Intensifying Treatment Beyond Monotherapy in T2DM: Where Do Newer Therapies Fit?
|
|
|
- Amice Robinson
- 5 years ago
- Views:
Transcription

1 Intensifying Treatment Beyond Monotherapy in T2DM: Where Do Newer Therapies Fit? Vanita R. Aroda, MD Scientific Director & Physician Investigator MedStar Community Clinical Research Center MedStar Health Research Institute Associate Professor of Medicine Endocrinology, Diabetes, and Metabolism Georgetown University School of Medicine June, 2017
2 Disclosures All activities have been conducted through my employer (MedStar Health Research Institute): Research activities (clinical trials): AstraZeneca, Boehringer Ingelheim, Calibra, Eisai, Novo Nordisk, Sanofi, Takeda Consultative activities: ADA, Adocia, Endocrine Society, Novo Nordisk, Sanofi, Tufts
3 Audience Question: What proportion of patients in your daily practice will require additional therapy after metformin within 5-6 years? Choose one A.0 25% B.25 50% C.50 75% D %
4 Patients failing monotherapy with metformin (%) Failure of maintaining stable glycemic control on monotherapy with metformin Clinical practice: 17%/year, decreased to ~12%/year with early initiation or lower baseline A1c Age, duration, and A1c at initiation were the only factors that predicted secondary failure Treatment-naïve Category patients 1 Dx ~4.4 years Follow up 5.5 years 1 Treatment-naïve patients Dx ~ 2 years Follow up 5 years 2 Treatment-naïve patients (UKPDS) Follow up 6 years 3 Metformin-treated patients months (KPNW) Follow up 2-5 years mean 2 years, 2 months 4 1. Ekström N et al. BMJ 2015;3:e e000068; 2. Kahn SE et al. N Engl J Med 2006;355: ; 3. Turner RC et al. JAMA 1999;281: ; 4. Brown JB et al. Diabetes Care 2010;33:



5 Going back 10 years to 2007
6 Case study (2007): 52-year-old female Patient characteristics Diabetes history Glucose-lowering therapy HbA 1c 8.1% Weight T2D for 8 years Metformin 1500 mg/day 99.4 kg BMI 34.2 kg/m 2 BMI, body mass index; HbA 1c, glycosylated haemoglobin; T2D, type 2 diabetes
7 Diabetes treatment options for our patient: Older therapies" Metformin Thiazolidinediones Human insulin 1950s 1960s 1970s 1980s 1990s 2000s 2010s Sulfonylureas Insulin analogues; AGIs; glinides AGI, alpha-glucosidase inhibitor
8 Audience Question: It is 2007 ( older therapies ). How would you intensify treatment in this patient to improve glycaemic control? T2DM 8 years, HbA 1c 8.1%, weight 99.4 kg, BMI 34.2 kg/m 2 Choose one A.Sulfonylurea B.Insulin analogue C.Thiazolidinedione D.Alpha glucosidase inhibitor E.Glinide BMI, body mass index; DPP-4i, dipeptidyl peptidase-4 inhibitor; GLP-1 RA, glucagon-like peptide-1 receptor agonist; HbA 1c, glycosylated haemoglobin; SGLT-2i, sodium-glucose co-transporter-2 inhibitor; T2D, type 2 diabetes
9 Paradigm shifts in the last decade Glucose control matters Get to goal safely Treat for the long run
10 Adjusted incidence per 1000 person-years (%) 2000: The lower the glycaemia, the lower the risk for complications, without a threshold 80 Myocardial infarction Microvascular endpoints Updated mean HbA 1c concentration (%) HbA 1c, glycosylated haemoglobin UKPDS 35. BMJ 2000;321:
11 2009: Intensive glycaemic treatment reduces cardiovascular outcomes, no mortality benefit Myocardial infarction Number of events (annual event rate, %) Trials More intensive Less intensive HbA 1c (%) Favours more intensive Favours less intensive Hazard ratio (95% CI) Myocardial infarction ACCORD 198 (1.18) 245 (1.51) ( ) ADVANCE 310 (1.18) 337 (1.28) ( ) UKPDS 150 (0.20) 76 (1.40) ( ) VADT 72 (1.65) 87 (1.99) ( ) Overall ( ) (Q=2.25, p=0.52, I 2 =0.0%) CI, confidence interval; HbA 1c, glycosylated haemoglobin Turnbull FM et al. Diabetologia 2009;52: Hazard ratio (95% CI)
12 2009: Intensive glycaemic treatment reduces cardiovascular outcomes, no mortality benefit All-cause mortality Number of events (annual event rate, %) Trials More intensive Less intensive HbA 1c (%) Favours more intensive Favours less intensive Hazard ratio (95% CI) All-cause mortality ACCORD 257 (1.41) 203 (1.14) ( ) ADVANCE 498 (1.86) 533 (1.99) ( ) UKPDS 123 (0.13) 53 (0.25) ( ) VADT 102 (2.22) 95 (2.06) ( ) Overall ( ) (Q=5.71, p=0.13, I 2 =47.5%) CI, confidence interval; HbA 1c, glycosylated haemoglobin Turnbull FM et al. Diabetologia 2009;52: Hazard ratio (95% CI)
13 Paradigm shifts in the last decade Glucose control matters Get to goal safely Treat for the long run
14 Percent patients, % Barriers to achieving treatment goals Target HbA 1c (%) <6.0 HbA 1c achieved (%) 6.4 ACCORD intensive therapy 1 Hypoglycaemia requiring assistance vs standard (% of patients) Weight gain >10 kg since baseline vs standard (%) 16.2 vs 5.1, p< vs 14.1, p< Exposure to prescribed glucose-lowering medication Secretagogue Thiazolidinedione Any insulin HbA 1c, glycosylated haemoglobin 1. Gerstein HC et al. N Engl J Med 2008;358: Intensive therapy Standard therapy
15 Limitations of older therapies Difficulty in achieving glycemic targets Unacceptable level of weight gain Significantly greater hypoglycemia ACCORD: 3X higher risk of hypoglycemia requiring medical assistance VADT: 2X higher risk of hypoglycemia requiring medical assistance
16 Type 2 diabetes in the 21 st century Perhaps the question is no longer how low our glycemic targets should be to prove macrovascular and mortality benefit, but whether we can make a difference if we get there safely.
17 Expansion of diabetes treatment options in the last decade Human insulin Metformin Thiazolidinediones DPP-4is 1950s 1960s 1970s 1980s 1990s 2000s 2010s Sulfonylureas GLP-1 RAs Insulin analogues; AGIs; glinides SGLT-2is AGI, alpha-glucosidase inhibitor; DPP-4i, dipeptidyl peptidase-4 inhibitor; GLP-1 RA, glucagon-like peptide-1 receptor agonist; SGLT-2i, sodium glucose co-transporter-2 inhibitor

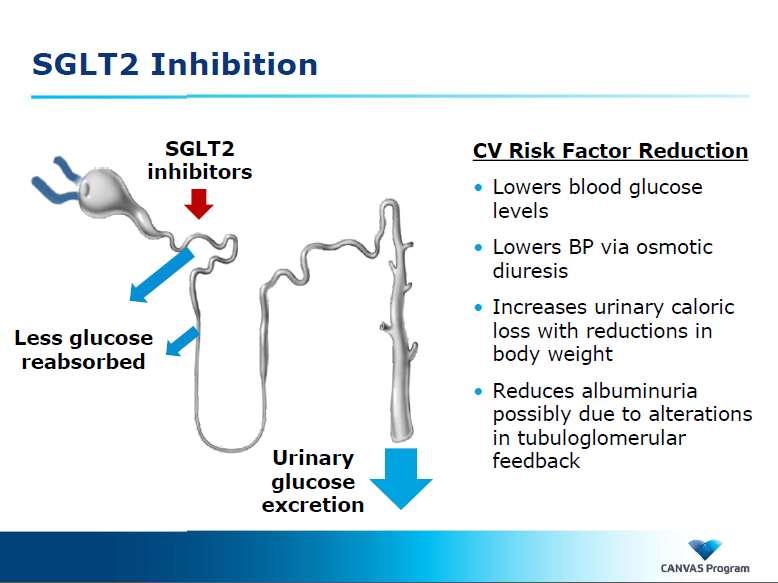
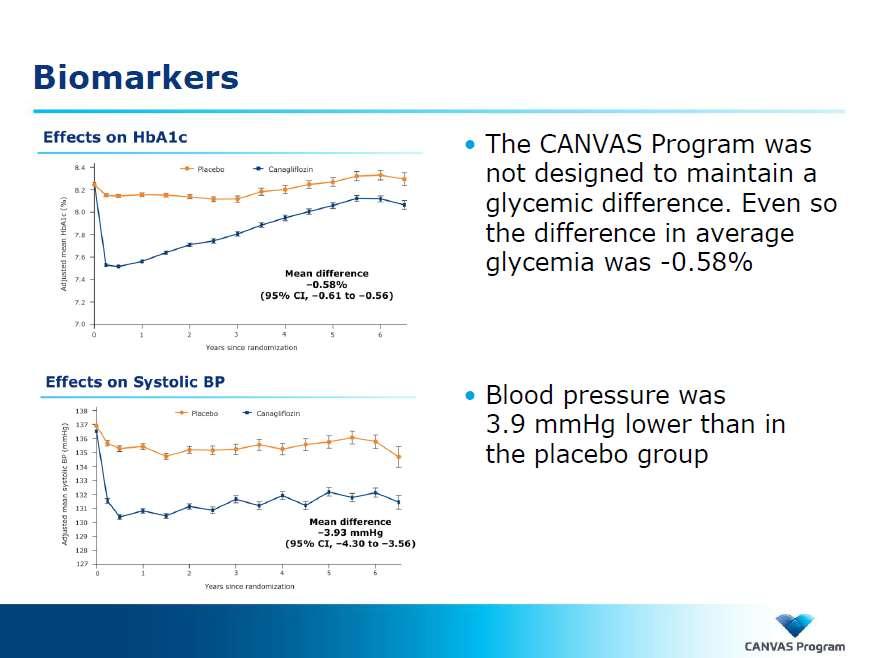
18
19 Methodology Reviewed timeline of all currently available FDAapproved medications for the treatment of type 2 diabetes Reviewed trials listed in clinicaltrials.gov as of August 10, 2016 that met the following criteria: Published phase 3 or phase 4 prospective, randomized interventional studies of current FDA-approved pharmacotherapy for the treatment of T2DM Therapies evaluated: Glucagon-like peptide-1 receptor agonists (GLP-1 RAs) Dipeptidyl peptidase-4 (DPP-4) inhibitors Sodium-glucose co-transporter 2 (SGLT2) inhibitors U.S. as a site Study population represented treatment intensification beyond monotherapy Kuhn A Aroda VR. Curr Cardiol Rep 2017

