Rehabilitation Considerations Following Surgical Arthroscopy of the Hip. Joy Anderson PT, ATC, CSCS
|
|
|
- Madeline Park
- 5 years ago
- Views:
Transcription
1 Rehabilitation Considerations Following Surgical Arthroscopy of the Hip Joy Anderson PT, ATC, CSCS


2 1 Best Rehab Program?
3 Review of the Evidence paucity of evidence surrounding post-operative rehabilitation after hip arthroscopy thus the superiority of a particular approach cannot be determined Post-Operative Rehabilitation after Hip Arthroscopy: A Search for the Evidence. J Sport Rehabil, 2014,Cheatham et al The current literature of hip arthroscopy rehabilitation lacks high-quality evidence to support a specific protocol Rehabilitation Following Hip Arthroscopy - A Systematic Review. Front Surg, 2015 May, Grzybowski et al,

4 Theory, Evidence, Experience
5 Three Main Phases Phase 1: Healing and Protection Set up for Success Phase 2: Functional Restoration Progressive restoration of ROM, Strength, MM control Phase 3: Return to Sport/Activity Progressive sport specific endurance, skill training,
6 Phase 1: 0 to 4-6 weeks Optimize Healing/Protect Repair Goals: Reduce inflammation Maintain muscle activation Prevent adhesions and scarring Time Based Progression

7 Phase 1: Healing and Protection Post-op ROM Restrictions Limit ER and Extension to 0 deg for 4-6 weeks to allow capsule repair to heal Limit Flexion to 90 deg for 4-6 weeks following a labrum repair to avoid irritating the repair CPM? Hip Brace? Anti-ER Boots?
8 Motion and Mobility Immediate goal is to prevent postoperative joint stiffness and avoid potential postoperative intra-articular adhesions Bike: Start 5-10 min progressing to 30 min -easy spin no resistance -stay upright, -spin with minimal resistance. -upright posture -avoid recumbent Assisted PROM: -Circumduction, -ABD to 45 deg, -IR Log Roll -Painfree Flexion to 90 deg Self Pendulums Quadriped Rocking
9 Weight Bearing TTWB x 2 weeks for FAI/repair NWB x 4-6 weeks for microfracture or hip dysplasia Foot flat gait with crutches



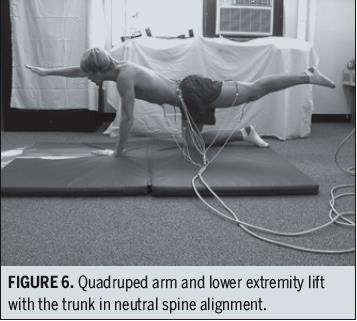
10 Muscle Activation/Strength Isometrics for first 2-3 weeks: -quads, glutes, Hams, abds Calf pumps Avoid active hip flexion/slr to avoid iliopsoas and capsular irritation Progress to isotonics as tolerated: -ER to neutral in supine -bridge to neutral -prone hip ext off table to neutral -Crunches, pelvic tilts, bird dogs
11 Considerations/Complications During Phase 1 Dysplasia Microfracture Capsular Repair Postoperative adhesions Follow protocol, and surgery specific MD instructions!!
12 Phase 2: Functional Restoration Goals of this Phase: Regain functional ROM Normalize muscle activation, strength, and endurance Normalize gait Address soft tissue restrictions Criteria Based Progressions
13 Challenges Encountered Muscle Inhibition Compensatory movements Muscle spasm/trigger point pain Difficulty restoring full ROM Decreased tolerance to prolonged standing & walking

14 Progressive Not Aggressive

15 Muscle and Soft Tissue
16 Interdependent Muscles That Cross the Hip Muscles That Connect the Trunk to the Pelvis Muscles of the Pelvic Floor Rectus femoris Sartorius Gracillis TFL Adductor Longus Adductor Magnus Adductor Brevis Pectineus Iliacus Psoas Gluteus Medius Gluteus Minimus Gluteus Maximus Piriformis Obterator Int/Ext Gemellis Inf/Sup Semi-membranosis Semi-tentinosis Bicep Femoris Rectus Abdominus Internal Oblique External Oblique Quadratus Lumborum Erector Spinae Latissimus Dorsi Grand Total: Hip Pelvis= 25 x2=50 (+PF) Knee= 12 A lot of them Muscles That Cross the Knee Gracillis Sartorius Quadratus x4 Hamstring x3 Popliteus Gastrocnemius Plantaris

17 Restricted: Soft Tissue: TFL, Ant/Lat Quads, Adductors Inhibited: Gluteus Medius Gluteus Maximus Facilitated: TFL Adductors Quads Core: Controls the acetabulum by controlling pelvis position Transfers force from the lower extremities
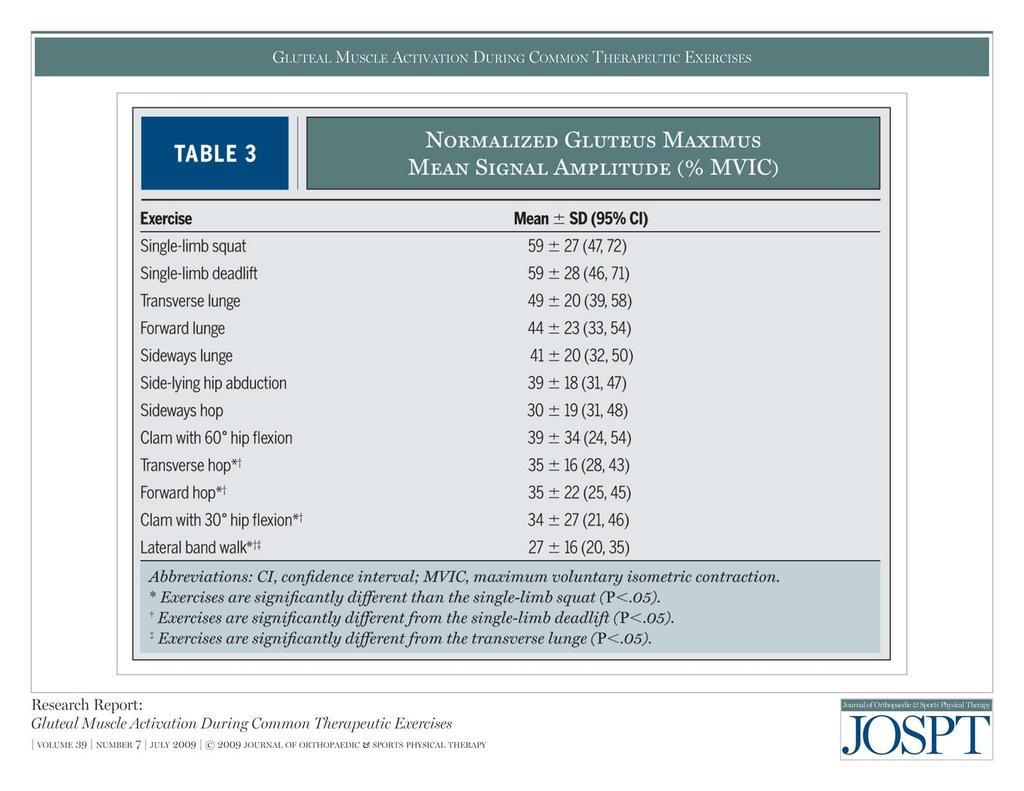
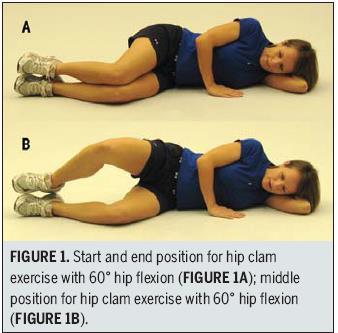
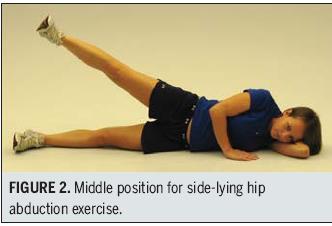
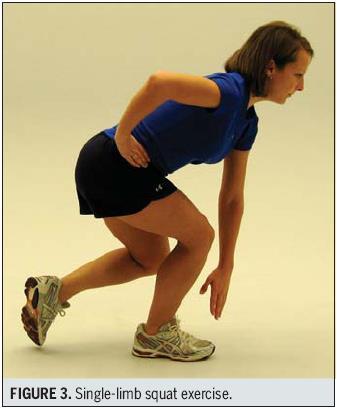
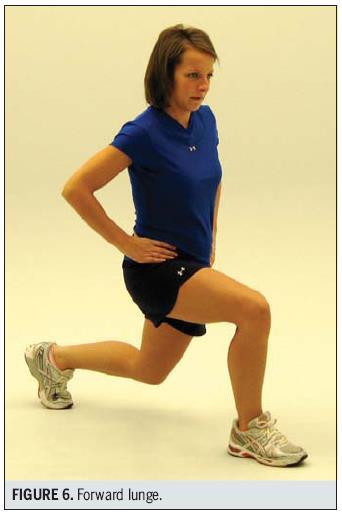
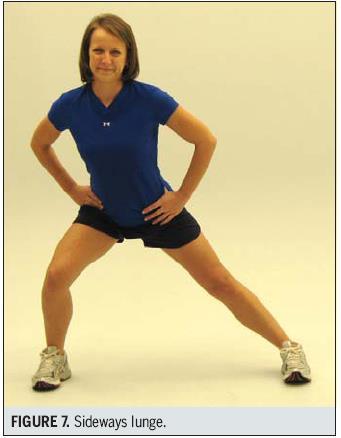
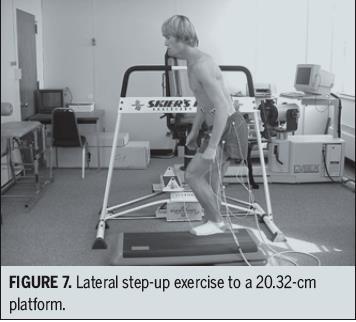
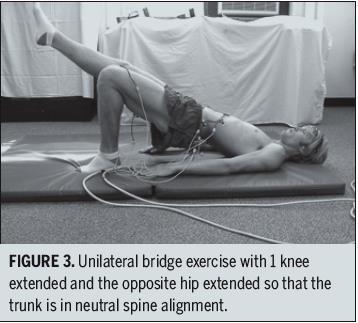
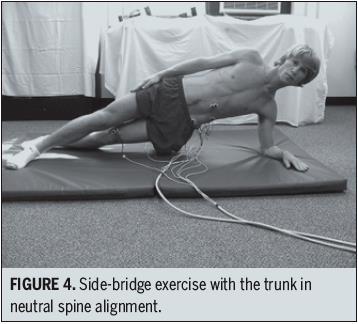
18 Improving Glute Med & Max Function Cue standing straight! Decrease anterior pelvic tilt Restore ROM: Hip Extension Good exercises to work glute med and max with minimal TFL contribution
19
20
21
22




