387
|
|
|
- Lucas Willis Robbins
- 5 years ago
- Views:
Transcription
1 387!
2 388!
3 389!
4 !! 390!

5
6


7

8

9 Ishihara Colorblindness Test A" B" C" D" E" F" 395


10 Optical Illusions A. Focus on the center circle and explain what you see. B. Is the center circle on the right or left larger? 396!


11 Optical Illusions C. There is a 3D image in this picture. Focus and unfocus your eyes until it pops out. What do you see? D. There is a 3D image in this picture. Focus and unfocus your eyes until it pops out. What do you see? 397


12 Optical Illusions E. Focus on the center of the image and explain what you see.! F. How many people are in this image? 398!


13 Optical Illusions G. Stare at the black spot for 30 sec, then look at a white wall or sheet of paper. Explain what you see. H. Stare at the nose for 30 sec, then look at a white wall or sheet of paper. Explain what you see


14 Optical Illusions I. Stare at the white spot for 30 sec, then look at a white wall or sheet of paper. Explain what you see. J. Stare at the center spot for 30 sec, then look at a white wall or sheet of paper. Explain what you see. 400!

15 ! 401


 Blood thinners Surgery to open clogged vessel")



16 Occurs when blood flow to a portion of the brain is halted Causes & Risk Factors Certain types are hereditary Blood vessel is clogged by plaque or blood clot Blood vessel bursts Diabetes High cholesterol Increasing age Unhealthy lifestyle choices Symptoms Treatment Options Severe headache Change in hearing, taste, touch, or vision Change in alertness Loss of coordination & balance Confusion or memory loss Muscle weakness or numbness (usually onesided) Hospitalization Blood clot = clot busting drugs (thrombolytics) Blood thinners Surgery to open clogged vessel Surgery to repair vessels Stroke rehabilitation C A B C D E A. B. C. D. E.




17 Causes & Risk Factors Hereditary Family history Age: over 60 High insulin levels Past head trauma A form of dementia associated with age Symptoms Memory loss Confusion & disorientation Mood & behavior changes Difficulty performing everyday functions Unfounded suspicions Difficulty speaking, swallowing, and/or walking Treatment Options Uncurable Medication Removing behavior triggers Psychological coping skills Herbal therapies Stem cells A B C A. B. C




18 Brain disorder that makes it difficult to communicate Causes & Risk Factors Cause is not well understood Family history Hereditary Mostly males Environmental Past medical issue Symptoms Delay in learning to talk/non-communicative Repeated behaviors Unusual attachment to object or routine Anxiety Depression A Treatment Options Medication Coping skills Specialized therapy Behavioral management Anxiety management B C C D A. B. C. D




19 Infection in the meninges surrounding the brain Causes & Risk Factors Bacteria or viral infection Drug allergies Fungi or parasites Chemical irritations Tumors Symptoms Nausea & vomiting Sensitivity to light Fever & chills Mental status change Stiff neck Severe headache Irritation Treatment Options Bacterial - hospitalization Antibiotics Medication to treat symptoms Prevention with vaccination A B D C A. B. C D.




20 Autoimmune disease that damages the myelin sheath Causes & Risk Factors Cause not well understood Hereditary Family history Diagnosed between Nerve damage caused by inflammation Possibly viral infection Environmental factors Symptoms Vary depending on location & severity Muscle weakness, spasms, tremors, & numbness Incontinence & frequent urination Constipation & stool leakage Vision & hearing loss Depression, dizziness, fatigue, & memory loss Treatment Options No known cure Medications to slow disease progress Steroid treatments Physical therapy Assistive devices Healthy lifestyle choices A B C D C A. B. C. D