20 Kuhn A Aroda VR. Curr Cardiol Rep 2017

21 Just tell me which one I should choose! Kuhn A Aroda VR. Curr Cardiol Rep 2017
22 Summary of clinical trial evidence of efficacy of DPP-4 Inhibitors in treatment intensification for T2DM Clinical Trials Study Number NCT Comparators SITA 100 mg QD (n=453) PBO (n=224) Baseline HbA1c & FPG 8.0% mg/dl Length (1 o outcome) Change in A1c (%) 24 weeks SITA: PBO: Change in Body Weight (kg) No differences in weight Hypoglycemia No differences in hypoglycemia NCT SITA 100 mg QD (n=96) PBO (n=94) % mg/dl 30 weeks 18 weeks: SITA: PBO: weeks: SITA: PBO: 0.04 No increase in weight No increase in hypoglycemia NCT LIRA 1.8 mg QD (n=218) LIRA 1.2 mg QD (n=221) SITA (n=219) 8.5% 180 mg/dl 26 weeks LIRA 1.8 mg: LIRA 1.2 mg: SITA: LIRA 1.8 mg: LIRA 1.2 mg: SITA: NCT Oral Strategy: SITA 100 mg QD (n=326), then GLIM if needed, Injectable Strategy: LIRA 1.2 mg/day (n=327), then uptitrate to 1.8 mg if needed % mg/dl 26 weeks Oral: -1.3 Injectable: -1.4 Greater hypoglycemia in oral strategy (with sulfonylurea) NCT EXEN 2mg once weekly (n=160) Vs SITA 100 mg QD (n=166) Vs PIO 45 mg QD (n=165) 8.5% 164 mg/dl 26 week EXEN: -1.5 SITA: -0.9 PIO: -1.2 EXEN: -2.3 SITA: -0.8 PIO: 2.8 low, similar NCT ALB once weekly 30 mg, titratable to 50 mg (mean dose 40.5 mg) (n=302), SITA 100 mg QD (n=302), GLIM 2 mg, titratable to 4 mg (mean dose 3.1 mg), QD (n=307), PBO (n=101) 8.1% - 8.2%, mg/dl 104 weeks ALB: SITA: GLIM: PBO: 0.27 ALB: SITA: GLIM: 1.17 PBO: ALB: 3% SITA: 1.7% GLIM: 17.9% PBO: 4% Kuhn A Aroda VR. Curr Cardiol Rep 2017
23 Clinical Trials Study Number Comparators Baseline HbA1c & FPG Length (1 o outcome) Change in A1c (%) Change in Body Weight (kg) Hypoglycemia NCT GLAR (n=250) SITA 100mg QD (n=265) 8.5% mg/dl 24 weeks GLAR: SITA: GLAR: 0.44 SITA: GLAR: 4.21 events per patientyear SITA: 0.50 events per patient-year NCT SAXA 2.5 mg twice daily (n=74), PBO (n=86) %, mg/dl 12 weeks SAXA: PBO: SAXA: PBO: SAXA: 5.4% PBO: 1.2% NCT SAXA 2.5 mg QD (n=192) SAXA 5 mg QD (n=191) SAXA 10 mg QD (n=181) PBO (n=179) 8.0% 176 mg/dl 24 weeks SAXA 2.5: SAXA 5: SAXA 10: PBO: 0.13 No difference compared to PBO No difference compared to PBO 4-year safety follow up with no increase in hypoglycemia or new safety concerns [100] NCT SAXA 5 mg QD (n=138) Uptitration MET to 2000 mg METXR QD (n=144) % 163 mg/dl 18 weeks SAXA: -0.8 Uptitrated METXR: SAXA: 0.4 Uptitrated METXR: -0.5 SAXA: 3.6% Uptitrated METXR: 1.4% NCT SAXA 5 mg/day + DAPA 10 mg/day (n=179), SAXA 5 mg/day + PBO (n=176), DAPA 10 mg/day + PBO (n=179) 8.9% mg/dl 24 weeks SAXA + DAPA: -1.5 SAXA: -0.9 DAPA: -1.2 SAXA + DAPA: -2.1 SAXA: 0.0 DAPA: -2.4 Low (1%) similar rates of hypoglycemia; no major hypoglycemia NCT ALO 12.5 mg QD (n=213), ALO 25 mg QD (n=210), PBO (n=104) 7.9-8% mg/dl 26 weeks ALO 12.5 mg: -0.6 ALO 25 mg: -0.6 PBO: -0.1 No significant difference in hypoglycemia NCT ALO 12.5 mg QD (n=880), ALO 25 mg QD (n=885) GLIP 5mg, titratable to 20 mg (mean final dose 5.2 mg) (n=874) 7.6% 104 weeks ALO 12.5mg: ALO 25mg: GLIP: ALO 12.5 mg: ALO 25 mg: GLIP: 0.95 ALO 12.5mg: 2.5% ALO 25 mg: 1.4% GLIP: 23.2% NCT LINA 5 mg QD (n=524) PBO (n=177) 8.1% 169 mg/dl 24 weeks LINA: PBO: 0.15 LINA: 0.6% PBO: 2.8% NCT LINA 5 mg QD (n=777), GLIM 1-4 mg QD (n=775) 7.7% mg/dl 104 weeks LINA: GLIM: LINA: -1.4 GLIM: 1.3 LINA: 7% GLIM: 36% NCT EMPA 25 mg/lina 5 mg QD (n=137), EMPA 10 mg/lina 5 mg QD (n=136), EMPA 25 mg QD (n=141), EMPA 10 mg QD (n=140), LINA 5 mg (n=132), % mg/dl 24 weeks EMPA 25 mg/lina 5 mg: EMPA 10 mg/lina 5 mg: EMPA 25 mg: EMPA 10 mg: LINA 5 mg: EMPA 25 mg/lina 5 mg: -3.0 EMPA 10 mg/lina 5 mg: -2.6 EMPA 25 mg: -3.2 EMPA 10 mg: -2.5 LINA 5 mg: -0.7 kg Similar adverse events across treatment arms
 Change in Body Weight (kg) Incidence of Hypoglycemia (%) NCT01106677 CANA 100mg (CANA100) QD (n=368), CANA 300mg QD (CANA300), (n=367), SITA 100 mg QD, (n=366), SITA + PBO (n=183) 7.")
24 Summary of clinical trial evidence of efficacy of SGLT-2 Inhibitors in treatment intensification for type 2 DM Clinical Trials Study Number Comparators Baseline HbA1c & FPG Length (1 o outcome) Change in A1c (%) Change in Body Weight (kg) Incidence of Hypoglycemia (%) NCT CANA 100mg (CANA100) QD (n=368), CANA 300mg QD (CANA300), (n=367), SITA 100 mg QD, (n=366), SITA + PBO (n=183) 7.9% mg/dl 26 weeks CANA300: CANA100: SITA: at week 52: CANA300: -3.7 CANA100: -3.3 SITA: -1.2 CANA300: 4.7 CANA100: 5.0 SITA: 4.2 SITA/PBO: 2.7 NCT CANA 100mg QD (n=483), CANA 300mg QD (n=485), GLIM (up to 6 mg or 8 mg QD), (n=482) 7.8% mg/dl 52 weeks CANA100: CANA300: GLIM: CANA300: -0.7 CANA100: -0.6 GLIM: +0.7 CANA300: 5 CANA100: 6 GLIM: 34 % NCT DAPA 10mg (DAPA10) QD (n=135), DAPA 5mg (DAPA5) (n=137), DAPA 2.5mg (DAPA2.5) (n=137) PBO (n=137) 8.1% mg/dl 102 weeks DAPA10: DAPA5: DAPA2.5: PBO: 0.02 DAPA10: DAPA5: DAPA2.5: PBO: 1.36 DAPA10: -5.2 DAPA5: DAPA2.5: PBO- 5.8 NCT DAPA10 (n=179), SAXA 5mg(SAXA5), (n=176), DAPA10/SAXA5 (n=179) 8.9% 186 mg/dl 24 weeks DAPA10: SAXA5: DAPA10/SAXA5: DAPA10: -2.4 SAXA5: 0.0 DAPA10/SAXA5: -2.1 DAPA10: 1 SAXA5: 1 DAPA10/SAXA5: 1 NCT EMPA 25mg (EMPA25), (n=141), EMPA 10mg (EMPA10), (n=140), LINA 5mg (LINA5) n=132, EMPA25/LINA5 (n=137), EMPA10/LINA5 (n=136) 7.98% mg/dl 24 weeks EMPA25: EMPA10: LINA5: EMPA25/LINA5: EMPA10/LINA5: EMPA25: -3.2 EMPA10: -2.5 LINA5: -0.7 EMPA25/LINA5: -3.0 EMPA10/LINA5: -2.6 EMPA25: 3.5 EMPA10: 1.4 LINA5: 2.3 EMPA25/LINA5: 3.6 EMPA10/LINA5: 2.2 NCT EMPA25 (n=213), EMPA10 (n=217), PBO (n=207) 7.9% mg/dl 24 weeks EMPA25: EMPA10: PBO EMPA25: EMPA10: PBO: EMPA25: 1.4 EMPA10: 1.8 PBO: 0.5 NCT EMPA25 (n=166), EMPA10 (n=166), SITA (n=56) 7.91% 177.4mg/dl 90 weeks (12 weeks blinded + 78 week openlabel extension) EMPA25: EMPA10: SITA: EMPA25: EMPA10: -3.1 SITA: -0.4 EMPA25: 1.8 EMPA10: 2.4 SITA: 3.6 Kuhn A Aroda VR. Curr Cardiol Rep 2017
25 Summary of clinical trial evidence of efficacy of SGLT-2 Inhibitors in treatment intensification for type 2 DM Clinical Trials Study Number Comparators Baseline HbA1c & FPG Length (1 o outcome) Change in A1c (%) Change in Body Weight (kg) Incidence of Hypoglycemia (%) NCT CANA 100mg (CANA100) QD (n=368), CANA 300mg QD (CANA300), (n=367), SITA 100 mg QD, (n=366), SITA + PBO (n=183) 7.9% mg/dl 26 weeks CANA300: CANA100: SITA: at week 52: CANA300: -3.7 CANA100: -3.3 SITA: -1.2 CANA300: 4.7 CANA100: 5.0 SITA: 4.2 SITA/PBO: 2.7 NCT CANA 100mg QD (n=483), CANA 300mg QD (n=485), GLIM (up to 6 mg or 8 mg QD), (n=482) 7.8% mg/dl 52 weeks CANA100: CANA300: GLIM: CANA300: -0.7 CANA100: -0.6 GLIM: +0.7 CANA300: 5 CANA100: 6 GLIM: 34 % NCT DAPA 10mg (DAPA10) QD (n=135), DAPA 5mg (DAPA5) (n=137), DAPA 2.5mg (DAPA2.5) (n=137) PBO (n=137) 8.1% mg/dl 102 weeks DAPA10: DAPA5: DAPA2.5: PBO: 0.02 DAPA10: DAPA5: DAPA2.5: PBO: 1.36 DAPA10: -5.2 DAPA5: DAPA2.5: PBO- 5.8 NCT DAPA10 (n=179), SAXA 5mg(SAXA5), (n=176), DAPA10/SAXA5 (n=179) 8.9% 186 mg/dl 24 weeks DAPA10: SAXA5: DAPA10/SAXA5: DAPA10: -2.4 SAXA5: 0.0 DAPA10/SAXA5: -2.1 DAPA10: 1 SAXA5: 1 DAPA10/SAXA5: 1 NCT EMPA 25mg (EMPA25), (n=141), EMPA 10mg (EMPA10), (n=140), LINA 5mg (LINA5) n=132, EMPA25/LINA5 (n=137), EMPA10/LINA5 (n=136) 7.98% mg/dl 24 weeks EMPA25: EMPA10: LINA5: EMPA25/LINA5: EMPA10/LINA5: EMPA25: -3.2 EMPA10: -2.5 LINA5: -0.7 EMPA25/LINA5: -3.0 EMPA10/LINA5: -2.6 EMPA25: 3.5 EMPA10: 1.4 LINA5: 2.3 EMPA25/LINA5: 3.6 EMPA10/LINA5: 2.2 NCT EMPA25 (n=213), EMPA10 (n=217), PBO (n=207) 7.9% mg/dl 24 weeks EMPA25: EMPA10: PBO EMPA25: EMPA10: PBO: EMPA25: 1.4 EMPA10: 1.8 PBO: 0.5 NCT EMPA25 (n=166), EMPA10 (n=166), SITA (n=56) 7.91% 177.4mg/dl 90 weeks (12 weeks blinded + 78 week openlabel extension) EMPA25: EMPA10: SITA: EMPA25: EMPA10: -3.1 SITA: -0.4 EMPA25: 1.8 EMPA10: 2.4 SITA: 3.6 Kuhn A Aroda VR. Curr Cardiol Rep 2017
26 Summary of clinical trial evidence of efficacy of SGLT-2 Inhibitors in treatment intensification for type 2 DM Clinical Trials Study Number Comparators Baseline HbA1c & FPG Length (1 o outcome) Change in A1c (%) Change in Body Weight (kg) Incidence of Hypoglycemia (%) NCT CANA 100mg (CANA100) QD (n=368), CANA 300mg QD (CANA300), (n=367), SITA 100 mg QD, (n=366), SITA + PBO (n=183) 7.9% mg/dl 26 weeks CANA300: CANA100: SITA: at week 52: CANA300: -3.7 CANA100: -3.3 SITA: -1.2 CANA300: 4.7 CANA100: 5.0 SITA: 4.2 SITA/PBO: 2.7 NCT CANA 100mg QD (n=483), CANA 300mg QD (n=485), GLIM (up to 6 mg or 8 mg QD), (n=482) 7.8% mg/dl 52 weeks CANA100: CANA300: GLIM: CANA300: -0.7 CANA100: -0.6 GLIM: +0.7 CANA300: 5 CANA100: 6 GLIM: 34 % NCT DAPA 10mg (DAPA10) QD (n=135), DAPA 5mg (DAPA5) (n=137), DAPA 2.5mg (DAPA2.5) (n=137) PBO (n=137) 8.1% mg/dl 102 weeks DAPA10: DAPA5: DAPA2.5: PBO: 0.02 DAPA10: DAPA5: DAPA2.5: PBO: 1.36 DAPA10: -5.2 DAPA5: DAPA2.5: PBO- 5.8 NCT DAPA10 (n=179), SAXA 5mg(SAXA5), (n=176), DAPA10/SAXA5 (n=179) 8.9% 186 mg/dl 24 weeks DAPA10: SAXA5: DAPA10/SAXA5: DAPA10: -2.4 SAXA5: 0.0 DAPA10/SAXA5: -2.1 DAPA10: 1 SAXA5: 1 DAPA10/SAXA5: 1 NCT EMPA 25mg (EMPA25), (n=141), EMPA 10mg (EMPA10), (n=140), LINA 5mg (LINA5) n=132, EMPA25/LINA5 (n=137), EMPA10/LINA5 (n=136) 7.98% mg/dl 24 weeks EMPA25: EMPA10: LINA5: EMPA25/LINA5: EMPA10/LINA5: EMPA25: -3.2 EMPA10: -2.5 LINA5: -0.7 EMPA25/LINA5: -3.0 EMPA10/LINA5: -2.6 EMPA25: 3.5 EMPA10: 1.4 LINA5: 2.3 EMPA25/LINA5: 3.6 EMPA10/LINA5: 2.2 NCT NCT EMPA25 (n=213), EMPA10 (n=217), PBO (n=207) EMPA25 (n=166), EMPA10 (n=166), SITA (n=56) 7.9% mg/dl 7.91% 177.4mg/dl 24 weeks EMPA25: EMPA10: PBO weeks (12 weeks blinded + 78 week openlabel extension) EMPA25: EMPA10: SITA: EMPA25: EMPA10: PBO: EMPA25: EMPA10: -3.1 SITA: -0.4 EMPA25: 1.4 EMPA10: 1.8 PBO: 0.5 EMPA25: 1.8 EMPA10: 2.4 SITA: 3.6 Kuhn A Aroda VR. Curr Cardiol Rep 2017