23

24 Which Exercises Target the Gluteal Muscles While Minimizing Activation of the Tensor Fascia Lata? Electromyographic Assessment Using Fine-Wire Electrodes Selkowitz et al, JOSPT Feb, 2013


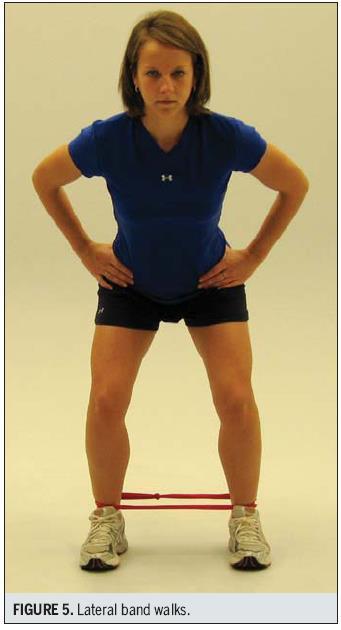
25 Band Walks Muscle Activation Depends on Positioning Lateral hips extended Lateral in squat position Backwards hips straight Backward/Forward Skates


26 What About the Hip Flexors?


27 Hip Flexors Iliopsoas Rectus Femoris TFL



28 Optimize Strengthening Work hip flexors from a very stable pelvis platform Start short lever before long lever. Start in a mid-range position before full hip extension Seated quad extensions Core and Hip Flexor Examples: Roller pelvic tilts Roller Pelvic tilts with knee raises Ball Hold Heel taps Ball hold knee extensions Front planks Front plank taps Dolly Pikes Modified Side Planks Side plank knee drives



29 Adductors Tend to be very tight/facillitated Start with side lying leg raises Progress to focus on eccentric control and mm coordination through full ROM

30 Mobility Considerations Myofascial restrictions of the TFL, Quad, Adductor Limited ROM: Hip Extension, Abduction, ER Compensations with movement and gait increase SI/lumbar load. Trigger point pain

31 Anterior/Lateral Tissue Scarring/Tightness


32 Trigger Point Referred Pain Dry Needling Guidelines 6 weeks post op in non-operative sites 12 weeks post-op in operative sites


33 Criteria For Return to Sport Progression Normal pain free gait Symmetrical ROM Manual muscle test of 5/5 or 90% with dynamometer Forward step down Y balance test 90%
34 Phase 3 Return to Sport/Activity Progression back to functional strength & endurance Sports Specific Criteria Based Progressions Ongoing treatment to limit sxs as stress and loads increase. Return to Sport Testing?


35 Return to Sport Testing Need to have the potential to succeed! Sport Specific: ROM, strength, endurance, reaction time Timed squat test Single leg squat to 90 + Sport cord tests Hop tests Timed core tests Criteria Based Progressions are the most important factor

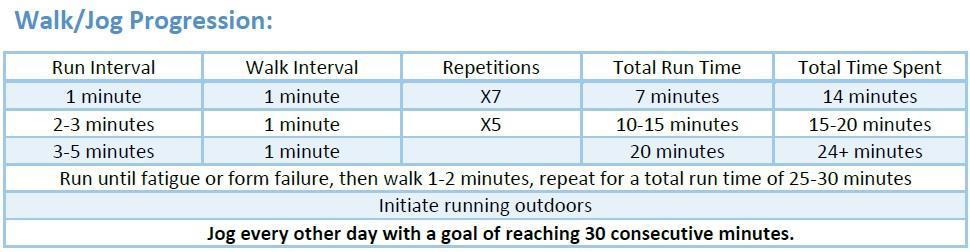
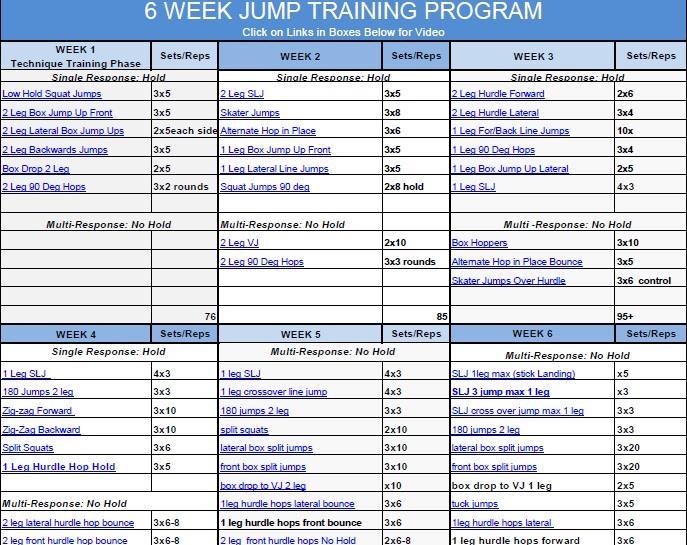
36 Return to Run
37
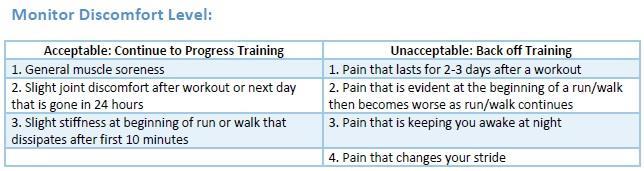
38 Pitfalls to Progression Not meeting basic ROM, Strength requirements Skipping progression steps Not getting timely treatment Not allowing enough time for recovery Pushing through pain

