2017 Stage 1 & 2 Medicaid Meaningful Use Guide
|
|
|
- Ethan Carson
- 5 years ago
- Views:
Transcription

1 2017 Stage 1 & 2 Medicaid Meaningful Use Guide
2 CONTENTS MEANINGFUL USE INTRODUCTION... 3 USING THIS GUIDE... 5 OBJECTIVES, MEASURES, CRITERIA & REQUIRED ANCILLARY SERVICES... 6 HOW TO RUN A MEANINGFUL USE REPORT HOW TO RUN A CLINICAL QUALITY REPORT HOW TO RUN THE PATIENT BY VOLUME REPORT FOR MEANINGFUL USE...15 TAKING SCREENSHOTS...18 OBJECTIVE #1: PROTECT PATIENT HEALTH INFORMATION...19 OBJECTIVE #2: CLINICAL DECISION SUPPORT...20 OBJECTIVE #3: CPOE OBJECTIVE #4: ELECTRONIC PRESCRIBING OBJECTIVE #5: HEALTH INFORMATION EXCHANGE OBJECTIVE #6: PATIENT SPECIFIC EDUCATION...49 OBJECTIVE#7: MEDICATION RECONCILIATION...51 OBJECTIVE #8: PATIENT ELECTRONIC ACCESS OBJECTIVE #9: SECURE MESSAGING OBJECTIVE #10: PUBLIC HEALTH REPORTING...59 CLINICAL QUALITY MEASURES
3 MEANINGFUL USE INTRODUCTION The Health Information Technology for Economic and Clinical Health (HITECH) Act, enacted as part of the American Recovery and Reinvestment Act (ARRA) of 2009, promotes the adoption and Meaningful Use of health information technology. One of its specific goals is to encourage physicians to adopt Electronic Health Record (EHR) software. The HITECH and ARRA acts include incentive payments to physicians who demonstrate Meaningful Use of a certified EHR application. One of its specific goals is to increase physician adoption of EHR applications to 90 percent by Participation in the Medicare EHR incentive program began in To receive incentive payments for EHR adoption, physicians must demonstrate that they are using a certified EHR in the manner proscribed by The Department of Health and Human Services as Meaningful Use. Pediatricians must have at minimum 20% Medicaid patient volume Check with your state requirements as some states require 30% for Pediatricians Non-Pediatrician providers must have at minimum 30% Medicaid patient volume The Department of Health and Human Services (HHS) definition of Meaningful Use expands over three stages: STAGE 1 Data capturing and sharing STAGE 2 Advanced clinical processes STAGE 3 Improved outcomes PROGRAM PENALTIES FOR NON-PARTICIPATION For Medicaid there are no program penalties. 3
4 EHR INCENTIVE PAYMENT SCHEDULE: MEDICAID Year $21, $8,500 $21, $8,500 $8,500 $21, $8,500 $8,500 $8,500 $21, $8,500 $8,500 $8,500 $8,500 $21, $8,500 $8,500 $8,500 $8,500 $8,500 $21, $0 $8,500 $8,500 $8,500 $8,500 $8, $0 $0 $8,500 $8,500 $8,500 $8, $0 $0 $0 $8,500 $8,500 $8, $0 $0 $0 $0 $8,500 $8, $0 $0 $0 $0 $0 $8,500 TOTAL $63,750 $63,750 $63,750 $63,750 $63,750 $63,750 4
5 USING THIS GUIDE This guide provides a general introduction to using Aprima PRM 2015 for Meaningful Use Stage 1 and 2 reporting in the 2017 calendar year for the Medicaid EHR Incentive Program. THIS DOCUMENT: Provides an in depth contextual explanation of each objective. Comes complete with screen shots from Aprima accompanied by easy to follow step-bystep instructions of how to meet each objective. Describes each Clinical Quality Measure supported by Aprima and how to successfully document these measures. 5
6 OBJECTIVES, MEASURES, CRITERIA & REQUIRED ANCILLARY SERVICES To demonstrate Meaningful Use for Stage 1 and Stage 2, you must report on: 10 core measure objectives Nine clinical quality measures REQUIREMENTS: (For both MU and CQM reporting) Provider tax identification number (ETIN) Provider National Provider Identification number (NPI) Provider Information: first and last name, specialty, phone number Patient Information: First name, last name, gender, date of birth, race, ethnicity, language Provide Patient Volume information to prove Medicaid Volume OBJECTIVES: Protect Patient Health Information. (security risk analysis) Clinical Decision Support. (must implement five rules as well as turn on drug formulary checks) Computerized Provider Order Entry (provider must order their own prescriptions, labs and radiology orders) Electronic Prescribing (medications being sent electronically) Health Information Exchange (direct mail, HISP) Patient Specific Education (education forms) Medication Reconciliation Patient Electronic Access (patient portal) Secure Messaging (communication via patient portal) Public Health Reporting (immunization registry, syndromic surveillance reporting, specialized registry reporting) 6
7 CLINICAL QUALITY MEASURES: Clinical quality measures must be selected from at least three of the six key health care policy domains defined by the Department of Health and Human Services National Quality Strategy. The health care policy domains are: Patient and Family Engagement Patient Safety Care Coordination Population and Public Health Efficient Use of Healthcare Resources Clinical Processes/Effectiveness ANCILLARY SERVICES: Ancillary Services are required for successful Meaningful Use attestation. These ancillary services provided at an additional cost and include: Aprima Patient Portal Direct Secure Mail Surescripts electronic pharmacy clearinghouse Interface with an immunization registry or immunization information systems Interface with public health agency Interface with specialized registry, other than for immunizations, syndromic surveillance or cancer INACTIVE ITEMS: (Before October 1, 2015) Record Demographics Record Vital Signs Record Smoking Status Clinical Summaries Structured Lab Results Patient List Patient Reminders Summary of Care Measure 1 Any Method 7
8 Measure 3 Test Electronic Notes Imaging Results Family Health History REPORTING PERIOD 2017 For all new participants, the EHR reporting period is a minimum of any continuous 90 days between January 1 and December 31, For all returning participants, the EHR reporting period is a full year between January 1 and December 31, For the 2017 EHR reporting period, the attestation deadline is February 28, ATTESTATION WEBSITE When you are ready to attest, you will access your state Medicaid website. If you need to modify your registration this can be done on the Medicare & Medicaid EHR Incentive Program Registration and Attestation System. To access this system please log on to using your username and password for the National Plan and Provider Enumeration System (NPPES). 8

9 HOW TO RUN A MEANINGFUL USE REPORT All reports are to be obtained directly out of Aprima for reporting purposes. To obtain a report please proceed to your report icon on your desktop. STEP BY STEP INSTRUCTIONS From your Aprima desktop, select the Reports icon. In the View Report window, select the Meaningful Use Stage report from the Clinical Quality menu. All providers regardless of stage will run this report as it shows you the list of measures based on the final rule released by the CMS in October

10 In the Filter Attributes select the provider you wish to run the report for and then select the reporting period. When checking your provider s status for the 2016 reporting period be sure to run it for the entire year. Select View to display the report. Leave the Provider Option on Billing Provider unless you are generating your report for midlevel provider for their Medicaid attestation and they bill under a different provider. In this instance select Rendering Provider. The report will then appear. To print the report, select the Print button. You may also export the report as a PDF, Word or Excel document using the floppy disk with a green arrow icon. If a measure has a N/A in the numerator/denominator column this means that the system was not able to calculate the data due to no data being entered or due to the measure being a Yes/No attestation instead of a threshold. To view more details about the measure, select the plus sign next to Measure Details. This will show you all of the patients who have been applied to the measure. You may select the patients name to access their chart from the report. 10
11 11

12 HOW TO RUN A CLINICAL QUALITY MEASURE REPORT FOR MEANINGFUL USE OBJECTIVE Allow the user to understand how to run the CQM report for Meaningful Use from the Reports icon. STEP BY STEP INSTRUCTIONS From your Aprima desktop, select the Reports icon. In the View Report window, select the CQM 2015 report from the Clinical Quality menu. All providers regardless of stage will run this report as it shows you the list of measures based on the final rule released by the CMS in October For the Filter Attributes: Select search next to your Filter Name to pull in a filter if you have created one. If you do not have a filter please proceed with the following items. The Description field is left blank. The CMS Program radio button should be on Meaningful Use Only. 12

13 The Payer field for both a Medicare and Medicaid provider will be left blank to pull in all insurance carriers. Search for and select the provider name the report is for in the Provider field. Leave the Provider Option on Billing Provider unless the provider the report is for is never the billing provider then select Rendering Provider. The Measure Date is for the entire reporting period (i.e. the entire year or 90 day reporting period as designated by your Meaningful Use Stage or by the CMS). Select the nine (or more) measures that you have predetermined. Leave the Financial Center and Service Site fields blank to include all visits and select VIEW. The QRDA Calculated Summary Report will display. The emeasure Identifier (MAT) is what you will use to identify the measure in the EHR Incentive Program reporting website. You will then use the Denominator, Numerator, Performance Rate, Exclusions and Exceptions when reporting the data. Select the blue printer icon to print the report. 13

14 *Should you have difficulty displaying the report contact your Account Manager. 14

15 HOW TO RUN THE PATIENT BY VOLUME REPORT FOR MEANINGFUL USE OBJECTIVE Allow the user to understand how to run the Patient by Volume for Meaningful Use report from the Reports icon for Medicaid Meaningful Use providers only. STEP BY STEP INSTRUCTIONS From your Aprima desktop, select the Reports icon. Select the Patient Volume for Meaningful Use report from the Clinical Quality menu. For the Filter Attributes: Leave the Provider Option on Billing Provider unless the provider the report is for is never a billing provider. Pull in the provider s name in the Provider field you wish to run the report for. (If you are running the report for the group volume numbers, leave this field blank.) If needed, select a specific Financial Center or Service Site. For the Render Option, select Insurance Payer. 15

16 Leave the Patient Account Type blank. Select all Medicaid payers in the Insurance Payer field. For the Visit Date, select the 90 period you will be using. Under Insurance Option chose to use Primary Insurance Only or to Include Secondary. You can choose to Group by Provider if you are using separate volumes for each provider. For the Insurance Payment option, you will typically leave it on All Visits. 16
17 When the report generates you can choose to select the payer to view the names of the patients included in the payer group or simply select the Print button to print the report. Select the back arrow to return to the main screen of the report. 17
18 TAKING SCREENSHOTS OBJECTIVE Inform physician on how to take appropriate screenshots for measures that are a Yes/No. STEP BY STEP INSTRUCTIONS For those measures requiring screen shots, you can accomplish this in two different ways. If a whole screen is necessary, simply use the Print Screen, [Prt Sc], button on your keyboard. This will copy the entire contents of your viewable monitor. If you have multiple monitors, this will capture both screens. If you need to capture a smaller section or an individual window, you can also use a combination of the [Alt] key and [Prt Sc] key. To use this combination, you will just need to make sure that the window that you intend to capture is selected as your main focus. This is done by simply using your mouse and clicking on the window intended for capture and then pressing the [Alt] and [Prt Sc] keys together. Once you have taken your screen shot it may appear that nothing has happened, but a copy of your screen has been saved to your clipboard. To retrieve your image, you will want to open any program that will allow you to paste an image. Once you have this program opened, you will want to use the Paste command by either right clicking in blank space on your document and selecting Paste, or by using the command [Ctrl] [V]. Save the document you have created with the name of the measure and the date the screen shot was taken for easy identification. The measures necessary to screenshot are: Objective 2 Measure 1- Clinical Decision Support Objective 2 Measure 2- Drug Screening Objective 9- Patient Portal Messaging Objective 10 Measure 1- Immunization Registry (if applicable) 18
19 OBJECTIVE #1: PROTECT ELECTRONIC HEALTH INFORMATION OBJECTIVE Allow provider to understand how to protect electronic information. CONTEXT Provers should protect electronic health information created or maintained by the certified EHR technology (CEHRT) through the implementation of appropriate technical capabilities. Conduct or review a Security Risk Analysis in accordance with the requirements under 45 CFR (a)(1), including addressing the security (to include encryption) of ephi created and maintained by Certified EHR Technology (CEHRT) in accordance with requirements in 45 CFR (a)(2)(iv) and 45 CFR (d)(3), and implement security updates as necessary and correct identified security deficiencies as part of the provider s risk management process for EPs. EXCLUSION None. STEP BY STEP INSTRUCTIONS No data entry is required to report on this measure. To meet the measure s goal, you must attest Yes to having conducted or reviewed a security risk analysis in accordance with the requirements under 45 CFR (a) (1) prior or during the EHR reporting period. You may complete your Security Risk Analysis by using DAS Health s SRA services (consult your Account Manager). DAS services reduce your required staff time, ensures completion of all requirements, and provides all necessary documentation. Alternatively, The Office of the National Coordinator for Health Information Technology has made available a downloadable Security Risk Analysis Tool (requires manual completion without support) that can be accessed from their website: 19
20 OBJECTIVE #2: CLINICAL DECISION SUPPORT RULE OBJECTIVE Allow provider to understand how to use Clinical Decision Support Rules, formally known as Health Maintenance Rules. CONTEXT Stage 1: Use clinical decision support to improve performance on high-priority health conditions. Measure 1: Implement one clinical decision support rule relevant to specialty or high clinical priority, along with the ability to track compliance with that rule. Stage 2: Use clinical decision support to improve performance on high-priority health conditions. Measure 1: Implement five clinical decision support interventions related to four or more clinical quality measures at a relevant point in patient care for the entire EHR reporting period. Absent four clinical quality measures related to an EP s scope of practice or patient population, the clinical decision support interventions must be related to high-priority health conditions. Measure 2: The EP has enabled and implemented the functionality for drug-drug and drug-allergy interaction checks for the entire EHR reporting period. EXCLUSIONS There are no exclusions for this rule. STEP BY STEP INSTRUCTIONS Measure 1: Create 1 Clinical Decision Support Rule for Stage 1 or 5 Clinical Decision Support Rules for Stage 2. For Stage 2, the Clinical Decision Support Rules must be associated with 4 Clinical Quality Measures from three different domains. 20

21 Start from the Aprima Desktop, go to List Editor, click on Clinical, then Clinical Decision Support Rules. Create the rule using the three tabs: General, Criteria and Care Team. The New Clinical Decision Support window will open to the General tab: Type the name of the rule in the Name field. Example: Well Woman Exam Place a check in the box if this rule is to "Report as Preventative Follow-up" Place a check in the box for "Procedures to be Completed" this will active the rest of the fields. In the Recurrence fields define how often you wish for the rule to occur for all patients. In this example it is occurring once a year (Every 1 to 1 years). To limit the recurrences, check the box next to Limit Recurrence and specify in the number in the Max Recurrence box. If an advanced warning is desired specify the time frame such as a 30-day warning before the due date. Specify the procedures to be completed in the Procedures find box. 21

22 Select the Criteria tab: Define the age range for which the rule is applicable, such as 3 to 6 months or 40 to 65 years. Define Gender. This choice is multi-select, so you can select Male and Female for any tests that are not gender specific. Define Patient Medical History. This field is multi-select, so you can add all medical history to which the rule will apply. Define the drug or drug class. These are multi-select fields, so you can add all the medications to which the rule will apply. However, you can only select by either drug or drug class; you cannot select by both drug and drug class. Define the lab result criteria: In the LOINC field, select the code for the laboratory test you want to associate with the health maintenance rule. In the Result Is field, select the operator for the value. For example, select the > operator if you are interested in results greater than a certain value. In the Value field, enter the lab result value. 22
 button. Select the desired Observation item.")
23 Define observation criteria if appropriate. Select the Edit Observation Criteria button. This accesses the Edit Observation Criteria window, where you can define an equation for observation values. You may want to write down your equation before you start to enter it. To enter a clause, select the open parentheses ( ) button. Select the desired Observation item. Select the Not button if appropriate. Select a comparison operator (=, <, >, Like, etc.). Enter the literal value for the observation. Select the Insert button to add the criteria to the equation. Your criteria will display in the Current Observation Criteria area. To close a clause, select the close parentheses ( ) button. If needed, select the And or Or buttons to begin another clause. Then repeat sub steps to enter the next clause. To edit the equation, select the << button to backspace through the equation. When finished, select the OK button to save the observation equation and return to the Clinical Decision Support window. Your equation displays in the Observation Criteria area. 23

24 Select the Care Team tab: Select the Care Team. Select the Msg (message) Recipient(s) for the rule. When a rule becomes due, a message is sent to the message recipients to alert them of the rule. The message recipients do not need to be members of the care team; they can be other users, such as front desk staff. Select which providers, if any, wish to opt out, that is do not wish to be associated with the rule. Repeat the sub steps for each care team that will use the rule. Within the Full Note Composer, access the CDS Slider > slide bar to far right > click action on the appropriate rule group. Action CDS by selecting either HM Hx, SO, SP, Plan or Declined. This will then trigger the next appropriate rule date. 24


25 Measure 2: From the Aprima Desktop, click on the Tools drop down menu > select Configure Practice Settings > Drug Screening. Make sure the box for Drug to Drug Interaction box is checked. 25


26 This measure is suggested to have a screen shots for supporting documentation. The following are examples of the suggested screen shots to support the measures. Measure 1 Screenshot #1: Screenshot of CDS Rules being tracked in a patient s chart. Include the date and time in the screenshot. 26


27 Measure 1 Screenshot #2: Screenshot of list of CDS rules from List Editor. Include the date and time in the screenshot. Measure 2 Screenshot: Screenshot of Drug Screening Configuration from Configure Practice Settings located in the Tools menu. Include the date and time in the screenshot. 27
28 OBJECTIVE #3: COMPUTERIZED PROVIDER ORDER ENTRY (CPOE) OBJECTIVE Allow provider to understand Computerized Provider Order Entry. CONTEXT Use computerized provider order entry (CPOE) for medication, laboratory, and radiology orders directly entered by any licensed healthcare professional who can enter orders into the medical record per state, local and professional guidelines. Stage 1: Providers use CPOE to document orders. Measure 1: More than 30 percent of all unique patients with at least one medication in their medication list seen by the EP during the EHR reporting period have at least one medication order entered using CPOE; or more than 30 percent of medication orders created by the EP during the reporting period during the EHR reporting period, are recorded using computerized provider order entry. Stage 2: Providers use CPOE to document orders. Measure 1: More than 60 percent of medication orders created by the EP during the EHR reporting period are recorded using computerized provider order entry. Measure 2: More than 30 percent of laboratory orders created by the EP during the EHR reporting period are recorded using computerized provider order entry. Measure 3: More than 30 percent of radiology orders created by the EP during the EHR reporting period are recorded using computerized provider order entry. 28

29 EXCLUSIONS Providers scheduled to be Stage 1 in 2016 may claim an exclusion for measure two (laboratory orders) and for measure three (radiology orders) of Stage 2 CPOE objective for an EHR reporting period in There are no exclusions for Stage 2 providers. Providers who write fewer than 100 medications, laboratory or radiology orders during the reporting period may exclude from this measure. STEP BY STEP INSTRUCTIONS For medication ordering create a Full Note Composer, navigate to RX Tab and enter desired medication. This medication can be printed or e-prescribed to calculate. 29


30 For laboratory ordering create a Full Note Composer, navigate to either the SO or SP Tab and enter desired laboratory order using a CPT code in the range of For radiology ordering- create a Full Note Composer, navigate to either the SO or SP Tab and enter desired radiology order using a CPT code in the code range of


31 If someone other than the provider is entering prescriptions, laboratory orders, or radiology orders they must be a Licensed Healthcare Professional. It is recommended to have a copy of their license on file in case of an audit. To mark a user as a Licensed Healthcare Professional, access the User option from the System menu of List Editor, search for the user and select Modify. From the Modify User window, select the Settings tab. Here you will check the box for Licensed Healthcare Professional and then click the OK button. 31
32 OBJECTIVE #4: ELECTRONIC PRESCRIBING OBJECTIVE Allow provider an understanding of how to generate and transmit permissible prescriptions electronically (erx). CONTEXT Stage 1: Providers in 2016 only, more than 40 percent of all permissible prescriptions written by the EP are transmitted electronically using CEHRT. Stage 2: Generate and transmit permissible prescriptions electronically (erx). More than 50 percent of all permissible prescriptions written by the EP are queried for a drug formulary and transmitted electronically using CEHRT. Please Note: This measure only applies to permissible medications; it does not apply to controlled substances. Prescriptions which are faxed to a pharmacy using a fax service do not meet requirements for this measure. EXCLUSION Any provider who: (1) Writes fewer than 100 prescriptions during the EHR reporting period or (2) does not have a pharmacy within their organization and there are no pharmacies that accept electronic prescriptions within 10 miles of the practice location at the start of the reporting period. 32


33 STEP BY STEP INSTRUCTIONS Initiate the download of drug formulary through the patient s demographics window. 33



34 View the patient formulary on the RX tab in the Full Note Composer From the RX tab search for and write a new RX or Refill an existing medication. 34
 are filled out or the prescription will not go successfully.")

35 In the SIG writer window make sure the Dosage, Form, Route, Frequency, Dose, Refills in needed, Quantity and Unit of Measure (UOM) are filled out or the prescription will not go successfully. Make sure that the patients pharmacy pulls into the pharmacy field. If it does not, then you need to select one before sending the prescription. It will then go electronically to the pharmacy. 35
36 OBJECTIVE #5: HEALTH INFORMATION EXCHANGE OBJECTIVE Allow provider to understand how to create a summary of care record for each referral order or transition of care. CONTEXT The EP who transitions their patient to another setting of care or provider of care or refers their patient to another provider of care (1) uses CEHRT to create a summary of care record; and (2) electronically transmits such summary to a receiving provider for more than 10 percent of transitions of care and referrals. EXCLUSION Any provider who transfers a patient to another setting or refers a patient to another provider less than 100 times during the EHR reporting period may exclude from this measure. STEP BY STEP INSTRUCTIONS First, the practice must add the providers Direct Mail address to the Referring Provider list in Aprima. To access this list, go to List Editor > System > Provider > then select the check box Include External Providers. *Please note- you must obtain the providers Direct Mail address by contacting the provider directly. 36


37 From the search window, find the provider whose Direct Mail address you would like to add and then select Modify. To add the address, find the tab called Direct Message and place the address in the To Address field and close the Provider window. The Direct Mail address has been added. GENERATING THE DIRECT SECURE MESSAGE Within the Full Note Composer, place a referral order by selecting the Referral Order from the SO Tab then click on the blue procedure note box to left of order and complete procedure note. Must enter Provider, Providers Role, Disclosure Reason, PPT Status, and CDA Section. If the provider is not sending the Direct Mail, please select Assign To and assign the referral order message to a staff member who will complete the order. 37

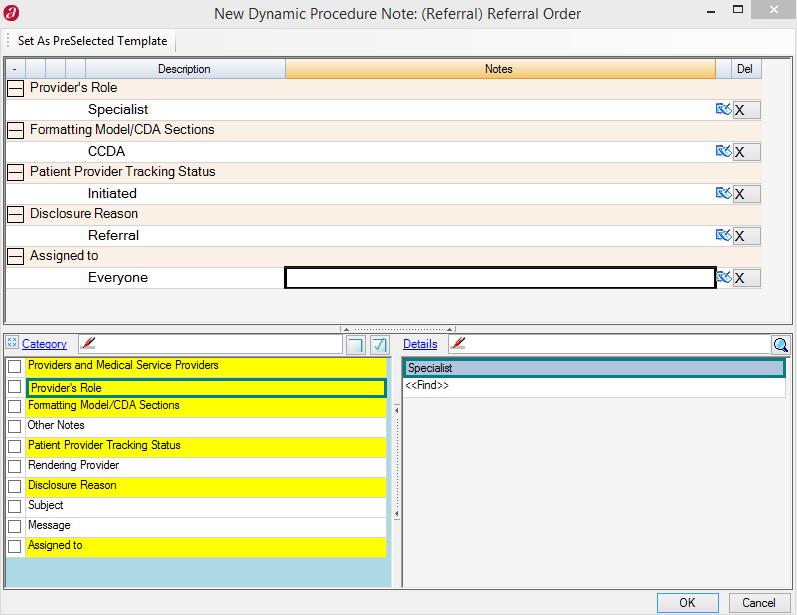
38 38

39 Once the provider completes their note, the Unified Summary window will appear. The provider must then select the Formatting Model C-CDA then click OK. 39
 and type a message in the Message field if desired.")
40 Next, the Send Documents window will appear. Pull in the sending providers Direct Mail Address (From) and type a message in the Message field if desired. Once all necessary fields are complete, select the Direct button at the bottom of the screen. The Direct Mail Message will then be sent. 40

41 If the provider will not be sending the Direct Mail but an office staff member will be, have the provider select the referral using the SO Referral Order in the Full Note Composer and complete the procedure box with the appropriate Assigned to. Once the note is closed, have the staff member open the Referral Order Message. The provider will not have the Unified Summary Window appear. *Please note- staff member must have security for Direct Mail access. This is located in List Editor under Provider > Clinical Delegate Security. Open the Referral Order Message in your message center by clicking on the date and time. Next, associate the necessary fields such as Provider s Role, Role Active, and Default Formatting Model. Once this is complete, click the Generate Document icon at the top of the message. 41

42 From the Document Generation Window, complete the necessary fields by first selecting Related Patient Referral then associate the Visit Date, and finally choose the appropriate formatting model by selecting Use Formatting Model and find CCDA. 42

43 The Send Document screen will appear. Pull in the sending providers Direct Mail Address and type a message in the Message filter if desired. Press Direct: mail will then be sent. 43

44 RECEIVING THE DIRECT MAIL MESSAGE When a practice sends you a Direct Mail Message, it will appear in your Attachment Approval message filter if the patient is already built in your database, or, it will appear in Document Linking under the Direct Mail folder if the patient is not built in your database. From the C-CDA, only the patient s medication list, allergies, and past medical history can be imported as discrete data. From the Attachment Approval message, click the date and time to open the message. You can then Approve Attachment or Reject Attachment. If you Reject Attachment, it will be sent to the Reject Folder in Document Linking for re-attachment. You can also import medication, allergies and problems from this message by clicking on the Import buttons at the top of the CCD document. Once you click an Import button, the Modify Import window appears. Here you can select the boxes to the left of the items you wish to import, then select Add to HX at the top. This will pull the selected items into the patient s chart. Once all desired items are reviewed and imported, complete the message to remove it from your inbox. 44


45 To import patient information from Document Linking, click the Document Linking icon from the Aprima desktop then select the Direct Mail folder. *Please note- no message is generated when a C-CDA is sent to Document Linking. Please have staff members check this folder regularly. 45

46 Drag the desired CCDA to the Document Linking window and attach to the desired patient. *Please note- this patient may need to be built, this can be completed from the Patient Name window in Document Linking. Select the document Type CCD for DataExchange Export. Name the document per practice desire. 46


47 Once all fields are complete, click Apply to link the document and OK to close the window. Proceed to Find Patient then click on Attachments to view linked C-CDA. Click the document name to open the C-CDA. From here, you can import medications, allergies and problems using the same method as above. Once all items have been imported, click close to exit the C-CDA. 47

48 VERIFYING DSM TRANSMISSION In order to track Direct Mail transmissions, please go to Interface Data Details from the Aprima desktop. Here, you will select the Logged From dates and select Search. A list of sent items will appear, you can then filter the Partner by Direct Message. A successful status indicates the Direct Mail was sent to Nitor. 48

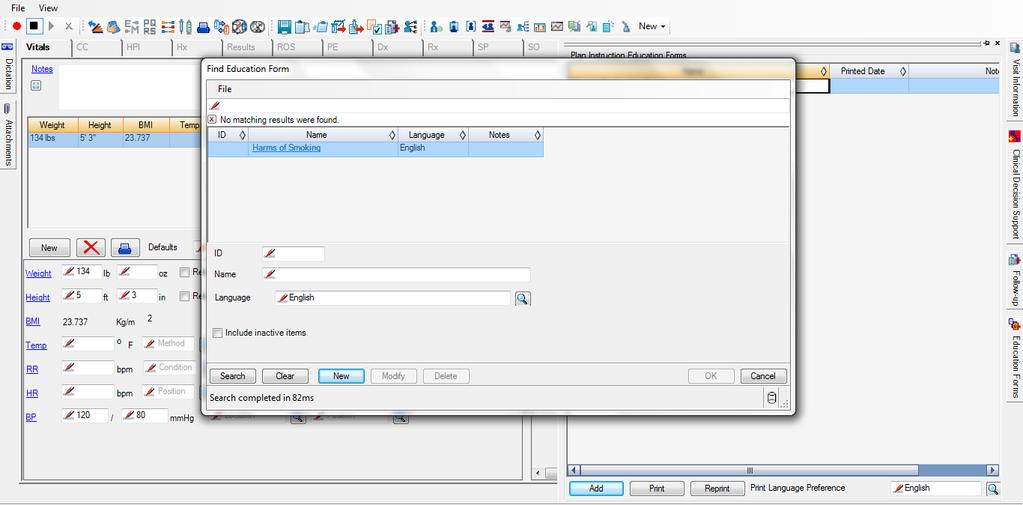
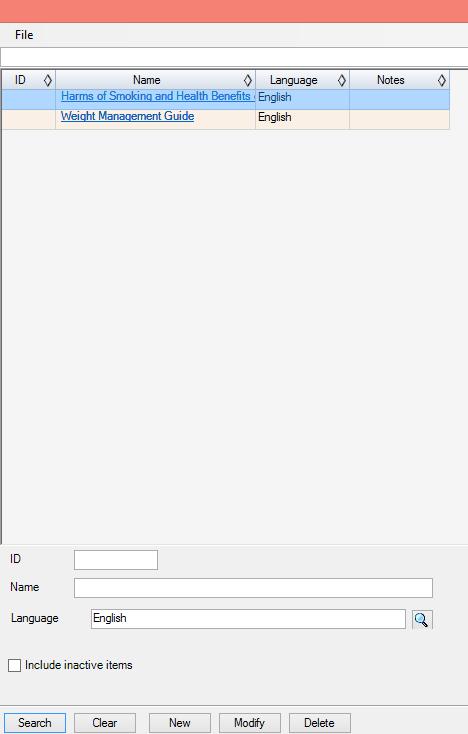
49 OBJECTIVE #6: PATIENT SPECIFIC EDUCATION OBJECTIVE Allow provider an understanding of how to attach appropriate education form to patient visit note. CONTEXT Use clinically relevant information from Certified EHR Technology to identify patient-specific education resources and provide those resources to the patient. Patient-specific education resources identified by Certified EHR Technology are provided to patients for more than 10 percent of all unique patients with office visits seen by the EP during the EHR reporting period. EXCLUSION None. STEP BY STEP INSTRUCTIONS Within the Full Note Composer, access the Education Slider. Click Add located at the bottom left corner > click Search to see available education forms > Select appropriate education form and click OK. The education form has now been attached to the patient s visit. 49
50 50
51 OBJECTIVE #7: MEDICATION RECONCILIATION OBJECTIVE Allow provider to understand how to reconcile medication history for patients. CONTEXT The EP who receives a patient from another setting of care or provider of care or believes an encounter is relevant should perform medication reconciliation. The EP who performs medication reconciliation for more than 50 percent of transitions of care in which the patient is transitioned into the care of the EP. EXCLUSION Any provider who was not the recipient of any transitions of care during the EHR reporting period. Stage 1 providers who did not intend to select Stage 1 Medication Reconciliation menu objective may exclude from this measure. STEP BY STEP INSTRUCTIONS To report on this measure, you must identify the patient as transitioning by selecting the Transition Of Care checkbox in Medication History category of the Hx tab of the Full Note Composer or other patient visit note window as well as check the box next to the Medication History category indicating that the Medication History was reviewed with the patient. 51


52 52
53 OBJECTIVE #8: PATIENT ELECTRONIC ACCESS OBJECTIVE Allow the provider to understand how to provide electronic health information to patients. CONTEXT Provide patients the ability to view online, download and transmit their health information within four business days of the information being available to the EP. Measure 1: More than 50 percent of all unique patients seen by the EP during the EHR reporting period are provided timely (available to the patient within four business days after the information is available to the EP) online access to their health information. Measure 2: For more than 5 percent of patient s seen by the EP during the EHR reporting period (or their authorized representatives) view, download, or transmit to a third party their health information. EXCLUSION Stage 1 providers can claim an exclusion to the second measure as Stage 1 does not have an equivalent measure. STEP BY STEP INSTRUCTIONS Measure 1: In the demographic window, enter patient s address. Then go to the Questionnaire tab and Create Web Account. 53


54 Measure 2: Provide patient user name and password for Patient Portal. Have patient log in and view, download, or transmit Clinical Summary. The patient may also transmit a CCDA to another provider. 54

55 Their Clinical Summary will the download. They can select the double arrow to choose an option of Printing their Summary or Downloading it. When they are done, they can select the Close button at the bottom. 55
56 OBJECTIVE #9: SECURE ELECTRONIC MESSAGING OBJECTIVE Allow provider to understand secure messaging between provider and patient via Aprima and the Patient Portal. CONTEXT Use secure electronic messaging to communicate with patients on relevant health information. For at least 5 percent of patient s seen by the EP during the reporting period, a secure message was sent using the electronic secure messaging function of CEHRT to the patient or in response to a message sent by the patient. The message must be sent by the provider for a patient seen during the reporting period for an E&M visit. EXCLUSION Any EP who has no office visits during the EHR reporting period, or any EP who conducts 50 percent or more of his or her patient encounters in a county that does not have 50 percent or more of its housing units with 4 Mbps broadband availability, according to the latest information available from the FCC on the first day of the EHR reporting period An EP may claim exclusion for the measure if for an EHR reporting period in 2015 they were scheduled to demonstrate Stage 1, which does not have an equivalent measure. STEP BY STEP INSTRUCTIONS Provide patient user name and password to Patient Portal. The patient must have an address entered to be able to send them a message. The clinician then needs to send the patient a message from their chart in Aprima. To send the patient a message from their chart select the New drop down menu and select New Patient Portal or . 56


57 The New Message window will open. Select a Sub-Type for the message. 57


58 The Reason for the message will automatically populate. Then type the message in the large box. Select the OK button when you are ready to send the message. The provider can also respond to a message sent from a patient s portal account for this measure. Type the reply in the white box and then select the reply button. Once you are finished with this select the complete button. 58
59 OBJECTIVE #10: PUBLIC HEALTH AND CLINICAL DATA REGISTRY REPORTING EXCLUSIONS If the EP qualifies for multiple exclusions and the remaining number of measures available to the EP is less than 2 (for Stage 2), the EP can meet the objective by meeting the one remaining measure available to them and claiming applicable exclusions. If no measures remain available, the EP can meet the objective by claiming applicable exclusions for all measures. MEASURE 1: IMMUNIZATION REGISTRY REPORTING OBJECTIVE Allow provider to understand how to send immunization information electronically to state immunization registry. CONTEXT The EP is in active engagement with a public health agency to submit immunization data. EXCLUSION An EP may exclude from this measure if they do not administer any immunizations to any of the populations for which data is collected by its jurisdiction's immunization registry or immunization information system during the EHR reporting period. An EP may exclude from this measure is they operate in a jurisdiction for which no immunization registry or immunization information system is capable or declared readiness to receive immunization data using the specific standards required to meet the CEHRT definition at the start of the reporting period. 59


60 STEP BY STEP INSTRUCTIONS Within the Full Note Composer or Order Note, select desired immunization to administer through the SP Tab > save the note using the floppy disk icon > access the Vaccine Administration Record icon and document administration accordingly. Upon completion of note, vaccine gets sent electronically to the interfaced state registry. 60


61 This measure requires screen shots for supporting documentation. The following is an example of the suggested screen shots to support the measures. From the Desktop menu select Integration Data Detail. Fill in the Partner field to say the name of your state immunization registry, Message Type to say the specific immunization registry message, and the Message Status of Successful and then select the search button. Click on the Partner link to open the New Interface Data Detail window to take your screenshot. MEASURE 1 SCREENSHOT: 61
62 MEASURE 2: SYNDROMIC SURVEILLANCE REPORTING OBJECTIVE Allow provider to understand submission of syndromic surveillance data to public health agency. CONTEXT The EP is in active engagement with a public health agency to submit syndromic surveillance data. EXCLUSION An EP meeting one or more of the following criteria may exclude from this measure: Is in a category of providers from which ambulatory syndromic surveillance data is collected by their jurisdiction's syndromic surveillance system; Operates in a jurisdiction for which no public health agency is capable of receiving electronic syndromic surveillance data from EPs in the specific standards required to meet the CEHRT definition at the start of the EHR reporting period; or Operates in a jurisdiction where no public health agency has declared readiness to receive syndromic surveillance data from EPs at the start of the EHR reporting period. STEP BY STEP INSTRUCTIONS *Check with your state health department to determine if your state is capable of reporting this measure. If they are capable please contact your Account Manager for further instructions. 62
63 MEASURE 3: SPECIALIZED REGISTRY REPORTING OBJECTIVE Allow provider to understand how to report to a specialized registry. CONTEXT The EP is in active engagement to submit data to a specialized registry. EXCLUSION Any EP meeting at least one of the following criteria may be excluded from the specialized registry reporting measure if the EP: Does not diagnose or directly treat any disease or condition associated with, or collect relevant data that is collected by, a specialized registry in their jurisdiction during the EHR reporting period; Operates in a jurisdiction for which no specialized registry is capable of accepting electronic registry transactions in the specific standards required to meet the CEHRT definition at the start of the EHR reporting period; or Operates in a jurisdiction where no specialized registry for which the EP is eligible has declared readiness to receive electronic registry transactions at the beginning of the EHR reporting period. STEP BY STEP INSTRUCTIONS *Check with your specialty societies and your state health department to determine their capability to meet this measure. 63
64 CLINICAL QUALITY MEASURES INTRODUCTION Each provider must perform nine of the available clinical quality measures (CQMs). The nine selected measures must cover three of the six domains. Aprima PRM 2015 is certified for 60 of the 64 CMS clinical quality measures. You must select measures for which the Aprima application is certified. The provider s performance on the CQMs are not evaluated for Meaningful Use, they simply need to report the percentage for each measure selected. All clinical quality measures have a denominator and numerator patient population. The denominator is the total qualifying patient population for the measure. The numerator is the patient populations for whom you have provided the service specified for the measure. Beginning in 2014, you must attest to nine CQM s that cover at least three of the six NQS areas/domains. DOMAINS: Patient and Family Engagement Efficient Use of Healthcare Resources Clinical Processes/Effectiveness Patient Safety Population and Health Care Coordination 64
65 CMS 2; NQF 0418; PQRS 134 PREVENTIVE CARE AND SCREENING: SCREENING FOR CLINICAL DEPRESSION AND FOLLOW-UP PLAN DOMAIN Population/Public Health MEASURE Percentage of patients aged 12 years and older screened for clinical depression on the date of the encounter using an age appropriate standardized depression screening tool AND if positive, a follow-up plan is documented on the date of the positive screen. EXCLUSIONS OR EXCEPTIONS Patient Reason(s): Patient refuses to participate. Medical Reason(s): Patient is in an urgent or emergent situation where time is of the essence and to delay treatment would jeopardize the patient s health status. Situations where the patient s functional capacity or motivation to improve may impact the accuracy of results of standardized depression assessment tools. For example: certain court appointed cases or cases of delirium. ENTERING DENOMINATOR DATA The patient must be 12 years and older at the beginning of the measurement period. The patient must have at least one eligible visit during the measurement period. ENTERING NUMERATOR DATA There are two numerators for this measure. The first numerator requires an appropriate depression screening. To chart the screening, you must enter a procedure code that is associated with a qualifying SNOMED code. You may enter the procedure code in either the SP or the SO tab of Full Note Composer or other clinical note type window. SNOMED CODES FOR THE SCREENING , , , , , , , , , , , , , , ,
66 The second numerator applies when the screening result is positive, and you diagnose the patient. Enter the diagnosis with a qualifying ICD-9 or ICD-10 code or a diagnosis code associated with a qualifying SNOMED code for depression in the Dx tab of Full Note Composer or other clinical note type window. ICD , , , 296.2, , , , , , , 296.3,296.31, , , , , , 298.0, 300.4, , 309.0, 309.1,309.28, 311 ICD-10 F31.1, F31.11, F31.12, F31.13, F31.2, F31.73, F31.74, F31.9, F01.51, F03, F32.0, F32.1, F32.2, F32.3, F32.4, F32.5, F32.8, F32.9, F33.0, F33.1, F33.2, F33.3, F33.42, F33.9, F34.1, F43.21, F43.23 SNOMED , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , 66
67 , , , , , , , , , , , , , , , , , , You must establish a follow up plan, which may include medication, an additional screening, or a referral to another qualifying medical services provider. To chart the screening, you must enter a procedure code that is associated with a qualifying SNOMED code. You may enter the in either the SP or the SO tab of Full Note Composer or other clinical note type window. SNOMED CODES FOR THE FOLLOW UP PLAN , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , To use a referral as the follow-up plan, you must order the referral by entering a procedure code that is associated with a qualifying SNOMED code. SNOMED CODES FOR DEPRESSION REFERRAL , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , ,
68 To use medication as the follow-up plan, you must prescribe a qualifying medication as the follow up plan. Write the prescription through the SIG Writer window, and then either print it or submit it electronically. 68
69 CMS 22 PREVENTIVE CARE AND SCREENING: SCREENING FOR HIGH BLOOD PRESSURE AND FOLLOW-UP DOCUMENTED DOMAIN Population/Public Health MEASURE Percentage of patients aged 18 years and older seen during the reporting period who were screened for high blood pressure AND a recommended follow-up plan is documented based on the current blood pressure (BP) reading as indicated. EXCLUSIONS OR EXCEPTIONS Patient Reason(s): Patient refuses to participate. OR Medical Reason(s): Patient is in an urgent or emergent medical situation where time is of the essence and to delay treatment would jeopardize the patient s health status. This may include but is not limited to severely elevated BP when immediate medical treatment is indicated. ENTERING DENOMINATOR DATA Patients must be 18 years old or older before the start of the measurement period. Patients do not already have an active diagnosis of hypertension. ENTERING NUMERATOR DATA Patients who were screened for high blood pressure AND a recommended follow-up plan is documented as indicated if the blood pressure is pre-hypertensive or hypertensive. To report on this measure, you must enter the patient s blood pressure (both systolic and diastolic values) in the Vitals tab of Full Note Composer or other clinical note type window. Use the system-defined blood pressure fields (Blood Pressure 1, 2, 3, or 4). These observation items for these blood pressure fields are associated with the appropriate LOIN codes. 69
70 The blood pressure measurement from the most recent visit is used to report on this measure. When that visit contains more than one blood pressure measurement, then the measurement with the lowest systolic and diastolic blood pressure is used. If the patient s blood pressure is between 120/80 and 140/90, then within one day of the visit, you must either: Order referral to another provider, or Document a plan to retest the blood pressure within a year and document lifestyle change recommendations that may include diet, exercise, weight loss, and alcohol consumption. If the patient s blood pressure is 140/90 or greater, but has not been high in the year prior to this visit, then within one day of the visit, you must either: Order referral to another provider, or Document a plan to retest the blood pressure within four weeks and document lifestyle change recommendations that may include diet, exercise, weight loss, and alcohol consumption. If the patient s blood pressure is 140/90 or greater, and has been high in the year prior to this visit, then within one day of the visit, you must either: Order referral to another provider, or Document a plan to retest the blood pressure within four weeks and document lifestyle change recommendations that may include diet, exercise, weight loss, and alcohol consumption, and either Write a prescription for medication, or Order a screening or test, such as a comprehensive metabolic panel or an electrocardiogram. To chart a referral to another provider, you must order the referral by entering a procedure code that is associated with a qualifying SNOMED code. The system-defined Referral Order procedure code is associated with SNOMED code You may associate other procedure codes with more specific qualifying SNOMED codes as needed. Enter the procedure code in 70
71 either the SP or the SO tab of Full Note Composer or other clinical note type window. SNOMED , , , , , , or You may also create the referral from Patient/Provider Tracking. When you create the referral in this way, you must create the referral within one day of the visit date and associate it with the visit. To chart that you plan to retest the blood pressure, you must one or more custom procedure codes and associate them with a qualifying SNOMED code that indicates the timeframe for the follow up test. Enter the procedure in the SP tab of Full Note Composer or other clinical note type window. Please note that simply entering the referral in Referral Tracking or Patient Provider Tracking will not count for this measure. SNOMED codes for retest within 4 weeks , , , , , , SNOMED codes for retest within 1 year , , , , , , , , , , , , , For diet, exercise, weight loss, or alcohol consumption recommendations, counseling, or education, you must chart an appropriate procedure. Select the desired procedure code in the SP or SO tab of Full Note Composer or other clinical note type window. If the procedure code is associated with an education form, such as for counseling, then selecting the education form from the Education Form slider will add the procedure code to the SP tab. 71
72 ALCOHOL SNOMED , , , , , , , DIET HCPCS G8417, S9452, S9470 DIET SNOMED , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , EXERCISE HCPCS GS9451 EXERCISE SNOMED , , , , , , , LIFESTYLE SNOMED , , , , , WEIGHT LOSS HCPCS S9449 WEIGHT LOSS SNOMED , , , , , , To use medication as part of the follow-up plan, you must prescribe a qualifying medication as the follow up plan. Write the prescription through the SIG Writer window, and then either print it or submit it electronically. 72
73 To chart a screening or test, you must enter a procedure code that is associated with a qualifying SNOMED code. You may enter the in either the SP or the SO tab of Full Note Composer or other clinical note type window. CPT 80047, 80048, 80050, 80053, or SNOMED , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , TROUBLESHOOTING This measure looks at both the systolic and diastolic measures. Both the patient s systolic measure and diastolic measure must be equal to or greater than the criteria to move to the next level. If either measure is less than the criteria, then the patient remains in the lower level group. 73
74 CMS 50; NQF NA; PQRS 374 CLOSING THE REFERRAL LOOP: RECEIPT OF SPECIALIST REPORT DOMAIN Care Coordination MEASURE Percentage of patients with referrals, regardless of age, for which the referring provider receives a report from the provider to whom the patient was referred. EXCLUSIONS OR EXCEPTIONS None ENTERING DENOMINATOR DATA The patient must have at least one visit during the measurement period. You must order the referral. This can be done in either of the following ways. In the visit note, enter a procedure code that is associated with a qualifying SNOMED code. Create the referral from Patient/Provider Tracking. When you create the referral in this way, you must associate the referral with the visit. The system-defined Referral Order procedure code is associated with SNOMED code You may associate other procedure codes with more specific qualifying SNOMED codes as needed. Enter the procedure code in either the SP or the SO tab of Full Note Composer or other clinical note type window. REFERRAL SNOMED , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , 74
75 , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , ENTERING NUMERATOR DATA When you receive the consultation report from the referred to physician or medical service provider, you must attach the consultation report to the referral record using Document Linking. You must use the attachment type Consultation Report when attaching the report to the referral. The Consultation Report attachment type has the SNOMED code in the ID field. Please note that referral entries with a status of Historical Reference or of Relationship are not included. 75
76 CMS 52; NQF 0405; PQRS 160 HIV/AIDS: PNEUMOCYSTIS JIROVECI PNEUMONIA (PCP) PROPHYLAXIS DOMAIN Clinical Process/Effectiveness MEASURE Percentage of patients aged 6 weeks and older with a diagnosis of HIV/AIDS who were prescribed Pneumocystis jiroveci pneumonia (PCP) prophylaxis EXCLUSIONS OR EXCEPTIONS Numerator 1: Patient did not receive PCP prophylaxis because there was a CD4 count above 200 cells/mm3 during the 3 months after a CD4 count below 200 cells/mm3 Numerator 2: Patient did not receive PCP prophylaxis because there was a CD4 count above 500 cells/mm3 or CD4 percentage above 15 percent during the three months after a CD4 count below 500 cells/mm3 or CD4 percentage below 15 percent. Numerator 3: None ENTERING DENOMINATOR DATA Denominator 1: All patients aged 6 years and older with a diagnosis of HIV/AIDS and a CD4 count below 200 cells/mm3 who had at least two visits during the measurement year, with at least 90 days in between each visit. The test must be performed less than 9 months after the start of the measurement period. Denominator 2: All patients aged 1-5 years of age with a diagnosis of HIV/AIDS and a CD4 count below 500 cells/mm3 or a CD4 percentage below 15 percent who had at least two visits during the measurement year, with at least 90 days in between each visit. The test must be performed less than 9 months after the start of the measurement period. Denominator 3: All patients aged 6 weeks to 12 months with a diagnosis of HIV who had at least two visits during the measurement year, with at least 90 days in between each visit. 76
77 To include a patient in the denominator, you must enter a qualifying diagnosis code or a diagnosis code associated with a qualifying SNOMED code in the Dx tab of Full Note Composer or other clinical note type window or enter a problem associated with a qualifying SNOMED code in the problem history category in either the Hx tab of Full Note Composer or the History window. ICD-9 042, V08 ICD-10 B20, Z21 SNOMED , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , To report on this measure, you must order or perform a CD4+Count or CD4+Percentage test, and then either enter the test results or receive them through an interface and give them a status of Resulted or Approved. Test results not received through an interface must be entered as discrete, quantifiable data. Enter the results in the Patients Results window using a lab template enabling you to enter the test result value. Results stored in the database as text notes or image file cannot be used for reporting. You must associate a LOINC code to the CD4+Count or CD4+Percentagetest item on each lab template for both manually entered and electronic results. CD4+Count LOINC: , , , , CD4+Percentage LOINC: , , , , , ,
78 ENTERING NUMERATOR DATA Numerator 1: Patients who were prescribed pneumocystis jiroveci pneumonia (PCP) prophylaxis within 3 months of CD4 count below 200 cells/mm3. Numerator 2: Patients who were prescribed pneumocystic jiroveci pneumonia (PCP) prophylaxis within 3 months of CD4 count below 500 cells/ mm3 or a CD4 percentage below 15%. Numerator 3: Patients who were prescribed Pneumocystic jiroveci pneumonia (PCP) prophylaxis at the time of diagnosis of HIV. To report on this measure, you must write a prescription for a Pneumocystic jiroveci pneumonia (PCP) prophylaxis medication through the SIG Writer window and either print it or submit it electronically through the Surescripts pharmacy clearinghouse. The prescription counts for the rendering provider on the visit note, even if another provider enters and submits the prescription. For numerators 1 and 2, you must write the prescription within 3 months of performing the CD4 test that had results qualifying for the numerator. For numerator 3, you must enter the diagnosis of HIV and the prescription in the same visit note. 78
79 CMS 56; NQF NA; PQRS 376 FUNCTIONAL STATUS ASSESSMENT FOR HIP REPLACEMENT DOMAIN Patient and Family Engagement MEASURE Percentage of patients aged 18 years and older with primary total hip arthroplasty (THA) who completed baseline and follow-up (patient-reported) functional status assessments. EXCLUSIONS OR EXCEPTIONS Patients with multiple trauma at the time of the total hip arthroplasty or patients with severe cognitive impairment. ENTERING DENOMINATOR DATA Adults aged 18 and older with a primary total hip arthroplasty (THA) and who had an outpatient encounter not more than 180 days prior to procedure, and at least 60 days and not more than 180 days after THA procedure. You must enter a qualifying procedure code or a procedure code associated with a qualifying SNOMED code for the hip replacement in the surgical history category in the Hx tab of Full Note Composer or the Patient History window. HCPCS S2118 CPT
80 SNOMED , , , , , , , , , , , , , , , , , , , , Please note that the system defined hip surgery question in the surgical history does not count for this measure. This is because that entry may be for any hip surgery; it is not specifically total hip arthroplasty. ENTERING NUMERATOR DATA Patients with patient reported functional status assessment results (e.g., VR- 12, VR-36, PROMIS-10- Global Health, PROMIS-29, HOOS) not more than 180 days prior to the primary THA procedure, and at least 60 days and not more than 180 days after the THA procedure. To report on this measure, you must have set up an observation item for the score of each assessment that you use, and put these observation items in an observation template. The observation item for each assessment s score must include the appropriate LOINC code for the functional status assessment. You must also have a clinical note type defined to include the Observation tab so that you can use the observation template to chart the assessment. None of the system-defined clinical note type windows (such as Full Note Composer) include the Observation tab. So, you must use a custom clinical note type window to chart patient visit notes that will include a functional status assessment. Enter the score of the functional status assessment in the observation template on the Observation tab. Please note that entries in the Cognitive and Functional Assessment history categories do not count for this measure. 80
81 ACTIVITIES OF DAILY LIVING LOINC CODE HOOS LOINC CODES , , PROMIS-10 LOINC CODES , , , PROMIS-29 LOINC CODES , , , , , , , , , , , , , , VR12 LOINC CODES , , , , , , , , , , , , , , , , , , , VR-36 LOINC CODES , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , ,
82 CMS 62; NQF 0403, PQRS 368 HIV/AIDS: MEDICAL VISIT DOMAIN Clinical Process/Effectiveness MEASURE Percentage of patients, regardless of age, with a diagnosis of HIV/AIDS with at least two medical visits during the measurement year with a minimum of 90 days between each visit. EXCLUSIONS OR EXCEPTIONS None ENTERING DENOMINATOR DATA All patients, regardless of age, with a diagnosis of HIV/AIDS seen within a 12-month period. To include a patient in the denominator, you must enter a qualifying diagnosis code or a diagnosis code associated with a qualifying SNOMED code in the Dx tab of Full Note Composer or other clinical note type window or enter a problem associated with a qualifying SNOMED code in the problem history category in either the Hx tab of Full Note Composer or the History window. ICD-9 042, V08 ICD-10 B20, Z21 SNOMED , , , , , , , , , , , , , , , , , , , ,
83 ENTERING NUMERATOR DATA Patients with at least two medical visits during the measurement year with a minimum of 90 days between visits. 83
84 CMS 65; NQF NA; PQRS 373 HYPERTENSION: IMPROVEMENT IN BLOOD MEASURE This measure requires a reporting period is greater than 6 months. You cannot use this measure if your reporting period is six months or less. Percentage of patients aged years of age with a diagnosis of hypertension whose blood pressure improved during the measurement period. DOMAIN Clinical Process/Effectiveness EXCLUSIONS OR EXCEPTIONS Exclude from the denominator all patients with evidence of end-stage renal disease (ESRD) on or prior to December 31 of the measurement year. Documentation of dialysis or renal transplant also meets the criteria for evidence of ESRD. Exclude from the denominator all patients with a diagnosis of pregnancy during the measurement year. ENTERING DENOMINATOR DATA All patients aged years of age, who had at least one outpatient visit in the first 6 months of the measurement year, who have a diagnosis of hypertension documented during that outpatient visit, and who have uncontrolled baseline blood pressure at the time of that visit. Enter the hypertension diagnosis with a qualifying diagnosis code or diagnosis code associated with a SNOMED code in the Dx tab of Full Note Composer or other clinical note type window or enter a problem associated with a qualifying SNOMED code in the problem history category in the Hx tab of Full Note Composer or the Patient History window. 84
85 ICD , 401.1, 401.9, , , , , , , , , , , , , , , , , , , , , , , , , , , , , , ICD-10 I10, I11.0, I11.9, I12.0, I12.9, I13.0, I13.10, I13.11, I13.2, I15.0, I15.1, I15.2, I15.8, I15.9 SNOMED , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , To report on this measure, you must enter the patient s blood pressure in the Vitals tab of Full Note Composer or other clinical note type window. You must enter both systolic and diastolic values, but this measure is only concerned with the systolic entry. The blood pressure measurement from the most recent visit is used to report on this measure. When that visit contains more than one blood pressure measurement, then the measurement with the lowest systolic and diastolic blood pressure is used. Please note that if the patient has a visit in the first six months of the reporting period and their blood pressure is not high at that time and they do not have a diagnosis or problem of hypertension, then the patient will not be counted for this measure even if the patient s blood press is high in a visit in during the last six months of the year. 85
86 ENTERING NUMERATOR DATA Patients whose follow-up systolic blood pressure is at least 10 mmhg less than their baseline blood pressure or is adequately controlled (systolic blood pressure is less than 140 mmhg). If a follow-up blood pressure reading is not recorded during the measurement year, the patient s blood pressure is assumed not improved. To report on this measure, the patient must have a second visit that is at least six months after the first visit and that is in the reporting period. The visit must include a blood pressure reading. Enter the patient s blood pressure in the Vitals tab of Full Note Composer or other clinical note type window. You must enter both systolic and diastolic values, but this measure is only concerned with the systolic entry. Use the system-defined blood pressure fields (Blood Pressure 1, 2, 3, or 4). These observation items for these blood pressure fields are associated with the appropriate LOINC codes. The blood pressure measurement from the most recent visit is used to report on this measure. When that visit contains more than one blood pressure measurement, then the measurement with the lowest systolic and diastolic blood pressure is use. 86
87 CMS 66; NQF NA; PQRS 375 FUNCTIONAL STATUS ASSESSMENT FOR KNEE REPLACEMENT DOMAIN Patient and Family Engagement MEASURE Percentage of patients aged 18 years and older with primary total knee arthroplasty (TKA) who completed baseline and follow-up (patient-reported) functional status assessments. EXCLUSIONS OR EXCEPTIONS Patients with multiple traumas at the time of the total knee arthroplasty or patients with severe cognitive impairment. ENTERING DENOMINATOR DATA Adults, aged 18 and older, with a primary total knee arthroplasty (TKA) and who had an outpatient encounter not more than 180 days prior to procedure, and at least 60 days and not more than 180 days after TKA procedure. You must enter a qualifying procedure code or a procedure code associated with a qualifying SNOMED code for the knee replacement in the surgical history category in the Hx tab of Full Note Composer or the Patient History window. CPT SNOMED , , , , , , , , ,
88 ENTERING NUMERATOR DATA Patients with patient reported functional status assessment results (e.g., VR- 12, VR-36, PROMIS-10 Global Health, PROMIS-29, KOOS) not more than 180 days prior to the primary TKA procedure, and at least 60 days and not more than 180 days after the TKA procedure. To report on this measure, you must have set up an observation item for the score of each assessment that you use, and put these observation items in an observation template. The observation item for each assessment s score must include the appropriate LOINC code for the functional status assessment. You must also have a clinical note type defined to include the Observation tab so that you can use the observation template to chart the assessment. None of the system-defined clinical note type windows (such as Full Note Composer) include the Observation tab. So, you must use a custom clinical note type window to chart patient visit notes that will include a functional status assessment. Enter the score of the functional status assessment in the observation template on the Observation tab. Please note that entries in the Cognitive and Functional Assessment history categories do not count for this measure. ACTIVITIES OF DAILY LIVING LOINC CODE KOOS LOINC CODES , , PROMIS-10 LOINC CODES , , ,
89 PROMIS-29 LOINC CODES , , , , , , , , , , , , , , VR12 LOINC CODES , , , , , , , , , , , , , , , , , , , VR-36 LOINC CODES , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , ,
90 CMS 68; NQF 0419; PQRS 130 DOCUMENTATION OF CURRENT MEDICATION IN THE MEDICAL RECORD DOMAIN Patient Safety MEASURE Percentage of specified visits for patients aged 18 years and older for which the eligible professional attests to documenting a list of current medications to the best of his/her knowledge and ability. This list must include ALL prescriptions, over-the-counters, herbals, and vitamin/mineral/dietary (nutritional) supplements AND must contain the medications' name, dosage, frequency, and route of administration. EXCLUSIONS OR EXCEPTIONS None ENTERING DENOMINATOR DATA The patient must be 18 years old or older at the beginning before the start of the measurement period. ENTERING NUMERATOR DATA To report on this measure, you must either: Select the checkbox for the Medication History category in the Hx tab of Full Note Composer or other clinical note type to indicate that you have reviewed the medication list, or Create a custom defined procedure code for documenting a list of the patient s current medications. This procedure code must be associated to SNOMED code You must then include this custom procedure code in visit notes for all patient visits during which you document a list of current medications. You may want to include your custom-defined procedure code in your SP charge ticket so that it is easy to select when charting visit notes. 90
91 CMS 69; NQF 0421; PQRS 128 PREVENTIVE CARE AND SCREENING: BODY MASS INDEX (BMI) SCREENING AND FOLLOW-UP DOMAIN Population/Public Health MEASURE Percentage of patients aged 18 years and older with an encounter during the reporting period with a documented calculated BMI during the encounter or during the previous six months, AND when the BMI is outside of normal parameters, follow-up is documented during the encounter or during the previous six months of the encounter with the BMI outside of normal parameters. Normal parameters for patients age 65 years and older is a BMI between 23 and <30. Normal parameters for patients age 18 years to 64 years is a BMI between 18.5 and <25. Denominator 1: All patients aged 65 years and older Numerator 1: Patients with BMI calculated within the past six months or during the current visit and a follow-up plan documented if the BMI is outside of parameters. Numerator Inclusions: Population Stratification 1: (BMI < 30 kg/m2 and 23 kg/m2) Denominator 2: All patients aged 18 through 64 years. Denominator Inclusions: Population Stratification 2: (Patients aged 18-64) Numerator 2: Patients with BMI calculated within the past six months or during the current visit and a follow-up plan documented if the BMI is outside of parameters. Numerator Inclusions: Population Stratification 2: (BMI < 25 kg/m2 and 18.5 kg/m2) EXCLUSIONS OR EXCEPTIONS Patients who are pregnant. ENTERING DENOMINATOR DATA For denominator 1, the patient must be 65 years of age or older before the beginning of the measurement period. The patient must have at least one eligible encounter during the measurement period. 91
92 For denominator 2, the patient must be between 18 and 64 years old before the beginning of the measurement period. For both denominators, the patient must have at least one eligible encounter during the measurement period. Eligible encounters do not include encounters where the patient is receiving palliative care, refuses BMI measurement, the patient is in an urgent or emergent medical situation where time is of the essence and to delay treatment would jeopardize the patient s health status, or there is any other reason documented in the medical record by the provider explaining why BMI measurement was not appropriate. ENTERING NUMERATOR DATA To report on this measure, you must enter the patient s height and weight in the Vitals tab of the patient visit note window. The BMI is calculated automatically from the height and weight entries, and then displayed on the Vitals tab and charted in the visit note. The application determines the appropriate LOINC code to associate with the BMI based on the patient s age. If there is a medical reason for not calculating the BMI, then you must enter one of the following HCPCS procedure codes and enter an appropriate negation reason on that procedure. HCPCS FOR BMI G8938, G8421, G8417, G8418, G8419, G8420, G8422, G8938 If the BMI is out of the established normal range, then you must establish a follow up plan, which may include medication, procedures, counseling, or a referral to another qualifying medical services provider. To document the follow-up plan using a procedure, counseling, or referral, use a procedure code that is associated with a qualifying SNOMED code. You may enter the procedure code in either the SP or the SO tab of Full Note Composer or other clinical note type window. If you are using an ICD-9 procedure code, enter it on the Dx tab of Full Note Composer or other clinical note type window. 92
93 If the procedure code you want has been associated with an education form, such as for counseling, then selecting the education form from the Education Form slider will add the procedure code to the SP tab. The education form assigned to the patient must be associated with a patient communication type of Overweight or Underweight. Please note that since only one patient communication type can be associated with an education form, you must have separate forms for these conditions. If you use an education form on a general topic, such as nutrition, for both underweight and overweight, then you must have two copies of education form in your database. Above Normal Follow Up CPT 43644, 43645, 43770, 43771, 43772, 43773, 43774, 43842, 43843, 43845, 43846, 43847, 43848, 97804, 98960, HCPCS G8417, S9449, S9451, S9452, S9470 ICD-9 V65.3, V65.41 SNOMED , , , , , , , , , , , , , , Above Normal Referral SNOMED , , , , , , , , , , , , , , 93
94 , , , , , , , , , , , , , , , , Below Normal Follow Up HCPCS G8418, S9449, S9452, S9470 ICD-9 V65.3 SNOMED , , , , , , , Below Normal Referral SNOMED , , , , , , , , , , , , , , , , , , , , , , , , , , , , , To document the follow-up plan using a medication, write a prescription for an appropriate medication using the SIG Writer window. Then print or electronically submit the prescription. 94
95 CMS 74; NQF NA; PQRS 379 PRIMARY CARIES PREVENTION INTERVENTION AS OFFERED BY PRIMARY CARE PROVIDERS, INCLUDING DENTISTS DOMAIN Clinical Process/Effectiveness MEASURE Percentage of children, age 0-20 years, who received a fluoride varnish application during the measurement period. EXCLUSIONS OR EXCEPTIONS None ENTERING DENOMINATOR DATA Children, age 0-20 years, with a visit during the measurement period. ENTERING NUMERATOR DATA Children who receive a fluoride varnish application. To report on this measure, you must enter a qualifying procedure code or a procedure code associated with a qualifying SNOMED code for a fluoride varnish application. HCPCS D1203, D1206 SNOMED , , ,
96 CMS 75; NQF NA; PQRS 378 CHILDREN WHO HAVE DENTAL DECAY OR CAVITIES DOMAIN Clinical Process/Effectiveness MEASURE Percentage of children, age 0 through 20 years, who have had tooth decay or cavities during the measurement period. EXCLUSIONS OR EXCEPTIONS None ENTERING DENOMINATOR DATA The patient must be 0 through 20 years old, and must have at least one visit during the measurement period. ENTERING NUMERATOR DATA To report on this measure, you must enter the diagnosis code in the Dx tab of Full Note Composer or other clinical note type window. ICD-9 CODES , , , , , , , , , ICD-10 K02.3, K02.51, K02.52, K02.53, K02.61, K02.62, K02.63, K02.7, K
97 CMS 77; NQF NA; PQRS 381 HIV/AIDS: RNA CONTROL OF PATIENTS WITH HIV DOMAIN Clinical Process/Effectiveness MEASURE Percentage of patients aged 13 years and older with a diagnosis of HIV/AIDS, with at least two visits during the measurement year, with at least 90 days between each visit, whose most recent HIV RNA level is <200 copies/ml. EXCLUSIONS OR EXCEPTIONS None ENTERING DENOMINATOR DATA All patients aged 13 years and older with a diagnosis of HIV/AIDS with at least two visits during the measurement year. To include a patient in the denominator, you must enter a qualifying diagnosis code or a diagnosis code associated with a qualifying SNOMED code in the Dx tab of Full Note Composer or other clinical note type window or enter a problem associated with a qualifying SNOMED code in the problem history category in either the Hx tab of Full Note Composer or the History window. ICD-9 042, V08 ICD-10 B20, Z21 SNOMED , , , , , , , , , , , , , , , , 97
98 , , , , , , , , , , , , , , , , , , , ENTERING NUMERATOR DATA Patients whose most recent HIV RNA level is <200 copies/ml. To report on this measure, you must order or perform an HIV RNA test, and then either enter the test results or receive them through an interface and give them a status of Resulted or Approved. Test results not received through an interface must be entered as discrete, quantifiable data. Enter the results in the Patients Results window using a lab template enabling you to enter the test result value. Results stored in the database as text notes or image file cannot be used for reporting. You must associate a LOINC code to the HIV RNA test item on each lab template for both manually entered and electronic results. LOINC CODES , , , , , ,
99 CMS 82; NQF 1401; PQRS 372 MATERNAL DEPRESSION SCREENING DOMAIN Population/Public Health MEASURE The percentage of children who turned 6 months of age during the measurement year, who had a face-to-face visit between the clinician and the child during child s first 6 months, and who had a maternal depression screening for the mother at least once between 0 and 6 months of life. EXCLUSIONS OR EXCEPTIONS None ENTERING DENOMINATOR DATA Children with a visit who turned 6 months of age in the measurement period. ENTERING NUMERATOR DATA Children with documentation of maternal screening or treatment for postpartum depression for the mother. Enter the mother s screening using a procedure code associated with the SNOMED code in the SP tab of Full Note Composer or other clinical note type. Enter the mother s treatment using a procedure code associated with the SNOMED code in the SP tab of Full Note Composer or other clinical note type. If you use the same procedure when screening or treating patients, then you may need to associate the procedure with two different SNOMED codes, one that indicates patient screening or treatment and one that indicates maternal screening or treatment. Or you can create custom procedure codes for the maternal screening and treatment, and associate those custom procedure codes with the appropriate SNOMED codes. 99
100 CMS 90; NQF NA; PQRS 377 FUNCTIONAL STATUS ASSESSMENT FOR COMPLEX CHRONIC CONDITIONS DOMAIN Patient and Family Engagement MEASURE Percentage of patients aged 65 years and older with heart failure who completed initial and follow-up patient-reported functional status assessments. EXCLUSIONS OR EXCEPTIONS Patients with severe cognitive impairment or patients with an active diagnosis of cancer. ENTERING DENOMINATOR DATA The patient must be 65 years old or older. The patient must have an active diagnosis of heart failure. ICD , , , , , , , , , 428.0, 428.1, , , , , , , , , , , , , ICD-10 I11.0, I13.0, I13.2, I50.1, I50.20, I50.21, I50.22, I50.23, I50.30, I50.31, I50.32, I50.33, I50.40, I50.41, I50.42, I50.43, I50.9 SNOMED , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , 100
101 , , , , , , , , , , This measure requires at least two patient visits. The first visit must be within the first 185 days of the measurement period (January 1 through July 4). The second visit must be within the assessment period, and must be at least 30 days after and not more than 180 days after the first visit. The assessment must be done during or within two weeks prior to each of these two visits. Because of the timing constraints on the first and second visit, this measure is not optimal if your reporting period is 90 days. ENTERING NUMERATOR DATA To report on this measure, you must have set up an observation item for the score of each assessment that you use, and put these observation items in an observation template. The observation item for each assessment s score must include the appropriate LOINC code for the functional status assessment. LOINC CODES , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , You must also have a clinical note type defined to include the Observation tab so that you can use the observation template to chart the assessment. None of the system-defined clinical note type windows (such as Full Note Composer) include the Observation tab. So, you must use a custom clinical note type window to chart patient visit notes that will include a functional status assessment for a complex chronic condition. 101
102 Enter the score of the functional status assessment in the observation template on the Observation tab. Please note that entries in the Cognitive and Functional Assessment history categories do not count for this measure. 102
103 CMS 117; NQF 0038; PQRS 240 CHILDHOOD IMMUNIZATION STATUS DOMAIN Population/Public Health MEASURE Percentage of children two years of age who had four diphtheria, tetanus and acellular pertussis (DTaP); three polio (IPV), one measles, mumps and rubella (MMR); three H influenza type B (HiB); three hepatitis B (Hep B); one chicken pox (VZV); four pneumococcal conjugate (PCV); one hepatitis A (Hep A); two or three rotavirus (RV); and two influenza (flu) vaccines by their second birthday. Denominator: All patients who turn two years of age during the measurement period. Numerator: Patients who received four diphtheria, tetanus and acellular pertussis (DTaP); three polio (IPV); one measles, mumps, rubella (MMR); three H influenza type B (HIB); three hepatitis B (Hep B); one chicken pox (VZV); four pneumococcal conjugate (PCV); two hepatitis A (Hep A); two or three rotavirus (RV); and two influenza (flu) vaccines by their second birthday. EXCLUSIONS OR EXCEPTIONS None ENTERING DENOMINATOR DATA The patient must turn two years old during the measurement period. The patient must have at least one visit during the measurement period. ENTERING NUMERATOR DATA To report on this measure, document the administration of the each of the required vaccines. To document an immunization, enter the appropriate CPT code for that immunization and enter the vaccination details in the Vaccine Administration Record. This can be done in the patient visit note or in the Patient History, Immunization History category. The vaccine type for the vaccination must be associated with the appropriate CVX code. 103
104 All vaccinations must be given according to the recommended schedule for the vaccine. The first DTaP, HIB, IPV, PCV vaccinations must be given when the patient is 42 days old or older. Vaccinations administered prior to 42 days are not counted. Patient refusal is not considered valid reporting for this measure and will be in denominator. 104
105 CMS 122; NQF 0059; PQRS 1 DIABETES: HEMOGLOBIN A1C POOR CONTROL DOMAIN Clinical Processes and Effectiveness MEASURE Percentage of patients years of age with diabetes who had hemoglobin A1c > 9.0% during the measurement period. EXCLUSIONS OR EXCEPTIONS Patients with a diagnosis of gestational diabetes during the measurement period. ENTERING DENOMINATOR DATA Patients years of age with diabetes with a visit during the measurement period. Enter the diabetes diagnosis with a qualifying diagnosis code or diagnosis code associated with a SNOMED code in the Dx tab of Full Note Composer or other clinical note type window or enter a problem associated with a qualifying SNOMED code in the problem history category in the Hx tab of Full Note Composer or the Patient History window. ICD , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , ICD-10 E10.10, E10.11, E10.21, E10.22, E10.29, E10.311, E10.319, E10.321, E10.329, E10.331, E10.339, E10.341, E10.349, E10.351, E10.359, E10.36, E10.39, E10.40, E10.41, E10.42, E10.43, E10.44, E10.49, E10.51, E10.52, E10.59, E10.610, E10.618, E10.620, E10.621, E10.622, E10.628, E10.630, E10.638, E10.641, E10.649, E10.65, E10.69, E10.8, E10.9, E11.00, E11.01, E11.21, E11.22, E11.29, E11.311, E11.319, E11.321, E11.329, E11.331, E11.339, E11.341, E11.349, E11.351, E11.359, E11.36, E11.39, E11.40, E11.41, E11.42, E11.43, E11.44, E11.49, E11.51, E11.52, E11.59, E11.610, 105
106 E11.618, E11.620, E11.621, E11.622, E11.628, E11.630, E11.638, E11.641, E11.649, E11.65, E11.69, E11.8, E11.9, O24.011, O24.012, O24.013, O24.019, O24.02, O24.03, O24.111, O24.112, O24.113, O24.119, O24.12, O24.13 SNOMED , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , ENTERING NUMERATOR DATA Patients whose most recent HbA1c level (performed during the measurement period) is >9.0%. Patients who do not have an HbA1c level entered during the measurement period are also included in the numerator. Please note that for this measure, a low numerator is the desired outcome. To report on this measure, you must order or perform an A1c test and then either enter the test results or receive them through an interface. You must associate the results with the order, and give them a status of Resulted or Approved. The A1c test results must be entered as discrete, quantifiable data. Enter the results in the Patients Results window using a lab template enabling you to enter the HGB A1c value. Results stored in the database as text notes or an image file cannot be used for reporting. You must associate a LOINC code to the A1C test item on each lab template for both manually entered and electronic results. LOINC codes for this result are , ,
107 CMS 123; NQF 0056; PQRS 163 DIABETES FOOT EXAM DOMAIN Clinical Processes and Effectiveness MEASURE Percentage of patients aged years of age with diabetes who had a foot exam during the measurement period. EXCLUSIONS OR EXCEPTIONS Patients with a diagnosis of gestational diabetes during the measurement period. Patients who have had both feet amputated. ENTERING DENOMINATOR DATA Patients years of age with diabetes with a visit during the measurement period. Enter the diabetes diagnosis with a qualifying diagnosis code or diagnosis code associated with a SNOMED code in the Dx tab of Full Note Composer or other clinical note type window or enter a problem associated with a qualifying SNOMED code in the problem history category in the Hx tab of Full Note Composer or the Patient History window. This diagnosis or problem must be active. ICD , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , ICD-10 E10.10, E10.11, E10.21, E10.22, E10.29, E10.311, E10.319, E10.321, E10.329, E10.331, E10.339, E10.341, E10.349, E10.351, E10.359, E10.36, E10.39, E10.40, E10.41, E10.42, E10.43, E10.44, E10.49, E10.51, E10.52, E10.59, E10.610, E10.618, E10.620, E10.621, E10.622, E10.628, E10.630, E10.638, E10.641, E10.649, E10.65, E10.69, E10.8, E10.9, E11.00, E11.01, E11.21, E11.22, E11.29, 107
108 E11.311, E11.319, E11.321, E11.329, E11.331, E11.339, E11.341, E11.349, E11.351, E11.359, E11.36, E11.39, E11.40, E11.41, E11.42, E11.43, E11.44, E11.49, E11.51, E11.52, E11.59, E11.610, E11.618, E11.620, E11.621, E11.622, E11.628, E11.630, E11.638, E11.641, E11.649, E11.65, E11.69, E11.8, E11.9, O24.011, O24.012, O24.013, O24.019, O24.02, O24.03, O24.111, O24.112, O24.113, O24.119, O24.12, O24.13 SNOMED , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , ENTERING NUMERATOR DATA Patients who received a foot exam during the measurement period. The foot exam must include a visual inspection and either a sensory exam or a pulse exam. To report on this measure, you must order or perform a visual foot exam, a sensory exam, and a pulse exam. You may chart the exams using procedure codes that are associated with the SNOMED codes for the exams. PULSE EXAM SENSORY EXAM VISUAL EXAM
109 The procedure codes 2028-F and G9226 are associated with the proper SNOMED codes, and configured to report as a complete foot exam (visual, sensory, and pulse). 109
110 CMS 124; NQF 0032; PQRS 309 CERVICAL CANCER SCREENING DOMAIN Clinical Processes and Effectiveness MEASURE Percentage of women years of age, who received one or more Pap tests to screen for cervical cancer. EXCLUSIONS OR EXCEPTIONS Women who had a hysterectomy with no residual cervix. ENTERING DENOMINATOR DATA Women years of age with a visit during the measurement period. ENTERING NUMERATOR DATA Women with one or more Pap tests during the measurement period or the two years prior to the measurement period. To report on this measure, you must order or perform a Pap test, and then either enter the test results or receive them through an interface and give them a status of Resulted or Approved. To chart the Pap test, to chart the screening, you must enter a procedure code that is associated with a qualifying LOINC code. You may enter the procedure in either the SP or the SO tab of Full Note Composer or other clinical note type window. Pap test results not received through an interface must be entered as discrete, quantifiable data. Enter the results in the Patients Results window using a lab template enabling you to enter the test result value. Results stored in the database as text notes or image file cannot be used for reporting. You must associate a LOINC code to the Chlamydia test item on each lab template for both manually entered and electronic results. LOINC CODES , , , , , , , , ,
111 CMS 125; NQF NA; PQRS 112 BREAST CANCER SCREENING DOMAIN Clinical Processes and Effectiveness MEASURE Percentage of women years of age who had a mammogram to screen for breast cancer. EXCLUSIONS OR EXCEPTIONS Women who had a bilateral mastectomy or for whom there is evidence of two unilateral mastectomies. ENTERING DENOMINATOR DATA Women years of age with a visit during the measurement period. ENTERING NUMERATOR DATA Women with one or more mammograms during the measurement period or the year prior to the measurement period. To report on this measure, you must order or perform the mammography and enter the result. The mammography may be ordered or performed within 12 months prior to the start of the measurement period or during the measurement period. To document the test and its results, order the mammography test using one of the HCPCS codes below. Then enter and approve the mammography results in the Patient Results window, and give them a status of Resulted or Approved. HCPCS CODES G0202, G0204, G
112 LOINC CODES , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , ,
113 CMS 126; NQF 0036; PQRS 311 USE OF APPROPRIATE MEDICATION FOR ASTHMA DOMAIN Clinical Processes and Effectiveness MEASURE Percentage of patients five through 64 years of age who were identified as having persistent asthma and were appropriately prescribed medication during the measurement period. EXCLUSIONS OR EXCEPTIONS Patients with emphysema, COPD, cystic fibrosis or acute respiratory failure during or prior to the measurement period. ENTERING DENOMINATOR DATA The patient must be between 5 and 64 years old. The patient must have at least one visit during the measurement period. You must identify patients with asthma with an appropriate ICD-10 code or with a SNOMED code associated with an ICD-9 code. The active diagnosis may be entered in the Problem/Diagnosis category in the Patient History window or in Dx tab of Full Note Composer. ICD-10 CODES J45.30, J45.31, J45.32, J45.40, J45.41, J45.42, J45.50, J45.51, J45.52 SNOMED CODES , , ENTERING NUMERATOR DATA To report on this measure, you must prescribe an asthma medication. To report the asthma medication, write the prescription through the SIG Writer window or prescription refill message and print the prescription or send it electronically. 113
114 TROUBLESHOOTING The diagnosis for persistent asthma cannot be made inactive or resolved prior to the start of the measurement period 114
115 CMS 127; NQF 0043; PQRS 111 PNEUMONIA VACCINATION STATUS FOR OLDER ADULTS DOMAIN Clinical Processes and Effectiveness MEASURE Percentage of patients 65 years of age and older who have ever received a pneumococcal vaccine. EXCLUSIONS OR EXCEPTIONS None ENTERING DENOMINATOR DATA Patients 65 years of age and older with a visit during the measurement period. Please note that the E&M codes and do not count for this measure. ENTERING NUMERATOR DATA Patients who have ever received a pneumococcal vaccination. To report on this measure, you must document the administration of the pneumonia vaccine or document it in the patient s history. The vaccination may have been given at any time prior to or during the measurement period. To document the pneumonia immunization, enter the administration using a procedure code associated to an appropriate SNOMED code. Enter the procedure in the SP tab of Full Note Composer or other clinical note type window. Then document the vaccination details in the vaccine administration record. Enter the vaccination in the vaccination history category in the Hx tab of Full Note Composer or in the Patient History window. Then, identify the type of vaccine when documenting the vaccine details in the vaccine administration record. CVX:
116 SNOMED FOR ADMINISTERING THE VACCINATION ,
117 CMS 128; PQRS 0105; PQRS 9 ANTI-DEPRESSANT MEDICATION MANAGEMENT *This measure requires a reporting period that is greater than six months. You cannot use this measure if your reporting period is six months or less. DOMAIN Clinical Processes and Effectiveness MEASURE Percentage of patients 18 years of age and older who were diagnosed with major depression and treated with antidepressant medication, and who remained on antidepressant medication treatment. Percentage of patients who remained on an antidepressant medication for at least 84 days (12 weeks). Percentage of patients who remained on an antidepressant medication for at least 180 days (6 months). EXCLUSIONS OR EXCEPTIONS Patients who were actively on an antidepressant medication in the 90 days prior to the Index Prescription Start Date. ENTERING DENOMINATOR DATA Patients 18 years of age and older with a diagnosis of major depression in the 180 days (6 months) prior to the measurement period or the first 180 days (6 months) of the measurement period, who were treated with antidepressant medication, and with a visit during the measurement period. Enter the diagnosis with a qualifying diagnosis code or diagnosis code associated with a SNOMED code in the Dx tab of Full Note Composer or other clinical note type window or with a 117
118 problem associated with a qualifying SNOMED code in the problem history category in the Hx tab of Full Note Composer or the Patient History window. ICD , , , , , , , , , , , , 298.0, 300.4, 309.1, 311 ICD-10 F32.0, F32.1, F32.2, F32.3, F32.4, F32.9, F33.0, F33.1, F33.2, F33.3, F33.40, F33.41, F33.8, F33.9, F34.1 SNOMED , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , A prescription for a qualifying antidepressant medication must have been written within 30 days prior to and 14 days after the visit in which depression was diagnosed. Write the prescription through the SIG Writer window or prescription refill message and print the prescription or send it electronically. ENTERING NUMERATOR DATA Numerator 1: Patients who have received antidepressant medication for at least 84 days (12 weeks) of continuous treatment during the 114-day period following the Index Prescription Start Date. 118
119 Numerator 2: Patients who have received antidepressant medications for at least 180 days (6 months) of continuous treatment during the 231-day period following the Index Prescription Start Date. To report on this measure for acute phase treatment, you must prescribe antidepressant medication for 84 days (12 weeks) within the 4 months following the new episode of major depression. To report on this measure for continuation phase treatment, you must prescribe antidepressant medication for 180 days (6 months) within 8 months following the new episode of major depression. To report the antidepressant therapy, write the prescription through the SIG Writer window or prescription refill message and print the prescription or send it electronically. 119
120 CMS 129; NQF 0389; PQRS 102 PROSTATE CANCER: AVOIDANCE OF OVERUSE OF BONE SCAN FOR STAGING LOW RISK PROSTATE CANCER PATIENTS DOMAIN Efficient Use of Healthcare Resources MEASURE Percentage of patients, regardless of age, with a diagnosis of prostate cancer at low risk of recurrence receiving interstitial prostate brachytherapy, OR external beam radiotherapy to the prostate, OR radical prostatectomy, OR cryotherapy who did not have a bone scan performed at any time since diagnosis of prostate cancer. EXCLUSIONS OR EXCEPTIONS Documentation of reason(s) for performing a bone scan (including documented pain, salvage therapy, other medical reasons, bone scan ordered by someone other than reporting physician). ENTERING DENOMINATOR DATA All patients, regardless of age, with a diagnosis of prostate cancer. The patient must be male, and must have an active diagnosis of prostate cancer before or during the measurement period with a low risk for prostate cancer recurrence and a PSA test of less than or equal to 10 ng/ml and a Gleason Score of less than or equal to 6 before or during the prostate cancer treatment. Enter the diagnosis with a qualifying diagnosis code or diagnosis code associated with a SNOMED code in the Dx tab of Full Note Composer or other clinical note type window or enter a problem associated with a qualifying SNOMED code in the problem history category in the Hx tab of Full Note Composer or the Patient History window. ICD
121 ICD-10 C61 SNOMED , , , , , , , , , , , You must order the desired lab test using the appropriate procedure code with the procedure code type Lab. Then either enters the test results or receives them through an interface and gives them a status of Resulted or Approved. The test results not received through an interface must be entered as discrete, quantifiable data. Enter the results in the Patients Results window using a lab template enabling you to enter the result values in a positive/negative or numerical format. The lab test in the template must be associated with an appropriate LOINC code. LOINC FOR GLEASON RESULTS LOINC FOR PSA RESULTS , , , , , , , , , , , You must perform at least one prostate cancer treatment during the measurement period. Enter an appropriate CPT code or a procedure coded associated with an appropriate SNOMED code on the SP or SO tab of the patient visit note window. CPT CODES FOR TREATMENT 55810, 55812, 55815, 55840, 55842, 55845, 55866, 55873, 55875, 55876, 77427, 77776, 77777, 77778, and
122 SNOMED FOR THERAPY , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , ENTERING NUMERATOR DATA Patients who did not have a bone scan performed at any time since diagnosis of prostate cancer. To report on this measure, you would not have ordered a bone scan for the patient at any time since diagnosis of prostate cancer. Therefore, you will not have received results for the bone scan, and none of the following LOINC codes would be in the patient s chart. To ensure accurate reporting, one of the following LOINC codes should be associated to all bone scan procedures performed or ordered by the practice. LOINC , , , , , , , , , , , , , , , , , , , , , , , , , , ,
123 CMS 130; NQF 0034; PQRS 113 COLORECTAL CANCER SCREENING DOMAIN Clinical Processes and Effectiveness MEASURE Percentage of adults years of age who had appropriate screening for colorectal cancer. EXCLUSIONS OR EXCEPTIONS Patients with a diagnosis or past history of total colectomy or colorectal cancer. ENTERING DENOMINATOR DATA Patients years of age with a visit during the measurement period ENTERING NUMERATOR DATA Patients with one or more screenings for colorectal cancer. Appropriate screenings are defined by any one of the following criteria below: Fecal occult blood test (FOBT) during the measurement period. Flexible sigmoidoscopy during the measurement period or the four years prior to the measurement period. Colonoscopy during the measurement period or the nine years prior to the measurement period. To report on this measure, you must perform the screening test and enter the results during or prior to measurement period. To document the test and its results, chart the performance of the screening test using one of the procedure codes listed below. Then enter and approve the screening results in the Patient Results window, and give them a status of Resulted or Approved. Test results not received through an interface must be entered as discrete, quantifiable data. Enter the results in the Patients Results window using a lab template enabling you to enter the 123
124 test result value. Results stored in the database as text notes or image file cannot be used for reporting. You must associate a LOINC code to the FOBT test item on each lab template for both manually entered and electronic results. FOBT LOINC CODES , , , , , , , , , , , , , , Flexible Sigmoidoscopy CPT CODES 45330, 45331, 45332, 45333, 45334, 45335, 45337, 45338, 45339, 45340, 45341, 45342, HCPCS CODES G0104 SNOMED CODES , , , Colonoscopy CPT CODES 44388, 44389, 44390, 44391, 44392, 44393, 44394, 44397, 45355, 45378, 45379, 45380, 45381, 45382, 45383, 45384, 45385, 45386, 45387, 45391, HCPCS CODES G0105, G0121 SNOMED CODES , , , , , , , , 124
125 , , , , , , , , , ,
126 CMS 131; NQF 0055; PQRS 117 DIABETIC: EYE EXAM DOMAIN Clinical Process/Effectiveness MEASURE Percentage of patients years of age with diabetes who had a retinal or dilated eye exam by an eye care professional during the measurement period or a negative retinal exam (no evidence of retinopathy) in the 12 months prior to the measurement period. EXCLUSIONS OR EXCEPTIONS Patients with a diagnosis of gestational diabetes during the measurement period. ENTERING DENOMINATOR DATA Patients years of age with diabetes with a visit during the measurement period. Enter the diagnosis with a qualifying diagnosis code or diagnosis code associated with a SNOMED code in the Dx tab of Full Note Composer or other clinical note type window or enter a problem associated with a qualifying SNOMED code in the problem history category in the Hx tab of Full Note Composer or the Patient History window. ICD , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , ICD-10 E10.10, E10.11, E10.21, E10.22, E10.29, E10.311, E10.319, E10.321, E10.329, E10.331, E10.339, E10.341, E10.349, E10.351, E10.359, E10.36, E10.39, E10.40, E10.41, E10.42, E10.43, E10.44, E10.49, E10.51, E10.52, E10.59, E10.610, E10.618, E10.620, E10.621, E10.622, E10.628, E10.630, E10.638, E10.641, E10.649, E10.65, E10.69, E10.8, E10.9, E11.00, E11.01, E11.21, E11.22, E11.29, 126
