Long-Term Complications of Diabetes Mellitus Macrovascular Complication
|
|
|
- Madison Wright
- 5 years ago
- Views:
Transcription
1 Long-Term Complications of Diabetes Mellitus Macrovascular Complication Sung Hee Choi MD, PhD Professor, Seoul National University College of Medicine, SNUBH, Bundang Hospital

2 Diabetes = CVD equivalent
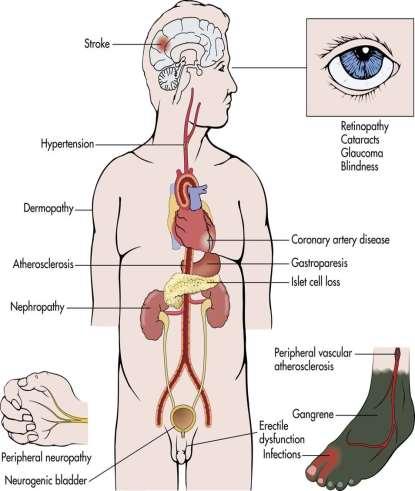
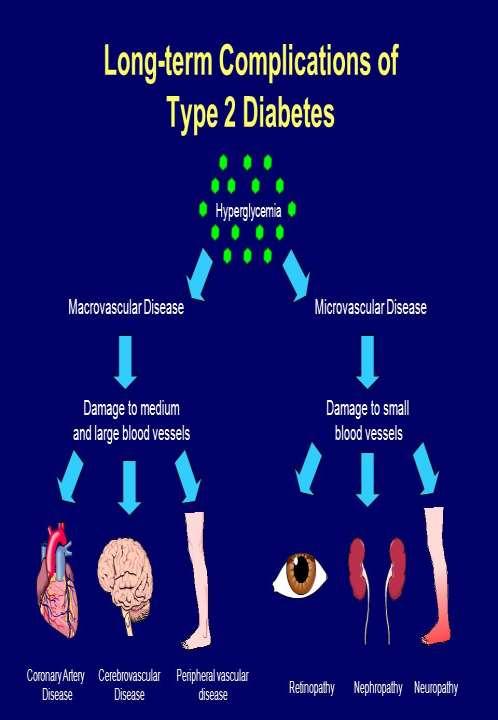
3 Long-term complications of diabetes mellitus
4 Chronic complications of diabetes Categories of long-term diabetic complications macrovascular disease : Large to medium siz ed artery, Atherosclerosis microvascular disease neuropathy Hypertension, Dyslipidemia major contributing factor especially in macrovascular disease

5 Macrovascular Changes Hypertension, Dyslipidemia, Platelet aggregation
6 Cardiovascular Disease and Risk Management 2017 standard care
7 Hypertension in Diabetes in Korea The prevalence and control rate of hypertension in persons with diabetes are 54.7% and 69.1%, respectively. In men aged 40~49 years with diabetes, fewer than half do not reach the blood pressure goal of < 140/85 mmhg Uncontrolled hypertension 1 2 단위 (%) Prevalence Control rate 30 years 65 years Men Women Hypertension is defined by systolic/diastolic blood pressure 140/90 mmhg and/or antihypertensive medications, and control rate is defined by blood pressure less than 140/85 mmhg based on the KDA guideline.
8 Blood Pressure Control & T2DM Action to Control Cardiovascular Risk in Diabetes (ACCORD): Does SBP <120 provide better cardiovascular protection than SBP ? No. ADVANCE-BP: Significant risk reduction American Diabetes Association Standards of Medical Care in Diabetes. Cardiovascular disease and risk management. Diabetes Care 2017; 40 (Suppl. 1): S75-S87
9 Recommendations: Hypertension/ Blood Pressure Control Screening and Diagnosis: Blood pressure should be measured at every routine visit. B Patients found to have elevated blood pressure should have blood pressure confirmed on a separate day. B American Diabetes Association Standards of Medical Care in Diabetes. Cardiovascular disease and risk management. Diabetes Care 2017; 40 (Suppl. 1): S75-S87
10 Recommendations: Hypertension/ Blood Pressure Control (2) Systolic Targets: People with diabetes and hypertension should be treated to a systolic blood pressure goal of <140 mmhg. A Lower systolic targets, such as <130 mmhg, may be appropriate for certain individuals at high risk of CVD, if they can be achieved without undue treatment burden. C American Diabetes Association Standards of Medical Care in Diabetes. Cardiovascular disease and risk management. Diabetes Care 2017; 40 (Suppl. 1): S75-S87
11 Recommendations: Hypertension/ Blood Pressure Control (3) Diastolic Targets: Patients with diabetes should be treated to a diastolic blood pressure <90 mmhg. A Lower diastolic targets, such as <80 mmhg, may be appropriate for certain individuals at high risk for CVD if they can be achieved without undue treatment burden. C American Diabetes Association Standards of Medical Care in Diabetes. Cardiovascular disease and risk management. Diabetes Care 2017; 40 (Suppl. 1): S75-S87
12 Recommendations: Hypertension/ Blood Pressure Treatment Patients with BP >120/80 should be advised on lifestyle changes to reduce BP. B Patients with confirmed BP >140/90 should, in addition to lifestyle therapy, have prompt initiation and timely subsequent titration of pharmacological therapy to achieve blood pressure goals. A American Diabetes Association Standards of Medical Care in Diabetes. Cardiovascular disease and risk management. Diabetes Care 2017; 40 (Suppl. 1): S75-S87
13 Recommendations: Hypertension/ Blood Pressure Treatment (3) Treatment for hypertension should include A ACE inhibitor Angiotensin II receptor blocker (ARB) Thiazide-like diuretic Dihydropyridine calcium channel blockers Multiple drug therapy (two or more agents at maximal doses) generally required to achieve BP targets. American Diabetes Association Standards of Medical Care in Diabetes. Cardiovascular disease and risk management. Diabetes Care 2017; 40 (Suppl. 1): S75-S87
14 Recommendations: Hypertension/ Blood Pressure Treatment (4) An ACE inhibitor or angiotensin receptor blocker, at the maximum tolerated dose indicated for blood pressure treatment, is the recommended first-line treatment for hypertension in patients with diabetes and urinary albumin to creatinine ratio >300 mg/g creatinine (A) or mg/g creatinine (B). If one class is not tolerated, the other should be substituted. B American Diabetes Association Standards of Medical Care in Diabetes. Cardiovascular disease and risk management. Diabetes Care 2017; 40 (Suppl. 1): S75-S87
15 Recommendations: Hypertension/ Blood Pressure Treatment (5) If using ACE inhibitors, ARBs, or diuretics, monitor serum creatinine / egfr & potassium levels. B American Diabetes Association Standards of Medical Care in Diabetes. Cardiovascular disease and risk management. Diabetes Care 2017; 40 (Suppl. 1): S75-S87

16 Hypertension management Monitor BP at every OPD visit 미만, 미만 Systolic < 140, Diastolic <85 mmhg
17 Hypercholesterolemia in Diabetes The prevalence and control rate of hypercholesterolemia in persons with diabetes are 31.6% and 49.8%, respectively. More than half of persons with diabetes do not reach the LDL-C goal of < 100 mg/dl Uncontrolled hypercholesterolemia 1 2 단위 (%) Prevalence 45.1 Control rate years 65 years Men Women Hypercholesterolemia is defined by total cholesterol 240 mg/dl or medication(s) and control rate is defined by low-density lipoprotein cholesterol (LDL-C) < 100 mg/dl based on KDA guideline.