39 Have patience. All things are difficult before they become easy SAADI
Post Operative Hip Arthroscopy Rehabilitation Protocol Labral Repair With or Without FAI Component
 Post Operative Hip Arthroscopy Rehabilitation Protocol Labral Repair With or Without FAI Component ROM Restrictions: -Perform PROM in patient s PAIN FREE Range FLEXION EXTENSION EXTERNAL ROTATION 90 degrees
Post Operative Hip Arthroscopy Rehabilitation Protocol Labral Repair With or Without FAI Component ROM Restrictions: -Perform PROM in patient s PAIN FREE Range FLEXION EXTENSION EXTERNAL ROTATION 90 degrees
ARTHROSCOPIC LABRAL REPAIR WITH CAPSULAR PLICATION PHYSICAL THERAPY PROTOCOL
 ARTHROSCOPIC LABRAL REPAIR WITH CAPSULAR PLICATION PHYSICAL THERAPY PROTOCOL Jovan R. Laskovski, M.D. Hip Arthroscopy Sports Medicine & Orthopaedic Surgery Crystal Clinic Orthopaedic Center Please use
ARTHROSCOPIC LABRAL REPAIR WITH CAPSULAR PLICATION PHYSICAL THERAPY PROTOCOL Jovan R. Laskovski, M.D. Hip Arthroscopy Sports Medicine & Orthopaedic Surgery Crystal Clinic Orthopaedic Center Please use
ARTHROSCOPIC GLUTEUS MEDIUS REPAIR PHYSICAL THERAPY PROTOCOL
 ARTHROSCOPIC GLUTEUS MEDIUS REPAIR PHYSICAL THERAPY PROTOCOL Jovan R. Laskovski, M.D. Hip Arthroscopy Sports Medicine & Orthopaedic Surgery Crystal Clinic Orthopaedic Center Please use appropriate clinical
ARTHROSCOPIC GLUTEUS MEDIUS REPAIR PHYSICAL THERAPY PROTOCOL Jovan R. Laskovski, M.D. Hip Arthroscopy Sports Medicine & Orthopaedic Surgery Crystal Clinic Orthopaedic Center Please use appropriate clinical
S p o r t s & O r t h o p a e d i c S p e c i a l i s t s D R. R Y A N F A D E R
 S p o r t s & O r t h o p a e d i c S p e c i a l i s t s D R. R Y A N F A D E R H I P A R T H R O S C O P Y W I T H This protocol provides appropriate guidelines for the rehabilitation of patients following
S p o r t s & O r t h o p a e d i c S p e c i a l i s t s D R. R Y A N F A D E R H I P A R T H R O S C O P Y W I T H This protocol provides appropriate guidelines for the rehabilitation of patients following
Internal Rotation (turning toes/knee toward other leg) 30 degree limit. limit
 30 degree limit. limit") Hip Arthroscopy Patient Education Use of Brace and Crutches: - Wear the brace all times of weight bearing for the first 3 weeks after surgery. This is done to protect your hip and motion into hip extension
Hip Arthroscopy Patient Education Use of Brace and Crutches: - Wear the brace all times of weight bearing for the first 3 weeks after surgery. This is done to protect your hip and motion into hip extension
Training Philosophy. There are numerous views on core conditioning.
 Abs Lab Presented by Helen Vanderburg BKin, ACE, CanFitPro, Yoga and Pilates 2005 IDEA Instructor of the Year 2006/ 1996 CanFitPro Presenter of the Year Nautilus and BOSU Fitness Education Team Introduction
Abs Lab Presented by Helen Vanderburg BKin, ACE, CanFitPro, Yoga and Pilates 2005 IDEA Instructor of the Year 2006/ 1996 CanFitPro Presenter of the Year Nautilus and BOSU Fitness Education Team Introduction
Labral Repair with a Microfracture
 Labral Repair with a Microfracture This protocol should be used as a guideline for progression and should be tailored to the needs of the individual patient. Strict protective weight bearing status for
Labral Repair with a Microfracture This protocol should be used as a guideline for progression and should be tailored to the needs of the individual patient. Strict protective weight bearing status for
Compiled and Designed by: Sport Dimensions - 2 -
 SOCCER TRAINING While all reasonable care has been taken during the preparation of this edition, neither the publisher, nor the authors can accept responsibility for any consequences arising from the use
SOCCER TRAINING While all reasonable care has been taken during the preparation of this edition, neither the publisher, nor the authors can accept responsibility for any consequences arising from the use
Post Operative Hip Arthroscopy Procedure Form
 Post Operative Hip Arthroscopy Procedure Form Femoracetabular Impingement (FAI) Femoral Osteochondroplasty Acetabular Rim Trimming Acetabular Labrum Repair Location: o clock to o clock Debridement Articular
Post Operative Hip Arthroscopy Procedure Form Femoracetabular Impingement (FAI) Femoral Osteochondroplasty Acetabular Rim Trimming Acetabular Labrum Repair Location: o clock to o clock Debridement Articular
Hip Arthroscopy Protocol
 The intent of this protocol is to provide guidelines for progression of rehabilitation, it is not intended to serve as a substitute for clinical decision making. Progression through each phase of rehabilitation
The intent of this protocol is to provide guidelines for progression of rehabilitation, it is not intended to serve as a substitute for clinical decision making. Progression through each phase of rehabilitation
Post Operative Hip Arthroscopy Rehabilitation Protocol Dr. David Hergan Labral Repair with or without FAI Component
 Post Operative Hip Arthroscopy Rehabilitation Protocol Dr. David Hergan Labral Repair with or without FAI Component Initial Joint Protection Guidelines- (P.O. Day 1-4 wks): Joint Protection Patient education
Post Operative Hip Arthroscopy Rehabilitation Protocol Dr. David Hergan Labral Repair with or without FAI Component Initial Joint Protection Guidelines- (P.O. Day 1-4 wks): Joint Protection Patient education
Protocol G Arthroscopic Surgery: Therapist Information
 Protocol G Arthroscopic Surgery: Therapist Information Please read entire protocol prior to initiating therapy Please do not hesitate to contact Dr. Wolff with questions or concerns. Rest is a vital component
Protocol G Arthroscopic Surgery: Therapist Information Please read entire protocol prior to initiating therapy Please do not hesitate to contact Dr. Wolff with questions or concerns. Rest is a vital component
S p o r t s & O r t h o p a e d i c S p e c i a l i s t s D R. R Y A N F A D E R
 S p o r t s & O r t h o p a e d i c S p e c i a l i s t s D R. R Y A N F A D E R H I P A R T H R O S C O P Y W I T H L A B R A L R E P A I R P R O T O C O L This protocol provides appropriate guidelines
S p o r t s & O r t h o p a e d i c S p e c i a l i s t s D R. R Y A N F A D E R H I P A R T H R O S C O P Y W I T H L A B R A L R E P A I R P R O T O C O L This protocol provides appropriate guidelines
Alejandro Verdugo, M.D.
 Alejandro Verdugo, M.D. Physical Therapy Protocol Gluteus Medius repair with or without labral repair The intent of this protocol is to provide guidelines for your patient s therapy progression. It is
Alejandro Verdugo, M.D. Physical Therapy Protocol Gluteus Medius repair with or without labral repair The intent of this protocol is to provide guidelines for your patient s therapy progression. It is
Initial Exercises (Weeks 1-3)
") Labral Repair This protocol should be used as a guideline for progression and should be tailored to the needs of the individual patient. Partial weight bearing (50%) (4 weeks). Encourage, but limit hip
Labral Repair This protocol should be used as a guideline for progression and should be tailored to the needs of the individual patient. Partial weight bearing (50%) (4 weeks). Encourage, but limit hip
Phase 1- Immediate Rehabilitation (1-3 weeks): Goals Precautions:
: Goals Precautions:") Phase 1- Immediate Rehabilitation (1-3 weeks): Goals: Protection of the repaired tissue Prevent muscular inhibition and gait abnormalities Diminish pain and inflammation Precautions: 20 lb. flat-foot weight-bearing
Phase 1- Immediate Rehabilitation (1-3 weeks): Goals: Protection of the repaired tissue Prevent muscular inhibition and gait abnormalities Diminish pain and inflammation Precautions: 20 lb. flat-foot weight-bearing
Hip Arthroscopy Femoroacetabular Impingement (FAI) Ryan W. Hess, MD Tracey Pederson, PCC Office: (763) Fax: (763)
