Restorations in Pediatric Dentisty. Dr. Sami Malik Abdulhameed B.D.S.; M.Sc.
|
|
|
- Brianna Booker
- 6 years ago
- Views:
Transcription

1 Restorations in Pediatric Dentisty Dr. Sami Malik Abdulhameed B.D.S.; M.Sc.
2 Objectives of the lecture To review the ideal dental office setup To review the moisture control and isolation To review the restorative materials used in pediatric dentistry To review the Matrices & bands To review different cavity preparation techniques and some modifications To review crown restorations for posterior & anterior teeth

3 Restorative Goals Relief pain & Cease disease process Restore function Improve esthetics Preserve space for permenant dentition
.")
4 Moisture Control In Restorative Pediatric Dentistry Copyright 2003, Elsevier Science (USA). All rights reserved.
.")
5 Introduction Objective: Maintain an environment that keeps the operating field free of excess water, saliva, blood, tooth fragments, and excess dental materials. Copyright 2003, Elsevier Science (USA). All rights reserved.
 Copyright 2003, Elsevier Science (USA).")
6 Oral Evacuation Systems The process of removing excess fluids and debris from the mouth. Two systems: Saliva ejector High-volume evacuator (HVE) Copyright 2003, Elsevier Science (USA). All rights reserved.
.")
7 Saliva Ejector Small, strawlike oral evacuator used during less invasive dental procedures. Indications for use: Preventive procedures such as a prophylaxis or fluoride treatments. Helps control saliva and moisture accumulation under the dental dam. For the cementation of crown or bridge. During an orthodontic bonding procedure. Copyright 2003, Elsevier Science (USA). All rights reserved.
.")
8 HVE Used for most dental procedures, especially when the dental handpiece is in use. Indications for use Keep the mouth free of saliva, blood, water, and debris. Retracts the tongue and cheek away from the field of operation. Reduces the bacterial aerosol caused by the high-speed handpiece. Copyright 2003, Elsevier Science (USA). All rights reserved.

9 HVE- cont d Oral evacuation tips Operative suction tips Designed with a straight or slight angle in the middle. Beveled working end. Made of durable plastic or stainless steel. Surgical suction tips Much smaller in circumference. Made of stainless steel. Copyright 2003, Elsevier Science (USA). All rights reserved.
.")
10 Grasping the HVE Thumb-to-nose grasp Pen grasp Right hand Copyright 2003, Elsevier Science (USA). All rights reserved.

11 Copyright 2003, Elsevier Science (USA). All rights reserved. Fig Grasping the HVE.
12 IDEAL ISOLATION Copyright 2003, Elsevier Science (USA). All rights reserved.

13 Objectives of Ideal Isolation Provide optimum visibility and access to operative site. Prevent moisture contamination of teeth. Retract and control soft tissue of tongue, lip, and mucosa. Protect patient against aspiration of dental instruments and materials. Provide patient comfort. Be easily and rapidly accomplished.
.")
14 Dry-Angles A triangular absorbent pad placed over the Stensen's duct blocks the flow of saliva and protects the tissues in this area. Copyright 2003, Elsevier Science (USA). All rights reserved.



15 Copyright 2003, Elsevier Science (USA). All rights reserved.
. All rights reserved.")
16 The Dental Dam A thin stretchable latex material becomes a barrier when appropriately applied to select teeth. Copyright 2003, Elsevier Science (USA). All rights reserved.


17 Rubber Dam Application
18 Types of Dental Materials F release material ( Glass Ionomer) Resin Modified Glass Ionomer Composite Amalgam Stainless Steel
19 Fluoride-Releasing Materials Glass Inomer & Resin Modified Glass Inomer
20 Glass Inomer Cement loses and gains water easily: Early moisture contamination leads to increased solubility and poor esthetics, (protect for first 7 minutes). Later desiccation causes shrinkage and crazing, (maybe even months later).
21 GIC - Fluoride Release halo effect around restoration ~ 3 mm. Level around restoration ~ 10 ppm. Level in saliva of average patient ~ 0.08 ppm. Fluorine release from GIC does not lead to restoration breakdown.
22 Classification OF GI ADA Classification Type I: luting agents (Ketac-Cem, Fuji I) Type II: restorative material a = tooth-colored (Ketac-Fil, Fuji IX) b = reinforced (Ketac-Silver, Miracle Mix ) Type III: fast-set liners and bases (Ketac-Bond)
23 GIC Physical Properties Strengths: Ionic exchange leads to adhesion to tooth structure (chemical bond). Fluoride release and rechargeable.
24 GIC Physical Properties Weaknesses Moisture sensitivity. Lack of command cure, i.e. doesn t cure with light. Esthetics. Not recommended for stress-bearing areas. Difficult handling.
25 GIC Indications High caries risk patient Atrumatic Restorative Treatment (ART) Pediatric dentistry Class V lesions Liners & bases & sandwich technique Luting agents Core buildups??? Maybe if > 2/3 of tooth structure remains Orthopedics (bone substitute material)

26 Steps of Clinical Use of Glass Inomer 1. Mechanical retention in preparation advised (no bevels).
. 3.")
27 Steps of Clinical Use of Glass Inomer 2. Dentin conditioning (10 % polyacrylic acid for seconds). 3. Inject into preparation. Overfill the preparation.
28 Steps of Clinical Use of Glass Inomer 4. Trim excess with finishing bur (wet, with very light pressure as the cement material cuts easily!) and polish (if necessary). Be cautious not to over-reduce, the material is softer than composite resin. 5. Dry the surface and paint on a thin layer of lightcured unfilled resin (smoothes the surface and prevents desiccation but lowers fluoride release. (optional)
 Fluoride rechargable Less")
29 Glass Ionomers Advantages Bond to tooth structure Physical properties similar to dentin Moisture tolerant Release fluoride (5 years) Fluoride rechargable Less microleakage

30 Glass Ionomers Disadvantages Not as strong Poor wear Increased setting time Not as esthetic as composite
31 Glass Ionomer Indications Smooth surface lesions Small anterior proximal lesions i.e. areas of low stress High caries risk patients Sealants Base underneath deep carious lesions Good cement for stainless steel crowns and brackets and bands Interim Therapeutic Restorations

32 Resin Modified Glass Ionomer Mixture of glass, an organic acid, and resin polymer that harden when light cured

33 Resin Modified Glass Ionomer Advantages Increased wear and fracture toughness Some fluoride release Comand cure Increased esthetics Disadvantages Not as strong as composite or amalgam Less fluoride release than glass ionomer
 Once mixed sets")
34 Amalgam mixture of mercury (43%-54%) and powdered alloy (silver, tin, zinc and copper) Once mixed sets automatically

35 Amalgam Advantages Quick and easy manipulation Less moisture sensitive Microleakage decreases with time Good mechanical properties economical

36 Amalgam Disadvantages Non bonding Bulk for strength Proper preparation to prevent fracture Wide isthmus Rounded line angles Poor esthetics Dental amalgam controversy
37 Composite Mixture of powdered glass and plastic resin Polymerization reaction initiated by light Various level of filler particles can change esthetics, mechanical properties, and viscosity

38 Composites Advantages Micromechanical Bond Esthetic and polishable Conservative preparation Preventative Sealants

39 Composites Disadvantages Moisture sensitive Technique sensitive Multiple steps Time consuming Polymerization shrinkage leads to microleakage


40 Composite Indications Small pit and fissure caries Class I, II, III, IV and V restorations in primary and permanent teeth


41 Anterior Strip Crowns Anterior Restorations Primary anterior crown forms

42 Stainless Steel Pre-fabricated Full coverage restoration Pre-crimped with 6 sizes Adapted to tooth

43 Stainless Steel Advantages Strongest Preventative Can be adapted for space maintainer Disadvantages Poor esthetics Post op discomfort

44 Stainless Steel Indications Pulpotomy Extensive caries Fractured teeth Hypoplastic molars

45 Stainless Steel Crown Indications Space Maintainer Distal Shoe / loop High caries risk children Patients that require general anesthetic for dental treatment

46 Stainless Steel Crown Crown and loop Placed on tooth that has extensive decay with space maintenance needs


47 Anterior Stainless Steel Crowns Anterior SSC with windows Flowable composite Acid etched Micromechanical and mechanical retention
. All rights reserved.")
48 Matrix Systems for Restorative Dentistry Copyright 2003, Elsevier Science (USA). All rights reserved.
.")
49 Introduction A matrix system provides and takes the place of the proximal tooth surface that was removed to restore the proximal contours and contact to their normal shape and function. Copyright 2003, Elsevier Science (USA). All rights reserved.
50 Types of Matrices w Tofflemire does not fit contour of primary tooth well difficult to fit multiple matrices W T-band w Spot welded allows for multiple matrix placement requires a spot welder chairside w Automatrix - costly
.")
51 Posterior Matrix System Universal retainer Also referred to as the Tofflemire retainer. This device holds the matrix band in position. The retainer is positioned most commonly from the buccal surface of the tooth being restored. Copyright 2003, Elsevier Science (USA). All rights reserved.
.")
52 Components of a Universal Retainer Copyright 2003, Elsevier Science (USA). All rights reserved.


53 Posterior Matrix Systemcont d Matrix bands Matrix bands are made of flexible stainless steel and are available in premolar, molar, and universal sizes and thicknesses. The larger circumference of the band is the occlusal edge and is always placed toward the occlusal surface. The smaller circumference of the band is the gingival edge and it is always placed toward the gingiva. Copyright 2003, Elsevier Science (USA). All rights reserved.
.")
54 Fig Types of matrix bands. Copyright 2003, Elsevier Science (USA). All rights reserved.

55 Automatrix System The automatrix system is an alternative to a universal retainer. There is no retainer used to hold the band in place. Bands are already formed into a circle and are available in assorted sizes in both metal and plastic. Each band has a coil like autolock loop. A tightening wrench is inserted into the coil and turned clockwise to tighten the band. When finished, the tightening wrench is inserted into the coil and turned counterclockwise to loosen the band. Removing pliers are used to cut the band. Copyright 2003, Elsevier Science (USA). All rights reserved.
 Copyright 2009, 2006 by Saunders, an imprint of Elsevier Inc.")
56 Fig Automatrix system. (Courtesy of Dentsply Caulk.) Copyright 2009, 2006 by Saunders, an imprint of Elsevier Inc. All rights reserved.

57

58 Matrix Systems for Primary Teeth The T-band is a T-shaped copper band. When formed, the top portion of the T allows the straight portion to adjust and fit the circumference of the primary molar. Copyright 2003, Elsevier Science (USA). All rights reserved.