21 Damage to the spinal cord Causes & Risk Factors Symptoms Treatment Options Direct injury or disease Assault, fall, accident Weakened vertebral column Fluid build-up around spinal cord Most common in men ages A Weakness Loss of feeling below damaged site Spastic muscles Loss of bladder & bowel control Pain and/or numbness Paralysis Completely severed spinal cord cannot be cured Medication to reduce swelling Surgery Bed rest Spinal traction Physical therapy B C C D A. C B. C D.
22 !.28 s.28 s.28 s.28 s.28 s.28 s.27 s.27 s.27 s.27 s.27 s.27 s.26 s.26 s.26 s.26 s.26 s.26 s.25 s.25 s.25 s.25 s.25 s.25 s.24 s.24 s.24 s.24 s.24 s.24 s.23 s.23 s.23 s.23 s.23 s.23 s.22 s.22 s.22 s.22 s.22 s.22 s.21 s.21 s.21 s.21 s.21 s.21 s.20 s.20 s.20 s.20 s.20 s.20 s.19 s.19 s.19 s.19 s.19 s.19 s.18 s.18 s.18 s.18 s.18 s.18 s.17 s.17 s.17 s.17 s.17 s.17 s.16 s.16 s.16 s.16 s.16 s.16 s.15 s.15 s.15 s.15 s.15 s.15 s.14 s.14 s.14 s.14 s.14 s.14 s.13 s.13 s.13 s.13 s.13 s.13 s.12 s.12 s.12 s.12 s.12 s.12 s.11 s.11 s.11 s.11 s.11 s.11 s.10 s.10 s.10 s.10 s.10 s.10 s.09 s.09 s.09 s.09 s.09 s.09 s.08 s.08 s.08 s.08 s.08 s.08 s.07 s.07 s.07 s.07 s.07 s.07 s.06 s.06 s.06 s.06 s.06 s.06 s.05 s.05 s.05 s.05 s.05 s.05 s.04. s.04. s.04. s.04. s.04. s.04. s! 407
23 408!
NEW PATIENT INFORMATION FORM
 NEW PATIENT INFORMATION FORM Name: LAST FIRST MIDDLE Date of Birth: Sex: Marital Status: SS Number: Address: City: State: Zip Phone: Home Cell Work Email: Communication Preference: Patient Portal Phone
NEW PATIENT INFORMATION FORM Name: LAST FIRST MIDDLE Date of Birth: Sex: Marital Status: SS Number: Address: City: State: Zip Phone: Home Cell Work Email: Communication Preference: Patient Portal Phone
Vascular Disorders. Nervous System Disorders (Part B-1) Module 8 -Chapter 14. Cerebrovascular disease S/S 1/9/2013
 Module 8 -Chapter 14. Cerebrovascular disease S/S 1/9/2013") Nervous System Disorders (Part B-1) Module 8 -Chapter 14 Overview ACUTE NEUROLOGIC DISORDERS Vascular Disorders Infections/Inflammation/Toxins Metabolic, Endocrinologic, Nutritional, Toxic Neoplastic Traumatic
Nervous System Disorders (Part B-1) Module 8 -Chapter 14 Overview ACUTE NEUROLOGIC DISORDERS Vascular Disorders Infections/Inflammation/Toxins Metabolic, Endocrinologic, Nutritional, Toxic Neoplastic Traumatic
HISTORY OF PRESENT ILLNESS A. TELL US ABOUT YOUR PAIN PROBLEM
 1 UT Health Austin Comprehensive Pain Management New Patient Questionnaire Thank you for scheduling a visit with the Comprehensive Pain Management Care Team. The responses you provide to these questions
1 UT Health Austin Comprehensive Pain Management New Patient Questionnaire Thank you for scheduling a visit with the Comprehensive Pain Management Care Team. The responses you provide to these questions
New Patient Pain Evaluation
 New Patient Pain Evaluation Name: Date: Using the following symbols, mark the areas of the body diagrams which are affected by your pain: \\ = Stabbing * = Electrical X = Aching N = Numbness 0 = Dull S
New Patient Pain Evaluation Name: Date: Using the following symbols, mark the areas of the body diagrams which are affected by your pain: \\ = Stabbing * = Electrical X = Aching N = Numbness 0 = Dull S
CENTRAL CARE POLICY SYMPTOMS OF ILLNESS. Policy: Consumers will be observed for symptoms of physical problems, distress, pain, or unusual behaviors.
 Page 1 of 5 CENTRAL CARE POLICY SYMPTOMS OF ILLNESS SUBJECT: SYMPTOMS OF ILLNESS ANNUAL REVIEW MONTH: June RESPONSIBLE FOR REVIEW: Director of Central Care LAST REVISION DATE: June 2009 Policy: Consumers
Page 1 of 5 CENTRAL CARE POLICY SYMPTOMS OF ILLNESS SUBJECT: SYMPTOMS OF ILLNESS ANNUAL REVIEW MONTH: June RESPONSIBLE FOR REVIEW: Director of Central Care LAST REVISION DATE: June 2009 Policy: Consumers
PERSONAL MEDICAL AND FAMILY HISTORY Please check applicable boxes.
 Name: DOB: PERSONAL MEDICAL AND FAMILY HISTORY Please check applicable boxes. TOBACCO USE: Quit Date Cigarettes Packs/Day Number of years smoked Pipe/Cigar Smokeless Tobacco Electronic or E-cigarette Secondhand
Name: DOB: PERSONAL MEDICAL AND FAMILY HISTORY Please check applicable boxes. TOBACCO USE: Quit Date Cigarettes Packs/Day Number of years smoked Pipe/Cigar Smokeless Tobacco Electronic or E-cigarette Secondhand
The Limits of Harm Reduction? Neil McKeganey Centre for Substance Use Research West of Scotland Science Park Glasgow Scotland
 The Limits of Harm Reduction? Neil McKeganey Centre for Substance Use Research West of Scotland Science Park Glasgow Scotland Principle of Harm Reduction First Do No Harm Hippocratic Oath I will use treatment
The Limits of Harm Reduction? Neil McKeganey Centre for Substance Use Research West of Scotland Science Park Glasgow Scotland Principle of Harm Reduction First Do No Harm Hippocratic Oath I will use treatment
MULTIPLE SCLEROSIS INTRODUCTION OBJECTIVES. When the student has finished this module, he/she will be able to:
 MULTIPLE SCLEROSIS INTRODUCTION Multiple sclerosis (MS) is a chronic disease of the nervous system. Multiple sclerosis causes inflammation and damage to the protective coatings in the brain and the nerves.
MULTIPLE SCLEROSIS INTRODUCTION Multiple sclerosis (MS) is a chronic disease of the nervous system. Multiple sclerosis causes inflammation and damage to the protective coatings in the brain and the nerves.
Corinna Mosher, M.D. A Medical Corporation 415 E. Rolling Oaks Drive Suite #280 Thousand Oaks, CA (805) Fax (805)
 Fax (805)") Patient Registration: Corinna Mosher, M.D. A Medical Corporation 415 E. Rolling Oaks Drive Suite #280 Thousand Oaks, CA 91361 (805) 496-8522 Fax (805) 496-0469 Last Name: First Name: MI: Address: City:
Patient Registration: Corinna Mosher, M.D. A Medical Corporation 415 E. Rolling Oaks Drive Suite #280 Thousand Oaks, CA 91361 (805) 496-8522 Fax (805) 496-0469 Last Name: First Name: MI: Address: City:
B G C F
 D E I A B G H C F http://2.bp.blogspot.com/_hhudkwzdma4/s1hz6-trldi/aaaaaaaaax4/isdfm81zqcw/s400/blood+vesssel.jpg 495 D D E F G J L M B A C H I K N O P Q R S T U V W X Y 496 Z http://antranik.org/wp-content/uploads/2011/12/gross-anatomy-of-the-heart-anterior-view.jpg
D E I A B G H C F http://2.bp.blogspot.com/_hhudkwzdma4/s1hz6-trldi/aaaaaaaaax4/isdfm81zqcw/s400/blood+vesssel.jpg 495 D D E F G J L M B A C H I K N O P Q R S T U V W X Y 496 Z http://antranik.org/wp-content/uploads/2011/12/gross-anatomy-of-the-heart-anterior-view.jpg
WELCOME TO THE NORTHSHORE UNIVERSITY HEALTHSYSTEM SLEEP CENTERS
 WELCOME TO THE NORTHSHORE UNIVERSITY HEALTHSYSTEM SLEEP CENTERS Prior to your office visit, we request that you complete this questionnaire. It asks questions not only about your sleeping habits and behavior
WELCOME TO THE NORTHSHORE UNIVERSITY HEALTHSYSTEM SLEEP CENTERS Prior to your office visit, we request that you complete this questionnaire. It asks questions not only about your sleeping habits and behavior
Multiple Sclerosis , The Patient Education Institute, Inc. nr Last reviewed: 04/17/2017 1
 Multiple Sclerosis Introduction Multiple sclerosis, or MS, is a disease of the brain and spinal cord. Most patients with multiple sclerosis are able to lead a very functional life. However, MS causes a
