointestinal tract and abdomen INTESTINAL OBSTRUCTION Phillip A. Bilderback, MD, Ryan K. Smith, BA, and W. Scott Helton, MD, FACS Intestinal obstruction is a common medical problem and accounts for
ASSESSING THE PLAIN ABDOMINAL RADIOGRAPH M A A M E F O S U A A M P O F O
 ASSESSING THE PLAIN ABDOMINAL RADIOGRAPH M A A M E F O S U A A M P O F O Introduction The abdomen (less formally called the belly, stomach, is that part of the body between the thorax (chest) and pelvis,
ASSESSING THE PLAIN ABDOMINAL RADIOGRAPH M A A M E F O S U A A M P O F O Introduction The abdomen (less formally called the belly, stomach, is that part of the body between the thorax (chest) and pelvis,
ENTEROCOLITIDES CAN YOU TELL THEM APART ON MDCT? Richard M. Gore, MD North Shore University Medical Center University of Chicago Evanston, Illinois
 ENTEROCOLITIDES CAN YOU TELL THEM APART ON MDCT? Richard M. Gore, MD North Shore University Medical Center University of Chicago Evanston, Illinois SCBT/MR 2010 San Diego, California March 8, 2010 13:40-14:00
ENTEROCOLITIDES CAN YOU TELL THEM APART ON MDCT? Richard M. Gore, MD North Shore University Medical Center University of Chicago Evanston, Illinois SCBT/MR 2010 San Diego, California March 8, 2010 13:40-14:00
In any operation. Indications. Anaesthesia. Position of the patient. Incision. Steps of the operation. Complications.
 In any operation Indications. Anaesthesia. Position of the patient. Incision. Steps of the operation. Complications. Abdominal operation I position for operation Supine Abdominal operation I position for
In any operation Indications. Anaesthesia. Position of the patient. Incision. Steps of the operation. Complications. Abdominal operation I position for operation Supine Abdominal operation I position for
Clinical Anatomy of the Biliary Apparatus: Relations & Variations
 Clinical Anatomy of the Biliary Apparatus: Relations & Variations Handout download: http://www.oucom.ohiou.edu/dbms-witmer/gs-rpac.htm 27 March 2007 Lawrence M. Witmer, PhD Professor of Anatomy Department
Clinical Anatomy of the Biliary Apparatus: Relations & Variations Handout download: http://www.oucom.ohiou.edu/dbms-witmer/gs-rpac.htm 27 March 2007 Lawrence M. Witmer, PhD Professor of Anatomy Department
GI Grand Rounds. A A Lifetime of Abdominal Pain 12/9/2004 Tim Edwards
 GI Grand Rounds A A Lifetime of Abdominal Pain 12/9/2004 Tim Edwards PMH Aug 25, 1992 4 year old male presents to a pediatric gastroenterologist for primary complaint of anorexia, intermittent abdominal
GI Grand Rounds A A Lifetime of Abdominal Pain 12/9/2004 Tim Edwards PMH Aug 25, 1992 4 year old male presents to a pediatric gastroenterologist for primary complaint of anorexia, intermittent abdominal
Postgastrectomy Syndromes
 Postgastrectomy Syndromes Postgastrectomy syndromes are iatrogenic conditions that may arise from partial gastrectomies, independent of whether the gastric surgery was initially performed for peptic ulcer
Postgastrectomy Syndromes Postgastrectomy syndromes are iatrogenic conditions that may arise from partial gastrectomies, independent of whether the gastric surgery was initially performed for peptic ulcer
no concerns hepatic shunt, high protein diet, kidney failure, metabolic acidosis
 TAKING THE WORK OUT OF INTERPRETING LAB WORK CACVT 2017 SPRING CONFERENCE - GREENWOOD VILLAGE, CO Brandy Helewa, CVT, RVT, VTS (ECC) Penn Foster College - Scranton, PA Knowing what the results on your
TAKING THE WORK OUT OF INTERPRETING LAB WORK CACVT 2017 SPRING CONFERENCE - GREENWOOD VILLAGE, CO Brandy Helewa, CVT, RVT, VTS (ECC) Penn Foster College - Scranton, PA Knowing what the results on your
A case of hypokalemia MIHO TAGAWA FIRST DEPARTMENT OF MEDICINE NARA MEDICAL UNIVERSITY
 A case of hypokalemia MIHO TAGAWA FIRST DEPARTMENT OF MEDICINE NARA MEDICAL UNIVERSITY Case 57 y.o. male CC: Weakness HPI: About 20 years ago, he developed bilateral lower extremity weakness. Laboratory
A case of hypokalemia MIHO TAGAWA FIRST DEPARTMENT OF MEDICINE NARA MEDICAL UNIVERSITY Case 57 y.o. male CC: Weakness HPI: About 20 years ago, he developed bilateral lower extremity weakness. Laboratory
Contrast Materials Patient Safety: What are contrast materials and how do they work?