127 E11.311, E11.319, E11.321, E11.329, E11.331, E11.339, E11.341, E11.349, E11.351, E11.359, E11.36, E11.39, E11.40, E11.41, E11.42, E11.43, E11.44, E11.49, E11.51, E11.52, E11.59, E11.610, E11.618, E11.620, E11.621, E11.622, E11.628, E11.630, E11.638, E11.641, E11.649, E11.65, E11.69, E11.8, E11.9, O24.011, O24.012, O24.013, O24.019, O24.02, O24.03, O24.111, O24.112, O24.113, O24.119, O24.12, O24.13 SNOMED , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , ENTERING NUMERATOR DATA Patients with an eye screening for diabetic retinal disease. This includes diabetics who had one of the following: A retinal or dilated eye exam by an eye care professional in the measurement period or A negative retinal exam (no evidence of retinopathy) by an eye care professional in the year prior to the measurement period. Please note that the application can only be used to report on the first option for this measure. The exam must be performed, and documented in the visit note. Please also note that the procedure must be performed by an ophthalmologist or optometrist. Other providers cannot use this measure. To report on this measure, you must perform the eye exam and enter it on the SP tab using a procedure code associated with one of the following SNOMED codes. SNOMED CODES , , , , , , , , 127
128 , , , , , , , , , , , , ,
129 CMS 132; NQF 0564; PQRS 192 CATARACTS: COMPLICATIONS WITHIN 30 DAYS FOLLOWING CATARACT SURGERY REQUIRING ADDITIONAL SURGICAL PROCEDURES DOMAIN Patient Safety MEASURE Percentage of patients aged 18 years and older with a diagnosis of uncomplicated cataract who had cataract surgery and had any of a specified list of surgical procedures in the 30 days following cataract surgery which would indicate the occurrence of any of the following major complications: retained nuclear fragments, endophthalmitis, dislocated or wrong power IOL, retinal detachment, or wound dehiscence. EXCLUSIONS OR EXCEPTIONS Patients with any one of a specified list of comorbid conditions that impact the surgical complication rate. ENTERING DENOMINATOR DATA All patients aged 18 years and older who had cataract surgery and no significant pre-operative ocular conditions impacting the surgical complication rate. Enter the procedure code or a procedure code associated with a SNOMED code for the cataract surgery in the SP or SO tab of Full Note Composer or other clinical note type or in the surgical history category of the Hx tab of Full Note Composer or the Patient History window. CPT 66840, 66850, 66852, 66920, 66930, 66940, 66982, 66983, SNOMED , , , , , , , , , , , , , , , , , , , , , , , , 129
130 , , , , , , , , , , , , , , , , , , , , ENTERING NUMERATOR DATA Patients who had one or more specified operative procedures for any of the following major complications within 30 days following cataract surgery: retained nuclear fragments, endophthalmitis, dislocated or wrong power IOL, retinal detachment, or wound dehiscence. Enter the procedure code or a procedure code associated with a SNOMED code in the SP or SO tab of Full Note Composer or other clinical note type or in the surgical history category of the Hx tab of Full Note Composer or the Patient History window. CPT 65235, 65900, 65920, 65930, 66030, 66250, 66820, 66825, 66830, 66852, 66986, 67005, 67010, 67015, 67025, 67028, 67030, 67031, 67036, 67039, 67041, 67042, 67043, 67101, 67105, 67107, 67108, 67110, 67112, 67141, 67145, 67250, SNOMED , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , ,
131 CMS 133; NQF 0565; PQRS 191 CATARACTS: 20/40 OR BETTER VISUAL ACUITY WITHIN 90 DAYS FOLLOWING CATARACT SURGERY DOMAIN Clinical Process/Effectiveness MEASURE Percentage of patients aged 18 years and older with a diagnosis of uncomplicated cataract who had cataract surgery and no significant ocular conditions impacting the visual outcome of surgery and had best-corrected visual acuity of 20/40 or better (distance or near) achieved within 90 days following the cataract surgery. EXCLUSIONS OR EXCEPTIONS Patients with specified comorbid conditions that impact the visual outcome of surgery. ENTERING DENOMINATOR DATA All patients aged 18 years and older who had cataract surgery. Enter the procedure code or a procedure code associated with a SNOMED code for the cataract surgery in the SP or SO tab of Full Note Composer or other clinical note type or in the surgical history category of the Hx tab of Full Note Composer or the Patient History window. CPT 66840, 66850, 66852, 66920, 66930, 66940, 66982, 66983, SNOMED , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , ,
132 ENTERING NUMERATOR DATA Patients who had best-corrected visual acuity of 20/40 or better (distance or near) achieved within 90 days following cataract surgery. There are two ways you can report on this measure. You can use observation items or you can use a physical exam item. To use observations, you must have set up an observation item or items for the visual acuity test, and put these observation items in an observation template. The observation item for must be associated with a qualifying SNOMED code for the test. SNOMED , , , You must also have a clinical note type defined to include the Observation tab so that you can use the observation template to chart the test. None of the system- defined clinical note type windows (such as Full Note Composer) include the Observation tab. So, you must use a custom clinical note type window to chart patient visit notes that will include a functional status assessment. Perform the visual acuity test, and enter the results in the observation template on the Observation tab. To use a physical exam, you must have set up a visual acuity finding in a physical exam. The finding must have SNOMED code in the ID field of the PE Finding window. Perform the visual acuity test, and select the finding in the physical exam. 132
133 CMS 134; NQF 0062; PQRS 119 DIABETES: URINE PROTEIN SCREENING DOMAIN Clinical Process/Effectiveness MEASURE The percentage of patients years of age with diabetes who had a nephropathy screening test or evidence of nephropathy during the measurement period. EXCLUSIONS OR EXCEPTIONS Patients with a diagnosis of gestational diabetes during the measurement period. ENTERING DENOMINATOR DATA Patients years of age with diabetes with a visit during the measurement period. Enter the diagnosis with a qualifying diagnosis code or diagnosis code associated with a SNOMED code in the Dx tab of Full Note Composer or other clinical note type window or enter a problem associated with a qualifying SNOMED code in the problem history category in the Hx tab of Full Note Composer or the Patient History window. ICD , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , ICD-10 E10.10, E10.11, E10.21, E10.22, E10.29, E10.311, E10.319, E10.321, E10.329, E10.331, E10.339, E10.341, E10.349, E10.351, E10.359, E10.36, E10.39, E10.40, E10.41, E10.42, E10.43, E10.44, E10.49, E10.51, E10.52, E10.59, E10.610, E10.618, E10.620, E10.621, E10.622, E10.628, E10.630, E10.638, E10.641, E10.649, E10.65, E10.69, E10.8, E10.9, E11.00, E11.01, E11.21, E11.22, E11.29, E11.311, E11.319, E11.321, E11.329, E11.331, E11.339, E11.341, E11.349, E11.351, E11.359, E11.36, E11.39, E11.40, E11.41, E11.42, E11.43, E11.44, E11.49, E11.51, E11.52, E11.59, E11.610, 133
134 E11.618, E11.620, E11.621, E11.622, E11.628, E11.630, E11.638, E11.641, E11.649, E11.65, E11.69, E11.8, E11.9, O24.011, O24.012, O24.013, O24.019, O24.02, O24.03, O24.111, O24.112, O24.113, O24.119, O24.12, O24.13 SNOMED , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , ENTERING NUMERATOR DATA Patients with a screening for nephropathy or evidence of nephropathy during the measurement period. To report on this measure, you must either diagnose the patient with nephropathy, or order or perform urine screening and then enter the results, or order or perform a procedure that indicates nephropathy. For this measure, a prescription for an ACE inhibitor or ARB medication is also an indication of nephropathy. To use the diagnosis, enter the diagnosis code in the Dx tab of Full Note Composer or other clinical note type window or enter a problem associated with a qualifying SNOMED code in the problem history category in the Hx tab of Full Note Composer or the Patient History window. ICD , , , ICD-10 E08.21, E08.22, E08.29, E09.21, E09.22, E09.29, E10.21, E10.22, E10.29, E11.21, E11.22, E11.29, E13.21, E13.22, E
135 SNOMED , , , , , , , , , To use the urine screening, perform the urine screening, and then either enter the test results or receive them through an interface and give them a status of Resulted or Approved. Test results not received through an interface must be entered as discrete, quantifiable data. Enter the results in the Patients Results window using a lab template enabling you to enter the urine microalbumin value. Results stored in the database as text notes or image file cannot be used for reporting. You must associate a LOINC code to the test item on each lab template for both manually entered and electronic results. MICROALBUMIN LOINC , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , MACROALBUMIN LOINC , , , , , , , , , To use a procedure that indicates nephropathy, you must enter a qualifying procedure code or a procedure code that is associated with a qualifying SNOMED code. You may enter the procedure in either the SP or the SO tab of Full Note Composer or other clinical note type window. 135
136 DIALYSIS EDUCATION SNOMED , , DIALYSIS SERVICES CPT 90920, 90921, 90924, 90925, 90935, 90937, 90940, 90945, DIALYSIS SERVICES HCPCS DIALYSIS SERVICES SNOMED , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , ESRD MONTHLY OUTPATIENT SERVICES CPT 90957, 90958, 90959, 90960, 90961, 90962, 90965, 90966, 90969, 90970, 90989, 90993, 90997, 90999, KIDNEY TRANSPLANT CPT 50300, 50320, 50340, 50360, 50365, 50370, KIDNEY TRANSPLANT SNOMED , , , , , , , , , , , OTHER SERVICES RELATED TO DIALYSIS SNOMED , , , , , ,
137 VASCULAR ACCESS FOR DIALYSIS CPT 36145, 36147, 36148, 36800, 36810, 36815, 36818, 36819, 36820, 36821, 36831, 36832, VASCULAR ACCESS FOR DIALYSIS SNOMED , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , To use medication as an indicator of nephropathy, enter the prescription for an ACE inhibitor or ARB medication in the SIG Writer window, and print or electronically submit the prescription. 137
138 CMS 135; NQF 0081; PQRS 5 HEART FAILURE (HF): ANGIOTENSIN-CONVERTING ENZYME (ACE) INHIBITOR OR ANGIOTENSIN RECEPTOR BLOCKER (ARB) THERAPY FOR LEFT VENTRICULAR SYSTOLIC DYSFUNCTION (LVSD) DOMAIN Clinical Process/Effectiveness MEASURE Percentage of patients aged 18 years and older with a diagnosis of heart failure (HF) with a current or prior left ventricular ejection fraction (LVEF) < 40% who were prescribed ACE inhibitor or ARB therapy either within a 12-month period when seen in the outpatient setting OR at each hospital discharge. EXCLUSIONS OR EXCEPTIONS Documentation of medical reason(s) for not prescribing ACE inhibitor or ARB therapy (e.g., hypotensive patients who are at immediate risk of cardiogenic shock, hospitalized patients who have experienced marked azotemia, allergy, intolerance, other medical reasons) Documentation of patient reason(s) for not prescribing ACE inhibitor or ARB therapy (e.g., patient declined, other patient reasons) Documentation of system reason(s) for not prescribing ACE inhibitor or ARB therapy (e.g., other system reasons) ENTERING DENOMINATOR DATA All patients aged 18 years and older with a diagnosis of heart failure. Enter the diagnosis with a qualifying diagnosis code or diagnosis code associated with a SNOMED code in the Dx tab of Full Note Composer or other clinical note type window or enter a problem associated with a qualifying SNOMED code in the problem history category in the Hx tab of Full Note Composer or the Patient History window. 138
139 ICD , , , , , , , , , 428.0, 428.1, , , , , , , , , , , , , ICD-10 I11.0, I13.0, I13.2, I50.1, I50.20, I50.21, I50.22, I50.23, I50.30, I50.31, I50.32, I50.33, I50.40, I50.41, I50.42, I50.43, I50.9 SNOMED , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , To report on this measure, you must order or perform an LVEF test and enter the result data. When the LVEF result is equal to or less than 40 percent, then you must prescribe either an ACE inhibitor or ARB therapy. LVEF test results may be entered as results in a lab template using LOINC codes, or as observation items in an observation template using SNOMED codes. To report the LVEF test using a lab template, the results must either be received through an interface or entered as discrete, quantifiable data in the Patient Results window using a lab template enabling you to enter the LVEF percentage. The results must be given a status of Resulted or Approved. Test results not received through an interface must be entered as discrete, quantifiable data. Enter the results in the Patients Results window using a lab template enabling you to enter the test result value. Results stored in the database as text notes or image file cannot be used for reporting. 139
140 You must associate a LOINC code to the LVEF test item on each lab template for both manually entered and electronic results. LOINC , , , , , , , , , , , , , , To report the LVEF test using an observation template, you must have set up an observation item for the LVEF test, and put the observation item in an observation template. The observation item must include the appropriate SNOMED code. SNOMED , , You must also have a clinical note type defined to include the Observation tab so that you can use the observation template to chart the LVEF test. None of the system -defined clinical note type windows (such as Full Note Composer) include the Observation tab. You must use a custom clinical note type window to chart patient visit notes that will include the test. ENTERING NUMERATOR DATA Patients who were prescribed ACE inhibitor or ARB therapy either within a 12-month period when seen in the outpatient setting or at hospital discharge. To report the ACE inhibitor or ARB therapy, write the prescription through the SIG Writer window or prescription refill message and print the prescription or send it electronically. 140
141 CMS 136; NQF 0108; PQRS 366 FOLLOW-UP CARE FOR CHILDREN PRESCRIBED ATTENTION DEFICIT/ HYPERACTIVITY DISORDER (ADHD) MEDICATION DOMAIN Clinical Processes and Effectiveness MEASURE Percentage of children 6 through 12 years of age and newly dispensed a medication for attention-deficit/hyperactivity disorder (ADHD) who had appropriate follow-up care. Two rates are reported. Percentage of children who had one follow-up visit with a practitioner with prescribing authority during the 30-Day Initiation Phase. Percentage of children who remained on ADHD medication for at least 210 days and who, in addition to the visit in the Initiation Phase, had at least two additional follow-up visits with a practitioner within 270 days (nine months) after the Initiation Phase ended. EXCLUSIONS OR EXCEPTIONS Denominator Exclusion 1: Exclude patients diagnosed with narcolepsy at any point in their history or during the measurement period. Exclude patients who had an acute inpatient stay with a principal diagnosis of mental health or substance abuse during the 30 days after the IPSD. Exclude patients who were actively on an ADHD medication in the 120 days prior to the Index Prescription Start Date. Denominator Exclusion 2: Exclude patients diagnosed with narcolepsy at any point in their history or during the measurement period. 141
142 Exclude patients who had an acute inpatient stay with a principal diagnosis of mental health or substance abuse during the 300 days after the IPSD. Exclude patients who were actively on an ADHD medication in the 120 days prior to the Index Prescription Start Date. ENTERING DENOMINATOR DATA The patient must be between 6 and 12 years of age, and must have at least one visit during the measurement period. For the first denominator, you must prescribe an ADHD medication for the patient for the first time will be included in the denominator. (The patient is excluded if already taking an ADHD medication.) The first prescription must be written between 90 days prior to start of the measurement period and no later than 60 days from the start of the measurement period. For the second denominator, the patient must meet the requirements for the first denominator and must remain on medication for at least 210 of the 300 days following the IPSD. Write the prescription through the SIG Writer window and print the prescription or send it electronically. ENTERING NUMERATOR DATA To include the patient in the numerator for the first part of this measure, you must conduct a follow-up visit with the patient within 30 of the initial ADHD prescription and within the measurement period. A patient must be in the numerator for the first part of this measure in order to be included in the numerator for the second part. To be included in the second numerator, you must conduct a second follow-up visit at least 31 days after and no more than 300 days after the initial ADHD prescription. The patient must also have been on the ADHD medication for at least 210 days. To report the medication, write the 142
143 prescriptions and/or refills through the SIG Writer window or prescription refill message and print the prescription or send it electronically. 143
144 CMS 137; NQF 0004; PQRS 305 INITIATIONS AND ENGAGEMENT OF ALCOHOL AND OTHER DRUG DEPENDENCE TREATMENT DOMAIN Clinical Process/Effectiveness MEASURE Percentage of patients 13 years of age and older with a new episode of alcohol and other drug (AOD) dependence who received the following. Two rates are reported. Percentage of patients who initiated treatment within 14 days of the diagnosis. Percentage of patients who initiated treatment and who had two or more additional services with an AOD diagnosis within 30 days of the initiation visit. EXCLUSIONS OR EXCEPTIONS Patients with a previous active diagnosis of alcohol or drug dependence in the 60 days prior to the first episode of alcohol or drug dependence. ENTERING DENOMINATOR DATA Patients age 13 years of age and older who were diagnosed with a new episode of alcohol or drug dependency during a visit in the first 11 months of the measurement period. Patients presenting with a subsequent episode of alcohol and other drug (AOD) dependence are not eligible for this measure. ICD , 291.1, 291.2, 291.3, 291.4, 291.5, , , , 291.9, 292.0, , , 292.2, , , , , , , 292.9, , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , 144
145 305.21, , , , , , , , , , , , , , , , , , , , , , , , , ICD-10 F10, F10.10, F10.120, F10.121, F10.129, F10.14, F10.150, F10.151, F10.159, F10.180, F10.181, F10.182, F10.188, F10.19, F10.20, F10.220, F10.221, F10.229, F10.230, F10.231, F10.232, F10.239, F10.24, F10.250, F10.251, F10.259, F10.26, F10.27, F10.280, F10.281, F10.282, F10.288, F10.29 F10.920, F10.921, F10.929, F10.94, F10.950, F10.951, F10.959, F10.96, F10.97, F10.980, F10.981, F10.982, F10.988, F10.99, F11.10, F11.120, F11.121, F11.122, F11.129, F11.14, F11.150, F11.151, F11.159, F11.181, F11.182, F11.188, F11.19, F11.20, F11.220, F11.221, F11.222, F11.229, F11.23, F11.24, F11.250, F11.251, F11.259, F11.281, F11.282, F11.288, F11.29, F11.90, F11.920, F11.921, F11.922, F11.929, F11.93, F11.94, F11.950, F11.951, F11.959, F11.981, F11.982, F11.988, F11.99, F12.10, F12.120, F12.121, F12.122, F12.129, F12.150, F12.151, F12.159, F12.180, F12.188, F12.19, F12.20, F12.220, F12.221, F12.222, F12.229, F12.250, F12.251, F12.259, F12.280, F12.288, F12.29, F12.90, F12.920, F12.921, F12.922, F12.929, F12.950, F12.951, F12.959, F12.980, F12.988, F12.99, F13.10, F13.120, F13.121, F13.129, F13.14, F13.150, F13.151, F13.159, F13.180, F13.181, F13.182, F13.188, F13.19, F13.20, F13.220, F13.221, F13.229, F13.230, F13.231, F13.232, F13.239, F13.24, F13.250, F13.251, F13.259, F13.26, F13.27, F13.280, F13.281, F13.282, F13.288, F13.29, F13.90, F13.920, F13.921, F13.929, F13.930, F13.931, F13.932, F13.939, F13.94, F13.950, F13.951, F13.959, F13.96, F13.97, F13.980, F13.981, F13.982, F13.988, F13.99, F14.10, F14.120, F14.121, F14.122, F14.129, F14.14, F14.150, F14.151, F14.159, F14.180, F14.181, F14.182, F14.188, F14.19, F14.20, F14.220, F14.221, F14.222, F14.229, F14.23, F14.24, F14.250, F14.251, F14.259, F14.280, F14.281, F14.282, F14.288, F14.29, F14.90, F14.920, F14.921, F14.922, F14.929, F14.94, F14.950, F14.951, F14.959, F14.980, F14.981, F14.982, F14.988, F14.99, F15.10, F15.120, F15.121, F15.122, F15.129, F15.14, F15.150, F15.151, F15.159, F15.180, F15.181, F15.182, F15.188, F15.19, F15.20, F15.220, F15.221, F15.222, F15.229, F15.23, F15.24, F15.250, F15.251, F15.259, F15.280, F15.281, F15.282, F15.288, F15.29, F15.90, F15.920, F15.921, F15.922, F15.929, F15.93, F15.94, F15.950, F15.951, F15.959, F15.980, F15.981, F15.982, F15.988, F15.99, F16.10, F16.120, F16.121, F16.122, F16.129, F16.14, F16.150, F16.151, F16.159, F16.180, F16.183, F16.188, F16.19, F16.20, F16.220, F16.221, F16.229, F16.24, F16.250, F16.251, F16.259, F16.280, F16.283, F16.288, 145
146 F16.29, F16.90, F16.920, F16.921, F16.929, F16.94, F16.950, F16.951, F16.959, F16.980, F16.983, F16.988, F16.99, F18.10, F18.120, F18.121, F18.129, F18.14, F18.150, F18.151, F18.159, F18.17, F18.180, F18.188, F18.19, F18.20, F18.220, F18.221, F18.229, F18.24, F18.250, F18.251, F18.259, F18.27, F18.280, F18.288, F18.29, F18.90, F18.920, F18.921, F18.929, F18.94, F18.950, F18.951, F18.959, F18.97, F18.980, F18.988, F18.99, F19.10, F19.120, F19.121, F19.122, F19.129, F19.14, F19.150, F19.151, F19.159, F19.16, F19.17, F19.180, F19.181, F19.182, F19.188, F19.19, F19.20, F19.220, F19.221, F19.222, F19.229, F19.230, F19.231, F19.232, F19.239, F19.24, F19.250, F19.251, F19.259, F19.26, F19.27, F19.280, F19.281, F19.282, F19.288, F19.29, F19.90, F19.920, F19.921, F19.922, F19.929, F19.930, F19.931, F19.932, F19.939, F19.94, F19.950, F19.951, F19.959, F19.96, F19.97, F19.980, F19.981, F19.982, F19.988, F19.99, F55.2, K29.20, K29.21, K70.10, K70.11 SNOMED , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , 146
147 , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , ENTERING NUMERATOR DATA Numerator 1: Patients who initiated treatment within 14 days of the diagnosis. Numerator 2: Patients who initiated treatment and who had two or more additional services with an AOD diagnosis within 30 days of the initiation visit. To report on this measure, you must document treatment using either a treatment procedure code associated with a SNOMED code or a psychotherapy visit procedure code. 147
148 You must enter the procedure code in the SP Tab of Full Note Composer or other clinical note type window. SNOMED FOR TREATMENT , , , , , , , , , , , , , , , , , , , , , , , , , , , CPT for psychotherapy 90832, 90834, For numerator 2, the patient must have initiated treatment within 14 days of the diagnosis, and then had two or more additional visits with treatment or psychotherapy visits within 30 days the initial encounter. 148
149 CMS 138; NQF 0028; PQRS 226 PREVENTIVE CARE AND SCREENING: TOBACCO USE - SCREENING AND CESSATION INTERVENTION DOMAIN Public Health MEASURE Percentage of patients aged 18 years and older who were screened for tobacco use one or more times within 24 months AND who received cessation counseling intervention if identified as a tobacco user. ENTERING DENOMINATOR DATA The patient must be 18 years old or older. This measure generally requires two office visits during the measurement period. Some types of office visits require only one during the measurement period. EXCLUSIONS OR EXCEPTIONS Documentation of medical reason(s) for not screening for tobacco use (eg, limited life expectancy, other medical reason). ENTERING NUMERATOR DATA To report on this measure, you must enter the patient s use or non-use of tobacco in the Hx tab, Social History category, in the patient visit note. When the patient is a tobacco user, then you must either: Enter CPT code or or HCPCS code G0436 to document the cessation counseling, OR Prescribe an approved cessation medication. If you have entered the patient s tobacco use in a prior measurement period and that use has not changed, then you must select the checkbox for the Social History category indicating that you have reviewed the patient s history, including tobacco use. 149
150 If you typically use an education form with or for cessation counseling, then you can associate the appropriate procedure code with the education form so that selecting the education form from the Education Form slider in Full Note Composer or other clinical note type will add the procedure code to the SP tab. The education form must also be associated with the Smoking Cessation patient communication type. Smoking and tobacco use counseling to the patient is reported using CPT code (smoking and tobacco cessation counseling visit; intermediate, greater than 3 minutes up to 10 minutes) or code (smoking and tobacco cessation counseling visit; intensive, greater than 10 minutes). Remember that these CPT codes are E&M codes, so if you use them along with another E&M code, you must include in the visit note proper documentation supporting the use of the procedure code. Counseling lasting less than 3 minutes is considered part of an evaluation and management (E/M) service and is not paid separately. Proper documentation for codes and includes the total time spent and what was discussed, including cessation techniques, resources and follow-up. The counseling services must be provided by a physician or other qualified health professional and must be provided face-to-face. Some Medicaid programs have not yet adopted payment for these codes. If you are using the optionally licensed Alere education forms, the Alere Smoking Cessation form is recommended. This education form is associated with HCPCS code G0436. This procedure code is associated with the SNOMED code which qualifies for this measure. If you not using the Alere education forms, then it is recommended that you associate the HCPCS code G0436 to the custom-defined education form that you use for this purpose. Write the prescription through the SIG Writer window, and either print or electronically submit the prescription. 150
151 CMS 139; NQF 0101; PQRS 318 SCREENING FOR FUTURE FALL RISK DOMAIN Patient Safety MEASURE Percentage of patients 65 years of age and older who were screened for future fall risk during the measurement period. EXCLUSIONS OR EXCEPTIONS Documentation of medical reason(s) for not screening for fall risk (e.g., patient is not ambulatory). ENTERING DENOMINATOR DATA Patients aged 65 years and older with a visit during the measurement period. ENTERING NUMERATOR DATA Patients who were screened for future fall risk at least once within the measurement period. To chart the screening, you must enter a procedure code that is associated with a qualifying SNOMED code. You may enter the in either the SP or the SO tab of Full Note Composer or other clinical note type window. SNOMED , , ,
152 CMS 140; NQF 0387; PQRS 71 BREAST CANCER: HORMONAL THERAPY FOR STAGE IC-III ESTROGEN RECEPTOR/PROGESTERONE RECEPTOR (ER/PR) POSITIVE BREAST CANCER Please note that Aprima PRM 2015 is not certified for this measure. Therefore, information about this measure is not included in this document. This measure cannot be submitted through Aprima PRM. 152
153 CMS 141; NQF 0385; PQRS 72 COLON CANCER: CHEMOTHERAPY FOR AJCC STAGE III COLON CANCER PATEINTS Please note that Aprima PRM 2015 is not certified for this measure. Therefore, information about this measure is not included in this document. This measure cannot be submitted through Aprima PRM. 153
154 CMS 142; NQF 0089; PQRS 19 DIABETIC RETINOPATHY: COMMUNICATION WITH THE PHYSICIAN MANAGING ONGOING DIABETES CARE DOMAIN Clinical Processes and Effectiveness MEASURE Percentage of patients aged 18 years and older with a diagnosis of diabetic retinopathy who had a dilated macular or fundus exam performed with documented communication to the physician who manages the ongoing care of the patient with diabetes mellitus regarding the findings of the macular or fundus exam at least once within 12 months. EXCLUSIONS OR EXCEPTIONS Documentation of medical reason(s) for not communicating the findings of the dilated macular or fundus exam to the physician who manages the ongoing care of the patient with diabetes. Documentation of patient reason(s) for not communicating the findings of the dilated macular or fundus exam to the physician who manages the on-going care of the patient with diabetes. ENTERING DENOMINATOR DATA All patients aged 18 years and older with a diagnosis of diabetic retinopathy. The patient must have two or more visits within the measurement period. Equals Initial Patient Population who had a dilated macular or fundus exam performed during the first visit. Enter the diagnosis with a qualifying diagnosis code or diagnosis code associated with a SNOMED code in the Dx tab of Full Note Composer or other clinical note type window or enter a problem associated with a qualifying SNOMED code in the problem history category in the Hx tab of Full Note Composer or the Patient History window. 154
155 ICD , , , , , ICD-10 E08.311, E08.319, E08.321, E08.329, E08.331, E08.339, E08.341, E08.349, E08.351, E08.359, E09.311, E09.319, E09.321, E09.329, E09.331, E09.339, E09.341, E09.349, E09.351, E09.359, E10.311, E10.319, E10.321, E10.329, E10.331, E10.339, E10.341, E10.349, E10.351, E10.359, E11.311, E11.319, E11.321, E11.329, E11.331, E11.339, E11.341, E11.349, E11.351, E11.359, E13.311, E13.319, E13.321, E13.329, E13.331, E13.339, E13.341, E13.349, E13.351, E SNOMED , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , To report on this measure, you must order or perform a dilated macular or fundus exam, and then either enter the test results or receive them through an interface and give them a status of Resulted or Approved. Test results not received through an interface must be entered as discrete, quantifiable data. Enter the results in the Patients Results window using a lab template enabling you to enter the test result value. Results stored in the database as text notes or image file cannot be used for reporting. You must associate the LOINC code to the test item on each lab template for both manually entered and electronic results. 155
156 ENTERING NUMERATOR DATA Patients with documentation, at least once within 12 months, of the findings of the dilated macular or fundus exam via communication to the physician who manages the patient s diabetic care. To report on this measure, you must define custom procedure codes for reporting this information to another provider. You will need three custom procedures codes: one for reporting macular edema findings present, one for reporting macular edema finds absent, and one for reporting the level of severity of retinopathy. Each of these procedure codes must be associated with an appropriate SNOMED code. REPORT MACULAR EDEMA FINDINGS PRESENT , , , , , , , , , , , , , , , , , , , , REPORT MACULAR EDEMA FINDINGS ABSENT REPORT LEVEL OF SEVERITY OF RETINOPATHY , , , , , ,
157 CMS 143; NQF 0086; PQRS 12 PRIMARY OPEN ANGLE GLAUCOMA (POAG): OPTIC NERVE ELEVATION DOMAIN Clinical Processes and Effectiveness MEASURE Percentage of patients aged 18 years and older with a diagnosis of POAG who have an optic nerve head evaluation during one or more office visits within 12 months. EXCLUSIONS OR EXCEPTIONS Documentation of medical reason(s) for not performing an optic nerve head evaluation. ENTERING DENOMINATOR DATA All patients aged 18 years and older with a diagnosis of primary open-angle glaucoma. The patient must have two visits within the measurement period. The first visit must include the diagnosis. Enter the diagnosis with a qualifying diagnosis code or diagnosis code associated with a SNOMED code in the Dx tab of Full Note Composer or other clinical note type window. ICD , , , ICD-10 H40.10, H40.11, H40.121, H40.122, H40.123, H40.129, H40.151, H40.152, H40.153, H SNOMED , , , , ,