27 Ferrannini E et al, Diabetes Care 2013; 36:
28 Change in HbA 1c (%) Change in HbA 1c across drug classes Add-on to metformin DPP-4i vs SGLT-2i DPP-4i vs GLP-1 RA Sita vs Cana 1 52 wk Empa vs Sita 2 24 wk DURATION wk LIRA-DPP wk HARMONY wk AWARD wk Baseline HbA 1c (%): n= n= n= n= n= n= n= n= n= n= n= n= n= n= n= *** * 1.3 *** 1.5 *** ** 1.1 ** Sitagliptin 100 mg Canagliflozin 300 mg Empagliflozin 10 mg Empagliflozin 25 mg Exenatide 10 mg Liraglutide 1.2 mg Liraglutide 1.8 mg Albiglutide Dulaglutide 0.75 mg Dulaglutide 1.5 mg *p<0.05; **p<0.001; ***p< DPP-4i, dipeptidyl peptidase-4 inhibitor; GLP-1 RA, glucagon-like peptide-1 receptor agonist; HbA 1c, glycosylated haemoglobin; SGLT-2i, sodium-glucose co-transporter-2 inhibitor 1. Lavalle-González FJ et al. Diabetologia 2013;56: ; 2. Roden M et al. Lancet Diabetes Endocrinol 2013;1: ; 3. Bergenstal R et al. Lancet 2010;376: ; 4. Pratley R et al. Int J Clin Pract 2011;65: ; 5. Ahren B et al. Diabetes Care 2014;37: ; 6. Nauck M et al. Diabetes Care 2014;37:
29 Change in weight (kg) Change in body weight across drug classes Add-on to metformin DPP-4i vs SGLT-2i DPP-4i vs GLP-1 RA Sita vs Cana 1 52 wk Empa vs Sita 2 24 wk DURATION wk LIRA-DPP wk HARMONY wk AWARD wk Baseline weight (kg): n= n= n= n= n= n= n= n= n= n= n= n= n= n= n= Sitagliptin 100 mg 3.7 ** *** *** Canagliflozin 300 mg ** *** Empagliflozin 10 mg 3.7 *** Empagliflozin 25 mg * ** Exenatide 10 mg Liraglutide 1.2 mg Liraglutide 1.8 mg Albiglutide Dulaglutide 0.75 mg Dulaglutide 1.5 mg *p<0.05; **p<0.001; ***p< DPP-4i, dipeptidyl peptidase-4 inhibitor; GLP-1 RA, glucagon-like peptide-1 receptor agonist; SGLT-2i, sodium-glucose co-transporter-2 inhibitor 1. Lavalle-González FJ et al. Diabetologia 2013;56: ; 2. Roden M et al. Lancet Diabetes Endocrinol 2013;1: ; 3. Bergenstal R et al. Lancet 2010;376: ; 4. Pratley R et al. Int J Clin Pract 2011;65: ; 5. Ahren B et al. Diabetes Care 2014;37: ; 6. Nauck M et al. Diabetes Care 2014;37:
30 Back to our case, in 2017: 52-year-old female Patient characteristics Diabetes history Glucose-lowering therapy HbA 1c 8.1% Weight T2D for 8 years Metformin 1500 mg/day 99.4 kg BMI 34.2 kg/m 2 BMI, body mass index; HbA 1c, glycosylated haemoglobin; T2D, type 2 diabetes
31 Audience Question: How would you intensify treatment in this patient to improve glycemic control? T2D 8 years, HbA 1c 8.1%, weight 99.4 kg, BMI 34.2 kg/m 2 Choose one A.Sulfonylurea B.Insulin analogue C.GLP-1 RA D.DPP-4i E.SGLT-2i BMI, body mass index; DPP-4i, dipeptidyl peptidase-4 inhibitor; GLP-1 RA, glucagon-like peptide-1 receptor agonist; HbA 1c, glycosylated haemoglobin; SGLT-2i, sodium-glucose co-transporter-2 inhibitor; T2D, type 2 diabetes
32 Paradigm shifts in the last decade Glucose control matters Get to goal safely Treat the whole patient, for the long run
33 Empagliflozin, cardiovascular outcomes and mortality in type 2 diabetes (EMPA-REG) CI, confidence interval; HR, hazard ratio Zinman B et al. N Engl J Med 2015 Sept 17
34 Liraglutide and Cardiovascular Outcomes in Type 2 Diabetes (LEADER) Compared to placebo, the rate of the first occurrence of death from cardiovascular causes, nonfatal myocardial infarction, or nonfatal stroke among patients with type 2 diabetes mellitus was lower with liraglutide. Marso SP et al. N Engl J Med 2016;375:
35 Liraglutide and Cardiovascular Outcomes in Type 2 Diabetes (LEADER) Marso SP et al. N Engl J Med 2016;375:


36
37 Audience Poll: Did you attend the CANVAS presentation at the ADA in San Diego this last week? A) Yes B) No
38