59 Copper T-band used for primary molars. Copyright 2009, 2006 by Saunders, an imprint of Elsevier Inc. All rights reserved.
.")
60 Additional Matrix Systems for Primary Teeth A spot-welded band is a form-fitted band placed around a prepared tooth, then removed and placed in a smaller form of a welder that fuses the metal together to make a custom band. Copyright 2003, Elsevier Science (USA). All rights reserved.
61 Spot Welded Matrix w Cut matrix and spot weld ends 3/16 wide and thin (..002 ) matrix w Form a loop w Hold ends in spot welder w Weld at low setting Copyright 2003, Elsevier Science (USA). All rights reserved.
.")
62 Fig Spot-welded band. Copyright 2003, Elsevier Science (USA). All rights reserved.
. All rights reserved.")
63 Matrices for Composite Restorations A plastic matrix, also referred to as a celluloid matrix or mylar strip, is used for class III and IV restorations in which the proximal wall of an anterior tooth is missing. Copyright 2003, Elsevier Science (USA). All rights reserved.

64 A clear matrix system. (Courtesy of Premier Dental Products.) Copyright 2003, Elsevier Science (USA). All rights reserved. Copyright 2009, 2006 by Saunders, an imprint of Elsevier Inc. All rights reserved.

65 The Use of a Clear Matrix The matrix is placed interproximally before the etching and priming of a tooth. This protects adjacent teeth from these materials. After placement of composite material, a matrix is pulled tightly around the tooth to help reconstruct its natural contour. The clear plastic matrix allows the curing light to penetrate the material and complete the curing process. Copyright 2003, Elsevier Science (USA). All rights reserved.
.")
66 Sectional Matrices A thin polished palodent-type band and a tension ring produce a tight anatomic contact for composite resin materials for class II restorations. Copyright 2003, Elsevier Science (USA). All rights reserved.
.")
67 Fig Sectional matrices. Copyright 2003, Elsevier Science (USA). All rights reserved.

68 Sectional matrices. (Courtesy of Garrison Dental Solutions.)

69 Wedges A wedge is either triangular or round and made of wood or plastic. The wedge is inserted into the lingual embrasure to position the matrix band firmly against the gingival margin of the preparation. Copyright 2003, Elsevier Science (USA). All rights reserved.
.")
70 Fig A wedge correctly positioned. Copyright 2003, Elsevier Science (USA). All rights reserved.

71 Restorative Dentistry for Children BY DR SAMI MALIK ABDULHAMEED.
72 Cavity Preparation Dr. Sami malik abdulhameed
73 Objectives wto be able to identify and distinguish morphologic differences between primary and permanent teeth. To apply the knowledge of morphology in clinical procedures for pediatric patients
74 Morphological Considerations in the Primary Dentition w The crowns of primary teeth are shorter have a narrower occlusal table have a more pronounced cervical constriction have thinner enamel and dentin layers
75 Morphological Considerations in the Primary Dentition w The crowns of primary teeth have enamel rods that run in a slightly occlusal direction from the DEJ have broad flat contact areas between primary molars have nearly the same mineral content as permanent teeth have a lighter, more homogeneous color
76 Contact Area Point contact Broad, flat contact

77 Morphological Considerations in the Primary Dentition w The pulps of primary teeth are larger than that of the permanent tooth in relation to crown size are closer to the outer surface of the tooth the mesial pulp horn is pronounced occlusally more closely follow the surface of the crown usually have a pulp horn under each cusp
78 Comparison of Pulps
79 Influences of Primary Tooth Morphology w Tooth Preparations Need to take into account tooth size, pulp size and enamel and dentin thickness
80 Instrumentation w Utilize a # 245 bur w Tip - measure width and length of cutting shank w High speed w Minimal use of hand instruments

81
82

83 Class I Amalgam Preps w Pulpal Floor Depth mm into dentin primary molars to 1.50mm w Intercuspal width - 1/3rd w Rounded internal line angles w B-L walls slightly undercut w M-D walls flare at marginal ridges
84 Mandibular Molars Outline Form
85 Maxillary Molars Outline Form

86
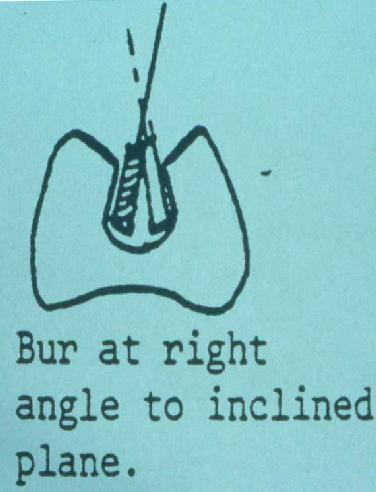
87 Internal Form of a Class I Prep w 1) depth.5-1mm into dentin w 2) angle of floor and walls is rounded w 3) slightly rounded pulpal floor Avoids pulp w 4) sharp cavosurface angle
88 General Considerations w Adhere to GV Black s principles with respect to outline, resistance, retention and convenience form and finishing of enamel walls.

89 Class II Cavity Prep - Mandibular

90 Class II Cavity Preps - Maxillary
91 Class II Amalgam Preps w Accomplish occlusal outline form w Extend proximal box into self cleaning area leave 90 degree cavosurface margins isthmus width 1/3 w Proximal box in an occlusal gingival direction is parallel to the long axis of the tooth
92 Class II, continued w B-L walls of box should converge occlusally w Gingival floor should be beneath the contact, at, or just beneath the gingival tissue w Axial wall should follow the contour of the tooth 1 mm in width
93 Cross-sectional View of Class II w 1a) gingival floor position 1b) box is perpendicular to long axis w 1c) rounded angles
94 Common Errors - Class II s
95 Modifications B View from distal surface of primary 1st molar L w Concave pulpal floor and gingival seat w Rounded internal line angles both decrease stress in the restoration

96 Modifications w Relatively wider isthmus width one-third the intercuspal distance w Conservative proximal extensions you can see light, but cannot pass an explorer tip through

97 Modifications w No proximal grooves w No reverse curves

98 Class 2 slot preparation

99 Class V Restorations A class V restoration is classified as a smooth surface restoration. These decayed lesions occur at: The gingival third of the facial or lingual surfaces of any tooth. The root of a tooth, near the cementoenamel junction. Copyright 2003, Elsevier Science (USA). All rights reserved.
100 Condensation and Carving w Back to back condensation of Class II s w Carving described as hill and valley w Polishing procedure is same as taught for permanent teeth
101 Condensation and Carving w Back to back condensation of Class II s w Carving described as hill and valley w Polishing procedure is same as taught for permanent teeth

102 Polishing!
103 Failures of Amalgam Restorations w Fracture of the isthmus of a Class II due to insufficient bulk of amalgam w Marginal failure in proximal box area due to excessive flare of the cavosurface margin w Recurrent caries failure to extend preparation adequately


104 Class III Cavity - Incisors What type of spacing would make a patient more susceptible?
105 Class III Cavity - Cuspids Dovetail is placed on lingual of maxillary cuspids and the facial of mandibular cuspids. Proximal box is placed perpendicuar to a line tangent to the surface on which the dovetail is placed.
106 Restoration of Proximal-Incisal Caries in Primary Anterior Teeth Esthetic Resin Restoration Stainless Steel Crown Open-Face Steel Crowns Direct Resin Crowns
107 Composite (Strip) Crowns
108 Preventive resin restoration
109 OBJECTIVES: PREVENTIVE RESIN RESTORATION (PRR) 1. List the indications and contra-indications for PRR for primary and permanent teeth. 2. Describe the PRR materials. 3. Describe the clinical procedures for PRR. 4. Identify the advantages of using PRR and their cost effectiveness.
110 Preventive resin restorations were first described a long time ago in paediatric dentistry. Today the technique is still very pertinent, and has been extended to include teenagers and adult patients. New flowable composites have made it possible to extend the indication area for preventive resin restorations. Although mostly considered as a base material for posterior restoration, flowable composites are now proving very useful for many different types of minimally invasive cavity preparations such as carious fissures

111

112

113

114

115

116

117

118

119

120

121

122

123

124

125

126

127

128

129

130

131

132

133

134
135

136

137

138

139


140 The patient presented with infiltration of the fissures an eroded amalgam The decayed fissures were opened using special burs, allowing the retention of healthy tissue to be maximised. The amalgam restoration was removed.the dentine was properly cleaned of carious tissue.






141

142 ATRAUMATIC RESTORATIVE TREATMENT A.R.T
143 INTRODUCTION Atraumatic restorative treatment (ART) is a procedure that involves removal of carious substance from the tooth using hand instruments and restoring with adhesive restorative material. This is being developed for less industrialized communities in special groups such as refugees and people living in financially deprived communities who are unable to obtain a restorative dental care. ART has broken many barriers and allowed delivery of dental restorative treatments possible despite unavailability of electricity or communities that can not afford dental treatment.
144 CONTINUED Glass Ionomer is the material of choice for ART that can be applied to early stages of caries development that would halt or slows the caries progression due to the slow release of fluoride. It is important to understand that ART is only a branch of oral health care that need to start with health promotion messages, healthy diet and good oral hygiene. With ART one attempts to conserve as much tooth structure as possible to prevent further decay to achieve the goal of Teeth for Life.
145 CONTINUED Instrument needed for ART is very convenient to carry around by bus or bicycle in a bag. In addition delivering this treatment oral care workers travel to rural communities for oral health education. ART is a very friendly procedure to patients that could be utilized to be effectively used on children and fearful adults. For this reason, ART is widely used even in industrialized countries because it supports minimal intervention and minimal invasion of the patient.

146 Interim Therapeutic Restorations Removing carious tissues using hand instruments only Less traumatic No need for electricity Conservation of tooth structure Low cost Glass Ionomer Bonds to tooth Releases fluoride
147 ART Applications Great technique for root caries Good alternative in field conditions Excellent for fearful children Good alternative in medically compromised patients Good alternative in mentally compromised
148 Quality of restorations depends on: Material Operator Patient
149 RESEARCH ART was pioneered in mid 1980s in Tanzania. In 1991 community field trial was started in Thailand comparing the difference between ART with traditional portable drilling equipment and amalgam. In 1993 another community field trial in Zimbabwe was set up based on experiences in Thailand. This showed that careful application yielded 85% of one surface fillings in permanent dentition survived for 3 years. In 1995 in Pakistan, a community field trial showed that pain is rarely experienced with this approach.
150 PRINCIPLES OF ART 2 main principles of ART are: 1. Removing carious tooth tissues using hand instruments only 2. Restoring the cavity with a restorative material that sticks to the tooth. Why GIC? It bonds chemically to both enamel and dentine, it is fluoride releasing and it does not inflame gingiva or pulp.