18 Recommendations: Lipid Management In adults not taking statins, a screening lipid profile is reasonable (E): At diabetes diagnosis At the initial medical evaluation And every 5 years, or more frequently if indicated Obtain a lipid profile at initiation of statin therapy, and periodically thereafter. E American Diabetes Association Standards of Medical Care in Diabetes. Cardiovascular disease and risk management. Diabetes Care 2017; 40 (Suppl. 1): S75-S87
19 Recommendations: Lipid Management (2) To improve lipid profile in patients with diabetes, recommend lifestyle modification A, focusing on: Weight loss (if indicated) Reduction of saturated fat, trans fat, cholesterol intake Increase of ω-3 fatty acids, viscous fiber, plant stanols/sterols Increased physical activity American Diabetes Association Standards of Medical Care in Diabetes. Cardiovascular disease and risk management. Diabetes Care 2017; 40 (Suppl. 1): S75-S87
20 Recommendations: Lipid Management (3) Intensify lifestyle therapy & optimize glycemic control for patients with: C Triglyceride levels >150 mg/dl (1.7 mmol/l) and/or HDL cholesterol <40 mg/dl (1.0 mmol/l) in men and <50 mg/dl (1.3 mmol/l) in women For patients with fasting triglyceride levels 500 mg/dl (5.7 mmol/l), evaluate for secondary causes and consider medical therapy to reduce the risk of pancreatitis. C American Diabetes Association Standards of Medical Care in Diabetes. Cardiovascular disease and risk management. Diabetes Care 2017; 40 (Suppl. 1): S75-S87
21 New ACC/AHA guideline Ultimate goals: prevent ASCVD and improve the management of patients with ASCVD

22 New ACC/AHA guideline
23 Focus on ASCVD Risk Reduction: 4 statin benefit groups* Clinical ASCVD LDL-C level 190 mg/dl Diabetes, aged years, with LDL-C mg/dl Estimated 10-year risk of ASCVD of 7.5%, years of age, and with LDL-C mg/dl * Moderate- or high-intensity statin therapy recommended for these 4 groups Clinical ASCVD defined as acute coronary syndromes, history of MI, stable or unstable angina, coronary or arterial revascul arization, stroke, transient ischemic attacks, or peripheral artery disease Estimated using Pooled Cohort Risk Assessment Equations Stone NJ, et al. J Am Coll Cardiol. 2013: doi: /j.jacc Available at: spx?articleid= Accessed November 13,
24 In Asian: can be considered lesser potent statin Intensity of Statin Therapy High-Intensity Statin Th erapy Moderate-Intensity Stai n Therapy Low-Intensity Statin Th erapy LDL C 50% LDL C 30% to <50% LDL C <30% Atorvastatin (40 ) 80 mg Rosuvastatin 20 (40) mg Atorvastatin 10 (20) mg Rosuvastatin (5) 10 mg Simvastatin mg Pravastatin 40 (80) mg Lovastatin 40 mg Fluvastatin XL 80 mg Fluvastatin 40 mg bid Pitavastatin 2 4 mg Simvastatin 10 mg Pravastatin mg Lovastatin 20 mg Fluvastatin mg Pitavastatin 1 mg Lifestyle modification remains a critical component of ASCVD risk reduction, both prior to and in concert with the us e of cholesterol lowering drug therapies. Statins/doses that were not tested in randomized controlled trials (RCTs) reviewed are listed in italics Evidence from 1 RCT only: down-titration if unable to tolerate atorvastatin 80 mg in IDEAL Initiation of or titration to simvastatin 80 mg not recommended by the FDA due to the increased risk of myopathy, including rhabdo myolysis. Stone NJ, et al. J Am Coll Cardiol. 2013: doi: /j.jacc Available at: spx?articleid= Accessed November 13, 2013.
25 Recommendations for Statin Treatment in People with Diabetes Age <40 years years >75 years None Risk Factors ASCVD risk factor(s) ASCVD None ASCVD risk factors ACS & LDL 50 or in patients with history of ASCVD who can t tolerate high dose statin None ASCVD risk factors ASCVD ACS & LDL 50 or in patients with history of ASCVD who can t tolerate high dose statin Statin Intensity * None Moderate or high High Moderate High Moderate + ezetimibe Moderate Moderate or high High Moderate + ezetimibe
26 Recommendations: Lipid Management (4) In clinical practice, providers may need to adjust intensity of statin therapy based on individual patient response to medication (e.g., side effects, tolerability, LDL cholesterol levels). E Ezetimibe + moderate intensity statin therapy provides add l CV benefit over moderate intensity statin therapy alone; consider for patients with a recent acute coronary syndrome w/ LDL 50mg/dL A or in patients with a history of ASCVD who can t tolerate high-intensity statin therapy. E American Diabetes Association Standards of Medical Care in Diabetes. Cardiovascular disease and risk management. Diabetes Care 2017; 40 (Suppl. 1): S75-S87
27 Recommendations: Lipid Management (5) Combination therapy (statin/fibrate) doesn t improve ASCVD outcomes and is generally not recommended A. Consider therapy with statin and fenofibrate for men with both trigs 204 mg/dl (2.3 mmol/l) and HDL 34 mg/dl (0.9 mmol/l). B Combination therapy (statin/niacin) hasn t demonstrated additional CV benefit over statins alone, may raise risk of stroke & is not generally recommended. A Statin therapy is contraindicated in pregnancy. B American Diabetes Association Standards of Medical Care in Diabetes. Cardiovascular disease and risk management. Diabetes Care 2017; 40 (Suppl. 1): S75-S87
28 Dyslipidemia management in Korea : NCEP + AHA
29 Mechanisms of Action Oral Antiplatelet Therapies Clopidogrel ADP Cilostazol Ticlopidine ADP phosphodiesterase ADP GP IIb/IIIa (fibrinogen receptor) COX TXA 2 camp Activation 5HT 2A collagen thrombin TXA 2 Sarpogrelate Aspirin ADP = adenosine diphosphate, TXA 2 = thromboxane A 2, COX = cyclooxygenase.
