Type 2 Diabetes Mellitus: Update on Pharmacotherapy 04/04/18
|
|
|
- Edward Weaver
- 6 years ago
- Views:
Transcription
1 Type 2 Diabetes Mellitus: Update on Pharmacotherapy 04/04/18
2 No conflicts of interest
3 Objectives for this talk Update on non-insulin drug therapy fro type 2 DM Appropriate use of insulin in type 2 DM
4 ADA Treatment Goals for Glycemic Control General goal for non-pregnant adults Pre-meal Peak post-meal (measure 1-2 h after start of meal) HbA1c < 7.0% (normal < 5.7%) mg/100 ml < 180 mg/100 ml More stringent for selected Individuals short duration of diabetes treatment with lifestyle or metformin only long life expectancy no significant cardiovascular disease. As close to normal as possible without significant hypoglycemia Less stringent for some patients hypoglycemia unawareness limited life expectancy co-morbidity long hx DM with minimal complications where control has been historically difficult HbA1c < 8.0 American Diabetes Association: Standards of Care (Diabetes Care 1, Jan a) Online
5 Metformin Near universal acceptance as initial drug therapy in absence of contraindication (e.g. renal failure, hypoxia) or intolerance Decrease hepatic glucose release and increases muscle glucose uptake Beneficial effects on weight and lipids Lack of hypoglycemia when used alone Generic drug with long history of use worldwide (over 50 yr) Evidence from several studies supports a reduction in CV events, improved carotid IMT UKPDS showed a significant reduction in MI and cardiac and all cause mortality by 39, 50, and 36% respectively when administered to obese patients (weight > 120% of ideal).
6 Severe hyperglycemia Insulin Initial Pharmacologic treatment Metformin Contraindication or intolerance to metformin) Goal achieved Goal not achieved Add second drug Another drug What drug?
7 Sulfonylureas Mechanism of action: β-cell insulin secretion by activating potassium channels Glipizide, Glimepiride Glyburide (glibenclamide) more hypoglycemia, maybe adverse interactions with cardiac channels Advantages: Well tolerated Low cost Disadvantages: Hypoglycemia Weight gain Sulfa allergy May have low durability
8 Sulfonylureas (CV effects) UGDP (1970s) increased CV mortality (controversial) Retrospective and some prospective analyses of databases support increased risk But major large scale trials (UKPDS, ADVANCE, ACCORD) do not support increased CV risk
9 Dipeptidyl peptidase -4 (DPP-4) inhibitors Several available Sitagliptin (Januvia) Alogliptin (Nesina) Saxagliptin (Onglyza) Linagliptin (Tradjenta) (no renal adjustment) Block degradation of endogenous GLP-1 Not very effective in lowering A1c Advantages Little or no hypoglycemia Disadvantages Urticaria, angioedema Pancreatitis risk
10 DPP-4 inhibitors (CV effects) Weight neutral Decrease TG, may reduce hscrp, may improve endothelial function, and improve reduce ischemia-reperfusion in animals, may decrease IMT (diabetes care Dec 2015 online) Two large CV outcome trials in high risk patients (SAVOR-TIMI and EXAMINE) showed no difference in outcomes Slight increase in hospitalization for CHF TECOS trial 14,671 patients to add either sitagliptin or placebo, no diff in CV events (839 vs. 851 No difference in hospitalization for CHF
11 GLP-1 agonists Several drugs differing in duration of action Exenatide (Byetta) Short-acting BID (needs renal adjustment) Long acting exenatide (Bydureon) Weekly (needs renal adjustment) Lixisenatide (Lyxumia) Intermediate-acting Daily Liraglutide (Victoza) Long-acting Weekly Dulaglutide (Trulicity) Long-acting Weekly Albiglutide (Tanzeum) Long-acting Weekly Activate GLP-1 receptors in pancreatic β -cell and nervous system glucose-induced insulin secretion, glucagon, gastric emptying, satiety Decreased hepatic glucose production Decreased post-prandial glucose Durable up to at least 3 years, may increase β -cell mass Mild weight loss Disadvantages Nausea, vomiting, or diarrhea Pancreatitis risk Medullary thyroid tumors
12 GLP-1 agonists (CV effects) Many favorable effects on CV risk factors: Decrease weight and visceral fat, decrease BP, increase urinary sodium, improved endothelial function, decrease TG, FFA levels LEADER trial Randomized double blind trial, 9340 subjects with type 2 diabetes at high risk for CV disease or with CV disease. Assessed the effect of liraglutide, a GLP-1 receptor agonist, versus placebo and standard care, on CV outcomes Mean age 64 years and mean duration of diabetes 13 years. Composite primary outcome (MI, stroke, or cardiovascular death) occurred in fewer participants in the treatment group (13.0%) when compared with the placebo group (14.9%) after a median follow-up of 3.8 years Whether this drug class will have similar effects in lower-risk patients with diabetes remains unknown. SUSTAIN-6 Studied 2375 patients with type 2 diabetes who were at high CV risk Primary outcome (MI, stroke, or cardiovascular death) occurred in 108 of 1648 patients (6.6%) in the semaglutide group and in 146 of 1649 patients (8.9%) in the placebo group (hazard ratio, p<0.001)
13
14 Sodium-glucose co-transporter-2 (SGLT2) inhibitors (SGLT2) Several drugs Canagliflozin (Invokana) Dapagliflozin (Farxiga) Empagliflozin (Jardiance) Inhibits hsglt2 (sodium/glucose cotransporter) in renal tubules Urine glucose mg/day At base HbA1c of 8, will drop by (similar to metformin at that base)
15 Sodium-glucose co-transporter-2 (SGLT2) inhibitors Avoid if renal dysfunction Advantages Hypoglycemia very unusual Familial renal glycosuria is a benign disease Unique action, Can combine with all other agents CV effects appear beneficial Disadvantages UTIs vulvovaginitis, balanitis Osmotic diuresis with possible dehydration and hypotension Increased hepatic glucose output Risk of DKA
16 Sodium-glucose co-transporter-2 inhibitors (CV effects) By inhibiting salt reabsorption in the proximal tubule vascular volume decreases with BP drop 4-6 mmhg. Weight loss of kg over 6-12 mos persisting for 2 years Small increase in LDL and HDL cholesterol Decrease in serum uric acid due to uric acid and glucose co-transport in proximal tubule Meta-analyses suggests decreased CV risk (HR 0.82) EMPA-REG NEJM Sept patients were treated (median observation time, 3.1 years). HR for combined CV event favored drug over placebo at 0.82 (10.5% vs, 12.1%) Decreased hospitalization for CHF (2.7% VS. 4.1%)
17 Cardiovascular Outcomes and Death from Any Cause. Zinman B et al. N Engl J Med 2015;373:
18 DKA induced by SGLT2 inhibition May not be recognized as glucose may not be as high as typically seen in DKA Mechanism not unresolved, several hypotheses: Increase in glucagon, decrease in insulin Increased reabsorption of ketone with concomitant delayed clearance of ketone (may not see ketonuria) Shift in substrate utilization to fatty acid with concomitant increase in ketone body production Weight loss with concomitant sarcopenia Associated dehydration, fluid loss (gastroenteritis) or poor fluid intake (vomiting) and infections, in a poor metabolic milieu, might also trigger this event, making the patient ketosis-prone.
19 SGLT2 inhibitors + Insulin 1402 subjects with type 1 DM on insulin randomized to sotagliflozin (400 mg per day) or placebo for 24 weeks. Sotagliflozin group significantly improved glycated hemoglobin (difference, 0.46 percentage points), weight ( 2.98 kg), systolic BP ( 3.5 mm Hg), and mean daily bolus dose of insulin ( 2.8 units per day) The rate of diabetic ketoacidosis was higher in the sotagliflozin group than in the placebo group (3.0% [21 patients] and 0.6% [4], respectively). Garg, et al NEJM Sept. 2017
20 Drug Actions Mechanism Advantages Disadvantages Meglitinides repaglinide nateglinide Thiazolidinediones (TZDs) pioglitazone rosiglitazone α-glucosidase Inhibitors acarbose miglitol β-cell insulin secretion Insulin sensitivity mainly in muscle intestinal glucose absorption Potassium channels Activate PPAR-γ Inhibit α- glucosidase Colesevelam Unclear Bile acid sequestrant Bromocriptine Drugs for type 2 diabetes beyond metformin (less often used) Insulin sensitivity Hypothalamic dopaminergic effect Action focused on time of food intake Pioglit HDL, TG No hypoglycemia Nonsystemic No hypoglycemia No hypoglycemia No hypoglycemia Not very effective Other concerns shared with sulfonylureas Any use is questionable Wt gain, edema, CHF, LDL, bone fractures, bladder CA Rosiglit CV events Not very effective GI gas, diarrhea Constipation, TGS absorption of meds Dizziness, syncope, nausea, fatigue, rhinitis, Long term safety?