151
152 INDICATION AND CONTRAINDICATIONS Indications: There is a cavity involving dentine Able to access the cavity with hand instruments. Contraindications: Presence of infection (abscess or fistula) Pulp is exposed Chronic inflammation of pulp Cavity is inaccessible with hand instruments.
153 PREPARING THE CAVITY Place a cotton roll and dry the working tooth. Use the dental hatchet to gain access and excavators to remove soft caries and unsupported enamel. It is very important that: 1. All soft caries is removed at enamel-dentine junction. 2. To avoid exposure of pulp in deep cavities, leave a small portion of affected dentine near pulp region.
154 CLEANING THE PREPARED CAVITY The purpose of cleaning the cavity walls is to improve chemical bonding of GIC to tooth structure. Cavity could be cleaned by: 1. Dentine conditioner (10% Polyacrylic acid) 2. The liquid supplied by GIC itself. With dentine conditioner clean the cavity walls for seconds and dry with cotton wool pellets. Repeat the procedure if contaminated by blood or saliva.
155 RESTORING THE CAVITY After cavity is washed and dried, start mixing GIC powder and liquid. Insert in small amounts using applier/carver to avoid air bubbles and build the restoration slightly high on occlusal surface. Insert material into corners and unsupported enamel first. With petroleum jelly on the gloved index finger press the soft material into the cavity, this is called the press-finger technique. Do not disturb the restoration during hardening phase.
156 CONTINUED After 1-2 minutes check the occlusion. If the ART restoration too high, remove the stained portion of restoration with a carver blade. Ask the patient not to eat for an hour.

157
158 PROCEDURE FOR RESTORING MULTIPLE SURFACE CAVITIES Prepare the cavity in a dry cotton rolls. environment using Place a matrix strip between teeth with a wedge for support under the contact point and gum margin. Condition the cavity and fill it with GIC completely. Use the finger press technique Remove excess and wait for 1-2 minuets. Check the occlusion and it is important to have non occluding contacts with the opposing tooth.

159

160 PRESS-FINGER TECHNIQUE

161 PRESS-FINGER TECHNIQUE

162 AFTER PRESSING

163 AFTER APPLYING WATERPROOFING

164 SURVIVAL OF GIC SEALANTS 3 year old glass-ionomer sealant

165 SURVIVAL OF GIC SEALANTS 2 year old glass-ionomer sealant


166
167 MONITORING It is important to collect any information if any pain is being experienced and if ART restoration was accepted. Assess if the patient is satisfactory with the restoration within first 4 weeks. The clinical evaluation is planned annually or biannually depending on the risk statues and oral hygiene.
168 FAILED OR DEFECTIVE RESTORATION A restoration is no longer satisfactory when : 1. It is completely missing 2. Fractured restoration 3. Much of the restorative material is worn away. 4. Caries have developed at the restoration margin or else where on the tooth surface.

169 Stainless Steel Crowns Indications and Techniques Dr. Sami Malik Abdulhameed B.D.S.M.Sc.
170 Use of Stainless Steel Crowns u Introduced to pediatric dentistry by Dr. William Humphrey in 1950 prior to that orthodontic bands filled with amalgam were a last resort necessity is the mother of invention u Considered superior to large multisurface amalgam restorations and have a longer clinical lifespan than two or three surface amalgams (Dawson et al., 1981)
171 Objectives u The student should be able to: Describe the indications for stainless steel crowns. Understand the principles of preparation, adaptation, and cementation of a successful stainless steel crown. To properly prep a dentoform tooth for a SSC and properly adapt a crown to fit it.
172 Crowns vs. Class II Amalgams Crowns 90% successful from date of placement, regardless of age Majority of failures are related to pulp failure, not restoration failure (false failure) Not as esthetic however More expensive Class II Amalgams Success rate is highest when life expectancy of the tooth is less than 3 years Better looking than crowns Cheaper than crowns Approximately 50% failure rate when placed in children <4 y.o.
173 Indications Rampant Caries Caries involving three or more surfaces Recurrent caries Following pulp therapy Developmental defects Fractured teeth Severe bruxism Orthodontic appliance fabrication

174 Rampant Caries

175 Indications Rampant caries

176 .:Indications Three surface radiographic decay

177 Indications Non-ideal two surface, or 3 surface decay

178 .:Indications Recurrent caries


179 .:Indications Following pulp therapy

180 Indications Developmental Defects

181 Indications Developmental Defects Following indirect pulp therapy on permanent first molars Restoration of large developmental defects on permanent first molars

182 .:Indications Fractured amalgams

183 .:Indications Severe Bruxism


184 .:Indications Orthodontic Appliance Fabrication Distal Shoe Crown / loop
185 Contraindications u Esthetics u Teeth that are nearing exfoliation u Mechanical problems space loss caries beneath the level of the bone u Permanent restoration in the permanent dentition


186 Types of Crowns Rocky Mountain Unitek Ion
187 Types of Crowns First crown developed, originally by an orthodontist Must be trimmed Must be contoured Not crimped Rocky Mountain Rarely used today due to significant time to fabricate at chairside

188 Types of Crowns Second crown developed Pre-trimmed Must be contoured Must be crimped Unitek Primarily composed of chromium and steel, this is strongest of the three crowns
189 Types of Crowns Latest evolution Pre-trimmed Pre-contoured Pre-crimped Ion Softer metal, but designed to snap over prep without any alterations
190 What you will need u Burs and stones #169 heatless stone u Pliers and instruments contouring plier crimping plier u Polishing
191 Clinical Procedures Pre-treatment evaluation Prior to placing rubber dam, check occlusion Vertical space loss? Horizontal space loss? Soft tissue change? Mobility? Rubber dam is mandatory!!! Crowns are very slippery when wet with saliva Must have adequate anesthesia, particularly on the palate.

192 Horizontal space loss: #E has shifted mesially into #D Vertical Space loss: U #E has palatal cusp erupted into L #E caries


193 Squares vs. rectangles (maxillary molars vs. mandibular molars) - Hint!!! - distal caries on a mandibular primary first molar will alter its shape to look more like a square! When this happens, choose a maxillary primary first molar crown from the opposite arch (I.e. - space loss on lower left primary first molar. Choose a crown from the upper right box!!!)
194 Managing Space Loss Another technique for managing space loss Using the Howe plier, grasp the Unitek crown on the marginal ridges and gently squeeze This causes the rectangular crown to become square. Doing this reduces the mesio-distal width of the crown, but inceases the buccolingual width Recontour and recrimp the crown.

195 Overview u Occlusal reduction u Proximal reduction u Buccal and lingual reduction u Beveling u Round all sharp line angles and corners
196 Crown preparation Key points to remember This is not a cast restoration. The crown does not rely on a precision fit. Retention relies on the natural undercuts, the adequacy of the crimp, and the luting material. This prep is completely different from that of a full gold crown prep Excessive buccal/linqual reduction may result in a non-retentive crown and an unplanned extraction!
197 Crown Preparation Armamentaria Burs --- No. 169L FG Tapered Diamond FG No. 6 or 8 RA No. 330 FG Heatless Stone Accessories--- Wire wheel No. 114 contour pliers No crimping pliers Howe pliers
198 Crown Preparation Occlusal reduction Occlusal beveling Interproximal reduction Line angle refinement

199 Crown Preparation Occlusal Reduction - prior to preparation

200 Crown Preparation Occlusal Reduction - using a 330FG or a round wheel diamond, remove approximately 1-1.5mm.

201 Crown Preparation Occlusal bevel - use 330FG or tapered diamond
202 Occlusal Reduction mm

203 Occlusal Reduction mm

204 Completed Occlusal Reduction u Check reduction with opposing arch

205 Crown Preparation Occlusal reduction completed - do not over-reduce the mesiobuccal aspect (high pulp horn)!!!
206 Proximal Reduction u Contact with adjacent teeth must be broken gingivally and buccolingually u proximal slices converge slightly toward the occlusal and lingual DO NOT OVER TAPER u The gingival margins should have a featheredge finish line u Adjacent tooth structure must not be damaged

207 Proximal Slices


208 Crown Preparation Interproximal reduction - tapered diamond used to avoid interproximal ledges which can prevent seating!!!
209 Crown Preparation Completed preparation - should be approximately mm below the plane of occlusion as judged by comparing adjacent marginal ridge height. Should be no sharp angles to prevent crown from seating Must not be ledged interproximally Margin should be approximately 1 mm below the marginal gingiva



210 Crown Preparation

211 Crowns for Guiding Teeth Ectopic Eruption Crown is indicated on a second molar AND the permanent first molar is hold-type ectopic

212 Crowns for Guiding Teeth Techniques Pulp treatment is completed in the usual manner Estimate amount of distal reduction required Carefully reduce so that first molar is not damaged Estimated reduction
213 Crowns for Guiding Teeth Technique (con t) Using perio probe, sound the mesial of the permanent molar Unitek crown is trimmed so that the distal margin extends below the mesial marginal ridge of the first molar. Solder???

214 Crowns as Space Maintainers The primary advantage of using a crown instead of a band is the increased stability. May be a one or two step procedure (usually two)

215 Angulation of Slices Proper slice Improper slice
216 Ledging u Proximal slice must be extended below tissue to to avoid leaving a ledge

217 Preserving the Outline u Remember: crown preparation if a significant part of the crown s retentive potential

218 Buccal-Lingual Reduction u Reduction is optional and is undertaken only if the buccal or lingual bulges are so prominent that the constricted margin of the crown will not go over he height of contour when required, no more than.5-1mm should be removed reductions must end in a feather edge
219 Beveling u A bevel at an angle of degrees removes the sharp cusp tips and creates a gentle slope in the occlusal third of the lingual and buccal surfaces
220 Round Sharp Line Angles u The buccal and lingual proximal line angles are rounded by holding the bur parallel to the tooth s long axis and blending the surfaces togetherthe finished contour should conform to the internal contour of the stainless steel crown

221 Crown Adaptation u Mark gingival line with a scaler & trim 1mm beneath the mark using C&B scissorsmargins should be trimmed to lie parallel with the contour of the gingival tissue and consist of a series of curves without sharp angles
222 Guidelines u Resistance in seating without tissue blanching. Check for high spots on occlusal surface ledges u Resistance in seating with tissue blanching. Check for crown too wide (preliminary contouring) crown too long tissue caught in margin

223 Contour the Crown u Use contouring pliers, bend the gingival third of the crown s margins inward to restore anatomic margins and to reduce the marginal circumference ensuring a good fit

224 u With the crowncrimping plier (#118) crimp the margin Replace crown on tooth and check margins with an explorer Crimp the crown


225 Finishing and Polishing u Use heatless stone to smooth jagged edgesthen use a rubber wheel to remove small scratches and smoothpolish surface of crown to a high shine with tripoli and rouge

226 u Clean crown and tooth u Fill crown with zinc phosphate cementseat crown, expressing cement form all margins and press into occlusionremove excess cement when partially set Cementation Cross-sectional View

227 Post-op instructions? u Although a welladapted and cemented crown should not come off under these circumstances, patients and parents should be warned of the possibility

