Orthodontic cases involving the extraction
|
|
|
- Piers Watts
- 6 years ago
- Views:
Transcription
1 SPECIAL ARTICLE For four sixes Paul Jonathan Sandler, BDS(Hons), MSc, FDSRCPS, DOrth, MOrth, a Robert Atkinson, BDS(Hons), LDSRCS, FDSRCS, b and Alison Margaret Murray, BDS, MSc, FDSRCPS, DOrth, MOrth c Chesterfield, UK This article reviews the literature on orthodontic treatment involving extraction of first molars and highlights many of the clinical considerations when treating such cases. Case reports illustrate the potential problems and indicate some solutions. (Am J Orthod Dentofacial Orthop 2000;117:418-34) Orthodontic cases involving the extraction of permanent first molars are thought to be technically more difficult to treat and that even a good result is in some way a compromise. Many cases that would benefit from this approach because of the doubtful long-term prognosis of the molars are treated with the extraction of healthy premolars (Fig 1). The avoidance of first molar cases may be due to a number of factors including the following: operator comfort with premolar extraction cases, lack of experience in handling molar extraction cases, and the inter-dependence for patients between endodontists, orthodontists, and crown and bridge specialists. This last factor is rarely an issue in the United Kingdom but may increase in the future as Specialist Registration has in 1998 become a reality. The extraction of first permanent molar teeth accounts for a considerable proportion of cases treated within the National Health Service. An analysis of patients referred to consultant orthodontists found that nearly 12% of all extraction cases involved first permanent molars. 1 The aim of this article is to discuss a rationale for extraction of first molars and to highlight some of the problems and pitfalls that surround provision of appliance therapy for these cases. LITERATURE REVIEW Approaches to first molar extraction cases range between unbridled enthusiasm claiming that the extraction of all 4 first permanent molar teeth at the age of years prevented not only malocclusion but also dental decay and pyorrhea 2 to total skepticism suggesting that significant occlusal disturbance, an increase in caries, and detrimental change in facial contour and appearance were all inevitable as a result of this intervention. 3 a Consultant Orthodontist, Royal Hospital Chesterfield. b Senior House Officer, Royal Hospital Chesterfield. c Consultant Orthodontist, Derbyshire Royal Infirmary. Reprint requests to: Paul Jonathan Sandler, BDS (Hons), MSc, FDSRCPS, DOrth, MOrth, Consultant Orthodontist, Royal Hospital Chesterfield, Calow, Chesterfield, S44 5BL United Kingdom; , JonSandler@aol.com. Copyright 1999 by the American Association of Orthodontists /99/$ /1/97617 doi /mod First permanent molar extractions doubling the treatment time and halving the prognosis was the phrase coined by Mills. 4 This statement may have been correct when orthodontics involved removable appliances but now has little relevance. On the other hand, Daugaard-Jensen 5 suggested that first molar cases are no more time consuming than 4 premolar cases and in many cases offer distinct advantages in terms of anchorage management. Houston et al 6 suggested that children undergoing first permanent molar extractions often had a deprived social background and that they showed a reduced interest in their dental care. This often presented difficulties in providing anything other than the most basic of orthodontic treatment thus inevitably leading to an orthodontic compromise. Space closure after the extraction of the first permanent molar teeth has been studied in some detail and has led to conclusions that satisfactory closure of spaces was best achieved on children and young adults. 7 Adults showed less bone apposition when moving second molar teeth into the narrowed space, and poor maintenance of the closed space and, in some cases, resorption of the second molar roots was also noted. Other authors 8 concluded that significant if not always complete closure could be achieved with the roots of the second molar teeth moving almost twice as far as the crowns. They agreed that most cases showed a crestal bone loss mesial to the second molars posttreatment but suggested that root resorption of the second molars was only minimal. Extraction of unopposed maxillary first permanent molars after the removal of the mandibular counterpart was thought to prevent the likely over eruption of the maxillary tooth. 9 Compensating extractions were not automatically advised after the loss of the maxillary first permanent molar because space closure in the mandibular arch was more problematic. The effect of various extraction patterns on provision of space both anteriorly and posteriorly within the arches was discussed in some detail by Williams and Hosila. 10 They highlighted the fact that first molar extraction cases are likely to have less effect on the profile than premolar 418







2 American Journal of Orthodontics and Dentofacial Orthopedics Sandler, Atkinson, and Murray 419 Volume 117, Number 4 Fig 1. Premolars extracted despite limited prognosis of first molars. Fig 2. Gentle forces essential regardless of the method of space closure. Fig 4. Upper second molars almost completely replace first molars regardless of timing of extraction. Fig 3. Nance button palatal arch will maximize intraoral anchorage. extraction cases. Also in their cases involving first molar extractions there was about a 90% chance of successful third molar eruption compared with approximately 55% chance with cases involving premolar extractions. CLINICAL INDICATIONS There are many clinical situations in which extraction of first permanent molars should at least be considered and these can be summarized as follows: Fig 5. Timing of lower first molar extraction is important if spontaneous space closure is desired.





3 420 Sandler, Atkinson, and Murray American Journal of Orthodontics and Dentofacial Orthopedics April 2000 Fig 7. Stainless steel tubing prevents arch wire distortion and movement. Fig 6. Class 2 elastics to lingual of lower molars to counter lingual roll. Extensively carious first molars Hypoplastic first molars Heavily filled first molars where premolars are perfectly healthy Apical pathoses or root treated first molars Crowding at the distal part of the arches and wisdom teeth reasonably positioned High maxillary/mandibular planes angle Anterior open bite cases Whether first molars are extracted is dependent on many factors, including the patient s attitude to fixed appliance therapy, the standard of oral hygiene, the amount and site of crowding, and the presence or absence of other permanent teeth. The patients suitability for this invariably lengthy course of fixed appliance therapy must be considered to ensure that the benefits of treatment far outweigh the potential risks. POTENTIAL PROBLEMS Lower Arch Space Closure Space closure is perhaps the most challenging aspect of first molar extraction cases. When the lower second molars are subjected to a mesially directed force, there is always a tendency for them to both tilt mesially and roll lingually. This tendency can be reduced by the use of full size (19/25) Fig 8. Distal twister aids turning in of arch wires stainless steel arch wires. Active space closure should rarely be attempted before the patient has full alignment of all the lower teeth and is in this full-sized working arch wire. The new McLaughlin, Bennett, Trevisi, (3M Unitek; Monravia, Calif) prescription should help the molar position during space closure in that they are specifically designed to reduce molar lingual roll considerably. The second molar prescription has 10 lingual crown torque, which is some 20 to 25 less torque than other popular prescriptions. When using either traction ligatures or nickel titanium coil springs, space closing forces should always


.")




4 American Journal of Orthodontics and Dentofacial Orthopedics Sandler, Atkinson, and Murray 421 Volume 117, Number 4 Fig 9. Pretreatment records of case 1. be gentle, which should once again minimize undesirable side effects (Fig 2). In many first molar cases the total treatment time is determined by the time taken to bring the lower second molars in a good relationship with the lower second premolars. Upper Arch Space Closure Closure of the upper first molar extraction spaces is rarely time consuming. Indeed, because space closure occurs so readily, the extraction of upper first molars

. This should provide several extra millimeters of space on either side of the arch compared with cases where anchorage was not reinforced.")


.")

5 422 Sandler, Atkinson, and Murray American Journal of Orthodontics and Dentofacial Orthopedics April 2000 Fig 9. Con d often does not provide much more than a few millimeters either side of the arch to relieve anterior crowding or to correct an increased overjet. If a reasonable amount of the extraction space is required, consideration should be given to provision of a palatal arch with Nance button on the second molars (Fig 3). This should provide several extra millimeters of space on either side of the arch compared with cases where anchorage was not reinforced. If all the first molar space is required either for relief of crowding or overjet reduction, headgear must be provided to the upper second molars to prevent them moving mesially. In these cases, the patient s compliance with headgear will determine the ultimate success or failure of treatment. This must be borne in mind when carrying out the formal space analysis; if much more than 8 mm of space is required on either side, some other approach to treatment may need to be considered. Timing of Extractions If the upper second molars are unerupted at the time of extraction of the upper first molars, they will almost completely replace them, thus contributing little space for correction of the malocclusion (Fig 4). It has been suggested that effective distalization of upper premolars with a removable appliance can be achieved if the first molars are extracted early. 11 This method, however, depends totally on superb patient cooperation with the patient wearing the headgear for at least 12 to Fig 10. Power chain to move the canine occlusally. 14 hours per day. Anything short of this and most if not all the space provided by the extractions will be lost. If there is a space requirement in the upper arch therefore, extraction of the first molars must be delayed until the second molars have erupted sufficiently to





6 American Journal of Orthodontics and Dentofacial Orthopedics Sandler, Atkinson, and Murray 423 Volume 117, Number 4 Fig /25 stainless steel working arch wires. allow a palatal arch with Nance button or headgear to be placed. With modern medicaments and pulp management techniques, it should be possible to delay extractions and keep first molars in almost every case that will direct the second molars into their normal position. This will subsequently provide useful space after extraction of the first molars. If space requirement in the upper arch is minimal, earlier extraction will allow nature to assist with much of the space closure. The second molars are often quite high and only need to alter their eruption pathway slightly more mesially to allow them to erupt almost into the first molar sockets. In the lower arch, timing of extractions is also critical. It is unlikely that the lower second molars will completely replace the lower first molars after their extraction as they have a much more vertical path of eruption. If little or no space is required in the lower arch for correction of the malocclusion, it is often advisable to extract lower first molars early, when the bifurcation dentine on second molars is calcifying and the roots are about half formed. This will maximize spontaneous space closure in the lower arch thus minimizing retraction of the lower labial segment, which is an undesirable side effect often seen during space closure (Fig 5). If, after space analysis, it is calculated that all the lower first molar space is required for relief of crowding, a lingual arch may be necessary until the premolars and canines have been retracted sufficiently to allow incisor alignment. Root Paralleling Toward the end of treatment, if there is any doubt whether root positions exist, an Orthopantomogram can be taken to assess whether the long axis second premolars and second molars are reasonably parallel. If 8 to 9 mm of space has been closed between the second premolar and second molar, there is always a slight tendency for divergence between the two roots and gentle tip back bends may be placed if necessary in the final rectangular wires to fully correct the root positions. Once space is closed and the crowns are correctly positioned, a dead ligature should be placed across the extraction spaces to hold them closed for a few months. This keeps these teeth in position while the gingival fibers reorganize and the bone around the teeth matures in the hope that this will minimize any tendency for the extraction spaces to reopen. Class II Elastics If Class II elastics are being used in first molar extraction cases, there is an increased tendency for lingual roll of the lower second permanent molars. Class II elastics should not be used until the patient is in a full-sized (19/25) stainless steel arch wire and, if necessary, buccal crown torque is applied to the lower molars. Another possibility is to run the Class II elastics from a lingual cleat on the lower molar bands, thus providing some lift to the lingual surface of the lower molars thus reducing any tendency to lingual roll (Fig 6).