 Contrast Materials Patient Safety: What are contrast materials and how do they work? Which imaging exams use contrast materials? How safe are contrast materials? How should I prepare for my imaging procedure
Contrast Materials Patient Safety: What are contrast materials and how do they work? Which imaging exams use contrast materials? How safe are contrast materials? How should I prepare for my imaging procedure
Gastrointestinal Obstruction
 Customer Name, Street Address, City, State, Zip code Phone number, Alt. phone number, Fax number, e-mail address, web site Gastrointestinal Obstruction (Blockage of the Gastrointestinal Tract) Basics OVERVIEW
Customer Name, Street Address, City, State, Zip code Phone number, Alt. phone number, Fax number, e-mail address, web site Gastrointestinal Obstruction (Blockage of the Gastrointestinal Tract) Basics OVERVIEW
PROFESSIONAL SKILLS 1 3RD YEAR SEMESTER 6 RADIOGRAPHY. THE URINARY SYSTEM Uz. Fatema shmus aldeen Tel
 PROFESSIONAL SKILLS 1 3RD YEAR SEMESTER 6 RADIOGRAPHY THE URINARY SYSTEM Uz. Fatema shmus aldeen Tel. 0925111552 Professional skills-2 THE URINARY SYSTEM The urinary system (review anatomy and physiology)
PROFESSIONAL SKILLS 1 3RD YEAR SEMESTER 6 RADIOGRAPHY THE URINARY SYSTEM Uz. Fatema shmus aldeen Tel. 0925111552 Professional skills-2 THE URINARY SYSTEM The urinary system (review anatomy and physiology)
Learning Radiology: Recognizing the Basics. Text with Student Consult Online Access Code
 Learning Radiology: Recognizing the Basics. Text with Student Consult Online Access Code Herring, W ISBN-13: 9780323074445 Table of Contents 1. Recognizing Anything The "colorful" world of radiology A
Learning Radiology: Recognizing the Basics. Text with Student Consult Online Access Code Herring, W ISBN-13: 9780323074445 Table of Contents 1. Recognizing Anything The "colorful" world of radiology A
Adult Intussusception: A Complication of Metastatic Melanoma or Primary Malignancy?
 January 2013 Adult Intussusception: A Complication of Metastatic Melanoma or Primary Malignancy? Johanna Sheu, Harvard Medical School Year III 1 Agenda Menu of tests Definition/anatomy/classification Pediatrics
January 2013 Adult Intussusception: A Complication of Metastatic Melanoma or Primary Malignancy? Johanna Sheu, Harvard Medical School Year III 1 Agenda Menu of tests Definition/anatomy/classification Pediatrics
Radiological Investigations of Abdominal Trauma
 76 77 Investigations of Abdominal Trauma Introduction: Trauma to abdominal organs is a common cause of patient morbidity and mortality among trauma patients. Causes of abdominal trauma include blunt injuries,
76 77 Investigations of Abdominal Trauma Introduction: Trauma to abdominal organs is a common cause of patient morbidity and mortality among trauma patients. Causes of abdominal trauma include blunt injuries,
The appendix is a small, tube-like structure attached to the first part of the large intestine, also called the colon. The appendix.
