Diabetes 2013: Achieving Goals Through Comprehensive Treatment. Session 2: Individualizing Therapy
|
|
|
- Letitia Stokes
- 5 years ago
- Views:
Transcription
1 Diabetes 2013: Achieving Goals Through Comprehensive Treatment Session 2: Individualizing Therapy Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism The George Washington University School of Medicine
2 Session 2 Agenda Diabetes treatment guidelines» Standardized evaluation and treatment recommendations» Establishing individualized treatment goals» Review of major classes of oral agents» Initial pharmacologic therapy and stepwise intensification Incretin-based therapy» Incretin physiology» GLP-1 analogues» DPP-4 inhibitors Intensifying insulin therapy» Implementation of basal bolus therapy» Combined insulin GLP-1 therapy

3 STANDARDS OF MEDICAL CARE IN DIABETES 2013 Supplement 1 January 2013
4 Treatment of Type 2 Diabetes: Lifestyle Intervention Diabetes education Knowledge about: disease process, potential risks, treatments, glucose monitoring, self-care Weight loss Nutrition Exercise Stop smoking
5 Patients on multiple-dose insulin (MDI) or insulin pump therapy should do SMBG At least prior to meals and snacks Occasionally post-prandially At bedtime Prior to exercise Recommendations: Glucose Monitoring (1) When they suspect low blood glucose After treating low blood glucose until they are normoglycemic Prior to critical tasks such as driving Diabetes Care 2013;36(suppl 1):S17.
6 Recommendations: Glucose Monitoring (2) When prescribed as part of a broader educational context, SMBG results may be helpful to guide treatment decisions and/or patient selfmanagement for patients using less frequent insulin injections or noninsulin therapies When prescribing SMBG, ensure that patients receive ongoing instruction and regular evaluation of SMBG technique and SMBG results, as well as their ability to use SMBG data to adjust therapy
7 Recommendations: Physical Activity Advise people with diabetes to perform at least 150 min/week of moderate-intensity aerobic physical activity (50 70% of maximum heart rate), spread over at least 3 days per week with no more than 2 consecutive days without exercise In absence of contraindications, adults with type 2 diabetes should be encouraged to perform resistance training at least twice per week
8 Blood Pressure Recommendations: Measure at each visit Dilated eye exam At diagnosis. Initially annually, then every 2-3 years after normal exam Foot exam Examination Annually Laboratory Evaluation A1C Lipids Creatinine Urine albumin Twice yearly for patients meeting treatment goals on stable therapy Yearly Yearly Yearly (spot urine albumin:creatinine ratio)
9 Guidelines for Blood Pressure & Lipid Control Blood pressure Lipids < 130/80 mmhg LDL: < 100 mg/dl (2.59 mmol/l) < 70 mg/dl (1.81 mmol/l) (with overt CVD) HDL: > 40 mg/dl (1.04 mmol/l) Men > 50 mg/dl (1.30 mmol/l)women TG: < 150 mg/dl (1.69 mmol/l) Statin therapy regardless of baseline lipids for patients with overt CVD or multiple risk factors ADA. Diabetes Care. 2013;36 (Suppl 1):S11-66
10 CHD Screening and Treatment Routine CAD screening not recommended in asymptomatic patients If CVD risk factors are treated, CAD screening does not improve outcomes Diabetes Care 2013;36(suppl 1):S17.
11 Recommendations: Antiplatelet Agents (1) Consider aspirin therapy ( mg/day) As a primary prevention strategy in those with type 1 or type 2 diabetes at increased cardiovascular risk (10-year risk >10%) Includes most men >50 years of age or women >60 years of age who have at least one additional major risk factor Family history of CVD Hypertension Smoking Dyslipidemia Albuminuria Diabetes Care 2013;36(suppl 1):S17.
12 Recommendations: Antiplatelet Agents (2) Aspirin should not be recommended for CVD prevention for adults with diabetes at low CVD risk, since potential adverse effects from bleeding likely offset potential benefits 10-year CVD risk <5%: men <50 and women <60 years of age with no major additional CVD risk factors In patients in these age groups with multiple other risk factors (10-year risk 5 10%), clinical judgment is required Diabetes Care 2013;36(suppl 1):S17.




13
14 Recommendations: Immunization (1) Provide influenza vaccine annually to all diabetic patients 6 months of age Administer pneumococcal polysaccharide vaccine to all diabetic patients 2 years One-time revaccination recommended for those >64 years previously immunized at <65 years if administered >5 years ago Other indications for repeat vaccination: nephrotic syndrome, chronic renal disease, immunocompromised states Diabetes Care 2013;36(suppl 1):S17.
15 Recommendations: Immunization (2) Administer hepatitis B vaccination to unvaccinated adults with diabetes who are aged 19 through 59 years Consider administering hepatitis B vaccination to unvaccinated adults with diabetes who are aged 60 years
16 Recommendations: Glycemic Goals in Adults (1) Lowering A1C to below or around 7% has been shown to reduce microvascular complications and, if implemented soon after the diagnosis of diabetes, is associated with long-term reduction in macrovascular disease Therefore, a reasonable A1C goal for many nonpregnant adults is <7% Plasma glucose: Pre-prandial PG <130 mg/dl (7.2 mmol/l) Post-prandial PG <180 mg/dl (10.0 mmol/l) ADA. V. Diabetes Care. Diabetes Care 2013;36(suppl 1):S19.
17 Correlation of A1C with Average Glucose Mean plasma glucose A1C (%) mg/dl mmol/l These estimates are based on ADAG data of ~2,700 glucose measurements over 3 months per A1C measurement in 507 adults with type 1, type 2, and no diabetes. The correlation between A1C and average glucose was A calculator for converting A1C results into estimated average glucose (eag), in either mg/dl or mmol/l, is available at
18 Recommendations: Glycemic Goals in Adults (2) Providers might reasonably suggest more stringent A1C goals (such as <6.5%) for selected individual patients, if this can be achieved without significant hypoglycemia or other adverse effects of treatment Appropriate patients might include those with short duration of diabetes, long life expectancy, and no significant CVD ADA. V. Diabetes Care. Diabetes Care 2013;36(suppl 1):S19.
