Individualizing Therapy int2dm With Insulin
|
|
|
- Lionel Tyler
- 5 years ago
- Views:
Transcription
1 Individualizing Therapy int2dm With Insulin Etie Moghissi, MD, FACP, FACE Clinical Associate Professor University of California, Los Angeles Los Angeles, California
2 OBJECTIVES: At the conclusion of this activity, participants should be able to: Compare the pharmacodynamic and therapeutic characteristics of ultralong-acting basal insulins with those of previously approved insulins Calculate appropriate doses of ultralong-acting basal insulin for patients with and without prior insulin treatment Identify simplified, patient-centered treatment regimens incorporating ultralong-acting insulin for advancing therapy in patients with T2DM
3 T2DM Is a Progressive Disease Glucose, mg/dl Prediabetes (obesity, IFG, IGT) Diabetes diagnosis Postmeal glucose Fasting glucose Relative Amount β-cell failure Insulin resistance Insulin level T2DM onset Years Disease progression occurs no matter how well patients self-manage: insulin therapy should not be used as a threat or described as failure Kendall DM, et al. Am J Med. 2009;122(6 suppl):s37-s50; Kendall DM, et al. Am J Manag Care. 2001;7(suppl):S327-S343; DeFronzo RA. Diabetes. 2009;58: ; Inzucchi SE, et al. Diabetes Care. 2015;38: ; American Diabetes Association. Diabetes Care. 2016;39(suppl 1):S1-S112.
4 Insulin Is the Universal Agent for Achieving Glycemic Control At diagnosis 1 In combination with non-insulin agents 2-5 In long-duration disease 3,6 Benefit especially likely in: Treatment-naive individuals with hyperglycemic symptoms and A1C > 9% Latent autoimmune diabetes in adults (LADA) Individuals with hyperlipidemia and/or hypertension Recommended for use in combination with most other major classes of antihyperglycemic agents Combinations reduce glycemic variability compared with insulin-only regimens Loss of β-cell function is inevitable as T2DM progresses With appropriate dose adjustment, insulin can be used in any patient (including those with comorbidities that preclude the use of other agents) 1. Owens DR. Diabetes Technol Ther. 2013;15: ; 2. Drugs@FDA. Accessed October 11, 2015; 3. American Diabetes Association. Diabetes Care. 2016;39(suppl 1):S1-S112; 4. Garber AJ, et al. Endocr Pract. 2016;22:84-113; 5. Hirsch IB, et al. Diabetes. 2015;64(suppl 1):A100 [abstract 385-OR]; 6. Lebovitz HE. Diabetes Rev. 1999;7:
5 Benefits and Limitations of Early Initiation of Insulin Therapy vs Conventional Care Benefit: Rapid normalization of blood glucose levels Benefit: Reduces risk of progression from prediabetes to T2DM Benefit: Consistently better long-term glycemic control Benefit: Reduces risk of microvascular complications if A1C > 6.4% Benefit: No increased CVD risk Limitation: Increased risk of severe hypoglycemia Hanefeld M, et al. Diabetes Ther Feb 10. [Epub ahead of print]/
6 Current Options Among Insulin Products Type Basal Insulins Prandial Insulins Premixed Insulins Human 1 U-100 NPH U-100 regular human insulin (RHI) U-500 RHI Technosphere inhaled insulin U /30 RHI Analogue 1 U-100 glargine U-100 glargine equivalent a U-100 detemir U-100 degludec U-200 degludec U-300 glargine U-100 lispro U-100 aspart U-100 glulisine U-200 lispro U /50 lispro U /30 aspart U /25 lispro U /30 degludec/aspart All recently approved insulins are only available in pens 1,e; red text denotes which insulins are only available in prefilled pens Analogue insulins are associated with less hypoglycemia than human insulins, although these differences are not always statistically significant 2 a In the US, U-100 glargine equivalent is not approved as a biosimilar product Drugs@FDA. Accessed January 8, 2016; 2. Singh SR, et al. CMAJ. 2009;180:
7 New slide Insulins Are Available in 4 Different Concentrations Concentrations and Number of Units per Container 1 Concentration Units/mL Units/Vial Units/Pen U a 300 b U Not available in vials U Not available in vials 600 b 450 c U ,000 d 1500 c Insulin pens significantly reduce the risk of dosing errors and hypoglycemic events 2 Pens completely eliminate the need for converting doses based on the volume of insulin injected Dosing errors with U-500 insulin vials are especially dangerous, but pens are now available 3,e a 10 units/vial; b 3 ml/pen; c 1.5 ml/pen; d 20 units/vial; e given the potential for a 5-fold higher insulin dose relative to the same volume of a U-100 insulin. 1. Drugs@FDA Newton C, et al. AACE Annual Meeting [abstract 271]. 3. Segal AR, et al. Am J Health Syst Pharm. 2010;67:
8 Comparing the Therapeutic Characteristics of Older and Newer Basal Insulins
9 Pharmacodynamic Profile of a Hypothetical Ideal Basal Insulin 400 Glucose, mg/dl Time 06:00 10:00 14:00 18:00 22:00 02:00 06:00 An ideal basal insulin would yield a flat glucose profile throughout the day, on different days, and in different people 1,2 1. Zinman B. N Engl J Med. 1989;321: Garber AJ. Diabetes Obes Metab. 2014;16:
10 Ultralong-Acting Basal Insulins Have Minimal Glycemic Variability GIR, mg/kg/min U-300 glargine 1,a Average glucose infusion rate (GIR) Time, h Period 1 Period 2 GIR, μmol/kg/min Older Basals 3,b NPH Detemir Glargine Blood Glucose Level, mmol/l U-100 degludec 2 a 2-period crossover study in T1DM; n = 50. b 3-period crossover study in T2DM. Individual patient profiles Mean profile Time Since Injection, h Time, h 1. Becker RH, et al. Diabetes Obes Metab. 2015;17: Haahr H, Heise T. Clin Pharmacokinet. 2014;53: Porcellati F, et al. Diabetes Care. 2011;34:
11

12
13
14
15
16
17

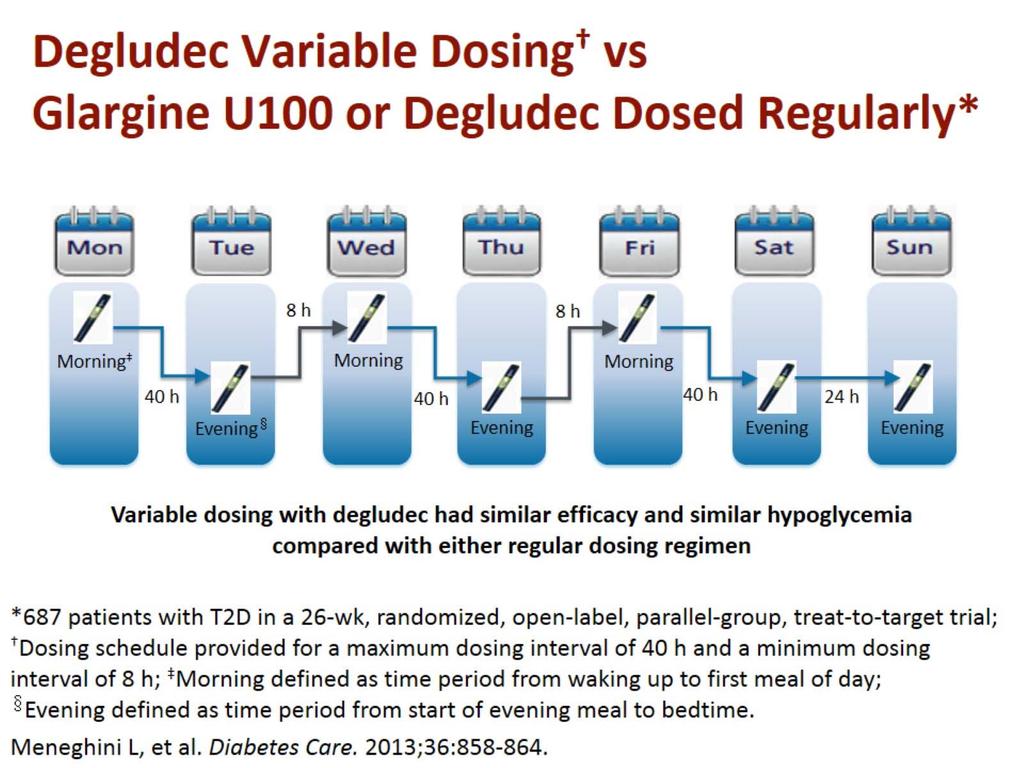
18 Trial Design SWITCH Reduce pre-trial insulin dose (basal and bolus) by 20% at V2 Reduce Treatment period A insulin dose (basal and bolus) by 20% at V34 T1DM patients currently on NPH or IDet OD or BID plus bolus IDeg once daily + IAsp 2-4 times daily IDeg once daily + IAsp 2-4 times daily IGlar once daily + IAsp 2-4 times daily IGlar once daily + IAsp 2-4 times daily Discontinue at V2 Treatment period A Treatment period B V1 V2 V34 V66 V67 Screening (0-2 weeks) switch Randomisation 1:1 16 weeks 16 weeks washout periodmaintenance period Crossover 16 weeks washout period 16 weeks maintenance period Follow-up (at least 1 week) 18
19 Results: Switch 1 Hypos during the maintenance period per 100 patient years Severe OR Severe OR % Sever e Rate of BG +Sx Conf BG Noc conf Severe Degludec Glargine Stats SS SS SS SS RRR 11% 36% 35%

20


 Equivalent insulin dose (0.42 vs 0.")



