PL CE LIVE July 2015 Forum
|
|
|
- Estella Haynes
- 5 years ago
- Views:
Transcription
 as a provider of continuing pharmacy education.")
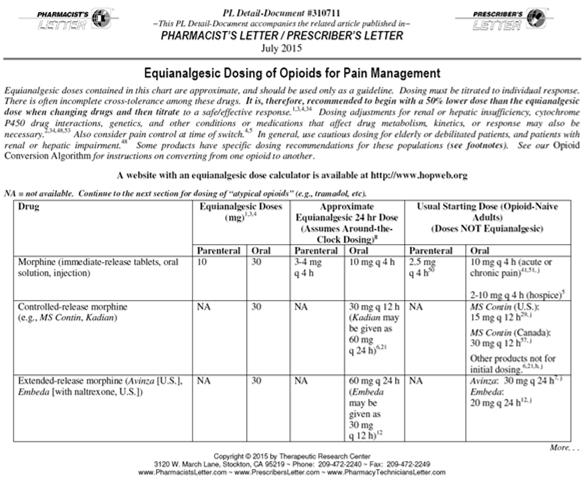
1 July 2015 PL CE LIVE Rachel Maynard, PharmD Associate Editor Pharmacist s Letter/Pharmacy Technician s Letter CE Information Pharmacist's Letter / Therapeutic Research Center is accredited by the Accreditation Council for Pharmacy Education (ACPE) as a provider of continuing pharmacy education. PL CE LIVE editors disclose: No financial interests related to the content No commercial support and no advertising Supported entirely by subscriptions PL CE LIVE Drug Information Consultant discloses: Dr. O Mara reports that her spouse is employed by Celgene. Pharmacist Objectives Identify emerging trends in drug therapy and their place in patient care practices. List two appropriate uses of atypical antipsychotics. Describe when non statins may be considered for dyslipidemia. Compare extended release carbidopa/levodopa (Rytary)to other formulations. Explain three strategies for safe use of fentanyl patches. Pharmacy Technician Objectives Identify emerging trends in drug therapy and their place in pharmacy practice and operations. List two appropriate uses of atypical antipsychotics. Describe when non statins may be considered for dyslipidemia. Compare extended release carbidopa/levodopa (Rytary) to other formulations. Explain three strategies for safe use of fentanyl patches. Inappropriate Use of Atypical Antipsychotics 1
 $7.")



2 Sovaldi (sofosbuvir) $7.9 billion Abilify (aripiprazole) $7.8 billion Humira (adalimumab) $7.2 billion Aripiprazole Generics Not as prone to weight gain and sedation as olanzapine or quetiapine But there are still concerns: Restlessness, risk of tardive dyskinesia, interactions, etc Generics won t provide immediate cost savings Efficacy Adverse Effects Varies by drug/condition Weight gain Metabolic effects (glucose, lipids, etc) Sedation QT prolongation Drug interactions Hyperprolactinemia Extrapyramidal side effects Tardive dyskinesia Depression Behavioral problems in children Insomnia Dementia 2
3 Use of Atypicals: Depression Suggest saving atypicals for patients with treatment resistant depression Those who don t respond well to: At least 2 different optimized antidepressants Combined antidepressant therapy Use of Atypicals: Depression Atypicals may be tried as augmenting agents One more patient in 9 will respond when an atypical is added to antidepressant therapy If needed, suggest a low dose of: Aripiprazole Quetiapine Olanzapine Use of Atypicals: Behavioral Problems Suggest saving atypicals for children with: Psychosis Severe aggressive or disruptive behaviors If needed, suggest aripiprazole or risperidone for severely impaired children with autism Use of Atypicals: Insomnia Discourage use of atypicals No evidence quetiapine or others improve sleep duration Recommend other options instead Sleep hygiene Treating underlying causes Zolpidem, trazodone, etc Use of Atypicals: Dementia Discourage use of atypicals One more death for every dementia patients treated with an atypical for 8 12 weeks BOXED WARNING Increased mortality in elderly patients with dementia related psychosis: Use of Atypicals: Dementia Recommend non drug measures and evaluate underlying causes first Recommend atypicals only for dementia patients: With disabling delusions, hallucinations, agitation Who pose danger to themselves or others Elderly patients with dementia related psychosis treated with antipsychotic drugs are at an increased risk of death. 3



4 Use of Atypicals: Dementia If needed, suggest ¼ to ½ the usual starting dose of: Risperidone Olanzapine Aripiprazole Quetiapine Reevaluate need every 3 6 months Suggest tapering if possible Practice Pearls In most cases, help optimize other drugs with better evidence and fewer side effects first Consider drug, dose, duration Recommend monitoring weight, blood glucose, and lipids Suggest using lowest effective dose of an atypical Role of Non-Statins for Dyslipidemia 4

5 Bile acid sequestrants Non statins Ezetimibe Fibrates LDL Goals Specific Statin Doses Proven to Benefit Niacin Omega 3 fatty acids Adding a non statin to a statin hasn t been proven to further reduce CV mortality Adding a non statin could lead to a suboptimal statin dose being used Suggest saving non-statins for special situations... and stopping them when there s no good reason to continue. 5
6 Evaluate Statin Use Emphasize adherence to lifestyle changes and evidence based statin dose first Assess statin tolerance Encourage patients to take stock of any muscle symptoms before starting the statin Look for potential interactions Especially with simvastatin, lovastatin, atorvastatin Consider a lower dose, different statin, etc Role of Non-Statins Add on therapy Monotherapy Bile acid sequestrants Advise saving nonstatin add ons for patients with a prior cardiovascular event Who can t tolerate a highintensity statin (atorvastatin 80 mg, etc) Who don t get expected % LDL lowering from a statin Non statins Ezetimibe Fibrates Niacin Omega 3 fatty acids Which Non-Statins to Consider as Add- On Therapy? No good evidence of improved CV outcomes when adding on: Bile acid sequestrants, fibrates, niacin, omega 3s Suggest ezetimibe if a non statin add on is needed Only non statin shown to improve CV outcomes when added to a statin Which Non-Statins to Consider as Add- On Therapy? Role of ezetimibe IMPROVE IT trial Modest benefit in specific high risk patients One less CV event for every 50 ACS patients on ezetimibe + simvastatin 40 mg x 7 years compared to simvastatin alone Did not reduce mortality No evidence of improved CV outcomes when Added to a statin in lower risk patients Used alone 6

7 Role of Non-Statins Add on therapy Monotherapy Suggest saving nonstatin monotherapy for certain patients High CV risk and can t use a statin Very high triglycerides Which Non-Statins to Consider as Monotherapy? For high cardiovascular risk, suggest meds that seem to reduce CV events when used alone: Bile acid sequestrant Gemfibrozil Niacin Which Non-Statins to Consider as Monotherapy? Bile acid sequestrants (cholestyramine, etc) For high LDL Gemfibrozil High triglycerides and low HDL Niacin Caution about hyperglycemia, muscle pain, liver toxicity, flushing, etc Which Non-Statins to Consider as Monotherapy? For very high triglycerides: Emphasize lifestyle changes Help optimize blood glucose control Recommend a statin first in most patients Suggest saving omega 3 fatty acids or fibrates if triglycerides 500 mg/dl or approaching 1000 mg/dl No proof using these meds to triglycerides improves CV outcomes 7







 Rotigotine (Neupro) MAO B")
 Anticholinergics")
 Amantadine COMT inhibitors")

8 Parkinson s Disease Background: Parkinson s Disease Progressive neurologic disease affecting movement Occurs due to: Lack of dopamine due to loss of nerve cells in certain areas of the brain Characterized by: Tremor, rigidity, bradykinesia, postural instability Carbidopa/ levodopa Dopamine agonists Other options Immediate release (Sinemet, etc) Sustained release (Sinemet CR, etc) Extended release (Rytary) Pramipexole (Mirapex, Mirapex ER, etc) Ropinirole (Requip, Requip XL, etc) Rotigotine (Neupro) MAO B inhibitors (selegiline, rasagiline, etc) Anticholinergics (benztropine, trihexyphenidyl, etc) Amantadine COMT inhibitors (entacapone, tolcapone, etc) Disease progression Drug efficacy Control of Parkinson s symptoms Dopaminerelated side effects 8