30 Overall effect in patients with diabetes not significant. Diabetes Care 2009
31 Recommendations: Antiplatelet Agents Consider aspirin therapy ( mg/day) C As a primary prevention strategy in those with type 1 or type 2 diabetes at increased cardiovascular risk Includes most men or women with diabetes age 50 years who have at least one additional major risk factor, including: Family history of premature ASCVD Hypertension Smoking Dyslipidemia Albuminuria American Diabetes Association Standards of Medical Care in Diabetes. Cardiovascular disease and risk management. Diabetes Care 2017; 40 (Suppl. 1): S75-S87
32 Recommendations: Antiplatelet Agents (2) Aspirin is not recommended for ASCVD prevention for adults with DM at low ASCVD risk, since potential adverse effects from bleeding likely offset potential benefits. C Low risk: such as in men or women with diabetes aged <50 years with no major additional ASCVD risk factors) In patients with diabetes <50 years of age with multiple other risk factors (e.g., 10-year risk 5 10%), clinical judgment is required. E American Diabetes Association Standards of Medical Care in Diabetes. Cardiovascular disease and risk management. Diabetes Care 2017; 40 (Suppl. 1): S75-S87
33 Recommendations: Antiplatelet Agents (3) Use aspirin therapy ( mg/day) as secondary prevention in those with diabetes and history of ASCVD. A For patients w/ ASCVD & aspirin allergy, clopidogrel (75 mg/day) should be used. B Dual antiplatelet therapy is reasonable for up to a year after an acute coronary syndrome. B American Diabetes Association Standards of Medical Care in Diabetes. Cardiovascular disease and risk management. Diabetes Care 2017; 40 (Suppl. 1): S75-S87
34 Recommendations: Coronary Heart Disease Screening In asymptomatic patients, routine screening for CAD isn t recommended & doesn t improve outcomes provided ASCVD risk factors are treated. A Consider investigations for CAD with: Atypical cardiac symptoms (e.g. unexplained dyspnea, chest discomfort) Signs or symptoms of associated vascular disease incl. carotid bruits, transient ischemic attack, stroke, claudication or PAD EKG abnormalities (e.g. Q waves) E Treadmill test, Multi-detector CT, SPECT, or Coronary angiography American Diabetes Association Standards of Medical Care in Diabetes. Cardiovascular disease and risk management. Diabetes Care 2017; 40 (Suppl. 1): S75-S87
35 Recommendations: Coronary Heart Disease (2) Treatment In patients with known ASCVD, use aspirin and statin therapy (if not contraindicated) A and consider ACE inhibitor therapy C to reduce risk of cardiovascular events. In patients with a prior MI, β-blockers should be continued for at least 2 years after the event. B American Diabetes Association Standards of Medical Care in Diabetes. Cardiovascular disease and risk management. Diabetes Care 2017; 40 (Suppl. 1): S75-S87
36 Conclusion To prevent macrovascular complication of diabetes mellitus (in Type 1 or Type2 DM) Glycemic control & management of Multiple CV risk factors Hypertension: <140/90 mmhg (but, we should modify the target for considering the degree of target organ damage) Dyslipidemia: over 40 yrs of diabetes, CV risk factors Statin therapy (intensified) is essential Low dose anti-platelet therapy Not for the primary prevention in DM patients with low ASCVD risk Definitely Yes!!! For the secondary prevention of CVD
Disclosures. Diabetes and Cardiovascular Risk Management. Learning Objectives. Atherosclerotic Cardiovascular Disease
 Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Dyslipidemia in the light of Current Guidelines - Do we change our Practice?
 Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
American Diabetes Association 2018 Guidelines Important Notable Points
 American Diabetes Association 2018 Guidelines Important Notable Points The Standards of Medical Care in Diabetes-2018 by ADA include the most current evidencebased recommendations for diagnosing and treating
American Diabetes Association 2018 Guidelines Important Notable Points The Standards of Medical Care in Diabetes-2018 by ADA include the most current evidencebased recommendations for diagnosing and treating
New Guidelines in Dyslipidemia Management
 The Fourth IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2018 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
The Fourth IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2018 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
New Guidelines in Dyslipidemia Management
 The Third IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2017 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
The Third IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2017 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
Diabetes and Cardiovascular Risk Management Denise M. Kolanczyk, PharmD, BCPS-AQ Cardiology
 Diabetes and Cardiovascular Risk Management Denise M. Kolanczyk, PharmD, BCPS-AQ Cardiology Disclosures In compliance with the accrediting board policies, the American Diabetes Association requires the
Diabetes and Cardiovascular Risk Management Denise M. Kolanczyk, PharmD, BCPS-AQ Cardiology Disclosures In compliance with the accrediting board policies, the American Diabetes Association requires the
What do the guidelines say about combination therapy?
 What do the guidelines say about combination therapy? Christie M. Ballantyne, MD Center for Cardiovascular Disease Prevention Methodist DeBakey Heart & Vascular Center Baylor College of Medicine Houston,
What do the guidelines say about combination therapy? Christie M. Ballantyne, MD Center for Cardiovascular Disease Prevention Methodist DeBakey Heart & Vascular Center Baylor College of Medicine Houston,
Diabetes Mellitus: A Cardiovascular Disease
 Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
Diabetes: Use of Adjunctive Therapy ACEs, ARBs, ASA & STATINs --Oh My! Veronica J. Brady, PhD, FNP-BC, BC-ADM, CDE Project ECHO April 19, 2018
 Diabetes: Use of Adjunctive Therapy ACEs, ARBs, ASA & STATINs --Oh My! Veronica J. Brady, PhD, FNP-BC, BC-ADM, CDE Project ECHO April 19, 2018 Points to Ponder ASCVD is the leading cause of morbidity
Diabetes: Use of Adjunctive Therapy ACEs, ARBs, ASA & STATINs --Oh My! Veronica J. Brady, PhD, FNP-BC, BC-ADM, CDE Project ECHO April 19, 2018 Points to Ponder ASCVD is the leading cause of morbidity
Standards of Medical Care in Diabetes 2016
 Standards of Medical Care in Diabetes 2016 Care Delivery Systems 33-49% of patients still do not meet targets for A1C, blood pressure, or lipids. 14% meet targets for all A1C, BP, lipids, and nonsmoking
Standards of Medical Care in Diabetes 2016 Care Delivery Systems 33-49% of patients still do not meet targets for A1C, blood pressure, or lipids. 14% meet targets for all A1C, BP, lipids, and nonsmoking
2013 ACC/AHA Cholesterol Guidelines JULIE HAMMOND, D.O. PGY-2 MATTHEW PAOLI, D.O. PGY-2
 2013 ACC/AHA Cholesterol Guidelines JULIE HAMMOND, D.O. PGY-2 MATTHEW PAOLI, D.O. PGY-2 GOALS ACC/AHA as publisher of guidelines Determining which patients are appropriate for statin therapy The treatment
2013 ACC/AHA Cholesterol Guidelines JULIE HAMMOND, D.O. PGY-2 MATTHEW PAOLI, D.O. PGY-2 GOALS ACC/AHA as publisher of guidelines Determining which patients are appropriate for statin therapy The treatment
Cholesterol Management Roy Gandolfi, MD
 Cholesterol Management 2017 Roy Gandolfi, MD Goals Interpreting cholesterol guidelines Cholesterol treatment in diabetics Statin use and side effects therapy Reporting- Comparison data among physicians
Cholesterol Management 2017 Roy Gandolfi, MD Goals Interpreting cholesterol guidelines Cholesterol treatment in diabetics Statin use and side effects therapy Reporting- Comparison data among physicians
Disclosures No relationships (not even to an employer) No off-label uses. Cholesterol Lowering Guidelines: What now?