21 Efficacy and Safety of U-100 Glargine Equivalent (LY ) vs U-100 Glargine in Insulin-naive Patients With T2DM a Overall Hypoglycemia b Nocturnal Hypoglycemia c Severe Hypoglycemia d P = NS P = NS P = NS Equivalent change in A1C ( 1.48% vs 1.54%, LY vs GLAR, P = NS) Equivalent insulin dose (0.42 vs 0.44 U/kg, LY vs GLAR, P = NS) Equivalent weight gain (2.0 vs 2.2 kg, LY vs GLAR, P = NS) a n = 221 (LY), n = 236 (GLAR), mean age = 58 y, duration of diabetes = 11 y, BL A1C = %, BL wt = kg, BL BMI = 32 kg/m 2 ; b plasma glucose 70 mg/dl or sign or symptom of hypoglycemia; c between bedtime and waking; d requiring assistance, baseline to month 6. Rosenstock J, et al. Diabetes Obes Metab. 2015;17:
22 Summary U-100 Glargine Equivalent 100 units/ml Biologically equivalent to U- 100 glargine Compared with U-100 glargine: Equally effective Equivalent hypoglycemia Equivalent weight gain U-300 Glargine 300 units/ml Same molecule as U-100 glargine but more concentrated Compared with U-100 glargine: Equally effective Less hypoglycemia a Equivalent weight gain U-100 and U-200 Degludec 100 or 200 units/ml Novel molecular configuration Compared with U-100 glargine a : Equally effective Less hypoglycemia b Equivalent weight gain U-100 glargine equivalent has the same therapeutic characteristics as U-100 glargine Ultralong-acting basal insulins have a flatter time-action profile, with less glycemic variability, and may be less likely to cause hypoglycemia than first-generation insulin analogues a Significantly less overall hypoglycemia in insulin-naive patients. b Significantly less nocturnal hypoglycemia in insulin-naive patients.
23 Meet Maria History & Vital Signs Woman, white 56 years old T2DM for 6 years Height: 5 ft 1 in Weight: 152 lb BMI: 28.7 kg/m 2 BP: 138/80 mm Hg Heart rate: 112 beats/minute (bpm) Current Medications Glycemic control Metformin XR: 2000 mg/d Glimepiride: 4 mg/d Other medications ACE inhibitor Statin Laboratory Results Fasting plasma glucose (FPG): 178 mg/dl A1C: 9.1% Lipids: Within normal limits (WNL) egfr: 72 ml/min/1.73 m 2 Liver function tests (LFTs): WNL Increasing A1C over past 2 years, despite increased dose of sulfonylurea Admits to missing her medication 1 day per week due to irregular schedule and work-related travel Has had minor hypoglycemia with glimepiride and would like to avoid going through that again Is hesitant but willing to consider adding insulin to her regimen if necessary
24 Initiating and Titrating Newer Ultralong- Acting Basal Insulins
25 Guideline Recommendations for Initiating and Titrating Basal Insulin in Patients With T2DM Initial dose Titration ADA/EASD Guidelines 10 U/d or U/kg 10%-15% or 2-4 U once or twice weekly to fasting blood glucose (FBG) of mg/dl Hypoglycemia: determine and address cause; reduce dose by the greater of 4 U or 10%-20% Once-daily basal insulin, with injection timing based on patient s schedule and glucose profile, is a convenient way to initiate insulin American Diabetes Association. Diabetes Care. 2016;39(suppl 1):S1-S112.
26 Guidance for Initiating and Titrating Newer Basal Insulins: U-100 or U-200 Degludec 1 Starting Dose of U-100 or U-200 Degludec in Insulin-Naive Patients 10 U, once daily Starting Dose of U-100 or U-200 Degludec in Patients Switching From Another Basal Insulin U-100 glargine U-100 detemir U-100 NPH Same dose 1 ; consider 20% dose reduction if switching from twice-daily basal insulin dosing 2 U-100 degludec Same dose for U-100 and U-200 U-300 glargine Injection time Titration step Not specified (but 20% reduction may be prudent) Once daily, any time ( 8 h since last dose) Calculate average FPG from the preceding 2 days, compare with goal: Uptitrate by 2 U if above goal Maintain dose if at goal Downtitrate by 2 U if below goal Max. titration frequency Dwell time 3-4 days, 1 but no more than weekly may be better 2 6 seconds 1. Drugs@FDA. Scripts/cder/DrugsatFDA. Accessed January 8, Vora J, et al. Diabetes Res Clin Pract. 2015;109:19-31.
 After injecting, keep the needle in the skin")
27 Insulin Pens Can Improve Outcomes and Are Associated With Lower Risks of Dosing Errors and Hypoglycemia Than Vial-and-Syringe Insulin Human insulins are generally administered with a vial and syringe Analogue insulins are generally administered with a pen Patient copayments for pens may be the same as for vials Use the shortest possible needles ( 8 mm) After injecting, keep the needle in the skin for the recommended dwell time Rotate sites to avoid lipohypertrophy Perez-Nieves M, et al. Curr Med Res Opin. 2015;31: ; Molife C, et al. Diabetes Technol Ther. 2009;11: ; Aetna Aetna Pharmacy Plan Drug List. Accessed January 27, 2016; Becton Dickinson Diabetes. Step by step injection guide. Accessed January 27, 2016; Frid A, et al. Diabetes Metab. 2010;36(suppl 1):S3-S18; Drugs@FDA. Accessed January 8, 2016.
28 Meet Joe History & Vital Signs Man, black 67 years old T2DM, 12 years Myocardial infarction, 11 years ago Height: 5 ft 9 in Weight: 217 lb BMI: 32 kg/m 2 BP: 144/80 mm Hg Heart rate: 78 bpm Current Medications Glycemic control Metformin XR: 2000 mg/d Sitagliptin: 100 mg/d U-100 glargine: 80 U/d, AM injection Other medications ARB and HCTZ Statin Aspirin Laboratory Results FPG: 175 mg/dl SMBG: mg/dl A1C: 8.5% Lipids: WNL egfr: 62 ml/min/1.73 m 2 LFTs ALT: 65 U/mL AST: 42 U/mL Recognizes that his FPG is not where it should be but doesn t want to increase his insulin dose because the injection volume is already uncomfortably large Does not want to split the insulin to AM and PM doses because he s a musician and is often busy in the evening, playing with his band
29 Simplifying Intensification of Basal Insulin Therapy in T2DM
30 Overview of Therapeutic Characteristics of New and Emerging Prandial Insulins U-200 lispro (approved) 1,2 Inhaled insulin (approved) 2,3 Faster-acting aspart (submitted) 4,5 Bioequivalent to U-100 lispro 1 Time-action characteristics similar to U-100 lispro 1,2 Prefilled pen injector 2 Concentration permits smaller injection volume 2 Much faster and shorter acting than subcutaneous (SC) insulins (variable bioavailability, inconsistent dosing effect) 2 Not as effective as SC but less weight gain 3 Significantly less severe hypoglycemia 3 Limit use to nonsmokers without pulmonary disease 2,3 Greater glucose-lowering effect within 90 minutes after dosing vs currently available aspart 4,a Significantly lower PPG for faster-acting aspart vs currently available aspart 5,b a Randomized, 3-way crossover study in 52 adults with T1DM. b Randomized trial in 43 adults with T1DM treated with continuous subcutaneous insulin infusion. 1. de la Peña A, et al. Clin Pharmacol Drug Dev. 2016;5: Drugs@FDA. Scripts/cder/DrugsatFDA. Accessed January 8, Pittas AG, et al. Lancet Diabetes Endocrinol. 2015;3: Heise T, et al. Diabetes Obes Metab. 2015;17: Bode B, et al. Diabetes. 2015;64(suppl 1):A253 [abstract 994-P].
31 Treatment Algorithms for Advancing Beyond Basal Insulin Therapy Have Been Updated ADA/EASD: consider a trial of a GLP-1 receptor agonist 1 AACE/ACE: consider a GLP-1 receptor agonist, an SGLT2 inhibitor, or a DPP-4 inhibitor 2 Approval Status for Use of GLP-1 receptor agonists in Combination With Insulin Agent Basal Prandia l Albiglutide mg QW 3 Dulaglutide mg QW 3 Exenatide 5-10 μg BID 3 Exenatide 2 mg QW 3 Liraglutide mg QD 3 Lixisenatide (NDA accepted by US FDA) 4 X X X See note 5,6 X Not Recommended X Note: Has been tested in combination with insulin glargine. 5,6 1. American Diabetes Association. Diabetes Care. 2016;39(suppl 1):S1-S112; 2. Garber AJ, et al. Endocr Pract. 2016;22:84-113; 3. Drugs@FDA. Accessed January 27, 2016; 4. Sanofi. Review-by-FDA. Accessed January 27, 2016; 5. Riddle MC, et al. Diabetes Care. 2013;36: ; 6. Meier JJ, et al. Diabetes Care. 2015;38:
32 Shared Decision-Making Points for Comparing a GLP-1 Receptor Agonist vs a Prandial Insulin Analogue Aspect of Care Number of additional injections, per week Dose adjustment for meals required? Dose adjustment for exercise required? Glucose monitoring needed multiple times daily? GLP-1 Receptor Agonist (GLP-1 RA) Prandial Insulin Analogue 1to 14 7to 21 No No No Yes Yes Yes Drugs@FDA. Scripts/cder/DrugsatFDA. Accessed January 8, 2016.