39 June 22, 2017
40

41 June 22,
42
43 June 22,

44 June 22,

45 June 22,

46 June 22,

47 June 22,

48 June 22,
49 June 22,

50 June 22,

51 June 22,
52 June 22,

53 June 22,

54 June 22,
55 June 22,
56 June 22,

57 June 22,

58 June 22,
59 June 22,

60 June 22,

61 Where DO newer therapies fit?

62 Where do newer therapies fit? Williams Textbook of Endocrinology 2016

63
64
65 NIH glycemia reduction approaches in diabetes: A comparative effectiveness study (GRADE) Screening T2D Treated with metformin alone HbA 1c 6.8% at screening <10 <10 years duration at screening Metformin run-in Titrate metformin to 1,000 (min) 2,000 (goal) mg/day HbA 1c % at final run-in visit Randomisation n=5,000 eligible participants Sulfonylurea (glimepiride) n=1,250 DPP-4 inhibitor (sitagliptin) n=1,250 GLP-1 RA (liraglutide) n=1,250 Insulin (glargine) n=1,250 DPP-4, dipeptidyl peptidase-4; GLP-1 RA, glucagon-like peptide-1 receptor agonist; HbA 1c, glycosylated haemoglobin; NIH, National Institutes of Health; T2D, type 2 diabetes Nathan DM et al. Diabetes Care 2013;36:
66 Case #3: Addressing postprandial glucose Ms LD 62-year-old patient with a 12-year history of T2DM She has been on metformin 1 g bid and glimepiride 8 mg daily for the past 5 years Because of an elevated A1c of 8.9%, bedtime glargine was added 1 yr ago. Currently on 46U hs Currently no symptoms of hyper- or hypoglycemia Otherwise well. No clinical history of CVD Meds: Atorvastatin 40 mg daily Irbesartan 300 mg daily On Exam: BMI=31.2 BP=134/ lb (82.7 kg) Abdominal obesity Otherwise Normal
67 Case #3 - Labs Lab: FPG=108 mg/dl A1c=7.9% Renal and liver function normal
68 Results of SMBG Breakfast Lunch Supper HS Before After Before After Before After Monday Tuesday Wednesday Thursday Friday
69 Diabetes Management Case Study Audience Response Question A) <6.5% B) <7.0% C) <7.5% D) <8.0% E) <8.5% What is your target A1c for her:
70 Case #3: Audience Response Question What would be your preferred strategy to bring her A1c to target? A) Change the dose or timing of the glargine B) Add a DPP4 inhibitor C) Add a GLP1 RA D) Add a thiazolidinedione E) Add an SGLT2 inhibitor Breakfast Lunch Supper HS Before After Before After Before After Monday Tuesday Wednesday Thursday Friday
71 LixiLan-L: Patients with T2DM not controlled on basal insulin DESIGN: Randomized, open label, parallel-group, 30-week treatment trial 7% HbA 1c 10% FPG 140 mg/dl iglar dose 50 U iglar ± Metformin n=369 T2DM patients with: Basal insulin >6 months Stable dose U/d Up to 2 OADs iglarlixi ± Metformin HbA 1c 7.5% 10% FPG mg/dl n=367 iglar introduced and/or titrated/ stabilized 6-week run-in phase iglar dose adjusted to SMPG target (80 to 100 mg/dl) and capped to 60 U/day in both groups 30-week treatment period Only metformin was continued. Non-metformin OADs were discontinued after the start of the run-in phase FPG, fasting plasma glucose; HbA 1c, glycated hemoglobin; OADs, oral antidiabetic drugs; SMPG, self-measured plasma glucose; T2DM, type 2 diabetes mellitus Aroda VR et al, Diabetes Care 2016
72 LixiLan-L: Demographic & Baseline Characteristics iglarlixi (n=367) iglar (n=369) All (N=736) Age (years) Female (%) Caucasian/Black (%) 92/5 92/6 92/5 Body weight (kg) at Baseline BMI (kg/m 2 ) at Baseline % Patients with BMI 30 kg/m Diabetes duration (yrs) Duration of basal insulin treatment (yrs) Basal insulin type at Screening (%) iglar Detemir NPH iglar dose (U) at Baseline OAD use at Screening (%) None Metformin Sulfonylurea (SU) DPP-4 inhibitor Metformin + SU Metformin + DPP-4 inhibitor BMI, body mass index; DPP-4, dipeptidyl peptidase 4; NPH, neutral protamine Hagedorn; OAD, oral antidiabetic drug Aroda VR et al, Diabetes Care 2016
73 Mean ± SE LixiLan-L: Mean HbA 1c Change HbA 1c over time (%) Screening iglarlixi 8.5 iglar Baseline Week LS mean change LS mean difference 95% CI, p-value ( to 0.397) p< % % mitt iglarlixi iglar S BL LOCF Week 77 BL, baseline; CI, confidence interval; HbA 1c, glycated hemoglobin; LS, Least squares; LOCF, Last observation carried forward; mitt, modified intent-to-treat; MMRM, mixed-effect model with repeated measures; S, Screening; SE, standard error Aroda VR et al, Diabetes Care 2016
74 Mean ± SE (mmol/l) LixiLan-L: Mean Plasma Glucose and Glucose Excursion* Mean plasma glucose (mg/dl) LS mean change from baseline iglarlixi iglar Plasma glucose LS mean difference 95% CI, p-value 60.0 ( 70.1 to 50.0) iglarlixi at baseline iglarlixi at Week 30 iglar at baseline iglar at Week 30 Glucose excursion LS mean difference 95% CI, p-value 61.8 ( 70.7 to 52.7) p< Mean ± SE (mg/dl) Pre-injection Pre-meal 30-minute postprandial 1-hour postprandial 2-hour postprandial *Standardized liquid breakfast meal; LS mean difference vs iglar. mitt; ANCOVA CI, confidence interval; LS, least squares; mitt, modified intent-to-treat; SE, standard error
75 Patients (%) LixiLan-L: Patients Reaching Target HbA 1c at Week %* 95% CI: 18.9 to 32.1 p< iglarlixi iglar %* 95% CI: 13.9 to 25.6 p< mitt HbA 1c <7% HbA 1c 6.5% *Weighted average of proportion difference between treatment groups CI, confidence interval; HbA 1c, glycated hemoglobin; mitt, modified intent-to-treat Aroda VR et al, Diabetes Care 2016
76 Audience Poll: How many saw the DUAL VII results at the ADA in San Diego this year? A) Yes B) No 81 June 22, 2017


77 DUAL VII: IDegLira vs Basal Bolus Insulin in Type 2 Diabetes IDegLira Adapted from

78 DUAL VII: IDegLira vs Basal-Bolus Insulin IDegLira IDegLira Adapted from: al/investor_presentations/2017/ %20- %20ADA%202017%20Investor%20presentation.pdf
79 IDegLira IDegLira Adapted from: rmaterial/investor_presentations/2017/ %20- %20ADA%202017%20Investor%20presentation.pdf

80 Included with permission from AACE, for educational purposes only, June 2017
81 Summary Allowing for individualizing of glycemic targets, achieving glucose control minimises long-term risk of complications and remains a forefront of diabetes care Over the past ~decade, a myriad of treatments have emerged to address efficacy while minimising weight gain and hypoglycemia GLP-1 RA and SGLT2 inhibitors demonstrate high glycemic efficacy DPP-4 inhibitors are well tolerated Treatment paradigms in diabetes are shifting toward longerterm comprehensive goals, including durability, safety and cardiovascular risk.