Multiple Sclerosis Introduction Multiple sclerosis, or MS, is a disease of the brain and spinal cord. Most patients with multiple sclerosis are able to lead a very functional life. However, MS causes a
New Patient Form. Patient Demographics. Emergency Information. Employment Information. Page 1 of 7. Family Health Chiropractic Care
 Page 1 of 7 Patient Demographics First Name* Last Name* Date Of Birth* Home Phone* Mobile Phone Phone Gender* Email Preferred Communication Street Address 1* Street Addresss 2 Zip* City* State* Emergency
Page 1 of 7 Patient Demographics First Name* Last Name* Date Of Birth* Home Phone* Mobile Phone Phone Gender* Email Preferred Communication Street Address 1* Street Addresss 2 Zip* City* State* Emergency
Questionnaire for Lipedema Patients
 Questionnaire for Lipedema Patients Name Date of diagnosis Date Name of physician making diagnosis Do you also have lymphedema? What areas of the body are affected? Outside of thighs Inner thighs Knees
Questionnaire for Lipedema Patients Name Date of diagnosis Date Name of physician making diagnosis Do you also have lymphedema? What areas of the body are affected? Outside of thighs Inner thighs Knees
Health History Questionaire
 Patient DOB: Patient Name: Date: Health History Questionaire Who referred your consultation? If no one referred you, how did you hear about us? Who is your primary care physician? Have you ever seen a
Patient DOB: Patient Name: Date: Health History Questionaire Who referred your consultation? If no one referred you, how did you hear about us? Who is your primary care physician? Have you ever seen a
The Rehabilitation Institute Cancer Rehabilitation
 DO NOT DRILL The Rehabilitation Institute Cancer Rehabilitation STAR Patient Intake Form Your Name: Date: Your date of birth: Age: Who referred you (if a healthcare provider, please provide address)? Doctors
DO NOT DRILL The Rehabilitation Institute Cancer Rehabilitation STAR Patient Intake Form Your Name: Date: Your date of birth: Age: Who referred you (if a healthcare provider, please provide address)? Doctors
How It Spreads Symptoms Can Include Complications
 OUR BEST SHOT: The Importance of Vaccines for Older Adults VACCINES QUICK GUIDE TO VACCINATION FOR ADULTS AGES 60+ Vaccines are an important step in protecting your health and the health of your family.
OUR BEST SHOT: The Importance of Vaccines for Older Adults VACCINES QUICK GUIDE TO VACCINATION FOR ADULTS AGES 60+ Vaccines are an important step in protecting your health and the health of your family.
PATIENT REGISTRATION
 P Account# PATIENT REGISTRATION Please answer all questions completely. PAYMENT IS EXPECTED WHEN SERVICES ARE RENDERED Date New Update Name Date of Birth Male Last First Middle Female Home Address City/State/Zip
P Account# PATIENT REGISTRATION Please answer all questions completely. PAYMENT IS EXPECTED WHEN SERVICES ARE RENDERED Date New Update Name Date of Birth Male Last First Middle Female Home Address City/State/Zip
Resources: Types of dementia
 1/5 Dementia is an umbrella term for a number of progressive conditions affecting the functioning of the brain. Different types of dementia have different causes. There are a great number of rare forms.
1/5 Dementia is an umbrella term for a number of progressive conditions affecting the functioning of the brain. Different types of dementia have different causes. There are a great number of rare forms.
PHARMA DYNAMICS CLOPIDOGREL 75 mg PATIENT INFORMATION LEAFLET
 PROPOSED PATIENT INFORMATION LEAFLET FOR PHARMA DYNAMICS CLOPIDOGREL 75 mg PATIENT INFORMATION LEAFLET SCHEDULING STATUS S3 PROPRIETARY NAME, STRENGTH AND PHARMACEUTICAL FORM PHARMA DYNAMICS CLOPIDOGREL
PROPOSED PATIENT INFORMATION LEAFLET FOR PHARMA DYNAMICS CLOPIDOGREL 75 mg PATIENT INFORMATION LEAFLET SCHEDULING STATUS S3 PROPRIETARY NAME, STRENGTH AND PHARMACEUTICAL FORM PHARMA DYNAMICS CLOPIDOGREL
HEALTH INFORMATION FORM
 #102, 506-71 Ave SW Calgary AB T2V 4V4 Ph 587.352.9199 Fax 1.888.501.1724 info@fullcirclecalgary.ca www.fullcirclecalgary.ca Part 1: BASIC INFORMATION HEALTH INFORMATION FORM Name: Date: Address: City:
#102, 506-71 Ave SW Calgary AB T2V 4V4 Ph 587.352.9199 Fax 1.888.501.1724 info@fullcirclecalgary.ca www.fullcirclecalgary.ca Part 1: BASIC INFORMATION HEALTH INFORMATION FORM Name: Date: Address: City:
Multiple Sclerosis. Brain Spinal Cord. Peripheral Nerves
 Multiple Sclerosis Introduction Multiple sclerosis, or MS, is a disease of the brain and spinal cord. It affects about 400,000 Americans at any one time. Most patients with multiple sclerosis are able
Multiple Sclerosis Introduction Multiple sclerosis, or MS, is a disease of the brain and spinal cord. It affects about 400,000 Americans at any one time. Most patients with multiple sclerosis are able
Address Street Address City State Zip Code. Address Street Address City State Zip Code
 Male Initial Visit Intake Form PATIENT INFORMATION Today s Date Last Name Mid Initial First Name Date of Birth Address Home Phone Social Security Number Street Address City State Zip Code Cell Phone E-mail
Male Initial Visit Intake Form PATIENT INFORMATION Today s Date Last Name Mid Initial First Name Date of Birth Address Home Phone Social Security Number Street Address City State Zip Code Cell Phone E-mail
Amarillo Surgical Group Doctor: Date:
 Office Visit Information (General Surgery) Amarillo Surgical Group Doctor: Date: Patient s Information Name: Last First Middle Social Security #: Date of Birth: Age Gender: [ Male / Female ] Marital Status:
Office Visit Information (General Surgery) Amarillo Surgical Group Doctor: Date: Patient s Information Name: Last First Middle Social Security #: Date of Birth: Age Gender: [ Male / Female ] Marital Status:
Headache Follow-up Visit Form
 !1 Headache Follow-up Visit Form We will be unable to see you unless this form is completely filled out. We appreciate your thoroughness. Name DOB Age Today s Date Referring doctor: Primary doctor: Neurologist:
!1 Headache Follow-up Visit Form We will be unable to see you unless this form is completely filled out. We appreciate your thoroughness. Name DOB Age Today s Date Referring doctor: Primary doctor: Neurologist:
Karl McManus Foundation Representing the Australian Lyme Disease Community Symptoms Monitoring Chart
 Name Diagnosis Date Pathogens Present Date GENERAL Fever Chills Night sweats Fatigue Poor Stamina Weight Loss/Gain Gernalised Pain Migratory Pain Shooting Pain Daytime Napping Menstrual Irregularity Milk
Name Diagnosis Date Pathogens Present Date GENERAL Fever Chills Night sweats Fatigue Poor Stamina Weight Loss/Gain Gernalised Pain Migratory Pain Shooting Pain Daytime Napping Menstrual Irregularity Milk
Cascadia Chiropractic Centre
 Name: Cascadia Chiropractic Centre New Patient Information & Clinical Record Date: Date of Birth: Your age: Care Card #: Address: City/Prov: Postal Code: Phone: Cell: Work Phone: E-mail Address: Marital
Name: Cascadia Chiropractic Centre New Patient Information & Clinical Record Date: Date of Birth: Your age: Care Card #: Address: City/Prov: Postal Code: Phone: Cell: Work Phone: E-mail Address: Marital