33 Investigational Coformulations of Basal Insulin and a GLP-1 RA Offer Potential for Intensifying Basal Insulin Therapy With a Single Daily Injection Coformulated a Liraglutide +Degludec 1,b vs Degludec vs Liraglutide Coformulated a Lixisenatide + Glargine 2,c vs Glargine Composite endpoint: A1C < 7% without weight gain or hypoglycemia a Not US FDA approved; b Baseline A1C, 8.3%; Baseline Wt, 87 kg; 26 weeks; c Baseline A1C, 8.0%; BL BMI, 32.1 kg/m 2 ; 24 weeks; * P <.0001 vs DEG; P <.0001 vs LIRA; P <.05 vs PBO + GLAR. All baseline characteristics stated as means values. 1. Gough SC, et al. Lancet Diabetes Endocrinol. 2014;2: Rosenstock J, et al. Diabetologia. 2014;57(suppl 1):S108 [abstract 241].
34 Summary U-100 Glargine Equivalent 100 units/ml Biologically equivalent to U- 100 glargine Compared with U-100 glargine: Equally effective Equivalent hypoglycemia Equivalent weight gain U-300 Glargine 300 units/ml Same molecule as U-100 glargine but more concentrated Compared with U-100 glargine: Equally effective Less hypoglycemia a Equivalent weight gain U-100 and U-200 Degludec 100 or 200 units/ml Novel molecular configuration Compared with U-100 glargine a : Equally effective Less hypoglycemia b Equivalent weight gain U-100 glargine equivalent has the same therapeutic characteristics as U-100 glargine Ultralong-acting basal insulins have a flatter time-action profile, with less glycemic variability, and may be less likely to cause hypoglycemia than first-generation insulin analogues a Significantly less overall hypoglycemia in insulin-naive patients. b Significantly less nocturnal hypoglycemia in insulin-naive patients.
35 Summary Prandial Insulins Improve glycemic control Greatest flexibility Stepwise initiation minimizes risks of hypoglycemia and weight gain Premixed insulin may be an appropriate alternative for some patients GLP-1 Receptor Agonists Improve glycemic control Potentially fewer daily injections than prandial insulin Low risks of hypoglycemia or weight gain Prescribing limitations in some patients
36 Summary Most patients with T2DM will eventually need insulin therapy Insulin is recommended throughout the progression of T2DM Earlier insulin use is associated with better long-term glycemic control than postponed insulin use With appropriate dose adjustment, insulin can be used alone or in combination with other antihyperglycemic agents in essentially all patients Insulin offers unmatched flexibility to individualize glycemic control, with 18 products in 7 different time-action categories
What s My Line? Identifying the Role of New Ultralong- Acting Insulins for the Treatment of T2DM
 What s My Line? Identifying the Role of New Ultralong- Acting Insulins for the Treatment of TDM Learning Objectives. Compare the pharmacodynamics and therapeutic characteristics of ultralong-acting basal
What s My Line? Identifying the Role of New Ultralong- Acting Insulins for the Treatment of TDM Learning Objectives. Compare the pharmacodynamics and therapeutic characteristics of ultralong-acting basal
Individualizing Therapy in T2DM With Insulin
 Developed by the Institute for Individualizing Therapy in TDM With Insulin Davida F Kruger, MSN, APN-BC, BC-ADM Certified Nurse Practitioner Division of Endocrinology, Diabetes, and Bone and Mineral Disorders
Developed by the Institute for Individualizing Therapy in TDM With Insulin Davida F Kruger, MSN, APN-BC, BC-ADM Certified Nurse Practitioner Division of Endocrinology, Diabetes, and Bone and Mineral Disorders
Individualizing Therapy int2dm With Insulin
 Individualizing Therapy int2dm With Insulin Etie Moghissi, MD, FACP, FACE Clinical Associate Professor University of California, Los Angeles Los Angeles, California OBJECTIVES: At the conclusion of this
Individualizing Therapy int2dm With Insulin Etie Moghissi, MD, FACP, FACE Clinical Associate Professor University of California, Los Angeles Los Angeles, California OBJECTIVES: At the conclusion of this
Beyond Basal Insulin: Intensification of Therapy Jennifer D Souza, PharmD, CDE, BC-ADM
 Beyond Basal Insulin: Intensification of Therapy Jennifer D Souza, PharmD, CDE, BC-ADM Disclosures Jennifer D Souza has no conflicts of interest to disclose. 2 When Basal Insulin Is Not Enough Learning
Beyond Basal Insulin: Intensification of Therapy Jennifer D Souza, PharmD, CDE, BC-ADM Disclosures Jennifer D Souza has no conflicts of interest to disclose. 2 When Basal Insulin Is Not Enough Learning
New basal insulins Are they any better? Matthew C. Riddle, MD Professor of Medicine Oregon Health & Science University Keystone Colorado 15 July 2011
 New basal insulins Are they any better? Matthew C. Riddle, MD Professor of Medicine Oregon Health & Science University Keystone Colorado 15 July 2011 Presenter Disclosure I have received the following
New basal insulins Are they any better? Matthew C. Riddle, MD Professor of Medicine Oregon Health & Science University Keystone Colorado 15 July 2011 Presenter Disclosure I have received the following
Timely!Insulinization In!Type!2! Diabetes,!When!and!How
 Timely!Insulinization In!Type!2! Diabetes,!When!and!How, FACP, FACE, CDE Professor of Internal Medicine UT Southwestern Medical Center Dallas, Texas Current Control and Targets 1 Treatment Guidelines for
Timely!Insulinization In!Type!2! Diabetes,!When!and!How, FACP, FACE, CDE Professor of Internal Medicine UT Southwestern Medical Center Dallas, Texas Current Control and Targets 1 Treatment Guidelines for
Update on Insulin-based Agents for T2D. Harry Jiménez MD, FACE
 Update on Insulin-based Agents for T2D Harry Jiménez MD, FACE Harry Jiménez MD, FACE Has received honorarium as Speaker and/or Consultant for the following pharmaceutical companies: Eli Lilly Merck Boehringer
Update on Insulin-based Agents for T2D Harry Jiménez MD, FACE Harry Jiménez MD, FACE Has received honorarium as Speaker and/or Consultant for the following pharmaceutical companies: Eli Lilly Merck Boehringer
UKPDS: Over Time, Need for Exogenous Insulin Increases
 UKPDS: Over Time, Need for Exogenous Insulin Increases Patients Requiring Additional Insulin (%) 60 40 20 Oral agents By 6 Chlorpropamide years, Glyburide more than 50% of UKPDS patients required insulin
UKPDS: Over Time, Need for Exogenous Insulin Increases Patients Requiring Additional Insulin (%) 60 40 20 Oral agents By 6 Chlorpropamide years, Glyburide more than 50% of UKPDS patients required insulin
Newer Insulins. Boca Raton Regional Hospital 15th Annual Internal Medicine Conference
 Newer Insulins Boca Raton Regional Hospital 15th Annual Internal Medicine Conference Luigi F. Meneghini, MD, MBA Professor of Internal Medicine, UT Southwestern Medical Center Executive Director, Global
Newer Insulins Boca Raton Regional Hospital 15th Annual Internal Medicine Conference Luigi F. Meneghini, MD, MBA Professor of Internal Medicine, UT Southwestern Medical Center Executive Director, Global
Update on Insulin-based Agents for T2D
 Update on Insulin-based Agents for T2D Injectable Therapies for Type 2 Diabetes Mellitus (T2DM) and Obesity This presentation will: Describe established and newly available insulin therapies for treatment
Update on Insulin-based Agents for T2D Injectable Therapies for Type 2 Diabetes Mellitus (T2DM) and Obesity This presentation will: Describe established and newly available insulin therapies for treatment
5/16/2018. Insulin Update: New and Emerging Insulins. Disclosures to Participants. Learning Objectives
 Insulin Update: New and Emerging Insulins Joshua J. Neumiller, PharmD, CDE, FASCP Vice Chair & Associate Professor, Department of Pharmacotherapy Washington State University Spokane, WA Disclosures to