82
83 EXTRA SLIDES 88 June 22, 2017
Update on Insulin-based Agents for T2D
 Update on Insulin-based Agents for T2D Injectable Therapies for Type 2 Diabetes Mellitus (T2DM) and Obesity This presentation will: Describe established and newly available insulin therapies for treatment
Update on Insulin-based Agents for T2D Injectable Therapies for Type 2 Diabetes Mellitus (T2DM) and Obesity This presentation will: Describe established and newly available insulin therapies for treatment
Syllabi/Slides for this program are a supplement to the live CME session and are not intended for other purposes.
 10:50-11:35am Cases in Type 2 Diabetes Management Disclosures The following relationships exist related to this presentation: Martin J. Abrahamson, MD, FACP: Advisory Board member for Novo Nordisk and
10:50-11:35am Cases in Type 2 Diabetes Management Disclosures The following relationships exist related to this presentation: Martin J. Abrahamson, MD, FACP: Advisory Board member for Novo Nordisk and
The first stop for professional medicines advice
 London Medicines Evaluation Network Overview: Glucagon-Like Peptide-1 receptor analogues The first stop for professional medicines advice 1 London Medicines Evaluation Network Overview: Glucagon-Like Peptide-1
London Medicines Evaluation Network Overview: Glucagon-Like Peptide-1 receptor analogues The first stop for professional medicines advice 1 London Medicines Evaluation Network Overview: Glucagon-Like Peptide-1
Early treatment for patients with Type 2 Diabetes
 Israel Society of Internal Medicine Kibutz Hagoshrim, June 22, 2012 Early treatment for patients with Type 2 Diabetes Eduard Montanya Hospital Universitari Bellvitge-IDIBELL CIBERDEM University of Barcelona
Israel Society of Internal Medicine Kibutz Hagoshrim, June 22, 2012 Early treatment for patients with Type 2 Diabetes Eduard Montanya Hospital Universitari Bellvitge-IDIBELL CIBERDEM University of Barcelona
GLP-1RA and insulin: friends or foes?
 Tresiba Expert Panel Meeting 28/06/2014 GLP-1RA and insulin: friends or foes? Matteo Monami Careggi Teaching Hospital. Florence. Italy Dr Monami has received consultancy and/or speaking fees from: Merck
Tresiba Expert Panel Meeting 28/06/2014 GLP-1RA and insulin: friends or foes? Matteo Monami Careggi Teaching Hospital. Florence. Italy Dr Monami has received consultancy and/or speaking fees from: Merck
The Many Faces of T2DM in Long-term Care Facilities
 The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
Current principles of diabetes management
 Current principles of diabetes management Prof. Martin Haluzík, MD, DSc. 3 Department of Medicine, General University Hospital and 1st Faculty of Medicine, Charles University in Prague, Czech Republic
Current principles of diabetes management Prof. Martin Haluzík, MD, DSc. 3 Department of Medicine, General University Hospital and 1st Faculty of Medicine, Charles University in Prague, Czech Republic
Can We Reduce Heart Failure by Treating Diabetes? CVOT Data on SGLT2 Inhibitors and GLP-1Receptor Agonists
 Can We Reduce Heart Failure by Treating Diabetes? CVOT Data on SGLT2 Inhibitors and GLP-1Receptor Agonists Robert R. Henry, MD Professor of Medicine University of California, San Diego Relevant Conflict
Can We Reduce Heart Failure by Treating Diabetes? CVOT Data on SGLT2 Inhibitors and GLP-1Receptor Agonists Robert R. Henry, MD Professor of Medicine University of California, San Diego Relevant Conflict
UKPDS: Over Time, Need for Exogenous Insulin Increases
 UKPDS: Over Time, Need for Exogenous Insulin Increases Patients Requiring Additional Insulin (%) 60 40 20 Oral agents By 6 Chlorpropamide years, Glyburide more than 50% of UKPDS patients required insulin
UKPDS: Over Time, Need for Exogenous Insulin Increases Patients Requiring Additional Insulin (%) 60 40 20 Oral agents By 6 Chlorpropamide years, Glyburide more than 50% of UKPDS patients required insulin
iglarlixi Reduces Glycated Hemoglobin to a Greater Extent Than Basal Insulin Regardless of Levels at Screening: Post Hoc Analysis of LixiLan-L
 Diabetes Ther (2018) 9:373 382 https://doi.org/10.1007/s13300-017-0336-6 BRIEF REPORT iglarlixi Reduces Glycated Hemoglobin to a Greater Extent Than Basal Insulin Regardless of Levels at Screening: Post
Diabetes Ther (2018) 9:373 382 https://doi.org/10.1007/s13300-017-0336-6 BRIEF REPORT iglarlixi Reduces Glycated Hemoglobin to a Greater Extent Than Basal Insulin Regardless of Levels at Screening: Post
Basal & GLP-1 Fixed Combination Use
 Basal & GLP-1 Fixed Combination Use Michelle M. Mangual, MD Diplomate of the American board of Internal Medicine and Endocrinology, Diabetes and Metabolism San Juan City hospital Learning Objectives o
Basal & GLP-1 Fixed Combination Use Michelle M. Mangual, MD Diplomate of the American board of Internal Medicine and Endocrinology, Diabetes and Metabolism San Juan City hospital Learning Objectives o
Update on Insulin-based Agents for T2D. Harry Jiménez MD, FACE
 Update on Insulin-based Agents for T2D Harry Jiménez MD, FACE Harry Jiménez MD, FACE Has received honorarium as Speaker and/or Consultant for the following pharmaceutical companies: Eli Lilly Merck Boehringer
Update on Insulin-based Agents for T2D Harry Jiménez MD, FACE Harry Jiménez MD, FACE Has received honorarium as Speaker and/or Consultant for the following pharmaceutical companies: Eli Lilly Merck Boehringer
The Highlights of the AWARD Clinical Program FRANCESCO GIORGINO
 The Highlights of the AWARD Clinical Program FRANCESCO GIORGINO DEPARTMENT OF EMERGENCY AND ORGAN TRANSPLANTATION SECTION OF INTERNAL MEDICINE, ENDOCRINOLOGY, ANDROLOGY AND METABOLIC DISEASES Disclaimer
The Highlights of the AWARD Clinical Program FRANCESCO GIORGINO DEPARTMENT OF EMERGENCY AND ORGAN TRANSPLANTATION SECTION OF INTERNAL MEDICINE, ENDOCRINOLOGY, ANDROLOGY AND METABOLIC DISEASES Disclaimer
GLP-1 (glucagon-like peptide-1) Agonists (Byetta, Bydureon, Tanzeum, Trulicity, Victoza ) Step Therapy and Quantity Limit Criteria Program Summary
 Agonists (Byetta, Bydureon, Tanzeum, Trulicity, Victoza ) Step Therapy and Quantity Limit Criteria Program Summary") OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) s (Byetta/exenatide, Bydureon/ exenatide extended-release, Tanzeum/albiglutide, Trulicity/dulaglutide, and Victoza/liraglutide) Step Therapy
OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) s (Byetta/exenatide, Bydureon/ exenatide extended-release, Tanzeum/albiglutide, Trulicity/dulaglutide, and Victoza/liraglutide) Step Therapy
Quando l insulina basale non basta più: differenti e nuove strategie terapeutiche
 Quando l insulina basale non basta più: differenti e nuove strategie terapeutiche Giorgio Sesti Università Magna Graecia di Catanzaro Potenziali conflitti di interesse Il Prof Giorgio Sesti dichiara di
Quando l insulina basale non basta più: differenti e nuove strategie terapeutiche Giorgio Sesti Università Magna Graecia di Catanzaro Potenziali conflitti di interesse Il Prof Giorgio Sesti dichiara di
Cardiovascular Outcomes With Newer Diabetes Drugs: Results From The EMPA-REG and LEADER Trials
 Cardiovascular Outcomes With Newer Diabetes Drugs: Results From The EMPA-REG and LEADER Trials Rajiv Roy, MD Endocrinology Sharp Rees-Stealy Medical Group Background Between 1990 and 2010: Incidence of
Cardiovascular Outcomes With Newer Diabetes Drugs: Results From The EMPA-REG and LEADER Trials Rajiv Roy, MD Endocrinology Sharp Rees-Stealy Medical Group Background Between 1990 and 2010: Incidence of
Update on Diabetes Cardiovascular Outcome Trials
 Update on Diabetes Cardiovascular Outcome Trials Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of Miami Miller School of Medicine
Update on Diabetes Cardiovascular Outcome Trials Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of Miami Miller School of Medicine
Faculty. Timothy S. Reid, MD (Co-Chair, Presenter) Medical Director Mercy Diabetes Center Janesville, WI
 Medical Director Mercy Diabetes Center Janesville, WI") Activity Overview In this case-based webcast, meet Jackie, a 62-year-old woman with type 2 diabetes. Her glycated hemoglobin (HbA1C) is 9.2%, and she is taking 2 oral agents and basal insulin; however,
Activity Overview In this case-based webcast, meet Jackie, a 62-year-old woman with type 2 diabetes. Her glycated hemoglobin (HbA1C) is 9.2%, and she is taking 2 oral agents and basal insulin; however,
Insulin Initiation and Intensification. Disclosure. Objectives
 Insulin Initiation and Intensification Neil Skolnik, M.D. Associate Director Family Medicine Residency Program Abington Memorial Hospital Professor of Family and Community Medicine Temple University School
Insulin Initiation and Intensification Neil Skolnik, M.D. Associate Director Family Medicine Residency Program Abington Memorial Hospital Professor of Family and Community Medicine Temple University School
LATE BREAKING STUDIES IN DM AND CAD. Will this change the guidelines?
 LATE BREAKING STUDIES IN DM AND CAD Will this change the guidelines? Objectives 1. Discuss current guidelines for prevention of CHD in diabetes. 2. Discuss the FDA Guidance for Industry regarding evaluating
LATE BREAKING STUDIES IN DM AND CAD Will this change the guidelines? Objectives 1. Discuss current guidelines for prevention of CHD in diabetes. 2. Discuss the FDA Guidance for Industry regarding evaluating
Timely!Insulinization In!Type!2! Diabetes,!When!and!How
 Timely!Insulinization In!Type!2! Diabetes,!When!and!How, FACP, FACE, CDE Professor of Internal Medicine UT Southwestern Medical Center Dallas, Texas Current Control and Targets 1 Treatment Guidelines for
Timely!Insulinization In!Type!2! Diabetes,!When!and!How, FACP, FACE, CDE Professor of Internal Medicine UT Southwestern Medical Center Dallas, Texas Current Control and Targets 1 Treatment Guidelines for
MOA: Long acting glucagon-like peptide 1 receptor agonist
 Alexandria Rydz MOA: Long acting glucagon-like peptide 1 receptor agonist Increases glucose dependent insulin secretion Decreases inappropriate glucagon secretion Increases β- cell growth and replication
Alexandria Rydz MOA: Long acting glucagon-like peptide 1 receptor agonist Increases glucose dependent insulin secretion Decreases inappropriate glucagon secretion Increases β- cell growth and replication
Diabete: terapia nei pazienti a rischio cardiovascolare
 Diabete: terapia nei pazienti a rischio cardiovascolare Giorgio Sesti Università Magna Graecia di Catanzaro Cardiovascular mortality in relation to diabetes mellitus and a prior MI: A Danish Population
Diabete: terapia nei pazienti a rischio cardiovascolare Giorgio Sesti Università Magna Graecia di Catanzaro Cardiovascular mortality in relation to diabetes mellitus and a prior MI: A Danish Population
GLP 1 agonists Winning the Losing Battle. Dr Bernard SAMIA. KCS Congress: Impact through collaboration
 GLP 1 agonists Winning the Losing Battle Dr Bernard SAMIA KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures I have
GLP 1 agonists Winning the Losing Battle Dr Bernard SAMIA KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures I have
ADA and AACE Glycemic Targets
 ADA and AACE Glycemic Targets HbA1C target should be individualized based on a number of factors including: Age Life expectancy Comorbidities Duration of diabetes Risk of hypoglycemia Patient motivation
