Hematology: Challenging Cases with Your Participation COPYRIGHT
|
|
|
- Ronald Jones
- 6 years ago
- Views:
Transcription

1 Hematology: Challenging Cases with Your Participation Reed E. Drews, MD Beth Israel Deaconess Medical Center Harvard Medical School Boston, MA

2 Question 1
3 Question 1 64-year-old man is evaluated during routine exam He takes aspirin and acetaminophen for osteoarthritis On exam, pallor is absent. BP = 116/72 with no orthostatic changes; P = 68.
4 Labs Hgb = 9.7 g/dl WBC = 5.8 K/μL MCV = 83 fl Plts = 265 K/μL Retic count = 0.5% LDH = 80 U/L Iron = 40 μg/dl TIBC = 200 μg/dl Ferritin = 210 ng/ml Peripheral smear is normal
5 Which of the following is the most likely diagnosis? A. Inflammatory anemia B. Hemoglobin C disease C. Iron deficiency D. Thalassemia
6 Answer = A
7 Anemia of Inflammation (AI) Characterized by low serum iron concentration and low TIBC with elevated serum ferritin concentration Initially normochromic, normocytic, can become hypochromic, microcytic Inflammatory cytokines block iron utilization, erythropoietin (EPO) production, and EPO responsiveness Hepcidin, made by the liver, decreases iron absorption from gut and decreases release of iron from macrophages Causes internalization of ferroportin ion channel
8 Hemoglobin C Disease Mild hemolytic anemia in persons of African ancestry Serum iron chemistries are typically normal Prominent targeting in addition to microcytosis on peripheral blood smear

9 Hgb CC
10 Iron Deficiency Anemia (IDA) Characterized by low serum iron concentration, elevated TIBC, and decreased serum ferritin

11 IDA
12 Thalassemia Hypochromic, microcytic anemia Evidence of hemolysis Targets, tear drops, and prominent basophilic stippling
")

13 Factors Distinguishing the 3 Most Common Causes of Microcytosis Iron deficiency anemia (IDA) Low serum ferritin Increased total iron binding capacity Low serum iron concentration Anemia of inflammation (AI) Low serum iron Low total iron binding capacity Normal to increased serum ferritin Alpha or beta thalassemia minor Patients may not be anemic Target cells, tear-drop forms, and basophilic stippling IDA b-thalassemia minor
14 Laboratory Characteristics of AI, IDA, and IDA + Inflammation From MKSAP 15 Parameter AI IDA IDA+AI MCV fl <85 fl <100 fl MCHC <36 g/dl <32 g/dl <32 g/dl Serum iron <60 μg/dl <60 μg/dl <60 μg/dl TIBC <250 μg/dl >400 μg/dl <400 μg/dl TIBC saturation 2%-20% <15% (usually <10%) <15% Ferritin >35 ng/ml < 15 ng/ml <100 ng/ml Bone marrow iron Present Absent Absent
15 Iron Deficiency Happens in Stages Iron deficiency without anemia Ferritin < 20 ng/ml; Fe/TIBC > 15% Iron deficiency with mild anemia Ferritin < 15 ng/ml; Fe/TIBC < 15% Severe iron deficiency with severe anemia Ferritin < 10 ng/ml; Fe/TIBC < 10% Bone marrow iron absent in all stages
16 Ferritin Levels in IDA Virtually all patients with serum ferritin levels <10 to 15 ng/ml are iron deficient Sensitivity 59%, specificity 99% 25% of women with absent stainable bone marrow iron have ferritin levels >15 ng/ml Assuming no inflammation, higher ferritin cutoff limits provide improved diagnostic efficiency 30 ng/ml: sensitivity 92%, specificity 98% 41 ng/ml: sensitivity 98%, specificity 98%
17 Anemia of Inflammation Inflammation decreases serum iron and plasma transferrin concentrations Transferrin saturations are in iron deficiency range in 20% of patients with anemia of inflammation 20 to 30% of patients with inflammatory anemia do not have underlying inflammatory condition Guyatt GH et al. Am J Med 1990;88:205.
18 Ferritin Levels in Iron Deficiency AND Inflammatory States Inflammation increases ferritin levels by about 3-fold Iron deficiency should be suspected in patients with inflammatory states and ferritin levels <100 ng/ml In anemic patients with rheumatoid arthritis, ferritin levels < 60 ng/ml predicted response to oral iron therapy with 83% accuracy (Hansen TM, Hansen NE. Ann Rheum Dis 1986;45:596)


19 Question 2
20 Question 2 27-year-old woman undergoes follow-up evaluation 5 months after diagnosis of unprovoked PE for which she was prescribed a 6-month course of anticoagulant therapy Family history Maternal grandmother took warfarin for many years for unknown reason Older brother with DVT at age 32 years Meds: no contraceptives or other medications Labs: CBC normal; INR = 3.0
21 Which of the following is the most appropriate next step in the evaluation of this patient? A. Immediate thrombophilic screening B. JAK2 mutation analysis C. No further evaluation needed D. Thrombophilic screening at least 2 weeks after therapy cessation
22 Answer = D
23 Thrombophilia Unprovoked PE + family history of VTE = high likelihood of underlying thrombophilic condition Screening decisions Strongly thrombophilic 1 st unprovoked VTE before 50 yrs of age; or History of recurrent thromboses; or 1 st -degree relative(s) with documented VTE before age 50 yrs Weakly thrombophilic All others Do NOT screen during acute episode or during anticoagulant therapy when heparin or warfarin influence certain tests Risk of recurrent VTE cannot be estimated without screening for inherited thrombophilia
24 Thrombophilic Disorders with High Risk for Recurrence Antithrombin, protein C or protein S deficiency Homozygous factor V Leiden (FVL) or prothrombin gene mutation (PTM) Compound heterozygous FVL + PTM Patients with these disorders are candidates for long-term, if not lifelong, anticoagulation therapy
25 Thrombophilia due to Myeloproliferative Neoplasm PV and ET predispose to venous and arterial thromboses, particularly when RBC mass and platelet count are not controlled JAK2 mutation is found in nearly all pts with PV and ~50% of pts with ET Routine screening for this mutation is not recommended unless pts have Budd-Chiari syndrome of portal vein thrombosis
26 Target INR Target INR of 1.5 to 2 has efficacy in preventing recurrent VTE However, target INR of 2 to 3 is more efficacious Risk for major bleeding is similar for the two target INR ranges (1) Ridker PM et al. Long-term, low-intensity warfarin therapy for the prevention of recurrent venous thromboembolism. N Engl J Med 2003; 348: (2) Kearon C et al. Comparison of low-intensity warfarin therapy with conventional-intensity warfarin therapy for long-term prevention of recurrent venous thromboembolism. N Engl J Med 2003; 349:631-9.
27 Major Risk Factors for Thrombosis: Acquired From MKSAP 15 Prior thrombosis Advancing age Obesity Immobilization Major surgery Estrogens (OCPs, HRT, SERMs) Malignancy Prolonged air travel Antiphospholipid antibody syndrome MPNs (PV, ET) PNH Hemoglobinuria HIT Inflammatory bowel disease Nephrotic syndrome
28 Major Risk Factors for Thrombosis: Inherited From MKSAP 15 Antithrombin deficiency Protein C deficiency Protein S deficiency Factor V Leiden (FVL) Prothrombin G20210A Dysfibrinogenemias (rare)
29 Uncertain Risk Factors for Venous Thrombosis From MKSAP 15 Hyperhomocysteinemia High levels of factor VIII APC-resistance in the absence of FVL High levels of factor IX High levels of factor XI High levels of TAFI Low levels of free TFPI Decreased fibrinolytic potential TAFI = thrombin-activatable fibrinolysis inhibitor; TFPI = tissue factor pathway inhibitor.
30 Risks and Incidence of a First Episode of Venous Thrombosis (From The Leiden Thrombophilia Study) Relative Risk Incidence/y (%) Normal Prothrombin G20210A mutation Oral contraceptives Factor V Leiden heterozygote Oral contraceptives + factor V Leiden Factor V Leiden homozygous to 1.0
31 Site of Thrombosis According to Coagulation Defect Abnormality Arterial Venous Factor V Leiden - + Antithrombin III deficiency - + Protein C deficiency - + Protein S deficiency - + Prothrombin gene mutation - + Hyperhomocysteinemia + - Lupus anticoagulant/apl + + APL = antiphospholipid antibody syndrome.
32 Testing for Risk Factors In all patients Cancer screening 20% of all patients with symptomatic VTE have cancer Unprovoked venous thrombosis and/or unexplained arterial thrombosis Antiphospholipid antibody syndrome (venous and/or arterial) Hyperhomocysteinemia (arterial) In patients younger than 50 years AT, protein C, protein S Less than 5% over 50 In patients older than 50 years FVL, prothrombin G20210A 26% of men over 60 in the Physicians Health Study
33 Indefinite Anticoagulation in Patients at High Risk 2 or more spontaneous events 1 spontaneous life-threatening event Near fatal pulmonary embolus Cerebral, mesenteric, or portal vein thrombosis 1 spontaneous event in association with Antiphospholipid antibody syndrome Antithrombin deficiency More than 1 genetic or allelic abnormality