9 Carbidopa/Levodopa Most effective drug for Parkinson s symptoms First line, especially in elderly patients Long term use associated with: Dyskinesias Motor fluctuations on off, wearing off Side effects Nausea, orthostatic hypotension, confusion, etc Carbidopa/Levodopa Immediate or controlled release can be used Start low, go slow with dosing Suggest titrating to lowest effective dose After the honeymoon is over... After the Honeymoon To reduce off time : Suggest levodopa dosing interval by minutes Point out sustained release (Sinemet CR, etc) does not reduce off time better than immediate release Probably because it takes ~2 hours for CR to kick in Some patients may take both IR + CR Other options: Adding a dopamine agonist, COMT inhibitor, or MAO B inhibitor Carbidopa/Levodopa Extended-Release (Rytary) Similar onset to immediate release Starts to work within an hour, faster than CR Similar duration to sustained release Lasts about 6 hours, longer than IR Reduces off time by ~70 minutes/day compared to IR Too soon to say how it compares to CR 9
 Explain a higher dose will be needed Rytary has")
 Advise swallowing capsule whole May also be sprinkled onto applesauce Watch for product mix ups Rytary is available in 4")
10 Carbidopa/Levodopa Extended-Release (Rytary) Suggest saving Rytary for advanced Parkinson s Consider it an alternative for patients: Taking both the IR + CR forms Who still have off time despite taking other carbidopa/levodopa forms 4 times daily Costs ~$700/month Compared to ~$200/month for generics Carbidopa/Levodopa Extended-Release (Rytary) Explain a higher dose will be needed Rytary has lower bioavailability than IR or CR Dyskinesiasmay worsen during a switch Ensure patients can handle high pill burden Usual dosage: 3 4 caps TID Check that other carbidopa/levodopa forms are stopped when Rytary is started Carbidopa/Levodopa Extended-Release (Rytary) Advise swallowing capsule whole May also be sprinkled onto applesauce Watch for product mix ups Rytary is available in 4 carbidopa/levodopa strengths mg/95 mg mg/145 mg mg/195 mg mg/245 mg Safe Use of Fentanyl Patches 10
11 Fentanyl Patches Fentanyl Patches *Note: products designated as 12 deliver dose of 12.5 *Note: products designated as 12 deliver dose of 12.5 Ensuring Safe Use of Fentanyl Patches Ensure fentanyl patches are used only in opioid tolerant patients with chronic pain In general, patients on oral morphine 60 mg/day or equivalent for 1 week Watch for use in acute, post op, or mild pain Ensuring Safe Use of Fentanyl Patches Be alert for patients with respiratory problems Watch for drug interactions with CYP3A4 CYP3A4 inhibitors may increase or prolong effects of fentanyl and could lead to respiratory depression Ketoconazole, clarithromycin, diltiazem, grapefruit juice, nefazodone, etc Ensuring Safe Use of Fentanyl Patches Continue to recommend starting with usual standard doses Recommend individualizing based on patient factors and clinical judgment Age, renal/liver function, interactions, etc Daily Dose of Oral Morphine Starting Fentanyl Patch Dose mg mg mg mg 100 Ensuring Safe Use of Fentanyl Patches When switching from fentanyl patch another opioid Do not use same conversion May overestimate new opioid dose 11

12 Intermediate Strength Fentanyl Patches Fentanyl Patches Suggest saving the intermediate strengths Consider if smaller steps needed during dose adjustments Consider to avoid using multiple patches *Note: products designated as 12 deliver dose of 12.5 Intermediate Strength Fentanyl Patches Intermediate strength patches may be more expensive than standard doses 25 $100/month 37.5 $450/month 50 $150/month Point out that using one patch is preferred to multiple patches to reduce risk of errors Ensuring Safe Use of Fentanyl Patches Avoid dispensing mishaps Select strengths carefully and closely look at Rxs 87.5 patch could be confused with 37.5 Watch decimal points What do you tell patients? Practice Pearls Remind patients to remove the old patch before applying a new one Fentanyl can still be absorbed from old patch Help patients set up a dosing calendar Advise avoiding heating pads, electric blankets, hot tubs, etc Heat can fentanyl absorp on Tell patients never to cut fentanyl patches 12

13 Practice Pearls Proper storage Keep out of reach of children auxiliary label Advise storing unused patches in a secure location away from children or pets Proper disposal Fold sticky sides of patch together and flush down toilet Remind patients not to dispose of fentanyl patches in household trash Practice Pearls Caution about use with other CNS depressants Educate patients and caregivers of signs of fentanyl overdose Shallow/slow breathing, extreme sleepiness, unresponsive, etc Dispense with a MedGuide Flozins and Ketoacidosis 13
14 SGLT2 Inhibitors and Ketoacidosis Risk of ketoacidosis seems to be a class effect Canagliflozin (Invokana, etc) Dapagliflozin (Farxiga, etc) Empagliflozin (Jardiance, etc) SGLT2 Inhibitors and Ketoacidosis Diabetic ketoacidosis usually occurs: When insulin levels are too low During prolonged fasting In patients with type 1 diabetes With very high blood glucose levels Ketoacidosis with SGLT2 inhibitors is different Seen in type 1 or 2 diabetes Glucose levels near normal or only slightly elevated SGLT2 Inhibitors and Ketoacidosis Watch for high risk patients Recent in insulin dose, acute illness, dehydration, renal impairment, reduced food/fluid intake Symptoms often occur within 2 weeks after starting the flozin But can happen at any time Bottom Line Tell patients to stop the flozin and seek medical help for symptoms of ketoacidosis: Difficulty breathing, nausea, vomiting, abdominal pain, confusion, unusual fatigue, etc Be aware ketoacidosis may occur even if blood glucose is not very high Continue to warn about other flozin side effects Yeast infections, UTIs, hypotension, etc Practice Pearls Continue to weigh pros and cons of flozins as a metformin add on for type 2 diabetes Caution about using flozins in renal impairment Moderate renal impairment: avoid dapagliflozin Severe renal impairment: avoid all flozins Report adverse effects of SGLT2 inhibitors to the FDA MedWatch program Polls/Questions 14
Best Medical Treatments for Parkinson s disease
 Best Medical Treatments for Parkinson s disease Bernadette Schöneburg, M.D. June 20 th, 2015 What is Parkinson s Disease (PD)? Progressive neurologic disorder that results from the loss of specific cells
Best Medical Treatments for Parkinson s disease Bernadette Schöneburg, M.D. June 20 th, 2015 What is Parkinson s Disease (PD)? Progressive neurologic disorder that results from the loss of specific cells
Medications used to treat Parkinson s disease
 Medications used to treat Parkinson s disease Edwin B. George, M.D., Ph.D. Director of Wayne State University Movement Disorder Clinic University Health Center Neurology Clinic University Health The John
Medications used to treat Parkinson s disease Edwin B. George, M.D., Ph.D. Director of Wayne State University Movement Disorder Clinic University Health Center Neurology Clinic University Health The John
What s new for diagnosing and treating Parkinson s Disease?