 No off-label uses. Cholesterol Lowering Guidelines: What now?") Disclosures No relationships (not even to an employer) No off-label uses Cholesterol Lowering Guidelines: What now?, FACP 1 2 65-year-old white woman Total cholesterol 175mg/dL HDL 54 mg/dl LDL 96 mg/dl
Disclosures No relationships (not even to an employer) No off-label uses Cholesterol Lowering Guidelines: What now?, FACP 1 2 65-year-old white woman Total cholesterol 175mg/dL HDL 54 mg/dl LDL 96 mg/dl
American Diabetes Association: Standards of Medical Care in Diabetes 2015
 American Diabetes Association: Standards of Medical Care in Diabetes 2015 Synopsis of ADA standards relevant to the 11 th Scope of Work under Task B.2 ASSESSMENT OF GLYCEMIC CONTROL Recommendations: Perform
American Diabetes Association: Standards of Medical Care in Diabetes 2015 Synopsis of ADA standards relevant to the 11 th Scope of Work under Task B.2 ASSESSMENT OF GLYCEMIC CONTROL Recommendations: Perform
Lipid Management 2013 Statin Benefit Groups
 Clinical Integration Steering Committee Clinical Integration Chronic Disease Management Work Group Lipid Management 2013 Statin Benefit Groups Approved by Board Chair Signature Name (Please Print) Date
Clinical Integration Steering Committee Clinical Integration Chronic Disease Management Work Group Lipid Management 2013 Statin Benefit Groups Approved by Board Chair Signature Name (Please Print) Date
No relevant financial relationships
 MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD
 2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD How do you interpret my blood test results? What are our targets for these tests? Before the ACC/AHA Lipid Guidelines A1c:
2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD How do you interpret my blood test results? What are our targets for these tests? Before the ACC/AHA Lipid Guidelines A1c:
Prevention of Cardiovascular Disease
 Save Thais from Heart Diseases 2019 Prevention of Cardiovascular Disease Orawan Anupraiwan, MD. Central Chest Institute of Thailand ASCVD Prevention Pyramid Risk categories Very high-risk High-risk Documented
Save Thais from Heart Diseases 2019 Prevention of Cardiovascular Disease Orawan Anupraiwan, MD. Central Chest Institute of Thailand ASCVD Prevention Pyramid Risk categories Very high-risk High-risk Documented
Cardiovascular risk reduction in diabetes Lipids (NICE CG181)
") Cardiovascular risk reduction in diabetes Lipids (NICE CG181) Primary Prevention T1DM Offer Atorvastatin 20mg if >40 years old Diabetes duration >10 years Established nephropathy Other CVS risk factors
Cardiovascular risk reduction in diabetes Lipids (NICE CG181) Primary Prevention T1DM Offer Atorvastatin 20mg if >40 years old Diabetes duration >10 years Established nephropathy Other CVS risk factors
Conflict of Interest Disclosure. Learning Objectives. Learning Objectives. Guidelines. Update on Lifestyle Guidelines
 Conflict of Interest Disclosure Updates for the Ambulatory Care Pharmacist: Dyslipidemia and CV Risk Assessment No conflicts of interest to disclose 2014 Updates to the Updates in Ambulatory Care Pharmacy
Conflict of Interest Disclosure Updates for the Ambulatory Care Pharmacist: Dyslipidemia and CV Risk Assessment No conflicts of interest to disclose 2014 Updates to the Updates in Ambulatory Care Pharmacy
Highlights of the new blood pressure and cholesterol guidelines: A whole new philosophy. Jeremy L. Johnson, PharmD, BCACP, CDE, BC-ADM
 Highlights of the new blood pressure and cholesterol guidelines: A whole new philosophy Jeremy L. Johnson, PharmD, BCACP, CDE, BC-ADM OSHP 2014 Annual Meeting Oklahoma City, OK April 4, 2014 1 Objectives
Highlights of the new blood pressure and cholesterol guidelines: A whole new philosophy Jeremy L. Johnson, PharmD, BCACP, CDE, BC-ADM OSHP 2014 Annual Meeting Oklahoma City, OK April 4, 2014 1 Objectives
How would you manage Ms. Gold
 How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
Placebo-Controlled Statin Trials EXPLAINING THE DECREASE IN DEATHS FROM CHD! PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN EXPLAINING THE DECREASE IN
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
PIEDMONT ACCESS TO HEALTH SERVICES, INC. Guidelines for Screening and Management of Dyslipidemia
 PIEDMONT ACCESS TO HEALTH SERVICES, INC. Policy Number: 01-09-021 SUBJECT: Guidelines for Screening and Management of Dyslipidemia EFFECTIVE DATE: 04/2008 REVIEWED/REVISED: 04/12/10, 03/17/2011, 4/10/2012,
PIEDMONT ACCESS TO HEALTH SERVICES, INC. Policy Number: 01-09-021 SUBJECT: Guidelines for Screening and Management of Dyslipidemia EFFECTIVE DATE: 04/2008 REVIEWED/REVISED: 04/12/10, 03/17/2011, 4/10/2012,
9/29/2015. Primary Prevention of Heart Disease: Objectives. Objectives. What works? What doesn t?
 Primary Prevention of Heart Disease: What works? What doesn t? Samia Mora, MD, MHS Associate Professor, Harvard Medical School Associate Physician, Brigham and Women s Hospital October 2, 2015 Financial
Primary Prevention of Heart Disease: What works? What doesn t? Samia Mora, MD, MHS Associate Professor, Harvard Medical School Associate Physician, Brigham and Women s Hospital October 2, 2015 Financial
American Diabetes Association Standards of Medical Care in Diabetes 2017: Focus on Complications
 American Diabetes Association Standards of Medical Care in Diabetes 2017: Focus on Complications Juan Pablo Frias, M.D., FACE President and CEO, National Research Institute, Los Angeles, CA Clinical Faculty,
American Diabetes Association Standards of Medical Care in Diabetes 2017: Focus on Complications Juan Pablo Frias, M.D., FACE President and CEO, National Research Institute, Los Angeles, CA Clinical Faculty,
Andrew Cohen, MD and Neil S. Skolnik, MD INTRODUCTION
 2 Hyperlipidemia Andrew Cohen, MD and Neil S. Skolnik, MD CONTENTS INTRODUCTION RISK CATEGORIES AND TARGET LDL-CHOLESTEROL TREATMENT OF LDL-CHOLESTEROL SPECIAL CONSIDERATIONS OLDER AND YOUNGER ADULTS ADDITIONAL
2 Hyperlipidemia Andrew Cohen, MD and Neil S. Skolnik, MD CONTENTS INTRODUCTION RISK CATEGORIES AND TARGET LDL-CHOLESTEROL TREATMENT OF LDL-CHOLESTEROL SPECIAL CONSIDERATIONS OLDER AND YOUNGER ADULTS ADDITIONAL
Clinical Recommendations: Patients with Periodontitis
 The American Journal of Cardiology and Journal of Periodontology Editors' Consensus: Periodontitis and Atherosclerotic Cardiovascular Disease. Friedewald VE, Kornman KS, Beck JD, et al. J Periodontol 2009;
The American Journal of Cardiology and Journal of Periodontology Editors' Consensus: Periodontitis and Atherosclerotic Cardiovascular Disease. Friedewald VE, Kornman KS, Beck JD, et al. J Periodontol 2009;
Disclosure. No relevant financial relationships. Placebo-Controlled Statin Trials
 MANAGEMENT OF HYPERLIPIDEMIA AND CARDIOVASCULAR RISK IN WOMEN: Balancing Benefits and Harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
MANAGEMENT OF HYPERLIPIDEMIA AND CARDIOVASCULAR RISK IN WOMEN: Balancing Benefits and Harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
Learning Objectives. Patient Case
 Joseph Saseen, Pharm.D., FASHP, FCCP, BCPS Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Learning Objectives Identify the 4 patient populations
Joseph Saseen, Pharm.D., FASHP, FCCP, BCPS Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Learning Objectives Identify the 4 patient populations
Standards of Medical Care In Diabetes
 Standards of Medical Care In Diabetes - 2017 Robert E. Ratner, MD, FACP, FACE Professor of Medicine Georgetown University School of Medicine Disclosed no conflict of interest Standards of Care Professional.diabetes.org/SOC
Standards of Medical Care In Diabetes - 2017 Robert E. Ratner, MD, FACP, FACE Professor of Medicine Georgetown University School of Medicine Disclosed no conflict of interest Standards of Care Professional.diabetes.org/SOC
Diabetes and Hypertension
 Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
Diabetes Complications Guideline Based Screening, Management, and Referral
 Diabetes Complications Guideline Based Screening, Management, and Referral Eric L. Johnson, M.D. Associate Professor Department of Family and Community Medicine Assistant Medical Director Altru Diabetes
Diabetes Complications Guideline Based Screening, Management, and Referral Eric L. Johnson, M.D. Associate Professor Department of Family and Community Medicine Assistant Medical Director Altru Diabetes
