How to Do the EDSS. Stephen S. Kamin, MD New Jersey Medical School
|
|
|
- Leon West
- 6 years ago
- Views:
Transcription

1 How to Do the EDSS Stephen S. Kamin, MD New Jersey Medical School John F. Kurtzke, MD
2 EDSS Expanded Disability Status Scale Devised by John Kurtzke in the 1960s and modified in the 1980s EDSS Advantages Widely used Provides a single number measure of disability Disadvantages Non-linear Bi-modal distribution Overemphasizes ambulation Minimizes cognition Limited inter-rater reliability Some ambiguities

3 EDSS MS Impairment Scale

4 EDSS vs. MSIS MS Severity Score

5 EDSS NeuroStatus A modification of the original Kurtzke scale by Kappos Eliminates some ambiguities In general use in clinical trials On-line training & certification Basis for this session

6 NeuroStatus NeuroStatus
7 EDSS Components Functional Systems Scores (FS) Disability Status Scores (DSS) Functional Systems Scores Visual Pyramidal Cerebellar Sensory Bowel and Bladder Cerebral Other
8 Visual 0- Normal 1- Disc pallor OR small scotoma OR better than 20/30 2- Worse eye 20/30 to 20/59 3- Large scotoma or moderate field defect OR Worse eye 20/60 to 20/99 4- Marked field defect OR Worse eye 20/100 to 20/200 OR Worse eye 20/60 to 20/99 and better eye < 20/60 Visual 5- Worse eye < 20/200 OR Worse eye 20/100 to 20/200 and better eye < 20/60 6- Worse eye < 20/200 AND Better eye < 20/60
9 Visual 4 worse eye with marked decrease of fields and/or maximal visual acuity (corrected) of 20 / 100 to 20 / 200 ( ); grade 3 plus maximal acuity of better eye of 20 / 60 (0.33) or less 5 worse eye with maximal visual acuity (corrected) less than 20 / 200 (0.1); grade 4 plus maximal acuity of better eye of 20 / 60 (0.33) or less 6 grade 5 plus maximal visual acuity of better eye of 20 / 60 (0.33) or less Vision Corrected Scores Score Corrected score
10 Visual Worse eye Better eye Fields Scotoma Pallor /20 20/20 Absent 1 1 > 20/30 Small Present /30-20/ /60-20/99 Moderate Large defect /100-20/200 Complete hemi /60-20/99 AND 20/ < 20/ /100-20/200 AND 20/ < 20/200 AND 20/60 Question 1 The patient has a left homonymous hemianopsia. Visual acuity is 20/30 in the intact field of both eyes.
11 Question 1 The Corrected Visual FSS is: A. 1 B. 2 C. 3 D. 4 Question 1 The Corrected Visual FSS is: 25% 25% 25% 25% A. 1 B. 2 C. 3 D
12 Visual Worse eye Better eye Fields Scotoma Pallor /20 20/20 Absent 1 1 > 20/30 Small Present /30-20/ /60-20/99 Moderate Large defect /100-20/200 Complete hemi /60-20/99 AND 20/ < 20/ /100-20/200 AND 20/ < 20/200 AND 20/60 Question 2 There is disc pallor of the right eye. The acuity is 20/20 bilaterally.
13 Question 2 The corrected visual FSS is: A. 0 B. 1 C. 2 Question 2 The corrected visual FSS is: A. 0 B. 1 C. 2 33% 33% 33% 0 of
14 Visual Worse eye Better eye Fields Scotoma Pallor /20 20/20 Absent 1 1 > 20/30 Small Present /30-20/ /60-20/99 Moderate Large defect /100-20/200 Complete hemi /60-20/99 AND 20/ < 20/ /100-20/200 AND 20/ < 20/200 AND 20/60 Question 3 The patient is blind in the left eye and has acuity of 20/100 in the right eye.
15 Question 3 The corrected visual FSS is: A. 3 B. 4 C. 5 D. 6 Question 3 The corrected visual FSS is: A. 3 B. 4 C. 5 D. 6
16 Visual Worse eye Better eye Fields Scotoma Pallor /20 20/20 Absent 1 1 > 20/30 Small Present /30-20/ /60-20/99 Moderate Large defect /100-20/200 Complete hemi /60-20/99 AND 20/ < 20/ /100-20/200 AND 20/ < 20/200 AND 20/60 Brainstem 0-Normal 1- Signs only 2- Moderate nystagmus OR moderate EOM impairment OR other mild disability
17 Brainstem 3- Severe nystagmus OR Marked extraocular weakness OR Moderate disability of other cranial nerves Brainstem 4- Marked dysarthria or other marked disability 5- Unable to swallow or speak
18 Brainstem EOM 0- Normal 1- Signs only: subtle and patient without complaints 2- Mild: Subtle and patient aware OR obvious and incomplete but patient unaware 3- Moderate: Obvious, incomplete and patient aware OR complete in one direction 4- Marked: Complete paralysis of >1 direction Brainstem Nystagmus 0- None 1- Signs only or mild (only beyond 30 ) 2- Moderate: at 30 but not in primary position 3- Severe: in primary position or interfering with vision OR complete INO OR oscillopsia
19 Brainstem Trigeminal 0- None 1- Signs only 2- Mild: Detectible (patient aware) 3- Moderate: Impaired sharp/dull OR trigeminal neuralgia in past 24 hours 4- Marked: No discrimination of sharp/dull Brainstem Facial 0- None 1- Signs only 2- Mild: Detectible, patient aware 3- Moderate: Incomplete eye closure or mouth closure with symptoms 4- Marked: Complete palsy
20 Brainstem Hearing 0-No loss 1- Signs only: Decreased finger rub OR lateralizing Weber, patient unaware 2- Mild: 1, but patient aware 3- Moderate: Absent finger rub OR impaired word discrimination 4- Marked: Absent word discrimination Brainstem Dysarthria 0- None 1- Signs only 2- Mild: Clinically detectible 3- Moderate: Impaired comprehensibility 4- Marked: Incomprehensible speech 5- Inability to speak
21 Brainstem Dysphagia 0- None 1- Signs only 2- Mild: Difficulty with liquids 3- Moderate: Difficulty with solids and liquids 4- Marked: Sustained difficulty, requires pureed diet 5- Unable to swallow Brainstem Other Cranial Nerves 0 Normal 1 Signs only 2 Mild: Detectible, patient usually aware 3 Moderate 4 Marked
22 Brainstem Score EOM Nystagmus CN V CN VII Hearing Dysarth ria 0 Dyspha gia 1 Signs only OR Mild Signs only OR Mild Signs only Signs only Signs only Signs only Signs only 2 Mod Mod Mild Mild Mild Mild Mild 3 Marked Severe Mod Mod Mod Mod Mod 4 Marked Marked Marked Marked Marked 5 Unable Unable Question 4 The patient has abduction nystagmus of the left eye but does not complain of diplopia. There is mild loss of sensation on the left side of the face, of which she is not aware.
23 Question 4 The Brainstem FSS is: A. 1 B. 2 C. 3 D. 4 A. 1 B. 2 C. 3 D. 4 Question 4 The Brainstem FSS is: 25% 25% 25% 25%
24 Brainstem Score EOM Nystagmus CN V CN VII Hearing Dysarth ria 0 Dyspha gia 1 Signs only OR Mild Signs only OR Mild Signs only Signs only Signs only Signs only Signs only 2 Mod Mod Mild Mild Mild Mild Mild 3 Marked Severe Mod Mod Mod Mod Mod 4 Marked Marked Marked Marked Marked 5 Unable Unable Question 5 The patient complains of diplopia on far rightward gaze but eye movements are not obviously impaired. There is incomplete closure of the right eye and mild dysarthria which does not impair comprehensibility.
25 Question 5 The brainstem FSS is: A. 1 B. 2 C. 3 D. 4 A. 1 B. 2 C. 3 D. 4 Question 5 The brainstem FSS is: 25% 25% 25% 25%
26 Brainstem Score EOM Nystagmus CN V CN VII Hearing Dysarth ria 0 Dyspha gia 1 Signs only OR Mild Signs only OR Mild Signs only Signs only Signs only Signs only Signs only 2 Mod Mod Mild Mild Mild Mild Mild 3 Marked Severe Mod Mod Mod Mod Mod 4 Marked Marked Marked Marked Marked 5 Unable Unable Question 6 The patient has speech which is difficult to understand. He complains of intermittent choking on both solids and liquids. There is nystagmus in all directions of gaze, but not in primary gaze.
27 Question 6 The brainstem FSS is: A. 1 B. 2 C. 3 D. 4 A. 1 B. 2 C. 3 D. 4 Question 6 The brainstem FSS is: 25% 25% 25% 25%
28 Brainstem Score EOM Nystagmus CN V CN VII Hearing Dysarth ria 0 Dyspha gia 1 Signs only OR Mild Signs only OR Mild Signs only Signs only Signs only Signs only Signs only 2 Mod Mod Mild Mild Mild Mild Mild 3 Marked Severe Mod Mod Mod Mod Mod 4 Marked Marked Marked Marked Marked 5 Unable Unable Pyramidal 0- Normal 1- Abnormal signs only (hyperreflexia, Babinski sign) 2- Minimal disability- fatigability OR reduced performance OR 4/5 in one or 2 muscle groups 3- Mild to moderate paraparesis or hemiparesis (usually 4/5 in > 2 muscle groups) OR 3/5 in 1 or 2 muscle groups OR severe monoparesis (< 2/5 in 1 group)
29 Pyramidal 4- Marked paraparesis or hemiparesis or moderate quadriparesis 3/5 in 3 or 4 limbs 2/5 in 2 limbs 1/5 in 1 limb 5- Paraplegia, hemiplegia or marked quadriparesis < 2/5 in 3 or 4 limbs 1/5 in at least 2 limbs 6- Quadriplegia Problems Pyramidal Muscle groups versus limbs Best interpretation: muscle groups = limbs (see rating of 3) But NOT for rating of 2
30 Pyramidal 1 limb 2 limbs 3 limbs 4 limbs 0 Normal 1 Signs only 2 4/5 3 2 or 3/5 3/5 4/5 4/5 4 0 or 1/5 2/5 3/5 3/5 5 0 or 1/5 2/5 2/5 6 0 or 1/5 Question 7 Strength is 4/5 in the right deltoids and right triceps. All other muscle groups are 5/5.