 What s new for diagnosing and treating Parkinson s Disease? Erika Driver-Dunckley, MD Associate Professor of Neurology Program Director Movement Disorders Fellowship Assistant Program Director Neurology
What s new for diagnosing and treating Parkinson s Disease? Erika Driver-Dunckley, MD Associate Professor of Neurology Program Director Movement Disorders Fellowship Assistant Program Director Neurology
parts of the gastrointenstinal tract. At the end of April 2008, it was temporarily withdrawn from the US Market because of problems related to
 parts of the gastrointenstinal tract. At the end of April 2008, it was temporarily withdrawn from the US Market because of problems related to crystallization of the drug, which caused unreliable drug
parts of the gastrointenstinal tract. At the end of April 2008, it was temporarily withdrawn from the US Market because of problems related to crystallization of the drug, which caused unreliable drug
Motor Fluctuations Stephen Grill, MD, PHD Parkinson s and Movement Disorders Center of Maryland and Johns Hopkins University
 Motor Fluctuations Stephen Grill, MD, PHD Parkinson s and Movement Disorders Center of Maryland and Johns Hopkins University I have no financial interest with any entity producing marketing, re-selling,
Motor Fluctuations Stephen Grill, MD, PHD Parkinson s and Movement Disorders Center of Maryland and Johns Hopkins University I have no financial interest with any entity producing marketing, re-selling,
Optimizing Clinical Communication in Parkinson s Disease:
 Optimizing Clinical Communication in Parkinson s Disease:,Strategies for improving communication between you and your neurologist PFNCA Symposium March 25, 2017 Pritha Ghosh, MD Assistant Professor of
Optimizing Clinical Communication in Parkinson s Disease:,Strategies for improving communication between you and your neurologist PFNCA Symposium March 25, 2017 Pritha Ghosh, MD Assistant Professor of
Treatment of Parkinson s Disease: Present and Future
 Treatment of Parkinson s Disease: Present and Future Karen Blindauer, MD Professor of Neurology Director of Movement Disorders Program Medical College of Wisconsin Neuropathology: Loss of Dopamine- Producing
Treatment of Parkinson s Disease: Present and Future Karen Blindauer, MD Professor of Neurology Director of Movement Disorders Program Medical College of Wisconsin Neuropathology: Loss of Dopamine- Producing
Parkinson s Disease Current Treatment Options
 Parkinson s Disease Current Treatment Options Daniel Kassicieh, D.O., FAAN Sarasota Neurology, P.A. PD: A Chronic Neurodegenerative Ds. 1 Million in USA Epidemiology 50,000 New Cases per Year Majority
Parkinson s Disease Current Treatment Options Daniel Kassicieh, D.O., FAAN Sarasota Neurology, P.A. PD: A Chronic Neurodegenerative Ds. 1 Million in USA Epidemiology 50,000 New Cases per Year Majority
Parkinson s Disease WHERE HAVE WE BEEN, WHERE ARE WE HEADING? CHARLECE HUGHES D.O.
 Parkinson s Disease WHERE HAVE WE BEEN, WHERE ARE WE HEADING? CHARLECE HUGHES D.O. Parkinson s Epidemiology AFFECTS 1% OF POPULATION OVER 65 MEAN AGE OF ONSET 65 MEN:WOMEN 1.5:1 IDIOPATHIC:HEREDITARY 90:10
Parkinson s Disease WHERE HAVE WE BEEN, WHERE ARE WE HEADING? CHARLECE HUGHES D.O. Parkinson s Epidemiology AFFECTS 1% OF POPULATION OVER 65 MEAN AGE OF ONSET 65 MEN:WOMEN 1.5:1 IDIOPATHIC:HEREDITARY 90:10
Scott J Sherman MD, PhD The University of Arizona PARKINSON DISEASE
 Scott J Sherman MD, PhD The University of Arizona PARKINSON DISEASE LEARNING OBJECTIVES The Course Participant will: 1. Be familiar with the pathogenesis of Parkinson s Disease (PD) 2. Understand clinical
Scott J Sherman MD, PhD The University of Arizona PARKINSON DISEASE LEARNING OBJECTIVES The Course Participant will: 1. Be familiar with the pathogenesis of Parkinson s Disease (PD) 2. Understand clinical
10th Medicine Review Course st July Prakash Kumar
 10th Medicine Review Course 2018 21 st July 2018 Drug Therapy for Parkinson's disease Prakash Kumar National Neuroscience Institute Singapore General Hospital Sengkang General Hospital Singhealth Duke-NUS
10th Medicine Review Course 2018 21 st July 2018 Drug Therapy for Parkinson's disease Prakash Kumar National Neuroscience Institute Singapore General Hospital Sengkang General Hospital Singhealth Duke-NUS
PL CE LIVE April 2012 Forum
 April 2012 PL CE LIVE Rachel Maynard, Pharm.D. Assistant Editor Pharmacist s Letter/Pharmacy Technician s Letter Sherri Boehringer, Pharm.D., BCPS Associate Editor Pharmacist s Letter/Pharmacy Technician
April 2012 PL CE LIVE Rachel Maynard, Pharm.D. Assistant Editor Pharmacist s Letter/Pharmacy Technician s Letter Sherri Boehringer, Pharm.D., BCPS Associate Editor Pharmacist s Letter/Pharmacy Technician
Drugs for Parkinson s Disease
 This Clinical Resource gives subscribers additional insight related to the Recommendations published in July 2017 ~ Resource #330705 Drugs for Parkinson s Disease Parkinson s disease is characterized by
This Clinical Resource gives subscribers additional insight related to the Recommendations published in July 2017 ~ Resource #330705 Drugs for Parkinson s Disease Parkinson s disease is characterized by
Cardinal Features of Parkinson s. Management of Parkinson s Disease. Drug Induced Parkinson s. Other Parkinson s Symptoms.
 Cardinal Features of Parkinson s Management of Parkinson s Disease Kristin S. Meyer, PharmD, CGP, FASHP Assistant Professor of Pharmacy Practice Drake University & Iowa Veterans Home Spring 2009 Tremor
Cardinal Features of Parkinson s Management of Parkinson s Disease Kristin S. Meyer, PharmD, CGP, FASHP Assistant Professor of Pharmacy Practice Drake University & Iowa Veterans Home Spring 2009 Tremor
Parkinson s Disease. Gillian Sare
 Parkinson s Disease Gillian Sare Outline Reminder about PD Parkinson s disease in the inpatient Surgical patients with PD Patients who cannot swallow End of life care Parkinson s disease PD is the second
Parkinson s Disease Gillian Sare Outline Reminder about PD Parkinson s disease in the inpatient Surgical patients with PD Patients who cannot swallow End of life care Parkinson s disease PD is the second
PD: Key Treatment Considerations
 PD: Key Treatment Considerations 2018 Management of Neurologic and Neurosurgical Disorders in Daily Practice Elise Anderson MD Medical Co-Director, PBSI Movement Disorders 11/27/2018 1 Outline Treatment
PD: Key Treatment Considerations 2018 Management of Neurologic and Neurosurgical Disorders in Daily Practice Elise Anderson MD Medical Co-Director, PBSI Movement Disorders 11/27/2018 1 Outline Treatment
Pharmacologic Treatment of Parkinson s Disease. Nicholas J. Silvestri, M.D. Assistant Professor of Neurology
 + Pharmacologic Treatment of Parkinson s Disease Nicholas J. Silvestri, M.D. Assistant Professor of Neurology + Overview n Brief review of Parkinson s disease (PD) n Clinical manifestations n Pathophysiology
+ Pharmacologic Treatment of Parkinson s Disease Nicholas J. Silvestri, M.D. Assistant Professor of Neurology + Overview n Brief review of Parkinson s disease (PD) n Clinical manifestations n Pathophysiology
Program Highlights. Michael Pourfar, MD Co-Director, Center for Neuromodulation New York University Langone Medical Center New York, New York
 Program Highlights David Swope, MD Associate Professor of Neurology Mount Sinai Health System New York, New York Michael Pourfar, MD Co-Director, Center for Neuromodulation New York University Langone
Program Highlights David Swope, MD Associate Professor of Neurology Mount Sinai Health System New York, New York Michael Pourfar, MD Co-Director, Center for Neuromodulation New York University Langone
Pharmacologic Treatment of Parkinson s Disease. Nicholas J. Silvestri, M.D. Associate Professor of Neurology
 + Pharmacologic Treatment of Parkinson s Disease Nicholas J. Silvestri, M.D. Associate Professor of Neurology + Disclosures n NO SIGNIFICANT FINANCIAL, GENERAL, OR OBLIGATION INTERESTS TO REPORT + Learning
+ Pharmacologic Treatment of Parkinson s Disease Nicholas J. Silvestri, M.D. Associate Professor of Neurology + Disclosures n NO SIGNIFICANT FINANCIAL, GENERAL, OR OBLIGATION INTERESTS TO REPORT + Learning
Parkinson s Disease Medications: Professionals Edition
 Parkinson s Disease Clinic and Research Center University of California, San Francisco 505 Parnassus Ave., Rm. 795-M, Box 0114 San Francisco, CA 94143-0114 (415) 476-9276 http://pdcenter.neurology.ucsf.edu
Parkinson s Disease Clinic and Research Center University of California, San Francisco 505 Parnassus Ave., Rm. 795-M, Box 0114 San Francisco, CA 94143-0114 (415) 476-9276 http://pdcenter.neurology.ucsf.edu
Drug Therapy of Parkinsonism. Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia
 Drug Therapy of Parkinsonism Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Parkinsonism is a progressive neurological disorder of muscle movement, usually
Drug Therapy of Parkinsonism Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Parkinsonism is a progressive neurological disorder of muscle movement, usually
Medication Management & Strategies When the levodopa honeymoon is over
 Medication Management & Strategies When the levodopa honeymoon is over Eric J Pappert, MD Parkinson s Disease & Movement Disorders Center Neurology Associates Medication Options in Parkinson s Carbidopa/Levodopa
Medication Management & Strategies When the levodopa honeymoon is over Eric J Pappert, MD Parkinson s Disease & Movement Disorders Center Neurology Associates Medication Options in Parkinson s Carbidopa/Levodopa
Evaluation and Management of Parkinson s Disease in the Older Patient
 Evaluation and Management of Parkinson s Disease in the Older Patient David A. Hinkle, MD, PhD Comprehensive Movement Disorders Clinic Pittsburgh Institute for Neurodegenerative Diseases University of
Evaluation and Management of Parkinson s Disease in the Older Patient David A. Hinkle, MD, PhD Comprehensive Movement Disorders Clinic Pittsburgh Institute for Neurodegenerative Diseases University of
Pharmacy Coverage Guidelines are subject to change as new information becomes available.