ADA and AACE Glycemic Targets HbA1C target should be individualized based on a number of factors including: Age Life expectancy Comorbidities Duration of diabetes Risk of hypoglycemia Patient motivation
razionale della combinazione insulina/glp-1 RAs
 Insulina e GLP-1 RAS: insieme o separati? razionale della combinazione insulina/glp-1 RAs Catania Mercure Catania Excelsior 10 ottobre 2017 Andrea Giaccari andrea.giaccari@unicatt.it Centro per le Malattie
Insulina e GLP-1 RAS: insieme o separati? razionale della combinazione insulina/glp-1 RAs Catania Mercure Catania Excelsior 10 ottobre 2017 Andrea Giaccari andrea.giaccari@unicatt.it Centro per le Malattie
COPYRIGHT. Treatment of Type 2 Diabetes: What To Do When Treatment with Metformin is Inadequate? Can We Achieve Therapeutic Goals More Safely?
 Treatment of Type 2 Diabetes: What To Do When Treatment with Metformin is Inadequate? Can We Achieve Therapeutic Goals More Safely? Martin J. Abrahamson, MD FACP Associate Professor of Medicine, Harvard
Treatment of Type 2 Diabetes: What To Do When Treatment with Metformin is Inadequate? Can We Achieve Therapeutic Goals More Safely? Martin J. Abrahamson, MD FACP Associate Professor of Medicine, Harvard
Francesca Porcellati
 XX Congresso Nazionale AMD Razionali e Benefici dell Aggiunta del GLP-1 RA Short-Acting all Insulina Basale Francesca Porcellati Dipartimento di Medicina Interna, Sezione di Medicina Interna, Endocrinologia
XX Congresso Nazionale AMD Razionali e Benefici dell Aggiunta del GLP-1 RA Short-Acting all Insulina Basale Francesca Porcellati Dipartimento di Medicina Interna, Sezione di Medicina Interna, Endocrinologia
New Drug Evaluation: lixisenatide injection, subcutaneous
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Scottish Medicines Consortium
 Scottish Medicines Consortium liraglutide 6mg/mL prefilled pen for injection (3mL) (Victoza ) Novo Nordisk Ltd. No. (585/09) 06 November 2009 The Scottish Medicines Consortium (SMC) has completed its assessment
Scottish Medicines Consortium liraglutide 6mg/mL prefilled pen for injection (3mL) (Victoza ) Novo Nordisk Ltd. No. (585/09) 06 November 2009 The Scottish Medicines Consortium (SMC) has completed its assessment
NMQF. Washington DC 2014
 NMQF Washington DC 2014 ACE/AACE Treatment Algorithm Jaime A. Davidson, MD, FACP, MACE Prof. of Medicine Division of Endocrinology, Diabetes and Metabolism President WorldWIDE Diabetes Advisor to the AACE
NMQF Washington DC 2014 ACE/AACE Treatment Algorithm Jaime A. Davidson, MD, FACP, MACE Prof. of Medicine Division of Endocrinology, Diabetes and Metabolism President WorldWIDE Diabetes Advisor to the AACE
Oral Agents. Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK
 Oral Agents Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What would your ideal diabetes drug do? Effective in lowering HbA1c No hypoglycaemia No effect on weight/ weight
Oral Agents Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What would your ideal diabetes drug do? Effective in lowering HbA1c No hypoglycaemia No effect on weight/ weight
OBESITY IN TYPE 2 DIABETES
 OBESITY IN TYPE 2 DIABETES Ashley Crowl, PharmD, BCACP Assistant Professor University of Kansas Objectives Review how to manage obesity in patients with type-2 diabetes mellitus Compare antiobesity agents
OBESITY IN TYPE 2 DIABETES Ashley Crowl, PharmD, BCACP Assistant Professor University of Kansas Objectives Review how to manage obesity in patients with type-2 diabetes mellitus Compare antiobesity agents
Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications
 Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications Nathan Woolever, Pharm.D., Resident Pharmacist Pharmacy Grand Rounds November 6 th, 2018 Franciscan Healthcare La Crosse, WI 2017
Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications Nathan Woolever, Pharm.D., Resident Pharmacist Pharmacy Grand Rounds November 6 th, 2018 Franciscan Healthcare La Crosse, WI 2017
Bedtime-to-Morning Glucose Difference and iglarlixi in Type 2 Diabetes: Post Hoc Analysis of LixiLan-L
 Diabetes Ther (2018) 9:2155 2162 https://doi.org/10.1007/s13300-018-0507-0 BRIEF REPORT Bedtime-to-Morning Glucose Difference and iglarlixi in Type 2 Diabetes: Post Hoc Analysis of LixiLan-L Ariel Zisman.
Diabetes Ther (2018) 9:2155 2162 https://doi.org/10.1007/s13300-018-0507-0 BRIEF REPORT Bedtime-to-Morning Glucose Difference and iglarlixi in Type 2 Diabetes: Post Hoc Analysis of LixiLan-L Ariel Zisman.
Management of Type 2 Diabetes Cardiovascular Outcomes Trials Tom Blevins MD Texas Diabetes and Endocrinology Austin, Texas
 Management of Type 2 Diabetes Cardiovascular Outcomes Trials 2018 Tom Blevins MD Texas Diabetes and Endocrinology Austin, Texas Speaker Disclosure Dr. Blevins has disclosed that he has received grant support
Management of Type 2 Diabetes Cardiovascular Outcomes Trials 2018 Tom Blevins MD Texas Diabetes and Endocrinology Austin, Texas Speaker Disclosure Dr. Blevins has disclosed that he has received grant support
Du gusts is megl che one. Edoardo Mannucci
 Du gusts is megl che one Edoardo Mannucci Conflitti di interessi Negli ultimi due anni, E. Mannucci ha ricevuto compensi per relazioni e/o consulenze da: Abbott, AstraZeneca, Boehringer Ingelheim, Eli
Du gusts is megl che one Edoardo Mannucci Conflitti di interessi Negli ultimi due anni, E. Mannucci ha ricevuto compensi per relazioni e/o consulenze da: Abbott, AstraZeneca, Boehringer Ingelheim, Eli
This program applies to Commercial, GenPlus and Health Insurance Marketplace formularies.
 OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) Agonists [Adlyxin (lixisenatide), Byetta (exenatide), Bydureon (exenatide extended-release), Tanzeum (albiglutide), Trulicity (dulaglutide),
OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) Agonists [Adlyxin (lixisenatide), Byetta (exenatide), Bydureon (exenatide extended-release), Tanzeum (albiglutide), Trulicity (dulaglutide),
Comprehensive Diabetes Treatment
 Comprehensive Diabetes Treatment Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism The George Washington University School of Medicine Diabetes
Comprehensive Diabetes Treatment Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism The George Washington University School of Medicine Diabetes
Managing Perioperative Diabetes What s new? Kathryn A. Myers MD FRCPC Chair Chief Division of GIM Professor of Medicine Western University
 Managing Perioperative Diabetes What s new? Kathryn A. Myers MD FRCPC Chair Chief Division of GIM Professor of Medicine Western University Objectives: By the end of this session, you will be able to: Identify
Managing Perioperative Diabetes What s new? Kathryn A. Myers MD FRCPC Chair Chief Division of GIM Professor of Medicine Western University Objectives: By the end of this session, you will be able to: Identify
Advances in Outpatient Diabetes Care: Algorithms for Care and the Role of Injectable Therapies. Module D
 Advances in Outpatient Diabetes Care: Algorithms for Care and the Role of Injectable Therapies Module D 1 Learning Objectives Apply the principles of the comprehensive diabetes algorithms to patients with
Advances in Outpatient Diabetes Care: Algorithms for Care and the Role of Injectable Therapies Module D 1 Learning Objectives Apply the principles of the comprehensive diabetes algorithms to patients with
PHARMACOLOGIC APPROACH TO ACHIEVE GLYCEMIC GOAL
 Dr Aurora Alcantara Endocrinology PHARMACOLOGIC APPROACH TO ACHIEVE GLYCEMIC GOAL SPED Convention and Diabetes Postgraduate Course May26-29 Wyndham Grand Rio Mar, PR DISCLOSURES Speaker for the following
Dr Aurora Alcantara Endocrinology PHARMACOLOGIC APPROACH TO ACHIEVE GLYCEMIC GOAL SPED Convention and Diabetes Postgraduate Course May26-29 Wyndham Grand Rio Mar, PR DISCLOSURES Speaker for the following
Non-insulin treatment in Type 1 DM Sang Yong Kim
 Non-insulin treatment in Type 1 DM Sang Yong Kim Chosun University Hospital Conflict of interest disclosure None Committee of Scientific Affairs Committee of Scientific Affairs Insulin therapy is the mainstay
Non-insulin treatment in Type 1 DM Sang Yong Kim Chosun University Hospital Conflict of interest disclosure None Committee of Scientific Affairs Committee of Scientific Affairs Insulin therapy is the mainstay
TRANSPARENCY COMMITTEE
 The legally binding text is the original French version TRANSPARENCY COMMITTEE Opinion 17 December 2014 JARDIANCE 10 mg, film-coated tablet B/30 tablets (CIP: 34009 278 928 5 1) JARDIANCE 25 mg, film-coated
The legally binding text is the original French version TRANSPARENCY COMMITTEE Opinion 17 December 2014 JARDIANCE 10 mg, film-coated tablet B/30 tablets (CIP: 34009 278 928 5 1) JARDIANCE 25 mg, film-coated
Multi-factor approach to reduce cardiovascular risk in diabetes
 Multi-factor approach to reduce cardiovascular risk in diabetes Prof. Nicola Napoli, MD PhD Division of Endocrinology and Diabetes Università Campus Bio-Medico di Roma Washington University in St Louis
Multi-factor approach to reduce cardiovascular risk in diabetes Prof. Nicola Napoli, MD PhD Division of Endocrinology and Diabetes Università Campus Bio-Medico di Roma Washington University in St Louis
DM-2 Therapy Update: GLP-1, SGLT-2 Inhibitors, and Inhaled Insulin, Oh My!
 DM-2 Therapy Update: GLP-1, SGLT-2 Inhibitors, and Inhaled Insulin, Oh My! Kevin M. Pantalone, DO, ECNU, CCD Associate Staff Director of Clinical Research Department of Endocrinology Endocrinology and
DM-2 Therapy Update: GLP-1, SGLT-2 Inhibitors, and Inhaled Insulin, Oh My! Kevin M. Pantalone, DO, ECNU, CCD Associate Staff Director of Clinical Research Department of Endocrinology Endocrinology and
The Flozins Quest for Clarity?
 The Flozins Quest for Clarity? Choosing Wisely with Academic Detailing 2018 ARE THEY THE REAL DEAL Disclosure statements The Academic Detailing Service is operated by Dalhousie Continuing Professional
The Flozins Quest for Clarity? Choosing Wisely with Academic Detailing 2018 ARE THEY THE REAL DEAL Disclosure statements The Academic Detailing Service is operated by Dalhousie Continuing Professional
insulin degludec/liraglutide 100 units/ml / 3.6mg/mL solution for injection pre-filled pen (Xultophy ) SMC No. (1088/15) Novo Nordisk A/S
 SMC No. (1088/15) Novo Nordisk A/S") insulin degludec/liraglutide 100 units/ml / 3.6mg/mL solution for injection pre-filled pen (Xultophy ) SMC No. (1088/15) Novo Nordisk A/S 4 September 2015 The Scottish Medicines Consortium (SMC) has completed
insulin degludec/liraglutide 100 units/ml / 3.6mg/mL solution for injection pre-filled pen (Xultophy ) SMC No. (1088/15) Novo Nordisk A/S 4 September 2015 The Scottish Medicines Consortium (SMC) has completed
Case Studies in Type 2 Diabetes Mellitus: Focus on Cardiovascular Outcomes Trials
 Case Studies in Type 2 Diabetes Mellitus: Focus on Cardiovascular Outcomes Trials Louis Kuritzky MD Clinical Assistant Professor Emeritus Department of Community Health and Family Medicine College of Medicine
Case Studies in Type 2 Diabetes Mellitus: Focus on Cardiovascular Outcomes Trials Louis Kuritzky MD Clinical Assistant Professor Emeritus Department of Community Health and Family Medicine College of Medicine
Albiglutide, a Once-Weekly GLP-1RA, for the Treatment of Type 2 Diabetes