Insulin Update: New and Emerging Insulins Joshua J. Neumiller, PharmD, CDE, FASCP Vice Chair & Associate Professor, Department of Pharmacotherapy Washington State University Spokane, WA Disclosures to
Basal & GLP-1 Fixed Combination Use
 Basal & GLP-1 Fixed Combination Use Michelle M. Mangual, MD Diplomate of the American board of Internal Medicine and Endocrinology, Diabetes and Metabolism San Juan City hospital Learning Objectives o
Basal & GLP-1 Fixed Combination Use Michelle M. Mangual, MD Diplomate of the American board of Internal Medicine and Endocrinology, Diabetes and Metabolism San Juan City hospital Learning Objectives o
What's New in Insulin Related Therapies 2018
 What's New in Insulin Related Therapies 2018 James Lenhard, MD (JLenhard@ChristianaCare.org) Section Chief, Endocrinology and Metabolism Christiana Care Health System Newark, DE Disclosures Speaker:Eli
What's New in Insulin Related Therapies 2018 James Lenhard, MD (JLenhard@ChristianaCare.org) Section Chief, Endocrinology and Metabolism Christiana Care Health System Newark, DE Disclosures Speaker:Eli
Injectable Agents for Type 2 Diabetes. Richard Christensen, MD AACE Diabetes Day, Boise, ID September 2017
 Injectable Agents for Type 2 Diabetes Richard Christensen, MD AACE Diabetes Day, Boise, ID September 2017 Financial Disclosures Sanofi speaker honoraria No other relevant financial disclosures Injectable
Injectable Agents for Type 2 Diabetes Richard Christensen, MD AACE Diabetes Day, Boise, ID September 2017 Financial Disclosures Sanofi speaker honoraria No other relevant financial disclosures Injectable
Insulin Initiation and Intensification. Disclosure. Objectives
 Insulin Initiation and Intensification Neil Skolnik, M.D. Associate Director Family Medicine Residency Program Abington Memorial Hospital Professor of Family and Community Medicine Temple University School
Insulin Initiation and Intensification Neil Skolnik, M.D. Associate Director Family Medicine Residency Program Abington Memorial Hospital Professor of Family and Community Medicine Temple University School
MYTH VS FACT #1: GLP-1 RECEPTOR AGONISTS SHOULD BE RESERVED FOR PATIENTS WITH LONG-STANDING T2DM
 15 mins for presentation & ARS MYTH VS FACT #1: GLP-1 RECEPTOR AGONISTS SHOULD BE RESERVED FOR PATIENTS WITH LONG-STANDING T2DM Carol Hatch Wysham, MD Clinical Associate Professor of Medicine University
15 mins for presentation & ARS MYTH VS FACT #1: GLP-1 RECEPTOR AGONISTS SHOULD BE RESERVED FOR PATIENTS WITH LONG-STANDING T2DM Carol Hatch Wysham, MD Clinical Associate Professor of Medicine University
INSULIN 101: When, How and What
 INSULIN 101: When, How and What Alice YY Cheng @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form
INSULIN 101: When, How and What Alice YY Cheng @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form
These Aren t Your Average Rookies: A Primer on New and Emerging Insulins. Alissa R. Segal, Pharm.D, CDE, CDTC, FCCP
 These Aren t Your Average Rookies: A Primer on New and Emerging Insulins Alissa R. Segal, Pharm.D, CDE, CDTC, FCCP Disclosures Eli Lilly & Company: Advisory board member Boehringer Ingelheim: Advisory
These Aren t Your Average Rookies: A Primer on New and Emerging Insulins Alissa R. Segal, Pharm.D, CDE, CDTC, FCCP Disclosures Eli Lilly & Company: Advisory board member Boehringer Ingelheim: Advisory
Faculty. Concentrated Insulin: Examining the Necessity of Newer Insulins for In-Hospital Diabetes Management. Disclosures. Learning Objectives
 Examining the Necessity of Newer Insulins for In-Hospital Diabetes Management Faculty Susan Cornell, PharmD, CDE, FAPhA, FAADE Associate Professor of Pharmacy Practice Associate Director of Experiential
Examining the Necessity of Newer Insulins for In-Hospital Diabetes Management Faculty Susan Cornell, PharmD, CDE, FAPhA, FAADE Associate Professor of Pharmacy Practice Associate Director of Experiential
COPYRIGHT. Advancing to Insulin Replacement Therapy: When, Why, and How? Update in Internal Medicine December 5, Richard S.
 Advancing to Insulin Replacement Therapy: When, Why, and How? Update in Internal Medicine - 2016 December 5, 2016 Richard S. Beaser, MD Medical Director, Professional Education Joslin Diabetes Center Associate
Advancing to Insulin Replacement Therapy: When, Why, and How? Update in Internal Medicine - 2016 December 5, 2016 Richard S. Beaser, MD Medical Director, Professional Education Joslin Diabetes Center Associate
Individualising Insulin Regimens: Premixed or basal plus/bolus?
 Individualising Insulin Regimens: Premixed or basal plus/bolus? Dr. Ted Wu Director, Diabetes Centre, Hospital Sydney, Australia Turkey, April 2015 Centre of Health Professional Education Optimising insulin
Individualising Insulin Regimens: Premixed or basal plus/bolus? Dr. Ted Wu Director, Diabetes Centre, Hospital Sydney, Australia Turkey, April 2015 Centre of Health Professional Education Optimising insulin
Natural History of Type 2 Diabetes
 Key Points About Insulin to Discuss Today We should be using insulin earlier in the natural history of type 2 diabetes How early and how do we know when to start insulin? Barriers to insulin therapy Goals
Key Points About Insulin to Discuss Today We should be using insulin earlier in the natural history of type 2 diabetes How early and how do we know when to start insulin? Barriers to insulin therapy Goals
Application of the Diabetes Algorithm to a Patient
 Application of the Diabetes Algorithm to a Patient Apply knowledge gained from this activity to improve disease management and outcomes for patients with T2DM and obesity Note: The cases in this deck represent
Application of the Diabetes Algorithm to a Patient Apply knowledge gained from this activity to improve disease management and outcomes for patients with T2DM and obesity Note: The cases in this deck represent
Agenda. Indications Different insulin preparations Insulin initiation Insulin intensification
 Insulin Therapy F. Hosseinpanah Obesity Research Center Research Institute for Endocrine sciences Shahid Beheshti University of Medical Sciences November 11, 2017 Agenda Indications Different insulin preparations
Insulin Therapy F. Hosseinpanah Obesity Research Center Research Institute for Endocrine sciences Shahid Beheshti University of Medical Sciences November 11, 2017 Agenda Indications Different insulin preparations
What s New? An Antihyperglycemic Medications Update
 What s New? An Antihyperglycemic Medications Update WADE 2016 Annual Conference Josh Neumiller, PharmD, CDE, FASCP Associate Professor Department of Pharmacotherapy Washington State University Disclosures
What s New? An Antihyperglycemic Medications Update WADE 2016 Annual Conference Josh Neumiller, PharmD, CDE, FASCP Associate Professor Department of Pharmacotherapy Washington State University Disclosures
Initiating Injectable Therapy in Type 2 Diabetes
 Initiating Injectable Therapy in Type 2 Diabetes David Doriguzzi, PA C Learning Objectives To understand current Diabetes treatment guidelines To understand how injectable medications fit into current
Initiating Injectable Therapy in Type 2 Diabetes David Doriguzzi, PA C Learning Objectives To understand current Diabetes treatment guidelines To understand how injectable medications fit into current
Optimizing Treatment Strategies to Improve Patient Outcomes in the Management of Type 2 Diabetes
 Optimizing Treatment Strategies to Improve Patient Outcomes in the Management of Type 2 Diabetes Philip Raskin, MD Professor of Medicine The University of Texas, Southwestern Medical Center NAMCP Spring
Optimizing Treatment Strategies to Improve Patient Outcomes in the Management of Type 2 Diabetes Philip Raskin, MD Professor of Medicine The University of Texas, Southwestern Medical Center NAMCP Spring
Learning Objectives. Are you ready for more insulin formulations?
