OwlFit Personal Training Packet Thank you for making a commitment to your health and wellness through Personal Training! Our goal is to help educate
|
|
|
- Daisy James
- 5 years ago
- Views:
Transcription


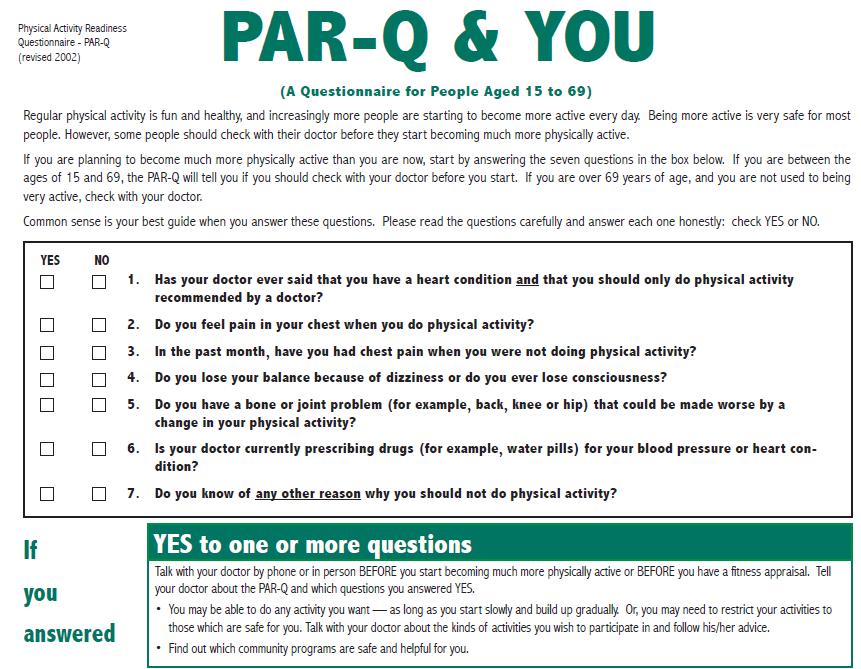
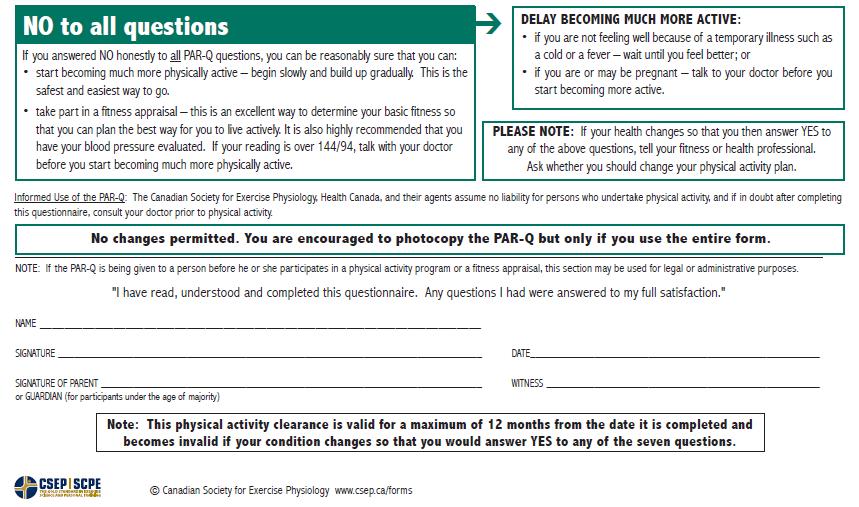
1 OwlFit Personal Training Packet Thank you for making a commitment to your health and wellness through Personal Training! Our goal is to help educate our patrons so that they may exercise safely and effectively for life. Pages 1-3 are for your records. Personal Training Sessions: Getting Started Prior to paying, scheduling, and implementing Personal Training (PT) sessions, patrons must complete this packet and return it to the Administration Office Suites, room 1101, of the Department of Sports and Recreation on the Kennesaw Campus or the Front Desk of the Recreation and Wellness Center on the Marietta Campus. Payment must be paid in cash or check in Administration Office Suites, room 1101, of the Department of Sports and Recreation on the Kennesaw Campus or the Front Desk of the Recreation and Wellness Center on the Marietta Campus. Students will have the option to have their Student Banner Account charged in lieu of cash or check and must complete the proper paperwork if elected. o Students will have 14 days from the time of the charge on their Banner Account to make a payment or a hold will be placed on their account. The packet will undergo an initial screening to ensure medical clearance is not needed, and then payment will be received. You will be contacted within 7 business days regarding your first personal training appointment. If the Personal Training staff determines you need medical clearance, your file will be put on hold for 4 weeks and you will be notified via until you receive medical clearance. Patrons may be required to complete and return a Medical Clearance form if he or she checks Yes to any questions on the PAR-Q Questionnaire or at the discretion of his or her personal trainer. The personal trainer may request a Medical Clearance form if he or she feels it is the best interest for the patron. This form must be completed PRIOR to scheduling or purchasing any training sessions. It is available in the Dept. of Sports and Recreation main office and website. PT packets are located in the Dept. of Sports and Recreation Administration Office Suites on the Kennesaw Campus, the front desk of the Recreation and Wellness Center on the Marietta Campus, or on the website of sportsrec.kennesaw.edu. Patrons must undergo an OwlFit assessment and consultation before beginning the first training session. The assessment will be your first appointment and included in the cost of purchasing a package. These assessments will last 1 and a half to 2 hours. No Refunds will be given except in extreme circumstances. For example: termination of employment, formal leave of absence, changes in medical condition leading to physical limitations. Must provide proper documentation. If in the event a patron schedules PT sessions and it is found that he or she is not eligible for any of the reasons outlined in this packet (for example: patron is a non-member, did not submit the required Medical Clearance, or submitted missing and/or incomplete paperwork), the Personal Trainer will not be able to train with the patron and the sessions will be forfeited. If the patron's eligibility status and/or medical status changes for any reason, it is the responsibility of the patron to notify the Dept. of Sports and Recreation and provide any required supporting documentation in writing 3-5 business days after change. At the end of each semester, incomplete packets will be shredded and discarded. If patrons have not worked with a personal trainer after one year, their packets will be archived. Personal Training is available for both campuses. You must select the Marietta Campus or the Kennesaw Campus in the packet. You will not be able to train at both simultaneously. If for any reason, you wish to change campuses, you must notify the Personal Training Staff at least 7 days prior to the appointment. A patron will be given a personal trainer based on goals and availability. The patron may request a personal trainer. Personal Training Sessions: General Information All KSU affiliates including students, alumni, faculty, and staff are available to register for personal training. In order to participate in the program they must be a valid member of the Department of Sports and Recreation Recreational Facilities. 1
2 In order to receive student pricing, students must be taking the appropriate amount of hours in to which the student recreation fee is paid. It is recommended that patrons schedule at least 1 appointment per week to get the entire benefit of the program. Patrons are expected to bring his or her KSU ID or membership pass to EVERY appointment. Personal Trainers schedule all PT Sessions. The personal trainers will contact the patron as soon as they receive the patrons s packet to schedule the OwlFit Assessment within 7 business days upon packet submission. PT sessions are non-transferable, may not to be traded or given to other clients, and may not be accumulated. Sessions not used after a period of 6 months of purchase, will be forfeited. If partner training is purchased, patrons must train with their partner at every session. Failure of either partner to attend each session will result in the session being docked for both partners. Patrons who purchase individual sessions may not participate in a session with another individual unless approved by the Personal Training Coordinator. A participant may request a specific Personal Trainer, which will be given top priority, unless the personal trainer is no longer available to take clients. If a patron is 15 minutes or less late, the session will only last until the end of the scheduled time. For example, if a session starts at 3:00pm and the patron arrives at 3:15pm the session will only last till 4:00pm. If a patron is more than 15 minutes late, the session will be considered a no show and the Personal Trainer will be under no obligation to train with the patron (see section on changes, cancellations, and no shows). If a patron with remaining sessions loses membership to the Department of Recreational Facilities (i.e. expired, graduation, failure to take classes such as in the summer semester, etc.), they must repurchase a membership to continue sessions or must pay the $10 Daily Guest Pass fee to participate in their session. All information regarding each patron s program and progress will be kept confidential and remain in our client files for 3 years following the cessation of participation in the program. Personal Trainers are required to adhere to HIPAA guidelines (visit for more information) to protect any vital health information given. At the completion of every semester and/or at the cessation of involvement with the PT program, patrons will have the opportunity to provide feedback. When sessions are complete, patrons may purchase additional training packages through the Administration Suites, Office of the Dept. of Sports and Recreation or the Front Desk of the Recreation and Wellness Center on the Marietta Campus. without the need of an OwlFit Assessment, if they have completed the OwlFit Assessment within one year of session purchase. It is recommended that you perform a follow up OwlFit assessment following completion of session s package. This can be registered through the Administration Office suites, room 1101, of the Kennesaw Campus Department of Sports and Recreation Facility or the Front Desk of the Recreation and Wellness Center on the Marietta Campus. Program guidelines are subject to change each semester. When possible, the Dept. of Sports and Recreation will notify existing patrons via and will publicize changes on its website. It is the responsibility of the patrons to become familiar with program changes. Personal Training: Changes, Cancellations, and No Show We understand that occasionally situations arise which warrant the need to make changes and ask that patrons make a good faith attempt to notify the Dept. of Sports and Recreation personal training staff as soon as possible of changes by calling the Personal Training office line at If calling the Personal Training office outside of operating hours or no response is received, please leave a detailed message. Any cancellation received outside of business operating hours will be documented as an 8AM cancellation on the following business day that the office is open. Business operating hours: Monday-Friday, 8AM-5PM. For example, if a patron cancels an appointment at 5PM on a Saturday, the appointment will be documented as received at 8AM on Monday morning. Patrons may file a session forfeit protest form only in those cases of an extreme emergency (ex: Hospitalization). Documentation will be required at the time the protest form is submitted (resubmissions will not be accepted). If an exception is determined, all other penalties will apply. PT session forfeit protest forms are available in the Personal 2