31 Question 7 The Pyramidal FSS is: A. 2 B. 3 C. 4 D. 5 A. 2 B. 3 C. 4 D. 5 Question 7 The Pyramidal FSS is: 25% 25% 25% 25%
32 Pyramidal 1 limb 2 limbs 3 limbs 4 limbs 0 Normal 1 Signs only 2 4/5 3 2 or 3/5 3/5 4/5 4/5 4 0 or 1/5 2/5 3/5 3/5 5 0 or 1/5 2/5 2/5 6 0 or 1/5 Question 8 Strength on the right is deltoids 3/5, biceps 4/5, triceps 3/5, wrist extensors 4/5, iliopsoas 2/5, hamstrings 3/5, anterior tibials 3/5. All other groups are 5/5.
33 Question 8 The Pyramidal FSS is: A. 2 B. 3 C. 4 D. 5 A. 2 B. 3 C. 4 D. 5 Question 8 The Pyramidal FSS is: 25% 25% 25% 25%
34 Pyramidal 1 limb 2 limbs 3 limbs 4 limbs 0 Normal 1 Signs only 2 4/5 3 2 or 3/5 3/5 4/5 4/5 4 0 or 1/5 2/5 3/5 3/5 5 0 or 1/5 2/5 2/5 6 0 or 1/5 Question 9 The strength in the left arm is deltoid 3/5, triceps 4/5, wrist extensors 4/5. In the legs iliopsoas are 2/5, hamstrings 3/5 and anterior tibials 2/5 bilaterally. All other muscle groups are at least 4/5.
35 Question 9 The Pyramidal FSS is: A. 2 B. 3 C. 4 D. 5 Question 9 The Pyramidal FSS is: A. 2 B. 3 C. 4 D. 5 25% 25% 25% 25%
36 Pyramidal 1 limb 2 limbs 3 limbs 4 limbs 0 Normal 1 Signs only 2 4/5 3 2 or 3/5 3/5 4/5 4/5 4 0 or 1/5 2/5 3/5 3/5 5 0 or 1/5 2/5 2/5 6 0 or 1/5 Cerebellar 0 normal 1 abnormal signs without disability 2 mild ataxia OR moderate station ataxia (Romberg) OR unable to tandem 3 moderate limb ataxia OR moderate or severe gait/truncal ataxia 4 severe gait/truncal ataxia AND severe ataxia in three or four limbs 5 unable to perform coordinated movements due to ataxia X pyramidal weakness (BMRC grade 3 or worse in limb strength) or sensory deficit interferes with testing
37 X ratings Cerebellar Score the actual performance and add X Limb ataxia Cerebellar 0 Normal 1 Signs only 2 Mild: Tremor or clumsiness easily seen, minor interference with function 3 Moderate: Interference with function in all spheres 4 Severe: Most functions very difficult
38 Trunk Cerebellar 0 Normal 1 Signs only 2 Mild: Sway with eyes closed 3 Moderate: Sway with eyes open 4 Severe: Requires assistance to sit Gait Cerebellar 0- Normal 1- Signs only 2- Mild: Balance problem recognized by patient or others 3- Moderate: Abnormal on ordinary walking 4- Severe: Unable to walk more than a few steps unassisted
39 Cerebellar Problems: Ambiguity of trunk/gait Use of Romberg for cerebellar testing Cerebellar Limb Trunk/Stance Gait 0 Normal Normal 1 Signs only Signs only Signs only 2 Mild Positive Romberg Unable to tandem 3 Moderate Moderate/severe Moderate/severe 4 Severe (3-4 limbs) AND Severe AND Severe 5 Action impossible X Weakness interferes
40 Question 10 The patient has bilateral intention tremor and has difficulty using eating utensils or buttoning clothes. Stance is normal with eyes open or closed. Tandem gait is impaired. Question 10 The Cerebellar FSS is: A. 1 B. 2 C. 3 D. 4
41 Question 10 The Cerebellar FSS is: 25% 25% 25% 25% A. 1 B. 2 C. 3 D Cerebellar Limb Trunk/Stance Gait 0 Normal Normal 1 Signs only Signs only Signs only 2 Mild Positive Romberg Unable to tandem 3 Moderate Moderate/severe Moderate/severe 4 Severe (3-4 limbs) AND Severe AND Severe 5 Action impossible X Weakness interferes
42 Question 11 The patient has minimal dysmetria of the arms. She requires a cane to walk because of falls secondary to imbalance. Question 11 The Cerebellar FSS is: A. 1 B. 2 C. 3 D. 4
43 Question 11 The Cerebellar FSS is: 25% 25% 25% 25% A. 1 B. 2 C. 3 D Cerebellar Limb Trunk/Stance Gait 0 Normal Normal 1 Signs only Signs only 2 Mild Positive Romberg Unable to tandem 3 Moderate Moderate/severe Moderate/severe 4 Severe (3-4 limbs) AND Severe AND Severe 5 Action impossible X Weakness interferes
44 Question 12 The patient has mild intention tremor which has a minor effect on her ADLs. She is plegic in the legs. Question 12 The Cerebellar FSS is: A. 2 B. 2X C. 3 D. X
45 Question 12 The Cerebellar FSS is: 25% 25% 25% 25% A. 2 B. 2X C. 3 D. X 10 A. B. C. D. Cerebellar Limb Trunk/Stance Gait 0 Normal Normal 1 Signs only Signs only 2 Mild Positive Romberg Unable to tandem 3 Moderate Moderate/severe Moderate/severe 4 Severe (3-4 limbs) AND Severe AND Severe 5 Action impossible X Weakness interferes
46 Sensory 0- Normal 1- Vibration or figure-writing or temperature decrease only in 1 or 2 limbs 2- Mild decrease in touch or pain or position sense in 1 or 2 limbs OR Moderate decrease in vibration in 1 or 2 limbs OR Mild decrease in vibration, figure writing or temp alone in 3 or 4 limbs Sensory 3- Moderate decreased in touch, pain or position sense OR Marked decrease in vibration in 1 or 2 limbs OR Mild decrease in touch or pain OR Moderate decrease in proprioception in 3 or 4 limbs
47 Sensory 4- Marked decrease in touch or pain in 1 or 2 limbs OR Moderate decrease in touch or pain OR Marked decrease in proprioception in 3 or 4 limbs Sensory 5- Loss of sensation in 1 or 2 limbs OR Moderate decrease in touch or pain OR Marked decrease in proprioception in Most of the body below the head 6- Sensation essentially lost below the head
48 Pain & light touch Sensory 0 Normal 1 Signs only: Abnormal but patient not aware 2 Mild: Aware of deficit but discriminates sharp & dull 3 Moderate: Impaired sharp-dull discrimination 4 Marked: Absent discrimination or absent light touch 5 Complete loss Vibration Sensory 0 Normal 1 Mild: 5-7/8 or > 10 sec 2 Moderate: 1-4/8 or 2-10 sec 3 Marked: Complete loss

49 Rydell-Seiffert Tuning Fork Position sense Sensory 0 Normal 1 Mild: 1-2 errors, only distal 2 Moderate: Many errors, proximal joints affected 3 Marked: Complete loss
50 Problems: Sensory Proprioception versus all proprioceptive tests Not all severity ratings are represented in the FSS standards Sensation absent below the head virtually never occurs Sensory Vib Vib Pain Pain JPS JPS Mild Nl Nl 2 Mod Mild Mild Mild 3 Marked Mod Mild Mod 3 Mod AND Mod 4 Marked Mod 4 Marked AND Marked 5 Absent AND Absent AND Absent 5 Mod* 5 Marked* AND Marked* 6 Absent* AND Absent* AND Absent*
51 Question 13 Vibration is 7/8 in the fingers and 6/8 in the toes. There is mild decrease in joint position sense in the toes. Pin prick sensation is intact. Question 13 The Sensory FSS is: A. 1 B. 2 C. 3 D. 4
52 Question 13 The Sensory FSS is: 25% 25% 25% 25% A. 1 B. 2 C. 3 D A. B. C. D. Sensory Vib Vib Pain Pain JPS JPS Mild Nl Nl 2 Mod Mild Mild Mild 3 Marked Mod Mild Mod 3 Mod AND Mod 4 Marked Mod 4 Marked AND Marked 5 Absent AND Absent AND Absent 5 Mod* 5 Marked* AND Marked* 6 Absent* AND Absent* AND Absent*
53 Question 14 Vibration is 4/8 in the fingers and 3/8 in the toes. The patient makes 1 or 2 errors in joint position sense in the toes. Pin prick sensation is intact. Question 14 The Sensory FSS is: A. 1 B. 2 C. 3 D. 4
54 Question 14 The Sensory FSS is: 25% 25% 25% 25% A. 1 B. 2 C. 3 D A. B. C. D. Rule of Thumb FSS If there is no rating listed for a particular function, find the next lower rating and add 1. For instance: vibration moderately decreased in 4 limbs Mild loss is rated 2.
55 Sensory Vib Vib Pain Pain JPS JPS Mild Nl Nl 2 Mod Mild Mild Mild 3 Marked Mod Mod Mild Mod 3 Mod AND Mod 4 Marked Mod 4 Marked AND Marked 5 Absent AND Absent AND Absent 5* Mod 5* Marked* AND Marked* 6 Absent* AND Absent* AND Absent* Rules of Thumb So the Sensory FS score is 3.
56 Question 15 Vibration and joint position sense are absent in all 4 limbs. There is impaired discrimination of sharp and dull in all 4 limbs. Question 15 The Sensory FSS is: A. 3 B. 4 C. 5 D. 6
57 Question 15 The Sensory FSS is: 25% 25% 25% 25% A. 3 B. 4 C. 5 D A. B. C. D. Sensory Vib Vib Pain Pain JPS JPS Mild Nl Nl 2 Mod Mild Mild Mild 3 Marked Mod Mild Mod 3 Mod AND Mod 4 Marked Mod 4 Marked AND Marked 5 Absent AND Absent AND Absent 5 Mod* 5 Marked* AND Marked* 6 Absent AND Absent AND Absent
58 Question 16 Vibration and joint position sense are absent in the feet and mildly decreased in the hands. Pin prick sensation is absent in the feet and impaired in the fingers. Question 16 The Sensory FSS is: A. 3 B. 4 C. 5 D. 6
59 Question 16 The Sensory FSS is: 25% 25% 25% 25% A. 3 B. 4 C. 5 D A. B. C. D. Sensory Vib Vib Pain Pain JPS JPS Mild Nl Nl 2 Mod Mild Mild Mild 3 Marked Mod Mild Mod 3 Mod AND Mod 4 Marked Mod 4 Marked AND Marked 5 Absent AND Absent AND Absent 5 Mod* 5 Marked* AND Marked* 6 Absent AND Absent AND Absent
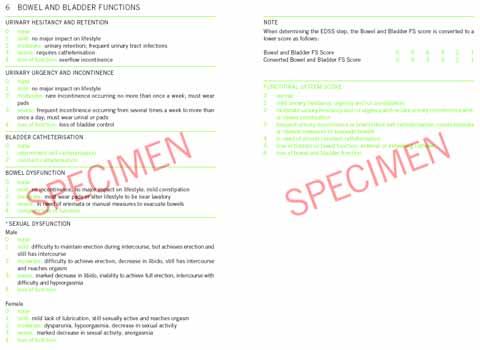
60 Bowel and Bladder 0- Normal 1- Mild urinary hesitancy, urgency or constipation 2- Moderate urinary hesitancy, retention, urgency or incontinence OR Moderate bowel dysfunction Bowel and Bladder 3- Frequent urinary incontinence OR Intermittent self-catheterization OR Enemas or manual bowel evacuation 4- In need of almost constant catheterization 5- Loss of bladder OR bowel function OR External or internal catheter 6- Loss of bowel AND bladder function
61 Bladder Hesitancy/Retention 0 None 1 Mild: No major impact on lifestyle 2 Moderate: Retention, frequent UTI 3 Severe: Catheterization 4 Loss of function: Overflow incontinence Bladder Urgency/Incontinence None Mild: No major impact on lifestyle Moderate: Incontinence < 1 per week Wears pads Severe: Frequent incontinence Loss of function: No control
62 Bowel None Mild: Mild constipation, no major impact on lifestyle Moderate: Pads or lifestyle change Severe: Enemas or manual measures Loss of function Bowel and Bladder Corrected Scores Score Corrected Score
63 Bowel & Bladder Score CS Bladder/ Incontinence Catheter Bowel 0 0 Nl Nl 1 1 Mild Mild 2 2 Mod/Rare Moderate /Frequent ISC Enemas etc 4 3 Almost constant 5 4 Absent Constant Absent 6 5 Absent AND Absent Cerebral 0- Normal 1- Signs only or mild fatigue 2- Mild decrease in mentation (history but not exam) or moderate to severe fatigue 3- Moderate decrease in mentation (O x 3) 4- Marked decrease in mentation (O x 1 or 2) 5- Dementia
64 Cerebral Depression and euphoria scored but don t affect FS or EDSS Fatigue: Depends upon study Cerebral Score Mentation Fatigue 0 Nl Nl 1 Signs only Mild 2 Mild Mod-severe 3 Mod 4 Marked 5 Dementia
65 Unrestricted Similar to normal EDSS 0 to 5.0 Fully Ambulatory Ambulation At least 500 m without assistance or rest, but not unrestricted EDSS 2.0 to 5.0 Pyramidal or cerebellar FS at least 2 EDSS Ambulation 1 AS Distance Restricted? Assistance EDSS m No None By FSS m Yes (Pyr or None By FSS Cereb None 4.5 or None None <100 - None 6.0
66 EDSS Ambulation 2 AS Distance Assistance EDSS 6 50 Unilateral <50 Unilateral Bilateral Bilateral 6.5 Ambulation An orthosis is NOT assistance for purposes of the EDSS
67 Rules of Thumb Assistance by person = bilateral assistance EDSS Ambulation 3 AS Ambulation Wheelchair Self-Care EDSS 10 5 m, transfers Standard chair Yes Few steps, Aid to transfer Standard with assistance, motorized Yes OOB - Many 8.0 Bed - Some 8.5 Bed - None 9.0 Bed - None 9.5
68 EDSS 4 and below Fully ambulatory (> 500 m) Defined exclusively by FS scores 4.5 & 5.0 FS scores OR ambulation More severe parameter governs 5.5 to 8.0 Ambulation or WC use only 8.5 and above Self-care and communication EDSS Problems Various exceptions to the ambulation distances ranges >120 M with bilateral assistance >50 M with unilateral assistance Combinations of lesser grades exceeding limits of previous steps
69 EDSS scoring by Functional systems Number of Functional System Scores at Grades 0-5 (total = 7) # of G0 # of G1 # of G2 # of G3 # of G4 # of G5 EDSS >= , 4 5 4, , 1, 2, 3 0, 1, 2, 3 0, , 1, 2, 3, 4 0, 1, 2, 3, , , , 2, 3, 4, , 4, 5, , , 5, ³ , 2, 3, 4,5,6 0, , 2, 3, 4, 5 1, 2, 3, 4, 5, 6 1, 2, ³ ³ EDSS scoring by ambulation Ambulatory status Kappos Kurtzke Walks unaided >= 500m, unrestricted Walks unaided ³300m, < 500m Walks unaided ³200m, < 300m Walks unaided ³100m, < 200m Walks unaided <100m?? Walks with aid ³100m 6.0 Walks with unilateral aid for ³100m (resting allowed) 6.0 Walks with bilateral aid for >120m 6.0 Walks with unilateral aid for >50m 6.0 Walks with assistance ³20m but not 100m 6.5 Walks with unilateral aid for <50m 6.5 Walks with bilateral aid m 6.5 Walks with bilateral aid for ³20m (no rest allowed) 6.5 Walks with bilateral aid >5m but <20m? close to 7.0 Walks with bilateral aid for >few steps but <5m Walks with bilateral aid for only a few steps Aid by another person equals bilateral assistance X AFO uni or bilateral by itself is not considered aid X Assignment is to that closest to his/her performance X *
70 EDSS 1. Determine all FSS 2. Determine maximal walking distance and independence 3. If 2 is less than 500 m, go to EDSS Ambulation chart 4. If 2 is at least 500 m, determine highest FSS and go to appropriate chart Ambulation 500 No Yes Use FSS Charts Assistance? Yes Wheelchair? No No Ambulation Chart 1 Ambulation Chart 2 Yes Ambulation Chart 3
71 Max FSS 1? Yes >1 FSS = 1? No EDSS = 1 No Yes EDSS = 1.5 Max FSS 2? Yes EDSS Chart 2 No Max FSS 3? Yes EDSS Chart 3 No EDSS Chart 4-5 EDSS EDSS
72 EDSS FSS EDSS EDSS FSS EDSS
73 Ambulation 500 No Yes Use FSS Charts Assistance? Yes Wheelchair? No No Ambulation Chart 1 Ambulation Chart 2 Yes Ambulation Chart 3 EDSS Visual 0 Brainstem 2 Pyramidal 3 Cerebellar 0 Sensory 3 Bowel/Bladder 1 Cerebral 1 Ambulation 500 m
74 What is the EDSS? Question 17 A. 3.5 B. 4.0 C. 4.5 D. 5.0 A. 3.5 B. 4.0 C. 4.5 D. 5.0 Question 17 What is the EDSS? 25% 25% 25% 25%
75 Max FSS 1? Yes >1 FSS = 1? No EDSS = 1 No Yes EDSS = 1.5 Max FSS 2? Yes EDSS Chart 2 No Max FSS 3? Yes EDSS Chart 3 No EDSS Chart 4-5 EDSS FSS EDSS
76 EDSS Visual 0 Brainstem 3 Pyramidal 3 Cerebellar 1 Sensory 3 Bowel/Bladder 1 Cerebral 1 Ambulation 350 m, no assistance Question 18 What is the EDSS? A. 3.0 B. 3.5 C. 4.0 D. 4.5
77 Question 18 What is the EDSS? 25% 25% 25% 25% A. 3.0 B. 3.5 C. 4.0 D Ambulation 500 No Yes Use FSS Charts Assistance? Yes Wheelchair? No No Ambulation Chart 1 Ambulation Chart 2 Yes Ambulation Chart 3
78 EDSS Ambulation 1 Distance Restricted? Assistance EDSS 500 m No None By FSS 500 m Yes (Pyr or None By FSS Cereb None 4.5* None None 5.5 Max FSS 1? Yes >1 FSS = 1? No EDSS = 1 No Yes EDSS = 1.5 Max FSS 2? Yes EDSS Chart 2 No Max FSS 3? Yes EDSS Chart 3 No EDSS Chart 4-5
79 EDSS FSS EDSS EDSS Visual 0 Brainstem 2 Pyramidal 2 Cerebellar 1 Sensory 5 Bowel/Bladder 1 Cerebral 0 Ambulation 350 m, no assistance
80 What is the EDSS? Question 19 A. 4.0 B. 4.5 C. 5.0 D. 5.5 Question 19 What is the EDSS? A. 4.0 B. 4.5 C. 5.0 D % 25% 25% 25%
81 Ambulation 500 No Yes Use FSS Charts Assistance? Yes Wheelchair? No No Ambulation Chart 1 Ambulation Chart 2 Yes Ambulation Chart 3 EDSS Ambulation 1 Distance Restricted? Assistance EDSS 500 m No None By FSS 500 m Yes (Pyr or None By FSS Cereb None 4.5* None None 5.5
82 Max FSS 1? Yes >1 FSS = 1? No EDSS = 1 No Yes EDSS = 1.5 Max FSS 2? Yes EDSS Chart 2 No Max FSS 3? Yes EDSS Chart 3 No EDSS Chart 4-5 EDSS FSS EDSS
83 EDSS Rules of Thumb When the EDSS as determined by FS and by ambulation do not agree, choose the higher EDSS. Question 20 The patient is able to walk 50 m by holding onto her husband s arm. She is too ataxic to use a cane.
84 What is the EDSS? Question 20 A. 5.0 B. 5.5 C. 6.0 D. 6.5 A. 5.0 B. 5.5 C. 6.0 D. 6.5 Question 20 What is the EDSS? 25% 25% 25% 25%
85 Ambulation 500 No Yes Use FSS Charts Assistance? Yes Wheelchair? No No Ambulation Chart 1 Ambulation Chart 2 Yes Ambulation Chart 3 EDSS Ambulation 2 Distance Assistance EDSS 100 Unilateral or 6.0 Intermittent Unilateral Unilateral 6.5 > 120 Bilateral Bilateral 6.5
86 Neurostatus Training
High Yield Neurological Examination
 High Yield Neurological Examination Vanja Douglas, MD Sara & Evan Williams Foundation Endowed Neurohospitalist Chair Director, Neurohospitalist Division Associate Professor of Clinical Neurology UCSF Department
High Yield Neurological Examination Vanja Douglas, MD Sara & Evan Williams Foundation Endowed Neurohospitalist Chair Director, Neurohospitalist Division Associate Professor of Clinical Neurology UCSF Department
quantified neurological examination and assessment of Kurtzke s Functional Systems and Expanded Disability Status Scale in Multiple Sclerosis Exposé
 Electronic Scoring Tools data for capture a standardised management neurological system examination for a standardized and quantified neurological examination and assessment of Kurtzke s Functional Systems
Electronic Scoring Tools data for capture a standardised management neurological system examination for a standardized and quantified neurological examination and assessment of Kurtzke s Functional Systems
A Hypothesis Driven Approach to the Neurological Exam
 A Hypothesis Driven Approach to the Neurological Exam Vanja Douglas, MD Assistant Clinical Professor UCSF Department of Neurology Disclosures None 1 Purpose of Neuro Exam Screen asymptomatic patients Screen
A Hypothesis Driven Approach to the Neurological Exam Vanja Douglas, MD Assistant Clinical Professor UCSF Department of Neurology Disclosures None 1 Purpose of Neuro Exam Screen asymptomatic patients Screen
Diagnostic Criteria, Clinical Courses, and Rating Scales in MS
 Diagnostic Criteria, Clinical Courses, and Rating Scales in MS Introduction and Objectives Introduction This module will focus on diagnostic tools utilized in randomized clinical trials (RCTs) in MS. Diagnostic
Diagnostic Criteria, Clinical Courses, and Rating Scales in MS Introduction and Objectives Introduction This module will focus on diagnostic tools utilized in randomized clinical trials (RCTs) in MS. Diagnostic
The High-Yield Neurologic Examination
 The High-Yield Neurologic Examination S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Chair, Department of Neurology Director, Neurohospitalist
The High-Yield Neurologic Examination S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Chair, Department of Neurology Director, Neurohospitalist
The Neurologic Examination: High-Yield Strategies
 The Neurologic Examination: High-Yield Strategies S. Andrew Josephson, MD Assistant Professor, Department of Neurology Divisions of Neurovascular and Behavioral Neurology University of California San Francisco
The Neurologic Examination: High-Yield Strategies S. Andrew Josephson, MD Assistant Professor, Department of Neurology Divisions of Neurovascular and Behavioral Neurology University of California San Francisco
The Neurologic Examination: High-Yield Strategies
 The Neurologic Examination: High-Yield Strategies S. Andrew Josephson, MD Examination Approach Two types of neurologic examinations 1. Screening Examination 2. Testing Hypotheses Select high-yield tests
The Neurologic Examination: High-Yield Strategies S. Andrew Josephson, MD Examination Approach Two types of neurologic examinations 1. Screening Examination 2. Testing Hypotheses Select high-yield tests
BRAIN STEM CASE HISTORIES CASE HISTORY VII
 463 Brain stem Case history BRAIN STEM CASE HISTORIES CASE HISTORY VII A 60 year old man with hypertension wakes one morning with trouble walking. He is feeling dizzy and is sick to his stomach. His wife
463 Brain stem Case history BRAIN STEM CASE HISTORIES CASE HISTORY VII A 60 year old man with hypertension wakes one morning with trouble walking. He is feeling dizzy and is sick to his stomach. His wife
Spinal Cord: Clinical Applications. Dr. Stuart Inglis
 Spinal Cord: Clinical Applications Dr. Stuart Inglis Tabes dorsalis, also known as syphilitic myelopathy, is a slow degeneration (specifically, demyelination) of the nerves in the dorsal funiculus of the
Spinal Cord: Clinical Applications Dr. Stuart Inglis Tabes dorsalis, also known as syphilitic myelopathy, is a slow degeneration (specifically, demyelination) of the nerves in the dorsal funiculus of the
Stroke School for Internists Part 1
 Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
An Illustrated Guide For Peripheral Nerve Examination. Bedside Teaching for 2 nd year medical Students
 An Illustrated Guide For Peripheral Nerve Examination Bedside Teaching for 2 nd year medical Students Prepared by: Dr. Farid Ghalli Clinical Teacher (Hon) November 2016 Before Examination : Wash hands
An Illustrated Guide For Peripheral Nerve Examination Bedside Teaching for 2 nd year medical Students Prepared by: Dr. Farid Ghalli Clinical Teacher (Hon) November 2016 Before Examination : Wash hands
Brain and Central Nervous System Cancers
 Brain and Central Nervous System Cancers NICE guidance link: https://www.nice.org.uk/guidance/ta121 Clinical presentation of brain tumours History and Examination Consider immediate referral Management
Brain and Central Nervous System Cancers NICE guidance link: https://www.nice.org.uk/guidance/ta121 Clinical presentation of brain tumours History and Examination Consider immediate referral Management
Neuro Exam Explained
 Neuro Exam Explained Michael Nelson M.D. Providence Neurological Specialties East Primary Care Conference October 26 rd, 2017 Michael Nelson M.D. Medical School: University of Missouri-Columbia Residency:
Neuro Exam Explained Michael Nelson M.D. Providence Neurological Specialties East Primary Care Conference October 26 rd, 2017 Michael Nelson M.D. Medical School: University of Missouri-Columbia Residency:
MRN# Provider: Appt. Date: Appt. Time:
 DEPARTMENT OF NEUROLOGY DIVISION OF MULTIPLE SCLEROSIS Appointments: (813)396-9478 http://ms.health.usf.edu/ MRN# Provider: Appt. Date: Appt. Time: Welcome to the University of South Florida Multiple Sclerosis
DEPARTMENT OF NEUROLOGY DIVISION OF MULTIPLE SCLEROSIS Appointments: (813)396-9478 http://ms.health.usf.edu/ MRN# Provider: Appt. Date: Appt. Time: Welcome to the University of South Florida Multiple Sclerosis
Neurological Assessment
 Neurological Assessment Name: Age: Gender: Date: History Review of history related to neurological system YES/NO If YES, provide details: General Neurological Mental Illness Neurological disease Severe
Neurological Assessment Name: Age: Gender: Date: History Review of history related to neurological system YES/NO If YES, provide details: General Neurological Mental Illness Neurological disease Severe
ID # COMPLETED: YES.. 1 DATE NO... 5 NEUROLOGICAL EXAM
 ID # COMPLETED: YES.. 1 DATE NO... 5 NEUROLOGICAL EXAM VIDEOTAPED: YES.. 1 NO... 5 COMMENT: NEUROLOGICAL EXAM "Normal, Abnormal, Other, Can't execute or Missing for each question. Always complete specify
ID # COMPLETED: YES.. 1 DATE NO... 5 NEUROLOGICAL EXAM VIDEOTAPED: YES.. 1 NO... 5 COMMENT: NEUROLOGICAL EXAM "Normal, Abnormal, Other, Can't execute or Missing for each question. Always complete specify
what do the numbers really mean? NIHSS Timothy Hehr, RN MA Stroke Program Outreach Coordinator Allina Health
 what do the numbers really mean? NIHSS Timothy Hehr, RN MA Stroke Program Outreach Coordinator Allina Health NIHSS The National Institutes of Health Stroke Scale (NIHSS) is a tool used to objectively quantify
what do the numbers really mean? NIHSS Timothy Hehr, RN MA Stroke Program Outreach Coordinator Allina Health NIHSS The National Institutes of Health Stroke Scale (NIHSS) is a tool used to objectively quantify
HISTORY TAKING ON NERVOUS SYSTEM. Dr. Amitesh Aggarwal
 HISTORY TAKING ON NERVOUS SYSTEM Dr. Amitesh Aggarwal General points History of neurological symptoms should also be taken from patient and close relative or friend Memory loss, intoxication, aphasia Patient
HISTORY TAKING ON NERVOUS SYSTEM Dr. Amitesh Aggarwal General points History of neurological symptoms should also be taken from patient and close relative or friend Memory loss, intoxication, aphasia Patient
Neurological Examination
 Neurological Examination Charles University in Prague 1st Medical Faculty and General University Hospital Neurological examination: Why important? clinical history taking and bedside examination: classical
Neurological Examination Charles University in Prague 1st Medical Faculty and General University Hospital Neurological examination: Why important? clinical history taking and bedside examination: classical
Approach to a Neurologic Diagnosis
 Approach to a Neurologic Diagnosis Neurologic Diagnosis History Physical & Neurological Examination Ancillary Procedures 3 Questions Asked Focal neurologic deficits Increased intracranial pressure Signs
Approach to a Neurologic Diagnosis Neurologic Diagnosis History Physical & Neurological Examination Ancillary Procedures 3 Questions Asked Focal neurologic deficits Increased intracranial pressure Signs
Divine Intervention Episode 58 Neurology Clerkship Shelf Review Part 7. Some PGY1
 Divine Intervention Episode 58 Neurology Clerkship Shelf Review Part 7 Some PGY1 1 Discussion of the pathway/information carried by the 3 HY spinal cord tracts (DCMLS, STT, CST). Description of the Romberg
Divine Intervention Episode 58 Neurology Clerkship Shelf Review Part 7 Some PGY1 1 Discussion of the pathway/information carried by the 3 HY spinal cord tracts (DCMLS, STT, CST). Description of the Romberg
Cancer Rehabilitation New Patient Intake Form
 _ I. Personal Information Date of Birth Age: Home Address: Home Phone: Cell Phone: Office Phone: Fax: E-Mail: II. Chief Complaint Please describe the major problem that brings you in today: Who referred
_ I. Personal Information Date of Birth Age: Home Address: Home Phone: Cell Phone: Office Phone: Fax: E-Mail: II. Chief Complaint Please describe the major problem that brings you in today: Who referred
IMPAIRMENT OF THE NERVOUS SYSTEM
 IMPAIRMENT OF THE NERVOUS SYSTEM The following information provides criteria for the evaluation of permanent impairment resulting from dysfunction brain, spinal cord and cranial nerves and certain peripheral
IMPAIRMENT OF THE NERVOUS SYSTEM The following information provides criteria for the evaluation of permanent impairment resulting from dysfunction brain, spinal cord and cranial nerves and certain peripheral
University of Manitoba - MPT: Neurological Clinical Skills Checklist
 Name: Site: Assessment Skills Observed Performed Becoming A. Gross motor function i. Describe movement strategies (quality, devices, timeliness, independence): supine sidelying sit stand supine long sitting
Name: Site: Assessment Skills Observed Performed Becoming A. Gross motor function i. Describe movement strategies (quality, devices, timeliness, independence): supine sidelying sit stand supine long sitting
Examination Approach. Examination Approach. Case 1: Mental Status. The Neurological Exam In the ICU: High Yield Techniques 5/8/2015
 The Neurological Exam In the ICU: High Yield Techniques Examination Approach Two types of neurologic examinations 1. Screening Examination 2. Testing Hypotheses Select high-yield tests and techniques S.