 Are you ready for more insulin formulations? Shara Elrod, PharmD, BCACP, BCGP Learning Objectives Review pharmacology and dosing of new insulin formulations Compare and contrast new insulin formulations
Are you ready for more insulin formulations? Shara Elrod, PharmD, BCACP, BCGP Learning Objectives Review pharmacology and dosing of new insulin formulations Compare and contrast new insulin formulations
Update on New Basal Insulins and Combinations: Starting, Titrating and Adding to Therapy
 Update on New Basal Insulins and Combinations: Starting, Titrating and Adding to Therapy Jerry Meece, BPharm, CDE, FACA, FAADE Director of Clinical Services Plaza Pharmacy and Wellness Center Gainesville,
Update on New Basal Insulins and Combinations: Starting, Titrating and Adding to Therapy Jerry Meece, BPharm, CDE, FACA, FAADE Director of Clinical Services Plaza Pharmacy and Wellness Center Gainesville,
Comprehensive Diabetes Treatment
 Comprehensive Diabetes Treatment Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism The George Washington University School of Medicine Diabetes
Comprehensive Diabetes Treatment Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism The George Washington University School of Medicine Diabetes
The New Age of Insulin: Exploring the Latest Trends in Insulin Therapy. The New Age of Insulin: Exploring the Latest Trends in Insulin Therapy
 The New Age of Insulin: Exploring the Latest Trends in Insulin Therapy Susan Cornell, PharmD, CDE, FAPhA, FAADE Associate Director of Experiential Education Associate Professor of Pharmacy Practice Midwestern
The New Age of Insulin: Exploring the Latest Trends in Insulin Therapy Susan Cornell, PharmD, CDE, FAPhA, FAADE Associate Director of Experiential Education Associate Professor of Pharmacy Practice Midwestern
Progressive Loss of β-cell Function in T2DM
 Disclaimer This slide deck in its original and unaltered format is for educational purposes and is current as of November 2015. The content and views presented in this educational activity are those of
Disclaimer This slide deck in its original and unaltered format is for educational purposes and is current as of November 2015. The content and views presented in this educational activity are those of
9/8/2016. Faculty. Examining the Role of Long-Acting Insulin within the Physiologic Approach to Glucose Control. Disclosures. Learning Objectives
 9/8/21 Faculty Examining the Role of Long-Acting within the Physiologic Approach to Glucose Control Dace Trence, MD, FACE Professor, Division of Metabolism, Endocrinology and Nutrition Director, Diabetes
9/8/21 Faculty Examining the Role of Long-Acting within the Physiologic Approach to Glucose Control Dace Trence, MD, FACE Professor, Division of Metabolism, Endocrinology and Nutrition Director, Diabetes
Advances in Outpatient Diabetes Care: Algorithms for Care and the Role of Injectable Therapies. Module D
 Advances in Outpatient Diabetes Care: Algorithms for Care and the Role of Injectable Therapies Module D 1 Learning Objectives Apply the principles of the comprehensive diabetes algorithms to patients with
Advances in Outpatient Diabetes Care: Algorithms for Care and the Role of Injectable Therapies Module D 1 Learning Objectives Apply the principles of the comprehensive diabetes algorithms to patients with
Tips and Tricks for Starting and Adjusting Insulin. MC MacSween The Moncton Hospital
 Tips and Tricks for Starting and Adjusting Insulin MC MacSween The Moncton Hospital Progression of type 2 diabetes Beta cell apoptosis Natural History of Type 2 Diabetes The Burden of Treatment Failure
Tips and Tricks for Starting and Adjusting Insulin MC MacSween The Moncton Hospital Progression of type 2 diabetes Beta cell apoptosis Natural History of Type 2 Diabetes The Burden of Treatment Failure
T2DM and Need for Insulin. Insulin Pharmacokinetics. When To Start Insulin in T2DM. FDA-approved Insulins for Subcutaneous Injection
 Plasma Insulin Levels Patients Requiring Insulin (%) Effective Use of Insulin in the Primary Care Practice: Insulin Therapy Initiation, Intensification, and the Insulinizing Complex Patients with T2DM:
Plasma Insulin Levels Patients Requiring Insulin (%) Effective Use of Insulin in the Primary Care Practice: Insulin Therapy Initiation, Intensification, and the Insulinizing Complex Patients with T2DM:
Pharmacology Updates. Quang T Nguyen, FACP, FACE, FTOS 11/18/17
 Pharmacology Updates Quang T Nguyen, FACP, FACE, FTOS 11/18/17 14 Classes of Drugs Available for the Treatment of Type 2 DM in the USA ### Class A1c Reduction Hypoglycemia Weight Change Dosing (times/day)
Pharmacology Updates Quang T Nguyen, FACP, FACE, FTOS 11/18/17 14 Classes of Drugs Available for the Treatment of Type 2 DM in the USA ### Class A1c Reduction Hypoglycemia Weight Change Dosing (times/day)
nocturnal hypoglycemia percentage of Hispanics in the insulin glargine than NPH during forced patients who previously This study excluded
 Clinical Trial Design/ Primary Objective Insulin glargine Treat-to-Target Trial, Riddle et al., 2003 (23) AT.LANTUS trial, Davies et al., 2005 (24) INSIGHT trial, Gerstein et al., 2006 (25) multicenter,
Clinical Trial Design/ Primary Objective Insulin glargine Treat-to-Target Trial, Riddle et al., 2003 (23) AT.LANTUS trial, Davies et al., 2005 (24) INSIGHT trial, Gerstein et al., 2006 (25) multicenter,
INSULIN THERAY دکتر رحیم وکیلی استاد غدد ومتابولیسم کودکان دانشگاه علوم پزشکی مشهد
 INSULIN THERAY DIABETES1 IN TYPE دکتر رحیم وکیلی استاد غدد ومتابولیسم کودکان دانشگاه علوم پزشکی مشهد Goals of management Manage symptoms Prevent acute and late complications Improve quality of life Avoid
INSULIN THERAY DIABETES1 IN TYPE دکتر رحیم وکیلی استاد غدد ومتابولیسم کودکان دانشگاه علوم پزشکی مشهد Goals of management Manage symptoms Prevent acute and late complications Improve quality of life Avoid
A Practical Approach to the Use of Diabetes Medications
 A Practical Approach to the Use of Diabetes Medications Juan Pablo Frias, M.D., FACE President, National Research Institute, Los Angles, CA Clinical Faculty, University of California, San Diego, CA OUTLINE
A Practical Approach to the Use of Diabetes Medications Juan Pablo Frias, M.D., FACE President, National Research Institute, Los Angles, CA Clinical Faculty, University of California, San Diego, CA OUTLINE
ADA and AACE Glycemic Targets
 ADA and AACE Glycemic Targets HbA1C target should be individualized based on a number of factors including: Age Life expectancy Comorbidities Duration of diabetes Risk of hypoglycemia Patient motivation
ADA and AACE Glycemic Targets HbA1C target should be individualized based on a number of factors including: Age Life expectancy Comorbidities Duration of diabetes Risk of hypoglycemia Patient motivation
Early treatment for patients with Type 2 Diabetes
 Israel Society of Internal Medicine Kibutz Hagoshrim, June 22, 2012 Early treatment for patients with Type 2 Diabetes Eduard Montanya Hospital Universitari Bellvitge-IDIBELL CIBERDEM University of Barcelona
Israel Society of Internal Medicine Kibutz Hagoshrim, June 22, 2012 Early treatment for patients with Type 2 Diabetes Eduard Montanya Hospital Universitari Bellvitge-IDIBELL CIBERDEM University of Barcelona
Insulin Initiation, titration & Insulin switch in the Primary Care-KISS
 Insulin Initiation, titration & Insulin switch in the Primary Care-KISS Rotorua GP CME 9 June 2012 Dr Kingsley Nirmalaraj FRACP Endocrinologist, BOPDHB & Suite 9, Promed House, Tenth Ave, Tauranga Linda
Insulin Initiation, titration & Insulin switch in the Primary Care-KISS Rotorua GP CME 9 June 2012 Dr Kingsley Nirmalaraj FRACP Endocrinologist, BOPDHB & Suite 9, Promed House, Tenth Ave, Tauranga Linda
New Drug Evaluation: Insulin degludec/aspart, subcutaneous injection
 New Drug Evaluation: Insulin degludec/aspart, subcutaneous injection Date of Review: March 2016 End Date of Literature Search: November 11, 2015 Generic Name: Insulin degludec and insulin aspart Brand
New Drug Evaluation: Insulin degludec/aspart, subcutaneous injection Date of Review: March 2016 End Date of Literature Search: November 11, 2015 Generic Name: Insulin degludec and insulin aspart Brand
Insulin Bootcamp: Dosing, Monitoring, Titrating, and Care Coordination. Stuart T. Haines, Pharm.D., BCPS, BCACP, BC ADM
 Insulin Bootcamp: Dosing, Monitoring, Titrating, and Care Coordination Stuart T. Haines, Pharm.D., BCPS, BCACP, BC ADM University of Mississippi School of Pharmacy Joshua J. Neumiller, Pharm.D., CDE, FAADE,
Insulin Bootcamp: Dosing, Monitoring, Titrating, and Care Coordination Stuart T. Haines, Pharm.D., BCPS, BCACP, BC ADM University of Mississippi School of Pharmacy Joshua J. Neumiller, Pharm.D., CDE, FAADE,
Achieving and maintaining good glycemic control is an
 Glycemic Efficacy, Weight Effects, and Safety of Once-Weekly Glucagon-Like Peptide-1 Receptor Agonists Yehuda Handelsman, MD, FACP, FNLA, FASPC, MACE; Kathleen Wyne, MD, PhD, FACE, FNLA; Anthony Cannon,
Glycemic Efficacy, Weight Effects, and Safety of Once-Weekly Glucagon-Like Peptide-1 Receptor Agonists Yehuda Handelsman, MD, FACP, FNLA, FASPC, MACE; Kathleen Wyne, MD, PhD, FACE, FNLA; Anthony Cannon,
Your Chart Review Data. Lara Zisblatt, MA Assistant Director Continuing Medical Education Boston University School of Medicine
 Your Chart Review Data Lara Zisblatt, MA Assistant Director Continuing Medical Education Boston University School of Medicine Participation 243 registered for the program 98 have completed the Practice
Your Chart Review Data Lara Zisblatt, MA Assistant Director Continuing Medical Education Boston University School of Medicine Participation 243 registered for the program 98 have completed the Practice
Faculty. Timothy S. Reid, MD (Co-Chair, Presenter) Medical Director Mercy Diabetes Center Janesville, WI
 Medical Director Mercy Diabetes Center Janesville, WI") Activity Overview In this case-based webcast, meet Jackie, a 62-year-old woman with type 2 diabetes. Her glycated hemoglobin (HbA1C) is 9.2%, and she is taking 2 oral agents and basal insulin; however,
Activity Overview In this case-based webcast, meet Jackie, a 62-year-old woman with type 2 diabetes. Her glycated hemoglobin (HbA1C) is 9.2%, and she is taking 2 oral agents and basal insulin; however,
Emerging Challenges in Primary Care: Safely Achieving Goals in Type 2 Diabetes (T2D): The Role of Concentrated and Long-Acting Insulins
: The Role of Concentrated and Long-Acting Insulins") Emerging Challenges in Primary Care: 2018 Safely Achieving Goals in Type 2 Diabetes (T2D): The Role of Concentrated and Long-Acting Insulins 1 Faculty Rodolfo J. Galindo, MD Assistant Professor of Medicine
Emerging Challenges in Primary Care: 2018 Safely Achieving Goals in Type 2 Diabetes (T2D): The Role of Concentrated and Long-Acting Insulins 1 Faculty Rodolfo J. Galindo, MD Assistant Professor of Medicine
MYTH VS FACT #1: GLP-1 RECEPTOR AGONISTS SHOULD BE RESERVED FOR PATIENTS WITH LONG-STANDING T2DM
 9:45 11: AM Separating Myth from Fact: The Role of Receptor Agonists for the Treatment of T2DM SPEAKERS James R. Gavin, III, MD, PhD John E. Anderson, MD Presenter Disclosure Information The following
9:45 11: AM Separating Myth from Fact: The Role of Receptor Agonists for the Treatment of T2DM SPEAKERS James R. Gavin, III, MD, PhD John E. Anderson, MD Presenter Disclosure Information The following
9/29/ Disclosure. Learning Objectives. Diabetes Update: Guidelines, Treatment Options & Trends
 + Diabetes Update: Guidelines, Treatment Options & Trends Melissa Max, PharmD, BC-ADM, CDE Assistant Professor of Pharmacy Practice Harding University College of Pharmacy + Disclosure Conflicts Of Interest
+ Diabetes Update: Guidelines, Treatment Options & Trends Melissa Max, PharmD, BC-ADM, CDE Assistant Professor of Pharmacy Practice Harding University College of Pharmacy + Disclosure Conflicts Of Interest
The Many Faces of T2DM in Long-term Care Facilities
 The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
Drug List. Drug List (cont d) Objectives. Case and Initial CME Questions. Presenter Disclosure Information
 Objectives. Case and Initial CME Questions. Presenter Disclosure Information") :3 :5 PM How to Select and Initiate Insulin Therapy in the Type Diabetes Patient SPEAKERS Intekhab Ahmed, MD, FACE, FACP Felice Caldarella, MD, FACE, FACP, CDE Presenter Disclosure Information The following
:3 :5 PM How to Select and Initiate Insulin Therapy in the Type Diabetes Patient SPEAKERS Intekhab Ahmed, MD, FACE, FACP Felice Caldarella, MD, FACE, FACP, CDE Presenter Disclosure Information The following
Diabetes: Three Core Deficits
 Diabetes: Three Core Deficits Fat Cell Dysfunction Impaired Incretin Function Impaired Appetite Suppression Obesity and Insulin Resistance in Muscle and Liver Hyperglycemia Impaired Insulin Secretion Islet
Diabetes: Three Core Deficits Fat Cell Dysfunction Impaired Incretin Function Impaired Appetite Suppression Obesity and Insulin Resistance in Muscle and Liver Hyperglycemia Impaired Insulin Secretion Islet
6/5/18. Emerging Challenges in Primary Care: Safely Achieving Goals in Type 2 Diabetes (T2D): The Role of Concentrated and Long- Acting Insulins
: The Role of Concentrated and Long- Acting Insulins") Emerging Challenges in Primary Care: 218 Safely Achieving Goals in Type 2 Diabetes (T2D): The Role of Concentrated and Long- Acting Insulins Faculty Rodolfo J. Galindo, MD Assistant Professor of Medicine
Emerging Challenges in Primary Care: 218 Safely Achieving Goals in Type 2 Diabetes (T2D): The Role of Concentrated and Long- Acting Insulins Faculty Rodolfo J. Galindo, MD Assistant Professor of Medicine
The first stop for professional medicines advice
 London Medicines Evaluation Network Overview: Glucagon-Like Peptide-1 receptor analogues The first stop for professional medicines advice 1 London Medicines Evaluation Network Overview: Glucagon-Like Peptide-1
London Medicines Evaluation Network Overview: Glucagon-Like Peptide-1 receptor analogues The first stop for professional medicines advice 1 London Medicines Evaluation Network Overview: Glucagon-Like Peptide-1
What s New in Type 2 Diabetes? 2018 Diabetes Updates
 What s New in Type 2 Diabetes? 2018 Diabetes Updates Gretchen Ray, PharmD, PhC, BCACP, CDE Associate Professor, UNM College of Pharmacy January 28, 2018 gray@salud.unm.edu OBJECTIVES Describe the most
What s New in Type 2 Diabetes? 2018 Diabetes Updates Gretchen Ray, PharmD, PhC, BCACP, CDE Associate Professor, UNM College of Pharmacy January 28, 2018 gray@salud.unm.edu OBJECTIVES Describe the most
Quando l insulina basale non basta più: differenti e nuove strategie terapeutiche
 Quando l insulina basale non basta più: differenti e nuove strategie terapeutiche Giorgio Sesti Università Magna Graecia di Catanzaro Potenziali conflitti di interesse Il Prof Giorgio Sesti dichiara di
Quando l insulina basale non basta più: differenti e nuove strategie terapeutiche Giorgio Sesti Università Magna Graecia di Catanzaro Potenziali conflitti di interesse Il Prof Giorgio Sesti dichiara di
5/16/2018. Insulin Workshop. Disclosures to Participants. Learning Objectives. This presentation will cover the following learning objectives:
 Insulin Workshop Joshua J. Neumiller, PharmD, CDE, FASCP Vice Chair & Associate Professor, Department of Pharmacotherapy Washington State University Spokane, WA Holly Divine, PharmD, BCACP, BCGP, CDE,
Insulin Workshop Joshua J. Neumiller, PharmD, CDE, FASCP Vice Chair & Associate Professor, Department of Pharmacotherapy Washington State University Spokane, WA Holly Divine, PharmD, BCACP, BCGP, CDE,
Medical therapy advances London/Manchester RCP February/June 2016
 Medical therapy advances London/Manchester RCP February/June 2016 Advances in medical therapies for diabetes mellitus Duality of interest: The speaker or institutions with which he is associated has received
Medical therapy advances London/Manchester RCP February/June 2016 Advances in medical therapies for diabetes mellitus Duality of interest: The speaker or institutions with which he is associated has received
Combatting T2DM Clinical Inertia: Evaluating the Evidence For Simultaneous Basal Insulin and GLP 1 Receptor Agonists
 Combatting T2DM Clinical Inertia: Evaluating the Evidence For Simultaneous Basal Insulin and GLP 1 Receptor Agonists Developed in Collaboration Instructions to Receive Credit To receive credit for your
Combatting T2DM Clinical Inertia: Evaluating the Evidence For Simultaneous Basal Insulin and GLP 1 Receptor Agonists Developed in Collaboration Instructions to Receive Credit To receive credit for your
Initiation and Titration of Insulin in Diabetes Mellitus Type 2
 Initiation and Titration of Insulin in Diabetes Mellitus Type 2 Greg Doelle MD, MS April 6, 2016 Disclosure I have no actual or potential conflicts of interest in relation to the content of this lecture.
Initiation and Titration of Insulin in Diabetes Mellitus Type 2 Greg Doelle MD, MS April 6, 2016 Disclosure I have no actual or potential conflicts of interest in relation to the content of this lecture.