3 Training Office. Protest forms will only be accepted for up to 30 days after the charge has posted to the patron s banner account. The following are considered changes to an appointment (refers to both Training and OwlFit Assessments): o Rescheduling an appointment o Cancellation of an appointment o No show appointments If changing appointments with 24-hour or more notice (including request to reschedule): Patrons will be able to change appointments over 24 hours with no charge. *If all sessions purchased are not used within 6 months they will be forfeited. If changing appointments with less than 24-hour notice (this includes no show appointments): If patron cancels under 24 hours, the session will be docked from the purchased package. If there is an emergency, the client must provide proper documentation. The personal trainers make the final decision to dock sessions, so contact the trainers in a timely manner. Personal Training: OwlFit Assessment Preparation Guide: Wear comfortable shoes, and comfortable, flexible clothing. This can include short sleeve shirts or a tank top. Athletic shorts that gives access to the thigh. Bring planner, so that you are able to schedule further appointments with your Personal Trainer. The patron will undergo different aspects of fitness assessment including: o Blood Pressure/Heart Rate o Height o Weight o Body Fat % o Body Imaging o Muscular Strength and Muscular Endurance o Flexibility o Cardiovascular Endurance Do not eat at least two hours prior to the test. Do not drink caffeine at least four hours prior to the test. Do not drink alcohol at least twelve hours prior to the test. Do not smoke two hours prior to the test. Take all regular medications prescribed. 3
4 4
5 This page is purposely left blank. Please Print Clearly PERSONAL TRAINING REGISTRATION Name: (Last) (First) (MI) Today s Date: / / (Month) (Day) (Year) Date of Birth: / / (Month) (Day) (Year) KSU ID # Male Female Local Address Phone: Apt # City State Zip Have you participated in our personal training program before? Yes No If yes, approximately when was your last appointment? Emergency Contact Name Relation to You Emergency Contact s Phone (primary) Secondary Phone Participation in any activity within the Department of Sports and Recreation facilities is at the sole discretion and judgment of the member and at his or her own risk. I, the undersigned, have received the Personal Training packet, policies and conduct of training sessions and understand there are limitations to my participation as outlined in the Personal Training packet. I, the undersigned, certify that the information I have given in this packet is complete and accurate. I, the undersigned, certify that I understand the changes, cancellation, and no show policy given in this packet. I, the undersigned, certify that I am at least 18 years old and have read and understood the conditions of my participation in this program. Applicant s Signature Date Parent Signature Date (If under 18 years of age) 5
6 Medical/Health History Status
7 Information you provide is personal and confidential. The information will enable us to better understand you and your health and fitness habits, as well as inform you of any potential risks. Please consult your physician before beginning any type of exercise program. NAME ID DATE / / Address: City, State Zip: Phone (H) (W) Date of Birth / / Male Female Physician s Name Phone Fax GENERAL Height ft Weight lbs Any unexplained significant weight loss/gain Within the last 6 months Within the last year No If yes, please explain What was your most recent blood pressure reading? / mm hg date Don t Know MEDICAL DIAGNOSES Have you ever had any of the following? Heart attack YES NO UNSURE Emboli (blood clot) YES NO UNSURE Angina YES NO UNSURE Coronary Artery Disease YES NO UNSURE Asthma YES NO UNSURE Stroke YES NO UNSURE Anemia YES NO UNSURE Cancer YES NO UNSURE Osteoporosis YES NO UNSURE Pulmonary Disease YES NO UNSURE Cardiovascular surgery YES NO UNSURE Heart Valve Problems YES NO UNSURE Currently pregnant YES NO UNSURE Rheumatic Fever YES NO UNSURE Emphysema YES NO UNSURE Allergies YES NO UNSURE Chronic Bronchitis YES NO UNSURE Hernia YES NO UNSURE Diabetes YES NO UNSURE Seizures YES NO UNSURE Phlebitis (inflammation of a vein) YES NO UNSURE YES NO Are you currently being treated for any bone, orthopedic or joint problem that could be aggravated with present physical activity? YES NO Have you been treated for any bone, orthopedic or joint problem that could be aggravated with present physical activity? If yes, how many years ago did this occur? Please list all known allergies Any special conditions not listed above If you answered YES to any of the above medical diagnoses, it is RECOMMENDED that you consult with your physician before beginning your exercise program. MEDICATIONS Please list any medications you are currently taking including but not limited to prescriptions, allergy medications, ergogenic aids, diet supplements, vitamins, minerals, etc. Medication Reason Dosage MAJOR RISK FACTORS 1. Are you a man over age of 45 or a woman over age of 55 who has had a hysterectomy or is postmenopausal?
8 YES NO UNSURE 2. Has your father or brother experienced a heart attack before age 55? Or has your mother or sister experienced a heart attack before the age of 65? YES NO UNSURE If yes, who? 3. Has your doctor ever told you that you might have high blood pressure? YES NO UNSURE 4. Do you have cholesterol above 200 ml/dl? YES NO UNSURE Total cholesterol HDL Date tested Unknown 5. Do you have impaired fasting glucose (pre-diabetes)? YES NO UNSURE If yes, do you take insulin? YES NO What year were you diagnosed? 6. Are you physically inactive (i.e. less than 30 min. of physical activity on at least 3 days per week? YES NO UNSURE 7. Do you currently smoke or have you quit smoking in the last 6 months? YES NO UNSURE I smoke (#) cigarettes per day/week (circle one) for years I smoked (#) cigarettes per day/week (circle one) years ago. If you are a man over the age of 45 or a woman over the age of 55 OR if you answered YES to two (2) or more of the above major risk factors, it is RECOMMENDED that you receive physician s clearance before beginning your exercise program. MAJOR SIGNS/SYMPTOMS SUGGESTIVE OF CARDIOVASCULAR AND PULMONARY DISEASE 1. Pain or discomfort (or angina equivalent) in the chest, neck, jaw, arms, or other areas that may be due to ischemia (decreased blood flow) either at rest or during exercise? YES NO UNSURE 2. Shortness of breath at rest or w/mild exertion YES NO UNSURE 3. Dizziness or syncope at rest or w/mild exertion YES NO UNSURE 4. Orthopnea/paroxysmal nocturnal dyspnea (shortness of breath) at rest or w/mild exertion YES NO UNSURE 5. Edema (excessive accumulation of tissue fluid) YES NO UNSURE 6. Palpitations or tachycardia (sudden rapid heartbeat) YES NO UNSURE 7. Intermittent claudication (lameness due to decreased blood flow) YES NO UNSURE 8. Known heart murmur (abnormal heart sound) YES NO UNSURE 9. Unusual fatigue or shortness of breath with usual activities YES NO UNSURE If you answered, YES to any of the above major signs and symptoms listed above OR have known cardiovascular, pulmonary or metabolic disease (see below), it is STRONGLY RECOMMENDED that you seek physician s clearance before beginning an exercise program. Cardiovascular cardiac, peripheral vascular, cerebrovascular disease Pulmonary chronic obstructive pulmonary disease, asthma, interstitial lung disease, or cystic fibrosis Metabolic Disease diabetes mellitus (types 1 and 2), thyroid disorders, renal or liver disease I understand this Health History Questionnaire has been provided to me for the purpose of helping me better understand any potential risks associated with a workout program. I also understand I should share this information with my physician and seek his or her approval prior to beginning an exercise program. I understand the information I have provided will be maintained in my membership file for use in case of a medical emergency. My signature signifies that all of the above is true, to the best of my knowledge. Any information left unanswered was done so intentionally. If any of the above information changes, I agree to submit these changes in writing to the Personal Training Coordinator for an update to my membership file. I, the undersigned, certify that I am at least 18 years old and have read and understood the conditions of my participation in this program. Signature Date Received by Date (Patron) (Personal Trainer) Parent Signature (if under 18 years of age) Date Note: All major risk factors, signs and symptoms classifications are taken directly from American College of Sports Medicine (ACSM) Guidelines for Exercise Testing and Prescription (Linda S. Pescatell, PhD, FACSM, ed. 2013)