158 ENTERING NUMERATOR DATA Patients who have an optic nerve head evaluation during one or more office visits within 12 months. To report on this measure, you must order or perform an optic nerve head evaluation. This evaluation must include a cup-to-disc ratio and an optic disc exam for structural abnormalities. Then enter the test results and give them a status of Resulted or Approved. Test results must be entered as discrete, quantifiable data. Enter the results in the Patients Results window using a lab template enabling you to enter the test result value. Results stored in the database as text notes or image file cannot be used for reporting. You must associate a LOINC code to the test item on each lab template for both manually entered and electronic results. CUP-TO-DISC RATIO LOINC , OPTIC DISC EXAM FOR STRUCTURAL ABNORMALITIES LOINC ,
159 CMS 144; NQF 0083; PQRS 8 HEART FAILURE (HF): BETA BLOCKER THERAPY FOR LEFT VENTRICULAR SYSTOLIC DYSFUNCTION (LVSD) DOMAIN Clinical Processes and Effectiveness MEASURE Percentage of patients aged 18 years and older with a diagnosis of heart failure (HF) with a current or prior left ventricular ejection fraction (LVEF) < 40% who were prescribed beta-blocker therapy either within a 12-month period when seen in the outpatient setting OR at each hospital discharge EXCLUSIONS OR EXCEPTIONS Documentation of medical reason(s) for not prescribing beta-blocker therapy (e.g., low blood pressure, fluid overload, asthma, patients recently treated with an intravenous positive inotropic agent, allergy, intolerance, other medical reasons). Documentation of patient reason(s) for not prescribing beta-blocker therapy (e.g., patient declined, other patient reasons). Documentation of system reason(s) for not prescribing betablocker therapy (e.g., other reasons attributable to the healthcare system). ENTERING DENOMINATOR DATA All patients aged 18 years and older with a diagnosis of heart failure, with a current or prior LVEF < 40%. The patient must have two or more visits during the measurement period. Enter the diagnosis with a qualifying diagnosis code or diagnosis code associated with a SNOMED code in the Dx tab of Full Note Composer or other clinical note type window or enter a problem associated with a qualifying SNOMED code in the problem history category in the Hx tab of Full Note Composer or the Patient History window. 159
160 ICD , , , , , , , , , 428.0, 428.1, , , , , , , , , , , , , ICD-10 I11.0, I13.0, I13.2, I50.1, I50.20, I50.21, I50.22, I50.23, I50.30, I50.31, I50.32, I50.33, I50.40, I50.41, I50.42, I50.43, I50.9 SNOMED , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , To include all patients in denominator, you must order or perform an LVEF test and enter the result data. The LVEF test results must either be received through an interface or entered as discrete, quantifiable data in the Patient Results window using a lab template enabling you to enter the LVEF percentage. The results must be given a status of Resulted or Approved. Enter the results in the Patients Results window using a lab template enabling you to enter the test result value. Results stored in the database as text notes or image file cannot be used for reporting. You must associate a LOINC code to the LVEF test item on each lab template for both manually entered and electronic results. LOINC , , , , , , , , , , , , , ,
161 ENTERING NUMERATOR DATA When the LVEF result is equal to or less than 40 percent, then you must prescribe either an ACE inhibitor or ARB therapy. Patients who were prescribed beta- blocker therapy either within a 12-month period when seen in the outpatient setting or at hospital discharge. To report the beta-blocker therapy, write the prescription through the SIG Writer window or prescription refill message and print the prescription or send it electronically. 161
162 CMS 145; NQF 0070; PQRS 7 CORONARY ARTERY DISEASE (CAD): BETA BLOCKER THERAPY PRIOR MYOCARDIAL INFARCTION (MI) OR LEFT VENTRICULAR SYSTOLIC DYSFUNCTION (LVEF <40%) DOMAIN Clinical Processes and Effectiveness MEASURE Percentage of patients aged 18 years and older with a diagnosis of coronary artery disease seen within a 12-month period who also have a prior MI or a current or prior LVEF <40% who were prescribed beta-blocker therapy. EXCLUSIONS OR EXCEPTIONS Documentation of medical reason(s) for not prescribing beta-blocker therapy (e.g., allergy, intolerance, other medical reasons). Documentation of patient reason(s) for not prescribing beta-blocker therapy (e.g., patient declined, other patient reasons). Documentation of system reason(s) for not prescribing beta-blocker therapy (e.g., other reasons attributable to the health care system). ENTERING DENOMINATOR DATA All patients aged 18 years and older with a diagnosis of coronary artery disease seen within a 12- month period. The patient must have two visits. Equals Initial Patient Population who also have prior MI or a current or prior LVEF <40%. Please note that this measure produces results for two denominator and numerator combinations. The denominator information given here is correct for both. 162
163 Enter the diagnosis with a qualifying diagnosis code or diagnosis code associated with a SNOMED code in the Dx tab of Full Note Composer or other clinical note type window or in the problem enter a problem associated with a qualifying SNOMED code in the problem history category in the Hx tab of Full Note Composer or the Patient History window. CAD ICD , 411.1, , , 413.0, 413.1, 413.9, , , , , , , , , 414.8, 414.9, V45.81, V45.82 CAD ICD-10 I20.0, I20.1, I20.8, I20.9, I24.0, I24.1, I24.8, I24.9, I25.10, I25.110, I25.111, I25.118, I25.119, I25.5, I25.6, I25.700, I25.701, I25.708, I25.709, I25.710, I25.711, I25.718, I25.719, I25.720, I25.721, I25.728, I25.729, I25.730, I25.731, I25.738, I25.739, I25.750, I25.751, I25.758, I25.759, I25.760, I25.761, I25.768, I25.769, I25.790, I25.791, I25.798, I25.799, I25.89, I25.9, Z95.1, Z95.5, Z98.61 CAD SNOMED , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , To document a prior MI, enter a problem associated with a SNOMED code in the problem history category in the Hx tab of Full Note Composer or the Patient History window. MI ICD , , , , , , , , , , , , , , , , , , , , , , , , 163
164 410.80, , , , , , 412 MI ICD-10 I21.01, I21.02, I21.09, I21.11, I21.19, I21.21, I21.29, I21.3, I21.4, I22.0, I22.1, I22.2, I22.8, I22.9, I24.1, I25.2 MI SNOMED , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , To document cardiac surgery, enter the procedure with a qualifying procedure code or procedure code associated with a SNOMED code in the SP or SO tab of Full Note Composer or other clinical note type window. Or enter the surgery in the surgical history category in the Hx tab of Full Note Composer or the Patient History window. The history question used to enter the cardiac surgery must be associated with a SNOMED code. CARDIAC SURGERY CPT 33140, 33510, 33511, 33512, 33513, 33514, 33516, 33517, 33518, 33519, 33521, 33522, 33523, 33533, 33534, 33535, 33536, 92920, 92924, 92928, 92933, 92937, 92941, 92943, 92980, 92981, 92982, 92984, 92995, CARDIAC SURGERY SNOMED , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , 164
165 , , , , , , , , , , To report on this measure, you must order or perform an LVEF test and enter the result data. When the LVEF result is equal to or less than 40 percent, then you must prescribe either an ACE inhibitor or ARB therapy. The LVEF test results must either be received through an interface or entered as discrete, quantifiable data in the Patient Results window using a lab template enabling you to enter the LVEF percentage. The results must be given a status of Resulted or Approved. Test results not received through an interface must be entered as discrete, quantifiable data. Enter the results in the Patients Results window using a lab template enabling you to enter the test result value. Results stored in the database as text notes or image file cannot be used for reporting. You must associate a LOINC code to the LVEF test item on each lab template for both manually entered and electronic results. LOINC , , , , , , , , , , , , , , ENTERING NUMERATOR DATA Patients who were prescribed beta-blocker therapy. To report the beta-blocker therapy, write the prescription through the SIG Writer window or prescription refill message and print the prescription or send it electronically. 165
166 CMS 146; NQF 0002; PQRS 66 APPROPRIATE TESTING FOR CHILDREN WITH PHARYNGITIS DOMAIN Health Resources MEASURE Percentage of children 2-18 years of age who were diagnosed with pharyngitis, ordered an antibiotic and received a group A streptococcus (strep) test for the episode. EXCLUSIONS OR EXCEPTIONS Children who are taking antibiotics in the 30 days prior to the diagnosis of pharyngitis. ENTERING DENOMINATOR DATA Children 2-18 years of age who had an outpatient or emergency department (ED) visit with a diagnosis of pharyngitis during the measurement period and an antibiotic ordered on or three days after the visit. You must diagnosis the patient with pharyngitis using one of the diagnosis codes below during a visit within the measurement period. ICD , 462, 463 ICD-10 J02.8, J02.9, J03.80, J03.81, J03.90, J03.91 SNOMED , , , , , , , , , , , , , , , , , , , , , , , , , ,
167 You must prescribe an antibiotic within three days following the visit. To report the antibiotic, write a prescription for an antibiotic using the SIG writer window and print the prescription or send it electronically. The antibiotic must be dispensed within three days after the qualifying visit. ENTERING NUMERATOR DATA Children with a group A streptococcus test in the seven-day period from three days prior through three days after the diagnosis of pharyngitis. To report on this measure, you must prescribe an antibiotic and order a group A streptococcus (strep) test and enter the test results. To report the antibiotic, write a prescription for an antibiotic using the SIG writer window and print the prescription or send it electronically. To report the strep test, order the test and then either enter the test results or receive them through an interface and give them a status of Resulted or Approved. The strep test results not received through an interface must be entered as discrete, quantifiable data. Enter the results in the Patients Results window using a lab template enabling you to enter the strep value. Results stored in the database as text notes or image file cannot be used for reporting. You must associate a LOINC code to the strep test item on each lab template for both manually entered and electronic results. LOINC codes for this result are listed below. LOINC 626-2, , , , , , , , , , , ,
168 CMS 147; NQF 0041; PQRS 110 PREVENTATIVE CARE AND SCREENING: INFLUENZA IMMUNIZATION DOMAIN Public Health MEASURE Percentage of patients aged 6 months and older seen for a visit between October 1 and March 31 who received an influenza immunization OR who reported previous receipt of an influenza immunization. EXCLUSIONS OR EXCEPTIONS Documentation of medical reason(s) for not receiving influenza immunization (eg, patient allergy, other medical reasons). Documentation of patient reason(s) for not receiving influenza immunization (eg, patient declined, other patient reasons). Documentation of system reason(s) for not receiving influenza immunization (eg, vaccine not available, other system reasons). ENTERING DENOMINATOR DATA Equals Initial Patient Population and seen for a visit between October 1 and March 31. The patient must have a visit during flu season, which is defined as October of the prior year through March of the current year. The patient must also have one, or in some circumstances two, additional visits during the reporting period. 168
169 ENTERING NUMERATOR DATA Patients who received an influenza immunization OR who reported previous receipt of an influenza immunization. To report on this measure, you must document the administration of the flu immunization, or enter it in the vaccine history category. The vaccine must have been administered between October of the prior year and March of the current year. To document the influenza immunization, enter the vaccination in the vaccine administration record using one of the following CPT codes or a procedure code associated with a SNOMED code. Enter the procedure in the SP tab of Full Note Composer or other clinical note type window. Then document the vaccination details in the vaccine administration record. You may also document the pneumonia immunization by using a type of vaccine associated with the qualifying CVX code. Identify the type of vaccine when documenting the vaccine details in the vaccine administration record. To document a vaccination given in the past, you must use a type of vaccine associated with the qualifying CVX code. Enter the vaccination in the vaccination history category in the Hx tab of Full Note Composer or in the Patient History window. Then, identify the type of vaccine when documenting the vaccine details in the vaccine administration record. Please note that you must make this entry in a visit during the flu season. CPT 90656, 90658, 90660, 90661, 90662, 90664, 90666, 90667, SNOMED , CVX 111, 135, 140, 141,
170 CMS 148; NQF 0060; PQRS 365 HEMOGLOBIN A1C TEST FOR PEDIATRIC PATIENTS DOMAIN Clinical Processes and Effectiveness MEASURE Percentage of patients 5-17 years of age with diabetes with an HbA1c test during the measurement period. EXCLUSIONS OR EXCEPTIONS Patients with a diagnosis of gestational diabetes during the measurement period. ENTERING DENOMINATOR DATA Patients 5 to 17 years of age with a diagnosis of diabetes and a face-to-face visit for diabetes care between the physician and the patient that predates the most recent visit by at least 12 months. Enter the diagnosis with a qualifying diagnosis code or diagnosis code associated with a SNOMED code in the Dx tab of Full Note Composer or other clinical note type window or enter a problem associated with a qualifying SNOMED code in the problem history category in the Hx tab of Full Note Composer or the Patient History window. ICD , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , ICD-10 E10.10, E10.11, E10.21, E10.22, E10.29, E10.311, E10.319, E10.321, E10.329, E10.331, E10.339, E10.341, E10.349, E10.351, E10.359, E10.36, E10.39, E10.40, E10.41, E10.42, E10.43, E10.44, E10.49, E10.51, E10.52, E10.59, E10.610, E10.618, E10.620, E10.621, E10.622, E10.628, E10.630, 170
171 E10.638, E10.641, E10.649, E10.65, E10.69, E10.8, E10.9, E11.00, E11.01, E11.21, E11.22, E11.29, E11.311, E11.319, E11.321, E11.329, E11.331, E11.339, E11.341, E11.349, E11.351, E11.359, E11.36, E11.39, E11.40, E11.41, E11.42, E11.43, E11.44, E11.49, E11.51, E11.52, E11.59, E11.610, E11.618, E11.620, E11.621, E11.622, E11.628, E11.630, E11.638, E11.641, E11.649, E11.65, E11.69, E11.8, E11.9, O24.011, O24.012, O24.013, O24.019, O24.02, O24.03, O24.111, O24.112, O24.113, O24.119, O24.12, O24.13 SNOMED , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , You must have charted a patient visit note for a face -to-face visit with the patient at least 12 months prior to the visit during the reporting period. ENTERING NUMERATOR DATA Patients with documentation of date and result for an HbA1c test during the measurement period. To report on this measure, you must order or perform an A1c test, and then either enter the test results or receive them through an interface and give them a status of Resulted or Approved. The A1c test results not received through an interface must be entered as discrete, quantifiable data. Enter the results in the Patients Results window using a lab template enabling you to enter the HGB A1c value. Results stored in the database as text notes or image file cannot be used reporting. 171
172 You must associate a LOINC code to the A1C test item on each lab template for both manually entered and electronic results. LOINC , ,
173 CMS 149; NQF NA; PQRS 281 DEMENTIA: COGNITIVE ASSESSMENT DOMAIN Clinical Processes and Effectiveness MEASURE Percentage of patients, regardless of age, with a diagnosis of dementia for whom an assessment of cognition is performed and the results reviewed at least once within a 12-month period. EXCLUSIONS OR EXCEPTIONS Documentation of medical reason(s) for not assessing cognition (e.g., patient with very advanced stage dementia, other medical reason). Documentation of patient reason(s) for not assessing cognition. ENTERING DENOMINATOR DATA All patients, regardless of age, with a diagnosis of dementia. The patient must have two visits. ICD , 290.0, , , , , , , 290.3, , , , , 290.8, 290.9, , , , , 294.8, 331.0, , , ICD-10 A52.17, F01.50, F01.51, F02.80, F02.81, F03.90, F03.91, F05, F06.0, F06.8, G30.0, G30.1, G30.8, G30.9, G31.01, G31.09, G31.83 SNOMED , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , 173
174 , , , , , , , , , , , , , , , , , ENTERING NUMERATOR DATA Patients for whom an assessment of cognition is performed and the results reviewed at least once within a 12-month period. To report on this measure, enter the assessment using a procedure code or a procedure code associated with a SNOMED code. You may enter the procedure in either the SP or the SO tab of Full Note Composer or other clinical note type window. CPT 97003, SNOMED , To report on this measure, you must have set up an observation item for the score of each assessment that you use, and put these observation items in an observation template. The observation item for each assessment s score must include the appropriate LOINC code for the functional status assessment. LOINC , , , , , , You must also have a clinical note type defined to include the Observation tab so that you can use the observation template to chart the assessment. None of the system-defined clinical note type windows (such as Full Note Composer) include the Observation tab. So, you must use a custom clinical note type window to chart patient visit notes that will include a functional status assessment. Enter the score of the functional status assessment in the observation template on 174
175 the Observation tab. Please note that entries in the Cognitive and Functional Assessment history categories do not count for this measure. 175
176 CMS 153; NQF 0033; PQRS 310 CHLAMYDIA SCREENING FOR WOMEN DOMAIN Public Health MEASURE Percentage of women 16 through 24 years of age who were identified as sexually active and who had at least one test for Chlamydia during the measurement period. EXCLUSIONS OR EXCEPTIONS Women who received a pregnancy test solely as a safety precaution before ordering an x-ray or specified medications. ENTERING DENOMINATOR DATA This measure reports for two groups of patients. Those aged 16 to 20, and those aged 21 to 24. The patient must have at least one visit during the measurement period. The patient must be identified as sexually active. Patients may identify as sexually active in a number of ways, including a procedure for a pregnancy test, a diagnosis for pregnancy or pregnancy related problem, a procedure for a birth, a lab test for or a diagnosis for a sexually transmitted infection, a prescription for contraceptives, a procedure for a contraceptive device, and a procedure for infertility treatments. Patients who received a pregnancy test solely as a safety precaution before ordering an x-ray or specified medications are excluded. However, this exclusion does not apply to patients who qualify for the initial patient population based on services other than the pregnancy test alone. ENTERING NUMERATOR DATA To report on this measure, you must order or perform a Chlamydia test, and then either enter the test results or receive them through an interface and give them a status of Resulted or Approved. 176
177 Chlamydia test results not received through an interface must be entered as discrete, quantifiable data. Enter the results in the Patients Results window using a lab template enabling you to enter the test result value. Results stored in the database as text notes or image file cannot be used for reporting. You must associate a LOINC code to the Chlamydia test item on each lab template for both manually entered and electronic results. LOINC CODES , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , ,
178 CMS 154; NQF 0069; PQRS 65 APPROPRIATE TREATMENT FOR CHILDREN WITH UPPER RESPIRATORY INFECTION (URI) DOMAIN Health Resources MEASURE Percentage of children 3 months through 18 years of age who were diagnosed with upper respiratory infection (URI) and were not dispensed an antibiotic prescription on or three days after the episode. Please note that for this measure, the desired outcome is to have the numerator be a low number. EXCLUSIONS OR EXCEPTIONS Exclude children who are taking antibiotics in the 30 days prior to the date of the encounter. Exclude children who had an encounter with a competing diagnosis within three days after the initial diagnosis. ENTERING DENOMINATOR DATA The patient must be between 3 months and 18 years of age. The patient must have an outpatient or emergency department visit with a diagnosis of upper respiratory infection (URI) during the measurement period. You must diagnosis the patient with an upper respiratory infection using a qualifying ICD-9 or SNOMED code. Enter the diagnosis code in the Dx tab of Full Note Composer or other clinical note type window. ICD-9 460, 465.0, 465.8, ICD-10 J00, J06.0, J
179 SNOMED , , , , , , ENTERING NUMERATOR DATA To report on this measure, you must not write a prescription for an antibiotic on the date of the visit or within three days of the visit. Patients for whom an antibiotic prescription is written are included in the denominator, but not in the numerator. 179
180 CMS 155; NQF 0024; PQRS 239 WEIGHT ASSESSMENT AND COUNSELING FOR NUTRITION AND PHYSICAL ACTIVITY FOR CHILDREN AND ADOLESCENTS DOMAIN Public Health MEASURE Percentage of patients 3 through 17 years of age who had an outpatient visit with a Primary Care Physician (PCP) or Obstetrician/Gynecologist (OB/GYN) and who had evidence of the following during the measurement period. Three rates are reported. Percentage of patients with height, weight, and body mass index (BMI) percentile documentation Percentage of patients with counseling for nutrition Percentage of patients with counseling for physical activity EXCLUSIONS OR EXCEPTIONS Patients who have a diagnosis of pregnancy during the measurement period. ENTERING DENOMINATOR DATA The patient must between 3 and 17 years old. The patient must have at least one visit with a primary care physician or an obstetrician/gynecologist (OB/GYN) during the measurement period. ENTERING NUMERATOR DATA This measure has three different numerators. To be included in the first numerator, you must enter the BMI. To record the BMI percentile, you must enter the patient s height and weight in the Vitals tab of the patient visit note. The application automatically calculates the BMI. For this measure, you must associate one of the qualifying LOINC codes with the system-defined BMI observation item. Please note that the LOINC codes appropriate for children and 180
181 adolescents are different from the LOINC code for adults. If you are also reporting on CMS 69 Preventive Care and Screening: Body Mass Index (BMI) Screening and Follow-Up, you will need to generate your CQM QRDA files twice. You will need to associate the LOINC code for adults to the BMI observation item, and generate the report to obtain your counts for the CMS 69 measure. Then you will need associate the LOINC code for children to the BMI observation item, and generate the report to obtain your counts for this measure. LOINC FOR CHILDREN AND ADOLESCENTS BMI , , To be included in the second numerator, you must record counseling for nutrition was performed. You can either enter the ICD-9 procedure code V65.3 in the Dx tab or enter one of the following. CPT CODES 97802, 97803, 97804, 98961, 98962, HCPCS G0270, G0271, G8417, S9451, S9452, S9449, S9470 To be included in the third numerator, you must record that counseling for physical activity was performed. You can either enter the ICD-9 procedure code V65.41 in the Dx tab and one of the following CPT or HCPCS codes in the SP tab of the patient visit note. CPT 98961, 98962, HCPCS S9449, S9451, G8417 If you typically use an education form with or for nutrition or physical activity counseling and the procedure code is associated with the education form, he selecting the education form from the 181
182 Education Form slider in Full Note Composer or other clinical note type will add the procedure code to the SP tab. The education form must also be associated with the patient communication type Nutrition or the patient communication type Physical Activity. 182
183 CMS 156; NQF 0022; PQRS 238 USE OF HIGH RISK MEDICATIONS IN THE ELDERLY DOMAIN Patient Safety MEASURE Percentage of patients 66 years of age and older who were ordered high-risk medications. Two rates are reported. Percentage of patients who were ordered at least one high-risk medication. Percentage of patients who were ordered at least two high-risk medications. EXCLUSIONS OR EXCEPTIONS None ENTERING DENOMINATOR DATA The patient must be 66 years old or older and must have at least one visit during the measurement period. ENTERING NUMERATOR DATA To report on this measure, you must write all prescriptions through the SIG Writer window or prescription refill message and print the prescriptions or send them electronically. Patients 66 years old or older are counted in the first numerator if there is a prescription for a high-risk medication. These patients are counted in the second numerator if there are prescriptions for two or more high-risk medications. 183
184 CMS 157; NQF 0384; PQRS 143 ONCOLOGY: MEDICAL AND RADIATION PAIN INTENSITY QUANTIFIED Please note that Aprima PRM 2015 is not certified for this measure. Therefore, information about this measure is not included in this document. This measure cannot be submitted through Aprima PRM. 184
185 CMS 158; NQF 0608; PQRS 369 PREGNANT WOMEN THAT HAD HBSAG TESTING DOMAIN Clinical Processes and Effectiveness MEASURE This measure identifies pregnant women who had a HBsAg (hepatitis B) test during their pregnancy. EXCLUSIONS OR EXCEPTIONS Patients with current or past Hepatitis B infection. ENTERING DENOMINATOR DATA All female patients aged 12 and older who had a full term delivery during the measurement period. To chart the delivery, you must enter a procedure code or a procedure code that is associated with a SNOMED code. You may enter the procedure in either the SP or the SO tab of Full Note Composer or other clinical note type window. CPT 59400, 59409, 59410, 59510, 59514, 59515, 59610, 59612, 59614, 59618, 59620, SNOMED , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , 185
186 , , , , , , , , , , , , , , , , , , , , , , , , , , You may also chart the delivery using a diagnosis code or a diagnosis code associated with a qualifying SNOMED code. Enter the diagnosis code in the Dx tab of Full Note Composer or other clinical note type window or in the problem/diagnosis category of the Patient History window. ICD , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , 650, , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , V27.0, V27.2, V27.3, V27.5, V27.6, V27.9 ICD-10 F53, O10.02, O10.03, O10.12, O10.13, O10.22, O10.23, O10.32, O10.33, O10.42, O10.43, O10.92, O10.93, O15.2, O24.02, O24.03, O24.12, O24.13, O24.32, O24.33, O24.420, O24.424, O24.429, O24.430, O24.434, O24.439, O24.82, O24.83, O24.92, O24.93, O25.2, O25.3, O26.62, O26.63, O26.72, O26.73, O60.20, O60.22, O60.23, O62.3, O62.4, O62.8, O62.9, O63.0, O63.1, 186
187 O63.2, O63.9, O64.0XX0, O64.1XX0, O64.2XX0, O64.3XX0, O64.4XX0, O64.5XX0, O64.8XX0, O64.9XX0, O65.0, O65.1, O65.2, O65.3, O65.4, O65.5, O65.8, O65.9, O66.0, O66.1, O66.2, O66.3, O66.41, O66.5, O66.6, O66.8, O66.9, O67.0, O67.8, O67.9, O68, O69.0, O69.1, O69.2, O69.3, O69.4, O69.5, O69.81, O69.82, O69.89, O69.9, O70.0, O70.1, O70.2, O70.3, O70.4, O70.9, O71.2, O71.3, O71.4, O71.5, O71.6, O71.7, O71.89, O71.9, O72.0, O72.1, O72.2, O73.0, O73.1, O74.0, O74.1, O74.2, O74.3, O74.4, O74.5, O74.6, O74.7, O74.8, O74.9, O75.0, O75.1, O75.5, O75.81, O75.89, O75.9, O76, O77.0, O77.1, O77.8, O77.9, O80, O82, O85, O86.81, O86.89, O87.0, O87.1, O87.2, O87.3, O87.4, O87.8, O87.9, O88.02, O88.03, O88.12, O88.13, O88.22, O88.23, O88.32, O88.33, O88.82, O88.83, O89.01, O89.09, O89.1, O89.2, O89.3, O89.4, O89.5, O89.6, O89.8, O89.9, O90.81, O90.89, O90.9, O91.02, O91.12, O91.22, O92.02, O92.12, O92.20, O92.29, O98.02, O98.03, O98.12, O98.13, O98.22, O98.23, O98.32, O98.33, O98.42, O98.43, O98.52, O98.53, O98.62, O98.63, O98.72, O98.73, O98.82, O98.83, O98.92, O98.93, O99.02, O99.03, O99.12, O99.13, O99.214, O99.215, O99.284, O99.285, O99.314, O99.315, O99.324, O99.325, O99.334, O99.335, O99.344, O99.345, O99.354, O99.355, O99.42, O99.43, O99.52, O99.53, O99.62, O99.63, O99.72, O99.73, O99.814, O99.815, O99.824, O99.825, O99.834, O99.835, O99.844, O99.845, O99.89, O9A.12, O9A.13, O9A.22, O9A.23, O9A.32, O9A.33, O9A.42, O9A.43, O9A.52, O9A.53, Z37.0, Z37.2, Z37.3, Z37.59, Z37.69, Z37.7 SNOMED , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , ENTERING NUMERATOR DATA Patients who were tested for Hepatitis B surface antigen (HBsAg) during pregnancy within 280 days prior to delivery. 187
188 To report on this measure, you must order or perform a HBsAg test, and then either enter the test results or receive them through an interface and give them a status of Resulted or Approved. Test results not received through an interface must be entered as discrete, quantifiable data. Enter the results in the Patients Results window using a lab template enabling you to enter the test result value. Results stored in the database as text notes or image file cannot be used for reporting. You must associate a LOINC code to the HBsAg test item on each lab template for both manually entered and electronic results. LOINC , , , , , , , , ,
189 CMS 159; NQF 0710; PQRS 370 DEPRESSION REMISSION AT TWELVE MONTHS DOMAIN Clinical Processes and Effectiveness MEASURE Adult patients age 18 and older with major depression or dysthymia and an initial PHQ-9 score > 9 who demonstrate remission at twelve months defined as PHQ-9 score less than five. This measure applies to both patients with newly diagnosed and existing depression whose current PHQ-9 score indicates a need for treatment. EXCLUSIONS OR EXCEPTIONS Patients who died. Patients who received hospice services. Patients who were permanent nursing home residents (> 1 year). Patients with a diagnosis of bipolar disorder. Patients with a diagnosis of personality disorder. ENTERING DENOMINATOR DATA Adults age 18 and older with a diagnosis of major depression or dysthymia and an initial PHQ-9 score greater than nine during an outpatient encounter. Enter the diagnosis with a qualifying diagnosis code or diagnosis code associated with a SNOMED code in the Dx tab of Full Note Composer or other clinical note type window or enter a problem associated with a qualifying SNOMED code in the problem history category in the Hx tab of Full Note Composer or the Patient History window. ICD , , , , , , , , , , , , 298.0, 300.4, 309.1,