7 424 Sandler, Atkinson, and Murray American Journal of Orthodontics and Dentofacial Orthopedics April 2000 Arch Wire Problems Fig 12. Final records of case 1.





.")

8 American Journal of Orthodontics and Dentofacial Orthopedics Sandler, Atkinson, and Murray 425 Volume 117, Number 4 Fig 12. Con d Fig 13. Pretreatment records of case 2. Arch Wire Problems The long span of arch wire between the second premolar and the second molar can lead to problems such as trauma to the soft tissues as well as deflection of the arch wire during mastication. This arch wire distortion can, on occasion, cause movement leading to the wire coming forward out of one tube and moving distally and piercing the cheek on the opposite side. Introduction of deflections and asymmetries into the arch will at the very least delay progression of treatment. The above consequences can all be avoided by placing 0.9 mm internal diameter stainless steel tubing over the arch wire in the extraction space. The tube should be only 1 to 2 mm short of the interbracket span for maximum rigidity of the arch wire section but also allowing some alignment and movement of the teeth (Fig 7). In addition, the arch wires up to but excluding the fullsized rectangular stainless steel should be annealed and turned down or in at the end. An instrument called a distal twister (Instrument number , American Orthodontics, Sheboygan, Wis), which hooks over the annealed end of the wire, allows this to be done with ease (Fig 8).








9 426 Sandler, Atkinson, and Murray American Journal of Orthodontics and Dentofacial Orthopedics April 2000 Fig 13. Con d



.")



10 American Journal of Orthodontics and Dentofacial Orthopedics Sandler, Atkinson, and Murray 427 Volume 117, Number 4 Fig 14. Stainless steel tubing to protect the arch wire Fig /25 stainless steel working arch wires, spaces almost completely closed, Class II elastics for lateral open bite. CASE REPORTS These cases are used to illustrate the kind of result that can be expected with careful case management after extraction of 4 first molars. Case Report 1 The patient presented at 12 years of age 11 with a Class II Division II incisor relationship on a skeletal I base. There was severe crowding in the upper labial segment with almost complete exclusion of the upper right canine and partial exclusion of the upper left canine. The lower buccal segments were moderately crowded. Dental examination revealed caries in 3 of the 4 first molar teeth and an OPT radiograph showed the presence of third molars (Fig 9). As the first molars were carious we decided to extract them. Careful anchorage management should allow sufficient space for relief of crowding, alignment of the labial segment teeth, and full correction of the malocclusion. We placed fixed appliances in January 1995 and progressed from nickel titanium through to 18/25 nickel titanium to 19/25 steel. Full-sized stainless steel arch wires were in place by the middle of 1995 at which stage push coil was used to reopen space for the upper right canine. We did not attempt space closure on the arch wires before the 19/25 stainless steel arch wires to minimize dumping or arch distortion in the extraction areas. Lengths of 0.9 mm internal diameter stainless steel tubing were used in the extraction sites on both of the aligning arch wires to make the arch wire more rigid thus preventing distortion during mastication. To aid correction of the upper right canine, a crimpable hook was placed on the arch wire in an inverted position and elastic chain attached to it from the bracket on the canine (Fig 10). Once the anterior teeth had been fully aligned onto the 19/25 arch wire, space closure was commenced. Traction ligatures were used in all 4 quadrants and renewed every 6 weeks until full space closure was achieved (Fig 11). We removed the stainless steel arch




.")
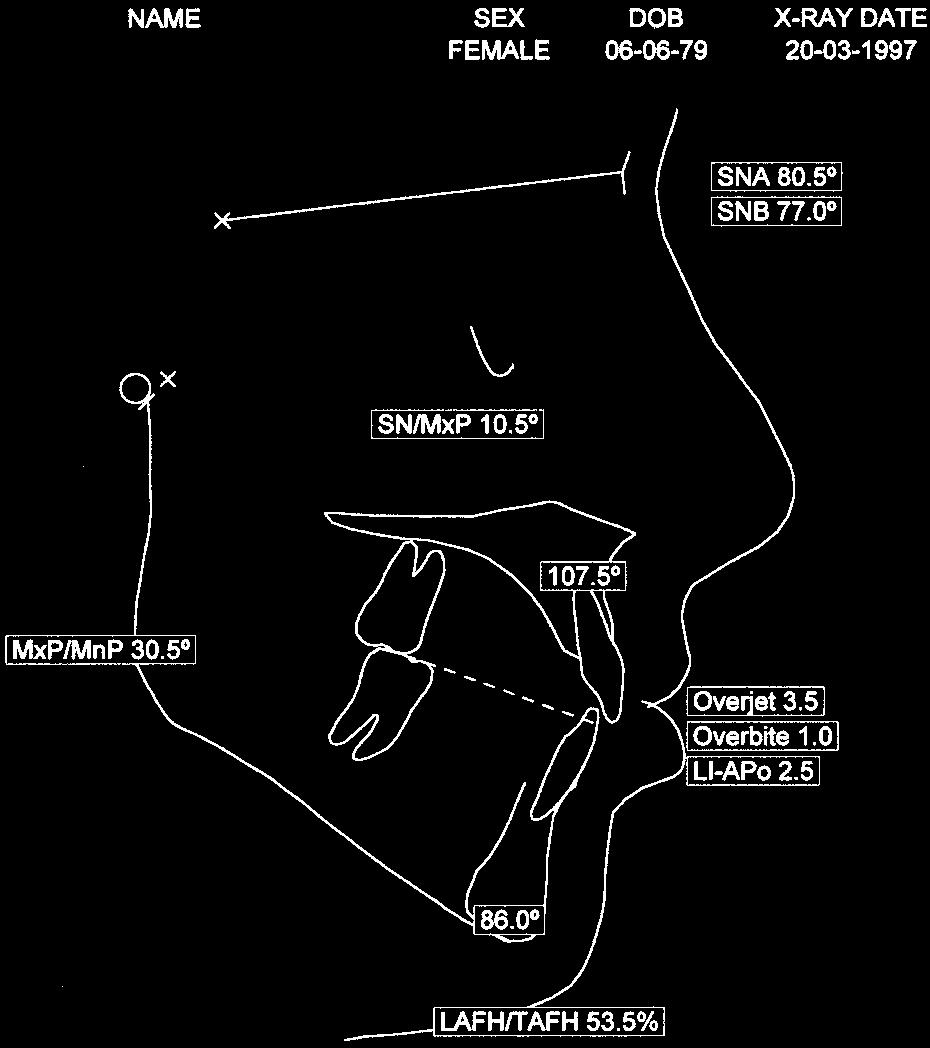
11 428 Sandler, Atkinson, and Murray American Journal of Orthodontics and Dentofacial Orthopedics April 2000 Fig stainless finishing wires for fine detailing of tooth position. wires every second visit to check arch wire coordination and to place gentle reverse curve in the lower arch and increased curve in the upper arch. We removed the appliances in August 1996, therefore, the total duration of active treatment to fully correct this malocclusion was 19 months (Fig 12). Cephalometric analysis revealed a small favorable change in the sagittal relationship of the jaws as a result of the 1 decrease in SNA and 1 increase in SNB. There was a small decrease in the maxillary-mandibular planes angle during treatment and superimposition demonstrates some forward mandibular growth that is most welcome. There was marked improvement in the inclinations of the incisors with a concomitant improvement in the interincisal angle. The OPT radiograph taken 12 months after treatment showed a marked improvement in the position of the third molars that are expected to erupt into a more than acceptable position over the next few years. Case Report 2 The patient presented at 14 years of age in full permanent dentition with a Class III incisor relationship on a Class I skeletal base. There was moderate crowding of the upper labial segment and mild to moderate crowding of the lower labial segment. The lower first molars had been restored, and the OPT revealed the presence and good morphologic characteristics of third molars (Fig 13). We decided that extraction of first molars would provide sufficient room for correction of the malocclusion and would also leave the patient with a completely healthy dentition. Flexible nickel titanium arch wires were used to provide initial alignment of the anterior teeth with the exception of the upper left lateral incisor. Stainless steel tubing protected the wire in the extraction spaces during this alignment phase (Fig 14). We progressed to an upper 19/25 stainless steel arch wire, then a nickel titanium pushcoil was used to reopen space for the upper lateral incisors. Vertical box elastics with a slight Class II element were used in the buccal segments on a 19/25 upper and 18/25 nickel titanium lower arch wire to encourage closure of the lateral open bites that developed during the course of treatment (Fig 15). Full space closure was achieved on 19/25 stainless steel arch wires. For the last 3 months of treatment, a high tensile stainless steel wire was used to allow final positioning of the teeth (Fig 16). The overjet, overbite, and buccal segment relationship was corrected in a period of 28 months (Fig 17). Cephalometric analysis revealed a small change in the sagittal relationship of the jaws, but the maxillarymandibular planes angle appeared not to change as a result of treatment. Superimposition demonstrated a counter-clockwise mandibular rotation largely due to the inherited growth pattern but also as a consequence of the extrusive nature of the orthodontic treatment. The upper incisors ended up 3 retroclined compared with the start and the lower incisors nearly 3 more proclined although not as far ahead of APo. The third molars are in an excellent position posttreatment and are expected to erupt normally in the near future. Case Report 3 This young man presented at 11 years of age with a Class III incisor relationship on a Class III skeletal base with a markedly increased mandibular planes





12 American Journal of Orthodontics and Dentofacial Orthopedics Sandler, Atkinson, and Murray 429 Volume 117, Number 4 Fig 17. Final records of case 2.








13 430 Sandler, Atkinson, and Murray American Journal of Orthodontics and Dentofacial Orthopedics April 2000 Fig 17. Con d Fig 18. Pretreatment views of case 3.




.")