19 Recommendations: Glycemic Goals in Adults (3) Less stringent A1C goals (such as <8%) may be appropriate for patients with History of severe hypoglycemia, limited life expectancy, advanced microvascular or macrovascular complications, extensive comorbid conditions Those with longstanding diabetes in whom the general goal is difficult to attain despite diabetes selfmanagement education, appropriate glucose monitoring, and effective doses of multiple glucose lowering agents including insulin
20 Cardiovascular Outcomes in Recent Prospective Trials n Known diabetes duration (y) Length of treatment intervention (y) A1c difference between groups Reduction of CV Events (CV composite) ADVANCE 11, % (7.3 vs 6.5) 6% (NS) ACCORD 10, % (7.5 vs 6.4) 10% (NS) Nonfatal MI: 24% (p =.004) VADT 1, % (8.4 vs 6.9) 12% (NS) Subsequent meta-analysis of these studies and the UKPDS showed no significant effect of intensive glycemic control on overall cardiovascular events or mortality, but did show a significant 15% decrease in fatal or non-fatal MI


21 Glycemic Control Decision Making Target HbA1C Lower Higher Inzucchi S et al. 2012; Diabetes Care. 35:
22 Selecting Anti-Hyperglycemic Medications Major Distinguishing Features Efficacy Risk of hypoglycemia Weight gain Side effects Costs Safety concerns and contraindications
 Muscle/Fat (+) ( ) Metformin ( ) GLP-1 agonist DPP-4 inhibitor Sulfonylureas Meglitinides Nateglinide Liver ( ) Insulin + Insulin Secretion Pancreas Insulin")
23 Antihyperglycemic Agents: Glycosuria Major Sites of Action Kidney Plasma glucose -Glucosidase inhibitors ( ) Carbohydrate Absorption GI tract Glucose Uptake Glucose Production SGLT2 (+) inhibitor Glitazones (+) Muscle/Fat (+) ( ) Metformin ( ) GLP-1 agonist DPP-4 inhibitor Sulfonylureas Meglitinides Nateglinide Liver ( ) Insulin + Insulin Secretion Pancreas Insulin Secretion
")

24 Glucose-Lowering Therapy in Type 2 Diabetes (1) Inzucchi S et al. 2012; Diabetes Care. 35:
25 Sulfonylurea Efficacy High Hypoglycemia Moderate risk Weight Gain Major side effects Hypoglycemia Costs Low Advantages Disadvantages Good initial efficacy Risk of hypoglycemia Extensive experience, widely available Weight gain Well tolerated Possible cardiovascular risk compared to metformin Inexpensive
26 Thiazolidinedione Pioglitazone Efficacy High Hypoglycemia Low risk Weight Gain Major side effects Fluid retention Costs High (However, soon will be generic) Advantages Disadvantages Decrease manifestations of insulin resistance Weight gain Durable activity, may diminish rate of deterioration of beta cell function Fluid retention and increased risk of CHF? Decrease in cardiovascular events Increased osteoporotic fractures in women Safety concerns
27 Thiazolidinediones Safety Concerns Increased risk of MI (rosiglitazone)» Initial concerns not supported by further studies Fluid retention and CHF» Not associated with increased risk of death, MI or stroke Increased risk of bone fracture in older women Possible association between pioglitazone and bladder cancer
28
29 Clinical Inertia in the Treatment of Type 2 Diabetes For patients on one oral agent with HbA1C 7% the median time until addition of another oral agent was years For patients on two oral agents with HbA1C 7% the median time until addition of another oral agent was >6.9 years For patients on two or three oral agents with HbA1C 7.5% the median time until initiation of insulin therapy was >6 years Khunti K, et al. Diabetes Care. 2013; 36:



30 Main Pathophysiological Defects in T2DM pancreatic insulin secretion incretin effect gut carbohydrate delivery & absorption pancreatic glucagon secretion HYPERGLYCEMIA hepatic glucose production peripheral glucose uptake Adapted from: Inzucchi SE, Sherwin RS in: Cecil Medicine 2011
31 Incretin-Based Therapy: GLP-1 Analogs & DPP-4 Inhibitors
32 Oral glucose (50g) or isoglycemic infusion IV glucose Oral glucose 2.0 * 200 C-Peptide (nmol/l) Plasma Glucose (mg/dl) The Incretin Effect: Difference in Response to Oral vs IV Glucose * * * * 1.0 * * Time (min) Time (min) Nauck MA, et al. J Clin Endocrinol Metab. 1986;63:
")
33 Glucagon-Like Peptide 1 (GLP-1) Linker region (15 17) N-terminal region Helical region (7 14) Helical region (18 29) Cleaved from proglucagon in intestinal L-cells and neurons in hindbrain/hypothalamus2 Rapid release from intestinal L cells in response to meals Potentiates insulin release Multiple biologic actions2 Rapidly degraded by protease dipeptidyl peptidase IV (DPP-4) 1. Image courtesy of Cyril Sarrauste de Menthière, PhD, Institute of Human Genetics, Montpellier, France ( 2. Vilsbøll T, Holst JJ. Diabetologia. 2004;47:
34 The Insulinotropic Effects of Infusion of GLP-1 and GIP in Healthy Subjects N=8, healthy males Insulin Concentration 250 Meal test Glucose clamp GLP-1 clamp Insulin, pmol/l 200 GIP clamp Time, min GLP-1 and GIP infusion 6mmol/L Fasting level 7mmol/L Plasma glucose levels during the 3 stepwise glucose clamps Time, min Adapted from Vilsbøll T et al. Regul Pept. 2003;114:
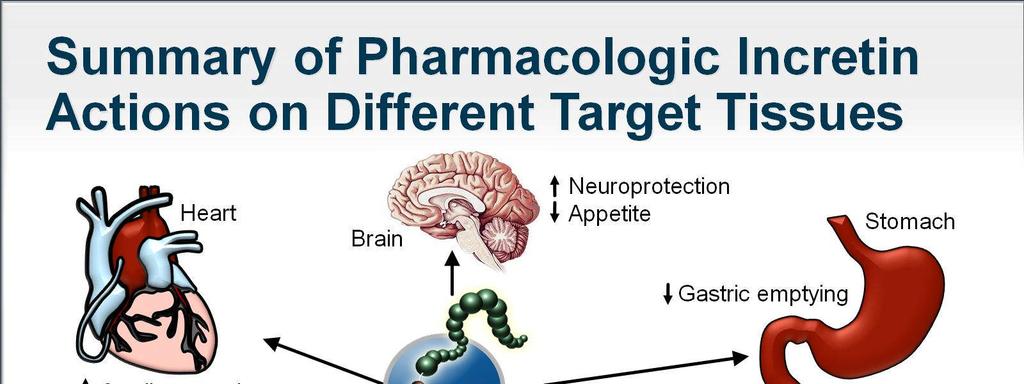
35 Incretins Improve Multiple Aspects of Islet-Cell Function GLP-1 (produced by L cells in the small intestine) alpha cells beta cells GIP (produced by K cells in the small intestine) Stimulates glucose-dependent insulin release Suppresses glucose-dependent glucagon release Increases insulin gene transcription and insulin biosynthesis Improves beta-cell responsiveness to glucose Increases expression of glucose transporter-2 (GLUT 2) and glucokinase Decreases proinsulin to insulin ratio Promotes differentiation of duct progenitor cells to beta cells, inhibits apotosis of beta cells Stimulates glucose-dependent insulin release Drucker DJ. Molecular Endocrinology. 2003;17: Farilla L et al. Endocrinology. 2002;143; Holst JJ. Diabetes Metab Res Rev. 2002;18: Orskov C et al. Endocrinology. 1988;123: Quddusi S et al. Diabetes Care. 2003;26: Stumvoll M et al. J Clin Endocrinol Metab. 2001;86:
36
37 The Incretin Effect in Subjects Without and With Type 2 Diabetes Control Subjects (n=8) 0.6 Incretin Effect Time, min nmol/l 0.2 nmol / L The incretin effect is diminished in type 2 diabetes. 0.5 IR Insulin, mu/l 80 IR Insulin, mu/l Patients With Type 2 Diabetes (n=14) Time, min Oral glucose load Intravenous (IV) glucose infusion Adapted with permission from Nauck M et al. Diabetologia. 1986;29: Copyright 1986 Springer-Verlag. 39
38 Continuous GLP-1 Infusion in Patients with Diabetes Rachman J, et al. Diabetologia 1997; 40:

 active")
")

39 GLP-1 and GIP Secretion and Mixed Inactivation meal Intestinal GLP-1 release t½ = 1 to 2 min GLP-1 (7-36) active DPP-4 DPP-4: Dipeptidyl peptidase 4 GLP-1 (9-36) inactive (>80% of pool) Adapted from Deacon CF, et al. Diabetes. 1995;44:
40 Incretin Pharmacotherapy GLP-1 has a very short half-life and therefore is not suitable for pharmacologic therapy Approaches to therapeutic use of incretins: GLP-1 agonists resistant to DPP-4 DPP-4 inhibition to extend the half-life of endogenous GLP-1
41
42 Effect of Exenatide on Fasting Plasma Glucose and Insulin in Type 2 Diabetes Glucose Insulin Placebo Placebo 0.05 µg/kg exenatide 0.1 µg/kg exenatide 15 Mean (SE) Serum Insulin (pmol/l) Mean (SE) Plasma Glucose (mmol/l) 0.05 µg/kg exenatide 0.2 µg/kg exenatide µg/kg exenatide µg/kg exenatide Time (h) Time (h) Kolterman OG, et al. J Clin Endocrinol Metab 2003; 88:
43
44
Comprehensive Diabetes Treatment
 Comprehensive Diabetes Treatment Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism The George Washington University School of Medicine Diabetes
Comprehensive Diabetes Treatment Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism The George Washington University School of Medicine Diabetes
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy
 Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
The Many Faces of T2DM in Long-term Care Facilities
 The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
Chief of Endocrinology East Orange General Hospital
 Targeting the Incretins System: Can it Improve Our Ability to Treat Type 2 Diabetes? Darshi Sunderam, MD Darshi Sunderam, MD Chief of Endocrinology East Orange General Hospital Age-adjusted Percentage
Targeting the Incretins System: Can it Improve Our Ability to Treat Type 2 Diabetes? Darshi Sunderam, MD Darshi Sunderam, MD Chief of Endocrinology East Orange General Hospital Age-adjusted Percentage
Management of Type 2 Diabetes
 Management of Type 2 Diabetes Pathophysiology Insulin resistance and relative insulin deficiency/ defective secretion Not immune mediated No evidence of β cell destruction Increased risk with age, obesity
Management of Type 2 Diabetes Pathophysiology Insulin resistance and relative insulin deficiency/ defective secretion Not immune mediated No evidence of β cell destruction Increased risk with age, obesity
Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable?
 Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable? Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of
Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable? Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of
Initiation and Titration of Insulin in Diabetes Mellitus Type 2
 Initiation and Titration of Insulin in Diabetes Mellitus Type 2 Greg Doelle MD, MS April 6, 2016 Disclosure I have no actual or potential conflicts of interest in relation to the content of this lecture.
Initiation and Titration of Insulin in Diabetes Mellitus Type 2 Greg Doelle MD, MS April 6, 2016 Disclosure I have no actual or potential conflicts of interest in relation to the content of this lecture.
Vipul Lakhani, MD Oregon Medical Group Endocrinology
 Vipul Lakhani, MD Oregon Medical Group Endocrinology Disclosures None Objectives Be able to diagnose diabetes and assess control Be able to identify appropriate classes of medications for diabetes treatment
Vipul Lakhani, MD Oregon Medical Group Endocrinology Disclosures None Objectives Be able to diagnose diabetes and assess control Be able to identify appropriate classes of medications for diabetes treatment
GLP 1 agonists Winning the Losing Battle. Dr Bernard SAMIA. KCS Congress: Impact through collaboration
 GLP 1 agonists Winning the Losing Battle Dr Bernard SAMIA KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures I have
GLP 1 agonists Winning the Losing Battle Dr Bernard SAMIA KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures I have
DPP-4 inhibitor. The new class drug for Diabetes
 DPP-4 inhibitor The new class drug for Diabetes 1 Cause of Death in Korea 1 st ; Neoplasm 2 nd ; Cardiovascular Disease 3 rd ; Cerebrovascular Disease Diabetes 2 Incidence of Fatal or Nonfatal MI During
DPP-4 inhibitor The new class drug for Diabetes 1 Cause of Death in Korea 1 st ; Neoplasm 2 nd ; Cardiovascular Disease 3 rd ; Cerebrovascular Disease Diabetes 2 Incidence of Fatal or Nonfatal MI During
Optimal glucose control. DM Treatment. Glucose Control one out of many. Many guidelines: Confusing. Theorectically easy
 DM Treatment How to Achieve Optimal Glycaemic Control The Tung Wah Eastern Hospital Experience of DM Share Care Experience Optimal glucose control Theorectically easy More challenging in the real world
DM Treatment How to Achieve Optimal Glycaemic Control The Tung Wah Eastern Hospital Experience of DM Share Care Experience Optimal glucose control Theorectically easy More challenging in the real world
Diabetes Mellitus: Implications of New Clinical Trials and New Medications
 Diabetes Mellitus: Implications of New Clinical Trials and New Medications Estimates of Diagnosed Diabetes in Adults, 2005 Alka M. Kanaya, MD Asst. Professor of Medicine UCSF, Primary Care CME October
Diabetes Mellitus: Implications of New Clinical Trials and New Medications Estimates of Diagnosed Diabetes in Adults, 2005 Alka M. Kanaya, MD Asst. Professor of Medicine UCSF, Primary Care CME October
Novel anti-diabetic therapies
 Prof. Manfredi Rizzo, MD, PhD ASSOCIATE PROFESSOR OF INTERNAL MEDICINE School of Medicine University of Palermo, Italy & ASSOCIATE PROFESSOR OF INTERNAL MEDICINE School of Medicine University of South
Prof. Manfredi Rizzo, MD, PhD ASSOCIATE PROFESSOR OF INTERNAL MEDICINE School of Medicine University of Palermo, Italy & ASSOCIATE PROFESSOR OF INTERNAL MEDICINE School of Medicine University of South
TREATMENT OF DIABETES AFTER METFORMIN GREGG GERETY, MD ALBANY MEDICAL COLLEGE, DIVISION OF COMMUNITY ENDOCRINOLOGY JULY 14, 2017
 TREATMENT OF DIABETES AFTER METFORMIN GREGG GERETY, MD ALBANY MEDICAL COLLEGE, DIVISION OF COMMUNITY ENDOCRINOLOGY JULY 14, 2017 Outline Review treatment algorithms from ADA/ EASD & ACE/AACE. Review positive
TREATMENT OF DIABETES AFTER METFORMIN GREGG GERETY, MD ALBANY MEDICAL COLLEGE, DIVISION OF COMMUNITY ENDOCRINOLOGY JULY 14, 2017 Outline Review treatment algorithms from ADA/ EASD & ACE/AACE. Review positive
Practical Strategies for the Clinical Use of Incretin Mimetics CME/CE. CME/CE Released: 09/15/2009; Valid for credit through 09/15/2010
 Practical Strategies for the Clinical Use of Incretin Mimetics CME/CE Robert R. Henry, MD Authors and Disclosures CME/CE Released: 09/15/2009; Valid for credit through 09/15/2010 Introduction Type 2 diabetes
Practical Strategies for the Clinical Use of Incretin Mimetics CME/CE Robert R. Henry, MD Authors and Disclosures CME/CE Released: 09/15/2009; Valid for credit through 09/15/2010 Introduction Type 2 diabetes
Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes
 Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes Genetics, environment, and lifestyle (obesity, inactivity, poor diet) Impaired fasting glucose Decreased β-cell
Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes Genetics, environment, and lifestyle (obesity, inactivity, poor diet) Impaired fasting glucose Decreased β-cell
Multiple Factors Should Be Considered When Setting a Glycemic Goal
 Multiple Facts Should Be Considered When Setting a Glycemic Goal Patient attitude and expected treatment effts Risks potentially associated with hypoglycemia, other adverse events Disease duration Me stringent
Multiple Facts Should Be Considered When Setting a Glycemic Goal Patient attitude and expected treatment effts Risks potentially associated with hypoglycemia, other adverse events Disease duration Me stringent
A Practical Approach to the Use of Diabetes Medications
 A Practical Approach to the Use of Diabetes Medications Juan Pablo Frias, M.D., FACE President, National Research Institute, Los Angles, CA Clinical Faculty, University of California, San Diego, CA OUTLINE
A Practical Approach to the Use of Diabetes Medications Juan Pablo Frias, M.D., FACE President, National Research Institute, Los Angles, CA Clinical Faculty, University of California, San Diego, CA OUTLINE
Role of incretins in the treatment of type 2 diabetes
 Role of incretins in the treatment of type 2 diabetes Jens Juul Holst Department of Medical Physiology Panum Institute University of Copenhagen Denmark Diabetes & Obesity Spanish Society of Internal Medicine
Role of incretins in the treatment of type 2 diabetes Jens Juul Holst Department of Medical Physiology Panum Institute University of Copenhagen Denmark Diabetes & Obesity Spanish Society of Internal Medicine
IMPROVED DIAGNOSIS OF TYPE 2 DIABETES AND TAILORING MEDICATIONS
 IMPROVED DIAGNOSIS OF TYPE 2 DIABETES AND TAILORING MEDICATIONS Dr Bidhu Mohapatra, MBBS, MD, FRACP Consultant Physician Endocrinology and General Medicine Introduction 382 million people affected by diabetes
IMPROVED DIAGNOSIS OF TYPE 2 DIABETES AND TAILORING MEDICATIONS Dr Bidhu Mohapatra, MBBS, MD, FRACP Consultant Physician Endocrinology and General Medicine Introduction 382 million people affected by diabetes
Management of Type 2 Diabetes. Why Do We Bother to Achieve Good Control in DM2. Insulin Secretion. The Importance of BP and Glucose Control
 Insulin Secretion Management of Type 2 Diabetes DG van Zyl Why Do We Bother to Achieve Good Control in DM2 % reduction 0-5 -10-15 -20-25 -30-35 -40 The Importance of BP and Glucose Control Effects of tight
Insulin Secretion Management of Type 2 Diabetes DG van Zyl Why Do We Bother to Achieve Good Control in DM2 % reduction 0-5 -10-15 -20-25 -30-35 -40 The Importance of BP and Glucose Control Effects of tight
American Diabetes Association 2018 Guidelines Important Notable Points
 American Diabetes Association 2018 Guidelines Important Notable Points The Standards of Medical Care in Diabetes-2018 by ADA include the most current evidencebased recommendations for diagnosing and treating
American Diabetes Association 2018 Guidelines Important Notable Points The Standards of Medical Care in Diabetes-2018 by ADA include the most current evidencebased recommendations for diagnosing and treating
STANDARDS OF MEDICAL CARE IN DIABETES 2014
 STANDARDS OF MEDICAL CARE IN DIABETES 2014 I. CLASSIFICATION AND DIAGNOSIS Classification of Diabetes Type 1 diabetes β-cell destruction Type 2 diabetes Progressive insulin secretory defect Other specific
STANDARDS OF MEDICAL CARE IN DIABETES 2014 I. CLASSIFICATION AND DIAGNOSIS Classification of Diabetes Type 1 diabetes β-cell destruction Type 2 diabetes Progressive insulin secretory defect Other specific
Diabetes Review Chris Paras, D.O. Assistant Prof of Medicine, NYIT & Touro COM Designated Institutional Official & Assoc. Clinical Dean, Brookdale
 Diabetes Review Chris Paras, D.O. Assistant Prof of Medicine, NYIT & Touro COM Designated Institutional Official & Assoc. Clinical Dean, Brookdale University Hospital Diabetes Care 2018 Jan; 41 Objectives
Diabetes Review Chris Paras, D.O. Assistant Prof of Medicine, NYIT & Touro COM Designated Institutional Official & Assoc. Clinical Dean, Brookdale University Hospital Diabetes Care 2018 Jan; 41 Objectives
Optimizing Treatment Strategies to Improve Patient Outcomes in the Management of Type 2 Diabetes
 Optimizing Treatment Strategies to Improve Patient Outcomes in the Management of Type 2 Diabetes Philip Raskin, MD Professor of Medicine The University of Texas, Southwestern Medical Center NAMCP Spring
Optimizing Treatment Strategies to Improve Patient Outcomes in the Management of Type 2 Diabetes Philip Raskin, MD Professor of Medicine The University of Texas, Southwestern Medical Center NAMCP Spring
Diabetes update - Diagnosis and Treatment
 Diabetes update - Diagnosis and Treatment Eugene J Barrett, MD,PhD Madge Jones Professor of Medicine Director, University of Virginia Diabetes Center Disclosures - None Case 1 - Screening for Diabetes
Diabetes update - Diagnosis and Treatment Eugene J Barrett, MD,PhD Madge Jones Professor of Medicine Director, University of Virginia Diabetes Center Disclosures - None Case 1 - Screening for Diabetes
la prise en charge du diabète de
 N21 XIII Congrès National de Diabétologie, 29 mai 2011, Alger Intérêt et place des Anti DPP4 dans la prise en charge du diabète de type 2 Nicolas PAQUOT, MD, PhD CHU Sart-Tilman, Université de Liège Belgique
N21 XIII Congrès National de Diabétologie, 29 mai 2011, Alger Intérêt et place des Anti DPP4 dans la prise en charge du diabète de type 2 Nicolas PAQUOT, MD, PhD CHU Sart-Tilman, Université de Liège Belgique
OBJECTIVES 4/7/2014. Diabetes Update Overview of the Diabetes Epidemic in the United States. ISHP Annual Spring Meeting
 Diabetes Update 2014 ISHP Annual Spring Meeting Hayley Miller MD April 13, 2014 OBJECTIVES Review diabetes guidelines. Understand diabetes management targets. Discuss current therapeutic strategies. Overview
Diabetes Update 2014 ISHP Annual Spring Meeting Hayley Miller MD April 13, 2014 OBJECTIVES Review diabetes guidelines. Understand diabetes management targets. Discuss current therapeutic strategies. Overview
Standards of Medical Care in Diabetes 2016
 Standards of Medical Care in Diabetes 2016 Care Delivery Systems 33-49% of patients still do not meet targets for A1C, blood pressure, or lipids. 14% meet targets for all A1C, BP, lipids, and nonsmoking
Standards of Medical Care in Diabetes 2016 Care Delivery Systems 33-49% of patients still do not meet targets for A1C, blood pressure, or lipids. 14% meet targets for all A1C, BP, lipids, and nonsmoking
Diabetes: What is the scope of the problem?
 Diabetes: What is the scope of the problem? Elizabeth R. Seaquist MD Division of Endocrinology and Diabetes Department of Medicine Director, General Clinical Research Center Pennock Family Chair in Diabetes
Diabetes: What is the scope of the problem? Elizabeth R. Seaquist MD Division of Endocrinology and Diabetes Department of Medicine Director, General Clinical Research Center Pennock Family Chair in Diabetes
GLP-1 agonists. Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK
 GLP-1 agonists Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What do GLP-1 agonists do? Physiology of postprandial glucose regulation Meal ❶ ❷ Insulin Rising plasma
GLP-1 agonists Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What do GLP-1 agonists do? Physiology of postprandial glucose regulation Meal ❶ ❷ Insulin Rising plasma
Diabetes: Definition Pathophysiology Treatment Goals. By Scott Magee, MD, FACE
 Diabetes: Definition Pathophysiology Treatment Goals By Scott Magee, MD, FACE Disclosures No disclosures to report Definition of Diabetes Mellitus Diabetes Mellitus comprises a group of disorders characterized
Diabetes: Definition Pathophysiology Treatment Goals By Scott Magee, MD, FACE Disclosures No disclosures to report Definition of Diabetes Mellitus Diabetes Mellitus comprises a group of disorders characterized
Newer Drugs in the Management of Type 2 Diabetes Mellitus
 Newer Drugs in the Management of Type 2 Diabetes Mellitus Dr. C. Dinesh M. Naidu Professor of Pharmacology, Kamineni Institute of Medical Sciences, Narketpally. 1 Presentation Outline Introduction Pathogenesis
Newer Drugs in the Management of Type 2 Diabetes Mellitus Dr. C. Dinesh M. Naidu Professor of Pharmacology, Kamineni Institute of Medical Sciences, Narketpally. 1 Presentation Outline Introduction Pathogenesis
Pathogenesis of Type 2 Diabetes
 9/23/215 Multiple, Complex Pathophysiological Abnmalities in T2DM incretin effect gut carbohydrate delivery & absption pancreatic insulin secretion pancreatic glucagon secretion HYPERGLYCEMIA? Pathogenesis
9/23/215 Multiple, Complex Pathophysiological Abnmalities in T2DM incretin effect gut carbohydrate delivery & absption pancreatic insulin secretion pancreatic glucagon secretion HYPERGLYCEMIA? Pathogenesis
ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES
 ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES Pr. Michel KOMAJDA Institute of Cardiology - IHU ICAN Pitie Salpetriere Hospital - University Pierre and Marie Curie, Paris (France) DEFINITION A
ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES Pr. Michel KOMAJDA Institute of Cardiology - IHU ICAN Pitie Salpetriere Hospital - University Pierre and Marie Curie, Paris (France) DEFINITION A
Clinical Practice Guidelines for Diabetes Management
 Clinical Practice Guidelines for Diabetes Management Diabetes is a disease in which blood glucose levels are above normal. Over the years, high blood glucose damages nerves and blood vessels, which can
Clinical Practice Guidelines for Diabetes Management Diabetes is a disease in which blood glucose levels are above normal. Over the years, high blood glucose damages nerves and blood vessels, which can
Treatment Options for Diabetes: An Update
 Treatment Options for Diabetes: An Update A/Prof. Marg McGill Manager, Diabetes Centre Dr. Ted Wu Staff Specialist Endocrinologist Diabetes Centre Centre of Health Professional Education Education Provider
Treatment Options for Diabetes: An Update A/Prof. Marg McGill Manager, Diabetes Centre Dr. Ted Wu Staff Specialist Endocrinologist Diabetes Centre Centre of Health Professional Education Education Provider
Modified version focused on CCNC Quality Measures and Feedback Processes
 Executive Summary: Standards of Medical Care in Diabetes 2010 Modified version focused on CCNC Quality Measures and Feedback Processes See http://care.diabetesjournals.org/content/33/supplement_1/s11.full
Executive Summary: Standards of Medical Care in Diabetes 2010 Modified version focused on CCNC Quality Measures and Feedback Processes See http://care.diabetesjournals.org/content/33/supplement_1/s11.full
Abbreviations DPP-IV dipeptidyl peptidase IV DREAM Diabetes REduction Assessment with ramipril and rosiglitazone
 Index Abbreviations DPP-IV dipeptidyl peptidase IV DREAM Diabetes REduction Assessment with ramipril and rosiglitazone Medication GAD glutamic acid decarboxylase GLP-1 glucagon-like peptide 1 NPH neutral
Index Abbreviations DPP-IV dipeptidyl peptidase IV DREAM Diabetes REduction Assessment with ramipril and rosiglitazone Medication GAD glutamic acid decarboxylase GLP-1 glucagon-like peptide 1 NPH neutral
Antihyperglycemic Agents in Diabetes. Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014
 Antihyperglycemic Agents in Diabetes Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014 Objectives Review 2014 ADA Standards of Medical Care in DM as they
Antihyperglycemic Agents in Diabetes Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014 Objectives Review 2014 ADA Standards of Medical Care in DM as they
Diabetes Mellitus II CPG
 1 Diabetes Mellitus II CPG Candidates for Screening Integrated Complex Care Patients: Check Yearly Prediabetes: Check Yearly No Diabetes Mellitus (DM) Risk Factors: Check at Age 45, Repeat Every 3 Years
1 Diabetes Mellitus II CPG Candidates for Screening Integrated Complex Care Patients: Check Yearly Prediabetes: Check Yearly No Diabetes Mellitus (DM) Risk Factors: Check at Age 45, Repeat Every 3 Years
Management of Hyperglycemia in Type 2 Diabetes Celeste C. Thomas MD, MS
 Management of Hyperglycemia in Type 2 Diabetes Celeste C. Thomas MD, MS Disclosures In compliance with the accrediting board policies, the American Diabetes Association requires the following disclosure
Management of Hyperglycemia in Type 2 Diabetes Celeste C. Thomas MD, MS Disclosures In compliance with the accrediting board policies, the American Diabetes Association requires the following disclosure
Diabetes and the Heart
 Diabetes and the Heart Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 6, 2012 Outline Screening for diabetes in patients with CAD Screening for CAD in patients with
Diabetes and the Heart Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 6, 2012 Outline Screening for diabetes in patients with CAD Screening for CAD in patients with
Adult Diabetes Clinician Guide NOVEMBER 2017
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Adult Diabetes Clinician Guide Introduction NOVEMBER 2017 This evidence-based guideline summary is based on the 2017 KP National Diabetes Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Adult Diabetes Clinician Guide Introduction NOVEMBER 2017 This evidence-based guideline summary is based on the 2017 KP National Diabetes Guideline.
INJECTABLE THERAPY FOR THE TREATMENT OF DIABETES
 INJECTABLE THERAPY FOR THE TREATMENT OF DIABETES ARSHNA SANGHRAJKA DIABETES SPECIALIST PRESCRIBING PHARMACIST OBJECTIVES EXPLORE THE TYPES OF INSULIN AND INJECTABLE DIABETES TREATMENTS AND DEVICES AVAILABLE
INJECTABLE THERAPY FOR THE TREATMENT OF DIABETES ARSHNA SANGHRAJKA DIABETES SPECIALIST PRESCRIBING PHARMACIST OBJECTIVES EXPLORE THE TYPES OF INSULIN AND INJECTABLE DIABETES TREATMENTS AND DEVICES AVAILABLE
Early treatment for patients with Type 2 Diabetes
 Israel Society of Internal Medicine Kibutz Hagoshrim, June 22, 2012 Early treatment for patients with Type 2 Diabetes Eduard Montanya Hospital Universitari Bellvitge-IDIBELL CIBERDEM University of Barcelona
Israel Society of Internal Medicine Kibutz Hagoshrim, June 22, 2012 Early treatment for patients with Type 2 Diabetes Eduard Montanya Hospital Universitari Bellvitge-IDIBELL CIBERDEM University of Barcelona
Changing Diabetes: The time is now!
 Midwest Cardiovascular Research Foundation Welcomes DANITA HARRISON, ARNP Ms. Harrison discloses speaking relationships with Lilly, Novo Nordisk and Pfizer. Changing Diabetes: The time is now! Danita Harrison
Midwest Cardiovascular Research Foundation Welcomes DANITA HARRISON, ARNP Ms. Harrison discloses speaking relationships with Lilly, Novo Nordisk and Pfizer. Changing Diabetes: The time is now! Danita Harrison
9/28/2012. Sponsored By: NDSU College of Pharmacy, Nursing and Allied Sciences
 Sponsored By: NDSU College of Pharmacy, Nursing and Allied Sciences By PresenterMedia.com Faculty: Wendy Brown Pharm.D, PA-C, AE-C Associate Professor Pharmacy Practice About the Patient Clinical Coordinator
Sponsored By: NDSU College of Pharmacy, Nursing and Allied Sciences By PresenterMedia.com Faculty: Wendy Brown Pharm.D, PA-C, AE-C Associate Professor Pharmacy Practice About the Patient Clinical Coordinator
Non-insulin treatment in Type 1 DM Sang Yong Kim
 Non-insulin treatment in Type 1 DM Sang Yong Kim Chosun University Hospital Conflict of interest disclosure None Committee of Scientific Affairs Committee of Scientific Affairs Insulin therapy is the mainstay
Non-insulin treatment in Type 1 DM Sang Yong Kim Chosun University Hospital Conflict of interest disclosure None Committee of Scientific Affairs Committee of Scientific Affairs Insulin therapy is the mainstay
Disclosures. Diabetes and Cardiovascular Risk Management. Learning Objectives. Atherosclerotic Cardiovascular Disease
 Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Diabetic Nephropathy 2009
 Diabetic Nephropathy 2009 Michael T McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Diabetic Nephropathy Clinical Stages Hyperfunction
Diabetic Nephropathy 2009 Michael T McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Diabetic Nephropathy Clinical Stages Hyperfunction
Diabetes Mellitus: A Cardiovascular Disease
 Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
The ABCs (A1C, BP and Cholesterol) of Diabetes
 of Diabetes") The ABCs (A1C, BP and Cholesterol) of Diabetes Gregg Simonson, PhD Director, Professional Training and Consulting International Diabetes Center; Adjunct Assistant Professor, University of Minnesota Department
The ABCs (A1C, BP and Cholesterol) of Diabetes Gregg Simonson, PhD Director, Professional Training and Consulting International Diabetes Center; Adjunct Assistant Professor, University of Minnesota Department
Professor Rudy Bilous James Cook University Hospital
 Professor Rudy Bilous James Cook University Hospital Rate per 100 patient years Rate per 100 patient years 16 Risk of retinopathy progression 16 Risk of developing microalbuminuria 12 12 8 8 4 0 0 5 6
Professor Rudy Bilous James Cook University Hospital Rate per 100 patient years Rate per 100 patient years 16 Risk of retinopathy progression 16 Risk of developing microalbuminuria 12 12 8 8 4 0 0 5 6
Clinical Practice Guidelines
 Clinical Practice Guidelines Diabetes Objective The purpose is to guide the appropriate diagnosis and management of Diabetes. This guideline is designed to assist the clinician by providing a framework
Clinical Practice Guidelines Diabetes Objective The purpose is to guide the appropriate diagnosis and management of Diabetes. This guideline is designed to assist the clinician by providing a framework
Society for Ambulatory Anesthesia Consensus Statement on Perioperative Blood Glucose Management in Diabetic Patients Undergoing Ambulatory Surgery
 Society for Ambulatory Anesthesia Consensus Statement on Perioperative Blood Glucose Management in Diabetic Patients Undergoing Ambulatory Surgery Girish P. Joshi, MB BS, MD, FFARCSI Anesthesia & Analgesia
Society for Ambulatory Anesthesia Consensus Statement on Perioperative Blood Glucose Management in Diabetic Patients Undergoing Ambulatory Surgery Girish P. Joshi, MB BS, MD, FFARCSI Anesthesia & Analgesia
Management of Hyperglycemia in Type 2 Diabetes, 2015: A Patient-Centered Approach
 Management of Hyperglycemia in Type 2 Diabetes, 2015: A Patient-Centered Approach Update to a Position Statement of the American Diabetes Association (ADA) and the European Association f the Study of Diabetes
Management of Hyperglycemia in Type 2 Diabetes, 2015: A Patient-Centered Approach Update to a Position Statement of the American Diabetes Association (ADA) and the European Association f the Study of Diabetes
Pharmacology Updates. Quang T Nguyen, FACP, FACE, FTOS 11/18/17
 Pharmacology Updates Quang T Nguyen, FACP, FACE, FTOS 11/18/17 14 Classes of Drugs Available for the Treatment of Type 2 DM in the USA ### Class A1c Reduction Hypoglycemia Weight Change Dosing (times/day)
Pharmacology Updates Quang T Nguyen, FACP, FACE, FTOS 11/18/17 14 Classes of Drugs Available for the Treatment of Type 2 DM in the USA ### Class A1c Reduction Hypoglycemia Weight Change Dosing (times/day)
Diabetes Overview. How Food is Digested
 Diabetes Overview You are The Teacher, The Coach and the Fan Pathophysiology of Diabetes Complications Know the Numbers Treatment Can Good Control Make a Difference? Can Tight Control Be too Tight? How
Diabetes Overview You are The Teacher, The Coach and the Fan Pathophysiology of Diabetes Complications Know the Numbers Treatment Can Good Control Make a Difference? Can Tight Control Be too Tight? How
NEW DIABETES CARE MEDICATIONS
 NEW DIABETES CARE MEDICATIONS James Bonucchi DO, ECNU, FACE Adult Medicine and Endocrinology Specialists Disclosures Speakers bureau Sanofi AZ BI Diabetes Diabetes cost ADA 2017 data Ever increasing disorder.
NEW DIABETES CARE MEDICATIONS James Bonucchi DO, ECNU, FACE Adult Medicine and Endocrinology Specialists Disclosures Speakers bureau Sanofi AZ BI Diabetes Diabetes cost ADA 2017 data Ever increasing disorder.
Cardiovascular Management of a Patient with Diabetes
 Cardiovascular Management of a Patient with Diabetes Dr Jeremy Krebs Clinical Leader Endocrinology and Diabetes Wellington Hospital Summary People with diabetes take a lot of medication Compliance and
Cardiovascular Management of a Patient with Diabetes Dr Jeremy Krebs Clinical Leader Endocrinology and Diabetes Wellington Hospital Summary People with diabetes take a lot of medication Compliance and
Sitagliptin: first DPP-4 inhibitor to treat type 2 diabetes Steve Chaplin MSc, MRPharmS and Andrew Krentz MD, FRCP
 Sitagliptin: first DPP-4 inhibitor to treat type 2 diabetes Steve Chaplin MSc, MRPharmS and Andrew Krentz MD, FRCP KEY POINTS sitagliptin (Januvia) is a DPP-4 inhibitor that blocks the breakdown of the
Sitagliptin: first DPP-4 inhibitor to treat type 2 diabetes Steve Chaplin MSc, MRPharmS and Andrew Krentz MD, FRCP KEY POINTS sitagliptin (Januvia) is a DPP-4 inhibitor that blocks the breakdown of the
01/09/2017. Outline. SGLT 2 inhibitor? Diabetes Patients: Complex and Heterogeneous. Association between diabetes and cardiovascular events
 MICROVASCULAR COMPLICATIONS Incidence of outcome g 1 Cardioprotective Effects of SGLT2s Relevant for Which T2 Diabetes Patient? SGLT 2 inhibitor? 58 year old, waist circumference 5 cm, PMH: IHD On statin,
MICROVASCULAR COMPLICATIONS Incidence of outcome g 1 Cardioprotective Effects of SGLT2s Relevant for Which T2 Diabetes Patient? SGLT 2 inhibitor? 58 year old, waist circumference 5 cm, PMH: IHD On statin,
What s New on the Horizon: Diabetes Medication Update
 What s New on the Horizon: Diabetes Medication Update Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors, and what s coming Revised ADA/EASD and AACE guidelines:
What s New on the Horizon: Diabetes Medication Update Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors, and what s coming Revised ADA/EASD and AACE guidelines:
Current Diabetes Care for Internists:2011
 Current Diabetes Care for Internists:2011 Petch Rawdaree, DM, MSc, DLSHTM Faculty of Medicine Vajira Hospital University of Bangkok Metropolis 19 th January 2011 ก ก 1. ก ก ก ก 2. ก ก ก ก ก 3. ก ก ก ก
Current Diabetes Care for Internists:2011 Petch Rawdaree, DM, MSc, DLSHTM Faculty of Medicine Vajira Hospital University of Bangkok Metropolis 19 th January 2011 ก ก 1. ก ก ก ก 2. ก ก ก ก ก 3. ก ก ก ก
Old oral antidiabetic agents in the armamentarium of diabetes mellitus treatment: Safety and efficacy
 Old oral antidiabetic agents in the armamentarium of diabetes mellitus treatment: Safety and efficacy Melpomeni Peppa Assistant Professor of Endocrinology 2 nd Dept of Internal Medicine-Propaedeutic, Athens
Old oral antidiabetic agents in the armamentarium of diabetes mellitus treatment: Safety and efficacy Melpomeni Peppa Assistant Professor of Endocrinology 2 nd Dept of Internal Medicine-Propaedeutic, Athens
The Diabetes Link to Heart Disease
 The Diabetes Link to Heart Disease Anthony Abe DeSantis, MD September 18, 2015 University of WA Division of Metabolism, Endocrinology and Nutrition Oswald Toosweet Case #1 68 yo M with T2DM Diagnosed DM
The Diabetes Link to Heart Disease Anthony Abe DeSantis, MD September 18, 2015 University of WA Division of Metabolism, Endocrinology and Nutrition Oswald Toosweet Case #1 68 yo M with T2DM Diagnosed DM
Pancreatic b-cell Dysfunction in Type 2 Diabetes ZIAD KAHWASH, M.D. Insulin resistance: Defects in Insulin Signaling
 Plasma insulin (mu/ml) ZIAD KAHWASH, M.D. resistance: Defects in Signaling Increased glucose production Glucose Insufficient glucose disposal X Liver glucagon insulin Pancreas Peripheral tissues (skeletal
Plasma insulin (mu/ml) ZIAD KAHWASH, M.D. resistance: Defects in Signaling Increased glucose production Glucose Insufficient glucose disposal X Liver glucagon insulin Pancreas Peripheral tissues (skeletal
Scope. History. History. Incretins. Incretin-based Therapy and DPP-4 Inhibitors
 Plasma Glucose (mg/dl) Plasma Insulin (pmol/l) Incretin-based Therapy and Inhibitors Scope Mechanism of action ผศ.ดร.นพ.ว ระเดช พ ศประเสร ฐ สาขาว ชาโภชนว ทยาคล น ก ภาคว ชาอาย รศาสตร คณะแพทยศาสตร มหาว ทยาล
Plasma Glucose (mg/dl) Plasma Insulin (pmol/l) Incretin-based Therapy and Inhibitors Scope Mechanism of action ผศ.ดร.นพ.ว ระเดช พ ศประเสร ฐ สาขาว ชาโภชนว ทยาคล น ก ภาคว ชาอาย รศาสตร คณะแพทยศาสตร มหาว ทยาล
IDF Regions and global projections of the number of people with diabetes (20-79 years), 2013 and Diabetes Atlas -sixth Edition: IDF 2013
, 2013 and Diabetes Atlas -sixth Edition: IDF 2013") IDF Regions and global projections of the number of people with diabetes (20-79 years), 2013 and 2035 Diabetes Atlas -sixth Edition: IDF 2013 Diabetes Atlas -sixth Edition: IDF 2013 Chronic complications
IDF Regions and global projections of the number of people with diabetes (20-79 years), 2013 and 2035 Diabetes Atlas -sixth Edition: IDF 2013 Diabetes Atlas -sixth Edition: IDF 2013 Chronic complications
Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes. Overview. Prevalence of Overweight in the U.S.
 Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes Geneva Clark Briggs, PharmD, BCPS Overview Underlying defects with Type 2 diabetes Importance of managing postprandial glucose
Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes Geneva Clark Briggs, PharmD, BCPS Overview Underlying defects with Type 2 diabetes Importance of managing postprandial glucose
New and Emerging Therapies for Type 2 DM
 Dale Clayton MHSc, MD, FRCPC Dalhousie University/Capital Health April 28, 2011 New and Emerging Therapies for Type 2 DM The science of today, is the technology of tomorrow. Edward Teller American Physicist
Dale Clayton MHSc, MD, FRCPC Dalhousie University/Capital Health April 28, 2011 New and Emerging Therapies for Type 2 DM The science of today, is the technology of tomorrow. Edward Teller American Physicist
RCHC Clinical Guidelines Type 2 Diabetes; Adults
 RCHC Clinical Guidelines Type 2 Diabetes; Adults Screening for diabetes in asymptomatic adults 1 Population: Aged > 45 years; Aged < 45 years who are overweight (BMI> 25kg/m 2 ) and have an additional
RCHC Clinical Guidelines Type 2 Diabetes; Adults Screening for diabetes in asymptomatic adults 1 Population: Aged > 45 years; Aged < 45 years who are overweight (BMI> 25kg/m 2 ) and have an additional
What s New on the Horizon: Diabetes Medication Update. Michael Shannon, MD Providence Endocrinology, Olympia WA
 What s New on the Horizon: Diabetes Medication Update Michael Shannon, MD Providence Endocrinology, Olympia WA 1 Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors,
What s New on the Horizon: Diabetes Medication Update Michael Shannon, MD Providence Endocrinology, Olympia WA 1 Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors,
Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes
 Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes Geneva Clark Briggs, PharmD, BCPS Adjunct Professor at University of Appalachia College of Pharmacy Clinical Associate, Medical
Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes Geneva Clark Briggs, PharmD, BCPS Adjunct Professor at University of Appalachia College of Pharmacy Clinical Associate, Medical
Diabetes Oral Agents Pharmacology. University of Hawai i Hilo Pre-Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D
 Diabetes Oral Agents Pharmacology University of Hawai i Hilo Pre-Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 1 Learning Objectives Understand the role of the utilization of free
Diabetes Oral Agents Pharmacology University of Hawai i Hilo Pre-Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 1 Learning Objectives Understand the role of the utilization of free
STANDARDS OF MEDICAL CARE IN DIABETES 2012
 STANDARDS OF MEDICAL CARE IN DIABETES 2012 Section Table of Contents ADA Evidence Grading System of Clinical Recommendations Slide No. I. Classification and Diagnosis 4-11 II. Testing for Diabetes in Asymptomatic
STANDARDS OF MEDICAL CARE IN DIABETES 2012 Section Table of Contents ADA Evidence Grading System of Clinical Recommendations Slide No. I. Classification and Diagnosis 4-11 II. Testing for Diabetes in Asymptomatic
Diabesity. Metabolic dysfunction that ranges from mild blood glucose imbalance to full fledged Type 2 DM Signs
 Diabesity Metabolic dysfunction that ranges from mild blood glucose imbalance to full fledged Type 2 DM Signs Abdominal obesity Low HDL, high LDL, and high triglycerides HTN High blood glucose (F>100l,
Diabesity Metabolic dysfunction that ranges from mild blood glucose imbalance to full fledged Type 2 DM Signs Abdominal obesity Low HDL, high LDL, and high triglycerides HTN High blood glucose (F>100l,
Pharmacology Update for the Adult Patient - Newer Oral Medications for Diabetes
 Pharmacology Update for the Adult Patient - Newer Oral Medications for Diabetes Brooke Hudspeth, PharmD, CDE, MLDE Director of Diabetes Prevention, Kroger Pharmacy Adjunct Assistant Professor, University
Pharmacology Update for the Adult Patient - Newer Oral Medications for Diabetes Brooke Hudspeth, PharmD, CDE, MLDE Director of Diabetes Prevention, Kroger Pharmacy Adjunct Assistant Professor, University
CURRENT CONTROVERSIES IN DIABETES CARE
 CURRENT CONTROVERSIES IN DIABETES CARE Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Diabetes Mellitus: U.S. Impact
CURRENT CONTROVERSIES IN DIABETES CARE Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Diabetes Mellitus: U.S. Impact
What s New in Diabetes Treatment. Disclosures
 What s New in Diabetes Treatment Shiri Levy M.D. Henry Ford Hospital Senior Staff Physician Service Chief, West Bloomfield Hospital Endocrinology, Metabolism, Bone and Mineral Disorders Disclosures None
What s New in Diabetes Treatment Shiri Levy M.D. Henry Ford Hospital Senior Staff Physician Service Chief, West Bloomfield Hospital Endocrinology, Metabolism, Bone and Mineral Disorders Disclosures None
Update on Diabetes Mellitus
 Update on Diabetes Mellitus Treatment: Targeting the Incretin System Overview Underlying defects with Type 2 diabetes Importance of managing postprandial glucose control Amylin Incretin Hormones New therapies
Update on Diabetes Mellitus Treatment: Targeting the Incretin System Overview Underlying defects with Type 2 diabetes Importance of managing postprandial glucose control Amylin Incretin Hormones New therapies
Age-adjusted Percentage of U.S. Adults Who Were Obese or Who Had Diagnosed Diabetes
 Age-adjusted Percentage of U.S. Adults Who Were Obese or Who Had Diagnosed Diabetes Obesity (BMI 30 kg/m 2 ) 1994 2000 2009 No Data 26.0% Diabetes 1994 2000 2009
Age-adjusted Percentage of U.S. Adults Who Were Obese or Who Had Diagnosed Diabetes Obesity (BMI 30 kg/m 2 ) 1994 2000 2009 No Data 26.0% Diabetes 1994 2000 2009
Diabetes mellitus. Treatment
 Diabetes mellitus Treatment Recommended glycemic targets for the clinical management of diabetes(ada) Fasting glycemia: 80-110 mg/dl Postprandial : 100-145 mg/dl HbA1c: < 6,5 % Total cholesterol: < 200
Diabetes mellitus Treatment Recommended glycemic targets for the clinical management of diabetes(ada) Fasting glycemia: 80-110 mg/dl Postprandial : 100-145 mg/dl HbA1c: < 6,5 % Total cholesterol: < 200
My Journey in Endocrinology. Samuel Cataland M.D
 My Journey in Endocrinology Samuel Cataland M.D. 1968-2015 Drs Berson M.D. Yalow phd Insulin Radioimmunoassay Nobel Prize Physiology or Medicine 1977 Rosalyn Yalow: Radioimmunoassay Technology Andrew Schally
My Journey in Endocrinology Samuel Cataland M.D. 1968-2015 Drs Berson M.D. Yalow phd Insulin Radioimmunoassay Nobel Prize Physiology or Medicine 1977 Rosalyn Yalow: Radioimmunoassay Technology Andrew Schally
Agenda. Indications Different insulin preparations Insulin initiation Insulin intensification
 Insulin Therapy F. Hosseinpanah Obesity Research Center Research Institute for Endocrine sciences Shahid Beheshti University of Medical Sciences November 11, 2017 Agenda Indications Different insulin preparations
Insulin Therapy F. Hosseinpanah Obesity Research Center Research Institute for Endocrine sciences Shahid Beheshti University of Medical Sciences November 11, 2017 Agenda Indications Different insulin preparations