Address: Yes! I would like to receive your Monday Morning Health Tips.
 Welcome to our Office! New Patient Intake Form Date Name Preferred Name Birthdate (D/M/Y) Age Sex F M Address Unit City Province Postal Code Home # Cell # May we contact you at work? Yes No Work # Extension
Welcome to our Office! New Patient Intake Form Date Name Preferred Name Birthdate (D/M/Y) Age Sex F M Address Unit City Province Postal Code Home # Cell # May we contact you at work? Yes No Work # Extension
What is your occupation? Company Name Do you have extended healthcare benefits? Yes No Benefits are personal or from work
 Welcome to our Office! New Patient Intake Form Date Name Preferred Name Birthdate (D/M/Y) Age Sex F M Address Unit City Province Postal Code Home # Cell # May we contact you at work? Yes No Work # Extension
Welcome to our Office! New Patient Intake Form Date Name Preferred Name Birthdate (D/M/Y) Age Sex F M Address Unit City Province Postal Code Home # Cell # May we contact you at work? Yes No Work # Extension
Interventional Pain Medicine. P. Tennent Slack, M.D. Dr. Greg Jackson, M.D. Ben Fleming, PA-C
 Interventional Pain Medicine P. Tennent Slack, M.D. Dr. Greg Jackson, M.D. Ben Fleming, PA-C Gainesville Braselton Medical Park 1, Suite 300 Medical Plaza B, Suite 402 1315 Jesse Jewell Parkway 1404 River
Interventional Pain Medicine P. Tennent Slack, M.D. Dr. Greg Jackson, M.D. Ben Fleming, PA-C Gainesville Braselton Medical Park 1, Suite 300 Medical Plaza B, Suite 402 1315 Jesse Jewell Parkway 1404 River
WELCOME TO FALLS CHIROPRACTIC AND INJURY!
 WELCOME TO FALLS CHIROPRACTIC AND INJURY! PATIENT INFORMATION (Most of the information below is required for insurance purposes) DATE: / / FIRST NAME: M.I.: LAST NAME: DATE OF BIRTH: / / CALLED NAME /
WELCOME TO FALLS CHIROPRACTIC AND INJURY! PATIENT INFORMATION (Most of the information below is required for insurance purposes) DATE: / / FIRST NAME: M.I.: LAST NAME: DATE OF BIRTH: / / CALLED NAME /
Angiostrongyliasis - Rat Lungworm Disease
 Hawaii Island Rat Lungworm Working Group Daniel K. Inouye College of Pharmacy University of Hawaii, Hilo Rat Lungworm IPM RLWL-10 Angiostrongyliasis - Rat Lungworm Disease Standards Addressed: Life Science
Hawaii Island Rat Lungworm Working Group Daniel K. Inouye College of Pharmacy University of Hawaii, Hilo Rat Lungworm IPM RLWL-10 Angiostrongyliasis - Rat Lungworm Disease Standards Addressed: Life Science
Extended Health Care Company Do you need any help retaining information about your health insurance coverage? Yes No
 PATIENT ENTRANCE FORM Date Circle: Male Female Name Birth Date (dd/mm/yy) Age Address Apt # City Province Postal Code Home # Cell # Work # E-MAIL Occupation Employer Name of Emergency Contact Contact #
PATIENT ENTRANCE FORM Date Circle: Male Female Name Birth Date (dd/mm/yy) Age Address Apt # City Province Postal Code Home # Cell # Work # E-MAIL Occupation Employer Name of Emergency Contact Contact #
Creve Coeur Family Medicine, LLC
 Creve Coeur Family Medicine, LLC Patient Name: Date of Birth: Medication List Medication Name (Over the counter medications too) Strength/ Dose (mg) Number of pills per dose Number of times per day Personal
Creve Coeur Family Medicine, LLC Patient Name: Date of Birth: Medication List Medication Name (Over the counter medications too) Strength/ Dose (mg) Number of pills per dose Number of times per day Personal
Central nervous system
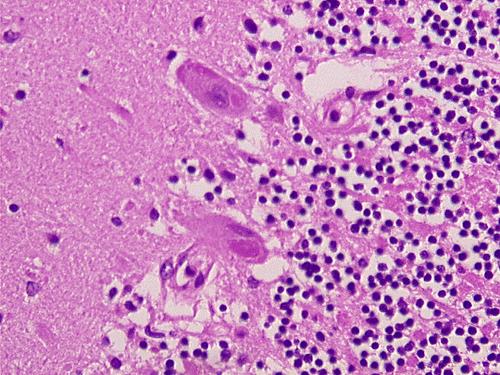
 Central nervous system By Dr. Mohsen Dashti Clinical Medicine & Pathology 316 7 th Lecture Lecture outline Review of structure & function. Symptoms, signs & tests. Specific diseases. Review of structure
Central nervous system By Dr. Mohsen Dashti Clinical Medicine & Pathology 316 7 th Lecture Lecture outline Review of structure & function. Symptoms, signs & tests. Specific diseases. Review of structure
Biology 3201 Nervous System # 7: Nervous System Disorders
 Biology 3201 Nervous System # 7: Nervous System Disorders Alzheimer's Disease first identified by German physician, Alois Alzheimer, in 1906 most common neurodegenerative disease two thirds of cases of
Biology 3201 Nervous System # 7: Nervous System Disorders Alzheimer's Disease first identified by German physician, Alois Alzheimer, in 1906 most common neurodegenerative disease two thirds of cases of
YOUR GUIDE TO TECENTRIQ (atezolizumab) non-small cell lung cancer (NSCLC)
 non-small cell lung cancer (NSCLC)") YOUR GUIDE TO TECENTRIQ (atezolizumab) For previouslytreated advanced non-small cell lung cancer (NSCLC) ABOUT THIS BOOKLET This booklet is for people with advanced non-small cell lung cancer (NSCLC) who
YOUR GUIDE TO TECENTRIQ (atezolizumab) For previouslytreated advanced non-small cell lung cancer (NSCLC) ABOUT THIS BOOKLET This booklet is for people with advanced non-small cell lung cancer (NSCLC) who
E X P L A I N I N G STROKE
 EXPLAINING STROKE Introduction Explaining Stroke is a practical step-by-step booklet that explains how a stroke happens, different types of stroke and how to prevent a stroke. Many people think a stroke
EXPLAINING STROKE Introduction Explaining Stroke is a practical step-by-step booklet that explains how a stroke happens, different types of stroke and how to prevent a stroke. Many people think a stroke
Discussing TECENTRIQ (atezolizumab) with your healthcare team
 with your healthcare team") Discussing TECENTRIQ (atezolizumab) with your healthcare team What is TECENTRIQ? TECENTRIQ is a prescription medicine used to treat: a type of lung cancer called non-small cell lung cancer (NSCLC). TECENTRIQ
Discussing TECENTRIQ (atezolizumab) with your healthcare team What is TECENTRIQ? TECENTRIQ is a prescription medicine used to treat: a type of lung cancer called non-small cell lung cancer (NSCLC). TECENTRIQ
Address City State Zip. Home Phone Cell Work. (For SHPT use only) Emergency Contact Phone
 Emergency Contact Phone") Somerset Hills Physical Therapy, PC 180 Mount Airy Road, Suite 103 Basking Ridge, NJ 07920 Phone (908) 766-1407 Fax (908) 953-8454 wwwsomersethillsptcom Patient Information: Name Sex M F Date of Birth
Somerset Hills Physical Therapy, PC 180 Mount Airy Road, Suite 103 Basking Ridge, NJ 07920 Phone (908) 766-1407 Fax (908) 953-8454 wwwsomersethillsptcom Patient Information: Name Sex M F Date of Birth
Please answer all questions in blue or black ink by filling in the blank or circling. SOCIAL HISTORY
 PATIENT QUESTIONNAIRE / ASSESSMENT Endocrinology Form Please answer all questions in blue or black ink by filling in the blank or circling. SOCIAL HISTORY Date Phone (H) (W) (C) Age Male Female Marital
PATIENT QUESTIONNAIRE / ASSESSMENT Endocrinology Form Please answer all questions in blue or black ink by filling in the blank or circling. SOCIAL HISTORY Date Phone (H) (W) (C) Age Male Female Marital
Patient Name: Date of Birth: Preferred Pharmacy: (name/location/phone #)
") Patient Name: Date of Birth: Referring Doctor: Primary Care Dr: Preferred Pharmacy: (name/location/phone #) CURRENT MEDICATIONS: Please list all Medication Dose Frequency 1 2 3 4 5 6 7 8 9 10 11 12 13
Patient Name: Date of Birth: Referring Doctor: Primary Care Dr: Preferred Pharmacy: (name/location/phone #) CURRENT MEDICATIONS: Please list all Medication Dose Frequency 1 2 3 4 5 6 7 8 9 10 11 12 13
Multiple Sclerosis. What is multiple sclerosis? What is the cause? What are the symptoms?
 What is multiple sclerosis? Multiple Sclerosis Multiple sclerosis (MS) is a disease of the central nervous system (the brain and spinal cord). Many people with multiple sclerosis are only mildly affected
What is multiple sclerosis? Multiple Sclerosis Multiple sclerosis (MS) is a disease of the central nervous system (the brain and spinal cord). Many people with multiple sclerosis are only mildly affected
HEALTH INFORMATION FORM
 #102, 506-71 Ave SW Calgary AB T2V 4V4 Ph 587.352.9199 Fax 1.888.501.1724 info@fullcirclecalgary.ca www.fullcirclecalgary.ca Part 1: BASIC INFORMATION HEALTH INFORMATION FORM Name: Date: Address: City:
#102, 506-71 Ave SW Calgary AB T2V 4V4 Ph 587.352.9199 Fax 1.888.501.1724 info@fullcirclecalgary.ca www.fullcirclecalgary.ca Part 1: BASIC INFORMATION HEALTH INFORMATION FORM Name: Date: Address: City:
Women s and Men s Health Intake Form Comprehensive Physical Therapy Center
 Name: (Last, First) DOB: Date: Age: Referring Physician: Next Physician Appointment: Today s visit: What is the main reason you came to the office today? When did it start? What treatments have you had
Name: (Last, First) DOB: Date: Age: Referring Physician: Next Physician Appointment: Today s visit: What is the main reason you came to the office today? When did it start? What treatments have you had
Form.NewPatientHstory_PrecisionEndoRev Page 1 of 5
 Patient s Name (First, Middle, Last): Address: City: State: Zip Code: Email: Main Contact#: Alternate#: Work#: Date of Birth: / / Sex: Male Female SS# (optional): Marital Status : Single Married Divorced
Patient s Name (First, Middle, Last): Address: City: State: Zip Code: Email: Main Contact#: Alternate#: Work#: Date of Birth: / / Sex: Male Female SS# (optional): Marital Status : Single Married Divorced
CONSULTATION ADMITTANCE FORM
 CONSULTATION ADMITTANCE FORM Last Name: First Name: Address: City Postal Code: Home Phone: Work Phone: Age: Birth date (dd/mm/yr): Sex: M / F Height Weight Occupation: Alberta Health Care #: PLEASE CHECK
CONSULTATION ADMITTANCE FORM Last Name: First Name: Address: City Postal Code: Home Phone: Work Phone: Age: Birth date (dd/mm/yr): Sex: M / F Height Weight Occupation: Alberta Health Care #: PLEASE CHECK
Adult Health Questionnaire
 Health for Life Chiropractic At Cloverdale Mall Unit #143-250 The East Mall Etobicoke, ON, M9B 3Y8 416-232-1822 416-232-0060 Dr. Chrystopher Sly B.Sc, D.C. Dr. Jesse Cracknell B.A., D.C. Adult Health Questionnaire
Health for Life Chiropractic At Cloverdale Mall Unit #143-250 The East Mall Etobicoke, ON, M9B 3Y8 416-232-1822 416-232-0060 Dr. Chrystopher Sly B.Sc, D.C. Dr. Jesse Cracknell B.A., D.C. Adult Health Questionnaire
Last Name First Name Middle Name MRN
 Dr. Byers Dr. Su Dr. Sponzilli Lisa Elvin, NP Spine Center New Patient Form Last Name First Name Middle Name MRN This form is used to gather information so that my doctor can maximize the time used to
Dr. Byers Dr. Su Dr. Sponzilli Lisa Elvin, NP Spine Center New Patient Form Last Name First Name Middle Name MRN This form is used to gather information so that my doctor can maximize the time used to
PATIENT HEALTH QUESTIONNAIRE Radiation Oncology
 REVIEWED DATE / INITIALS Safety: Yes No Are you at risk for falls? Do you have a Pacemaker? Females; Is there a possibility you may be pregnant? Allergies: Yes No If YES, please list medication allergies:
REVIEWED DATE / INITIALS Safety: Yes No Are you at risk for falls? Do you have a Pacemaker? Females; Is there a possibility you may be pregnant? Allergies: Yes No If YES, please list medication allergies:
KEY TO LIFE CHIROPRACTIC
 KEY TO LIFE CHIROPRACTIC REGISTRATION FORM Date Home Phone Cell Phone Email Last Name First Name Middle Initial Street Address City State Zip Sex M F Birth Date Occupation How did you hear about this office?
KEY TO LIFE CHIROPRACTIC REGISTRATION FORM Date Home Phone Cell Phone Email Last Name First Name Middle Initial Street Address City State Zip Sex M F Birth Date Occupation How did you hear about this office?
CONSULTATION ADMITTANCE FORM
 CONSULTATION ADMITTANCE FORM Last Name: _ First Name: Sex: M / F Address: City Postal Code: Home Phone: Work Phone: Cell Phone: Cell Phone Provider: E-mail: Occupation: Marital Status: No. of children:
CONSULTATION ADMITTANCE FORM Last Name: _ First Name: Sex: M / F Address: City Postal Code: Home Phone: Work Phone: Cell Phone: Cell Phone Provider: E-mail: Occupation: Marital Status: No. of children:
REDROCK MEDICAL GROUP INITIAL HISTORY AND PHYSICAL
 REDROCK MEDICAL GROUP INITIAL HISTORY AND PHYSICAL NAME: BIRTH DATE: AGE: SEX: M F OCCUPATION: RACE: WHO REFERRED YOU TO OUR OFFICE? _ WHAT IS YOUR MAIN COMPLAINT? HOW LONG HAS THIS BEEN A PROBLEM? IS
REDROCK MEDICAL GROUP INITIAL HISTORY AND PHYSICAL NAME: BIRTH DATE: AGE: SEX: M F OCCUPATION: RACE: WHO REFERRED YOU TO OUR OFFICE? _ WHAT IS YOUR MAIN COMPLAINT? HOW LONG HAS THIS BEEN A PROBLEM? IS
Patient Name: Date of Birth: Patient Name: DOB: Patient Guardian/Representative: How old are you. Handed: Right Left Ambidextrous Male
 Patient Name: Welcome to Cerebrum Health Centers. Carefully complete all of the following health history questionnaires. The accuracy of your answers will help us better diagnose and treat your condition.
Patient Name: Welcome to Cerebrum Health Centers. Carefully complete all of the following health history questionnaires. The accuracy of your answers will help us better diagnose and treat your condition.
Please have your health insurance card(s), a valid picture ID, and any applicable copayment ready when you check-in.
, a valid picture ID, and any applicable copayment ready when you check-in.") Please have your health insurance card(s), a valid picture ID, and any applicable copayment ready when you check-in. We have enclosed a questionnaire for you to complete and bring to the visit. Please
Please have your health insurance card(s), a valid picture ID, and any applicable copayment ready when you check-in. We have enclosed a questionnaire for you to complete and bring to the visit. Please
DEEP BRAIN STIMULATION SURGICAL CANDIDACY EVALUATION FORM
 Name: MR#: Date: DEEP BRAIN STIMULATION SURGICAL CANDIDACY EVALUATION FORM Referring Physician s Name: Primary Care Provider s Name: 1. What was/were your first movement disorder symptoms? What did you
Name: MR#: Date: DEEP BRAIN STIMULATION SURGICAL CANDIDACY EVALUATION FORM Referring Physician s Name: Primary Care Provider s Name: 1. What was/were your first movement disorder symptoms? What did you
Sydney Chiropractic, DR. DAVID DUNN
 PERSONAL HISTORY Name: Address: City: Province: Postal Code: Home Phone: Birthdate: Age: Sex: M F # of Children Business/Employer: Business Phone: Type of Work You Do: E-mail: Emergency Contact: Phone
