Neuroanatomy of a Stroke. Joni Clark, MD Professor of Neurology Barrow Neurologic Institute
|
|
|
- Corey Brooks
- 5 years ago
- Views:
Transcription
1 Neuroanatomy of a Stroke Joni Clark, MD Professor of Neurology Barrow Neurologic Institute
2 No disclosures
3 Stroke case presentations Review signs and symptoms Review pertinent exam findings Identify the neuroanatomy of the stroke Identify the vascular territory Discuss likely etiology
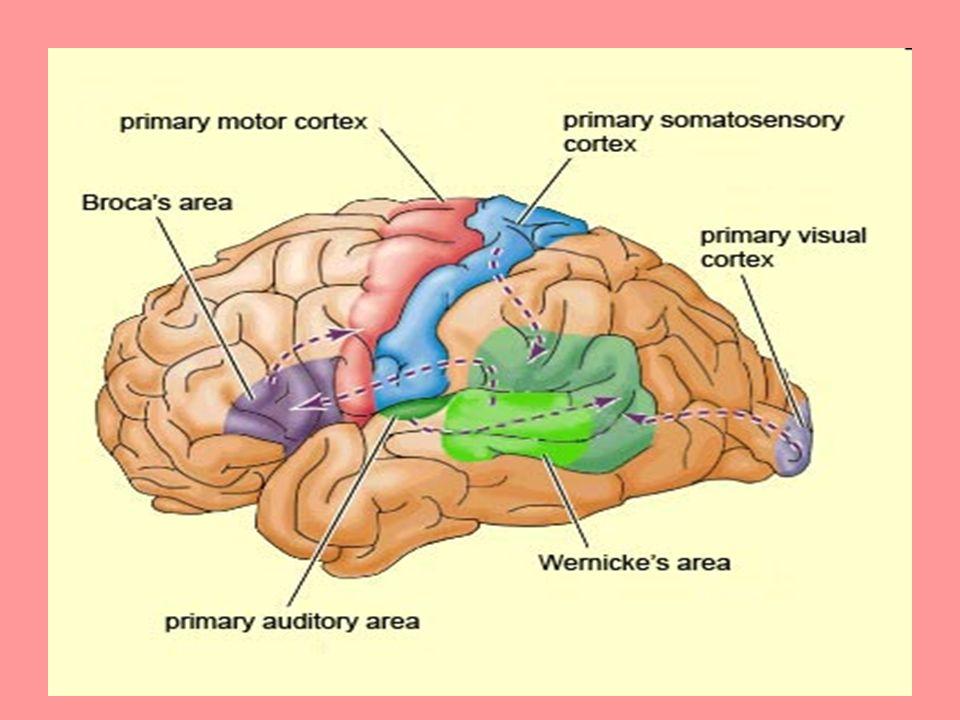
4 Case 1 75 yr old female presents to the ER with trouble speaking and rt face, arm and leg weakness Exam BP= 160/90 HR= 90 irregularly irregular Expressive aphasia Left gaze preference Right homonymous hemianopia Right hemiparesis/hemianesthesia
5
6
7 Radiopaedia Frank Gaillard

8 Left MCA Occlusion
9 Etiology Embolic stroke EKG: atrial fibrillation Likely etiology is cardiac embolus secondary to atrial fibrillation Treatment: long term anticoagulation
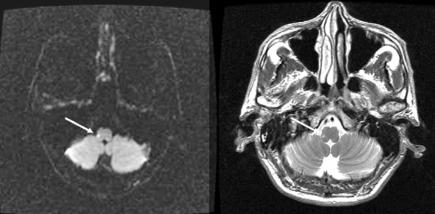
10 Case 2 70 yr old male with a history of HTN and DM presents with the following symptoms: Vertigo Veers to rt on walking Nausea and vomiting Numbness rt cheek
11
12
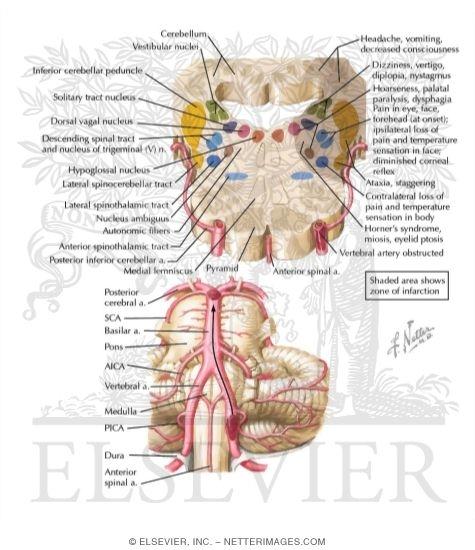
13 Lateral Medullary Syndrome Symptoms Ataxia Numbness Dysphagia Vertigo Nausea/Vomiting Dysarthria Diplopia or blurred vision Hoarseness Facial Pain Hiccups
14 Lateral Medullary Syndrome Neurologic Findings Pain and temperature hypesthesia (contralateral limbs) Horner s syndrome (sympathetic tract) Gait and limb ataxia Facial hypesthesia (ipsilateral) Nystagmus Pharyngeal and vocal cord paralysis
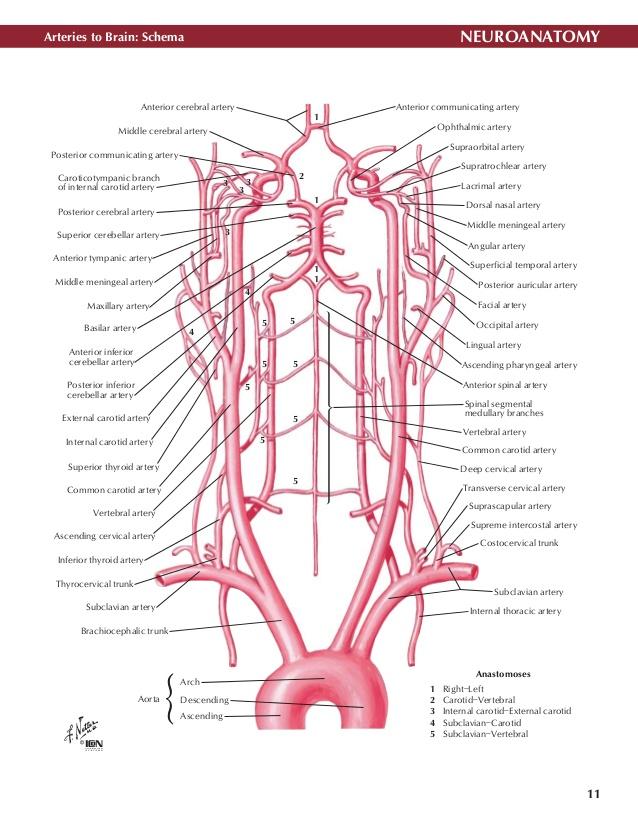
15 Etiology Most frequent arterial lesion is occlusion of the vertebral artery ¾ are thrombotic and remainder cardioembolic Rarely is the lesion confined only to the PICA In young patients with headache vertebral artery dissection may be the cause
16 Case 3 85 yr old male with HTN presents with face, arm and leg weakness; Exam significant for rt facial weakness and 0/5 strength in the rt arm and leg
17
18
19
20
21
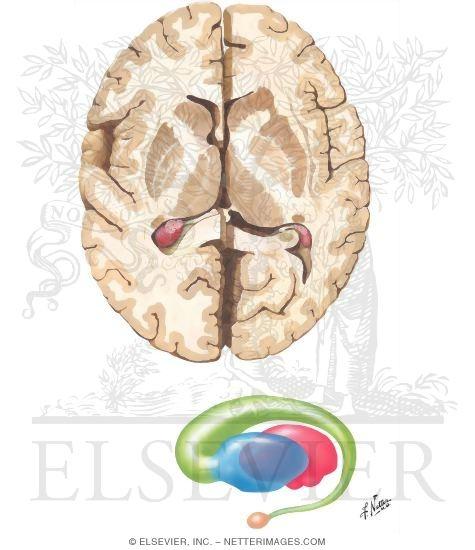
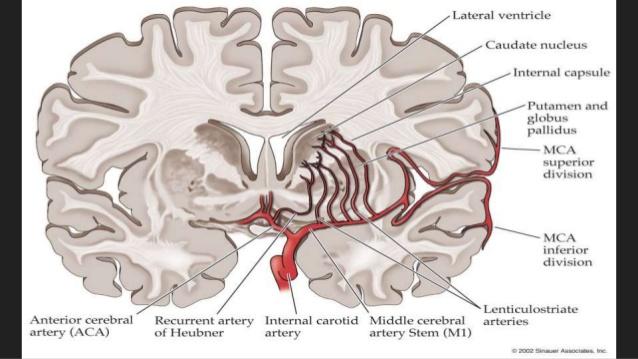
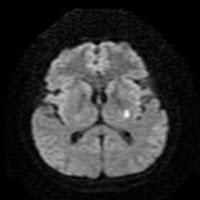
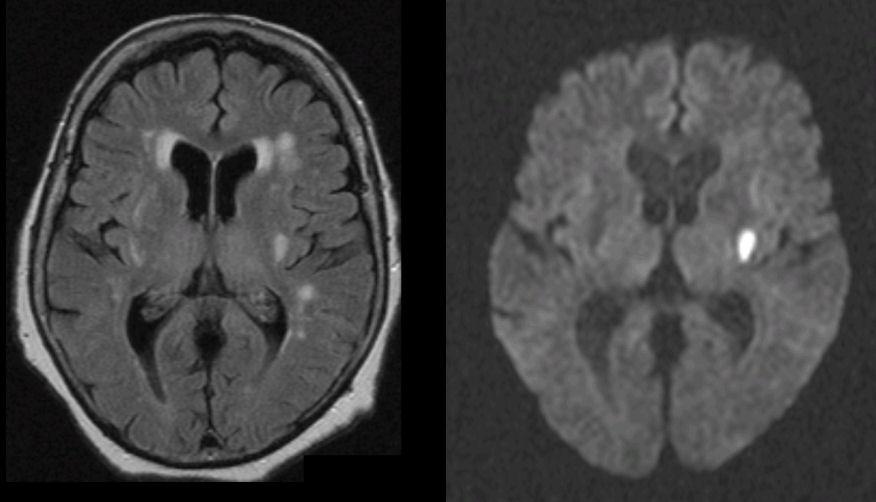
22 Lacunar Strokes Infarct caused by the occlusion of a single penetrating artery Lacunar infarcts are less than 15 mm in diameter
23 Clinical Lacunar Syndromes Pure Motor Hemiparesis Pure Sensory Hemiparesis Mixed motor/sensory Dysarthria clumsy hand syndrome Ataxic Hemiparesis
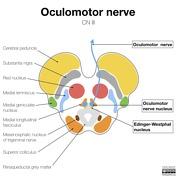
24 Case 4 70 yr old male with DM presents with complaints of double vision and weakness on the rt face, arm and leg Exam shows left third nerve palsy and rt face, arm and leg weakness
25 Radiopaedia
26 Oculomotor Nerve Clinical signs of CN III injury are: Ptosis (drooping upper eyelid) due to paralysis of the levator palpabrae superioris Eyeball resting in the down and out position due to the paralysis of the superior, inferior and medical rectus and the inferior oblique. The patient is unable to elevate, depress or adduct the eye. Dilated pupil due to the unopposed action of the dilator pupillae muscle

27
28 Weber Syndrome Ipsilateral third nerve palsy and crossed hemiplegia Likely to be due to occlusion of the posterior cerebral artery at the P1 segment

29 Case courtesy of A.Prof Frank Gaillard, Radiopaedia.org, rid: 2665
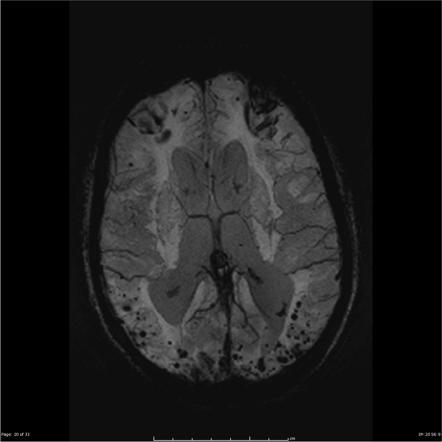
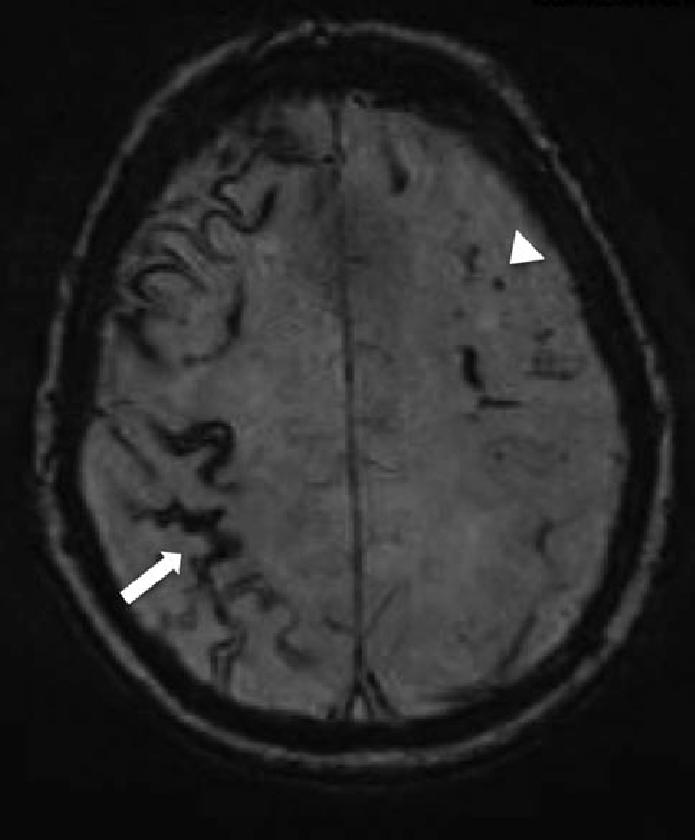
30 Case 5 A 78 yr old male began having episodes of rt arm numbness, decreased coordination and weakness lasting 5 min. and self resolved He was diagnosed with TIAs and started on aspirin Work up was reported as normal Spells stopped but had a slowly progressive cognitive decline He presented to the ER two years later with several days of increased confusion and walking into walls

31
32 Cerebral Microhemorrhages
33
34
35 Cerebral Amyloid Angiopathy Characterized by amyloid B fibril deposition in the media of small to medium sized vessels Risk factor: increased age Recurrent hemorrhages : lobar Can have superficial siderosis Age 55 or older Microhemorrahges on MRI GRE images
36 CAA About 20% of patients may have transient focal neurologic spells, amyloid spells Usually seen in those with superficial siderosis
37 CAA No treatment but avoid anti-platelet agents and anticoagulants.
/ / / / / / Hospital Abstraction: Stroke/TIA. Participant ID: Hospital Code: Multi-Ethnic Study of Atherosclerosis
 Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
Stroke School for Internists Part 1
 Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
CVA. Alison Atwater PA-C
 CVA Alison Atwater PA-C Types of CVAs Ischemic strokes 80% of strokes 2/3 are thrombotic 1/3 are embolic emboli from the heart or arteries feeding the brain such as carotids, vertebral and basilar etc
CVA Alison Atwater PA-C Types of CVAs Ischemic strokes 80% of strokes 2/3 are thrombotic 1/3 are embolic emboli from the heart or arteries feeding the brain such as carotids, vertebral and basilar etc
Overview of Stroke: Etiologies, Demographics, Syndromes, and Outcomes. Alex Abou-Chebl, MD, FSVIN Medical Director, Stroke Baptist Health Louisville
 Overview of Stroke: Etiologies, Demographics, Syndromes, and Outcomes Alex Abou-Chebl, MD, FSVIN Medical Director, Stroke Baptist Health Louisville Disclosure Statement of Financial Interest Within the
Overview of Stroke: Etiologies, Demographics, Syndromes, and Outcomes Alex Abou-Chebl, MD, FSVIN Medical Director, Stroke Baptist Health Louisville Disclosure Statement of Financial Interest Within the
Nicolas Bianchi M.D. May 15th, 2012
 Nicolas Bianchi M.D. May 15th, 2012 New concepts in TIA Differential Diagnosis Stroke Syndromes To learn the new definitions and concepts on TIA as a condition of high risk for stroke. To recognize the
Nicolas Bianchi M.D. May 15th, 2012 New concepts in TIA Differential Diagnosis Stroke Syndromes To learn the new definitions and concepts on TIA as a condition of high risk for stroke. To recognize the
The NIHSS score is 4 (considering 2 pts for the ataxia involving upper and lower limbs.
 Neuroscience case 5 1. Speech comprehension, ability to speak, and word use were normal in Mr. Washburn, indicating that aphasia (cortical language problem) was not involved. However, he did have a problem
Neuroscience case 5 1. Speech comprehension, ability to speak, and word use were normal in Mr. Washburn, indicating that aphasia (cortical language problem) was not involved. However, he did have a problem
Key Clinical Concepts
 Cerebrovascular Review and General Vascular Syndromes, Including Those That Impact Dizziness Key Clinical Concepts Basic Review of Cerebrovascular Circulation Circulation to the brain is divided into anterior
Cerebrovascular Review and General Vascular Syndromes, Including Those That Impact Dizziness Key Clinical Concepts Basic Review of Cerebrovascular Circulation Circulation to the brain is divided into anterior
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination pulse 80/min reg, BP 160/95
Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination pulse 80/min reg, BP 160/95
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with Non-fluent dysphasia R facial weakness Background Ischaemic heart disease Hypertension Hyperlipidemia L MCA branch
Alan Barber Professor of Clinical Neurology University of Auckland Presented with Non-fluent dysphasia R facial weakness Background Ischaemic heart disease Hypertension Hyperlipidemia L MCA branch
CEREBRO VASCULAR ACCIDENTS
 CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
Assessing the Stroke Patient. Arlene Boudreaux, MSN, RN, CCRN, CNRN
 Assessing the Stroke Patient Arlene Boudreaux, MSN, RN, CCRN, CNRN Cincinnati Pre-Hospital Stroke Scale May be done by EMS o One of many o F facial droop on one side o A arm drift (hold a pizza box, close
Assessing the Stroke Patient Arlene Boudreaux, MSN, RN, CCRN, CNRN Cincinnati Pre-Hospital Stroke Scale May be done by EMS o One of many o F facial droop on one side o A arm drift (hold a pizza box, close
Stroke/TIA. Tom Bedwell
 Stroke/TIA Tom Bedwell tab1g11@soton.ac.uk The Plan Definitions Anatomy Recap Aetiology Pathology Syndromes Brocas / Wernickes Investigations Management Prevention & Prognosis TIAs Key Definitions Transient
Stroke/TIA Tom Bedwell tab1g11@soton.ac.uk The Plan Definitions Anatomy Recap Aetiology Pathology Syndromes Brocas / Wernickes Investigations Management Prevention & Prognosis TIAs Key Definitions Transient
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination P 80/min reg, BP 160/95, normal
Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination P 80/min reg, BP 160/95, normal
Initial symptom or syndrome: (1) FOCAL WEAKNESS OR NUMBNESS
 FOCAL WEAKNESS OR NUMBNESS") View the referenced DVD patient cases, especially if few hospital or clinic patients are encountered for any one symptom or syndrome. The DVD patient cases are referenced by initial symptom or syndrome
View the referenced DVD patient cases, especially if few hospital or clinic patients are encountered for any one symptom or syndrome. The DVD patient cases are referenced by initial symptom or syndrome
Stroke: clinical presentations, symptoms and signs
 Stroke: clinical presentations, symptoms and signs Professor Peter Sandercock University of Edinburgh EAN teaching course Burkina Faso 8 th November 2017 Clinical diagnosis is important to Ensure stroke
Stroke: clinical presentations, symptoms and signs Professor Peter Sandercock University of Edinburgh EAN teaching course Burkina Faso 8 th November 2017 Clinical diagnosis is important to Ensure stroke
BRAIN STEM CASE HISTORIES CASE HISTORY VII
 463 Brain stem Case history BRAIN STEM CASE HISTORIES CASE HISTORY VII A 60 year old man with hypertension wakes one morning with trouble walking. He is feeling dizzy and is sick to his stomach. His wife
463 Brain stem Case history BRAIN STEM CASE HISTORIES CASE HISTORY VII A 60 year old man with hypertension wakes one morning with trouble walking. He is feeling dizzy and is sick to his stomach. His wife
Cerebrovascular Disorders. Blood, Brain, and Energy. Blood Supply to the Brain 2/14/11
 Cerebrovascular Disorders Blood, Brain, and Energy 20% of body s oxygen usage No oxygen/glucose reserves Hypoxia - reduced oxygen Anoxia - Absence of oxygen supply Cell death can occur in as little as
Cerebrovascular Disorders Blood, Brain, and Energy 20% of body s oxygen usage No oxygen/glucose reserves Hypoxia - reduced oxygen Anoxia - Absence of oxygen supply Cell death can occur in as little as
Module 5. Ischemia in Vertebral-basilar Territory
 T I Module 5. Ischemia in Vertebral-basilar Territory Introduction and Key Clinical Examples Ischemia in Vertebrobasilar branches Objectives for Module 5 Knowledge! List 4 common symptoms that patients
T I Module 5. Ischemia in Vertebral-basilar Territory Introduction and Key Clinical Examples Ischemia in Vertebrobasilar branches Objectives for Module 5 Knowledge! List 4 common symptoms that patients
TIA AND STROKE. Topics/Order of the day 1. Topics/Order of the day 2 01/08/2012
 Charles Ashton Medical Director TIA AND STROKE Topics/Order of the day 1 What Works? Clinical features of TIA inc the difference between Carotid and Vertebral territories When is a TIA not a TIA TIA management
Charles Ashton Medical Director TIA AND STROKE Topics/Order of the day 1 What Works? Clinical features of TIA inc the difference between Carotid and Vertebral territories When is a TIA not a TIA TIA management
Stroke 101. Maine Cardiovascular Health Summit. Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013
 Stroke 101 Maine Cardiovascular Health Summit Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013 Stroke Statistics Definition of stroke Risk factors Warning signs Treatment
Stroke 101 Maine Cardiovascular Health Summit Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013 Stroke Statistics Definition of stroke Risk factors Warning signs Treatment
[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]
![[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]](/thumbs/89/98619893.jpg "[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]") 2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
: STROKE. other pertinent information such as recent trauma, illicit drug use, pertinent medical history or use of oral contraceptives.
 INTRODUCTION A cerebral vascular accident (CVA) or stroke is a lack of blood supply to the brain as a result of either ischemia or hemorrhage. 80% of CVAs are a result of ischemia (embolic or thrombotic)
INTRODUCTION A cerebral vascular accident (CVA) or stroke is a lack of blood supply to the brain as a result of either ischemia or hemorrhage. 80% of CVAs are a result of ischemia (embolic or thrombotic)
Identifying Cerebrovascular Disorders. Wengui Yu, MD, PhD Department of Neurology, University of California, Irvine
 Identifying Cerebrovascular Disorders Wengui Yu, MD, PhD Department of Neurology, University of California, Irvine Objectives Review different types of cerebrovascular disorders. Briefly discuss etiology,
Identifying Cerebrovascular Disorders Wengui Yu, MD, PhD Department of Neurology, University of California, Irvine Objectives Review different types of cerebrovascular disorders. Briefly discuss etiology,
STROKE UPDATE ANTHEA PARRY MAY 2010
 STROKE UPDATE ANTHEA PARRY MAY 2010 Delivery of stroke care Clinical presentations Management Health Care for London plan 8 HASU (hyperacute) units 20 stroke units TIA services Hyperacute stroke units
STROKE UPDATE ANTHEA PARRY MAY 2010 Delivery of stroke care Clinical presentations Management Health Care for London plan 8 HASU (hyperacute) units 20 stroke units TIA services Hyperacute stroke units
University Journal of Medicine and Medical Sciences
 ISSN 2455-2852 Volume 2 Issue 5 2016 Case report -Opalski's syndrome A rare variant of lateral medullary syndrome in TAKAYASUS ARTERITIS SHANKAR GANESH N NAINAR Department of Neurology, MADRAS MEDICAL
ISSN 2455-2852 Volume 2 Issue 5 2016 Case report -Opalski's syndrome A rare variant of lateral medullary syndrome in TAKAYASUS ARTERITIS SHANKAR GANESH N NAINAR Department of Neurology, MADRAS MEDICAL
What Do You Think of My Posterior?
 What Do You Think of My Posterior? Posterior Stroke and Stroke Mimics Peter Panagos, MD, FACEP, FAHA Associate Professor Emergency Medicine and Neurology Washington University School of Medicine Disclosures
What Do You Think of My Posterior? Posterior Stroke and Stroke Mimics Peter Panagos, MD, FACEP, FAHA Associate Professor Emergency Medicine and Neurology Washington University School of Medicine Disclosures
10/13/2017. AllinaHealthSystems. Stroke Recognition Sandra K Hanson, MD Medical Director United Hospital Stroke Program
 Agenda Stroke Recognition Sandra K Hanson, MD Medical Director United Hospital Stroke Program Vascular anatomy NIH Stroke Scale Recognizing the hard to recognize Distinguishing stroke mimics 1 Symptoms
Agenda Stroke Recognition Sandra K Hanson, MD Medical Director United Hospital Stroke Program Vascular anatomy NIH Stroke Scale Recognizing the hard to recognize Distinguishing stroke mimics 1 Symptoms
TIA: Updates and Management 2008
 TIA: Updates and Management 2008 S. Andrew Josephson, MD Department of Neurology, Neurovascular Division University of California San Francisco Commonly Held TIA Misconceptions TIA is easy to diagnose
TIA: Updates and Management 2008 S. Andrew Josephson, MD Department of Neurology, Neurovascular Division University of California San Francisco Commonly Held TIA Misconceptions TIA is easy to diagnose
It s Always a Stroke; Except For When It s Not..
 It s Always a Stroke; Except For When It s Not.. TREVOR PHINNEY, D.O. Disclosures No Relevant Disclosures 1 Objectives Discuss variables of differential diagnosis for stroke Review when to TPA and when
It s Always a Stroke; Except For When It s Not.. TREVOR PHINNEY, D.O. Disclosures No Relevant Disclosures 1 Objectives Discuss variables of differential diagnosis for stroke Review when to TPA and when
Posterior Circulation Stroke
 Posterior Circulation Stroke Brett Kissela, MD, MS Professor and Chair Department of Neurology and Rehabilitation Medicine Senior Associate Dean of Clinical Research University of Cincinnati College of
Posterior Circulation Stroke Brett Kissela, MD, MS Professor and Chair Department of Neurology and Rehabilitation Medicine Senior Associate Dean of Clinical Research University of Cincinnati College of
Vascular Disorders. Nervous System Disorders (Part B-1) Module 8 -Chapter 14. Cerebrovascular disease S/S 1/9/2013
 Module 8 -Chapter 14. Cerebrovascular disease S/S 1/9/2013") Nervous System Disorders (Part B-1) Module 8 -Chapter 14 Overview ACUTE NEUROLOGIC DISORDERS Vascular Disorders Infections/Inflammation/Toxins Metabolic, Endocrinologic, Nutritional, Toxic Neoplastic Traumatic
Nervous System Disorders (Part B-1) Module 8 -Chapter 14 Overview ACUTE NEUROLOGIC DISORDERS Vascular Disorders Infections/Inflammation/Toxins Metabolic, Endocrinologic, Nutritional, Toxic Neoplastic Traumatic
Acute stroke. Ischaemic stroke. Characteristics. Temporal classification. Clinical features. Interpretation of Emergency Head CT
 Ischaemic stroke Characteristics Stroke is the third most common cause of death in the UK, and the leading cause of disability. 80% of strokes are ischaemic Large vessel occlusive atheromatous disease
Ischaemic stroke Characteristics Stroke is the third most common cause of death in the UK, and the leading cause of disability. 80% of strokes are ischaemic Large vessel occlusive atheromatous disease
Stroke & the Emergency Department. Dr. Barry Moynihan, March 2 nd, 2012
 Stroke & the Emergency Department Dr. Barry Moynihan, March 2 nd, 2012 Outline Primer Stroke anatomy & clinical syndromes Diagnosing stroke Anterior / Posterior Thrombolysis Haemorrhage The London model
Stroke & the Emergency Department Dr. Barry Moynihan, March 2 nd, 2012 Outline Primer Stroke anatomy & clinical syndromes Diagnosing stroke Anterior / Posterior Thrombolysis Haemorrhage The London model
Stroke - Intracranial hemorrhage. Dr. Amitesh Aggarwal Associate Professor Department of Medicine
 Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
Vague Neurological Conditions
 Vague Neurological Conditions Dr. John Lefebre, MD, FRCPC Chief Regional Medical Director Europe, India, South Africa, Middle East and Turkey Canada 2014 2 3 4 Agenda Dr. John Lefebre, M.D., FRCPC 1. TIA
Vague Neurological Conditions Dr. John Lefebre, MD, FRCPC Chief Regional Medical Director Europe, India, South Africa, Middle East and Turkey Canada 2014 2 3 4 Agenda Dr. John Lefebre, M.D., FRCPC 1. TIA
Unclogging The Pipes. Zahraa Rabeeah MD Chief Resident February 9,2018
 Unclogging The Pipes Zahraa Rabeeah MD Chief Resident February 9,2018 Please join Polleverywhere by texting: ZRABEEAH894 to 37607 Disclosures None Objectives Delineate the differences between TPA vs thrombectomy
Unclogging The Pipes Zahraa Rabeeah MD Chief Resident February 9,2018 Please join Polleverywhere by texting: ZRABEEAH894 to 37607 Disclosures None Objectives Delineate the differences between TPA vs thrombectomy
How to Think like a Neurologist Review of Exam Process and Assessment Findings
 Lehigh Valley Health Network LVHN Scholarly Works Neurology Update for the Non-Neurologist 2013 Neurology Update for the Non-Neurologist Feb 20th, 5:10 PM - 5:40 PM How to Think like a Neurologist Review
Lehigh Valley Health Network LVHN Scholarly Works Neurology Update for the Non-Neurologist 2013 Neurology Update for the Non-Neurologist Feb 20th, 5:10 PM - 5:40 PM How to Think like a Neurologist Review
 CLINICAL FEATURES THAT SUPPORT ATHEROSCLEROTIC STROKE 1. cerebral cortical impairment (aphasia, neglect, restricted motor involvement, etc.) or brain stem or cerebellar dysfunction 2. lacunar clinical
CLINICAL FEATURES THAT SUPPORT ATHEROSCLEROTIC STROKE 1. cerebral cortical impairment (aphasia, neglect, restricted motor involvement, etc.) or brain stem or cerebellar dysfunction 2. lacunar clinical
MEET 2007: Evaluation and treatment of the stroke and TIA patient for the non-neurointerventionist. neurointerventionist
 MEET 2007: Evaluation and treatment of the stroke and TIA patient for the non-neurointerventionist neurointerventionist Steve Ramee, MD Ochsner Medical Center New Orleans DISCLOSURE Nothing Nothing to
MEET 2007: Evaluation and treatment of the stroke and TIA patient for the non-neurointerventionist neurointerventionist Steve Ramee, MD Ochsner Medical Center New Orleans DISCLOSURE Nothing Nothing to
TIA Transient Ischaemic Attack?
 TIA Transient Ischaemic Attack? OR Transient loss of function (TLOF) Tal Anjum Consultant Stroke Physician, Morriston Hospital Training & education lead, WASP (Welsh Association of Stroke Physicians) Qs.
TIA Transient Ischaemic Attack? OR Transient loss of function (TLOF) Tal Anjum Consultant Stroke Physician, Morriston Hospital Training & education lead, WASP (Welsh Association of Stroke Physicians) Qs.
Blood Supply. Allen Chung, class of 2013
 Blood Supply Allen Chung, class of 2013 Objectives Understand the importance of the cerebral circulation. Understand stroke and the types of vascular problems that cause it. Understand ischemic penumbra
Blood Supply Allen Chung, class of 2013 Objectives Understand the importance of the cerebral circulation. Understand stroke and the types of vascular problems that cause it. Understand ischemic penumbra
Approach to a Neurologic Diagnosis
 Approach to a Neurologic Diagnosis Neurologic Diagnosis History Physical & Neurological Examination Ancillary Procedures 3 Questions Asked Focal neurologic deficits Increased intracranial pressure Signs
Approach to a Neurologic Diagnosis Neurologic Diagnosis History Physical & Neurological Examination Ancillary Procedures 3 Questions Asked Focal neurologic deficits Increased intracranial pressure Signs
Starting or Resuming Anticoagulation or Antiplatelet Therapy after ICH: A Neurology Perspective
 Starting or Resuming Anticoagulation or Antiplatelet Therapy after ICH: A Neurology Perspective Cathy Sila MD George M Humphrey II Professor and Vice Chair of Neurology Director, Comprehensive Stroke Center
Starting or Resuming Anticoagulation or Antiplatelet Therapy after ICH: A Neurology Perspective Cathy Sila MD George M Humphrey II Professor and Vice Chair of Neurology Director, Comprehensive Stroke Center
Divine Intervention Episode 58 Neurology Clerkship Shelf Review Part 7. Some PGY1
 Divine Intervention Episode 58 Neurology Clerkship Shelf Review Part 7 Some PGY1 1 Discussion of the pathway/information carried by the 3 HY spinal cord tracts (DCMLS, STT, CST). Description of the Romberg
Divine Intervention Episode 58 Neurology Clerkship Shelf Review Part 7 Some PGY1 1 Discussion of the pathway/information carried by the 3 HY spinal cord tracts (DCMLS, STT, CST). Description of the Romberg
Management of Acute Ischemic Stroke. Learning Objec=ves. What is a Stroke? Jen Simpson Neurohospitalist
 Management of Acute Ischemic Stroke Jen Simpson Neurohospitalist Learning Objec=ves Iden=fy signs/symptoms of stroke Recognize pa=ents who may be eligible for treatment of acute stroke What is a Stroke?
Management of Acute Ischemic Stroke Jen Simpson Neurohospitalist Learning Objec=ves Iden=fy signs/symptoms of stroke Recognize pa=ents who may be eligible for treatment of acute stroke What is a Stroke?
Management of TIA. Dr Ali Ali Consultant Stroke and Geriatrics Royal Hallamshire Hospital
 Management of TIA Dr Ali Ali Consultant Stroke and Geriatrics Royal Hallamshire Hospital Objectives Definition TIA and stroke TIA: Diagnosis & mimics Risk assessment Referral and emergency management Secondary
Management of TIA Dr Ali Ali Consultant Stroke and Geriatrics Royal Hallamshire Hospital Objectives Definition TIA and stroke TIA: Diagnosis & mimics Risk assessment Referral and emergency management Secondary
MD SUBTYPE ADJUDICATION VARIABLE DEFINITIONS MANUAL The following is a list of variables and how to complete each one:
 MD SUBTYPE ADJUDICATION VARIABLE DEFINITIONS MANUAL 2014-15 The following is a list of variables and how to complete each one: (PHY-1) Case, per physician review: The most important task for the physicians
MD SUBTYPE ADJUDICATION VARIABLE DEFINITIONS MANUAL 2014-15 The following is a list of variables and how to complete each one: (PHY-1) Case, per physician review: The most important task for the physicians
Patent Foramen Ovale and Cryptogenic Stroke: Do We Finally Have Closure? Christopher Streib, MD, MS
 Patent Foramen Ovale and Cryptogenic Stroke: Do We Finally Have Closure? Christopher Streib, MD, MS 11-8-18 Outline 1. Background 2. Anatomy of patent foramen ovale (PFO) 3. Relationship between PFO and
Patent Foramen Ovale and Cryptogenic Stroke: Do We Finally Have Closure? Christopher Streib, MD, MS 11-8-18 Outline 1. Background 2. Anatomy of patent foramen ovale (PFO) 3. Relationship between PFO and
Cerebral Vascular Diseases. Nabila Hamdi MD, PhD
 Cerebral Vascular Diseases Nabila Hamdi MD, PhD Outline I. Stroke statistics II. Cerebral circulation III. Clinical symptoms of stroke IV. Pathogenesis of cerebral infarcts (Stroke) 1. Ischemic - Thrombotic
Cerebral Vascular Diseases Nabila Hamdi MD, PhD Outline I. Stroke statistics II. Cerebral circulation III. Clinical symptoms of stroke IV. Pathogenesis of cerebral infarcts (Stroke) 1. Ischemic - Thrombotic
Neurosurgical Management of Stroke
 Overview Hemorrhagic Stroke Ischemic Stroke Aneurysmal Subarachnoid hemorrhage Neurosurgical Management of Stroke Jesse Liu, MD Instructor, Neurological Surgery Initial management In hospital management
Overview Hemorrhagic Stroke Ischemic Stroke Aneurysmal Subarachnoid hemorrhage Neurosurgical Management of Stroke Jesse Liu, MD Instructor, Neurological Surgery Initial management In hospital management
It s Not All One Sided. James Smith, MD (Smitty)
") It s Not All One Sided James Smith, MD (Smitty) Disclosures Chair, NE State EMS Board Medical Director, Emergency Services, GPH Medical Director, GPH LifeNet, NPFD, Maxwell, Tryon, Chase County, NP Rec
It s Not All One Sided James Smith, MD (Smitty) Disclosures Chair, NE State EMS Board Medical Director, Emergency Services, GPH Medical Director, GPH LifeNet, NPFD, Maxwell, Tryon, Chase County, NP Rec
Acute Stroke Management LUKE BRADBURY, MD 10/8/14 FALL WAPA CONFERENCE
 Objectives Acute Stroke Management LUKE BRADBURY, MD 10/8/14 FALL WAPA CONFERENCE Recognize the clinical signs of acute stroke Differentiate between stroke and some of the more common stroke mimics Review
Objectives Acute Stroke Management LUKE BRADBURY, MD 10/8/14 FALL WAPA CONFERENCE Recognize the clinical signs of acute stroke Differentiate between stroke and some of the more common stroke mimics Review
Stroke in the ED. Dr. William Whiteley. Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian
 Stroke in the ED Dr. William Whiteley Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian 2016 RCP Guideline for Stroke RCP guidelines for acute ischaemic stroke
Stroke in the ED Dr. William Whiteley Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian 2016 RCP Guideline for Stroke RCP guidelines for acute ischaemic stroke
Redgrave JN, Coutts SB, Schulz UG et al. Systematic review of associations between the presence of acute ischemic lesions on
 6. Imaging in TIA 6.1 What type of brain imaging should be used in suspected TIA? 6.2 Which patients with suspected TIA should be referred for urgent brain imaging? Evidence Tables IMAG1: After TIA/minor
6. Imaging in TIA 6.1 What type of brain imaging should be used in suspected TIA? 6.2 Which patients with suspected TIA should be referred for urgent brain imaging? Evidence Tables IMAG1: After TIA/minor
P1: OTA/XYZ P2: ABC c01 BLBK231-Ginsberg December 23, :43 Printer Name: Yet to Come. Part 1. The Neurological Approach COPYRIGHTED MATERIAL
 Part 1 The Neurological Approach COPYRIGHTED MATERIAL 1 2 Chapter 1 Neurological history-taking The diagnosis and management of diseases of the nervous system have been revolutionized in recent years by
Part 1 The Neurological Approach COPYRIGHTED MATERIAL 1 2 Chapter 1 Neurological history-taking The diagnosis and management of diseases of the nervous system have been revolutionized in recent years by
Brain Attacks and Acute Stroke Management
 Brain Attacks and Acute Stroke Management WWW.RN.ORG Reviewed January, 2017, Expires January, 2019 Provider Information and Specifics available on our Website Unauthorized Distribution Prohibited 2017
Brain Attacks and Acute Stroke Management WWW.RN.ORG Reviewed January, 2017, Expires January, 2019 Provider Information and Specifics available on our Website Unauthorized Distribution Prohibited 2017
A Hypothesis Driven Approach to the Neurological Exam
 A Hypothesis Driven Approach to the Neurological Exam Vanja Douglas, MD Assistant Clinical Professor UCSF Department of Neurology Disclosures None 1 Purpose of Neuro Exam Screen asymptomatic patients Screen
A Hypothesis Driven Approach to the Neurological Exam Vanja Douglas, MD Assistant Clinical Professor UCSF Department of Neurology Disclosures None 1 Purpose of Neuro Exam Screen asymptomatic patients Screen
THE CERVICAL SPINE: WHAT GUIDES CURRENT 'BEST PRACTICE' IN OSTEOPATHY?
 THE CERVICAL SPINE: WHAT GUIDES CURRENT 'BEST PRACTICE' IN OSTEOPATHY? LOS 20th May 2008 Laurence Butler BA(hons); DO(hons); MSc/D.Ost My thanks go to: Barry Jacobs (slides on cervical rotation) Steve
THE CERVICAL SPINE: WHAT GUIDES CURRENT 'BEST PRACTICE' IN OSTEOPATHY? LOS 20th May 2008 Laurence Butler BA(hons); DO(hons); MSc/D.Ost My thanks go to: Barry Jacobs (slides on cervical rotation) Steve
Lacunar Infarct. Dr. Tapas Kumar Banerjee Medical Director & Chief Consultant Neurologist National Neurosciences Centre Calcutta
 Lacunar Infarct Dr. Tapas Kumar Banerjee Medical Director & Chief Consultant Neurologist National Neurosciences Centre Calcutta Aetiologies of Ischemic Stroke Atherothrombo-embolic Cardio-embolic Aetiologies
Lacunar Infarct Dr. Tapas Kumar Banerjee Medical Director & Chief Consultant Neurologist National Neurosciences Centre Calcutta Aetiologies of Ischemic Stroke Atherothrombo-embolic Cardio-embolic Aetiologies
ANASTAMOSIS FOR BRAIN STEM ISCHEMIA/Khodadad et al.
 ANASTAMOSIS FOR BRAIN STEM ISCHEMIA/Khodadad et al. visualization of the posterior inferior cerebellar artery. The patient, now 11 months post-operative, has shown further neurological improvement since
ANASTAMOSIS FOR BRAIN STEM ISCHEMIA/Khodadad et al. visualization of the posterior inferior cerebellar artery. The patient, now 11 months post-operative, has shown further neurological improvement since
Pre-Hospital Stroke Care: Bringing It To The Street. by Bob Atkins, NREMT-Paramedic AEMD EMS Director Bedford Regional Medical Center
 Pre-Hospital Stroke Care: Bringing It To The Street by Bob Atkins, NREMT-Paramedic AEMD EMS Director Bedford Regional Medical Center Overview/Objectives Explain the reasons or rational behind the importance
Pre-Hospital Stroke Care: Bringing It To The Street by Bob Atkins, NREMT-Paramedic AEMD EMS Director Bedford Regional Medical Center Overview/Objectives Explain the reasons or rational behind the importance
STROKE INTRODUCTION OBJECTIVES. When the student has finished this module, he/she will be able to:
 STROKE INTRODUCTION Stroke is the medical term for a specific type of neurological event that causes damage to the brain. There are two types of stroke, but both types of stroke cause the same type of
STROKE INTRODUCTION Stroke is the medical term for a specific type of neurological event that causes damage to the brain. There are two types of stroke, but both types of stroke cause the same type of
Stroke Transfer Checklist
 Stroke Transfer Checklist When preparing to transfer an acute stroke patient to the UF Health Shands Comprehensive Stroke Center, please make every attempt to include the following information: Results
Stroke Transfer Checklist When preparing to transfer an acute stroke patient to the UF Health Shands Comprehensive Stroke Center, please make every attempt to include the following information: Results
Permanent foramen ovale: when to close?
 Permanent foramen ovale: when to close? Pierre Amarenco INSERM U-698 and Denis Diderot University - Paris VII Department of Neurology and Stroke Center Bichat hospital, Paris, France PFO - Pathology TEE
Permanent foramen ovale: when to close? Pierre Amarenco INSERM U-698 and Denis Diderot University - Paris VII Department of Neurology and Stroke Center Bichat hospital, Paris, France PFO - Pathology TEE
Adequacy of Initial History and Physical Examination
 October 13 th 2015 I am an Associate Professor in the Department of Emergency Medicine, University of Ottawa. I have expertise in Emergency Medicine and hold a certificate of special competency with the
October 13 th 2015 I am an Associate Professor in the Department of Emergency Medicine, University of Ottawa. I have expertise in Emergency Medicine and hold a certificate of special competency with the
NEURORADIOLOGY DIL part 4
 NEURORADIOLOGY DIL part 4 Strokes and infarcts K. Agyem MD, G. Hall MD, D. Palathinkal MD, Alexandre Menard March/April 2015 OVERVIEW Introduction to Neuroimaging - DIL part 1 Basic Brain Anatomy - DIL
NEURORADIOLOGY DIL part 4 Strokes and infarcts K. Agyem MD, G. Hall MD, D. Palathinkal MD, Alexandre Menard March/April 2015 OVERVIEW Introduction to Neuroimaging - DIL part 1 Basic Brain Anatomy - DIL
Disclosure Statement: Dr. Knoefel has nothing to disclose
 Stroke Janice E. Knoefel, MD, MPH Professor of Medicine & Neurology University of New Mexico Geriatrics/Extended Care (retired) New Mexico VA Healthcare System Albuquerque, NM Disclosure Statement: Dr.
Stroke Janice E. Knoefel, MD, MPH Professor of Medicine & Neurology University of New Mexico Geriatrics/Extended Care (retired) New Mexico VA Healthcare System Albuquerque, NM Disclosure Statement: Dr.
Imaging Acute Stroke and Cerebral Ischemia
 Department of Radiology University of California San Diego Imaging Acute Stroke and Cerebral Ischemia John R. Hesselink, M.D. Causes of Stroke Arterial stenosis Thrombosis Embolism Dissection Hypotension
Department of Radiology University of California San Diego Imaging Acute Stroke and Cerebral Ischemia John R. Hesselink, M.D. Causes of Stroke Arterial stenosis Thrombosis Embolism Dissection Hypotension
Management of intracranial atherosclerotic stenosis (ICAS)/intracranial atherosclerosis
/intracranial atherosclerosis") Management of intracranial atherosclerotic stenosis (ICAS)/intracranial atherosclerosis Tim Mikesell, D.O. Oct 22, 2016 Stroke facts Despite progress in decreasing stroke incidence and mortality, stroke
Management of intracranial atherosclerotic stenosis (ICAS)/intracranial atherosclerosis Tim Mikesell, D.O. Oct 22, 2016 Stroke facts Despite progress in decreasing stroke incidence and mortality, stroke
Cerebrovascular Disease. RTC Conference Resident Presenter: Dr. Christina Bailey Faculty: Dr. Jeff Dattilo October 2, 2009
 Cerebrovascular Disease RTC Conference Resident Presenter: Dr. Christina Bailey Faculty: Dr. Jeff Dattilo October 2, 2009 Cerebrovascular Disease Stroke is the 3 rd leading cause of death and the leading
Cerebrovascular Disease RTC Conference Resident Presenter: Dr. Christina Bailey Faculty: Dr. Jeff Dattilo October 2, 2009 Cerebrovascular Disease Stroke is the 3 rd leading cause of death and the leading
Stroke Update. Lacunar 19% Thromboembolic 6% SAH 13% ICH 13% Unknown 32% Hemorrhagic 26% Ischemic 71% Other 3% Cardioembolic 14%
 Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
GENERAL PRINCIPLES OF NEUROLOGY- John W. Day, M.D., Ph.D.
 I. TAKE HOME POINTS FOR THIS LECTURE A. Localizing the disease is the first step in diagnosing a neurological disorder. B. Time course of the disease (acute, subacute, or chronic) indicates the pathophysiological
I. TAKE HOME POINTS FOR THIS LECTURE A. Localizing the disease is the first step in diagnosing a neurological disorder. B. Time course of the disease (acute, subacute, or chronic) indicates the pathophysiological
THE BRAINSTEM. Raymond S. Price, MD University of Pennsylvania
 THE BRAINSTEM Raymond S. Price, MD University of Pennsylvania Overview of Brainstem Functions The brainstem serves numerous crucial neurologic functions. The most clinically relevant functions include:
THE BRAINSTEM Raymond S. Price, MD University of Pennsylvania Overview of Brainstem Functions The brainstem serves numerous crucial neurologic functions. The most clinically relevant functions include:
Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine
 Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine Institute The Oregon Clinic Disclosure I declare that neither
Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine Institute The Oregon Clinic Disclosure I declare that neither
The Language of Stroke
 The Language of Stroke Examination / Imaging / Diagnosis / Treatment Dr Suzanne Busch A lot of letters! CBF CVA ICH CVD CBV DWI US MRI/MRA CAA CTA CTP ICA MCA SAH WMD TIA MCA Agnosia A lot of big words!
The Language of Stroke Examination / Imaging / Diagnosis / Treatment Dr Suzanne Busch A lot of letters! CBF CVA ICH CVD CBV DWI US MRI/MRA CAA CTA CTP ICA MCA SAH WMD TIA MCA Agnosia A lot of big words!
Cerebrovascular Disease
 Cerebrovascular Disease I. INTRODUCTION Cerebrovascular disease (CVD) includes all disorders in which an area of the brain is transiently or permanently affected by ischemia or bleeding and one or more
Cerebrovascular Disease I. INTRODUCTION Cerebrovascular disease (CVD) includes all disorders in which an area of the brain is transiently or permanently affected by ischemia or bleeding and one or more
CEREBROVASCULAR ANATOMY
 No disclosures STROKE SYNDROMES Andrew Huffer 32 nd Annual Review Course in Physical Medicine and Rehabilitation March 20, 2105 Overview Anatomy General Principles Large vessel Thromboembolism Anterior
No disclosures STROKE SYNDROMES Andrew Huffer 32 nd Annual Review Course in Physical Medicine and Rehabilitation March 20, 2105 Overview Anatomy General Principles Large vessel Thromboembolism Anterior
Spinal Cord: Clinical Applications. Dr. Stuart Inglis
 Spinal Cord: Clinical Applications Dr. Stuart Inglis Tabes dorsalis, also known as syphilitic myelopathy, is a slow degeneration (specifically, demyelination) of the nerves in the dorsal funiculus of the
Spinal Cord: Clinical Applications Dr. Stuart Inglis Tabes dorsalis, also known as syphilitic myelopathy, is a slow degeneration (specifically, demyelination) of the nerves in the dorsal funiculus of the
CRANIAL NERVES. Dr. Amani A. Elfaki Associate Professor Department of Anatomy
 CRANIAL NERVES Dr. Amani A. Elfaki Associate Professor Department of Anatomy LEARNING OBJECTIVES Named the cranial nerves Identify the funcunal component of each cranial nerve Identify the effect of each
CRANIAL NERVES Dr. Amani A. Elfaki Associate Professor Department of Anatomy LEARNING OBJECTIVES Named the cranial nerves Identify the funcunal component of each cranial nerve Identify the effect of each
Code Stroke!! Amit Kansara, MD, FAHA. Joint EMS Conference Providence Brain and Spine Institute Providence Heart and Vascular Institute
 Code Stroke!! Amit Kansara, MD, FAHA Joint EMS Conference Providence Brain and Spine Institute Providence Heart and Vascular Institute February 22, 2019 Patient History: Dispatch 20:45: You are dispatched
Code Stroke!! Amit Kansara, MD, FAHA Joint EMS Conference Providence Brain and Spine Institute Providence Heart and Vascular Institute February 22, 2019 Patient History: Dispatch 20:45: You are dispatched
TIAs and posterior circulation problems
 TIAs and posterior circulation problems A/Professor Helen Dewey Head, Stroke Service Austin Health Austin Health How many strokes and TIAs are out there? depends on the definition! ~60,000 strokes in
TIAs and posterior circulation problems A/Professor Helen Dewey Head, Stroke Service Austin Health Austin Health How many strokes and TIAs are out there? depends on the definition! ~60,000 strokes in
REVIEW OF HEAD AND NECK CRANIAL NERVES AND EVERYTHING ELSE
 REVIEW OF HEAD AND NECK CRANIAL NERVES AND EVERYTHING ELSE OLFACTORY NERVE CN I ANTERIOR CRANIAL FOSSA CRISTA GALLI OF ETHMOID OLFACTORY FORAMINA IN CRIBIFORM PLATE OF ETHMOID BONE CN I OLFACTORY NERVE
REVIEW OF HEAD AND NECK CRANIAL NERVES AND EVERYTHING ELSE OLFACTORY NERVE CN I ANTERIOR CRANIAL FOSSA CRISTA GALLI OF ETHMOID OLFACTORY FORAMINA IN CRIBIFORM PLATE OF ETHMOID BONE CN I OLFACTORY NERVE
HEAD AND NECK ANATOMY PRACTICE QUESTIONS
 HEAD AND NECK ANATOMY PRACTICE QUESTIONS 1. A patient complains that he has lost sensation on his face and that the skin of his face feels numb. The physician tests tactile acuity by touching the forehead
HEAD AND NECK ANATOMY PRACTICE QUESTIONS 1. A patient complains that he has lost sensation on his face and that the skin of his face feels numb. The physician tests tactile acuity by touching the forehead
Essentials of Clinical MR, 2 nd edition. 14. Ischemia and Infarction II
 14. Ischemia and Infarction II Lacunar infarcts are small deep parenchymal lesions involving the basal ganglia, internal capsule, thalamus, and brainstem. The vascular supply of these areas includes the
14. Ischemia and Infarction II Lacunar infarcts are small deep parenchymal lesions involving the basal ganglia, internal capsule, thalamus, and brainstem. The vascular supply of these areas includes the
Difficult Diagnosis: An Interactive Session
 Difficult Diagnosis: An Interactive Session W A D E S M I T H, M. D. D E P T. O F N E U R O L O G Y, U C S F F E B R U A R Y 1 5, 2 0 1 3 58-year-old man with HTN and HLD Recurrent episodes of dizziness
Difficult Diagnosis: An Interactive Session W A D E S M I T H, M. D. D E P T. O F N E U R O L O G Y, U C S F F E B R U A R Y 1 5, 2 0 1 3 58-year-old man with HTN and HLD Recurrent episodes of dizziness
Stroke Mimics. Paul Guyler
 Stroke Mimics Paul Guyler Consultant Stroke Physician at Southend University Hospital Clinical Lead for Acute Stroke Essex Cardiac and Stroke Network Aims Why worry? Stroke Recognition Tools History, Examination
Stroke Mimics Paul Guyler Consultant Stroke Physician at Southend University Hospital Clinical Lead for Acute Stroke Essex Cardiac and Stroke Network Aims Why worry? Stroke Recognition Tools History, Examination
57y WRH woman, controlled HTN only, presents with sudden LOC, fixed and dilated, quadraplegic Intubated on arrival and CT is negative CTA and CTP
 Case # 1 Hx 57y WRH woman, controlled HTN only, presents with sudden LOC, fixed and dilated, quadraplegic Intubated on arrival and CT is negative CTA and CTP show left PCA occlusion, some basilar stenosis,
Case # 1 Hx 57y WRH woman, controlled HTN only, presents with sudden LOC, fixed and dilated, quadraplegic Intubated on arrival and CT is negative CTA and CTP show left PCA occlusion, some basilar stenosis,
Stroke Awareness. Presented by: Duane Anderson, MD Snoqualmie Valley Hospital Emergency Department Medical Director
 Stroke Awareness Presented by: Duane Anderson, MD Snoqualmie Valley Hospital Emergency Department Medical Director What is a stroke? Stroke can happen to anyone. Stroke is the fourth leading cause of death
Stroke Awareness Presented by: Duane Anderson, MD Snoqualmie Valley Hospital Emergency Department Medical Director What is a stroke? Stroke can happen to anyone. Stroke is the fourth leading cause of death
Page 1 CVHNS Bulletin, Volume 13, Issue 1, Spring, 2018
 Page 1 CVHNS Bulletin, Volume 13, Issue 1, Spring, 2018 The Bulletin Welcome to the Cardiovascular Health Nova Scotia (CVHNS) e-mail bulletin, produced 3 times annually. The Bulletin has been created to
Page 1 CVHNS Bulletin, Volume 13, Issue 1, Spring, 2018 The Bulletin Welcome to the Cardiovascular Health Nova Scotia (CVHNS) e-mail bulletin, produced 3 times annually. The Bulletin has been created to
PFO closure group total no. PFO closure group no. of males
 Suppl Table. Characteristics of the five trials included in this meta-analysis. Trial name Device used for Definition of medical Primary Endpoint group total no. group no. of males group age (yrs) group
Suppl Table. Characteristics of the five trials included in this meta-analysis. Trial name Device used for Definition of medical Primary Endpoint group total no. group no. of males group age (yrs) group
Pathophysiology. Central Nervous System (CNS) Peripheral Nervous System (PNS) Consists of. Consists of brain/spinal
 Peripheral Nervous System (PNS) Consists of. Consists of brain/spinal") Neurological Emergencies Pathophysiology Central Nervous System (CNS) Consists of brain/spinal cord Peripheral Nervous System (PNS) Consists of everything else Afferent (sensory) Efferent (motor) Autonomic
Neurological Emergencies Pathophysiology Central Nervous System (CNS) Consists of brain/spinal cord Peripheral Nervous System (PNS) Consists of everything else Afferent (sensory) Efferent (motor) Autonomic
Code Stroke in real life. Disclosures. Parkland Memorial Hospital. I have no disclosures. Has 1 million patient visits annually. Level 1 Trauma Center
 Code Stroke in real life Alejandro Magadán, M.D. University of Texas Southwestern Medical Center Medical Director for Stroke Parkland Memorial Hospital Disclosures I have no disclosures Parkland Memorial
Code Stroke in real life Alejandro Magadán, M.D. University of Texas Southwestern Medical Center Medical Director for Stroke Parkland Memorial Hospital Disclosures I have no disclosures Parkland Memorial
Definition of Stroke. Non modifiable Risk Factors. Modifiable Risk Factors. Modifiable Risk Factors cont.. STROKE Rehabilitation 3/28/2013
 Definition of Stroke STROKE Rehabilitation Sudden focal neurological deficit secondary to occlusion or rupture of blood vessels supplying the brain. TIA (transient ischemic attack)= stroke symptoms that
Definition of Stroke STROKE Rehabilitation Sudden focal neurological deficit secondary to occlusion or rupture of blood vessels supplying the brain. TIA (transient ischemic attack)= stroke symptoms that
VISUAL REFLEXES. B. The oculomotor nucleus, Edinger-Westphal nucleus, and oculomotor nerve at level of the superior colliculus.
 Neuroanatomy Suzanne Stensaas February 24, 2011, 10:00-12:00 p.m. Reading: Waxman Ch. 15 HyperBrain: Ch 7 with quizzes and or Lab 7 videotape http://www-medlib.med.utah.edu/kw/hyperbrain/anim/reflex.html
Neuroanatomy Suzanne Stensaas February 24, 2011, 10:00-12:00 p.m. Reading: Waxman Ch. 15 HyperBrain: Ch 7 with quizzes and or Lab 7 videotape http://www-medlib.med.utah.edu/kw/hyperbrain/anim/reflex.html
PFO Management update
 PFO Management update May 12, 2017 Peter Casterella, MD Swedish Heart and Vascular 1 PFO Update 2017: Objectives Review recently released late outcomes of RESPECT trial and subsequent FDA approval of PFO
PFO Management update May 12, 2017 Peter Casterella, MD Swedish Heart and Vascular 1 PFO Update 2017: Objectives Review recently released late outcomes of RESPECT trial and subsequent FDA approval of PFO
TACLS-Chapter-2-Body-Structure.pdf Essential Resources
 Stroke Network 1. http://www.strokebestpractices.ca/wp-content/uploads/2016/01/ TACLS-Chapter-2-Body-Structure.pdf Essential Resources Stroke Rehabilitation Unit Orientation Module 1: Pathophysiology of
Stroke Network 1. http://www.strokebestpractices.ca/wp-content/uploads/2016/01/ TACLS-Chapter-2-Body-Structure.pdf Essential Resources Stroke Rehabilitation Unit Orientation Module 1: Pathophysiology of
Evaluation of the Dizzy Patient
 Evaluation of the Dizzy Patient S. Andrew Josephson, MD Department of Neurology University of California San Francisco October 1, 2007 Who Sees Dizzy Patients? ED physicians Internists Neurologists ENT
Evaluation of the Dizzy Patient S. Andrew Josephson, MD Department of Neurology University of California San Francisco October 1, 2007 Who Sees Dizzy Patients? ED physicians Internists Neurologists ENT
Stroke Workshop. Pre-Workshop Handout. With Walter Himmel, Meeta Patel & Anton Helman
 2018 Stroke Workshop Pre-Workshop Handout With Walter Himmel, Meeta Patel & Anton Helman Instructions for Getting the Most Out of The EMU Stroke Workshop Handout This workshop has been designed around
2018 Stroke Workshop Pre-Workshop Handout With Walter Himmel, Meeta Patel & Anton Helman Instructions for Getting the Most Out of The EMU Stroke Workshop Handout This workshop has been designed around
WHAT IS A STROKE? What causes a stroke? What disabilities can result from a stroke?
 Know Stroke Stroke is the third leading cause of death in the United States and a leading cause of serious, long-term disability in adults. About 600,000 new strokes are reported in the U.S. each year.
Know Stroke Stroke is the third leading cause of death in the United States and a leading cause of serious, long-term disability in adults. About 600,000 new strokes are reported in the U.S. each year.