34 T H G I R Question Y P O C 3
35 Question 3 A 68-year old woman has hypertension for which she takes HCTZ and low-dose aspirin daily. On routine blood testing, she is found to have a high total protein. On exam, she appears well without lymphadenopathy, hepatosplenomegaly or bony pain to palpation or percussion. Hgb = 12.9 g/dl; WBC = 6.2K/μL; platelets = 245K/μL. SPEP shows 1.2 g/dl monoclonal IgG-kappa. UPEP is negative for protein, including Bence Jones protein.
36 Question 3 (continued) Bone marrow biopsy shows 7% plasma cells, and skeletal survey is normal, without lytic lesions. Which is the most appropriate management for this patient? 1. Obtain a bone scan 2. Begin bisphosphonate therapy 3. Begin thalidomide + dexamethasone 4. Monitor expectantly and repeat the SPEP and UPEP in 3 to 6 months
37 Answer = 4
38 Monoclonal gammopathy of undetermined significance No symptoms No end organ damage related to plasma cell dyscrasia or a related B cell lymphoproliferative disorder No lymphadenopathy, organomegaly, hypercalcemia, renal failure, anemia, bone abnormalities (skeletal survey)* Relatively low paraprotein level (<3 g/dl) < 10% plasmacytosis in bone marrow Phenomenon of aging *No role for bone scans or PET scans
39 Prevalence of MGUS According to Age Group and Sex among Residents of Olmsted County, Minnesota Age Men Women Total percent yr yr yr yr Total Kyle RA et al. Prevalence of monoclonal gammopathy of undetermined significance. N Engl J Med 2006; 354:
40 Management of MGUS No role for anti-plasma cell therapy Monitor expectantly Monitor for signs and symptoms of progression to multiple myeloma Follow CBCs, BUN/cre, albumin/calcium, SPEP, UPEP, and free serum kappa & lambda light chains Assess risk for progression Lowest with paraprotein levels 0.9 g/dl Highest with paraprotein levels 3 g/dl Serum free light chain assay (FLC) Ratio of serum free kappa to serum free lambda
41 Risk of progression to myeloma or related disorder in 1148 pts with MGUS Rajkumar SV et al. Blood 2005; 106:812-7
42 Risk of progression of MGUS in patients with abnormal FLC ratio Rajkumar SV et al. Blood 2005; 106:812-7
43 Diagnostic criteria for myeloma Myeloma Serum or urinary monoclonal protein Clonal plasma cell in bone marrow or plasmacytoma End organ damage related to plasma cell dyscrasia Aymptomatic (smoldering) myeloma Serum monoclonal protein 3 g/dl and/or bone marrow plasma cells 10 percent No end organ damage related to plasma cell dyscrasia
44 Treatment of Myeloma Alkylating agent and corticosteroid Melphalan mainstay of myeloma therapy for more than 40 years Now use cyclophosphamide + bortezomib +/- lenalidomide +/- dexamethasone Thalidomide Fetal malformations; VTE; somnolence; neuropathy Bortezomib Neuropathy Carfilzomib Less neuropathy; more heart failure Lenalidomide Myelosuppression; VTE; less somnolence & neuropathy than thalidomide Autologous stem cell transplantation with high-dose melphalan Improves survival to a median of 4.5 to 5 years Bisphosphonate therapy once monthly (1-2 years) Osteonecrosis of jaw; renal dysfunction

45

46 Other Findings of Undetermined Significance Steensma DP et al. Blood 2015; 126:9.

47 Question 4
48 Question 4 A 65-year old presents with cervical adenopathy and splenomegaly. HCT = 37%; WBC = 34,000/µL with 2% polys and 98% lymphs; platelets = 177,000/µL. Peripheral blood smear review reveals mature appearing lymphocytes and smudge cells (see next slide).
49
50 Question 4 (continued) Which of the following is true of this patient? 1. Patients in late childhood or young adulthood are as likely to have this disease as older patients 2. One should be alert for the blast phase of disease 3. The patient might present with autoimmune hemolytic anemia and/or immune thrombocytopenia 4. The evidence favors early treatment
51 Answer = 3


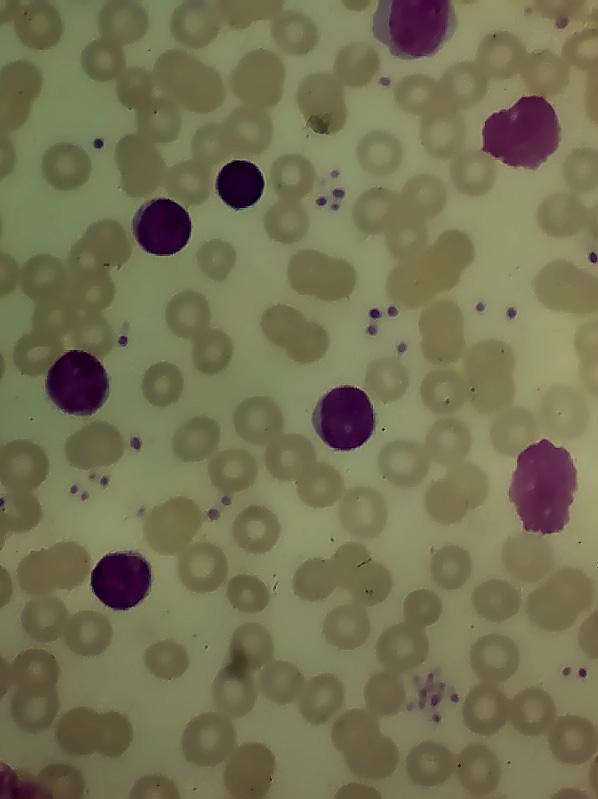
52 HCL CLL PLL
53 Approximate Median Time to Treatment and Median Survival of Patients with Early-Stage Disease according to Prognostic Variables Prognostic Variable Median Time to Treatment, y Median Survival, y Result of FISH 13q- (sole abnormality) 7.5 >11 to 15 Normal karyotype 4 >10 to q- 1 6 to 9 17p- <1 2 to 4 IgV H gene mutation status ZAP-70 CD38 Mutated 8 20 Not mutated <4 7 to 10 Negative 9 to Positive 3 to 4 8 to 10 Negative 5 20 Positive <4 8 to 10

54 Question 5
55 Question 5 A 63-year old patient develops exertional dyspnea. On exam, sclerae are slightly icteric. HCT = 28% with MCV = 105; reticulocyte count = 9%; WBC and platelet counts are normal. The laboratory reports bite cells on peripheral blood smear (see next slide).

56
57 Question 5 (continued) What is the most likely underlying mechanism of anemia in this patient? 1. Autoimmune hemolysis 2. Microangiopathic hemolytic anemia 3. Oxidant hemolysis 4. Paroxysmal nocturnal hemoglobinuria
58 Answer = 3
 from")
59 Bite cells Heinz body prep By Carola von Kapff, SH (ASCP) from UpToDateÒ
60 Drugs and chemicals in glucose-6- phosphate dehydrogenase deficiency Acetanilid Dapsone Furazolidone Methylene blue Nalidixic acid Unsafe for class I, II, and III variants Naphthalene (mothballs, henna) Niridazole Nitrofurantoin Phenazopyridine Phenylhydrazine Primaquine Sulfacetamide Sulfamethoxazole Source: UpToDate Sulfanilamide Sulfapyridine Thiazosulfone Toluidine blue Trinitrotoluene
61 Drugs and chemicals in glucose-6- phosphate dehydrogenase deficiency Acetaminophen Safe for class II and III variants* Ascorbic acid (except in very high doses) Phenacetin Phenytoin Aspirin Probenecid Chloramphenicol Chloroquine Colchicine Diphenhydramine Isoniazid L-DOPA Pyrimethamine Quinine Streptomycin Sulfisoxazole Trimethoprim Vitamin K * Safety for class I variants is usually not known. Source: UpToDate

62 Question 6
63 Question 6 A 24-year old patient develops dyspnea and is found to be anemic with HCT = 28%, MCV = 104 fl, and reticulocyte count = 6%. The laboratory reports 2+ spherocytes on peripheral blood smear (see next slide).