PERSONAL HISTORY Name: Address: City: Province: Postal Code: Home Phone: Birthdate: Age: Sex: M F # of Children Business/Employer: Business Phone: Type of Work You Do: E-mail: Emergency Contact: Phone
WELCOME TO THE MILLER CHIROPRACTIC CLINIC
 WELCOME TO THE MILLER CHIROPRACTIC CLINIC We are pleased that you have chosen to consult us regarding your health. In order to help us evaluate your condition thoroughly, please complete the following
WELCOME TO THE MILLER CHIROPRACTIC CLINIC We are pleased that you have chosen to consult us regarding your health. In order to help us evaluate your condition thoroughly, please complete the following
Laser Vein Center Thomas Wright MD Page 1 of 4
 Demographics Laser Vein Center Thomas Wright MD Page 1 of 4 Patient Name: Address: City, St, Zip Primary Phone: Alternate: DOB: Social Security #: Insurance Information Primary Insurance ID# Group# Subscriber
Demographics Laser Vein Center Thomas Wright MD Page 1 of 4 Patient Name: Address: City, St, Zip Primary Phone: Alternate: DOB: Social Security #: Insurance Information Primary Insurance ID# Group# Subscriber
NEW PATIENT REGISTRATION PLEASE COMPLETE ALL ITEMS ON EACH PAGE. Name (Last, First, M.I.) Address. City State Zip Code. Phone ( ) Work ( ) Cell ( )
 Address. City State Zip Code. Phone ( ) Work ( ) Cell ( )") NEW PATIENT REGISTRATION PLEASE COMPLETE ALL ITEMS ON EACH PAGE Date Name (Last, First, M.I.) Address City State Zip Code Phone ( ) Work ( ) Cell ( ) Date of Birth Age Marital Status SSN Employer Employer
NEW PATIENT REGISTRATION PLEASE COMPLETE ALL ITEMS ON EACH PAGE Date Name (Last, First, M.I.) Address City State Zip Code Phone ( ) Work ( ) Cell ( ) Date of Birth Age Marital Status SSN Employer Employer
Pain Management Questionnaire
 In order to make the most of your visit, we require this form to be completed to the best of your ability and sent to the Pain Management Clinic a copy should be shared with your Primary Care Provider
In order to make the most of your visit, we require this form to be completed to the best of your ability and sent to the Pain Management Clinic a copy should be shared with your Primary Care Provider
Past Surgical History
 Name: DOB: Check All That Apply Past Medical History o Anemia o Aneurysm o Asthma o Bipolar o Bleeding Disorder o Blood Clot o Brain Tumor o Bronchitis o Cancer o Crohn s Disease/Ulcerative Colitis o Depression
Name: DOB: Check All That Apply Past Medical History o Anemia o Aneurysm o Asthma o Bipolar o Bleeding Disorder o Blood Clot o Brain Tumor o Bronchitis o Cancer o Crohn s Disease/Ulcerative Colitis o Depression
Emotional Relationships Social Life Sexually Recreation
 Name Date Address City State Zip Married Single Partner Divorced Widowed Date of Birth SS# Email Work Phone Home Phone Cell Phone Occupation Referred by Emergency Contact Family Physician Contact May we
Name Date Address City State Zip Married Single Partner Divorced Widowed Date of Birth SS# Email Work Phone Home Phone Cell Phone Occupation Referred by Emergency Contact Family Physician Contact May we
Patient Name: Date of Birth:
 Patient Name: Date of Birth: Marital Status: Single Married Divorced Widowed Height: Referring Doctor: Weight: Primary Care Dr.: Preferred Pharmacy:(name/address) ALLERGIES: Do you have any drug allergies?
Patient Name: Date of Birth: Marital Status: Single Married Divorced Widowed Height: Referring Doctor: Weight: Primary Care Dr.: Preferred Pharmacy:(name/address) ALLERGIES: Do you have any drug allergies?
Capital Health Medical Center - Hopewell NEUROSURGICAL-ONCOLOGY Patient History
 Capital Health Medical Center - Hopewell NEUROSURGICAL-ONCOLOGY Patient History Please take a few minutes and complete the following questions before you see the doctors so that we may learn a bit more
Capital Health Medical Center - Hopewell NEUROSURGICAL-ONCOLOGY Patient History Please take a few minutes and complete the following questions before you see the doctors so that we may learn a bit more
The Rehabilitation Institute Cancer Rehabilitation
 DO NOT DRILL The Rehabilitation Institute Cancer Rehabilitation Patient Intake Form Your Name: Date: Your date of birth: Age: Who referred you (if a healthcare provider, please provide address)? Doctors
DO NOT DRILL The Rehabilitation Institute Cancer Rehabilitation Patient Intake Form Your Name: Date: Your date of birth: Age: Who referred you (if a healthcare provider, please provide address)? Doctors
New Patient Questionnaire HIP Adult Reconstruction & Joint Replacement
 New Patient Questionnaire HIP Adult Reconstruction & Joint Replacement Name: DOB: Date: Height: Weight: Age: Chief Complaint Laterality Left Right Both Please describe your symptoms: (Mark all that apply)
New Patient Questionnaire HIP Adult Reconstruction & Joint Replacement Name: DOB: Date: Height: Weight: Age: Chief Complaint Laterality Left Right Both Please describe your symptoms: (Mark all that apply)
Symptom Review (page 1) Name Date
 Name Date") v2.4, 2/13 JonathanTreasure.com Botanical Medicine & Cancer Herb Drug Interactions Herbalism 3.0 Symptom Review (page 1) Name Date INSTRUCTIONS Please read each section below carefully and, after each
v2.4, 2/13 JonathanTreasure.com Botanical Medicine & Cancer Herb Drug Interactions Herbalism 3.0 Symptom Review (page 1) Name Date INSTRUCTIONS Please read each section below carefully and, after each
Brisbin Family Chiropractic
 Information reviewed with patient: Dr. Initials Today s Date Brisbin Family Chiropractic Name: Sex: Male Female Address: City: Postal Code: Home Ph# Work# Ext# Cell# Preferred number (circle one) Home
Information reviewed with patient: Dr. Initials Today s Date Brisbin Family Chiropractic Name: Sex: Male Female Address: City: Postal Code: Home Ph# Work# Ext# Cell# Preferred number (circle one) Home
SECTION OF NEUROSURGERY PATIENT INFORMATION SHEET
 SECTION OF NEUROSURGERY PATIENT INFORMATION SHEET EC#: (for office use only) Patient s Name: Today s Date: Age: Date of Birth: Height: Weight: Physician you are seeing today: Marital Status: Married Work
SECTION OF NEUROSURGERY PATIENT INFORMATION SHEET EC#: (for office use only) Patient s Name: Today s Date: Age: Date of Birth: Height: Weight: Physician you are seeing today: Marital Status: Married Work
Name: [Type text] Date of Birth: ENDOCRINOLOGY HEALTH HISTORY. What is the reason for your visit?
![Name: [Type text] Date of Birth: ENDOCRINOLOGY HEALTH HISTORY. What is the reason for your visit?](/thumbs/87/97078208.jpg "Name: [Type text] Date of Birth: ENDOCRINOLOGY HEALTH HISTORY. What is the reason for your visit?") ENDOCRINOLOGY HEALTH HISTORY What is the reason for your visit? MEDICATIONS List current prescription and over-the-counter medications. Also list current vitamin, herbal, and nutritional supplements: MEDICATION/SUPPLEMENT
ENDOCRINOLOGY HEALTH HISTORY What is the reason for your visit? MEDICATIONS List current prescription and over-the-counter medications. Also list current vitamin, herbal, and nutritional supplements: MEDICATION/SUPPLEMENT