 St. Onge et al. Medical Research Archives, vol. 5, issue 11, November 2017 issue Page 1 of 10 REVIEW ARTICLE Albiglutide, a Once-Weekly GLP-1RA, for the Treatment of Type 2 Diabetes Erin St. Onge 1*, Shannon
St. Onge et al. Medical Research Archives, vol. 5, issue 11, November 2017 issue Page 1 of 10 REVIEW ARTICLE Albiglutide, a Once-Weekly GLP-1RA, for the Treatment of Type 2 Diabetes Erin St. Onge 1*, Shannon
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy
 Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
MANAGING DIABETES IN 2016 WHAT TO ADD, WHEN AND WHY?
 MANAGING DIABETES IN 2016 WHAT TO ADD, WHEN AND WHY? Faculty: Maria Wolfs MD, MHSc, FRCPC Assistant Professor, University of Toronto Staff Endocrinologist, St. Michael's Hospital Relationships with commercial
MANAGING DIABETES IN 2016 WHAT TO ADD, WHEN AND WHY? Faculty: Maria Wolfs MD, MHSc, FRCPC Assistant Professor, University of Toronto Staff Endocrinologist, St. Michael's Hospital Relationships with commercial
Incretin-based Therapies for Type 2 Diabetes Comparisons Between Glucagon-like Peptide-1 Receptor Agonists and Dipeptidyl Peptidase-4 Inhibitors
 Incretin-based Therapies for Type 2 Diabetes Comparisons Between Glucagon-like Peptide-1 Receptor Agonists and Dipeptidyl Peptidase-4 Inhibitors Timothy Bailey, MD, FACE, CPI Director, AMCR Institute,
Incretin-based Therapies for Type 2 Diabetes Comparisons Between Glucagon-like Peptide-1 Receptor Agonists and Dipeptidyl Peptidase-4 Inhibitors Timothy Bailey, MD, FACE, CPI Director, AMCR Institute,
Achieving and maintaining good glycemic control is an
 Glycemic Efficacy, Weight Effects, and Safety of Once-Weekly Glucagon-Like Peptide-1 Receptor Agonists Yehuda Handelsman, MD, FACP, FNLA, FASPC, MACE; Kathleen Wyne, MD, PhD, FACE, FNLA; Anthony Cannon,
Glycemic Efficacy, Weight Effects, and Safety of Once-Weekly Glucagon-Like Peptide-1 Receptor Agonists Yehuda Handelsman, MD, FACP, FNLA, FASPC, MACE; Kathleen Wyne, MD, PhD, FACE, FNLA; Anthony Cannon,
A Practical Approach to the Use of Diabetes Medications
 A Practical Approach to the Use of Diabetes Medications Juan Pablo Frias, M.D., FACE President, National Research Institute, Los Angles, CA Clinical Faculty, University of California, San Diego, CA OUTLINE
A Practical Approach to the Use of Diabetes Medications Juan Pablo Frias, M.D., FACE President, National Research Institute, Los Angles, CA Clinical Faculty, University of California, San Diego, CA OUTLINE
Clinical Overview of Combination Therapy with Sitagliptin and Metformin
 Clinical Overview of Combination Therapy with Sitagliptin and Metformin 1 Contents Pathophysiology of type 2 diabetes and mechanism of action of sitagliptin Clinical data overview of sitagliptin: Monotherapy
Clinical Overview of Combination Therapy with Sitagliptin and Metformin 1 Contents Pathophysiology of type 2 diabetes and mechanism of action of sitagliptin Clinical data overview of sitagliptin: Monotherapy
Preventing Serious Health Consequences of Type 2 Diabetes
 Preventing Serious Health Consequences of Type 2 Diabetes The Evidence Hertzel C. Gerstein MD MSc FRCPC Professor and Population Health Institute Chair in Diabetes Research McMaster University and Hamilton
Preventing Serious Health Consequences of Type 2 Diabetes The Evidence Hertzel C. Gerstein MD MSc FRCPC Professor and Population Health Institute Chair in Diabetes Research McMaster University and Hamilton
Efficacy and Safety of Sitagliptin in Various Clinical Settings of T2DM
 Efficacy and Safety of Sitagliptin in arious Clinical Settings of T2DM Young Min Cho, MD, PhD Division of Endocrinology and Metabolism Department of Internal Medicine Seoul National University College
Efficacy and Safety of Sitagliptin in arious Clinical Settings of T2DM Young Min Cho, MD, PhD Division of Endocrinology and Metabolism Department of Internal Medicine Seoul National University College
Individualizing Care for Patients with Type 2 Diabetes
 Individualizing Care for Patients with Type 2 Diabetes Disclosures Speaker: AstraZeneca, Novo Nordisk, BI/Lilly, Valeritas, Takeda Advisor: Tandem Diabetes, Sanofi Objectives Develop individualized approaches
Individualizing Care for Patients with Type 2 Diabetes Disclosures Speaker: AstraZeneca, Novo Nordisk, BI/Lilly, Valeritas, Takeda Advisor: Tandem Diabetes, Sanofi Objectives Develop individualized approaches
Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable?
 Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable? Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of
Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable? Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of
No Increased Cardiovascular Risk for Lixisenatide in ELIXA
 ON ISSUES IN THE MANAGEMENT OF TYPE 2 DIABETES JUNE 2015 Coverage of data from ADA 2015, June 5 9 in Boston, Massachusetts No Increased Cardiovascular Risk for Lixisenatide in ELIXA First Cardiovascular
ON ISSUES IN THE MANAGEMENT OF TYPE 2 DIABETES JUNE 2015 Coverage of data from ADA 2015, June 5 9 in Boston, Massachusetts No Increased Cardiovascular Risk for Lixisenatide in ELIXA First Cardiovascular
Management of Diabetes
 Management of Diabetes Mellitus: Which Drugs for Which Patients? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu Disclosure No relevant financial relationships
Management of Diabetes Mellitus: Which Drugs for Which Patients? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu Disclosure No relevant financial relationships
Lilly Diabetes: Pipeline Update
 Lilly Diabetes: Pipeline Update June 16, 2014 Safe Harbor Provision This presentation contains forward-looking statements that are based on management's current expectations, but actual results may differ
Lilly Diabetes: Pipeline Update June 16, 2014 Safe Harbor Provision This presentation contains forward-looking statements that are based on management's current expectations, but actual results may differ
GLP-1 agonists. Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK
 GLP-1 agonists Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What do GLP-1 agonists do? Physiology of postprandial glucose regulation Meal ❶ ❷ Insulin Rising plasma
GLP-1 agonists Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What do GLP-1 agonists do? Physiology of postprandial glucose regulation Meal ❶ ❷ Insulin Rising plasma
Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes
 Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes Genetics, environment, and lifestyle (obesity, inactivity, poor diet) Impaired fasting glucose Decreased β-cell
Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes Genetics, environment, and lifestyle (obesity, inactivity, poor diet) Impaired fasting glucose Decreased β-cell
Help the Heart. An Update on GLP-1 Agonists and SGLT2 Inhibitors. Tara Hawley, PharmD PGY1 Pharmacy Resident Mayo Clinic Health System Eau Claire
 Help the Heart An Update on GLP-1 Agonists and SGLT2 Inhibitors Tara Hawley, PharmD PGY1 Pharmacy Resident Mayo Clinic Health System Eau Claire Mayo Clinic Grand Rounds May 16, 2017 2017 MFMER slide-1
Help the Heart An Update on GLP-1 Agonists and SGLT2 Inhibitors Tara Hawley, PharmD PGY1 Pharmacy Resident Mayo Clinic Health System Eau Claire Mayo Clinic Grand Rounds May 16, 2017 2017 MFMER slide-1
Updates in Diabetes and Cardiovascular Disease Management: Are You Making the Link?
 Updates in Diabetes and Cardiovascular Disease Management: Are You Making the Link? Denise Kolanczyk, PharmD, BCPS AQ Cardiology 1 Erika Hellenbart, PharmD, BCPS 2 Jennifer D Souza, PharmD, CDE, BC ADM
Updates in Diabetes and Cardiovascular Disease Management: Are You Making the Link? Denise Kolanczyk, PharmD, BCPS AQ Cardiology 1 Erika Hellenbart, PharmD, BCPS 2 Jennifer D Souza, PharmD, CDE, BC ADM
Empagliflozin (Jardiance ) for the treatment of type 2 diabetes mellitus, the EMPA REG OUTCOME study
 for the treatment of type 2 diabetes mellitus, the EMPA REG OUTCOME study") Empagliflozin (Jardiance ) for the treatment of type 2 diabetes mellitus, the EMPA REG OUTCOME study POSITION STATEMENT: Clinicians should continue to follow MHRA advice and NICE technology appraisal guidance
Empagliflozin (Jardiance ) for the treatment of type 2 diabetes mellitus, the EMPA REG OUTCOME study POSITION STATEMENT: Clinicians should continue to follow MHRA advice and NICE technology appraisal guidance
ADA Analyst Presentation Saturday 9 th June
 ADA Analyst Presentation Saturday 9 th June Carlo Russo Senior Vice-President & Albiglutide Team Leader, GSK Property of GlaxoSmithKline Agenda Welcome & introduction to the Harmony Clinical Programme
ADA Analyst Presentation Saturday 9 th June Carlo Russo Senior Vice-President & Albiglutide Team Leader, GSK Property of GlaxoSmithKline Agenda Welcome & introduction to the Harmony Clinical Programme
Agenda. Indications Different insulin preparations Insulin initiation Insulin intensification
 Insulin Therapy F. Hosseinpanah Obesity Research Center Research Institute for Endocrine sciences Shahid Beheshti University of Medical Sciences November 11, 2017 Agenda Indications Different insulin preparations
Insulin Therapy F. Hosseinpanah Obesity Research Center Research Institute for Endocrine sciences Shahid Beheshti University of Medical Sciences November 11, 2017 Agenda Indications Different insulin preparations
Update on Cardiovascular Outcome Trials in Diabetes Jay S. Skyler, MD, MACP
 Update on Cardiovascular Outcome Trials in Diabetes Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research InsAtute University of Miami Miller School of Medicine
Update on Cardiovascular Outcome Trials in Diabetes Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research InsAtute University of Miami Miller School of Medicine
Beyond Basal Insulin: Intensification of Therapy Jennifer D Souza, PharmD, CDE, BC-ADM
 Beyond Basal Insulin: Intensification of Therapy Jennifer D Souza, PharmD, CDE, BC-ADM Disclosures Jennifer D Souza has no conflicts of interest to disclose. 2 When Basal Insulin Is Not Enough Learning
Beyond Basal Insulin: Intensification of Therapy Jennifer D Souza, PharmD, CDE, BC-ADM Disclosures Jennifer D Souza has no conflicts of interest to disclose. 2 When Basal Insulin Is Not Enough Learning
Your Chart Review Data. Lara Zisblatt, MA Assistant Director Continuing Medical Education Boston University School of Medicine
 Your Chart Review Data Lara Zisblatt, MA Assistant Director Continuing Medical Education Boston University School of Medicine Participation 243 registered for the program 98 have completed the Practice
Your Chart Review Data Lara Zisblatt, MA Assistant Director Continuing Medical Education Boston University School of Medicine Participation 243 registered for the program 98 have completed the Practice
New Drug Evaluation: Dulaglutide
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
What s New in Type 2? Peter Hammond Consultant Physician Harrogate District Hospital
 What s New in Type 2? Peter Hammond Consultant Physician Harrogate District Hospital Therapy considerations in T2DM Thiazoledinediones DPP IV inhibitors GLP 1 agonists Insulin Type Delivery Horizon scanning
What s New in Type 2? Peter Hammond Consultant Physician Harrogate District Hospital Therapy considerations in T2DM Thiazoledinediones DPP IV inhibitors GLP 1 agonists Insulin Type Delivery Horizon scanning
Diabetes new challenges, new agents, new order