What s New in Diabetes Medications. Jena Torpin, PharmD
 What s New in Diabetes Medications Jena Torpin, PharmD 1 Objectives Discuss new medications in the management of diabetes Understand the mechanism of the medications discussed Understand the side effects
What s New in Diabetes Medications Jena Torpin, PharmD 1 Objectives Discuss new medications in the management of diabetes Understand the mechanism of the medications discussed Understand the side effects
Clinical Overview of Combination Therapy with Sitagliptin and Metformin
 Clinical Overview of Combination Therapy with Sitagliptin and Metformin 1 Contents Pathophysiology of type 2 diabetes and mechanism of action of sitagliptin Clinical data overview of sitagliptin: Monotherapy
Clinical Overview of Combination Therapy with Sitagliptin and Metformin 1 Contents Pathophysiology of type 2 diabetes and mechanism of action of sitagliptin Clinical data overview of sitagliptin: Monotherapy
Joslin Diabetes Center Joslin Diabetes Forum 2013: The Impact of Comorbidities on Glucose Control Scenario 2: Reduced Renal Function
 Scenario 2: Reduced Renal Function 62 y.o. white man with type 2 diabetes for 18 years Hypertension and hypercholesterolemia Known proliferative retinopathy Current medications: Metformin 1000 mg bid Glyburide
Scenario 2: Reduced Renal Function 62 y.o. white man with type 2 diabetes for 18 years Hypertension and hypercholesterolemia Known proliferative retinopathy Current medications: Metformin 1000 mg bid Glyburide
Executive Summary: Standards of Medical Care in Diabetes 2010
 E X E C U T I V E S U M M A R Y Executive Summary: Standards of Medical Care in Diabetes 2010 Current criteria for the diagnosis of diabetes A1C 6.5%: The test should be performed in a laboratory using
E X E C U T I V E S U M M A R Y Executive Summary: Standards of Medical Care in Diabetes 2010 Current criteria for the diagnosis of diabetes A1C 6.5%: The test should be performed in a laboratory using
YOU HAVE DIABETES. Angie O Connor Community Diabetes Nurse Specialist 25th September 2013
 YOU HAVE DIABETES Angie O Connor Community Diabetes Nurse Specialist 25th September 2013 Predicated 2015 figures are already met 1 in 20 have diabetes:1in8 over 60years old Definite Diagnosis is key Early
YOU HAVE DIABETES Angie O Connor Community Diabetes Nurse Specialist 25th September 2013 Predicated 2015 figures are already met 1 in 20 have diabetes:1in8 over 60years old Definite Diagnosis is key Early
GLP-1 (glucagon-like peptide-1) Agonists (Byetta, Bydureon, Tanzeum, Trulicity, Victoza ) Step Therapy and Quantity Limit Criteria Program Summary
 Agonists (Byetta, Bydureon, Tanzeum, Trulicity, Victoza ) Step Therapy and Quantity Limit Criteria Program Summary") OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) s (Byetta/exenatide, Bydureon/ exenatide extended-release, Tanzeum/albiglutide, Trulicity/dulaglutide, and Victoza/liraglutide) Step Therapy
OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) s (Byetta/exenatide, Bydureon/ exenatide extended-release, Tanzeum/albiglutide, Trulicity/dulaglutide, and Victoza/liraglutide) Step Therapy
9/12/2014. Main Pathophysiological Defect in T1DM. Main Pathophysiological Defects in T2DM. Personalizing Diabetes Care: The Alphabet Soup of Options
 9/12/2014 Baptist Health South Florida 13th Annual Primary Focus Symposium June 28, 2014 Silvio Inzucchi MD Section of Endocrinology Yale University School of Medicine Half-Century of HTN & T2DM Medications
9/12/2014 Baptist Health South Florida 13th Annual Primary Focus Symposium June 28, 2014 Silvio Inzucchi MD Section of Endocrinology Yale University School of Medicine Half-Century of HTN & T2DM Medications
Diabetes and New Meds for Cardiovascular Risk Reduction. F. Dwight Chrisman, MD, FACC. Disclosures: BI Boehringer Ingelheim speaker
 Diabetes and New Meds for Cardiovascular Risk Reduction F. Dwight Chrisman, MD, FACC Disclosures: BI Boehringer Ingelheim speaker 1 Prevalence of DM DM state specific prevalence 2006 4%-6% 6-8% 8-10% 10-12%
Diabetes and New Meds for Cardiovascular Risk Reduction F. Dwight Chrisman, MD, FACC Disclosures: BI Boehringer Ingelheim speaker 1 Prevalence of DM DM state specific prevalence 2006 4%-6% 6-8% 8-10% 10-12%
T2DM is a global epidemic with
 : a new option for the management of type 2 diabetes Marc Evans MRCP, MD, Consultant Diabetologist, Llandough Hospital, Cardiff Incretin-based therapies for the treatment of diabetes mellitus (T2DM) present
: a new option for the management of type 2 diabetes Marc Evans MRCP, MD, Consultant Diabetologist, Llandough Hospital, Cardiff Incretin-based therapies for the treatment of diabetes mellitus (T2DM) present
Pre-diabetes. Pharmacological Approaches to Delay Progression to Diabetes
 Pre-diabetes Pharmacological Approaches to Delay Progression to Diabetes Overview Definition of Pre-diabetes Risk Factors for Pre-diabetes Clinical practice guidelines for diabetes Management, including
Pre-diabetes Pharmacological Approaches to Delay Progression to Diabetes Overview Definition of Pre-diabetes Risk Factors for Pre-diabetes Clinical practice guidelines for diabetes Management, including
Incretinas e inhibidores de la DPP-4. Dr. Ramon Gomis Hospital Clínic Barcelona
 Incretinas e inhibidores de la DPP-4 Dr. Ramon Gomis Hospital Clínic Barcelona El páncreas normal y el islote de Langerhans lóbulos conducto intralobulillar islote vaso Islote de Langerhans Adaptado de
Incretinas e inhibidores de la DPP-4 Dr. Ramon Gomis Hospital Clínic Barcelona El páncreas normal y el islote de Langerhans lóbulos conducto intralobulillar islote vaso Islote de Langerhans Adaptado de
New Treatments for Type 2 diabetes. Nandini Seevaratnam April 2016 Rushcliffe Patient Forum
 New Treatments for Type 2 diabetes Nandini Seevaratnam April 2016 Rushcliffe Patient Forum Overview Growing population of Type 2 diabetes Basic science on what goes wrong Current treatments Why there is
New Treatments for Type 2 diabetes Nandini Seevaratnam April 2016 Rushcliffe Patient Forum Overview Growing population of Type 2 diabetes Basic science on what goes wrong Current treatments Why there is
DISCLOSURES. Learning objectives NAVIGATING THE TREATMENT OF TYPE 2 DIABETES: WHAT S NEW? Investigator Initiated Trial Support:
 NAVIGATING THE TREATMENT OF TYPE 2 DIABETES: WHAT S NEW? Jane E-B Reusch MD Professor of Medicine, Biochemistry and Bioengineering Associate Director Center for Women s Health Research University of Colorado
NAVIGATING THE TREATMENT OF TYPE 2 DIABETES: WHAT S NEW? Jane E-B Reusch MD Professor of Medicine, Biochemistry and Bioengineering Associate Director Center for Women s Health Research University of Colorado
MOA: Long acting glucagon-like peptide 1 receptor agonist
 Alexandria Rydz MOA: Long acting glucagon-like peptide 1 receptor agonist Increases glucose dependent insulin secretion Decreases inappropriate glucagon secretion Increases β- cell growth and replication
Alexandria Rydz MOA: Long acting glucagon-like peptide 1 receptor agonist Increases glucose dependent insulin secretion Decreases inappropriate glucagon secretion Increases β- cell growth and replication