Cardiovascular Health Practice Guideline Outpatient Management of Coronary Artery Disease 2003
 Authorized By: Medical Management Guideline Committee Approval Date: 12/13/01 Revision Date: 12/11/03 Beta-Blockers Nitrates Calcium Channel Blockers MEDICATIONS Indicated in post-mi, unstable angina,
Authorized By: Medical Management Guideline Committee Approval Date: 12/13/01 Revision Date: 12/11/03 Beta-Blockers Nitrates Calcium Channel Blockers MEDICATIONS Indicated in post-mi, unstable angina,
CLINICAL OUTCOME Vs SURROGATE MARKER
 CLINICAL OUTCOME Vs SURROGATE MARKER Statin Real Experience Dr. Mostafa Sherif Senior Medical Manager Pfizer Egypt & Sudan Objective Difference between Clinical outcome and surrogate marker Proper Clinical
CLINICAL OUTCOME Vs SURROGATE MARKER Statin Real Experience Dr. Mostafa Sherif Senior Medical Manager Pfizer Egypt & Sudan Objective Difference between Clinical outcome and surrogate marker Proper Clinical
Introduction. Objective. Critical Questions Addressed
 Introduction Objective To provide a strong evidence-based foundation for the treatment of cholesterol for the primary and secondary prevention of ASCVD in women and men Critical Questions Addressed CQ1:
Introduction Objective To provide a strong evidence-based foundation for the treatment of cholesterol for the primary and secondary prevention of ASCVD in women and men Critical Questions Addressed CQ1:
MOLINA HEALTHCARE OF CALIFORNIA
 MOLINA HEALTHCARE OF CALIFORNIA HIGH BLOOD CHOLESTEROL IN ADULTS GUIDELINE Molina Healthcare of California has adopted the Third Report of the National Cholesterol Education Program (NCEP) Expert Panel
MOLINA HEALTHCARE OF CALIFORNIA HIGH BLOOD CHOLESTEROL IN ADULTS GUIDELINE Molina Healthcare of California has adopted the Third Report of the National Cholesterol Education Program (NCEP) Expert Panel
No relevant financial relationships
 MANAGEMENT OF LIPID DISORDERS: WHERE DO WE STAND WITH THE NEW PRACTICE GUIDELINES? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant financial relationships
MANAGEMENT OF LIPID DISORDERS: WHERE DO WE STAND WITH THE NEW PRACTICE GUIDELINES? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant financial relationships
Complications of Diabetes mellitus. Dr Bill Young 16 March 2015
 Complications of Diabetes mellitus Dr Bill Young 16 March 2015 Complications of diabetes Multi-organ involvement 2 The extent of diabetes complications At diagnosis as many as 50% of patients may have
Complications of Diabetes mellitus Dr Bill Young 16 March 2015 Complications of diabetes Multi-organ involvement 2 The extent of diabetes complications At diagnosis as many as 50% of patients may have
Lipid Therapy: Statins and Beyond. Ivan Anderson, MD RIHVH Cardiology
 Lipid Therapy: Statins and Beyond Ivan Anderson, MD RIHVH Cardiology Outline The cholesterol hypothesis and lipid metabolism The Guidelines 4 Groups that Benefit from Lipid therapy Initiation and monitoring
Lipid Therapy: Statins and Beyond Ivan Anderson, MD RIHVH Cardiology Outline The cholesterol hypothesis and lipid metabolism The Guidelines 4 Groups that Benefit from Lipid therapy Initiation and monitoring
Cardiovascular Risk Reduction and Other Co-Morbidities in Type 2 Diabetes
 Cardiovascular Risk Reduction and Other Co-Morbidities in Type 2 Diabetes Following this presentation, you will be able to: Describe the relationship between major CV risk factors and CVD outcomes Select
Cardiovascular Risk Reduction and Other Co-Morbidities in Type 2 Diabetes Following this presentation, you will be able to: Describe the relationship between major CV risk factors and CVD outcomes Select
Primary Prevention Patients aged 85yrs and over
 Rotherham Guideline for the management of Non-Familial Hypercholesterolaemia Type 1 Diabetes Offer lifestyle advice Over 40yrs of age? Diabetic for more than 10 years? Established nephropathy? Other CVD
Rotherham Guideline for the management of Non-Familial Hypercholesterolaemia Type 1 Diabetes Offer lifestyle advice Over 40yrs of age? Diabetic for more than 10 years? Established nephropathy? Other CVD
Coronary Artery Disease Clinical Practice Guidelines
 Coronary Artery Disease Clinical Practice Guidelines Guidelines are systematically developed statements to assist patients and providers in choosing appropriate healthcare for specific clinical conditions.
Coronary Artery Disease Clinical Practice Guidelines Guidelines are systematically developed statements to assist patients and providers in choosing appropriate healthcare for specific clinical conditions.
Disclosure. No relevant financial relationships. Placebo-Controlled Statin Trials
 PREVENTING CARDIOVASCULAR DISEASE IN WOMEN: Current Guidelines for Hypertension, Lipids and Aspirin Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
PREVENTING CARDIOVASCULAR DISEASE IN WOMEN: Current Guidelines for Hypertension, Lipids and Aspirin Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
Placebo-Controlled Statin Trials Prevention Of CVD in Women"
 MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
Placebo-Controlled Statin Trials MANAGEMENT OF HIGH BLOOD CHOLESTEROL MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES
 MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
Case Studies The Role of Non-Statin Therapies for LDL-C Lowering in the Management of ASCVD Risk
 Case Studies The Role of Non-Statin Therapies for LDL-C Lowering in the Management of ASCVD Risk Kim K. Birtcher, PharmD, MS, AACC Clinical Professor University of Houston College of Pharmacy Houston,
Case Studies The Role of Non-Statin Therapies for LDL-C Lowering in the Management of ASCVD Risk Kim K. Birtcher, PharmD, MS, AACC Clinical Professor University of Houston College of Pharmacy Houston,
Sanger Heart & Vascular Institute Symposium 2015
 Sanger Heart & Vascular Institute Symposium 2015 Cardiovascular Update For Primary Care Physicians William E. Downey, MD FACC FSCAI Medical Director, Interventional Cardiology Sanger Heart & Vascular Institute
Sanger Heart & Vascular Institute Symposium 2015 Cardiovascular Update For Primary Care Physicians William E. Downey, MD FACC FSCAI Medical Director, Interventional Cardiology Sanger Heart & Vascular Institute
Management of Lipid Disorders and Hypertension: Implications of the New Guidelines
 Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Lipid Panel Management Refresher Course for the Family Physician
 Lipid Panel Management Refresher Course for the Family Physician Objectives Understand the evidence that was evaluated to develop the 2013 ACC/AHA guidelines Discuss the utility and accuracy of the new
Lipid Panel Management Refresher Course for the Family Physician Objectives Understand the evidence that was evaluated to develop the 2013 ACC/AHA guidelines Discuss the utility and accuracy of the new
Environmental. Vascular / Tissue. Metabolics
 Global Risk Reduction--WINS Picking Mom and Dad-2016 Environmental Vascular / Tissue Metabolics Stop smoking-1b Physical activity-1b Weight control-1b Chelation therapy-3c Influenza vaccination-1b Blood
Global Risk Reduction--WINS Picking Mom and Dad-2016 Environmental Vascular / Tissue Metabolics Stop smoking-1b Physical activity-1b Weight control-1b Chelation therapy-3c Influenza vaccination-1b Blood
DYSLIPIDEMIA TREATMENT: HYBRIDIZING CLINICAL PRACTICE GUIDELINES
 DYSLIPIDEMIA TREATMENT: HYBRIDIZING CLINICAL PRACTICE GUIDELINES SATURDAY/4:30-5:30PM ACPE UAN: 0107-9999-17-249-L01-P 0.1 CEU/1.0 hr Activity Type: Knowledge-Based Learning Objectives for Pharmacists:
DYSLIPIDEMIA TREATMENT: HYBRIDIZING CLINICAL PRACTICE GUIDELINES SATURDAY/4:30-5:30PM ACPE UAN: 0107-9999-17-249-L01-P 0.1 CEU/1.0 hr Activity Type: Knowledge-Based Learning Objectives for Pharmacists:
4/7/ The stats on heart disease. + Deaths & Age-Adjusted Death Rates for
 + Update on Lipid Management Stacey Gardiner, MD Assistant Professor Division of Cardiovascular Medicine Medical College of Wisconsin + The stats on heart disease Over the past 10 years for which statistics
+ Update on Lipid Management Stacey Gardiner, MD Assistant Professor Division of Cardiovascular Medicine Medical College of Wisconsin + The stats on heart disease Over the past 10 years for which statistics
New Lipid Guidelines. PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids.