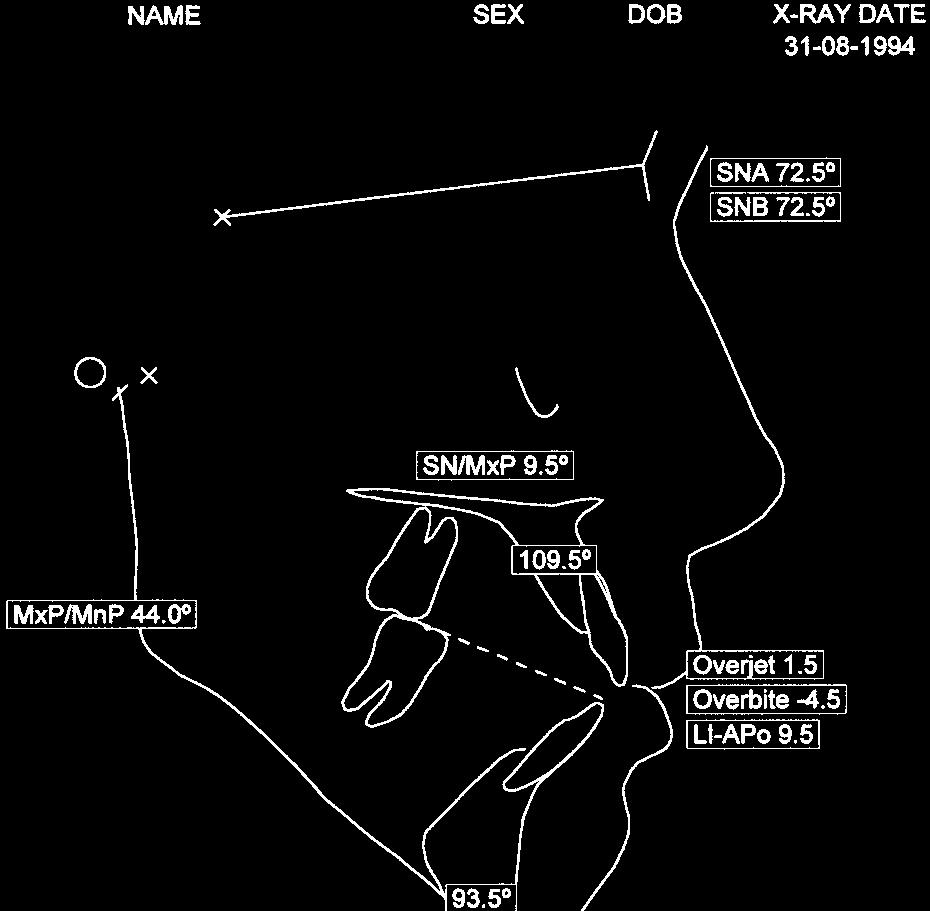
14 American Journal of Orthodontics and Dentofacial Orthopedics Sandler, Atkinson, and Murray 431 Volume 117, Number 4 Fig 18. Con d. Fig nickel titanium for initial alignment, tubing to protect arch wire. angle of 44. He was in the permanent dentition with a normally inclined upper labial segment, a proclined lower labial segment, and an anterior open bite of 3 mm. The upper and lower right first molars were very heavily filled, and the lower left first molar was very heavily decayed (Fig 18). We appreciated that this young man would be a difficult case to treat and that the prognosis for successful closure of the anterior open bite was limited with orthodontics alone. However, the patient was not interested in considering any form of orthognathic surgery. A decision was made to attempt to get as much correction as possible with orthodontic therapy alone. We felt that posterior extractions may help with closure of the anterior open bite and that in this high angle case space closure was unlikely to be a major problem. We decided that the patient would benefit from the removal of all 4 first molars to relieve the crowding in the upper labial segment and to improve the interarch relationships.

 and 18/25 nickel titanium arch wires (Fig 20) as cooperation with treatment was not really forthcoming, and the patient had 17 breakages repaired")

, we finally removed the appliances in July 1997.")

. Essix upper and lower retainers were used, and the overbite correction will be monitored over the next few years.")


15 432 Sandler, Atkinson, and Murray American Journal of Orthodontics and Dentofacial Orthopedics April 2000 Fig 20. Second stage alignment with 18/25 nickel titanium. Fig /25 stainless steel working arch wires to achieve space closure. We placed the appliances in December 1994 (Fig 19). We made very slow progress through flexible (0.016) and 18/25 nickel titanium arch wires (Fig 20) as cooperation with treatment was not really forthcoming, and the patient had 17 breakages repaired during his course of treatment. We finally progressed up to 19/25 stainless steel. At each appointment chlorhexidine varnish was applied to the upper incisor brackets in the hope that this would reduce enamel damage during treatment (Fig 21). Elastic traction ligatures were regularly replaced and space closure eventually achieved. After 1 visit in stainless steel finishing wires to finalize tooth positions (Fig 22), we finally removed the appliances in July Active treatment time for correction of the malocclusion was years. We felt that this was acceptable in view of the number of breakages and the many failed appointments. Final intraoral photographs show reasonable buccal segment interdigitation, correction of the labial segments and correction of the anterior open bite (Fig 23). Essix upper and lower retainers were used, and the overbite correction will be monitored over the next few years. Near the end of treatment, cephalometric analysis shows slight retroclination of the upper labial segment and retroclination of the previously proclined lower labial segment that was necessary to close the anterior open bite. The mandibular planes angle did not increase during treatment although the lower anterior facial height proportion increased slightly. Superimposition shows closure of the anterior open bite and a moderate change in the jaw positions, which is largely in a vertical direction. An OPT radiograph taken 2 months before debonding shows good root paralleling and some slight root resorption on the distal root of both lower second molars. The treatment had been unnecessarily prolonged as a result of the poor patient cooperation, and this will have contributed to the root resorption. The upper second molars were in a reasonable position to the upper second premolars and there should now be sufficient room for the third molars to erupt into the mouth. SUMMARY Even with careful planning and execution of treatment any orthodontic case involving the extraction of first






16 American Journal of Orthodontics and Dentofacial Orthopedics Sandler, Atkinson, and Murray 433 Volume 117, Number 4 Fig 22. Finishing on stainless steel, near end of treatment radiographs.