9 Exercise History and Lifestyle Name Date Demographic and Background Information: 1. How did you hear about our Personal Training program? Friend Flier Class Tour Staff Member Other, please specify: 2. Are you participating in our Personal Training program as part of an academic class? [ ] Yes [ ] No If yes, which class? 3. What part of the Personal Training program MOST interests you? 4. Have you participated in another personal training program previously either at another university or exercise facility? [ ] Yes [ ] No If yes, where? 5. What other Department of Sports and Recreation programs interest you? Group Exercise Bike Shop Services/Events Intramural Sports Personal Training Club Sports Becoming a Personal Trainer Special Events Becoming a Group Exercise Instructor Nature Bound Trips/Events Exercise History: 1. Please rank your top 3 fitness goals in order of importance: Most Important: Second Most Important: Third Most Important: 2. Were you a high school and/or college athlete? [ ] Yes [ ] No If yes, please specify 3. In the past 6 months, how often have you been engaged in physical activity? [ ] Regularly 1. (3-4 times / week) [ ] Semi-regular (1 to 2 times/week) [ ] Sporadic (1 to 2 times/month) [ ] None 4. In what other exercise, sports, or recreational activities have you participated? In the past 6 months: In the past few years:
10 5. Are you currently involved in regular cardiorespiratory (aerobic) exercise? [ ] Yes [ ] No If yes, please specify the type of exercise: Days per week: Minutes per day: If no, why did you stop or why do you not exercise currently? 6. Are you currently involved in a regular weight training program? [ ] Yes [ ] No If yes, please specify the type of exercise: Days per week: Minutes per day: If no, why did you stop or why do you not exercise currently? 7. Do you participate in some other physical activity that you would like to acknowledge: YES NO If yes, what is it: How long have you been engaged in this activity: 8. Rate your perception of the exertion of your exercise program (circle the number): (1) Light (2) Fairly Light (3) Somewhat hard (4) Hard 9. Do you have any negative feelings toward, or have you had any bad experiences with, physical activity programs including specific experiences at the Department of Sports and Recreation facilities)? [ ] Yes If yes, please explain [ ] No 10. Do you start exercise programs but then find yourself unable to stick with them? [ ] Yes If yes, please explain [ ] No 11. Have you ever experienced soreness after a workout? [ ] Yes If yes, circle the best description of the experience: a. Pleasurable b. Tolerable c. Never want that again! [ ] No 12. What types of physical activity do you consider fun and/or interest you? (Circle all that apply) Walking Cycling (indoor or outdoor) Stair climbing Jogging Elliptical striding Strength Training Yoga Pilates Cardio Kickboxing Dance-based Aerobics Water-based Aerobics Balance Training Plyometric Training Outdoor Adventures Climbing Swimming Martial Arts Racquet Sports Intramural Sports Other:
11 13. Is there anything specific (activity, equipment, type of training, etc.) that you would like to make sure is included in your exercise program? 14. How much time are you willing to devote to an exercise program outside of your scheduled training sessions? Minutes per day Days per week - General Lifestyle Information On a scale of 1-10 how would you rate your current strength training efforts? Not very good Doing really well On a scale of 1-10, how would you rate your current cardio training efforts? Not very good Doing really well On a scale of 1-10, how would you rate your current sleeping habits? Not very good Doing really well On a scale of 1-10, how would you rate your current dietary habits? Not very good Doing really well On a scale of 1-10, how would you rate your current hydration status? Not very good Doing really well On a scale of 1-10, how would you rate your current stress management abilities? Not very good Doing really well Would you be interested in learning more about a comprehensive nutrition assessment and individualized nutrition consultation? [ ] Yes [ ] No Other: Please describe any other considerations or information your Personal Trainer should be aware of before getting started? (ex. medications, supplements, injuries, exercise or activities you can't/won't perform, effective motivation techniques for you.)
12 Please use this page to fill out your availability Sunday: Monday: Tuesday: Wednesday: Thursday: Friday: Saturday: Please circle which campus you would like to meet with your Personal Trainer: Kennesaw Marietta Please indicate below if you would prefer a specific Personal Trainer. Please indicate below how many days per week you wish to meet with your Personal Trainer.
13 Informed Consent for Personal Training I,, hereby voluntarily give consent to Kennesaw State University s Department of Sports and Recreation Facilities to engage in a fitness program(s). I understand that the personal trainers at the Kennesaw State University Student Recreation and Activities Center may be employees of Kennesaw State University. Participation in a regular program of physical activity has been shown to produce positive changes in a number of organ systems. These changes include but are not limited to increased work capacity, improved cardiovascular efficiency, and increased muscular strength, flexibility, power and endurance. I recognize that exercise carries some risk to the musculoskeletal system (sprains, strains) and the cardiorespiratory system (abnormal blood pressure, fainting, disorders of heart beat, and very rare instances of heart attack, stroke, or death). I understand that every effort will be made to minimize problems by preliminary examination and observation during exercise. I understand that I am responsible for monitoring my own condition throughout exercise, and should any unusual symptoms occur, I will cease my participation and inform the trainer of the symptoms. Unusual symptoms include, but are not limited to; chest discomfort, nausea, difficulty in breathing, and joint or muscle injury. Also, in consideration of being allowed to participate in a fitness program, I agree to assume all risks of such fitness exercise, and hereby release and hold harmless the Board of Regents of the University System of Georgia, Kennesaw State University, KSU Department of Sports and Recreation Facilities, and their employees, supervisors, agents, representatives, or anyone affiliated with the Recreation programs, from any and all health claims, suits, losses, or causes of action for damages, for injury or death, including claims for negligence, arising out of or related to my participation in the fitness program. At any time, I can stop exercising for any reason. If a trainer directs me to a specific exercise and I do not feel comfortable, I feel pain, or any other symptoms undesirable, the exercise will cease. I have read the foregoing carefully and I understand its content. Any questions which may have occurred to me concerning this informed consent have been answered to my satisfaction. I certify that I am at least 18 years old and have read and understood the conditions of my participation in this program. Print Name Signature Date
14 Personal Trainer Use Only Notes Follow up on goals (what, why, when, how) Follow up on experience (what, why, when, how) Follow up on medical questions and injuries as needed (what, why, when, how)
Thanks again, The BodyEvolver team Fitness Technology Partners, LLC bodyevolver.com
 Thank you for downloading this comprehensive client intake package. It is our pleasure to provide this tested document which we know will help your business. A complete on-line version of this intake package
Thank you for downloading this comprehensive client intake package. It is our pleasure to provide this tested document which we know will help your business. A complete on-line version of this intake package
Personal Training Initial Packet
 Personal Training Initial Packet ****Please complete and return to the reception desk at least 2 days prior to your scheduled Fitness Assessment**** Name: D.O.B: Today s Date: Member or Non-member (circle
Personal Training Initial Packet ****Please complete and return to the reception desk at least 2 days prior to your scheduled Fitness Assessment**** Name: D.O.B: Today s Date: Member or Non-member (circle
For New Clients TO BE COMPLETED BY FRONT DESK STAFF. Date received: Payment $ Receipt# Staff Initials: TO BE COMPLETED BY SUPERVISOR
 For New Clients Client s Name: Phone: R#: Email: Age: Sex: M F Trainer Preferred: M F Name: Check all that apply: Individual Packages: **3-16 sessions must be completed in the same semester purchased 3
For New Clients Client s Name: Phone: R#: Email: Age: Sex: M F Trainer Preferred: M F Name: Check all that apply: Individual Packages: **3-16 sessions must be completed in the same semester purchased 3
New Client Reformer Session Packet
 New Client Reformer Session Packet Welcome and thank you for your interest in the Pilates Reformer program with University Recreation. You are taking the first steps towards improved health and wellness.
New Client Reformer Session Packet Welcome and thank you for your interest in the Pilates Reformer program with University Recreation. You are taking the first steps towards improved health and wellness.