 ZELAPAR (selegiline hydrochloride) orally disintegrating tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific
ZELAPAR (selegiline hydrochloride) orally disintegrating tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific
Anticholinergics. COMT* Inhibitors. Dopaminergic Agents. Dopamine Agonists. Combination Product
 Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-945-5220 Fax 503-947-1119 Class Update: Parkinson s Drugs Month/Year of Review:
Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-945-5220 Fax 503-947-1119 Class Update: Parkinson s Drugs Month/Year of Review:
BLONANSERIN. THERAPEUTICS Brands Lonasen see index for additional brand names
 BLONANSERIN THERAPEUTICS Brands Lonasen see index for additional brand names Generic? No Class Atypical antipsychotic (serotonin dopamine antagonist; second-generation antipsychotic; also a potential mood
BLONANSERIN THERAPEUTICS Brands Lonasen see index for additional brand names Generic? No Class Atypical antipsychotic (serotonin dopamine antagonist; second-generation antipsychotic; also a potential mood
Advanced Therapies for Motor Symptoms in PD. Matthew Boyce MD
 Advanced Therapies for Motor Symptoms in PD Matthew Boyce MD Medtronic Education Teva Speakers Bureau Acadia Speakers Bureau Disclosures Discuss issues in advanced PD Adjunct therapies to levo-dopa Newer
Advanced Therapies for Motor Symptoms in PD Matthew Boyce MD Medtronic Education Teva Speakers Bureau Acadia Speakers Bureau Disclosures Discuss issues in advanced PD Adjunct therapies to levo-dopa Newer
The Role of Pharmacists in Treating & Managing Parkinson s Disease Author: Mary Jo Carden, RPh, JD Principal, Carden Associates
 The Role of Pharmacists in Treating & Managing Parkinson s Disease Author: Mary Jo Carden, RPh, JD Principal, Carden Associates Editor: Marsha K. Millonig, MBA, RPh President/CEO Catalyst Enterprises,
The Role of Pharmacists in Treating & Managing Parkinson s Disease Author: Mary Jo Carden, RPh, JD Principal, Carden Associates Editor: Marsha K. Millonig, MBA, RPh President/CEO Catalyst Enterprises,
The symptoms of the Parkinson s disease may vary from person to person. The symptoms might include the following:
 1 PARKINSON S DISEASE Parkinson's disease is a long term disease related to the central nervous system that mainly affects the motor system, resulting in the loss of dopamine, which helps in producing
1 PARKINSON S DISEASE Parkinson's disease is a long term disease related to the central nervous system that mainly affects the motor system, resulting in the loss of dopamine, which helps in producing
Prior Authorization with Quantity Limit Program Summary
 Gocovri (amantadine) Prior Authorization with Quantity Limit Program Summary This prior authorization applies to Commercial, NetResults A series, SourceRx and Health Insurance Marketplace formularies.
Gocovri (amantadine) Prior Authorization with Quantity Limit Program Summary This prior authorization applies to Commercial, NetResults A series, SourceRx and Health Insurance Marketplace formularies.
THIOTHIXENE. THERAPEUTICS Brands Navane see index for additional brand names. Generic? Yes
 THIOTHIXENE THERAPEUTICS Brands Navane see index for additional brand names Generic? Yes Class Conventional antipsychotic (neuroleptic, thioxanthene, dopamine 2 antagonist) Commonly Prescribed for (bold
THIOTHIXENE THERAPEUTICS Brands Navane see index for additional brand names Generic? Yes Class Conventional antipsychotic (neuroleptic, thioxanthene, dopamine 2 antagonist) Commonly Prescribed for (bold
PARKINSON S MEDICATION
 PARKINSON S MEDICATION History 1940 50 s Neurosurgeons operated on basal ganglia. Improved symptoms. 12% mortality 1960 s: Researchers identified low levels of dopamine caused Parkinson s leading to development
PARKINSON S MEDICATION History 1940 50 s Neurosurgeons operated on basal ganglia. Improved symptoms. 12% mortality 1960 s: Researchers identified low levels of dopamine caused Parkinson s leading to development
Communicating About OFF Episodes With Your Doctor
 Communicating About OFF Episodes With Your Doctor Early in Parkinson s disease (PD), treatment with levodopa and other anti-pd drugs provides continuous benefit. As the disease progresses, however, symptom
Communicating About OFF Episodes With Your Doctor Early in Parkinson s disease (PD), treatment with levodopa and other anti-pd drugs provides continuous benefit. As the disease progresses, however, symptom
LURASIDONE. THERAPEUTICS Brands LATUDA see index for additional brand names
 LURASIDONE THERAPEUTICS Brands LATUDA see index for additional brand names Generic? No Class Neuroscience-based Nomenclature: dopamine, serotonin receptor antagonist (DS-RAn) Atypical antipsychotic (serotonin-dopamine
LURASIDONE THERAPEUTICS Brands LATUDA see index for additional brand names Generic? No Class Neuroscience-based Nomenclature: dopamine, serotonin receptor antagonist (DS-RAn) Atypical antipsychotic (serotonin-dopamine
PL CE LIVE February 2011 Forum
 February 2011 PL CE LIVE Kristin W. Weitzel, Pharm.D., CDE, FAPhA Associate Editor and Director of Editorial Projects Pharmacist s Letter/Prescriber s Letter Atypical Antipsychotics Atypical Antipsychotics
February 2011 PL CE LIVE Kristin W. Weitzel, Pharm.D., CDE, FAPhA Associate Editor and Director of Editorial Projects Pharmacist s Letter/Prescriber s Letter Atypical Antipsychotics Atypical Antipsychotics
Parkinson s Disease Update. Presented by Joanna O Leary, MD Movement disorder neurologist Providence St. Vincent s
 Parkinson s Disease Update Presented by Joanna O Leary, MD Movement disorder neurologist Providence St. Vincent s What is a movement disorder? Neurological disorders that affect ability to move by causing
Parkinson s Disease Update Presented by Joanna O Leary, MD Movement disorder neurologist Providence St. Vincent s What is a movement disorder? Neurological disorders that affect ability to move by causing
Key Concepts and Issues in Parkinson s Disease in 2016
 Key Concepts and Issues in Parkinson s Disease in 2016 Michael Rezak, M.D., Ph.D. Section Chief, Neurosciences Institute Director, Movement Disorders and Neurodegenerative Diseases Center Northwestern
Key Concepts and Issues in Parkinson s Disease in 2016 Michael Rezak, M.D., Ph.D. Section Chief, Neurosciences Institute Director, Movement Disorders and Neurodegenerative Diseases Center Northwestern
Antipsychotic Use in the Elderly
 Antipsychotic Use in the Elderly Presented by: Fatima M. Ali, PharmD, RPh, BCPS Clinical Consultant Pharmacist MediSystem Pharmacy, Kingston Originally Prepared by: Nicole Tisi BScPhm, RPh ACPR Disclosure
Antipsychotic Use in the Elderly Presented by: Fatima M. Ali, PharmD, RPh, BCPS Clinical Consultant Pharmacist MediSystem Pharmacy, Kingston Originally Prepared by: Nicole Tisi BScPhm, RPh ACPR Disclosure
Drugs used in Parkinsonism
 Drugs used in Parkinsonism قادة فريق علم األدوية : لي التميمي & عبدالرحمن ذكري الشكر موصول ألعضاء الفريق املتميزين : جومانة القحطاني ندى الصومالي روان سعد القحطاني pharma436@outlook.com @pharma436 Your
Drugs used in Parkinsonism قادة فريق علم األدوية : لي التميمي & عبدالرحمن ذكري الشكر موصول ألعضاء الفريق املتميزين : جومانة القحطاني ندى الصومالي روان سعد القحطاني pharma436@outlook.com @pharma436 Your
What is Parkinson s Disease?