228 Managing Clinical Variations u Space Loss

229 Managing Space Loss u May need to increase the buccal and lingual reductionsmay need to compress crown form on mesial and distal with Howe pliers

230 Clinical Variations u Back-to-back chrome crowns First & Second primary molars
231 Composite Crowns BY DR. SAMI MALIK ABDULHAMEED
232 Objectives u To describe the indications for a composite crown on a primary incisor.to properly prepare a dentoform tooth for a composite crown.to properly adapt a crown form and to restore a dentoform tooth.
233 Restoration of Class IV Caries in Primary Anterior Teeth u u u u Esthetic Resin Restoration Stainless Steel Crown Open-Face Steel Crowns Composite Crowns

234 Anterior Stainless Steel Crowns u Esthetics - poor u Durability - very good u Time for placement - fastest u Selection criteria - severely decayed, esthetics of minimal importance, gingival hemorrhage not controlled, inadequate patient cooperation

235 Open Faced Stainless Steel Crown u Esthetics - okay u Durability - good, although facing may be dislodgedtime for placement - takes longest to place due to two-step procedureselection criteria - severely decayed teeth, durabilty needed, esthetics are a concern
 of the tooth s incisal edge, or by direct")
236 Crown Form Selection u Select the appropriate crown form size from the mesio-distal measurement (mm) of the tooth s incisal edge, or by direct comparison
237 Tooth Preparation u Incisal reduction mm u Proximal reduction - parallel mesial and distal slices to break contact with the adjacent tooth and to allow enough bulk to give strength to the final restoration.5-1 mm

238 Utilize a fine diamond or a 699
239 Tooth Preparation u Buccal reduction - to allow the placement of the restoration within the normal buccal lingual width of the tooth restored.5-1 mm u Lingual reduction - to allow for the necessary bulk for the strength of the crown and to prevent for any occlusal interferences

240 Buccal Reduction

241 Lingual Reduction

242 Circumfrential Undercut Shoulder u Terminates at the crest of the gingiva u Shoulder depth should be.75-1 mm u Use inverted cone
243 Variation Cervical undercut on facial only Removal of caries may also provide undercuts

244 Crown Adaptation u Carefully trim off the cervical collar with curved festooning scissorstrim crown form so that when seated, it covers the shoulder but extends no more than 1 mm past tge shoulder

245 Trial Fitting of Crown Form u Try on trimmed crown form Incisal edges should line up Place hole in incisal edge of crown with an explorer to allow vent for composite to flow through during crown placement

246 Crown Placement u Etch tooth with phosphoric acid for 30 seconds u Thoroughly wash and dry etched surface u Apply bonding agent according to specifications

247 Crown Placement u Carefully pack the crown form resin to avoid entrapment of air bubbles

248 u u Position the filled crown form over the prepared tooth so it extends 1mm over the gingival marginremove excess resin from margins with an explorer before polymerizing Slice crown form

249 Minimal Finishing and Polishing u u u u Peel it away from composite crown Finish margins Adjust occlusion DO NOT FINISH the labial surface polymerization of the resin against the plastic provides the smoothest and most stain resistant surface