 Ryan W. Hess, MD Tracey Pederson, PCC Office: (763) Fax: (763)") Hip Arthroscopy Femoroacetabular Impingement (FAI) Ryan W. Hess, MD Tracey Pederson, PCC Office: (763) 302-2223 Fax: (763) 302-2401 GENERAL GUIDELINES: Despite the minimally invasive nature of hip arthroscopy,
Hip Arthroscopy Femoroacetabular Impingement (FAI) Ryan W. Hess, MD Tracey Pederson, PCC Office: (763) 302-2223 Fax: (763) 302-2401 GENERAL GUIDELINES: Despite the minimally invasive nature of hip arthroscopy,
Post Operative Hip Arthroscopy Procedure Form
 Post Operative Hip Arthroscopy Procedure Form Femoracetabular Impingement (FAI) Femoral Osteochondroplasty Acetabular Rim Trimming Acetabular Labrum Repair Location: o clock to o clock Debridement Articular
Post Operative Hip Arthroscopy Procedure Form Femoracetabular Impingement (FAI) Femoral Osteochondroplasty Acetabular Rim Trimming Acetabular Labrum Repair Location: o clock to o clock Debridement Articular
EXERCISE PHOTOS, TIPS AND INSTRUCTIONS
 Page 1 of 21 EXERCISE PHOTOS, TIPS AND INSTRUCTIONS Page 2. Squat Page 12. Crab Walks Page 3. Single Leg Squat Page 13. Bench Press Page 4. Split Squat Page 14. Bench Pull Page 5. Deadlift Page 15. Shoulder
Page 1 of 21 EXERCISE PHOTOS, TIPS AND INSTRUCTIONS Page 2. Squat Page 12. Crab Walks Page 3. Single Leg Squat Page 13. Bench Press Page 4. Split Squat Page 14. Bench Pull Page 5. Deadlift Page 15. Shoulder
Travis G. - 1 Maak, - MD Sports Medicine University of Utah Orthopaedics 590 Wakara Way Salt Lake City, UT Tel: Fax:
 Travis G. - 1 Maak, - MD Rehabilitation for Arthroscopic Osteochondroplasty with or without Labral Repair/Debridement General Guidelines: Normalize gait pattern with brace and crutches Continuous Passive
Travis G. - 1 Maak, - MD Rehabilitation for Arthroscopic Osteochondroplasty with or without Labral Repair/Debridement General Guidelines: Normalize gait pattern with brace and crutches Continuous Passive
BENJAMIN G. DOMB, MD
 Physical Therapy Protocol Partial or full thickness gluteus medius repair with or without labral repair The intent of this protocol is to provide guidelines for your patient s therapy progression. It is
Physical Therapy Protocol Partial or full thickness gluteus medius repair with or without labral repair The intent of this protocol is to provide guidelines for your patient s therapy progression. It is
Hip Arthroscopy Rehabilitation Gluteus Medius Repair with or without Labral Debridement. Normalize gait pattern with brace (if indicated) and crutches
 and crutches") General Guidelines: Hip Arthroscopy Rehabilitation Gluteus Medius Repair with or without Labral Debridement Normalize gait pattern with brace (if indicated) and crutches Weight-bearing: 20 lbs foot flat
General Guidelines: Hip Arthroscopy Rehabilitation Gluteus Medius Repair with or without Labral Debridement Normalize gait pattern with brace (if indicated) and crutches Weight-bearing: 20 lbs foot flat
S p o r t s & O r t h o p a e d i c S p e c i a l i s t s D R. R Y A N F A D E R
 S p o r t s & O r t h o p a e d i c S p e c i a l i s t s D R. R Y A N F A D E R H I P A R T H R O S C O P Y W I T H L A B R A L R E P A I R P R O T O C O L This protocol provides appropriate guidelines
S p o r t s & O r t h o p a e d i c S p e c i a l i s t s D R. R Y A N F A D E R H I P A R T H R O S C O P Y W I T H L A B R A L R E P A I R P R O T O C O L This protocol provides appropriate guidelines
JOHN M. REDMOND, M.D.
 Physical Therapy Protocol Gluteus Medius repair with or without labral repair The intent of this protocol is to provide guidelines for your patient s therapy progression. It is not intended to serve as
Physical Therapy Protocol Gluteus Medius repair with or without labral repair The intent of this protocol is to provide guidelines for your patient s therapy progression. It is not intended to serve as
Protocol D Arthroscopic Surgery: Therapist Information
 Protocol D Arthroscopic Surgery: Therapist Information Please read entire protocol prior to initiating therapy Please do not hesitate to contact Dr. Wolff with questions or concerns. Rest is a vital component
Protocol D Arthroscopic Surgery: Therapist Information Please read entire protocol prior to initiating therapy Please do not hesitate to contact Dr. Wolff with questions or concerns. Rest is a vital component
Protocol A Arthroscopic Surgery: Therapist Information
 Protocol A Arthroscopic Surgery: Therapist Information Please read entire protocol prior to initiating therapy Please do not hesitate to contact Dr. Wolff with questions or concerns. Rest is a vital component
Protocol A Arthroscopic Surgery: Therapist Information Please read entire protocol prior to initiating therapy Please do not hesitate to contact Dr. Wolff with questions or concerns. Rest is a vital component
Abductor Repair (Gluteus Medius/Minimus Repair)
") (Gluteus Medius/Minimus Repair) This protocol should be used as a guideline for progression and should be tailored to the needs of the individual patient. Strict protective weight bearing status for 8
(Gluteus Medius/Minimus Repair) This protocol should be used as a guideline for progression and should be tailored to the needs of the individual patient. Strict protective weight bearing status for 8
HIP ARTHROSCOPY REHAB 0-2 WEEKS
 HIP ARTHROSCOPY REHAB 0-2 WEEKS Protect the surgical repair Patient education regarding: gait and surgical findings. o Protected weight-bearing (PWB): weight bearing as tolerated with crutches o Ensure
HIP ARTHROSCOPY REHAB 0-2 WEEKS Protect the surgical repair Patient education regarding: gait and surgical findings. o Protected weight-bearing (PWB): weight bearing as tolerated with crutches o Ensure
Lower Crossed Syndrome
 Lower Crossed Syndrome Sang mi Yun October 23 rd 2017 Costa Mesa 2016 Abstract Lower-Crossed Syndrome (LCS) is also referred to as distal or pelvic crossed syndrome. In LCS, tightness of the thoracolumbar
Lower Crossed Syndrome Sang mi Yun October 23 rd 2017 Costa Mesa 2016 Abstract Lower-Crossed Syndrome (LCS) is also referred to as distal or pelvic crossed syndrome. In LCS, tightness of the thoracolumbar
BENJAMIN G. DOMB, M.D.
 Arthroscopic Hip Surgery Physical Therapy Protocol The intent of this protocol is to provide guidelines for your patient s therapy progression. It is not intended to serve as a recipe for treatment. We
Arthroscopic Hip Surgery Physical Therapy Protocol The intent of this protocol is to provide guidelines for your patient s therapy progression. It is not intended to serve as a recipe for treatment. We
Gluteal Strengthening Exercises: A Review of the Literature
 Common Imbalances Female Athlete Hip Injuries: Exploring the CORE of Patterns and Prevention Kelly McInnis, DO Irene Davis, PhD, PT, FAPTA, FACSM, FASB David Nolan, PT, DPT, MS, OCS, SCS, CSCS Gluteal
Common Imbalances Female Athlete Hip Injuries: Exploring the CORE of Patterns and Prevention Kelly McInnis, DO Irene Davis, PhD, PT, FAPTA, FACSM, FASB David Nolan, PT, DPT, MS, OCS, SCS, CSCS Gluteal
Bryan T. Kelly, MD Center for Hip Pain and Preservation Hospital for Special Surgery
 Hip Arthroscopy Rehabilitation Labral refixation with or without FAI Component General Guidelines: Limited external rotation to 20 degrees (2 weeks) No hyperextension (4 weeks) Normalize gait pattern with
Hip Arthroscopy Rehabilitation Labral refixation with or without FAI Component General Guidelines: Limited external rotation to 20 degrees (2 weeks) No hyperextension (4 weeks) Normalize gait pattern with
Travis G. - 1 Maak, - MD Sports Medicine University of Utah Orthopaedics 590 Wakara Way Salt Lake City, UT Tel: Fax:
 General Guidelines: Travis G. - 1 Maak, - MD Rehabilitation for Arthroscopic or Open Gluteus Medius Repair with or without Labral Debridement Normalize gait pattern with brace and crutches Weight-bearing:
General Guidelines: Travis G. - 1 Maak, - MD Rehabilitation for Arthroscopic or Open Gluteus Medius Repair with or without Labral Debridement Normalize gait pattern with brace and crutches Weight-bearing:
Total Knee Health Exercises
 Total Knee Health Exercises Self-Massage Exercises 4 Adductors 4 Calves 4 Foot, Underside 5 Front of Shin 5 Gluteus Maximus 6 Gluteus Medius 6 Hamstrings 6 Iliotibial Band 7 Piriformis 7 Quadriceps: Rectus
Total Knee Health Exercises Self-Massage Exercises 4 Adductors 4 Calves 4 Foot, Underside 5 Front of Shin 5 Gluteus Maximus 6 Gluteus Medius 6 Hamstrings 6 Iliotibial Band 7 Piriformis 7 Quadriceps: Rectus
Hip Arthroscopy. Labral Repair/Debridement with Femoroplasty
 Precautions for weeks 1 4 post-op: Hip Arthroscopy Labral Repair/Debridement with Femoroplasty Patient Education o For 1 week, Assist the involved LE during all transfers o For 2 weeks, Do not sit with
Precautions for weeks 1 4 post-op: Hip Arthroscopy Labral Repair/Debridement with Femoroplasty Patient Education o For 1 week, Assist the involved LE during all transfers o For 2 weeks, Do not sit with
Diagnosis: Gluteus Medius Tear, Labral Tear, CAM / Pincer
 Physical Therapy Prescription: Hip Arthroscopy Diagnosis: Gluteus Medius Tear, Labral Tear, CAM / Pincer Procedure: Gluteus Medius Repair, CAM / Pincer Decompression, Labral refixation / Capsular Shift
Physical Therapy Prescription: Hip Arthroscopy Diagnosis: Gluteus Medius Tear, Labral Tear, CAM / Pincer Procedure: Gluteus Medius Repair, CAM / Pincer Decompression, Labral refixation / Capsular Shift
Proximal Hamstring Rupture: Physical Therapy Protocol
 Proximal Hamstring Rupture: Physical Therapy Protocol The intent of this protocol is to provide guidelines for your patient s therapy progression. It is not intended to serve as a recipe for treatment.
Proximal Hamstring Rupture: Physical Therapy Protocol The intent of this protocol is to provide guidelines for your patient s therapy progression. It is not intended to serve as a recipe for treatment.
Microfracture. This protocol should be used as a guideline for progression and should be tailored to the needs of the individual patient.
 This protocol should be used as a guideline for progression and should be tailored to the needs of the individual patient. Strict protective weight bearing status for two months (8-9 weeks). Allow to place
This protocol should be used as a guideline for progression and should be tailored to the needs of the individual patient. Strict protective weight bearing status for two months (8-9 weeks). Allow to place
Precautions following Hip Arthroscopy/FAI: (Refixation/Osteochondroplasty)
") Physical Therapy Prescription: Hip Arthroscopy Diagnosis: Labral Tear, CAM / Pincer Procedure: Labral Repair / Capsular Shift, CAM / Pincer Decompression RX: Evaluate / Treat, and follow attached protocol
Physical Therapy Prescription: Hip Arthroscopy Diagnosis: Labral Tear, CAM / Pincer Procedure: Labral Repair / Capsular Shift, CAM / Pincer Decompression RX: Evaluate / Treat, and follow attached protocol
Training the Joint Replacement Client
 KNEE PRE-OP SAMPLE EXERCISE PLAN Quadricep: Shuttle 1 leg and 2 legs (focus on 1 leg) Leg Press 1 and 2 legs (focus on 1 leg) Sit to Stand (if no pain or compensation) Supine Circle Foam knee extension
KNEE PRE-OP SAMPLE EXERCISE PLAN Quadricep: Shuttle 1 leg and 2 legs (focus on 1 leg) Leg Press 1 and 2 legs (focus on 1 leg) Sit to Stand (if no pain or compensation) Supine Circle Foam knee extension
Exercises to Correct Muscular Imbalances. presented by: Darrell Barnes, LAT, ATC, CSCS
 Exercises to Correct Muscular Imbalances presented by: Darrell Barnes, LAT, ATC, CSCS Objectives Review Functional Anatomy Identify physical imbalances that lead to injury and/or decrease performance
Exercises to Correct Muscular Imbalances presented by: Darrell Barnes, LAT, ATC, CSCS Objectives Review Functional Anatomy Identify physical imbalances that lead to injury and/or decrease performance
Travis G. Maak, MD Sports Medicine University of Utah Orthopaedics 590 Wakara Way Salt Lake City, UT Tel: Fax:
 General Guidelines: Hip Arthroscopy Rehabilitation Capsular Shift with or without FAI Labral Components No external rotation greater than 30 degrees for 4 weeks No hyperextension for 4 weeks Normalize
General Guidelines: Hip Arthroscopy Rehabilitation Capsular Shift with or without FAI Labral Components No external rotation greater than 30 degrees for 4 weeks No hyperextension for 4 weeks Normalize
Lowe w r e r B ody Resistance Training
 Lower Body Resistance Training Tibialis Anterior Extensor Hallucis Longus Extensor Digitorum Longus Proneus Tertius AROM 25-40 degrees Extensor active-insufficiency Flexion & Eversion (Pronation) Flexion
Lower Body Resistance Training Tibialis Anterior Extensor Hallucis Longus Extensor Digitorum Longus Proneus Tertius AROM 25-40 degrees Extensor active-insufficiency Flexion & Eversion (Pronation) Flexion
Human anatomy reference:
 Human anatomy reference: Weak Glut Activation Weak gluteal activation comes from poor biomechanics, poor awareness when training or prolonged exposure in deactivated positions such as sitting. Weak Glut
Human anatomy reference: Weak Glut Activation Weak gluteal activation comes from poor biomechanics, poor awareness when training or prolonged exposure in deactivated positions such as sitting. Weak Glut
Hip Arthroscopy Rehabilitation Labral Refixation with or without FAI Component. Limited external rotation to 20 degrees (2 weeks)
") General Guidelines: 4140 Centennial Hills Boulevard Casper, WY 82609 (307) 265-7205 Hip Arthroscopy Rehabilitation Labral Refixation with or without FAI Component Limited external rotation to 20 degrees
General Guidelines: 4140 Centennial Hills Boulevard Casper, WY 82609 (307) 265-7205 Hip Arthroscopy Rehabilitation Labral Refixation with or without FAI Component Limited external rotation to 20 degrees
REHABILITATION PROTOCOL Criteria-Based Postoperative ACL Reconstruction Rehabilitation Protocol
 REHABILITATION PROTOCOL Criteria-Based Postoperative ACL Reconstruction Rehabilitation Protocol Phase I (Days 1 7) WEIGHTBEARING STATUS 1- Two crutches, weightbearing as tolerated. Exercises 1- Heel slides/wall
REHABILITATION PROTOCOL Criteria-Based Postoperative ACL Reconstruction Rehabilitation Protocol Phase I (Days 1 7) WEIGHTBEARING STATUS 1- Two crutches, weightbearing as tolerated. Exercises 1- Heel slides/wall
Avon Office 2 Simsbury Rd. Avon, CT Office: (860) Fax: (860) Acetabuloplasty
 Fax: (860) Acetabuloplasty") Katherine J. Coyner, MD UCONN Musculoskeletal Institute Medical Arts & Research Building 263 Farmington Ave. Farmington, CT 06030 Office: (860) 679-6600 Fax: (860) 679-6649 www.drcoyner.com This protocol
Katherine J. Coyner, MD UCONN Musculoskeletal Institute Medical Arts & Research Building 263 Farmington Ave. Farmington, CT 06030 Office: (860) 679-6600 Fax: (860) 679-6649 www.drcoyner.com This protocol
CENTER FOR ORTHOPAEDICS AND SPINE CARE PHYSICAL THERAPY PROTOCOL ACUTE PROXIMAL HAMSTRING TENDON REPAIR BENJAMIN J. DAVIS, MD
 Weeks 0-6 Goal: 1) Protection of the surgical repair Precautions: 1) Non-weight bearing with crutches for 6 weeks with foot flat or with knee Knee flexed to 90 degrees with sitting 2) No active hamstring
Weeks 0-6 Goal: 1) Protection of the surgical repair Precautions: 1) Non-weight bearing with crutches for 6 weeks with foot flat or with knee Knee flexed to 90 degrees with sitting 2) No active hamstring
Prater Chiropractic Wellness Center 903 W. South St. Kalamazoo, MI PH: (269)
") Purpose of Program After an injury or surgery, an exercise conditioning program will help you return to daily activities and enjoy a more active, healthy lifestyle. Following a well-structured conditioning
Purpose of Program After an injury or surgery, an exercise conditioning program will help you return to daily activities and enjoy a more active, healthy lifestyle. Following a well-structured conditioning
Rehabilitation. Friday, October 14, :00 11:45am General Session Rehabilitation following FAI Surgery Mark Ryan, MS, ATC, CSCS USA