A New Basal Insulin Option: The BEGIN Trials in Patients With Type 2 Diabetes
 A New Basal Insulin Option: The BEGIN Trials in Patients With Type 2 Diabetes Reviewed by Dawn Battise, PharmD STUDIES Initiating insulin degludec (study A): Zinman B, Philis-Tsimikas A, Cariou B, Handelsman
A New Basal Insulin Option: The BEGIN Trials in Patients With Type 2 Diabetes Reviewed by Dawn Battise, PharmD STUDIES Initiating insulin degludec (study A): Zinman B, Philis-Tsimikas A, Cariou B, Handelsman
Incredible Incretins Abby Frye, PharmD, BCACP
 Incredible Incretins Abby Frye, PharmD, BCACP Objectives & Disclosures Review the pathophysiology of T2DM and the impact of the incretin system Describe the defining characteristics of the available glucagonlike
Incredible Incretins Abby Frye, PharmD, BCACP Objectives & Disclosures Review the pathophysiology of T2DM and the impact of the incretin system Describe the defining characteristics of the available glucagonlike
Diabetes and Chronic Kidney Disease DR. JEREMY GILBERT, MD FRCPC ASSISTANT PROFESSOR, U OF T
 Diabetes and Chronic Kidney Disease DR. JEREMY GILBERT, MD FRCPC ASSISTANT PROFESSOR, U OF T Objectives Recognize the impact that CKD has on diabetes management Review the current Canadian Diabetes Association
Diabetes and Chronic Kidney Disease DR. JEREMY GILBERT, MD FRCPC ASSISTANT PROFESSOR, U OF T Objectives Recognize the impact that CKD has on diabetes management Review the current Canadian Diabetes Association
INSULIN INITIATION AND INTENSIFICATION WITH A FOCUS ON HYPOGLYCEMIA REDUCTION
 INSULIN INITIATION AND INTENSIFICATION WITH A FOCUS ON HYPOGLYCEMIA REDUCTION Jaiwant Rangi, MD, FACE Nov 10 th 2018 DISCLOSURES Speaker Novo Nordisk Sanofi-Aventis Boheringer Ingleheim Merck Abbvie Abbott
INSULIN INITIATION AND INTENSIFICATION WITH A FOCUS ON HYPOGLYCEMIA REDUCTION Jaiwant Rangi, MD, FACE Nov 10 th 2018 DISCLOSURES Speaker Novo Nordisk Sanofi-Aventis Boheringer Ingleheim Merck Abbvie Abbott
Diabetes Update: Intensifying Insulin Therapy Nuts, Bolts and Other Items
 Diabetes Update: Intensifying Insulin Therapy Nuts, Bolts and Other Items Hayley A. Miller, MD Physician, Internal Medicine, Diabetes and Metabolism, Sandy Clinic, Intermountain Healthcare Objectives:
Diabetes Update: Intensifying Insulin Therapy Nuts, Bolts and Other Items Hayley A. Miller, MD Physician, Internal Medicine, Diabetes and Metabolism, Sandy Clinic, Intermountain Healthcare Objectives:
Insulin glargine U300 (Toujeo ) and insulin glargine biosimilar (Abasaglar )
 and insulin glargine biosimilar (Abasaglar )") Insulin glargine U300 (Toujeo ) and insulin glargine biosimilar (Abasaglar ) Lead author: Stephen Erhorn Regional Drug & Therapeutics Centre (Newcastle) November 2015 2015 Summary Toujeo uses the same
Insulin glargine U300 (Toujeo ) and insulin glargine biosimilar (Abasaglar ) Lead author: Stephen Erhorn Regional Drug & Therapeutics Centre (Newcastle) November 2015 2015 Summary Toujeo uses the same
Chief of Endocrinology East Orange General Hospital
 Targeting the Incretins System: Can it Improve Our Ability to Treat Type 2 Diabetes? Darshi Sunderam, MD Darshi Sunderam, MD Chief of Endocrinology East Orange General Hospital Age-adjusted Percentage
Targeting the Incretins System: Can it Improve Our Ability to Treat Type 2 Diabetes? Darshi Sunderam, MD Darshi Sunderam, MD Chief of Endocrinology East Orange General Hospital Age-adjusted Percentage
GLP-1 agonists. Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK
 GLP-1 agonists Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What do GLP-1 agonists do? Physiology of postprandial glucose regulation Meal ❶ ❷ Insulin Rising plasma
GLP-1 agonists Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What do GLP-1 agonists do? Physiology of postprandial glucose regulation Meal ❶ ❷ Insulin Rising plasma
Intensifying Treatment Beyond Monotherapy in T2DM: Where Do Newer Therapies Fit?
 Intensifying Treatment Beyond Monotherapy in T2DM: Where Do Newer Therapies Fit? Vanita R. Aroda, MD Scientific Director & Physician Investigator MedStar Community Clinical Research Center MedStar Health
Intensifying Treatment Beyond Monotherapy in T2DM: Where Do Newer Therapies Fit? Vanita R. Aroda, MD Scientific Director & Physician Investigator MedStar Community Clinical Research Center MedStar Health
Complete this CE activity online at ProCE.com/InsulinPart2
 Complete this CE activity online at ProCE.com/InsulinPart2 Case 1: A 67 year old male with T2DM History and Presentation John is a 67 year old retiree who has been visiting your pharmacy/clinic for over
Complete this CE activity online at ProCE.com/InsulinPart2 Case 1: A 67 year old male with T2DM History and Presentation John is a 67 year old retiree who has been visiting your pharmacy/clinic for over
Non-insulin treatment in Type 1 DM Sang Yong Kim
 Non-insulin treatment in Type 1 DM Sang Yong Kim Chosun University Hospital Conflict of interest disclosure None Committee of Scientific Affairs Committee of Scientific Affairs Insulin therapy is the mainstay
Non-insulin treatment in Type 1 DM Sang Yong Kim Chosun University Hospital Conflict of interest disclosure None Committee of Scientific Affairs Committee of Scientific Affairs Insulin therapy is the mainstay
GLP-1RA and insulin: friends or foes?
 Tresiba Expert Panel Meeting 28/06/2014 GLP-1RA and insulin: friends or foes? Matteo Monami Careggi Teaching Hospital. Florence. Italy Dr Monami has received consultancy and/or speaking fees from: Merck
Tresiba Expert Panel Meeting 28/06/2014 GLP-1RA and insulin: friends or foes? Matteo Monami Careggi Teaching Hospital. Florence. Italy Dr Monami has received consultancy and/or speaking fees from: Merck
OBESITY IN TYPE 2 DIABETES
 OBESITY IN TYPE 2 DIABETES Ashley Crowl, PharmD, BCACP Assistant Professor University of Kansas Objectives Review how to manage obesity in patients with type-2 diabetes mellitus Compare antiobesity agents
OBESITY IN TYPE 2 DIABETES Ashley Crowl, PharmD, BCACP Assistant Professor University of Kansas Objectives Review how to manage obesity in patients with type-2 diabetes mellitus Compare antiobesity agents
Type 2 Diabetes Mellitus Insulin Therapy 2012
 Type 2 Diabetes Mellitus Therapy 2012 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Preparations Onset Peak Duration
Type 2 Diabetes Mellitus Therapy 2012 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Preparations Onset Peak Duration
New Drug Evaluation: Insulin degludec, subcutaneous injection
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Francesca Porcellati
 XX Congresso Nazionale AMD Razionali e Benefici dell Aggiunta del GLP-1 RA Short-Acting all Insulina Basale Francesca Porcellati Dipartimento di Medicina Interna, Sezione di Medicina Interna, Endocrinologia
XX Congresso Nazionale AMD Razionali e Benefici dell Aggiunta del GLP-1 RA Short-Acting all Insulina Basale Francesca Porcellati Dipartimento di Medicina Interna, Sezione di Medicina Interna, Endocrinologia
Insulin Therapies for T2DM
 Insulin Therapies for T2DM Defects in T2DM Decreased insulin secretion Inefficient glucose uptake (skeletal muscles) Increased hepatic glucose production Decreased incretin effect Increased glucagon secretion
Insulin Therapies for T2DM Defects in T2DM Decreased insulin secretion Inefficient glucose uptake (skeletal muscles) Increased hepatic glucose production Decreased incretin effect Increased glucagon secretion
Joslin Diabetes Center Joslin Diabetes Forum 2013: The Impact of Comorbidities on Glucose Control Scenario 2: Reduced Renal Function
 Scenario 2: Reduced Renal Function 62 y.o. white man with type 2 diabetes for 18 years Hypertension and hypercholesterolemia Known proliferative retinopathy Current medications: Metformin 1000 mg bid Glyburide
Scenario 2: Reduced Renal Function 62 y.o. white man with type 2 diabetes for 18 years Hypertension and hypercholesterolemia Known proliferative retinopathy Current medications: Metformin 1000 mg bid Glyburide
Update on Therapies for Type 2 Diabetes: Angela D. Mazza, DO July 31, 2015
 Update on Therapies for Type 2 Diabetes: 2015 Angela D. Mazza, DO July 31, 2015 Objectives To present the newer available therapies for the management of T2D To discuss the advantages and disadvantages
Update on Therapies for Type 2 Diabetes: 2015 Angela D. Mazza, DO July 31, 2015 Objectives To present the newer available therapies for the management of T2D To discuss the advantages and disadvantages
ANGELA GINN-MEADOW RD LDN CDE
 DIABETES DRUGS & TRENDS MADE SIMPLE PHARMD TO RD ANGELA GINN-MEADOW RD LDN CDE OBJECTIVES At the end of this presentation, participants should be able to: Evaluate the emerging role of GLP-1 Agonists for
DIABETES DRUGS & TRENDS MADE SIMPLE PHARMD TO RD ANGELA GINN-MEADOW RD LDN CDE OBJECTIVES At the end of this presentation, participants should be able to: Evaluate the emerging role of GLP-1 Agonists for
This program applies to Commercial, GenPlus and Health Insurance Marketplace formularies.
 OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) Agonists [Adlyxin (lixisenatide), Byetta (exenatide), Bydureon (exenatide extended-release), Tanzeum (albiglutide), Trulicity (dulaglutide),
OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) Agonists [Adlyxin (lixisenatide), Byetta (exenatide), Bydureon (exenatide extended-release), Tanzeum (albiglutide), Trulicity (dulaglutide),
Application of the Diabetes Algorithm to Patients
 Application of the Diabetes Algorithm to Patients Apply knowledge gained from this activity to improve disease management and outcomes for patients with T2DM and obesity Note: The cases in this deck represent
Application of the Diabetes Algorithm to Patients Apply knowledge gained from this activity to improve disease management and outcomes for patients with T2DM and obesity Note: The cases in this deck represent
Individualizing Care for Patients with Type 2 Diabetes
 Individualizing Care for Patients with Type 2 Diabetes Disclosures Speaker: AstraZeneca, Novo Nordisk, BI/Lilly, Valeritas, Takeda Advisor: Tandem Diabetes, Sanofi Objectives Develop individualized approaches
Individualizing Care for Patients with Type 2 Diabetes Disclosures Speaker: AstraZeneca, Novo Nordisk, BI/Lilly, Valeritas, Takeda Advisor: Tandem Diabetes, Sanofi Objectives Develop individualized approaches
Mixed Insulins Pick Me
 Mixed Insulins Pick Me Alvin Goo, PharmD Clinical Associate Professor University of Washington School of Pharmacy and Department of Family Medicine Objectives Critically evaluate the evidence comparing
Mixed Insulins Pick Me Alvin Goo, PharmD Clinical Associate Professor University of Washington School of Pharmacy and Department of Family Medicine Objectives Critically evaluate the evidence comparing
Type 2 Diabetes Management: Case 1: Reducing Hypoglycemic Risk Case 2: Reducing Cardiovascular Risk
 Type 2 Diabetes Management M. Susan Burke, MD, FACP Clinical Associate Professor of Medicine Sidney Kimmel Medical College at Thomas Jefferson University Senior Advisor, Lankenau Medical Associates Lankenau
Type 2 Diabetes Management M. Susan Burke, MD, FACP Clinical Associate Professor of Medicine Sidney Kimmel Medical College at Thomas Jefferson University Senior Advisor, Lankenau Medical Associates Lankenau
!"#$%&%'(!)*+'(,(&)%-!'(.#!%('"./0%(( /1#).!(&2()!(((
*+'(,(&)%-!'(.#!%('./0%(( /1#).!(&2()!(((") !"#%&%'(!)*+'(,(&)%-!'(.#!%('"./0%(( /1#).!(&2()!((( 26%5&"7%'( At the end of this presentation, participants should be able to: Evaluate the emerging role of GLP-1 Agonists for weight loss Understand
!"#%&%'(!)*+'(,(&)%-!'(.#!%('"./0%(( /1#).!(&2()!((( 26%5&"7%'( At the end of this presentation, participants should be able to: Evaluate the emerging role of GLP-1 Agonists for weight loss Understand
New Drug Evaluation: lixisenatide injection, subcutaneous
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Drug List. Drug List (cont.) Objectives. Case 1 Bruce. Presenter Disclosure Information
 Objectives. Case 1 Bruce. Presenter Disclosure Information") 1:15 :3 PM GLP-1 Receptor Agonists and Basal Insulin Combination: A Complementary Strategy for Type Diabetes Treatment Intensification SPEAKERS Vivian Fonseca, MD Dace Trence, MD, FACE Presenter Disclosure
1:15 :3 PM GLP-1 Receptor Agonists and Basal Insulin Combination: A Complementary Strategy for Type Diabetes Treatment Intensification SPEAKERS Vivian Fonseca, MD Dace Trence, MD, FACE Presenter Disclosure
razionale della combinazione insulina/glp-1 RAs
 Insulina e GLP-1 RAS: insieme o separati? razionale della combinazione insulina/glp-1 RAs Catania Mercure Catania Excelsior 10 ottobre 2017 Andrea Giaccari andrea.giaccari@unicatt.it Centro per le Malattie
Insulina e GLP-1 RAS: insieme o separati? razionale della combinazione insulina/glp-1 RAs Catania Mercure Catania Excelsior 10 ottobre 2017 Andrea Giaccari andrea.giaccari@unicatt.it Centro per le Malattie
Pramlintide & Weight. Diane M Karl MD. The Endocrine Clinic & Oregon Health & Science University Portland, Oregon
 Pramlintide & Weight Diane M Karl MD The Endocrine Clinic & Oregon Health & Science University Portland, Oregon Conflict of Interest Speakers Bureau: Amylin Pharmaceuticals Consultant: sanofi-aventis Grant
Pramlintide & Weight Diane M Karl MD The Endocrine Clinic & Oregon Health & Science University Portland, Oregon Conflict of Interest Speakers Bureau: Amylin Pharmaceuticals Consultant: sanofi-aventis Grant
Insulin Intensification: A Patient-Centered Approach
 MARTIN J. ABRAHAMSON, MD Harvard Medical School, Boston, MA Insulin Intensification: A Patient-Centered Approach Dr Abrahamson is associate professor of medicine at Harvard Medical School and medical director
MARTIN J. ABRAHAMSON, MD Harvard Medical School, Boston, MA Insulin Intensification: A Patient-Centered Approach Dr Abrahamson is associate professor of medicine at Harvard Medical School and medical director
Vipul Lakhani, MD Oregon Medical Group Endocrinology
 Vipul Lakhani, MD Oregon Medical Group Endocrinology Disclosures None Objectives Be able to diagnose diabetes and assess control Be able to identify appropriate classes of medications for diabetes treatment
Vipul Lakhani, MD Oregon Medical Group Endocrinology Disclosures None Objectives Be able to diagnose diabetes and assess control Be able to identify appropriate classes of medications for diabetes treatment
No Increased Cardiovascular Risk for Lixisenatide in ELIXA
 ON ISSUES IN THE MANAGEMENT OF TYPE 2 DIABETES JUNE 2015 Coverage of data from ADA 2015, June 5 9 in Boston, Massachusetts No Increased Cardiovascular Risk for Lixisenatide in ELIXA First Cardiovascular
ON ISSUES IN THE MANAGEMENT OF TYPE 2 DIABETES JUNE 2015 Coverage of data from ADA 2015, June 5 9 in Boston, Massachusetts No Increased Cardiovascular Risk for Lixisenatide in ELIXA First Cardiovascular
What s New in Type 2 Diabetes? 2018 Diabetes Updates
 What s New in Type 2 Diabetes? 2018 Diabetes Updates Jessica Conklin, PharmD, PhC, BCACP, CDE, AAHIP Associate Professor, UNM College of Phar macy jeconklin@salud.unm.edu Luis Gonzales, PharmD, PhC UNM
What s New in Type 2 Diabetes? 2018 Diabetes Updates Jessica Conklin, PharmD, PhC, BCACP, CDE, AAHIP Associate Professor, UNM College of Phar macy jeconklin@salud.unm.edu Luis Gonzales, PharmD, PhC UNM
INSULIN THERAPY. Rungnapa Laortanakul, MD Maharat Nakhon Ratchasima hospital
 INSULIN THERAPY Rungnapa Laortanakul, MD Maharat Nakhon Ratchasima hospital 3 Sep. 2013 Case Somsak is a 64-year-old man was diagnosed with T2DM, HT, and dyslipidemia 9 years ago. No history of hypoglycemia
INSULIN THERAPY Rungnapa Laortanakul, MD Maharat Nakhon Ratchasima hospital 3 Sep. 2013 Case Somsak is a 64-year-old man was diagnosed with T2DM, HT, and dyslipidemia 9 years ago. No history of hypoglycemia
CURRENT CONTROVERSIES IN DIABETES CARE
 CURRENT CONTROVERSIES IN DIABETES CARE Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Diabetes Mellitus: U.S. Impact
CURRENT CONTROVERSIES IN DIABETES CARE Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Diabetes Mellitus: U.S. Impact
DEMYSTIFYING INSULIN THERAPY
 DEMYSTIFYING INSULIN THERAPY ASHLYN SMITH, PA-C ENDOCRINOLOGY ASSOCIATES SCOTTSDALE, AZ SECRETARY, AMERICAN SOCIETY OF ENDOCRINE PHYSICIAN ASSISTANTS ARIZONA STATE ASSOCIATION OF PHYSICIAN ASSISTANTS SPRING
DEMYSTIFYING INSULIN THERAPY ASHLYN SMITH, PA-C ENDOCRINOLOGY ASSOCIATES SCOTTSDALE, AZ SECRETARY, AMERICAN SOCIETY OF ENDOCRINE PHYSICIAN ASSISTANTS ARIZONA STATE ASSOCIATION OF PHYSICIAN ASSISTANTS SPRING
Let s not sugarcoat it! Update on Pharmacologic Management of Type II DM
 Let s not sugarcoat it! Update on Pharmacologic Management of Type II DM Gregory Castelli, PharmD, BCPS, BC-ADM Clinical Pharmacist UPMC St. Margaret Objectives By the end of this presentation, participants
Let s not sugarcoat it! Update on Pharmacologic Management of Type II DM Gregory Castelli, PharmD, BCPS, BC-ADM Clinical Pharmacist UPMC St. Margaret Objectives By the end of this presentation, participants