64
65 Question 6 (continued) Coombs testing is positive for IgG and negative for C3. What is the most appropriate management in this patient? 1. Transfuse packed red blood cells 2. Begin prednisone 1 mg/kg and folic acid 5 mg daily 3. Begin danazol 4. Administer rituximab
66 Answer = 2

67 Macrophage Ingesting an IgG-Coated RBC Bessis M. Corpuscles. Atlas of Red Cell Shape. Berlin, Springer- Verlag, 1974
68 Etiologies of WAIHA Idiopathic Viral infections (usually in children) Autoimmune and connective tissue diseases (particularly SLE) Malignancies of the immune system NHL; CLL Treatment with purine nucleoside analogs Immune deregulation Prior allogeneic blood transfusion or HSCT Certain drugs Hydralazine, isoniazid, methyldopa, penicillin, procainamide, quinidine, quinine
69 Lab Findings in WAIHA Combination of increased LDH and reduced haptoglobin 90% specific for diagnosing hemolysis Combination of normal LDH and haptoglobin > 25 mg/dl 92% sensitive for ruling out hemolysis Reticulocytosis > 4-5% (median, 9%) Lower than expected degree of reticulocytosis in 20-37% Lag in marrow responsiveness to hemolytic stress Hemolysis of reticulocytes Parvovirus B19 infection Spherocytosis with elevated MCHC May not be obvious in milder cases (1) Liesveld JL et al. Blood 1987; 69:820. (2) Marchand A et al. JAMA 1980; 243:1909. (3) Galen RS. Clin Lab Med 1982; 2:685. (4) Conley CL et al. JAMA 1980; 244:1688.
70 Treatment of WAIHA Can present as a medical emergency requiring immediate PRBC transfusion Contact Blood Bank personnel Stop any possible offending drug (e.g., penicillin) Treat underlying disease (e.g., SLE, CLL) Reduce autoantibody production
71 Reduction in Antibody Production Corticosteroids (Wendell Rosse & Stanley Schrier) Prednisone 1 mg/kg per day Maintain high dose for 1 week beyond goal Hgb level (e.g., >10 g/dl) Rapidly taper by 20 mg increments every 1 to 2 weeks to 20 mg/day Maintain 20 mg/day for 1 month If remission persists Gradually reduce dose on alternate days to 10 mg/day and maintain for 1 month Omit the dose on alternate days Reduce dose to 10 mg/day on alternate days Maintain this dose as long as remission persists and the DAT remains positive Danazol (may be steroid sparing)
72 Reduction in Antibody Production Immunosuppressive and cytotoxic agents Azathioprine 100 to 150 mg/day Cyclophosphamide 100 mg/day by mouth 500 to 700 mg IV every 3 to 4 weeks High-dose (as in aplastic anemia) 50 mg/kg per day IV for 4 days with Mesna and G-CSF Cyclosporine and mycophenolate mofetil Vincristine Rituximab Alemtuzumab
73 Reduction in Antibody Effectiveness Splenectomy IVIg Less effective than in management of ITP