 Rehabilitation Friday, October 14, 2011 11:00 11:45am General Session Rehabilitation following FAI Surgery Mark Ryan, MS, ATC, CSCS USA Best Tip Srino Bharam, MD USA Best Tip Robroy Martin, PhD, PT USA
Rehabilitation Friday, October 14, 2011 11:00 11:45am General Session Rehabilitation following FAI Surgery Mark Ryan, MS, ATC, CSCS USA Best Tip Srino Bharam, MD USA Best Tip Robroy Martin, PhD, PT USA
Presentation Overview 8/8/12. Muscle Imbalances Revealed Assessment & Exercise for Personal Training
 Presentation Overview Common issues seen in many athletes from different sports Some important assessments that can be used for many varieties of athletes Exercise progressions that can fix imbalances
Presentation Overview Common issues seen in many athletes from different sports Some important assessments that can be used for many varieties of athletes Exercise progressions that can fix imbalances
Hip Arthroscopy with CAM resection/labral Repair Protocol
 Hip Arthroscopy with CAM resection/labral Repair Protocol As tolerated should be understood to perform with safety for the reconstruction/repair. Pain, limp, swelling, or other undesirable factors are
Hip Arthroscopy with CAM resection/labral Repair Protocol As tolerated should be understood to perform with safety for the reconstruction/repair. Pain, limp, swelling, or other undesirable factors are
Hip Arthroscopy Labral Repair Protocol
 Hip Arthroscopy Labral Repair Protocol Applicability: Physician Practices Date Effective: 09/2013 Department: Rehabilitation Services Date Last Reviewed: 1/2018 Supersedes: n/a Administration Approval:
Hip Arthroscopy Labral Repair Protocol Applicability: Physician Practices Date Effective: 09/2013 Department: Rehabilitation Services Date Last Reviewed: 1/2018 Supersedes: n/a Administration Approval:
Hip Arthroscopy with Labral Repair and Osteoplasties PT Rehab Protocol
 Matthew T. Mantell, MD 128 Medical Circle Winchester, VA 22601 Phone: 540-667-8975 Email: mattmantellmd@gmail.com Web: www.mattmantellmd.com Hip Arthroscopy with Labral Repair and Osteoplasties PT Rehab
Matthew T. Mantell, MD 128 Medical Circle Winchester, VA 22601 Phone: 540-667-8975 Email: mattmantellmd@gmail.com Web: www.mattmantellmd.com Hip Arthroscopy with Labral Repair and Osteoplasties PT Rehab
How to Build Strength and Flexibility Pre and Post-Op Hip Replacement Surgery due to Acetabular Dysplasia
 How to Build Strength and Flexibility Pre and Post-Op Hip Replacement Surgery due to Acetabular Dysplasia Ulrika Egner December 2017 CTTC 2017 Pretoria South Africa Abstract This paper examines how one
How to Build Strength and Flexibility Pre and Post-Op Hip Replacement Surgery due to Acetabular Dysplasia Ulrika Egner December 2017 CTTC 2017 Pretoria South Africa Abstract This paper examines how one
Routine Arthroscopic Procedure
 Katherine J. Coyner, MD UCONN Musculoskeletal Institute Medical Arts & Research Building 263 Farmington Ave. Farmington, CT 06030 Office: (860) 679-6600 Fax: (860) 679-6649 www.drcoyner.com Avon Office
Katherine J. Coyner, MD UCONN Musculoskeletal Institute Medical Arts & Research Building 263 Farmington Ave. Farmington, CT 06030 Office: (860) 679-6600 Fax: (860) 679-6649 www.drcoyner.com Avon Office
Alejandro Verdugo m.d.
 Alejandro Verdugo m.d. Proximal Hamstring Rupture: Physical Therapy Protocol The intent of this protocol is to provide guidelines for your patient s therapy progression. It is not intended to serve as
Alejandro Verdugo m.d. Proximal Hamstring Rupture: Physical Therapy Protocol The intent of this protocol is to provide guidelines for your patient s therapy progression. It is not intended to serve as
Evaluating the Athlete Questionnaire
 Evaluating the Athlete Questionnaire Prior to developing the strength and conditioning training plan the coach should first evaluate factors from the athlete s questionnaire that may impact the strength
Evaluating the Athlete Questionnaire Prior to developing the strength and conditioning training plan the coach should first evaluate factors from the athlete s questionnaire that may impact the strength
Hip Arthroscopy Rehabilitation Protocol
 Hip Arthroscopy Rehabilitation Protocol 1. Concepts: a. Range of motion and weight bearing restrictions must be adhered to during the initial rehab process (4 total weeks of ROM and weight bearing restrictions)
Hip Arthroscopy Rehabilitation Protocol 1. Concepts: a. Range of motion and weight bearing restrictions must be adhered to during the initial rehab process (4 total weeks of ROM and weight bearing restrictions)
Hip Labrum and FAI Post-Surgical Rehabilitation Guideline
 Hip Labrum and FAI Post-Surgical Rehabilitation Guideline This rehabilitation program is designed to return the individual to their activities as quickly and safely as possible. It is designed for rehabilitation
Hip Labrum and FAI Post-Surgical Rehabilitation Guideline This rehabilitation program is designed to return the individual to their activities as quickly and safely as possible. It is designed for rehabilitation
Direct Anterior Total Hip Replacement Rehabilitation Program
 Direct Anterior Total Hip Replacement Rehabilitation Program The rehabilitation protocol following Direct Anterior Total Hip Replacement is an integral part of the recovery process. This document includes
Direct Anterior Total Hip Replacement Rehabilitation Program The rehabilitation protocol following Direct Anterior Total Hip Replacement is an integral part of the recovery process. This document includes
Dr Schock High Tibial Osteotomy
 Dr Schock High Tibial Osteotomy Goals for phase 1 Control pain Control edema Initiate ROM and quad strengthening Maintain WB restrictions Appropriate brace wear Criteria for progression to Phase 2 Edema
Dr Schock High Tibial Osteotomy Goals for phase 1 Control pain Control edema Initiate ROM and quad strengthening Maintain WB restrictions Appropriate brace wear Criteria for progression to Phase 2 Edema
Main Menu. Joint and Pelvic Girdle click here. The Power is in Your Hands
 1 Hip Joint and Pelvic Girdle click here Main Menu K.6 http://www.handsonlineeducation.com/classes//k6entry.htm[3/23/18, 2:01:12 PM] Hip Joint (acetabular femoral) Relatively stable due to : Bony architecture
1 Hip Joint and Pelvic Girdle click here Main Menu K.6 http://www.handsonlineeducation.com/classes//k6entry.htm[3/23/18, 2:01:12 PM] Hip Joint (acetabular femoral) Relatively stable due to : Bony architecture
Spine Conditioning Program Purpose of Program
 Prepared for: Prepared by: Purpose of Program After an injury or surgery, an exercise conditioning program will help you return to daily activities and enjoy a more active, healthy lifestyle. Following
Prepared for: Prepared by: Purpose of Program After an injury or surgery, an exercise conditioning program will help you return to daily activities and enjoy a more active, healthy lifestyle. Following
Muscles of the Gluteal Region
 Muscles of the Gluteal Region 1 Some of the most powerful in the body Extend the thigh during forceful extension Stabilize the iliotibial band and thoracolumbar fascia Related to shoulders and arms because
Muscles of the Gluteal Region 1 Some of the most powerful in the body Extend the thigh during forceful extension Stabilize the iliotibial band and thoracolumbar fascia Related to shoulders and arms because
Rehabilitation of Hip Labral Tears and Femoroacetabular Impingement
 Rehabilitation of Hip Labral Tears and Femoroacetabular Impingement Michael Newsome PT, OCS, SCS, CSCS Hip injuries account for 3.1% of all injuries in the NFL from 1997-2006 (Feeley 2008) 59% strains
Rehabilitation of Hip Labral Tears and Femoroacetabular Impingement Michael Newsome PT, OCS, SCS, CSCS Hip injuries account for 3.1% of all injuries in the NFL from 1997-2006 (Feeley 2008) 59% strains
Figure 1 - Hip and Pelvis
 Hip Figure 1 - Hip and Pelvis The terms hip and pelvis are frequently used interchangeably, but strictly speaking, the pelvis is a girdle of bones and the hip is a joint. The pelvis consists of The sacrum
Hip Figure 1 - Hip and Pelvis The terms hip and pelvis are frequently used interchangeably, but strictly speaking, the pelvis is a girdle of bones and the hip is a joint. The pelvis consists of The sacrum
Diagnosis: Labral Tear, Internal Snapping Hip, CAM / Pincer. Procedure: Partial Psoas Release with CAM / Pincer Decompression and Labral Debridement
 Physical Therapy Prescription: Hip Arthroscopy Diagnosis: Labral Tear, Internal Snapping Hip, CAM / Pincer Procedure: Partial Psoas Release with CAM / Pincer Decompression and Labral Debridement RX: Evaluate
Physical Therapy Prescription: Hip Arthroscopy Diagnosis: Labral Tear, Internal Snapping Hip, CAM / Pincer Procedure: Partial Psoas Release with CAM / Pincer Decompression and Labral Debridement RX: Evaluate
Role Of The Fitness Professional. Causes of Fitness Related Injuries. The Assessments. Screening & Assessing: A Holistic Approach 2/9/2016
 Screening & Assessing: A Holistic Approach Role Of The Fitness Professional Fitness professionals must assess clientele, but need to understand the difference between medical diagnosis vs fitness limitations.
Screening & Assessing: A Holistic Approach Role Of The Fitness Professional Fitness professionals must assess clientele, but need to understand the difference between medical diagnosis vs fitness limitations.
Hip joint and pelvic girdle. Lower Extremity. Pelvic Girdle 6/5/2017
 Hip joint and pelvic girdle Lower Extremity The relationship between the pelvic girdle and hip is similar to that between the shoulder girdle and shoulder joint. The lower limbs are attached to the axial
Hip joint and pelvic girdle Lower Extremity The relationship between the pelvic girdle and hip is similar to that between the shoulder girdle and shoulder joint. The lower limbs are attached to the axial
Primary Movements. Which one? Rational - OHS. Assessment. Rational - OHS 1/1/2013. Two Primary Movement Assessment: Dynamic Assessment (other)
") Primary Movements Practical Application for Athletic Trainers Two Primary Movement Assessment: NASM-CES Overhead Squat Single-leg Squat Dynamic Assessment (other) Single-leg Step Off Functional Movement
Primary Movements Practical Application for Athletic Trainers Two Primary Movement Assessment: NASM-CES Overhead Squat Single-leg Squat Dynamic Assessment (other) Single-leg Step Off Functional Movement
DISTANCE RUNNER MECHANICS AMY BEGLEY
 DISTANCE RUNNER MECHANICS AMY BEGLEY FORM Forward motion is thought to be automatic and hard to change. Changing one thing can cause a chain reaction. Can improve: Balance Strength Flexibility Alignment
DISTANCE RUNNER MECHANICS AMY BEGLEY FORM Forward motion is thought to be automatic and hard to change. Changing one thing can cause a chain reaction. Can improve: Balance Strength Flexibility Alignment
Bony Anatomy. Femur. Femoral Head Femoral Neck Greater Trochanter Lesser Trochanter Intertrochanteric Crest Intertrochanteric Line Gluteal Tuberosity
 Hip Anatomy Bony Anatomy Femur Femoral Head Femoral Neck Greater Trochanter Lesser Trochanter Intertrochanteric Crest Intertrochanteric Line Gluteal Tuberosity Bony Anatomy Pelvic Girdle Acetabulum 3 bones
Hip Anatomy Bony Anatomy Femur Femoral Head Femoral Neck Greater Trochanter Lesser Trochanter Intertrochanteric Crest Intertrochanteric Line Gluteal Tuberosity Bony Anatomy Pelvic Girdle Acetabulum 3 bones
Snow Angels on Foam Roll
 Thoracic Mobilization on Foam Roll Lie on your back with a foam roller positioned horizontally across your mid back, and arms crossed in front of your body. Bend your knees so your feet are resting flat
Thoracic Mobilization on Foam Roll Lie on your back with a foam roller positioned horizontally across your mid back, and arms crossed in front of your body. Bend your knees so your feet are resting flat
Flexibility. STRETCH: Kneeling gastrocnemius. STRETCH: Standing gastrocnemius. STRETCH: Standing soleus. Adopt a press up position
 STRETCH: Kneeling gastrocnemius Adopt a press up position Rest one knee on mat with the opposite leg straight Maintain a neutral spine position Push through arms to lever ankle into increased dorsiflexion
STRETCH: Kneeling gastrocnemius Adopt a press up position Rest one knee on mat with the opposite leg straight Maintain a neutral spine position Push through arms to lever ankle into increased dorsiflexion
Move to IMPROVE. Strength Program
 Move to IMPROVE Strength Program Intro Our activities of daily living involve both static and dynamic postures. Static posture is how one presents itself in stance and is the base form from which an individual
Move to IMPROVE Strength Program Intro Our activities of daily living involve both static and dynamic postures. Static posture is how one presents itself in stance and is the base form from which an individual
Provide movement Maintain posture/stability Generate heat
 How we move.. What do muscles do for us? Provide movement Maintain posture/stability Generate heat (skeletal muscle accounts for 40% body mass) So looking at skeletal muscles.. What do skeletal muscles
How we move.. What do muscles do for us? Provide movement Maintain posture/stability Generate heat (skeletal muscle accounts for 40% body mass) So looking at skeletal muscles.. What do skeletal muscles
APPLICATION OF THE MOVEMENT SYSTEMS MODEL TO THE MANAGEMENT COMMON HIP PATHOLOGIES
 APPLICATION OF THE MOVEMENT SYSTEMS MODEL TO THE MANAGEMENT COMMON HIP PATHOLOGIES Tracy Porter, PT, DPT Des Moines University Department of Physical Therapy Objectives Review current literature related
APPLICATION OF THE MOVEMENT SYSTEMS MODEL TO THE MANAGEMENT COMMON HIP PATHOLOGIES Tracy Porter, PT, DPT Des Moines University Department of Physical Therapy Objectives Review current literature related
How to GET RESULTS BETWEEN SESSIONS LumboPelvic Hip Complex HOMEWORK. LPHC Homework Presented by Dr. Bruce Costello
 How to GET RESULTS BETWEEN SESSIONS LumboPelvic Hip Complex HOMEWORK LPHC Homework Presented by Dr. Bruce Costello Spinal Mobilization Reaching for the Stars Side-Bend Modified Karate Punch Session Objectives
How to GET RESULTS BETWEEN SESSIONS LumboPelvic Hip Complex HOMEWORK LPHC Homework Presented by Dr. Bruce Costello Spinal Mobilization Reaching for the Stars Side-Bend Modified Karate Punch Session Objectives
Beginner and advanced exercises. utilizing a stability ball. Professionally managed by:
 Beginner and advanced exercises utilizing a stability ball Professionally managed by: Mission: The National Institute for Fitness and Sport is committed to enhancing human health, physical fitness and
Beginner and advanced exercises utilizing a stability ball Professionally managed by: Mission: The National Institute for Fitness and Sport is committed to enhancing human health, physical fitness and
Rehabilitation Guidelines for Open Hip Abductor (Gluteus Medius) Repair
 Repair") UW HEALTH SPORTS REHABILITATION Rehabilitation Guidelines for Open Hip Abductor (Gluteus Medius) Repair The hip joint is composed of the femur (the thigh bone) and the acetabulum (the socket which is from
UW HEALTH SPORTS REHABILITATION Rehabilitation Guidelines for Open Hip Abductor (Gluteus Medius) Repair The hip joint is composed of the femur (the thigh bone) and the acetabulum (the socket which is from
Stretching the Major Muscle Groups of the Lower Limb
 Preface In 1964, at the beginning of my PhD studies at Southern Illinois University, I was first introduced to the theory and practice of proprioceptive neuromuscular facilitation (PNF). One specific application,
Preface In 1964, at the beginning of my PhD studies at Southern Illinois University, I was first introduced to the theory and practice of proprioceptive neuromuscular facilitation (PNF). One specific application,
Chapter 3: Applied Kinesiology. ACE Personal Trainer Manual Third Edition
 Chapter 3: Applied Kinesiology ACE Personal Trainer Manual Third Edition Introduction Kinesiology is the study of the body s infinite number of movements, positions, and postures and is grounded in the
Chapter 3: Applied Kinesiology ACE Personal Trainer Manual Third Edition Introduction Kinesiology is the study of the body s infinite number of movements, positions, and postures and is grounded in the
The psoas minor is medial to the psoas major. The iliacus is a fan-shaped muscle that when contracted helps bring the swinging leg forward in walking
 1 p.177 2 3 The psoas minor is medial to the psoas major. The iliacus is a fan-shaped muscle that when contracted helps bring the swinging leg forward in walking and running. The iliopsoas and adductor
1 p.177 2 3 The psoas minor is medial to the psoas major. The iliacus is a fan-shaped muscle that when contracted helps bring the swinging leg forward in walking and running. The iliopsoas and adductor
CAPPAGH NATIONAL ORTHOPAEDIC HOSPITAL, FINGLAS, DUBLIN 11. The Sisters of Mercy. Hip Arthroscopy
 1.0 Policy Statement... 2 2.0 Purpose... 2 3.0 Scope... 2 4.0 Health & Safety... 2 5.0 Responsibilities... 2 6.0 Definitions and Abbreviations... 3 7.0 Guideline... 3 7.1 Rehabilitation Phase 1 (Day 1
1.0 Policy Statement... 2 2.0 Purpose... 2 3.0 Scope... 2 4.0 Health & Safety... 2 5.0 Responsibilities... 2 6.0 Definitions and Abbreviations... 3 7.0 Guideline... 3 7.1 Rehabilitation Phase 1 (Day 1
Prevention of common running injuries
 Prevention of common running injuries Lower limb and hip joint pain, along with soft tissue structures of the lower leg, can be extremely painful and frustrating injuries. Some of the most common running
Prevention of common running injuries Lower limb and hip joint pain, along with soft tissue structures of the lower leg, can be extremely painful and frustrating injuries. Some of the most common running
Guide To ACL Reconstruction Rehabilitation
 Guide To ACL Reconstruction Rehabilitation Welcome to our ACL Reconstruction Rehabilitation video series. The goal of these videos is to help maximize your recovery following ACL reconstruction surgery.
Guide To ACL Reconstruction Rehabilitation Welcome to our ACL Reconstruction Rehabilitation video series. The goal of these videos is to help maximize your recovery following ACL reconstruction surgery.
Hip Arthroscopy Rehabilitation Labral Debridement with or without FAI Component. Normalize gait pattern with brace and crutches
 Hip Arthroscopy Rehabilitation Labral Debridement with or without FAI Component General Guidelines: Normalize gait pattern with brace and crutches Weightbearing as per procedure performed Continuous Passive
Hip Arthroscopy Rehabilitation Labral Debridement with or without FAI Component General Guidelines: Normalize gait pattern with brace and crutches Weightbearing as per procedure performed Continuous Passive
Muscle Imbalances and the Performance Client
 Muscle Imbalances and the Performance Client Assessments and Exercise Progressions to Improve Performance and Prevent Injury Nick Rosencutter, CSCS, NSCA-CPT, LMT About Me Strength Coach and Manual Therapist
Muscle Imbalances and the Performance Client Assessments and Exercise Progressions to Improve Performance and Prevent Injury Nick Rosencutter, CSCS, NSCA-CPT, LMT About Me Strength Coach and Manual Therapist
Pilates for the Post Periacetabular Osteotomy (PAO) Client
 Client") Pilates for the Post Periacetabular Osteotomy (PAO) Client Stacey Barnes September 28, 2014 Oceanside, CA 1 Abstract This paper examines how Pilates is used as a conditioning program for a client post
Pilates for the Post Periacetabular Osteotomy (PAO) Client Stacey Barnes September 28, 2014 Oceanside, CA 1 Abstract This paper examines how Pilates is used as a conditioning program for a client post
Anterior Pelvic Tilt (APT) Samantha Peralta & Joshua Moore Rowan University
 Samantha Peralta & Joshua Moore Rowan University") Anterior Pelvic Tilt (APT) Samantha Peralta & Joshua Moore Rowan University Anterior Pelvic Tilt What is it? Occurs when the front of the pelvis drops and the back of the pelvis rises Anatomy of The Pelvis
Anterior Pelvic Tilt (APT) Samantha Peralta & Joshua Moore Rowan University Anterior Pelvic Tilt What is it? Occurs when the front of the pelvis drops and the back of the pelvis rises Anatomy of The Pelvis
Non Surgical Hip Therapy Athletic Hip Injury: Therapist Information
 Non Surgical Hip Therapy Athletic Hip Injury: Therapist Information Please read entire protocol prior to initiating therapy Please note: Individual hip injuries vary widely. This therapy protocol should
Non Surgical Hip Therapy Athletic Hip Injury: Therapist Information Please read entire protocol prior to initiating therapy Please note: Individual hip injuries vary widely. This therapy protocol should
ACL Reconstruction Rehabilitation Protocol
 ACL Reconstruction Rehabilitation Protocol 1. Pre-OP Visit: a. Patient Education b. Exercises c. Gait Outline rehabilitation timeline. Discuss: Swelling/effusion control (PRICE). Quadriceps inhibition
ACL Reconstruction Rehabilitation Protocol 1. Pre-OP Visit: a. Patient Education b. Exercises c. Gait Outline rehabilitation timeline. Discuss: Swelling/effusion control (PRICE). Quadriceps inhibition
Stretching. Back (Latissimus dorsi) "Chicken Wings" Chest (Pec. major + Ant. deltoid) "Superman" Method: Method: 1) Stand tall and maintain proper
 Chicken Wings Chest (Pec. major + Ant. deltoid) Superman Method: Method: 1) Stand tall and maintain proper") Chest (Pec. major + Ant. deltoid) "Chicken Wings" Back (Latissimus dorsi) "Superman" 1) Stand tall and maintain proper 1) Reach hands overhead and lumbar curve. grasp one wrist. 2) Place palms on lower
Chest (Pec. major + Ant. deltoid) "Chicken Wings" Back (Latissimus dorsi) "Superman" 1) Stand tall and maintain proper 1) Reach hands overhead and lumbar curve. grasp one wrist. 2) Place palms on lower
The Hip (Iliofemoral) Joint. Presented by: Rob, Rachel, Alina and Lisa
 Joint. Presented by: Rob, Rachel, Alina and Lisa") The Hip (Iliofemoral) Joint Presented by: Rob, Rachel, Alina and Lisa Surface Anatomy: Posterior Surface Anatomy: Anterior Bones: Os Coxae Consists of 3 Portions: Ilium Ischium Pubis Bones: Pubis Portion
The Hip (Iliofemoral) Joint Presented by: Rob, Rachel, Alina and Lisa Surface Anatomy: Posterior Surface Anatomy: Anterior Bones: Os Coxae Consists of 3 Portions: Ilium Ischium Pubis Bones: Pubis Portion
BLUE SKY SCHOOL OF PROFESSIONAL MASSAGE AND THERAPEUTIC BODYWORK Musculoskeletal Anatomy & Kinesiology POSTURE & GAIT ASSESSMENT
 BLUE SKY SCHOOL OF PROFESSIONAL MASSAGE AND THERAPEUTIC BODYWORK Musculoskeletal Anatomy & Kinesiology POSTURE & GAIT ASSESSMENT MSAK201-I Session 4 LEARNING OBJECTIVES: By the end of session 4, the student
BLUE SKY SCHOOL OF PROFESSIONAL MASSAGE AND THERAPEUTIC BODYWORK Musculoskeletal Anatomy & Kinesiology POSTURE & GAIT ASSESSMENT MSAK201-I Session 4 LEARNING OBJECTIVES: By the end of session 4, the student
Muscle Energy Technique
 PRACTICE SESSION: Muscle Energy Technique BE AN ARTIST and work out the best way for you to use the Muscle Energy Technique (MET). This technique works best when muscles are shortened. If you try MET on
PRACTICE SESSION: Muscle Energy Technique BE AN ARTIST and work out the best way for you to use the Muscle Energy Technique (MET). This technique works best when muscles are shortened. If you try MET on
Total Hip Replacement Rehabilitation: Progression and Restrictions
 Total Hip Replacement Rehabilitation: Progression and Restrictions The success of total hip replacement (THR) is a result of predictable pain relief, improvements in quality of life, and restoration of
Total Hip Replacement Rehabilitation: Progression and Restrictions The success of total hip replacement (THR) is a result of predictable pain relief, improvements in quality of life, and restoration of