Department of Campus Recreation: SouthFit Personal Training
 Steps to sign up Step 1: Choose the personal training package that you would like on page 2. Personal training is only available to members of the USA Student Recreation Center. Step 2: Fill out all pages
Steps to sign up Step 1: Choose the personal training package that you would like on page 2. Personal training is only available to members of the USA Student Recreation Center. Step 2: Fill out all pages
Fitness Training Services Application
 Fitness Training Services Application Thank you for your interest in one of our fitness training services with Boston College Campus Recreation. We are committed to helping Boston College students, faculty,
Fitness Training Services Application Thank you for your interest in one of our fitness training services with Boston College Campus Recreation. We are committed to helping Boston College students, faculty,
Personal Training New Client Schedule Form
 Personal Training New Client Schedule Form (To be completed by Client prior to payment. Packet submission does not guarantee immediate service.) Client Name: UGA ID #: Client Phone: Client E-mail: Returning
Personal Training New Client Schedule Form (To be completed by Client prior to payment. Packet submission does not guarantee immediate service.) Client Name: UGA ID #: Client Phone: Client E-mail: Returning
Personal Training Initial Packet
 Personal Training Initial Packet ****Please complete and return to the reception desk at least 2 days prior to your scheduled Fitness Assessment**** Name: D.O.B: Today s Date: Member or Non-member (circle
Personal Training Initial Packet ****Please complete and return to the reception desk at least 2 days prior to your scheduled Fitness Assessment**** Name: D.O.B: Today s Date: Member or Non-member (circle
Fitness Training Services Application
 Fitness Training Services Application Thank you for your interest in one of our fitness training services with Boston College Campus Recreation. We are committed to helping Boston College students, faculty,
Fitness Training Services Application Thank you for your interest in one of our fitness training services with Boston College Campus Recreation. We are committed to helping Boston College students, faculty,
GEORGE MASON UNIVERSITY PERSONAL TRAINING REGISTRATION FORM NEW CLIENT
 GEORGE MASON UNIVERSITY PERSONAL TRAINING REGISTRATION FORM NEW CLIENT PLEASE PRINT, COMPLETE, AND DELIVER THIS FORM TO THE AQUATIC and FITNESS CENTER, RAC, OR SKYLINE FITNESS FRONT DESK: Ethan Carter
GEORGE MASON UNIVERSITY PERSONAL TRAINING REGISTRATION FORM NEW CLIENT PLEASE PRINT, COMPLETE, AND DELIVER THIS FORM TO THE AQUATIC and FITNESS CENTER, RAC, OR SKYLINE FITNESS FRONT DESK: Ethan Carter
CU Recreation Center
 CU Recreation Center Personal Training Congratulations on your decision to invest in yourself! Our qualified, nationally certified personal trainers will provide you with the right information and right
CU Recreation Center Personal Training Congratulations on your decision to invest in yourself! Our qualified, nationally certified personal trainers will provide you with the right information and right
We look forward to helping you achieve your fitness goals!
 Personal Training Congratulations on your decision to invest in yourself! Our qualified, nationally certified personal trainers will provide you with the right information and right training to help you
Personal Training Congratulations on your decision to invest in yourself! Our qualified, nationally certified personal trainers will provide you with the right information and right training to help you
MEMBER PERSONAL TRAINING PACKET
 Dear YMCA Member, MEMBER PERSONAL TRAINING PACKET Congratulations on the decision to improve your health and well-being and work with one of our nationally certified personal trainers! THIS ENTIRE PACKET
Dear YMCA Member, MEMBER PERSONAL TRAINING PACKET Congratulations on the decision to improve your health and well-being and work with one of our nationally certified personal trainers! THIS ENTIRE PACKET
Personal Training New Client Packet Personal Training/Fit for Hire
 Personal Training New Client Packet Personal Training/Fit for Hire Date / / Name Address City State Zip Phone Number Email Trainer Preference Male Female No Preference **If you would like to work with
Personal Training New Client Packet Personal Training/Fit for Hire Date / / Name Address City State Zip Phone Number Email Trainer Preference Male Female No Preference **If you would like to work with
PERSONAL TRAINING POLICIES
 PERSONAL TRAINING POLICIES SCHEDULING: To schedule your initial session: 1. Complete Interest Form, Health History Questionnaire, and Policies forms and return them to the Fitness Department. 2. Register
PERSONAL TRAINING POLICIES SCHEDULING: To schedule your initial session: 1. Complete Interest Form, Health History Questionnaire, and Policies forms and return them to the Fitness Department. 2. Register
Jumpstart, Fitness Assessment, & Body Composition
 Jumpstart, Fitness Assessment, & Body Composition Waiver, Release and Hold Harmless Agreement In consideration of permission granted by Purdue University allowing me to participate in Personal Training
Jumpstart, Fitness Assessment, & Body Composition Waiver, Release and Hold Harmless Agreement In consideration of permission granted by Purdue University allowing me to participate in Personal Training
Waiver, Release and Hold Harmless Agreement Personal Training Services
 Waiver, Release and Hold Harmless Agreement Personal Training Services I,, the undersigned, affirm that I am participating voluntarily in Personal Training Services. (Print name) I (together with my parent
Waiver, Release and Hold Harmless Agreement Personal Training Services I,, the undersigned, affirm that I am participating voluntarily in Personal Training Services. (Print name) I (together with my parent
PERSONAL TRAINING AT MCGAW YMCA
 PERSONAL TRAINING AT MCGAW YMCA Welcome to personal training at the McGaw YMCA! Our personal trainers look forward to working with you and helping you meet your health and fitness goals! There are a few
PERSONAL TRAINING AT MCGAW YMCA Welcome to personal training at the McGaw YMCA! Our personal trainers look forward to working with you and helping you meet your health and fitness goals! There are a few
Spring 2018 Small Group Training Registration
 Spring 2018 Small Group Training Registration Small Group Training Information Packet General Information Session Dates: Monday, February 19 th - Thursday, April 20 th (8 weeks) Free class demos will be
Spring 2018 Small Group Training Registration Small Group Training Information Packet General Information Session Dates: Monday, February 19 th - Thursday, April 20 th (8 weeks) Free class demos will be
Personal Training Intake Form
 Personal Training Intake Form Name: Date: Cell Phone: Office Phone: E-Mail: USC Affiliation: STUDENT ALUMNI FACULTY/STAFF FACULTY/STAFF SPOUSE Sex: Male Female Age: Trainer preference (if any): How many
Personal Training Intake Form Name: Date: Cell Phone: Office Phone: E-Mail: USC Affiliation: STUDENT ALUMNI FACULTY/STAFF FACULTY/STAFF SPOUSE Sex: Male Female Age: Trainer preference (if any): How many
Personal Training Health Screening Questionnaire
 RC Health and Fitness, LLC. 10350 Ironbridge Road Chester, VA 23831 (804)248-0222 Personal Training Health Screening Questionnaire Personal Information Today s date: Title: O DR. O Mr. O Mrs. O Ms. Name:
RC Health and Fitness, LLC. 10350 Ironbridge Road Chester, VA 23831 (804)248-0222 Personal Training Health Screening Questionnaire Personal Information Today s date: Title: O DR. O Mr. O Mrs. O Ms. Name:
FORMS 1) PAR Q & YOU:
 PAR Q & YOU:") Personal Training New Client Registration Congratulations on taking the first step to healthier and better you! The certified trainers are screened by the Vanderbilt Recreation & Wellness Center (the Rec)
Personal Training New Client Registration Congratulations on taking the first step to healthier and better you! The certified trainers are screened by the Vanderbilt Recreation & Wellness Center (the Rec)
FORMS 1) PAR Q & YOU:
 PAR Q & YOU:") Personal Training New Client Registration Congratulations on taking the first step to healthier and better you! The certified trainers are screened by the Vanderbilt Recreation & Wellness Center (the Rec)
Personal Training New Client Registration Congratulations on taking the first step to healthier and better you! The certified trainers are screened by the Vanderbilt Recreation & Wellness Center (the Rec)
Personal Training Information Packet
 Personal Training Information Packet Dubuque Community YMCA/YWCA 35 North Booth Street Dubuque, Iowa 52001 P 563.556.3371 F 563.556.2728 www.dubuquey.org Dear Member: Congratulations! You have just taken
Personal Training Information Packet Dubuque Community YMCA/YWCA 35 North Booth Street Dubuque, Iowa 52001 P 563.556.3371 F 563.556.2728 www.dubuquey.org Dear Member: Congratulations! You have just taken
Personal Training Registration Packet
 Registration Packet Client name: Sessions Purchased: 3 Sessions 30 Minutes 60 Minutes 5 Sessions 10 Sessions 15 Sessions Purchase Date: General and Healthy History Questionnaire Name: Penn ID: Date of
Registration Packet Client name: Sessions Purchased: 3 Sessions 30 Minutes 60 Minutes 5 Sessions 10 Sessions 15 Sessions Purchase Date: General and Healthy History Questionnaire Name: Penn ID: Date of
For MWC Staff: Personal Information: Emergency Contact:
 Masonic Wellness Center and Pool Member Application 361-5699 or ext. 33783 on campus Personal Information: Name: (Mr., Mrs., Ms.) (First) (Last) (MI) Birth Date: Phone: (H): (W): Address: E-mail Address
Masonic Wellness Center and Pool Member Application 361-5699 or ext. 33783 on campus Personal Information: Name: (Mr., Mrs., Ms.) (First) (Last) (MI) Birth Date: Phone: (H): (W): Address: E-mail Address
Body Structure Medical Fitness Facility 2600 Gribbin Drive 410 Redding Rd Lexington, KY (859) General Information
 General Information") Body Structure Medical Fitness Facility 2600 Gribbin Drive 410 Redding Rd Lexington, KY 40517 (859) 268-8190 General Information Full Name Birth date / / Date / / Social Security # - - Driver s License
Body Structure Medical Fitness Facility 2600 Gribbin Drive 410 Redding Rd Lexington, KY 40517 (859) 268-8190 General Information Full Name Birth date / / Date / / Social Security # - - Driver s License
Complete enrollment packet and schedule a time to meet with Louie Morphew.