74 The End
Hematology: Challenging Cases with Your Participation COPYRIGHT
 Hematology: Challenging Cases with Your Participation Reed E. Drews, MD Beth Israel Deaconess Medical Center Harvard Medical School Boston, MA Question 1 Question 1 64-year-old man is evaluated during
Hematology: Challenging Cases with Your Participation Reed E. Drews, MD Beth Israel Deaconess Medical Center Harvard Medical School Boston, MA Question 1 Question 1 64-year-old man is evaluated during
Thrombophilia: To test or not to test
 Kenneth Bauer, MD Harvard Medical School, Boston, MA Professor of Medicine VA Boston Healthcare System Chief, Hematology Section Beth Israel Deaconess Medical Center, Boston, MA Director, Thrombosis Clinical
Kenneth Bauer, MD Harvard Medical School, Boston, MA Professor of Medicine VA Boston Healthcare System Chief, Hematology Section Beth Israel Deaconess Medical Center, Boston, MA Director, Thrombosis Clinical
General Characterisctics
 Anemia General Characterisctics Definition: anemia is a decrease in red blood cells. Happens due to underproduction, increased destruction or loss of red cells. Diagnosis of anemia: Hgb < 135 (men) Hgb
Anemia General Characterisctics Definition: anemia is a decrease in red blood cells. Happens due to underproduction, increased destruction or loss of red cells. Diagnosis of anemia: Hgb < 135 (men) Hgb
Case # 1. RBC Loss. CASE #1 (Continued) Blood Loss Is the Most Common Cause of Anemia. AGA Definition of Occult Blood Loss
 Blood Loss Is the Most Common Cause of Anemia. AGA Definition of Occult Blood Loss") Case # 1 A 42-yo woman with heavy menses presents with rectal bleeding. Except for pallor, exam is normal. HCT = 17.1% (normal, 36-48) HGB = 5.3 g/dl (normal, 12.0-16.0) MCV = 76 fl (normal, 82-98) RBC
Case # 1 A 42-yo woman with heavy menses presents with rectal bleeding. Except for pallor, exam is normal. HCT = 17.1% (normal, 36-48) HGB = 5.3 g/dl (normal, 12.0-16.0) MCV = 76 fl (normal, 82-98) RBC
2013 AAIM Pathology Workshop
 2013 AAIM Pathology Workshop John Schmieg, M.D., Ph.D. None Disclosures 1 Pathology Workshop Objectives Define the general philosophy of reviewing pathology reports Review the various components of Bone
2013 AAIM Pathology Workshop John Schmieg, M.D., Ph.D. None Disclosures 1 Pathology Workshop Objectives Define the general philosophy of reviewing pathology reports Review the various components of Bone
Thrombophilia. Diagnosis and Management. Kevin P. Hubbard, DO, FACOI
 Thrombophilia Diagnosis and Management Kevin P. Hubbard, DO, FACOI Clinical Professor of Medicine Kansas City University of Medicine and Biosciences-College of Osteopathic Medicine Kansas City, Missouri
Thrombophilia Diagnosis and Management Kevin P. Hubbard, DO, FACOI Clinical Professor of Medicine Kansas City University of Medicine and Biosciences-College of Osteopathic Medicine Kansas City, Missouri
Anemia. A case-based approach. David B. Sykes, MD, PhD Hematology, MGH Cancer Center June 8, 2017
 Anemia A case-based approach David B. Sykes, MD, PhD Hematology, MGH Cancer Center June 8, 2017 Recognizing trends Learning Objectives MCV, RDW, Ferritin, LDH, Reticulocytes Managing complex patients 1.
Anemia A case-based approach David B. Sykes, MD, PhD Hematology, MGH Cancer Center June 8, 2017 Recognizing trends Learning Objectives MCV, RDW, Ferritin, LDH, Reticulocytes Managing complex patients 1.
11. An acute leukemia causing. 12. An adult patient presents with acute. 13. Anemia due to renal failure may be
 Hematology Study online at 1. A 23 year old white female has weakness, fatigue and has developed a habit of chewing ice. What are the expected findings in regard to TIBC and Ferritin? 2. A 25 year old
Hematology Study online at 1. A 23 year old white female has weakness, fatigue and has developed a habit of chewing ice. What are the expected findings in regard to TIBC and Ferritin? 2. A 25 year old
Taking The Fear Out of Abnormal CBC s Problems of Production, Destruction or loss
 Taking The Fear Out of Abnormal CBC s Problems of Production, Destruction or loss Joanne Eddington, MN, FNP, AOCN Providence Oncology and Hematology Care Clinic - Eastside Blood Cell Abnormalities Abnormalities
Taking The Fear Out of Abnormal CBC s Problems of Production, Destruction or loss Joanne Eddington, MN, FNP, AOCN Providence Oncology and Hematology Care Clinic - Eastside Blood Cell Abnormalities Abnormalities
Year 2003 Paper two: Questions supplied by Tricia
 QUESTION 65 A 36-year-old man presents in a post-ictal state after an observed generalised seizure. Full blood investigation shows: haemoglobin 0 g/l [128-175] mean corpuscular volume (MCV) 106 fl [80-7]
QUESTION 65 A 36-year-old man presents in a post-ictal state after an observed generalised seizure. Full blood investigation shows: haemoglobin 0 g/l [128-175] mean corpuscular volume (MCV) 106 fl [80-7]
M-Protien, what to do next? Ismail A Sharif MD, FRCPc Internal Medicine Day 22 nd April 2016
 + M-Protien, what to do next? Ismail A Sharif MD, FRCPc Internal Medicine Day 22 nd April 2016 + Disclosures Advisory Boards: AMGEN, Lundbeck, NOVARTIS + Subtypes of Plasma Cell Disorders Increased Plasma
+ M-Protien, what to do next? Ismail A Sharif MD, FRCPc Internal Medicine Day 22 nd April 2016 + Disclosures Advisory Boards: AMGEN, Lundbeck, NOVARTIS + Subtypes of Plasma Cell Disorders Increased Plasma
Hematologic Disorders. Assistant professor of anesthesia
 Preoperative Evaluation Hematologic Disorders Dr M.Razavi Assistant professor of anesthesia Anemia Evaluation needs to consider the extent and type of surgery, the anticipated blood loss, and the patient's
Preoperative Evaluation Hematologic Disorders Dr M.Razavi Assistant professor of anesthesia Anemia Evaluation needs to consider the extent and type of surgery, the anticipated blood loss, and the patient's
QUESTIONS OF HEMATOLOGY AND THEIR ANSWERS
 QUESTIONS OF HEMATOLOGY AND THEIR ANSWERS WHAT IS TRUE AND WHAT IS FALSE? Questions 1 Iron deficiency anemia a) Is usually associated with a raised MCV. b) The MCH is usually low. c) Is most commonly due
QUESTIONS OF HEMATOLOGY AND THEIR ANSWERS WHAT IS TRUE AND WHAT IS FALSE? Questions 1 Iron deficiency anemia a) Is usually associated with a raised MCV. b) The MCH is usually low. c) Is most commonly due
Are there still any valid indications for thrombophilia screening in DVT?
 Carotid artery stenosis and risk of stroke Are there still any valid indications for thrombophilia screening in DVT? Armando Mansilha MD, PhD, FEBVS Faculty of Medicine of University of Porto Munich, 2016
Carotid artery stenosis and risk of stroke Are there still any valid indications for thrombophilia screening in DVT? Armando Mansilha MD, PhD, FEBVS Faculty of Medicine of University of Porto Munich, 2016
Mabel Labrada, MD Miami VA Medical Center
 Mabel Labrada, MD Miami VA Medical Center *1-Treatment for acute DVT with underlying malignancy is for 3 months. *2-Treatment of provoked acute proximal DVT can be stopped after 3months of treatment and
Mabel Labrada, MD Miami VA Medical Center *1-Treatment for acute DVT with underlying malignancy is for 3 months. *2-Treatment of provoked acute proximal DVT can be stopped after 3months of treatment and
Anemia in the elderly. Nattiya Teawtrakul MD., PhD
 Anemia in the elderly Nattiya Teawtrakul MD., PhD Contents Definition of anemia in the elderly The impact of anemia in the elderly Etiology of anemia in the elderly Management of anemia in the elderly
Anemia in the elderly Nattiya Teawtrakul MD., PhD Contents Definition of anemia in the elderly The impact of anemia in the elderly Etiology of anemia in the elderly Management of anemia in the elderly
Evaluation of Anemia. Md. Shafiqul Bari Associate professor (Medicine) SOMC
 SOMC") Evaluation of Anemia Md. Shafiqul Bari Associate professor (Medicine) SOMC Definition Anemia is operationally defined as a reduction in one or more of the major RBC measurements Hemoglobin concentration
Evaluation of Anemia Md. Shafiqul Bari Associate professor (Medicine) SOMC Definition Anemia is operationally defined as a reduction in one or more of the major RBC measurements Hemoglobin concentration
Case Workshop of Society for Hematopathology and European Association for Haematopathology
 Case 148 2007 Workshop of Society for Hematopathology and European Association for Haematopathology Robert P Hasserjian Department of Pathology Massachusetts General Hospital Boston, MA Clinical history
Case 148 2007 Workshop of Society for Hematopathology and European Association for Haematopathology Robert P Hasserjian Department of Pathology Massachusetts General Hospital Boston, MA Clinical history
HAEMATOLOGICAL EVALUATION OF ANEMIA. Sitalakshmi S Professor and Head Department of Clinical Pathology St John s medical College, Bangalore
 HAEMATOLOGICAL EVALUATION OF ANEMIA Sitalakshmi S Professor and Head Department of Clinical Pathology St John s medical College, Bangalore Learning Objectives Laboratory tests for the evaluation of anemia
HAEMATOLOGICAL EVALUATION OF ANEMIA Sitalakshmi S Professor and Head Department of Clinical Pathology St John s medical College, Bangalore Learning Objectives Laboratory tests for the evaluation of anemia
UNUSUAL PRESENTATIONS OF SYSTEMIC LUPUS ERYTHEMATOSUS
 UNUSUAL PRESENTATIONS OF SYSTEMIC LUPUS ERYTHEMATOSUS Presenter- Dr. Meghana B S Prof Dr. NAGARAJA B S Prof Dr. NIRMALA A C Dr. SIVARANJANI H Dr. B C PRAKASH Dr. MUMTAZ ALI KHAN A 60 year old lady, k/c/o