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
New Cholesterol Guidelines What the LDL are we supposed to do now?!
 New Cholesterol Guidelines What the LDL are we supposed to do now?! Michael D. Shapiro Assistant Professor of Medicine and Radiology Knight Cardiovascular Institute Oregon Health & Science University 2013
New Cholesterol Guidelines What the LDL are we supposed to do now?! Michael D. Shapiro Assistant Professor of Medicine and Radiology Knight Cardiovascular Institute Oregon Health & Science University 2013
Disclosures. Overview 9/30/ ACC/AHA Guidelines on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults
 2013 ACC/AHA Guidelines on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults 2014 AAHP Fall Seminar Sherry Myatt, PharmD, BCPS Assistant Director of Pharmacy for
2013 ACC/AHA Guidelines on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults 2014 AAHP Fall Seminar Sherry Myatt, PharmD, BCPS Assistant Director of Pharmacy for
New Hypertension Guideline Recommendations for Adults July 7, :45-9:30am
 Advances in Cardiovascular Disease 30 th Annual Convention and Reunion UERM-CMAA, Inc. Annual Convention and Scientific Meeting July 5-8, 2018 New Hypertension Guideline Recommendations for Adults July
Advances in Cardiovascular Disease 30 th Annual Convention and Reunion UERM-CMAA, Inc. Annual Convention and Scientific Meeting July 5-8, 2018 New Hypertension Guideline Recommendations for Adults July
Diabetes Update: Diabetes Management In Primary Care. Jonathon M. Firnhaber, MD, FAAFP
 Diabetes Update: Diabetes Management In Primary Care Jonathon M. Firnhaber, MD, FAAFP Learning objectives 1. Critically evaluate the evidence emerging within diabetes research as it applies to recommendations
Diabetes Update: Diabetes Management In Primary Care Jonathon M. Firnhaber, MD, FAAFP Learning objectives 1. Critically evaluate the evidence emerging within diabetes research as it applies to recommendations
Review of guidelines for management of dyslipidemia in diabetic patients
 2012 international Conference on Diabetes and metabolism (ICDM) Review of guidelines for management of dyslipidemia in diabetic patients Nan Hee Kim, MD, PhD Department of Internal Medicine, Korea University
2012 international Conference on Diabetes and metabolism (ICDM) Review of guidelines for management of dyslipidemia in diabetic patients Nan Hee Kim, MD, PhD Department of Internal Medicine, Korea University
Module 2. Global Cardiovascular Risk Assessment and Reduction in Women with Hypertension
 Module 2 Global Cardiovascular Risk Assessment and Reduction in Women with Hypertension 1 Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored,
Module 2 Global Cardiovascular Risk Assessment and Reduction in Women with Hypertension 1 Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored,
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN
 1980 to 2000: Death rate fell from: 542.9 to 266.8 per 100K men 263.3 to 134.4 per 100K women 341,745 fewer deaths from CHD in 2000 Ford ES, NEJM, 2007 47% from CHD treatments, 44% from risk factor modification
1980 to 2000: Death rate fell from: 542.9 to 266.8 per 100K men 263.3 to 134.4 per 100K women 341,745 fewer deaths from CHD in 2000 Ford ES, NEJM, 2007 47% from CHD treatments, 44% from risk factor modification
Acute Coronary Syndromes (ACS)
") Sally A. Arif, Pharm.D., BCPS (AQ Cardiology) Assistant Professor of Pharmacy Practice Midwestern University, Chicago College of Pharmacy Cardiology Clinical Specialist, Rush University Medical Center
Sally A. Arif, Pharm.D., BCPS (AQ Cardiology) Assistant Professor of Pharmacy Practice Midwestern University, Chicago College of Pharmacy Cardiology Clinical Specialist, Rush University Medical Center
Approach to Dyslipidemia among diabetic patients
 Approach to Dyslipidemia among diabetic patients Farzad Hadaegh, MD, Professor of Internal Medicine & Endocrinology Prevention of Metabolic Disorders Research Center, Research Institute for Endocrine Sciences
Approach to Dyslipidemia among diabetic patients Farzad Hadaegh, MD, Professor of Internal Medicine & Endocrinology Prevention of Metabolic Disorders Research Center, Research Institute for Endocrine Sciences
9/18/2017 DISCLOSURES. Consultant: RubiconMD. Research: Amgen, NHLBI OUTLINE OBJECTIVES. Review current CV risk assessment tools.
 UW MEDICINE UW MEDICINE UCSF ASIAN TITLE HEALTH OR EVENT SYMPOSIUM 2017 DISCLOSURES Consultant: RubiconMD ESTIMATING CV RISK IN ASIAN AMERICANS AND PREVENTION OF CVD Research: Amgen, NHLBI EUGENE YANG,
UW MEDICINE UW MEDICINE UCSF ASIAN TITLE HEALTH OR EVENT SYMPOSIUM 2017 DISCLOSURES Consultant: RubiconMD ESTIMATING CV RISK IN ASIAN AMERICANS AND PREVENTION OF CVD Research: Amgen, NHLBI EUGENE YANG,
Updates in Cardiovascular Recommendations for Diabetic Patients
 Updates in Cardiovascular Recommendations for Diabetic Patients Chris Tawwater, Pharm.D., BCPS Clinical Pharmacist, Abilene Regional Medical Center Assistant Professor, Adult Medicine Division Pharmacotherapy
Updates in Cardiovascular Recommendations for Diabetic Patients Chris Tawwater, Pharm.D., BCPS Clinical Pharmacist, Abilene Regional Medical Center Assistant Professor, Adult Medicine Division Pharmacotherapy
hypertension Head of prevention and control of CVD disease office Ministry of heath
 hypertension t. Samavat MD,Cadiologist,MPH Head of prevention and control of CVD disease office Ministry of heath RECOMMENDATIONS FOR HYPERTENSION DIAGNOSIS, ASSESSMENT, AND TREATMENT Definition of hypertension
hypertension t. Samavat MD,Cadiologist,MPH Head of prevention and control of CVD disease office Ministry of heath RECOMMENDATIONS FOR HYPERTENSION DIAGNOSIS, ASSESSMENT, AND TREATMENT Definition of hypertension
Conflicts of interest. What's the Skinny on the Lipid Guidelines? Key Differences. Are you applying the new ACC/AHA Lipid guidelines in your practice?