 Fitness Intake Packet (Personal Training and Adaptive Fitness Clients) Please follow the step-by-step instructions listed below. If you have any questions or concerns, please e-mail Louie Morphew at Lmorphe1@msudenver.edu.
Fitness Intake Packet (Personal Training and Adaptive Fitness Clients) Please follow the step-by-step instructions listed below. If you have any questions or concerns, please e-mail Louie Morphew at Lmorphe1@msudenver.edu.
Personal Training Program Information and Policies
 Personal Training Program Information and Policies Welcome to the Student Recreation Center s (SRC) Personal Training Program! We are delighted that you chose us as a part of your commitment to health
Personal Training Program Information and Policies Welcome to the Student Recreation Center s (SRC) Personal Training Program! We are delighted that you chose us as a part of your commitment to health
RISK REVIEW & PHYSICIAN APPROVAL FORM
 RISK REVIEW & PHYSICIAN APPROVAL FORM Burke Restorative Neurology Clinic is offering services meant to target community members with neurological impairments. The program is supervised by medical professionals
RISK REVIEW & PHYSICIAN APPROVAL FORM Burke Restorative Neurology Clinic is offering services meant to target community members with neurological impairments. The program is supervised by medical professionals
MEMBERSHIP APPLICATION
 MEMBERSHIP APPLICATION Join Date: Full Pay Draft 20/20 Membership Type: Household One Parent Household Two Adult Household Senior Household Adult Young Adult Youth Senior First Name MI Last Birth Date
MEMBERSHIP APPLICATION Join Date: Full Pay Draft 20/20 Membership Type: Household One Parent Household Two Adult Household Senior Household Adult Young Adult Youth Senior First Name MI Last Birth Date
FITNESS ASSESSMENT & WAIVER
 Nutrition Counseling & Services/ Eat Well, Be Fit! www.eatwellbefit.com FITNESS ASSESSMENT & WAIVER Client Name: Date: Date of Birth: Age: Sex: Address: City: State: Zip: Phone: (Home): ( ) (Work): ( )
Nutrition Counseling & Services/ Eat Well, Be Fit! www.eatwellbefit.com FITNESS ASSESSMENT & WAIVER Client Name: Date: Date of Birth: Age: Sex: Address: City: State: Zip: Phone: (Home): ( ) (Work): ( )
MEDICAL INFORMATION: Physician s Name: Phone #: When was your last physical examination?:
 PERSONAL INFORMATION: HEALTH STATUS QUESTIONNAIRE Name: Phone (hm): (bus): Address: City: State: Zip: Occupation: Male/Female: Age: Height: Weight: Lbs.: Emergency Contact: Phone: Relationship: MEDICAL
PERSONAL INFORMATION: HEALTH STATUS QUESTIONNAIRE Name: Phone (hm): (bus): Address: City: State: Zip: Occupation: Male/Female: Age: Height: Weight: Lbs.: Emergency Contact: Phone: Relationship: MEDICAL
HEALTH/MEDICAL QUESTIONNAIRE PHYSICAL ACTIVITY READINESS QUESTIONNAIRE (PAR-Q)
") WRC Staff Use Only WRC Staff Initials Physician s Clearance received? Yes No N/A Orientation complete? Yes No Health/Medical History form signed? Yes No Assumption of Risk form signed? Yes No PAR-Q signed?
WRC Staff Use Only WRC Staff Initials Physician s Clearance received? Yes No N/A Orientation complete? Yes No Health/Medical History form signed? Yes No Assumption of Risk form signed? Yes No PAR-Q signed?
PERSONAL TRAINING. Welcome. Program policies & procedures
 Welcome PERSONAL TRAINING Welcome and thank you for your interest in personal training at Auburn University. You have taken the first step towards better overall health! We thank you for allowing our Campus
Welcome PERSONAL TRAINING Welcome and thank you for your interest in personal training at Auburn University. You have taken the first step towards better overall health! We thank you for allowing our Campus
Warrior Personal Training Registration Packet
 Warrior Personal Training Registration Packet Information and Policies This is personal training tailored to help you reach your desired fitness level. Your exercise program will be personalized to help
Warrior Personal Training Registration Packet Information and Policies This is personal training tailored to help you reach your desired fitness level. Your exercise program will be personalized to help
Trees Hall. Bellefield Hall
 Classes Begin: Monday, 5/7/2018 Classes End: Friday, 8/10/2018 No Class: Memorial Day: 5/28/2018 & Independence Day: 7/4/2018 Trees Hall Indoor Cycling 4400 Monday / Wednesday 12:00-12:55 PM HFC Indoor
Classes Begin: Monday, 5/7/2018 Classes End: Friday, 8/10/2018 No Class: Memorial Day: 5/28/2018 & Independence Day: 7/4/2018 Trees Hall Indoor Cycling 4400 Monday / Wednesday 12:00-12:55 PM HFC Indoor
Adult Pre Participation Screening and Exercise Prescription Practicum
 Adult Pre Participation Screening and Exercise Prescription Practicum Objectives of this exercise: To administer pre participation screening and risk stratification for clients To write an appropriate
Adult Pre Participation Screening and Exercise Prescription Practicum Objectives of this exercise: To administer pre participation screening and risk stratification for clients To write an appropriate
PERSONAL TRAINING CLIENT INFORMATION PACKAGE
 WEST VANCOUVER COMMUNITY CENTRE PERSONAL TRAINING PERSONAL TRAINING CLIENT INFORMATION PACKAGE At West Vancouver Community Services, our approach to health and fitness is balanced. Being healthy means
WEST VANCOUVER COMMUNITY CENTRE PERSONAL TRAINING PERSONAL TRAINING CLIENT INFORMATION PACKAGE At West Vancouver Community Services, our approach to health and fitness is balanced. Being healthy means
Personal Training Packet
 Personal Training Packet Personal Power Small Group Partner Personal Training Waiver Personal Training Policies All cancellations must be made 24 hours in advance of your appointment time. No-shows and/or
Personal Training Packet Personal Power Small Group Partner Personal Training Waiver Personal Training Policies All cancellations must be made 24 hours in advance of your appointment time. No-shows and/or
The University of Texas Fitness Institute of Texas Health and Fitness Screening Questionnaire. Name Date Sex Date of Birth Address Phone UTEID
 The University of Texas Fitness Institute of Texas Health and Fitness Screening Questionnaire Name Date Sex Date of Birth Address Phone Email UTEID Please answer the following questions to the best of
The University of Texas Fitness Institute of Texas Health and Fitness Screening Questionnaire Name Date Sex Date of Birth Address Phone Email UTEID Please answer the following questions to the best of
Nutrition Solutions, LLC Cancellation Policies
 , LLC Cancellation Policies Thank you for choosing. Our mission is to educate, inspire and guide you to better health and wellness with balanced nutrition. Due to high demand for appointments we ve had
, LLC Cancellation Policies Thank you for choosing. Our mission is to educate, inspire and guide you to better health and wellness with balanced nutrition. Due to high demand for appointments we ve had
Welcome to the CANYON WELLNESS PROGRAM!
 Welcome to the CANYON WELLNESS PROGRAM! This program is designed to allow you to continue/initiate the pursuit of your health/wellness goals. You may have just completed a course of Physical Therapy or
Welcome to the CANYON WELLNESS PROGRAM! This program is designed to allow you to continue/initiate the pursuit of your health/wellness goals. You may have just completed a course of Physical Therapy or
The University of Texas Fitness Institute of Texas Health and Fitness Screening Questionnaire
 The University of Texas Fitness Institute of Texas Health and Fitness Screening Questionnaire ID Please answer the following questions to the best of your knowledge by checking either yes or no. Section
The University of Texas Fitness Institute of Texas Health and Fitness Screening Questionnaire ID Please answer the following questions to the best of your knowledge by checking either yes or no. Section
PAR-Q & LIABILITY WAIVER
 PAR-Q & LIABILITY WAIVER Full name: Address: Post code: Mobile: Home phone: Email address: Date of Birth: Occupation: Emergency contact name: Relationship to you: Emergency contact phone number: Tara Blackaby
PAR-Q & LIABILITY WAIVER Full name: Address: Post code: Mobile: Home phone: Email address: Date of Birth: Occupation: Emergency contact name: Relationship to you: Emergency contact phone number: Tara Blackaby
Colorado Mesa University Campus Rec Services Personal Training Request Packet
 Colorado Mesa University Campus Rec Services Personal Training Request Packet Personal Training Services are a fee-based service available to current CMU students, Faculty & Staff membership holders, as
Colorado Mesa University Campus Rec Services Personal Training Request Packet Personal Training Services are a fee-based service available to current CMU students, Faculty & Staff membership holders, as
Weight training is based on individual needs. Beginning weights are provided. Please bring your mat or towel to lay on the floor.