UNUSUAL PRESENTATIONS OF SYSTEMIC LUPUS ERYTHEMATOSUS Presenter- Dr. Meghana B S Prof Dr. NAGARAJA B S Prof Dr. NIRMALA A C Dr. SIVARANJANI H Dr. B C PRAKASH Dr. MUMTAZ ALI KHAN A 60 year old lady, k/c/o
(anemia) ก hemoglobin concentration, hematocrit deviation 1 1 ก hemoglobin, hematocrit mean corpuscular volume (MCV) 2
 ก hemoglobin concentration, hematocrit deviation 1 1 ก hemoglobin, hematocrit mean corpuscular volume (MCV) 2") ก ก. ก ก.. ก (anemia) ก hemoglobin concentration, hematocrit ก ก ก 2 Standard deviation 1 1 ก hemoglobin, hematocrit mean corpuscular volume (MCV) 2 Hemoglobin hematocrit MCV (g/dl) (%) (fl) ( ) 0.5-1.9
ก ก. ก ก.. ก (anemia) ก hemoglobin concentration, hematocrit ก ก ก 2 Standard deviation 1 1 ก hemoglobin, hematocrit mean corpuscular volume (MCV) 2 Hemoglobin hematocrit MCV (g/dl) (%) (fl) ( ) 0.5-1.9
Approach to Thrombosis
 Approach to Thrombosis Theera Ruchutrakool, M.D. Division of Hematology Department of Medicine Siriraj Hospital Faculty of Medicine Mahidol University Approach to Thrombosis Thrombosis: thrombus formation
Approach to Thrombosis Theera Ruchutrakool, M.D. Division of Hematology Department of Medicine Siriraj Hospital Faculty of Medicine Mahidol University Approach to Thrombosis Thrombosis: thrombus formation
SOLIRIS (eculizumab) Slide # 1. How do we treat PNH?
 Slide # 1. How do we treat PNH?") Treating PNH How do we treat PNH? Hemolytic anemia Iron, folic acid Transfusion Steroids Eculizumab Thrombosis Coumadin prophylaxis Acute treatment with lytic agents (clot busters) Anticoagulation therapy
Treating PNH How do we treat PNH? Hemolytic anemia Iron, folic acid Transfusion Steroids Eculizumab Thrombosis Coumadin prophylaxis Acute treatment with lytic agents (clot busters) Anticoagulation therapy
I. Definitions. V. Evaluation A. History B. Physical Exam C. Laboratory evaluation D. Bone marrow examination E. Specialty referrals
 I. Definitions II. III. Red blood cell life cycle Iron metabolism IV. Causes of anemia A. Kinetic approach 1. decreased production 2. increased destruction 3. blood loss B. Morphologic approach 1. normocytic
I. Definitions II. III. Red blood cell life cycle Iron metabolism IV. Causes of anemia A. Kinetic approach 1. decreased production 2. increased destruction 3. blood loss B. Morphologic approach 1. normocytic
Thrombosis. By Dr. Sara Mohamed Abuelgasim
 Thrombosis By Dr. Sara Mohamed Abuelgasim 1 Thrombosis Unchecked, blood coagulation would lead to dangerous occlusion of blood vessels if the protective mechanisms of coagulation factor inhibitors, blood
Thrombosis By Dr. Sara Mohamed Abuelgasim 1 Thrombosis Unchecked, blood coagulation would lead to dangerous occlusion of blood vessels if the protective mechanisms of coagulation factor inhibitors, blood
Laboratory Examination
 Todd Zimmerman, M.D. 64 year old African American male presents to establish care with PCG. Meds: Norvasc 5 mg daily PMHx: HTN x 20 years, poorly controlled SHx: No tobacco, illicit; rare EtOH ROS: Negative
Todd Zimmerman, M.D. 64 year old African American male presents to establish care with PCG. Meds: Norvasc 5 mg daily PMHx: HTN x 20 years, poorly controlled SHx: No tobacco, illicit; rare EtOH ROS: Negative
New phase 2 Clinical Trial Enrolling Now
 New phase 2 Clinical Trial Enrolling Now Warm Autoimmune Hemolytic Anemia (waiha) and Cold Agglutinin Disease (CAD) Designed for patients Age 18 or older With a primary diagnosis of waiha who had a recurrence,
New phase 2 Clinical Trial Enrolling Now Warm Autoimmune Hemolytic Anemia (waiha) and Cold Agglutinin Disease (CAD) Designed for patients Age 18 or older With a primary diagnosis of waiha who had a recurrence,
Diagnostic Approach to Patients with Anemia
 J KMA Special Issue Diagnostic Approach to Patients with Anemia Seonyang Park, MD Department of Internal Medicine, Seoul National University College of Medicine E mail : seonpark@snu.ac.kr J Korean Med
J KMA Special Issue Diagnostic Approach to Patients with Anemia Seonyang Park, MD Department of Internal Medicine, Seoul National University College of Medicine E mail : seonpark@snu.ac.kr J Korean Med
Microcytic Hypochromic Anemia An Approach to Diagnosis
 Microcytic Hypochromic Anemia An Approach to Diagnosis Decreased hemoglobin synthesis gives rise to microcytic hypochromic anemias. Hypochromic anemias are characterized by normal cellular proliferation
Microcytic Hypochromic Anemia An Approach to Diagnosis Decreased hemoglobin synthesis gives rise to microcytic hypochromic anemias. Hypochromic anemias are characterized by normal cellular proliferation
Anemia (3).ms4.25.Oct.15 Hemolytic Anemia. Abdallah Abbadi
.ms4.25.Oct.15 Hemolytic Anemia. Abdallah Abbadi") Anemia (3).ms4.25.Oct.15 Hemolytic Anemia Abdallah Abbadi Case 3 24 yr old female presented with anemia syndrome and jaundice. She was found to have splenomegaly. Hb 8, wbc 12k, Plt 212k, retics 12%, LDH
Anemia (3).ms4.25.Oct.15 Hemolytic Anemia Abdallah Abbadi Case 3 24 yr old female presented with anemia syndrome and jaundice. She was found to have splenomegaly. Hb 8, wbc 12k, Plt 212k, retics 12%, LDH
Anemia In the Insurance Applicant What do the numbers mean?
 Anemia In the Insurance Applicant What do the numbers mean? Lisa Duckett, M.D. Vice President and Medical Director September 12, 2017 Goals of the presentation Develop a consistent way to analyze Complete
Anemia In the Insurance Applicant What do the numbers mean? Lisa Duckett, M.D. Vice President and Medical Director September 12, 2017 Goals of the presentation Develop a consistent way to analyze Complete
Hematology Case Conference 8/5/03
 Hematology Case Conference 8/5/03 Bone Marrow Case Patient: Emmxxx Lylexxx 74 year old AA female S/P craniotomy for SDH. Pt has Hx of HTN, DM, Crohn s disease, (R) nephrectomy. Bone marrow for abnormal
Hematology Case Conference 8/5/03 Bone Marrow Case Patient: Emmxxx Lylexxx 74 year old AA female S/P craniotomy for SDH. Pt has Hx of HTN, DM, Crohn s disease, (R) nephrectomy. Bone marrow for abnormal
BONE MARROW PERIPHERAL BLOOD Erythrocyte
 None Disclaimer Objectives Define anemia Classify anemia according to pathogenesis & clinical significance Understand Red cell indices Relate the red cell indices with type of anemia Interpret CBC to approach
None Disclaimer Objectives Define anemia Classify anemia according to pathogenesis & clinical significance Understand Red cell indices Relate the red cell indices with type of anemia Interpret CBC to approach
Hemostasis. PHYSIOLOGICAL BLOOD CLOTTING IN RESPONSE TO INJURY OR LEAK no disclosures
 Hemostasis PHYSIOLOGICAL BLOOD CLOTTING IN RESPONSE TO INJURY OR LEAK no disclosures Disorders of Hemostasis - Hemophilia - von Willebrand Disease HEMOPHILIA A defect in the thrombin propagation phase
Hemostasis PHYSIOLOGICAL BLOOD CLOTTING IN RESPONSE TO INJURY OR LEAK no disclosures Disorders of Hemostasis - Hemophilia - von Willebrand Disease HEMOPHILIA A defect in the thrombin propagation phase
CASE 106. Pancytopenia in the setting of marrow hypoplasia, a PNH clone, and a DNMT3A mutation
 CASE 106 Pancytopenia in the setting of marrow hypoplasia, a PNH clone, and a DNMT3A mutation Gabriel C. Caponetti, MD University of Pennsylvania, US Clinical history 69, F peripheral neuropathy, refractory
CASE 106 Pancytopenia in the setting of marrow hypoplasia, a PNH clone, and a DNMT3A mutation Gabriel C. Caponetti, MD University of Pennsylvania, US Clinical history 69, F peripheral neuropathy, refractory
Collect and label sample according to standard protocols. Gently invert tube 8-10 times immediately after draw. DO NOT SHAKE. Do not centrifuge.
 Complete Blood Count CPT Code: CBC with Differential: 85025 CBC without Differential: 85027 Order Code: CBC with Differential: C915 Includes: White blood cell, Red blood cell, Hematocrit, Hemoglobin, MCV,
Complete Blood Count CPT Code: CBC with Differential: 85025 CBC without Differential: 85027 Order Code: CBC with Differential: C915 Includes: White blood cell, Red blood cell, Hematocrit, Hemoglobin, MCV,
Hematologic changes in systemic diseases. Chittima Sirijerachai
 Hematologic changes in systemic diseases Chittima Sirijerachai Systemic diseases Infection Renal diseases Liver diseases Connective tissue diseases Malignancy Anemia of chronic disease (ACD) Chronic infections:
Hematologic changes in systemic diseases Chittima Sirijerachai Systemic diseases Infection Renal diseases Liver diseases Connective tissue diseases Malignancy Anemia of chronic disease (ACD) Chronic infections:
Hematology AHD Test Review September Jayne M Peterson, MD Regan Memmott, MD, PhD
 Hematology AHD Test Review September 2017 Jayne M Peterson, MD Regan Memmott, MD, PhD Question 1 Which of the following is the most appropriate management of this patient's thrombocytopenia? A. Emergent
Hematology AHD Test Review September 2017 Jayne M Peterson, MD Regan Memmott, MD, PhD Question 1 Which of the following is the most appropriate management of this patient's thrombocytopenia? A. Emergent
Paroxysmal Nocturnal Hemoglobinuria
 Paroxysmal Nocturnal Hemoglobinuria Barry Skikne MD, FACP, FCP(SA) Professor of Hematology Division of Hematologic Malignancies and Cellular Therapeutics Cardinal Clinical Manifestations PNH Clonal disease
Paroxysmal Nocturnal Hemoglobinuria Barry Skikne MD, FACP, FCP(SA) Professor of Hematology Division of Hematologic Malignancies and Cellular Therapeutics Cardinal Clinical Manifestations PNH Clonal disease
Scott M. Stevens, MD. Co-Director, Thrombosis Clinic. Associate Professor of Clinical Medicine
 Scott M. Stevens, MD Co-Director, Thrombosis Clinic Intermountain Medical Center Associate Professor of Clinical Medicine The University of Utah School of Medicine No Relevant Financial Relationships Research
Scott M. Stevens, MD Co-Director, Thrombosis Clinic Intermountain Medical Center Associate Professor of Clinical Medicine The University of Utah School of Medicine No Relevant Financial Relationships Research
Genetic Tests for the Better Outcome of VTE? 서울대학교병원혈액종양내과윤성수
 Genetic Tests for the Better Outcome of VTE? 서울대학교병원혈액종양내과윤성수 Thrombophilia A hereditary or acquired disorder predisposing to thrombosis Questions Why should we test? Who should we test For what disorders?
Genetic Tests for the Better Outcome of VTE? 서울대학교병원혈액종양내과윤성수 Thrombophilia A hereditary or acquired disorder predisposing to thrombosis Questions Why should we test? Who should we test For what disorders?
Evaluation of the Inpatient with Anemia
 Evaluation of the Inpatient with Anemia Camila Masias, M.D. Assistant Professor Division of Hematology The Ohio State University Wexner Medical Center Case 1 22 yo woman presents to the ED with fatigue
Evaluation of the Inpatient with Anemia Camila Masias, M.D. Assistant Professor Division of Hematology The Ohio State University Wexner Medical Center Case 1 22 yo woman presents to the ED with fatigue
Evaluation of the Inpatient with Anemia
 Evaluation of the Inpatient with Anemia Camila Masias, M.D. Assistant Professor Division of Hematology The Ohio State University Wexner Medical Center Case 1 22 yo woman presents to the ED with fatigue
Evaluation of the Inpatient with Anemia Camila Masias, M.D. Assistant Professor Division of Hematology The Ohio State University Wexner Medical Center Case 1 22 yo woman presents to the ED with fatigue
Faculty of Medicine Dr. Tariq Aladily
 Iron deficiency anemia The most common anemia worldwide Only 10% of ingested iron is absorbed Most dietary iron occurs in meat products Absorbed in duodenum Hepcidin By inhibiting ferroportin, hepcidin
Iron deficiency anemia The most common anemia worldwide Only 10% of ingested iron is absorbed Most dietary iron occurs in meat products Absorbed in duodenum Hepcidin By inhibiting ferroportin, hepcidin
Warm Autoantibodies in a Patient with Hemophagocytic Lymphohistiocytosis: A Case Report
 Warm Autoantibodies in a Patient with Hemophagocytic Lymphohistiocytosis: A Case Report Emily Coberly, MD Department of Pathology and Anatomical Sciences University of Missouri Columbia April 30, 2013
Warm Autoantibodies in a Patient with Hemophagocytic Lymphohistiocytosis: A Case Report Emily Coberly, MD Department of Pathology and Anatomical Sciences University of Missouri Columbia April 30, 2013
Introduction and Approach to Anemia
 2 nd lecture in Hematology by Dr.Alaa Fadhil Alwan Introduction and Approach to Anemia Anemia is defined clinically as a blood hemoglobin or hematocrit value that is below the appropriate reference range
2 nd lecture in Hematology by Dr.Alaa Fadhil Alwan Introduction and Approach to Anemia Anemia is defined clinically as a blood hemoglobin or hematocrit value that is below the appropriate reference range
Symptoms and Signs in Hematology (2)/ 2013
/ 2013") Symptoms and Signs in Hematology (2)/ 2013 Abdallah Abbadi.MD.FRCP Professor of Medicine,Hematology & Oncology University of Jordan & JUH Email: abdalla.awidi@gmail.com Case one: A 24 yr old female complains
Symptoms and Signs in Hematology (2)/ 2013 Abdallah Abbadi.MD.FRCP Professor of Medicine,Hematology & Oncology University of Jordan & JUH Email: abdalla.awidi@gmail.com Case one: A 24 yr old female complains
New phase 2 Clinical Trial Enrolling Now
 New phase 2 Clinical Trial Enrolling Now Warm Autoimmune Hemolytic Anemia (waiha) and Cold Agglutinin Disease (CAD) Designed for patients Age 18 or older With a primary diagnosis of waiha who had a recurrence,
New phase 2 Clinical Trial Enrolling Now Warm Autoimmune Hemolytic Anemia (waiha) and Cold Agglutinin Disease (CAD) Designed for patients Age 18 or older With a primary diagnosis of waiha who had a recurrence,
YEREVAN STATE MEDICAL UNIVERSITY DEPARTMENT OF HEMATOLOGY COURSE DESCRIPTION HEMATOLOGY
 1. Module/unit Code II. 1.2. 2. Module/unit Title Hematology 3. Subject Field Internal Diseases Group 4. Faculty/Department General Medicine, Department of Hematology 5. Programme(s) to which the Doctor
1. Module/unit Code II. 1.2. 2. Module/unit Title Hematology 3. Subject Field Internal Diseases Group 4. Faculty/Department General Medicine, Department of Hematology 5. Programme(s) to which the Doctor
Extra Notes 3. Warm. In the core (center) of the body, where the temperature is 37 C.
 of the body, where the temperature is 37 C.") Extra Notes 3 *The numbers of the slides are according to the last year slides. Slide 33 Autoimmune hemolytic anemia : Abnormal circulating antibodies that target normal antigen on the RBC and cause lysis.
Extra Notes 3 *The numbers of the slides are according to the last year slides. Slide 33 Autoimmune hemolytic anemia : Abnormal circulating antibodies that target normal antigen on the RBC and cause lysis.
Candidates must answer ALL questions
 Time allowed: Three hours. Part 1 examination Haematology: First paper Tuesday 22 March 2016 Candidates must answer ALL questions Question 1: General Haematology A 16 year old non-european is referred
Time allowed: Three hours. Part 1 examination Haematology: First paper Tuesday 22 March 2016 Candidates must answer ALL questions Question 1: General Haematology A 16 year old non-european is referred
Anaemias and other Pesky Haematology Questions
 Anaemias and other Pesky Haematology Questions 3 main topics How do I work out an anaemia.. That oh too common paraprotein patient. Those mildly raised lymphocyte count GP discussed patient with me over
Anaemias and other Pesky Haematology Questions 3 main topics How do I work out an anaemia.. That oh too common paraprotein patient. Those mildly raised lymphocyte count GP discussed patient with me over
Updates for your practice August 2013 TLALELETSO. HIV & Anemia. Continued on Page 2
 dates for your practice August 2013 TLALELETSO HIV & Anemia In this issue we review anemia and HIV. Medical professionals across all disciplines need to be alert to the hematological complications of HIV
dates for your practice August 2013 TLALELETSO HIV & Anemia In this issue we review anemia and HIV. Medical professionals across all disciplines need to be alert to the hematological complications of HIV
Overview of Aplastic Anemia. Overview of Aplastic Anemia. Epidemiology of aplastic anemia. Normal hematopoiesis 10/6/2017
 Overview of Aplastic Anemia Overview of Aplastic Anemia Peter Westervelt, MD, PhD Professor of Medicine Chief, BMT/Leukemia Section Washington University School of Medicine Epidemiology Normal hematopoiesis
Overview of Aplastic Anemia Overview of Aplastic Anemia Peter Westervelt, MD, PhD Professor of Medicine Chief, BMT/Leukemia Section Washington University School of Medicine Epidemiology Normal hematopoiesis
Disorders of Blood Cells & Blood Coagulation
 Disorders of Blood Cells & Blood Coagulation HIHIM 409 WBC count RBC count WBC differential Hemoglobin (HGB) Hematocrit (HCT) % of volume occupied by RBCs CBC Red cell indices Mean cell volume (MCV) average
Disorders of Blood Cells & Blood Coagulation HIHIM 409 WBC count RBC count WBC differential Hemoglobin (HGB) Hematocrit (HCT) % of volume occupied by RBCs CBC Red cell indices Mean cell volume (MCV) average
Dairion Gatot, Soegiarto Ganie, Savita Handayani. Divisi Hematologi & Onkologi Medik Departemen Ilmu Penyakit Dalam FK-USU/RS H.Adam Malik Medan 2009
 HAEMOLYTIC ANAEMIA Dairion Gatot, Soegiarto Ganie, Savita Handayani. Divisi Hematologi & Onkologi Medik Departemen Ilmu Penyakit Dalam FK-USU/RS H.Adam Malik Medan 2009 WHEN BY THEN Hb 9 g% transfusion
HAEMOLYTIC ANAEMIA Dairion Gatot, Soegiarto Ganie, Savita Handayani. Divisi Hematologi & Onkologi Medik Departemen Ilmu Penyakit Dalam FK-USU/RS H.Adam Malik Medan 2009 WHEN BY THEN Hb 9 g% transfusion
Approach to a pale child
 Approach to a pale child Dr. Dafalla Ahmed Babiker Jazan university objectives Definition of anemia Classification and causes Important points in history and physical examination Investigations. Definition
Approach to a pale child Dr. Dafalla Ahmed Babiker Jazan university objectives Definition of anemia Classification and causes Important points in history and physical examination Investigations. Definition
Hematology Unit Lab 1 Review Material
 Hematology Unit Lab 1 Review Material - 2018 Objectives Laboratory instructors: 1. Assist students during lab session Students: 1. Review the introductory material 2. Study the case histories provided
Hematology Unit Lab 1 Review Material - 2018 Objectives Laboratory instructors: 1. Assist students during lab session Students: 1. Review the introductory material 2. Study the case histories provided
Common Haematological Problems in Primary Care
 23 rd March 2019 GP Hot Topics In Primary Care Common Haematological Problems in Primary Care Dr Samar Kulkarni Consultant Haematologist-Oncologist and The Christie Private Care Manchester, UK. Haematology?
23 rd March 2019 GP Hot Topics In Primary Care Common Haematological Problems in Primary Care Dr Samar Kulkarni Consultant Haematologist-Oncologist and The Christie Private Care Manchester, UK. Haematology?
Acute haemolysis and appearance of PNH-like clones in patients with vitamin B12 deficiency and iron deficiency after iron dextran administration
 Acute haemolysis and appearance of PNH-like clones in patients with vitamin B12 deficiency and iron deficiency after iron dextran administration Chun-Liang Lin 1, Chin-Chan Lin 1,Wen-Jyi Lo 2,Yu-Chien
Acute haemolysis and appearance of PNH-like clones in patients with vitamin B12 deficiency and iron deficiency after iron dextran administration Chun-Liang Lin 1, Chin-Chan Lin 1,Wen-Jyi Lo 2,Yu-Chien
Anemia (3).ms Hemolytic Anemia. Abdallah Abbadi Feras Fararjeh
.ms Hemolytic Anemia. Abdallah Abbadi Feras Fararjeh") Anemia (3).ms4.26.2.18 Hemolytic Anemia Abdallah Abbadi Feras Fararjeh Case 3 24 yr old female presented with anemia syndrome and jaundice. She was found to have splenomegaly. Hb 8, wbc 12k, Plt 212k,
Anemia (3).ms4.26.2.18 Hemolytic Anemia Abdallah Abbadi Feras Fararjeh Case 3 24 yr old female presented with anemia syndrome and jaundice. She was found to have splenomegaly. Hb 8, wbc 12k, Plt 212k,
Management. (By the World Health Organization according to the magnitude of the enzyme deficiency and the severity of hemolysis)
") Glucose-6-Phosphate Dehydrogenase (G6PD) Deficiency Management Definition: Glucose-6-phosphate dehydrogenase (G6PD) deficiency is an inherited disorder caused by a genetic defect in the red blood cell
Glucose-6-Phosphate Dehydrogenase (G6PD) Deficiency Management Definition: Glucose-6-phosphate dehydrogenase (G6PD) deficiency is an inherited disorder caused by a genetic defect in the red blood cell
Approach to the abnormal CBC
 Approach to the abnormal CBC Robert T. Means, Jr., M.D. Hematology and Blood & Marrow Transplant Division University of Kentucky and VA Medical Center Lexington KY General Considerations Always repeat
Approach to the abnormal CBC Robert T. Means, Jr., M.D. Hematology and Blood & Marrow Transplant Division University of Kentucky and VA Medical Center Lexington KY General Considerations Always repeat
PNH Glossary of Terms
 AA Absolute neutrophil count Alendronate Allergen ALT Anemia Antibodies Anticoagulant Anticoagulation Antigen Antithymocyte globulin (ATG) Aplastic Aplastic anemia Band Bilirubin Blast cells Bone marrow
AA Absolute neutrophil count Alendronate Allergen ALT Anemia Antibodies Anticoagulant Anticoagulation Antigen Antithymocyte globulin (ATG) Aplastic Aplastic anemia Band Bilirubin Blast cells Bone marrow
The primary medical content categories of the blueprint are shown below, with the percentage assigned to each for a typical exam:
 Hematology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified hematologist
Hematology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified hematologist
Inherited Thrombophilia Testing. George Rodgers, MD, PhD Kristi Smock MD
 Inherited Thrombophilia Testing George Rodgers, MD, PhD Kristi Smock MD Prevalence and risk associated with inherited thrombotic disorders Inherited Risk Factor % General Population % Patients w/ Thrombosis
Inherited Thrombophilia Testing George Rodgers, MD, PhD Kristi Smock MD Prevalence and risk associated with inherited thrombotic disorders Inherited Risk Factor % General Population % Patients w/ Thrombosis
PCCN Review Hematology
 PCCN Review Hematology Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Anemia Definition reduction in RBC concentration Causes iron deficiency
PCCN Review Hematology Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Anemia Definition reduction in RBC concentration Causes iron deficiency
Approach to the child with anemia. Nittaya Wisanuyothin,MD. Pediatrics Department, Maharat Nakhonratchasima Hospital
 Approach to the child with anemia Nittaya Wisanuyothin,MD. Pediatrics Department, Maharat Nakhonratchasima Hospital Definition of anemia Hb< 2 SD or P2.5 below the mean for a healthy of the same gender
Approach to the child with anemia Nittaya Wisanuyothin,MD. Pediatrics Department, Maharat Nakhonratchasima Hospital Definition of anemia Hb< 2 SD or P2.5 below the mean for a healthy of the same gender
Welcome to Master Class for Oncologists. Session 3: 9:15 AM - 10:00 AM
 Welcome to Master Class for Oncologists Session 3: 9:15 AM - 10:00 AM Miami, FL December 18, 2009 Myeloproliferative Neoplasms: Bringing Order to Complexity and Achieving Optimal Outcomes Speaker: Andrew
Welcome to Master Class for Oncologists Session 3: 9:15 AM - 10:00 AM Miami, FL December 18, 2009 Myeloproliferative Neoplasms: Bringing Order to Complexity and Achieving Optimal Outcomes Speaker: Andrew
Med Chem 535 ~ Diagnostic Medicinal Chemistry. Hematology ~ Erythrocytes (Red Blood Cells, RBCs)
") Med Chem 535 ~ Diagnostic Medicinal Chemistry Hematology ~ Erythrocytes (Red Blood Cells, RBCs) I. Tests A. Red Blood Cell Count (RBC)* B. Hemoblobin (Hb or Hgb)* C. Hematocrit (Hct)* D. Wintrobe Indices
Med Chem 535 ~ Diagnostic Medicinal Chemistry Hematology ~ Erythrocytes (Red Blood Cells, RBCs) I. Tests A. Red Blood Cell Count (RBC)* B. Hemoblobin (Hb or Hgb)* C. Hematocrit (Hct)* D. Wintrobe Indices
C. treatment with Desferal (deferoxamine mesylate USP, iron-chelating agent)
") HEMOLYTIC ANEMIAS Single choice tests 1. Select the clinical manifestation that is not characteristic for the hemolytic crisis: A. decrease of the red blood cell count B. reticulocytosis C. jaundice D.
HEMOLYTIC ANEMIAS Single choice tests 1. Select the clinical manifestation that is not characteristic for the hemolytic crisis: A. decrease of the red blood cell count B. reticulocytosis C. jaundice D.
CLINICAL CASE PRESENTATION
 European Winter School of Internal Medicine 2015 Riga, Latvia, 26-30 January CLINICAL CASE PRESENTATION Vasiliy Chulkov South Ural State Medical University (Chelyabinsk, Russia) CHELYABINSK CLINICAL HISTORY
European Winter School of Internal Medicine 2015 Riga, Latvia, 26-30 January CLINICAL CASE PRESENTATION Vasiliy Chulkov South Ural State Medical University (Chelyabinsk, Russia) CHELYABINSK CLINICAL HISTORY
Case #1. Robert J. Glinert, M.D. David C. Fisher, M.D. Dana Farber Cancer Institute
 Case #1 Robert J. Glinert, M.D. David C. Fisher, M.D. Dana Farber Cancer Institute Patient History Part I 76 year-old man 1997 diagnosed with MGUS (biclonal) during evaluation of (self-limited) anemia.
Case #1 Robert J. Glinert, M.D. David C. Fisher, M.D. Dana Farber Cancer Institute Patient History Part I 76 year-old man 1997 diagnosed with MGUS (biclonal) during evaluation of (self-limited) anemia.
Dr Kirsten Herbert. Dr Melita Kenealy. MBBS(Hons) FRCPA FRACP. Common Blood Tests
 FRCPA FRACP. Common Blood Tests") Common Blood Tests Your Haematologist may order numerous blood and urine tests to help diagse or manage your condition. Listed below are some of the more common tests that can be ordered in a haematology
Common Blood Tests Your Haematologist may order numerous blood and urine tests to help diagse or manage your condition. Listed below are some of the more common tests that can be ordered in a haematology
The function of the bone marrow. Living with Aplastic Anemia. A Case Study - I. Hypocellular bone marrow failure 5/14/2018
 The function of the bone marrow Larry D. Cripe, MD Indiana University Simon Cancer Center Bone Marrow Stem Cells Mature into Blood Cells Mature Blood Cells and Health Type Function Term Red Cells Carry
The function of the bone marrow Larry D. Cripe, MD Indiana University Simon Cancer Center Bone Marrow Stem Cells Mature into Blood Cells Mature Blood Cells and Health Type Function Term Red Cells Carry
Diagnosis / Lab Findings
 Diagnosis / Lab Findings During at acute episode may see Peripheral smear bite cells, Heinz bodies Reticulocytosis Increased indirect bilirubin G6PD will be normal or high during an acute crisis Repeat
Diagnosis / Lab Findings During at acute episode may see Peripheral smear bite cells, Heinz bodies Reticulocytosis Increased indirect bilirubin G6PD will be normal or high during an acute crisis Repeat
Management of anemia in CKD
 Management of anemia in CKD Pierre Cochat, MD PhD Professor of Pediatrics Chair, Pediatrics & Pediatric Surgery Department Head, Center for Rare Renal Diseases Néphrogones Hospices Civils de Lyon & University
Management of anemia in CKD Pierre Cochat, MD PhD Professor of Pediatrics Chair, Pediatrics & Pediatric Surgery Department Head, Center for Rare Renal Diseases Néphrogones Hospices Civils de Lyon & University
VENOUS THROMBOEMBOLISM AND CORONARY ARTERY DISEASE: IS THERE A LINK?
 VENOUS THROMBOEMBOLISM AND CORONARY ARTERY DISEASE: IS THERE A LINK? Ayman El-Menyar (1), MD, Hassan Al-Thani (2),MD (1)Clinical Research Consultant, (2) Head of Vascular Surgery, Hamad General Hospital
VENOUS THROMBOEMBOLISM AND CORONARY ARTERY DISEASE: IS THERE A LINK? Ayman El-Menyar (1), MD, Hassan Al-Thani (2),MD (1)Clinical Research Consultant, (2) Head of Vascular Surgery, Hamad General Hospital
Cytopaenias in HIV. Dr Maresce Bizaare Specialist Physician Clinical Haematology Fellow IALCH
 Cytopaenias in HIV Dr Maresce Bizaare Specialist Physician Clinical Haematology Fellow IALCH Introduction Cytopaenias in HIV are common Anaemias multifactorial causes Thrombocytopaenias may be the first