17 434 Sandler, Atkinson, and Murray American Journal of Orthodontics and Dentofacial Orthopedics April 2000 Fig 23. Final photos of case 3. molars will almost certainly take between 6 and 9 months longer than an equivalent case in which 4 premolars are extracted. Careful case assessment must be undertaken before treatment to ensure that the benefits of treatment will outweigh any potential disadvantages of this extended treatment. A knowledge of the potential problems with first molar cases will allow the necessary action to be taken before many of these problems arise. REFERENCES 1. Bradbury AJ. A current view on patterns of extraction therapy in British health service orthodontics. Br Dent J 1985;159: Wilkinson AA. The first permanent molar again. Br Dent J 1940;8: Salzmann JA. A study of orthodontic and facial changes and effects on dentition attending the loss of first molars in five hundred adults. J Am Dent Assoc 1938;25: Mills JRE. Principles and practice of orthodontics, 2nd edition, New York: Churchill Livingstone; p Daugaard-Jensen I. Extraction of first molars in discrepancy cases. Am J Orthod 1973;64: Houston WJB, Stephens CD, Tulley WJ. A textbook of orthodontics, 2nd edition, Oxford: John Wright; p Stepovich ML. A clinical study on closing edentulous spaces in the mandible. Angle Orthod 1979;49: Hom BM, Turley PK. The effects of space closure of the mandibular first molar area in adults. Am J Orthod 1984;4: Mitchell L. An introduction to orthodontics, Oxford, England: Oxford University Press; p Williams R, Hosila L. The effect of different extraction sites upon incisor retraction. Am J Orthod 1976;69: Orton H, Carter NE. Initial management of first molar extraction cases. J Clin Orthod 1988;22:230-8.
Extractions of first permanent molars in orthodontics: Treatment planning, technical considerations and two clinical case reports
 Case Report 41 Extractions of first permanent molars in orthodontics: Treatment planning, technical considerations and two clinical case reports Ashok Surana a, Siddhartha Dhar b, SurajitChakrabarty c,
Case Report 41 Extractions of first permanent molars in orthodontics: Treatment planning, technical considerations and two clinical case reports Ashok Surana a, Siddhartha Dhar b, SurajitChakrabarty c,
Dr Robert Drummond. BChD, DipOdont Ortho, MChD(Ortho), FDC(SA) Ortho. Canad Inn Polo Park Winnipeg 2015
, FDC(SA) Ortho. Canad Inn Polo Park Winnipeg 2015") Dr Robert Drummond BChD, DipOdont Ortho, MChD(Ortho), FDC(SA) Ortho Canad Inn Polo Park Winnipeg 2015 Severely compromised FPM with poor prognosis Children often present with a developing dentition affected
Dr Robert Drummond BChD, DipOdont Ortho, MChD(Ortho), FDC(SA) Ortho Canad Inn Polo Park Winnipeg 2015 Severely compromised FPM with poor prognosis Children often present with a developing dentition affected
The Modified Twin Block Appliance in the Treatment of Class II Division 2 Malocclusions
 Journal of Orthodontics/Vol. 28/2001/271 280 The Modified Twin Block Appliance in the Treatment of Class II Division 2 Malocclusions F. M. V. DYER H. F. MCKEOWN P. J. SANDLER Department of Orthodontics,
Journal of Orthodontics/Vol. 28/2001/271 280 The Modified Twin Block Appliance in the Treatment of Class II Division 2 Malocclusions F. M. V. DYER H. F. MCKEOWN P. J. SANDLER Department of Orthodontics,
Treatment Planning for the Loss of First Permanent Molars D.S. GILL, R.T. LEE AND C.J. TREDWIN
 O R T H O D O N T I C S Treatment Planning for the Loss of First Permanent Molars D.S. GILL, R.T. LEE AND C.J. TREDWIN Abstract: During the mixed-dentition stage of dental development, dentists may encounter
O R T H O D O N T I C S Treatment Planning for the Loss of First Permanent Molars D.S. GILL, R.T. LEE AND C.J. TREDWIN Abstract: During the mixed-dentition stage of dental development, dentists may encounter
The Tip-Edge appliance and
 Figure 1: Internal surfaces of the edgewise archwire slot are modified to create the Tip-Edge archwire slot. Tipping surfaces (T) limit crown tipping during retraction. Uprighting surfaces (U) control
Figure 1: Internal surfaces of the edgewise archwire slot are modified to create the Tip-Edge archwire slot. Tipping surfaces (T) limit crown tipping during retraction. Uprighting surfaces (U) control
Gentle-Jumper- Non-compliance Class II corrector
 15 CASE REPORT Gentle-Jumper- Non-compliance Class II corrector Amit Prakash 1,O.P.Mehta 2, Kshitij Gupta 3 Swapnil Pandey 4 Deep Kumar Suryawanshi 4 1 Senior lecturer Bhopal - INDIA 2 Professor Bhopal
15 CASE REPORT Gentle-Jumper- Non-compliance Class II corrector Amit Prakash 1,O.P.Mehta 2, Kshitij Gupta 3 Swapnil Pandey 4 Deep Kumar Suryawanshi 4 1 Senior lecturer Bhopal - INDIA 2 Professor Bhopal
Class II Correction using Combined Twin Block and Fixed Orthodontic Appliances: A Case Report
 Case Report Print ISSN: 2321-6379 Online ISSN: 2321-595X DOI: 10.17354/ijss/2017/506 Class II Correction using Combined Twin Block and Fixed Orthodontic Appliances: A Case Report Ahmed Alassiry Assistant
Case Report Print ISSN: 2321-6379 Online ISSN: 2321-595X DOI: 10.17354/ijss/2017/506 Class II Correction using Combined Twin Block and Fixed Orthodontic Appliances: A Case Report Ahmed Alassiry Assistant
Case Report: Long-Term Outcome of Class II Division 1 Malocclusion Treated with Rapid Palatal Expansion and Cervical Traction
 Case Report Case Report: Long-Term Outcome of Class II Division 1 Malocclusion Treated with Rapid Palatal Expansion and Cervical Traction Roberto M. A. Lima, DDS a ; Anna Leticia Lima, DDS b Abstract:
Case Report Case Report: Long-Term Outcome of Class II Division 1 Malocclusion Treated with Rapid Palatal Expansion and Cervical Traction Roberto M. A. Lima, DDS a ; Anna Leticia Lima, DDS b Abstract:
Correction of Crowding using Conservative Treatment Approach
 Case Report Correction of Crowding using Conservative Treatment Approach Dr Tapan Shah, 1 Dr Tarulatha Shyagali, 2 Dr Kalyani Trivedi 3 1 Senior Lecturer, 2 Professor, Department of Orthodontics, Darshan
Case Report Correction of Crowding using Conservative Treatment Approach Dr Tapan Shah, 1 Dr Tarulatha Shyagali, 2 Dr Kalyani Trivedi 3 1 Senior Lecturer, 2 Professor, Department of Orthodontics, Darshan
Hypodontia is the developmental absence of at
 CASE REPORT Orthodontic treatment for a patient with hypodontia involving the maxillary lateral incisors Saud A. Al-Anezi Kuwait City, Kuwait Developmental absence of maxillary lateral incisors is not
CASE REPORT Orthodontic treatment for a patient with hypodontia involving the maxillary lateral incisors Saud A. Al-Anezi Kuwait City, Kuwait Developmental absence of maxillary lateral incisors is not
Experience with Contemporary Tip-Edge plus Technique A Case Report.
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861. Volume 13, Issue 3 Ver. I. (Mar. 2014), PP 12-17 Experience with Contemporary Tip-Edge plus Technique A Case
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861. Volume 13, Issue 3 Ver. I. (Mar. 2014), PP 12-17 Experience with Contemporary Tip-Edge plus Technique A Case
A Modified Three-piece Base Arch for en masse Retraction and Intrusion in a Class II Division 1 Subdivision Case
 Dhaval Ranjitbhai Lekhadia, Gautham Hegde RESEARCH ARTICLE 10.5005/jp-journals-10029-1149 A Modified Three-piece Base Arch for en masse Retraction and Intrusion in a Class II Division 1 Subdivision Case
Dhaval Ranjitbhai Lekhadia, Gautham Hegde RESEARCH ARTICLE 10.5005/jp-journals-10029-1149 A Modified Three-piece Base Arch for en masse Retraction and Intrusion in a Class II Division 1 Subdivision Case
EUROPEAN SOCIETY OF LINGUAL ORTHODONTISTS
 EUROPEAN SOCIETY OF LINGUAL ORTHODONTISTS CANDIDATE NUMBER:44 CASE NUMBER: 2 Year: 2010 ESLO 01 RÉSUMÉ OF CASE 5 CASE CATEGORY: CLASS II DIVISION 1 MALOCCLUSION A MALOCCLUSION WITH SIGNIFICANT MANDIBULAR
EUROPEAN SOCIETY OF LINGUAL ORTHODONTISTS CANDIDATE NUMBER:44 CASE NUMBER: 2 Year: 2010 ESLO 01 RÉSUMÉ OF CASE 5 CASE CATEGORY: CLASS II DIVISION 1 MALOCCLUSION A MALOCCLUSION WITH SIGNIFICANT MANDIBULAR
Use of a Tip-Edge Stage-1 Wire to Enhance Vertical Control During Straight Wire Treatment: Two Case Reports
 Case Report Use of a Tip-Edge Stage-1 Wire to Enhance Vertical Control During Straight Wire Treatment: Two Case Reports Helen Taylor, BDS, MScD, DOrth, MOrth, FDSRCS(Eng) a Abstract: Vertical control is
Case Report Use of a Tip-Edge Stage-1 Wire to Enhance Vertical Control During Straight Wire Treatment: Two Case Reports Helen Taylor, BDS, MScD, DOrth, MOrth, FDSRCS(Eng) a Abstract: Vertical control is
The Tip-Edge Concept: Eliminating Unnecessary Anchorage Strain
 Welcome Ron Not Ron? Click here. My Account The Tip-Edge Concept: Eliminating Unnecessary Anchorage Strain VOLUME 26 : NUMBER 03 : PAGES (165-178) 1992 CHRISTOPHER K. KESLING, DDS, MS Tooth movement in
Welcome Ron Not Ron? Click here. My Account The Tip-Edge Concept: Eliminating Unnecessary Anchorage Strain VOLUME 26 : NUMBER 03 : PAGES (165-178) 1992 CHRISTOPHER K. KESLING, DDS, MS Tooth movement in
ORTHODONTICS Treatment of malocclusion Assist.Lec.Kasem A.Abeas University of Babylon Faculty of Dentistry 5 th stage
 Lec: Treatment of class I malocclusion Class I occlusion can be defined by Angles, classification as the mesiobuccal cusp of the upper 1 st permanent molar occlude with the developmental groove of the
Lec: Treatment of class I malocclusion Class I occlusion can be defined by Angles, classification as the mesiobuccal cusp of the upper 1 st permanent molar occlude with the developmental groove of the
ORTHOdontics SLIDING MECHANICS
 ORTHOdontics PGI/II SLIDING MECHANICS FOCUS ON TARGETED SPACE GAINING AND ITS APPLICATIONS, INCLUDING WITH RAPID PALATAL EXPANDIONS. ALSO INCLUDES RETENTION AND CLINICAL PEARLS FACULTY: Joseph Ghafari,
ORTHOdontics PGI/II SLIDING MECHANICS FOCUS ON TARGETED SPACE GAINING AND ITS APPLICATIONS, INCLUDING WITH RAPID PALATAL EXPANDIONS. ALSO INCLUDES RETENTION AND CLINICAL PEARLS FACULTY: Joseph Ghafari,