250
Stainless Steel Crowns
 Stainless Steel Crowns Objectives Indications for use of stainless steel crowns Technique used in preparing and placing a stainless steel crown restoration on a primary molar. Indications for SSC Restoration
Stainless Steel Crowns Objectives Indications for use of stainless steel crowns Technique used in preparing and placing a stainless steel crown restoration on a primary molar. Indications for SSC Restoration
Essentials of. Dental Assisting. Edition 6. Debbie S. Robinson Doni L. Bird
 Essentials of Dental Assisting Edition 6 Debbie S. Robinson Doni L. Bird CHAPTER21 Restorative Procedures http://evolve.elsevier.com/robinson/essentials/ LEARNING OBJECTIVES KEY TERMS 1. Pronounce, define,
Essentials of Dental Assisting Edition 6 Debbie S. Robinson Doni L. Bird CHAPTER21 Restorative Procedures http://evolve.elsevier.com/robinson/essentials/ LEARNING OBJECTIVES KEY TERMS 1. Pronounce, define,
Restorative Dentistry for the Primary Dentition. References : pinkham, chapter 21
 In The Name Of God Restorative Dentistry for the Primary Dentition References : pinkham, chapter 21 INSTRUMENTATION High speed Handpiece(100,000 to 300,000 rpm) Low speed handpiece(500 to 15,000 rpm) hand
In The Name Of God Restorative Dentistry for the Primary Dentition References : pinkham, chapter 21 INSTRUMENTATION High speed Handpiece(100,000 to 300,000 rpm) Low speed handpiece(500 to 15,000 rpm) hand
Lec. 3-4 Dr. Saif Alarab Clinical Technique for Class I Amalgam Restorations The outline form
 Lec. 3-4 Dr. Saif Alarab Clinical Technique for Class I Amalgam Restorations Class I refers to -Restorations on the occlusal surfaces of posterior teeth, - The occlusal two thirds of facial and lingual
Lec. 3-4 Dr. Saif Alarab Clinical Technique for Class I Amalgam Restorations Class I refers to -Restorations on the occlusal surfaces of posterior teeth, - The occlusal two thirds of facial and lingual
Indications The selection of amalgam as a restorative material for class V cavity should involve the following considerations:
 1 Lec.7 د.عبد املنعم اخلفاجي CLASS V CAVITY PREPARATION FOR AMAGLAM Indications The selection of amalgam as a restorative material for class V cavity should involve the following considerations: 1- Caries:
1 Lec.7 د.عبد املنعم اخلفاجي CLASS V CAVITY PREPARATION FOR AMAGLAM Indications The selection of amalgam as a restorative material for class V cavity should involve the following considerations: 1- Caries:
CLASS II CAVITY PREPARATION CHARACTERISTICS OF AN IDEAL CLASS II
 CLASS II CAVITY PREPARATION CHARACTERISTICS OF AN IDEAL CLASS II Contact area carious lesion Proximal view Vertical section - Buccal view Class II carious lesions are diagnosed using bitewing radiographs.
CLASS II CAVITY PREPARATION CHARACTERISTICS OF AN IDEAL CLASS II Contact area carious lesion Proximal view Vertical section - Buccal view Class II carious lesions are diagnosed using bitewing radiographs.
Cutting instruments. Instruments
 Instruments أﻧﺲ اﻟﻌﺒﯿﺪي. د The removal and shaping of tooth structure are essential aspects of restorative dentistry. Initially this was a difficult process accomplished entirely by the use of - Hand instruments.
Instruments أﻧﺲ اﻟﻌﺒﯿﺪي. د The removal and shaping of tooth structure are essential aspects of restorative dentistry. Initially this was a difficult process accomplished entirely by the use of - Hand instruments.
أ.م. هدى عباس عبد اهلل CROWN AND BRIDGE جامعة تكريت كلية. Lec. (2) طب االسنان
 طب االسنان") Lec. (2) CROWN AND BRIDGE أ.م. هدى عباس عبد اهلل Patient selection and examination A thorough diagnosis must first be made of the patient's dental condition, considering both hard and soft tissues. this
Lec. (2) CROWN AND BRIDGE أ.م. هدى عباس عبد اهلل Patient selection and examination A thorough diagnosis must first be made of the patient's dental condition, considering both hard and soft tissues. this
M. Molitor REMOVAL OF ORTHODONTIC BANDS AND CEMENT REMOVAL WITH A HAND INSTRUMENT
 M. Molitor REMOVAL OF ORTHODONTIC BANDS AND CEMENT REMOVAL WITH A HAND INSTRUMENT REMOVAL OF ORTHODONTIC BANDS AND CEMENT REMOVAL WITH A HAND INSTRUMENT COURSE OUTLINE, ACTIVITIES AND HOUR BREAKDOWN 1.
M. Molitor REMOVAL OF ORTHODONTIC BANDS AND CEMENT REMOVAL WITH A HAND INSTRUMENT REMOVAL OF ORTHODONTIC BANDS AND CEMENT REMOVAL WITH A HAND INSTRUMENT COURSE OUTLINE, ACTIVITIES AND HOUR BREAKDOWN 1.
BOCL-01: Bonding Materials Checklist
 Task 19: Gather materials to bond partner using toothpaste as etchant Take a photo of gathered materials and submit with this completed checklist BOCL-01: Bonding Materials Checklist Date: Patient: Operator:
Task 19: Gather materials to bond partner using toothpaste as etchant Take a photo of gathered materials and submit with this completed checklist BOCL-01: Bonding Materials Checklist Date: Patient: Operator:
Operative dentistry. Lec: 10. Zinc oxide eugenol (ZOE):
:") Operative dentistry Lec: 10 د.عبذالمنعم الخفاجي Zinc oxide eugenol (ZOE): There are 2 types: 1) Unreinforced ZOE (ordinary type): supplied as powder (zinc oxide + some additives like zinc acetate, white
Operative dentistry Lec: 10 د.عبذالمنعم الخفاجي Zinc oxide eugenol (ZOE): There are 2 types: 1) Unreinforced ZOE (ordinary type): supplied as powder (zinc oxide + some additives like zinc acetate, white
روپ قداص رتکد ناشخرد یاھدادعتسا رتفد
 CLASS II (pp 658-664 664, 696-708 708) دکتر صادق پور دفتر استعدادھای درخشان Seven Steps of Cavity Preparation 1) Establish the outline form 2) Establish resistance form 3) Establish retention form 4) Provide
CLASS II (pp 658-664 664, 696-708 708) دکتر صادق پور دفتر استعدادھای درخشان Seven Steps of Cavity Preparation 1) Establish the outline form 2) Establish resistance form 3) Establish retention form 4) Provide
ORTHODONTIC BANDING AND CEMENTATION. Materials
 ORTHODONTIC BANDING AND CEMENTATION Materials Required Materials for fitting bands: 1. Selection of bands of different sizes for the teeth to which you are fitting bands 2. Tweezers to take the bands out
ORTHODONTIC BANDING AND CEMENTATION Materials Required Materials for fitting bands: 1. Selection of bands of different sizes for the teeth to which you are fitting bands 2. Tweezers to take the bands out
CLASS II AMALGAM RESTORATIONS. Amalgam restorations that restore one or both of the proximal surfaces of the tooth
 CLASS II AMALGAM RESTORATIONS Amalgam restorations that restore one or both of the proximal surfaces of the tooth Initial Tooth Preparation Occlusal outline form (occlusal step).the occlusal outline form
CLASS II AMALGAM RESTORATIONS Amalgam restorations that restore one or both of the proximal surfaces of the tooth Initial Tooth Preparation Occlusal outline form (occlusal step).the occlusal outline form
Part II National Board Review Operative Dentistry. Module 3D General Questions Answers in BOLD (usually the first answer)
") Part II National Board Review Operative Dentistry Module 3D General Questions Answers in BOLD (usually the first answer) Howard E. Strassler, DMD University of Maryland Dental School With special acknowledgements
Part II National Board Review Operative Dentistry Module 3D General Questions Answers in BOLD (usually the first answer) Howard E. Strassler, DMD University of Maryland Dental School With special acknowledgements
Fundamental & Preventive Curvatures of Teeth and Tooth Development. Lecture Three Chapter 15 Continued; Chapter 6 (parts) Dr. Margaret L.
 Dr. Margaret L.") Fundamental & Preventive Curvatures of Teeth and Tooth Development Lecture Three Chapter 15 Continued; Chapter 6 (parts) Dr. Margaret L. Dennis Proximal contact areas Contact areas are on the mesial and
Fundamental & Preventive Curvatures of Teeth and Tooth Development Lecture Three Chapter 15 Continued; Chapter 6 (parts) Dr. Margaret L. Dennis Proximal contact areas Contact areas are on the mesial and
Dr.Adel F.Ibraheem Partial Veneer Crown(Three quarter crown) Three quarter (¾ )crown: Uses: Indications ---- For posterior teeth ;
 Three quarter (¾ )crown: Uses: Indications ---- For posterior teeth ;") Lecture.9 Dr.Adel F.Ibraheem Partial Veneer Crown(Three quarter crown) *It is a cast metal crown restoration that cover only a part of the clinical crown, most commonly used type of partial veneer crown
Lecture.9 Dr.Adel F.Ibraheem Partial Veneer Crown(Three quarter crown) *It is a cast metal crown restoration that cover only a part of the clinical crown, most commonly used type of partial veneer crown
Primary Teeth Chapter 18. Dental Anatomy 2016
 Primary Teeth Chapter 18 Dental Anatomy 2016 Primary Teeth - Introduction Synonyms deciduous teeth, baby teeth, temporary teeth, milk teeth. There are 20 primary teeth, designated as A thru T in the Universal
Primary Teeth Chapter 18 Dental Anatomy 2016 Primary Teeth - Introduction Synonyms deciduous teeth, baby teeth, temporary teeth, milk teeth. There are 20 primary teeth, designated as A thru T in the Universal
Fuji II LC. A Perfect Choice
 A Perfect Choice is a remarkable restorative material The world s first resin-reinforced glass ionomer has remained the benchmark for light cured glass ionomer cements, delivering more than 15 years of
A Perfect Choice is a remarkable restorative material The world s first resin-reinforced glass ionomer has remained the benchmark for light cured glass ionomer cements, delivering more than 15 years of
DH220 Dental Materials
 DH220 Dental Materials Lecture #5 Prof. Lamanna RDH, MS Restorative Dentistry: Glass Ionomer Bird & Robinson p.740-741 I. Use Liner Base Luting agent Restorative material: Class III, V, & eroded/abraded
DH220 Dental Materials Lecture #5 Prof. Lamanna RDH, MS Restorative Dentistry: Glass Ionomer Bird & Robinson p.740-741 I. Use Liner Base Luting agent Restorative material: Class III, V, & eroded/abraded
Preparation and making fillings Class V., III., IV.
 Preparation and making fillings Class V., III., IV. Class V. Cervical defects - Dental caries - Non carious lesions (erosion, abrasion, V shaped defects) Types of defects Caries Erosion Abrasion V shaped
Preparation and making fillings Class V., III., IV. Class V. Cervical defects - Dental caries - Non carious lesions (erosion, abrasion, V shaped defects) Types of defects Caries Erosion Abrasion V shaped
riva helping you help your patients
 riva helping you help your patients what is a glass ionomer? how will a dentist benefit from using glass ionomers? how will a patient benefit from their glass ionomer? Glass ionomer is the generic name
riva helping you help your patients what is a glass ionomer? how will a dentist benefit from using glass ionomers? how will a patient benefit from their glass ionomer? Glass ionomer is the generic name
General dentists in private practice place numerous
 PROACTIVE INTERVENTION DENTISTRY Incorporating Glass Ionomers into Everyday Dental Practice Todd Snyder, DDS, FAACD, FIADFE Introduction General dentists in private practice place numerous direct tooth
PROACTIVE INTERVENTION DENTISTRY Incorporating Glass Ionomers into Everyday Dental Practice Todd Snyder, DDS, FAACD, FIADFE Introduction General dentists in private practice place numerous direct tooth
Protemp Crown Temporization Material
 Clinical Case Studies Introduction from 3M ESPE is the world s first preformed, malleable temporary crown, providing speed and simplicity in temporization like never before. With this revolutionary light-curable
Clinical Case Studies Introduction from 3M ESPE is the world s first preformed, malleable temporary crown, providing speed and simplicity in temporization like never before. With this revolutionary light-curable
For the Perfect Class V and All Cervical Area Gingival Margins when Placing Direct Composites, Create an Injection Molding Matrix
 Cronicon OPEN ACCESS EC DENTAL SCIENCE Case Report For the Perfect Class V and All Cervical Area Gingival Margins when Placing Direct Composites, Create an Injection Molding Paul C Belvedere* Adjunct Professor,