New Patient Medical History Form
 New Patient Medical History Form Date: Name: Date of Birth: Address: City: ZIP: Home Phone #: Cell Phone #: Emergency Contact: Relationship: Emergency Contact Phone #: Primary Care Physician: Referring
New Patient Medical History Form Date: Name: Date of Birth: Address: City: ZIP: Home Phone #: Cell Phone #: Emergency Contact: Relationship: Emergency Contact Phone #: Primary Care Physician: Referring
Dr. Gary Malstrom B.Sc.(Hon.), D.C., C.Ac Brant Street, Burlington, Ontario L7R 2J9 (905) Fax (905)
, D.C., C.Ac Brant Street, Burlington, Ontario L7R 2J9 (905) Fax (905)") Dr. Gary Malstrom B.Sc.(Hon.), D.C., C.Ac. Personal History: Name: Address: City: Province: Postal Code: Birth date: day /month /year Age: Sex: M F Home Phone: Business Phone: Cell Phone: E-mail: Health
Dr. Gary Malstrom B.Sc.(Hon.), D.C., C.Ac. Personal History: Name: Address: City: Province: Postal Code: Birth date: day /month /year Age: Sex: M F Home Phone: Business Phone: Cell Phone: E-mail: Health
Health History Intake Form;
 Health History Intake Form; Today s Date: Patient Name: Date of Birth: Age: Previous Primary Care Physician (if any): Phone: Address: Other Physicians involved in your care: Reason for visit today: Allergies
Health History Intake Form; Today s Date: Patient Name: Date of Birth: Age: Previous Primary Care Physician (if any): Phone: Address: Other Physicians involved in your care: Reason for visit today: Allergies
New Patient Documentation. Name: (Last) (First) (Middle) Address: (Street) (Apt#) (City) (State) (Zip) Home Phone: ( ) Cell: ( ) Work: ( )
 (First) (Middle) Address: (Street) (Apt#) (City) (State) (Zip) Home Phone: ( ) Cell: ( ) Work: ( )") New Patient Documentation Name: (Last) (First) (Middle) Address: (Street) (Apt#) (City) (State) (Zip) Home Phone: ( ) Cell: ( ) Work: ( ) Age: Birthdate: E Email: Social: Sex: Male Female Height: Weight:
New Patient Documentation Name: (Last) (First) (Middle) Address: (Street) (Apt#) (City) (State) (Zip) Home Phone: ( ) Cell: ( ) Work: ( ) Age: Birthdate: E Email: Social: Sex: Male Female Height: Weight:
Adult New Patient Intake. Your Health Summary
 Adult New Patient Intake Name Age Birth Date / / Soc. Sec. # - - Home Phone Cell Phone Address: City: State: Zip: Occupation: Email Marital Status: M W D S Spouse s Name: Children # and Ages: Whom may
Adult New Patient Intake Name Age Birth Date / / Soc. Sec. # - - Home Phone Cell Phone Address: City: State: Zip: Occupation: Email Marital Status: M W D S Spouse s Name: Children # and Ages: Whom may
Providence Neurosurgery PATIENT INFORMATION SHEET
 Date: Staff only: Weight: Height: BP: Pain Age Patient Name Date of Birth Street Address City State Zip Code Home Phone Work Phone Cell Phone Right handed Left handed Please mark one Referring Physician
Date: Staff only: Weight: Height: BP: Pain Age Patient Name Date of Birth Street Address City State Zip Code Home Phone Work Phone Cell Phone Right handed Left handed Please mark one Referring Physician
PATIENT HEALTH QUESTIONNAIRE Radiation Oncology
 REVIEWED DATE / INITIALS Safety: Are you at risk for falls? Do you have a Pacemaker? Females; Is there a possibility you may be pregnant? Allergies: If YES, please list medication allergies: Do you have
REVIEWED DATE / INITIALS Safety: Are you at risk for falls? Do you have a Pacemaker? Females; Is there a possibility you may be pregnant? Allergies: If YES, please list medication allergies: Do you have
Child (0-17) New Patient Intake Form. Child s Health Summary
 New Patient Intake Form. Child s Health Summary") Child (0-17) New Patient Intake Form Child s Name Age Birth Date / / Soc. Sec. # - - Parent/Guardian Name: Address: City: State: Zip: Parent/Guardian Email: Parent/Guardian Phone: Whom may we thank for
Child (0-17) New Patient Intake Form Child s Name Age Birth Date / / Soc. Sec. # - - Parent/Guardian Name: Address: City: State: Zip: Parent/Guardian Email: Parent/Guardian Phone: Whom may we thank for
LAKES INTERNAL MEDICINE
 LAKES INTERNAL MEDICINE HEALTH HISTORY QUESTIONNAIRE Please print this and complete and bring to your initial appointment. Today's Date Last Name First Name Middle Initial Date of Birth Male Female Education
LAKES INTERNAL MEDICINE HEALTH HISTORY QUESTIONNAIRE Please print this and complete and bring to your initial appointment. Today's Date Last Name First Name Middle Initial Date of Birth Male Female Education
HISTORY PAPERWORK FOR APPOINTMENTS WITH DAVID A. PROPST, D.O.
 HISTORY PAPERWORK FOR APPOINTMENTS WITH DAVID A. PROPST, D.O. Name: Age: Room Number: Sex: MALE or FEMALE Dominant Hand: RIGHT or LEFT Height Weight Blood pressure HISTORY 1. Did your first symptoms begin
HISTORY PAPERWORK FOR APPOINTMENTS WITH DAVID A. PROPST, D.O. Name: Age: Room Number: Sex: MALE or FEMALE Dominant Hand: RIGHT or LEFT Height Weight Blood pressure HISTORY 1. Did your first symptoms begin
PLEASE COMPLETE ALL SECTIONS OF THIS FORM
 PLEASE COMPLETE ALL SECTIONS OF THIS FORM Patient Name: Date of Birth: Referring Doctor? (Name, telephone number and address) Chief Complaint: Why have you come here? How did it start? What are the symptoms?
PLEASE COMPLETE ALL SECTIONS OF THIS FORM Patient Name: Date of Birth: Referring Doctor? (Name, telephone number and address) Chief Complaint: Why have you come here? How did it start? What are the symptoms?
Patient Name: DOB: Age: Sex: Male Female Height: Weight: Dominant Hand: Right Left HISTORY OF PRESENT ILLNESS
 CAPS PAINCARE Page 1 of 5 Today s : / / SSN (last 4 digits): xxx-xx - Patient Name: DOB: Age: Sex: Male Female Height: Weight: Dominant Hand: Right Left Type of Accident/Injury: Auto Work Personal Injury
CAPS PAINCARE Page 1 of 5 Today s : / / SSN (last 4 digits): xxx-xx - Patient Name: DOB: Age: Sex: Male Female Height: Weight: Dominant Hand: Right Left Type of Accident/Injury: Auto Work Personal Injury
New Patient Packet. Patient Name: DOB: Age: Address: City: State: Zip: Address: City: State: Zip: Name: Address: Phone: Fax:
 New Patient Packet Patient Name: DOB: Age: Sex: Male / Female Height: Weight: PHYSICIAN CARE Primary Care Physician: Address: City: State: Zip: Phone: Fax: Referring Physician (if different from PCP):
New Patient Packet Patient Name: DOB: Age: Sex: Male / Female Height: Weight: PHYSICIAN CARE Primary Care Physician: Address: City: State: Zip: Phone: Fax: Referring Physician (if different from PCP):
MULTI-SYSTEMIC INFECTIOUS DISEASE SYNDROME SYMPTOM QUESTIONNAIRE
 MULTI-SYSTEMIC INFECTIOUS DISEASE SYNDROME SYMPTOM QUESTIONNAIRE SECTION 1: SYMPTOM FREQUENCY SCORE Select the frequency of each of the following symptoms. 0 = None 1 = Mild 2 = Moderate 3 = Severe 1.
MULTI-SYSTEMIC INFECTIOUS DISEASE SYNDROME SYMPTOM QUESTIONNAIRE SECTION 1: SYMPTOM FREQUENCY SCORE Select the frequency of each of the following symptoms. 0 = None 1 = Mild 2 = Moderate 3 = Severe 1.
COMPREHENSIVE HEALTH & WELLNESS PROFILE
 Patient Name DOB COMPREHENSIVE HEALTH & WELLNESS PROFILE The human body is designed to be healthy. Throughout life, events occur which damage your natural health expression. As a full spectrum Chiropractic