System Orthodontic Treatment Program By Dr. Richard McLaughlin, Dr. John Bennett and Dr. Hugo Trevisi
 A Clinical Review of the MBT Versatile+ Appliance System Orthodontic Treatment Program By Dr. Richard McLaughlin, Dr. John Bennett and Dr. Hugo Trevisi Treatment Philosophy of the MBT Appliance System
A Clinical Review of the MBT Versatile+ Appliance System Orthodontic Treatment Program By Dr. Richard McLaughlin, Dr. John Bennett and Dr. Hugo Trevisi Treatment Philosophy of the MBT Appliance System
A New Fixed Interarch Device for Class II Correction
 A New Fixed Interarch Device for Class II Correction WILLIAM VOGT, DDS Fixed devices are increasingly being used for molar distalization in Class II treatment because they eliminate the need for special
A New Fixed Interarch Device for Class II Correction WILLIAM VOGT, DDS Fixed devices are increasingly being used for molar distalization in Class II treatment because they eliminate the need for special
6. Timing for orthodontic force
 6. Timing for orthodontic force Orthodontic force is generally less than 300gm, so early mechanical stability is enough for immediate orthodontic force. There is no actually difference in success rate
6. Timing for orthodontic force Orthodontic force is generally less than 300gm, so early mechanical stability is enough for immediate orthodontic force. There is no actually difference in success rate
Keeping all these knowledge in mind I will show you 3 cases treated with the Forsus appliance.
 Due to technical difficulties there were some audio problems with the webinar recording. Starting at 27:54, please use this guide to follow along with Dr. Kercelli s presentation. Keeping all these knowledge
Due to technical difficulties there were some audio problems with the webinar recording. Starting at 27:54, please use this guide to follow along with Dr. Kercelli s presentation. Keeping all these knowledge
The ASE Example Case Report 2010
 The ASE Example Case Report 2010 The Requirements for Case Presentation in The Angle Society of Europe are specified in the Appendix I to the Bylaws. This example case report exemplifies how these requirements
The ASE Example Case Report 2010 The Requirements for Case Presentation in The Angle Society of Europe are specified in the Appendix I to the Bylaws. This example case report exemplifies how these requirements
Unilateral Horizontally Impacted Maxillary Canine and First Premolar Treated with a Double Archwire Technique
 Case Report Unilateral Horizontally Impacted Maxillary Canine and First Premolar Treated with a Double Archwire Technique Chien-Lun Peng a ; Yu-Yu Su b ; Sheng-Yang Lee c Abstract: A patient with a unilateral
Case Report Unilateral Horizontally Impacted Maxillary Canine and First Premolar Treated with a Double Archwire Technique Chien-Lun Peng a ; Yu-Yu Su b ; Sheng-Yang Lee c Abstract: A patient with a unilateral
OF LINGUAL ORTHODONTICS
 EUROPEAN SOCIETY OF LINGUAL ORTHODONTICS CANDIDATE NUMBER: KDr. KP. kanarelis CASE NUMBER: 1 Year: 2010 WBLO 01 RESUME OF CASE 1 CASE CATEGORY: ADULT MALOCCLUSION NAME : IOANNIS.G BORN: 03.01.1989 SEX:
EUROPEAN SOCIETY OF LINGUAL ORTHODONTICS CANDIDATE NUMBER: KDr. KP. kanarelis CASE NUMBER: 1 Year: 2010 WBLO 01 RESUME OF CASE 1 CASE CATEGORY: ADULT MALOCCLUSION NAME : IOANNIS.G BORN: 03.01.1989 SEX:
The management of impacted
 Using a rigid hook and spring auxiliary slid onto the archwire to direct eruption of impacted teeth BY S. JAY BOWMAN, DMD, MSD, AND ALDO CARANO, DR ODONT, MS, SPEC ORTHOD Figure 1: A 12-year-old female
Using a rigid hook and spring auxiliary slid onto the archwire to direct eruption of impacted teeth BY S. JAY BOWMAN, DMD, MSD, AND ALDO CARANO, DR ODONT, MS, SPEC ORTHOD Figure 1: A 12-year-old female
Forsus Class II Correctors as an Effective and Efficient Form of Anchorage in Extraction Cases
 Forsus Class II Correctors as an Effective and Efficient Form of Anchorage in Extraction Cases by Lisa Alvetro, DDS, MSD After receiving her DDS summa cum laude from Ohio State University, Dr. Alvetro
Forsus Class II Correctors as an Effective and Efficient Form of Anchorage in Extraction Cases by Lisa Alvetro, DDS, MSD After receiving her DDS summa cum laude from Ohio State University, Dr. Alvetro
EUROPEAN SOCIETY OF LINGUAL ORTHODONTISTS
 EUROPEAN SOCIETY OF LINGUAL ORTHODONTISTS CANDIDATE NUMBER : 13 Dr. Masatoshi Sana CASE NUMBER : Year : ESLO 01 RÉSUMÉ OF CASE 2 CASE CATEGORY: CLASS I MALOCCLUSION NAME: BORN: SEX: Yukari K. 08/03/1979
EUROPEAN SOCIETY OF LINGUAL ORTHODONTISTS CANDIDATE NUMBER : 13 Dr. Masatoshi Sana CASE NUMBER : Year : ESLO 01 RÉSUMÉ OF CASE 2 CASE CATEGORY: CLASS I MALOCCLUSION NAME: BORN: SEX: Yukari K. 08/03/1979
Treatment of Class II, Division 2 Malocclusion with Miniscrew Supported En-Masse Retraction: Is Deepbite Really an Obstacle for Extraction Treatment?
 TURKISH JOURNAL of DOI: 10.5152/TurkJOrthod.2017.17034 CASE REPORT Treatment of Class II, Division 2 Malocclusion with Miniscrew Supported En-Masse Retraction: Is Deepbite Really an Obstacle for Extraction
TURKISH JOURNAL of DOI: 10.5152/TurkJOrthod.2017.17034 CASE REPORT Treatment of Class II, Division 2 Malocclusion with Miniscrew Supported En-Masse Retraction: Is Deepbite Really an Obstacle for Extraction
Angle Class II, division 2 malocclusion with deep overbite
 BBO Case Report Angle Class II, division 2 malocclusion with deep overbite Arno Locks 1 Angle Class II, division 2, malocclusion is characterized by a Class II molar relation associated with retroclined
BBO Case Report Angle Class II, division 2 malocclusion with deep overbite Arno Locks 1 Angle Class II, division 2, malocclusion is characterized by a Class II molar relation associated with retroclined
ISW for the treatment of adult anterior crossbite with severe crowding combined facial asymmetry case
 International Research Journal of Medicine and Biomedical Sciences Vol.3 (2),pp. 15-29, November 2018 Available online at http://www.journalissues.org/irjmbs/ https://doi.org/10.15739/irjmbs.18.004 Copyright
International Research Journal of Medicine and Biomedical Sciences Vol.3 (2),pp. 15-29, November 2018 Available online at http://www.journalissues.org/irjmbs/ https://doi.org/10.15739/irjmbs.18.004 Copyright
MBT System as the 3rd Generation Programmed and Preadjusted Appliance System (PPAS) by Masatada Koga, D.D.S., Ph.D
 by Masatada Koga, D.D.S., Ph.D") MBT System as the 3rd Generation Programmed and Preadjusted Appliance System (PPAS) by Masatada Koga, D.D.S., Ph.D Dr. Masatada Koga, D.D.S., Ph.D, is an assistant professor in the Department of Orthodontics
MBT System as the 3rd Generation Programmed and Preadjusted Appliance System (PPAS) by Masatada Koga, D.D.S., Ph.D Dr. Masatada Koga, D.D.S., Ph.D, is an assistant professor in the Department of Orthodontics
Significant improvement with limited orthodontics anterior crossbite in an adult patient
 VARIA Significant improvement with limited orthodontics anterior crossbite in an adult patient Arzu Ari-Demirkaya Istanbul, Turkey Summary Objectives. Orthodontic treatment is known to last as long as
VARIA Significant improvement with limited orthodontics anterior crossbite in an adult patient Arzu Ari-Demirkaya Istanbul, Turkey Summary Objectives. Orthodontic treatment is known to last as long as
EUROPEAN SOCIETY OF LINGUAL ORTHODONTICS
 EUROPEAN SOCIETY OF LINGUAL ORTHODONTICS CANDIDATE NUMBER: Dr. Stefan Blasius Year: 2010 WBLO 01 EUROPEAN SOCIETY OF LINGUAL ORTHODONTICS CANDIDATE NUMBER: Dr. Stefan Blasius Year: 2010 WBLO 01 RÉSUMÉ
EUROPEAN SOCIETY OF LINGUAL ORTHODONTICS CANDIDATE NUMBER: Dr. Stefan Blasius Year: 2010 WBLO 01 EUROPEAN SOCIETY OF LINGUAL ORTHODONTICS CANDIDATE NUMBER: Dr. Stefan Blasius Year: 2010 WBLO 01 RÉSUMÉ
Crowded Class II Division 2 Malocclusion
 Class II Division 2 Malocclusion Crowded Class II Division 2 Malocclusion Clinicians: Drs. Chris Chang, Hsin-Yin Yeh, Sophia Pei-Wen Shu, W. Eugene Roberts Patient: Miss Jhan Pre-treatment Diagnosis An
Class II Division 2 Malocclusion Crowded Class II Division 2 Malocclusion Clinicians: Drs. Chris Chang, Hsin-Yin Yeh, Sophia Pei-Wen Shu, W. Eugene Roberts Patient: Miss Jhan Pre-treatment Diagnosis An
THE MBT VERSATILE+ APPLIANCE SYSTEM
 THE MBT VERSATILE+ APPLIANCE SYSTEM McLaughlin, Bennett, Trevisi The MBT Versatile+ Appliance System THE DEVELOPMENT OF A TREATMENT MECHANICS AND APPLIANCE PHILOSOPHY The first fully programmed preadjusted
THE MBT VERSATILE+ APPLIANCE SYSTEM McLaughlin, Bennett, Trevisi The MBT Versatile+ Appliance System THE DEVELOPMENT OF A TREATMENT MECHANICS AND APPLIANCE PHILOSOPHY The first fully programmed preadjusted
ISW for the treatment of moderate crowding dentition with unilateral second molar impaction
 International Research Journal of Public and Environmental Health Vol.5 (6),pp. 90-103, September 2018 Available online at https://www.journalissues.org/irjpeh/ https://doi.org/10.15739/irjpeh.18.013 Copyright
International Research Journal of Public and Environmental Health Vol.5 (6),pp. 90-103, September 2018 Available online at https://www.journalissues.org/irjpeh/ https://doi.org/10.15739/irjpeh.18.013 Copyright
Nonsurgical Treatment of Adult Open Bite Using Edgewise Appliance Combined with High-Pull Headgear and Class III Elastics
 Case Report Nonsurgical Treatment of Adult Open Bite Using Edgewise Appliance Combined with High-Pull Headgear and Class III Elastics Isao Saito, DDS, PhD a ; Masaki Yamaki, DDS, PhD b ; Kooji Hanada,
Case Report Nonsurgical Treatment of Adult Open Bite Using Edgewise Appliance Combined with High-Pull Headgear and Class III Elastics Isao Saito, DDS, PhD a ; Masaki Yamaki, DDS, PhD b ; Kooji Hanada,
Non Extraction philosophy: Distalization using Jone s Jig appliance- a case report
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 13, Issue 9 Ver. IV (Sep. 2014), PP 36-41 Non Extraction philosophy: Distalization using Jone s Jig appliance-
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 13, Issue 9 Ver. IV (Sep. 2014), PP 36-41 Non Extraction philosophy: Distalization using Jone s Jig appliance-