Cronicon OPEN ACCESS EC DENTAL SCIENCE Case Report For the Perfect Class V and All Cervical Area Gingival Margins when Placing Direct Composites, Create an Injection Molding Paul C Belvedere* Adjunct Professor,
Advancing the Art of Freehand Cosmetic Contouring
 Advancing the Art of Freehand Cosmetic Goldfogel Instruments Goldfogel XTS Instruments Goldfogel Anterior Instruments Created by Dr. Michael Goldfogel, the XTS Instruments represent an important step forward
Advancing the Art of Freehand Cosmetic Goldfogel Instruments Goldfogel XTS Instruments Goldfogel Anterior Instruments Created by Dr. Michael Goldfogel, the XTS Instruments represent an important step forward
Direct composite restorations for large posterior cavities extended range of applications for high-performance materials
 Direct composite restorations for large posterior cavities extended range of applications for high-performance materials A case study by Ann-Christin Meier, Dr. med. dent., Stapelfeld, Germany When large
Direct composite restorations for large posterior cavities extended range of applications for high-performance materials A case study by Ann-Christin Meier, Dr. med. dent., Stapelfeld, Germany When large
Filtek LS Low Shrink Posterior Restorative System Case 1: Cusp build-up
 Case 1 This case study focuses on the restoration of an upper molar. Filtek LS Low Shrink Posterior Restorative System Case 1: Cusp build-up The existing, inadequate restoration led to the development
Case 1 This case study focuses on the restoration of an upper molar. Filtek LS Low Shrink Posterior Restorative System Case 1: Cusp build-up The existing, inadequate restoration led to the development
CLASS II AMALGAM RESTORATION 36MO
 INTERNATIONAL PEER REVIEW CLASS II AMALGAM RESTORATION 36MO Leung Kwan Yu, Steve BDS II - Class 2019, The University of Hong Kong instruments Mirror Periodontal probe Hatchets Gingival margin trimmers
INTERNATIONAL PEER REVIEW CLASS II AMALGAM RESTORATION 36MO Leung Kwan Yu, Steve BDS II - Class 2019, The University of Hong Kong instruments Mirror Periodontal probe Hatchets Gingival margin trimmers
Hands-on Posterior Tooth Preparation. Practical Skills Courses, SWL, 25/11/2016
 Hands-on Posterior Tooth Preparation Practical Skills Courses, SWL, 25/11/2016 Hands-On Didactic Teaching A Tooth-Friendly-Approach - Hands-on Tooth Preparation Course - Dental Simulation to include: Posterior
Hands-on Posterior Tooth Preparation Practical Skills Courses, SWL, 25/11/2016 Hands-On Didactic Teaching A Tooth-Friendly-Approach - Hands-on Tooth Preparation Course - Dental Simulation to include: Posterior
Dr.Zainab. second. step): The. proximal
: The. proximal") Class II Amalgam Restorations Dr.Zainab This section introduces the principles and techniques of a Class II tooth preparation for an amalgam restoration involving a carious lesion on one proximal surface.
Class II Amalgam Restorations Dr.Zainab This section introduces the principles and techniques of a Class II tooth preparation for an amalgam restoration involving a carious lesion on one proximal surface.
Arrangement of the artificial teeth:
 Lecture Prosthodontic Dr. Osama Arrangement of the artificial teeth: It s the placement of the teeth on a denture with definite objective in mind or it s the setting of teeth on temporary bases. Rules
Lecture Prosthodontic Dr. Osama Arrangement of the artificial teeth: It s the placement of the teeth on a denture with definite objective in mind or it s the setting of teeth on temporary bases. Rules
IFURH0017.V04 NOV2017 INSTRUCTIONS FOR USE CLINICAL PROCEDURE
 IFURH0017.V04 NOV2017 H Y B R I D INSTRUCTIONS FOR USE CLINICAL PROCEDURE OVC PROCEDURE 1. OVC Selection Determine the mesial-distal (M-D) distance of the affected tooth using the appropriate Selector
IFURH0017.V04 NOV2017 H Y B R I D INSTRUCTIONS FOR USE CLINICAL PROCEDURE OVC PROCEDURE 1. OVC Selection Determine the mesial-distal (M-D) distance of the affected tooth using the appropriate Selector
Clinical report. Drs Paul and Alexandre MIARA and F. CONNOLLY COMPOSITE POSTERIOR FILLINGS. How to control. layering? 8 - Dentoscope n 124
 COMPOSITE POSTERIOR FILLINGS How to control layering? 8 - Dentoscope n 124 CV FLASH Dr Paul MIARA Dental surgeon Dr Alexandre MIARA Dental surgeon Dr F. CONNOLLY Dental surgeon Thanks to continuous improvements
COMPOSITE POSTERIOR FILLINGS How to control layering? 8 - Dentoscope n 124 CV FLASH Dr Paul MIARA Dental surgeon Dr Alexandre MIARA Dental surgeon Dr F. CONNOLLY Dental surgeon Thanks to continuous improvements
Lecture 2 Maxillary central incisor
 Lecture 2 Maxillary central incisor Generally The deciduous tooth appears in the mouth at 3 18 months of age, with 6 months being the average and is replaced by the permanent tooth around 7 8 years of
Lecture 2 Maxillary central incisor Generally The deciduous tooth appears in the mouth at 3 18 months of age, with 6 months being the average and is replaced by the permanent tooth around 7 8 years of
ASSIGNMENT 16. Book Assignment: Operative Dentistry, pages 16-1 to 16-33
 ASSIGNMENT 16 Book Assignment: Operative Dentistry, pages 16-1 to 16-33 16-1. Operative dentistry is concerned with the prevention and treatment of defects of what tooth surfaces? 1. Enamel and cementum
ASSIGNMENT 16 Book Assignment: Operative Dentistry, pages 16-1 to 16-33 16-1. Operative dentistry is concerned with the prevention and treatment of defects of what tooth surfaces? 1. Enamel and cementum
INDICATIONS. Fixed Appliances are indicated when precise tooth movements are required
 DEFINITION Fixed Appliances are devices or equipments that are attached to the teeth, cannot be removed by the patient and are capable of causing tooth movement. INDICATIONS Fixed Appliances are indicated
DEFINITION Fixed Appliances are devices or equipments that are attached to the teeth, cannot be removed by the patient and are capable of causing tooth movement. INDICATIONS Fixed Appliances are indicated
Class I Cavity Preparation. Alaa Sabrah, BDS, MSD, PhD Nov,
 بسم اهلل الرحمن الرحيم Class I Cavity Preparation Alaa Sabrah, BDS, MSD, PhD Nov, 2015 15 Goals and Objectives?Define class I carious lesion.1 Describe the clinical technique for treating class I?carious
بسم اهلل الرحمن الرحيم Class I Cavity Preparation Alaa Sabrah, BDS, MSD, PhD Nov, 2015 15 Goals and Objectives?Define class I carious lesion.1 Describe the clinical technique for treating class I?carious
Contouring vs. Orthodontics. Contouring to Eliminate Fractures and Enhance Proportions
 Contouring vs. Orthodontics Photo 1 Maxillary central incisors are overlapped. Patient chose rapid tooth movement instead of contouring. Photo 2 Maxillary central incisors after six months of orthodontic
Contouring vs. Orthodontics Photo 1 Maxillary central incisors are overlapped. Patient chose rapid tooth movement instead of contouring. Photo 2 Maxillary central incisors after six months of orthodontic
Pulpal Protection: bases, liners, sealers, caries control Module D: Pulp capping-caries control
 Readings: Fundamentals of Operative Dentistry, 3 nd Edition; Summitt, et al Chapters 5, 6 and 8 Pulpal Protection: bases, liners, sealers, caries control Module D: Pulp capping-caries control REST 528A
Readings: Fundamentals of Operative Dentistry, 3 nd Edition; Summitt, et al Chapters 5, 6 and 8 Pulpal Protection: bases, liners, sealers, caries control Module D: Pulp capping-caries control REST 528A
stabilisation and surface protection
 Guiding the way to caries stabilisation and surface protection Fissure sealing MI restorations Pulp capping Hypersensitivity Protection Caries stabilisation Fuji Triage from GC. Temporary restorations
Guiding the way to caries stabilisation and surface protection Fissure sealing MI restorations Pulp capping Hypersensitivity Protection Caries stabilisation Fuji Triage from GC. Temporary restorations
MemRx Orthodontic Appliances
 MemRx Orthodontic Appliances Uses and Instructions The MemRx Fundamentals As the need for faster, more efficient treatment of non-compliant patients increases, orthodontic!technology and materials has
MemRx Orthodontic Appliances Uses and Instructions The MemRx Fundamentals As the need for faster, more efficient treatment of non-compliant patients increases, orthodontic!technology and materials has
DENTAL MATERIALS STUDY GUIDE
 DENTAL MATERIALS STUDY GUIDE WORKSHEET Dentalelle Tutoring www.dentalelle.com Study Guide for Dental Materials Dentalelle Tutoring 1. When completing a large composite restoration, how should the composite
DENTAL MATERIALS STUDY GUIDE WORKSHEET Dentalelle Tutoring www.dentalelle.com Study Guide for Dental Materials Dentalelle Tutoring 1. When completing a large composite restoration, how should the composite
EQUIA. Self-Adhesive, Bulk Fill, Rapid Restorative System
 EQUIA EQUIA Fil EQUIA Coat + Self-Adhesive, Bulk Fill, Rapid Restorative System From the World Leader in Glass Ionomer Technology - A Complete Glass Ionomer Based Bulk Fill Rapid Restorative System Class
EQUIA EQUIA Fil EQUIA Coat + Self-Adhesive, Bulk Fill, Rapid Restorative System From the World Leader in Glass Ionomer Technology - A Complete Glass Ionomer Based Bulk Fill Rapid Restorative System Class
SURVEYING OF REMOVABLE PARITAL DENTURES FEB, 11, 2015
 SURVEYING OF REMOVABLE PARITAL DENTURES FEB, 11, 2015 Dental Surveyor: It is a mechanical device used to determine the relative parallelism of the teeth surfaces and the undercuts areas in relation to
SURVEYING OF REMOVABLE PARITAL DENTURES FEB, 11, 2015 Dental Surveyor: It is a mechanical device used to determine the relative parallelism of the teeth surfaces and the undercuts areas in relation to
Press Release. Press Contact. The concept for Class II restoration Delicate preparation, rapid procedure and reliable results
 Press Release The concept for Class II restoration Delicate preparation, rapid procedure and reliable results by Dr. Arzu Tuna and Dr. Umut Baysal, Attendorn, Germany Composite restorations have always
Press Release The concept for Class II restoration Delicate preparation, rapid procedure and reliable results by Dr. Arzu Tuna and Dr. Umut Baysal, Attendorn, Germany Composite restorations have always
SPACE MAINTAINER. Multimedia Health Education. Disclaimer
 Disclaimer This movie is an educational resource only and should not be used to manage your health. All decisions about the management of premature loss of primary teeth and use of space maintainers must
Disclaimer This movie is an educational resource only and should not be used to manage your health. All decisions about the management of premature loss of primary teeth and use of space maintainers must
ARAB AMERICAN UNIVERSITY. Lab. Manual. Prosthetic Dentistry1; Removable Prosthodontics. 3 rd year
 ARAB AMERICAN UNIVERSITY Lab. Manual Prosthetic Dentistry1; Removable Prosthodontics 3 rd year Department of Fixed and removable prosthetic Dentistry Faculty of Dentistry 2012/2013 Course Instructor Dr.
ARAB AMERICAN UNIVERSITY Lab. Manual Prosthetic Dentistry1; Removable Prosthodontics 3 rd year Department of Fixed and removable prosthetic Dentistry Faculty of Dentistry 2012/2013 Course Instructor Dr.
1. What is the highest and sharpest cusp on the lower first deciduous molar? 2. Which of the following is NOT the correct location of an embrasure?
 1 1. What is the highest and sharpest cusp on the lower first deciduous molar? a. mesiobuccal b. distobuccal c. distolingual d.mesiolingual 2. Which of the following is NOT the correct location of an embrasure?
1 1. What is the highest and sharpest cusp on the lower first deciduous molar? a. mesiobuccal b. distobuccal c. distolingual d.mesiolingual 2. Which of the following is NOT the correct location of an embrasure?
Device Technical File
 Device Technical File ContactPro Matrix System Instructions for Use 1.0 Product Description A. For placement of restorations in the posterior area of the oral cavity, the Microbrush ContactPro Sectional
Device Technical File ContactPro Matrix System Instructions for Use 1.0 Product Description A. For placement of restorations in the posterior area of the oral cavity, the Microbrush ContactPro Sectional