 Conflicts of interest What's the Skinny on the Lipid Guidelines? The presenter has no relevant conflicts of interest to disclose. Kathleen Vest, PharmD, CDE, BCACP At the end of this presentation, pharmacist
Conflicts of interest What's the Skinny on the Lipid Guidelines? The presenter has no relevant conflicts of interest to disclose. Kathleen Vest, PharmD, CDE, BCACP At the end of this presentation, pharmacist
Standards of Medical Care in Diabetes 2018
 Standards of Medical Care in Diabetes 2018 Eric L. Johnson, M.D. Associate Professor University of North Dakota School of Medicine and Health Sciences Assistant Medical Director Altru Diabetes Center Grand
Standards of Medical Care in Diabetes 2018 Eric L. Johnson, M.D. Associate Professor University of North Dakota School of Medicine and Health Sciences Assistant Medical Director Altru Diabetes Center Grand
Modified version focused on CCNC Quality Measures and Feedback Processes
 Executive Summary: Standards of Medical Care in Diabetes 2010 Modified version focused on CCNC Quality Measures and Feedback Processes See http://care.diabetesjournals.org/content/33/supplement_1/s11.full
Executive Summary: Standards of Medical Care in Diabetes 2010 Modified version focused on CCNC Quality Measures and Feedback Processes See http://care.diabetesjournals.org/content/33/supplement_1/s11.full
Clinical Practice Guideline
 Clinical Practice Guideline Secondary Prevention for Patients with Coronary and Other Vascular Disease Since the 2001 update of the American Heart Association (AHA)/American College of Cardiology (ACC)
Clinical Practice Guideline Secondary Prevention for Patients with Coronary and Other Vascular Disease Since the 2001 update of the American Heart Association (AHA)/American College of Cardiology (ACC)
Praluent. Praluent (alirocumab) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.40.06 Subject: Praluent Page: 1 of 10 Last Review Date: September 20, 2018 Praluent Description Praluent
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.40.06 Subject: Praluent Page: 1 of 10 Last Review Date: September 20, 2018 Praluent Description Praluent
2003 World Health Organization (WHO) / International Society of Hypertension (ISH) Statement on Management of Hypertension.
 / International Society of Hypertension (ISH) Statement on Management of Hypertension.") 2003 World Health Organization (WHO) / International Society of Hypertension (ISH) Statement on Management of Hypertension Writing Group: Background Hypertension worldwide causes 7.1 million premature
2003 World Health Organization (WHO) / International Society of Hypertension (ISH) Statement on Management of Hypertension Writing Group: Background Hypertension worldwide causes 7.1 million premature
Antiplatelet agents treatment
 Session III Comprehensive management of diabetic patients Antiplatelet agents treatment Chonnam National University Hospital Department of Internal Medicine Dong-Hyeok Cho CONTENTS Introduction Prothrombotic
Session III Comprehensive management of diabetic patients Antiplatelet agents treatment Chonnam National University Hospital Department of Internal Medicine Dong-Hyeok Cho CONTENTS Introduction Prothrombotic
Antihypertensive Trial Design ALLHAT
 1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
Lipid Management: The Next Level How Will the New ACC/AHA Guidelines Change My Practice
 Lipid Management: The Next Level How Will the New ACC/AHA Guidelines Change My Practice Vera Bittner, MD, MSPH Professor of Medicine Section Head, Preventive Cardiology Medical Director, Cardiac Rehabilitation
Lipid Management: The Next Level How Will the New ACC/AHA Guidelines Change My Practice Vera Bittner, MD, MSPH Professor of Medicine Section Head, Preventive Cardiology Medical Director, Cardiac Rehabilitation
Dyslipedemia New Guidelines
 Dyslipedemia New Guidelines New ACC/AHA Prevention Guidelines on Blood Cholesterol November 12, 2013 Mohammed M Abd El Ghany Professor of Cardiology Cairo Universlty 1 1 0 Cholesterol Management Pharmacotherapy
Dyslipedemia New Guidelines New ACC/AHA Prevention Guidelines on Blood Cholesterol November 12, 2013 Mohammed M Abd El Ghany Professor of Cardiology Cairo Universlty 1 1 0 Cholesterol Management Pharmacotherapy
Pharmacology Challenges: Managing Statin Myalgia
 Clinical Case: RM is a 50 year-old African American woman with a past medical history of type diabetes, dyslipidemia, hypertension and peripheral arterial disease. She had been prescribed simvastatin 80
Clinical Case: RM is a 50 year-old African American woman with a past medical history of type diabetes, dyslipidemia, hypertension and peripheral arterial disease. She had been prescribed simvastatin 80
Pharmacy Drug Class Review
 Pharmacy Drug Class Review January 22, 2014 Authored By: Christina Manciocchi, Pharm.D. BCACP Disclaimer: Specific agents may have variations Edited By: Richard J. Kraft, Pharm.D.BCPS NEW CHOLESTEROL GUIDELINES
Pharmacy Drug Class Review January 22, 2014 Authored By: Christina Manciocchi, Pharm.D. BCACP Disclaimer: Specific agents may have variations Edited By: Richard J. Kraft, Pharm.D.BCPS NEW CHOLESTEROL GUIDELINES
Cardiovascular Complications of Diabetes
 VBWG Cardiovascular Complications of Diabetes Nicola Abate, M.D., F.N.L.A. Professor and Chief Division of Endocrinology and Metabolism The University of Texas Medical Branch Galveston, Texas Coronary
VBWG Cardiovascular Complications of Diabetes Nicola Abate, M.D., F.N.L.A. Professor and Chief Division of Endocrinology and Metabolism The University of Texas Medical Branch Galveston, Texas Coronary
The Diabetes Link to Heart Disease
 The Diabetes Link to Heart Disease Anthony Abe DeSantis, MD September 18, 2015 University of WA Division of Metabolism, Endocrinology and Nutrition Oswald Toosweet Case #1 68 yo M with T2DM Diagnosed DM
The Diabetes Link to Heart Disease Anthony Abe DeSantis, MD September 18, 2015 University of WA Division of Metabolism, Endocrinology and Nutrition Oswald Toosweet Case #1 68 yo M with T2DM Diagnosed DM
2019 Update on Recent Guideline Releases for Diabetes, Hypertension, and Dyslipidemia: Can We, Please, All Just Get on the Same Page?!