ortho case report Sagittal First international magazine of orthodontics By Dr. Luis Carrière Special Reprint
 Cover image courtesy of K Line Europe GmbH (www.kline-europe.de) ortho Special Reprint international magazine of orthodontics 1 2017 case report Sagittal First By Dr. Luis Carrière Sagittal First Author:
Cover image courtesy of K Line Europe GmbH (www.kline-europe.de) ortho Special Reprint international magazine of orthodontics 1 2017 case report Sagittal First By Dr. Luis Carrière Sagittal First Author:
EUROPEAN SOCIETY OF LINGUAL ORTHODONTISTS
 EUROPEAN SOCIETY OF LINGUAL ORTHODONTISTS CANDIDATE NUMBER: 44 CASE NUMBER: 1 Year: ESLO 01 RÉSUMÉ OF CASE 1 CASE CATEGORY: ADULT MALOCCLUSION NAME: K.N BORN: 03/03/1980 SEX: Male PRE-TREATMENT RECORDS:
EUROPEAN SOCIETY OF LINGUAL ORTHODONTISTS CANDIDATE NUMBER: 44 CASE NUMBER: 1 Year: ESLO 01 RÉSUMÉ OF CASE 1 CASE CATEGORY: ADULT MALOCCLUSION NAME: K.N BORN: 03/03/1980 SEX: Male PRE-TREATMENT RECORDS:
Treatment planning of nonskeletal problems. in preadolescent children
 In the name of GOD Treatment planning of nonskeletal problems in preadolescent children Presented by: Dr Somayeh Heidari Orthodontist Reference: Contemporary Orthodontics Chapter 7 William R. Proffit,
In the name of GOD Treatment planning of nonskeletal problems in preadolescent children Presented by: Dr Somayeh Heidari Orthodontist Reference: Contemporary Orthodontics Chapter 7 William R. Proffit,
KJLO. A Sequential Approach for an Asymmetric Extraction Case in. Lingual Orthodontics. Case Report INTRODUCTION DIAGNOSIS
 KJLO Korean Journal of Lingual Orthodontics Case Report A Sequential Approach for an Asymmetric Extraction Case in Lingual Orthodontics Ji-Sung Jang 1, Kee-Joon Lee 2 1 Dream Orthodontic Clinic, Gimhae,
KJLO Korean Journal of Lingual Orthodontics Case Report A Sequential Approach for an Asymmetric Extraction Case in Lingual Orthodontics Ji-Sung Jang 1, Kee-Joon Lee 2 1 Dream Orthodontic Clinic, Gimhae,
MemRx Orthodontic Appliances
 MemRx Orthodontic Appliances Uses and Instructions The MemRx Fundamentals As the need for faster, more efficient treatment of non-compliant patients increases, orthodontic!technology and materials has
MemRx Orthodontic Appliances Uses and Instructions The MemRx Fundamentals As the need for faster, more efficient treatment of non-compliant patients increases, orthodontic!technology and materials has
Case Report Unilateral Molar Distalization: A Nonextraction Therapy
 Case Reports in Dentistry Volume 2012, Article ID 846319, 4 pages doi:10.1155/2012/846319 Case Report Unilateral Molar Distalization: A Nonextraction Therapy M. Bhanu Prasad and S. Sreevalli Department
Case Reports in Dentistry Volume 2012, Article ID 846319, 4 pages doi:10.1155/2012/846319 Case Report Unilateral Molar Distalization: A Nonextraction Therapy M. Bhanu Prasad and S. Sreevalli Department
Segmental Orthodontics for the Correction of Cross Bites
 10.5005/jp-journals-10005-1080 CASE REPORT IJCPD Segmental Orthodontics for the Correction of Cross Bites 1 Anirudh Agarwal, 2 Rinku Mathur 1 Professor and Head, Department of Orthodontics, Rajasthan Dental
10.5005/jp-journals-10005-1080 CASE REPORT IJCPD Segmental Orthodontics for the Correction of Cross Bites 1 Anirudh Agarwal, 2 Rinku Mathur 1 Professor and Head, Department of Orthodontics, Rajasthan Dental
Checklist with summary points
 Checklist with summary points Question 1: Are your doctor Invisalign preferences on your home page up to date? Go to your doctor home page and open up your doctor preferences pages. Be sure to update item
Checklist with summary points Question 1: Are your doctor Invisalign preferences on your home page up to date? Go to your doctor home page and open up your doctor preferences pages. Be sure to update item
Class II correction with Invisalign - Combo treatments. Carriere Distalizer.
 Tips from your peers to help you treat with confidence. Class II correction with Invisalign - Combo treatments. Carriere Distalizer. Dr. Clark D. Colville. Carriere Distalizer and Invisalign Combo. A distalization
Tips from your peers to help you treat with confidence. Class II correction with Invisalign - Combo treatments. Carriere Distalizer. Dr. Clark D. Colville. Carriere Distalizer and Invisalign Combo. A distalization
#45 Ortho-Tain, Inc PREVENTIVE ERUPTION GUIDANCE -- PREVENTIVE OCCLUSAL DEVELOPMENT
 #45 Ortho-Tain, Inc. 1-800-541-6612 PREVENTIVE ERUPTION GUIDANCE -- PREVENTIVE OCCLUSAL DEVELOPMENT Analysis and Diagnosis of Occlusion: The ideal child of 5 y ears of age that probably has the best chance
#45 Ortho-Tain, Inc. 1-800-541-6612 PREVENTIVE ERUPTION GUIDANCE -- PREVENTIVE OCCLUSAL DEVELOPMENT Analysis and Diagnosis of Occlusion: The ideal child of 5 y ears of age that probably has the best chance
Case Report n 2. Patient. Age: ANB 8 OJ 4.5 OB 5.5
 Case Report n 2 Patient Age: 12.11 Diagnosis Angle cl.ii div.2 ANB 8 OJ 4.5 OB 5.5 Author: Dr. Case History The patient is a thirteen year old girl who exhibits delayed development, both physically and
Case Report n 2 Patient Age: 12.11 Diagnosis Angle cl.ii div.2 ANB 8 OJ 4.5 OB 5.5 Author: Dr. Case History The patient is a thirteen year old girl who exhibits delayed development, both physically and
Fixed Twin Blocks. Guidelines for case selection are similar to those for removable Twin Block appliances.
 Fixed Twin Blocks Development of Fixed Twin Blocks Dr Clark has enjoyed the cooperation of Dynaflex in developing the Fixed Twin Block. Six years of clinical testing has confirmed that this technique produces
Fixed Twin Blocks Development of Fixed Twin Blocks Dr Clark has enjoyed the cooperation of Dynaflex in developing the Fixed Twin Block. Six years of clinical testing has confirmed that this technique produces
An Effectiv Rapid Molar Derotation: Keles K
 An Effectiv ective e and Precise Method forf Rapid Molar Derotation: Keles K TPA Ahmet Keles, DDS, DMSc 1 /Sedef Impar, DDS 2 Most of the time, Class II molar relationships occur due to the mesiopalatal
An Effectiv ective e and Precise Method forf Rapid Molar Derotation: Keles K TPA Ahmet Keles, DDS, DMSc 1 /Sedef Impar, DDS 2 Most of the time, Class II molar relationships occur due to the mesiopalatal
Buccally Malposed Mesially Angulated Maxillary Canine Management
 Buccally Malposed Mesially Angulated Maxillary Canine Management Suhad. H. Manhal,* Summery: Maxillary canine is an important tooth in all fields of dentistry. However, malposed upper canine is seemed
Buccally Malposed Mesially Angulated Maxillary Canine Management Suhad. H. Manhal,* Summery: Maxillary canine is an important tooth in all fields of dentistry. However, malposed upper canine is seemed
Mesial Step Class I or Class III Dependent upon extent of step seen clinically and patient s growth pattern Refer for early evaluation (by 8 years)
") Orthodontics and Dentofacial Development Overview Development of Dentition Treatment Retention and Relapse Growth of Naso-Maxillary Complex Develops postnatally entirely by intramenbranous ossification
Orthodontics and Dentofacial Development Overview Development of Dentition Treatment Retention and Relapse Growth of Naso-Maxillary Complex Develops postnatally entirely by intramenbranous ossification
Treatment of Class II, Division 2 Malocclusion in Adults: Biomechanical Considerations FLAVIO URIBE, DDS, MDS RAVINDRA NANDA, BDS, MDS, PHD
 REPRINTED FROM JOURNAL OF CLINICAL ORTHODONTICS 1828 PEARL STREET, BOULDER, COLORADO 80302 Treatment of Class II, Division 2 Malocclusion in Adults: Biomechanical Considerations FLAVIO URIBE, DDS, MDS
REPRINTED FROM JOURNAL OF CLINICAL ORTHODONTICS 1828 PEARL STREET, BOULDER, COLORADO 80302 Treatment of Class II, Division 2 Malocclusion in Adults: Biomechanical Considerations FLAVIO URIBE, DDS, MDS
EUROPEAN SOCIETY OF LINGUAL ORTHODONTISTS
 EUROPEAN SOCIETY OF LINGUAL ORTHODONTISTS Dr. Masatoshi Sana Year: ESLO 01 RÉSUMÉ OF CASE 8 CASE CATEGORY: TRANS / VERTICAL DISCREPANCY NAME: Akiko T. BORN : 15/03/1973 SEX: F PRE-TREATMENT RECORDS: AGE:
EUROPEAN SOCIETY OF LINGUAL ORTHODONTISTS Dr. Masatoshi Sana Year: ESLO 01 RÉSUMÉ OF CASE 8 CASE CATEGORY: TRANS / VERTICAL DISCREPANCY NAME: Akiko T. BORN : 15/03/1973 SEX: F PRE-TREATMENT RECORDS: AGE:
From Plan B to Plan A : Using Forsus Class II Correctors as a Regular Mode of Treatment
 From Plan B to Plan A : Using Forsus Class II Correctors as a Regular Mode of Treatment by Lisa Alvetro, DDS After receiving her DDS summa cum laude from Ohio State University, Dr. Lisa Alvetro completed
From Plan B to Plan A : Using Forsus Class II Correctors as a Regular Mode of Treatment by Lisa Alvetro, DDS After receiving her DDS summa cum laude from Ohio State University, Dr. Lisa Alvetro completed
eral Maxillary y Molar Distalization with Sliding Mechanics: Keles Slider
 Bilater eral Maxillary y Molar Distalization with Sliding Mechanics: Keles Slider Ahmet Keles, DDS, DMSc 1 /Binnur Pamukcu, DDS 2 /Ebru Cetinkaya Tokmak, DDS 2 Aim: To introduce a new intraoral appliance
Bilater eral Maxillary y Molar Distalization with Sliding Mechanics: Keles Slider Ahmet Keles, DDS, DMSc 1 /Binnur Pamukcu, DDS 2 /Ebru Cetinkaya Tokmak, DDS 2 Aim: To introduce a new intraoral appliance
OF LINGUAL ORTHODONTICS
 EUROPEAN SOCIETY OF LINGUAL ORTHODONTICS CANDIDATE NUMBER: KDr. KP. kanarelis CASE NUMBER: 2 Year: 2010 WBLO 01 RESUME OF CASE 2 CASE CATEGORY: ADULT MALOCCLUSION NAME : MARIA A. BORN: 18.04.1983 SEX:
EUROPEAN SOCIETY OF LINGUAL ORTHODONTICS CANDIDATE NUMBER: KDr. KP. kanarelis CASE NUMBER: 2 Year: 2010 WBLO 01 RESUME OF CASE 2 CASE CATEGORY: ADULT MALOCCLUSION NAME : MARIA A. BORN: 18.04.1983 SEX:
An estimated 25-30% of all orthodontic patients can benefit from maxillary
 2017 JCO, Inc. May not be distributed without permission. www.jco-online.com A New Appliance for Efficient Molar Distalization VAIBHAV GANDHI, BDS, MDS FALGUNI MEHTA, BDS, MDS HARSHIK PAREKH, BDS, MDS
2017 JCO, Inc. May not be distributed without permission. www.jco-online.com A New Appliance for Efficient Molar Distalization VAIBHAV GANDHI, BDS, MDS FALGUNI MEHTA, BDS, MDS HARSHIK PAREKH, BDS, MDS