Efficient Bonding Protocol for the Insignia Custom Bracket System
 Efficient Bonding Protocol for the Insignia Custom Bracket System Abstract The Insignia appliance is reverse-engineered from a digital set-up of the prescribed dental alignment. Each bracket configuration,
Efficient Bonding Protocol for the Insignia Custom Bracket System Abstract The Insignia appliance is reverse-engineered from a digital set-up of the prescribed dental alignment. Each bracket configuration,
Principles of. By: Dr. Ahmad Rabah
 Principles of By: Dr. Ahmad Rabah 1. Utilize what's present: Whenever possible, select a design that fits the teeth and soft tissues, rather than choosing one that requires tissue alteration. When minimal
Principles of By: Dr. Ahmad Rabah 1. Utilize what's present: Whenever possible, select a design that fits the teeth and soft tissues, rather than choosing one that requires tissue alteration. When minimal
FIVE THINGS YOU NEED TO KNOW ABOUT GLASS IONOMERS
 FIVE THINGS YOU NEED TO KNOW ABOUT GLASS IONOMERS FIVE THINGS YOU NEED TO KNOW ABOUT GLASS IONOMERS Glass Ionomers Solve Clinicians Quandaries Amalgam fillings have been around for almost two centuries,
FIVE THINGS YOU NEED TO KNOW ABOUT GLASS IONOMERS FIVE THINGS YOU NEED TO KNOW ABOUT GLASS IONOMERS Glass Ionomers Solve Clinicians Quandaries Amalgam fillings have been around for almost two centuries,
Central Incisor DR.Ahmed Al-Jobory B.D.S.,M.Sc. Conservative Department
 Dental Anatomy Lecture 3 Central Incisor DR.Ahmed Al-Jobory B.D.S.,M.Sc. Conservative Department The permanent maxillary Incisors Maxillary incisor are four in number. The maxillary central incisor is
Dental Anatomy Lecture 3 Central Incisor DR.Ahmed Al-Jobory B.D.S.,M.Sc. Conservative Department The permanent maxillary Incisors Maxillary incisor are four in number. The maxillary central incisor is
PRE-FINISHER APPLIANCE AND BONDABLE LINGUAL RETAINERS. tportho.com cosmeticbraces.com. POD_TPOC_09_PreFinisher_Retainers_2015, Rev.
 9 PRE-FINISHER APPLIANCE AND BONDABLE LINGUAL RETAINERS tportho.com cosmeticbraces.com POD_TPOC_09_PreFinisher_Retainers_2015, Rev. 0 PRE-FINISHER APPLIANCE AND BONDABLE LINGUAL RETAINERS Pre-Finisher
9 PRE-FINISHER APPLIANCE AND BONDABLE LINGUAL RETAINERS tportho.com cosmeticbraces.com POD_TPOC_09_PreFinisher_Retainers_2015, Rev. 0 PRE-FINISHER APPLIANCE AND BONDABLE LINGUAL RETAINERS Pre-Finisher
Key points for starting off
 Key points for starting off First off, the five questions to ask yourself about a loose tooth before identifying it are: 1. 2. 3. 4. 5. Category (incisor, canine, premolar or molar)? Permanent or deciduous?
Key points for starting off First off, the five questions to ask yourself about a loose tooth before identifying it are: 1. 2. 3. 4. 5. Category (incisor, canine, premolar or molar)? Permanent or deciduous?
Detailed Step-by Step Instruction for Chairside Splinting
 Dentapreg TM Splint - Procedures Basic Procedures in Short Splinting with Dentapreg TM strip always includes several basic procedures repeated in all particular clinical situations: (A) Clean the bonding
Dentapreg TM Splint - Procedures Basic Procedures in Short Splinting with Dentapreg TM strip always includes several basic procedures repeated in all particular clinical situations: (A) Clean the bonding
6610 NE 181st Street, Suite #1, Kenmore, WA
 660 NE 8st Street, Suite #, Kenmore, WA 9808 www.northshoredentalacademy.com.08.900 READ CHAPTER The Professional Dental Assistant (p.-9) No Key Terms Recall Questions:,,,, and 6 CLASS SYLLABUS DAY READ
660 NE 8st Street, Suite #, Kenmore, WA 9808 www.northshoredentalacademy.com.08.900 READ CHAPTER The Professional Dental Assistant (p.-9) No Key Terms Recall Questions:,,,, and 6 CLASS SYLLABUS DAY READ
The width of the MCXL step bur is 1.4 mm wide and has a blunt end. As the bur approaches the inside of
 As I teach first year dental students how to prep a tooth for a full gold crown, get an impression, pour and mount models, wax-up, cast and polish, they are almost always amazed at all the required steps
As I teach first year dental students how to prep a tooth for a full gold crown, get an impression, pour and mount models, wax-up, cast and polish, they are almost always amazed at all the required steps
Lec11 يجافخلا معنملاذبع د 0 Dental Amalgam:- Advantages:- Disadvantages:- Composition: -
 Operative dentistry Lec11 د 0 عبذالمنعم الخفاجي Dental Amalgam:-Is a union of mercury (liquid) with amalgam alloys (powder) to give a plastic mass, which, hardens in the cavity. Amalgam alloy:- Is a combination
Operative dentistry Lec11 د 0 عبذالمنعم الخفاجي Dental Amalgam:-Is a union of mercury (liquid) with amalgam alloys (powder) to give a plastic mass, which, hardens in the cavity. Amalgam alloy:- Is a combination
Morphology of an Anatomic Crown. By: Assistant Professor Dr. Baydaa Ali Al - Rawi
 Morphology of an Anatomic Crown By: Assistant Professor Dr. Baydaa Ali Al - Rawi October 4, 2009 Elevated landmarks Depressed landmarks A) Elevated landmarks : 1. Dental lobe : is one of the primary centers
Morphology of an Anatomic Crown By: Assistant Professor Dr. Baydaa Ali Al - Rawi October 4, 2009 Elevated landmarks Depressed landmarks A) Elevated landmarks : 1. Dental lobe : is one of the primary centers
PH-04A: Clinical Photography Production Checklist With A Small Camera
 PH-04A: Clinical Photography Production Checklist With A Small Camera Operator Name Total 0-49, Passing 39 Your Score Patient Name Date of Series Instructions: Evaluate your Series of photographs first.
PH-04A: Clinical Photography Production Checklist With A Small Camera Operator Name Total 0-49, Passing 39 Your Score Patient Name Date of Series Instructions: Evaluate your Series of photographs first.
Restoration of the worn dentition
 Clin Dent Rev (2017) 1:4 https://doi.org/10.1007/s41894-017-0003-3 TREATMENT Restoration of the worn dentition Paul King 1 Received: 16 March 2017 / Accepted: 31 May 2017 / Published online: 30 June 2017
Clin Dent Rev (2017) 1:4 https://doi.org/10.1007/s41894-017-0003-3 TREATMENT Restoration of the worn dentition Paul King 1 Received: 16 March 2017 / Accepted: 31 May 2017 / Published online: 30 June 2017
Fixed Twin Blocks. Guidelines for case selection are similar to those for removable Twin Block appliances.
 Fixed Twin Blocks Development of Fixed Twin Blocks Dr Clark has enjoyed the cooperation of Dynaflex in developing the Fixed Twin Block. Six years of clinical testing has confirmed that this technique produces
Fixed Twin Blocks Development of Fixed Twin Blocks Dr Clark has enjoyed the cooperation of Dynaflex in developing the Fixed Twin Block. Six years of clinical testing has confirmed that this technique produces
Polycarbonate Crowns for Primary teeth Revisited. Restorative options, Technique & Case reports
 Polycarbonate Crowns for Primary teeth Revisited Restorative options, Technique & Case reports Karthik Venkataraghavan 1, John Chan 2 1 Pediatric Dentist, Vibha Dental Care Centre, Bangalore, India. 2
Polycarbonate Crowns for Primary teeth Revisited Restorative options, Technique & Case reports Karthik Venkataraghavan 1, John Chan 2 1 Pediatric Dentist, Vibha Dental Care Centre, Bangalore, India. 2
Dowel restorations Treatment with a post and core
 Dowel restorations Treatment with a post and core A post and core is a dental restoration used to sufficiently buildup tooth structure for future restoration with a crown when there is not enough tooth
Dowel restorations Treatment with a post and core A post and core is a dental restoration used to sufficiently buildup tooth structure for future restoration with a crown when there is not enough tooth
Metal-Free Restorations PROCEDURES FOR POSTERIOR DIRECT & SEMI-DIRECT COMPOSITE RESTORATIONS D I D I E R D I E T S C H I. For.
 PROCEDURES FOR POSTERIOR DIRECT & SEMI-DIRECT COMPOSITE RESTORATIONS Metal-Free Restorations D I D I E R D I E T S C H I The Geneva Smile Center D.M.D, PhD, Privat-Docent 2, Quai Gustave Ador 1207 Geneva
PROCEDURES FOR POSTERIOR DIRECT & SEMI-DIRECT COMPOSITE RESTORATIONS Metal-Free Restorations D I D I E R D I E T S C H I The Geneva Smile Center D.M.D, PhD, Privat-Docent 2, Quai Gustave Ador 1207 Geneva
Control the Environment. Control Dentistry. isolitesystems.com
 Control the Environment. Control Dentistry. isolitesystems.com 866-584-0469 Total Control of the Oral Environment. Increase Productivity Improves clinical outcomes with consistent results. Frees assistants
Control the Environment. Control Dentistry. isolitesystems.com 866-584-0469 Total Control of the Oral Environment. Increase Productivity Improves clinical outcomes with consistent results. Frees assistants
Jet Carbides. Enduring esthetics. Effortless efficiency. Precisely.
 Jet Carbides Enduring esthetics. Effortless efficiency. Precisely. Your practice inspires Kerr to bring the highest quality, most innovative products to the dental community. Shank Type Code Shank Type
Jet Carbides Enduring esthetics. Effortless efficiency. Precisely. Your practice inspires Kerr to bring the highest quality, most innovative products to the dental community. Shank Type Code Shank Type
Prosthetic Options in Implant Dentistry. Hakimeh Siadat, DDS, MSc Associate Professor
 Prosthetic Options in Dentistry Hakimeh Siadat, DDS, MSc Associate Professor Dental Research Center, Department of Prosthodontics & Dental s Faculty of Dentistry, Tehran University of Medical Sciences
Prosthetic Options in Dentistry Hakimeh Siadat, DDS, MSc Associate Professor Dental Research Center, Department of Prosthodontics & Dental s Faculty of Dentistry, Tehran University of Medical Sciences
Indirect retainers. 1 i
 8 1 i Indirect retainers Factors Influencing Effectiveness Indirect Retainers Auxiliary Functions Indirect Retainers Forms Indirect Retainers Auxiliary occlusal rest Canine extensions fiom occlusal rests
8 1 i Indirect retainers Factors Influencing Effectiveness Indirect Retainers Auxiliary Functions Indirect Retainers Forms Indirect Retainers Auxiliary occlusal rest Canine extensions fiom occlusal rests
Preclinical Dentistry. I. Dental Caries Non carious lesions: trauma, erosion. abrasion, wedge shaped defects. Lenka Roubalíková
 Preclinical Dentistry I. Dental Caries Non carious lesions: trauma, erosion. abrasion, wedge shaped defects Lenka Roubalíková Understanding dental caries crown pulp chamber neck root canal root Dental
Preclinical Dentistry I. Dental Caries Non carious lesions: trauma, erosion. abrasion, wedge shaped defects Lenka Roubalíková Understanding dental caries crown pulp chamber neck root canal root Dental
DPI Luting Cement. DPI Restorative Cement
 DPI Luting Cement DPI Luting Cement is Type I glass ionomer white luting cement. DPI glass ionomers are remarkably biocompatible and can be safely used in deep cavities provided the pulp is not exposed,
DPI Luting Cement DPI Luting Cement is Type I glass ionomer white luting cement. DPI glass ionomers are remarkably biocompatible and can be safely used in deep cavities provided the pulp is not exposed,
UDELL DENTAL LABORATORY Instructions for Use PREAT Precision Attachments
 Indications Instructions The Locator Root Attachment is designed for use with overdentures or partial dentures, retained in whole or in part by endodontically treated roots in the mandibular or maxilla.
Indications Instructions The Locator Root Attachment is designed for use with overdentures or partial dentures, retained in whole or in part by endodontically treated roots in the mandibular or maxilla.
BASCD Trainers Pack for Caries Prevalence Studies. Updated: June 2014 for UK Training & Calibration exercise for the Deciduous Dentition
 BASCD Trainers Pack for Caries Prevalence Studies Updated: June 2014 for UK Training & Calibration exercise for the Deciduous Dentition Prepared by Helen Paisley, Cynthia Pine and Girvan Burnside Administrative