 The appendix is a small, tube-like structure attached to the first part of the large intestine, also called the colon. The appendix is located in the lower right portion of the abdomen. It has no known
The appendix is a small, tube-like structure attached to the first part of the large intestine, also called the colon. The appendix is located in the lower right portion of the abdomen. It has no known
Chapter 18 - Gastrointestinal & Urologic Emergencies
 1 2 3 4 5 6 7 8 Chapter 18 Gastrointestinal and Urologic National EMS Education Standard Competencies (1 of 4) Medicine Applies fundamental knowledge to provide basic emergency care and transportation
1 2 3 4 5 6 7 8 Chapter 18 Gastrointestinal and Urologic National EMS Education Standard Competencies (1 of 4) Medicine Applies fundamental knowledge to provide basic emergency care and transportation
Pancreas Quizzes c. Both A and B a. Directly into the blood stream (not using ducts)
") Pancreas Quizzes Quiz 1 1. The pancreas produces hormones. Which type of hormone producing organ is the pancreas? a. Endocrine b. Exocrine c. Both A and B d. Neither A or B 2. Endocrine indicates hormones
Pancreas Quizzes Quiz 1 1. The pancreas produces hormones. Which type of hormone producing organ is the pancreas? a. Endocrine b. Exocrine c. Both A and B d. Neither A or B 2. Endocrine indicates hormones
Adult Intussusception
 Bahrain Medical Bulletin, Vol. 27, No. 3, September 2005 Adult Intussusception Suhair Alsaad, MBCHB, CABS, FRCSI* Mariam Al-Muftah, MBCHB** Objectives: Adult intussusception is a rare entity. We present
Bahrain Medical Bulletin, Vol. 27, No. 3, September 2005 Adult Intussusception Suhair Alsaad, MBCHB, CABS, FRCSI* Mariam Al-Muftah, MBCHB** Objectives: Adult intussusception is a rare entity. We present
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal pain, abdominal considerations in, 183 184 antiemetics in, 182 auscultation in, 170 C-reactive protein in, 174 175 character
Index Note: Page numbers of article titles are in boldface type. A Abdominal pain, abdominal considerations in, 183 184 antiemetics in, 182 auscultation in, 170 C-reactive protein in, 174 175 character
A novel plain abdominal radiograph sign to diagnose malrotation with volvulus
 A novel plain abdominal radiograph sign to diagnose malrotation with volvulus Nataraja RM 1, Mahomed AA 1* 1. Department of Paediatric Surgery, Royal Alexandra Hospital for Sick Children, Brighton,UK *
A novel plain abdominal radiograph sign to diagnose malrotation with volvulus Nataraja RM 1, Mahomed AA 1* 1. Department of Paediatric Surgery, Royal Alexandra Hospital for Sick Children, Brighton,UK *
Acute Mesenteric Ischemia. Michael Klein, MD SUNY Downstate Medical Center August 20, 2015
 Acute Mesenteric Ischemia Michael Klein, MD SUNY Downstate Medical Center August 20, 2015 85F www.downstatesurgery.org 5 months of intermittent diffuse abdominal pain Approximately 30-lb weight loss Abdominal
Acute Mesenteric Ischemia Michael Klein, MD SUNY Downstate Medical Center August 20, 2015 85F www.downstatesurgery.org 5 months of intermittent diffuse abdominal pain Approximately 30-lb weight loss Abdominal
Multimodal Approach for Managing Postoperative Ileus: Role of Health- System Pharmacists (ACPE program H01P)
") 1. In the normal gastrointestinal tract, what percent of nutrient absorption occurs in the jejunum? a. 20%. b. 40%. c. 70%. d. 90%. 2. According to Dr. Erstad, the four components of gastrointestinal control
1. In the normal gastrointestinal tract, what percent of nutrient absorption occurs in the jejunum? a. 20%. b. 40%. c. 70%. d. 90%. 2. According to Dr. Erstad, the four components of gastrointestinal control
East and Central African Journal of Surgery Volume 12 Number 1 - April 2007
 Surgically Treated Acute Abdomen at Gondar University Hospital, Ethiopia. 53 S. Tsegaye 1, M. Osman 2, A. Bekele 3, 1 School of public Health, University of Gondar, 2 Associate Professor of Surgery, University
Surgically Treated Acute Abdomen at Gondar University Hospital, Ethiopia. 53 S. Tsegaye 1, M. Osman 2, A. Bekele 3, 1 School of public Health, University of Gondar, 2 Associate Professor of Surgery, University
SMALL GROUP DISCUSSION
 MHD II, Session 1 Student Copy Page 1 SMALL GROUP DISCUSSION MHD II Session 1 Gastroinestinal Monday, January 9, 2017 STUDENT COPY MHD II, Session 1 Student Copy Page 2 CASE 1 CHIEF CONCERN: "I'm passing
MHD II, Session 1 Student Copy Page 1 SMALL GROUP DISCUSSION MHD II Session 1 Gastroinestinal Monday, January 9, 2017 STUDENT COPY MHD II, Session 1 Student Copy Page 2 CASE 1 CHIEF CONCERN: "I'm passing
Case conference. Welcome Dr. Lawrence Tierney
 Case conference Welcome Dr. Lawrence Tierney Case: 18 year-old male CC) hamatomesis, Fever and cough HPI) 1 st admission One month ago, he admitted to our hospital because of hematemesis. He had weight
Case conference Welcome Dr. Lawrence Tierney Case: 18 year-old male CC) hamatomesis, Fever and cough HPI) 1 st admission One month ago, he admitted to our hospital because of hematemesis. He had weight
Fecal incontinence causes 196 epidemiology 8 treatment 196
 Subject Index Achalasia course 93 differential diagnosis 93 esophageal dysphagia 92 95 etiology 92, 93 treatment 93 95 work-up 93 Aminosalicylates, pharmacokinetics and aging effects 36 Antibiotics diarrhea
Subject Index Achalasia course 93 differential diagnosis 93 esophageal dysphagia 92 95 etiology 92, 93 treatment 93 95 work-up 93 Aminosalicylates, pharmacokinetics and aging effects 36 Antibiotics diarrhea
Supplementary appendix
 Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Williams CM, Maher CG, Latimer J, et al. Efficacy
Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Williams CM, Maher CG, Latimer J, et al. Efficacy
Pediatric Abdomen Trauma
 Pediatric Abdomen Trauma Susan D. John, MD, FACR Pediatric Trauma Trauma is leading cause of death and disability in children and adolescents Causes and effects vary between age groups Blunt trauma predominates
Pediatric Abdomen Trauma Susan D. John, MD, FACR Pediatric Trauma Trauma is leading cause of death and disability in children and adolescents Causes and effects vary between age groups Blunt trauma predominates
9/21/15. Joshua Pruitt, MD, FAAEM Medical Director, LifeGuard Air Ambulance Iowa PA Society Fall CME Conference September 29, 2015
 Unless they prove otherwise. ~Every ED attending ever Joshua Pruitt, MD, FAAEM Medical Director, LifeGuard Air Ambulance Iowa PA Society Fall CME Conference September 29, 2015 AAA with rupture Mesenteric
Unless they prove otherwise. ~Every ED attending ever Joshua Pruitt, MD, FAAEM Medical Director, LifeGuard Air Ambulance Iowa PA Society Fall CME Conference September 29, 2015 AAA with rupture Mesenteric
58 year old male complaining of 3-week history of increasing epigastric pain
 Peptic Ulcer Disease 58 year old male complaining of 3-week history of increasing epigastric pain Has had dyspepsia in the past for which he took Tums, but this is much worse and only partially relieved
Peptic Ulcer Disease 58 year old male complaining of 3-week history of increasing epigastric pain Has had dyspepsia in the past for which he took Tums, but this is much worse and only partially relieved
Back to Basics: What Imaging Test should I order? Jeanne G. Hill, M.D. Pediatric Radiology Medical University of South Carolina
 Back to Basics: What Imaging Test should I order? Jeanne G. Hill, M.D. Pediatric Radiology Medical University of South Carolina Disclosure Neither I nor any member of my immediate family has a relevant
Back to Basics: What Imaging Test should I order? Jeanne G. Hill, M.D. Pediatric Radiology Medical University of South Carolina Disclosure Neither I nor any member of my immediate family has a relevant