Treatment of a severe class II division 1 malocclusion with twin-block appliance
 2018; 4(5): 167-171 ISSN Print: 2394-7500 ISSN Online: 2394-5869 Impact Factor: 5.2 IJAR 2018; 4(5): 167-171 www.allresearchjournal.com Received: 27-03-2018 Accepted: 28-04-2018 Dr. Sheetal Bohra Resident
2018; 4(5): 167-171 ISSN Print: 2394-7500 ISSN Online: 2394-5869 Impact Factor: 5.2 IJAR 2018; 4(5): 167-171 www.allresearchjournal.com Received: 27-03-2018 Accepted: 28-04-2018 Dr. Sheetal Bohra Resident
UNILATERAL UPPER MOLAR DISTALIZATION IN A SEVERE CASE OF CLASS II MALOCCLUSION. CASE PRESENTATION. 1*
 UNILATERAL UPPER MOLAR DISTALIZATION IN A SEVERE CASE OF CLASS II MALOCCLUSION. CASE PRESENTATION. 1* Department of Orthodontics and Pedodontics 1 Faculty of Dental Medicine, University of Medicine and
UNILATERAL UPPER MOLAR DISTALIZATION IN A SEVERE CASE OF CLASS II MALOCCLUSION. CASE PRESENTATION. 1* Department of Orthodontics and Pedodontics 1 Faculty of Dental Medicine, University of Medicine and
Correction of a maxillary canine-first premolar transposition using mini-implant anchorage
 CASE REPORT Correction of a maxillary canine-first premolar transposition using mini-implant anchorage Mehmet Oguz Oztoprak, DDS, MSc, a Cigdem Demircan, DDS, b Tulin Arun, PhD, DDS, MSc c Transposition
CASE REPORT Correction of a maxillary canine-first premolar transposition using mini-implant anchorage Mehmet Oguz Oztoprak, DDS, MSc, a Cigdem Demircan, DDS, b Tulin Arun, PhD, DDS, MSc c Transposition
Attachment G. Orthodontic Criteria Index Form Comprehensive D8080. ABBREVIATIONS CRITERIA for Permanent Dentition YES NO
 First Review IL HFS Dental Program Models Second Review Ortho cad Attachment G Orthodontic Criteria Index Form Comprehensive D8080 Ceph Film X-Rays Photos Narrative Patient Name: DOB: ABBREVIATIONS CRITERIA
First Review IL HFS Dental Program Models Second Review Ortho cad Attachment G Orthodontic Criteria Index Form Comprehensive D8080 Ceph Film X-Rays Photos Narrative Patient Name: DOB: ABBREVIATIONS CRITERIA
Congenitally missing mandibular premolars treatment options for space closure. Educational aims and objectives. Expected outcomes
 Congenitally missing mandibular premolars treatment options for space closure Dr. Mark W. McDonough discusses recognition and treatment planning for congenitally missing second premolars Introduction The
Congenitally missing mandibular premolars treatment options for space closure Dr. Mark W. McDonough discusses recognition and treatment planning for congenitally missing second premolars Introduction The
The practice of orthodontics is faced with new
 CLINICIAN S CORNER A new approach to correction of crowding William Randol Womack, DDS, a Jae H. Ahn, DDS, MSD, b Zahra Ammari, DDS, MDSc, c and Anamaría Castillo, DDS, MS c Phoenix, Ariz, and Santa Clara,
CLINICIAN S CORNER A new approach to correction of crowding William Randol Womack, DDS, a Jae H. Ahn, DDS, MSD, b Zahra Ammari, DDS, MDSc, c and Anamaría Castillo, DDS, MS c Phoenix, Ariz, and Santa Clara,
Class III malocclusion occurs in less than 5%
 CDABO CASE REPORT Orthodontic correction of a Class III malocclusion in an adolescent patient with a bonded RPE and protraction face mask Steven W. Smith, DDS, a and Jeryl D. English, DDS, MS b Dallas,
CDABO CASE REPORT Orthodontic correction of a Class III malocclusion in an adolescent patient with a bonded RPE and protraction face mask Steven W. Smith, DDS, a and Jeryl D. English, DDS, MS b Dallas,
With judicious treatment planning, the clinical
 CLINICIAN S CORNER Selecting custom torque prescriptions for the straight-wire appliance Earl Johnson San Francisco, Calif Selecting custom torque prescriptions based on the treatment needs of each patient
CLINICIAN S CORNER Selecting custom torque prescriptions for the straight-wire appliance Earl Johnson San Francisco, Calif Selecting custom torque prescriptions based on the treatment needs of each patient
Orthodontic Treatment Using The Dental VTO And MBT System
 Orthodontic Treatment Using The Dental VTO And MBT System by Dr. Hideyuki Iyano Dr. Hideyuki Iyano, Department of Orthodontics, Ohu University School of Dentistry, Japan. He is also a member of the Japan
Orthodontic Treatment Using The Dental VTO And MBT System by Dr. Hideyuki Iyano Dr. Hideyuki Iyano, Department of Orthodontics, Ohu University School of Dentistry, Japan. He is also a member of the Japan
Management of Crowded Class 1 Malocclusion with Serial Extractions: Report of a Case
 Management of Crowded Class 1 Malocclusion with Serial Extractions: Report of a Case Hayder A. Hashim, BDS, MSc Abstract Aim: The purpose of this article is to show the value of serial extractions in a
Management of Crowded Class 1 Malocclusion with Serial Extractions: Report of a Case Hayder A. Hashim, BDS, MSc Abstract Aim: The purpose of this article is to show the value of serial extractions in a
Mx1 to NA = 34 & 10 mm. Md1 to NB = 21 & 3 mm.
 Chapter 16 Clinical cases: mixed dentition and adolescent, CLII non-extraction 219 Full CLII div I OJ = 15 OB = 8 SNA = 82 SNB = 75 Mx1 to NA = 34 & 10 mm. Md1 to NB = 21 & 3 mm. Md1 to A-pog = -2 GO-GN
Chapter 16 Clinical cases: mixed dentition and adolescent, CLII non-extraction 219 Full CLII div I OJ = 15 OB = 8 SNA = 82 SNB = 75 Mx1 to NA = 34 & 10 mm. Md1 to NB = 21 & 3 mm. Md1 to A-pog = -2 GO-GN
Treatment of a malocclusion characterized
 CONTINUING EDUCATION ARTICLE Cephalometric evaluation of open bite treatment with NiTi arch wires and anterior elastics Nazan Küçükkeleș, DDS, PhD, a Ahu Acar, DDS, PhD, b Arzu A. Demirkaya, DDS, c Berna
CONTINUING EDUCATION ARTICLE Cephalometric evaluation of open bite treatment with NiTi arch wires and anterior elastics Nazan Küçükkeleș, DDS, PhD, a Ahu Acar, DDS, PhD, b Arzu A. Demirkaya, DDS, c Berna
Holy Nexus of Variable Wire Cross-section: New Vistas in Begg s Technique
 10.5005/jp-journals-10021-1012 ORIGINAL ARTICLE Holy Nexus of Variable Wire Cross-section: New Vistas in Begg s Technique 1 Anil Miglani, 2 Ranjit Kumar Reena, 3 Pawanjit Singh Walia, 4 Varun Grover ABSTRACT
10.5005/jp-journals-10021-1012 ORIGINAL ARTICLE Holy Nexus of Variable Wire Cross-section: New Vistas in Begg s Technique 1 Anil Miglani, 2 Ranjit Kumar Reena, 3 Pawanjit Singh Walia, 4 Varun Grover ABSTRACT
Class II Correction with Invisalign Molar rotation.
 Tips from your peers to help you treat with confidence. Class II Correction with Invisalign Molar rotation. Dr. Mazyar Moshiri. Class II Correction with Invisalign Molar Rotation. Dr. Mazyar Moshiri. Orthodontic
Tips from your peers to help you treat with confidence. Class II Correction with Invisalign Molar rotation. Dr. Mazyar Moshiri. Class II Correction with Invisalign Molar Rotation. Dr. Mazyar Moshiri. Orthodontic
2007 JCO, Inc. May not be distributed without permission.
 2007 JCO, Inc. May not be distributed without permission. www.jco-online.com CSE REPORT Correction of an symmetrical Class II Malocclusion Using Predictable Force Systems PIERO PLCIOS, DDS, MDS FLVIO URIBE,
2007 JCO, Inc. May not be distributed without permission. www.jco-online.com CSE REPORT Correction of an symmetrical Class II Malocclusion Using Predictable Force Systems PIERO PLCIOS, DDS, MDS FLVIO URIBE,
Treatment of a Patient with Class I Malocclusion and Severe Tooth Crowding Using Invisalign and Fixed Appliances
 36 Dental Medicine Research 34 1 36 40, 2014 Case Report Treatment of a Patient with Class I Malocclusion and Severe Tooth Crowding Using Invisalign and Fixed Appliances Yumiko OGURA, Wakana YANAGISAWA,
36 Dental Medicine Research 34 1 36 40, 2014 Case Report Treatment of a Patient with Class I Malocclusion and Severe Tooth Crowding Using Invisalign and Fixed Appliances Yumiko OGURA, Wakana YANAGISAWA,
Maxillary Expansion and Protraction in Correction of Midface Retrusion in a Complete Unilateral Cleft Lip and Palate Patient
 Case Report Maxillary Expansion and Protraction in Correction of Midface Retrusion in a Complete Unilateral Cleft Lip and Palate Patient Masayoshi Kawakami, DDS, PhD a ; Takakazu Yagi, DDS, PhD b ; Kenji
Case Report Maxillary Expansion and Protraction in Correction of Midface Retrusion in a Complete Unilateral Cleft Lip and Palate Patient Masayoshi Kawakami, DDS, PhD a ; Takakazu Yagi, DDS, PhD b ; Kenji
Angle Class II, division 2 malocclusion with severe overbite and pronounced discrepancy*
 O C a s e R e p o r t ngle Class II, division 2 malocclusion with severe overbite and pronounced discrepancy* Daniela Kimaid Schroeder** bstract This article reports the treatment of a young patient at
O C a s e R e p o r t ngle Class II, division 2 malocclusion with severe overbite and pronounced discrepancy* Daniela Kimaid Schroeder** bstract This article reports the treatment of a young patient at
Ectopic upper canine associated to ectopic lower second bicuspid. Case report
 Original Article Published on 15-06-2001 In Italiano, per favore En Español, por favor Ectopic upper canine associated to ectopic lower second bicuspid. Case report A.R. Mazzocchi* * MD DDS. Corresponding
Original Article Published on 15-06-2001 In Italiano, per favore En Español, por favor Ectopic upper canine associated to ectopic lower second bicuspid. Case report A.R. Mazzocchi* * MD DDS. Corresponding
Several studies have shown that a Twin-block appliance
 ORIGINAL ARTICLE Comparison of 2 modifications of the Twinblock appliance in matched Class II samples Nicola Ann Parkin, BDS, MMedSci, FDS RCS(Eng), M Orth RCS(Eng), a Helen Fiona McKeown, BDS, MMedSci,
ORIGINAL ARTICLE Comparison of 2 modifications of the Twinblock appliance in matched Class II samples Nicola Ann Parkin, BDS, MMedSci, FDS RCS(Eng), M Orth RCS(Eng), a Helen Fiona McKeown, BDS, MMedSci,
A SIMPLE METHOD FOR CORRECTION OF BUCCAL CROSSBITE OF MAXILLARY SECOND MOLAR
 Short Communication International Journal of Dental and Health Sciences Volume 01,Issue 03 A SIMPLE METHOD FOR CORRECTION OF BUCCAL CROSSBITE OF MAXILLARY SECOND MOLAR Sumit Yadav 1,Davender Kumar 2,Achla