 2018 Update in Parkinson s Disease: Treatments and Future Plans Arita McCoy, MSN, CRNP Johns Hopkins Parkinson s Disease and Movement Disorder Center A National Parkinson Foundation Center of Excellence
2018 Update in Parkinson s Disease: Treatments and Future Plans Arita McCoy, MSN, CRNP Johns Hopkins Parkinson s Disease and Movement Disorder Center A National Parkinson Foundation Center of Excellence
ASENAPINE. THERAPEUTICS Brands SAPHRIS see index for additional brand names
 ASENAPINE THERAPEUTICS Brands SAPHRIS see index for additional brand names Generic? No Class Neuroscience-based Nomenclature: dopamine, serotonin, norepinephrine receptor antagonist (DSN-RAn) Atypical
ASENAPINE THERAPEUTICS Brands SAPHRIS see index for additional brand names Generic? No Class Neuroscience-based Nomenclature: dopamine, serotonin, norepinephrine receptor antagonist (DSN-RAn) Atypical
Dosing & Administration
 Dosing & Administration REAL LIFE. REAL RESULTS. INDICATION INVEGA SUSTENNA (paliperidone palmitate) is indicated for the treatment of: Schizophrenia. Schizoaffective disorder as monotherapy and as an
Dosing & Administration REAL LIFE. REAL RESULTS. INDICATION INVEGA SUSTENNA (paliperidone palmitate) is indicated for the treatment of: Schizophrenia. Schizoaffective disorder as monotherapy and as an
WHAT DEFINES YOPD? HANDLING UNIQUE CONCERNS REBECCA GILBERT, MD, PHD VICE PRESIDENT, CHIEF SCIENTIFIC OFFICER, APDA MARCH 14, 2019
 WHAT DEFINES YOPD? HANDLING UNIQUE CONCERNS REBECCA GILBERT, MD, PHD VICE PRESIDENT, CHIEF SCIENTIFIC OFFICER, APDA MARCH 14, 2019 YOUNG ONSET PARKINSON S DISEASE Definition: Parkinson s disease diagnosed
WHAT DEFINES YOPD? HANDLING UNIQUE CONCERNS REBECCA GILBERT, MD, PHD VICE PRESIDENT, CHIEF SCIENTIFIC OFFICER, APDA MARCH 14, 2019 YOUNG ONSET PARKINSON S DISEASE Definition: Parkinson s disease diagnosed
Abilify (aripiprazole)
") Abilify (aripiprazole) FDA ALERT [04/2005] Abilify is a type of medicine called an atypical antipsychotic. FDA has found that older patients treated with atypical antipsychotics for dementia had a higher
Abilify (aripiprazole) FDA ALERT [04/2005] Abilify is a type of medicine called an atypical antipsychotic. FDA has found that older patients treated with atypical antipsychotics for dementia had a higher
Non-Statin Lipid-Lowering Agents M Holler - Last updated: 10/2016
 Drug/Class Cholestyramine (Questran) Bile acid sequestrant Generic? Lipid Effects Y/N (monotherapy) Y LDL : 9% (4 g to 8 ; 21% (16 g to 20 ; 23% to 28% (>20 HDL : 4% to 8% (16 to 24 TG : 11% to 28% (4
Drug/Class Cholestyramine (Questran) Bile acid sequestrant Generic? Lipid Effects Y/N (monotherapy) Y LDL : 9% (4 g to 8 ; 21% (16 g to 20 ; 23% to 28% (>20 HDL : 4% to 8% (16 to 24 TG : 11% to 28% (4
Objectives. Emerging Treatments in Parkinson s s Disease. Pathology. As Parkinson s progresses it eventually affects large portions of the brain.
 Objectives Emerging Treatments in Parkinson s s Disease 1) Describe recent developments in the therapies for Parkinson s Disease Jeff Kraakevik MD Assistant Professor OHSU/Portland VAMC Parkinson s Center
Objectives Emerging Treatments in Parkinson s s Disease 1) Describe recent developments in the therapies for Parkinson s Disease Jeff Kraakevik MD Assistant Professor OHSU/Portland VAMC Parkinson s Center
ACUTE MANAGEMENT OF PARKINSON S PATIENTS WHO ARE NIL BY MOUTH (NBM) OR WHO HAVE A COMPROMISED SWALLOW NHS LANARKSHIRE PARKINSON S TEAM
 OR WHO HAVE A COMPROMISED SWALLOW NHS LANARKSHIRE PARKINSON S TEAM") ACUTE MANAGEMENT OF PARKINSON S PATIENTS WHO ARE NIL BY MOUTH (NBM) OR WHO HAVE A COMPROMISED SWALLOW NHS LANARKSHIRE PARKINSON S TEAM 1 CONTENTS: TOPIC PAGE Introduction 3 What should you do when a PD
ACUTE MANAGEMENT OF PARKINSON S PATIENTS WHO ARE NIL BY MOUTH (NBM) OR WHO HAVE A COMPROMISED SWALLOW NHS LANARKSHIRE PARKINSON S TEAM 1 CONTENTS: TOPIC PAGE Introduction 3 What should you do when a PD
PARKINSON S DISEASE. Nigrostriatal Dopaminergic Neurons 5/11/16 CARDINAL FEATURES OF PARKINSON S DISEASE. Parkinson s disease
 5/11/16 PARKINSON S DISEASE Parkinson s disease Prevalence increases with age (starts 40s60s) Seen in all ethnic groups, M:F about 1.5:1 Second most common neurodegenerative disease Genetics role greater
5/11/16 PARKINSON S DISEASE Parkinson s disease Prevalence increases with age (starts 40s60s) Seen in all ethnic groups, M:F about 1.5:1 Second most common neurodegenerative disease Genetics role greater
MANAGEMENT OF PATIENTS WITH PARKINSON S DISEASE WHO ARE NIL BY MOUTH OR WITH A COMPROMISED SWALLOW
 MANAGEMENT OF PATIENTS WITH PARKINSON S DISEASE WHO ARE NIL BY MOUTH OR WITH A COMPROMISED SWALLOW Author: Gordon W Duncan Status: Approved Authorised by: Clinical Policy Group Version: 1.0 Review date:
MANAGEMENT OF PATIENTS WITH PARKINSON S DISEASE WHO ARE NIL BY MOUTH OR WITH A COMPROMISED SWALLOW Author: Gordon W Duncan Status: Approved Authorised by: Clinical Policy Group Version: 1.0 Review date:
COMMON DRUG RELATED PROBLEMS SEEN IN PACE AND MECHANISMS TO MITIGATE RISK
 COMMON DRUG RELATED PROBLEMS SEEN IN PACE AND MECHANISMS TO MITIGATE RISK Robert L Alesiani, PharmD, CGP Chief Pharmacotherapy Officer CareKinesis, Inc. (a Tabula Rasa Healthcare Company) 2 3 4 5 Pharmacogenomics
COMMON DRUG RELATED PROBLEMS SEEN IN PACE AND MECHANISMS TO MITIGATE RISK Robert L Alesiani, PharmD, CGP Chief Pharmacotherapy Officer CareKinesis, Inc. (a Tabula Rasa Healthcare Company) 2 3 4 5 Pharmacogenomics
TRANSPARENCY COMMITTEE OPINION. 18 March 2009
 The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 18 March 2009 REQUIP LP 2 mg extended-release tablet Box of 21 tablets (CIP: 379 214-8) Box of 28 tablets (CIP: 379
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 18 March 2009 REQUIP LP 2 mg extended-release tablet Box of 21 tablets (CIP: 379 214-8) Box of 28 tablets (CIP: 379
Medication Audit Checklist- Antipsychotics - Atypical
 Medication Audit checklist Page 1 of 7 10-2018 Audit number: Client number: Ordering Provider: INDICATIONS 1) Disorders with psychotic symptoms (schizophrenia, schizoaffective disorder, manic disorders,