BASCD Trainers Pack for Caries Prevalence Studies Updated: June 2014 for UK Training & Calibration exercise for the Deciduous Dentition Prepared by Helen Paisley, Cynthia Pine and Girvan Burnside Administrative
Case Study. Case # 1 Author: Dr. Suheil Boutros (USA) 2013 Zimmer Dental, Inc. All rights reserved. 6557, Rev. 03/13.
 2013 Zimmer Dental, Inc. All rights reserved. 6557, Rev. 03/13.") Placement of a Zimmer Trabecular Metal Dental Implant with Simultaneous Ridge Augmentation and Immediate Non-Functional Loading Following Tooth Extraction and Orthodontic Treatment for Implant Site Development
Placement of a Zimmer Trabecular Metal Dental Implant with Simultaneous Ridge Augmentation and Immediate Non-Functional Loading Following Tooth Extraction and Orthodontic Treatment for Implant Site Development
Introduction to Layering with Filtek Supreme Plus Universal Restorative. Filtek. Supreme Plus Universal Restorative
 Introduction to Layering with Filtek Supreme Plus Universal Restorative Filtek Supreme Plus Universal Restorative Introduction to Layering with Filtek Supreme Plus Universal Restorative TM. Multishade
Introduction to Layering with Filtek Supreme Plus Universal Restorative Filtek Supreme Plus Universal Restorative Introduction to Layering with Filtek Supreme Plus Universal Restorative TM. Multishade
CLINICAL GUIDE CLINICAL GUIDE. by DR. NOBORU TAKAHASHI BY DR. NOBORU TAKAHASHI
 CLINICAL GUIDE by DR. NOBORU TAKAHASHI CLINICAL GUIDE BY DR. NOBORU TAKAHASHI Introduction Easy ESTELITE ASTERIA is developed to realize simplifi ed 2 step layering composite restorations as well as outstanding
CLINICAL GUIDE by DR. NOBORU TAKAHASHI CLINICAL GUIDE BY DR. NOBORU TAKAHASHI Introduction Easy ESTELITE ASTERIA is developed to realize simplifi ed 2 step layering composite restorations as well as outstanding
Amalgam restoration of posterior proximal cavities with deep and concave gingival outlines
 Amalgam restoration of posterior proximal cavities with deep and concave gingival outlines M. Darveniza, MDSc, FRACDS* Abstract A technique for making a matrix and wedges for amalgam restoration of deep
Amalgam restoration of posterior proximal cavities with deep and concave gingival outlines M. Darveniza, MDSc, FRACDS* Abstract A technique for making a matrix and wedges for amalgam restoration of deep
Table of Contents Section 6 Table of Contents
 Table of Contents Section 6 Table of Contents bands and attachments 6 3M Victory Series First Molar Bands... 6.2 3M Victory Series Second Molar Bands... 6.6 3M Unitek General Purpose Molar Bands... 6.10
Table of Contents Section 6 Table of Contents bands and attachments 6 3M Victory Series First Molar Bands... 6.2 3M Victory Series Second Molar Bands... 6.6 3M Unitek General Purpose Molar Bands... 6.10
CAD/CAM PREPARATION GUIDELINES & TISSUE MANAGEMENT TECHNIQUES RECOMMENDATIONS FOR OPTIMAL SCANNING, DESIGNING, AND MILLING
 CAD/CAM PREPARATION GUIDELINES & TISSUE MANAGEMENT TECHNIQUES RECOMMENDATIONS FOR OPTIMAL SCANNING, DESIGNING, AND MILLING CROWN PREPARATION GUIDELINES IDEAL CROWN PREPARATIONS POSTERIOR RESTORATIONS Rounded
CAD/CAM PREPARATION GUIDELINES & TISSUE MANAGEMENT TECHNIQUES RECOMMENDATIONS FOR OPTIMAL SCANNING, DESIGNING, AND MILLING CROWN PREPARATION GUIDELINES IDEAL CROWN PREPARATIONS POSTERIOR RESTORATIONS Rounded
Core build-up using post systems
 Core build-up using post systems Dr. Gergely Pataky Department of Conservative Dentistry What to speak about today General considerations Classification of post systems Dowel-core or fibre post? Biologic
Core build-up using post systems Dr. Gergely Pataky Department of Conservative Dentistry What to speak about today General considerations Classification of post systems Dowel-core or fibre post? Biologic
2. Gap closure and replacement of the missing tooth 35 with directly modelled bridge region 34-36
 GrandTEC Test Kit Dear User, This Test Kit has been put together to enable you to test GrandTEC on the model before using it in a clinical situation. GrandTEC is a resin-impregnated glass fibre strip.
GrandTEC Test Kit Dear User, This Test Kit has been put together to enable you to test GrandTEC on the model before using it in a clinical situation. GrandTEC is a resin-impregnated glass fibre strip.
No Prep And Minimal Prep Veneers
 Ajay Juneja No Prep And Minimal Prep Veneers 12 Apr 2016 It has been now an established entity for more then two decades since No Preparation Ceramic Veneers are being used. The very ideology of preserving
Ajay Juneja No Prep And Minimal Prep Veneers 12 Apr 2016 It has been now an established entity for more then two decades since No Preparation Ceramic Veneers are being used. The very ideology of preserving
Component parts of Chrome Cobalt Removable Partial Denture
 Lec. 5 د.بسام الطريحي Component parts of Chrome Cobalt Removable Partial Denture Major connectors: Are either bars or plates, the difference between them is in the amount of tissue covers. Plates are broad
Lec. 5 د.بسام الطريحي Component parts of Chrome Cobalt Removable Partial Denture Major connectors: Are either bars or plates, the difference between them is in the amount of tissue covers. Plates are broad
Occlusal Surface Management
 Occlusal Surface Management Sealant With Fluoride? Preventive Class I Resin Restoration Class I Glass Ionomer Primary Teeth Class I Composite Class I Amalgam PIT and FISSURE SEALANTS Contraindications
Occlusal Surface Management Sealant With Fluoride? Preventive Class I Resin Restoration Class I Glass Ionomer Primary Teeth Class I Composite Class I Amalgam PIT and FISSURE SEALANTS Contraindications
Principle Investigators: Overview of Study Methods: Dr. John Burgess Dr. Carlos Muñoz
 Principle Investigators: Dr. John Burgess Dr. Carlos Muñoz Overview of Study Methods: Subjects in need of Class I and/or Class II restorations were enrolled in two clinical trials conducted in US dental
Principle Investigators: Dr. John Burgess Dr. Carlos Muñoz Overview of Study Methods: Subjects in need of Class I and/or Class II restorations were enrolled in two clinical trials conducted in US dental
The Facts About Fillings
 The Facts About Fillings DENTAL BOARD OF CALIFORNIA 1432 Howe Avenue Sacramento, California 95825 www.dbc.ca.gov Dental Materials Fact Sheet What About the Safety of Filling Materials? Patient health and
The Facts About Fillings DENTAL BOARD OF CALIFORNIA 1432 Howe Avenue Sacramento, California 95825 www.dbc.ca.gov Dental Materials Fact Sheet What About the Safety of Filling Materials? Patient health and
Types of prostetic appliances Dr. Barbara Kispélyi
 Semmelweis University Faculty of Dentistry Department of Prosthodontics Types of prostetic appliances Dr. Barbara Kispélyi Types of prostetic appliances Types of the fixed prostetic appliances According
Semmelweis University Faculty of Dentistry Department of Prosthodontics Types of prostetic appliances Dr. Barbara Kispélyi Types of prostetic appliances Types of the fixed prostetic appliances According
For many years, patients with
 Dr. Robert Lowe is one of the great teachers in dentistry. Recently, he received the Gordon J. Christensen Award from the Chicago Dental Society in recognition of his excellence in teaching. Some of my
Dr. Robert Lowe is one of the great teachers in dentistry. Recently, he received the Gordon J. Christensen Award from the Chicago Dental Society in recognition of his excellence in teaching. Some of my
Dental Anatomy High Yield Notes. **Atleast 35 questions comes from these areas of old lectures**
 Dental Anatomy High Yield Notes **Atleast 35 questions comes from these areas of old lectures** This review notes compiled and prepared by my sister for her own study, as a last day review session for
Dental Anatomy High Yield Notes **Atleast 35 questions comes from these areas of old lectures** This review notes compiled and prepared by my sister for her own study, as a last day review session for
illustrated technique guide
 DENTSPLY Caulk 38 West Clarke Avenue Milford, DE 9963 www.dentsply.com www.caulk.com -302-422-45 In Canada call -800-263-437 illustrated technique guide Complete Luting System for: 2006 DENTSPLY International.
DENTSPLY Caulk 38 West Clarke Avenue Milford, DE 9963 www.dentsply.com www.caulk.com -302-422-45 In Canada call -800-263-437 illustrated technique guide Complete Luting System for: 2006 DENTSPLY International.
Management of ECC and Minimally Invasive Dentistry
 Management of ECC and Minimally Invasive Dentistry Ranbir Singh DMD MPH NYU-Lutheran Phoenix Pgy1 Pediatric Dental Resident Phoenix ECC Management Management of dental caries includes identification of
Management of ECC and Minimally Invasive Dentistry Ranbir Singh DMD MPH NYU-Lutheran Phoenix Pgy1 Pediatric Dental Resident Phoenix ECC Management Management of dental caries includes identification of
Filling materials are used to replace missing parts of the tooth.
 Filling materials are used to replace missing parts of the tooth. 1- Dental caries. 2- Trauma. 3- Abrasion. Parts of teeth which require replacement by restorative materials vary in size of cavity, shape,
Filling materials are used to replace missing parts of the tooth. 1- Dental caries. 2- Trauma. 3- Abrasion. Parts of teeth which require replacement by restorative materials vary in size of cavity, shape,
Fixed Partial Denture
 University of Minnesota School of Dentistry Fixed Partial Denture Self-guided Instructional Material for Dental Students Authors Ranier M. Adarve, DMD, MS, MHPE Lisa Fedor James, DDS, Cert. Pros. Fixed
University of Minnesota School of Dentistry Fixed Partial Denture Self-guided Instructional Material for Dental Students Authors Ranier M. Adarve, DMD, MS, MHPE Lisa Fedor James, DDS, Cert. Pros. Fixed
Preclinical Dentistry. I. Dental Caries. defects. Lenka Roubalíková. 1
 Preclinical Dentistry I. Dental Caries Non carious lesions: : trauma, erosion. abrasion, wedge shaped defects Lenka Roubalíková lenka.roubalikova@tiscali.cz 1 Understanding dental caries lenka.roubalikova@tiscali.cz
Preclinical Dentistry I. Dental Caries Non carious lesions: : trauma, erosion. abrasion, wedge shaped defects Lenka Roubalíková lenka.roubalikova@tiscali.cz 1 Understanding dental caries lenka.roubalikova@tiscali.cz
Dental materials and cements, and its use in children
 Dental materials and cements, and its use in children Study objectives Discuss amalgam restorations Discuss resin restorations Describe the history and evolution of use of silicate cement Discuss the role
Dental materials and cements, and its use in children Study objectives Discuss amalgam restorations Discuss resin restorations Describe the history and evolution of use of silicate cement Discuss the role
TOOTH PREPARATION. (Boucher's Clinical Dental Terminology, 4th ed, p239)
") Budapest, 2017 TOOTH PREPARATION The selected form given to a natural tooth when it is reduced by instrumentation to receive a prosthesis (e.g. artificial crown or a retainer for a fixed or removable prosthesis)
Budapest, 2017 TOOTH PREPARATION The selected form given to a natural tooth when it is reduced by instrumentation to receive a prosthesis (e.g. artificial crown or a retainer for a fixed or removable prosthesis)
Restoring Deep Cavity Preparations
 Restoring Deep Cavity Preparations Townies share techniques and discuss restoring posterior teeth with composites Dentaltown.com > Message Boards > Cosmetic Dentistry > Restoring Deep Cavity Preparations
Restoring Deep Cavity Preparations Townies share techniques and discuss restoring posterior teeth with composites Dentaltown.com > Message Boards > Cosmetic Dentistry > Restoring Deep Cavity Preparations
LMArte. Sculpt masterpieces
 LMArte Sculpt masterpieces LMArte LMArte by Style Italiano Designed by Walter Devoto DDS and Angelo Putignano MD, DDS. Esthetic layering - succeed with LM-Arte LM-Arte is a set of innovative instruments
LMArte Sculpt masterpieces LMArte LMArte by Style Italiano Designed by Walter Devoto DDS and Angelo Putignano MD, DDS. Esthetic layering - succeed with LM-Arte LM-Arte is a set of innovative instruments