21 Severe hyperglycemia Insulin Initial Pharmacologic treatment Metformin Contraindication or intolerance to metformin) Goal achieved Goal not achieved Add second drug Another drug What drug?
22 What drug after metformin? Ask what you want to accomplish (see next slide) Consider other possible adverse effects and contraindications Acceptance of injections Higher Hb A1c favors insulin Cost
23 Drug Efficacy # Metformin High No GLP-1 agonists DPP-4 inhibitors SGLP-2 inhibitors High No Weight change Neutral to modest Cost ASCVD CHF Low Less High Neutral or Benefit Neutral or Benefit Low * No Neutral High Neutral Neutral Neutral Possible risk Hypoglycemia Intermediate No Less High Benefit Benefit Sulfonylureas High Yes More Low Neutral Neutral Thiazolidinediones High No More Low Neutral or Benefit Increased risk Insulin Highest Yes More High Neutral Neutral * ADA classifies as intermediate, low in presenter s experience # High HbA1c change up to 2% (may be less), intermediate 0.5 to 1% American Diabetes Association: Standards of Care (Diabetes Care 1, Jan a) Online
24 Insulin Advantages Disadvantages Most effective Natural Once daily for many patients Less weight gain than TZD Essentially no side effects apart from hypoglycemia Hypoglycemia Weight gain Injections
25 Does insulin impose CV risk or mortality? UK cohort study of 165,308 adults with type 2 DM. After applying structural models, insulin dose was not associated with mortality in any group. Study provides reassurance. In the DCCT/Epidemiology of Diabetes Interventions and Complications (EDIC) cohort, there were fewer CV events in the intensive arm, where subjects received higher insulin doses, than in the conventional arm. In the UKPDS no increase in CV events was found among in individuals assigned to treatment with insulin After adjustment for baseline covariates, no significant association of insulin dose with CV risk in ACCORD. Diabetes Care 2015;38: Gamble et. al. Lancet Diabetes Endocrinol (1):43-52;2017
26 Insulin effects to keep in mind Insulin can increase sodium retention and stimulate the sympathetic nervous system. Insulin has been shown to be anti-inflammatory, antioxidant, and profibrinolytic and cardioprotective in patients with acute myocardial infarction. Overall, insulin does not induce ASCVD when administered properly for diabetes control in humans and lowering glucose to target range is desirable in many ways. Mirza SA Comment, Arch Intern Med 167; Sun et. al. World J Diabetes 5(2):
27

28 Degludec 42 h
29 Insulin regimens Simple: once or twice daily Complex: basal and bolus Rx using multiple doses Choice depends on severity of diabetes JAMA 289: , 2003 Med Clin N Am 88, , 2004
30
31 Basal Insulin
32 Bolus Basal
33 Basal
34 Insulin dosing in type 2 DM With lower A1c and relatively stable glucose, control may require only basal insulin Weight based (may not be the best approach) Start with units depending on A1c or 0.2 units/kg Can often start with a low dose, but very large amounts may eventually be needed due to resistance requiring vigorous titration. May need large amounts in sick patients due to stress, steroids, tube feeds, etc Severely insulin deficient: needs may approach like that in type 1 diabetes requiring basal/bolus regimen or insulin pump therapy
35 756 subjects with type 2 DM age Followed algorithm Diabetes Care, Nov. 2003
36
37
38 Basal/bolus (MDI or pump) For marked insulin deficiency approximately one-half of the total dose should be given as a basal insulin, either as once or twice per day long-acting insulin. (glargine or detemir) or as twice per day intermediateacting insulin (NPH). Glargine or detemir can be given either at bedtime or in the morning. May need to change to BID Bolus insulin is given as short or rapid-acting insulin, divided before meals. The pre-meal dosing is determined by the pre-meal glucose level, meal size and content, as well as activity and exercise pattern.
39 Adjust for exercise Match food to activity - Take enough extra food to balance out activity Take additional food during and/or after activity Reduce insulin if the goal is weight loss
40 Types of insulin Non-analog (biosynthetic human insulin) sold as Humulin N or Humulin R, Novolin N or Novolin R N = NPH, R = regular Commonly used analogs Long acting: glargine, detemir Fast acting: lispro, aspart, glulisine Newer insulin preparations U-500 vial or pen form U-300 glargine (sold as Toujeo) U-200 lispro Degludec: extra long acting (sold as Tresiba) Inhaled (sold as Afrezza) Pre-mixed long acting/short acting, 50-75/25-50
41 Degludec (Tresiba) Duration 42h, onset Administered daily Modified insulin that has one single amino acid deleted in comparison to human insulin, and is conjugated to hexadecanedioic acid via gamma-lglutamyl spacer at the amino acid lysine at position B29. BEGIN Basal-Bolus Type 2 trial (755 pts on degludec, 251 on glargine), less hypoglycemia and less nocturnal hypoglycemia, otherwise non-inferior to glargine


42 U-500 insulin 500 units/ml (as opposed to 100 units/ml for U-100 insulin There are no U-500 syringes so, e.g. 25 units drawn in a U-100 syringe will deliver 125 units of insulin. Formulated as regular insulin but duration longer than regular Generally used in multiple doses pre-meals and sometimes HS but does not match well to meal glucose absorption Can be used in pumps Prescribing information, Eli Lilly Co, Indianapolis, IN
43 U-500 regular insulin Sold as Humulin R U-500 Now approved in pen form Do not convert dosing Pen can deliver up to 300 units in a single injection
44 Other concentrated insulins U-300 glargine (Toujeo) U-200 lispro Degludec available as U-100 or U-200
45 S.C. Insulin Pumps (CSII) Use estimated as about 40% of patients with type 1 DM in the USA and with increasing frequency in type 2 DM. Can be used with a real-time S.C. sensor but (currently) does not act on monitored blood glucose except in limited fashion. Does require calibration using fingerstick recordings. Requires pump needle insertion recommended every three days. Advantages: Convenient, better control of basal insulin, can use a square wave, can be linked to sensors Indications: Type 1 or Type 2 with substantial insulin deficiency. Educated patient able to use pump effectively.

46 Original Insulin Pump 1963 First insulin pump Basal and bolus infusions used.



47 Continuous subcutaneous insulin infusion

48 Mini Med 670G/Enlite 3 Hybrid Closed loop system The MiniMed 670G is FDA approved for people with type 1 diabetes ages 14 and over, though a pediatric study (7-13 year olds) is currently underway to investigate an expansion in how it can be prescribed. The device cannot be used in children less than seven years old and those on less than eight units of insulin per day.