 2019 Update on Recent Guideline Releases for Diabetes, Hypertension, and Dyslipidemia: Can We, Please, All Just Get on the Same Page?! Jeremy L. Johnson, PharmD, BCACP, CDE, BC-ADM Assistant Professor,
2019 Update on Recent Guideline Releases for Diabetes, Hypertension, and Dyslipidemia: Can We, Please, All Just Get on the Same Page?! Jeremy L. Johnson, PharmD, BCACP, CDE, BC-ADM Assistant Professor,
Clinical Practice Guidelines for Diabetes Management
 Clinical Practice Guidelines for Diabetes Management Diabetes is a disease in which blood glucose levels are above normal. Over the years, high blood glucose damages nerves and blood vessels, which can
Clinical Practice Guidelines for Diabetes Management Diabetes is a disease in which blood glucose levels are above normal. Over the years, high blood glucose damages nerves and blood vessels, which can
2017 Cardiovascular Summit for Primary Care Thursday 30th & Friday 31st March Crowne Plaza, Dublin
 2017 Cardiovascular Summit for Primary Care Thursday 30th & Friday 31st March 2017 - Crowne Plaza, Dublin 2016 ESC Guidelines on Cardiovascular Risk and elevated lipids Carlos Brotons Sardenya Primary
2017 Cardiovascular Summit for Primary Care Thursday 30th & Friday 31st March 2017 - Crowne Plaza, Dublin 2016 ESC Guidelines on Cardiovascular Risk and elevated lipids Carlos Brotons Sardenya Primary
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
4/24/15. AHA/ACC 2013 Guideline Key Points
 Review of the ACC/AHA 2013 Guidelines Anita Ralstin, MS, CNS, CNP Next Step Health Consultant, LLC 1! Discuss the rationale for the change in lipid guidelines and how that affects the decision to implement
Review of the ACC/AHA 2013 Guidelines Anita Ralstin, MS, CNS, CNP Next Step Health Consultant, LLC 1! Discuss the rationale for the change in lipid guidelines and how that affects the decision to implement
ATP IV: Predicting Guideline Updates
 Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
An update on lipidology and cardiovascular risk management. Lipids, Metabolism & Vascular Risk Section - Royal Society of Medicine
 An update on lipidology and cardiovascular risk management Lipids, Metabolism & Vascular Risk Section - Royal Society of Medicine National and international lipid modification guidelines: A critical appraisal
An update on lipidology and cardiovascular risk management Lipids, Metabolism & Vascular Risk Section - Royal Society of Medicine National and international lipid modification guidelines: A critical appraisal
Adult Diabetes Clinician Guide NOVEMBER 2017
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Adult Diabetes Clinician Guide Introduction NOVEMBER 2017 This evidence-based guideline summary is based on the 2017 KP National Diabetes Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Adult Diabetes Clinician Guide Introduction NOVEMBER 2017 This evidence-based guideline summary is based on the 2017 KP National Diabetes Guideline.
Treatment of Cardiovascular Risk Factors. Kevin M Hayes D.O. F.A.C.C. First Coast Heart and Vascular Center
 Treatment of Cardiovascular Risk Factors Kevin M Hayes D.O. F.A.C.C. First Coast Heart and Vascular Center Disclosures: None Objectives What do risk factors tell us What to check and when Does treatment
Treatment of Cardiovascular Risk Factors Kevin M Hayes D.O. F.A.C.C. First Coast Heart and Vascular Center Disclosures: None Objectives What do risk factors tell us What to check and when Does treatment
Hypertension Guidelines: JNC- Late, JNC- 8, or JNC- Fake?
 Hypertension Guidelines: JNC- Late, JNC- 8, or JNC- Fake? Brian G. Choi, MD, MBA, FACC Associate Professor of Medicine Co-Director, Advanced Cardiac Imaging November 14, 2014 Washington, DC Disclosures
Hypertension Guidelines: JNC- Late, JNC- 8, or JNC- Fake? Brian G. Choi, MD, MBA, FACC Associate Professor of Medicine Co-Director, Advanced Cardiac Imaging November 14, 2014 Washington, DC Disclosures
Pharmaceutical Help to Control Cholesterol
 Pharmaceutical Help to Control Cholesterol Catherine E. Cooke, PharmD, BCPS, PAHM President, PosiHealth, Inc. Clinical Associate Professor, Univ. of Maryland This program has been brought to you by PharmCon
Pharmaceutical Help to Control Cholesterol Catherine E. Cooke, PharmD, BCPS, PAHM President, PosiHealth, Inc. Clinical Associate Professor, Univ. of Maryland This program has been brought to you by PharmCon
CVD risk assessment using risk scores in primary and secondary prevention
 CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
PCSK9 Agents Drug Class Prior Authorization Protocol
 PCSK9 Agents Drug Class Prior Authorization Protocol Line of Business: Medicaid P & T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review of medical
PCSK9 Agents Drug Class Prior Authorization Protocol Line of Business: Medicaid P & T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review of medical
Management of Post-transplant hyperlipidemia
 Management of Post-transplant hyperlipidemia B. Gisella Carranza Leon, MD Assistant Professor of Medicine Lipid Clinic - Vanderbilt Heart and Vascular Institute Division of Diabetes, Endocrinology and
Management of Post-transplant hyperlipidemia B. Gisella Carranza Leon, MD Assistant Professor of Medicine Lipid Clinic - Vanderbilt Heart and Vascular Institute Division of Diabetes, Endocrinology and
LLL Session - Nutrition support in diabetes and dyslipidemia. Dyslipidemia: targeting the management of cardiovascular risk factors. M.
 ESPEN Congress Leipzig 2013 LLL Session - Nutrition support in diabetes and dyslipidemia Dyslipidemia: targeting the management of cardiovascular risk factors M. Leon Sanz (ES) Dyslipidemia: Targeting
ESPEN Congress Leipzig 2013 LLL Session - Nutrition support in diabetes and dyslipidemia Dyslipidemia: targeting the management of cardiovascular risk factors M. Leon Sanz (ES) Dyslipidemia: Targeting
Lipids & Hypertension Update
 Lipids & Hypertension Update No financial disclosures Michael W. Cullen, MD, FACC Senior Associate Consultant, Assistant Professor of Medicine Mayo Clinic Department of Cardiovascular Diseases 34 th Annual
Lipids & Hypertension Update No financial disclosures Michael W. Cullen, MD, FACC Senior Associate Consultant, Assistant Professor of Medicine Mayo Clinic Department of Cardiovascular Diseases 34 th Annual
Reducing Cardiovascular Risk Through Non-Statins. Kim K. Birtcher, PharmD Joseph Saseen, PharmD
 Reducing Cardiovascular Risk Through Non-Statins Kim K. Birtcher, PharmD Joseph Saseen, PharmD Target Audience: Pharmacists ACPE#: 0202-0000-18-049-L01-P Activity Type: Application-based This activity
Reducing Cardiovascular Risk Through Non-Statins Kim K. Birtcher, PharmD Joseph Saseen, PharmD Target Audience: Pharmacists ACPE#: 0202-0000-18-049-L01-P Activity Type: Application-based This activity
Treating dyslipidemia
 Treating dyslipidemia in patients with type 2 diabetes mellitus 18 The Nurse Practitioner Vol. 40, No. 18 www.tnpj.com 2.0 CONTACT HOURS 1.0 CONTACT HOURS Abstract: Type 2 diabetes mellitus is associated
Treating dyslipidemia in patients with type 2 diabetes mellitus 18 The Nurse Practitioner Vol. 40, No. 18 www.tnpj.com 2.0 CONTACT HOURS 1.0 CONTACT HOURS Abstract: Type 2 diabetes mellitus is associated
Lipid Management C. Samuel Ledford, MD Interventional Cardiology Chattanooga Heart Institute
 Lipid Management 2018 C. Samuel Ledford, MD Interventional Cardiology Chattanooga Heart Institute Disclosures No Financial Disclosures Disclosures I am an Interventional Cardiologist I put STENTS in for
Lipid Management 2018 C. Samuel Ledford, MD Interventional Cardiology Chattanooga Heart Institute Disclosures No Financial Disclosures Disclosures I am an Interventional Cardiologist I put STENTS in for
Diabetes and the Heart
 Diabetes and the Heart Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 6, 2012 Outline Screening for diabetes in patients with CAD Screening for CAD in patients with
Diabetes and the Heart Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 6, 2012 Outline Screening for diabetes in patients with CAD Screening for CAD in patients with