 BENEFITS OF THE PROGRAM: IMPROVE MUSCLE MASS & STRENGTH REDUCE RISK OF OSTEOPOROSIS & RELATED FRACTURES REDUCE THE RISK FOR DIABETES, HEART DISEASE, DEPRESSION & OBESITY IMPROVE SELF-CONFIDENCE, SLEEP
BENEFITS OF THE PROGRAM: IMPROVE MUSCLE MASS & STRENGTH REDUCE RISK OF OSTEOPOROSIS & RELATED FRACTURES REDUCE THE RISK FOR DIABETES, HEART DISEASE, DEPRESSION & OBESITY IMPROVE SELF-CONFIDENCE, SLEEP
P: F: balance. Some exercise equipment will be used such as treadmills, NuSteps and resistance devices.
 The Burke Rehabilitation Hospital recognizes the need to stay physically fit at all ages and functional levels. The Fit 4 Life After Stroke exercise program provides an exercise setting for people who
The Burke Rehabilitation Hospital recognizes the need to stay physically fit at all ages and functional levels. The Fit 4 Life After Stroke exercise program provides an exercise setting for people who
Training Application for
 STRENGTH Rx REAL TRAINING NO GIMMICKS HARD WORK REAL RESULTS Training Application for STRENGTH Rx Welcome to STRENGTH Rx. We offer Strength & Conditioning training for all athletes looking to improve all
STRENGTH Rx REAL TRAINING NO GIMMICKS HARD WORK REAL RESULTS Training Application for STRENGTH Rx Welcome to STRENGTH Rx. We offer Strength & Conditioning training for all athletes looking to improve all
Personal Training Packet. Please complete and submit to the Fitness Center desk and you will be contacted. YMCA Mission
 HEALTH FITNESS LIFE Personal Training Packet Please complete and submit to the Fitness Center desk and you will be contacted. YMCA Mission To put Christian principles into practice through programs that
HEALTH FITNESS LIFE Personal Training Packet Please complete and submit to the Fitness Center desk and you will be contacted. YMCA Mission To put Christian principles into practice through programs that
Trees Hall. Bellefield Hall. Add a Fitness Center Membership for a small additional price!
 Classes Begin: Tuesday, 9/5/2017 Classes End: Friday, 12/8/2017 No Class: Labor Day: 9/4/2017 & Thanksgiving Break: 11/23-24/2017 Trees Hall Kettle + Conditioning Fitness Kickboxing Fitness Kickboxing
Classes Begin: Tuesday, 9/5/2017 Classes End: Friday, 12/8/2017 No Class: Labor Day: 9/4/2017 & Thanksgiving Break: 11/23-24/2017 Trees Hall Kettle + Conditioning Fitness Kickboxing Fitness Kickboxing
Non-Member Health Screening
 Non-Member Health Screening 1390 Taylor Avenue, Winnipeg, Manitoba, R3M 3V8 Phone: 204-488-8023 / Fax: 204-488-4819 Please select Non-Member type: Adult Guest (with member) Adult Guest (without member)
Non-Member Health Screening 1390 Taylor Avenue, Winnipeg, Manitoba, R3M 3V8 Phone: 204-488-8023 / Fax: 204-488-4819 Please select Non-Member type: Adult Guest (with member) Adult Guest (without member)
P: F: Session Information Sessions are held quarterly, registration is ongoing. Monday, Wednesday 2:00PM 3:00PM
 The Burke Rehabilitation Hospital recognizes the need to stay physically fit at all ages and functional levels. The Fit 4 Life After Stroke exercise program provides an exercise setting for people who
The Burke Rehabilitation Hospital recognizes the need to stay physically fit at all ages and functional levels. The Fit 4 Life After Stroke exercise program provides an exercise setting for people who
Physical Activity Readiness Questionnaire
 page 1 Health/Medical History Questionnaire This information is used solely as an aid and will not be released without your knowledge and consent. Name Date Birth date Address Street City State Zip Phone
page 1 Health/Medical History Questionnaire This information is used solely as an aid and will not be released without your knowledge and consent. Name Date Birth date Address Street City State Zip Phone
The StrongWomen Program
 A National Fitness Program for Women Cooperative Extension Service 1675 C Street, #100 Anchorage, AK 99501 Leslie Shallcross, M.S., R.D., L.D. Associate Professor of Extension 907-786-6300 Name Address
A National Fitness Program for Women Cooperative Extension Service 1675 C Street, #100 Anchorage, AK 99501 Leslie Shallcross, M.S., R.D., L.D. Associate Professor of Extension 907-786-6300 Name Address
The University of Texas at Dallas Department of Recreational Sports Nutritional Guidance Registration Form
 The University of Texas at Dallas Department of Recreational Sports Nutritional Guidance Registration Form Directions: Please, fill out as much information as possible. If you are unsure, leave that question
The University of Texas at Dallas Department of Recreational Sports Nutritional Guidance Registration Form Directions: Please, fill out as much information as possible. If you are unsure, leave that question
P: F:
 Fit 4 Life Exercise Programs provide an exercise setting for people who do not require ongoing physical therapy or occupational therapy. Fit For Life l Strength and Conditioning 1 The Strength and Conditioning
Fit 4 Life Exercise Programs provide an exercise setting for people who do not require ongoing physical therapy or occupational therapy. Fit For Life l Strength and Conditioning 1 The Strength and Conditioning
ADULT PRE-EXERCISE SCREENING TOOL
 ADULT PRE-EXERCISE SCREENING TOOL This screening tool does not provide advice on a particular matter, nor does it substitute for advice from an appropriately qualified medical professional. warranty of
ADULT PRE-EXERCISE SCREENING TOOL This screening tool does not provide advice on a particular matter, nor does it substitute for advice from an appropriately qualified medical professional. warranty of
Name: Phone #: Address: Cell Phone #: Address: I d like to participate in:
 Strong Women and Strong Women Advance Program 12-Week Participant Registration Form January 8-April 2*, 2018 *Good Friday Week Schedule Changes: Strong Classes class will meet Monday (3/26) instead of
Strong Women and Strong Women Advance Program 12-Week Participant Registration Form January 8-April 2*, 2018 *Good Friday Week Schedule Changes: Strong Classes class will meet Monday (3/26) instead of
CARDIOVASCULAR FITNESS CENTER COMMUNITY PROGRAM
 CARDIOVASCULAR FITNESS CENTER COMMUNITY PROGRAM The Community Exercise Program (located on the 1st floor of Mountainside Medical Center) is a medically supervised program for individuals who wish to learn
CARDIOVASCULAR FITNESS CENTER COMMUNITY PROGRAM The Community Exercise Program (located on the 1st floor of Mountainside Medical Center) is a medically supervised program for individuals who wish to learn
Client Contact Information. Training Information
 Client Contact Information Name Address (Street) (City) (State) (Zip) Home Phone ( ) Cell Phone ( ) Work Phone ( ) Email Date of Birth / / Training Information Type Personal Training - $35 Partner Training
Client Contact Information Name Address (Street) (City) (State) (Zip) Home Phone ( ) Cell Phone ( ) Work Phone ( ) Email Date of Birth / / Training Information Type Personal Training - $35 Partner Training
WAIVER AND RELEASE FROM LIABILITY
 COACHING CONTRACT I hereby contract Start-Tri.Com as my personal coach for endurance sports. I agree to pay for coaching services up front at the rate of $255/month for the Tier I package, $165/month for
COACHING CONTRACT I hereby contract Start-Tri.Com as my personal coach for endurance sports. I agree to pay for coaching services up front at the rate of $255/month for the Tier I package, $165/month for
Name: Date: Address: City: State: Zip: Birthday: / /
 PERSONAL TRAINING Name: Date: Address: City: State: Zip: Birthday: / / Sex: Male Female Name of Gym: Occupation: Phone (home): Phone (work): Body Weight: Body Fat: Height: Personal Goals 1. Primary Training
PERSONAL TRAINING Name: Date: Address: City: State: Zip: Birthday: / / Sex: Male Female Name of Gym: Occupation: Phone (home): Phone (work): Body Weight: Body Fat: Height: Personal Goals 1. Primary Training
Welcome to the Healthplex!