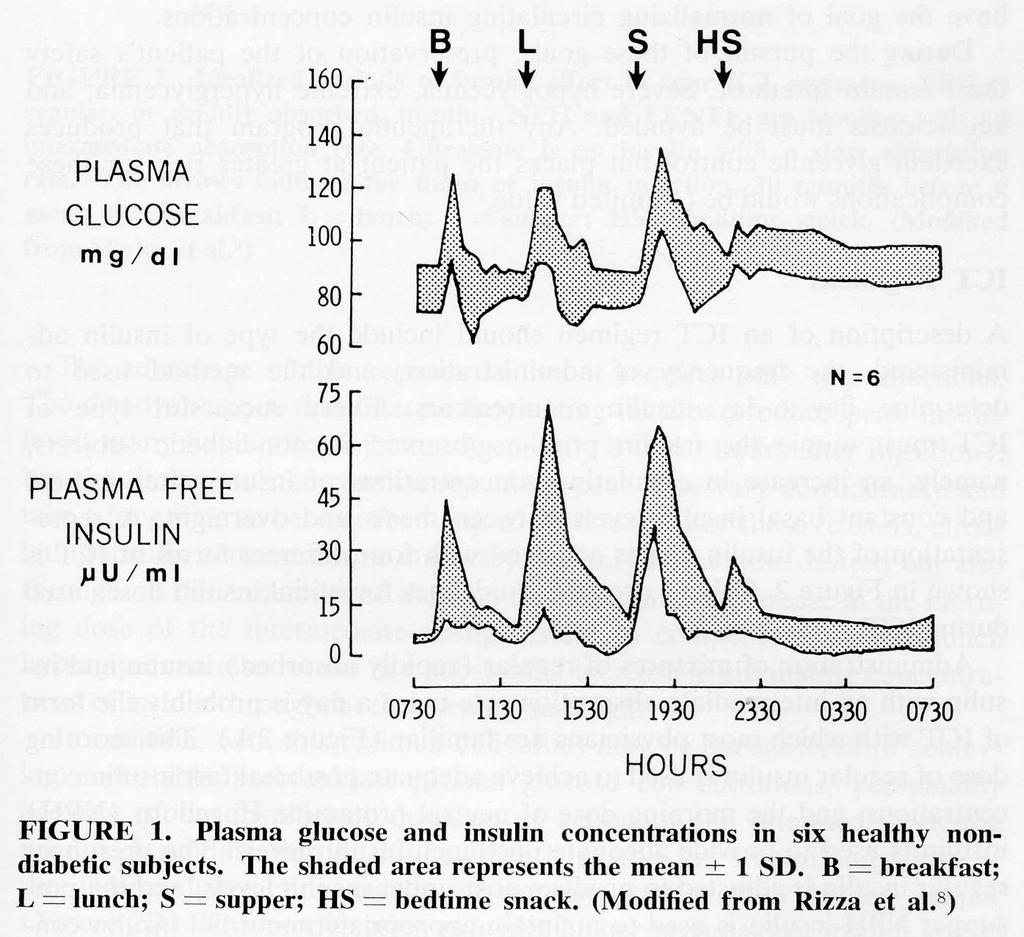
49 The Artificial Pancreas For the future
, plasma insulin levels (D), and glucagon levels (E)")

50 Mean (SD) of venous PG (A), CGMG (B), insulin and glucagon doses (C), plasma insulin levels (D), and glucagon levels (E) for all experiments. 6 subjects, followed 48h q 15 min venous blood measurement. Russell et.al. Diabetes Care, 35: ,2012
51 END
Pharmacology Updates. Quang T Nguyen, FACP, FACE, FTOS 11/18/17
 Pharmacology Updates Quang T Nguyen, FACP, FACE, FTOS 11/18/17 14 Classes of Drugs Available for the Treatment of Type 2 DM in the USA ### Class A1c Reduction Hypoglycemia Weight Change Dosing (times/day)
Pharmacology Updates Quang T Nguyen, FACP, FACE, FTOS 11/18/17 14 Classes of Drugs Available for the Treatment of Type 2 DM in the USA ### Class A1c Reduction Hypoglycemia Weight Change Dosing (times/day)
Type 2 Diabetes: Where Do We Start with Treatment? DIABETES EDUCATION. Diabetes Mellitus: Complications and Co-Morbid Conditions
 Diabetes Mellitus: Complications and Co-Morbid Conditions ADA Guidelines for Glycemic Control: 2016 Retinopathy Between 2005-2008, 28.5% of patients with diabetes 40 years and older diagnosed with diabetic
Diabetes Mellitus: Complications and Co-Morbid Conditions ADA Guidelines for Glycemic Control: 2016 Retinopathy Between 2005-2008, 28.5% of patients with diabetes 40 years and older diagnosed with diabetic
The Death of Sulfonylureas? A Review of New Diabetes Medications
 The Death of Sulfonylureas? A Review of New Diabetes Medications Kelly Hoenig, Pharm.D., BCPS Cedar Rapids Family Medicine Residency 2/4/17 Objectives Review GLP-1 Agonists, DPP-IV Inhibitors and SGLT-2
The Death of Sulfonylureas? A Review of New Diabetes Medications Kelly Hoenig, Pharm.D., BCPS Cedar Rapids Family Medicine Residency 2/4/17 Objectives Review GLP-1 Agonists, DPP-IV Inhibitors and SGLT-2
What s New in Diabetes Medications. Jena Torpin, PharmD
 What s New in Diabetes Medications Jena Torpin, PharmD 1 Objectives Discuss new medications in the management of diabetes Understand the mechanism of the medications discussed Understand the side effects
What s New in Diabetes Medications Jena Torpin, PharmD 1 Objectives Discuss new medications in the management of diabetes Understand the mechanism of the medications discussed Understand the side effects
Update on Therapies for Type 2 Diabetes: Angela D. Mazza, DO July 31, 2015
 Update on Therapies for Type 2 Diabetes: 2015 Angela D. Mazza, DO July 31, 2015 Objectives To present the newer available therapies for the management of T2D To discuss the advantages and disadvantages
Update on Therapies for Type 2 Diabetes: 2015 Angela D. Mazza, DO July 31, 2015 Objectives To present the newer available therapies for the management of T2D To discuss the advantages and disadvantages
What s New in Type 2 Diabetes? 2018 Diabetes Updates
 What s New in Type 2 Diabetes? 2018 Diabetes Updates Gretchen Ray, PharmD, PhC, BCACP, CDE Associate Professor, UNM College of Pharmacy January 28, 2018 gray@salud.unm.edu OBJECTIVES Describe the most
What s New in Type 2 Diabetes? 2018 Diabetes Updates Gretchen Ray, PharmD, PhC, BCACP, CDE Associate Professor, UNM College of Pharmacy January 28, 2018 gray@salud.unm.edu OBJECTIVES Describe the most
Jonathan Stoehr, MD PhD Endocrinology, Diabetes, Metabolism and Nutrition Virginia Mason Medical Center Seattle, WA 2012 Virginia Mason Medical
 Jonathan Stoehr, MD PhD Endocrinology, Diabetes, Metabolism and Nutrition Virginia Mason Medical Center Seattle, WA There is no conflict of interest that could be perceived as prejudicing the impartiality
Jonathan Stoehr, MD PhD Endocrinology, Diabetes, Metabolism and Nutrition Virginia Mason Medical Center Seattle, WA There is no conflict of interest that could be perceived as prejudicing the impartiality
Objectives. Recognize all available medical treatment options for diabetes. Individualize treatment and glycemic target based on patient factors
 No disclosure Objectives Recognize all available medical treatment options for diabetes Individualize treatment and glycemic target based on patient factors Should be able to switch to more affordable
No disclosure Objectives Recognize all available medical treatment options for diabetes Individualize treatment and glycemic target based on patient factors Should be able to switch to more affordable
What s New in Type 2 Diabetes? 2018 Diabetes Updates
 What s New in Type 2 Diabetes? 2018 Diabetes Updates Jessica Conklin, PharmD, PhC, BCACP, CDE, AAHIP Associate Professor, UNM College of Phar macy jeconklin@salud.unm.edu Luis Gonzales, PharmD, PhC UNM
What s New in Type 2 Diabetes? 2018 Diabetes Updates Jessica Conklin, PharmD, PhC, BCACP, CDE, AAHIP Associate Professor, UNM College of Phar macy jeconklin@salud.unm.edu Luis Gonzales, PharmD, PhC UNM
What the Pill Looks Like. How it Works. Slows carbohydrate absorption. Reduces amount of sugar made by the liver. Increases release of insulin
 Diabetes s Oral s - Pills These are some of the pills that are currently available in Canada to treat diabetes. Each medication has benefits and side effects you should be aware of. Your diabetes team
Diabetes s Oral s - Pills These are some of the pills that are currently available in Canada to treat diabetes. Each medication has benefits and side effects you should be aware of. Your diabetes team
Diabetes Oral Agents Pharmacology. University of Hawai i Hilo Pre-Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D
 Diabetes Oral Agents Pharmacology University of Hawai i Hilo Pre-Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 1 Learning Objectives Understand the role of the utilization of free
Diabetes Oral Agents Pharmacology University of Hawai i Hilo Pre-Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 1 Learning Objectives Understand the role of the utilization of free
Objectives. How Medicine Works to Control Blood Sugar Levels. What Happens When We Eat? What is diabetes? High Blood Glucose (Hyperglycemia)
") How Medicine Works to Control Blood Sugar Levels Stacie Petersen, RN, CDE Objectives Define Diabetes List how medications work (ominous octet) Identify side effects of medications for diabetes What is
How Medicine Works to Control Blood Sugar Levels Stacie Petersen, RN, CDE Objectives Define Diabetes List how medications work (ominous octet) Identify side effects of medications for diabetes What is
GLP-1 (glucagon-like peptide-1) Agonists (Byetta, Bydureon, Tanzeum, Trulicity, Victoza ) Step Therapy and Quantity Limit Criteria Program Summary
 Agonists (Byetta, Bydureon, Tanzeum, Trulicity, Victoza ) Step Therapy and Quantity Limit Criteria Program Summary") OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) s (Byetta/exenatide, Bydureon/ exenatide extended-release, Tanzeum/albiglutide, Trulicity/dulaglutide, and Victoza/liraglutide) Step Therapy
OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) s (Byetta/exenatide, Bydureon/ exenatide extended-release, Tanzeum/albiglutide, Trulicity/dulaglutide, and Victoza/liraglutide) Step Therapy
Images have been removed from the PowerPoint slides in this handout due to copyright restrictions. Insulins. Rapid Short Intermediate Long Mix
 Diabetes Medications Diabetes Medications Type 1 Insulin is needed Type 2 Oral Diabetes Medications Or Oral Diabetes Medications plus Insulin Or Insulin Alone Diabetes Medications Secretagogues Glipizide
Diabetes Medications Diabetes Medications Type 1 Insulin is needed Type 2 Oral Diabetes Medications Or Oral Diabetes Medications plus Insulin Or Insulin Alone Diabetes Medications Secretagogues Glipizide
Table 1. Antihyperglycemic agents for use in type 2 diabetes
 Table 1. Antihyperglycemic agents for use in type 2 diabetes DRUG IN ALPHA-GLUCOSIDASE INHIBITOR: inhibits pancreatic alpha-amyle and intestinal alpha-glucoside Acarbose (Glucobay) 0.6% Negligible Not