Medication Audit checklist Page 1 of 7 10-2018 Audit number: Client number: Ordering Provider: INDICATIONS 1) Disorders with psychotic symptoms (schizophrenia, schizoaffective disorder, manic disorders,
9/26/18. Objectives. Disclosures. Parkinson s Disease Update Clinical and Operational Considerations
 Parkinson s Disease Update Clinical and Operational Considerations Dana Saffel, PharmD, BCGP, CPh, FASCP President, CEO PharmaCare Strategies, Inc. September 2018 Objectives Describe epidemiology and pathophysiology
Parkinson s Disease Update Clinical and Operational Considerations Dana Saffel, PharmD, BCGP, CPh, FASCP President, CEO PharmaCare Strategies, Inc. September 2018 Objectives Describe epidemiology and pathophysiology
Antipsychotics. Something Old, Something New, Something Used to Treat the Blues
 Antipsychotics Something Old, Something New, Something Used to Treat the Blues Objectives To provide an overview of the key differences between first and second generation agents To an overview the newer
Antipsychotics Something Old, Something New, Something Used to Treat the Blues Objectives To provide an overview of the key differences between first and second generation agents To an overview the newer
The Shaking Palsy of 1817
 The Shaking Palsy of 1817 A Treatment Update on Parkinson s Disease Dr Eitzaz Sadiq Neurologist CH Baragwanath Acadamic Hospital Parkinson s Disease O Premature death of dopaminergic neurons O Symptoms
The Shaking Palsy of 1817 A Treatment Update on Parkinson s Disease Dr Eitzaz Sadiq Neurologist CH Baragwanath Acadamic Hospital Parkinson s Disease O Premature death of dopaminergic neurons O Symptoms
PD ExpertBriefings: Parkinson s Medications: Today and Tomorrow Led By: Cynthia L. Comella, M.D., F.A.A.N.
 PD ExpertBriefings: Parkinson s Medications: Today and Tomorrow Led By: Cynthia L. Comella, M.D., F.A.A.N. To hear the session live on: Tuesday, April 17, 2012 at 1:00 PM ET. DIAL: 1 (888) 272-8710 and
PD ExpertBriefings: Parkinson s Medications: Today and Tomorrow Led By: Cynthia L. Comella, M.D., F.A.A.N. To hear the session live on: Tuesday, April 17, 2012 at 1:00 PM ET. DIAL: 1 (888) 272-8710 and
Pharmacy Coverage Guidelines are subject to change as new information becomes available.
 ZELAPAR (selegiline hydrochloride) orally disintegrating tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific
ZELAPAR (selegiline hydrochloride) orally disintegrating tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific
Clinical Guideline for the management of inpatients with Parkinson s disease
 Clinical Guideline for the management of inpatients with Parkinson s disease Introduction: Parkinson s disease (PD) is the second most common neurodegenerative disorder, characterised by bradykinesia,
Clinical Guideline for the management of inpatients with Parkinson s disease Introduction: Parkinson s disease (PD) is the second most common neurodegenerative disorder, characterised by bradykinesia,
MEDICATION GUIDE. Quetiapine (kwe-tye-a-peen) Tablets USP
 Tablets USP") MEDICATION GUIDE Quetiapine (kwe-tye-a-peen) Tablets USP Read this Medication Guide before you start taking quetiapine tablets and each time you get a refill. There may be new information. This information
MEDICATION GUIDE Quetiapine (kwe-tye-a-peen) Tablets USP Read this Medication Guide before you start taking quetiapine tablets and each time you get a refill. There may be new information. This information
Where do you get most of your information about medications?
 DRUG ACTION AND RLS Jacquelyn Bainbridge, Pharm.D., FCCP Professor Pei Shieen Wong, Pharm.D., BCPS University of Colorado Anschutz Medical Campus, Skaggs School of Pharmacy and Pharmaceutical Sciences,
DRUG ACTION AND RLS Jacquelyn Bainbridge, Pharm.D., FCCP Professor Pei Shieen Wong, Pharm.D., BCPS University of Colorado Anschutz Medical Campus, Skaggs School of Pharmacy and Pharmaceutical Sciences,
Parkinson s Disease Update. Colleen Peach, RN, MSN, FNP Movement Disorders Clinic Emory University School of Medicine March 7, 2015
 Parkinson s Disease Update Colleen Peach, RN, MSN, FNP Movement Disorders Clinic Emory University School of Medicine March 7, 2015 Parkinson s Disease Progressive, chronic, neurodegenerative disease Slow,
Parkinson s Disease Update Colleen Peach, RN, MSN, FNP Movement Disorders Clinic Emory University School of Medicine March 7, 2015 Parkinson s Disease Progressive, chronic, neurodegenerative disease Slow,
Parkinson s Disease. Prevalence. Mark S. Baron, M.D. Cardinal Features. Clinical Characteristics. Not Just a Movement Disorder
 Prevalence Parkinson s Disease Mark S. Baron, M.D. Associate Professor of Neurology Movement Disorders Section VCU School of Medicine Common disorder Approaching 1% by 65 yrs of age, 2% by 80 yrs of age
Prevalence Parkinson s Disease Mark S. Baron, M.D. Associate Professor of Neurology Movement Disorders Section VCU School of Medicine Common disorder Approaching 1% by 65 yrs of age, 2% by 80 yrs of age
Page 1 of RECENT MAJOR CHANGES Warnings and Precautions, Falls (5.
 HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use QUETIAPINE FUMARATE EXTENDED-RELEASE TABLETS safely and effectively. See full prescribing information
HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use QUETIAPINE FUMARATE EXTENDED-RELEASE TABLETS safely and effectively. See full prescribing information
VI.2 Elements for a public summary. VI.2.1 Overview of disease epidemiology
 VI.2 Elements for a public summary VI.2.1 Overview of disease epidemiology Incidence and prevalence of target indication Schizophrenia is a mental disorder characterized by a breakdown of thought processes
VI.2 Elements for a public summary VI.2.1 Overview of disease epidemiology Incidence and prevalence of target indication Schizophrenia is a mental disorder characterized by a breakdown of thought processes
PL CE LIVE May 2012 Forum
 CE Information CE Information Pharmacist's Letter / Therapeutic Research Center is accredited by the Accreditation Council for Pharmacy Education (ACPE) as a provider of continuing pharmacy education.
CE Information CE Information Pharmacist's Letter / Therapeutic Research Center is accredited by the Accreditation Council for Pharmacy Education (ACPE) as a provider of continuing pharmacy education.