Cytopaenias in HIV Dr Maresce Bizaare Specialist Physician Clinical Haematology Fellow IALCH Introduction Cytopaenias in HIV are common Anaemias multifactorial causes Thrombocytopaenias may be the first
9/23/2018. Investigation of Hemolysis in the Clinical Laboratory. Objectives. What is hemolysis?
 Investigation of Hemolysis in the Clinical Laboratory Jason Anderson, MPH, MT(ASCP) Field Product Specialist Objectives 1. Define hemolysis. 2. Distinguish between intrinsic and extrinsic hemolysis 3.
Investigation of Hemolysis in the Clinical Laboratory Jason Anderson, MPH, MT(ASCP) Field Product Specialist Objectives 1. Define hemolysis. 2. Distinguish between intrinsic and extrinsic hemolysis 3.
HEMATOLOGY Maintenance of Certification (MOC) Examination Blueprint
 Examination Blueprint") HEMATOLOGY Maintenance of Certification (MOC) Examination Blueprint ABIM invites diplomates to help develop the Hematology MOC exam blueprint Based on feedback from physicians that MOC assessments should
HEMATOLOGY Maintenance of Certification (MOC) Examination Blueprint ABIM invites diplomates to help develop the Hematology MOC exam blueprint Based on feedback from physicians that MOC assessments should
Smoldering Multiple Myeloma. A Case Study
 Smoldering Multiple Myeloma A Case Study Case Presentation 53-Year-Old Male Patient presented for a routine exam No prior history of disease or family history of fhematologic disorders d or malignancies,
Smoldering Multiple Myeloma A Case Study Case Presentation 53-Year-Old Male Patient presented for a routine exam No prior history of disease or family history of fhematologic disorders d or malignancies,
Smoldering Myeloma: Leave them alone!
 Smoldering Myeloma: Leave them alone! David H. Vesole, MD, PhD Co-Director, Myeloma Division Director, Myeloma Research John Theurer Cancer Center Hackensack University Medical Center Prevalence 1960 2002
Smoldering Myeloma: Leave them alone! David H. Vesole, MD, PhD Co-Director, Myeloma Division Director, Myeloma Research John Theurer Cancer Center Hackensack University Medical Center Prevalence 1960 2002
TYPE 1 GAUCHER DISEASE PRESENTING AS PERSISTENT THROMBOCYTOPENIA, ASSOCIATED FACTOR XI DEFICIENCY & EMERGENT MYELOMA
 TYPE 1 GAUCHER DISEASE PRESENTING AS PERSISTENT THROMBOCYTOPENIA, ASSOCIATED FACTOR XI DEFICIENCY & EMERGENT MYELOMA Trish Hyland, Medical Scientist, Department of Haematology, Cork University Hospital
TYPE 1 GAUCHER DISEASE PRESENTING AS PERSISTENT THROMBOCYTOPENIA, ASSOCIATED FACTOR XI DEFICIENCY & EMERGENT MYELOMA Trish Hyland, Medical Scientist, Department of Haematology, Cork University Hospital
Susan Stegman, MD Medical Director AXA Equitable Life May 3, 2016
 Susan Stegman, MD Medical Director AXA Equitable Life May 3, 2016 Underwriting impact Anemia overview Classification of anemia Specific anemia topics Iron deficiency anemia Thalassemia Megaloblastic anemia
Susan Stegman, MD Medical Director AXA Equitable Life May 3, 2016 Underwriting impact Anemia overview Classification of anemia Specific anemia topics Iron deficiency anemia Thalassemia Megaloblastic anemia
SAUDI FELLOWSHIP TRAINING PROGRAM. Adult Haematology. Final Written Examination 2019
 SAUDI FELLOWSHIP TRAINING PROGRAM Adult Haematology Final Written Examination 2019 Examination Format: A. The Saudi fellowship specialty final written examination shall consist of one paper with 80-120
SAUDI FELLOWSHIP TRAINING PROGRAM Adult Haematology Final Written Examination 2019 Examination Format: A. The Saudi fellowship specialty final written examination shall consist of one paper with 80-120
Updates in the Management of Anemia in Cancer. Taylor M. Ortiz, MD May 19, 2017
 Updates in the Management of Anemia in Cancer Taylor M. Ortiz, MD May 19, 2017 Objectives Recall common causes of anemia in patients with cancer Understand risks/benefits of blood transfusion in patients
Updates in the Management of Anemia in Cancer Taylor M. Ortiz, MD May 19, 2017 Objectives Recall common causes of anemia in patients with cancer Understand risks/benefits of blood transfusion in patients
Treatment of Waldenström s Macroglobulinemia Mayo Consensus
 Treatment of Waldenström s Macroglobulinemia Mayo Consensus Scottsdale, Arizona Rochester, Minnesota Jacksonville, Florida Mayo Clinic College of Medicine Mayo Clinic Comprehensive Cancer Center Mayo Clinic
Treatment of Waldenström s Macroglobulinemia Mayo Consensus Scottsdale, Arizona Rochester, Minnesota Jacksonville, Florida Mayo Clinic College of Medicine Mayo Clinic Comprehensive Cancer Center Mayo Clinic
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Acute lymphoblastic leukemia, in India, 439 440 pediatric, global approach to, 420 424 core resources in low- and middle-income countries, 423
Note: Page numbers of article titles are in boldface type. A Acute lymphoblastic leukemia, in India, 439 440 pediatric, global approach to, 420 424 core resources in low- and middle-income countries, 423
Platelet and WBC disorders
 Division of Family Practice Platelet and WBC disorders Adrian Yee MD FRCPC Clinical hematologist Assistant Dean, undergraduate education, IMP asyee@uvic.ca When we understand that slide, we'll have won
Division of Family Practice Platelet and WBC disorders Adrian Yee MD FRCPC Clinical hematologist Assistant Dean, undergraduate education, IMP asyee@uvic.ca When we understand that slide, we'll have won
Don t Miss Causes of Anemia. Reed E. Drews, M.D. Beth Israel Deaconess Medical Center Harvard Medical School Boston, MA COPYRIGHT
 Don t Miss Causes of Anemia Reed E. Drews, M.D. Beth Israel Deaconess Medical Center Harvard Medical School Boston, MA Conflicts of Interest UpToDate Section Editor & Author Royalties I do not have other
Don t Miss Causes of Anemia Reed E. Drews, M.D. Beth Israel Deaconess Medical Center Harvard Medical School Boston, MA Conflicts of Interest UpToDate Section Editor & Author Royalties I do not have other
FBC CASES Vernon Louw Clinical Haematology 2010
 FBC CASES Vernon Louw Clinical Haematology 2010 FOR EACH OF THE FOLLOWING PATIENTS, SELECT THE MOST LIKELY FINDING FROM THE ANALYSIS OF THE PERIPHERAL BLOOD. A patient with infectious mononucleosis. A
FBC CASES Vernon Louw Clinical Haematology 2010 FOR EACH OF THE FOLLOWING PATIENTS, SELECT THE MOST LIKELY FINDING FROM THE ANALYSIS OF THE PERIPHERAL BLOOD. A patient with infectious mononucleosis. A
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Anemia(s), 412 426 categories in morphologic approach to, macrocytic, 412 414 microcytic, 412 414 normocytic, 412 413 categorizing, 412
Index Note: Page numbers of article titles are in boldface type. A Anemia(s), 412 426 categories in morphologic approach to, macrocytic, 412 414 microcytic, 412 414 normocytic, 412 413 categorizing, 412
5/5/2010. Goldilocks picture from
 Sometimes platelet counts are TOO LOW; Goldilocks and the Three Platelets Robert T. Means, Jr., M.D. Professor & Senior Associate Chair Department of Internal Medicine University of Kentucky Lexington
Sometimes platelet counts are TOO LOW; Goldilocks and the Three Platelets Robert T. Means, Jr., M.D. Professor & Senior Associate Chair Department of Internal Medicine University of Kentucky Lexington
FBC interpretation. Dr. Gergely Varga
 FBC interpretation Dr. Gergely Varga #1 71 Y/O female, c/o weakness Test Undertaken : FBC (FBC) Sample Type: Whole Blood [ - 26.09.11 14:59] Hb 7.3 g/dl* 12.0-15.5 RBC 3.5 10^12/l * 3.80-5.60 Hct 0.24
FBC interpretation Dr. Gergely Varga #1 71 Y/O female, c/o weakness Test Undertaken : FBC (FBC) Sample Type: Whole Blood [ - 26.09.11 14:59] Hb 7.3 g/dl* 12.0-15.5 RBC 3.5 10^12/l * 3.80-5.60 Hct 0.24
Marc Geirnaert Director of Provincial Oncology Drug Program CancerCare Manitoba
 Marc Geirnaert Director of Provincial Oncology Drug Program CancerCare Manitoba Advisory board participant for lenalidomide in 2013 Not applicable Understand the role of prophylaxis for herpes zoster Be
Marc Geirnaert Director of Provincial Oncology Drug Program CancerCare Manitoba Advisory board participant for lenalidomide in 2013 Not applicable Understand the role of prophylaxis for herpes zoster Be
An Oncologist s Approach to Anemia in Adults Christie J. Hilton, DO
 An Oncologists Approach to Anemia in Adults (There are not many updates) Christie Hilton DO POMA Winter Symposium 2019 Nemicolin Woodlands 8 Disclosures None 9 Objectives Define anemia Review the classification
An Oncologists Approach to Anemia in Adults (There are not many updates) Christie Hilton DO POMA Winter Symposium 2019 Nemicolin Woodlands 8 Disclosures None 9 Objectives Define anemia Review the classification
Cancer and Thrombosis
 Cancer and Thrombosis The close relationship between venous thromboembolism and cancer has been known since at least the 19th century by Armand Trousseau. Thrombosis is a major cause of morbidity and mortality
Cancer and Thrombosis The close relationship between venous thromboembolism and cancer has been known since at least the 19th century by Armand Trousseau. Thrombosis is a major cause of morbidity and mortality
Hematology 101. Rachid Baz, M.D. 5/16/2014
 Hematology 101 Rachid Baz, M.D. 5/16/2014 Florida 101 Epidemiology Estimated prevalence 8,000 individuals in U.S (compare with 80,000 MM patients) Annual age adjusted incidence 3-8/million-year 1 More
Hematology 101 Rachid Baz, M.D. 5/16/2014 Florida 101 Epidemiology Estimated prevalence 8,000 individuals in U.S (compare with 80,000 MM patients) Annual age adjusted incidence 3-8/million-year 1 More