The Neurological Exam In the ICU: High Yield Techniques Examination Approach Two types of neurologic examinations 1. Screening Examination 2. Testing Hypotheses Select high-yield tests and techniques S.
The Neurological System. Neurological Exam 5 Components. Mental Status Examination
 The Neurological System 1 Neurological Exam 5 Components Mental status Cranial nerves Reflexes Motor- includes Cerebellar function Sensory 2 Mental Status Examination Examination - ABCT Appearance Behavior
The Neurological System 1 Neurological Exam 5 Components Mental status Cranial nerves Reflexes Motor- includes Cerebellar function Sensory 2 Mental Status Examination Examination - ABCT Appearance Behavior
Neuroanatomy of a Stroke. Joni Clark, MD Professor of Neurology Barrow Neurologic Institute
 Neuroanatomy of a Stroke Joni Clark, MD Professor of Neurology Barrow Neurologic Institute No disclosures Stroke case presentations Review signs and symptoms Review pertinent exam findings Identify the
Neuroanatomy of a Stroke Joni Clark, MD Professor of Neurology Barrow Neurologic Institute No disclosures Stroke case presentations Review signs and symptoms Review pertinent exam findings Identify the
3) Approach to Ataxia - Dr. Zana
 Approach to Ataxia - Dr. Zana") 3) Approach to Ataxia - Dr. Zana Introduction Ataxia is derived from Greek word a -not, taxis -orderly, (not orderly/ not in order) Ataxia is the inability to make smooth, accurate and coordinated movements
3) Approach to Ataxia - Dr. Zana Introduction Ataxia is derived from Greek word a -not, taxis -orderly, (not orderly/ not in order) Ataxia is the inability to make smooth, accurate and coordinated movements
GENERAL PRINCIPLES OF NEUROLOGY- John W. Day, M.D., Ph.D.
 I. TAKE HOME POINTS FOR THIS LECTURE A. Localizing the disease is the first step in diagnosing a neurological disorder. B. Time course of the disease (acute, subacute, or chronic) indicates the pathophysiological
I. TAKE HOME POINTS FOR THIS LECTURE A. Localizing the disease is the first step in diagnosing a neurological disorder. B. Time course of the disease (acute, subacute, or chronic) indicates the pathophysiological
3/3/2016. International Standards for the Neurologic Classification of Spinal Cord Injury (ISNCSCI)
") International Standards for the Neurologic Classification of Spinal Cord Injury (ISNCSCI) American Spinal Injury Association International Spinal Cord Society Presented by Adam Stein, MD Chairman and Professor
International Standards for the Neurologic Classification of Spinal Cord Injury (ISNCSCI) American Spinal Injury Association International Spinal Cord Society Presented by Adam Stein, MD Chairman and Professor
Pre-Return Visit Questionnaire for Multiple Sclerosis
 Question Multiple Choice Option Comments 1a 1b Have you had a relapse (new or worsening symptoms occurring in the absence of infection and lasting more than 24 hours) since your last visit? If the answer
Question Multiple Choice Option Comments 1a 1b Have you had a relapse (new or worsening symptoms occurring in the absence of infection and lasting more than 24 hours) since your last visit? If the answer
A CASE OF GIANT AXONAL NEUROPATHY HEMANANTH T SECOND YEAR POST GRADUATE IN PAEDIATRICS INSTITUTE OF SOCIAL PAEDIATRICS GOVERNMENT STANLEY HOSPITAL
 A CASE OF GIANT AXONAL NEUROPATHY HEMANANTH T SECOND YEAR POST GRADUATE IN PAEDIATRICS INSTITUTE OF SOCIAL PAEDIATRICS GOVERNMENT STANLEY HOSPITAL CASE HISTORY Nine year old male child Second born Born
A CASE OF GIANT AXONAL NEUROPATHY HEMANANTH T SECOND YEAR POST GRADUATE IN PAEDIATRICS INSTITUTE OF SOCIAL PAEDIATRICS GOVERNMENT STANLEY HOSPITAL CASE HISTORY Nine year old male child Second born Born
SARASOTA MEMORIAL HOSPITAL. NURSING PROCEDURE NATIONAL INSTITUTE OF HEALTH STROKE SCALE (neu04) Nursing
 Nursing") SARASOTA MEMORIAL HOSPITAL TITLE: ISSUED FOR: NURSING PROCEDURE NATIONAL INSTITUTE OF HEALTH Nursing DATE: REVIEWED: PAGES: PS1094 7/01 3/18 1 of 5 RESPONSIBILITY: RN, LPN PURPOSE: OBJECTIVE: DEFINITION:
SARASOTA MEMORIAL HOSPITAL TITLE: ISSUED FOR: NURSING PROCEDURE NATIONAL INSTITUTE OF HEALTH Nursing DATE: REVIEWED: PAGES: PS1094 7/01 3/18 1 of 5 RESPONSIBILITY: RN, LPN PURPOSE: OBJECTIVE: DEFINITION:
The Neurologic Examination
 The Neurologic Examination Cheryl L. Chrisman, DVM, MS, EdS, DACVIM (Neurology) The neurologic examination is a series of observations and tests done to answer the following four questions: h Is a lesion
The Neurologic Examination Cheryl L. Chrisman, DVM, MS, EdS, DACVIM (Neurology) The neurologic examination is a series of observations and tests done to answer the following four questions: h Is a lesion
Cesarean section for breech presentation. Jonathan H. Waters, M.D.
 Cesarean section for breech presentation Jonathan H. Waters, M.D. 1 26 y.o. G1P0 presented to triage in labor at 38 weeks. Patient was a known breech with a failed version 5 days before presentation. PMH
Cesarean section for breech presentation Jonathan H. Waters, M.D. 1 26 y.o. G1P0 presented to triage in labor at 38 weeks. Patient was a known breech with a failed version 5 days before presentation. PMH
How to Think like a Neurologist Review of Exam Process and Assessment Findings
 Lehigh Valley Health Network LVHN Scholarly Works Neurology Update for the Non-Neurologist 2013 Neurology Update for the Non-Neurologist Feb 20th, 5:10 PM - 5:40 PM How to Think like a Neurologist Review
Lehigh Valley Health Network LVHN Scholarly Works Neurology Update for the Non-Neurologist 2013 Neurology Update for the Non-Neurologist Feb 20th, 5:10 PM - 5:40 PM How to Think like a Neurologist Review
Practical Approach to the Neurologic History and Examination. Dr. Kathryn Giles MD, MSc, FRCPC Neurologist Cambridge, Ontario
 Practical Approach to the Neurologic History and Examination Dr. Kathryn Giles MD, MSc, FRCPC Neurologist Cambridge, Ontario Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document
Practical Approach to the Neurologic History and Examination Dr. Kathryn Giles MD, MSc, FRCPC Neurologist Cambridge, Ontario Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document
Key Clinical Concepts
 Cerebrovascular Review and General Vascular Syndromes, Including Those That Impact Dizziness Key Clinical Concepts Basic Review of Cerebrovascular Circulation Circulation to the brain is divided into anterior
Cerebrovascular Review and General Vascular Syndromes, Including Those That Impact Dizziness Key Clinical Concepts Basic Review of Cerebrovascular Circulation Circulation to the brain is divided into anterior
U n i f i e d P a r k i n s o n s D i s e a s e R a t i n g S c a l e ( U P D R S )
") Patient last name:................................. Date of birth:.... /.... /........ Patient first name:................................. Date:.... /.... /........ U n i f i e d P a r k i n s o n s D
Patient last name:................................. Date of birth:.... /.... /........ Patient first name:................................. Date:.... /.... /........ U n i f i e d P a r k i n s o n s D
SCI EXAM & FUNCTIONAL PROGNOSIS
 SCI EXAM & FUNCTIONAL PROGNOSIS MARCH 20, 2015 JUAN L ASANZA, MD STAFF PHYSICIAN VA PUGET SOUND HEALTH CARE SYSTEM SPINAL CORD INJURY UNIVERSITY OF WASHINGTON PHYSICAL MEDICINE & REHABILITATION OBJECTIVES
SCI EXAM & FUNCTIONAL PROGNOSIS MARCH 20, 2015 JUAN L ASANZA, MD STAFF PHYSICIAN VA PUGET SOUND HEALTH CARE SYSTEM SPINAL CORD INJURY UNIVERSITY OF WASHINGTON PHYSICAL MEDICINE & REHABILITATION OBJECTIVES
THE NATURAL HISTORY OF MS: DIAGNOSIS, CLINICAL COURSE, AND EPIDEMIOLOGY
 THE NATURAL HISTORY OF MS: DIAGNOSIS, CLINICAL COURSE, AND EPIDEMIOLOGY John R. Rinker II, MD University of Alabama at Birmingham Birmingham VA Medical Center May 29, 2014 DISCLOSURES Salary/Research:
THE NATURAL HISTORY OF MS: DIAGNOSIS, CLINICAL COURSE, AND EPIDEMIOLOGY John R. Rinker II, MD University of Alabama at Birmingham Birmingham VA Medical Center May 29, 2014 DISCLOSURES Salary/Research:
Data Collection Worksheet
 Data Collection Worksheet To maximize consistency, the authors of the scale state that it is essential that clinicians adhere to the scale instructions. They also advise that the scales be administrated
Data Collection Worksheet To maximize consistency, the authors of the scale state that it is essential that clinicians adhere to the scale instructions. They also advise that the scales be administrated
UF NEUROLOGY HISTORY AND PHYSICAL GUIDELINES
 UF NEUROLOGY HISTORY AND PHYSICAL GUIDELINES HISTORY Chief Complaint A maximally succinct statement of the patient age, handedness, gender, main problem, and its duration (e.g. 56 year old right-handed
UF NEUROLOGY HISTORY AND PHYSICAL GUIDELINES HISTORY Chief Complaint A maximally succinct statement of the patient age, handedness, gender, main problem, and its duration (e.g. 56 year old right-handed
Assessing the Stroke Patient. Arlene Boudreaux, MSN, RN, CCRN, CNRN
 Assessing the Stroke Patient Arlene Boudreaux, MSN, RN, CCRN, CNRN Cincinnati Pre-Hospital Stroke Scale May be done by EMS o One of many o F facial droop on one side o A arm drift (hold a pizza box, close
Assessing the Stroke Patient Arlene Boudreaux, MSN, RN, CCRN, CNRN Cincinnati Pre-Hospital Stroke Scale May be done by EMS o One of many o F facial droop on one side o A arm drift (hold a pizza box, close
Lack of muscle control (Stroke, bladder control, neurological disorders) Mechanical movement therapist assisted
 Mechanical movement therapist assisted") By Lisa Rosenberg Electrical Current Stimulates muscles and nerves Produces movement Helps Individuals with Disabilities Lack of muscle control (Stroke, bladder control, neurological disorders) Passive
By Lisa Rosenberg Electrical Current Stimulates muscles and nerves Produces movement Helps Individuals with Disabilities Lack of muscle control (Stroke, bladder control, neurological disorders) Passive
ID # COMPLETED: YES 1 DATE NO 2
 ID # COMPLETED: YES 1 DATE NO 2 NEUROLOGICAL EXAM "Normal, Abnormal, Other, Can't execute or Missing for each question. If you circle "Abnormal" or Other, also check the appropriate reason why or explain
ID # COMPLETED: YES 1 DATE NO 2 NEUROLOGICAL EXAM "Normal, Abnormal, Other, Can't execute or Missing for each question. If you circle "Abnormal" or Other, also check the appropriate reason why or explain
DIAGNOSTIC FORM FOR SPINOCEREBELLAR DEGENERATION (ATAXIA AND/OR SPASTIC PARAPARESIS) Sex: Follow up n :
 Sex: Follow up n :") SPATAX-EUROSPA proposal 9--6 DIAGNOSTIC FORM FOR SPINOCEREBELLAR DEGENERATION (ATAXIA AND/OR SPASTIC PARAPARESIS) Date: / / Center: Neurologist: Stick the identification tag Code ID patient: Birthdate:
SPATAX-EUROSPA proposal 9--6 DIAGNOSTIC FORM FOR SPINOCEREBELLAR DEGENERATION (ATAXIA AND/OR SPASTIC PARAPARESIS) Date: / / Center: Neurologist: Stick the identification tag Code ID patient: Birthdate:
CVA. Alison Atwater PA-C
 CVA Alison Atwater PA-C Types of CVAs Ischemic strokes 80% of strokes 2/3 are thrombotic 1/3 are embolic emboli from the heart or arteries feeding the brain such as carotids, vertebral and basilar etc
CVA Alison Atwater PA-C Types of CVAs Ischemic strokes 80% of strokes 2/3 are thrombotic 1/3 are embolic emboli from the heart or arteries feeding the brain such as carotids, vertebral and basilar etc
NEUROLOGY CLERKSHIP CORE CURRICULUM GUIDELINES
 NEUROLOGY CLERKSHIP CORE CURRICULUM GUIDELINES Endorsed by the following organizations - October 2000: American Academy of Neurology Association of University Professors of Neurology American Neurological
NEUROLOGY CLERKSHIP CORE CURRICULUM GUIDELINES Endorsed by the following organizations - October 2000: American Academy of Neurology Association of University Professors of Neurology American Neurological
Unit VIII Problem 5 Physiology: Cerebellum
 Unit VIII Problem 5 Physiology: Cerebellum - The word cerebellum means: the small brain. Note that the cerebellum is not completely separated into 2 hemispheres (they are not clearly demarcated) the vermis
Unit VIII Problem 5 Physiology: Cerebellum - The word cerebellum means: the small brain. Note that the cerebellum is not completely separated into 2 hemispheres (they are not clearly demarcated) the vermis
Clinical Caveats for Functional Disorders. Kalpesh Jivan Division of Neurology Department of Neurosciences
 Clinical Caveats for Functional Disorders Kalpesh Jivan Division of Neurology Department of Neurosciences How common are functional symptoms? ± ⅓ of new neurological outpatients Definitions Conversion(functional)
Clinical Caveats for Functional Disorders Kalpesh Jivan Division of Neurology Department of Neurosciences How common are functional symptoms? ± ⅓ of new neurological outpatients Definitions Conversion(functional)
Practical Functional Assessment of Elderly Persons: A Primary- Care Approach
 Practical Functional Assessment of Elderly Persons: A Primary- Care Approach The following is abstracted from: Fleming KC, Evans JM, Weber DC and Chutka DS. Practical Functional Assessment of Elderly Persons:
Practical Functional Assessment of Elderly Persons: A Primary- Care Approach The following is abstracted from: Fleming KC, Evans JM, Weber DC and Chutka DS. Practical Functional Assessment of Elderly Persons:
Clinical Information for Wheeled Mobility Page 1 of 6
 Clinical Information for Wheeled Mobility Page 1 of 6 PART A: PATIENT / PROVIDER INFORMATION - Please Print Name: Sponsor Soc. Sec. No: Address: City: St: Zip: Phone: ( ) Age: Sex: Height: Weight: Date
Clinical Information for Wheeled Mobility Page 1 of 6 PART A: PATIENT / PROVIDER INFORMATION - Please Print Name: Sponsor Soc. Sec. No: Address: City: St: Zip: Phone: ( ) Age: Sex: Height: Weight: Date
MOLLOY COLLEGE THE BARBARA H. HAGAN SCHOOL OF NURSING NURSE PRACTITIONER PROGRAMS. Study Guide for the Basic Physical Assessment Exam
 THE BARBARA H. HAGAN SCHOOL OF NURSING S Study Guide for the Basic Physical Assessment Exam Questions will be based on following chapters in, Bickley, L.S. (2016). (12 th ed). Bates guide to physical examination
THE BARBARA H. HAGAN SCHOOL OF NURSING S Study Guide for the Basic Physical Assessment Exam Questions will be based on following chapters in, Bickley, L.S. (2016). (12 th ed). Bates guide to physical examination
Acute Vestibular Syndrome (VS or Stroke?) Three-step H.I.N.T.S. eye examination
 Three-step H.I.N.T.S. eye examination") Acute Vestibular Syndrome (VS or Stroke?) Three-step H.I.N.T.S. eye examination Head Impulse (right- and leftward) Nystagmus type Test of Skew (cover test for skew deviation) Stroke findings: I.N.F.A.R.C.T.
Acute Vestibular Syndrome (VS or Stroke?) Three-step H.I.N.T.S. eye examination Head Impulse (right- and leftward) Nystagmus type Test of Skew (cover test for skew deviation) Stroke findings: I.N.F.A.R.C.T.
Neurological Assessment. Lecture 8
 Neurological Assessment Lecture 8 Nervous System Central Nervous System Brain Spinal cord Peripheral Nervous System Cranial nerves Spinal nerves Central Nervous System-Brain Central Nervous System-Spinal
Neurological Assessment Lecture 8 Nervous System Central Nervous System Brain Spinal cord Peripheral Nervous System Cranial nerves Spinal nerves Central Nervous System-Brain Central Nervous System-Spinal
Gary Rea MD PhD Medical Director OSU Comprehensive Spine Center
 Gary Rea MD PhD Medical Director OSU Comprehensive Spine Center 1. The less specific the patient is about symptoms and pain, the less likely a specific diagnosis will be made and the less likely the patient
Gary Rea MD PhD Medical Director OSU Comprehensive Spine Center 1. The less specific the patient is about symptoms and pain, the less likely a specific diagnosis will be made and the less likely the patient
General Procedure and Rules
 General Procedure and Rules PROCEDURE Description: This assessment is a measure of upper extremity (UE) and lower extremity (LE) motor and sensory impairment. Equipment: A chair, bedside table, reflex
General Procedure and Rules PROCEDURE Description: This assessment is a measure of upper extremity (UE) and lower extremity (LE) motor and sensory impairment. Equipment: A chair, bedside table, reflex
Stroke: clinical presentations, symptoms and signs
 Stroke: clinical presentations, symptoms and signs Professor Peter Sandercock University of Edinburgh EAN teaching course Burkina Faso 8 th November 2017 Clinical diagnosis is important to Ensure stroke
Stroke: clinical presentations, symptoms and signs Professor Peter Sandercock University of Edinburgh EAN teaching course Burkina Faso 8 th November 2017 Clinical diagnosis is important to Ensure stroke
Motor, Reflex, Coordination and Sensory Screening Examination
 Motor, Reflex, Coordination and Sensory Screening Examination K. Jeffrey Miller, DC, DABCO Miller 2002 2002-2012 K Jeffrey Miller DC DABCO Motor Function Neurological Testing Handedness Right or Left Handed
Motor, Reflex, Coordination and Sensory Screening Examination K. Jeffrey Miller, DC, DABCO Miller 2002 2002-2012 K Jeffrey Miller DC DABCO Motor Function Neurological Testing Handedness Right or Left Handed
Neurological and Trauma Impairment Set Version 10
 Neurological and Trauma Impairment Set Version 10 Admission/Discharge - Neurological + Trauma Impairment Set Version 10 (Please circle reason for assessment) Name: Severity scores - extent to which deficit
Neurological and Trauma Impairment Set Version 10 Admission/Discharge - Neurological + Trauma Impairment Set Version 10 (Please circle reason for assessment) Name: Severity scores - extent to which deficit
QUESTIONS CASE HISTORY XII
 615 Case History XII A 80 year old ex-president of the United States was out riding his horse when the horse stumbled and the ex-president fell off the horse hitting his head on the ground. He did not
615 Case History XII A 80 year old ex-president of the United States was out riding his horse when the horse stumbled and the ex-president fell off the horse hitting his head on the ground. He did not
NEUROLOGIC EXAMINATION
 Página 1 de 6 NEUROLOGIC EXAMINATION Part of "1 - NEUROPSYCHIATRIC EXAMINATION" The neurologic examination complements the clinical history and mental status examinations that preceded it (3). In the neurologic
Página 1 de 6 NEUROLOGIC EXAMINATION Part of "1 - NEUROPSYCHIATRIC EXAMINATION" The neurologic examination complements the clinical history and mental status examinations that preceded it (3). In the neurologic
/ / / / / / Hospital Abstraction: Stroke/TIA. Participant ID: Hospital Code: Multi-Ethnic Study of Atherosclerosis
 Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
Multiple sclerosis. Tünde Csépány MD. PhD
 Multiple sclerosis Tünde Csépány MD. PhD. 11. 19. 2008. Multiple Sclerosis Approximately 350 000 people in the United States are affected by MS Prevalence strongly dependent on latitude (25-224/100 000
Multiple sclerosis Tünde Csépány MD. PhD. 11. 19. 2008. Multiple Sclerosis Approximately 350 000 people in the United States are affected by MS Prevalence strongly dependent on latitude (25-224/100 000
The Deconstructed Neurological Examination
 The Deconstructed Neurological Examination Marguerite Knipe, DVM, Diplomate ACVIM (Neurology) I. MENTATION: Normal, Quiet, Obtunded (mild, moderate, severe), Stuporous, Comatose Define stuporous and comatose.
The Deconstructed Neurological Examination Marguerite Knipe, DVM, Diplomate ACVIM (Neurology) I. MENTATION: Normal, Quiet, Obtunded (mild, moderate, severe), Stuporous, Comatose Define stuporous and comatose.
Anatomy of Nervous System. Neurological Assessment. Brain. Brain. Spinal Cord. Spinal Cord 03/23/2010. Central. Peripheral
 Anatomy of Nervous System Neurological Assessment Central Brain Spinal cord Peripheral Spinal Nerves Brain Cerebral cortex ( rind ) gray matter Frontal Parietal Temporal Occipital Wernicke s area receptive
Anatomy of Nervous System Neurological Assessment Central Brain Spinal cord Peripheral Spinal Nerves Brain Cerebral cortex ( rind ) gray matter Frontal Parietal Temporal Occipital Wernicke s area receptive
EVALUATION AND MANAGEMENT OF CERVICAL SPINE DISORDERS
 CERVICAL SPINE EVALUATION AND MANAGEMENT OF CERVICAL SPINE DISORDERS Gregory M Yoshida MD Supports the skull Allows movement of the head Houses the spinal cord CERVICAL SPINE Unique anatomy Upper C spine
CERVICAL SPINE EVALUATION AND MANAGEMENT OF CERVICAL SPINE DISORDERS Gregory M Yoshida MD Supports the skull Allows movement of the head Houses the spinal cord CERVICAL SPINE Unique anatomy Upper C spine
Gait Disorders. Nicholas J. Silvestri, MD
 Gait Disorders Nicholas J. Silvestri, MD Disclosures NO SIGNIFICANT FINANCIAL, GENERAL, OR OBLIGATION INTERESTS TO REPORT Learning Objectives Explain the normal development of gait Describe various gait
Gait Disorders Nicholas J. Silvestri, MD Disclosures NO SIGNIFICANT FINANCIAL, GENERAL, OR OBLIGATION INTERESTS TO REPORT Learning Objectives Explain the normal development of gait Describe various gait
P1: OTA/XYZ P2: ABC c01 BLBK231-Ginsberg December 23, :43 Printer Name: Yet to Come. Part 1. The Neurological Approach COPYRIGHTED MATERIAL
 Part 1 The Neurological Approach COPYRIGHTED MATERIAL 1 2 Chapter 1 Neurological history-taking The diagnosis and management of diseases of the nervous system have been revolutionized in recent years by
Part 1 The Neurological Approach COPYRIGHTED MATERIAL 1 2 Chapter 1 Neurological history-taking The diagnosis and management of diseases of the nervous system have been revolutionized in recent years by
LOCALIZATION NEUROLOGY EPISODE VI HEARING LOSS AND GAIT ATAXIA
 LOCALIZATION NEUROLOGY EPISODE VI HEARING LOSS AND GAIT ATAXIA EPISODE VI HEARING LOSS APPROACH and DIAGNOSIS 2 Cochlea and Auditory nerve Pons (superior olive) lateral lemniscus Inferior colliculus Thalamus
LOCALIZATION NEUROLOGY EPISODE VI HEARING LOSS AND GAIT ATAXIA EPISODE VI HEARING LOSS APPROACH and DIAGNOSIS 2 Cochlea and Auditory nerve Pons (superior olive) lateral lemniscus Inferior colliculus Thalamus
CRANIAL NERVE TESTING FOR THE PRIMARY CARE OPTOMETRIST
 CRANIAL NERVE TESTING FOR THE PRIMARY CARE OPTOMETRIST Hannah Shinoda, OD Caroline Ooley, OD, FAAO Assistant Professors Pacific University College of Optometry The authors have no financial interest in
CRANIAL NERVE TESTING FOR THE PRIMARY CARE OPTOMETRIST Hannah Shinoda, OD Caroline Ooley, OD, FAAO Assistant Professors Pacific University College of Optometry The authors have no financial interest in
Objectives_ Series II
 Interaction Between the Development of Posture Control and Executive Function of Attention (Reilly et. al 2008) Journal of Motor Behavior, Vol. 40, No. 2, 90 102 Objectives_ Series II Gain an understanding
Interaction Between the Development of Posture Control and Executive Function of Attention (Reilly et. al 2008) Journal of Motor Behavior, Vol. 40, No. 2, 90 102 Objectives_ Series II Gain an understanding
Residual Functional Capacity Questionnaire MULTIPLE SCLEROSIS
 Residual Functional Capacity Questionnaire MULTIPLE SCLEROSIS Patient: DOB: Physician completing this form: Please complete the following questions regarding this patient's impairments and attach all supporting
Residual Functional Capacity Questionnaire MULTIPLE SCLEROSIS Patient: DOB: Physician completing this form: Please complete the following questions regarding this patient's impairments and attach all supporting
Unified Parkinson Disease Rating Scale (UPDRS)
") Unified Parkinson Disease Rating Scale (UPDRS) The UPDRS is a rating tool to follow the longitudinal course of Parkinson's Disease. It is made up of the 1)Mentation, Behavior, and Mood, 2)ADL and 3)Motor
Unified Parkinson Disease Rating Scale (UPDRS) The UPDRS is a rating tool to follow the longitudinal course of Parkinson's Disease. It is made up of the 1)Mentation, Behavior, and Mood, 2)ADL and 3)Motor
The Fresco Institute for Parkinson's and Movement Disorders
 The Fresco Institute for Parkinson's and Movement Disorders Follow Up Patient Questionnaire Name: Date: Accompanied by: Do you smoke? CURRENT PAST NEVER Which neurological symptom bothers you most right
The Fresco Institute for Parkinson's and Movement Disorders Follow Up Patient Questionnaire Name: Date: Accompanied by: Do you smoke? CURRENT PAST NEVER Which neurological symptom bothers you most right
Worksheet 3: Physician Medical Information Worksheet
 Worksheet 3: Physician Medical Information Worksheet FOR PHYSICIAN USE The purpose of this worksheet is to assist you in supporting your patient s Social Security Disability Insurance application, in compiling
Worksheet 3: Physician Medical Information Worksheet FOR PHYSICIAN USE The purpose of this worksheet is to assist you in supporting your patient s Social Security Disability Insurance application, in compiling
MULTIPLE SCLEROSIS PROFILE
 MULTIPLE SCLEROSIS PROFILE What is Multiple Sclerosis? Multiple sclerosis (MS) is a chronic, inflammatory disease of unknown etiology that involves an immune-mediated attack on the central nervous system
MULTIPLE SCLEROSIS PROFILE What is Multiple Sclerosis? Multiple sclerosis (MS) is a chronic, inflammatory disease of unknown etiology that involves an immune-mediated attack on the central nervous system
Painless, progressive weakness Could this be Motor Neurone Disease?
 Painless, progressive weakness Could this be Motor Neurone Disease? The importance of early diagnosis removal of uncertainty for the person experiencing symptoms allowing for care and support to start
Painless, progressive weakness Could this be Motor Neurone Disease? The importance of early diagnosis removal of uncertainty for the person experiencing symptoms allowing for care and support to start
Slide 1. Slide 2. Slide 3. Intro to Physical Therapy for Neuromuscular Conditions. PT Evaluation. PT Evaluation
 Slide 1 Intro to Physical Therapy for Neuromuscular Conditions PTA 103 Introduction to Clinical Practice 2 Slide 2 Mental status: consciousness, attention, orientation, cognition Communication: speech
Slide 1 Intro to Physical Therapy for Neuromuscular Conditions PTA 103 Introduction to Clinical Practice 2 Slide 2 Mental status: consciousness, attention, orientation, cognition Communication: speech
MYASTHENIA GRAVIS. Mr. D.Raju, M.pharm, Lecturer
 MYASTHENIA GRAVIS Mr. D.Raju, M.pharm, Lecturer OUTLINE Background Anatomy Pathophysiology Clinical Presentation Treatment BACKGROUND Acquired autoimmune disorder Clinically characterized by: Weakness
MYASTHENIA GRAVIS Mr. D.Raju, M.pharm, Lecturer OUTLINE Background Anatomy Pathophysiology Clinical Presentation Treatment BACKGROUND Acquired autoimmune disorder Clinically characterized by: Weakness
ABNORMAL STROKE EXAM FINDINGS:
 Stroke Assessment Scenario Case Information PATIENT INFORMATION: 68-year-old male patient complaining of left sided weakness and an unsteady gait. Reported last normal time 3 minutes prior to EMS arrival
Stroke Assessment Scenario Case Information PATIENT INFORMATION: 68-year-old male patient complaining of left sided weakness and an unsteady gait. Reported last normal time 3 minutes prior to EMS arrival
A comparison of two patients with Guillain-Barre Syndrome J O H N C O R S I N O, S P T
 A comparison of two patients with Guillain-Barre Syndrome J O H N C O R S I N O, S P T Guillain-Barre Acute inflammatory demyelinating polyneuropathy Highly diverse presentation, course, outcome Miller-Fisher:
A comparison of two patients with Guillain-Barre Syndrome J O H N C O R S I N O, S P T Guillain-Barre Acute inflammatory demyelinating polyneuropathy Highly diverse presentation, course, outcome Miller-Fisher:
The Neurologic Examination. John W. Engstrom, M.D. University of California San Francisco School of Medicine
 The Neurologic Examination John W. Engstrom, M.D. University of California San Francisco School of Medicine Overview The Neurologic Examination Mental status demonstration/questions Cranial nerves demonstration/questions
The Neurologic Examination John W. Engstrom, M.D. University of California San Francisco School of Medicine Overview The Neurologic Examination Mental status demonstration/questions Cranial nerves demonstration/questions
Vague Neurological Disorders
 Vague Neurological Disorders Dr. Philip Smalley MD FRCPC SVP & Global Chief Medical Officer RGA International Rose Conference, September 17, 2015 Agenda Vague neurological symptoms associated with: Alzheimer
Vague Neurological Disorders Dr. Philip Smalley MD FRCPC SVP & Global Chief Medical Officer RGA International Rose Conference, September 17, 2015 Agenda Vague neurological symptoms associated with: Alzheimer
Assessment Form Post Polio Syndrome and Late Effects of Polio
 FULL NAME: DATE OF BIRTH: PHONE NUMBER: CURRENT HOME ADDRESS: EMAIL ADDRESS: THERAPIST: REFERRAL SOURCE: CURRENT GP: NEXT OF KIN: ACC/NHI NUMBER: PATIENT GOALS OF TODAY S ASSESSMENT: MAIN PROBLEMS PATIENT
FULL NAME: DATE OF BIRTH: PHONE NUMBER: CURRENT HOME ADDRESS: EMAIL ADDRESS: THERAPIST: REFERRAL SOURCE: CURRENT GP: NEXT OF KIN: ACC/NHI NUMBER: PATIENT GOALS OF TODAY S ASSESSMENT: MAIN PROBLEMS PATIENT
Assessment Instruments for Your Patients with Myasthenia Gravis (MG)
") Assessment Instruments for Your Patients with Myasthenia Gravis (MG) Table of Contents Reported by patient Myasthenia Gravis Activities of Daily Living (MG-ADL): ~10 minutes 8-item outcome measure that
Assessment Instruments for Your Patients with Myasthenia Gravis (MG) Table of Contents Reported by patient Myasthenia Gravis Activities of Daily Living (MG-ADL): ~10 minutes 8-item outcome measure that
ORIGINAL CONTRIBUTION. Multiple Sclerosis That Is Progressive From the Time of Onset
 ORIGINAL CONTRIBUTION Multiple Sclerosis That Is Progressive From the Time of Onset Clinical Characteristics and Progression of Disability P. B. Andersson, MBChB, DPhil; E. Waubant, MD; L. Gee, MPH; D.
ORIGINAL CONTRIBUTION Multiple Sclerosis That Is Progressive From the Time of Onset Clinical Characteristics and Progression of Disability P. B. Andersson, MBChB, DPhil; E. Waubant, MD; L. Gee, MPH; D.
A Case of Vascular MCI
 A Case of Vascular MCI Charles DeCarli, MD Victor and Genevieve Orsi Chair in Alzheimer s Research Director Alzheimer s Disease Center University of California at Davis Initial Evaluation 78 y.o. Rt. Handed
A Case of Vascular MCI Charles DeCarli, MD Victor and Genevieve Orsi Chair in Alzheimer s Research Director Alzheimer s Disease Center University of California at Davis Initial Evaluation 78 y.o. Rt. Handed
Done By: manar aljebreen Abdulrahman alsharidah
 Female Side Male side Done By: manar aljebreen Abdulrahman alsharidah Revised By: Nour Al-Khawajah Mohammed Asiri 2 Slide No.( 1 ) Slide No.( 2 ) 3 Slide No.( 3 ) Slide No.( 4 ) Upper motor neurons are
Female Side Male side Done By: manar aljebreen Abdulrahman alsharidah Revised By: Nour Al-Khawajah Mohammed Asiri 2 Slide No.( 1 ) Slide No.( 2 ) 3 Slide No.( 3 ) Slide No.( 4 ) Upper motor neurons are
Differential Diagnosis of Hypokinetic Movement Disorders
 Differential Diagnosis of Hypokinetic Movement Disorders Dr Donald Grosset Consultant Neurologist - Honorary Professor Institute of Neurological Sciences - Glasgow University Hypokinetic Parkinson's Disease
Differential Diagnosis of Hypokinetic Movement Disorders Dr Donald Grosset Consultant Neurologist - Honorary Professor Institute of Neurological Sciences - Glasgow University Hypokinetic Parkinson's Disease
Therapy Goals and Reassessments: Setting the Expectations
 Therapy Goals and Reassessments: Setting the Expectations Presented by: Cindy Krafft PT, MS Director of Rehabilitation Consulting Services Fazzi Associates, Inc. 243 King Street, Suite 246 Northampton,
Therapy Goals and Reassessments: Setting the Expectations Presented by: Cindy Krafft PT, MS Director of Rehabilitation Consulting Services Fazzi Associates, Inc. 243 King Street, Suite 246 Northampton,
SCALES SCALES SCALES. Performance Scales WHAT SHOULD THE RAINBOW FISH DO WITH ALL OF THESE SCALES?? KPS FAST ECOG PPS NYHA MRI ALSFRS
 SCALES SCALES SCALES WHAT SHOULD THE RAINBOW FISH DO WITH ALL OF THESE SCALES?? Karen L. Cross, MD, FAAHPM Performance Scales KPS FAST ECOG PPS NYHA MRI ALSFRS PPS = 30, 40, or 50 ECOG = 2, 3, or 4 NYHA
SCALES SCALES SCALES WHAT SHOULD THE RAINBOW FISH DO WITH ALL OF THESE SCALES?? Karen L. Cross, MD, FAAHPM Performance Scales KPS FAST ECOG PPS NYHA MRI ALSFRS PPS = 30, 40, or 50 ECOG = 2, 3, or 4 NYHA
Neurology. Clerkship. Syllabus
 Neurology Clerkship Syllabus Clerkship Website http://depts.washington.edu/neurolog/education/clerkships/home.html Neurology Clerkship Identifying data Name: Dates of clerkship: / / to / / Location: Contact
Neurology Clerkship Syllabus Clerkship Website http://depts.washington.edu/neurolog/education/clerkships/home.html Neurology Clerkship Identifying data Name: Dates of clerkship: / / to / / Location: Contact
Cerebral Palsy. What is Cerebral Palsy? Clues to Diagnosis of Cerebral Palsy 12/30/2012
 What is Cerebral Palsy? Cerebral Palsy Hamza Alsayouf,MD American Board Of neurology with Special Qualification in Child Neurology American Board of Pediatric Neurology In 2005, a committee of the American
What is Cerebral Palsy? Cerebral Palsy Hamza Alsayouf,MD American Board Of neurology with Special Qualification in Child Neurology American Board of Pediatric Neurology In 2005, a committee of the American
Cranial Nerves Exam. 1. To learn how to examine the functions of the 12 pairs of cranial nerves.
 Cranial Nerves Exam [Purpose] 1. To learn how to examine the functions of the 12 pairs of cranial nerves. 2. To understand the function of the 12 pairs of cranial nerves. [Principle] The cranial nerves
Cranial Nerves Exam [Purpose] 1. To learn how to examine the functions of the 12 pairs of cranial nerves. 2. To understand the function of the 12 pairs of cranial nerves. [Principle] The cranial nerves
by Dr. J. Marc Girard MD FRCP (C) 2nd Edition Multiple Sclerosis Society of Canada Quebec Division
 2nd Edition Multiple Sclerosis Society of Canada Quebec Division") by Dr. J. Marc Girard MD FRCP (C) 2nd Edition Multiple Sclerosis Society of Canada Quebec Division Production: Multiple Sclerosis Society of Canada (Quebec Division) Text: Dr. J. Marc Girard, MD FRCP(C)
by Dr. J. Marc Girard MD FRCP (C) 2nd Edition Multiple Sclerosis Society of Canada Quebec Division Production: Multiple Sclerosis Society of Canada (Quebec Division) Text: Dr. J. Marc Girard, MD FRCP(C)
Human Anatomy and Physiology - ANAT 14 Sensory System Lab Goals Activities
 Sensory System Human Anatomy and Physiology - ANAT 14 Lab Goals Observe many characteristics of our somatic and special senses. Activity descriptions noted in your lab manual are specified. Activities
Sensory System Human Anatomy and Physiology - ANAT 14 Lab Goals Observe many characteristics of our somatic and special senses. Activity descriptions noted in your lab manual are specified. Activities
Slide 1. Slide 2 Disclosure. Slide 3 Objectives. Functional Mobility and Activities of Daily Living: Assessing and Treating Patients in Rehabilitation
 Slide 1 Functional Mobility and Activities of Daily Living: Assessing and Treating Patients in Rehabilitation Terry Carolan, MSPT, NCS Slide 2 Disclosure Terry Carolan has no industry disclosures to make
Slide 1 Functional Mobility and Activities of Daily Living: Assessing and Treating Patients in Rehabilitation Terry Carolan, MSPT, NCS Slide 2 Disclosure Terry Carolan has no industry disclosures to make
Canadian Stroke Best Practices Table 3.3A Screening and Assessment Tools for Acute Stroke
 Canadian Stroke Best Practices Table 3.3A Screening and s for Acute Stroke Neurological Status/Stroke Severity assess mentation (level of consciousness, orientation and speech) and motor function (face,
Canadian Stroke Best Practices Table 3.3A Screening and s for Acute Stroke Neurological Status/Stroke Severity assess mentation (level of consciousness, orientation and speech) and motor function (face,