190 ICD-10 F32.0, F32.1, F32.2, F32.3, F32.4, F32.9, F33.0, F33.1, F33.2, F33.3, F33.40, F33.41, F33.8, F33.9, F34.1, F34.1 SNOMED , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , To report on this measure, you must have set up an observation item for the PHQ-9 assessment score, and put the observation item in an observation template. The observation item must include the appropriate LOINC code for the PHQ-9 assessment. LOINC , , , You must also have a clinical note type defined to include the Observation tab so that you can use the observation template to chart the assessment. None of the system-defined clinical note type windows (such as Full Note Composer) include the Observation tab. So, you must use a custom clinical note type window to chart patient visit notes that will include a functional status assessment. Enter the score of the PHQ-9 assessment in the observation template on the Observation tab. 190
191 ENTERING NUMERATOR DATA Adults who achieved remission at twelve months as demonstrated by a twelve month (+/- 30 days) PHQ-9 score of less than five. The visit that includes the follow up PHQ-9 assessment must be at least 11 months after and less than 13 months after the first assessment. To report on this measure, you must have set up an observation item for the PHQ-9 assessment score, and put the observation item in an observation template. The observation item must include the appropriate LOINC code for the PHQ-9 assessment. LOINC , , , You must also have a clinical note type defined to include the Observation tab so that you can use the observation template to chart the assessment. None of the system-defined clinical note type windows (such as Full Note Composer) include the Observation tab. So, you must use a custom clinical note type window to chart patient visit notes that will include a functional status assessment. Enter the score of the PHQ-9 assessment in the observation template on the Observation tab. 191
192 CMS 160; NQF 0712; PQRS 371 DEPRESSION UTILIZATION OF THE PHQ-9 TOOL This measure cannot be reported on if the reporting period is less than one year. DOMAIN Clinical Processes and Effectiveness MEASURE Adult patients age 18 and older with the diagnosis of major depression or dysthymia who have a PHQ-9 tool administered at least once during a 4-month period in which there was a qualifying visit. EXCLUSIONS OR EXCEPTIONS Patients who died. Patients who received hospice services. Patients who were permanent nursing home residents (> 1 year). Patients with a diagnosis of bipolar disorder. Patients with a diagnosis of personality disorder. ENTERING DENOMINATOR DATA Adult patients age 18 and older with an office visit and the diagnosis of major depression or dysthymia during each four-month period. Denominator 1: The patient must have an active diagnosis of major depression or dysthymia during the last 4 months of the measurement year. Denominator 2: The patient must have an active diagnosis of major depression or dysthymia during the 5 th to 8 th month of the measurement year. Denominator 3: The patient must have an active diagnosis of major depression or dysthymia during the first 4 months of the measurement year. Enter the diagnosis with a qualifying diagnosis code or diagnosis code associated with a SNOMED code in the Dx tab of Full Note Composer or other clinical note type window or enter a problem associated with a qualifying SNOMED code in the problem history category in the Hx tab of Full Note Composer or the Patient History window. 192
193 ICD , , , , , , , , , , , , 298.0, 300.4, 309.1, 311 ICD-10 F32.0, F32.1, F32.2, F32.3, F32.4, F32.9, F33.0, F33.1, F33.2, F33.3, F33.40, F33.41, F33.8, F33.9, F34.1, F34.1 SNOMED , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , ENTERING NUMERATOR DATA Adult patients who have a PHQ-9 tool administered at least once during the four-month period. Numerator 1: The PHQ-9 assessment must be performed in the last 4 months of the measurement year. Numerator 2: The PHQ-9 assessment must be performed in the 5th to 8th months of the measurement year. Numerator 3: The PHQ-9 assessment must be performed in the first 4 months of the measurement year. To report on this measure, you must have set up an observation item for the PHQ-9 assessment score, and put the observation item in an observation template. The observation item must include the appropriate LOINC code for the PHQ-9 assessment. 193
194 LOINC , , , You must also have a clinical note type defined to include the Observation tab so that you can use the observation template to chart the assessment. None of the system-defined clinical note type windows (such as Full Note Composer) include the Observation tab. So, you must use a custom clinical note type window to chart patient visit notes that will include a functional status assessment. Enter the score of the PHQ-9 assessment in the observation template on the Observation tab. 194
195 CMS 161; NQF 0104; PQRS 107 MAJOR DEPRESSIVE DISORDER (MDD): SUICIDE RISK ASSESSMENT DOMAIN Clinical Processes and Effectiveness MEASURE Percentage of patients aged 18 years and older with a new diagnosis or recurrent episode of MDD who had a suicide risk assessment completed at each visit during the measurement period. EXCLUSIONS OR EXCEPTIONS None ENTERING DENOMINATOR DATA All patients aged 18 years and older with a new diagnosis or recurrent episode of MDD. Enter the diagnosis with a qualifying diagnosis code or diagnosis code associated with a SNOMED code in the Dx tab of Full Note Composer or other clinical note type window or enter a problem associated with a qualifying SNOMED code in the problem history category in the Hx tab of Full Note Composer or the Patient History window. ICD , , , , , , , , , ICD-10 F32.0, F32.1, F32.2, F32.3, F32.9, F33.0, F33.1, F33.2, F33.3, F33.9, SNOMED , , , , , , , , , , , , , , , , , , , , , , , , , 195
196 , , , , , , , , , , ENTERING NUMERATOR DATA Patients who had suicide risk assessment completed at each visit. To chart the assessment, you must enter a procedure code that is associated with the SNOMED code Enter the procedure in the SP tab of Full Note Composer or other clinical note type window. 196
197 CMS 163; NQF 0064; PQRS 2 DIABETES: LOW DENSITY LIPOPROTEIN (LDL) MANAGEMENT DOMAIN Clinical Processes and Effectiveness MEASURE Percentage of patients years of age with diabetes whose LDL-C was adequately controlled (<100 mg/dl) during the measurement period. EXCLUSIONS OR EXCEPTIONS Exclude patients with a diagnosis of gestational diabetes during the measurement period. ENTERING DENOMINATOR DATA Patients years of age with diabetes with a visit during the measurement period. Enter the diagnosis with a qualifying diagnosis code or diagnosis code associated with a SNOMED code in the Dx tab of Full Note Composer or other clinical note type window or enter a problem associated with a qualifying SNOMED code in the problem history category in the Hx tab of Full Note Composer or the Patient History window. The diagnosis must be active. ICD , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , ICD-10 E10.10, E10.11, E10.21, E10.22, E10.29, E10.311, E10.319, E10.321, E10.329, E10.331, E10.339, E10.341, E10.349, E10.351, E10.359, E10.36, E10.39, E10.40, E10.41, E10.42, E10.43, E10.44, E10.49, E10.51, E10.52, E10.59, E10.610, E10.618, E10.620, E10.621, E10.622, E10.628, E10.630, E10.638, E10.641, E10.649, E10.65, E10.69, E10.8, E10.9, E11.00, E11.01, E11.21, E11.22, E11.29, 197
198 E11.311, E11.319, E11.321, E11.329, E11.331, E11.339, E11.341, E11.349, E11.351, E11.359, E11.36, E11.39, E11.40, E11.41, E11.42, E11.43, E11.44, E11.49, E11.51, E11.52, E11.59, E11.610, E11.618, E11.620, E11.621, E11.622, E11.628, E11.630, E11.638, E11.641, E11.649, E11.65, E11.69, E11.8, E11.9, O24.011, O24.012, O24.013, O24.019, O24.02, O24.03, O24.111, O24.112, O24.113, O24.119, O24.12, O24.13 SNOMED , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , ENTERING NUMERATOR DATA Patients whose most recent LDL-C level performed during the measurement period is <100 mg/dl. To report on this measure, you must order or perform an LDL- C test, and then either enter the test results or receive them through an interface and give them a status of Resulted or Approved. Test results not received through an interface must be entered as discrete, quantifiable data. Enter the results in the Patients Results window using a lab template enabling you to enter the test result value. Results stored in the database as text notes or image file cannot be used for reporting. You must associate a LOINC code to the LDL-C test item on each lab template for both manually entered and electronic results. This uses the most recent test results. LOINC , ,
199 CMS 164; NQF 0068; PQRS 204 ISCHEMIC VASCULAR DISEASE (IVD): USE OF ASPIRIN OR ANOTHER ANTITHROMBIC MEDICATION DOMAIN Clinical Processes and Effectiveness MEASURE Percentage of patients 18 years of age and older who were discharged alive for acute myocardial infarction (AMI), coronary artery bypass graft (CABG) or percutaneous coronary interventions (PCI) in the 12 months prior to the measurement period, or who had an active diagnosis of ischemic vascular disease (IVD) during the measurement period, and who had documentation of use of aspirin or another antithrombotic during the measurement period. EXCLUSIONS OR EXCEPTIONS None ENTERING DENOMINATOR DATA Patients 18 years of age and older with a visit during the measurement period, and an active diagnosis of ischemic vascular disease (IVD) or who were discharged alive for acute myocardial infarction (AMI), coronary artery bypass graft (CABG) or percutaneous coronary interventions (PCI) in the 12 months prior to the measurement period. THE PATIENT MUST EITHER Have an active diagnosis of IVD during the measurement period, or Have an active diagnosis of AMI within 12 months before the start of the measurement period and still active during the measurement period, or Have had a PCI performed less than 12 months before the start of the measurement period, or Have had CABG performed less than 12 months before the start of the measurement period. 199
200 Enter the diagnosis with a qualifying diagnosis code or diagnosis code associated with a SNOMED code in the Dx tab of Full Note Composer or other clinical note type window or enter a problem associated with a qualifying SNOMED code in the problem history category in the Hx tab of Full Note Composer or the Patient History window. Acute Myocardial Infarction ICD , , , , , , , , , ICD-10 I21.01, I21.02, I21.09, I21.11, I21.19, I21.21, I21.29, I21.3, I21.4 SNOMED , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , Ischemic Vascular Disease ICD , 411.1, , , 413.0, 413.1, 413.9, , , , , , , , , 414.2, 414.8, 414.9, 429.2, , , , , , , , , , , , , , , , , , , 440.1, , , , , , , 440.4, 444.0, 444.1, , , , , 444.9, , , ICD-10 I20.0, I20.1, I20.8, I20.9, I24.0, I24.1, I24.8, I24.9, I25.10, I25.110, I25.111, I25.118, I25.119, I25.5, I25.6, I25.700, I25.701, I25.708, I25.709, I25.710, I25.711, I25.718, I25.719, I25.720, I25.721, I25.728, I25.729, I25.730, I25.731, I25.738, I25.739, I25.750, I25.751, I25.758, I25.759, 200
201 I25.760, I25.761, I25.768, I25.769, I25.790, I25.791, I25.798, I25.799, I25.810, I25.811, I25.812, I25.82, I25.89, I25.9, I63.00, I63.011, I63.012, I63.019, I63.02, I63.031, I63.032, I63.039, I63.09, I63.10, I63.111, I63.112, I63.119, I63.12, I63.131, I63.132, I63.139, I63.19, I63.20, I63.211, I63.212, I63.219, I63.22, I63.231, I63.232, I63.239, I63.29, I63.30, I63.311, I63.312, I63.319, I63.321, I63.322, I63.329, I63.331, I63.332, I63.339, I63.341, I63.342, I63.349, I63.39, I63.40, I63.411, I63.412, I63.419, I63.421, I63.422, I63.429, I63.431, I63.432, I63.439, I63.441, I63.442, I63.449, I63.49, I63.50, I63.511, I63.512, I63.519, I63.521, I63.522, I63.529, I63.531, I63.532, I63.539, I63.541, I63.542, I63.549, I63.59, I63.6, I63.8, I63.9, I65.01, I65.02, I65.03, I65.09, I65.1, I65.21, I65.22, I65.23, I65.29, I65.8, I65.9, I66.01, I66.02, I66.03, I66.09, I66.11, I66.12, I66.13, I66.19, I66.21, I66.22, I66.23, I66.29, I66.3, I66.8, I66.9, I70.1, I70.201, I70.202, I70.203, I70.208, I70.209, I70.211, I70.212, I70.213, I70.218, I70.219, I70.221, I70.222, I70.223, I70.228, I70.229, I70.231, I70.232, I70.233, I70.234, I70.235, I70.238, I70.239, I70.241, I70.242, I70.243, I70.244, I70.245, I70.248, I70.249, I70.25, I70.261, I70.262, I70.263, I70.268, I70.269, I70.291, I70.292, I70.293, I70.298, I70.299, I70.92, I74.0, I74.10, I74.11, I74.19, I74.2, I74.3, I74.4, I74.5, I74.8, I74.9, I75.011, I75.012, I75.013, I75.019, I75.021, I75.022, I75.023, I75.029, I75.81, I75.89 SNOMED , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , 201
202 , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , To chart the CABG or PCI, enter a procedure code or a procedure code that is associated with a qualifying SNOMED code. You may enter the procedure in either the SP or the SO tab of Full Note Composer or other clinical note type window. Coronary Artery Bypass Graft HCPCS S2205, S2206, S2207, S2208, S2209 CPT 33510, 33511, 33512, 33513, 33514, 33516, 33517, 33518, 33519, 33521, 33522, 33523, 33533, 33534, 33535, SNOMED , , , , , , , , , , , , , , , 202
203 , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , Percutaneous Coronary Interventions HCPCS G0290 CPT 33140, 92980, 92982, SNOMED , , , , , , , , , , , , , , , , , , ENTERING NUMERATOR DATA Patients who have documentation of use of aspirin or another antithrombotic during the measurement period. To report the aspirin or other antithrombotic therapy, write the prescription through the SIG Writer window or prescription refill message and print the prescription or send it electronically. 203
204 CMS 165; NQF 0018; PQRS 236 CONTROLLING HIGH BLOOD PRESSURE DOMAIN Clinical Processes and Effectiveness MEASURE Percentage of patients 18 through 85 years of age who had a diagnosis of hypertension and whose blood pressure was adequately controlled (<140/90mmHg) during the measurement period. EXCLUSIONS OR EXCEPTIONS Patients with evidence of end stage renal disease (ESRD), dialysis or renal transplant before or during the measurement period. Also exclude patients with a diagnosis of pregnancy during the measurement period. ENTERING DENOMINATOR DATA The patient must be between 18 and 85 years old. The patient must have had a diagnosis of essential hypertension at any time prior to the measurement period or be given this diagnosis within the first six months of the measurement period. You may enter the diagnosis in the Dx tab of Full Note Composer or another clinical note type window, or in the Problem/Diagnosis category in the Hx tab of Full Note Composer or in the Patient History window. ICD , 401.1, ICD-10 I10 SNOMED , , , , , , , , , , , , , ,
205 ENTERING NUMERATOR DATA To report on this measure, enter the patient s blood pressure (both systolic and diastolic values) in the Vitals tab of Full Note Composer. These observation items for these blood pressure fields are associated with the appropriate LOIN codes. Patients are included in the numerator if the blood pressure entered for the most recent visit in the measurement period exceeds the target blood pressure. 205
206 CMS 166; NQF 0052; PQRS 312 USE OF IMAGING STUDIES FOR LOW BACK PAIN DOMAIN Health Resources MEASURE Percentage of patients 18 through 50 years of age with a diagnosis of low back pain who did not have an imaging study (plain X-ray, MRI, CT scan) within 28 days of the diagnosis. EXCLUSIONS OR EXCEPTIONS Exclude patients with a diagnosis of cancer any time in their history or patients with a diagnosis of recent trauma, IV drug abuse, or neurologic impairment during the 12-month period prior to the outpatient or emergency department visit. Exclude patients with a diagnosis of low back pain within the 180 days prior to the outpatient or emergency department visit. ENTERING DENOMINATOR DATA The patient must be between 18 and 50 years old. The patient must be given a diagnosis of low back pain during an outpatient or emergency department visit. This visit must occur prior to the last 28 days of the measurement period (that is, within the first 337 days of the measurement period). You must diagnosis the patient with lower back pain using a qualifying ICD-9 or SNOMED code. Enter the diagnosis code in the Dx tab of Full Note Composer or other clinical note type window. ICD , , , , , , , 724.2, 724.3, 724.5, 724.6, , 738.5, 739.3, 739.4, 846.0, 846.1, 846.2, 846.3, 846.8, 846.9,
207 ICD-10 M43.27, M43.28, M46.46, M46.47, M47.26, M47.27, M47.28, M47.816, M47.817, M47.818, M47.896, M47.897, M47.898, M48.06, M48.07, M51.26, M51.27, M51.36, M51.37, M51.46, M51.47, M51.86, M51.87, M53.2X7, M53.2X8, M53.3, M53.86, M53.87, M53.88, M54.30, M54.31, M54.32, M54.40, M54.41, M54.42, M54.5, M54.89, M54.9, M99.03, M99.04, M99.23, M99.33, M99.43, M99.53, M99.63, M99.73, S33.6XXA, S33.8XXA, S33.9XXA SNOMED , , , , , , , , , , , PATIENTS ARE EXCLUDED FROM THE DENOMINATOR OF THIS MEASURE IF THEY HAVE A diagnosis of cancer any time in their history, or A diagnosis of trauma, IV drug abuse, or neurologic impairment during the 12-month period prior to the visit in which lower back pain is diagnosed, or A diagnosis of low back pain within the 180 days prior to the visit in which lower back pain is diagnosed. ENTERING NUMERATOR DATA To report on this measure, the patient would not have a CT scan, MRI, or x-ray of the lower spine performed within 28 days of diagnosis of low back pain. To ensure accurate reporting, you must associate the procedure codes for all CT scans, MRIs, x- rays, and other imaging studies of the lower spine with one of the following LOINC codes. LOINC CODES , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , 207
208 , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , ,
209 CMS167; NQF 0088; PQRS 18 DIABETIC RETINOPATHY: DOCUMENTATION OF PRESENCE OR ABSENCE OF MACULAR EDEMA AND LEVEL OF SEVERITY OF RETINOPATHY DOMAIN Clinical Processes and Effectiveness MEASURE Percentage of patients aged 18 years and older with a diagnosis of diabetic retinopathy who had a dilated macular or fundus exam performed which included documentation of the level of severity of retinopathy and the presence or absence of macular edema during one or more office visits within 12 months. EXCLUSIONS OR EXCEPTIONS Documentation of medical reason(s) for not performing a dilated macular or fundus examination. Documentation of patient reason(s) for not performing a dilated macular or fundus examination. ENTERING DENOMINATOR DATA All patients aged 18 years and older with a diagnosis of diabetic retinopathy. ICD , , , , , ICD-10 E08.311, E08.319, E08.321, E08.329, E08.331, E08.339, E08.341, E08.349, E08.351, E08.359, E09.311, E09.319, E09.321, E09.329, E09.331, E09.339, E09.341, E09.349, E09.351, E09.359, E10.311, E10.319, E10.321, E10.329, E10.331, E10.339, E10.341, E10.349, E10.351, E10.359, E11.311, E11.319, E11.321, E11.329, E11.331, E11.339, E11.341, E11.349, E11.351, E11.359, E13.311, E13.319, E13.321, E13.329, E13.331, E13.339, E13.341, E13.349, E13.351, E
210 SNOMED , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , ENTERING NUMERATOR DATA Patients who had a dilated macular or fundus exam performed which included documentation of the level of severity of retinopathy AND the presence or absence of macular edema during one or more office visits within 12-months. To report on this measure, you must order or perform a dilated macular or fundus exam during the measurement period. Then you must document the level of severity of retinopathy and the presence or absence of macular edema as test results. To chart the dilated macular or fundus exam, you must use a procedure code associated with the macula findings LOINC code You may enter the procedure in either the SP or the SO tab of Full Note Composer or other clinical note type window. Macula test results not received through an interface must be entered as discrete, quantifiable data. Enter the results in the Patients Results window using a lab template enabling you to enter the test result value. Results stored in the database as text notes or image file cannot be used for reporting. You can also enter the findings for macula edema and the severity of retinopathy using a procedure code associated with one of the following SNOMED codes. Enter the procedure code in the SP or SO tab of Full Note Composer or other clinical note type window. 210
211 MACULA EDEMA ABSENT SNOMED MACULA EDEMA PRESENT SNOMED , , , , , , , , , , , , , , , , , , , , SEVERITY OF RETINOPATHY SNOMED , , , , , , You may also document the severity of retinopathy and the macular edema findings as two separate items. Here is the code list for these. SNOMED CODES FOR SEVERITY OF RETINOPATHY , , , , , , SNOMED CODES FOR MACULAR EDEMA FINDINGS , , , , , , , , , , , , , , , , , , , , , ,
212 CMS 169; NQF 0110; PQRS 367 BIPOLAR DISORDER AND MAJOR DEPRESSION: APPRAISAL FOR ALCOHOL OR CHEMICAL SUBSTANCE USE DOMAIN Clinical Processes and Effectiveness MEASURE Percentage of patients with depression or bipolar disorder with evidence of an initial assessment that includes an appraisal for alcohol or chemical substance use. EXCLUSIONS OR EXCEPTIONS None ENTERING DENOMINATOR DATA Patients 18 years of age or older at the start of the measurement period. Patients in the Initial Patient Population with a new diagnosis of unipolar depression or bipolar disorder during the first 323 days of the measurement period, and evidence of treatment for unipolar depression or bipolar disorder within 42 days of diagnosis. The existence of a 'new diagnosis' is established by the absence of diagnoses and treatments of unipolar depression or bipolar disorder during the 180 days prior to the diagnosis. Depression or bipolar disorder may be identified by a diagnosis or by procedures for depression counseling or therapy or antidepressant or mood stabilizer medications. Enter the diagnosis with a qualifying diagnosis code or diagnosis code associated with a SNOMED code in the Dx tab of Full Note Composer or other clinical note type window or enter a problem associated with a qualifying SNOMED code in the problem history category in the Hx tab of Full Note Composer or the Patient History window. 212
213 ICD , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , 296.7, , , , , 300.4, , 311 ICD-10 F30.10, F30.11, F30.12, F30.13, F30.2, F30.3, F30.8, F30.9, F31.0, F31.10, F31.11, F31.12, F31.13, F31.2, F31.30, F31.31, F31.32, F31.4, F31.5, F31.60, F31.61, F31.62, F31.63, F31.64, F31.70, F31.71, F31.73, F31.75, F31.77, F31.81, F31.89, F31.9, F34.0, F32.0, F32.1, F32.2, F32.3, F32.4, F32.8, F32.9, F33.0, F33.1, F33.2, F33.3, F33.40, F33.41, F33.8, F33.9, F34.1 SNOMED , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , 213
214 , , , , , , , , , Counseling or therapy for depression is indicated by a qualifying procedure code or procedure code associated with qualifying SNOMED codes entered in either the SP or SO tab of Full Note Composer or other clinical note type window. COUNSELING FOR DEPRESSION SNOMED ELECTROCONVULSIVE THERAPY CPT ELECTROCONVULSIVE THERAPY SNOMED , , , , , , Medication for depression is indicated by a prescription for a qualifying antidepressant or mood stabilizer medication written through the SIG Writer window, and then either printed or submitted electronically. Or, by a qualifying medication in the patient s medication history. ENTERING NUMERATOR DATA Patients in the denominator with evidence of an assessment for alcohol or other substance use following or concurrent with the new diagnosis, and prior to or concurrent with the initiation of treatment for that diagnosis. Note: the endorsed measure calls for the assessment to be performed prior to discussion of the treatment plan with the patient, but the current approach was considered more feasible in an EHR setting. The "Assessment for Alcohol or Other Drug Use" required in the numerator is meant to capture a provider's assessment of the patient's symptoms of substance use. The essence of the measure is to avoid treating the patient for unipolar depression or bipolar disorder without an assessment of their use of alcohol or other drugs. 214
215 Enter the assessment using a procedure code or a procedure code that is associated with a qualifying SNOMED code. Enter the procedure in either the SP tab of Full Note Composer or other clinical note type window. HCPCS H0001, H0049 CPT 99408, SNOMED , , , , , , ,
216 CMS 177; NQF 1365; PQRS 382 CHILD AND ADOLESCENT MAJOR DEPRESSIVE DISORDER: SUICIDE RISK ASSESSMENT DOMAIN Patient Safety MEASURE Percentage of patient visits for those patients aged 6 through 17 years with a diagnosis of major depressive disorder with an assessment for suicide risk. Please note that the numerator and denominator counts on this measure are a count of distinct visits, not of distinct patients. Therefore, on the CQM 2014 report, the denominator and numerator counts on the summary page will not equal the count of patients in the patient list accessed through the hyperlink for the denominator or numerator. EXCLUSIONS OR EXCEPTIONS None ENTERING DENOMINATOR DATA All patient visits for those patients aged 6 through 17 years with a diagnosis of major depressive disorder. Enter the diagnosis with a qualifying diagnosis code or diagnosis code associated with a SNOMED code in the Dx tab of Full Note Composer or other clinical note type window or enter a problem associated with a qualifying SNOMED code in the problem history category in the Hx tab of Full Note Composer or the Patient History window. ICD , , , , , , , , ,
217 ICD-10 F32.0, F32.1, F32.2, F32.3, F32.9, F33.0, F33.1, F33.2, F33.3, F33.9 SNOMED , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , ENTERING NUMERATOR DATA Patient visits with an assessment for suicide risk. To chart the assessment, you must enter a procedure code that is associated with the SNOMED code Enter the procedure in the SP tab of Full Note Composer or other clinical note type window. 217
218 CMS 179; NQF NA; PQRS 380 ADE PREVENTION AND MONITORING: WARFIN AND TIME IN THERAPEUTIC RANGE Please note that Aprima PRM 2015 is not certified for this measure. Therefore, information about this measure is not included in this document. This measure cannot be submitted through Aprima PRM. 218
219 CMS 182; NQF 0075; PQRS 241 ISCHEMIC VASCULAR DISEASE (IVD): COMPLETE LIPID PANEL AND LDL CONTROL DOMAIN Clinical Processes and Effectiveness MEASURE Percentage of patients 18 years of age and older who were discharged alive for acute myocardial infarction (AMI), coronary artery bypass graft (CABG) or percutaneous coronary interventions (PCI) in the 12-months prior to the measurement period, or who had an active diagnosis of ischemic vascular disease (IVD) during the measurement period, and who had a complete lipid profile performed during the measurement period and whose LDL-C was adequately controlled (< 100 mg/dl). EXCLUSIONS OR EXCEPTIONS None ENTERING DENOMINATOR DATA Patients 18 years of age and older with a visit during the measurement period, and an active diagnosis of ischemic vascular disease (IVD) during the measurement period, or who were discharged alive for acute myocardial infarction (AMI), coronary artery bypass graft (CABG) or percutaneous coronary interventions (PCI) in the 12 months prior to the measurement period. THE PATIENT MUST EITHER: Have an active diagnosis of IVD during the measurement period, or Have had PTCA performed between January 1 through November 1 of the year prior to the measurement period and a qualifying visit, or Have an active diagnosis of AMI 12 months before the start and still be active during the measurement period or have had CABG performed within 12 months before the start of the measurement period 219
220 Enter the diagnosis with a qualifying diagnosis code or diagnosis code associated with a SNOMED code in the Dx tab of Full Note Composer or other clinical note type window or enter a problem associated with a qualifying SNOMED code in the problem history category in the Hx tab of Full Note Composer or the Patient History window. Acute Myocardial Infarction ICD , , , , , , , , , ICD-10 I21.01, I21.02, I21.09, I21.11, I21.19, I21.21, I21.29, I21.3, I21.4 SNOMED , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , Ischemic Vascular Disease ICD , 411.1, , , 413.0, 413.1, 413.9, , , , , , , , , 414.2, 414.8, 414.9, 429.2, , , , , , , , , , , , , , , , , , , 440.1, , , , , , , 440.4, 444.0, 444.1, , , , , 444.9, , , ICD-10 I20.0, I20.1, I20.8, I20.9, I24.0, I24.1, I24.8, I24.9, I25.10, I25.110, I25.111, I25.118, I25.119, I25.5, I25.6, I25.700, I25.701, I25.708, I25.709, I25.710, I25.711, I25.718, I25.719, I25.720, I25.721, I25.728, I25.729, I25.730, I25.731, I25.738, I25.739, I25.750, I25.751, I25.758, I25.759, 220
221 I25.760, I25.761, I25.768, I25.769, I25.790, I25.791, I25.798, I25.799, I25.810, I25.811, I25.812, I25.82, I25.89, I25.9, I63.00, I63.011, I63.012, I63.019, I63.02, I63.031, I63.032, I63.039, I63.09, I63.10, I63.111, I63.112, I63.119, I63.12, I63.131, I63.132, I63.139, I63.19, I63.20, I63.211, I63.212, I63.219, I63.22, I63.231, I63.232, I63.239, I63.29, I63.30, I63.311, I63.312, I63.319, I63.321, I63.322, I63.329, I63.331, I63.332, I63.339, I63.341, I63.342, I63.349, I63.39, I63.40, I63.411, I63.412, I63.419, I63.421, I63.422, I63.429, I63.431, I63.432, I63.439, I63.441, I63.442, I63.449, I63.49, I63.50, I63.511, I63.512, I63.519, I63.521, I63.522, I63.529, I63.531, I63.532, I63.539, I63.541, I63.542, I63.549, I63.59, I63.6, I63.8, I63.9, I65.01, I65.02, I65.03, I65.09, I65.1, I65.21, I65.22, I65.23, I65.29, I65.8, I65.9, I66.01, I66.02, I66.03, I66.09, I66.11, I66.12, I66.13, I66.19, I66.21, I66.22, I66.23, I66.29, I66.3, I66.8, I66.9, I70.1, I70.201, I70.202, I70.203, I70.208, I70.209, I70.211, I70.212, I70.213, I70.218, I70.219, I70.221, I70.222, I70.223, I70.228, I70.229, I70.231, I70.232, I70.233, I70.234, I70.235, I70.238, I70.239, I70.241, I70.242, I70.243, I70.244, I70.245, I70.248, I70.249, I70.25, I70.261, I70.262, I70.263, I70.268, I70.269, I70.291, I70.292, I70.293, I70.298, I70.299, I70.92, I74.0, I74.10, I74.11, I74.19, I74.2, I74.3, I74.4, I74.5, I74.8, I74.9, I75.011, I75.012, I75.013, I75.019, I75.021, I75.022, I75.023, I75.029, I75.81, I75.89 SNOMED , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , 221
222 , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , To chart the CABG or PCI, enter a procedure code or a procedure code that is associated with a qualifying SNOMED code. You may enter the procedure in either the SP or the SO tab of Full Note Composer or other clinical note type window. Coronary Artery Bypass Graft HCPCS S2205, S2206, S2207, S2208, S2209 CPT 33510, 33511, 33512, 33513, 33514, 33516, 33517, 33518, 33519, 33521, 33522, 33523, 33533, 33534, 33535, SNOMED , , , , , , , , , , , , , , , 222
223 , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , Percutaneous Coronary Interventions HCPCS G0290 CPT 33140, 92980, 92982, SNOMED , , , , , , , , , , , , , , , , , , ENTERING NUMERATOR DATA Numerator 1: Patients with a complete lipid profile performed during the measurement period. Numerator 2: Patients whose most recent LDL-C level performed during the measurement period is <100 mg/dl. To report on this measure, you must order or perform an LDL- C test, and then either enter the test results or receive them through an interface and give them a status of Resulted or Approved. Test results not received through an interface must be entered as discrete, quantifiable data. Enter the results in the Patients Results window using a lab template enabling you to enter the test result value. Results stored in the database as text notes or image file cannot be used for reporting. 223
224 You must associate a LOINC code to the test item on each lab template for both manually entered and electronic results. COMPLETE LIPID PROFILE LOINC , TOTAL CHOLESTEROL LOINC HDL-C LOINC LDL-C LOINC , , TRIGLYCERIDES LOINC ,