Scottish Medicines Consortium
 Scottish Medicines Consortium rotigotine 2mg/24 hours, 4mg/24 hours, 6mg/24 hours, 8mg/24 hours transdermal patch (Neupro ) (No: 289/06) Schwarz Pharma Ltd. 7 July 2006 The Scottish Medicines Consortium
Scottish Medicines Consortium rotigotine 2mg/24 hours, 4mg/24 hours, 6mg/24 hours, 8mg/24 hours transdermal patch (Neupro ) (No: 289/06) Schwarz Pharma Ltd. 7 July 2006 The Scottish Medicines Consortium
MEDICATION GUIDE Quetiapine Fumarate Extended-Release Tablets (Kwe-TYE-a-peen FUE-ma-rate)
") MEDICATION GUIDE Quetiapine Fumarate Extended-Release Tablets (Kwe-TYE-a-peen FUE-ma-rate) Read this Medication Guide before you start taking quetiapine fumarate extended-release tablets and each time
MEDICATION GUIDE Quetiapine Fumarate Extended-Release Tablets (Kwe-TYE-a-peen FUE-ma-rate) Read this Medication Guide before you start taking quetiapine fumarate extended-release tablets and each time
Objectives. Epidemiology. Diagnosis 3/27/2013. Identify positive and negative symptoms used for diagnosis of schizophrenia
 Objectives Identify positive and negative symptoms used for diagnosis of schizophrenia Mohamed Sallout, Pharm D. Pharmacist Resident St. Luke s Magic Valley Regional Medical Center List medications used
Objectives Identify positive and negative symptoms used for diagnosis of schizophrenia Mohamed Sallout, Pharm D. Pharmacist Resident St. Luke s Magic Valley Regional Medical Center List medications used
CENTENE PHARMACY AND THERAPEUTICS NEW DRUG REVIEW 3Q17 July August
 BRAND NAME Xadago GENERIC NAME Safinamide MANUFACTURER Newron Pharmaceuticals SpA holds license; granted approval. US WorldMeds, LLC exclusive licensee and distributor in the U.S. DATE OF APPROVAL March
BRAND NAME Xadago GENERIC NAME Safinamide MANUFACTURER Newron Pharmaceuticals SpA holds license; granted approval. US WorldMeds, LLC exclusive licensee and distributor in the U.S. DATE OF APPROVAL March
Parkinson s disease Therapeutic strategies. Surat Tanprawate, MD Division of Neurology University of Chiang Mai
 Parkinson s disease Therapeutic strategies Surat Tanprawate, MD Division of Neurology University of Chiang Mai 1 Scope Modality of treatment Pathophysiology of PD and dopamine metabolism Drugs Are there
Parkinson s disease Therapeutic strategies Surat Tanprawate, MD Division of Neurology University of Chiang Mai 1 Scope Modality of treatment Pathophysiology of PD and dopamine metabolism Drugs Are there
Participating Hospital Certification Form
 Participating Hospital Certification Form ATTENTION: this Certification Form is only applicable for Free Trial Product Units of ABILIFY MAINTENA (aripiprazole). Instructions: The Authorized Representative
Participating Hospital Certification Form ATTENTION: this Certification Form is only applicable for Free Trial Product Units of ABILIFY MAINTENA (aripiprazole). Instructions: The Authorized Representative
PERPHENAZINE. THERAPEUTICS Brands Trilafon see index for additional brand names. Generic? Yes
 PERPHENAZINE THERAPEUTICS Brands Trilafon see index for additional brand names Generic? Yes Class Neuroscience-based Nomenclature: dopamine receptor antagonist (D-RAn) Conventional antipsychotic (neuroleptic,
PERPHENAZINE THERAPEUTICS Brands Trilafon see index for additional brand names Generic? Yes Class Neuroscience-based Nomenclature: dopamine receptor antagonist (D-RAn) Conventional antipsychotic (neuroleptic,
Any interventions, where RCTs in PD are not available, are not included in the tables.
 Tables Interventions where new studies have been published are indicated in bold italics. Changes in conclusions are indicated in italics and are highlighted in yellow. Any interventions, where RCTs in
Tables Interventions where new studies have been published are indicated in bold italics. Changes in conclusions are indicated in italics and are highlighted in yellow. Any interventions, where RCTs in
What is the best medical therapy for early Parkinson's disease? Medications Commonly Used for Parkinson's Disease
 FPIN's Clinical Inquiries Treatment of Early Parkinson's Disease Clinical Question What is the best medical therapy for early Parkinson's disease? Evidence-Based Answer Treatment of early Parkinson's disease
FPIN's Clinical Inquiries Treatment of Early Parkinson's Disease Clinical Question What is the best medical therapy for early Parkinson's disease? Evidence-Based Answer Treatment of early Parkinson's disease
N e w s R e l e a s e
 Sunovion Pharmaceuticals Inc. 84 Waterford Drive, Marlborough, MA 01752-7010 Tel 508-481-6700 N e w s R e l e a s e Contact: Patrick Gaffey Senior Director, Corporate Communications Sunovion Pharmaceuticals
Sunovion Pharmaceuticals Inc. 84 Waterford Drive, Marlborough, MA 01752-7010 Tel 508-481-6700 N e w s R e l e a s e Contact: Patrick Gaffey Senior Director, Corporate Communications Sunovion Pharmaceuticals
CE on SUNDAY Newark, NJ October 18, 2009
 CE on SUNDAY Newark, NJ October 18, 2009 Date: Sunday, October 18, 2009 Time: 10:30 AM 11:45 AM Location: Sheraton Newark Airport Hotel Title: Speaker(s): Treating Parkinson s Disease: A Pharmacist s Overview
CE on SUNDAY Newark, NJ October 18, 2009 Date: Sunday, October 18, 2009 Time: 10:30 AM 11:45 AM Location: Sheraton Newark Airport Hotel Title: Speaker(s): Treating Parkinson s Disease: A Pharmacist s Overview
INSTRUCTIONS FOR USE Please read complete instructions prior to use
 INSTRUCTIONS FOR USE Please read complete instructions prior to use For deltoid or gluteal intramuscular injection only 3 MONTHS Administer every 3 months 1 With the syringe tip pointing up, shake syringe
INSTRUCTIONS FOR USE Please read complete instructions prior to use For deltoid or gluteal intramuscular injection only 3 MONTHS Administer every 3 months 1 With the syringe tip pointing up, shake syringe
Parkinson s Disease. Sirilak yimcharoen
 Parkinson s Disease Sirilak yimcharoen EPIDEMIOLOGY ~1% of people over 55 years Age range 35 85 years peak age of onset is in the early 60s ~5% of cases characterized by an earlier age of onset (typically
Parkinson s Disease Sirilak yimcharoen EPIDEMIOLOGY ~1% of people over 55 years Age range 35 85 years peak age of onset is in the early 60s ~5% of cases characterized by an earlier age of onset (typically
LOXAPINE. THERAPEUTICS Brands Loxitane Adasuve (Staccato loxapine, inhaled loxapine) see index for additional brand names. Generic?
 see index for additional brand names. Generic?") LOXAPINE THERAPEUTICS Brands Loxitane Adasuve (Staccato loxapine, inhaled loxapine) see index for additional brand names Generic? Yes Class Neuroscience-based Nomenclature: dopamine and serotonin receptor
LOXAPINE THERAPEUTICS Brands Loxitane Adasuve (Staccato loxapine, inhaled loxapine) see index for additional brand names Generic? Yes Class Neuroscience-based Nomenclature: dopamine and serotonin receptor
2/20/18. History of Parkinson s. What is happening in the brain? DOPAMINE! Epidemiology. Parkinson s Disease. It s much more than tremor
 Parkinson s Disease History of Parkinson s It s much more than tremor Laura Dixon, DNP, MPA, APRN, FNP-BC University of Louisville Department of Neurology Movement Disorders Division Parkinson s Disease
Parkinson s Disease History of Parkinson s It s much more than tremor Laura Dixon, DNP, MPA, APRN, FNP-BC University of Louisville Department of Neurology Movement Disorders Division Parkinson s Disease
475 GERIATRIC PSYCHOPHARMACOLOGY (p.1)
") 475 GERIATRIC PSYCHOPHARMACOLOGY (p.1) I. General Information? Use lower doses? Start low and go slow? Expect prolonged elimination ½ lives? Expect sedative-hypnotics to be dementing, to impair cognitive
475 GERIATRIC PSYCHOPHARMACOLOGY (p.1) I. General Information? Use lower doses? Start low and go slow? Expect prolonged elimination ½ lives? Expect sedative-hypnotics to be dementing, to impair cognitive
Literature Scan: Anti-Parkinson s Agents
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Update on the Treatment of Parkinson s Disease. Neurotherapeutics for Rehab Professionals November 6 th, 2015
 Brent Bluett, DO Dr. Brent Bluett completed medical school at Touro Unviersity Nevada College of Osteopathic Medicine, neurology residency at the University of Texas Southwestern at Austin, and a Movement
Brent Bluett, DO Dr. Brent Bluett completed medical school at Touro Unviersity Nevada College of Osteopathic Medicine, neurology residency at the University of Texas Southwestern at Austin, and a Movement
By using this card, you acknowledge that you currently meet the following eligibility requirements:
 175941133 LATUDA Copay Savings Program Terms and Conditions By using this card, you acknowledge that you currently meet the following eligibility requirements: You must be 18 years of age or older to accept
175941133 LATUDA Copay Savings Program Terms and Conditions By using this card, you acknowledge that you currently meet the following eligibility requirements: You must be 18 years of age or older to accept
Drugs Affecting the Central Nervous System
 Asst Prof Inam S Arif isamalhaj@yahoo.com Drugs Affecting the Central Nervous System Ass Efferent neurons in ANS Neurodegenerative Diseases Parkinson s Disease Multiple Sclerosis Alzheimer s Disease
Asst Prof Inam S Arif isamalhaj@yahoo.com Drugs Affecting the Central Nervous System Ass Efferent neurons in ANS Neurodegenerative Diseases Parkinson s Disease Multiple Sclerosis Alzheimer s Disease
Enhanced Primary Care Pathway: Parkinson s Disease
 Enhanced Primary Care Pathway: Parkinson s Disease 1. Focused summary of PD relevant to primary care Parkinson s Disease (PD) and Essential tremor (ET) are two of the most common movement disorders encountered
Enhanced Primary Care Pathway: Parkinson s Disease 1. Focused summary of PD relevant to primary care Parkinson s Disease (PD) and Essential tremor (ET) are two of the most common movement disorders encountered
MEDICATION GUIDE Quetiapine Fumarate Tablets
 MEDICATION GUIDE Quetiapine Fumarate Tablets Read this Medication Guide before you start taking quetiapine fumarate tablets and each time you get a refill. There may be new information. This Medication
MEDICATION GUIDE Quetiapine Fumarate Tablets Read this Medication Guide before you start taking quetiapine fumarate tablets and each time you get a refill. There may be new information. This Medication
Faculty Information 2/15/2013
 Timothy Reilly, PharmD, BCPS, CGP, FASCP Clinical Assistant Professor Ernest Mario School of Pharmacy Rutgers, The State University of New Jersey tjreilly@pharmacy.rutgers.edu Faculty Information Presenter:
Timothy Reilly, PharmD, BCPS, CGP, FASCP Clinical Assistant Professor Ernest Mario School of Pharmacy Rutgers, The State University of New Jersey tjreilly@pharmacy.rutgers.edu Faculty Information Presenter:
Presented by Rengena Chan-Ting, DO, CMD, FACOI Jenna D. Toniatti, PharmD
 Presented by Rengena Chan-Ting, DO, CMD, FACOI Jenna D. Toniatti, PharmD Define BPSD and review the spectrum of associated symptoms Review pharmacologic and non-pharmacologic treatments for BPSD Evaluate
Presented by Rengena Chan-Ting, DO, CMD, FACOI Jenna D. Toniatti, PharmD Define BPSD and review the spectrum of associated symptoms Review pharmacologic and non-pharmacologic treatments for BPSD Evaluate
History Parkinson`s disease. Parkinson's disease was first formally described in 1817 by a London physician named James Parkinson
 Parkinsonismm History Parkinson`s disease Parkinson's disease was first formally described in 1817 by a London physician named James Parkinson Definition : Parkinsonism: Parkinsonism is a progressive neurological
Parkinsonismm History Parkinson`s disease Parkinson's disease was first formally described in 1817 by a London physician named James Parkinson Definition : Parkinsonism: Parkinsonism is a progressive neurological
Technician Training Tutorial: Safety Considerations with Opioids
 (Page 1 of 5) Technician Training Tutorial: Safety Considerations with Opioids Opioids as a drug class are considered to be high-alert drugs. This class includes codeine, methadone, oxycodone, etc. When
(Page 1 of 5) Technician Training Tutorial: Safety Considerations with Opioids Opioids as a drug class are considered to be high-alert drugs. This class includes codeine, methadone, oxycodone, etc. When
Alison Charleston 1 st September 2016
 Alison Charleston 1 st September 2016 Clinical features of Parkinson s disease Differential diagnosis Management of the motor features Non-motor and neuropsychiatric aspects 100-200 per 100,000 prevalence
Alison Charleston 1 st September 2016 Clinical features of Parkinson s disease Differential diagnosis Management of the motor features Non-motor and neuropsychiatric aspects 100-200 per 100,000 prevalence
Concomitant Use of a Moderate CYP3A4 Inducer: It may be necessary to increase the dose of LATUDA (2.6, 7.1).
.") 1 HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use safely and effectively. See full prescribing information for. (lurasidone hydrochloride) tablets,
1 HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use safely and effectively. See full prescribing information for. (lurasidone hydrochloride) tablets,
) and serotonin Type 2 (5-HT 2A
 and serotonin Type 2 (5-HT 2A") Latuda (lurasidone HCl) Fact Sheet Schizophrenia FREQUENTLY ASKED QUESTIONS What type of patient with schizophrenia is appropriate for LATUDA? LATUDA is an atypical antipsychotic agent indicated for the
Latuda (lurasidone HCl) Fact Sheet Schizophrenia FREQUENTLY ASKED QUESTIONS What type of patient with schizophrenia is appropriate for LATUDA? LATUDA is an atypical antipsychotic agent indicated for the
DRUGS THAT ACT IN THE CNS
 DRUGS THAT ACT IN THE CNS Drugs for Neurodegenerative Diseases 2 Dr Karamallah S. Mahmood PhD Clinical Pharmacology 1 DRUGS USED IN PARKINSON S DISEASE/ B. Selegiline and rasagiline Selegiline, also called
DRUGS THAT ACT IN THE CNS Drugs for Neurodegenerative Diseases 2 Dr Karamallah S. Mahmood PhD Clinical Pharmacology 1 DRUGS USED IN PARKINSON S DISEASE/ B. Selegiline and rasagiline Selegiline, also called
Drug Management of Parkinsonism. By Prof. Mohammad Saleh M. Hassan PhD. (Pharma); MSc. (Ped.); MHPE (Ed.)
; MSc. (Ped.); MHPE (Ed.)") Drug Management of Parkinsonism By Prof. Mohammad Saleh M. Hassan PhD. (Pharma); MSc. (Ped.); MHPE (Ed.) Drug management of Parkinsonism Levodopa Ergot derivatives noamine Oxidaes Inhibitors Catechol-Omethyl
Drug Management of Parkinsonism By Prof. Mohammad Saleh M. Hassan PhD. (Pharma); MSc. (Ped.); MHPE (Ed.) Drug management of Parkinsonism Levodopa Ergot derivatives noamine Oxidaes Inhibitors Catechol-Omethyl
Appendix 2: Admissions checklists for people with Parkinson s
 Appendix 2: Admissions checklists for people with Parkinson s This document is intended to form the basis of a locally developed tool and so it has been built to be amended with relevant local information,
Appendix 2: Admissions checklists for people with Parkinson s This document is intended to form the basis of a locally developed tool and so it has been built to be amended with relevant local information,
MEDICATION GUIDE. Aripiprazole Tablets (AR-i-PIP-ra-zole)
") MEDICATION GUIDE Aripiprazole Tablets (AR-i-PIP-ra-zole) What is the most important information I should know about aripiprazole tablets? (For other side effects, also see What are the possible side effects
MEDICATION GUIDE Aripiprazole Tablets (AR-i-PIP-ra-zole) What is the most important information I should know about aripiprazole tablets? (For other side effects, also see What are the possible side effects
Re-Submission. Scottish Medicines Consortium. rasagiline 1mg tablet (Azilect ) (No. 255/06) Lundbeck Ltd / Teva Pharmaceuticals Ltd.
 (No. 255/06) Lundbeck Ltd / Teva Pharmaceuticals Ltd.") Scottish Medicines Consortium Re-Submission rasagiline 1mg tablet (Azilect ) (No. 255/06) Lundbeck Ltd / Teva Pharmaceuticals Ltd 10 November 2006 The Scottish Medicines Consortium (SMC) has completed
Scottish Medicines Consortium Re-Submission rasagiline 1mg tablet (Azilect ) (No. 255/06) Lundbeck Ltd / Teva Pharmaceuticals Ltd 10 November 2006 The Scottish Medicines Consortium (SMC) has completed