Supplementary Online Content
|
|
|
- Jayson Richardson
- 5 years ago
- Views:
Transcription
1 Supplementary Online Content Tseng ZH, Hayward RM, Clark NM, et al. Sudden death in patients with cardiac implantable electronic devices. JAMA Intern Med. Published online June 22, doi: /jamainternmed etable. Details of Investigation for SCDs With Cardiovascular Implantable Electronic Devices efigure 1. Case 5 efigure 2. Case 1 efigure 3. Case 2 efigure 4. Case 3 efigure 5. Case 4 efigure 6. Case 15 efigure 7. Case 18 efigure 8. Case 19 efigure 9. Case 20 efigure 10. Case 21 This supplementary material has been provided by the authors to give readers additional information about their work.
2 etable 1. Details of Investigation for SCDs with Cardiovascular Implantable Electronic Devices Case Patient Details Device Autopsy Findings Device Interrogation Terminal Rhythm Adjudicated COD Device Concern Sudden battery depletion from 2.62V (5 weeks prior to death) to 2.17V Presumed profound Yes (Battery; Hardware 1 70 with CHB, AF DC PPM No MI or other acute COD Arrhythmic (day of death). See efigure 2. bradycardia/asystole failure) Yes (ICD was indicated at 42 with CHB, HCM, Hypertrophic CM with 3.0 cm 2 DC PPM Normal PPM function with VF at time of death. See efigure 3. VF Arrhythmic time of PPM; Improper syncope septum. No acute MI device selection) 3 77 with sick sinus syndrome, advanced AV block, CAD s/p MI, CVA, Alzheimer's dz DC PPM 4 60 with CHB, AF DC PPM No MI; acute bronchopneumonia Rectal adenocarcinoma, cardiomegaly, 30% LAD stenosis, and severe myocardial fibrosis. No MI or acute COD No VT/VF. Rapid rise in RV lead impedance (650 >1620 ohms) 1wk prior to death concerning for lead fracture. See efigure 4. Increase in RV lead impedance 2 days prior to death. PMVT/VF at the time of death. See efigure 5. PEA PMVT/VF Pneumonia Arrhythmic Yes (RV lead; Possible hardware failure) Yes (RV lead; Hardware failure) 5 26 with 2nd deg. HB, L Normal PPM function w/o recorded events at time of death. See efigure Massive pulmonary DC PPM Massive pulmonary hemorrhage PEA TGA s/p mechanical TVR 1. hemorrhage No 6 87 with 2nd deg. HB, Intracranial DC PPM Intracranial hemorrhage Acute increase in RV lead impedance (380 >1340 ohms) post mortem. AF w/ RVR >Asystole AF, CAD s/p MI hemorrhage No 7 98 with CHB, AF DC PPM Cardiac (heart Pulmonary edema and scar from Normal PPM function w/o recorded events at the time of death. PEA (AS VP) failure), nonarrhythmic remote MI but no acute MI No 8 70 with sinus node Scar from remote MI. No acute MI DC PPM dysfunction or other COD Normal PPM function with VF at the time of death. VF Arrhythmic No 9 84 with CHB, AF DC PPM No acute cause of death No electrograms recorded (device was ERI), but intervals suggest VF. VF Arrhythmic No with CHB, CHF DC PPM Dilated CM w/o MI or other acute COD Normal PPM function. Device at ERI, full interrogation not possible. Unknown Arrhythmic No with AF and Blunt force injuries of head/neck DC PPM bradycardia w/ CAD Normal PPM function. AF with RVR at time of death. AF with RVR Occult trauma No with CHB, AF, CAD s/p MI, CHF 87 with tachy brady syndrome 77 with CHB, CAD, idiopathic CM DC PPM DC PPM with Dilated CM DC ICD with Ischemic CM, AF, CAD 70 with Ischemic CM, CHF 74 with CAD s/p MI, ischemic CM, AF, VT No MI. Acute lung inflammation due to pneumonia No MI or other acute COD. 50% LAD stenosis Normal PPM function. NSVT > Idioventricular rhythm Pneumonia Normal PPM function with VF at time of death. VF Arrhythmic No CRT P N/A No device interrogation. VF recorded by paramedics. VF Arrhythmic No DC ICD CRT D DC ICD Massive subarachnoid hemorrhage, cardiomegaly (heart 760g) Scar from remote MI and CM but no acute MI or other COD CM without acute MI or other COD Scar from remote MI and 99% LAD stenosis but no acute MI VF documented at time of death (likely secondary to subarachnoid hemorrhage). See efigure 6. Episodes of VF during EMS rescue were not recorded by device and required external shocks for rescue. Delay to shock due to ATP programming in the VF zone. See Figure 2. VF undersensed with device interpreting return to sinus rhythm (no shock delivered). See Figure 3. VF with undersensing. 40 VF and 2 VT episodes identified and 17/42 shocks aborted due to undersensing. The second event showed significant undersensing with a significant delay in therapy. See efigure 7. VF VF VF Subarachnoid hemorrhage Arrhythmic Arrhythmic No No Yes (VF episodes missed; Programming and Device algorithm issue) Yes (VF undersensing; Device algorithm issue) VF Arrhythmic Yes (VF undersensing)
3 with dilated CM, ESRD on HD 71 with AF, CAD, ischemic CM 80 with ischemic CM, CAD, CHF 80 with Ischemic CM, AF DC ICD SC ICD CRT D DC ICD N/A Acute RCA thrombus. Cardiomegaly, cirrhosis, COPD N/A Hypertensive heart disease, COPD VT that was undersensed. This was treated with ATP but wavering VT cycle length resulted in a delayed shock. VT degraded into fine VF that was undersensed. Patient left in VF/VT and device stopped recording and was unable to detect after that point. See efigure 8. Extended VF with undersensing leading to a delay in interval counts that delayed therapy. See efigure 9. VF storm with 4 shocks and multiple rounds of ATP. Final event shows VT but device did not rescue due to programming of tachycardia zone. See efigure 10. VF with successful defibrillation x 3 followed by RV lead noise and increase in lead impedance with 4th shock suggesting lead fracture. See Figure 4. VF Arrhythmic Yes (VT undersensing) VF VT VF Arrhythmic Arrhythmic Arrhythmic Yes (VF undersensing, Programming and Device algorithm issue) Yes (VT slower than VT zone; Programming) Yes (Lead fracture; Hardware failure) AF atrial fibrillation, CAD coronary artery disease, CHB complete heart block, CHF congestive heart failure, CM cardiomyopathy, COD cause of death, CRT P cardiac resynchronization therapy pacemaker, CRT D cardiac resynchronization therapy defibrillator, DC dual chamber, MI myocardial infarction, PEA pulseless electrical activity, PPM permanent pacemaker, RV right ventricle, RVR rapid ventricular response, SC single chamber, VF ventricular fibrillation, VT ventricular tachycardia
 demonstrating dilated bronchial veins (arrows) and hemosiderin laden macrophages (arrowheads). Reprinted with permission from Hayward RM, Ursell PC, Foster E, Tseng ZH.")
4 efigure 1 (Case 5). Left: Post mortem device interrogation showing no ventricular high rate episodes. Right: H&E section of lung (12.5X) demonstrating dilated bronchial veins (arrows) and hemosiderin laden macrophages (arrowheads). Reprinted with permission from Hayward RM, Ursell PC, Foster E, Tseng ZH. Sudden death due to nonarrhythmic cause in a patient with L TGA. Ann Noninvasive Electrocardiol. 2014;19(3):
5 efigure 2 (Case 1). Top: PPM interrogation 5 weeks prior to death shows estimated battery longevity of 6 months and > 95% ventricular pacing. The patient s PVC burden was at least 3%, which accounted for most of the non-paced ventricular beats and underlying rhythm at device check was sinus bradycardia with complete heart block and a slow junctional escape. The patient s ventricular pacing threshold at this this time was 2.5V with a pulse width of 0.4 ms. Bottom: Pacemaker interrogation within 1 day after death demonstrates excessive voltage decrease of 0.46 V consistent with rapid battery depletion and no ventricular high rate episodes.
6 efigure 3 (Case 2). Top: Atrial marker channel. Middle: Ventricular marker channel. Bottom: Intervals. VF at the time of death. ICD is a IIa recommendation in 2008 ACC/AHA/HRS Guidelines for HCM patients with unexplained syncope and septal thickness > 30 mm. This patient died of VF with a PPM in place.

7 efigure 4 (Case 3). Postmortem PPM interrogation demonstrating a rapid substantial increase in atrial and ventricular lead impedances that was first detected 2 days prior to death. The patient died suddenly on January 13, The intrinsic R-wave was measured at 5.5 mv on the day prior to death, suggesting intrinsic ventricular activity. However, lead fracture can be intermittent and the sensing could have been due to junctional or ventricular escape beats. Atrial lead impedance also increased, raising the possibility of changes due to acidosis or electrolyte disturbances, but atrial lead impedance normalized on the day of death. In this case, although pneumonia was found on autopsy and occult pneumonia was adjudicated as the COD, right ventricular lead fracture or a global pacemaker problem resulting in profound bradycardia or asystole could not be excluded as a contributor to sudden death.
8 efigure 5 (Case 4). Top: Increase in ventricular lead impedance 2 days prior to death (the patient died suddenly on 11/3/13). Bottom: Ventricular electrogram shows PMVT/VF at the time of death. No acute COD was found on autopsy. The lead malfunction may have led directly to VT/VF via pause dependent mechanism caused by inconsistent ventricular capture or R on T phenomenon due to undersensing.
.")
9 efigure 6 (Case 15). 78M with dilated CM and VF documented at the time of death which was recognized and treated by the ICD (Left). VF was due to hemorrhage in the right insular cortex (Right) leading to arrhythmia (neurocardiogenic VF).
10
11 efigure 7 (Case 18). The patient had 40 VF and 2 VT episodes identified and 17 of 42 shocks aborted due to undersensing. Top: atrial electrogram. Middle: ventricular electrogram. Bottom: device markers. Strips are continuous. This event shows a return to sinus (*) after the previous shock due to undersensing of VF (arrowheads). This resulted in a significant delay in therapy.
12 efigure 8 (Case 19). Top: atrial electrogram. Middle: ventricular electrogram. Bottom: Shock electrogram. After 3 unsuccessful ATP attempts, the patient was in VT/VF. Undersensing resulted in a wavering VT cycle length and diversion of charging (*). The device redetected VF and delivered a shock, but undersensing resulted in a delay to therapy of 12.2 seconds (A). Ultimately, the patient was left in VF that the device was unable to detect and stopped recording (B). The patient s final recorded rhythm, which showed undersensing of VF. Intervals show varying cycle lengths wavering in and out of VT zone (C).

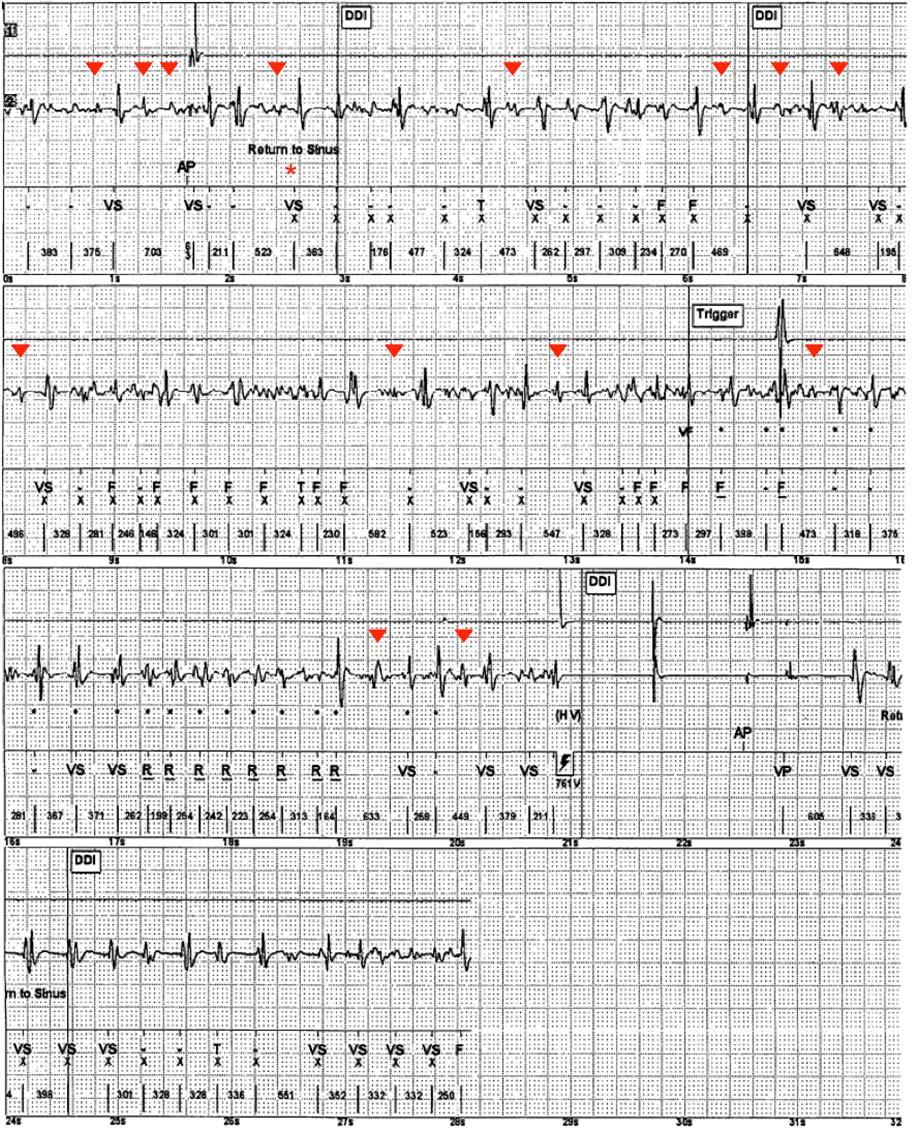
13 efigure 9 (Case 20). Top and Middle Strips (continuous): Extended VF event with undersensing (arrowheads) that delays therapy. In addition, ATP delays shock therapy. Less than 1 minute later, the patient had multiple additional episodes of VT/VF requiring defibrillation. Bottom Strip: 4 minutes later, the final rhythm recorded by the device was VF with no further shocks delivered. Autopsy showed acute RCA thrombus. Cumulative delays to shock may have resulted in refractoriness of VF and further opportunity for undersensing.
 but the device did not rescue due to the programming of the")
14 efigure 10 (Case 21). Top: atrial electrogram. Middle: ventricular electrogram. Bottom: device markers. After 4 shocks and multiple rounds of ATP, the patient is left in VT (mean cycle length 447 msec) but the device did not rescue due to the programming of the tachycardia zone (VT detection zone >166 bpm or <360 msec).
EHRA Accreditation Exam - Sample MCQs Cardiac Pacing and ICDs
 EHRA Accreditation Exam - Sample MCQs Cardiac Pacing and ICDs Dear EHRA Member, Dear Colleague, As you know, the EHRA Accreditation Process is becoming increasingly recognised as an important step for
EHRA Accreditation Exam - Sample MCQs Cardiac Pacing and ICDs Dear EHRA Member, Dear Colleague, As you know, the EHRA Accreditation Process is becoming increasingly recognised as an important step for
PERMANENT PACEMAKERS AND IMPLANTABLE DEFIBRILLATORS Considerations for intensivists
 PERMANENT PACEMAKERS AND IMPLANTABLE DEFIBRILLATORS Considerations for intensivists Craig A. McPherson, MD, FACC Associate Professor of Medicine Constantine Manthous, MD, FACP, FCCP Associate Clinical
PERMANENT PACEMAKERS AND IMPLANTABLE DEFIBRILLATORS Considerations for intensivists Craig A. McPherson, MD, FACC Associate Professor of Medicine Constantine Manthous, MD, FACP, FCCP Associate Clinical
Tachycardia Devices Indications and Basic Trouble Shooting
 Tachycardia Devices Indications and Basic Trouble Shooting Peter A. Brady, MD., FRCP Cardiology Review Course London, March 6 th, 2014 2011 MFMER 3134946-1 Tachycardia Devices ICD Indications Primary and
Tachycardia Devices Indications and Basic Trouble Shooting Peter A. Brady, MD., FRCP Cardiology Review Course London, March 6 th, 2014 2011 MFMER 3134946-1 Tachycardia Devices ICD Indications Primary and
Cardiac Rhythm Device Management. PBL STOP Your acronym for a standardized follow-up
 Cardiac Rhythm Device Management PBL STOP Your acronym for a standardized follow-up What s in it for you? What do you need to feel comfortable with a pacemaker/icd follow-up? 2 CORE OBJECTIVE Provide a
Cardiac Rhythm Device Management PBL STOP Your acronym for a standardized follow-up What s in it for you? What do you need to feel comfortable with a pacemaker/icd follow-up? 2 CORE OBJECTIVE Provide a
ICD: Basics, Programming and Trouble-shooting
 ICD: Basics, Programming and Trouble-shooting Amir AbdelWahab, MD Electrophysiology and Pacing Service Cardiology Department Cairo University Feb 2013 Evolution of ICD Technology ICD Evolution Indications
ICD: Basics, Programming and Trouble-shooting Amir AbdelWahab, MD Electrophysiology and Pacing Service Cardiology Department Cairo University Feb 2013 Evolution of ICD Technology ICD Evolution Indications
The Nuts and Bolts of ICD Therapy
 Electrical Management of Cardiac Rhythm Disorders For Cardiology Fellows December 5-8 Austin, Texas The Nuts and Bolts of ICD Therapy 1 2 Action Potential Localized Differences in Conduction Conduction
Electrical Management of Cardiac Rhythm Disorders For Cardiology Fellows December 5-8 Austin, Texas The Nuts and Bolts of ICD Therapy 1 2 Action Potential Localized Differences in Conduction Conduction
Sudden Cardiac Death What an electrophysiologist thinks a cardiologist should know
 Sudden Cardiac Death What an electrophysiologist thinks a cardiologist should know Steven J. Kalbfleisch, M.D. Medical Director Electrophysiology Laboratory Ross Heart Hospital Wexner Medical Center Sudden
Sudden Cardiac Death What an electrophysiologist thinks a cardiologist should know Steven J. Kalbfleisch, M.D. Medical Director Electrophysiology Laboratory Ross Heart Hospital Wexner Medical Center Sudden
Review Packet EKG Competency This packet is a review of the information you will need to know for the proctored EKG competency test.
 Review Packet EKG Competency 2015 This packet is a review of the information you will need to know for the proctored EKG competency test. Normal Sinus Rhythm Rhythm: Regular Ventricular Rate: 60-100 bpm
Review Packet EKG Competency 2015 This packet is a review of the information you will need to know for the proctored EKG competency test. Normal Sinus Rhythm Rhythm: Regular Ventricular Rate: 60-100 bpm
Practice Questions.
 IBHRE Prep Practice Questions Question 1 The relative refractory yperiod of the ventricular myocardium corresponds to which of the following phases of the action potential? A. (0) B. (1) C. (2) D. (3)
IBHRE Prep Practice Questions Question 1 The relative refractory yperiod of the ventricular myocardium corresponds to which of the following phases of the action potential? A. (0) B. (1) C. (2) D. (3)
Device Interrogation- Pacemakers, ICD and Loop Recorders. Dulce Obias-Manno, RN, MHSA, CCDS,CEPS, FHRS Device Clinic Coordinator, MHVI
 Device Interrogation- Pacemakers, ICD and Loop Recorders Dulce Obias-Manno, RN, MHSA, CCDS,CEPS, FHRS Device Clinic Coordinator, MHVI Disclosures Consultant: Medtronic Speaker s Bureau: St. Jude Medical
Device Interrogation- Pacemakers, ICD and Loop Recorders Dulce Obias-Manno, RN, MHSA, CCDS,CEPS, FHRS Device Clinic Coordinator, MHVI Disclosures Consultant: Medtronic Speaker s Bureau: St. Jude Medical
Different indications for pacemaker implantation are the following:
 Patient Resources: ICD/Pacemaker Overview ICD/Pacemaker Overview What is a pacemaker? A pacemaker is a device that uses low energy electrical pulses to prompt the heart to beat whenever a pause in the
Patient Resources: ICD/Pacemaker Overview ICD/Pacemaker Overview What is a pacemaker? A pacemaker is a device that uses low energy electrical pulses to prompt the heart to beat whenever a pause in the
Cardiac Implanted Electronic Devices Pacemakers, Defibrillators, Cardiac Resynchronization Devices, Loop Recorders, etc.
 Cardiac Implanted Electronic Devices Pacemakers, Defibrillators, Cardiac Resynchronization Devices, Loop Recorders, etc. The Miracle of Living February 21, 2018 Matthew Ostrom MD,FACC,FHRS Division of
Cardiac Implanted Electronic Devices Pacemakers, Defibrillators, Cardiac Resynchronization Devices, Loop Recorders, etc. The Miracle of Living February 21, 2018 Matthew Ostrom MD,FACC,FHRS Division of
Troubleshooting ICD. NASPE Training Lancashire & South Cumbria Cardiac Network
 Troubleshooting ICD NASPE Training Lancashire & South Cumbria Cardiac Network Bradycardia Pacing by ICD Isolated ICD discharge Multiple discharges Appropriate Inappropriate No ICD Therapy or delay in ICD
Troubleshooting ICD NASPE Training Lancashire & South Cumbria Cardiac Network Bradycardia Pacing by ICD Isolated ICD discharge Multiple discharges Appropriate Inappropriate No ICD Therapy or delay in ICD
Arrhythmic Complications of MI. Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine
 Arrhythmic Complications of MI Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine Objectives Brief overview -Pathophysiology of Arrhythmia ECG review of typical
Arrhythmic Complications of MI Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine Objectives Brief overview -Pathophysiology of Arrhythmia ECG review of typical
Programming of Bradycardic Parameters. C. W. Israel, M.D. Dept. of Cardiology Evangelical Hospital Bielefeld Germany
 Programming of Bradycardic Parameters C. W. Israel, M.D. Dept. of Cardiology Evangelical Hospital Bielefeld Germany Carsten.Israel@evkb.de Programming of ICD Brady Parameters Conflict of Interest Biotronik
Programming of Bradycardic Parameters C. W. Israel, M.D. Dept. of Cardiology Evangelical Hospital Bielefeld Germany Carsten.Israel@evkb.de Programming of ICD Brady Parameters Conflict of Interest Biotronik
ICD Diagnostics: Making the most of it
 ICD Basics and Beyond ICD Diagnostics: Making the most of it Dulce Obias-Manno RN, BSN, MHSA, FHRS, CCDS, CEPS Cardiac Arrhythmia Center, Device Clinic Washington Hospital Center, Washington DC Objectives
ICD Basics and Beyond ICD Diagnostics: Making the most of it Dulce Obias-Manno RN, BSN, MHSA, FHRS, CCDS, CEPS Cardiac Arrhythmia Center, Device Clinic Washington Hospital Center, Washington DC Objectives
Puzzling Pacemakers Cheryl Herrmann, APN, CCRN, CCNS-CSC-CMC
 Puzzling Pacemakers Cheryl Herrmann, APN, CCRN, CCNS-CSC-CMC Pacemaker: An electric device implanted in the body to regulate the heart beat. Delivers electrical stimuli over leads with electrodes in contact
Puzzling Pacemakers Cheryl Herrmann, APN, CCRN, CCNS-CSC-CMC Pacemaker: An electric device implanted in the body to regulate the heart beat. Delivers electrical stimuli over leads with electrodes in contact
HRC Carole Joyce. Bradford Royal Infirmary. Senior Chief Cardiac Physiologist. Pacing & Invasive Services.
 HRC 2010 Carole Joyce Carole.joyce@bradfordhospitals.nhs.uk Pacing & Invasive Services Carole Joyce Introduction Basic Protocol Troubleshooting Case Studies Questions & Answer Carole Joyce ICD Troubleshooting
HRC 2010 Carole Joyce Carole.joyce@bradfordhospitals.nhs.uk Pacing & Invasive Services Carole Joyce Introduction Basic Protocol Troubleshooting Case Studies Questions & Answer Carole Joyce ICD Troubleshooting
EKG Competency for Agency
 EKG Competency for Agency Name: Date: Agency: 1. The upper chambers of the heart are known as the: a. Atria b. Ventricles c. Mitral Valve d. Aortic Valve 2. The lower chambers of the heart are known as
EKG Competency for Agency Name: Date: Agency: 1. The upper chambers of the heart are known as the: a. Atria b. Ventricles c. Mitral Valve d. Aortic Valve 2. The lower chambers of the heart are known as
NEIL CISPER TECHNICAL FIELD ENGINEER ICD/CRTD BASICS
 NEIL CISPER TECHNICAL FIELD ENGINEER ICD/CRTD BASICS OBJECTIVES Discuss history of ICDs Review the indications for ICD and CRT therapy Describe basic lead and device technology Discuss different therapies
NEIL CISPER TECHNICAL FIELD ENGINEER ICD/CRTD BASICS OBJECTIVES Discuss history of ICDs Review the indications for ICD and CRT therapy Describe basic lead and device technology Discuss different therapies
La strategia diagnostica: il monitoraggio ecg prolungato. Michele Brignole
 La strategia diagnostica: il monitoraggio ecg prolungato Michele Brignole ECG monitoring and syncope In-hospital monitoring Holter Monitoring External loop recorder Remote (at home) telemetry Implantable
La strategia diagnostica: il monitoraggio ecg prolungato Michele Brignole ECG monitoring and syncope In-hospital monitoring Holter Monitoring External loop recorder Remote (at home) telemetry Implantable
Supplemental Material
 Supplemental Material 1 Table S1. Codes for Patient Selection Cohort Codes Primary PM CPT: 33206 or 33207 or 33208 (without 33225) ICD-9 proc: 37.81, 37.82, 37.83 Primary ICD Replacement PM Replacement
Supplemental Material 1 Table S1. Codes for Patient Selection Cohort Codes Primary PM CPT: 33206 or 33207 or 33208 (without 33225) ICD-9 proc: 37.81, 37.82, 37.83 Primary ICD Replacement PM Replacement
Is This Thing Working?
 Is This *#@!* Thing Working? Pacemaker (and ICD) ECG and Telemetry Pitfalls Wayne O. Adkisson, MD adki0004@umn.edu Disclosures I currently receive research support from Medtronic, Inc. I have been compensated
Is This *#@!* Thing Working? Pacemaker (and ICD) ECG and Telemetry Pitfalls Wayne O. Adkisson, MD adki0004@umn.edu Disclosures I currently receive research support from Medtronic, Inc. I have been compensated
Managing Hypertrophic Cardiomyopathy with Imaging. Gisela C. Mueller University of Michigan Department of Radiology
 Managing Hypertrophic Cardiomyopathy with Imaging Gisela C. Mueller University of Michigan Department of Radiology Disclosures Gadolinium contrast material for cardiac MRI Acronyms Afib CAD Atrial fibrillation
Managing Hypertrophic Cardiomyopathy with Imaging Gisela C. Mueller University of Michigan Department of Radiology Disclosures Gadolinium contrast material for cardiac MRI Acronyms Afib CAD Atrial fibrillation
Tech Corner. ATP in the Fast VT zone
 Tech Corner ATP in the Fast VT zone NOTE: PLEASE NOTE THAT THE FOLLOWING INFORMATION IS A GENERAL DESCRIPTION OF THE FUNCTION. DETAILS AND PARTICULAR CASES ARE NOT DESCRIBED IN THE ARTICLE. FOR ADDITIONAL
Tech Corner ATP in the Fast VT zone NOTE: PLEASE NOTE THAT THE FOLLOWING INFORMATION IS A GENERAL DESCRIPTION OF THE FUNCTION. DETAILS AND PARTICULAR CASES ARE NOT DESCRIBED IN THE ARTICLE. FOR ADDITIONAL
Pediatric pacemakers & ICDs:
 Pediatric pacemakers & ICDs: perioperative management Manchula Navaratnam Clinical Assistant Professor LPCH, Stanford SPA 2016 Conflict of interest: none Objectives Indications in pediatrics Components
Pediatric pacemakers & ICDs: perioperative management Manchula Navaratnam Clinical Assistant Professor LPCH, Stanford SPA 2016 Conflict of interest: none Objectives Indications in pediatrics Components
SVT Discriminators. Definition of SVT Discrimination. Identify which patient populations might benefit from these features
 Definition of SVT Discrimination Identify which patient populations might benefit from these features Understand the 4 types of SVT discriminators used by St Jude Medical Be aware of programmable parameters
Definition of SVT Discrimination Identify which patient populations might benefit from these features Understand the 4 types of SVT discriminators used by St Jude Medical Be aware of programmable parameters
Cardiac Arrhythmias. Cathy Percival, RN, FALU, FLMI VP, Medical Director AIG Life and Retirement Company
 Cardiac Arrhythmias Cathy Percival, RN, FALU, FLMI VP, Medical Director AIG Life and Retirement Company The Cardiovascular System Three primary functions Transport of oxygen, nutrients, and hormones to
Cardiac Arrhythmias Cathy Percival, RN, FALU, FLMI VP, Medical Director AIG Life and Retirement Company The Cardiovascular System Three primary functions Transport of oxygen, nutrients, and hormones to
BHRS Prep course Pub style Quiz NOT A
 BHRS Prep course Pub style Quiz NOT A Round 1 Quiz questions Common ECG s in CRM Colin Cunnington Over the past 3 months, a 24-yearold man who works as a truck driver has had frequent episodes of pre-syncope
BHRS Prep course Pub style Quiz NOT A Round 1 Quiz questions Common ECG s in CRM Colin Cunnington Over the past 3 months, a 24-yearold man who works as a truck driver has had frequent episodes of pre-syncope
11/21/18. EKG Pop Quiz. Michael Giocondo, MD Cardiac Electrophysiology Saint Luke s Cardiovascular Consultants
 EKG Pop Quiz Michael Giocondo, MD Cardiac Electrophysiology Saint Luke s Cardiovascular Consultants 1 Disclosures No financial relationships to disclose. EKG #1 75 y/o woman with a dual-chamber pacemaker
EKG Pop Quiz Michael Giocondo, MD Cardiac Electrophysiology Saint Luke s Cardiovascular Consultants 1 Disclosures No financial relationships to disclose. EKG #1 75 y/o woman with a dual-chamber pacemaker
PACEMAKER INTERPRETATION AND DEVICE MANAGEMENT PART II
 1 PACEMAKER INTERPRETATION AND DEVICE MANAGEMENT PART II 2012 Cynthia Webner DNP, RN, CCNS, CCRN-CMC Karen Marzlin DNP, RN, CCNS, CCRN-CMC 2 ADDITIVES IN DEVICE THERAPY Key Choice / CNEA 1 Adaptive Rate
1 PACEMAKER INTERPRETATION AND DEVICE MANAGEMENT PART II 2012 Cynthia Webner DNP, RN, CCNS, CCRN-CMC Karen Marzlin DNP, RN, CCNS, CCRN-CMC 2 ADDITIVES IN DEVICE THERAPY Key Choice / CNEA 1 Adaptive Rate
GDT1000 SENSING ACUTE STUDY
 CAUTION: Federal law restricts this device to sale by or on the order of a physician trained or experienced in device implant and follow-up procedures. CLINICAL SUMMARY GDT1000 SENSING ACUTE STUDY Boston
CAUTION: Federal law restricts this device to sale by or on the order of a physician trained or experienced in device implant and follow-up procedures. CLINICAL SUMMARY GDT1000 SENSING ACUTE STUDY Boston
KNOW YOUR ECG. G. Somasekhar MD DM FEp Consultant Electro physiologist, Aayush Hospital, Vijayawada
 KNOW YOUR ECG G. Somasekhar MD DM FEp Consultant Electro physiologist, Aayush Hospital, Vijayawada CASE DETAILS A 48-year-old female non hypertensive, non diabetic presented with history of shortness of
KNOW YOUR ECG G. Somasekhar MD DM FEp Consultant Electro physiologist, Aayush Hospital, Vijayawada CASE DETAILS A 48-year-old female non hypertensive, non diabetic presented with history of shortness of
Diagnostic capabilities of the implantable therapeutic systems
 Cardiac pacing 2012 and beyound Monday August 27, 2012 Diagnostic capabilities of the implantable therapeutic systems Pekka Raatikainen Heart Center Co. Tampere University Hospital and University of Tampere
Cardiac pacing 2012 and beyound Monday August 27, 2012 Diagnostic capabilities of the implantable therapeutic systems Pekka Raatikainen Heart Center Co. Tampere University Hospital and University of Tampere
Dual-Chamber Implantable Cardioverter-Defibrillator
 February 1998 9 Dual-Chamber Implantable Cardioverter-Defibrillator A.SH. REVISHVILI A.N. Bakoulev Research Center for Cardiovascular Surgery, Russian Academy of Medical Sciences, Moscow, Russia Summary
February 1998 9 Dual-Chamber Implantable Cardioverter-Defibrillator A.SH. REVISHVILI A.N. Bakoulev Research Center for Cardiovascular Surgery, Russian Academy of Medical Sciences, Moscow, Russia Summary
Conduction disorders
 Conduction disorders L.V. Bogun, N.I. Yabluchansky, F.M. Abdueva, O.Y. Bichkova, A.N. Fomich, P.A. Garkavyi, A.L. Kulik, N.V. Lysenko, N.V. Makienko, L.A. Martimyanova, I.V. Soldatenko, E.E. Tomina Department
Conduction disorders L.V. Bogun, N.I. Yabluchansky, F.M. Abdueva, O.Y. Bichkova, A.N. Fomich, P.A. Garkavyi, A.L. Kulik, N.V. Lysenko, N.V. Makienko, L.A. Martimyanova, I.V. Soldatenko, E.E. Tomina Department
Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition
 Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition Table of Contents Volume 1 Chapter 1: Cardiovascular Anatomy and Physiology Basic Cardiac
Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition Table of Contents Volume 1 Chapter 1: Cardiovascular Anatomy and Physiology Basic Cardiac
Improving Patient Outcomes with a Syncope Center. Suneet Mittal, MD
 Improving Patient Outcomes with a Syncope Center Suneet Mittal, MD Improving Patient Outcomes with a Syncope Center: Early Risk Stratification of Patients who Require Device Therapy Suneet Mittal, MD Director,
Improving Patient Outcomes with a Syncope Center Suneet Mittal, MD Improving Patient Outcomes with a Syncope Center: Early Risk Stratification of Patients who Require Device Therapy Suneet Mittal, MD Director,
Newer pacemakers also can monitor your blood temperature, breathing, and other factors and adjust your heart rate to changes in your activity.
 Pacemakers & Defibrillators A pacemaker system consists of a battery, a computerized generator and wires with sensors called electrodes on one end. The battery powers the generator, and both are surrounded
Pacemakers & Defibrillators A pacemaker system consists of a battery, a computerized generator and wires with sensors called electrodes on one end. The battery powers the generator, and both are surrounded
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Implantable cardioverter defibrillators for the treatment of arrhythmias and cardiac resynchronisation therapy for the treatment of heart failure (review
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Implantable cardioverter defibrillators for the treatment of arrhythmias and cardiac resynchronisation therapy for the treatment of heart failure (review
UNDERSTANDING YOUR ECG: A REVIEW
 UNDERSTANDING YOUR ECG: A REVIEW Health professionals use the electrocardiograph (ECG) rhythm strip to systematically analyse the cardiac rhythm. Before the systematic process of ECG analysis is described
UNDERSTANDING YOUR ECG: A REVIEW Health professionals use the electrocardiograph (ECG) rhythm strip to systematically analyse the cardiac rhythm. Before the systematic process of ECG analysis is described
Heart Rhythm Disorders. How do you quantify risk?
 Heart Rhythm Disorders How do you quantify risk? Heart Rhythm Disorders Scale of the Problem 1/2 population will have an episode of transient loss of consciousness (T-LOC) at some stage in their life.
Heart Rhythm Disorders How do you quantify risk? Heart Rhythm Disorders Scale of the Problem 1/2 population will have an episode of transient loss of consciousness (T-LOC) at some stage in their life.
Presented By: Barbara Furry, RN-BC, MS, CCRN, FAHA Director The Center of Excellence in Education Director of HERO
 Presented By: Barbara Furry, RN-BC, MS, CCRN, FAHA Director The Center of Excellence in Education Director of HERO Follow me on Twitter! CEE Med Updates@BarbaraFurryRN Like me on Facebook! What is a
Presented By: Barbara Furry, RN-BC, MS, CCRN, FAHA Director The Center of Excellence in Education Director of HERO Follow me on Twitter! CEE Med Updates@BarbaraFurryRN Like me on Facebook! What is a
How Do I Balance Bradycardia with Rate Control in Atrial Fibrillation?
 How Do I Balance Bradycardia with Rate Control in Atrial Fibrillation? Thang Nguyen MD FRCPC Assistant Professor Section of Cardiology Department of Internal Medicine University of Manitoba Objectives
How Do I Balance Bradycardia with Rate Control in Atrial Fibrillation? Thang Nguyen MD FRCPC Assistant Professor Section of Cardiology Department of Internal Medicine University of Manitoba Objectives
CSI Skills Lab #5: Arrhythmia Interpretation and Treatment
 CSI 202 - Skills Lab #5: Arrhythmia Interpretation and Treatment Origins of the ACLS Approach: CSI 202 - Skills Lab 5 Notes ACLS training originated in Nebraska in the early 1970 s. Its purpose was to
CSI 202 - Skills Lab #5: Arrhythmia Interpretation and Treatment Origins of the ACLS Approach: CSI 202 - Skills Lab 5 Notes ACLS training originated in Nebraska in the early 1970 s. Its purpose was to
Endpoints When Treating VT/VF in Patients with ICDs Programming Wojciech Zareba, MD, PhD
 Endpoints When Treating VT/VF in Patients with ICDs Programming Wojciech Zareba, MD, PhD Professor of Cardiology/Medicine Director of the Heart Research Follow Up Program, University of Rochester, Rochester,
Endpoints When Treating VT/VF in Patients with ICDs Programming Wojciech Zareba, MD, PhD Professor of Cardiology/Medicine Director of the Heart Research Follow Up Program, University of Rochester, Rochester,
Rhythm ECG Characteristics Example. Normal Sinus Rhythm (NSR)
") Normal Sinus Rhythm (NSR) Rate: 60-100 per minute Rhythm: R- R = P waves: Upright, similar P-R: 0.12-0.20 second & consistent P:qRs: 1P:1qRs Sinus Tachycardia Exercise Hypovolemia Medications Fever Substances
Normal Sinus Rhythm (NSR) Rate: 60-100 per minute Rhythm: R- R = P waves: Upright, similar P-R: 0.12-0.20 second & consistent P:qRs: 1P:1qRs Sinus Tachycardia Exercise Hypovolemia Medications Fever Substances
PACEMAKER INTERPRETATION AND DEVICE MANAGEMENT PART I
 1 PACEMAKER INTERPRETATION AND DEVICE MANAGEMENT PART I Cynthia Webner DNP, RN, CCNS, CCRN-CMC Karen Marzlin DNP, RN, CCNS, CCRN-CMC 2 PROFESSIONAL NURSING PRACTICE CAN ONLY ADVANCE AS MUCH AS INDIVIDUAL
1 PACEMAKER INTERPRETATION AND DEVICE MANAGEMENT PART I Cynthia Webner DNP, RN, CCNS, CCRN-CMC Karen Marzlin DNP, RN, CCNS, CCRN-CMC 2 PROFESSIONAL NURSING PRACTICE CAN ONLY ADVANCE AS MUCH AS INDIVIDUAL
RN-BC, MS, CCRN, FAHA
 Presented By: Barbara Furry, RN-BC, MS, CCRN, FAHA Director The Center of Excellence in Education Director of HERO Follow me on Twitter! CEE Med Updates@BarbaraFurryRN Like me on Facebook! 1 A. Atropine
Presented By: Barbara Furry, RN-BC, MS, CCRN, FAHA Director The Center of Excellence in Education Director of HERO Follow me on Twitter! CEE Med Updates@BarbaraFurryRN Like me on Facebook! 1 A. Atropine
Cardiac Pacing. Learning outcomes. Introduction. The cardiac impulse - its formation and its failure CHAPTER. To understand:
 Cardiac Pacing CHAPTER 10 Learning outcomes To understand: The indications for cardiac pacing in the peri-arrest setting How to perform percussion pacing How to apply non-invasive, transcutaneous electrical
Cardiac Pacing CHAPTER 10 Learning outcomes To understand: The indications for cardiac pacing in the peri-arrest setting How to perform percussion pacing How to apply non-invasive, transcutaneous electrical
Teaching Rounds in Cardiac Electrophysiology
 Teaching Rounds in Cardiac Electrophysiology Sustained Multiple Railroad Tracks on Implantable Cardiac Defibrillator Interval Plots Mechanisms and Management Alex Y. Tan, MD; Kenneth A. Ellenbogen, MD;
Teaching Rounds in Cardiac Electrophysiology Sustained Multiple Railroad Tracks on Implantable Cardiac Defibrillator Interval Plots Mechanisms and Management Alex Y. Tan, MD; Kenneth A. Ellenbogen, MD;
Review of Pacemakers and ICD Therapy: Overview and Patient Management
 Review of Pacemakers and ICD Therapy: Overview and Patient Management Pacing Systems Charles J. Love, MD FACC FAHA FHRS CCDS Professor of Medicine Director, Cardiac Rhythm Device Services OSU Division
Review of Pacemakers and ICD Therapy: Overview and Patient Management Pacing Systems Charles J. Love, MD FACC FAHA FHRS CCDS Professor of Medicine Director, Cardiac Rhythm Device Services OSU Division
Shock Reduction Strategies Michael Geist E. Wolfson MC
 Shock Reduction Strategies Michael Geist E. Wolfson MC Shock Therapy Thanks, I needed that! Why Do We Need To Reduce Shocks Long-term outcome after ICD and CRT implantation and influence of remote device
Shock Reduction Strategies Michael Geist E. Wolfson MC Shock Therapy Thanks, I needed that! Why Do We Need To Reduce Shocks Long-term outcome after ICD and CRT implantation and influence of remote device
SUDDEN CARDIAC DEATH(SCD): Definition
: Definition") SUDDEN CARDIAC DEATH EPIDEMIOLOGY, PATHOPHYSIOLOGY, PREVENTION & THERAPY Hasan Garan, M.D. Columbia University Medical Center SUDDEN CARDIAC DEATH(SCD): Definition DEATH DUE TO A CARDIAC CAUSE IN A CLINICALLY
SUDDEN CARDIAC DEATH EPIDEMIOLOGY, PATHOPHYSIOLOGY, PREVENTION & THERAPY Hasan Garan, M.D. Columbia University Medical Center SUDDEN CARDIAC DEATH(SCD): Definition DEATH DUE TO A CARDIAC CAUSE IN A CLINICALLY
EKG Rhythm Interpretation Exam
 as EKG Rhythm Interpretation Exam Name: Date: ID# Unit Assume each strip is a 6 second strip. Passing is 80%. 1. Identify the following rhythm: a. Asystole b. Ventricular fibrillation c. Atrial fibrillation
as EKG Rhythm Interpretation Exam Name: Date: ID# Unit Assume each strip is a 6 second strip. Passing is 80%. 1. Identify the following rhythm: a. Asystole b. Ventricular fibrillation c. Atrial fibrillation
Implantable Device Endpoints: Implications for Clinical Trial Design
 Implantable Device Endpoints: Implications for Clinical Trial Design MINTU TURAKHIA, MD MAS Associate Professor of Medicine Senior Director of Research & Innovation Center for Digital Health Stanford University
Implantable Device Endpoints: Implications for Clinical Trial Design MINTU TURAKHIA, MD MAS Associate Professor of Medicine Senior Director of Research & Innovation Center for Digital Health Stanford University
Permanent Pacemaker Implantation Post Cardiac Surgery: A Cautionary Tale
 Permanent Pacemaker Implantation Post Cardiac Surgery: A Cautionary Tale Jason Collinson & Stuart Tan Essex Cardiothoracic Centre, Basildon and Thurrock University Hospital. Contact: jason.collinson@nhs.net
Permanent Pacemaker Implantation Post Cardiac Surgery: A Cautionary Tale Jason Collinson & Stuart Tan Essex Cardiothoracic Centre, Basildon and Thurrock University Hospital. Contact: jason.collinson@nhs.net
Inappropriate ICD Discharge Related to Electrical Muscle Stimulation in Chiropractic Therapy: A Case Report
 Cardiol Ther (2017) 6:139 143 DOI 10.1007/s40119-017-0086-6 CASE REPORT Inappropriate ICD Discharge Related to Electrical Muscle Stimulation in Chiropractic Therapy: A Case Report Abhishek Shenoy. Abhishek
Cardiol Ther (2017) 6:139 143 DOI 10.1007/s40119-017-0086-6 CASE REPORT Inappropriate ICD Discharge Related to Electrical Muscle Stimulation in Chiropractic Therapy: A Case Report Abhishek Shenoy. Abhishek
Advances in Ablation Therapy for Ventricular Tachycardia
 Advances in Ablation Therapy for Ventricular Tachycardia Nitish Badhwar, MD, FACC, FHRS Director, Cardiac Electrophysiology Training Program University of California, San Francisco For those of you who
Advances in Ablation Therapy for Ventricular Tachycardia Nitish Badhwar, MD, FACC, FHRS Director, Cardiac Electrophysiology Training Program University of California, San Francisco For those of you who
Case Description A 25 years old male served in a combat unit for 3 years (GOLANY) Implantation of Dual chamber ICD in 7/2010 due to Severe Non ischemi
 Implantation of Dual chamber ICD in 7/2010 due to Severe Non ischemi") ICD Case Study tracing your own images Prof Glikson, Sandra Schor-Wider Nadav Hayman Case Description A 25 years old male served in a combat unit for 3 years (GOLANY) Implantation of Dual chamber ICD in
ICD Case Study tracing your own images Prof Glikson, Sandra Schor-Wider Nadav Hayman Case Description A 25 years old male served in a combat unit for 3 years (GOLANY) Implantation of Dual chamber ICD in
Cardiac arrhythmias. Janusz Witowski. Department of Pathophysiology Poznan University of Medical Sciences. J. Witowski
 Cardiac arrhythmias Janusz Witowski Department of Pathophysiology Poznan University of Medical Sciences A 68-year old man presents to the emergency department late one evening complaining of increasing
Cardiac arrhythmias Janusz Witowski Department of Pathophysiology Poznan University of Medical Sciences A 68-year old man presents to the emergency department late one evening complaining of increasing
CAPTIVATE SUMMARY CLINICAL SUMMARY. CAPTure Information Via Automatic Threshold Evaluation
 CLINICAL SUMMARY CAPTIVATE SUMMARY CAPTure Information Via Automatic Threshold Evaluation CAUTION: Federal law restricts this device to sale by or on the order of a physician trained or experienced in
CLINICAL SUMMARY CAPTIVATE SUMMARY CAPTure Information Via Automatic Threshold Evaluation CAUTION: Federal law restricts this device to sale by or on the order of a physician trained or experienced in
Implantable Cardioverter-Defibril. Defibrillators. Ratko Magjarević
 Implantable Cardioverter-Defibril Defibrillators Ratko Magjarević University of Zagreb Faculty of Electrical Engineering and Computing Croatia ratko.magjarevic@fer.hr Ventricular Fibrillation Ventricular
Implantable Cardioverter-Defibril Defibrillators Ratko Magjarević University of Zagreb Faculty of Electrical Engineering and Computing Croatia ratko.magjarevic@fer.hr Ventricular Fibrillation Ventricular
Arrhythmias and Heart Failure Dr Chris Lang Consultant Cardiologist and Electrophysiologist Royal Infirmary of Edinburgh
 Arrhythmias and Heart Failure Dr Chris Lang Consultant Cardiologist and Electrophysiologist Royal Infirmary of Edinburgh Arrhythmias and Heart Failure Ventricular Supraventricular VT/VF Primary prevention
Arrhythmias and Heart Failure Dr Chris Lang Consultant Cardiologist and Electrophysiologist Royal Infirmary of Edinburgh Arrhythmias and Heart Failure Ventricular Supraventricular VT/VF Primary prevention
SUDDEN CARDIAC DEATH(SCD): Definition
: Definition") SUDDEN CARDIAC DEATH EPIDEMIOLOGY, PATHOPHYSIOLOGY, PREVENTION & THERAPY Hasan Garan, M.D. Columbia University Medical Center SUDDEN CARDIAC DEATH(SCD): Definition DEATH DUE TO A CARDIAC CAUSE IN A CLINICALLY
SUDDEN CARDIAC DEATH EPIDEMIOLOGY, PATHOPHYSIOLOGY, PREVENTION & THERAPY Hasan Garan, M.D. Columbia University Medical Center SUDDEN CARDIAC DEATH(SCD): Definition DEATH DUE TO A CARDIAC CAUSE IN A CLINICALLY
Sudden death from abnormal heart rhythm: Am I at risk?
 DISCLAIMER: The views and opinions expressed in this presentation are those of the author. The slides in this presentation are prepared as talking points. It is possible that key substantive elements were
DISCLAIMER: The views and opinions expressed in this presentation are those of the author. The slides in this presentation are prepared as talking points. It is possible that key substantive elements were
ECG Cases and Questions. Ashish Sadhu, MD, FHRS, FACC Electrophysiology/Cardiology
 ECG Cases and Questions Ashish Sadhu, MD, FHRS, FACC Electrophysiology/Cardiology 32 yo female Life Insurance Physical 56 yo male with chest pain Terminology Injury ST elevation Ischemia T wave inversion
ECG Cases and Questions Ashish Sadhu, MD, FHRS, FACC Electrophysiology/Cardiology 32 yo female Life Insurance Physical 56 yo male with chest pain Terminology Injury ST elevation Ischemia T wave inversion
Need to Know: Implantable Devices. Carolyn Brown RN, MN, CCRN Education Coordinator Emory Healthcare Atlanta, Georgia
 Need to Know: Implantable Devices Carolyn Brown RN, MN, CCRN Education Coordinator Emory Healthcare Atlanta, Georgia Disclosure Statement I have no relationships to disclose. Objectives Discuss the most
Need to Know: Implantable Devices Carolyn Brown RN, MN, CCRN Education Coordinator Emory Healthcare Atlanta, Georgia Disclosure Statement I have no relationships to disclose. Objectives Discuss the most
The ECG Course. Boone County Fire Protection District EMS Education
 The ECG Course Level I G rated material AV Blocks What Causes AV Block? Long list of bad things that includes ischemia and.. Old age / disease Medications or drugs Electrolyte imbalances Physiologic Blocks
The ECG Course Level I G rated material AV Blocks What Causes AV Block? Long list of bad things that includes ischemia and.. Old age / disease Medications or drugs Electrolyte imbalances Physiologic Blocks
Tachyarrhythmia Suspicion and Detection
 Tech Corner Tachyarrhythmia Suspicion and Detection NOTE: PLEASE NOTE THAT THE FOLLOWING INFORMATION IS A GENERAL DESCRIPTION OF THE FUNCTION. DETAILS AND PARTICULAR CASES ARE NOT DESCRIBED IN THE ARTICLE.
Tech Corner Tachyarrhythmia Suspicion and Detection NOTE: PLEASE NOTE THAT THE FOLLOWING INFORMATION IS A GENERAL DESCRIPTION OF THE FUNCTION. DETAILS AND PARTICULAR CASES ARE NOT DESCRIBED IN THE ARTICLE.
SPORTS AND EXERCISE ADVICE IN PATIENTS WITH ICD AND PPM
 SPORTS AND EXERCISE ADVICE IN PATIENTS WITH ICD AND PPM Rio De Janeiro 2016 Sport and Exercise Cardiology Symposium SBC/SOCERJ ACC Sharlene M. Day, MD Associate Professor, Cardiovascular Medicine Director,
SPORTS AND EXERCISE ADVICE IN PATIENTS WITH ICD AND PPM Rio De Janeiro 2016 Sport and Exercise Cardiology Symposium SBC/SOCERJ ACC Sharlene M. Day, MD Associate Professor, Cardiovascular Medicine Director,
-RHYTHM PRACTICE- By Dr.moanes Msc.cardiology Assistant Lecturer of Cardiology Al Azhar University. OBHG Education Subcommittee
 -RHYTHM PRACTICE- By Dr.moanes Msc.cardiology Assistant Lecturer of Cardiology Al Azhar University The Normal Conduction System Sinus Node Normal Sinus Rhythm (NSR) Sinus Bradycardia Sinus Tachycardia
-RHYTHM PRACTICE- By Dr.moanes Msc.cardiology Assistant Lecturer of Cardiology Al Azhar University The Normal Conduction System Sinus Node Normal Sinus Rhythm (NSR) Sinus Bradycardia Sinus Tachycardia
Do All Patients With An ICD Indication Need A BiV Pacing Device?
 Do All Patients With An ICD Indication Need A BiV Pacing Device? Muhammad A. Hammouda, MD Electrophysiology Laboratory Department of Critical Care Medicine Cairo University Etiology and Pathophysiology
Do All Patients With An ICD Indication Need A BiV Pacing Device? Muhammad A. Hammouda, MD Electrophysiology Laboratory Department of Critical Care Medicine Cairo University Etiology and Pathophysiology
PATIENT WITH ARRHYTHMIA IN DENTIST S OFFICE. Małgorzata Kurpesa, MD., PhD. Chair&Department of Cardiology
 PATIENT WITH ARRHYTHMIA IN DENTIST S OFFICE Małgorzata Kurpesa, MD., PhD. Chair&Department of Cardiology Medical University of Łódź The heart is made up of four chambers Left Atrium Right Atrium Left Ventricle
PATIENT WITH ARRHYTHMIA IN DENTIST S OFFICE Małgorzata Kurpesa, MD., PhD. Chair&Department of Cardiology Medical University of Łódź The heart is made up of four chambers Left Atrium Right Atrium Left Ventricle
John H. Ip, M.D FACC Associate Professor of Medicine Michigan State University Medical Director, EP Service
 ICD Trouble shooting: Case study John H. Ip, M.D FACC Associate Professor of Medicine Michigan State University Medical Director, EP Service Bullet proof evidence: ICD does prevent sudden death Disclosures
ICD Trouble shooting: Case study John H. Ip, M.D FACC Associate Professor of Medicine Michigan State University Medical Director, EP Service Bullet proof evidence: ICD does prevent sudden death Disclosures
Device Update Implantable Cardioverter Defibrillator (ICD) 박상원
 박상원") 2012 년춘계학술대회 Device Update Implantable Cardioverter Defibrillator (ICD) 박상원 Arrhythmia Center, KUMC www.korea-heartrhythm.com Korea University Medical Center Seoul, Korea The Development of ICD by a team
2012 년춘계학술대회 Device Update Implantable Cardioverter Defibrillator (ICD) 박상원 Arrhythmia Center, KUMC www.korea-heartrhythm.com Korea University Medical Center Seoul, Korea The Development of ICD by a team
Emergency Cardiovascular Care: EMT-Intermediate Treatment Algorithms. Introduction to the Algorithms
 Emergency Cardiovascular Care: EMT-Intermediate Treatment Algorithms Introduction to the Algorithms Cardiac Arrest Algorithms Prehospital Medication Profiles Perspective regarding the EMT- Intermediate
Emergency Cardiovascular Care: EMT-Intermediate Treatment Algorithms Introduction to the Algorithms Cardiac Arrest Algorithms Prehospital Medication Profiles Perspective regarding the EMT- Intermediate
CONTAK RENEWAL 3 AVT CLINICAL SUMMARY
 CAUTION: Federal law restricts this device to sale by or on the order of a physician trained or experienced in device implant and follow-up procedures. CLINICAL SUMMARY CONTAK RENEWAL 3 AVT Boston Scientific
CAUTION: Federal law restricts this device to sale by or on the order of a physician trained or experienced in device implant and follow-up procedures. CLINICAL SUMMARY CONTAK RENEWAL 3 AVT Boston Scientific
The ARREST Trial: Amiodarone for Resuscitation After Out-of-Hospital Cardiac Arrest Due to Ventricular Fibrillation
 The ARREST Trial: Amiodarone for Resuscitation After Out-of-Hospital Cardiac Arrest Due to Ventricular Fibrillation Introduction The ARREST (Amiodarone in out-of-hospital Resuscitation of REfractory Sustained
The ARREST Trial: Amiodarone for Resuscitation After Out-of-Hospital Cardiac Arrest Due to Ventricular Fibrillation Introduction The ARREST (Amiodarone in out-of-hospital Resuscitation of REfractory Sustained
Advanced ICD Concepts
 1 4 2 5 7 3 6 8 Advanced ICD Concepts This presentation is provided with the understanding that the slide content must not be altered in any manner as the content is subject to FDA regulations. This presentation
1 4 2 5 7 3 6 8 Advanced ICD Concepts This presentation is provided with the understanding that the slide content must not be altered in any manner as the content is subject to FDA regulations. This presentation
A Prospective Study Comparing the Sensed R Wave in Bipolar and Extended Bipolar Configurations: The PropR Study
 A Prospective Study Comparing the Sensed R Wave in Bipolar and Extended Bipolar Configurations: The PropR Study ANEESH V. TOLAT, M.D.,* MELISSA WOICIECHOWSKI, M.S.N.,* ROSEMARIE KAHR, R.C.I.S.,* JOSEPH
A Prospective Study Comparing the Sensed R Wave in Bipolar and Extended Bipolar Configurations: The PropR Study ANEESH V. TOLAT, M.D.,* MELISSA WOICIECHOWSKI, M.S.N.,* ROSEMARIE KAHR, R.C.I.S.,* JOSEPH
ECG S: A CASE-BASED APPROACH December 6,
 ECG S: A CASE-BASED APPROACH December 6, 2018 1 Faculty Disclosure Faculty: Lorne Gula MD, FRCPC Professor, Western University Cardiologist, Hearth Rhythm Specialist Director, Electrophysiology Laboratory,
ECG S: A CASE-BASED APPROACH December 6, 2018 1 Faculty Disclosure Faculty: Lorne Gula MD, FRCPC Professor, Western University Cardiologist, Hearth Rhythm Specialist Director, Electrophysiology Laboratory,
2) Heart Arrhythmias 2 - Dr. Abdullah Sharif
 Heart Arrhythmias 2 - Dr. Abdullah Sharif") 2) Heart Arrhythmias 2 - Dr. Abdullah Sharif Rhythms from the Sinus Node Sinus Tachycardia: HR > 100 b/m Causes: o Withdrawal of vagal tone & Sympathetic stimulation (exercise, fight or flight) o Fever
2) Heart Arrhythmias 2 - Dr. Abdullah Sharif Rhythms from the Sinus Node Sinus Tachycardia: HR > 100 b/m Causes: o Withdrawal of vagal tone & Sympathetic stimulation (exercise, fight or flight) o Fever
Subcutaneous Implantable Cardioverter Defibrillator (S-ICD)
") Subcutaneous Implantable Cardioverter Defibrillator (S-ICD) D. D. MANOLATOS, MD, PhD, FESC Electrophysiology and Device Lab General Hospital Evangelismos, Athens The Problem: 300,000 people die each year
Subcutaneous Implantable Cardioverter Defibrillator (S-ICD) D. D. MANOLATOS, MD, PhD, FESC Electrophysiology and Device Lab General Hospital Evangelismos, Athens The Problem: 300,000 people die each year
Friedman, Rott, Wokhlu, Asirvatham, Hayes 201. Figure 65.7 Shortening of the AV interval during pacing.
 Friedman, Rott, Wokhlu, Asirvatham, Hayes 201 Figure.7 Shortening of the AV interval during pacing. 202 A Case-Based Approach to Pacemakers, ICDs, and Cardiac Resynchronization Figure.8 is obtained from
Friedman, Rott, Wokhlu, Asirvatham, Hayes 201 Figure.7 Shortening of the AV interval during pacing. 202 A Case-Based Approach to Pacemakers, ICDs, and Cardiac Resynchronization Figure.8 is obtained from
Inappropriate electrical shocks: Tackling the beast
 ESC Paris 2011 Inappropriate electrical shocks: Tackling the beast Gerhard Hindricks University of Leipzig Heart Center Dept. of Electrophysiology ESC Paris 2011 Inappropriate electrical shocks: Tackling
ESC Paris 2011 Inappropriate electrical shocks: Tackling the beast Gerhard Hindricks University of Leipzig Heart Center Dept. of Electrophysiology ESC Paris 2011 Inappropriate electrical shocks: Tackling
Arrhythmia Study Guide 3 Junctional and Ventricular Rhythms
 Arrhythmia Study Guide 3 Junctional and Ventricular Rhythms JUNCTIONAL RHYTHMS The AV Junction (Bundle of His and surrounding cells) only acts as pacemaker of the heart when the SA Node is not firing normally
Arrhythmia Study Guide 3 Junctional and Ventricular Rhythms JUNCTIONAL RHYTHMS The AV Junction (Bundle of His and surrounding cells) only acts as pacemaker of the heart when the SA Node is not firing normally
Assessment of Defibrillation Threshold upon Implantable Cardioverter-Defibrillator implant in Relation to patient s prognosis
 Assessment of Defibrillation Threshold upon Implantable Cardioverter-Defibrillator implant in Relation to patient s prognosis Investigator: Keiko Saito, MD Mentor: Yuji Saito, MD, PhD, FACP, FACC Department
Assessment of Defibrillation Threshold upon Implantable Cardioverter-Defibrillator implant in Relation to patient s prognosis Investigator: Keiko Saito, MD Mentor: Yuji Saito, MD, PhD, FACP, FACC Department
4/14/15 HTEC 91. Topics for Today. Guess That Rhythm. Premature Ventricular Contractions (PVCs) Ventricular Rhythms
 Ventricular Rhythms") 4/14/15 Topics for Today HTEC 91 Medical Office Diagnostic Tests Week 5 Ventricular Rhythms PVCs: Premature Ventricular Contractions VT: Ventricular Tachycardia VF: Ventricular Fibrillation Asystole Study
4/14/15 Topics for Today HTEC 91 Medical Office Diagnostic Tests Week 5 Ventricular Rhythms PVCs: Premature Ventricular Contractions VT: Ventricular Tachycardia VF: Ventricular Fibrillation Asystole Study
Implantable Cardioverter Defibrillator (ICD)
") Medical Coverage Policy Effective Date... 3/15/2018 Next Review Date... 3/15/2019 Coverage Policy Number... 0181 Implantable Cardioverter Defibrillator (ICD) Table of Contents Related Coverage Resources
Medical Coverage Policy Effective Date... 3/15/2018 Next Review Date... 3/15/2019 Coverage Policy Number... 0181 Implantable Cardioverter Defibrillator (ICD) Table of Contents Related Coverage Resources
IHCP bulletin INDIANA HEALTH COVERAGE PROGRAMS BT JANUARY 24, 2012
 IHCP bulletin INDIANA HEALTH COVERAGE PROGRAMS BT201203 JANUARY 24, 2012 The IHCP to reimburse implantable cardioverter defibrillators separately from outpatient implantation Effective March 1, 2012, the
IHCP bulletin INDIANA HEALTH COVERAGE PROGRAMS BT201203 JANUARY 24, 2012 The IHCP to reimburse implantable cardioverter defibrillators separately from outpatient implantation Effective March 1, 2012, the
Seek and Ye Shall Find: Surprising Findings When Using the ILR-LINQ
 Seek and Ye Shall Find: Surprising Findings When Using the ILR-LINQ Suneet Mittal, MD, FACC, FHRS Director, Electrophysiology Laboratory Valley Health System www.arrhythmia.org; @drsuneet October 31, 2015
Seek and Ye Shall Find: Surprising Findings When Using the ILR-LINQ Suneet Mittal, MD, FACC, FHRS Director, Electrophysiology Laboratory Valley Health System www.arrhythmia.org; @drsuneet October 31, 2015
The implantable cardioverter defibrillator is not enough: Ventricular Tachycardia Catheter Ablation in Patients with Structural Heart Disease
 The implantable cardioverter defibrillator is not enough: Ventricular Tachycardia Catheter Ablation in Patients with Structural Heart Disease Paolo Della Bella, MD Arrhythmia Department and Clinical Electrophysiology
The implantable cardioverter defibrillator is not enough: Ventricular Tachycardia Catheter Ablation in Patients with Structural Heart Disease Paolo Della Bella, MD Arrhythmia Department and Clinical Electrophysiology
Paroxysmal Supraventricular Tachycardia PSVT.
 Atrial Tachycardia; is the name for an arrhythmia caused by a disorder of the impulse generation in the atrium or the AV node. An area in the atrium sends out rapid signals, which are faster than those
Atrial Tachycardia; is the name for an arrhythmia caused by a disorder of the impulse generation in the atrium or the AV node. An area in the atrium sends out rapid signals, which are faster than those
McHenry Western Lake County EMS System Optional CE for EMT-B, Paramedics and PHRN s Bradycardia and Treatments Optional #7 2018
 McHenry Western Lake County EMS System Optional CE for EMT-B, Paramedics and PHRN s Bradycardia and Treatments Optional #7 2018 This month we will be looking at a specific ECG Rhythm and its treatments
McHenry Western Lake County EMS System Optional CE for EMT-B, Paramedics and PHRN s Bradycardia and Treatments Optional #7 2018 This month we will be looking at a specific ECG Rhythm and its treatments
Advanced ICD Troubleshooting: Part II REVIEW
 REVIEW Advanced ICD Troubleshooting: Part II CHARLES D. SWERDLOW* and PAUL A. FRIEDMAN From the *Cedars-Sinai Medical Center, Los Angeles, California, and Mayo Clinic, Rochester, Minnesota, USA Failure
REVIEW Advanced ICD Troubleshooting: Part II CHARLES D. SWERDLOW* and PAUL A. FRIEDMAN From the *Cedars-Sinai Medical Center, Los Angeles, California, and Mayo Clinic, Rochester, Minnesota, USA Failure
Defibrillation threshold testing should no longer be performed: contra
 Defibrillation threshold testing should no longer be performed: contra Andreas Goette St. Vincenz-Hospital Paderborn Dept. of Cardiology and Intensive Care Medicine Germany No conflict of interest to disclose
Defibrillation threshold testing should no longer be performed: contra Andreas Goette St. Vincenz-Hospital Paderborn Dept. of Cardiology and Intensive Care Medicine Germany No conflict of interest to disclose
Etienne Aliot. University of Nancy - France
 Etienne Aliot University of Nancy - France Disclosures Consulting fees : - Bayer, Boehringer Ingelheim,GSK, MedaPharma, Pfizer/BMS,Sanofi Aventis. - Biotronik,Medtronic,St Jude Medical. Electrical vs Pharmacological
Etienne Aliot University of Nancy - France Disclosures Consulting fees : - Bayer, Boehringer Ingelheim,GSK, MedaPharma, Pfizer/BMS,Sanofi Aventis. - Biotronik,Medtronic,St Jude Medical. Electrical vs Pharmacological
ΔΠΔΜΒΑΣΙΚΗ ΘΔΡΑΠΔΙΑ ΚΟΙΛΙΑΚΩΝ ΑΡΡΤΘΜΙΩΝ
 ΔΠΔΜΒΑΣΙΚΗ ΘΔΡΑΠΔΙΑ ΚΟΙΛΙΑΚΩΝ ΑΡΡΤΘΜΙΩΝ ΣΔΛΙΟ ΠΑΡΑΚΔΤΑÏΓΗ ΓΙΔΤΘΤΝΣΗ ΔΤ Α Καρδιολογική Κλινική ΑΠΘ, Νοζοκομείο ΑΧΕΠΑ, Θεζζαλονίκη NO CONFLICT OF INTEREST INTRODUCTION Sustained VT is an important cause
ΔΠΔΜΒΑΣΙΚΗ ΘΔΡΑΠΔΙΑ ΚΟΙΛΙΑΚΩΝ ΑΡΡΤΘΜΙΩΝ ΣΔΛΙΟ ΠΑΡΑΚΔΤΑÏΓΗ ΓΙΔΤΘΤΝΣΗ ΔΤ Α Καρδιολογική Κλινική ΑΠΘ, Νοζοκομείο ΑΧΕΠΑ, Θεζζαλονίκη NO CONFLICT OF INTEREST INTRODUCTION Sustained VT is an important cause
Temporary pacemaker 삼성서울병원 심장혈관센터심장검사실 박정왜 RN, CCDS
 Temporary pacemaker 삼성서울병원 심장혈관센터심장검사실 박정왜 RN, CCDS NBG Codes 1st Letter 2nd Letter 3rd Letter A V D Chamber(s) Paced = atrium = ventricle = dual (both atrium and ventricle) Chamber(s) Sensed A = atrium
Temporary pacemaker 삼성서울병원 심장혈관센터심장검사실 박정왜 RN, CCDS NBG Codes 1st Letter 2nd Letter 3rd Letter A V D Chamber(s) Paced = atrium = ventricle = dual (both atrium and ventricle) Chamber(s) Sensed A = atrium