Short Communication International Journal of Dental and Health Sciences Volume 01,Issue 03 A SIMPLE METHOD FOR CORRECTION OF BUCCAL CROSSBITE OF MAXILLARY SECOND MOLAR Sumit Yadav 1,Davender Kumar 2,Achla
S.H. Age: 15 Years 3 Months Diagnosis: Class I Nonextraction Severe crowding, very flat profile. Background:
 S.H. Age: 15 Years 3 Months Diagnosis: Class I Nonextraction Severe crowding, very flat profile Background: This case was selected to illustrate the long-term impact of treatment planning on the face and
S.H. Age: 15 Years 3 Months Diagnosis: Class I Nonextraction Severe crowding, very flat profile Background: This case was selected to illustrate the long-term impact of treatment planning on the face and
Outline the significance of the pre-adjusted Edgewise appliance system and useful bracket variations in orthodontics
 Outline the significance of the pre-adjusted Edgewise appliance system and useful bracket variations in orthodontics Dr MJ Rowland-Warmann BSc BDS (Manc) MSc Aes.Med. (Lond) MJDF RCS (Eng) GDC: 178642
Outline the significance of the pre-adjusted Edgewise appliance system and useful bracket variations in orthodontics Dr MJ Rowland-Warmann BSc BDS (Manc) MSc Aes.Med. (Lond) MJDF RCS (Eng) GDC: 178642
Removable appliances
 Removable appliances Melinda Madléna DMD, PhD associate professor Department of Pedodontics and Orthodontics Faculty of Dentistry Semmelweis University Budapest Classification of the orthodontic anomalies
Removable appliances Melinda Madléna DMD, PhD associate professor Department of Pedodontics and Orthodontics Faculty of Dentistry Semmelweis University Budapest Classification of the orthodontic anomalies
Correction of Class II Division 2 Malocclusion by Fixed Functional Class II Corrector Appliance: Case Report
 Case Report To cite: Kumar M, Sharma H, Bohara P. Correction of class II division 2 malocclusion by fixed functional class II corrector appliance: case report. Journal of contemporary orthodontics, February
Case Report To cite: Kumar M, Sharma H, Bohara P. Correction of class II division 2 malocclusion by fixed functional class II corrector appliance: case report. Journal of contemporary orthodontics, February
CLASS II CORRECTION SIMPLIFIED
 C L A S S I I C O R R E C T O R CLASS II CORRECTION SIMPLIFIED PowerScope 2 delivers simple, efficient Class II correction like you ve never seen before. The latest generation of PowerScope features a
C L A S S I I C O R R E C T O R CLASS II CORRECTION SIMPLIFIED PowerScope 2 delivers simple, efficient Class II correction like you ve never seen before. The latest generation of PowerScope features a
Problems of First Permanent Molars - The first group of permanent teeth erupt in the oral cavity. - Deep groove and pit
 Management of the poor first permanent e molar Assoc. Prof. Kadkao Vongsavan * Asst. Prof. Praphasri Rirattanapong* Dr. Pongsakorn Sakkamathya** ** * Department of Pediatric Dentistry Faculty of Dentistry,
Management of the poor first permanent e molar Assoc. Prof. Kadkao Vongsavan * Asst. Prof. Praphasri Rirattanapong* Dr. Pongsakorn Sakkamathya** ** * Department of Pediatric Dentistry Faculty of Dentistry,
INDICATIONS. Fixed Appliances are indicated when precise tooth movements are required
 DEFINITION Fixed Appliances are devices or equipments that are attached to the teeth, cannot be removed by the patient and are capable of causing tooth movement. INDICATIONS Fixed Appliances are indicated
DEFINITION Fixed Appliances are devices or equipments that are attached to the teeth, cannot be removed by the patient and are capable of causing tooth movement. INDICATIONS Fixed Appliances are indicated
TWO PHASE FOR A BETTER FACE!! TWIN BLOCK AND HEADGEAR FOLLOWED BY FIXED THERAPY FOR CLASS II CORRECTION
 Case Report NUJHS Vol. 5, No.2, June 2015, ISSN 2249-7110 TWO PHASE FOR A BETTER FACE!! TWIN BLOCK AND HEADGEAR FOLLOWED BY FIXED THERAPY FOR CLASS II CORRECTION 1 2 3 4 U S Krishna Nayak, Ashutosh Shetty,
Case Report NUJHS Vol. 5, No.2, June 2015, ISSN 2249-7110 TWO PHASE FOR A BETTER FACE!! TWIN BLOCK AND HEADGEAR FOLLOWED BY FIXED THERAPY FOR CLASS II CORRECTION 1 2 3 4 U S Krishna Nayak, Ashutosh Shetty,
DonnishJournals
 DonnishJournals 2041-3144 Donnish Journal of Dentistry and Oral Hygiene Vol 1(2) pp. 007-011 May, 2015 http:///djdoh Copyright 2015 Donnish Journals Original Research Article Orthodontic Management of
DonnishJournals 2041-3144 Donnish Journal of Dentistry and Oral Hygiene Vol 1(2) pp. 007-011 May, 2015 http:///djdoh Copyright 2015 Donnish Journals Original Research Article Orthodontic Management of
MEDICAL ASSISTANCE BULLETIN COMMONWEALTH OF PENNSYLVANIA DEPARTMENT OF PUBLIC WELFARE
 MEDICAL ASSISTANCE BULLETIN COMMONWEALTH OF PENNSYLVANIA DEPARTMENT OF PUBLIC WELFARE ISSUE DATE EFFECTIVE DATE NUMBER October 21,1996 October 28,1996 03-96-06 SUBJECT BY Information on New Procedures
MEDICAL ASSISTANCE BULLETIN COMMONWEALTH OF PENNSYLVANIA DEPARTMENT OF PUBLIC WELFARE ISSUE DATE EFFECTIVE DATE NUMBER October 21,1996 October 28,1996 03-96-06 SUBJECT BY Information on New Procedures
Class II. Bilateral Cleft Lip and Palate. Clinician: Dr. Mike Mayhew, Boone, NC Patient: R.S. Cleft Lip and Palate.
 Bilateral Cleft Lip and Palate Clinician: Dr. Mike Mayhew, Boone, NC Patient: R.S. Class II Cleft Lip and Palate Pretreatment Diagnosis Class II dolichofacial female, age 22 years 11 months, presented
Bilateral Cleft Lip and Palate Clinician: Dr. Mike Mayhew, Boone, NC Patient: R.S. Class II Cleft Lip and Palate Pretreatment Diagnosis Class II dolichofacial female, age 22 years 11 months, presented
Skeletal Anchorage for Orthodontic Correction of Severe Maxillary Protrusion after Previous Orthodontic Treatment
 The Angle Orthodontist: Vol. 78, No. 1, pp. 181 188. Skeletal Anchorage for Orthodontic Correction of Severe Maxillary Protrusion after Previous Orthodontic Treatment Eiji Tanaka; a Akiko Nishi-Sasaki;
The Angle Orthodontist: Vol. 78, No. 1, pp. 181 188. Skeletal Anchorage for Orthodontic Correction of Severe Maxillary Protrusion after Previous Orthodontic Treatment Eiji Tanaka; a Akiko Nishi-Sasaki;
Case Report Orthodontic Replacement of Lost Permanent Molar with Neighbor Molar: A Six-Year Follow-Up
 Hindawi Case Reports in Dentistry Volume 2017, Article ID 4206435, 9 pages https://doi.org/10.1155/2017/4206435 Case Report Orthodontic Replacement of Lost Permanent Molar with Neighbor Molar: A Six-Year
Hindawi Case Reports in Dentistry Volume 2017, Article ID 4206435, 9 pages https://doi.org/10.1155/2017/4206435 Case Report Orthodontic Replacement of Lost Permanent Molar with Neighbor Molar: A Six-Year
Intraoral molar-distalization appliances that
 2014 JCO, Inc. May not be distributed without permission. www.jco-online.com Distalization with the Miniscrew- Supported EZ Slider Auxiliary ENIS GÜRAY, DDS, PHD FARUK IZZET UCAR, DDS, PHD NISA GUL, DDS
2014 JCO, Inc. May not be distributed without permission. www.jco-online.com Distalization with the Miniscrew- Supported EZ Slider Auxiliary ENIS GÜRAY, DDS, PHD FARUK IZZET UCAR, DDS, PHD NISA GUL, DDS
Molar distalisation with skeletal anchorage
 Molar distalisation with skeletal anchorage Antonio Gracco, Lombardo Luca and Giuseppe Siciliani Department of Orthodontics, University of Ferrara, Ferrara, Italy Background: Distalisation of the upper
Molar distalisation with skeletal anchorage Antonio Gracco, Lombardo Luca and Giuseppe Siciliani Department of Orthodontics, University of Ferrara, Ferrara, Italy Background: Distalisation of the upper
Angle Class I malocclusion with anterior open bite treated with extraction of permanent teeth
 Angle Class I malocclusion with anterior open bite treated with extraction of permanent teeth Matheus Melo Pithon 1 This clinical case reports the orthodontic treatment of a Class I malocclusion with anterior
Angle Class I malocclusion with anterior open bite treated with extraction of permanent teeth Matheus Melo Pithon 1 This clinical case reports the orthodontic treatment of a Class I malocclusion with anterior
RETENTION AND RELAPSE
 RETENTION AND RELAPSE DEFINITION Maintaining newly moved teeth long enough to aid in stabilizing their correction MOYERS loss of any correction achieved by any orthodontic treatment RELAPSE CAUSES OF RELAPSE
RETENTION AND RELAPSE DEFINITION Maintaining newly moved teeth long enough to aid in stabilizing their correction MOYERS loss of any correction achieved by any orthodontic treatment RELAPSE CAUSES OF RELAPSE
The conservative treatment of Class I malocclusion with maxillary transverse deficiency and anterior teeth crowding
 B B O C a s e R e p o r t The conservative treatment of Class I malocclusion with maxillary transverse deficiency and anterior teeth crowding Lincoln I. Nojima* Abstract This report describes the treatment
B B O C a s e R e p o r t The conservative treatment of Class I malocclusion with maxillary transverse deficiency and anterior teeth crowding Lincoln I. Nojima* Abstract This report describes the treatment
The role of removable appliances in contemporary orthodontics S. J. Littlewood, 1 A. G. Tait, 2 N. A. Mandall, 3 and D. H.
 The role of removable in contemporary S. J. Littlewood, 1 A. G. Tait, 2 N. A. Mandall, 3 and D. H. Lewis, 4 The contemporary uses of removable are considerably more limited than in the past. This article
The role of removable in contemporary S. J. Littlewood, 1 A. G. Tait, 2 N. A. Mandall, 3 and D. H. Lewis, 4 The contemporary uses of removable are considerably more limited than in the past. This article
Canine Extrusion Technique with SmartClip Self-Ligating Brackets
 Canine Extrusion Technique with SmartClip Self-Ligating Brackets Dr. Luis Huanca Ghislanzoni Dr. Luis Huanca received his DDS in 2006 and the MS and Specialist in Orthodontics in 2009 from the University
Canine Extrusion Technique with SmartClip Self-Ligating Brackets Dr. Luis Huanca Ghislanzoni Dr. Luis Huanca received his DDS in 2006 and the MS and Specialist in Orthodontics in 2009 from the University