225 TM 225
EHR Incentive Programs for Eligible Professionals: What You Need to Know for 2015 Tipsheet
 EHR Incentive Programs for Eligible Professionals: What You Need to Know for 2015 Tipsheet CMS recently published a final rule that specifies criteria that eligible professionals (EPs), eligible hospitals,
EHR Incentive Programs for Eligible Professionals: What You Need to Know for 2015 Tipsheet CMS recently published a final rule that specifies criteria that eligible professionals (EPs), eligible hospitals,
Final Meaningful Use Objectives for 2017
 Final Meaningful Use Objectives Stage 3 All Eligible Hospitals (EH) and Critical Access Hospitals (CAH) must attest to all objectives for Stage 3 using a 2015 Edition CEHRT. If it is available, EHs and
Final Meaningful Use Objectives Stage 3 All Eligible Hospitals (EH) and Critical Access Hospitals (CAH) must attest to all objectives for Stage 3 using a 2015 Edition CEHRT. If it is available, EHs and
Final Meaningful Use Objectives for Program Year 2018
 Final Meaningful Use Objectives Modified Stage 2 All Eligible Hospitals (EH) and Critical Access Hospitals (CAH) must attest to all objectives using a 2014 Edition CEHRT. If it is available, EHs and CAHs
Final Meaningful Use Objectives Modified Stage 2 All Eligible Hospitals (EH) and Critical Access Hospitals (CAH) must attest to all objectives using a 2014 Edition CEHRT. If it is available, EHs and CAHs
CMS-3311-P 100 TABLE 6: MEANINGFUL USES OBJECTIVES AND MEASURES FOR 2015 THROUGH 2017
 CMS-3311-P 100 TABLE 6: MEANINGFUL USES OBJECTIVES AND MEASURES FOR 2015 THROUGH 2017 Provider Type Eligible Professional Proposed Objectives for 2015, 2016 and 2017 CPOE Prescribing Clinical Decision
CMS-3311-P 100 TABLE 6: MEANINGFUL USES OBJECTIVES AND MEASURES FOR 2015 THROUGH 2017 Provider Type Eligible Professional Proposed Objectives for 2015, 2016 and 2017 CPOE Prescribing Clinical Decision
Final Meaningful Use Objectives for 2016
 Final Meaningful Use Objectives Modified Stage 2 All Eligible Hospitals (EH) and Critical Access Hospitals (CAH) must attest to all objectives using a 2014 Edition CEHRT. Modified Stage 2 Objective Protect
Final Meaningful Use Objectives Modified Stage 2 All Eligible Hospitals (EH) and Critical Access Hospitals (CAH) must attest to all objectives using a 2014 Edition CEHRT. Modified Stage 2 Objective Protect
PCC EHR Meaningful Use Measures. Maria Horn July 18, :15 pm. Including CQM Reports
 PCC EHR Meaningful Use Measures Maria Horn July 18, 2014 2:15 pm Including CQM Reports Meaningful Use and PCC EHR This presentation reviews the measures that are housed in PCC EHR which is 2011 CEHRT (Certified
PCC EHR Meaningful Use Measures Maria Horn July 18, 2014 2:15 pm Including CQM Reports Meaningful Use and PCC EHR This presentation reviews the measures that are housed in PCC EHR which is 2011 CEHRT (Certified
Final Meaningful Use Objectives for 2017
 Final Meaningful Use Objectives Modified Stage 2 All Eligible Hospitals (EH) and Critical Access Hospitals (CAH) must attest to all objectives using a 2014 Edition CEHRT. Modified Stage 2 Objective Protect
Final Meaningful Use Objectives Modified Stage 2 All Eligible Hospitals (EH) and Critical Access Hospitals (CAH) must attest to all objectives using a 2014 Edition CEHRT. Modified Stage 2 Objective Protect
Medicare & Medicaid EHR Incentive Programs
 Medicare & Medicaid EHR Incentive Programs Stage 2 NPRM Overview Robert Anthony March 6, 2012 Proposed Rule Everything discussed in this presentation is part of a notice of proposed rulemaking (NPRM).
Medicare & Medicaid EHR Incentive Programs Stage 2 NPRM Overview Robert Anthony March 6, 2012 Proposed Rule Everything discussed in this presentation is part of a notice of proposed rulemaking (NPRM).
Allscripts Version 11.2 Enhancements Front Desk and Medical Records Staff
 QUILLEN ETSU PHYSICIANS Allscripts Version 11.2 Enhancements Front Desk and Medical Records Staff Task List The functionality of the Task List tab is the same, but the appearance has been slightly changed.
QUILLEN ETSU PHYSICIANS Allscripts Version 11.2 Enhancements Front Desk and Medical Records Staff Task List The functionality of the Task List tab is the same, but the appearance has been slightly changed.
ProScript User Guide. Pharmacy Access Medicines Manager
 User Guide Pharmacy Access Medicines Manager Version 3.0.0 Release Date 01/03/2014 Last Reviewed 11/04/2014 Author Rx Systems Service Desk (T): 01923 474 600 Service Desk (E): servicedesk@rxsystems.co.uk
User Guide Pharmacy Access Medicines Manager Version 3.0.0 Release Date 01/03/2014 Last Reviewed 11/04/2014 Author Rx Systems Service Desk (T): 01923 474 600 Service Desk (E): servicedesk@rxsystems.co.uk
MIPS: Quality Direct EHR Manual for Aprima Users
 MIPS: Quality Direct EHR Manual for Aprima Users CONTENTS QUALITY INTRODUCTION... 5 CMS 2: SCREENING FOR CLINICAL DEPRESSION AND FOLLOWUP PLAN....6 CMS 22: SCREENING FOR HIGH BLOOD PRESSURE AND FOLLOWUP
MIPS: Quality Direct EHR Manual for Aprima Users CONTENTS QUALITY INTRODUCTION... 5 CMS 2: SCREENING FOR CLINICAL DEPRESSION AND FOLLOWUP PLAN....6 CMS 22: SCREENING FOR HIGH BLOOD PRESSURE AND FOLLOWUP
Practice Director Support
 Table of Contents AOA MORE Enrollment 2 AOA MORE Practice Director Version.2-3 Practice Director Update Instructions. 3-4 AOA Management Setup....5-6 AOA Submission Trial and Production Submission Run
Table of Contents AOA MORE Enrollment 2 AOA MORE Practice Director Version.2-3 Practice Director Update Instructions. 3-4 AOA Management Setup....5-6 AOA Submission Trial and Production Submission Run
Meaningful Use Simple Guide
 Meaningful Use Simple Guide 2011-2012 CORE Measures 1. CPOE for Medication Orders 2. Drug Interaction Checks * 3. Maintain Problem & Diagnosis List 4. eprescribing (erx) escripts 5. Active Medication List
Meaningful Use Simple Guide 2011-2012 CORE Measures 1. CPOE for Medication Orders 2. Drug Interaction Checks * 3. Maintain Problem & Diagnosis List 4. eprescribing (erx) escripts 5. Active Medication List
Electronic Health Records (EHR) HP Provider Relations October 2012
 HP Provider Relations October 2012") Electronic Health Records (EHR) HP Provider Relations October 2012 Agenda Session Objectives Electronic Health Record (EHR) EHR Incentive Program Certified Technology EHR Meaningful Use EHR Incentive Program
Electronic Health Records (EHR) HP Provider Relations October 2012 Agenda Session Objectives Electronic Health Record (EHR) EHR Incentive Program Certified Technology EHR Meaningful Use EHR Incentive Program
PBSI-EHR Off the Charts!
 PBSI-EHR Off the Charts! Enhancement Release 3.2.1 TABLE OF CONTENTS Description of enhancement change Page Encounter 2 Patient Chart 3 Meds/Allergies/Problems 4 Faxing 4 ICD 10 Posting Overview 5 Master
PBSI-EHR Off the Charts! Enhancement Release 3.2.1 TABLE OF CONTENTS Description of enhancement change Page Encounter 2 Patient Chart 3 Meds/Allergies/Problems 4 Faxing 4 ICD 10 Posting Overview 5 Master
Meaningful Use Overview
 Eligibility Providers may be eligible for incentives from either Medicare or Medicaid, but not both. In addition, providers may not be hospital based. Medicare: A Medicare Eligible Professional (EP) is
Eligibility Providers may be eligible for incentives from either Medicare or Medicaid, but not both. In addition, providers may not be hospital based. Medicare: A Medicare Eligible Professional (EP) is
LibreHealth EHR Student Exercises
 LibreHealth EHR Student Exercises 1. Exercises with Test Patients created by students a. Create a new Encounter using the Bronchitis form (template) i. While your patient s chart is open, go to either
LibreHealth EHR Student Exercises 1. Exercises with Test Patients created by students a. Create a new Encounter using the Bronchitis form (template) i. While your patient s chart is open, go to either
The Alabama Regional Extension Center
 The Alabama Regional Extension Center Mission Statement The Alabama Regional Extension Center is part of the Center for Strategic Health Innovation (CSHI) in the College of Medicine at the University of
The Alabama Regional Extension Center Mission Statement The Alabama Regional Extension Center is part of the Center for Strategic Health Innovation (CSHI) in the College of Medicine at the University of
MU - Selection & Configuration of Measures
 MU - Selection & Configuration of Measures Presenter: Christy Erickson October 14, 2011 Objectives Review the 15 Core Measures and highlight some findings from the field Discuss the MU Menu and Clinical
MU - Selection & Configuration of Measures Presenter: Christy Erickson October 14, 2011 Objectives Review the 15 Core Measures and highlight some findings from the field Discuss the MU Menu and Clinical
CHRONIC CARE REPORTS. V 9.0, October eclinicalworks, All rights reserved
 CHRONIC CARE REPORTS V 9.0, October 2011 eclinicalworks, 2011. All rights reserved CONTENTS ABOUT THIS GUIDE 3 Product Documentation 3 Finding the Documents 3 Webinars 3 eclinicalworks Newsletter 4 Getting
CHRONIC CARE REPORTS V 9.0, October 2011 eclinicalworks, 2011. All rights reserved CONTENTS ABOUT THIS GUIDE 3 Product Documentation 3 Finding the Documents 3 Webinars 3 eclinicalworks Newsletter 4 Getting
MedsCheck Reviews. Ontario
 MedsCheck Reviews Ontario Contents Configuration... 1 Configuring Electronic Signatures... 1 Configuring Electronic MedsCheck Reviews... 2 Creating an ODB MedsCheck Consent Record... 3 Electronic MedsCheck
MedsCheck Reviews Ontario Contents Configuration... 1 Configuring Electronic Signatures... 1 Configuring Electronic MedsCheck Reviews... 2 Creating an ODB MedsCheck Consent Record... 3 Electronic MedsCheck
Documenting Patient Immunization. New Brunswick 2018/19
 Documenting Patient Immunization New Brunswick 2018/19 Table of Contents Documenting Patient Immunization New Brunswick...3 Immunization Module Features...4 Configuration...5 Marketing Message Setup...6
Documenting Patient Immunization New Brunswick 2018/19 Table of Contents Documenting Patient Immunization New Brunswick...3 Immunization Module Features...4 Configuration...5 Marketing Message Setup...6
Content Part 2 Users manual... 4
 Content Part 2 Users manual... 4 Introduction. What is Kleos... 4 Case management... 5 Identity management... 9 Document management... 11 Document generation... 15 e-mail management... 15 Installation
Content Part 2 Users manual... 4 Introduction. What is Kleos... 4 Case management... 5 Identity management... 9 Document management... 11 Document generation... 15 e-mail management... 15 Installation
Entering HIV Testing Data into EvaluationWeb
 Entering HIV Testing Data into EvaluationWeb User Guide Luther Consulting, LLC July, 2014/v2.2 All rights reserved. Table of Contents Introduction... 3 Accessing the CTR Form... 4 Overview of the CTR Form...
Entering HIV Testing Data into EvaluationWeb User Guide Luther Consulting, LLC July, 2014/v2.2 All rights reserved. Table of Contents Introduction... 3 Accessing the CTR Form... 4 Overview of the CTR Form...
Documenting Patient Immunization. Ontario 2018/19
 Documenting Patient Immunization Ontario 2018/19 Table of Contents Documenting Patient Immunization Ontario...3 Immunization Module Features...4 Configuration...5 Marketing Message Setup...6 Paper Mode...9
Documenting Patient Immunization Ontario 2018/19 Table of Contents Documenting Patient Immunization Ontario...3 Immunization Module Features...4 Configuration...5 Marketing Message Setup...6 Paper Mode...9
Lessons Learned from Meaningful Use Implementation. Cynthia L. Bero, MPH Partners HealthCare May 19, 2011
 Lessons Learned from Meaningful Use Implementation Cynthia L. Bero, MPH Partners HealthCare May 9, 20 Meaningful Use Plan of Action Learn the HITECH program Certified EHR Technology. Analyze gap between
Lessons Learned from Meaningful Use Implementation Cynthia L. Bero, MPH Partners HealthCare May 9, 20 Meaningful Use Plan of Action Learn the HITECH program Certified EHR Technology. Analyze gap between
CrystalPM - AOA MORE Integration and MIPS (CQM) Tutorial
 Tutorial") CrystalPM - AOA MORE Integration and MIPS (CQM) Tutorial Introduction: This is a full overview of the logic of the Clinical Quality Measures (CQMs) supported by AOA MORE and CrystalPM, as well as examples
CrystalPM - AOA MORE Integration and MIPS (CQM) Tutorial Introduction: This is a full overview of the logic of the Clinical Quality Measures (CQMs) supported by AOA MORE and CrystalPM, as well as examples
Diabetes Management App. Instruction Manual
 Diabetes Management App Instruction Manual Accu-Chek Connect Diabetes Management App Overview The Accu-Chek Connect diabetes management app (hereafter referred to as the app) is designed to help you: Transfer
Diabetes Management App Instruction Manual Accu-Chek Connect Diabetes Management App Overview The Accu-Chek Connect diabetes management app (hereafter referred to as the app) is designed to help you: Transfer
Managing Immunizations
 Managing Immunizations In this chapter: Viewing Immunization Information Entering Immunizations Editing Immunizations Entering a Lead Test Action Editing a Lead Test Action Entering Opt-Out Immunizations
Managing Immunizations In this chapter: Viewing Immunization Information Entering Immunizations Editing Immunizations Entering a Lead Test Action Editing a Lead Test Action Entering Opt-Out Immunizations
Stage 2 Meaningful Use: Core Objectives. James R. Christina, DPM Director Scientific Affairs APMA
 Stage 2 Meaningful Use: Core Objectives James R. Christina, DPM Director Scientific Affairs APMA What Stage Am I In? 2 2 EHR Must Have 2014 ONC Certification Reporting Period for 2014 Stage 2 Requirements
Stage 2 Meaningful Use: Core Objectives James R. Christina, DPM Director Scientific Affairs APMA What Stage Am I In? 2 2 EHR Must Have 2014 ONC Certification Reporting Period for 2014 Stage 2 Requirements
OneTouch Reveal Web Application. User Manual for Healthcare Professionals Instructions for Use
 OneTouch Reveal Web Application User Manual for Healthcare Professionals Instructions for Use Contents 2 Contents Chapter 1: Introduction...4 Product Overview...4 Intended Use...4 System Requirements...
OneTouch Reveal Web Application User Manual for Healthcare Professionals Instructions for Use Contents 2 Contents Chapter 1: Introduction...4 Product Overview...4 Intended Use...4 System Requirements...
Clay Tablet Connector for hybris. User Guide. Version 1.5.0
 Clay Tablet Connector for hybris User Guide Version 1.5.0 August 4, 2016 Copyright Copyright 2005-2016 Clay Tablet Technologies Inc. All rights reserved. All rights reserved. This document and its content
Clay Tablet Connector for hybris User Guide Version 1.5.0 August 4, 2016 Copyright Copyright 2005-2016 Clay Tablet Technologies Inc. All rights reserved. All rights reserved. This document and its content
Costs and Limitations
 Costs and Limitations For Certified Healthcare IT EHR EMR Version 10.0 07/14/2017 Penn Medical Informatics Systems, Inc Costs and Limitations for EyeDoc EMR Version 10.0 Capability and Description 2014
Costs and Limitations For Certified Healthcare IT EHR EMR Version 10.0 07/14/2017 Penn Medical Informatics Systems, Inc Costs and Limitations for EyeDoc EMR Version 10.0 Capability and Description 2014
MIPS Improvement Activities: Building Blocks for Value and Quality Care
 MIPS Improvement Activities: Building Blocks for Value and Quality Care Agenda Basics of MIPS MIPS 2017 The MIPS-Medicaid MU relationship Improvement activities as building blocks Improvement Activity
MIPS Improvement Activities: Building Blocks for Value and Quality Care Agenda Basics of MIPS MIPS 2017 The MIPS-Medicaid MU relationship Improvement activities as building blocks Improvement Activity
BlueBayCT - Warfarin User Guide
 BlueBayCT - Warfarin User Guide December 2012 Help Desk 0845 5211241 Contents Getting Started... 1 Before you start... 1 About this guide... 1 Conventions... 1 Notes... 1 Warfarin Management... 2 New INR/Warfarin
BlueBayCT - Warfarin User Guide December 2012 Help Desk 0845 5211241 Contents Getting Started... 1 Before you start... 1 About this guide... 1 Conventions... 1 Notes... 1 Warfarin Management... 2 New INR/Warfarin
PQRS in TRAKnet 2015 GUIDE TO SUBMIT TING AND REPORTING PQRS IN 2015 THROUGH TRAKNET
 PQRS in TRAKnet 2015 GUIDE TO SUBMITTING AND REPORTING PQRS IN 2015 THROUGH TRAKNET What is PQRS? PQRS is a quality reporting program that uses negative payment adjustments to promote reporting of quality
PQRS in TRAKnet 2015 GUIDE TO SUBMITTING AND REPORTING PQRS IN 2015 THROUGH TRAKNET What is PQRS? PQRS is a quality reporting program that uses negative payment adjustments to promote reporting of quality
Sleep Apnea Therapy Software Clinician Manual
 Sleep Apnea Therapy Software Clinician Manual Page ii Sleep Apnea Therapy Software Clinician Manual Notices Revised Notice Trademark Copyright Sleep Apnea Therapy Software Clinician Manual 103391 Rev A
Sleep Apnea Therapy Software Clinician Manual Page ii Sleep Apnea Therapy Software Clinician Manual Notices Revised Notice Trademark Copyright Sleep Apnea Therapy Software Clinician Manual 103391 Rev A
Disclosure. From the London Times... What Is Meaningful Use? 11/7/2011. Overview. The Road to Meaningful Use and Beyond
 Disclosure The Road to and Beyond A Simple Overview of a Complex Topic I have no relevant financial relationships to disclose. HIT Subcommittee Dr. Charles King II, Chair Dr. Robert Warren Itara Barnes,
Disclosure The Road to and Beyond A Simple Overview of a Complex Topic I have no relevant financial relationships to disclose. HIT Subcommittee Dr. Charles King II, Chair Dr. Robert Warren Itara Barnes,
The Hospital Anxiety and Depression Scale Guidance and Information
 The Hospital Anxiety and Depression Scale Guidance and Information About Testwise Testwise is the powerful online testing platform developed by GL Assessment to host its digital tests. Many of GL Assessment
The Hospital Anxiety and Depression Scale Guidance and Information About Testwise Testwise is the powerful online testing platform developed by GL Assessment to host its digital tests. Many of GL Assessment
GE Healthcare. Delivering the capabilities you need for Stage 2 in the Ambulatory Setting
 GE Healthcare Delivering the capabilities you need for Stage 2 in the Ambulatory Setting March 12, 2013 Topics Certification Criteria Attestation Requirements Functional Measures Clinical Quality Measures
GE Healthcare Delivering the capabilities you need for Stage 2 in the Ambulatory Setting March 12, 2013 Topics Certification Criteria Attestation Requirements Functional Measures Clinical Quality Measures
Dementia Direct Enhanced Service
 Vision 3 Dementia Direct Enhanced Service England Outcomes Manager Copyright INPS Ltd 2015 The Bread Factory, 1A Broughton Street, Battersea, London, SW8 3QJ T: +44 (0) 207 501700 F:+44 (0) 207 5017100
Vision 3 Dementia Direct Enhanced Service England Outcomes Manager Copyright INPS Ltd 2015 The Bread Factory, 1A Broughton Street, Battersea, London, SW8 3QJ T: +44 (0) 207 501700 F:+44 (0) 207 5017100
Meaningful Use Stage 2: ONC Request for Comments. Ivy Baer, Jennifer Faerberg
 Meaningful Use Stage 2: ONC Request for Comments Ivy Baer, ibaer@aamc.org Jennifer Faerberg jfaerberg@aamc.org Stages of Meaningful Use By Payment Year First Payment Year Payment Year 2011 2012 2013 2014
Meaningful Use Stage 2: ONC Request for Comments Ivy Baer, ibaer@aamc.org Jennifer Faerberg jfaerberg@aamc.org Stages of Meaningful Use By Payment Year First Payment Year Payment Year 2011 2012 2013 2014
RESULTS REPORTING MANUAL. Hospital Births Newborn Screening Program June 2016
 RESULTS REPORTING MANUAL Hospital Births Newborn Screening Program June 2016 CONTENTS GETTING STARTED... 1 Summary... 1 Logging In... 1 Access For New Hires... 2 Reporting Parental Refusals... 3 Adding
RESULTS REPORTING MANUAL Hospital Births Newborn Screening Program June 2016 CONTENTS GETTING STARTED... 1 Summary... 1 Logging In... 1 Access For New Hires... 2 Reporting Parental Refusals... 3 Adding
CaseBuilder - Quick Reference Guide
 ADP UNEMPLOYMENT COMPENSATION MANAGEMENT CaseBuilder - Quick Reference Guide After signing into CaseBuilder, the first screen the user will see is called the Dashboard. The user can then navigate to any
ADP UNEMPLOYMENT COMPENSATION MANAGEMENT CaseBuilder - Quick Reference Guide After signing into CaseBuilder, the first screen the user will see is called the Dashboard. The user can then navigate to any
Abstract. Introduction. Providers stand to lose $1.15 billion in CMS reimbursements under MU
 Abstract As of November 1, 2014, only 2% of eligible professionals had attested to Meaningful Use 2 1. This is not good news for the thousands of independent physician practices that rely on Medicare payments:
Abstract As of November 1, 2014, only 2% of eligible professionals had attested to Meaningful Use 2 1. This is not good news for the thousands of independent physician practices that rely on Medicare payments:
Known Issue Summary Topic Found in Version
 Advanced Audit Audit KI90525 Messaging Service Log files in the C:\NextGen\Services\.NGPr od.auditmessaging\logs are generate logs extremely fast. When opening the log files it is filled
Advanced Audit Audit KI90525 Messaging Service Log files in the C:\NextGen\Services\.NGPr od.auditmessaging\logs are generate logs extremely fast. When opening the log files it is filled
DTSS Online Application Suite User Manual. Version 1.2
 DTSS Online Application Suite User Manual Version 1.2 Contents Dental Application Suite... 3 How to install your Sha2 Certificate using Internet Explorer... 3 Claiming... 5 Dental Claim Entry... 5 A1 Dental
DTSS Online Application Suite User Manual Version 1.2 Contents Dental Application Suite... 3 How to install your Sha2 Certificate using Internet Explorer... 3 Claiming... 5 Dental Claim Entry... 5 A1 Dental
Meaningful Use Exam Protocol Stage 1
 Meaningful Use Exam Protocol Stage 1 During the attestation period there are a few steps to be conscious about while recording patient data. This guide will explain what to do on each screen and tab in
Meaningful Use Exam Protocol Stage 1 During the attestation period there are a few steps to be conscious about while recording patient data. This guide will explain what to do on each screen and tab in
Lead the Way with Advanced Care Management. Workbook
 Lead the Way with Advanced Care Management Workbook TPCA Training 10.2018 Section 1: Using i2itracks for Chronic Disease Management Chronic Disease Tracking in 2018 Disease Management Definition A system
Lead the Way with Advanced Care Management Workbook TPCA Training 10.2018 Section 1: Using i2itracks for Chronic Disease Management Chronic Disease Tracking in 2018 Disease Management Definition A system
Lionbridge Connector for Hybris. User Guide
 Lionbridge Connector for Hybris User Guide Version 2.1.0 November 24, 2017 Copyright Copyright 2017 Lionbridge Technologies, Inc. All rights reserved. Published in the USA. March, 2016. Lionbridge and
Lionbridge Connector for Hybris User Guide Version 2.1.0 November 24, 2017 Copyright Copyright 2017 Lionbridge Technologies, Inc. All rights reserved. Published in the USA. March, 2016. Lionbridge and
NH State Medicaid HIT Plan
 INFORMATION ON INTERNAL PROVIDER AUDITING PROCEDURES AND PROCESSES HAVE BEEN REMOVED FROM THIS DOCUMENT. NH State Medicaid HIT Plan June 30 2014 Describes how the New Hampshire Department of Health and
INFORMATION ON INTERNAL PROVIDER AUDITING PROCEDURES AND PROCESSES HAVE BEEN REMOVED FROM THIS DOCUMENT. NH State Medicaid HIT Plan June 30 2014 Describes how the New Hampshire Department of Health and
mehealth for ADHD Parent Manual
 mehealth for ADHD adhd.mehealthom.com mehealth for ADHD Parent Manual al Version 1.0 Revised 11/05/2008 mehealth for ADHD is a team-oriented approach where parents and teachers assist healthcare providers
mehealth for ADHD adhd.mehealthom.com mehealth for ADHD Parent Manual al Version 1.0 Revised 11/05/2008 mehealth for ADHD is a team-oriented approach where parents and teachers assist healthcare providers
Controlled IOP Uncontrolled IOP Diabetes with or without retinopathy
 PQRS Guidelines I. Introduction A. The reporting of these additional codes are used to determine the quality of care a provider gives to patients with certain diseases. B. All PQRS codes including the
PQRS Guidelines I. Introduction A. The reporting of these additional codes are used to determine the quality of care a provider gives to patients with certain diseases. B. All PQRS codes including the
1. Automatically create Flu Shot encounters in AHLTA in 2 mouse clicks. 2. Ensure accurate DX and CPT codes used for every encounter, every time.
 In clinics around the MHS, upwards of 70% of all flu shot workload credit is lost because the encounters are not documented within AHLTA. Let the Immunization KAT s PASBA approved coding engine do the
In clinics around the MHS, upwards of 70% of all flu shot workload credit is lost because the encounters are not documented within AHLTA. Let the Immunization KAT s PASBA approved coding engine do the
SIM HIT Assessment. Table 1: Practice Capacity to Support Data Elements
 SIM HIT Assessment This interactive document allows the Clinical Health Information Technology Advisors (CHITAs) to work with a SIM practice to institute sustainable quality improvement. The SIM HIT Assessment:
SIM HIT Assessment This interactive document allows the Clinical Health Information Technology Advisors (CHITAs) to work with a SIM practice to institute sustainable quality improvement. The SIM HIT Assessment:
Glossary 3189 Report - Discontinued 2007 see Supplemental Vaccine Certification Form
 Glossary 3189 Report - Discontinued 2007 see Supplemental Vaccine Certification Form 3231 Report see Certificate of Immunization ACIP Advisory Committee on Immunization Practices. Along with the Centers
Glossary 3189 Report - Discontinued 2007 see Supplemental Vaccine Certification Form 3231 Report see Certificate of Immunization ACIP Advisory Committee on Immunization Practices. Along with the Centers
EHs and CAHs have the option of attesting or ereporting CQMs in 2015 through 2017
 CMS-3310-FC & CMS-3311-FC: MU Stage 3 Proposed Reporting on Clinical Quality Measures Using Certified EHR Technology Requirements for Eligible Hospitals & Critical Access Hospitals 2015-2018 Key Takeaways
CMS-3310-FC & CMS-3311-FC: MU Stage 3 Proposed Reporting on Clinical Quality Measures Using Certified EHR Technology Requirements for Eligible Hospitals & Critical Access Hospitals 2015-2018 Key Takeaways
MIPS in Jeffrey D. Lehrman, DPM, FASPS, FACFAS, MAPWCA
 MIPS in 2017 Jeffrey D. Lehrman, DPM, FASPS, FACFAS, MAPWCA APMA Coding Committee APMA MACRA Task Force Expert Panelist, Codingline Fellow, American Academy of Podiatric Practice Management Board of Directors,
MIPS in 2017 Jeffrey D. Lehrman, DPM, FASPS, FACFAS, MAPWCA APMA Coding Committee APMA MACRA Task Force Expert Panelist, Codingline Fellow, American Academy of Podiatric Practice Management Board of Directors,
Introduced ICD Changes in Charting... 2
 Table of Contents InSync Product Release Notes January 2014 Introduced ICD-10... 2 Changes in Charting... 2 Configuring ICD-10 at Practice Level... 2 ICD-10 Master List... 3 Practice Favorite List... 4
Table of Contents InSync Product Release Notes January 2014 Introduced ICD-10... 2 Changes in Charting... 2 Configuring ICD-10 at Practice Level... 2 ICD-10 Master List... 3 Practice Favorite List... 4
Creating a reminder for GSK vaccines in Allscripts Professional EHR
 Vaccine reminders Ensure timely and appropriate vaccine orders and administration Keeping track of patient vaccination requirements is an important aspect in the delivery of ongoing patient care. Alerts
Vaccine reminders Ensure timely and appropriate vaccine orders and administration Keeping track of patient vaccination requirements is an important aspect in the delivery of ongoing patient care. Alerts
CMS EHR Incentive Program: Proposed Rules for Stage 2 and Stage 3 Meaningful Use Focus on Eligible Hospitals
 CMS EHR Incentive Program: Proposed Rules for Stage 2 and Stage 3 Meaningful Use Focus on Eligible Hospitals April 28, 2015 Hosted by: Sponsored by: Today s Event Sponsored By One of the nation s largest
CMS EHR Incentive Program: Proposed Rules for Stage 2 and Stage 3 Meaningful Use Focus on Eligible Hospitals April 28, 2015 Hosted by: Sponsored by: Today s Event Sponsored By One of the nation s largest
WEdoc: Therapy Documentation System Basics
 WEdoc: Therapy Documentation System Basics Complete Insurance Verification Request Form (Form may be found on TWG Website) Select Employees Select Payroll Website Enter username and password Select TWG
WEdoc: Therapy Documentation System Basics Complete Insurance Verification Request Form (Form may be found on TWG Website) Select Employees Select Payroll Website Enter username and password Select TWG
Cortex Gateway 2.0. Administrator Guide. September Document Version C
 Cortex Gateway 2.0 Administrator Guide September 2015 Document Version C Version C of the Cortex Gateway 2.0 Administrator Guide had been updated with editing changes. Contents Preface... 1 About Cortex
Cortex Gateway 2.0 Administrator Guide September 2015 Document Version C Version C of the Cortex Gateway 2.0 Administrator Guide had been updated with editing changes. Contents Preface... 1 About Cortex
Diabetes Management Software V1.3 USER S MANUAL
 Diabetes Management Software V1.3 Manufacturer: BIONIME CORPORATION No. 100, Sec. 2, Daqing St., South Dist., Taichung City 40242, Taiwan http: //www.bionime.com E-mail: info@bionime.com Made in Taiwan
Diabetes Management Software V1.3 Manufacturer: BIONIME CORPORATION No. 100, Sec. 2, Daqing St., South Dist., Taichung City 40242, Taiwan http: //www.bionime.com E-mail: info@bionime.com Made in Taiwan
Data Management System (DMS) User Guide
 User Guide") Data Management System (DMS) User Guide Eversense and the Eversense logo are trademarks of Senseonics, Incorporated. Other brands and their products are trademarks or registered trademarks of their respective
Data Management System (DMS) User Guide Eversense and the Eversense logo are trademarks of Senseonics, Incorporated. Other brands and their products are trademarks or registered trademarks of their respective
Creating an alert for GSK vaccines in e-mds EHR
 Immunization Alerts in e-mds Ensure timely and appropriate immunization orders and administration Keeping track of patient vaccination requirements is an important aspect in the delivery of ongoing patient
Immunization Alerts in e-mds Ensure timely and appropriate immunization orders and administration Keeping track of patient vaccination requirements is an important aspect in the delivery of ongoing patient
PedCath IMPACT User s Guide
 PedCath IMPACT User s Guide Contents Overview... 3 IMPACT Overview... 3 PedCath IMPACT Registry Module... 3 More on Work Flow... 4 Case Complete Checkoff... 4 PedCath Cath Report/IMPACT Shared Data...
PedCath IMPACT User s Guide Contents Overview... 3 IMPACT Overview... 3 PedCath IMPACT Registry Module... 3 More on Work Flow... 4 Case Complete Checkoff... 4 PedCath Cath Report/IMPACT Shared Data...
MCIR USER REFERENCE GUIDE: REPORTS
 MCIR USER REFERENCE GUIDE: REPORTS MCIR User Reference Guide: Reports, ver.08.01.2017, Page 1 of 30 Table of Contents: How to Retrieve, Print and Delete MCIR Reports... 4 AFIX... 6 Batch... 6 Inventory...
MCIR USER REFERENCE GUIDE: REPORTS MCIR User Reference Guide: Reports, ver.08.01.2017, Page 1 of 30 Table of Contents: How to Retrieve, Print and Delete MCIR Reports... 4 AFIX... 6 Batch... 6 Inventory...
Marathon ehealth Portal User Guide
 Marathon ehealth Portal User Guide Contents Page 2 Page 3 Getting Started Home Page 4 My Health Record Goals 20 Winooski Falls Way, Suite 400 Summary Winooski, VT 05404 History p 802-857-0400 Screening
Marathon ehealth Portal User Guide Contents Page 2 Page 3 Getting Started Home Page 4 My Health Record Goals 20 Winooski Falls Way, Suite 400 Summary Winooski, VT 05404 History p 802-857-0400 Screening
Corporate Online. Using Term Deposits
 Corporate Online. Using Term Deposits About this Guide About Corporate Online Westpac Corporate Online is an internet-based electronic platform, providing a single point of entry to a suite of online transactional
Corporate Online. Using Term Deposits About this Guide About Corporate Online Westpac Corporate Online is an internet-based electronic platform, providing a single point of entry to a suite of online transactional
OC TOBER 19, Quality Payment Program Overview
 OC TOBER 19, 2 016 Quality Payment Program Overview Quality Payment Program Panel TOM S. LEE, PHD CEO & Founder SA Ignite BETH HOUCK, MBA Vice President, Client Services SA Ignite MATTHEW FUSAN Director,
OC TOBER 19, 2 016 Quality Payment Program Overview Quality Payment Program Panel TOM S. LEE, PHD CEO & Founder SA Ignite BETH HOUCK, MBA Vice President, Client Services SA Ignite MATTHEW FUSAN Director,
MiPCT Dashboard. User Guide RELEA S E Document File Name MiPCT_Dashboard_UG_v20_00.docx. Document Author Kendra Mallon. Created October 9, 2017
 User Guide RELEA S E 20.0 Document File Name MiPCT_Dashboard_UG_v20_00.docx Document Author Kendra Mallon Created October 9, 2017 U S E R G U I D E Copyright 2017 University of Michigan Health System (UMHS).
User Guide RELEA S E 20.0 Document File Name MiPCT_Dashboard_UG_v20_00.docx Document Author Kendra Mallon Created October 9, 2017 U S E R G U I D E Copyright 2017 University of Michigan Health System (UMHS).
Complex just became comfortable.
 Complex just became comfortable. DENTRIX ENTERPRISE Work Well With Others To serve your community, your clinic must work well with others other providers, other clinics, other organizations. To be effective,
Complex just became comfortable. DENTRIX ENTERPRISE Work Well With Others To serve your community, your clinic must work well with others other providers, other clinics, other organizations. To be effective,
NOA 3rd Party Newsletter PQRS EDITION - Page 1 CONTENTS. Traffic Sheet P.3. Flowsheet & Detailed Directions P.11.
 NOA 3rd Party Newsletter - 2016 PQRS EDITION - Page 1 CONTENTS EYE MEASURES Measure #12 :Primary Open-Angle Glaucoma: Optic Nerve Evaluation Traffic Sheet P.2. Flowsheet & Detailed Directions P.8. Measure
NOA 3rd Party Newsletter - 2016 PQRS EDITION - Page 1 CONTENTS EYE MEASURES Measure #12 :Primary Open-Angle Glaucoma: Optic Nerve Evaluation Traffic Sheet P.2. Flowsheet & Detailed Directions P.8. Measure
TMWSuite. DAT Interactive interface
 TMWSuite DAT Interactive interface DAT Interactive interface Using the DAT Interactive interface Using the DAT Interactive interface... 1 Setting up the system to use the DAT Interactive interface... 1
TMWSuite DAT Interactive interface DAT Interactive interface Using the DAT Interactive interface Using the DAT Interactive interface... 1 Setting up the system to use the DAT Interactive interface... 1
Medtech32 Diabetes Get Checked II Advanced Form Release Notes
 Medtech32 Diabetes Get Checked II Advanced Form Release Notes These Release Notes contain important information for all Medtech32 Users. Please ensure that they are circulated amongst all your staff. We
Medtech32 Diabetes Get Checked II Advanced Form Release Notes These Release Notes contain important information for all Medtech32 Users. Please ensure that they are circulated amongst all your staff. We
2017 Wellness Program Guide. East Central College
 2017 Wellness Program Guide East Central College CHC Wellness and East Central College know the importance of a healthy lifestyle. When you live healthy, you live happy. That is why we are partnering together
2017 Wellness Program Guide East Central College CHC Wellness and East Central College know the importance of a healthy lifestyle. When you live healthy, you live happy. That is why we are partnering together
HL7 s Version 2 standards and submission to immunization registries
 HL7 s Version 2 standards and submission to immunization registries Alean Kirnak Cochair HL7 Public Health and Emergency Response Workgroup American Immunization Registry Association Software Partners
HL7 s Version 2 standards and submission to immunization registries Alean Kirnak Cochair HL7 Public Health and Emergency Response Workgroup American Immunization Registry Association Software Partners
2017 Bankmed Personal Health Assessment (PHA) and HIV/AIDS Counselling and Testing (HCT) Provider Manual
 and HIV/AIDS Counselling and Testing (HCT) Provider Manual") 2017 Bankmed Personal Health Assessment (PHA) and HIV/AIDS Counselling and Testing (HCT) Provider Manual Bankmed Personal Health Assessment and HIV/AIDS Counselling and Testing Handbook 2017 The World
2017 Bankmed Personal Health Assessment (PHA) and HIV/AIDS Counselling and Testing (HCT) Provider Manual Bankmed Personal Health Assessment and HIV/AIDS Counselling and Testing Handbook 2017 The World
Instructor Guide to EHR Go
 Instructor Guide to EHR Go Introduction... 1 Quick Facts... 1 Creating your Account... 1 Logging in to EHR Go... 5 Adding Faculty Users to EHR Go... 6 Adding Student Users to EHR Go... 8 Library... 9 Patients
Instructor Guide to EHR Go Introduction... 1 Quick Facts... 1 Creating your Account... 1 Logging in to EHR Go... 5 Adding Faculty Users to EHR Go... 6 Adding Student Users to EHR Go... 8 Library... 9 Patients
Information Management in General Practice
 Information Management in General Practice Using PEN Clinical Audit Tool Training Workbook for General Practice Written by Noel Stewart March 2010 Workbook and Training Course for General Practice Acknowledgments:
Information Management in General Practice Using PEN Clinical Audit Tool Training Workbook for General Practice Written by Noel Stewart March 2010 Workbook and Training Course for General Practice Acknowledgments:
MNSCREEN TRAINING MANUAL Hospital Births Newborn Screening Program October 2015
 MNSCREEN TRAINING MANUAL Hospital Births Newborn Screening Program October 2015 CONTENTS PART 1: GETTING STARTED... 2 Logging In... 2 Access for New Hires... 2 Reporting Refusals... 3 Adding Patient Records...
MNSCREEN TRAINING MANUAL Hospital Births Newborn Screening Program October 2015 CONTENTS PART 1: GETTING STARTED... 2 Logging In... 2 Access for New Hires... 2 Reporting Refusals... 3 Adding Patient Records...
university client training program
 COURSE OFFERINGS university client training program Dear Valued Client, Since our inception in 1997, TSI Healthcare has followed a guiding principle that support and training do not end after implementation.
COURSE OFFERINGS university client training program Dear Valued Client, Since our inception in 1997, TSI Healthcare has followed a guiding principle that support and training do not end after implementation.
Cerner COMPASS ICD-10 Transition Guide
 Cerner COMPASS ICD-10 Transition Guide Dx Assistant Purpose: To educate Seton clinicians regarding workflow changes within Cerner COMPASS subsequent to ICD-10 transition. Scope: Basic modules and functionality
Cerner COMPASS ICD-10 Transition Guide Dx Assistant Purpose: To educate Seton clinicians regarding workflow changes within Cerner COMPASS subsequent to ICD-10 transition. Scope: Basic modules and functionality
Data Management, Data Management PLUS User Guide
 Data Management, Data Management PLUS User Guide Table of Contents Introduction 3 SHOEBOX Data Management and Data Management PLUS (DM+) for Individual Users 4 Portal Login 4 Working With Your Data 5 Manually
Data Management, Data Management PLUS User Guide Table of Contents Introduction 3 SHOEBOX Data Management and Data Management PLUS (DM+) for Individual Users 4 Portal Login 4 Working With Your Data 5 Manually
CHCANYS NYS HCCN ecw Webinar 4
 CHCANYS NYS HCCN ecw Webinar 4 Meaningful Use Data Capture and Configuration Clinical Quality Measures for Stage 1 and 2 August 14, 2014 Stephanie Rose, Project Director Desiree Railine, HIT Implementation
CHCANYS NYS HCCN ecw Webinar 4 Meaningful Use Data Capture and Configuration Clinical Quality Measures for Stage 1 and 2 August 14, 2014 Stephanie Rose, Project Director Desiree Railine, HIT Implementation
SleepImage Website Instructions for Use
 SleepImage Website Instructions for Use Wellness Clinician Account Version 1 MyCardio SleepImage Website Copyright 2017 MyCardio. All rights reserved. Distributed by MyCardio LLC Issued Sept, 2017 Printed
SleepImage Website Instructions for Use Wellness Clinician Account Version 1 MyCardio SleepImage Website Copyright 2017 MyCardio. All rights reserved. Distributed by MyCardio LLC Issued Sept, 2017 Printed
Agile Product Lifecycle Management for Process
 Nutrition Surveillance Management User Guide Release 5.2.1 Part No. E13901-01 September 2008 Copyrights and Trademarks Copyright 1995, 2008, Oracle Corporation and/or its affiliates. All rights reserved.
Nutrition Surveillance Management User Guide Release 5.2.1 Part No. E13901-01 September 2008 Copyrights and Trademarks Copyright 1995, 2008, Oracle Corporation and/or its affiliates. All rights reserved.
LibreHealth EHR Student Exercises
 LibreHealth EHR Student Exercises 1. Exercises with Test Patients created by students a. Create a new Encounter using the Bronchitis form (template) i. While your patient s chart is open, go to either
LibreHealth EHR Student Exercises 1. Exercises with Test Patients created by students a. Create a new Encounter using the Bronchitis form (template) i. While your patient s chart is open, go to either
User Guide Seeing and Managing Patients with AASM SleepTM
 User Guide Seeing and Managing Patients with AASM SleepTM Once you have activated your account with AASM SleepTM, your next step is to begin interacting with and seeing patients. This guide is designed
User Guide Seeing and Managing Patients with AASM SleepTM Once you have activated your account with AASM SleepTM, your next step is to begin interacting with and seeing patients. This guide is designed
Sleep Apnea Therapy Software User Manual
 Sleep Apnea Therapy Software User Manual Page ii Notices Revised Notice Trademark Copyright 103392 Rev B Published February 8, 2013 and supersedes all previous versions. The information contained in this
Sleep Apnea Therapy Software User Manual Page ii Notices Revised Notice Trademark Copyright 103392 Rev B Published February 8, 2013 and supersedes all previous versions. The information contained in this
Medtech Training Guide
 Medtech Training Guide Clinical Audit Tool Copyright Medtech Limited Page 1 of 80 Clinical Audit Tool v4.0 Contents Chapter 1: Getting Started... 3 Logging In... 3 Logging Out... 3 Setting the Preliminary
Medtech Training Guide Clinical Audit Tool Copyright Medtech Limited Page 1 of 80 Clinical Audit Tool v4.0 Contents Chapter 1: Getting Started... 3 Logging In... 3 Logging Out... 3 Setting the Preliminary
Florida Standards Assessments
 Florida Standards Assessments Assessment Viewing Application User Guide 2017 2018 Updated February 9, 2018 Prepared by the American Institutes for Research Florida Department of Education, 2018 Descriptions
Florida Standards Assessments Assessment Viewing Application User Guide 2017 2018 Updated February 9, 2018 Prepared by the American Institutes for Research Florida Department of Education, 2018 Descriptions
The Clinical Information Data Entry Screen is the main screen in the DQCMS application.
 DATA ENTRY Clinical Information The Clinical Information Data Entry Screen is the main screen in the DQCMS application. To enter data, a patient must first be selected from the Patient pull-down list.
DATA ENTRY Clinical Information The Clinical Information Data Entry Screen is the main screen in the DQCMS application. To enter data, a patient must first be selected from the Patient pull-down list.
Certified Health IT Transparency and Disclosure Information 2014 Edition
 Certified Health IT Transparency and Disclosure Information 2014 Edition 2015 Edition Certified Health IT Transparency and Disclosure Information I. Disclaimer This Complete EHR is 2014 Edition compliant
Certified Health IT Transparency and Disclosure Information 2014 Edition 2015 Edition Certified Health IT Transparency and Disclosure Information I. Disclaimer This Complete EHR is 2014 Edition compliant
Updating immunization schedules to reflect GSK vaccines
 in Professional EHR Manually updating immunization schedules in Professional Updating immunization schedules to reflect GSK vaccines E-Prescribing vaccines in Epic EHR The Centers for Disease Control and
in Professional EHR Manually updating immunization schedules in Professional Updating immunization schedules to reflect GSK vaccines E-Prescribing vaccines in Epic EHR The Centers for Disease Control and
USING THE WEBEX Q&A FEATURE
 USING THE WEBEX Q&A FEATURE All lines are placed on mute to block out background noises. However, you can send in questions to the panelists via the Q&A button. Follow the directions below to use the Q&A
USING THE WEBEX Q&A FEATURE All lines are placed on mute to block out background noises. However, you can send in questions to the panelists via the Q&A button. Follow the directions below to use the Q&A
How Immunisations work in Best Practice?
 How Immunisations work in Best Practice? There are a number of areas in Best Practice related to Immunisations:- Recording and updating Immunisation records Searching and Printing Immunisations List Printing
How Immunisations work in Best Practice? There are a number of areas in Best Practice related to Immunisations:- Recording and updating Immunisation records Searching and Printing Immunisations List Printing
POPULATION TRACKER MIDS USER GUIDE
 POPULATION TRACKER MIDS USER GUIDE December 2018 IFU-0003 14 TABLE OF CONTENTS TABLE OF CONTENTS... 1 Intended Use... 1 Warnings... 1 Contraindications... 1 Compatible Browsers... 2 Treatment Plan Templates
POPULATION TRACKER MIDS USER GUIDE December 2018 IFU-0003 14 TABLE OF CONTENTS TABLE OF CONTENTS... 1 Intended Use... 1 Warnings... 1 Contraindications... 1 Compatible Browsers... 2 Treatment Plan Templates