 Welcome to the Healthplex! Program Please check program that applies to you. If unsure, please ask our staff. Aftercare Employee Health Pulmonary Rehab Lung Gym Cardiac Rehab Health Improvement Prenatal/Post-Partum
Welcome to the Healthplex! Program Please check program that applies to you. If unsure, please ask our staff. Aftercare Employee Health Pulmonary Rehab Lung Gym Cardiac Rehab Health Improvement Prenatal/Post-Partum
select class BEST VALUE! $85 $90 $55 $60 $40 $45
 Tomahawk Strong Bones Participant Registration Form Mondays and Thursdays January 9 May 25, 2017 Location: United Methodist Church (1104 School Rd, Tomahawk, WI 54487) Our Strong Bones Program follows
Tomahawk Strong Bones Participant Registration Form Mondays and Thursdays January 9 May 25, 2017 Location: United Methodist Church (1104 School Rd, Tomahawk, WI 54487) Our Strong Bones Program follows
The Strong Women Program A National Fitness Program for Women. Join the Strong Women Program Today! Sign up Now! ENROLLMENT IS LIMITED!
 Join the Strong Women Program Today! Sign up Now! ENROLLMENT IS LIMITED! Classes for new participants Friday, October 5 to Friday, January 4, 2013: 8-9 a.m. Monday, Wednesday & Friday Noon 1 p.m. Monday,
Join the Strong Women Program Today! Sign up Now! ENROLLMENT IS LIMITED! Classes for new participants Friday, October 5 to Friday, January 4, 2013: 8-9 a.m. Monday, Wednesday & Friday Noon 1 p.m. Monday,
REQUIREMENTS: PROGRAM INCLUDES: IMPORTANT DATES: CHALLENGE WINNERS: HOW DO I PARTICIPATE IN AUBURN STRONG?
 REQUIREMENTS: Auburn University student, faculty or staff Physician clearance/par Q Completed registration form 3 day food log prior to nutritional assessment Nutritional Assessment Attend @ least 2 semi-private
REQUIREMENTS: Auburn University student, faculty or staff Physician clearance/par Q Completed registration form 3 day food log prior to nutritional assessment Nutritional Assessment Attend @ least 2 semi-private
Client Assessment Readiness Questionnaire
 Client Assessment Readiness Questionnaire The following questions will help determine your level of readiness for change, your motivation towards reaching your goals, and identifying obstacles to your
Client Assessment Readiness Questionnaire The following questions will help determine your level of readiness for change, your motivation towards reaching your goals, and identifying obstacles to your
Lose Dat WEIGHT LOSS/BODY COMPOSITION Challenge
 Lose Dat WEIGHT LOSS/BODY COMPOSITION Challenge is an 8-week program designed to educate all participants on how to lead a healthier lifestyle in every facet of life. This program is designed for men and
Lose Dat WEIGHT LOSS/BODY COMPOSITION Challenge is an 8-week program designed to educate all participants on how to lead a healthier lifestyle in every facet of life. This program is designed for men and
FITNESS CONSULTATION JOURNAL
 FITNESS CONSULTATION JOURNAL 1 Table of Contents Guide to the ProFitness Program 2 Personal Information 3 Pre-Consultation Instructions 3 Personal Fitness Profile / History 4 Medical History 5-6 Injuries
FITNESS CONSULTATION JOURNAL 1 Table of Contents Guide to the ProFitness Program 2 Personal Information 3 Pre-Consultation Instructions 3 Personal Fitness Profile / History 4 Medical History 5-6 Injuries
Participant Summary Information Sheet
 Participant Summary Information Sheet Name: Address: Who was your referral source? (Friend, Doctor, Newspaper, Radio - Please name source) Phone Number: Email Address: Date of Birth: Program Site: Age:
Participant Summary Information Sheet Name: Address: Who was your referral source? (Friend, Doctor, Newspaper, Radio - Please name source) Phone Number: Email Address: Date of Birth: Program Site: Age:
Therapeutic Pilates- Intake Form
 Therapeutic Pilates- Intake Form Doctor of Physical Therapy National Certified Pilates Method Alliance Pilates Instructor-PhysicalMind Polestar Pilates Practitioner APTA Certified Expert in Exercise for
Therapeutic Pilates- Intake Form Doctor of Physical Therapy National Certified Pilates Method Alliance Pilates Instructor-PhysicalMind Polestar Pilates Practitioner APTA Certified Expert in Exercise for
New Patient Information
 New Patient Information First Name: Last Name: M.I.: Address: City: State: Zip Code: Mobile Phone: Home Phone: Email: Preferred method of communication: Mobile Phone Home Phone Email Date of Birth: Age:
New Patient Information First Name: Last Name: M.I.: Address: City: State: Zip Code: Mobile Phone: Home Phone: Email: Preferred method of communication: Mobile Phone Home Phone Email Date of Birth: Age:
Personalized Training Request Form
 Personalized Training Request Form Date Name E-mail Member # Birthdate Desired Dates & Times Phone Desired Instructor (staff bios on back) Please note the following: 1. Personalized Training is sold in
Personalized Training Request Form Date Name E-mail Member # Birthdate Desired Dates & Times Phone Desired Instructor (staff bios on back) Please note the following: 1. Personalized Training is sold in
Gym Memberships. The cost of the membership is per month, plus a one off cost of 5 for the band.
 Gym Memberships Membership Form Name: Address: Membership Start Date: Payment Details The cost of the membership is 18.50 per month, plus a one off cost of 5 for the band. This Payment should be made either
Gym Memberships Membership Form Name: Address: Membership Start Date: Payment Details The cost of the membership is 18.50 per month, plus a one off cost of 5 for the band. This Payment should be made either
2017 FIT FOR LIFE: 6 Week Program Stay Fit Through The Holidays Fall 2017: October 30 th December 15 th
 FOR YOUTH DEVELOPMENT FOR HEALTHY LIVING FOR SOCIAL RESPONSIBILITY 2017 FIT FOR LIFE: 6 Week Program Stay Fit Through The Holidays Fall 2017: October 30 th December 15 th Application for Participation
FOR YOUTH DEVELOPMENT FOR HEALTHY LIVING FOR SOCIAL RESPONSIBILITY 2017 FIT FOR LIFE: 6 Week Program Stay Fit Through The Holidays Fall 2017: October 30 th December 15 th Application for Participation
Pedaling for Parkinson s Colorado What is Pedaling for Parkinson s?
 What is Pedaling for Parkinson s? PFP is a non-profit organization focused on improving the quality of life for people with Parkinson s disease. Through a simple innovative exercise program using stationary
What is Pedaling for Parkinson s? PFP is a non-profit organization focused on improving the quality of life for people with Parkinson s disease. Through a simple innovative exercise program using stationary
Join the StrongWomen Program today!