Table 1. Antihyperglycemic agents for use in type 2 diabetes DRUG IN ALPHA-GLUCOSIDASE INHIBITOR: inhibits pancreatic alpha-amyle and intestinal alpha-glucoside Acarbose (Glucobay) 0.6% Negligible Not
What s New in Diabetes Treatment. Disclosures
 What s New in Diabetes Treatment Shiri Levy M.D. Henry Ford Hospital Senior Staff Physician Service Chief, West Bloomfield Hospital Endocrinology, Metabolism, Bone and Mineral Disorders Disclosures None
What s New in Diabetes Treatment Shiri Levy M.D. Henry Ford Hospital Senior Staff Physician Service Chief, West Bloomfield Hospital Endocrinology, Metabolism, Bone and Mineral Disorders Disclosures None
New Therapies for Diabetes
 Type 2 diabetes is increasingly prevalent New Therapies for Diabetes Lynn Mack, M.D. Associate Professor Diabetes, Endocrinology, & Metabolism The Nebraska Medical Center lmack@unmc.edu No Conflicts of
Type 2 diabetes is increasingly prevalent New Therapies for Diabetes Lynn Mack, M.D. Associate Professor Diabetes, Endocrinology, & Metabolism The Nebraska Medical Center lmack@unmc.edu No Conflicts of
Diabetes Mellitus II CPG
 1 Diabetes Mellitus II CPG Candidates for Screening Integrated Complex Care Patients: Check Yearly Prediabetes: Check Yearly No Diabetes Mellitus (DM) Risk Factors: Check at Age 45, Repeat Every 3 Years
1 Diabetes Mellitus II CPG Candidates for Screening Integrated Complex Care Patients: Check Yearly Prediabetes: Check Yearly No Diabetes Mellitus (DM) Risk Factors: Check at Age 45, Repeat Every 3 Years
Let s not sugarcoat it! Update on Pharmacologic Management of Type II DM
 Let s not sugarcoat it! Update on Pharmacologic Management of Type II DM Gregory Castelli, PharmD, BCPS, BC-ADM Clinical Pharmacist UPMC St. Margaret Objectives By the end of this presentation, participants
Let s not sugarcoat it! Update on Pharmacologic Management of Type II DM Gregory Castelli, PharmD, BCPS, BC-ADM Clinical Pharmacist UPMC St. Margaret Objectives By the end of this presentation, participants
Ertugliflozin (Steglatro ) 5 mg daily. May increase to 15 mg daily. Take in the morning +/- food. < 60: Do not initiate; discontinue therapy
 5 mg daily. May increase to 15 mg daily. Take in the morning +/- food. < 60: Do not initiate; discontinue therapy") Sodium-glucose Cotransporter-2 (SGLT2) s Inhibit SGLT in proximal renal tubules, reducing reabsorption of filtered glucose from tubular lumen Lowers renal threshold for glucose à increase urinary excretion
Sodium-glucose Cotransporter-2 (SGLT2) s Inhibit SGLT in proximal renal tubules, reducing reabsorption of filtered glucose from tubular lumen Lowers renal threshold for glucose à increase urinary excretion
Antihyperglycemic Agents in Diabetes. Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014
 Antihyperglycemic Agents in Diabetes Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014 Objectives Review 2014 ADA Standards of Medical Care in DM as they
Antihyperglycemic Agents in Diabetes Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014 Objectives Review 2014 ADA Standards of Medical Care in DM as they
Multiple Small Feedings of the Mind: Diabetes. Sonja K Fredrickson, MD, BC-ADM March 7, 2014
 Multiple Small Feedings of the Mind: Diabetes Sonja K Fredrickson, MD, BC-ADM March 7, 2014 Question 1: Setting A1c Goals Describe the evidence based approach to determining the target HgbA1c in different
Multiple Small Feedings of the Mind: Diabetes Sonja K Fredrickson, MD, BC-ADM March 7, 2014 Question 1: Setting A1c Goals Describe the evidence based approach to determining the target HgbA1c in different
DIABETES. overview of pharmacologic agents used in the management of. Overview 4/3/2014 OBJECTIVES. Injectable Agents
 overview of pharmacologic agents used in the management of DIABETES Kyle Roberts, Pharm.D. PGY-1 Pharmacy Resident Saint Alphonsus RMC 1. List the different classes of diabetes medications, including the
overview of pharmacologic agents used in the management of DIABETES Kyle Roberts, Pharm.D. PGY-1 Pharmacy Resident Saint Alphonsus RMC 1. List the different classes of diabetes medications, including the
Diabetes Update Bryan Heart Conference September 5, 2015 Shannon Wakeley, MD. Disclosures. Objectives 9/1/2015
 Diabetes Update Bryan Heart Conference September 5, 2015 Shannon Wakeley, MD Disclosures I speak on behalf of the following companies: Astra Zeneca, Boehringer Ingelheim, Johnson & Johnson, Sanofi and
Diabetes Update Bryan Heart Conference September 5, 2015 Shannon Wakeley, MD Disclosures I speak on behalf of the following companies: Astra Zeneca, Boehringer Ingelheim, Johnson & Johnson, Sanofi and
What s New on the Horizon: Diabetes Medication Update
 What s New on the Horizon: Diabetes Medication Update Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors, and what s coming Revised ADA/EASD and AACE guidelines:
What s New on the Horizon: Diabetes Medication Update Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors, and what s coming Revised ADA/EASD and AACE guidelines:
4/9/2018 HOW TO REGULATE DIABETES MEDICATIONS. By Sarah Froemsdorf MSN, RNC, CDE, FNP DISCLOSURES NONE. Diagnosis
 HOW TO REGULATE DIABETES MEDICATIONS By Sarah Froemsdorf MSN, RNC, CDE, FNP DISCLOSURES NONE Diagnosis 1 NORMAL BODY The normal pancreas releases one unit of insulin every hour all day. The normal pancreas
HOW TO REGULATE DIABETES MEDICATIONS By Sarah Froemsdorf MSN, RNC, CDE, FNP DISCLOSURES NONE Diagnosis 1 NORMAL BODY The normal pancreas releases one unit of insulin every hour all day. The normal pancreas
Initiating Injectable Therapy in Type 2 Diabetes
 Initiating Injectable Therapy in Type 2 Diabetes David Doriguzzi, PA C Learning Objectives To understand current Diabetes treatment guidelines To understand how injectable medications fit into current
Initiating Injectable Therapy in Type 2 Diabetes David Doriguzzi, PA C Learning Objectives To understand current Diabetes treatment guidelines To understand how injectable medications fit into current
Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications
 Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications Nathan Woolever, Pharm.D., Resident Pharmacist Pharmacy Grand Rounds November 6 th, 2018 Franciscan Healthcare La Crosse, WI 2017
Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications Nathan Woolever, Pharm.D., Resident Pharmacist Pharmacy Grand Rounds November 6 th, 2018 Franciscan Healthcare La Crosse, WI 2017
What s New on the Horizon: Diabetes Medication Update. Michael Shannon, MD Providence Endocrinology, Olympia WA
 What s New on the Horizon: Diabetes Medication Update Michael Shannon, MD Providence Endocrinology, Olympia WA 1 Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors,
What s New on the Horizon: Diabetes Medication Update Michael Shannon, MD Providence Endocrinology, Olympia WA 1 Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors,
Wayne Gravois, MD August 6, 2017
 Wayne Gravois, MD August 6, 2017 Americans with Diabetes (Millions) 40 30 Source: National Diabetes Statistics Report, 2011, 2017 Millions 20 10 0 1980 2009 2015 2007 - $174 Billion 2015 - $245 Billion
Wayne Gravois, MD August 6, 2017 Americans with Diabetes (Millions) 40 30 Source: National Diabetes Statistics Report, 2011, 2017 Millions 20 10 0 1980 2009 2015 2007 - $174 Billion 2015 - $245 Billion
6/1/2018. Lou Haenel, IV, DO, FACE, FACOI Endocrinology Roper St Francis Charleston, SC THE OMINOUS OCTET: HOW PATHOPHYSIOLOGY AND THERAPY MERGE
 Lou Haenel, IV, DO, FACE, FACOI Endocrinology Roper St Francis Charleston, SC THE OMINOUS OCTET: HOW PATHOPHYSIOLOGY AND THERAPY MERGE 1 2 3 Sulfonylureas Glipizide Glyburide Glimeperide 4 Metformin Gold
Lou Haenel, IV, DO, FACE, FACOI Endocrinology Roper St Francis Charleston, SC THE OMINOUS OCTET: HOW PATHOPHYSIOLOGY AND THERAPY MERGE 1 2 3 Sulfonylureas Glipizide Glyburide Glimeperide 4 Metformin Gold
Clinical Cases in Diabetes Management. Joseph Cook D.O.
 Clinical Cases in Diabetes Management Joseph Cook D.O. Objectives State the prevalence of Diabetes Mellitus in Ohio State the percentage of diabetic patients in the U.S. treated by Primary Care Physicians
Clinical Cases in Diabetes Management Joseph Cook D.O. Objectives State the prevalence of Diabetes Mellitus in Ohio State the percentage of diabetic patients in the U.S. treated by Primary Care Physicians
RPCC Pharmacy Forum. The Type 2 Diabetes Issue. Type 2 Diabetes: The Basics
 Nov/Dec 2015 Issue 11 RPCC Pharmacy Forum Special Interest Articles: Diabetes Medication Chart Insulin Chart Afreeza Did you know? Exanatide, marketed as Byetta, is the synthetic form of exendin-4, which
Nov/Dec 2015 Issue 11 RPCC Pharmacy Forum Special Interest Articles: Diabetes Medication Chart Insulin Chart Afreeza Did you know? Exanatide, marketed as Byetta, is the synthetic form of exendin-4, which
Side Effects of: GLP-1 agonists DPP-4 inhibitors SGLT-2 inhibitors. Bryce Fukunaga PharmD April 25, 2018
 Side Effects of: GLP-1 agonists DPP-4 inhibitors SGLT-2 inhibitors Bryce Fukunaga PharmD April 25, 2018 Objectives For each drug class: Identify the overall place in therapy Explain the mechanism of action
Side Effects of: GLP-1 agonists DPP-4 inhibitors SGLT-2 inhibitors Bryce Fukunaga PharmD April 25, 2018 Objectives For each drug class: Identify the overall place in therapy Explain the mechanism of action
Management of Type 2 Diabetes Mellitus. Heather Corn, MD, MS Endocrinology, Diabetes, and Metabolism
 Management of Type 2 Diabetes Mellitus Heather Corn, MD, MS Endocrinology, Diabetes, and Metabolism Disclosures Working for Intermountain Healthcare Some of the views represented are the opinion of ABIM-certified
Management of Type 2 Diabetes Mellitus Heather Corn, MD, MS Endocrinology, Diabetes, and Metabolism Disclosures Working for Intermountain Healthcare Some of the views represented are the opinion of ABIM-certified
Pharmacologic Agents for Treatment of Type 2 Diabetes
 Pharmacologic Agents for Treatment of Type 2 Diabetes SCAN Drugs Medication Biguanides 1 1 er uncoated tabs 500 mg & 750 mg Sulfonylureas 1 1 500 850 mg QD - TID 500 2000 mg glimepiride 1 1 1 8 mg glipizide
Pharmacologic Agents for Treatment of Type 2 Diabetes SCAN Drugs Medication Biguanides 1 1 er uncoated tabs 500 mg & 750 mg Sulfonylureas 1 1 500 850 mg QD - TID 500 2000 mg glimepiride 1 1 1 8 mg glipizide
Hot Topics: The Future of Diabetes Management Cutting Edge Medication and Technology-Based Care
 Hot Topics: The Future of Diabetes Management Cutting Edge Medication and Technology-Based Care Mary Jean Christian, MA, MBA, RD, CDE Diabetes Program Coordinator UC Irvine Health Hot Topics: Diabetes
Hot Topics: The Future of Diabetes Management Cutting Edge Medication and Technology-Based Care Mary Jean Christian, MA, MBA, RD, CDE Diabetes Program Coordinator UC Irvine Health Hot Topics: Diabetes
Comprehensive Diabetes Treatment
 Comprehensive Diabetes Treatment Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism The George Washington University School of Medicine Diabetes
Comprehensive Diabetes Treatment Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism The George Washington University School of Medicine Diabetes
Diabetes Medication Updates Erica Bukovich, PharmD, BC-ADM, CDE September 20, 2018
 Diabetes Medication Updates Erica Bukovich, PharmD, BC-ADM, CDE September 20, 2018 Learning Objectives Identify medication classes available for treatment of individuals with diabetes. Demonstrate understanding
Diabetes Medication Updates Erica Bukovich, PharmD, BC-ADM, CDE September 20, 2018 Learning Objectives Identify medication classes available for treatment of individuals with diabetes. Demonstrate understanding
Diabetes 2016: Strategies for achieving optimal diabetes control
 PHASE Safety Net Community Benefit Diabetes 2016: Strategies for achieving optimal diabetes control Presented by: Lisa Gilliam, MD, PhD Clinical Leader Diabetes Program Kaiser Permanente Northern California
PHASE Safety Net Community Benefit Diabetes 2016: Strategies for achieving optimal diabetes control Presented by: Lisa Gilliam, MD, PhD Clinical Leader Diabetes Program Kaiser Permanente Northern California
NEW DIABETES CARE MEDICATIONS
 NEW DIABETES CARE MEDICATIONS James Bonucchi DO, ECNU, FACE Adult Medicine and Endocrinology Specialists Disclosures Speakers bureau Sanofi AZ BI Diabetes Diabetes cost ADA 2017 data Ever increasing disorder.
NEW DIABETES CARE MEDICATIONS James Bonucchi DO, ECNU, FACE Adult Medicine and Endocrinology Specialists Disclosures Speakers bureau Sanofi AZ BI Diabetes Diabetes cost ADA 2017 data Ever increasing disorder.
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy
 Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
Insulin Initiation and Intensification. Disclosure. Objectives
 Insulin Initiation and Intensification Neil Skolnik, M.D. Associate Director Family Medicine Residency Program Abington Memorial Hospital Professor of Family and Community Medicine Temple University School
Insulin Initiation and Intensification Neil Skolnik, M.D. Associate Director Family Medicine Residency Program Abington Memorial Hospital Professor of Family and Community Medicine Temple University School
7/8/2016. Sol Jacobs MD, FACE Division of Endocrinology Emory University School of Medicine
 Sol Jacobs MD, FACE Division of Endocrinology Emory University School of Medicine Participation in investigator initiated clinical research supported by: Merck Boehringer Ingelheim Novo Nordisk Astra Zeneca
Sol Jacobs MD, FACE Division of Endocrinology Emory University School of Medicine Participation in investigator initiated clinical research supported by: Merck Boehringer Ingelheim Novo Nordisk Astra Zeneca
STEP THERAPY CRITERIA
 CATEGORY DRUG CLASS BRAND NAME (generic) STEP THERAPY CRITERIA AMYLIN ANALOG: SYMLIN/SYMLINPEN (pramlintide acetate) ANTIDIABETIC AGENTS GLUCAGON-LIKE PEPTIDE-1 RECEPTOR AGONIST (GLP-1): ADLYXIN (lixisenatide)
CATEGORY DRUG CLASS BRAND NAME (generic) STEP THERAPY CRITERIA AMYLIN ANALOG: SYMLIN/SYMLINPEN (pramlintide acetate) ANTIDIABETIC AGENTS GLUCAGON-LIKE PEPTIDE-1 RECEPTOR AGONIST (GLP-1): ADLYXIN (lixisenatide)
Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol
 Inhibitors Drug Class Prior Authorization Protocol") Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has
Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has
The Many Faces of T2DM in Long-term Care Facilities
 The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
Collaborative Practice Agreement
 Collaborative Practice Agreement [community pharmacy name] [address] [phone number] [physician practice] [address] [phone number] Effective: [date] Expiration: [date] 1 Table of Contents 1.0 Introduction...4
Collaborative Practice Agreement [community pharmacy name] [address] [phone number] [physician practice] [address] [phone number] Effective: [date] Expiration: [date] 1 Table of Contents 1.0 Introduction...4
Drug Class Review Newer Diabetes Medications and Combinations
 Drug Class Review Newer Diabetes Medications and Combinations Final Update 2 Report July 2016 The purpose reports is to make available information regarding the comparative clinical effectiveness and harms
Drug Class Review Newer Diabetes Medications and Combinations Final Update 2 Report July 2016 The purpose reports is to make available information regarding the comparative clinical effectiveness and harms
Newer Therapies for Type 2 Diabetes
 Newer Therapies for Type 2 Diabetes Sandra Indacochea Sobel, MD Clinical Assistant Professor of Medicine Clinical Chief of Endocrinology, UPMC Mercy Division of Endocrinology, Diabetes, and Metabolism
Newer Therapies for Type 2 Diabetes Sandra Indacochea Sobel, MD Clinical Assistant Professor of Medicine Clinical Chief of Endocrinology, UPMC Mercy Division of Endocrinology, Diabetes, and Metabolism
Achieving and maintaining good glycemic control is an
 Glycemic Efficacy, Weight Effects, and Safety of Once-Weekly Glucagon-Like Peptide-1 Receptor Agonists Yehuda Handelsman, MD, FACP, FNLA, FASPC, MACE; Kathleen Wyne, MD, PhD, FACE, FNLA; Anthony Cannon,
Glycemic Efficacy, Weight Effects, and Safety of Once-Weekly Glucagon-Like Peptide-1 Receptor Agonists Yehuda Handelsman, MD, FACP, FNLA, FASPC, MACE; Kathleen Wyne, MD, PhD, FACE, FNLA; Anthony Cannon,
Help the Heart. An Update on GLP-1 Agonists and SGLT2 Inhibitors. Tara Hawley, PharmD PGY1 Pharmacy Resident Mayo Clinic Health System Eau Claire
 Help the Heart An Update on GLP-1 Agonists and SGLT2 Inhibitors Tara Hawley, PharmD PGY1 Pharmacy Resident Mayo Clinic Health System Eau Claire Mayo Clinic Grand Rounds May 16, 2017 2017 MFMER slide-1
Help the Heart An Update on GLP-1 Agonists and SGLT2 Inhibitors Tara Hawley, PharmD PGY1 Pharmacy Resident Mayo Clinic Health System Eau Claire Mayo Clinic Grand Rounds May 16, 2017 2017 MFMER slide-1
Medical therapy advances London/Manchester RCP February/June 2016
 Medical therapy advances London/Manchester RCP February/June 2016 Advances in medical therapies for diabetes mellitus Duality of interest: The speaker or institutions with which he is associated has received
Medical therapy advances London/Manchester RCP February/June 2016 Advances in medical therapies for diabetes mellitus Duality of interest: The speaker or institutions with which he is associated has received
New Therapies for Diabetes Management: Hope or Headache?
 New Therapies for Diabetes Management: Hope or Headache? Elizabeth Stephens, MD, FACP PMG- Endocrinology Elizabeth.Stephens@providence.org November 2018 Disclosures None 1 Objectives Discussion of 3 rd
New Therapies for Diabetes Management: Hope or Headache? Elizabeth Stephens, MD, FACP PMG- Endocrinology Elizabeth.Stephens@providence.org November 2018 Disclosures None 1 Objectives Discussion of 3 rd
Newer Drugs in the Management of Type 2 Diabetes Mellitus
 Newer Drugs in the Management of Type 2 Diabetes Mellitus Dr. C. Dinesh M. Naidu Professor of Pharmacology, Kamineni Institute of Medical Sciences, Narketpally. 1 Presentation Outline Introduction Pathogenesis
Newer Drugs in the Management of Type 2 Diabetes Mellitus Dr. C. Dinesh M. Naidu Professor of Pharmacology, Kamineni Institute of Medical Sciences, Narketpally. 1 Presentation Outline Introduction Pathogenesis
Oral and Injectable Non-insulin Antihyperglycemic Agents
 Appendix 5: Diabetes Education and Medical Management in Adults with Diabetes Oral and Injectable Non-insulin s This directive will be implemented by RPhs, RNs or RDs who have been deemed authorized implementers.
Appendix 5: Diabetes Education and Medical Management in Adults with Diabetes Oral and Injectable Non-insulin s This directive will be implemented by RPhs, RNs or RDs who have been deemed authorized implementers.
Society for Ambulatory Anesthesia Consensus Statement on Perioperative Blood Glucose Management in Diabetic Patients Undergoing Ambulatory Surgery
 Society for Ambulatory Anesthesia Consensus Statement on Perioperative Blood Glucose Management in Diabetic Patients Undergoing Ambulatory Surgery Girish P. Joshi, MB BS, MD, FFARCSI Anesthesia & Analgesia
Society for Ambulatory Anesthesia Consensus Statement on Perioperative Blood Glucose Management in Diabetic Patients Undergoing Ambulatory Surgery Girish P. Joshi, MB BS, MD, FFARCSI Anesthesia & Analgesia
Diabetes Treatment Update
 Diabetes Treatment Update Timothy C. Evans, MD PhD FACP University of Washington Department of Medicine Disclosure: Dr. Evans has no significant financial interest in any of the products or manufacturers
Diabetes Treatment Update Timothy C. Evans, MD PhD FACP University of Washington Department of Medicine Disclosure: Dr. Evans has no significant financial interest in any of the products or manufacturers
Physician Drug Reference Chart for Diabetes Antidiabetic Medications
 Drug Class Compound Brand Name Mechanism of Action Advantages Disadvantages Alpha-glucosidase inhibitors Medium Cost by Bayer Healthcare, Pfizer, Takeda Research Acarbose Miglitol Voglibose Precose Glyset
Drug Class Compound Brand Name Mechanism of Action Advantages Disadvantages Alpha-glucosidase inhibitors Medium Cost by Bayer Healthcare, Pfizer, Takeda Research Acarbose Miglitol Voglibose Precose Glyset
Disclosures. Objectives. Bryan Cardiology Conference DM2 & Cardiovascular Outcome Trials 8/28/2017
 Bryan Cardiology Conference DM2 & Cardiovascular Outcome Trials Shannon Wakeley MD Complete Endocrinology 9/2/2017 Disclosures Speakers Bureau: Astra Zeneca, Sanofi, Abbvie, Boehringer-Ingelheim, Medtronic,
Bryan Cardiology Conference DM2 & Cardiovascular Outcome Trials Shannon Wakeley MD Complete Endocrinology 9/2/2017 Disclosures Speakers Bureau: Astra Zeneca, Sanofi, Abbvie, Boehringer-Ingelheim, Medtronic,
Vipul Lakhani, MD Oregon Medical Group Endocrinology
 Vipul Lakhani, MD Oregon Medical Group Endocrinology Disclosures None Objectives Be able to diagnose diabetes and assess control Be able to identify appropriate classes of medications for diabetes treatment
Vipul Lakhani, MD Oregon Medical Group Endocrinology Disclosures None Objectives Be able to diagnose diabetes and assess control Be able to identify appropriate classes of medications for diabetes treatment
INSULIN INITIATION AND INTENSIFICATION WITH A FOCUS ON HYPOGLYCEMIA REDUCTION
 INSULIN INITIATION AND INTENSIFICATION WITH A FOCUS ON HYPOGLYCEMIA REDUCTION Jaiwant Rangi, MD, FACE Nov 10 th 2018 DISCLOSURES Speaker Novo Nordisk Sanofi-Aventis Boheringer Ingleheim Merck Abbvie Abbott
INSULIN INITIATION AND INTENSIFICATION WITH A FOCUS ON HYPOGLYCEMIA REDUCTION Jaiwant Rangi, MD, FACE Nov 10 th 2018 DISCLOSURES Speaker Novo Nordisk Sanofi-Aventis Boheringer Ingleheim Merck Abbvie Abbott
How can we improve outcomes in Type 2 diabetes?
 How can we improve outcomes in Type 2 diabetes? Earlier diagnosis Better patient education Stress central role of lifestyle management Identify and treat all risk factors Use rational pharmacological therapy
How can we improve outcomes in Type 2 diabetes? Earlier diagnosis Better patient education Stress central role of lifestyle management Identify and treat all risk factors Use rational pharmacological therapy
Non-insulin treatment in Type 1 DM Sang Yong Kim
 Non-insulin treatment in Type 1 DM Sang Yong Kim Chosun University Hospital Conflict of interest disclosure None Committee of Scientific Affairs Committee of Scientific Affairs Insulin therapy is the mainstay
Non-insulin treatment in Type 1 DM Sang Yong Kim Chosun University Hospital Conflict of interest disclosure None Committee of Scientific Affairs Committee of Scientific Affairs Insulin therapy is the mainstay
2/9/2016. The Evolving Armamentarium for Type 2 Diabetes: Incorporating New Classes in the Treatment of Our Patients. Objectives: Pharmacists
 WAYNE STATE UNIVERSITY COLLEGE OF PHARMACY & HEALTH SCIENCES FEBRUARY 28, 2016 The Evolving Armamentarium for Type 2 Diabetes: Clinical Assistant Professor, Department of Pharmacy Practice Ambulatory Care
WAYNE STATE UNIVERSITY COLLEGE OF PHARMACY & HEALTH SCIENCES FEBRUARY 28, 2016 The Evolving Armamentarium for Type 2 Diabetes: Clinical Assistant Professor, Department of Pharmacy Practice Ambulatory Care
DIABETES DEBATE - IS NEW BETTER?
 DIABETES DEBATE - IS NEW BETTER? WHAT MEDICATION CLASS AFTER METFORMIN TO CONTROL BLOOD SUGAR Dr. Lydia Hatcher, MD, CCFP, FCFP, CHE, D-CAPM Associate Clinical Professor of Family Medicine, McMaster Chief
DIABETES DEBATE - IS NEW BETTER? WHAT MEDICATION CLASS AFTER METFORMIN TO CONTROL BLOOD SUGAR Dr. Lydia Hatcher, MD, CCFP, FCFP, CHE, D-CAPM Associate Clinical Professor of Family Medicine, McMaster Chief
TABLE 1A : Formulary Coverage of Insulin Therapies & Indications for Use in Various Populations
 177 TABLE 1A : Formulary Coverage of Insulin Therapies & Indications for Use in Various Populations Formulary Coverage Indication for use with: INSULIN THERAPY NS NB NL PE ADULTS PEDIATRICS PREGNANCY BOLUS
177 TABLE 1A : Formulary Coverage of Insulin Therapies & Indications for Use in Various Populations Formulary Coverage Indication for use with: INSULIN THERAPY NS NB NL PE ADULTS PEDIATRICS PREGNANCY BOLUS
Glucagon-like peptide-1 (GLP-1) Agonists Drug Class Prior Authorization Protocol
 Agonists Drug Class Prior Authorization Protocol") Glucagon-like peptide-1 (GLP-1) Agonists Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed
Glucagon-like peptide-1 (GLP-1) Agonists Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed
Learning Objectives. Impact of Diabetes II UPDATES IN TYPE 2 DIABETES. David Doriguzzi, PA-C
 UPDATES IN TYPE 2 DIABETES David Doriguzzi, PA-C Learning Objectives Upon completion of this educational activity, the participant should be able to: Overcome barriers and attitudes that limit Clinician/Patient
UPDATES IN TYPE 2 DIABETES David Doriguzzi, PA-C Learning Objectives Upon completion of this educational activity, the participant should be able to: Overcome barriers and attitudes that limit Clinician/Patient
MANAGING DIABETES IN 2016 WHAT TO ADD, WHEN AND WHY?
 MANAGING DIABETES IN 2016 WHAT TO ADD, WHEN AND WHY? Faculty: Maria Wolfs MD, MHSc, FRCPC Assistant Professor, University of Toronto Staff Endocrinologist, St. Michael's Hospital Relationships with commercial
MANAGING DIABETES IN 2016 WHAT TO ADD, WHEN AND WHY? Faculty: Maria Wolfs MD, MHSc, FRCPC Assistant Professor, University of Toronto Staff Endocrinologist, St. Michael's Hospital Relationships with commercial
Oral Medication for the Management of Diabetes Mechanism of. Duration of Daily Dosing Action
 Glyburide (Micronase, Diabeta, Glynase) Glipizide (Glucotrol) Glipizide XL (Glucotrol XL) Glimepiride (Amaryl) Prandin (Repaglinide) Starlix (Nateglinide) 1.25, 2.5, 5mg tabs, Dosing: 2.5-20 mg 12- (Glynase:
Glyburide (Micronase, Diabeta, Glynase) Glipizide (Glucotrol) Glipizide XL (Glucotrol XL) Glimepiride (Amaryl) Prandin (Repaglinide) Starlix (Nateglinide) 1.25, 2.5, 5mg tabs, Dosing: 2.5-20 mg 12- (Glynase:
TREATMENTS FOR TYPE 2 DIABETES. Susan Henry Diabetes Specialist Nurse
 TREATMENTS FOR TYPE 2 DIABETES Susan Henry Diabetes Specialist Nurse How can we improve outcomes in Type 2 diabetes? Earlier diagnosis Better patient education Stress central role of lifestyle management
TREATMENTS FOR TYPE 2 DIABETES Susan Henry Diabetes Specialist Nurse How can we improve outcomes in Type 2 diabetes? Earlier diagnosis Better patient education Stress central role of lifestyle management
FARXIGA (dapagliflozin) Jardiance (empagliflozin) tablets. Synjardy (empagliflozin and metformin hydrochloride) tablets. GLUCOPHAGE* (metformin)
 Jardiance (empagliflozin) tablets. Synjardy (empagliflozin and metformin hydrochloride) tablets. GLUCOPHAGE* (metformin)") Type 2 Medications Drug Class How It Works Brand and Generic Names Manufacturers Usual Starting Dose The kidneys filter sugar and either absorb it back into your body for energy or remove it through your
Type 2 Medications Drug Class How It Works Brand and Generic Names Manufacturers Usual Starting Dose The kidneys filter sugar and either absorb it back into your body for energy or remove it through your
This program applies to Commercial, GenPlus and Health Insurance Marketplace formularies.
 OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) Agonists [Adlyxin (lixisenatide), Byetta (exenatide), Bydureon (exenatide extended-release), Tanzeum (albiglutide), Trulicity (dulaglutide),
OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) Agonists [Adlyxin (lixisenatide), Byetta (exenatide), Bydureon (exenatide extended-release), Tanzeum (albiglutide), Trulicity (dulaglutide),
IMPROVED DIAGNOSIS OF TYPE 2 DIABETES AND TAILORING MEDICATIONS
 IMPROVED DIAGNOSIS OF TYPE 2 DIABETES AND TAILORING MEDICATIONS Dr Bidhu Mohapatra, MBBS, MD, FRACP Consultant Physician Endocrinology and General Medicine Introduction 382 million people affected by diabetes
IMPROVED DIAGNOSIS OF TYPE 2 DIABETES AND TAILORING MEDICATIONS Dr Bidhu Mohapatra, MBBS, MD, FRACP Consultant Physician Endocrinology and General Medicine Introduction 382 million people affected by diabetes
Diabetes Management: A diagnostic perspective
 Diabetes Management: A diagnostic perspective Images: http://www.engadget.com/2009/09/23/bayer-introduces-countour-usb-glucose-meter/ http://www.medtronicdiabetes.com/treatment-and-products/minimed-530g-diabetes-system-with-enlite
Diabetes Management: A diagnostic perspective Images: http://www.engadget.com/2009/09/23/bayer-introduces-countour-usb-glucose-meter/ http://www.medtronicdiabetes.com/treatment-and-products/minimed-530g-diabetes-system-with-enlite
Incredible Incretins Abby Frye, PharmD, BCACP
 Incredible Incretins Abby Frye, PharmD, BCACP Objectives & Disclosures Review the pathophysiology of T2DM and the impact of the incretin system Describe the defining characteristics of the available glucagonlike
Incredible Incretins Abby Frye, PharmD, BCACP Objectives & Disclosures Review the pathophysiology of T2DM and the impact of the incretin system Describe the defining characteristics of the available glucagonlike
Improving Patient Outcomes with Individualized Therapy in the Management of Type 2 Diabetes
 Improving Patient Outcomes with Individualized Therapy in the Management of Type 2 Diabetes Timothy S. Reid, M.D. Mercy Diabetes Center Janesville, WI Duality Statement Dr. Reid is a Speaker and Consultant
Improving Patient Outcomes with Individualized Therapy in the Management of Type 2 Diabetes Timothy S. Reid, M.D. Mercy Diabetes Center Janesville, WI Duality Statement Dr. Reid is a Speaker and Consultant
The Alphabet Soup of Diabetes. Egils Bogdanovics M.D. Hungerford Diabetes Center
 The Alphabet Soup of Diabetes Egils Bogdanovics M.D. Hungerford Diabetes Center Insulin: January 11, 1922 12 year old Leonard Thompson, on a starvation diet for 2 years received his first insulin injection
The Alphabet Soup of Diabetes Egils Bogdanovics M.D. Hungerford Diabetes Center Insulin: January 11, 1922 12 year old Leonard Thompson, on a starvation diet for 2 years received his first insulin injection
Individualizing Care for Patients with Type 2 Diabetes
 Individualizing Care for Patients with Type 2 Diabetes Disclosures Speaker: AstraZeneca, Novo Nordisk, BI/Lilly, Valeritas, Takeda Advisor: Tandem Diabetes, Sanofi Objectives Develop individualized approaches
Individualizing Care for Patients with Type 2 Diabetes Disclosures Speaker: AstraZeneca, Novo Nordisk, BI/Lilly, Valeritas, Takeda Advisor: Tandem Diabetes, Sanofi Objectives Develop individualized approaches
Overview T2DM medications. Winnie Ho
 Overview T2DM medications Winnie Ho Diabetes in Australia 1.7 million Australians with diabetes, of these 85% have T2DM 2-fold excess risk CV death in patients with diabetes Risk factor for progression
Overview T2DM medications Winnie Ho Diabetes in Australia 1.7 million Australians with diabetes, of these 85% have T2DM 2-fold excess risk CV death in patients with diabetes Risk factor for progression
Update Diabetes Therapie. Marc Y Donath
 Update Diabetes Therapie Marc Y Donath Recent CV outcome studies in Diabetes N Engl J Med. 2015 373:2117-28 (Empa-Reg outcome study) N Engl J Med. 2016 June 13 (LEADER trial) N Engl J Med. 2017 June 12
Update Diabetes Therapie Marc Y Donath Recent CV outcome studies in Diabetes N Engl J Med. 2015 373:2117-28 (Empa-Reg outcome study) N Engl J Med. 2016 June 13 (LEADER trial) N Engl J Med. 2017 June 12
INJECTABLE THERAPY FOR THE TREATMENT OF DIABETES
 INJECTABLE THERAPY FOR THE TREATMENT OF DIABETES ARSHNA SANGHRAJKA DIABETES SPECIALIST PRESCRIBING PHARMACIST OBJECTIVES EXPLORE THE TYPES OF INSULIN AND INJECTABLE DIABETES TREATMENTS AND DEVICES AVAILABLE
INJECTABLE THERAPY FOR THE TREATMENT OF DIABETES ARSHNA SANGHRAJKA DIABETES SPECIALIST PRESCRIBING PHARMACIST OBJECTIVES EXPLORE THE TYPES OF INSULIN AND INJECTABLE DIABETES TREATMENTS AND DEVICES AVAILABLE
Clinical Practice Guidelines
 Clinical Practice Guidelines Diabetes Objective The purpose is to guide the appropriate diagnosis and management of Diabetes. This guideline is designed to assist the clinician by providing a framework
Clinical Practice Guidelines Diabetes Objective The purpose is to guide the appropriate diagnosis and management of Diabetes. This guideline is designed to assist the clinician by providing a framework
The Management of Diabetes in Primary Care Kelly Krawtz, PharmD, BCPS, BCACP
 The Management of Diabetes in Primary Care Kelly Krawtz, PharmD, BCPS, BCACP Objectives Explain the current pharmacologic options for the management of diabetes Describe the latest technologies available
The Management of Diabetes in Primary Care Kelly Krawtz, PharmD, BCPS, BCACP Objectives Explain the current pharmacologic options for the management of diabetes Describe the latest technologies available
Diabesity. Metabolic dysfunction that ranges from mild blood glucose imbalance to full fledged Type 2 DM Signs
 Diabesity Metabolic dysfunction that ranges from mild blood glucose imbalance to full fledged Type 2 DM Signs Abdominal obesity Low HDL, high LDL, and high triglycerides HTN High blood glucose (F>100l,
Diabesity Metabolic dysfunction that ranges from mild blood glucose imbalance to full fledged Type 2 DM Signs Abdominal obesity Low HDL, high LDL, and high triglycerides HTN High blood glucose (F>100l,
Age-adjusted Percentage of U.S. Adults Who Were Obese or Who Had Diagnosed Diabetes
 Age-adjusted Percentage of U.S. Adults Who Were Obese or Who Had Diagnosed Diabetes Obesity (BMI 30 kg/m 2 ) 1994 2000 2009 No Data 26.0% Diabetes 1994 2000 2009
Age-adjusted Percentage of U.S. Adults Who Were Obese or Who Had Diagnosed Diabetes Obesity (BMI 30 kg/m 2 ) 1994 2000 2009 No Data 26.0% Diabetes 1994 2000 2009
TABLE 1A: Formulary Coverage of Insulin Therapies & Indications for Use in Various Populations
 177 TABLE 1A: Formulary Coverage of Insulin Therapies & Indications for Use in Various Populations TABLE 1A : Formulary Coverage of Insulin Therapies & Indications for Use in Various Populations Formulary
177 TABLE 1A: Formulary Coverage of Insulin Therapies & Indications for Use in Various Populations TABLE 1A : Formulary Coverage of Insulin Therapies & Indications for Use in Various Populations Formulary
Welcome to the PHASE Learning Community! October 31, 2018
 Welcome to the PHASE Learning Community! October 31, 2018 Webinar Housekeeping 1. Dial in for audio: 303-248-0285, Access Code: 5617817 2. Lines are muted. You can chat in questions or unmute your line
Welcome to the PHASE Learning Community! October 31, 2018 Webinar Housekeeping 1. Dial in for audio: 303-248-0285, Access Code: 5617817 2. Lines are muted. You can chat in questions or unmute your line
I. General Considerations
 1 2 3 I. General Considerations A. Type I ( Juvenile Onset or IDDM) IDDM results from autoimmune destruction of beta cells inability to secrete insulin --> ketone formation --> DKA 4 Diabetic Ketoacidosis
1 2 3 I. General Considerations A. Type I ( Juvenile Onset or IDDM) IDDM results from autoimmune destruction of beta cells inability to secrete insulin --> ketone formation --> DKA 4 Diabetic Ketoacidosis
Navigating the New Options for the Management of Type 2 Diabetes
 Navigating the New Options for the Management of Type 2 Diabetes Clinical Associate Professor Mark Kennedy Department of General Practice, University of Melbourne Chair, Primary Care Diabetes Society of
Navigating the New Options for the Management of Type 2 Diabetes Clinical Associate Professor Mark Kennedy Department of General Practice, University of Melbourne Chair, Primary Care Diabetes Society of
Innovative, Unusual Therapies for DM-2: Insulin U-500, Bromocriptine, Colesevelam, and SGLT2 inhibitors. April 3 rd, 2014
 Innovative, Unusual Therapies for DM-2: Insulin U-500, Bromocriptine, Colesevelam, and SGLT2 inhibitors April 3 rd, 2014 KM Pantalone Associate Staff Endocrinology Speaker Bureau: Disclosures Bristol-Myers
Innovative, Unusual Therapies for DM-2: Insulin U-500, Bromocriptine, Colesevelam, and SGLT2 inhibitors April 3 rd, 2014 KM Pantalone Associate Staff Endocrinology Speaker Bureau: Disclosures Bristol-Myers
Pharmacology Update for the Adult Patient - Newer Oral Medications for Diabetes
 Pharmacology Update for the Adult Patient - Newer Oral Medications for Diabetes Brooke Hudspeth, PharmD, CDE, MLDE Director of Diabetes Prevention, Kroger Pharmacy Adjunct Assistant Professor, University
Pharmacology Update for the Adult Patient - Newer Oral Medications for Diabetes Brooke Hudspeth, PharmD, CDE, MLDE Director of Diabetes Prevention, Kroger Pharmacy Adjunct Assistant Professor, University
9/29/ Disclosure. Learning Objectives. Diabetes Update: Guidelines, Treatment Options & Trends
 + Diabetes Update: Guidelines, Treatment Options & Trends Melissa Max, PharmD, BC-ADM, CDE Assistant Professor of Pharmacy Practice Harding University College of Pharmacy + Disclosure Conflicts Of Interest
+ Diabetes Update: Guidelines, Treatment Options & Trends Melissa Max, PharmD, BC-ADM, CDE Assistant Professor of Pharmacy Practice Harding University College of Pharmacy + Disclosure Conflicts Of Interest
Making Sense of New DM Therapies and Technologies
 Making Sense of New DM Therapies and Technologies Sandra Indacochea Sobel, MD Clinical Assistant Professor of Medicine Clinical Chief of Endocrinology, UPMC Mercy Division of Endocrinology, Diabetes, and
Making Sense of New DM Therapies and Technologies Sandra Indacochea Sobel, MD Clinical Assistant Professor of Medicine Clinical Chief of Endocrinology, UPMC Mercy Division of Endocrinology, Diabetes, and
Management of Type 2 Diabetes Cardiovascular Outcomes Trials Tom Blevins MD Texas Diabetes and Endocrinology Austin, Texas
 Management of Type 2 Diabetes Cardiovascular Outcomes Trials 2018 Tom Blevins MD Texas Diabetes and Endocrinology Austin, Texas Speaker Disclosure Dr. Blevins has disclosed that he has received grant support
Management of Type 2 Diabetes Cardiovascular Outcomes Trials 2018 Tom Blevins MD Texas Diabetes and Endocrinology Austin, Texas Speaker Disclosure Dr. Blevins has disclosed that he has received grant support
DM Fundamentals Class 4 Meds for Type 2
 DM Fundamentals Class 4 Meds for Type 2 Beverly Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Copyright 1999 2015, Diabetes Education Services, All Rights Reserved. Diabetes Meds
DM Fundamentals Class 4 Meds for Type 2 Beverly Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Copyright 1999 2015, Diabetes Education Services, All Rights Reserved. Diabetes Meds
DM Fundamentals Class 4 Meds for Type 2
 DM Fundamentals Class 4 Meds for Type 2 Beverly Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Copyright 1999 2015, Diabetes Education Services, All Rights Reserved. Diabetes Meds
DM Fundamentals Class 4 Meds for Type 2 Beverly Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Copyright 1999 2015, Diabetes Education Services, All Rights Reserved. Diabetes Meds
2018 Diabetes Summit Managing Diabetes: An Art and a Science
 2018 Diabetes Summit Managing Diabetes: An Art and a Science Natasha Petry, PharmD, BCACP NDSU College of Health Professions, School of Pharmacy, Department of Pharmacy Practice Patient-Centered Medical
2018 Diabetes Summit Managing Diabetes: An Art and a Science Natasha Petry, PharmD, BCACP NDSU College of Health Professions, School of Pharmacy, Department of Pharmacy Practice Patient-Centered Medical
DM-2 Therapy Update: GLP-1, SGLT-2 Inhibitors, and Inhaled Insulin, Oh My!
 DM-2 Therapy Update: GLP-1, SGLT-2 Inhibitors, and Inhaled Insulin, Oh My! Kevin M. Pantalone, DO, ECNU, CCD Associate Staff Director of Clinical Research Department of Endocrinology Endocrinology and
DM-2 Therapy Update: GLP-1, SGLT-2 Inhibitors, and Inhaled Insulin, Oh My! Kevin M. Pantalone, DO, ECNU, CCD Associate Staff Director of Clinical Research Department of Endocrinology Endocrinology and