Patient Name DOB COMPREHENSIVE HEALTH & WELLNESS PROFILE The human body is designed to be healthy. Throughout life, events occur which damage your natural health expression. As a full spectrum Chiropractic
Personal &Work Information Date: Patient Name: Age: City: State: Zip: Primary Care Physician: PCP Phone:
 Personal &Work Information Date: Patient Name: Age: Birth Date: / / Preferred Name: Gender: Home Phone: Address: Mobile Phone: City: State: Zip: Occupation: Employer: Work Phone: Email: Emergency Contact:
Personal &Work Information Date: Patient Name: Age: Birth Date: / / Preferred Name: Gender: Home Phone: Address: Mobile Phone: City: State: Zip: Occupation: Employer: Work Phone: Email: Emergency Contact:
Cascadia Chiropractic Centre
 Name: Address: Dr. Simpson Leung Cascadia Chiropractic Centre New Patient Information & Clinical Record Date: City: Province: Postal Code: Phone: Cell: Work Phone: Date of Birth: E-mail Address: Care Card
Name: Address: Dr. Simpson Leung Cascadia Chiropractic Centre New Patient Information & Clinical Record Date: City: Province: Postal Code: Phone: Cell: Work Phone: Date of Birth: E-mail Address: Care Card
Labrynthitis. It causes a delicate structure deep inside your ear called the labyrinth to become inflamed, which affects your hearing and balance.
 Labyrinthitis is an inner ear infection. Labrynthitis It causes a delicate structure deep inside your ear called the labyrinth to become inflamed, which affects your hearing and balance. Symptoms of labyrinthitis
Labyrinthitis is an inner ear infection. Labrynthitis It causes a delicate structure deep inside your ear called the labyrinth to become inflamed, which affects your hearing and balance. Symptoms of labyrinthitis
History of Present Problem
 Patient Name: Date: If you are not the patient: Guardian name: Relationship to Patient: Height: Ft In Weight: lbs Age: Birth Date: Dominant Hand: Right Left Shoe Size: Primary Care Physician: Specialists:
Patient Name: Date: If you are not the patient: Guardian name: Relationship to Patient: Height: Ft In Weight: lbs Age: Birth Date: Dominant Hand: Right Left Shoe Size: Primary Care Physician: Specialists:
VCU CENTER FOR SLEEP MEDICINE NEW PATIENT QUESTIONNAIRE
 VCU CENTER FOR SLEEP MEDICINE NEW PATIENT QUESTIONNAIRE Name:_ DOB: MR#: Date: Sex: Age: Height: Referring physician: Primary care physician: What is your primary sleep problem? Please explain any strange
VCU CENTER FOR SLEEP MEDICINE NEW PATIENT QUESTIONNAIRE Name:_ DOB: MR#: Date: Sex: Age: Height: Referring physician: Primary care physician: What is your primary sleep problem? Please explain any strange
Placer Private Physicians: Patient Health Questionnaire [2]
![Placer Private Physicians: Patient Health Questionnaire [2]](/thumbs/87/96006031.jpg "Placer Private Physicians: Patient Health Questionnaire [2]") Dr.Br own 7. Do you feel you eat a healthy diet? 8. Please describe why or why not? 9. Do you exercise regularly? Yes No 10. If yes, what type of exercises and how many days per week? 11. Have you ever
Dr.Br own 7. Do you feel you eat a healthy diet? 8. Please describe why or why not? 9. Do you exercise regularly? Yes No 10. If yes, what type of exercises and how many days per week? 11. Have you ever
Faculty of Clinical Forensic Medicine Committee 1/2018
 Guideline Subject: Clinical Forensic Assessment and Management of Non-Fatal Strangulation Approval Date: January 2018 Review Date: January 2021 Review By: Number: Faculty of Clinical Forensic Medicine
Guideline Subject: Clinical Forensic Assessment and Management of Non-Fatal Strangulation Approval Date: January 2018 Review Date: January 2021 Review By: Number: Faculty of Clinical Forensic Medicine
CECILIA P MARGRET MD PhD MPH Child, Adolescent and Adult Psychiatry NE 24th ST Suite 104, Bellevue WA 98007, Phone / Fax: +1 (425)
") IDENTIFYING INFORMATION PATIENT INFORMATION FORM Patient's Name: DOB: Ethnicity/race: Gender: Primary language if other than English: Address: Phone: Home/ Mobile/ Work Email: Occupation: Marital Status:
IDENTIFYING INFORMATION PATIENT INFORMATION FORM Patient's Name: DOB: Ethnicity/race: Gender: Primary language if other than English: Address: Phone: Home/ Mobile/ Work Email: Occupation: Marital Status:
Osher Center for Integrative Medicine Pediatric Intake Form Name: Date: Date of Birth: Age: Current Pediatrician:
 Pediatric Intake Form Name: Date: Date of Birth: Age: Current Pediatrician: How did you hear about us? What are your goals for this visit? Where would you like to see improvement in your child s health?
Pediatric Intake Form Name: Date: Date of Birth: Age: Current Pediatrician: How did you hear about us? What are your goals for this visit? Where would you like to see improvement in your child s health?
DISORDERS OF THE NERVOUS SYSTEM
 DISORDERS OF THE NERVOUS SYSTEM Bell Work What s your reaction time? Go to this website and check it out: https://www.justpark.com/creative/reaction-timetest/ Read the following brief article and summarize
DISORDERS OF THE NERVOUS SYSTEM Bell Work What s your reaction time? Go to this website and check it out: https://www.justpark.com/creative/reaction-timetest/ Read the following brief article and summarize
Integrative Consult Patient Background Form
 Let Us Know More - So We Can Help Thank you for choosing to schedule an integrative medicine consultation with UC Health. To help us meet your needs during your visit, please take some time to sit in a
Let Us Know More - So We Can Help Thank you for choosing to schedule an integrative medicine consultation with UC Health. To help us meet your needs during your visit, please take some time to sit in a
Understanding Dementia
 Dementia Handbook for Carers Essex Understanding Dementia What is dementia? 1 Summary of dementia symptoms 4 Medication and treatment 5 1 Dementia is the name for several conditions that lead to the progressive
Dementia Handbook for Carers Essex Understanding Dementia What is dementia? 1 Summary of dementia symptoms 4 Medication and treatment 5 1 Dementia is the name for several conditions that lead to the progressive
Bridges Family Wellness PC. New Patient Intake. Bridges Family Wellness Intake Form SE Lake Rd, Suite 102 Milwaukie, OR
 New Patient Intake Bridges Family Wellness Intake Form Full Name: * What is your birthdate? MM/DD/YYYY * What is your gender identity? * Home address: * Cell Phone * Other Phone number(s): Emergency Contact
New Patient Intake Bridges Family Wellness Intake Form Full Name: * What is your birthdate? MM/DD/YYYY * What is your gender identity? * Home address: * Cell Phone * Other Phone number(s): Emergency Contact
New Patient Information
 Geoffrey G Glidden MD PA New Patient Information Name Address City/State/Zip Cell Phone Home Phone DL# SSN# Age of Birth Sex: Male / Female Your employer Occupation Work Phone E-Mail Referring Physician
Geoffrey G Glidden MD PA New Patient Information Name Address City/State/Zip Cell Phone Home Phone DL# SSN# Age of Birth Sex: Male / Female Your employer Occupation Work Phone E-Mail Referring Physician