 Diabetes new challenges, new agents, new order Ken Earle St Georges University Hospitals NHS Foundation Trust Overview Cardiovascular disease unmet needs Treating evident and residual risk Integrating
Diabetes new challenges, new agents, new order Ken Earle St Georges University Hospitals NHS Foundation Trust Overview Cardiovascular disease unmet needs Treating evident and residual risk Integrating
Optimizing Treatment Strategies to Improve Patient Outcomes in the Management of Type 2 Diabetes
 Optimizing Treatment Strategies to Improve Patient Outcomes in the Management of Type 2 Diabetes Philip Raskin, MD Professor of Medicine The University of Texas, Southwestern Medical Center NAMCP Spring
Optimizing Treatment Strategies to Improve Patient Outcomes in the Management of Type 2 Diabetes Philip Raskin, MD Professor of Medicine The University of Texas, Southwestern Medical Center NAMCP Spring
Application of the Diabetes Algorithm to a Patient
 Application of the Diabetes Algorithm to a Patient Apply knowledge gained from this activity to improve disease management and outcomes for patients with T2DM and obesity Note: The cases in this deck represent
Application of the Diabetes Algorithm to a Patient Apply knowledge gained from this activity to improve disease management and outcomes for patients with T2DM and obesity Note: The cases in this deck represent
Pharmacology Updates. Quang T Nguyen, FACP, FACE, FTOS 11/18/17
 Pharmacology Updates Quang T Nguyen, FACP, FACE, FTOS 11/18/17 14 Classes of Drugs Available for the Treatment of Type 2 DM in the USA ### Class A1c Reduction Hypoglycemia Weight Change Dosing (times/day)
Pharmacology Updates Quang T Nguyen, FACP, FACE, FTOS 11/18/17 14 Classes of Drugs Available for the Treatment of Type 2 DM in the USA ### Class A1c Reduction Hypoglycemia Weight Change Dosing (times/day)
COMMISSIONING POLICY RECOMMENDATION TREATMENT ADVISORY GROUP Policy agreed by (Vale of York CCG/date)
") Drug, Treatment, Device name ( Vipidia; Takeda) COMMISSIONING POLICY RECOMMENDATION TREATMENT ADVISORY GROUP Policy agreed by (Vale of York CCG/date) Licensed indication To improve glycaemic control in
Drug, Treatment, Device name ( Vipidia; Takeda) COMMISSIONING POLICY RECOMMENDATION TREATMENT ADVISORY GROUP Policy agreed by (Vale of York CCG/date) Licensed indication To improve glycaemic control in
La lezione dei trials di safety cardiovascolare. Edoardo Mannucci
 La lezione dei trials di safety cardiovascolare Edoardo Mannucci Conflitti di interessi Negli ultimi due anni, E. Mannucci ha ricevuto compensi per relazioni e/o consulenze da: Abbott, AstraZeneca, Boehringer
La lezione dei trials di safety cardiovascolare Edoardo Mannucci Conflitti di interessi Negli ultimi due anni, E. Mannucci ha ricevuto compensi per relazioni e/o consulenze da: Abbott, AstraZeneca, Boehringer
Professor Rudy Bilous James Cook University Hospital
 Professor Rudy Bilous James Cook University Hospital Rate per 100 patient years Rate per 100 patient years 16 Risk of retinopathy progression 16 Risk of developing microalbuminuria 12 12 8 8 4 0 0 5 6
Professor Rudy Bilous James Cook University Hospital Rate per 100 patient years Rate per 100 patient years 16 Risk of retinopathy progression 16 Risk of developing microalbuminuria 12 12 8 8 4 0 0 5 6
Reviewing Diabetes Guidelines. Newsletter compiled by Danny Jaek, Pharm.D. Candidate
 Reviewing Diabetes Guidelines Newsletter compiled by Danny Jaek, Pharm.D. Candidate AL AS KA N AT IV E DI AB ET ES TE A M Volume 6, Issue 1 Spring 2011 Dia bet es Dis pat ch There are nearly 24 million
Reviewing Diabetes Guidelines Newsletter compiled by Danny Jaek, Pharm.D. Candidate AL AS KA N AT IV E DI AB ET ES TE A M Volume 6, Issue 1 Spring 2011 Dia bet es Dis pat ch There are nearly 24 million
Evidence-Based Glucose Management in Type 2 Diabetes
 Evidence-Based Glucose Management in Type 2 Diabetes James R. Gavin III, MD, PhD CEO and Chief Medical Officer Healing Our Village, Inc. Clinical Professor of Medicine Emory University School of Medicine
Evidence-Based Glucose Management in Type 2 Diabetes James R. Gavin III, MD, PhD CEO and Chief Medical Officer Healing Our Village, Inc. Clinical Professor of Medicine Emory University School of Medicine
An Update on Guidelines and Evidence of the Treatment of Type 2 Diabetes Mellitus
 Nevada Academy of Family Physicians 29 th Annual Summer CME Meeting August 3 5, 2018 An Update on Guidelines and Evidence of the Treatment of Type 2 Diabetes Mellitus Presented by: James D. Honeycutt,
Nevada Academy of Family Physicians 29 th Annual Summer CME Meeting August 3 5, 2018 An Update on Guidelines and Evidence of the Treatment of Type 2 Diabetes Mellitus Presented by: James D. Honeycutt,
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE. Single Technology Appraisal. Canagliflozin in combination therapy for treating type 2 diabetes
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Single Technology Appraisal Canagliflozin in combination therapy for Final scope Remit/appraisal objective To appraise the clinical and cost effectiveness
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Single Technology Appraisal Canagliflozin in combination therapy for Final scope Remit/appraisal objective To appraise the clinical and cost effectiveness
Alia Gilani Health Inequalities Pharmacist
 Alia Gilani Health Inequalities Pharmacist THE SOUTH ASIAN HEALTH FOUNDATION (U.K.) (Registered Charity No. 1073178) 1. Case Study 2. Factors influencing prescribing 3. Special Considerations 4. Prescribing
Alia Gilani Health Inequalities Pharmacist THE SOUTH ASIAN HEALTH FOUNDATION (U.K.) (Registered Charity No. 1073178) 1. Case Study 2. Factors influencing prescribing 3. Special Considerations 4. Prescribing
sitagliptin, 25mg, 50mg and 100mg film-coated tablets (Januvia ) SMC No. (1083/15) Merck Sharp and Dohme UK Ltd
 SMC No. (1083/15) Merck Sharp and Dohme UK Ltd") sitagliptin, 25mg, 50mg and 100mg film-coated tablets (Januvia ) SMC No. (1083/15) Merck Sharp and Dohme UK Ltd 07 August 2015 The Scottish Medicines Consortium (SMC) has completed its assessment of the
sitagliptin, 25mg, 50mg and 100mg film-coated tablets (Januvia ) SMC No. (1083/15) Merck Sharp and Dohme UK Ltd 07 August 2015 The Scottish Medicines Consortium (SMC) has completed its assessment of the
Newer Diabetes Treatments Drug Class Update with New Drug Evaluation: Semaglutide and Ertugliflozin
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Type 2 Diabetes Management: Case 1: Reducing Hypoglycemic Risk Case 2: Reducing Cardiovascular Risk
 Type 2 Diabetes Management M. Susan Burke, MD, FACP Clinical Associate Professor of Medicine Sidney Kimmel Medical College at Thomas Jefferson University Senior Advisor, Lankenau Medical Associates Lankenau
Type 2 Diabetes Management M. Susan Burke, MD, FACP Clinical Associate Professor of Medicine Sidney Kimmel Medical College at Thomas Jefferson University Senior Advisor, Lankenau Medical Associates Lankenau
Dr Karen McNeil Consultant Endocrinologist
 Dr Karen McNeil Consultant Endocrinologist Aged 53 Type 2 Diabetes 2010 HbA1c 7.9% ACR 5.3 mg/mmol What treatment? MF 500 mg bd (misses midday dose) Control Symptoms, BGL Complications DR, DN, PN Associations
Dr Karen McNeil Consultant Endocrinologist Aged 53 Type 2 Diabetes 2010 HbA1c 7.9% ACR 5.3 mg/mmol What treatment? MF 500 mg bd (misses midday dose) Control Symptoms, BGL Complications DR, DN, PN Associations
Chief of Endocrinology East Orange General Hospital
 Targeting the Incretins System: Can it Improve Our Ability to Treat Type 2 Diabetes? Darshi Sunderam, MD Darshi Sunderam, MD Chief of Endocrinology East Orange General Hospital Age-adjusted Percentage
Targeting the Incretins System: Can it Improve Our Ability to Treat Type 2 Diabetes? Darshi Sunderam, MD Darshi Sunderam, MD Chief of Endocrinology East Orange General Hospital Age-adjusted Percentage
Medical therapy advances London/Manchester RCP February/June 2016
 Medical therapy advances London/Manchester RCP February/June 2016 Advances in medical therapies for diabetes mellitus Duality of interest: The speaker or institutions with which he is associated has received
Medical therapy advances London/Manchester RCP February/June 2016 Advances in medical therapies for diabetes mellitus Duality of interest: The speaker or institutions with which he is associated has received
Drug Therapy for Diabetes Mellitus. Adj A/Prof Daniel Chew Dept of Endocrinology 8 th July 2017
 Drug Therapy for Diabetes Mellitus Adj A/Prof Daniel Chew Dept of Endocrinology 8 th July 2017 Diabetes Subtypes Optimal Treatment Ominous Octet DeFronzo. DIABETES, VOL. 58, APRIL 2009 Schematic Overview
Drug Therapy for Diabetes Mellitus Adj A/Prof Daniel Chew Dept of Endocrinology 8 th July 2017 Diabetes Subtypes Optimal Treatment Ominous Octet DeFronzo. DIABETES, VOL. 58, APRIL 2009 Schematic Overview
Pramlintide & Weight. Diane M Karl MD. The Endocrine Clinic & Oregon Health & Science University Portland, Oregon
 Pramlintide & Weight Diane M Karl MD The Endocrine Clinic & Oregon Health & Science University Portland, Oregon Conflict of Interest Speakers Bureau: Amylin Pharmaceuticals Consultant: sanofi-aventis Grant
Pramlintide & Weight Diane M Karl MD The Endocrine Clinic & Oregon Health & Science University Portland, Oregon Conflict of Interest Speakers Bureau: Amylin Pharmaceuticals Consultant: sanofi-aventis Grant
Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC
 Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC Choosing the Right Agent for your Patient with diabetes: Individualizing type 2 diabetes management in light of the expanding therapies
Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC Choosing the Right Agent for your Patient with diabetes: Individualizing type 2 diabetes management in light of the expanding therapies
Drug Class Update with New Drug Evaluation: Non-insulin Diabetes Treatments (SGLT-2 Inhibitors and GLP-1 Receptor Agonists)
") Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
The Alphabet Soup of Diabetes. Egils Bogdanovics M.D. Hungerford Diabetes Center
 The Alphabet Soup of Diabetes Egils Bogdanovics M.D. Hungerford Diabetes Center Insulin: January 11, 1922 12 year old Leonard Thompson, on a starvation diet for 2 years received his first insulin injection
The Alphabet Soup of Diabetes Egils Bogdanovics M.D. Hungerford Diabetes Center Insulin: January 11, 1922 12 year old Leonard Thompson, on a starvation diet for 2 years received his first insulin injection
What s New in Type 2 Diabetes? 2018 Diabetes Updates
 What s New in Type 2 Diabetes? 2018 Diabetes Updates Gretchen Ray, PharmD, PhC, BCACP, CDE Associate Professor, UNM College of Pharmacy January 28, 2018 gray@salud.unm.edu OBJECTIVES Describe the most
What s New in Type 2 Diabetes? 2018 Diabetes Updates Gretchen Ray, PharmD, PhC, BCACP, CDE Associate Professor, UNM College of Pharmacy January 28, 2018 gray@salud.unm.edu OBJECTIVES Describe the most
Glucagon-like peptide-1 (GLP-1) Agonists Drug Class Prior Authorization Protocol
 Agonists Drug Class Prior Authorization Protocol") Glucagon-like peptide-1 (GLP-1) Agonists Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed
Glucagon-like peptide-1 (GLP-1) Agonists Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed