Sean Kelcey CCPA EM PA Selkirk Regional Health Center Selkirk, MB CAPA 2017
|
|
|
- Hollie Russell
- 5 years ago
- Views:
Transcription
1 Sean Kelcey CCPA EM PA Selkirk Regional Health Center Selkirk, MB CAPA 2017
2 I HAVE NO FINANCIAL DISCLOSURES TO MENTION AND DO NOT REPRESENT ANY DRUG DEALERS, LEGAL OR OTHERWISE ANY MENTION OF BRAND NAME AGENTS IS PURELY BY ACCIDENT OR BECAUSE THEY RE EASIER TO SAY GENERIC NAMES WILL ONLY BE SHOWN HERE IN TEXT FORM
3 CASE INTRODUCTIONS MIGRAINE TYPES TYPICALLY SEEN NON-SINISTER HEADACHES THAT MIMIC MIGRAINE SINISTER HEADACHES THAT MIMIC MIGRAINE PHARMACOLOGIC AGENTS USED IN TREATMENT OF ACUTE MIGRAINE CANADIAN AND US HEADACHE SOCIETY GUIDELINES SEAN S MIGRAINE APPROACH AND COCKTAILS CASE RESOLUTIONS
4 MIGRAINE AFFECTS ~ 4 MILLION PEOPLE IN CANADA ~25% OF CANADIAN WOMEN AND ~7-10% OF CANDIAN MEN ARE THOUGHT TO BE AFFECTED A TOP 20 REASON FOR MEDICAL DISABILITY WORLDWIDE LOTS OF THEORIES NOT MANY ANSWERS, YET
5 EVER NOTICE HOW EVERY H/A IN THE ER IS A MIGRAINE? AND EVER NOTICE HOW MANY OF THESE HEADACHES CAUSE US MIGRAINES IN THE ER? EVER NOTICE MONDAYS SUCK?
6 35 YO F, H/A X 5/7 KNOWN MIGRAINEUR, Dx By FMD, 6/12 post-partum, otherwise healthy; H/A s started during pregnancy (+) Phono/photosensitivity, N/V; pain hemispheric to (L), pounding; visual disturbance prior - dancing lights Onset was insidious; usual abortive therapy not effective Denies N/T or focal loss of function, Fever/chills/ns/neck stiffness or sick contacts/bad habits/known triggers
7 I had a bad reaction to something they gave me last time LOOKS UNWELL; eyes covered, wants lights out
8 42 YO F, 2/52 Hx HA I have a migraine No formal Dx Migraine; generally healthy Pain is unilateral but changes side, squeezing /c scalp burning; some relief with NSAID s (+) phonosensitivity and some nausea; ^ personal stressors Denies fever/chills/ns/urti symptoms/vomiting/focal neuro symptoms/bad habits/aura Looks tired in a well lit room
9 26 YO F, H/A x 1/7 No known migraine Hx, healthy Pain is (L) scalp/eye with pain increasing /c turning head I get a shock when I do that ; insidious onset; little change with NSAID s (+) photo/phonosensitive, mild nausea; moves keeping head still Denies Fever/chills/ns/vomiting/focal neuro symptoms/aura Looks in pain in a well lit room, squinting but cooperative

10 A. At least 5 attacks fulfilling criteria B-D B. Headache attacks lasting 4-72 hours (untreated or unsuccessfully treated) C. Headache has at least two of the following characteristics: - unilateral location - pulsating quality - moderate or severe pain intensity - aggravation by or causing avoidance of routine physical activity (e.g., walking or climbing stairs)
11 D. during headache, at least one of the following is present: - nausea and / or vomiting - photophobia and phonophobia E. not attributed to another disorder
12 A. At least 2 attacks fulfilling criteria B-D B. Aura consisting of at least one of the following, but no motor weakness: 1. fully reversible visual symptoms including positive features (e.g., flickering lights, spots or lines) and/or negative features (i.e., loss of vision) 2. fully reversible sensory symptoms including positive features (i.e., pins and needles) and/or negative features (i.e., numbness) 3. fully reversible dysphasic speech disturbance
13 C. At least two of the following: 1. homonymous visual symptoms and/or unilateral sensory symptoms 2. at least one aura symptom develops gradually over 5 minutes and/or different aura symptoms occur in succession over 5 minutes 3. each symptom lasts 5 and 60 minutes
14 D. Headache fulfilling criteria B-D for Migraine without aura begins during the aura or follows aura within 60 minutes E. not attributed to another disorder
15 Migraine lasting > 72 hours, despite or without treatment
16 NON SINISTER MIMICS CLUSTER HEADACHES SINUSITIS TENSION HEADACHE DRUG OVERUSE HEADACHE OCCIPITAL NEURALGIA SINISTER MIMICS SAH MENINGITIS/ENCEPHALITIS STROKE/TIA GCA
17 WHILE NOT TRUE MIGRAINE, ARE DEBILITATITING AND DO PRESENT TO ER AND SOMETIMES RESPOND TO TYPICAL MIGRAINE MEDS CRITERIA FOR CLUSTER H/A: FREQUENT (up to 8/day) BRIEF (<3hours) RECURRENT (Days/weeks at a time, then stop) UNILATERAL
18 CONJUCTIVAL INJECTION/TEARING/FACIAL SWELLING TO IPSILATERAL SIDE MALE>FEMALE ~4:1 (women do get them though don t ignore)
19 HEADACHE CAN BE UNILATERAL OVER AFFECTED SINUS OR BILATERAL OVER AFFECTED SINUSES CAN BE AT THE VERTEX (sphenoidal sinuses) ASSOCIATED WITH PHOTOPHOBIA, SOMETIMES FEVER, USUALLY URTI/ALLERGIC RHINITIS SYMPTOMS SINUSES USUALLY TENDER; IF MAXILLARY, OFTEN ASSOCIATED WITH DENTAL PAIN
20 USUALLY DON T MEET CRITERIA FOR MIGRAINE TYPICALLY ARE: BILATERAL, SQUEEZING, WITH MILD TO MODERATE INTENSITY NON-PULSATING NOT WORSENED BY ACTIVITY USUALLY NON-NAUSEATING
21 Often seen in migraine patients, undiagnosed migraine patients or patients with tension H/A s that are using primary meds at least 15 days a month Some chronic migraineurs are on the wrong abortive meds and haven t discussed changing with their PCP Some patients have an underlying dyscopia chronic pain, depression, PD, etc
22 Common offenders are triptans, NSAID s, ASA/APAP preps, especially those with caffeine, and opiods. These people need a withdrawal strategy, with a frank discussion regarding expectations of pain management They also need to try a new abortive med new triptan, DHE or alternative with an adjunct until the H/A s lessen in frequency, as well as exercise, stress management and management of underlying D/O
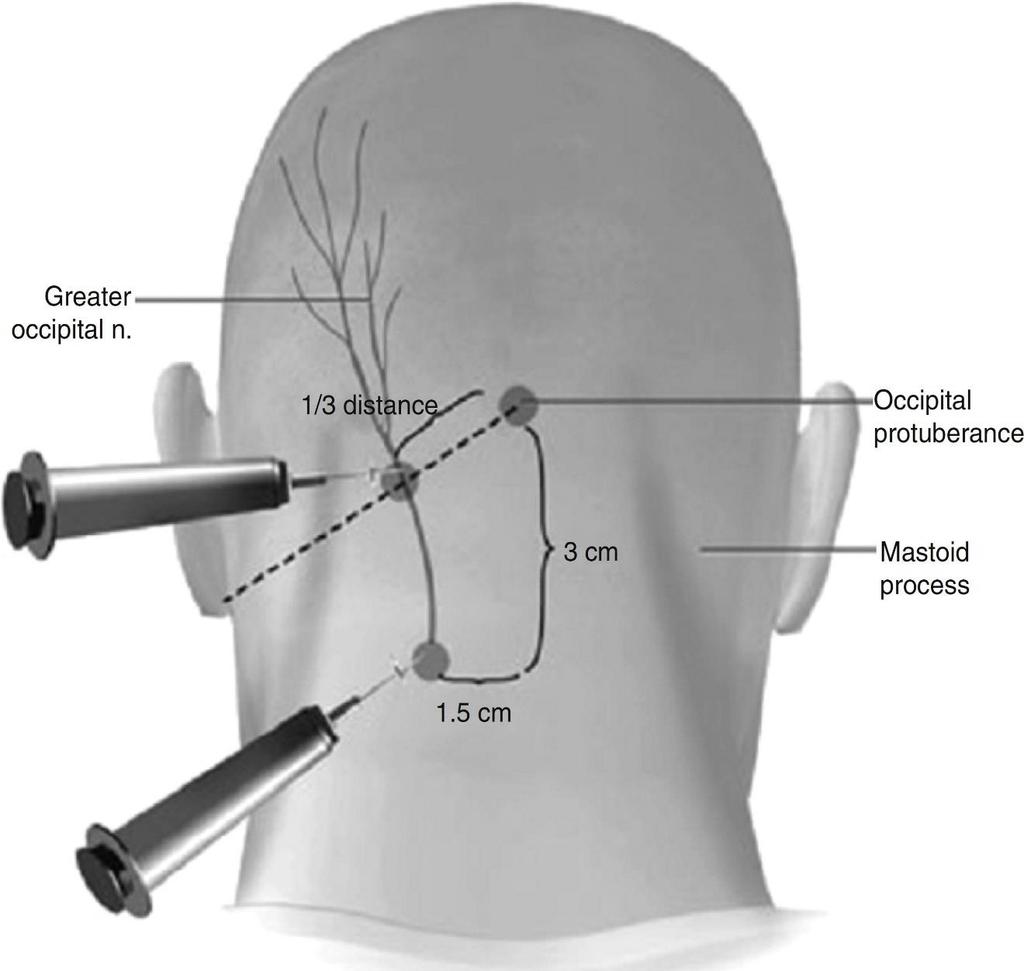
23 A TYPE OF HEADACHE THAT CAN OFTEN BE SEEN WITH MIGRAINE OR AS STAND ALONE POOR UNDERSTANDING OF MECHANISM OFTEN ASSOCIATED WITH TENSION/SPASM OF TRAPS/PARACERVICAL MUSCLES PAIN CAN BE UNILATERAL OR BILATERAL, BURNING/STABBING IN QUALITY, INCREASING WITH MOVEMENT, OFTEN AN ELECTRIC SHOCK SENSATION
24 TENDERNESS ALONG GREATER/LESSER OCCIPITAL NERVE DISTRIBUTION SOME PEOPLE EXHIBIT PHOTOSENSITIVITY AND NAUSEA CAN BE TREATED WITH CONSERVATIVE MEASURES, PHYSIO +/- A NERVE BLOCK /C OR /S STEROIDS
25
26 ONE OF THOSE CAN T MISS H/A S ACCOUNT FOR LESS THAN 1% OF ER VISITS BUT MISSED ONES ARE A LEADING CAUSE OF ACTIVATION OF MALPRACTICE COVERAGE DON T GET SUCKERED BY A MIGRAINEUR WITH HEADACHE IF IT S A CHANGE IN PATTERN, ESPECIALLY ABRUPT ONSET AND AURA MIMICS IN FORM OF FOCAL NEURO SYMPTOMS
27 HEADACHES THAT ARE ABRUPT, THUNDERCLAP OR ABSOLUTE WORST HEADACHE OF MY LIFE (ESPECIALLY IN A MIGRAINEUR), SUSPECT SAH S&S CAN MIMIC MIGRAINE WITH AURA, ALONG WITH SORE/STIFF NECK, DECREASING LOC, OTHER FOCAL NEURO SYMPTOMS MAY HAVE HX OF TRAUMA, HTN, SMOKING, AVM, OR ON ANTICOAGULANTS
28 IF YOU EVEN REMOTELY SUSPECT IT, CT THE HEAD!!!!!!!!!
29 ANOTHER CAUSE OF ACTIVATION OF MALPRACTICE INSURANCE USUALLY PRESENT WITH PRODROMAL SYMPTOMS FEVER, MYALGIA, ANTECEDENT URTI, POSSIBLE EPIDEMIC EXPOSURE CAN MIMIC MIGRAINE /C OR /S AURA; OFTEN HAVE STIFF NECK ASSOCIATED, BOTH TO ACTIVE/PASSIVE MOVEMENT REMEMBER FORMAL BRUDZYNSKI AND KERNIG SIGNS ARE ONLY (+) 50% ISH
30 IF YOU RE CONCERNED, ORDER LABS, CT/LP AND TREAT EMPIRICALY FOR WHAT YOU RE SUSPECTING
31 ODDLY ENOUGH, CAN MIMIC MIGRAINE WITH AURA AND VICE VERSA KEY IS AURA ON/OFF TIMINGS IF PATIENT PRESENTS LIKE MIGRAINE WITH AURA, BUT HAS NO PREVIOUS HX, ASSUME STROKE UNTIL PROVEN OTHEWISE IF MIGRAINEUR PRESENTING WITH ATYPICAL H/A FOR THEMSELVES, ACTIVATE STROKE PROTOCOL
32 IF MISSED, CAN RESULT IN VISION LOSS KEY POINTS USUALLY AN OLDER PERSON (>60 YO) PAIN IS ASSOCIATED WITH JAW CLAUDICATION, USUALLY NO N/V PATIENTS OFTEN HAVE COMORBID PMR PROXIMAL MUSCLE PAIN/WEAKNESS
33 TRIPTANS : SELECTIVE SEROTONIN 5-HT1B/D AGONISTS MOST RECOMMENDATIONS ARE FOR SC SUMITRIPTAN 6MG, RIZATRITPAN 10MG WAFER OR ZOLMATRIPTAN 5MG I/N SPRAY (MORE STUDIES VS SUMITRIPTAN 20MG I/N) UP TO 2 DOSES IN 24HRS FOR MOST OF THESE DRUGS
34 DOPAMINERGICS MOST RECCOMENDED/STUDIED ARE PROCHLORPERAZINE 10-20MG IV OR METOCLOPRAMIDE 10-20MG IV CAN BE USED IN COMBINATION OR AS STAND ALONE METOCLOPRAMIDE HAS ADDED BENEFIT OF ACTING ON 5-HT RECEPTORS
35 ERGOT DERIVATIVES DIHYDROERGOTAMINE (DHE45) CAN BE USED I/N (2MG), SC/IM/IV 1MG POTENT VASOACTIVE AGENT; PREG TEST ALL FEMALE PATIENTS IF CONSIDERING AGENT SHOWN GOOD RESULTS IN LONG TERM RELIEF
36 NSAID S CAN USE PO MEDS IF NOT VOMITING BEST STUDIED ARE NAPROXEN, IBUPROFEN AND ASA; DICLOFENAC SHOWED POOR RESULTS IN STUDIES HOWEVER, IN THE ER, MOST PATIENTS AREN T WILLING TO TRY PO INJECTABLE KETOROLAC IS AVAILABLE IN MOST ER S
37 OXYGEN EFFECTIVE FOR USE IN CLUSTER HEADACHES, HIGH FLOW (12-15LPM) FOR ~15 MINUTES STEROIDS EFFECTIVE FOR PREVENTING RELAPSE OR FOR CONCOMITANT USE WITH OCCIPITAL NERVE BLOCKS; NOT FOR ACUTE H/A
38 LOCAL ANAESTHETICS USUALLY USED FOR OCCIPITAL NERVE BLOCKS COMBO LIDO/BUPIVICAINE +/- STEROID CAN ALSO BE USED IN TRIGGER POINT INJECTIONS FOR PROLONGED TENSION/DRUG OVER USE H/A SMALL STUDIES FOR I/N LIDOCAINE, POOR EVIDENCE
39 CANADIAN AND US GUIDELINES ARE PRETTY SIMILAR BOTH SUGGEST TRIPTANS AS FIRST LINE AGENTS FOR ACUTE ABORTIVE THERAPY IF AVAILABLE AND WITHIN DOSING TIMELINES BOTH ALSO SUGGEST DOPAMINERGIC ANTI-NAUSEANT AGENTS +/- AN NSAID DHE IS ALSO RECOMMENDED AS AN AGENT OF CHOICE
40 ALL UNIVERSALLY RECOMMEND AGAINST OPIOIDS AS FIRST LINE AGENTS STEROIDS ARE RECOMMENDED ONLY TO PREVENT RECURRENCE, NOT AS ACUTE THERAPY SUGGEST H/A DIARY IF NEW PATIENT OR IF TRIGGERS STILL NOT KNOWN, DISCUSS SELF CARE, DRUG OVER USE, ETC WHEN D/C
41 EYEBALL THE PATIENT AND GET A QUICK, TARGETED HX, INCLUDING MEDS USED RAPID NEURO ASSESSMENT INCLUDING TRYING TO GET A LOOK AT THEIR FUNDI AND CHECK THEIR NECK AND LISTEN FOR BRUITS GET IV ACCESS IF NOT ALREADY THERE, GIVE SOME FLUID AND DECIDE ON ABORTIVE THERAPY

42 ONCE H/A IS SETTLING, DO A CLOSER EXAM, ESPECIALLY THE FUNDI ALWAYS HAVE A BACK UP PLAN IN PLACE WITH SECONDARY/TERTIARY MEDS
43 COCKTAIL #1=> 1OOOcc N/S or R/L + ketorolac 15mg/metoclopramide 10mg/diphenhydramine 25mg IV COCKTAIL #2=> see #1, replace metoclopramide with prochlorperazine COCKTAIL #3=> Sumatriptan 6mg sc (if available); may add fluid/ketorolac/antinauseant/diphenhydramine prn
44 COCKTAIL #4=> More fluid, DHE 1mg im/iv, dexamethasone 10mg iv (status migrainosus cocktail or non-responder) Offer occipital nerve block(s) and/or trigger point injections if residual pain in the nerve distribution
45 DX=? STATUS MIGRAINOSUS TMT: MRS A TRIAL OF COCKTAIL #1; PARTIAL RESOLUTION RECEIVED #4 AND WAS PAIN FREE AFTER 4 HOURS AND D/C SAW THEM AGAIN 2/52 LATER, RECEIVED #1 + DEX, OCCIPTAL NERVE BLOCK; WAS GIVE Rx for CCB as a preventative
46 DX?: TENSION TYPE HEADACHE MISS B TMT: Ketorolac IV, trigger point injections/occipital nerve block, stretching exercises, stress management regimen. Returned a few days later requesting another nerve block to opposite side of head was much happier

47 DX?: OCCIPITAL NEURALGIA TMT: MISS C Initially received Cocktail #1, 2/10 change on pain scale observably improved with occipital nerve block with steroid. Discharged ~ 2hours post initial assessment.
48 QUESTIONS? QUERIES? RUDE COMMENTS?
49
Headache Mary D. Hughes, MD Neuroscience Associates
 Headache Mary D. Hughes, MD Neuroscience Associates Case 1 22 year old female presents with recurrent headaches. She has had headaches for the past 3 years. They start on the right side of her head and
Headache Mary D. Hughes, MD Neuroscience Associates Case 1 22 year old female presents with recurrent headaches. She has had headaches for the past 3 years. They start on the right side of her head and
Headache Master School Japan-Osaka 2016 (HMSJ-Osaka2016) October 23, II. Management of Refractory Headaches
 October 23, II. Management of Refractory Headaches") Headache Master School Japan-Osaka 2016 (HMSJ-Osaka2016) October 23, 2016 II. Management of Refractory Headaches Case presentation 1: A case of intractable daily-persistent headache Keio University School
Headache Master School Japan-Osaka 2016 (HMSJ-Osaka2016) October 23, 2016 II. Management of Refractory Headaches Case presentation 1: A case of intractable daily-persistent headache Keio University School
HEADACHE: Benign or Severe Dr Gobinda Chandra Roy
 HEADACHE: Benign or Severe Dr Gobinda Chandra Roy Associate Professor, Department of Medicine, Shaheed Suhrawardy Medical College and Hospital Outlines 1. Introduction 2. Classification of headache 3.
HEADACHE: Benign or Severe Dr Gobinda Chandra Roy Associate Professor, Department of Medicine, Shaheed Suhrawardy Medical College and Hospital Outlines 1. Introduction 2. Classification of headache 3.
MIGRAINE UPDATE. Objectives & Disclosures. Learn techniques used to diagnose headaches. Become familiar with medications used for headache treatment.
 MIGRAINE UPDATE Karen L. Bremer, MD November 16, 2018 Objectives & Disclosures Learn techniques used to diagnose headaches. Become familiar with medications used for headache treatment. Disclosure: I am
MIGRAINE UPDATE Karen L. Bremer, MD November 16, 2018 Objectives & Disclosures Learn techniques used to diagnose headaches. Become familiar with medications used for headache treatment. Disclosure: I am
Paediatric headaches. Dr Jaycen Cruickshank Director of Clinical Training Ballarat Health Services. Brevity, levity, repetition
 Paediatric headaches Dr Jaycen Cruickshank Director of Clinical Training Ballarat Health Services Brevity, levity, repetition Paediatric)headache?)! Headache!in!children!is!not!that!common.!The!question!is!which!headaches!do!I!
Paediatric headaches Dr Jaycen Cruickshank Director of Clinical Training Ballarat Health Services Brevity, levity, repetition Paediatric)headache?)! Headache!in!children!is!not!that!common.!The!question!is!which!headaches!do!I!
MIGRAINE A MYSTERY HEADACHE
 MIGRAINE A MYSTERY HEADACHE The migraine is a chronic neurological disease that is characterized by moderate to severe episodes of headache that is mostly associated with other central nervous system (CNS)
MIGRAINE A MYSTERY HEADACHE The migraine is a chronic neurological disease that is characterized by moderate to severe episodes of headache that is mostly associated with other central nervous system (CNS)
HEADACHE. Dr Nick Pendleton. September Headache
 HEADACHE Dr Nick Pendleton September 2017 Headache Tension Type Headache Cranial Nerve Examination Migraine Migraine Treatment Medication Overuse Headache Headache Red Flags Sinusitis Headache Raised ICP
HEADACHE Dr Nick Pendleton September 2017 Headache Tension Type Headache Cranial Nerve Examination Migraine Migraine Treatment Medication Overuse Headache Headache Red Flags Sinusitis Headache Raised ICP
They are updated regularly as new NICE guidance is published. To view the latest version of this NICE Pathway see:
 bring together everything NICE says on a topic in an interactive flowchart. are interactive and designed to be used online. They are updated regularly as new NICE guidance is published. To view the latest
bring together everything NICE says on a topic in an interactive flowchart. are interactive and designed to be used online. They are updated regularly as new NICE guidance is published. To view the latest
25/09/2018 HEADACHE. Dr Nick Pendleton
 HEADACHE Dr Nick Pendleton September 2018 1 Small Group Work Tension Type Headache Cranial Nerve Examination Migraine Migraine Treatment Medication Overuse Headache Headache Red Flags Sinusitis Headache
HEADACHE Dr Nick Pendleton September 2018 1 Small Group Work Tension Type Headache Cranial Nerve Examination Migraine Migraine Treatment Medication Overuse Headache Headache Red Flags Sinusitis Headache
How do we treat migraine? New SIGN Guidelines
 How do we treat migraine? New SIGN Guidelines Managing your migraine Migraine Trust, Edinburgh 2018 Callum Duncan Consultant Neurologist Aberdeen Royal Infirmary Chair SIGN Guideline 155 Premonitory Mood
How do we treat migraine? New SIGN Guidelines Managing your migraine Migraine Trust, Edinburgh 2018 Callum Duncan Consultant Neurologist Aberdeen Royal Infirmary Chair SIGN Guideline 155 Premonitory Mood
A case of a patient with chronic headache. Focus on Migraine. None related to the presentation Grants to conduct clinical trials from: Speaker bureau:
 Chronic Daily Headache Bassel F. Shneker, MD, MBA Associate Professor Vice Chair, OSU Neurology The Ohio State University Wexner Medical Center Financial Disclosures None related to the presentation Grants
Chronic Daily Headache Bassel F. Shneker, MD, MBA Associate Professor Vice Chair, OSU Neurology The Ohio State University Wexner Medical Center Financial Disclosures None related to the presentation Grants
Disclosures. Triptans for Kids 5/16/13
 5/16/13 Disclosures Triptans for Kids Amy A. Gelfand, MD GelfandA@neuropeds.ucsf.edu Departments of Neurology and Pediatrics UCSF Child Neurology and Headache Center I receive grant funding from: NIH/NINDS
5/16/13 Disclosures Triptans for Kids Amy A. Gelfand, MD GelfandA@neuropeds.ucsf.edu Departments of Neurology and Pediatrics UCSF Child Neurology and Headache Center I receive grant funding from: NIH/NINDS
Headache Classifica-on
 Headache Classifica-on 2 Tension-Type Headache Criteria -Infrequent episodic tension-type headache- A. At least 10 episodes occurring on < 1 day per month on average (< 12 days per year) and fulfilling
Headache Classifica-on 2 Tension-Type Headache Criteria -Infrequent episodic tension-type headache- A. At least 10 episodes occurring on < 1 day per month on average (< 12 days per year) and fulfilling
Can I send this headache patient home? Dr Nicola Giffin Consultant Neurologist Bath, Nov 2017
 Can I send this headache patient home? Dr Nicola Giffin Consultant Neurologist Bath, Nov 2017 SAH v benign thunderclap headaches Other pathologies not apparent on CT Severe primary headaches: management
Can I send this headache patient home? Dr Nicola Giffin Consultant Neurologist Bath, Nov 2017 SAH v benign thunderclap headaches Other pathologies not apparent on CT Severe primary headaches: management
PAEDIATRIC ACUTE CARE GUIDELINE. Headache. This document should be read in conjunction with this DISCLAIMER
 Princess Margaret Hospital for Children PAEDIATRIC ACUTE CARE GUIDELINE Scope (Staff): Scope (Area): All Emergency Department Clinicians Emergency Department This document should be read in conjunction
Princess Margaret Hospital for Children PAEDIATRIC ACUTE CARE GUIDELINE Scope (Staff): Scope (Area): All Emergency Department Clinicians Emergency Department This document should be read in conjunction
The best defense is a good offense. Optimizing the Acute Treatment of Migraine. Disclosures 11/10/2017
 Optimizing the Acute Treatment of Migraine Brian M. Plato, DO, FAHS Norton Neuroscience Institute Louisville, KY Disclosures Speakers Bureau (personal): Allergan, Depomed, Avanir Research Funding (paid
Optimizing the Acute Treatment of Migraine Brian M. Plato, DO, FAHS Norton Neuroscience Institute Louisville, KY Disclosures Speakers Bureau (personal): Allergan, Depomed, Avanir Research Funding (paid
Managing Headache in Acute Medicine. Ben Lovell Consultant Physician in Acute Medicine University College London Hospital
 Managing Headache in Acute Medicine Ben Lovell Consultant Physician in Acute Medicine University College London Hospital Some ED headache stats Arrive by ambulance 31% Median age 39 Worst ever headache
Managing Headache in Acute Medicine Ben Lovell Consultant Physician in Acute Medicine University College London Hospital Some ED headache stats Arrive by ambulance 31% Median age 39 Worst ever headache
Disclosures. Objectives 6/2/2017
 Classification: Migraine and Trigeminal Autonomic Cephalalgias Lauren Doyle Strauss, DO, FAHS Assistant Professor, Child Neurology Assistant Director, Child Neurology Residency @StraussHeadache No disclosures
Classification: Migraine and Trigeminal Autonomic Cephalalgias Lauren Doyle Strauss, DO, FAHS Assistant Professor, Child Neurology Assistant Director, Child Neurology Residency @StraussHeadache No disclosures
A synopsis of: Diagnosis and Management of Headaches in Adults: A national clinical guideline. Scottish intercollegiate Guidelines Network SIGN
 A synopsis of: Diagnosis and Management of Headaches in Adults: A national clinical guideline Scottish intercollegiate Guidelines Network SIGN November 2008. PETER FRAMPTON MSc MCOptom BAppSc (Optom)(AUS)
A synopsis of: Diagnosis and Management of Headaches in Adults: A national clinical guideline Scottish intercollegiate Guidelines Network SIGN November 2008. PETER FRAMPTON MSc MCOptom BAppSc (Optom)(AUS)
Faculty Disclosures. Learning Objectives. Acute Treatment Strategies
 WWW.AMERICANHEADACHESOCIETY.ORG Acute Treatment Strategies Content developed by: Lawrence C. Newman, MD, FAHS Donna Gutterman, PharmD Faculty Disclosures LAWRENCE C. NEWMAN, MD, FAHS Dr. Newman has received
WWW.AMERICANHEADACHESOCIETY.ORG Acute Treatment Strategies Content developed by: Lawrence C. Newman, MD, FAHS Donna Gutterman, PharmD Faculty Disclosures LAWRENCE C. NEWMAN, MD, FAHS Dr. Newman has received
Current Migraine Treatment Therapy. Daniel Kassicieh, DO, FAAN
 Current Migraine Treatment Therapy Daniel Kassicieh, DO, FAAN Migraine a Disease Process Migraines are a chronic disease process similar to many other chronic medical conditions Migraine has a low mortality
Current Migraine Treatment Therapy Daniel Kassicieh, DO, FAAN Migraine a Disease Process Migraines are a chronic disease process similar to many other chronic medical conditions Migraine has a low mortality
What A Headache! Theresa Biesiada March 8, 2012
 What A Headache! Theresa Biesiada March 8, 2012 Objectives Describe the EM relevance of headaches and migraines Discuss the rationale for steroid therapy Review the evidence Conclusions My inspiration
What A Headache! Theresa Biesiada March 8, 2012 Objectives Describe the EM relevance of headaches and migraines Discuss the rationale for steroid therapy Review the evidence Conclusions My inspiration
Faculty Disclosure. Karen L. Bremer, MD. Dr. Bremer has listed no financial interest/arrangement that would be considered a conflict of interest.
 Faculty Disclosure Karen L. Bremer, MD Dr. Bremer has listed no financial interest/arrangement that would be considered a conflict of interest. HEADACHE UPDATE Karen L. Bremer, MD November 10, 2017 karen.bremer@creighton.edu
Faculty Disclosure Karen L. Bremer, MD Dr. Bremer has listed no financial interest/arrangement that would be considered a conflict of interest. HEADACHE UPDATE Karen L. Bremer, MD November 10, 2017 karen.bremer@creighton.edu
Chronic Daily Headaches
 Chronic Daily Headaches ANWARUL HAQ, MD, MRCP(UK), FAHS DIRECTOR BAYLOR HEADACHE CENTER, DALLAS, TEXAS DISCLOSURES: None OBJECTIVES AT THE CONCLUSION OF THIS ACTIVITY, PARTICIPANTS WILL BE ABLE TO: define
Chronic Daily Headaches ANWARUL HAQ, MD, MRCP(UK), FAHS DIRECTOR BAYLOR HEADACHE CENTER, DALLAS, TEXAS DISCLOSURES: None OBJECTIVES AT THE CONCLUSION OF THIS ACTIVITY, PARTICIPANTS WILL BE ABLE TO: define
Adult with headache. Problem-specific video guides to diagnosing patients and helping them with management and prevention
 Adult with headache Problem-specific video guides to diagnosing patients and helping them with management and prevention London Strategic Clinical Networks London Neuroscience Strategic Clinical Network
Adult with headache Problem-specific video guides to diagnosing patients and helping them with management and prevention London Strategic Clinical Networks London Neuroscience Strategic Clinical Network
Chronic Migraine in Primary Care. December 11 th, 2017 Werner J. Becker University of Calgary
 Chronic Migraine in Primary Care December 11 th, 2017 Werner J. Becker University of Calgary Disclosures Faculty: Werner J. Becker Relationships with commercial interests: Grants/Research Support: Clinical
Chronic Migraine in Primary Care December 11 th, 2017 Werner J. Becker University of Calgary Disclosures Faculty: Werner J. Becker Relationships with commercial interests: Grants/Research Support: Clinical
Overview INTRODUCTION 3/15/2018. Headache Emergencies. Other way to differentiate between them? Is there an easy way to differentiate between them?
 Overview Headache Emergencies Primary versus Secondary headache disorder Red flags 4 cases of unusual headache emergencies Disclaimer: we will not talk about brain bleed as patients usually go the ED.
Overview Headache Emergencies Primary versus Secondary headache disorder Red flags 4 cases of unusual headache emergencies Disclaimer: we will not talk about brain bleed as patients usually go the ED.
Acute Migraine Treatment: What you and your family should know to help you make the best choices with your doctor
 Acute Migraine Treatment: What you and your family should know to help you make the best choices with your doctor TAKE CONTROL OF YOUR MIGRAINES! ABOUT THIS PATIENT GUIDE: Migraine attacks are often debilitating
Acute Migraine Treatment: What you and your family should know to help you make the best choices with your doctor TAKE CONTROL OF YOUR MIGRAINES! ABOUT THIS PATIENT GUIDE: Migraine attacks are often debilitating
Headache and Facial Pain. Mohammed ALEssa MBBS, FRCSC Assistant Professor Consultant Otolaryngology,Head & Neck Surgical Oncology
 Headache and Facial Pain Mohammed ALEssa MBBS, FRCSC Assistant Professor Consultant Otolaryngology,Head & Neck Surgical Oncology Introduction It is the most common neurologic complain The diagnosis usually
Headache and Facial Pain Mohammed ALEssa MBBS, FRCSC Assistant Professor Consultant Otolaryngology,Head & Neck Surgical Oncology Introduction It is the most common neurologic complain The diagnosis usually
HEADACHES THE RED FLAGS
 HEADACHES THE RED FLAGS FAYYAZ AHMED CONSULTANT NEUROLOGIST HON. SENIOR LECTURER HULL YORK MEDICAL SCHOOL SECONDARY VS PRIMARY HEADACHES COMMON SECONDARY HEADACHES UNCOMMON BUT SERIOUS SECONDARY HEADACHES
HEADACHES THE RED FLAGS FAYYAZ AHMED CONSULTANT NEUROLOGIST HON. SENIOR LECTURER HULL YORK MEDICAL SCHOOL SECONDARY VS PRIMARY HEADACHES COMMON SECONDARY HEADACHES UNCOMMON BUT SERIOUS SECONDARY HEADACHES
Neurological Dilemmas in Primary Care
 Neurological Dilemmas in Primary Care David Clark, DO dclark@oregonneurology.com When to test? How to test? Pitfalls in testing? When to treat? How to treat? How long to treat? Neurological Dilemmas Seizure
Neurological Dilemmas in Primary Care David Clark, DO dclark@oregonneurology.com When to test? How to test? Pitfalls in testing? When to treat? How to treat? How long to treat? Neurological Dilemmas Seizure
Headache Assessment In Primary Eye Care
 Headache Assessment In Primary Eye Care Spencer Johnson, O.D., F.A.A.O. Northeastern State University Oklahoma College of Optometry johns137@nsuok.edu Course Objectives Review headache classification Understand
Headache Assessment In Primary Eye Care Spencer Johnson, O.D., F.A.A.O. Northeastern State University Oklahoma College of Optometry johns137@nsuok.edu Course Objectives Review headache classification Understand
Jessica Ailani MD FAHS Director, Georgetown Headache Center Associate Professor Neurology Medstar Georgetown University Hospital
 Jessica Ailani MD FAHS Director, Georgetown Headache Center Associate Professor Neurology Medstar Georgetown University Hospital Honorarium from Current Pain and Headache Reports; Section Editor Unusual
Jessica Ailani MD FAHS Director, Georgetown Headache Center Associate Professor Neurology Medstar Georgetown University Hospital Honorarium from Current Pain and Headache Reports; Section Editor Unusual
6/4/2018. Headache. Headaches. Headache. Migraine Headaches. Headache. Red Flag signs and symptoms. Imaging CT without contrast.
 Presented by M.D. Shepherd, M.D. OH MY ACHING HEAD! Estimated that one half of the adult population is affected by a headache disorder International Society Classification Primary : Tension s 40% of the
Presented by M.D. Shepherd, M.D. OH MY ACHING HEAD! Estimated that one half of the adult population is affected by a headache disorder International Society Classification Primary : Tension s 40% of the
10/31/2017 PRIMARY CARE AND HEADACHE DISCLOSURES WHERE DO THOSE WITH HEADACHE SEEK MEDICAL CARE? Primary Care 67%
 PRIMARY CARE AND HEADACHE Sonja Potrebic MD PhD Regional Headache Specialist Kaiser LAMC 1 WHERE DO THOSE WITH HEADACHE SEEK MEDICAL CARE? Column1 Primary Care 67% Primary Care Headache Specialty Other
PRIMARY CARE AND HEADACHE Sonja Potrebic MD PhD Regional Headache Specialist Kaiser LAMC 1 WHERE DO THOSE WITH HEADACHE SEEK MEDICAL CARE? Column1 Primary Care 67% Primary Care Headache Specialty Other
Tears of Pain SUNCT and SUNA A/PROFESSOR ARUN AGGARWAL RPAH PAIN MANAGEMENT CENTRE
 Tears of Pain SUNCT and SUNA A/PROFESSOR ARUN AGGARWAL RPAH PAIN MANAGEMENT CENTRE IHS Classification 1989 (updated 2004) Primary Headaches 4 categories Migraine Tension-type Cluster and other trigeminal
Tears of Pain SUNCT and SUNA A/PROFESSOR ARUN AGGARWAL RPAH PAIN MANAGEMENT CENTRE IHS Classification 1989 (updated 2004) Primary Headaches 4 categories Migraine Tension-type Cluster and other trigeminal
MIGRAINE ASSOCIATION OF IRELAND
 MIGRAINE ASSOCIATION OF IRELAND HEADACHE IN MEN: THE FACTS This leaflet was composed by Paolo Rossi M.D., Ph.D. of the European Headache Alliance to mark European Migraine Day of Action 2014. Why a leaflet
MIGRAINE ASSOCIATION OF IRELAND HEADACHE IN MEN: THE FACTS This leaflet was composed by Paolo Rossi M.D., Ph.D. of the European Headache Alliance to mark European Migraine Day of Action 2014. Why a leaflet
Painless, progressive weakness Could this be Motor Neurone Disease?
 APPENDIX 1 Painless, progressive weakness Could this be Motor Neurone Disease? 1. Does the patient have one or more of these? Bulbar features Limb features Respiratory features Cognitive features (rare)
APPENDIX 1 Painless, progressive weakness Could this be Motor Neurone Disease? 1. Does the patient have one or more of these? Bulbar features Limb features Respiratory features Cognitive features (rare)
Headache. Section 1. Migraine headache. Clinical presentation
 Section 1 Headache Migraine headache 1 Clinical presentation It is important to recognize just how significant a problem migraine headache is. It has been estimated that migraine affects 11% of the United
Section 1 Headache Migraine headache 1 Clinical presentation It is important to recognize just how significant a problem migraine headache is. It has been estimated that migraine affects 11% of the United
Headache A Practical Approach
 Headache A Practical Approach Integrated Pain Symposium December 1, 2017 Alyssa Lettich. MD Neurosciences Institute/Neurosciences Clinical Program Medical Director Headache and Pain Development Teams Disclosures:
Headache A Practical Approach Integrated Pain Symposium December 1, 2017 Alyssa Lettich. MD Neurosciences Institute/Neurosciences Clinical Program Medical Director Headache and Pain Development Teams Disclosures:
National Hospital for Neurology and Neurosurgery. Migraine Associated Dizziness. Department of Neuro-otology
 National Hospital for Neurology and Neurosurgery Migraine Associated Dizziness Department of Neuro-otology If you would like this document in another language or format or if you require the services of
National Hospital for Neurology and Neurosurgery Migraine Associated Dizziness Department of Neuro-otology If you would like this document in another language or format or if you require the services of
Migraine Management. Jane Melling Headache nurse Mater Misericordiae Hospital
 Migraine Management Jane Melling Headache nurse Mater Misericordiae Hospital Migraine facts Among the most common disorders of the nervous system 3 rd most prevalent medical disorder on the planet (lancet
Migraine Management Jane Melling Headache nurse Mater Misericordiae Hospital Migraine facts Among the most common disorders of the nervous system 3 rd most prevalent medical disorder on the planet (lancet
Treatment of Headache in the ED
 Treatment of Headache in the ED Benjamin W. Friedman, MD, MS, FAAEM Associate professor of Emergency Medicine Albert Einstein College of Medicine Montefiore Medical Center Disclosure Topics of Discussion
Treatment of Headache in the ED Benjamin W. Friedman, MD, MS, FAAEM Associate professor of Emergency Medicine Albert Einstein College of Medicine Montefiore Medical Center Disclosure Topics of Discussion
Migraine: Past, Present and Future Edward O Sullivan September 12 th 2015 Dublin 12/09/2015
 1 Migraine: Past, Present and Future Edward O Sullivan September 12 th 2015 Dublin Tour de France 2015: Mark Renshaw Yesterday at the end of the stage 17 I came down with a migraine before the final climb
1 Migraine: Past, Present and Future Edward O Sullivan September 12 th 2015 Dublin Tour de France 2015: Mark Renshaw Yesterday at the end of the stage 17 I came down with a migraine before the final climb
I have no financial relationships to disclose. I will not discuss investigational use of medication in my presentation.
 I have no financial relationships to disclose. I will not discuss investigational use of medication in my presentation. In 1962, Bille published landmark epidemiologic survey of headache among 9,000 school
I have no financial relationships to disclose. I will not discuss investigational use of medication in my presentation. In 1962, Bille published landmark epidemiologic survey of headache among 9,000 school
I. Migraine management in the Emergency Department
 Comer Children s Hospital Pediatric Guidelines Guideline: Migraine management in the ED Guideline #: PED-06 Section: Neurology Page: 1 of 10 Developed date: 11/17/2016 Revision date: none Review date:
Comer Children s Hospital Pediatric Guidelines Guideline: Migraine management in the ED Guideline #: PED-06 Section: Neurology Page: 1 of 10 Developed date: 11/17/2016 Revision date: none Review date:
Headaches. Mini Medical School. November 10, A. Laine Green MSc, MD FRCP(C) Assistant Professor Department of Medicine (Neurology)
 Assistant Professor Department of Medicine (Neurology)") Headaches. Mini Medical School. November 10, 2016 A. Laine Green MSc, MD FRCP(C) Assistant Professor Department of Medicine (Neurology) Artist Agnes Cecile Disclosures I have received an honorarium from
Headaches. Mini Medical School. November 10, 2016 A. Laine Green MSc, MD FRCP(C) Assistant Professor Department of Medicine (Neurology) Artist Agnes Cecile Disclosures I have received an honorarium from
Strategies in Migraine Care
 Strategies in Migraine Care Julie L. Roth, MD Rhode Island Hospital Assistant Professor, Neurology The Warren Alpert Medical School of Brown University March 28, 2015 Financial Disclosures None. Objectives
Strategies in Migraine Care Julie L. Roth, MD Rhode Island Hospital Assistant Professor, Neurology The Warren Alpert Medical School of Brown University March 28, 2015 Financial Disclosures None. Objectives
Migraine. What are the symptoms of a migraine attack?
 Migraine Migraine causes attacks of headaches, often with feeling sick or vomiting. Treatment options include: avoiding possible 'triggers', painkillers, antiinflammatory painkillers, anti-sickness medicines,
Migraine Migraine causes attacks of headaches, often with feeling sick or vomiting. Treatment options include: avoiding possible 'triggers', painkillers, antiinflammatory painkillers, anti-sickness medicines,
Headaches in the Pediatric Emergency Dept
 Headaches in Children February 23, 2011 Jinny Tavee, MD Associate Professor Neuromuscular Center Cleveland Clinic Foundation Cleveland, OH 1 Headaches in the Pediatric Emergency Dept Burton Gutierrez Kan
Headaches in Children February 23, 2011 Jinny Tavee, MD Associate Professor Neuromuscular Center Cleveland Clinic Foundation Cleveland, OH 1 Headaches in the Pediatric Emergency Dept Burton Gutierrez Kan
1. On how many days in the last 3 months did you miss work or school because of your headaches?
 The Migraine Disability Assessment Test The MIDAS (Migraine Disability Assessment) questionnaire was put together to help you measure the impact your headaches have on your life. The information on this
The Migraine Disability Assessment Test The MIDAS (Migraine Disability Assessment) questionnaire was put together to help you measure the impact your headaches have on your life. The information on this
Outpatient Headache Care Guideline
 1 Outpatient Care Guideline Inclusion criteria: children > 3 yrs with headaches Is urgent emergency department, neuroimaging, or Neurology consultation indicated? Referral to ED if: New severe headache
1 Outpatient Care Guideline Inclusion criteria: children > 3 yrs with headaches Is urgent emergency department, neuroimaging, or Neurology consultation indicated? Referral to ED if: New severe headache
11/10/2017. THE BRIDGE Course Objectives. THE BRIDGE Course Objectives
 THE BRIDGE Course Objectives Describe clinical characteristics associated with migraine diagnosis in adult and pediatric populations. Identify barriers and risk factors impacting the clinical course of
THE BRIDGE Course Objectives Describe clinical characteristics associated with migraine diagnosis in adult and pediatric populations. Identify barriers and risk factors impacting the clinical course of
OH, MY ACHING HEAD! I HAVE NO DISCLOSURES OR CONFLICTS OF INTERESTS TO DECLARE MANAGING HEADACHE IN THE OUTPATIENT SETTING SECONDARY HEADACHES
 1 JUSTIN A. OSSMAN, MD CHATTANOOGA FAMILY MEDICINE UPDATE OH, MY ACHING HEAD! MANAGING HEADACHE IN THE OUTPATIENT SETTING 2 I HAVE NO DISCLOSURES OR CONFLICTS OF INTERESTS TO DECLARE OBJECTIVES International
1 JUSTIN A. OSSMAN, MD CHATTANOOGA FAMILY MEDICINE UPDATE OH, MY ACHING HEAD! MANAGING HEADACHE IN THE OUTPATIENT SETTING 2 I HAVE NO DISCLOSURES OR CONFLICTS OF INTERESTS TO DECLARE OBJECTIVES International
ONZETRA XSAIL (sumatriptan) nasal powder
 nasal powder") ONZETRA XSAIL (sumatriptan) nasal powder Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy
ONZETRA XSAIL (sumatriptan) nasal powder Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy
What Do You Think of My Posterior?
 What Do You Think of My Posterior? Posterior Stroke and Stroke Mimics Peter Panagos, MD, FACEP, FAHA Associate Professor Emergency Medicine and Neurology Washington University School of Medicine Disclosures
What Do You Think of My Posterior? Posterior Stroke and Stroke Mimics Peter Panagos, MD, FACEP, FAHA Associate Professor Emergency Medicine and Neurology Washington University School of Medicine Disclosures
10/17/2017 CHRONIC MIGRAINES BOTOX: TO INJECT OR NOT INJECT? IN CHRONIC MIGRAINE PROPHYLAXIS OBJECTIVES PATIENT CASE EPIDEMIOLOGY EPIDEMIOLOGY
 BOTOX: TO INJECT OR NOT INJECT? IN CHRONIC MIGRAINE PROPHYLAXIS OBJECTIVES JENNIFER SHIN, PHARMD PGY2 AMBULATORY CARE PHARMACY RESIDENT COMMUNITYCARE HEALTH CENTERS PHARMACOTHERAPY ROUNDS OCTOBER 20, 2017
BOTOX: TO INJECT OR NOT INJECT? IN CHRONIC MIGRAINE PROPHYLAXIS OBJECTIVES JENNIFER SHIN, PHARMD PGY2 AMBULATORY CARE PHARMACY RESIDENT COMMUNITYCARE HEALTH CENTERS PHARMACOTHERAPY ROUNDS OCTOBER 20, 2017
Do you suffer from Headaches? - November/Dec 2011
 Do you suffer from Headaches? - November/Dec 2011 Inside this month's issue Headaches Acute single headaches Recurring Headaches: Migraine What causes Migraine? Treatments for migraine & prevention Headaches
Do you suffer from Headaches? - November/Dec 2011 Inside this month's issue Headaches Acute single headaches Recurring Headaches: Migraine What causes Migraine? Treatments for migraine & prevention Headaches
Lynda J. Krasenbaum, MSN, ANP BC. Associate Director New York Headache Center
 Diagnosing Headache in Adults and Adolescents Lynda J. Krasenbaum, MSN, ANP BC Associate Director New York Headache Center New York, New York Learning Objectives Understand the diagnostic challenges of
Diagnosing Headache in Adults and Adolescents Lynda J. Krasenbaum, MSN, ANP BC Associate Director New York Headache Center New York, New York Learning Objectives Understand the diagnostic challenges of
Adult & Pediatric Patients. Stanford Health Care, Division Pain Medicine
 Acute Treatment Strategies in Adult & Pediatric Patients Theresa Mallick Searle, MS, RN BC, ANP BC Disclosures Speakers Bureau: Allergan, Depomed Acute Treatment Strategies in Adult & Pediatric Patients
Acute Treatment Strategies in Adult & Pediatric Patients Theresa Mallick Searle, MS, RN BC, ANP BC Disclosures Speakers Bureau: Allergan, Depomed Acute Treatment Strategies in Adult & Pediatric Patients
HEADACHE. Summary of British Association on the Study of Headaches {click to visit}
 F:M=3:1 Affects 15% adults HEADACHE Summary of British Association on the Study of Headaches {click to visit} Primary: Migraine (with aura 1/3, without aura 2/3) Tension Cluster Other Secondary Neuralgia
F:M=3:1 Affects 15% adults HEADACHE Summary of British Association on the Study of Headaches {click to visit} Primary: Migraine (with aura 1/3, without aura 2/3) Tension Cluster Other Secondary Neuralgia
What You Should Know About Your HEADACHE. Learn more about headache types, triggers, and treatments, when to get help, and how to help yourself
 What You Should Know About Your HEADACHE Learn more about headache types, triggers, and treatments, when to get help, and how to help yourself Introduction The purpose of this brochure is to give you a
What You Should Know About Your HEADACHE Learn more about headache types, triggers, and treatments, when to get help, and how to help yourself Introduction The purpose of this brochure is to give you a
Risk Factors, Clinical Course, and Barriers to Care in Adults and Pediatrics. Rebecca R. Buttaccio, PA-C Dent Neurologic Institute
 Risk Factors, Clinical Course, and Barriers to Care in Adults and Pediatrics Rebecca R. Buttaccio, PA-C Dent Neurologic Institute Speaker for Avanir Disclosures Learning Objectives 1. Review the risk factors
Risk Factors, Clinical Course, and Barriers to Care in Adults and Pediatrics Rebecca R. Buttaccio, PA-C Dent Neurologic Institute Speaker for Avanir Disclosures Learning Objectives 1. Review the risk factors
Update on Diagnosis and Management of Migraines
 Update on Diagnosis and Management of Migraines Joel J. Heidelbaugh, MD, FAAFP, FACG Clinical Professor Departments of Family Medicine and Urology University of Michigan Learning Objectives To distinguish
Update on Diagnosis and Management of Migraines Joel J. Heidelbaugh, MD, FAAFP, FACG Clinical Professor Departments of Family Medicine and Urology University of Michigan Learning Objectives To distinguish
Headache Management in Primary Care Dr Niranjanan Nirmalananthan Consultant Neurologist
 Headache Management in Primary Care Dr Niranjanan Nirmalananthan Consultant Neurologist Wednesday 10 th of April 2019 Summary Why does it matter? Classification and diagnosis Who to refer / scan? Serious
Headache Management in Primary Care Dr Niranjanan Nirmalananthan Consultant Neurologist Wednesday 10 th of April 2019 Summary Why does it matter? Classification and diagnosis Who to refer / scan? Serious
Daniel Kassicieh, DO, FAAN
 Daniel Kassicieh, DO, FAAN Migraine a Disease Process Migraine is a chronic disease process similar to many other chronic medical conditions Migraine has a low mortality but high morbidity 38 million Americans
Daniel Kassicieh, DO, FAAN Migraine a Disease Process Migraine is a chronic disease process similar to many other chronic medical conditions Migraine has a low mortality but high morbidity 38 million Americans
SUMAVEL DOSEPRO (sumatriptan succinate) solution for injection
 solution for injection") SUMAVEL DOSEPRO (sumatriptan succinate) solution for injection Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit
SUMAVEL DOSEPRO (sumatriptan succinate) solution for injection Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit
Study No.: Title: Rationale: Phase: Study Period: Study Design: Centers: Indication: Treatment: Objectives: Primary Outcome/Efficacy Variable:
 The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
Clinical Learning Days November 10, 2017
 Migraine Clinical Learning Days November 10, 2017 Alyssa Lettich. MD Neurosciences Institute/Neurosciences Clinical Program Medical Director Headache Disclosures: none Learning Objectives: At the conclusion
Migraine Clinical Learning Days November 10, 2017 Alyssa Lettich. MD Neurosciences Institute/Neurosciences Clinical Program Medical Director Headache Disclosures: none Learning Objectives: At the conclusion
Primary Care Adult Headache Management Pathway (formerly North West Headache Management Guideline for Adults) Version 1.0
 Version 1.0") Primary Care Adult Headache Management Pathway (formerly rth West Headache Management Guideline for Adults) Version 1.0 1 VERSION CONTROL Version Date Amendments made Version 1.0 October 2018 Reformatted
Primary Care Adult Headache Management Pathway (formerly rth West Headache Management Guideline for Adults) Version 1.0 1 VERSION CONTROL Version Date Amendments made Version 1.0 October 2018 Reformatted
ADVANCES IN MIGRAINE MANAGEMENT
 ADVANCES IN MIGRAINE MANAGEMENT Joanna Girard Katzman, M.D.MSPH Assistant Professor, Dept. of Neurology Project ECHO, Chronic Pain Program University of New Mexico Outline Migraine throughout the decades
ADVANCES IN MIGRAINE MANAGEMENT Joanna Girard Katzman, M.D.MSPH Assistant Professor, Dept. of Neurology Project ECHO, Chronic Pain Program University of New Mexico Outline Migraine throughout the decades
Extended Health Care Company Do you need any help retaining information about your health insurance coverage? Yes No
 PATIENT ENTRANCE FORM Date Circle: Male Female Name Birth Date (dd/mm/yy) Age Address Apt # City Province Postal Code Home # Cell # Work # E-MAIL Occupation Employer Name of Emergency Contact Contact #
PATIENT ENTRANCE FORM Date Circle: Male Female Name Birth Date (dd/mm/yy) Age Address Apt # City Province Postal Code Home # Cell # Work # E-MAIL Occupation Employer Name of Emergency Contact Contact #
MIGRAINE CLASSIFICATION
 MIGRAINE CLASSIFICATION Nada Šternić At most, only 30% of migraineurs have classic aura The same patient may have migraine headache without aura, migraine headache with aura as well as migraine aura without
MIGRAINE CLASSIFICATION Nada Šternić At most, only 30% of migraineurs have classic aura The same patient may have migraine headache without aura, migraine headache with aura as well as migraine aura without
Management options for Migraine. Prof. Dr. Khwaja Nazimuddin Head Dept. of Internal Medicine BIRDEM
 Management options for Migraine Prof. Dr. Khwaja Nazimuddin Head Dept. of Internal Medicine BIRDEM Assessment The Migraine Disability Assessment Score MIDAS Complete loss of work Partial loss of work Off
Management options for Migraine Prof. Dr. Khwaja Nazimuddin Head Dept. of Internal Medicine BIRDEM Assessment The Migraine Disability Assessment Score MIDAS Complete loss of work Partial loss of work Off
Index. Prim Care Clin Office Pract 31 (2004) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Prim Care Clin Office Pract 31 (2004) 441 447 Index Note: Page numbers of article titles are in boldface type. A Abscess, brain, headache in, 388 Acetaminophen for migraine, 406 407 headache from, 369
Prim Care Clin Office Pract 31 (2004) 441 447 Index Note: Page numbers of article titles are in boldface type. A Abscess, brain, headache in, 388 Acetaminophen for migraine, 406 407 headache from, 369
Headache Pain Generators
 Objectives 1. Define the major categories of headache. 2. Take a history directed at characterizing a headache pattern in an individual patient and identify the cause or triggers of the headache. 3. Understand
Objectives 1. Define the major categories of headache. 2. Take a history directed at characterizing a headache pattern in an individual patient and identify the cause or triggers of the headache. 3. Understand
Migraine Management. Dr Helen Brown Director of Neurology and Stroke The Princess Alexandra Hospital
 Migraine Management Dr Helen Brown Director of Neurology and Stroke The Princess Alexandra Hospital Referral Criteria for Migraine Migraine Management Migraine Diagnosis Spot on Health Migraine pathway
Migraine Management Dr Helen Brown Director of Neurology and Stroke The Princess Alexandra Hospital Referral Criteria for Migraine Migraine Management Migraine Diagnosis Spot on Health Migraine pathway
Diagnosis of Primary Headache Syndromes. Gerald W. Smetana, M.D. Division of General Medicine Beth Israel Deaconess Medical Center
 Diagnosis of Primary Headache Syndromes Gerald W. Smetana, M.D. Division of General Medicine Beth Israel Deaconess Medical Center Goals Distinguish primary from secondary headaches Recognize typical histories
Diagnosis of Primary Headache Syndromes Gerald W. Smetana, M.D. Division of General Medicine Beth Israel Deaconess Medical Center Goals Distinguish primary from secondary headaches Recognize typical histories
Management of headache
 Management of headache TJ Steiner Imperial College London Based on European principles of management of common headache disorders TJ Steiner, K Paemeleire, R Jensen, D Valade, L Savi, MJA Lainez, H-C Diener,
Management of headache TJ Steiner Imperial College London Based on European principles of management of common headache disorders TJ Steiner, K Paemeleire, R Jensen, D Valade, L Savi, MJA Lainez, H-C Diener,
11. HEADACHE 1. Pablo Lapuerta, MD, Steven Asch, MD, MPH, and Kenneth Clark, MD, MPH
 11. HEADACHE 1 Pablo Lapuerta, MD, Steven Asch, MD, MPH, and Kenneth Clark, MD, MPH We identified articles on the evaluation and management of headache by conducting a MEDLINE search of English language
11. HEADACHE 1 Pablo Lapuerta, MD, Steven Asch, MD, MPH, and Kenneth Clark, MD, MPH We identified articles on the evaluation and management of headache by conducting a MEDLINE search of English language
Home. About RELPAX. About Migraines. Migraine Tools & Resources. RELPAX Success Stories. The C.A.L.M. Program. Is Your Headache A Migraine?
 About Types of What is a migraine? A migraine is not just a bad headache. It is an intense, throbbing pain. can also cause nausea and sensitivity to light and sound. Most experts agree that migraine pain
About Types of What is a migraine? A migraine is not just a bad headache. It is an intense, throbbing pain. can also cause nausea and sensitivity to light and sound. Most experts agree that migraine pain
Prevention and Treatment of Migraines CAITLIN BARNES, PHARM.D. CANDIDATE AMBULATORY CARE JOE CAMMILLERI, PHARM.D. NATOHYA MALLORY, PHARM.D.
 Prevention and Treatment of Migraines CAITLIN BARNES, PHARM.D. CANDIDATE AMBULATORY CARE JOE CAMMILLERI, PHARM.D. NATOHYA MALLORY, PHARM.D. Objectives Present patient case Review epidemiology/pathophysiology
Prevention and Treatment of Migraines CAITLIN BARNES, PHARM.D. CANDIDATE AMBULATORY CARE JOE CAMMILLERI, PHARM.D. NATOHYA MALLORY, PHARM.D. Objectives Present patient case Review epidemiology/pathophysiology
Faculty/Presenter Disclosure
 Headache Pathway Overview How can I help my migraine patient? Dr Elizabeth Leroux, MD, FRCPC Headache Program University of Calgary Banff 2018 Faculty/Presenter Disclosure Faculty/Presenter: Dr. Elizabeth
Headache Pathway Overview How can I help my migraine patient? Dr Elizabeth Leroux, MD, FRCPC Headache Program University of Calgary Banff 2018 Faculty/Presenter Disclosure Faculty/Presenter: Dr. Elizabeth
Understanding Migraine & other headaches
 Understanding Migraine & other headaches Dr Anne MacGregor Published by Family Doctor Publications Limited in association with the British Medical Association IMPORTANT NOTICE This book is intended not
Understanding Migraine & other headaches Dr Anne MacGregor Published by Family Doctor Publications Limited in association with the British Medical Association IMPORTANT NOTICE This book is intended not
Headache Questionnaire
 Date: All Headache Patients We would appreciate your cooperation in filling out this form. In our evaluation of headache, your history is typically our most valuable tool for diagnosis and subsequent treatment.
Date: All Headache Patients We would appreciate your cooperation in filling out this form. In our evaluation of headache, your history is typically our most valuable tool for diagnosis and subsequent treatment.
Hoofdpijn in de apotheek
 Hoofdpijn in de apotheek Prof. Dr. Koen Paemeleire Dienst Neurologie, Universitair Ziekenhuis Gent Vakgroep Medische Basiswetenschappen, Universiteit Gent Overzicht 1. Epidemiologie 2. Red flags 3. Medication-overuse
Hoofdpijn in de apotheek Prof. Dr. Koen Paemeleire Dienst Neurologie, Universitair Ziekenhuis Gent Vakgroep Medische Basiswetenschappen, Universiteit Gent Overzicht 1. Epidemiologie 2. Red flags 3. Medication-overuse
Headache is the most common symptom in patients with Idiopathic Intracranial Hypertension (IIH). Not everybody with IIH gets headache.
. Not everybody with IIH gets headache.") Headaches in Idiopathic Intracranial Hypertension Headache is the most common symptom in patients with Idiopathic Intracranial Hypertension (). Not everybody with gets headache. Headaches can be there
Headaches in Idiopathic Intracranial Hypertension Headache is the most common symptom in patients with Idiopathic Intracranial Hypertension (). Not everybody with gets headache. Headaches can be there
Sumatran Relief 50mg Tablets. Pharmacist General Migraine Information. Table of content
 Sumatran Relief 50mg Tablets Pharmacist General Migraine Information Table of content 1. Introduction 2. Sumatran Relief indication 3. Mechanism of action 4. Supply criteria 5. Migraine: Description, symptoms,
Sumatran Relief 50mg Tablets Pharmacist General Migraine Information Table of content 1. Introduction 2. Sumatran Relief indication 3. Mechanism of action 4. Supply criteria 5. Migraine: Description, symptoms,
Guidance for Industry Migraine: Developing Drugs for Acute Treatment
 Guidance for Industry Migraine: Developing Drugs for Acute Treatment DRAFT GUIDANCE This guidance document is being distributed for comment purposes only. Comments and suggestions regarding this draft
Guidance for Industry Migraine: Developing Drugs for Acute Treatment DRAFT GUIDANCE This guidance document is being distributed for comment purposes only. Comments and suggestions regarding this draft
The Big 3 of Vertigo
 They feel it, you see it, few know it: Common vertigo conditions seen, but rarely diagnosed Peter Johns MD, FRCPC University of Ottawa pjohns@toh.ca Twitter @peterjohns84 The Big 3 of Vertigo BPPV Vestibular
They feel it, you see it, few know it: Common vertigo conditions seen, but rarely diagnosed Peter Johns MD, FRCPC University of Ottawa pjohns@toh.ca Twitter @peterjohns84 The Big 3 of Vertigo BPPV Vestibular
HEADACHES AND MIGRAINES
 HEADACHES AND MIGRAINES CONTENT CREATED BY Learn more at www.health.harvard.edu TALK WITH YOUR DOCTOR Table of Contents Whether this is your first visit or a follow-up, answer these questions for your
HEADACHES AND MIGRAINES CONTENT CREATED BY Learn more at www.health.harvard.edu TALK WITH YOUR DOCTOR Table of Contents Whether this is your first visit or a follow-up, answer these questions for your
July 2012 Target Population. Adult patients 18 years or older in primary care settings.
 Guideline for Primary Care Management of Headache in Adults July 2012 Target Population Adult patients 18 years or older in primary care settings. Exclusions: This guideline does not provide recommendations
Guideline for Primary Care Management of Headache in Adults July 2012 Target Population Adult patients 18 years or older in primary care settings. Exclusions: This guideline does not provide recommendations
MEASURE #1: MEDICATION PRESCRIBED FOR ACUTE MIGRAINE ATTACK Headache
 MEASURE #1: MEDICATION PRESCRIBED FOR ACUTE MIGRAINE ATTACK Headache Measure Description Percentage of patients age 12 years and older with a diagnosis of migraine who were prescribed a guideline recommended
MEASURE #1: MEDICATION PRESCRIBED FOR ACUTE MIGRAINE ATTACK Headache Measure Description Percentage of patients age 12 years and older with a diagnosis of migraine who were prescribed a guideline recommended
HEADACHE Transient discomfort, chronic nuisance, or looming disaster?
 HEADACHE Transient discomfort, chronic nuisance, or looming disaster? Hussien H. Rizk, MD Cairo University Medical School ١ Headache Second most common o symptom (after pain) Migraine alone afflicts 12
HEADACHE Transient discomfort, chronic nuisance, or looming disaster? Hussien H. Rizk, MD Cairo University Medical School ١ Headache Second most common o symptom (after pain) Migraine alone afflicts 12
Neuralgias tend to be sudden, brief, intermittent severe, stabbing or lightning pains or electric shock sensations.
 Neuralgia is the term used to describe pain arising from a nerve. There are many different neuralgias which have been described in the medical literature, but I will only touch upon a few more common ones.
Neuralgia is the term used to describe pain arising from a nerve. There are many different neuralgias which have been described in the medical literature, but I will only touch upon a few more common ones.
Headache. Karen Thaxter
 Headache Karen Thaxter An eight year old girl is taken to her paediatrician because she has been complaining of almost daily pain at the back of her head for the past 4 months. She states that each headache
Headache Karen Thaxter An eight year old girl is taken to her paediatrician because she has been complaining of almost daily pain at the back of her head for the past 4 months. She states that each headache
Headache evaluation and management after concussion. Assistant Professor
 Headache evaluation and management after concussion Juliette Preston, M.D. Assistant Professor OHSU Headache Center OVERVIEW Introduction Definition Acute post-traumatic headache Red flags Persistent post-traumatic
Headache evaluation and management after concussion Juliette Preston, M.D. Assistant Professor OHSU Headache Center OVERVIEW Introduction Definition Acute post-traumatic headache Red flags Persistent post-traumatic
Headache. Susan Hickenbottom MD, MS February 24, 2015
 Headache Susan Hickenbottom MD, MS February 24, 2015 Epidemiology One of most common complaints in primary care 90% of US population 50% at least one severe 25% recurrent disabling attacks 5% chronic daily
Headache Susan Hickenbottom MD, MS February 24, 2015 Epidemiology One of most common complaints in primary care 90% of US population 50% at least one severe 25% recurrent disabling attacks 5% chronic daily
What Causes Headaches?
 5 What Causes Headaches? It is important to remember that headache is just a symptom. It is not a disease. There are hundreds or thousands of possible causes of headache. However, diagnosis is usually
5 What Causes Headaches? It is important to remember that headache is just a symptom. It is not a disease. There are hundreds or thousands of possible causes of headache. However, diagnosis is usually
Emerging Challenges in Primary Care: Brainstorm: A Symposium on Migraine Treatment and Management
 Emerging Challenges in Primary Care: 2017 Brainstorm: A Symposium on Migraine Treatment and Management 1 Faculty Jeff Unger, MD, ABFM, FACE Director, Unger Primary Care Medical Group Rancho Cucamonga,
Emerging Challenges in Primary Care: 2017 Brainstorm: A Symposium on Migraine Treatment and Management 1 Faculty Jeff Unger, MD, ABFM, FACE Director, Unger Primary Care Medical Group Rancho Cucamonga,