WHY IS MIGRAINE IMPORTANT
|
|
|
- Julia Preston
- 5 years ago
- Views:
Transcription

1 WHY IS MIGRAINE IMPORTANT
2 Migraine is a complex disorder characterized by recurrent episodes of headache, most often unilateral and in some cases associated with visual or sensory symptoms collectively known as an aura that arise most often before the head pain but that may occur during or afterward
3 Signs and symptoms Typical symptoms of migraine include the following: Throbbing or pulsatile headache, with moderate to severe pain that intensifies with movement or physical activity Unilateral and localized pain in the frontotemporal and ocular area, but the pain may be felt anywhere around the head or neck Pain builds up over a period of 1-2 hours, progressing posteriorly and becoming diffuse Headache lasts 4-72 hours Nausea (80%) and vomiting (50%), including anorexia and food intolerance, and light-headedness Sensitivity to light and sound

4 Features of migraine aura are as follows: May precede or accompany the headache phase or may occur in isolation Usually develops over 5-20 minutes and lasts less than 60 minutes Most commonly visual but can be sensory, motor, or any combination of these Visual symptoms may be positive or negative The most common positive visual phenomenon is the scintillating scotoma, an arc or band of absent vision with a shimmering or glittering zigzag border
 Adie-type pupil (ie, poor light reactivity,")
5 Physical findings during a migraine headache may include the following: Cranial/cervical muscle tenderness Horner syndrome (ie, relative miosis with 1-2 mm of ptosis on the same side as the headache) Conjunctival injection Tachycardia or bradycardia Hypertension or hypotension Hemisensory or hemiparetic neurologic deficits (ie, complicated migraine) Adie-type pupil (ie, poor light reactivity, with near dissociation from light)
6 Classification of migraine is as follows: Migraine without aura (formerly, common migraine) Probable migraine without aura Migraine with aura (formerly, classic migraine) Probable migraine with aura Chronic migraine Chronic migraine associated with analgesic overuse Childhood periodic syndromes that may not be precursors to or associated with migraine Complications of migraine Migrainous disorder not fulfilling above criteria
7 Migraine variants include the following: Childhood periodic syndromes Late-life migrainous accompaniments Basilar-type migraine Hemiplegic migraine Status migrainosus Ophthalmoplegic migraine Retinal migraine
8 NOT TO DO The American Headache Society released a list of 5 commonly performed tests or procedures that are not always necessary in the treatment of migraine and headache, as part of the American Board of Internal Medicine (ABIM) Foundation's Choosing Wisely campaign. The recommendations include [2, 3] : Don't perform neuroimaging studies in patients with stable headaches that meet criteria for migraine. Don't perform computed tomography imaging for headache when magnetic resonance imaging is available, except in emergency settings. Don't recommend surgical deactivation of migraine trigger points outside of a clinical trial. Don't prescribe opioid or butalbital-containing medications as first-line treatment for recurrent headache disorders. Don't recommend prolonged or frequent use of over-the-counter pain medications for headache.
9 PREVALENCE OF MIGRAINE Migraine is the 3rd most prevalent and 7th leading cause of disability worldwide. Age-standardized 1-year prevalence was 25.2% (95% CI: %; 10.6% definite, 14.6% probable migraine). Point prevalence (headache yesterday) was 2.7%. Prevalence was greater among females (31.6% vs 18.5%; OR=2.03 [95% CI: ]) and in rural areas (28.9% vs 21.7%; OR=1.45 [95% CI: ]). Prevalence peaked between years in both genders. Median frequency was 24 days/year, with a sizeable minority (6.6%) reporting >60 days/year. Headache intensity was severe in 40%. Lost productive time correlated with attack frequency. The overall mean total was 3.7 ±6.1 days/3 months, representing a loss of 6.1% of productive days, of which 2.1 ±4.0 days/3 months were lost at home and 1.4 ±4.1 days/months were lost in the work place. Disability was higher among women and in rural areas. A positive family history of headache was observed in 24.7% of probands with a possible maternal inheritance on clinical grounds in 29 of 41 families (70.7%)
10 AETIOLOGY Migraines are currently thought to be caused by dysfunction of the nerves in the brain. [10] Previously, migraines were thought to be caused by a primary problem with the blood vessels in the brain. [11] This vascular theory, which was developed in the 20th century by Wolff, suggested that the aura in migraines is caused by constriction of intracranial vessels (vessels inside the brain), and the headache itself is caused by rebound dilation of extracranial vessels (vessels just outside the brain). Dilation of these extracranial blood vessels activates the pain receptors in the surrounding nerves, causing a headache. The vascular theory is no longer accepted. [10][12] Studies have shown migraine head pain is not accompanied by extracranial vasodilation, but rather only has some mild intracranial vasodilation. [13]
11 Currently, most specialists think migraines are due to a primary problem with the nerves in the brain. [10] Auras are thought to be caused by a wave of increased activity of neurons in the cerebral cortex (a part of the brain) known as cortical spreading depression [14] followed by a period of depressed activity. [15] Some people think headaches are caused by the activation of sensory nerves which release peptides, such as serotonin, causing inflammation in arteries, dura and meninges and also cause some vasodilation. Triptans, medications which treat migraines, block serotonin receptors and constrict blood vessels. [16] People who are more susceptible to experience migraines without headache are those who have a family history of migraines, women, and women who are experiencing hormonal changes or are taking birth control pills or are prescribed hormone replacement therapy
12 targeting calcitonin gene-related peptide (CGRP), a small protein that plays a role in the initiation, transmission, and heightened sensitivity to migraine pain, might improve outcomes for patients. There are two main approaches for targeting CGRP in migraine: monoclonal antibodies given by injection to prevent attacks and small molecule, orally absorbable agents for use as acute treatment.
13 Differential diagnosis of headaches Tension headache New daily persistent headache Cluster headache Migraine mild to moderate dull or aching pain severe pain moderate to severe pain duration of 30 minutes to several hours duration of at least four hours daily duration of 30 minutes to 3 hours duration of 4 hours to 3 days Occur in periods of 15 days a month for three months may happen multiple times in a day for months periodic occurrence; several per month to several per year located as tightness or pressure across head located on one or both sides of head located one side of head focused at eye or temple located on one or both sides of head consistent pain pain describable as sharp or stabbing pulsating or throbbing pain no nausea or vomiting no aura no aura auras nausea, perhaps with vomiting uncommonly, light sensitivity or noise sensitivity may be accompanied by running nose, tears, and drooping eyelid, often only on one side sensitivity to movement, light, and noise exacerbated by regular use of acetaminophen or NSA IDS may exist with tension headache [20

14
15 Management Pharmacologic agents used for the treatment of migraine can be classified as abortive (ie, for alleviating the acute phase) or prophylactic (ie, preventive). Acute/abortive medications Acute treatment aims to reverse, or at least stop the progression of, a headache. It is most effective when given within 15 minutes of pain onset and when pain is mild. [4] Abortive medications include the following: Selective serotonin receptor (5-hydroxytryptamine 1, or 5-HT1) agonists (triptans) Ergot alkaloids (eg, ergotamine, dihydroergotamine [DHE]) Analgesics Nonsteroidal anti-inflammatory drugs (NSAIDs) Combination products Antiemetics
16 Preventive/prophylactic medications The following may be considered indications for prophylactic migraine therapy: Frequency of migraine attacks is greater than 2 per month Duration of individual attacks is longer than 24 hours The headaches cause major disruptions in the patient's lifestyle, with significant disability that lasts 3 or more days Abortive therapy fails or is overused Symptomatic medications are contraindicated or ineffective Use of abortive medications more than twice a week Migraine variants such as hemiplegic migraine or rare headache attacks producing profound disruption or risk of permanent neurologic injury [5]
17 Prophylactic medications include the following: Antiepileptic drugs Beta blockers Tricyclic antidepressants Calcium channel blockers Selective serotonin reuptake inhibitors (SSRIs) NSAIDs Serotonin antagonists Botulinum toxin Other measures Treatment of migraine may also include the following: Reduction of migraine triggers (eg, lack of sleep, fatigue, stress, certain foods) Nonpharmacologic therapy (eg, biofeedback, cognitive-behavioral therapy) Integrative medicine (eg, butterbur, riboflavin, magnesium, feverfew, coenzyme Q10)
18 AVOID COMPLICATIONS COMPLICATED MIGRAINE STATUS MIGRAINOSUS MEDICATION OVERUSE HEADACHE MIXED HEADACHES MIGRAINOUS INFARCTS
19 In cases of status migrainosus, aggressive therapy is warranted, including the following 5 components: Rehydration Analgesics (eg, ketorolac, naproxen, or indomethacin; ideally, narcotics should be avoided) Specific antimigraine medications (eg, triptans, valproate, or dihydroergotamine) Antiemetics (eg, prochlorperazine or metoclopramide) Sedatives (eg, diphenhydramine or a benzodiazepine) Steroids
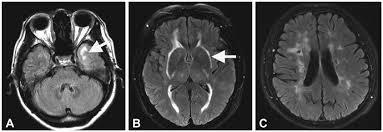
20 MIGRANOUS INFARCTS Migrainous infarction is a term that was originally coined by the International Headache Society to describe strokes which occur in the setting of a migraine attack. The word infarction, as used in this term, has the same meaning as the word stroke. Thus, this condition is also known as "migraineinduced stroke".
21 migrainous infarction mostly occurs in the posterior circulation, and in younger women with a history of migraine with aura. Acute ischemic lesions were often multiple and located in distinct arterial territories. As there were no overlapping ischemic lesions, hemodynamic compromise during the development of migraine is unlikely the cause of infarction The prevalence of a patent foramen ovale was high (64.7%)
22 MI is diagnosed when one or more aura symptoms last longer than 60 minutes, and neuroradiological studies demonstrate ischemic stroke that potentially explains the symptoms.

23
24 WOMEN WITH MIGRAINE CHILD BEARING AGE PREGNANT OC PILLS MENSTRUAL IRREGULARITIES
25 CO MORBIDITIES EPILEPSY DEPRESSION ANXIETY WEIGHT GAIN OBSTRUCTIVE AIRWAY DISEASE
26 CHILDHOOD MIGRAINE EPISODIC VOMITING ABDOMEN PAIN FAMILY HISTORY OF MIGRAINE
27 Recognized childhood syndromes assumed to be pathophysiologically related to migraine include the following: Benign paroxysmal vertigo of childhood Abdominal migraine Cyclic vomiting of childhood Acute confusional migraine (acute confusional state) Paroxysmal torticollis Infant colic (epidemiologic association with migraine)
28 Infants may present with only episodic head banging Preschool children often have episodes involving an ill appearance, abdominal pain, vomiting, and the need to go to sleep; they may exhibit pain by irritability, crying, rocking, or seeking a dark room in which to sleep Children aged 5-10 years typically have bifrontal, bitemporal, or retro-orbital headache; nausea; abdominal cramping; vomiting; photophobia; phonophobia; a need to sleep; migraine facies; tearing, swollen nasal passages; thirst; edema; excessive sweating; increased urination; or diarrhea Older children may experience increasing headache intensity and duration; a pulsating or throbbing character to the headache; and a shift to a unilateral, temporal location
29 Measures that may be helpful for managing acute attacks include the following: Advising the child to lie down in a cool, dark, quiet room during the attack and go to sleep Providing simple analgesics (eg, acetaminophen or ibuprofen); in some cases, stronger agents (eg, butalbital) may be necessary Applying ice or pressure to the affected artery Using nonpharmacologic treatment modalities such as selfrelaxation, biofeedback, and self-hypnosis Employing specific pharmacologic abortive therapies for acute attacks (ie, ergot preparations or triptans) Analgesic and abortive therapies are for occasional acute attacks and should not be used frequently (frequent use may result in rebound headaches).
30 Possible medications for migraine prophylaxis include the following: Amitriptyline Propranolol Selective serotonin reuptake inhibitors Anticonvulsants (eg, gabapentin, valproate, and topiramate) Riboflavin Tricyclic antidepressants The agents that seem to be the most effective for prophylaxis in children are those that block the serotonin 5-HT2 receptor, such as the following: Beta blockers Cyproheptadine Methysergide

31 CADASIL
32 The American Headache Society recommends using "SSNOOP", a mnemonic to remember the red flags for identifying a secondary headache: [22] Systemic symptoms (fever or weight loss) Systemic disease (HIV infection, malignancy) Neurologic symptoms or signs Onset sudden (thunderclap headache) Onset after age 40 years Previous headache history (first, worst, or different headache)
33 REAL EMERGENCY Emergency phone call 26yrs female presented with acute headaches with vomiting not relieved with migranil,action 500,saridon History dates back So called new onset headaches Relief of symptoms

34 CURABLE TREATABLE
35 Management of pediatric migraine has the following 3 facets: Educate patients and parents concerning migraine triggers Formulate a plan of treatment for the acute attacks Consider prophylaxis for patients with frequent migraines Treatment of mild, infrequent attacks consists primarily of rest, trigger avoidance, and stress reduction. Education regarding migraine triggers includes the following: Explaining the disease to the child and the parents Encouraging parents to maintain a regular bedtime and strict meal schedules for the child and to avoid overloading the child s schedule with activities Helping the child recognize and avoid precipitating triggers to the extent possible, while maintaining realistic expectations (ie, migraine frequency may be reduced, but headaches will not be entirely eliminated) Helping the child keep a headache diary to record unique triggers and features of attacks
36 PRESCRIPTION ERRORS MIGRANIL PAIN KILLERS SIBELIUM-acute treatment Subordinate prescription


37
38 Papilledema Severe headache following head trauma Inability to move a limb Change in personality, consciousness, or mental status Headache triggered by cough, exertion or while engaged in sexual intercourse hypertension (pseudo (from inside the tumor brain) and causes cerebri), meningitis papilledema. Brain bleeds (intracranial hemorrhage, subdura l hematoma, epidural hematoma), posttraumatic headache Arteriovenous malformation, collagen vascular disease, intracranial mass lesion Trauma can cause bleeding in the brain or shake the nerves, causing a posttraumatic headache Other red flag symptoms include: [6][22][23][25] Central nervous system infection, intracranial bleed, mass Mass lesion, subarachnoid hemorrhage lumbar puncture Neuroimaging of brain, skull, and possibly cervical spine Focal neurological signs indicate Neuroimaging, blood something is pushing tests for collagen against nerves in the vascular diseases brain responsible for one part of the body Change in mental status indicates a global infection or inflammation of the brain, or a large bleed compressing the brainstem where the consciousness centers lie Blood tests, lumbar puncture, neuroimaging Coughing and exertion increases the intra cranial pressure, which may cause a vessel to burst, causing a subarachnoid hemorrhage. A mass Neuroimaging, lesion already lumbar puncture increases intracranial pressure, so an
Headache Assessment In Primary Eye Care
 Headache Assessment In Primary Eye Care Spencer Johnson, O.D., F.A.A.O. Northeastern State University Oklahoma College of Optometry johns137@nsuok.edu Course Objectives Review headache classification Understand
Headache Assessment In Primary Eye Care Spencer Johnson, O.D., F.A.A.O. Northeastern State University Oklahoma College of Optometry johns137@nsuok.edu Course Objectives Review headache classification Understand
MIGRAINE A MYSTERY HEADACHE
 MIGRAINE A MYSTERY HEADACHE The migraine is a chronic neurological disease that is characterized by moderate to severe episodes of headache that is mostly associated with other central nervous system (CNS)
MIGRAINE A MYSTERY HEADACHE The migraine is a chronic neurological disease that is characterized by moderate to severe episodes of headache that is mostly associated with other central nervous system (CNS)
Index. Prim Care Clin Office Pract 31 (2004) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Prim Care Clin Office Pract 31 (2004) 441 447 Index Note: Page numbers of article titles are in boldface type. A Abscess, brain, headache in, 388 Acetaminophen for migraine, 406 407 headache from, 369
Prim Care Clin Office Pract 31 (2004) 441 447 Index Note: Page numbers of article titles are in boldface type. A Abscess, brain, headache in, 388 Acetaminophen for migraine, 406 407 headache from, 369
MIGRAINE UPDATE. Objectives & Disclosures. Learn techniques used to diagnose headaches. Become familiar with medications used for headache treatment.
 MIGRAINE UPDATE Karen L. Bremer, MD November 16, 2018 Objectives & Disclosures Learn techniques used to diagnose headaches. Become familiar with medications used for headache treatment. Disclosure: I am
MIGRAINE UPDATE Karen L. Bremer, MD November 16, 2018 Objectives & Disclosures Learn techniques used to diagnose headaches. Become familiar with medications used for headache treatment. Disclosure: I am
Chronic Daily Headaches
 Chronic Daily Headaches ANWARUL HAQ, MD, MRCP(UK), FAHS DIRECTOR BAYLOR HEADACHE CENTER, DALLAS, TEXAS DISCLOSURES: None OBJECTIVES AT THE CONCLUSION OF THIS ACTIVITY, PARTICIPANTS WILL BE ABLE TO: define
Chronic Daily Headaches ANWARUL HAQ, MD, MRCP(UK), FAHS DIRECTOR BAYLOR HEADACHE CENTER, DALLAS, TEXAS DISCLOSURES: None OBJECTIVES AT THE CONCLUSION OF THIS ACTIVITY, PARTICIPANTS WILL BE ABLE TO: define
Faculty Disclosure. Karen L. Bremer, MD. Dr. Bremer has listed no financial interest/arrangement that would be considered a conflict of interest.
 Faculty Disclosure Karen L. Bremer, MD Dr. Bremer has listed no financial interest/arrangement that would be considered a conflict of interest. HEADACHE UPDATE Karen L. Bremer, MD November 10, 2017 karen.bremer@creighton.edu
Faculty Disclosure Karen L. Bremer, MD Dr. Bremer has listed no financial interest/arrangement that would be considered a conflict of interest. HEADACHE UPDATE Karen L. Bremer, MD November 10, 2017 karen.bremer@creighton.edu
ADVANCES IN MIGRAINE MANAGEMENT
 ADVANCES IN MIGRAINE MANAGEMENT Joanna Girard Katzman, M.D.MSPH Assistant Professor, Dept. of Neurology Project ECHO, Chronic Pain Program University of New Mexico Outline Migraine throughout the decades
ADVANCES IN MIGRAINE MANAGEMENT Joanna Girard Katzman, M.D.MSPH Assistant Professor, Dept. of Neurology Project ECHO, Chronic Pain Program University of New Mexico Outline Migraine throughout the decades
HEADACHE: Benign or Severe Dr Gobinda Chandra Roy
 HEADACHE: Benign or Severe Dr Gobinda Chandra Roy Associate Professor, Department of Medicine, Shaheed Suhrawardy Medical College and Hospital Outlines 1. Introduction 2. Classification of headache 3.
HEADACHE: Benign or Severe Dr Gobinda Chandra Roy Associate Professor, Department of Medicine, Shaheed Suhrawardy Medical College and Hospital Outlines 1. Introduction 2. Classification of headache 3.
I have no financial relationships to disclose. I will not discuss investigational use of medication in my presentation.
 I have no financial relationships to disclose. I will not discuss investigational use of medication in my presentation. In 1962, Bille published landmark epidemiologic survey of headache among 9,000 school
I have no financial relationships to disclose. I will not discuss investigational use of medication in my presentation. In 1962, Bille published landmark epidemiologic survey of headache among 9,000 school
Strategies in Migraine Care
 Strategies in Migraine Care Julie L. Roth, MD Rhode Island Hospital Assistant Professor, Neurology The Warren Alpert Medical School of Brown University March 28, 2015 Financial Disclosures None. Objectives
Strategies in Migraine Care Julie L. Roth, MD Rhode Island Hospital Assistant Professor, Neurology The Warren Alpert Medical School of Brown University March 28, 2015 Financial Disclosures None. Objectives
Controlling Migraine Pain
 Migraine Stats Controlling Migraine Pain Alan Zacharias, M.D. Associated Neurologists, Boulder Community Health 303-622-3365 Women 15% Men 5% Usually starts in 2 nd and 3 rd Decade Major Impact on days
Migraine Stats Controlling Migraine Pain Alan Zacharias, M.D. Associated Neurologists, Boulder Community Health 303-622-3365 Women 15% Men 5% Usually starts in 2 nd and 3 rd Decade Major Impact on days
A synopsis of: Diagnosis and Management of Headaches in Adults: A national clinical guideline. Scottish intercollegiate Guidelines Network SIGN
 A synopsis of: Diagnosis and Management of Headaches in Adults: A national clinical guideline Scottish intercollegiate Guidelines Network SIGN November 2008. PETER FRAMPTON MSc MCOptom BAppSc (Optom)(AUS)
A synopsis of: Diagnosis and Management of Headaches in Adults: A national clinical guideline Scottish intercollegiate Guidelines Network SIGN November 2008. PETER FRAMPTON MSc MCOptom BAppSc (Optom)(AUS)
HMFP Comprehensive Headache Center Department of Anesthesia, Critical Care and Pain Medicine Beth Israel Deaconess Medical Center Instructor in
 HMFP Comprehensive Headache Center Department of Anesthesia, Critical Care and Pain Medicine Beth Israel Deaconess Medical Center Instructor in Anesthesia and Neurology Harvard Medical School Limited time
HMFP Comprehensive Headache Center Department of Anesthesia, Critical Care and Pain Medicine Beth Israel Deaconess Medical Center Instructor in Anesthesia and Neurology Harvard Medical School Limited time
A case of a patient with chronic headache. Focus on Migraine. None related to the presentation Grants to conduct clinical trials from: Speaker bureau:
 Chronic Daily Headache Bassel F. Shneker, MD, MBA Associate Professor Vice Chair, OSU Neurology The Ohio State University Wexner Medical Center Financial Disclosures None related to the presentation Grants
Chronic Daily Headache Bassel F. Shneker, MD, MBA Associate Professor Vice Chair, OSU Neurology The Ohio State University Wexner Medical Center Financial Disclosures None related to the presentation Grants
Update on Diagnosis and Management of Migraines
 Update on Diagnosis and Management of Migraines Joel J. Heidelbaugh, MD, FAAFP, FACG Clinical Professor Departments of Family Medicine and Urology University of Michigan Learning Objectives To distinguish
Update on Diagnosis and Management of Migraines Joel J. Heidelbaugh, MD, FAAFP, FACG Clinical Professor Departments of Family Medicine and Urology University of Michigan Learning Objectives To distinguish
How could I be having migraine when I don't have a headache?
 Migraine Your doctor thinks you may have migraine. Classic migraine attacks start with visual symptoms (often zig-zag colored lights or flashes of light expanding to one side over 10-30 minutes) followed
Migraine Your doctor thinks you may have migraine. Classic migraine attacks start with visual symptoms (often zig-zag colored lights or flashes of light expanding to one side over 10-30 minutes) followed
Regulatory Status FDA approved indication: Migranal Nasal Spray is indicated for the acute treatment of migraine headaches with or without aura (1).
.") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.60 Subject: Migranal Nasal Spray Page: 1 of 5 Last Review Date: November 30, 2018 Migranal Nasal Spray
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.60 Subject: Migranal Nasal Spray Page: 1 of 5 Last Review Date: November 30, 2018 Migranal Nasal Spray
Case Presentation. Case Presentation. Case Presentation. Truths about Headaches (2017) Most headaches were muscle-tension headaches
 Most headaches were muscle-tension headaches") Agenda Case presentation Migraine Morphology Primary and Premonitory Phase Secondary Headache Aura Headache Primer on Pain Medication Overuse Headache Case Presentation RT is a 25 year old woman with daily
Agenda Case presentation Migraine Morphology Primary and Premonitory Phase Secondary Headache Aura Headache Primer on Pain Medication Overuse Headache Case Presentation RT is a 25 year old woman with daily
ปวดศ รษะมา 5 ป ก นยาแก ปวดก ย งไม ข น นพ.พาว ฒ เมฆว ช ย โรงพยาบาลนครราชส มา
 ปวดศ รษะมา 5 ป ก นยาแก ปวดก ย งไม ข น นพ.พาว ฒ เมฆว ช ย โรงพยาบาลนครราชส มา 1 CONTENT 1 2 3 Chronic Daily Headache Medical Overused Headache Management Headaches are one of the most common symptoms List
ปวดศ รษะมา 5 ป ก นยาแก ปวดก ย งไม ข น นพ.พาว ฒ เมฆว ช ย โรงพยาบาลนครราชส มา 1 CONTENT 1 2 3 Chronic Daily Headache Medical Overused Headache Management Headaches are one of the most common symptoms List
Outpatient Headache Care Guideline
 1 Outpatient Care Guideline Inclusion criteria: children > 3 yrs with headaches Is urgent emergency department, neuroimaging, or Neurology consultation indicated? Referral to ED if: New severe headache
1 Outpatient Care Guideline Inclusion criteria: children > 3 yrs with headaches Is urgent emergency department, neuroimaging, or Neurology consultation indicated? Referral to ED if: New severe headache
HEADACHE. Dr Nick Pendleton. September Headache
 HEADACHE Dr Nick Pendleton September 2017 Headache Tension Type Headache Cranial Nerve Examination Migraine Migraine Treatment Medication Overuse Headache Headache Red Flags Sinusitis Headache Raised ICP
HEADACHE Dr Nick Pendleton September 2017 Headache Tension Type Headache Cranial Nerve Examination Migraine Migraine Treatment Medication Overuse Headache Headache Red Flags Sinusitis Headache Raised ICP
25/09/2018 HEADACHE. Dr Nick Pendleton
 HEADACHE Dr Nick Pendleton September 2018 1 Small Group Work Tension Type Headache Cranial Nerve Examination Migraine Migraine Treatment Medication Overuse Headache Headache Red Flags Sinusitis Headache
HEADACHE Dr Nick Pendleton September 2018 1 Small Group Work Tension Type Headache Cranial Nerve Examination Migraine Migraine Treatment Medication Overuse Headache Headache Red Flags Sinusitis Headache
Headache Syndrome. Karen Alvarez, D.O Nemours Children s Specialty Care Jacksonville, FL
 Headache Syndrome Karen Alvarez, D.O Nemours Children s Specialty Care Jacksonville, FL What is a headache? A headache or cephalgia is defined as pain anywhere in the region of head or neck Where does
Headache Syndrome Karen Alvarez, D.O Nemours Children s Specialty Care Jacksonville, FL What is a headache? A headache or cephalgia is defined as pain anywhere in the region of head or neck Where does
Disclosures. Objectives 6/2/2017
 Classification: Migraine and Trigeminal Autonomic Cephalalgias Lauren Doyle Strauss, DO, FAHS Assistant Professor, Child Neurology Assistant Director, Child Neurology Residency @StraussHeadache No disclosures
Classification: Migraine and Trigeminal Autonomic Cephalalgias Lauren Doyle Strauss, DO, FAHS Assistant Professor, Child Neurology Assistant Director, Child Neurology Residency @StraussHeadache No disclosures
MIGRAINE CLASSIFICATION
 MIGRAINE CLASSIFICATION Nada Šternić At most, only 30% of migraineurs have classic aura The same patient may have migraine headache without aura, migraine headache with aura as well as migraine aura without
MIGRAINE CLASSIFICATION Nada Šternić At most, only 30% of migraineurs have classic aura The same patient may have migraine headache without aura, migraine headache with aura as well as migraine aura without
Understanding. Migraine. Amy, diagnosed in 1989, with her family.
 Understanding Migraine Amy, diagnosed in 1989, with her family. What Is a Migraine? A migraine is a recurring moderate to severe headache. The pain usually occurs on one side of the head. It is typically
Understanding Migraine Amy, diagnosed in 1989, with her family. What Is a Migraine? A migraine is a recurring moderate to severe headache. The pain usually occurs on one side of the head. It is typically
Chronic Migraine in Primary Care. December 11 th, 2017 Werner J. Becker University of Calgary
 Chronic Migraine in Primary Care December 11 th, 2017 Werner J. Becker University of Calgary Disclosures Faculty: Werner J. Becker Relationships with commercial interests: Grants/Research Support: Clinical
Chronic Migraine in Primary Care December 11 th, 2017 Werner J. Becker University of Calgary Disclosures Faculty: Werner J. Becker Relationships with commercial interests: Grants/Research Support: Clinical
How do we treat migraine? New SIGN Guidelines
 How do we treat migraine? New SIGN Guidelines Managing your migraine Migraine Trust, Edinburgh 2018 Callum Duncan Consultant Neurologist Aberdeen Royal Infirmary Chair SIGN Guideline 155 Premonitory Mood
How do we treat migraine? New SIGN Guidelines Managing your migraine Migraine Trust, Edinburgh 2018 Callum Duncan Consultant Neurologist Aberdeen Royal Infirmary Chair SIGN Guideline 155 Premonitory Mood
Dubai Standards of Care (Migraine)
") Dubai Standards of Care 2018 (Migraine) Preface Migraine is one of the most common problem dealt with in daily practice. In Dubai, the management of migraine is done through various different strategies.
Dubai Standards of Care 2018 (Migraine) Preface Migraine is one of the most common problem dealt with in daily practice. In Dubai, the management of migraine is done through various different strategies.
Tears of Pain SUNCT and SUNA A/PROFESSOR ARUN AGGARWAL RPAH PAIN MANAGEMENT CENTRE
 Tears of Pain SUNCT and SUNA A/PROFESSOR ARUN AGGARWAL RPAH PAIN MANAGEMENT CENTRE IHS Classification 1989 (updated 2004) Primary Headaches 4 categories Migraine Tension-type Cluster and other trigeminal
Tears of Pain SUNCT and SUNA A/PROFESSOR ARUN AGGARWAL RPAH PAIN MANAGEMENT CENTRE IHS Classification 1989 (updated 2004) Primary Headaches 4 categories Migraine Tension-type Cluster and other trigeminal
Headache Mary D. Hughes, MD Neuroscience Associates
 Headache Mary D. Hughes, MD Neuroscience Associates Case 1 22 year old female presents with recurrent headaches. She has had headaches for the past 3 years. They start on the right side of her head and
Headache Mary D. Hughes, MD Neuroscience Associates Case 1 22 year old female presents with recurrent headaches. She has had headaches for the past 3 years. They start on the right side of her head and
Zomig. Zomig / Zomig-ZMT (zolmitriptan) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.22 Subject: Zomig Page: 1 of 5 Last Review Date: November 30, 2018 Zomig Description Zomig / Zomig-ZMT
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.22 Subject: Zomig Page: 1 of 5 Last Review Date: November 30, 2018 Zomig Description Zomig / Zomig-ZMT
Headache. Section 1. Migraine headache. Clinical presentation
 Section 1 Headache Migraine headache 1 Clinical presentation It is important to recognize just how significant a problem migraine headache is. It has been estimated that migraine affects 11% of the United
Section 1 Headache Migraine headache 1 Clinical presentation It is important to recognize just how significant a problem migraine headache is. It has been estimated that migraine affects 11% of the United
Headaches in Children
 How common are headaches? What is the impact? Very common! 20% of kids from preschool through teenage report frequent or severe headaches in any given year 2 Headaches are more common in children who have
How common are headaches? What is the impact? Very common! 20% of kids from preschool through teenage report frequent or severe headaches in any given year 2 Headaches are more common in children who have
Migranal Nasal Spray. Migranal Nasal Spray (dihydroergotamine) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.60 Subject: Migranal Nasal Spray Page: 1 of 5 Last Review Date: June 22, 2017 Migranal Nasal Spray
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.60 Subject: Migranal Nasal Spray Page: 1 of 5 Last Review Date: June 22, 2017 Migranal Nasal Spray
Ishaq Abu Arafeh Consultant Paediatrician Royal Hospital for Children, Glasgow Forth Valley Royal Hospital, Larbert
 Ishaq Abu Arafeh Consultant Paediatrician Royal Hospital for Children, Glasgow Forth Valley Royal Hospital, Larbert Childhood headache: Is it really difficult to manage? It shouldn t be... But it can be...
Ishaq Abu Arafeh Consultant Paediatrician Royal Hospital for Children, Glasgow Forth Valley Royal Hospital, Larbert Childhood headache: Is it really difficult to manage? It shouldn t be... But it can be...
Classification of headaches
 Classification of headaches Primary headaches OR Idiopathic headaches Secondary headaches OR Symptomatic headaches THE HEADACHE IS ITSELF THE DISEASE NO ORGANIC LESION IN THE BEACKGROUND TREAT THE HEADACHE!
Classification of headaches Primary headaches OR Idiopathic headaches Secondary headaches OR Symptomatic headaches THE HEADACHE IS ITSELF THE DISEASE NO ORGANIC LESION IN THE BEACKGROUND TREAT THE HEADACHE!
They are updated regularly as new NICE guidance is published. To view the latest version of this NICE Pathway see:
 bring together everything NICE says on a topic in an interactive flowchart. are interactive and designed to be used online. They are updated regularly as new NICE guidance is published. To view the latest
bring together everything NICE says on a topic in an interactive flowchart. are interactive and designed to be used online. They are updated regularly as new NICE guidance is published. To view the latest
Migraine Management. Jane Melling Headache nurse Mater Misericordiae Hospital
 Migraine Management Jane Melling Headache nurse Mater Misericordiae Hospital Migraine facts Among the most common disorders of the nervous system 3 rd most prevalent medical disorder on the planet (lancet
Migraine Management Jane Melling Headache nurse Mater Misericordiae Hospital Migraine facts Among the most common disorders of the nervous system 3 rd most prevalent medical disorder on the planet (lancet
Paediatric headaches. Dr Jaycen Cruickshank Director of Clinical Training Ballarat Health Services. Brevity, levity, repetition
 Paediatric headaches Dr Jaycen Cruickshank Director of Clinical Training Ballarat Health Services Brevity, levity, repetition Paediatric)headache?)! Headache!in!children!is!not!that!common.!The!question!is!which!headaches!do!I!
Paediatric headaches Dr Jaycen Cruickshank Director of Clinical Training Ballarat Health Services Brevity, levity, repetition Paediatric)headache?)! Headache!in!children!is!not!that!common.!The!question!is!which!headaches!do!I!
10/31/2017 PRIMARY CARE AND HEADACHE DISCLOSURES WHERE DO THOSE WITH HEADACHE SEEK MEDICAL CARE? Primary Care 67%
 PRIMARY CARE AND HEADACHE Sonja Potrebic MD PhD Regional Headache Specialist Kaiser LAMC 1 WHERE DO THOSE WITH HEADACHE SEEK MEDICAL CARE? Column1 Primary Care 67% Primary Care Headache Specialty Other
PRIMARY CARE AND HEADACHE Sonja Potrebic MD PhD Regional Headache Specialist Kaiser LAMC 1 WHERE DO THOSE WITH HEADACHE SEEK MEDICAL CARE? Column1 Primary Care 67% Primary Care Headache Specialty Other
Sumatriptan Tablets, Nasal Spray (Imitrex), Nasal Powder (Onzetra Xsail), sumatriptan and naproxen sodium (Treximet tablets)
, Nasal Powder (Onzetra Xsail), sumatriptan and naproxen sodium (Treximet tablets)") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 0 Subject: Sumatriptan Page: 1 of 6 Last Review Date: November 30, 2018 Sumatriptan Description Sumatriptan
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 0 Subject: Sumatriptan Page: 1 of 6 Last Review Date: November 30, 2018 Sumatriptan Description Sumatriptan
Headache Pain Generators
 Objectives 1. Define the major categories of headache. 2. Take a history directed at characterizing a headache pattern in an individual patient and identify the cause or triggers of the headache. 3. Understand
Objectives 1. Define the major categories of headache. 2. Take a history directed at characterizing a headache pattern in an individual patient and identify the cause or triggers of the headache. 3. Understand
11. HEADACHE 1. Pablo Lapuerta, MD, Steven Asch, MD, MPH, and Kenneth Clark, MD, MPH
 11. HEADACHE 1 Pablo Lapuerta, MD, Steven Asch, MD, MPH, and Kenneth Clark, MD, MPH We identified articles on the evaluation and management of headache by conducting a MEDLINE search of English language
11. HEADACHE 1 Pablo Lapuerta, MD, Steven Asch, MD, MPH, and Kenneth Clark, MD, MPH We identified articles on the evaluation and management of headache by conducting a MEDLINE search of English language
Headache and Facial Pain. Mohammed ALEssa MBBS, FRCSC Assistant Professor Consultant Otolaryngology,Head & Neck Surgical Oncology
 Headache and Facial Pain Mohammed ALEssa MBBS, FRCSC Assistant Professor Consultant Otolaryngology,Head & Neck Surgical Oncology Introduction It is the most common neurologic complain The diagnosis usually
Headache and Facial Pain Mohammed ALEssa MBBS, FRCSC Assistant Professor Consultant Otolaryngology,Head & Neck Surgical Oncology Introduction It is the most common neurologic complain The diagnosis usually
ONZETRA XSAIL (sumatriptan) nasal powder
 nasal powder") ONZETRA XSAIL (sumatriptan) nasal powder Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy
ONZETRA XSAIL (sumatriptan) nasal powder Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy
GENERAL APPROACH AND CLASSIFICATION OF HEADACHES
 GENERAL APPROACH AND CLASSIFICATION OF HEADACHES CLASSIFICATION Headache is one of the most common medical complaints. Most of the population will have experienced headache, and over 5% will seek medical
GENERAL APPROACH AND CLASSIFICATION OF HEADACHES CLASSIFICATION Headache is one of the most common medical complaints. Most of the population will have experienced headache, and over 5% will seek medical
MEASURE #3: PREVENTIVE MIGRAINE MEDICATION PRESCRIBED Headache
 MEASURE #3: PREVENTIVE MIGRAINE MEDICATION PRESCRIBED Headache Measure Description Percentage of patients age 18 years old and older diagnosed with migraine headache whose migraine frequency is 4 migraine
MEASURE #3: PREVENTIVE MIGRAINE MEDICATION PRESCRIBED Headache Measure Description Percentage of patients age 18 years old and older diagnosed with migraine headache whose migraine frequency is 4 migraine
Headaches. Mini Medical School. November 10, A. Laine Green MSc, MD FRCP(C) Assistant Professor Department of Medicine (Neurology)
 Assistant Professor Department of Medicine (Neurology)") Headaches. Mini Medical School. November 10, 2016 A. Laine Green MSc, MD FRCP(C) Assistant Professor Department of Medicine (Neurology) Artist Agnes Cecile Disclosures I have received an honorarium from
Headaches. Mini Medical School. November 10, 2016 A. Laine Green MSc, MD FRCP(C) Assistant Professor Department of Medicine (Neurology) Artist Agnes Cecile Disclosures I have received an honorarium from
Zomig. Zomig / Zomig-ZMT (zolmitriptan) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.22 Subject: Zomig Page: 1 of 5 Last Review Date: March 16, 2018 Zomig Description Zomig / Zomig-ZMT
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.22 Subject: Zomig Page: 1 of 5 Last Review Date: March 16, 2018 Zomig Description Zomig / Zomig-ZMT
July 2012 Target Population. Adult patients 18 years or older in primary care settings.
 Guideline for Primary Care Management of Headache in Adults July 2012 Target Population Adult patients 18 years or older in primary care settings. Exclusions: This guideline does not provide recommendations
Guideline for Primary Care Management of Headache in Adults July 2012 Target Population Adult patients 18 years or older in primary care settings. Exclusions: This guideline does not provide recommendations
Do you suffer from Headaches? - November/Dec 2011
 Do you suffer from Headaches? - November/Dec 2011 Inside this month's issue Headaches Acute single headaches Recurring Headaches: Migraine What causes Migraine? Treatments for migraine & prevention Headaches
Do you suffer from Headaches? - November/Dec 2011 Inside this month's issue Headaches Acute single headaches Recurring Headaches: Migraine What causes Migraine? Treatments for migraine & prevention Headaches
Common Headaches. Types and Natural Treatments
 Common Headaches Types and Natural Treatments by Heidi Fritz, MA, ND Bolton Naturopathic Clinic 64 King St W, Bolton, Ontario, L7E1C7 www.boltonnaturopathic.ca Three Common Types of Headaches Headaches
Common Headaches Types and Natural Treatments by Heidi Fritz, MA, ND Bolton Naturopathic Clinic 64 King St W, Bolton, Ontario, L7E1C7 www.boltonnaturopathic.ca Three Common Types of Headaches Headaches
CYCLIC VOMITING SYNDROME. C. Prakash Gyawali, MD Professor of Medicine Washington University in St. Louis
 CYCLIC VOMITING SYNDROME C. Prakash Gyawali, MD Professor of Medicine Washington University in St. Louis Case 26 year old male Symptoms began at age 19 yr 5-6 day episodes of recurrent, severe vomiting
CYCLIC VOMITING SYNDROME C. Prakash Gyawali, MD Professor of Medicine Washington University in St. Louis Case 26 year old male Symptoms began at age 19 yr 5-6 day episodes of recurrent, severe vomiting
Current Migraine Treatment Therapy. Daniel Kassicieh, DO, FAAN
 Current Migraine Treatment Therapy Daniel Kassicieh, DO, FAAN Migraine a Disease Process Migraines are a chronic disease process similar to many other chronic medical conditions Migraine has a low mortality
Current Migraine Treatment Therapy Daniel Kassicieh, DO, FAAN Migraine a Disease Process Migraines are a chronic disease process similar to many other chronic medical conditions Migraine has a low mortality
Sumatriptan Tablets, Nasal Spray (Imitrex), Nasal Powder (Onzetra Xsail), sumatriptan and naproxen sodium (Treximet tablets)
, Nasal Powder (Onzetra Xsail), sumatriptan and naproxen sodium (Treximet tablets)") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 05.70.10 Subject: Sumatriptan Page: 1 of 6 Last Review Date: March 16, 2018 Sumatriptan Description Sumatriptan
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 05.70.10 Subject: Sumatriptan Page: 1 of 6 Last Review Date: March 16, 2018 Sumatriptan Description Sumatriptan
HEADACHES THE RED FLAGS
 HEADACHES THE RED FLAGS FAYYAZ AHMED CONSULTANT NEUROLOGIST HON. SENIOR LECTURER HULL YORK MEDICAL SCHOOL SECONDARY VS PRIMARY HEADACHES COMMON SECONDARY HEADACHES UNCOMMON BUT SERIOUS SECONDARY HEADACHES
HEADACHES THE RED FLAGS FAYYAZ AHMED CONSULTANT NEUROLOGIST HON. SENIOR LECTURER HULL YORK MEDICAL SCHOOL SECONDARY VS PRIMARY HEADACHES COMMON SECONDARY HEADACHES UNCOMMON BUT SERIOUS SECONDARY HEADACHES
Clinical case. Clinical case 3/15/2018 OVERVIEW. Refractory headaches and update on novel treatment. Refractory headache.
 OVERVIEW Refractory headaches and update on novel treatment Definition of refractory headache Treatment approach Medications Neuromodulation In the pipeline Juliette Preston, MD OHSU Headache Center Refractory
OVERVIEW Refractory headaches and update on novel treatment Definition of refractory headache Treatment approach Medications Neuromodulation In the pipeline Juliette Preston, MD OHSU Headache Center Refractory
Goals. Primary Headache Syndromes. One-Year Prevalence of Common Headache Disorders
 Goals One-Year Prevalence of Common Headache Disorders Impact of primary headache syndromes Non pharmacologic Rx of migraine individualized to patient triggers Complementary and alternative Rx of migraine
Goals One-Year Prevalence of Common Headache Disorders Impact of primary headache syndromes Non pharmacologic Rx of migraine individualized to patient triggers Complementary and alternative Rx of migraine
What You Should Know About Your HEADACHE. Learn more about headache types, triggers, and treatments, when to get help, and how to help yourself
 What You Should Know About Your HEADACHE Learn more about headache types, triggers, and treatments, when to get help, and how to help yourself Introduction The purpose of this brochure is to give you a
What You Should Know About Your HEADACHE Learn more about headache types, triggers, and treatments, when to get help, and how to help yourself Introduction The purpose of this brochure is to give you a
2) Headache - Dr. Hawar
 Headache - Dr. Hawar") 2) Headache - Dr. Hawar Headache is caused by traction, displacement, inflammation, vascular spasm, or distention of the painsensitive structures in the head or neck. Isolated involvement of the bony skull,
2) Headache - Dr. Hawar Headache is caused by traction, displacement, inflammation, vascular spasm, or distention of the painsensitive structures in the head or neck. Isolated involvement of the bony skull,
What is it? A severe painful headache with no cure Accompanied or preceded by sensory warning signs such as. Usually affects one side of the brain
 Migraines What is it? A severe painful headache with no cure Accompanied or preceded by sensory warning signs such as flashes of light blind spots, tingling in the arms and legs nausea vomiting increased
Migraines What is it? A severe painful headache with no cure Accompanied or preceded by sensory warning signs such as flashes of light blind spots, tingling in the arms and legs nausea vomiting increased
Painless, progressive weakness Could this be Motor Neurone Disease?
 APPENDIX 1 Painless, progressive weakness Could this be Motor Neurone Disease? 1. Does the patient have one or more of these? Bulbar features Limb features Respiratory features Cognitive features (rare)
APPENDIX 1 Painless, progressive weakness Could this be Motor Neurone Disease? 1. Does the patient have one or more of these? Bulbar features Limb features Respiratory features Cognitive features (rare)
Preventive treatment of migraine. Rebecca Burch, MD Brigham and Women s Faulkner Hospital Harvard Medical School Boston, MA
 Preventive treatment of migraine Rebecca Burch, MD Brigham and Women s Faulkner Hospital Harvard Medical School Boston, MA No disclosures Disclosures Many preventive treatments for migraine are not FDA-approved
Preventive treatment of migraine Rebecca Burch, MD Brigham and Women s Faulkner Hospital Harvard Medical School Boston, MA No disclosures Disclosures Many preventive treatments for migraine are not FDA-approved
Headache Why headaches hurt When to see a doctor Diagnosing your headache
 Headache Why headaches hurt Information about touch, pain, temperature, and vibration in the head and neck is sent to the brain by the trigeminal nerve, one of 12 pairs of cranial nerves that start at
Headache Why headaches hurt Information about touch, pain, temperature, and vibration in the head and neck is sent to the brain by the trigeminal nerve, one of 12 pairs of cranial nerves that start at
CHRONIC HEADACHES IN CHILDHOOD
 CHRONIC HEADACHES IN CHILDHOOD EDWIN LIU, MD PEDIATRIC NEUROLOGISTS OF PALM BEACH PEDIATRIC SLEEP CENTERS OF FLORIDA ASSISTANT CLINICAL PROFESSOR FSU ASSISTANT CLINICAL PROFESSOR NOVA SOUTHEASTERN PEDIATRIC
CHRONIC HEADACHES IN CHILDHOOD EDWIN LIU, MD PEDIATRIC NEUROLOGISTS OF PALM BEACH PEDIATRIC SLEEP CENTERS OF FLORIDA ASSISTANT CLINICAL PROFESSOR FSU ASSISTANT CLINICAL PROFESSOR NOVA SOUTHEASTERN PEDIATRIC
Headache Master School Japan-Osaka 2016 (HMSJ-Osaka2016) October 23, II. Management of Refractory Headaches
 October 23, II. Management of Refractory Headaches") Headache Master School Japan-Osaka 2016 (HMSJ-Osaka2016) October 23, 2016 II. Management of Refractory Headaches Case presentation 1: A case of intractable daily-persistent headache Keio University School
Headache Master School Japan-Osaka 2016 (HMSJ-Osaka2016) October 23, 2016 II. Management of Refractory Headaches Case presentation 1: A case of intractable daily-persistent headache Keio University School
Managing Headache in Acute Medicine. Ben Lovell Consultant Physician in Acute Medicine University College London Hospital
 Managing Headache in Acute Medicine Ben Lovell Consultant Physician in Acute Medicine University College London Hospital Some ED headache stats Arrive by ambulance 31% Median age 39 Worst ever headache
Managing Headache in Acute Medicine Ben Lovell Consultant Physician in Acute Medicine University College London Hospital Some ED headache stats Arrive by ambulance 31% Median age 39 Worst ever headache
OH, MY ACHING HEAD! I HAVE NO DISCLOSURES OR CONFLICTS OF INTERESTS TO DECLARE MANAGING HEADACHE IN THE OUTPATIENT SETTING SECONDARY HEADACHES
 1 JUSTIN A. OSSMAN, MD CHATTANOOGA FAMILY MEDICINE UPDATE OH, MY ACHING HEAD! MANAGING HEADACHE IN THE OUTPATIENT SETTING 2 I HAVE NO DISCLOSURES OR CONFLICTS OF INTERESTS TO DECLARE OBJECTIVES International
1 JUSTIN A. OSSMAN, MD CHATTANOOGA FAMILY MEDICINE UPDATE OH, MY ACHING HEAD! MANAGING HEADACHE IN THE OUTPATIENT SETTING 2 I HAVE NO DISCLOSURES OR CONFLICTS OF INTERESTS TO DECLARE OBJECTIVES International
Headaches in the Pediatric Emergency Dept
 Headaches in Children February 23, 2011 Jinny Tavee, MD Associate Professor Neuromuscular Center Cleveland Clinic Foundation Cleveland, OH 1 Headaches in the Pediatric Emergency Dept Burton Gutierrez Kan
Headaches in Children February 23, 2011 Jinny Tavee, MD Associate Professor Neuromuscular Center Cleveland Clinic Foundation Cleveland, OH 1 Headaches in the Pediatric Emergency Dept Burton Gutierrez Kan
Primary Care Adult Headache Management Pathway (formerly North West Headache Management Guideline for Adults) Version 1.0
 Version 1.0") Primary Care Adult Headache Management Pathway (formerly rth West Headache Management Guideline for Adults) Version 1.0 1 VERSION CONTROL Version Date Amendments made Version 1.0 October 2018 Reformatted
Primary Care Adult Headache Management Pathway (formerly rth West Headache Management Guideline for Adults) Version 1.0 1 VERSION CONTROL Version Date Amendments made Version 1.0 October 2018 Reformatted
COMBINATION THERAPIES PREVENTATIVE THERAPIES BETA BLOCKERS
 ACUTE THEAPIES TIPTANS TICYCLIC ANTIDEPESSANTS When starting acute treatment, healthcare professionals should warn patients about the risk of developing medication-overuse headache. ASPIIN Aspirin (900
ACUTE THEAPIES TIPTANS TICYCLIC ANTIDEPESSANTS When starting acute treatment, healthcare professionals should warn patients about the risk of developing medication-overuse headache. ASPIIN Aspirin (900
Disclosures. Triptans for Kids 5/16/13
 5/16/13 Disclosures Triptans for Kids Amy A. Gelfand, MD GelfandA@neuropeds.ucsf.edu Departments of Neurology and Pediatrics UCSF Child Neurology and Headache Center I receive grant funding from: NIH/NINDS
5/16/13 Disclosures Triptans for Kids Amy A. Gelfand, MD GelfandA@neuropeds.ucsf.edu Departments of Neurology and Pediatrics UCSF Child Neurology and Headache Center I receive grant funding from: NIH/NINDS
Headaches in Children and Adolescents. Paul Shillito
 Headaches in Children and Adolescents Paul Shillito Topics For Discussion What s different about childhood migraine Chronic daily headache (CDH) Tumours and other things to worry about Management of childhood
Headaches in Children and Adolescents Paul Shillito Topics For Discussion What s different about childhood migraine Chronic daily headache (CDH) Tumours and other things to worry about Management of childhood
MEASURE #4: Overuse of Barbiturate Containing Medications for Primary Headache Disorders Headache
 MEASURE #4: Overuse of Barbiturate Containing Medications for Primary Headache Disorders Headache Measure Description Percentage of patients age 18 years old and older with a diagnosis of primary headache
MEASURE #4: Overuse of Barbiturate Containing Medications for Primary Headache Disorders Headache Measure Description Percentage of patients age 18 years old and older with a diagnosis of primary headache
By Nathan Hall Associate Editor
 By Nathan Hall Associate Editor 34 Practical Neurology March 2005 These new rules may change the definition of head pain, but some practitioners may find the new guidelines themselves to be a source of
By Nathan Hall Associate Editor 34 Practical Neurology March 2005 These new rules may change the definition of head pain, but some practitioners may find the new guidelines themselves to be a source of
SIGN on the pharmacological management of migraine
 GUIDELINES SIGN on the pharmacological management of migraine STEVE CHAPLIN In February 2018, the Scottish Intercollegiate Guidelines Network (SIGN) published a new guideline on the pharmacological management
GUIDELINES SIGN on the pharmacological management of migraine STEVE CHAPLIN In February 2018, the Scottish Intercollegiate Guidelines Network (SIGN) published a new guideline on the pharmacological management
Migraine Clinical Guideline
 Migraine Clinical Guideline Definition: Migraine refers to a chronic neurological disorder characterized by episodic attacks often in association with enhanced sensitivity of the nervous system and activation
Migraine Clinical Guideline Definition: Migraine refers to a chronic neurological disorder characterized by episodic attacks often in association with enhanced sensitivity of the nervous system and activation
Headache is the most common symptom in patients with Idiopathic Intracranial Hypertension (IIH). Not everybody with IIH gets headache.
. Not everybody with IIH gets headache.") Headaches in Idiopathic Intracranial Hypertension Headache is the most common symptom in patients with Idiopathic Intracranial Hypertension (). Not everybody with gets headache. Headaches can be there
Headaches in Idiopathic Intracranial Hypertension Headache is the most common symptom in patients with Idiopathic Intracranial Hypertension (). Not everybody with gets headache. Headaches can be there
UCNS Course A Review of ICHD-3b
 UCNS Course A Review of ICHD-3b Andrew D. Hershey, M.D., Ph.D., FAHS Endowed Chair and Director of Neurology Director, Cincinnati Children s Headache Center Professor of Neurology and Pediatrics University
UCNS Course A Review of ICHD-3b Andrew D. Hershey, M.D., Ph.D., FAHS Endowed Chair and Director of Neurology Director, Cincinnati Children s Headache Center Professor of Neurology and Pediatrics University
6/4/2018. Headache. Headaches. Headache. Migraine Headaches. Headache. Red Flag signs and symptoms. Imaging CT without contrast.
 Presented by M.D. Shepherd, M.D. OH MY ACHING HEAD! Estimated that one half of the adult population is affected by a headache disorder International Society Classification Primary : Tension s 40% of the
Presented by M.D. Shepherd, M.D. OH MY ACHING HEAD! Estimated that one half of the adult population is affected by a headache disorder International Society Classification Primary : Tension s 40% of the
Headaches in Pregnancy Before, During, and After
 Headaches in Pregnancy Before, During, and After Robert Kaniecki, MD Director, UPMC Headache Center Assistant Professor of Neurology University of Pittsburgh Headaches and Pregnancy Pre-pregnancy counseling
Headaches in Pregnancy Before, During, and After Robert Kaniecki, MD Director, UPMC Headache Center Assistant Professor of Neurology University of Pittsburgh Headaches and Pregnancy Pre-pregnancy counseling
SUMAVEL DOSEPRO (sumatriptan succinate) solution for injection
 solution for injection") SUMAVEL DOSEPRO (sumatriptan succinate) solution for injection Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit
SUMAVEL DOSEPRO (sumatriptan succinate) solution for injection Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit
HEADACHE Transient discomfort, chronic nuisance, or looming disaster?
 HEADACHE Transient discomfort, chronic nuisance, or looming disaster? Hussien H. Rizk, MD Cairo University Medical School ١ Headache Second most common o symptom (after pain) Migraine alone afflicts 12
HEADACHE Transient discomfort, chronic nuisance, or looming disaster? Hussien H. Rizk, MD Cairo University Medical School ١ Headache Second most common o symptom (after pain) Migraine alone afflicts 12
HEADACHES AND MIGRAINES
 HEADACHES AND MIGRAINES CONTENT CREATED BY Learn more at www.health.harvard.edu TALK WITH YOUR DOCTOR Table of Contents Whether this is your first visit or a follow-up, answer these questions for your
HEADACHES AND MIGRAINES CONTENT CREATED BY Learn more at www.health.harvard.edu TALK WITH YOUR DOCTOR Table of Contents Whether this is your first visit or a follow-up, answer these questions for your
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 CGRP Page 1 of 8 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: CGRP (calcitonin gene-related peptide) Prime Therapeutics will review Prior Authorization requests
CGRP Page 1 of 8 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: CGRP (calcitonin gene-related peptide) Prime Therapeutics will review Prior Authorization requests
Tutorials. By Dr Sharon Truter
 Tutorials By Dr Sharon Truter To the Tutorials By Dr Sharon Truter What to expect from the Tutorials What to expect from these tutorials Outlines, structure, guided reading, explanations, mnemonics Begin
Tutorials By Dr Sharon Truter To the Tutorials By Dr Sharon Truter What to expect from the Tutorials What to expect from these tutorials Outlines, structure, guided reading, explanations, mnemonics Begin
ACUTE TREATMENT FOR MIGRAINE. Cristina Tassorelli
 The European Headache School 2012 ACUTE TREATMENT FOR MIGRAINE Cristina Tassorelli Headache Science Centre, IRCCS Neurological Institute C. Mondino Foundation - Pavia University Centre for Adaptive Disorders
The European Headache School 2012 ACUTE TREATMENT FOR MIGRAINE Cristina Tassorelli Headache Science Centre, IRCCS Neurological Institute C. Mondino Foundation - Pavia University Centre for Adaptive Disorders
Sumatriptan Injection (Imitrex / Alsuma / Sumavel / Zembrace)
") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.11 Subject: Sumatriptan Injection Page: 1 of 6 Last Review Date: March 16, 2018 Sumatriptan Injection
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.11 Subject: Sumatriptan Injection Page: 1 of 6 Last Review Date: March 16, 2018 Sumatriptan Injection
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 CGRP Page 1 of 13 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: CGRP (calcitonin gene-related peptide) Prime Therapeutics will review Prior Authorization requests
CGRP Page 1 of 13 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: CGRP (calcitonin gene-related peptide) Prime Therapeutics will review Prior Authorization requests
HEADACHE P of o. G. G Z u Z l u iani
 HEADACHE Prof. G. Zuliani General Statistics Everyone has headaches (HA) Second most common complain after back pain in the population More than 80 million Emergency Room visits in USA per year Frequency
HEADACHE Prof. G. Zuliani General Statistics Everyone has headaches (HA) Second most common complain after back pain in the population More than 80 million Emergency Room visits in USA per year Frequency
Subject: CGRP Inhibitors
 ARCHIVED (NOT ACTIVE RETIRED) Archived: 08/01/18 09-J2000-98 Original Effective Date: 06/15/18 Reviewed: 05/09/18 Revised: 08/01/18 Next Review: ARCHIVED (NOT ACTIVE RETIRED) Subject: CGRP Inhibitors THIS
ARCHIVED (NOT ACTIVE RETIRED) Archived: 08/01/18 09-J2000-98 Original Effective Date: 06/15/18 Reviewed: 05/09/18 Revised: 08/01/18 Next Review: ARCHIVED (NOT ACTIVE RETIRED) Subject: CGRP Inhibitors THIS
HEADACHE 1 Pablo Lapuerta, M.D., and Steven Asch, M.D., M.P.H.
 - 253-13. HEADACHE 1 Pablo Lapuerta, M.D., and Steven Asch, M.D., M.P.H. We identified articles on the evaluation and management of headache by conducting a MEDLINE search of English language articles
- 253-13. HEADACHE 1 Pablo Lapuerta, M.D., and Steven Asch, M.D., M.P.H. We identified articles on the evaluation and management of headache by conducting a MEDLINE search of English language articles
ACUTE MIGRAINE: OLD AND NEW DRUGS JOHN ROBROCK MD FORT WILLIAM FAMILY HEALTH TEAM
 ACUTE MIGRAINE: OLD AND NEW DRUGS JOHN ROBROCK MD FORT WILLIAM FAMILY HEALTH TEAM Conflict of Interest Declaration: Nothing to Disclose Presenter: John Robrock, MD Title of Presentation: Acute Migraine:
ACUTE MIGRAINE: OLD AND NEW DRUGS JOHN ROBROCK MD FORT WILLIAM FAMILY HEALTH TEAM Conflict of Interest Declaration: Nothing to Disclose Presenter: John Robrock, MD Title of Presentation: Acute Migraine:
Pearls in Child Neurology. Edgard Andrade, MD, FAAP Assistant Professor University of Florida
 Pearls in Child Neurology Edgard Andrade, MD, FAAP Assistant Professor University of Florida Outline 1. Autism 2. Bell s Palsy 3. First unprovoked seizure in children 4. Migraine headache Objectives 1.
Pearls in Child Neurology Edgard Andrade, MD, FAAP Assistant Professor University of Florida Outline 1. Autism 2. Bell s Palsy 3. First unprovoked seizure in children 4. Migraine headache Objectives 1.
MIGRAINE ASSOCIATION OF IRELAND
 MIGRAINE ASSOCIATION OF IRELAND HEADACHE IN MEN: THE FACTS This leaflet was composed by Paolo Rossi M.D., Ph.D. of the European Headache Alliance to mark European Migraine Day of Action 2014. Why a leaflet
MIGRAINE ASSOCIATION OF IRELAND HEADACHE IN MEN: THE FACTS This leaflet was composed by Paolo Rossi M.D., Ph.D. of the European Headache Alliance to mark European Migraine Day of Action 2014. Why a leaflet
Measure Components Numerator Statement
 MEASURE #5: OVERUSE OF OPIOID CONTAINING MEDICATIONS FOR PRIMARY HEADACHE DISORDERS Headache For Quality Improvement Only. Not to be used for Public Reporting or Accountability Measure Description Percentage
MEASURE #5: OVERUSE OF OPIOID CONTAINING MEDICATIONS FOR PRIMARY HEADACHE DISORDERS Headache For Quality Improvement Only. Not to be used for Public Reporting or Accountability Measure Description Percentage
Background. Background. Headache Examination. Headache History. Primary vs. Secondary Headaches. Headaches In Children: Why Worry?
 Background Headaches In Children: Why Worry? Marcy Yonker MD FAHS Associate Professor of Pediatrics University of Arizona Director, Pediatric Headache Program Phoenix Children s Hospital Headaches are
Background Headaches In Children: Why Worry? Marcy Yonker MD FAHS Associate Professor of Pediatrics University of Arizona Director, Pediatric Headache Program Phoenix Children s Hospital Headaches are
Headache A Practical Approach
 Headache A Practical Approach Integrated Pain Symposium December 1, 2017 Alyssa Lettich. MD Neurosciences Institute/Neurosciences Clinical Program Medical Director Headache and Pain Development Teams Disclosures:
Headache A Practical Approach Integrated Pain Symposium December 1, 2017 Alyssa Lettich. MD Neurosciences Institute/Neurosciences Clinical Program Medical Director Headache and Pain Development Teams Disclosures:
florida child neurology
 Headaches florida child neurology You re sitting at your desk, working on a difficult task, when it suddenly feels as if a belt or vice is being tightened around the top of your head. Or you have periodic
Headaches florida child neurology You re sitting at your desk, working on a difficult task, when it suddenly feels as if a belt or vice is being tightened around the top of your head. Or you have periodic