Headache Board Review: Pharmacology of Drugs, Guidelines and Evidence-Based
|
|
|
- Alexander Hopkins
- 6 years ago
- Views:
Transcription
1 Headache Board Review: Pharmacology of Drugs, Guidelines and Evidence-Based Medicine Michael Marmura Thomas Jefferson University Department of Neurology, Jefferson Headache Center June 9,
2 Disclosures: Dr. Marmura has royalty payments from Cambridge, Devos Medical, and Medlink Neurology. He receives salary support from Teva for work as a principal investigator in clinical trials and has received compensation for consultations from Teva and Supernus. This talk discusses therapeutic treatments for headache, h many of which hare off-label. l He will discuss which are FDA-approved and which are not during this lecture.
3 Objectives: Summarize the mechanism of action for known preventive and acute pharmacologic treatments for headache. Differentiate medications which have the greatest evidence for effectiveness in headache h based on published trials from treatments with no proven efficacy. Summarize recent guidelines for acute and preventive migraine treatment.
4 Key points: Know general principles p for treating acute migraine/cluster and preventing attacks Know mechanisms of action Know common and serious adverse events of essential medications Know evidence basis for commonly used medications Open-label studies/case reports are low yield
5 Preventive Treatment t
6 Why use preventatives? Too many headaches Too severe Too many acute medications (MOH) Too sick to take medications (contraindications) Too disabled Too little warning or severe for acute treatment to work Toomuchtodo(patientpreference) preference) Too much aura (i.e. hemiplegic migraine) Too scary PREVENTIVES ARE GENERALLY UNDERUTILIZED Lipton RB et al. Headache. 2001; Lipton RB et al. Neurology. 2002
7 Types of preventive treatment Pre-emptive For a known trigger e.g. exercise, sexual activity. Treat prior to exposure or activity. Short term prophylaxis For time-limited i exposure such as peri-menstrual. Ch i ti ( i f ) Chronic prevention (main focus) Treat on a regular basis for a long period of time.
8 Potential mechanisms of action of migraine preventives Inhibiting cortical spreading depression (CSD) Inhibiting peripheral/central sensitization Blocking neurogenic inflammation (release of inflammatory cytokines such as CGRP) Enhancing anti-nociception i Modulating autonomic nervous system tone Gap junction inhibition (to prevent CSD)





9 Migraine Prophylaxis and CSD Ayata et al Ann Neurol. 2006
10 Level of Evidence Level A: Established as effective (or ineffective) for acute migraine (supported by at least two Class I studies ). Level B: Probably effective (or ineffective) for acute migraine (supported by one Class I study or two Class II studies). Level C: Possibly effective (or ineffective) for acute migraine (supported by one Class II study or two Class III studies). Level U: Evidence is conflicting or inadequate to support or refute the use of the medication(s) for acute migraine. Gronseth et al. AAN Clinical Practice Guidelines Manual 2011 Edition.





11 Preventive Guidelines (Episodic Migraine) Neurology Apr 24;78(17):
12 receptor antagonists Non-selective * Propranolol (inderal) mg/d * Timolol (blocadren) mg/d Ndll( Nadolol (corgard) mg/d 1 selective Metoprolol (lopressor) Atenolol (tenormin) mg/d mg/d *FDA approved




13 Reduction in cortical excitability Treatment with betablockers in patients with migraine increases phosphene thresholds with transcranial magnetic stimulation Gerwig M et al. The Journal of Headache and Pain 2012
14 receptor antagonists: AEs CV: hypotension, bradycardia, fatigue decreased exercise tolerance, may worsen PVD and Raynaud disease CNS: drowsiness, nightmares, insomnia, depression (?) Other: masking symptoms of hypoglycemia rebound hypertension or tachycardia Potential uses: Hypertension, tachycardia, POTS, anxiety, essential tremor Recent data suggests depression-β-blocker link unlikely Ranchord A. American Heart Journal 2016
15 Antidepressants (none are Level A) Monoamine reuptake inhibitors non-selective (TCAs). Amitriptyline up to 75 mg selective serotonin reuptake inhibitors (SSRIs) fluoxetine? effective (chronic daily headache) serotonin and norepinephrine (SNRIs). Venlafaxine 150 mg Monoamine oxidase inhibitors (MAOIs) Anti-depressants do not work in HA by treating masked depression
16 TCAs Antidepressants amitriptyline has been consistently tl shown as effective as effective as propranolol and superior to placebo benefit is independent of antidepressant effect other TCAs: little evidence in migraine (nortriptyline is effective for neuropathic pain) SSRIs fluoxetine may be effective (chronic daily headache) SNRIs venlafaxine: migraine prevention dose 150 mg or greater
17 Tricyclic antidepressants - AEs Anti cholinergic-related dry mouth, constipation, tachycardia, palpitations, blurry vision (poor accommodation), urinary retention, confusion. Anti-adrenergic (α 1 )-related orthostatic hypotension Serotonergic nausea, sweating Anti histamine (H 1 )-related drowsiness, fatigue Na channel effect-related cardiac conduction delay. Other Weight gain, lowered seizure threshold, sexual dysfunction, mania.
18 Calcium Channel Antagonists Drugs Verapamil (unknown effectiveness in migraine) to 620mg/d Flunarizine (probably effective in migraine) - 5 to 10mg/d AEs Verapamil - constipation, AV block, CHF Flunarizine - weight gain, somnolence, dizziness, hypotension, extrapyramidal reactions Contraindications CHF, heart block, hypotension, sick sinus syndrome
19 Topiramate: Broad spectrum anticonvulsant used in migraine Antagonist of AMPA/kainate subtype of glutamate receptors (Main reason for effectiveness in migraine/epilepsy?) Augments the GABA A1 receptor (Less sedating than most anxiolytics) Blocks voltage-dependent calcium and sodium channels Inhibits carbonic anhydrase isoenzymes II and IV. (metabolic acidosis, paresthesias) May inhibit protein kinase activity (? weight regulation / glucose homeostasis) Possible serotonin activity on 5-HT 2C receptor (cause of weight loss?) Dose: mg/day given QD-BID. Available as extended release. Effective for migraine, chronic migraine, cluster headache AEs: weight loss, tingling, concentration /memory / language impairment, decrease sex hormone levels (>200 mg), pallinopsia, kidney stones, acute angle closure glaucoma Gryder DS J Neurosci. 2003; O Neil PM Obesity 2012
20
21 Topiramate for Chronic Migraine Headache: The Journal of Head and Face Pain Volume 47, Issue 2, pages , 13 FEB 2007 DOI: /j x
22 Divalproex Sodium Drug Valproic acid/sodium valproate (Depakote) mg/d Therapeutic blood level mcg/ml AEs Nausea, sedation, platelet dysfunction, hair loss, tremor, change in cognition, hepatotoxicity (young children), weight gain, pancreatitis, polycystic ovaries Comments Use in presence of co-morbid mania, epilepsy Check LFTs and CBC before and as needed during therapy Expert Opin Drug Metab Toxicol Apr;6(4):
23 Other Preventive Medications Cyproheptadine serotonin antogonist, antihistamine acts mostly at 5HT-1a and 5HT-2 receptors treats serotonin syndrome may reduce antidepressant effectiveness Gabapentin conflicting evidence, requires higher doses (1800+ mg) Candesartan 16 mg angiotensin receptor blocker Vitamins, Minerals, Herbs Riboflavin (B2) 400 mg Co- enzyme Q 10 Magnesium, Feverfew, Petadolex (Petasites hybridus)
24 Candesartan and Propanolol vs Placebo Copyright by International Headache Society Lars J Stovner et al. Cephalalgia 2013;
25 OnabotulinumtoxinA Injection Approved: Chronic Migraine (15 or more ha d 4 hours, 50% migraine/probable migraine PREEMPT 1 and 2 trials: U every 12 weeks Allows for additional i injections i (follow-the-pain strategy) AEs: neck pain, ptosis, weakness Mech of action: cleavage of SNAP-25, preventing acetylcholine vesicle binding and release at the motor end plate Other possible mechanism of actions in pain/migraine: effects on excitatory neurotransmitter release/fusion, spinal c-fos expression, epesso,cgrp Peease release
26


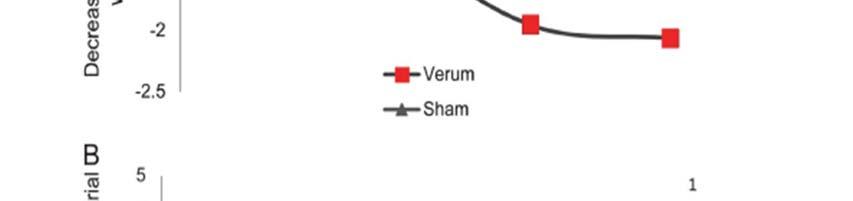
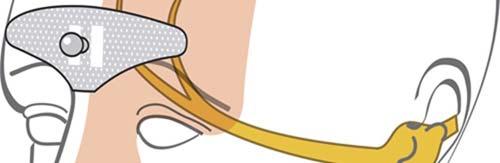




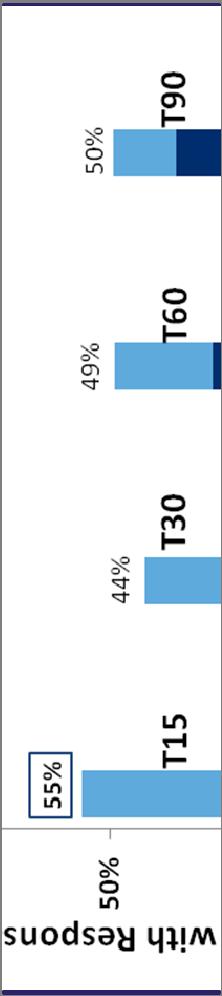
27 Supraorbital transcutaneous stimulator Schoenen J et al. Neurology 2013;80:

,")
28 Prevention of Cluster No large clinical trials with high level evidence Corticosteroids at cycle onset High dose verapamil ( mg) Lithium ( mg) Methysergide Divalproex sodium Topiramate Devices (VNS), OnabotulinumtoxinA


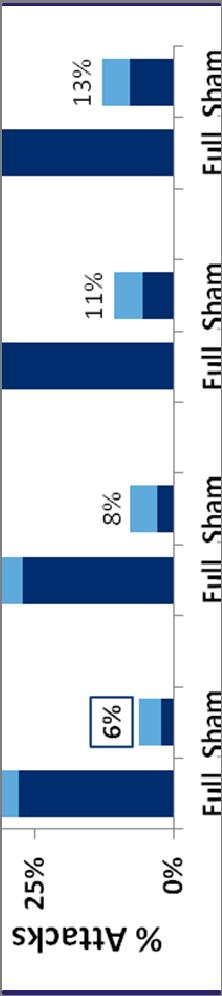

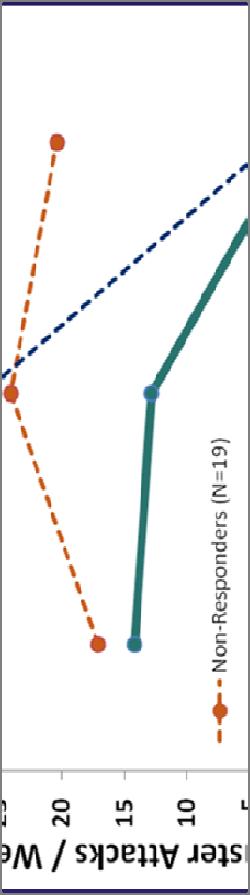
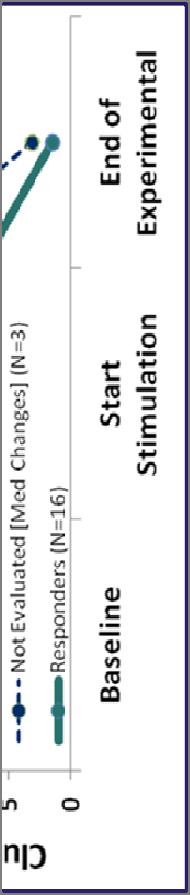
29 Sphenopalantine p ganglion g stimulation for chronic cluster headache: Schoenen et al Cephalalgia 2013




30 Vagal Nerve Stimulation Cluster Headache Decrease in daily number of attacks and severity for patients after starting treatment with nvns. Marin et al., Cephalalgia 2012
31 Acute Treatment t
32 Principles of Acute Treatment Evidence-Based Guidelines Treat attacks rapidly and consistently without recurrence Restore the patient s ability to function Minimize the use of back-up and rescue medications Optimize self-care and reduce subsequent use of resources Be cost-effective for overall management Have minimal i or no adverse events 5
33 Acute Migraine Treatment: Drug Classes Antiemetics: medications designed to help relieve nausea and vomiting Analgesics & NSAIDS: nonspecific pain relievers; often used as first-line therapy (many are available over the counter) Triptans & Ergots: migraine-specific prescription medications for use by patients with moderate to severe migraines Rescue Therapies - Opioids (narcotic pain relievers) - Corticosteroids (steroid hormones) - Neuroleptics (anti-psychotics) 6
34 Strategies of Acute Care Step Care Stratified Care Attack No Stage 1: OTC analgesic Stage 2: NSAID Stage 3: Triptan, DHE, or ergot Therapy: Choose treatment based on attack profile, associated symptoms, and level of disability 1 Increase Rx Stage 4: Rescue therapy: opioid, corticosteroid, neuroleptic 7
35 Acute Guidelines for acute migraine: Level A: All triptans including Sumatriptan/naproxen 85/500 mg, DHE NS/Inhaler, NSAIDs: diclofenac, aspirin, naproxen, ibuprofen, acetaminophen/aspirin/caffeine 500/500/130 mg, Acetaminophen 1000 mg g( (for non- incapacitating attacks), Butorphanol nasal spray 1 mg Level B: Chlorpromazine IV, Droperidol IV, Metoclopramide IV Prochlorperazine, IM/IV DHE, Ketorolac, Codeine/acetaminophen, Tramadol/acetaminophen Marmura MJ et al. Headache Jan;55(1):3-20.
36 Serotonin agonists: Triptans 5HT1B ti trigeminal i ganglia, vessels (constriction, titi MMA > MCA) 5HT1D - trigeminovascular afferents, PAG To a lesser extent 5HT1F








37 Triptans: Tolerability Similar side effect profiles across triptans Most common side effects: - Dizziness - Somnolence - Asthenia/fatigue - Paresthesias - Warmth/flushing - Chest tightness Chest pressure/tightness in 2 to 4% Most side effects are mild and transient 23

 bind to presynaptic 5HT1B/1D receptors on terminals of both the peripheral and")

38 Triptans: How they Work 5 HT1B/D Receptor Agonists Designed as cerebral vessel vasoconstrictors Block the transmission of trigeminal nerve to the trigeminal nucleus caudalis Prevent release of inflammatory neuropeptides Inhibitors of neurogenic inflammation a. Minutes after the onset of migraine, activated meningeal nociceptors enter a new physiological state b. Systemically administered triptan molecules (green circles) bind to presynaptic 5HT1B/1D receptors on terminals of both the peripheral and central branches of the meningeal nociceptor, resulting in blockade of neuropeptide release. c. After the establishment of central sensitization, the pain continues to throb and the skin becomes allodynic. d. Blockade of synaptic transmission provides only partial pain relief terminates the throbbing, but does not resolve the allodynia 24
39 TABLE 5: Serotonin 5-HT 1B/1D Agonists (Triptans) Medication Formulations Doses (mg) Tmax Half-life (hours) (hours) Almotriptan PO 6.25, Eletriptan PO 20, Frovatriptan PO 2.5 ~2.5 ~26 Naratriptan PO 1, Rizatriptan PO, tablet or 5, dissolvable (ODT) Sumatriptan t PO 25, 50, NS SC 4, Sumatriptan/naproxen PO 85/500 Zolmitriptan PO, tablet or ODT 2.5, 5 NS 5 3 3

40 New formulations of sumatriptan Zecuity patch h mg: Delivered over 4 hours Pain freedom 18% vs 9% placebo p at 2 hours, p= ; headache relief 53% vs 29%, p= 0.001
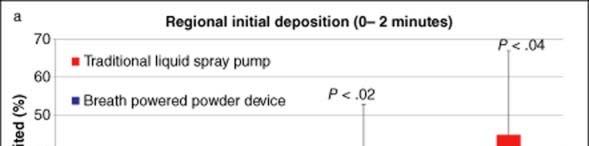

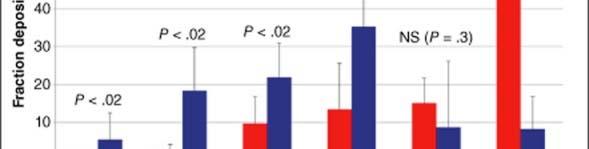

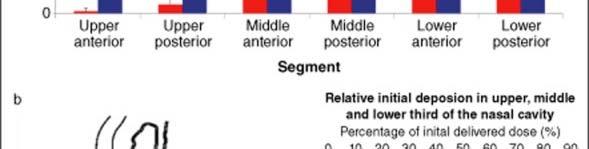

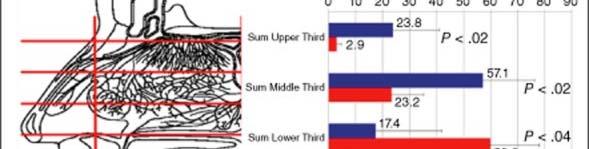
41 22 mg breath-powered intranasal system
42 Triptans of Note Fast-acting, Cluster headache Effectiveness Sumatripan sc >> NS (suma/zolmi) Rizatriptan, Eletriptan Almotriptan, Sumatriptan 25 mg, Fewer AEs Naratriptan,? Sumatriptan transdermal Preventative Non MAO metabolism Frovatriptan > Naratriptan, Eletriptan Eletriptan (CYP 3a4), Frovatriptan, Naratriptan 26
43 DHE and ergotamines: Ergotamines Dihydroergotamine: α-adrenergic activity in addition to 5HT1B/D activity More nausea (especially ergotamines, iv DHE) than triptans Vasoconstrictive May increase blood pressure Work later in attack (status migranosus, infusion therapy) DHE minimal oral absorption (NS, IM, IV)
44 Neuroleptics in Migraine Medication Route Dose (mg) Metoclopramide PO, IM, IV 5-20 Prochlorperazine PO 5-10 PR 25 IV 5-10 Droperidol IM, IV Chlorpromazine PO PR IV Haloperidol IM 5 IV 2-5 Olanzepine PO



 QTc")


45 Neuroleptic side effects Extrapyramidal, tardive dystonias Hyperprolactinemia Anticholinergic Wiht Weight gain, metabolic tb syndrome Sedation Hypotension (chlorpromazine) QTc prolongation (droperidol, haloperidol, chlorpromazine) Lowered seizure threshold QTc prolongation can predispose the patient to life-threatening arrhythmias 33
46 Opioids Bind to opioid receptors: mu, kappa, and delta mainly Variable evidence for migraine (Butorphanol LevelA)but generally not recommended as initial treatment or regular use Methadone also has NMDA antagonism Tramadol low potency mu agonist, has SNRI activity Butorphenol - partial agonist and antagonist activity Naloxone (for overdose) and naltrexone (used in addiction) are antagonists Be familiar with rational use, risk factors for misuse, risk of worsening headache control, dependancy/addiction
47 Combination medications including barbiturates Best evidence for aspirin-acetaminophen-caffeine Isometheptene-dichoralphenazone-APAP (Midrin), Isometheptene-APAP (Migraten): contraindications include glaucoma, renal failure, severe hypertension, heart or renal disease and MAO inhibitors Barbiturates: Banned in some countries, high risk of rebound, may be used to self-treat anxiety. May include codeine 47
48 NSAIDs in migraine May suppress inflammation (mast cell activation, sensitization, s fluid extravasation) May treating central sensitization by blocking glial production of prostaglandins May treat non-traditional migraine symptoms, such as neck pain and sinus pressure Easy to combine with other treatments (triptans, antiemetics) Adverse events: peptic ulcers or renal disease, may increase the risk of myocardial infarction and stroke (except aspirin, maybe naproxen), inflammatory bowel disease Lower risk of medication-overuse? 48
49 Mechanism of Action 49
50 Drug Route Dose (mg) Naproxyn Indomethacin Ketoprofen Ibuprofen PO PO, PR 25-75, 50 PO PO Piroxicam i SL 40 Ketorolac Diclofenac Aspirin Celecoxib Tolfenamic acid ASA- acetominophen- caffeine IM, IV 30-60, PO PO PO 400 PO PO
51 Indomethacin: Putative mechanisms of action Inhibits nitric i oxide production. Decreases intracranial pressure Cox-1 inhibition n inhibiting synthesis sis of prostaglandins Structural similarity to serotonin inhibits the metabolism of an active progesterone metabolite Can be used for acute migraine or as daily medication for indomethacin-responsive headaches Usual dose mg
52 Indomethacin-responsive headache Absolute responders Hemicrania Continua Paroxysmal Hemicrania syndromes Possible responders Valsalva-induced headaches (cough headache) Primary stabbing headache (ice-pick headache or jabs and jolts syndrome) Hypnic headache? Exertional headache?
53 Treatment of uncommon headache syndromes Cluster headache SC sumatriptan,high-flow oxygen Idiopathic Intracranial hypertension acetazolamide SUNA/SUNCT lamotrigine, IV lidocaine Hypnic headache caffeine High-altitude headache acetazolamide, dexamethasone, NSAIDs Trigeminal neuralgia (non-surgical) g g ( g ) carbamazepine, other AEDs, baclofen
54 Primary endpoints: Acute treatment: Two-hour pain relief, two-hour pain freedom most common for oral medication. Less common: Time to pain relief/freedom, change in pain intensity, 24-hour sustained relief. Nausea/vomiting, photo and phonophobia usually secondary Preventive treatment: Reduction in headache days Reduction in migraine days Frequency of headache h episodes s Reduction in moderate-severe days Reduction in acute medication use
55 General Advice Focus on drugs studied in placebo-controlledcontrolled trials (more than open-label or comparative trials): use guidelines as a reference Know commonly used doses, drug interactions, and serious adverse events for major drugs Be comfortable with both the two-for-one concept and using best drug for the condition in question
Goals. Primary Headache Syndromes. One-Year Prevalence of Common Headache Disorders
 Goals One-Year Prevalence of Common Headache Disorders Impact of primary headache syndromes Non pharmacologic Rx of migraine individualized to patient triggers Complementary and alternative Rx of migraine
Goals One-Year Prevalence of Common Headache Disorders Impact of primary headache syndromes Non pharmacologic Rx of migraine individualized to patient triggers Complementary and alternative Rx of migraine
HMFP Comprehensive Headache Center Department of Anesthesia, Critical Care and Pain Medicine Beth Israel Deaconess Medical Center Instructor in
 HMFP Comprehensive Headache Center Department of Anesthesia, Critical Care and Pain Medicine Beth Israel Deaconess Medical Center Instructor in Anesthesia and Neurology Harvard Medical School Limited time
HMFP Comprehensive Headache Center Department of Anesthesia, Critical Care and Pain Medicine Beth Israel Deaconess Medical Center Instructor in Anesthesia and Neurology Harvard Medical School Limited time
ADVANCES IN MIGRAINE MANAGEMENT
 ADVANCES IN MIGRAINE MANAGEMENT Joanna Girard Katzman, M.D.MSPH Assistant Professor, Dept. of Neurology Project ECHO, Chronic Pain Program University of New Mexico Outline Migraine throughout the decades
ADVANCES IN MIGRAINE MANAGEMENT Joanna Girard Katzman, M.D.MSPH Assistant Professor, Dept. of Neurology Project ECHO, Chronic Pain Program University of New Mexico Outline Migraine throughout the decades
MIGRAINE UPDATE. Objectives & Disclosures. Learn techniques used to diagnose headaches. Become familiar with medications used for headache treatment.
 MIGRAINE UPDATE Karen L. Bremer, MD November 16, 2018 Objectives & Disclosures Learn techniques used to diagnose headaches. Become familiar with medications used for headache treatment. Disclosure: I am
MIGRAINE UPDATE Karen L. Bremer, MD November 16, 2018 Objectives & Disclosures Learn techniques used to diagnose headaches. Become familiar with medications used for headache treatment. Disclosure: I am
Treatment of Primary Headache Syndromes
 Presenter Disclosure Information 2:45 3:45pm Treatment of Primary Headache Syndromes SPEAKER Gerald W. Smetana, MD The following relationships exist related to this presentation: Gerald W.Smetana, MD,
Presenter Disclosure Information 2:45 3:45pm Treatment of Primary Headache Syndromes SPEAKER Gerald W. Smetana, MD The following relationships exist related to this presentation: Gerald W.Smetana, MD,
Index. Prim Care Clin Office Pract 31 (2004) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Prim Care Clin Office Pract 31 (2004) 441 447 Index Note: Page numbers of article titles are in boldface type. A Abscess, brain, headache in, 388 Acetaminophen for migraine, 406 407 headache from, 369
Prim Care Clin Office Pract 31 (2004) 441 447 Index Note: Page numbers of article titles are in boldface type. A Abscess, brain, headache in, 388 Acetaminophen for migraine, 406 407 headache from, 369
Short Clinical Guidelines: Headache, Key Points for Diagnosis and Treatment
 Clinical Highlights 1. Headache is diagnosed by history and physical examination with limited need for imaging or laboratory tests. 2. Warning signs of possible disorder other than primary headache are:
Clinical Highlights 1. Headache is diagnosed by history and physical examination with limited need for imaging or laboratory tests. 2. Warning signs of possible disorder other than primary headache are:
Strategies in Migraine Care
 Strategies in Migraine Care Julie L. Roth, MD Rhode Island Hospital Assistant Professor, Neurology The Warren Alpert Medical School of Brown University March 28, 2015 Financial Disclosures None. Objectives
Strategies in Migraine Care Julie L. Roth, MD Rhode Island Hospital Assistant Professor, Neurology The Warren Alpert Medical School of Brown University March 28, 2015 Financial Disclosures None. Objectives
Management of headache
 Management of headache TJ Steiner Imperial College London Based on European principles of management of common headache disorders TJ Steiner, K Paemeleire, R Jensen, D Valade, L Savi, MJA Lainez, H-C Diener,
Management of headache TJ Steiner Imperial College London Based on European principles of management of common headache disorders TJ Steiner, K Paemeleire, R Jensen, D Valade, L Savi, MJA Lainez, H-C Diener,
Adult & Pediatric Patients. Stanford Health Care, Division Pain Medicine
 Acute Treatment Strategies in Adult & Pediatric Patients Theresa Mallick Searle, MS, RN BC, ANP BC Disclosures Speakers Bureau: Allergan, Depomed Acute Treatment Strategies in Adult & Pediatric Patients
Acute Treatment Strategies in Adult & Pediatric Patients Theresa Mallick Searle, MS, RN BC, ANP BC Disclosures Speakers Bureau: Allergan, Depomed Acute Treatment Strategies in Adult & Pediatric Patients
How do we treat migraine? New SIGN Guidelines
 How do we treat migraine? New SIGN Guidelines Managing your migraine Migraine Trust, Edinburgh 2018 Callum Duncan Consultant Neurologist Aberdeen Royal Infirmary Chair SIGN Guideline 155 Premonitory Mood
How do we treat migraine? New SIGN Guidelines Managing your migraine Migraine Trust, Edinburgh 2018 Callum Duncan Consultant Neurologist Aberdeen Royal Infirmary Chair SIGN Guideline 155 Premonitory Mood
Faculty Disclosures. Learning Objectives. Acute Treatment Strategies
 WWW.AMERICANHEADACHESOCIETY.ORG Acute Treatment Strategies Content developed by: Lawrence C. Newman, MD, FAHS Donna Gutterman, PharmD Faculty Disclosures LAWRENCE C. NEWMAN, MD, FAHS Dr. Newman has received
WWW.AMERICANHEADACHESOCIETY.ORG Acute Treatment Strategies Content developed by: Lawrence C. Newman, MD, FAHS Donna Gutterman, PharmD Faculty Disclosures LAWRENCE C. NEWMAN, MD, FAHS Dr. Newman has received
Faculty Disclosure. Karen L. Bremer, MD. Dr. Bremer has listed no financial interest/arrangement that would be considered a conflict of interest.
 Faculty Disclosure Karen L. Bremer, MD Dr. Bremer has listed no financial interest/arrangement that would be considered a conflict of interest. HEADACHE UPDATE Karen L. Bremer, MD November 10, 2017 karen.bremer@creighton.edu
Faculty Disclosure Karen L. Bremer, MD Dr. Bremer has listed no financial interest/arrangement that would be considered a conflict of interest. HEADACHE UPDATE Karen L. Bremer, MD November 10, 2017 karen.bremer@creighton.edu
Medication For Migraine Chart: Table 1: Acute Treatment when the attack begins
 Medication For Migraine Chart: Table 1: Acute Treatment when the attack begins Page a Analgesics (painkillers) Non-steroidal antiinflammatory drugs (NSAIDs) Prescription required Brand Name Formulation
Medication For Migraine Chart: Table 1: Acute Treatment when the attack begins Page a Analgesics (painkillers) Non-steroidal antiinflammatory drugs (NSAIDs) Prescription required Brand Name Formulation
Update on Diagnosis and Management of Migraines
 Update on Diagnosis and Management of Migraines Joel J. Heidelbaugh, MD, FAAFP, FACG Clinical Professor Departments of Family Medicine and Urology University of Michigan Learning Objectives To distinguish
Update on Diagnosis and Management of Migraines Joel J. Heidelbaugh, MD, FAAFP, FACG Clinical Professor Departments of Family Medicine and Urology University of Michigan Learning Objectives To distinguish
Case Presentation. Case Presentation. Case Presentation. Truths about Headaches (2017) Most headaches were muscle-tension headaches
 Most headaches were muscle-tension headaches") Agenda Case presentation Migraine Morphology Primary and Premonitory Phase Secondary Headache Aura Headache Primer on Pain Medication Overuse Headache Case Presentation RT is a 25 year old woman with daily
Agenda Case presentation Migraine Morphology Primary and Premonitory Phase Secondary Headache Aura Headache Primer on Pain Medication Overuse Headache Case Presentation RT is a 25 year old woman with daily
ONZETRA XSAIL (sumatriptan) nasal powder
 nasal powder") ONZETRA XSAIL (sumatriptan) nasal powder Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy
ONZETRA XSAIL (sumatriptan) nasal powder Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy
Management options for Migraine. Prof. Dr. Khwaja Nazimuddin Head Dept. of Internal Medicine BIRDEM
 Management options for Migraine Prof. Dr. Khwaja Nazimuddin Head Dept. of Internal Medicine BIRDEM Assessment The Migraine Disability Assessment Score MIDAS Complete loss of work Partial loss of work Off
Management options for Migraine Prof. Dr. Khwaja Nazimuddin Head Dept. of Internal Medicine BIRDEM Assessment The Migraine Disability Assessment Score MIDAS Complete loss of work Partial loss of work Off
Disclosures. Triptans for Kids 5/16/13
 5/16/13 Disclosures Triptans for Kids Amy A. Gelfand, MD GelfandA@neuropeds.ucsf.edu Departments of Neurology and Pediatrics UCSF Child Neurology and Headache Center I receive grant funding from: NIH/NINDS
5/16/13 Disclosures Triptans for Kids Amy A. Gelfand, MD GelfandA@neuropeds.ucsf.edu Departments of Neurology and Pediatrics UCSF Child Neurology and Headache Center I receive grant funding from: NIH/NINDS
What is new in the migraine world! Modar Khalil Consultant neurologist Hull Royal Infirmary
 What is new in the migraine world! Modar Khalil Consultant neurologist Hull Royal Infirmary Overview Understanding the burden Commonly used terms Acute therapy What we currently have What we are going
What is new in the migraine world! Modar Khalil Consultant neurologist Hull Royal Infirmary Overview Understanding the burden Commonly used terms Acute therapy What we currently have What we are going
My patient s pain in the head, is a pain in Greg Jicha, M.D., Ph.D.
 My patient s pain in the head, is a pain in the @%$*&# Greg Jicha, M.D., Ph.D. Kentucky Neurologic Institute University of Kentucky, Lexington, KY Migraine is More Common than Asthma & Diabetes Combined
My patient s pain in the head, is a pain in the @%$*&# Greg Jicha, M.D., Ph.D. Kentucky Neurologic Institute University of Kentucky, Lexington, KY Migraine is More Common than Asthma & Diabetes Combined
Preventive treatment of migraine. Rebecca Burch, MD Brigham and Women s Faulkner Hospital Harvard Medical School Boston, MA
 Preventive treatment of migraine Rebecca Burch, MD Brigham and Women s Faulkner Hospital Harvard Medical School Boston, MA No disclosures Disclosures Many preventive treatments for migraine are not FDA-approved
Preventive treatment of migraine Rebecca Burch, MD Brigham and Women s Faulkner Hospital Harvard Medical School Boston, MA No disclosures Disclosures Many preventive treatments for migraine are not FDA-approved
Prevention and Treatment of Migraines CAITLIN BARNES, PHARM.D. CANDIDATE AMBULATORY CARE JOE CAMMILLERI, PHARM.D. NATOHYA MALLORY, PHARM.D.
 Prevention and Treatment of Migraines CAITLIN BARNES, PHARM.D. CANDIDATE AMBULATORY CARE JOE CAMMILLERI, PHARM.D. NATOHYA MALLORY, PHARM.D. Objectives Present patient case Review epidemiology/pathophysiology
Prevention and Treatment of Migraines CAITLIN BARNES, PHARM.D. CANDIDATE AMBULATORY CARE JOE CAMMILLERI, PHARM.D. NATOHYA MALLORY, PHARM.D. Objectives Present patient case Review epidemiology/pathophysiology
Treatments for migraine
 Treatments for migraine Information for patients and carers Department of Neurology Aberdeen Royal Infirmary Contents Page About this leaflet Abortive medication for migraine Painkillers Antisickness medication
Treatments for migraine Information for patients and carers Department of Neurology Aberdeen Royal Infirmary Contents Page About this leaflet Abortive medication for migraine Painkillers Antisickness medication
ปวดศ รษะมา 5 ป ก นยาแก ปวดก ย งไม ข น นพ.พาว ฒ เมฆว ช ย โรงพยาบาลนครราชส มา
 ปวดศ รษะมา 5 ป ก นยาแก ปวดก ย งไม ข น นพ.พาว ฒ เมฆว ช ย โรงพยาบาลนครราชส มา 1 CONTENT 1 2 3 Chronic Daily Headache Medical Overused Headache Management Headaches are one of the most common symptoms List
ปวดศ รษะมา 5 ป ก นยาแก ปวดก ย งไม ข น นพ.พาว ฒ เมฆว ช ย โรงพยาบาลนครราชส มา 1 CONTENT 1 2 3 Chronic Daily Headache Medical Overused Headache Management Headaches are one of the most common symptoms List
Clinical Learning Days November 10, 2017
 Migraine Clinical Learning Days November 10, 2017 Alyssa Lettich. MD Neurosciences Institute/Neurosciences Clinical Program Medical Director Headache Disclosures: none Learning Objectives: At the conclusion
Migraine Clinical Learning Days November 10, 2017 Alyssa Lettich. MD Neurosciences Institute/Neurosciences Clinical Program Medical Director Headache Disclosures: none Learning Objectives: At the conclusion
Headache A Practical Approach
 Headache A Practical Approach Integrated Pain Symposium December 1, 2017 Alyssa Lettich. MD Neurosciences Institute/Neurosciences Clinical Program Medical Director Headache and Pain Development Teams Disclosures:
Headache A Practical Approach Integrated Pain Symposium December 1, 2017 Alyssa Lettich. MD Neurosciences Institute/Neurosciences Clinical Program Medical Director Headache and Pain Development Teams Disclosures:
M0BCore Safety Profile. Pharmaceutical form(s)/strength: ordispersible tablet SE/H/PSUR/0022/002 Date of FAR:
/strength: ordispersible tablet SE/H/PSUR/0022/002 Date of FAR:") M0BCore Safety Profile Active substance: Zolmitriptan Pharmaceutical form(s)/strength: ordispersible tablet P-RMS: SE/H/PSUR/0022/002 Date of FAR: 15.03.2014 4.3 Contraindications Zolmitriptan is contraindicated
M0BCore Safety Profile Active substance: Zolmitriptan Pharmaceutical form(s)/strength: ordispersible tablet P-RMS: SE/H/PSUR/0022/002 Date of FAR: 15.03.2014 4.3 Contraindications Zolmitriptan is contraindicated
Headache. Susan Hickenbottom MD, MS February 24, 2015
 Headache Susan Hickenbottom MD, MS February 24, 2015 Epidemiology One of most common complaints in primary care 90% of US population 50% at least one severe 25% recurrent disabling attacks 5% chronic daily
Headache Susan Hickenbottom MD, MS February 24, 2015 Epidemiology One of most common complaints in primary care 90% of US population 50% at least one severe 25% recurrent disabling attacks 5% chronic daily
Clinical Policy: Triptans Reference Number: CP.CPA.217 Effective Date: Last Review Date: Line of Business: Commercial
 Clinical Policy: Reference Number: CP.CPA.217 Effective Date: 11.16.16 Last Review Date: 11.17 Line of Business: Commercial Revision Log See Important Reminder at the end of this policy for important regulatory
Clinical Policy: Reference Number: CP.CPA.217 Effective Date: 11.16.16 Last Review Date: 11.17 Line of Business: Commercial Revision Log See Important Reminder at the end of this policy for important regulatory
SUMAVEL DOSEPRO (sumatriptan succinate) solution for injection
 solution for injection") SUMAVEL DOSEPRO (sumatriptan succinate) solution for injection Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit
SUMAVEL DOSEPRO (sumatriptan succinate) solution for injection Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit
Migraine Acute treatment
 Migraine Acute treatment Elizabeth Loder, MD, MPH Professor of Neurology, Harvard Medical School Chief, Division of Headache, Department of Neurology, Brigham and Women s Hospital, Boston, MA Disclosures
Migraine Acute treatment Elizabeth Loder, MD, MPH Professor of Neurology, Harvard Medical School Chief, Division of Headache, Department of Neurology, Brigham and Women s Hospital, Boston, MA Disclosures
OH, MY ACHING HEAD! I HAVE NO DISCLOSURES OR CONFLICTS OF INTERESTS TO DECLARE MANAGING HEADACHE IN THE OUTPATIENT SETTING SECONDARY HEADACHES
 1 JUSTIN A. OSSMAN, MD CHATTANOOGA FAMILY MEDICINE UPDATE OH, MY ACHING HEAD! MANAGING HEADACHE IN THE OUTPATIENT SETTING 2 I HAVE NO DISCLOSURES OR CONFLICTS OF INTERESTS TO DECLARE OBJECTIVES International
1 JUSTIN A. OSSMAN, MD CHATTANOOGA FAMILY MEDICINE UPDATE OH, MY ACHING HEAD! MANAGING HEADACHE IN THE OUTPATIENT SETTING 2 I HAVE NO DISCLOSURES OR CONFLICTS OF INTERESTS TO DECLARE OBJECTIVES International
Migraine Management. Jane Melling Headache nurse Mater Misericordiae Hospital
 Migraine Management Jane Melling Headache nurse Mater Misericordiae Hospital Migraine facts Among the most common disorders of the nervous system 3 rd most prevalent medical disorder on the planet (lancet
Migraine Management Jane Melling Headache nurse Mater Misericordiae Hospital Migraine facts Among the most common disorders of the nervous system 3 rd most prevalent medical disorder on the planet (lancet
MANAGEMENT OF DIABETIC NEUROPATHY. Chungnam University Hospital Soo-Kyung, Bok, M.D., Ph.D.
 MANAGEMENT OF DIABETIC NEUROPATHY Chungnam University Hospital Soo-Kyung, Bok, M.D., Ph.D. The Diabetic neuropathy cannot be reversed Not to restore function to damaged nerve Slowly progress no initial
MANAGEMENT OF DIABETIC NEUROPATHY Chungnam University Hospital Soo-Kyung, Bok, M.D., Ph.D. The Diabetic neuropathy cannot be reversed Not to restore function to damaged nerve Slowly progress no initial
Tears of Pain SUNCT and SUNA A/PROFESSOR ARUN AGGARWAL RPAH PAIN MANAGEMENT CENTRE
 Tears of Pain SUNCT and SUNA A/PROFESSOR ARUN AGGARWAL RPAH PAIN MANAGEMENT CENTRE IHS Classification 1989 (updated 2004) Primary Headaches 4 categories Migraine Tension-type Cluster and other trigeminal
Tears of Pain SUNCT and SUNA A/PROFESSOR ARUN AGGARWAL RPAH PAIN MANAGEMENT CENTRE IHS Classification 1989 (updated 2004) Primary Headaches 4 categories Migraine Tension-type Cluster and other trigeminal
Chronic Daily Headaches
 Chronic Daily Headaches ANWARUL HAQ, MD, MRCP(UK), FAHS DIRECTOR BAYLOR HEADACHE CENTER, DALLAS, TEXAS DISCLOSURES: None OBJECTIVES AT THE CONCLUSION OF THIS ACTIVITY, PARTICIPANTS WILL BE ABLE TO: define
Chronic Daily Headaches ANWARUL HAQ, MD, MRCP(UK), FAHS DIRECTOR BAYLOR HEADACHE CENTER, DALLAS, TEXAS DISCLOSURES: None OBJECTIVES AT THE CONCLUSION OF THIS ACTIVITY, PARTICIPANTS WILL BE ABLE TO: define
I have no financial relationships to disclose. I will not discuss investigational use of medication in my presentation.
 I have no financial relationships to disclose. I will not discuss investigational use of medication in my presentation. In 1962, Bille published landmark epidemiologic survey of headache among 9,000 school
I have no financial relationships to disclose. I will not discuss investigational use of medication in my presentation. In 1962, Bille published landmark epidemiologic survey of headache among 9,000 school
HEADACHE. Primary vs Secondary Headaches SNOOP4. Classification of Primary Headaches. Novel Approaches to Diagnosis and Treatment.
 HEADACHE Novel Approaches to Diagnosis and Treatment Primary vs Secondary Headaches SNOOP4 S - systemic signs and symptoms (fever, weight loss) or secondary risk factors (HIV, cancer) N - neurological
HEADACHE Novel Approaches to Diagnosis and Treatment Primary vs Secondary Headaches SNOOP4 S - systemic signs and symptoms (fever, weight loss) or secondary risk factors (HIV, cancer) N - neurological
Lost in Translation: Making Sense of Clinical Treatment Guidelines
 Lost in Translation: Making Sense of Clinical Treatment Guidelines Charles E. Argoff, MD, CPE Disclosures: Charles Argoff Financial Disclosure: Consultant: Teva, Daiichi Sakyo, Pfizer, Nektar, Purdue,
Lost in Translation: Making Sense of Clinical Treatment Guidelines Charles E. Argoff, MD, CPE Disclosures: Charles Argoff Financial Disclosure: Consultant: Teva, Daiichi Sakyo, Pfizer, Nektar, Purdue,
10/13/17. Christy M. Jackson, MD Director, Dalessio Headache Center Scripps Clinic, La Jolla Clinical Professor, Neurosciences UCSD
 Christy M. Jackson, MD Director, Dalessio Headache Center Scripps Clinic, La Jolla Clinical Professor, Neurosciences UCSD } Depomed Consultant 2014 to present } Avanir Consultant 2014 to present } Amgen
Christy M. Jackson, MD Director, Dalessio Headache Center Scripps Clinic, La Jolla Clinical Professor, Neurosciences UCSD } Depomed Consultant 2014 to present } Avanir Consultant 2014 to present } Amgen
IF I M NOT TREATING WITH OPIOIDS, THEN WHAT AM I SUPPOSED TO USE?
 NON-OPIOID TREATMENT OPTIONS FOR CHRONIC PAIN Alison Knutson, PharmD, BCACP Medication Management Pharmacist Park Nicollet Creekside Clinic Dr. Knutson indicated no potential conflict of interest to this
NON-OPIOID TREATMENT OPTIONS FOR CHRONIC PAIN Alison Knutson, PharmD, BCACP Medication Management Pharmacist Park Nicollet Creekside Clinic Dr. Knutson indicated no potential conflict of interest to this
Prescription Pain Management. University of Hawai i Hilo Pre- Nursing Program NURS 203 General Pharmacology Danita 1 Narciso Pharm D
 Prescription Pain Management University of Hawai i Hilo Pre- Nursing Program NURS 203 General Pharmacology Danita 1 Narciso Pharm D 2 Objectives Understand how to preform a pain assessment Know which medications
Prescription Pain Management University of Hawai i Hilo Pre- Nursing Program NURS 203 General Pharmacology Danita 1 Narciso Pharm D 2 Objectives Understand how to preform a pain assessment Know which medications
Migraine is a primary headache disorder ... REPORTS... Migraine: Diagnosis, Management, and New Treatment Options
 ... REPORTS... Migraine: Diagnosis, Management, and New Treatment Options R. Michael Gallagher, DO; and F. Michael Cutrer, MD Abstract Objective: The safety and tolerability of medications used to treat
... REPORTS... Migraine: Diagnosis, Management, and New Treatment Options R. Michael Gallagher, DO; and F. Michael Cutrer, MD Abstract Objective: The safety and tolerability of medications used to treat
Clinical Policy: Triptans Reference Number: CP.HNMC.217 Effective Date: Last Review Date: Line of Business: Medicaid Medi-Cal
 Clinical Policy: Reference Number: CP.HNMC.217 Effective Date: 11.16.16 Last Review Date: 11.17 Line of Business: Medicaid Medi-Cal Revision Log See Important Reminder at the end of this policy for important
Clinical Policy: Reference Number: CP.HNMC.217 Effective Date: 11.16.16 Last Review Date: 11.17 Line of Business: Medicaid Medi-Cal Revision Log See Important Reminder at the end of this policy for important
Migraine Migraine Age Specific Prevalence in the United States. Headache International Headache Society Classification
 28 Primary Care Medicine Principles and Practice 29 October 28 Professor Peter J. Goadsby Peter.Goadsby@headache.ucsf.edu Department of Neurology Headache International Headache Society Classification
28 Primary Care Medicine Principles and Practice 29 October 28 Professor Peter J. Goadsby Peter.Goadsby@headache.ucsf.edu Department of Neurology Headache International Headache Society Classification
2008 Migraine Update Migraine Update Migraine Update. Epidemiology. Yousef Mohammad MD., MSc. Epidemiology
 2008 Migraine Update Yousef Mohammad MD., MSc Assistant Professor of Neurology Ohio State University Medical Center 2008 Migraine Update Epidemiology 2008 Migraine Update Epidemiology Abortive Treatment
2008 Migraine Update Yousef Mohammad MD., MSc Assistant Professor of Neurology Ohio State University Medical Center 2008 Migraine Update Epidemiology 2008 Migraine Update Epidemiology Abortive Treatment
Headache. Section 1. Migraine headache. Clinical presentation
 Section 1 Headache Migraine headache 1 Clinical presentation It is important to recognize just how significant a problem migraine headache is. It has been estimated that migraine affects 11% of the United
Section 1 Headache Migraine headache 1 Clinical presentation It is important to recognize just how significant a problem migraine headache is. It has been estimated that migraine affects 11% of the United
New Zealand Data Sheet
 Arrow - Sumatriptan Sumatriptan Injection 6mg/0.5mL Presentation New Zealand Data Sheet ARROW SUMATRIPTAN Injection 6mg/0.5mL is a clear, colourless to pale yellow solution in a prefilled syringe. Uses
Arrow - Sumatriptan Sumatriptan Injection 6mg/0.5mL Presentation New Zealand Data Sheet ARROW SUMATRIPTAN Injection 6mg/0.5mL is a clear, colourless to pale yellow solution in a prefilled syringe. Uses
MEASURE #3: PREVENTIVE MIGRAINE MEDICATION PRESCRIBED Headache
 MEASURE #3: PREVENTIVE MIGRAINE MEDICATION PRESCRIBED Headache Measure Description Percentage of patients age 18 years old and older diagnosed with migraine headache whose migraine frequency is 4 migraine
MEASURE #3: PREVENTIVE MIGRAINE MEDICATION PRESCRIBED Headache Measure Description Percentage of patients age 18 years old and older diagnosed with migraine headache whose migraine frequency is 4 migraine
UPDATE IN MIGRAINE MANAGEMENT
 UPDATE IN MIGRAINE MANAGEMENT Eric P. Baron, DO Cleveland Clinic Neurological Institute Center for Neurological Restoration Headache and Chronic Pain Medicine barone2@ccf.org @Neuralgroover Disclosures
UPDATE IN MIGRAINE MANAGEMENT Eric P. Baron, DO Cleveland Clinic Neurological Institute Center for Neurological Restoration Headache and Chronic Pain Medicine barone2@ccf.org @Neuralgroover Disclosures
Çiçek Wöber-Bingöl HEADACHE UNIT FOR CHILDREN AND ADOLESCENCE
 Headache in children and adolescents Çiçek Wöber-Bingöl HEADACHE UNIT FOR CHILDREN AND ADOLESCENCE Dept. of Psychiatry of Childhood and Adolescence Medical University of Vienna, Vienna, Austria Impact
Headache in children and adolescents Çiçek Wöber-Bingöl HEADACHE UNIT FOR CHILDREN AND ADOLESCENCE Dept. of Psychiatry of Childhood and Adolescence Medical University of Vienna, Vienna, Austria Impact
ACUTE TREATMENT FOR MIGRAINE. Cristina Tassorelli
 The European Headache School 2012 ACUTE TREATMENT FOR MIGRAINE Cristina Tassorelli Headache Science Centre, IRCCS Neurological Institute C. Mondino Foundation - Pavia University Centre for Adaptive Disorders
The European Headache School 2012 ACUTE TREATMENT FOR MIGRAINE Cristina Tassorelli Headache Science Centre, IRCCS Neurological Institute C. Mondino Foundation - Pavia University Centre for Adaptive Disorders
Antidepressants: Prof. Riyadh Al_Azzawi F.R.C.Psych
 Antidepressants: Prof. Riyadh Al_Azzawi F.R.C.Psych A. Heterocyclic antidepressants: (tricyclic and tetracyclic ), e.g.amitryptaline,imipramine. B. Monoamine oxidase inhibitors(m.a.o.i), e.g.phenelzine.
Antidepressants: Prof. Riyadh Al_Azzawi F.R.C.Psych A. Heterocyclic antidepressants: (tricyclic and tetracyclic ), e.g.amitryptaline,imipramine. B. Monoamine oxidase inhibitors(m.a.o.i), e.g.phenelzine.
MIGRAINE A MYSTERY HEADACHE
 MIGRAINE A MYSTERY HEADACHE The migraine is a chronic neurological disease that is characterized by moderate to severe episodes of headache that is mostly associated with other central nervous system (CNS)
MIGRAINE A MYSTERY HEADACHE The migraine is a chronic neurological disease that is characterized by moderate to severe episodes of headache that is mostly associated with other central nervous system (CNS)
Core Safety Profile. Pharmaceutical form(s)/strength: Tablets and Oral lyophilisates (wafers) 5 and 10 mg NL/H/PSUR/0002/001 Date of FAR:
/strength: Tablets and Oral lyophilisates (wafers) 5 and 10 mg NL/H/PSUR/0002/001 Date of FAR:") Core Safety Profile Active substance: Rizatriptan Pharmaceutical form(s)/strength: Tablets and Oral lyophilisates (wafers) 5 and 10 mg P RMS: NL/H/PSUR/0002/001 Date of FAR: 23.05.2011 4.3 Contraindications
Core Safety Profile Active substance: Rizatriptan Pharmaceutical form(s)/strength: Tablets and Oral lyophilisates (wafers) 5 and 10 mg P RMS: NL/H/PSUR/0002/001 Date of FAR: 23.05.2011 4.3 Contraindications
CHAPTER 4 PAIN AND ITS MANAGEMENT
 CHAPTER 4 PAIN AND ITS MANAGEMENT Pain Definition: An unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage. Types of Pain
CHAPTER 4 PAIN AND ITS MANAGEMENT Pain Definition: An unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage. Types of Pain
Migraine Treatment What you need to know
 Migraine Treatment What you need to know DR NICOLE LIMBERG ST ANDREWS PLACE SPRING HILL www.migrainespecialist.com.au Migraine what is it? Primary neurobiological condition Waves of reduced brain activity
Migraine Treatment What you need to know DR NICOLE LIMBERG ST ANDREWS PLACE SPRING HILL www.migrainespecialist.com.au Migraine what is it? Primary neurobiological condition Waves of reduced brain activity
MEASURE #4: Overuse of Barbiturate Containing Medications for Primary Headache Disorders Headache
 MEASURE #4: Overuse of Barbiturate Containing Medications for Primary Headache Disorders Headache Measure Description Percentage of patients age 18 years old and older with a diagnosis of primary headache
MEASURE #4: Overuse of Barbiturate Containing Medications for Primary Headache Disorders Headache Measure Description Percentage of patients age 18 years old and older with a diagnosis of primary headache
Triptans Quantity Limit Program Summary
 Triptans Quantity Limit Program Summary FDA APPROVED INDICATIONS AND DOSAGE 1-13,14,23,24 Agents Amerge (naratriptan) 1, 2.5 tablets Axert (almotriptan) 6.25, 12.5 tablets migraine attacks with/without
Triptans Quantity Limit Program Summary FDA APPROVED INDICATIONS AND DOSAGE 1-13,14,23,24 Agents Amerge (naratriptan) 1, 2.5 tablets Axert (almotriptan) 6.25, 12.5 tablets migraine attacks with/without
SIGN on the pharmacological management of migraine
 GUIDELINES SIGN on the pharmacological management of migraine STEVE CHAPLIN In February 2018, the Scottish Intercollegiate Guidelines Network (SIGN) published a new guideline on the pharmacological management
GUIDELINES SIGN on the pharmacological management of migraine STEVE CHAPLIN In February 2018, the Scottish Intercollegiate Guidelines Network (SIGN) published a new guideline on the pharmacological management
Migraine Management. Roger Cady, MD Headache Care Center Springfield, MO
 Migraine Management Roger Cady, MD Headache Care Center Springfield, MO Disclosures Objectives The evolution of migraine From benign episodic (benign) headache to potentially a devastating chronic disease
Migraine Management Roger Cady, MD Headache Care Center Springfield, MO Disclosures Objectives The evolution of migraine From benign episodic (benign) headache to potentially a devastating chronic disease
ACUTE MIGRAINE: OLD AND NEW DRUGS JOHN ROBROCK MD FORT WILLIAM FAMILY HEALTH TEAM
 ACUTE MIGRAINE: OLD AND NEW DRUGS JOHN ROBROCK MD FORT WILLIAM FAMILY HEALTH TEAM Conflict of Interest Declaration: Nothing to Disclose Presenter: John Robrock, MD Title of Presentation: Acute Migraine:
ACUTE MIGRAINE: OLD AND NEW DRUGS JOHN ROBROCK MD FORT WILLIAM FAMILY HEALTH TEAM Conflict of Interest Declaration: Nothing to Disclose Presenter: John Robrock, MD Title of Presentation: Acute Migraine:
10/31/2017 PRIMARY CARE AND HEADACHE DISCLOSURES WHERE DO THOSE WITH HEADACHE SEEK MEDICAL CARE? Primary Care 67%
 PRIMARY CARE AND HEADACHE Sonja Potrebic MD PhD Regional Headache Specialist Kaiser LAMC 1 WHERE DO THOSE WITH HEADACHE SEEK MEDICAL CARE? Column1 Primary Care 67% Primary Care Headache Specialty Other
PRIMARY CARE AND HEADACHE Sonja Potrebic MD PhD Regional Headache Specialist Kaiser LAMC 1 WHERE DO THOSE WITH HEADACHE SEEK MEDICAL CARE? Column1 Primary Care 67% Primary Care Headache Specialty Other
A synopsis of: Diagnosis and Management of Headaches in Adults: A national clinical guideline. Scottish intercollegiate Guidelines Network SIGN
 A synopsis of: Diagnosis and Management of Headaches in Adults: A national clinical guideline Scottish intercollegiate Guidelines Network SIGN November 2008. PETER FRAMPTON MSc MCOptom BAppSc (Optom)(AUS)
A synopsis of: Diagnosis and Management of Headaches in Adults: A national clinical guideline Scottish intercollegiate Guidelines Network SIGN November 2008. PETER FRAMPTON MSc MCOptom BAppSc (Optom)(AUS)
Sumatriptan Tablets, Nasal Spray (Imitrex), Nasal Powder (Onzetra Xsail), sumatriptan and naproxen sodium (Treximet tablets)
, Nasal Powder (Onzetra Xsail), sumatriptan and naproxen sodium (Treximet tablets)") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 0 Subject: Sumatriptan Page: 1 of 6 Last Review Date: November 30, 2018 Sumatriptan Description Sumatriptan
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 0 Subject: Sumatriptan Page: 1 of 6 Last Review Date: November 30, 2018 Sumatriptan Description Sumatriptan
10/19/12. Headache: Tips and Tools for Management. Michael A. Rogawski, MD, PhD Disclosures
 10/19/12 Headache: Tips and Tools for Management Michael A. Rogawski, MD, PhD University of California, Davis Sacramento, CA Michael A. Rogawski, MD, PhD Disclosures Grants: Congressionally Directed Medical
10/19/12 Headache: Tips and Tools for Management Michael A. Rogawski, MD, PhD University of California, Davis Sacramento, CA Michael A. Rogawski, MD, PhD Disclosures Grants: Congressionally Directed Medical
Anti-Depressant Medications
 Anti-Depressant Medications A Introduction: This topic may be a little bit underestimated here in Jordan, while in western countries it has more significance. The function of anti-depressants is to change
Anti-Depressant Medications A Introduction: This topic may be a little bit underestimated here in Jordan, while in western countries it has more significance. The function of anti-depressants is to change
Headache. Headache Case. Migraine Headache. Eric Kraus, MD. Types» Without aura (common)» With aura (classic)
» With aura (classic)") Headache Eric Kraus, MD Headache Case This 23 year-old female has headaches behind the right eye that cause her to lay down in a quiet room. They have a throbbing quality and she may vomit. Migraine Headache
Headache Eric Kraus, MD Headache Case This 23 year-old female has headaches behind the right eye that cause her to lay down in a quiet room. They have a throbbing quality and she may vomit. Migraine Headache
The best defense is a good offense. Optimizing the Acute Treatment of Migraine. Disclosures 11/10/2017
 Optimizing the Acute Treatment of Migraine Brian M. Plato, DO, FAHS Norton Neuroscience Institute Louisville, KY Disclosures Speakers Bureau (personal): Allergan, Depomed, Avanir Research Funding (paid
Optimizing the Acute Treatment of Migraine Brian M. Plato, DO, FAHS Norton Neuroscience Institute Louisville, KY Disclosures Speakers Bureau (personal): Allergan, Depomed, Avanir Research Funding (paid
Understanding Migraines and Treatment Options. Simplified Diagnosis of Migraine. Migraine Prevalence American Migraine Study II
 Understanding Migraines and Treatment Options Deborah C. Zajac, RN-BC Center for Headache and Pain Neurological Institute Cleveland Clinic Simplified Diagnosis of Migraine Any person with a stable pattern
Understanding Migraines and Treatment Options Deborah C. Zajac, RN-BC Center for Headache and Pain Neurological Institute Cleveland Clinic Simplified Diagnosis of Migraine Any person with a stable pattern
Migraine Management. Dr Helen Brown Director of Neurology and Stroke The Princess Alexandra Hospital
 Migraine Management Dr Helen Brown Director of Neurology and Stroke The Princess Alexandra Hospital Referral Criteria for Migraine Migraine Management Migraine Diagnosis Spot on Health Migraine pathway
Migraine Management Dr Helen Brown Director of Neurology and Stroke The Princess Alexandra Hospital Referral Criteria for Migraine Migraine Management Migraine Diagnosis Spot on Health Migraine pathway
Zonisamide for migraine prophylaxis in refractory patients
 Thomas Jefferson University Jefferson Digital Commons Department of Neurology Faculty Papers Department of Neurology March 2006 Zonisamide for migraine prophylaxis in refractory patients Avi Ashkenazi
Thomas Jefferson University Jefferson Digital Commons Department of Neurology Faculty Papers Department of Neurology March 2006 Zonisamide for migraine prophylaxis in refractory patients Avi Ashkenazi
Treatment of Neuropathic Pain: What Does the Evidence Say? or Just the Facts Ma am
 Treatment of Neuropathic Pain: What Does the Evidence Say? or Just the Facts Ma am Tim R Brown, PharmD, BCACP, FASHP Director of Clinical Pharmacotherapy Cleveland Clinic Akron General Center for Family
Treatment of Neuropathic Pain: What Does the Evidence Say? or Just the Facts Ma am Tim R Brown, PharmD, BCACP, FASHP Director of Clinical Pharmacotherapy Cleveland Clinic Akron General Center for Family
COLUMBIA UNIVERSITY HEADACHE CENTER: NEW PATIENT QUESTIONNAIRE
 COLUMBIA UNIVERSITY HEADACHE CENTER: NEW PATIENT QUESTIONNAIRE HEADACHE CHARACTERISTICS Frequency and Severity 1. At what AGE did you get your first headache, of ANY kind? 2. At what AGE did your headaches
COLUMBIA UNIVERSITY HEADACHE CENTER: NEW PATIENT QUESTIONNAIRE HEADACHE CHARACTERISTICS Frequency and Severity 1. At what AGE did you get your first headache, of ANY kind? 2. At what AGE did your headaches
Sumatriptan Tablets, Nasal Spray (Imitrex), Nasal Powder (Onzetra Xsail), sumatriptan and naproxen sodium (Treximet tablets)
, Nasal Powder (Onzetra Xsail), sumatriptan and naproxen sodium (Treximet tablets)") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 05.70.10 Subject: Sumatriptan Page: 1 of 6 Last Review Date: March 16, 2018 Sumatriptan Description Sumatriptan
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 05.70.10 Subject: Sumatriptan Page: 1 of 6 Last Review Date: March 16, 2018 Sumatriptan Description Sumatriptan
Triptan Quantity Limit
 *- Florida Healthy Kids Triptan Quantity Limit Override(s) Quantity Limit Approval Duration 1 year Oral Tablets Axert (almotriptan) tablets Relpax (eletriptan) tablets 6 tablets (6.25 mg) 12 tablets (12.5
*- Florida Healthy Kids Triptan Quantity Limit Override(s) Quantity Limit Approval Duration 1 year Oral Tablets Axert (almotriptan) tablets Relpax (eletriptan) tablets 6 tablets (6.25 mg) 12 tablets (12.5
Acute Migraine Treatment: What you and your family should know to help you make the best choices with your doctor
 Acute Migraine Treatment: What you and your family should know to help you make the best choices with your doctor TAKE CONTROL OF YOUR MIGRAINES! ABOUT THIS PATIENT GUIDE: Migraine attacks are often debilitating
Acute Migraine Treatment: What you and your family should know to help you make the best choices with your doctor TAKE CONTROL OF YOUR MIGRAINES! ABOUT THIS PATIENT GUIDE: Migraine attacks are often debilitating
MEASURE #1: MEDICATION PRESCRIBED FOR ACUTE MIGRAINE ATTACK Headache
 MEASURE #1: MEDICATION PRESCRIBED FOR ACUTE MIGRAINE ATTACK Headache Measure Description Percentage of patients age 12 years and older with a diagnosis of migraine who were prescribed a guideline recommended
MEASURE #1: MEDICATION PRESCRIBED FOR ACUTE MIGRAINE ATTACK Headache Measure Description Percentage of patients age 12 years and older with a diagnosis of migraine who were prescribed a guideline recommended
Slide 1. Slide 2. Slide 3. Opioid (Narcotic) Analgesics and Antagonists. Lesson 6.1. Lesson 6.1. Opioid (Narcotic) Analgesics and Antagonists
 Analgesics and Antagonists. Lesson 6.1. Lesson 6.1. Opioid (Narcotic) Analgesics and Antagonists") Slide 1 Opioid (Narcotic) Analgesics and Antagonists Chapter 6 1 Slide 2 Lesson 6.1 Opioid (Narcotic) Analgesics and Antagonists 1. Explain the classification, mechanism of action, and pharmacokinetics
Slide 1 Opioid (Narcotic) Analgesics and Antagonists Chapter 6 1 Slide 2 Lesson 6.1 Opioid (Narcotic) Analgesics and Antagonists 1. Explain the classification, mechanism of action, and pharmacokinetics
Clinical case. Clinical case 3/15/2018 OVERVIEW. Refractory headaches and update on novel treatment. Refractory headache.
 OVERVIEW Refractory headaches and update on novel treatment Definition of refractory headache Treatment approach Medications Neuromodulation In the pipeline Juliette Preston, MD OHSU Headache Center Refractory
OVERVIEW Refractory headaches and update on novel treatment Definition of refractory headache Treatment approach Medications Neuromodulation In the pipeline Juliette Preston, MD OHSU Headache Center Refractory
How could I be having migraine when I don't have a headache?
 Migraine Your doctor thinks you may have migraine. Classic migraine attacks start with visual symptoms (often zig-zag colored lights or flashes of light expanding to one side over 10-30 minutes) followed
Migraine Your doctor thinks you may have migraine. Classic migraine attacks start with visual symptoms (often zig-zag colored lights or flashes of light expanding to one side over 10-30 minutes) followed
Controlling Migraine Pain
 Migraine Stats Controlling Migraine Pain Alan Zacharias, M.D. Associated Neurologists, Boulder Community Health 303-622-3365 Women 15% Men 5% Usually starts in 2 nd and 3 rd Decade Major Impact on days
Migraine Stats Controlling Migraine Pain Alan Zacharias, M.D. Associated Neurologists, Boulder Community Health 303-622-3365 Women 15% Men 5% Usually starts in 2 nd and 3 rd Decade Major Impact on days
What You Should Know About Your HEADACHE. Learn more about headache types, triggers, and treatments, when to get help, and how to help yourself
 What You Should Know About Your HEADACHE Learn more about headache types, triggers, and treatments, when to get help, and how to help yourself Introduction The purpose of this brochure is to give you a
What You Should Know About Your HEADACHE Learn more about headache types, triggers, and treatments, when to get help, and how to help yourself Introduction The purpose of this brochure is to give you a
Practice parameter: Evidence-based guidelines for migraine headache (an evidence-based review)
") Special Article Neurology 2000;55:754 763 Practice parameter: Evidence-based guidelines for migraine headache (an evidence-based review) Report of the Quality Standards Subcommittee of the American Academy
Special Article Neurology 2000;55:754 763 Practice parameter: Evidence-based guidelines for migraine headache (an evidence-based review) Report of the Quality Standards Subcommittee of the American Academy
Long-Term Care Updates
 Long-Term Care Updates September 2017 By Lindsay Slowiczek, PharmD Migraines are often considered to be a condition affecting younger or middle-aged patients, during which patients experience episodic,
Long-Term Care Updates September 2017 By Lindsay Slowiczek, PharmD Migraines are often considered to be a condition affecting younger or middle-aged patients, during which patients experience episodic,
TREXIMET UTILIZATION MANAGEMENT CRITERIA
 TREXIMET UTILIZATION MANAGEMENT CRITERIA DRUG CLASS: BRAND (generic) NAME: 5HT1 agonists Treximet (sumatriptan/naproxen sodium) 85 mg / 500 mg tablet FDA INDICATIONS: Sumatriptan/naproxen is indicated
TREXIMET UTILIZATION MANAGEMENT CRITERIA DRUG CLASS: BRAND (generic) NAME: 5HT1 agonists Treximet (sumatriptan/naproxen sodium) 85 mg / 500 mg tablet FDA INDICATIONS: Sumatriptan/naproxen is indicated
Ishaq Abu Arafeh Consultant Paediatrician Royal Hospital for Children, Glasgow Forth Valley Royal Hospital, Larbert
 Ishaq Abu Arafeh Consultant Paediatrician Royal Hospital for Children, Glasgow Forth Valley Royal Hospital, Larbert Childhood headache: Is it really difficult to manage? It shouldn t be... But it can be...
Ishaq Abu Arafeh Consultant Paediatrician Royal Hospital for Children, Glasgow Forth Valley Royal Hospital, Larbert Childhood headache: Is it really difficult to manage? It shouldn t be... But it can be...
Clinical Policy: Triptans Reference Number: CP.CPA.217 Effective Date: Last Review Date: Line of Business: Commercial
 Clinical Policy: Reference Number: CP.CPA.217 Effective Date: 11.16.16 Last Review Date: 11.18 Line of Business: Commercial Revision Log See Important Reminder at the end of this policy for important regulatory
Clinical Policy: Reference Number: CP.CPA.217 Effective Date: 11.16.16 Last Review Date: 11.18 Line of Business: Commercial Revision Log See Important Reminder at the end of this policy for important regulatory
Migraine Controversies in Women s Health. Professor Peter J. Goadsby 5 December Department of Neurology
 Migraine 2008 Controversies in Women s Health 5 December 2008 Professor Peter J. Goadsby Peter.Goadsby@headache.ucsf.edu Department of Neurology Headache International Headache Society Classification Primary
Migraine 2008 Controversies in Women s Health 5 December 2008 Professor Peter J. Goadsby Peter.Goadsby@headache.ucsf.edu Department of Neurology Headache International Headache Society Classification Primary
Overuse of barbiturate and opioid containing medications for primary headache disorders Description
 Measure Title Overuse of barbiturate and opioid containing medications for primary headache disorders Description Percentage of s age 12 years and older with a diagnosis of primary headache who were prescribed
Measure Title Overuse of barbiturate and opioid containing medications for primary headache disorders Description Percentage of s age 12 years and older with a diagnosis of primary headache who were prescribed
Neuro Basics SLO Practice (online) Page 1 of 5
 Page 1 of 5") Neuro Basics SLO Practice (online) Page 1 of 5 1) Biogenic amines include ACh, NE, EPI and? a) Melatonin b) Dopamine c) Serotonin d) Histamine e) All of the neurotransmitters listed are biogenic amines.
Neuro Basics SLO Practice (online) Page 1 of 5 1) Biogenic amines include ACh, NE, EPI and? a) Melatonin b) Dopamine c) Serotonin d) Histamine e) All of the neurotransmitters listed are biogenic amines.
Classification of headaches
 Classification of headaches Primary headaches OR Idiopathic headaches Secondary headaches OR Symptomatic headaches THE HEADACHE IS ITSELF THE DISEASE NO ORGANIC LESION IN THE BEACKGROUND TREAT THE HEADACHE!
Classification of headaches Primary headaches OR Idiopathic headaches Secondary headaches OR Symptomatic headaches THE HEADACHE IS ITSELF THE DISEASE NO ORGANIC LESION IN THE BEACKGROUND TREAT THE HEADACHE!
If Not Opioids then LEAH EDMONDS CSHP OCTOBER 26, 2017
 If Not Opioids then what LEAH EDMONDS CSHP OCTOBER 26, 2017 Disclosure Nothing to disclose Objectives Identify various non-opioid options for the treatment of chronic non cancer pain Choose appropriate
If Not Opioids then what LEAH EDMONDS CSHP OCTOBER 26, 2017 Disclosure Nothing to disclose Objectives Identify various non-opioid options for the treatment of chronic non cancer pain Choose appropriate
ISSN doi: /head VC 2015 American Headache Society Published by Wiley Periodicals, Inc.
 ISSN 0017-8748 Headache doi: 10.1111/head.12746 VC 2015 American Headache Society Published by Wiley Periodicals, Inc. Review Article Acute Treatment Therapies for Pediatric Migraine: A Qualitative Systematic
ISSN 0017-8748 Headache doi: 10.1111/head.12746 VC 2015 American Headache Society Published by Wiley Periodicals, Inc. Review Article Acute Treatment Therapies for Pediatric Migraine: A Qualitative Systematic
NARAMIG QUALITATIVE AND QUANTITATIVE COMPOSITION
 NARAMIG Naratriptan QUALITATIVE AND QUANTITATIVE COMPOSITION Tablets containing 2.5 mg of naratriptan as naratriptan hydrochloride. PHARMACEUTICAL FORM Film coated tablets. CLINICAL PARTICULARS Indications
NARAMIG Naratriptan QUALITATIVE AND QUANTITATIVE COMPOSITION Tablets containing 2.5 mg of naratriptan as naratriptan hydrochloride. PHARMACEUTICAL FORM Film coated tablets. CLINICAL PARTICULARS Indications
Practice parameter: Evidence-based guidelines for migraine headache (an evidence-based review)
") Copyright 2000 American Academy of Neurology Special Article Practice parameter: Evidence-based guidelines for headache (an evidence-based review) Report of the Quality Standards Subcommittee of the American
Copyright 2000 American Academy of Neurology Special Article Practice parameter: Evidence-based guidelines for headache (an evidence-based review) Report of the Quality Standards Subcommittee of the American
Dubai Standards of Care (Migraine)
") Dubai Standards of Care 2018 (Migraine) Preface Migraine is one of the most common problem dealt with in daily practice. In Dubai, the management of migraine is done through various different strategies.
Dubai Standards of Care 2018 (Migraine) Preface Migraine is one of the most common problem dealt with in daily practice. In Dubai, the management of migraine is done through various different strategies.
Migraine, Tension, and Cluster Headache: Primary Care for Primary Headaches. Jonathon M. Firnhaber, MD, FAAFP
 Migraine, Tension, and Cluster Headache: Primary Care for Primary Headaches Jonathon M. Firnhaber, MD, FAAFP Learning objectives 1. Utilize evidence-based strategies to diagnose patients presenting with
Migraine, Tension, and Cluster Headache: Primary Care for Primary Headaches Jonathon M. Firnhaber, MD, FAAFP Learning objectives 1. Utilize evidence-based strategies to diagnose patients presenting with
ARxCH. Annual Review of Changes in Healthcare. Calcitonin Gene-Related Peptide Receptors and the Prevention of Migraines. Abstract
 Calcitonin Gene-Related Peptide Receptors and the Prevention of Migraines Brian Schuler, PharmD Candidate 2018 1 1 University of Findlay College of Pharmacy Abstract Migraines are the third most prevalent
Calcitonin Gene-Related Peptide Receptors and the Prevention of Migraines Brian Schuler, PharmD Candidate 2018 1 1 University of Findlay College of Pharmacy Abstract Migraines are the third most prevalent