 Join the StrongWomen Program today! Dr. Miriam Nelson, a professor at Tufts University in Boston, Massachusetts, has developed a strength-training program specifically for midlife and older women. The
Join the StrongWomen Program today! Dr. Miriam Nelson, a professor at Tufts University in Boston, Massachusetts, has developed a strength-training program specifically for midlife and older women. The
PATIENT REGISTRATION PERSON TO NOTIFY IN CASE OF EMERGENCY. Name: Relationship: Phone:
 PATIENT REGISTRATION Patient's Name (Last, First, MI): Date Date of Birth: Age: Sex: M / F Social Security Number: Address: Apt. # City: State: Zip: Home Number: Mobile Number: Work Number: PERSON TO NOTIFY
PATIENT REGISTRATION Patient's Name (Last, First, MI): Date Date of Birth: Age: Sex: M / F Social Security Number: Address: Apt. # City: State: Zip: Home Number: Mobile Number: Work Number: PERSON TO NOTIFY
Initial Client Questionnaire
 Initial Client Questionnaire First Name: Middle Initial: Last Name: How did you hear about my services: Medical History Pregnant: Yes No Nursing: Yes No When was your last physical exam? What are your
Initial Client Questionnaire First Name: Middle Initial: Last Name: How did you hear about my services: Medical History Pregnant: Yes No Nursing: Yes No When was your last physical exam? What are your
Lake Psychological Services, LLC
 Lake Psychological Services, LLC Welcome to Lake Psychological Services and thanks for choosing our office for your health care needs. Seeking treatment is not an easy decision and you may have questions
Lake Psychological Services, LLC Welcome to Lake Psychological Services and thanks for choosing our office for your health care needs. Seeking treatment is not an easy decision and you may have questions
Release of Liability. Participant Signature: Participant Name (please print): Signature of Witness:
: Signature of Witness:") Release of Liability In consideration of being allowed to use NextEra Energy Health & Well-Being Fitness Center facilities and equipment, and being allowed to participate in fitness and wellness program
Release of Liability In consideration of being allowed to use NextEra Energy Health & Well-Being Fitness Center facilities and equipment, and being allowed to participate in fitness and wellness program
Fitness Fever Requirements Application Process Upon acceptance into the Fitness Fever program, participants will receive Application Checklist
 Fitness Fever Requirements Able to commit two to three hours a week Complete participant packet Participate in two group workouts a week and participate in one other exercise activity Program cost University
Fitness Fever Requirements Able to commit two to three hours a week Complete participant packet Participate in two group workouts a week and participate in one other exercise activity Program cost University
STRENGTH & CONDITIONING INFORMATION AND PRE-ACTIVITY SCREENING
 STRENGTH & CONDITIONING INFORMATION AND PRE-ACTIVITY SCREENING Please take the time to read through all the information and ensure all relevant forms are completed. The following questionnaire and waivers
STRENGTH & CONDITIONING INFORMATION AND PRE-ACTIVITY SCREENING Please take the time to read through all the information and ensure all relevant forms are completed. The following questionnaire and waivers
STAMPS HEALTH SERVICES Allergy Injection Information
 Allergy Injection Information Phone: (404) 385-4995 Fax: (404) 894-6254 Website: www.health.gatech.edu Hours of Operation: Monday, Tuesday, Wednesday, & Friday 8-3 Thursdays: 9-3 1. All students requesting
Allergy Injection Information Phone: (404) 385-4995 Fax: (404) 894-6254 Website: www.health.gatech.edu Hours of Operation: Monday, Tuesday, Wednesday, & Friday 8-3 Thursdays: 9-3 1. All students requesting
Tidelands HealthPoint Stronger Through Movement Program Participant Information
 Tidelands HealthPoint Stronger Through Movement Program Participant Information Please Print: Name: DOB: First Middle Last Address: Phone: Street City Zip Email Address: Emergency Contact: Phone: First
Tidelands HealthPoint Stronger Through Movement Program Participant Information Please Print: Name: DOB: First Middle Last Address: Phone: Street City Zip Email Address: Emergency Contact: Phone: First
Fitness Guide (316)
") Fitness Guide (316)-978-5278 Getting Started The Heskett Center offers and maintains facilities and programs of the highest quality in order to help its members reach their fitness goals. The staff is
Fitness Guide (316)-978-5278 Getting Started The Heskett Center offers and maintains facilities and programs of the highest quality in order to help its members reach their fitness goals. The staff is
Patient Information Form
 Patient Information Form Patient Name: (Last) (First) (MI) Name you prefer to be called: Mailing address: City: State: Zip: Best daytime phone: May we leave a message there? Yes No Alternate phone number:
Patient Information Form Patient Name: (Last) (First) (MI) Name you prefer to be called: Mailing address: City: State: Zip: Best daytime phone: May we leave a message there? Yes No Alternate phone number:
Runner BOOTCAMP Registration Form
 Runner BOOTCAMP Registration Form Registration for (Enter camp start date): Monday 6:15pm - Wednesdays 7:15pm - Saturday 8:15am (12 sessions) $160 Can come to all sessions for 4 consecutive weeks Payment
Runner BOOTCAMP Registration Form Registration for (Enter camp start date): Monday 6:15pm - Wednesdays 7:15pm - Saturday 8:15am (12 sessions) $160 Can come to all sessions for 4 consecutive weeks Payment
LETTER TO PARTICIPANT. Civilian Employee Wellness Program Participant Marine Corps Community Service Base Henderson Hall
 Dear Participant, MARINE CORPS COMMUNITY SERVICES HENDERSON HALL HEADQUARTERS & SERVICE BATTALION, HEADQUARTERS MARINE CORPS, HENDERSON HALL P.O. BOX 4009, ARLINGTON, VIRGINIA 22204 0009 LETTER TO PARTICIPANT
Dear Participant, MARINE CORPS COMMUNITY SERVICES HENDERSON HALL HEADQUARTERS & SERVICE BATTALION, HEADQUARTERS MARINE CORPS, HENDERSON HALL P.O. BOX 4009, ARLINGTON, VIRGINIA 22204 0009 LETTER TO PARTICIPANT
YWCA LOWER CAPE FEAR 2815 S College Rd Wilmington, NC (910)
") 2815 S College Rd Wilmington, NC 28412 FLOW MOTION REGISTRATION Full Name: APPLICANT INFORMATION Last First M.I. Address: Street Address Apartment/Unit # City State ZIP Code Primary Phone: Email Mobile
2815 S College Rd Wilmington, NC 28412 FLOW MOTION REGISTRATION Full Name: APPLICANT INFORMATION Last First M.I. Address: Street Address Apartment/Unit # City State ZIP Code Primary Phone: Email Mobile
COST One on One.$60.00 per hour One on One..$30.00 per half hour Small Group $40/hour/person. Thank you for your interest in our program.
 Personal Training New Client Registration Congratulations on taking the first step to healthier and better you! The certified trainers are screened by the Vanderbilt Recreation & Wellness Center (the Rec)
Personal Training New Client Registration Congratulations on taking the first step to healthier and better you! The certified trainers are screened by the Vanderbilt Recreation & Wellness Center (the Rec)
PATIENT REGISTRATION PERSON TO NOTIFY IN CASE OF EMERGENCY. Name: Relationship: Phone:
 PATIENT REGISTRATION Patient's Name (Last, First, MI): Date of Birth: Age: Sex: M / F Social Security Number: Address: Apt. # City: State: Zip: Home Number: Mobile Number: Work Number: Employment Status:
PATIENT REGISTRATION Patient's Name (Last, First, MI): Date of Birth: Age: Sex: M / F Social Security Number: Address: Apt. # City: State: Zip: Home Number: Mobile Number: Work Number: Employment Status:
(FIRST) (MIDDLE) (LAST) STREET: CITY: STATE: ZIP CODE:
 (MIDDLE) (LAST) STREET: CITY: STATE: ZIP CODE:") PATIENT INFORMATION EMAIL: MARITAL STATUS: [ ]MARRIED [ ]SINGLE [ ]DIVORCED [ ]WIDOWED NAME: (FIRST) (MIDDLE) (LAST) STREET: CITY: STATE: ZIP CODE: DOB: PHONE: [ ]Home [ ]Work [ ]Cell PHONE: [ ]Home [
PATIENT INFORMATION EMAIL: MARITAL STATUS: [ ]MARRIED [ ]SINGLE [ ]DIVORCED [ ]WIDOWED NAME: (FIRST) (MIDDLE) (LAST) STREET: CITY: STATE: ZIP CODE: DOB: PHONE: [ ]Home [ ]Work [ ]Cell PHONE: [ ]Home [
p e r s o n a l t r a i n i n g NEW CLIENT PACKET
 p e r s o n a l t r a i n i n g NEW CLIENT PACKET GET FIT STAY FIT! The Lodge Des Peres Fitness Center Phone 314.835.6180 - Fax 314.835.6151 www.thelodgedesperes.com Daniel Boyle, Fitness Supervisor ~
p e r s o n a l t r a i n i n g NEW CLIENT PACKET GET FIT STAY FIT! The Lodge Des Peres Fitness Center Phone 314.835.6180 - Fax 314.835.6151 www.thelodgedesperes.com Daniel Boyle, Fitness Supervisor ~
There are a number of subscription types available to suit you and your family with annual fee or direct debit payment options available.
 Dear Prospective Member, Thank you for your enquiry regarding the facilities at Monkton Sports Club. We are delighted to offer members use of the School's outstanding sporting facilities alongside a comprehensive
Dear Prospective Member, Thank you for your enquiry regarding the facilities at Monkton Sports Club. We are delighted to offer members use of the School's outstanding sporting facilities alongside a comprehensive
DeKalb Medical Wellness Center 2665 North Decatur Road, Suite 10 Decatur, Georgia Membership Application
 DeKalb Medical Wellness Center 2665 North Decatur Road, Suite 10 Decatur, Georgia 30033 Membership Application Member #: 2 nd Member #: Welcome! The information you provide below will be entered into our
DeKalb Medical Wellness Center 2665 North Decatur Road, Suite 10 Decatur, Georgia 30033 Membership Application Member #: 2 nd Member #: Welcome! The information you provide below will be entered into our
Release & Waiver Synergy Studio
 Release & Waiver Synergy Studio I,, have enrolled in a program of physical activity, including but not limited to, body conditioning machinery used during the workouts offered by Synergy Studio. I affirm
Release & Waiver Synergy Studio I,, have enrolled in a program of physical activity, including but not limited to, body conditioning machinery used during the workouts offered by Synergy Studio. I affirm
Dr. Janet L. Yarger 510 Baxter Road, Suite 8, Chesterfield, MO
 Registration Form Date: / / Name: Social Security #: - - Address: City: State: Zip Code: Home Phone #: ( ) - Age: Date of Birth / / Cell Phone #: ( ) - Best Phone to call you at: HOME/CELL/WORK Email Address:
Registration Form Date: / / Name: Social Security #: - - Address: City: State: Zip Code: Home Phone #: ( ) - Age: Date of Birth / / Cell Phone #: ( ) - Best Phone to call you at: HOME/CELL/WORK Email Address: