FEVAR FIFTEEN YEARS OF EFFICIENCY E.DUCASSE MD PHD FEBVS CHU DE BORDEAUX
|
|
|
- Carol Stone
- 5 years ago
- Views:
Transcription


1 FEVAR FIFTEEN YEARS OF EFFICIENCY E.DUCASSE MD PHD FEBVS CHU DE BORDEAUX 2018




2

3 A BIT OF HISTORY First use of F-EVAR : 1990s Park et al. J Vasc Interv Radiol. 1996;7: Faruqi et al. J Endovasc Surg. 1999;6: Browne et al. Eur J Vasc Endovasc Surg. 1999;18: Kinney et al. J Endovasc Ther. 2000;7: First series of patients from Australia : 2001 Anderson et al. J Endovasc Ther. 2001;8:3-15. Early experience in the US with physician-sponsored (PS)-IDE trials : 2005 Much of procedural protocols, device enhancements, and understanding of device and repair durability have arisen from these assessments Roy Greenberg and the Cleveland Clinic First fenestrated endograft : 2001 more rudimentary than those employed in the US ZFEN clinical trial, as they lacked reinforced fenestrations First report : 2004 (22 patients) Greenberg et al. J Vasc Surg. 2004;39: Second report : 2006 (119 patients, 302 renal and visceral vessels) O Neill et al. Eur J Vasc Endovasc Surg. 2006;32: April 2012 : FDA approval of the ZFEN system (Cook Medical) in the US for short infrarenal necks (4 14 mm) Long-term results : 2015 (607 patients with a mean follow-up of 8 years) Mastracci et al. Twelve-year results. J Vasc Surg. 2015;61:
 Postoperative permanent dialysis 1 1.00 (95%CI: 0.99-1.01) BUT Transient renal failure 0.03 1.06 (95%CI: 1.01-1.12) Early reintervention 0.0001 0.87 (95%CI: 0.83-0.")
4 MAIN RESULTS : VS OSR No randomised studies were identified F-EVAR 8 cohort studies 368 patients OSR 12 cohort studies 1164 patients OSR vs F-EVAR P value RR 30-day mortality 2% (95%CI: ) Postoperative permanent dialysis (95%CI: ) BUT Transient renal failure (95%CI: ) Early reintervention (95%CI: )
5 MAIN RESULTS : VS OSR OSR and F-EVAR are offered to different population targets may be secondary to the selection bias of F-EVAR being offered to high-risk patients?
6 MAIN RESULTS : VS OSR

7 GLOBALSTAR F-EVAR UK Multicentric study (14) Retrospective January 2007-December patients Median FU : 6 months Technical success 99% 30-day mortality 4.1% F-EVAR 85% 94% 91% 89% Survival 1y 2y 3y 30% Reinterventions 3y Patency 3y


 patients had sac enlargement associated")
8 F-EVAR French Multicenter Restrospective 403 visceral vessels Patency 97% May 2004-January patients Median FU : 15 months 1 intraoperative conversion to OSR F-EVAR 30-day mortality 2% Reinterventions 6 to correct EL 93% 1y 86% 2y 12 Survival No rupture F-EVAR Transient Dialysis 3% (4) Permanent Dialysis 1% (2) >5 mm 1y 2y 3y 3 (4%) patients had sac enlargement associated with a persistent EL


9 F-EVAR IDE protocole Retrospective study In a tertiary referral centre November 2001-April patients Median FU : 24 months Technical success 1 intraoperative conversion to OSR 3 target vessel occlusions F-EVAR 97% 30-day mortality 1% Reinterventions 9% (11) Patency 93% Survival 90% No rupture 84% 59% 1y 2y 5y serum creat. clear. >30% F-EVAR 25 Dialysis 2 stent occlusions all occurred within the first 2y (4 stent fractures 3 occlusions) 5y
10 F-EVAR US Multicenter (14) Prospective patients Mean FU : 37 months F-EVAR Technical success 100% 30-day mortality 1.5% Migration >10mm 3% Reinterventions 11 to correct target vessel stenosis/occlusion 4 to correct EL Freedom from MAEs 22% (15) 79% 5y Survival 91% No rupture 178 visceral vessels Patency F-EVAR Occlusion 3% (4) Stenosis 9% (12) Freedom from AKI 100% Despite 10% of radiographic evidence of renal embolization 97% 81% 5y
11 607 patients
12 20% Overall Survival 8 years With 2% aortic-related mortality Worse survival for patients requiring Celiac Fen


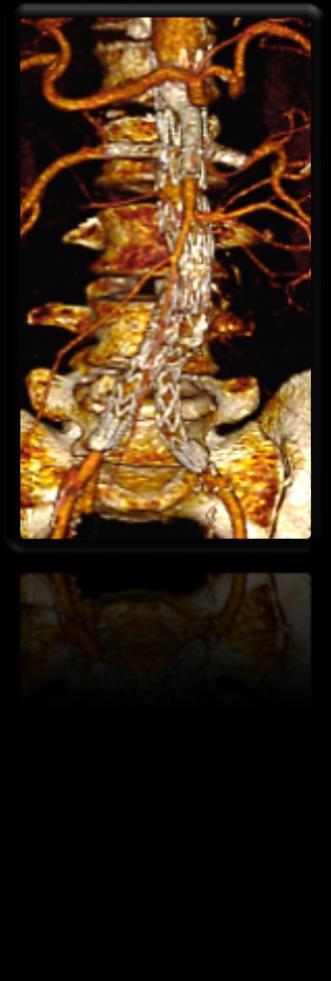
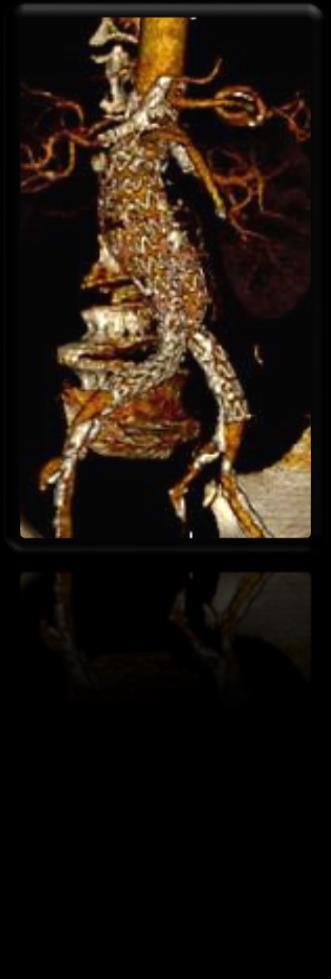
13 OVER TIME: Celiac fen configurations Celiac scallop configurations BUT ALSO: 2 renal fen + SMA scallop configurations

14 OVERALL Technical failure inadequate device design suboptimal procedure planning 30-day mortality Overall Survival Outcome measures after F-EVAR % in specialized centers 1-3% in specialized centers 3y 5y 10y Minimally invasive No laparotomy No suprarenal cross-clamping Long-term Results are now reported And they are mostly GOOD in specialized centers Aneurysm related death 10y But Expertice is of paramount importance Covered bridging stent use was associated with a lower rate of renal artery 1y Target vessel patency stenosis compared to bare-metal stents 5y Failed cannulation or Stent stenosis/occlusion can be catastrophic Postop BUT Excellent renal impairment However, results were there reported was no difference at the Cleveland 0-29% in branch Clinic vessel occlusion rates Death Secondary Need for hemodialysis procedures divided equally between 0-6% restenosis/occlusion and Renal function deterioration EL development This has led to the primary use of covered stents when performing F-EVAR, Type I EL 3% transient/permanent dialysis 0.6% regardless of celiac arteries of the need to obtain a seal with the fenestration at that location Bowel ischemia Type II EL 4% of SMA 16% 6% of right renal arteries Type III EL 5% of left renal arteries 4.6% Freedom from branch reintervention : 5y 1y This requires an active surveillance program in order to Aneurysm diameter decrease 5 mm 3y identify stented branch vessels at risk for failure Mastracci et al. J Vasc Surg. 2013;57: y Migration 10 mm 1-7% Revised duplex criteria are necessary in F-EVAR given the hemodynamic alterations induced by adding stiff stent systems 29% EL related PSV to >280 cm/sec to identify 60-99% renal artery Reinterventions 26% target vessel stenosis related 13% graft limb related improved Se (93%), Sp (100%) and PPV/NPV (99%) Mohabbat et al. J Vasc Surg. 2009;49:

15 OVERALL Technical failure inadequate device design suboptimal procedure planning 30-day mortality Overall Survival Aneurysm related death Target vessel patency Postop renal impairment Need for hemodialysis Type I EL 3% Type II EL 16% Outcome measures after F-EVAR % in specialized centers 1-3% in specialized centers 3y 5y 10y 10y 1y 5y 0-29% 0-6% Type III EL 4.6% 1y Aneurysm One of the diameter greatest decrease concerns 5 mm : 3y Manipulation and stenting of the renal arteries 5y Use of iodinated contrast during the procedure and repeated FU imaging Migration 10 mm 1-7% However, similar rates have been observed after 29% EL OSR related and EVAR Reinterventions 26% target vessel related Martin-Gonzalez et al. J Vasc Surg. 2015;62: % graft limb related 16% of patients without preoperative renal insufficiency 39% of those with chronic renal disease incidence of permanent dialysis mortality. egfr stabilize within 6months of index surgery with a Mastracci et al. J Vasc Surg. 2015;61:
16 OVERALL Technical failure inadequate device design suboptimal procedure planning 30-day mortality Overall Survival Aneurysm related death Target vessel patency Postop renal impairment Need for hemodialysis Outcome measures after F-EVAR % in specialized centers 1-3% in specialized centers 3y 5y 10y 10y 1y 5y 0-29% 0-6% Type I EL 3% Longevity of the repair? Type F-EVAR II EL requires more re-interventions in the 16% long-term vs OSR 12.7% vs 4.9%, p < Type III EL 4.6% Poor patient seletion Disease progression +++ 1y Aneurysm diameter 2-3% will decrease develop a 5 mm proximal type I EL 64% given 3y enough time 5y O Callaghan et al. J Vasc Surg. 2015;61: possible ( 15-mm) Migration 10 mm 1-13% Reinterventions 29% EL related 26% target vessel related 13% graft limb related type I EL in patients receiving device configurations with only renal fenestrations We first attempted to treat patients with the shortest amount of coverage We now search for Higher sealing zones A high % of ELs eventually require redo operations As aneurysms become more complex the rates of reintervention appear to over time Currently, we attempt to achieve a 2- to 3-cm landing zone when extending a repair into the visceral aortic segment while balancing the risks of developing other complications such as spinal cord ischemia Mastracci et al. J Vasc Surg. 2015;61: Eagleton et al. J Vasc Surg. 2016;63:


17 OVERALL Technical failure inadequate device design suboptimal procedure planning 30-day mortality Overall Survival Aneurysm related death Outcome measures after F-EVAR % in specialized centers 1-3% in specialized centers 3y 5y 10y 10y 1y Target Most of vessel these patency patients had < 2-stent 5y Postop An algorithm renal impairment was developed to assess the risk 0-29% of potential component separation Need for hemodialysis 0-6% Type It I EL predicted the maximum amount of possible 3% intercomponent movement thereby deriving the minimum overlap required Type II EL 16% Type A new III EL baseline at attempting to achieve three- 4.6% to four-stent overlap was determined 1y Aneurysm Dowdall et diameter al. Eur J Vasc decrease Endovasc 5 mm Surg. 2008;36:2-9. 3y 5y Migration 10 mm 1-13% Reinterventions 29% EL related 26% target vessel related 13% graft limb related Risk of Target vessel/limb stent crushing and occlusion Rupture

 3/ Target vessel small diameter ( 5mm) 4/ Close proximity of SMA and highest renal ( 15mm) 5/ Prior aortic reconstruction anastomotic")
18 BUT. A lot of Patient remain uneligible for CM F-EVAR : Elective only (6-8 weeks delay) NOT FOR Life threatening aneurysms : Rapidly expanding Symptomatic / Ruptured Diameter 70mm* Limited availability & Elevated cost Requires Advanced endovascular skills Learning curve during which deaths because of technical errors or intraoperative complications are not uncommon Only available in expert centers REQUIRES Favorable anatomy, NOT FOR: 1/ Hostile iliac access 20/22 Fr sheaths = minimum 7.7/8.5 mm outer diameter 2/ Caudal-directed renal arteries ( -30 ) 3/ Target vessel small diameter ( 5mm) 4/ Close proximity of SMA and highest renal ( 15mm) 5/ Prior aortic reconstruction anastomotic pseudo-aneurysm or type Ia EL 6/ Tortuous aortic neck (> 45 ) 7/ Outcomes strongly correlated to the level and proximal extension of aneurysm disease poorer long-term outcomes with a device that requires coverage above the celiac artery
19 TAKE HOME MESSAGE Available results in specialized centers clearly demonstrate successful use of F-EVAR More complex designs Lower rates of type I EL 98% freedom from aneurysm-related mortality BUT higher rates of reintervention F-EVAR is still in its early phases even though it has the longest reported outcomes compared to other endovascular strategies in JRAs The current FDA-approved device has limitations and many patients still cannot be treated at this time There is the need for more advanced devices easier to use allowing for the incorporation of more visceral vessels and more cephalad extension for improved durability with the same efficacy and safety of use Failure modes are better understood, but in the light of recent findings related to the long-term outcome of infrarenal EVAR, defining the longterm outcome of F-EVAR should remain a priority


20 THANK YOU FOR YOUR ATTENTION
ChEVAR Vs. fevar for juxtarenal Aneurysm. E.Ducasse MD PhD FEVBS Unit of vascular surgery CHU bordeaux
 ChEVAR Vs. fevar for juxtarenal Aneurysm E.Ducasse MD PhD FEVBS Unit of vascular surgery CHU bordeaux CH-EVAR VS. F-EVAR IN JAAAs Meta-analysis, 2001-2012 5 CH-EVAR studies (94 patients, 151 target vessels)
ChEVAR Vs. fevar for juxtarenal Aneurysm E.Ducasse MD PhD FEVBS Unit of vascular surgery CHU bordeaux CH-EVAR VS. F-EVAR IN JAAAs Meta-analysis, 2001-2012 5 CH-EVAR studies (94 patients, 151 target vessels)
Associate Professor Walter W. Buckley Endowed Chair in Research Cleveland Clinic Lerner College of Medicine-CWRU. Houston Aortic Symposium 2017
 Matthew J. Eagleton, MD Associate Professor Walter W. Buckley Endowed Chair in Research Cleveland Clinic Lerner College of Medicine-CWRU Houston Aortic Symposium 2017 Aortica: Advisory Board Centerline
Matthew J. Eagleton, MD Associate Professor Walter W. Buckley Endowed Chair in Research Cleveland Clinic Lerner College of Medicine-CWRU Houston Aortic Symposium 2017 Aortica: Advisory Board Centerline
The Ventana Off-the-Shelf Graft for Pararenal AAA. Andrew Holden Associate Professor of Radiology Auckland Hospital
 The Ventana Off-the-Shelf Graft for Pararenal AAA Andrew Holden Associate Professor of Radiology Auckland Hospital Disclosures Andrew Holden, MBChB, FRANZCR Investigator in Nellix and Ventana Trials Clinical
The Ventana Off-the-Shelf Graft for Pararenal AAA Andrew Holden Associate Professor of Radiology Auckland Hospital Disclosures Andrew Holden, MBChB, FRANZCR Investigator in Nellix and Ventana Trials Clinical
COMBINED TECHNIQUE CHIMNEY + FENESTRATED ENDOGRAFT FOR COMPLEX ANEURYSMS ERIC DUCASSE - MD PHD FEVBS CHU BORDEAUX
 COMBINED TECHNIQUE CHIMNEY + FENESTRATED ENDOGRAFT FOR COMPLEX ANEURYSMS ERIC DUCASSE - MD PHD FEVBS CHU BORDEAUX DISCLOSURE SPEAKER NAME: PR. E. DUCASSE I HAVE THE FOLLOWING POTENTIAL CONFLICTS OF INTEREST
COMBINED TECHNIQUE CHIMNEY + FENESTRATED ENDOGRAFT FOR COMPLEX ANEURYSMS ERIC DUCASSE - MD PHD FEVBS CHU BORDEAUX DISCLOSURE SPEAKER NAME: PR. E. DUCASSE I HAVE THE FOLLOWING POTENTIAL CONFLICTS OF INTEREST
Robert F. Cuff, MD FACS SHMG Vascular Surgery
 Robert F. Cuff, MD FACS SHMG Vascular Surgery Objectives To become familiar with the commercially available fenestrated EVAR graft Discuss techniques to increase success Review available data to determine
Robert F. Cuff, MD FACS SHMG Vascular Surgery Objectives To become familiar with the commercially available fenestrated EVAR graft Discuss techniques to increase success Review available data to determine
Aortic Neck Issues Associated Clinical Sequelae/Implications for Graft Choice
 Aortic Neck Issues Associated Clinical Sequelae/Implications for Graft Choice Eric Verhoeven, MD, PhD, A. Katsargyris, MD Department of Vascular and Endovascular Surgery, Paracelsus Medical University,
Aortic Neck Issues Associated Clinical Sequelae/Implications for Graft Choice Eric Verhoeven, MD, PhD, A. Katsargyris, MD Department of Vascular and Endovascular Surgery, Paracelsus Medical University,
for Thoracoabdominal Aneurysms
 Durability of F/BEVAR for Thoracoabdominal Aneurysms Athanasios Katsargyris, MD, Eric Verhoeven MD, PhD Department of Vascular and Endovascular Surgery Paracelsus Medical University, Nuremberg, Germany
Durability of F/BEVAR for Thoracoabdominal Aneurysms Athanasios Katsargyris, MD, Eric Verhoeven MD, PhD Department of Vascular and Endovascular Surgery Paracelsus Medical University, Nuremberg, Germany
Treatment options of late failures of EVAS. Michel Reijnen Rijnstate Arnhem The Netherlands
 Treatment options of late failures of EVAS Michel Reijnen Rijnstate Arnhem The Netherlands Disclosure Speaker name: Michel Reijnen I have the following potential conflicts of interest to report: Consulting
Treatment options of late failures of EVAS Michel Reijnen Rijnstate Arnhem The Netherlands Disclosure Speaker name: Michel Reijnen I have the following potential conflicts of interest to report: Consulting
Lessons learned from Ch-EVAR for the treatment of. Miltos Matsagkas MD, PhD, FEBVS Professor of Vascular Surgery University of Thessaly
 Lessons learned from Ch-EVAR for the treatment of pararenal AAAs Miltos Matsagkas MD, PhD, FEBVS Professor of Vascular Surgery University of Thessaly Ch-EVAR Ch-EVAR = Chimney-EVAR Placement of single
Lessons learned from Ch-EVAR for the treatment of pararenal AAAs Miltos Matsagkas MD, PhD, FEBVS Professor of Vascular Surgery University of Thessaly Ch-EVAR Ch-EVAR = Chimney-EVAR Placement of single
Disclosures. EVAR follow-up: actual recommendation. EVAR follow-up: critical issues
 Disclosures is it time to discuss individualized follow-up schemes based on preoperative anatomy and high quality completion angiography? Consultant / Speaker / Proctor Cook Cordis Medtronic Invatec W.L.
Disclosures is it time to discuss individualized follow-up schemes based on preoperative anatomy and high quality completion angiography? Consultant / Speaker / Proctor Cook Cordis Medtronic Invatec W.L.
GORE EXCLUDER AAA Endoprosthesis demonstrates long-term durability. Michel Reijnen Rijnstate Hospital Arnhem, The Netherlands
 GORE EXCLUDER AAA Endoprosthesis demonstrates long-term durability Michel Reijnen Rijnstate Hospital Arnhem, The Netherlands Disclosure Speaker name: Michel Reijnen I have the following potential conflicts
GORE EXCLUDER AAA Endoprosthesis demonstrates long-term durability Michel Reijnen Rijnstate Hospital Arnhem, The Netherlands Disclosure Speaker name: Michel Reijnen I have the following potential conflicts
Conflicts of Interest. When and Why Complex EVAR in Tx of juxta/suprarenal AAA? Summary. Infrarenal EVAR for short necks 2y postop
 When and Why Complex EVAR in Tx of juxta/suprarenal AAA? Tim Resch MD Vascular Center Skane University Hospital Conflicts of Interest COOK Medical - Consulting, Speakers Bureau, IP, Research support Medtronic
When and Why Complex EVAR in Tx of juxta/suprarenal AAA? Tim Resch MD Vascular Center Skane University Hospital Conflicts of Interest COOK Medical - Consulting, Speakers Bureau, IP, Research support Medtronic
My personal experience with INCRAFT in standard and challenging cases
 My personal experience with INCRAFT in standard and challenging cases G Pratesi, MD Vascular Surgery University of Rome Tor Vergata giovanni.pratesi@uniroma2.it Disclosure Speaker name: Giovanni Pratesi,
My personal experience with INCRAFT in standard and challenging cases G Pratesi, MD Vascular Surgery University of Rome Tor Vergata giovanni.pratesi@uniroma2.it Disclosure Speaker name: Giovanni Pratesi,
Outcome of the target vessels in endovascular TAAA repair Case #1
 Outcome of the target vessels in endovascular TAAA repair Case #1 Nuno Dias Paris Endovascular Aortic Course Paris, 2018-05-31 7.5 cm Type IV TAAA T-branch 1 month Postoperative CT 2.5 months Postoperatively
Outcome of the target vessels in endovascular TAAA repair Case #1 Nuno Dias Paris Endovascular Aortic Course Paris, 2018-05-31 7.5 cm Type IV TAAA T-branch 1 month Postoperative CT 2.5 months Postoperatively
Endoleaks after F-BEVAR How to Assess & Treat? Gustavo S. Oderich, MD Mayo Clinic Rochester, MN
 Endoleaks after F-BEVAR How to Assess & Treat? Gustavo S. Oderich, MD Mayo Clinic Rochester, MN FACULTY DISCLOSURE Gustavo S. Oderich MD Consulting, DSMB, CEC* Cook Medical Inc., WL Gore, Lombardi Honoraria
Endoleaks after F-BEVAR How to Assess & Treat? Gustavo S. Oderich, MD Mayo Clinic Rochester, MN FACULTY DISCLOSURE Gustavo S. Oderich MD Consulting, DSMB, CEC* Cook Medical Inc., WL Gore, Lombardi Honoraria
Endovascular Treatment of the Aorta with Fenestrated and Branched Grafts
 Endovascular Treatment of the Aorta with Fenestrated and Branched Grafts Eric LG Verhoeven,MD, PhD, A. Katsargyris, MD Vascular and Endovascular Surgery, Paracelsus Medical University, Nuremberg, Germany
Endovascular Treatment of the Aorta with Fenestrated and Branched Grafts Eric LG Verhoeven,MD, PhD, A. Katsargyris, MD Vascular and Endovascular Surgery, Paracelsus Medical University, Nuremberg, Germany
Current Status of EVAR for Infrarenal AAA. 31 st Annual Florida Vascular Society. PENN Surgery
 Current Status of EVAR for Infrarenal AAA 31 st Annual Florida Vascular Society PENN Surgery No Disclosures Stent Grafts Design Related Differences What really matters? Modular Unibody Supported Unsupported
Current Status of EVAR for Infrarenal AAA 31 st Annual Florida Vascular Society PENN Surgery No Disclosures Stent Grafts Design Related Differences What really matters? Modular Unibody Supported Unsupported
Bilateral use of the Gore IBE device for bilateral CIA aneurysms and a first interim analysis of the prospective Iceberg registry
 Bilateral use of the Gore IBE device for bilateral CIA aneurysms and a first interim analysis of the prospective Iceberg registry Michel MPJ Reijnen, MD, PhD Department of Vascular Surgery, Rijnstate Hospital
Bilateral use of the Gore IBE device for bilateral CIA aneurysms and a first interim analysis of the prospective Iceberg registry Michel MPJ Reijnen, MD, PhD Department of Vascular Surgery, Rijnstate Hospital
ENCORE, a Study to Investigate the Durability of Polymer EVAR with Ovation A Contemporary Review of 1296 Patients
 ENCORE, a Study to Investigate the Durability of Polymer EVAR with Ovation A Contemporary Review of 1296 Patients The Ovation System is approved to treat infrarenal abdominal aortic aneurysms and is not
ENCORE, a Study to Investigate the Durability of Polymer EVAR with Ovation A Contemporary Review of 1296 Patients The Ovation System is approved to treat infrarenal abdominal aortic aneurysms and is not
When to use standard EVAR with EndoAnchors or CHEVAR in short-neck AAAs LINC ASIA 18
 When to use standard EVAR with EndoAnchors or CHEVAR in short-neck AAAs JEAN-PAUL P.M. DE VRIES, DIRECTOR OF VASCULAR SURGERY ST.ANTONIUS HOSPITAL NIEUWEGEIN, THE NETHERLANDS. LINC ASIA-PACIFIC HongKong,
When to use standard EVAR with EndoAnchors or CHEVAR in short-neck AAAs JEAN-PAUL P.M. DE VRIES, DIRECTOR OF VASCULAR SURGERY ST.ANTONIUS HOSPITAL NIEUWEGEIN, THE NETHERLANDS. LINC ASIA-PACIFIC HongKong,
Standardization of the CHEVAR procedure: How a standard approach has improved outcomes. Prof Peter Holt St George s, London
 Standardization of the CHEVAR procedure: How a standard approach has improved outcomes Prof Peter Holt St George s, London Disclosure Speaker name: Prof Peter Holt I have the following potential conflicts
Standardization of the CHEVAR procedure: How a standard approach has improved outcomes Prof Peter Holt St George s, London Disclosure Speaker name: Prof Peter Holt I have the following potential conflicts
Talent Abdominal Stent Graft
 Talent Abdominal with THE Xcelerant Hydro Delivery System Expanding the Indications for EVAR Treat More Patients Short Necks The Talent Abdominal is the only FDA-approved device for proximal aortic neck
Talent Abdominal with THE Xcelerant Hydro Delivery System Expanding the Indications for EVAR Treat More Patients Short Necks The Talent Abdominal is the only FDA-approved device for proximal aortic neck
How to select FEVAR versus EVAR + endoanchors in short-necked AAAs
 How to select FEVAR versus EVAR + endoanchors in short-necked AAAs Jean-Paul P.M. de Vries, Richte C.L. Schuurmann St. Antonius Hospital Nieuwegein, The Netherlands 21st Critical Issues Congress Nuernberg,
How to select FEVAR versus EVAR + endoanchors in short-necked AAAs Jean-Paul P.M. de Vries, Richte C.L. Schuurmann St. Antonius Hospital Nieuwegein, The Netherlands 21st Critical Issues Congress Nuernberg,
Insights from the PROTAGORAS/PERICLES Registries: impact on ChEVAR results
 Insights from the PROTAGORAS/PERICLES Registries: impact on ChEVAR results Konstantinos P. Donas, Giovanni Torsello Department of Vascular Surgery St. Franziskus Hospital Münster, Germany Disclosure Speaker
Insights from the PROTAGORAS/PERICLES Registries: impact on ChEVAR results Konstantinos P. Donas, Giovanni Torsello Department of Vascular Surgery St. Franziskus Hospital Münster, Germany Disclosure Speaker
Chungbuk Regional Cardiovascular Center, Division of Cardiology, Departments of Internal Medicine, Chungbuk National University Hospital Sangmin Kim
 Endovascular Procedures for Isolated Common Iliac and Internal Iliac Aneurysm Chungbuk Regional Cardiovascular Center, Division of Cardiology, Departments of Internal Medicine, Chungbuk National University
Endovascular Procedures for Isolated Common Iliac and Internal Iliac Aneurysm Chungbuk Regional Cardiovascular Center, Division of Cardiology, Departments of Internal Medicine, Chungbuk National University
The Auckland Experience with the Nellix EVAS System. Andrew Holden, MBChB, FRANZCR
 The Auckland Experience with the Nellix EVAS System Andrew Holden, MBChB, FRANZCR Disclosure Speaker name: Associate Professor Andrew Holden I have the following potential conflicts of interest to report:
The Auckland Experience with the Nellix EVAS System Andrew Holden, MBChB, FRANZCR Disclosure Speaker name: Associate Professor Andrew Holden I have the following potential conflicts of interest to report:
Outcomes of endovascular repair of isolated iliac artery aneurysms. A. Stella
 Alma Mater Studiorum Bologna University S.Orsola-Malpighi, Bologna, Italy Vascular Surgery Outcomes of endovascular repair of isolated iliac artery aneurysms A. Stella Isolated iliac artery aneurysms treated
Alma Mater Studiorum Bologna University S.Orsola-Malpighi, Bologna, Italy Vascular Surgery Outcomes of endovascular repair of isolated iliac artery aneurysms A. Stella Isolated iliac artery aneurysms treated
OUTCOMES OF ENDOVASCULAR TAAA REPAIR
 OUTCOMES OF ENDOVASCULAR TAAA REPAIR Gustavo S. Oderich MD Professor of Surgery Director of Aortic Center Director of Advanced Endovascular Aortic Program Division of Vascular and Endovascular Surgery
OUTCOMES OF ENDOVASCULAR TAAA REPAIR Gustavo S. Oderich MD Professor of Surgery Director of Aortic Center Director of Advanced Endovascular Aortic Program Division of Vascular and Endovascular Surgery
Anatomical challenges in EVAR
 Anatomical challenges in EVAR M.H. EL DESSOKI, MD,FRCS PROFESSOR OF VASCULAR SURGERY CAIRO UNIVERSITY Disclosure Speaker name:... I have the following potential conflicts of interest to report: Consulting
Anatomical challenges in EVAR M.H. EL DESSOKI, MD,FRCS PROFESSOR OF VASCULAR SURGERY CAIRO UNIVERSITY Disclosure Speaker name:... I have the following potential conflicts of interest to report: Consulting
Abdominal and thoracic aneurysm repair
 Abdominal and thoracic aneurysm repair William A. Gray MD Director, Endovascular Intervention Cardiovascular Research Foundation Columbia University Medical Center Abdominal Aortic Aneurysm Endografts
Abdominal and thoracic aneurysm repair William A. Gray MD Director, Endovascular Intervention Cardiovascular Research Foundation Columbia University Medical Center Abdominal Aortic Aneurysm Endografts
CUSTOM-MADE SCALLOPED THORACIC ENDOGRAFTS IN DIFFERENT HOSTILE AORTIC ANATOMIES
 CUSTOM-MADE SCALLOPED THORACIC ENDOGRAFTS IN DIFFERENT HOSTILE AORTIC ANATOMIES A SERIES OF THREE CASE REPORTS Joel Sousa Department of Department of Angiology and Vascular Surgery Hospital S. João, Porto,
CUSTOM-MADE SCALLOPED THORACIC ENDOGRAFTS IN DIFFERENT HOSTILE AORTIC ANATOMIES A SERIES OF THREE CASE REPORTS Joel Sousa Department of Department of Angiology and Vascular Surgery Hospital S. João, Porto,
Increased Flexibility of AneuRx Stent-Graft Reduces Need for Secondary Intervention Following Endovascular Aneurysm Repair
 583 Increased Flexibility of AneuRx Stent-Graft Reduces Need for Secondary Intervention Following Endovascular Aneurysm Repair Frank R. Arko, MD; W. Anthony Lee, MD; Bradley B. Hill, MD; Paul Cipriano,
583 Increased Flexibility of AneuRx Stent-Graft Reduces Need for Secondary Intervention Following Endovascular Aneurysm Repair Frank R. Arko, MD; W. Anthony Lee, MD; Bradley B. Hill, MD; Paul Cipriano,
Percutaneous Approaches to Aortic Disease in 2018
 Percutaneous Approaches to Aortic Disease in 2018 Wendy Tsang, MD, SM Assistant Professor, University of Toronto Toronto General Hospital, University Health Network Case 78 year old F Lower CP and upper
Percutaneous Approaches to Aortic Disease in 2018 Wendy Tsang, MD, SM Assistant Professor, University of Toronto Toronto General Hospital, University Health Network Case 78 year old F Lower CP and upper
Nellix Endovascular System: Clinical Outcomes and Device Overview
 Nellix Endovascular System: Clinical Outcomes and Device Overview Jeffrey P. Carpenter, MD Professor and Chief, Department of Surgery CAUTION: Investigational device. This product is under clinical investigation
Nellix Endovascular System: Clinical Outcomes and Device Overview Jeffrey P. Carpenter, MD Professor and Chief, Department of Surgery CAUTION: Investigational device. This product is under clinical investigation
Considerations for a Durable Repair
 Considerations for a Durable Repair Eric Verhoeven, MD, PhD, A. Katsargyris, MD Department of Vascular and Endovascular Surgery, Paracelsus Medical University, Nuremberg, Germany Disclosures William Cook
Considerations for a Durable Repair Eric Verhoeven, MD, PhD, A. Katsargyris, MD Department of Vascular and Endovascular Surgery, Paracelsus Medical University, Nuremberg, Germany Disclosures William Cook
Durable outcomes. Proven performance.
 Durable outcomes. Proven performance. GORE EXCLUDER AAA Endoprosthesis GORE EXCLUDER Iliac Branch Endoprosthesis GORE EXCLUDER AAA Endoprosthesis The most-studied* EVAR stent graft designed for durable
Durable outcomes. Proven performance. GORE EXCLUDER AAA Endoprosthesis GORE EXCLUDER Iliac Branch Endoprosthesis GORE EXCLUDER AAA Endoprosthesis The most-studied* EVAR stent graft designed for durable
A New EVAR Device for Infrarenal AAAs
 A New EVAR Device for Infrarenal AAAs Peter Nelson, MD, MS Assistant Professor of Surgery MM0203 Rev. 01 Current U.S. EVAR Devices Anatomical Fixation Proximal Fixation Powerlink - Endologix Excluder WL
A New EVAR Device for Infrarenal AAAs Peter Nelson, MD, MS Assistant Professor of Surgery MM0203 Rev. 01 Current U.S. EVAR Devices Anatomical Fixation Proximal Fixation Powerlink - Endologix Excluder WL
Reinterventions After Fenestrated and Branched Endovascular Aortic Aneurysm Repair
 Reinterventions After Fenestrated and Branched Endovascular Aortic Aneurysm Repair Andres Schanzer, MD Division of Vascular and Endovascular Surgery UMass Medical School June 15 th, 2018 PNEC, Seattle,
Reinterventions After Fenestrated and Branched Endovascular Aortic Aneurysm Repair Andres Schanzer, MD Division of Vascular and Endovascular Surgery UMass Medical School June 15 th, 2018 PNEC, Seattle,
Durability of The Endurant Stent-Graft through 5 Years
 Durability of The Endurant Stent-Graft through 5 Years Michel S. Makaroun MD Co-Director, UPMC Heart and Vascular Institute Professor and Chair, Division of Vascular Surgery University of Pittsburgh School
Durability of The Endurant Stent-Graft through 5 Years Michel S. Makaroun MD Co-Director, UPMC Heart and Vascular Institute Professor and Chair, Division of Vascular Surgery University of Pittsburgh School
LOWERING THE PROFILE RAISING THE BAR
 LOWERING THE PROFILE RAISING THE BAR INNOVATIVE LOW PROFILE. ADVANCED CLINICAL PERFORMANCE. The AFX TM Endovascular AAA System integrates anatomical fixation with an advanced delivery system and graft
LOWERING THE PROFILE RAISING THE BAR INNOVATIVE LOW PROFILE. ADVANCED CLINICAL PERFORMANCE. The AFX TM Endovascular AAA System integrates anatomical fixation with an advanced delivery system and graft
Thoracoabdominal Aorta: Advances and Novel Therapies
 Thoracoabdominal Aorta: Advances and Novel Therapies Robert Meisner, MD FACS Sidney Kimmel Medical Center Assistant Professor of Surgery Vascular / Endovascular Surgeon at Lankenau Medical Center November
Thoracoabdominal Aorta: Advances and Novel Therapies Robert Meisner, MD FACS Sidney Kimmel Medical Center Assistant Professor of Surgery Vascular / Endovascular Surgeon at Lankenau Medical Center November
Case Report A Case of Successful Coil Embolization for a Late-Onset Type Ia Endoleak after Endovascular Aneurysm Repair with the Chimney Technique
 Case Reports in Vascular Medicine Volume 2016, Article ID 5307416, 4 pages http://dx.doi.org/10.1155/2016/5307416 Case Report A Case of Successful Coil Embolization for a Late-Onset Type Ia Endoleak after
Case Reports in Vascular Medicine Volume 2016, Article ID 5307416, 4 pages http://dx.doi.org/10.1155/2016/5307416 Case Report A Case of Successful Coil Embolization for a Late-Onset Type Ia Endoleak after
Now that Endoanchors are Approved (and paid for) We have a Durable Solution to Short Necks That s so Easy!
 We have a Durable Solution to Short Necks That s so Easy!") Now that Endoanchors are Approved (and paid for) We have a Durable Solution to Short Necks That s so Easy! David H. Deaton, MD Vascular Surgery / University of South Carolina / Palmetto Health Chief Medical
Now that Endoanchors are Approved (and paid for) We have a Durable Solution to Short Necks That s so Easy! David H. Deaton, MD Vascular Surgery / University of South Carolina / Palmetto Health Chief Medical
Endovascular therapy for Ischemic versus Nonischemic complicated acute type B aortic dissection (catbad).
.") Endovascular therapy for Ischemic versus Nonischemic complicated acute type B aortic dissection (catbad). AS. Eleshra, MD 1, T. Kölbel, MD, PhD 1, F. Rohlffs, MD 1, N. Tsilimparis, MD, PhD 1,2 Ahmed Eleshra
Endovascular therapy for Ischemic versus Nonischemic complicated acute type B aortic dissection (catbad). AS. Eleshra, MD 1, T. Kölbel, MD, PhD 1, F. Rohlffs, MD 1, N. Tsilimparis, MD, PhD 1,2 Ahmed Eleshra
EndoVascular Aneurysm Sealing (EVAS) with Nellix
 with Nellix") 1 2 EndoVascular Aneurysm Sealing (EVAS) with Nellix Designed to seal entire aneurysm with contained biostable polymer Non-modular design with complete fixation Expands endovascular patient eligibility
1 2 EndoVascular Aneurysm Sealing (EVAS) with Nellix Designed to seal entire aneurysm with contained biostable polymer Non-modular design with complete fixation Expands endovascular patient eligibility
Endovascular Repair o Abdominal. Aortic Aneurysms. Cesar E. Mendoza, M.D. Jackson Memorial Hospital Miami, Florida
 Endovascular Repair o Abdominal Aortic Aneurysms Cesar E. Mendoza, M.D. Jackson Memorial Hospital Miami, Florida Disclosure Nothing to disclose. 2 Mr. X AAA Mr. X. Is a 70 year old male who presented to
Endovascular Repair o Abdominal Aortic Aneurysms Cesar E. Mendoza, M.D. Jackson Memorial Hospital Miami, Florida Disclosure Nothing to disclose. 2 Mr. X AAA Mr. X. Is a 70 year old male who presented to
Anatomy-Driven Endograft Selection for Abdominal Aortic Aneurysm Repair S. Jay Mathews, MD, MS, FACC
 Anatomy-Driven Endograft Selection for Abdominal Aortic Aneurysm Repair S. Jay Mathews, MD, MS, FACC Interventional Cardiologist/Endovascular Specialist Bradenton Cardiology Center Bradenton, FL, USA Disclosures
Anatomy-Driven Endograft Selection for Abdominal Aortic Aneurysm Repair S. Jay Mathews, MD, MS, FACC Interventional Cardiologist/Endovascular Specialist Bradenton Cardiology Center Bradenton, FL, USA Disclosures
Influence of patient selection and IFU compliance on outcomes following EVAS
 Influence of patient selection and IFU compliance on outcomes following EVAS LUNCH SYMPOSIUM LINC 2017 Jan MM Heyligers, MD, PhD, FEBVS Consultant Vascular Surgeon Elisabeth TweeSteden Hospital Tilburg,
Influence of patient selection and IFU compliance on outcomes following EVAS LUNCH SYMPOSIUM LINC 2017 Jan MM Heyligers, MD, PhD, FEBVS Consultant Vascular Surgeon Elisabeth TweeSteden Hospital Tilburg,
History of the Powerlink System Design and Clinical Results. Edward B. Diethrich Arizona Heart Hospital Phoenix, AZ
 History of the Powerlink System Design and Clinical Results Edward B. Diethrich Arizona Heart Hospital Phoenix, AZ Powerlink System: Unibody-Bifurcated Design Long Main Body Low-Porosity Proprietary eptfe
History of the Powerlink System Design and Clinical Results Edward B. Diethrich Arizona Heart Hospital Phoenix, AZ Powerlink System: Unibody-Bifurcated Design Long Main Body Low-Porosity Proprietary eptfe
Off-the-Shelf Devices. Mark A Farber, MD FACS Director, Aortic Center Professor of Radiology and Surgery University of North Carolina
 Off-the-Shelf Devices Mark A Farber, MD FACS Director, Aortic Center Professor of Radiology and Surgery University of North Carolina Disclosures Cook - Research Support, Consultant, Clinical Trials WL
Off-the-Shelf Devices Mark A Farber, MD FACS Director, Aortic Center Professor of Radiology and Surgery University of North Carolina Disclosures Cook - Research Support, Consultant, Clinical Trials WL
The Management and Treatment of Ruptured Abdominal Aortic Aneurysm (RAAA)
") The Management and Treatment of Ruptured Abdominal Aortic Aneurysm (RAAA) Disclosure Speaker name: Ren Wei, Li Zhui, Li Fenghe, Zhao Yu Department of Vascular Surgery, The First Affiliated Hospital of
The Management and Treatment of Ruptured Abdominal Aortic Aneurysm (RAAA) Disclosure Speaker name: Ren Wei, Li Zhui, Li Fenghe, Zhao Yu Department of Vascular Surgery, The First Affiliated Hospital of
Access More Patients. Customize Each Seal.
 Access More. Customize Each Seal. The Least Invasive Path Towards Proven Patency ULTRA LOW PROFILE TO EASE ADVANCEMENT The flexible, ultra-low 12F ID Ovation ix delivery system enables you to navigate
Access More. Customize Each Seal. The Least Invasive Path Towards Proven Patency ULTRA LOW PROFILE TO EASE ADVANCEMENT The flexible, ultra-low 12F ID Ovation ix delivery system enables you to navigate
Important Update to Field Safety Notice Nellix EndoVascular Aneurysm Sealing System Updated Instructions for Use (IFU)
") October 6, 2017 Important Update to Field Safety Notice Nellix EndoVascular Aneurysm Sealing System Updated Instructions for Use (IFU) Dear Physician, This notification is to provide you with further information
October 6, 2017 Important Update to Field Safety Notice Nellix EndoVascular Aneurysm Sealing System Updated Instructions for Use (IFU) Dear Physician, This notification is to provide you with further information
Feasibility of aortic neck anatomy for endovascular aneurysm repair in Korean patients with abdominal aortic aneurysm
 LINC 2019 Leipzig, Germany Feasibility of aortic neck anatomy for endovascular aneurysm repair in Korean patients with abdominal aortic aneurysm Deokbi Hwang, Sujin Park, Hyung-Kee Kim, Seung Huh Division
LINC 2019 Leipzig, Germany Feasibility of aortic neck anatomy for endovascular aneurysm repair in Korean patients with abdominal aortic aneurysm Deokbi Hwang, Sujin Park, Hyung-Kee Kim, Seung Huh Division
THORACOABDOMINAL AORTIC ANEURYSMS HYBRID REPAIR
 Update on Open and Endovascular Therapeutic Option for Aortic Repair CENTRE CARDIO-TORACIQUE DE MONACO Friday November 7 th, 2014 THORACOABDOMINAL AORTIC ANEURYSMS HYBRID REPAIR Roberto Chiesa Vascular
Update on Open and Endovascular Therapeutic Option for Aortic Repair CENTRE CARDIO-TORACIQUE DE MONACO Friday November 7 th, 2014 THORACOABDOMINAL AORTIC ANEURYSMS HYBRID REPAIR Roberto Chiesa Vascular
The clinical update for the Zenith AAA Endovascular Graft has included results from the Zenith AAA Endovascular Graft multi-center clinical study,
 The clinical update for the Zenith AAA Endovascular Graft has included results from the Zenith AAA Endovascular Graft multi-center clinical study, the 36 mm diameter Zenith Flex AAA Endovascular Graft
The clinical update for the Zenith AAA Endovascular Graft has included results from the Zenith AAA Endovascular Graft multi-center clinical study, the 36 mm diameter Zenith Flex AAA Endovascular Graft
Accessi Iliaci Ostili
 Alma Mater Studiorum Bologna University S.Orsola-Malpighi, Bologna, Italy Vascular Surgery Accessi Iliaci Ostili nel trattamento della patologia aortica E. Gallitto Iliac Navigations Alma Mater Studiorum
Alma Mater Studiorum Bologna University S.Orsola-Malpighi, Bologna, Italy Vascular Surgery Accessi Iliaci Ostili nel trattamento della patologia aortica E. Gallitto Iliac Navigations Alma Mater Studiorum
Optimizing Accuracy of Aortic Stent Grafts in Short Necks
 Optimizing Accuracy of Aortic Stent Grafts in Short Necks Venkatesh Ramaiah, MD, FACS Medical Director Arizona Heart Hospital Director Peripheral Vascular and Endovascular Research Arizona Heart Institute
Optimizing Accuracy of Aortic Stent Grafts in Short Necks Venkatesh Ramaiah, MD, FACS Medical Director Arizona Heart Hospital Director Peripheral Vascular and Endovascular Research Arizona Heart Institute
Jean M Panneton, MD Professor of Surgery Program Director Vascular Surgery Chief EVMS. Arch Pathology: The Endovascular Era is here
 Jean M Panneton, MD Professor of Surgery Program Director Vascular Surgery Chief EVMS Arch Pathology: The Endovascular Era is here Disclosures Consultant: Cook Medical, Bolton Medical, Medtronic Inc, Volcano,
Jean M Panneton, MD Professor of Surgery Program Director Vascular Surgery Chief EVMS Arch Pathology: The Endovascular Era is here Disclosures Consultant: Cook Medical, Bolton Medical, Medtronic Inc, Volcano,
Improving Endograft Durability with EndoAnchors
 Improving Endograft Durability with EndoAnchors William D. Jordan, Jr., M.D. John E. Skandalakis Chair in Surgery Professor and Chief Division of Vascular Surgery and Endovascular Therapy Emory University
Improving Endograft Durability with EndoAnchors William D. Jordan, Jr., M.D. John E. Skandalakis Chair in Surgery Professor and Chief Division of Vascular Surgery and Endovascular Therapy Emory University
Experience of endovascular procedures on abdominal and thoracic aorta in CA region
 Experience of endovascular procedures on abdominal and thoracic aorta in CA region May 14-15, 2015, Dubai Dr. Viktor Zemlyanskiy National Research Center of Emergency Care Astana, Kazakhstan Region Characteristics
Experience of endovascular procedures on abdominal and thoracic aorta in CA region May 14-15, 2015, Dubai Dr. Viktor Zemlyanskiy National Research Center of Emergency Care Astana, Kazakhstan Region Characteristics
FLEXIBLE, BALOON EXPANDABLE
 EARLY RESULTS OF A CLINICAL TRIAL OF FLEXIBLE, BALOON EXPANDABLE COVERED STENT GRAFT IN ILIAC OCCLUSIVE DISEASE Chris LeCroy Coastal Vascular and Interventional Pensacola, Florida Clinical Trial WL GORE
EARLY RESULTS OF A CLINICAL TRIAL OF FLEXIBLE, BALOON EXPANDABLE COVERED STENT GRAFT IN ILIAC OCCLUSIVE DISEASE Chris LeCroy Coastal Vascular and Interventional Pensacola, Florida Clinical Trial WL GORE
Treatment of Thoracoabdominal Aneurysms Is there a need for custom-made devices?
 : FETURED TECHNOLOGY: JOTEC E-XTR DESIGN ENGINEERING Treatment of Thoracoabdominal neurysms Is there a need for custom-made devices? INTERVIEW ND CSE PRESENTTIONS WITH DNIEL RNZN, MD, ND NDREJ SCHMIDT,
: FETURED TECHNOLOGY: JOTEC E-XTR DESIGN ENGINEERING Treatment of Thoracoabdominal neurysms Is there a need for custom-made devices? INTERVIEW ND CSE PRESENTTIONS WITH DNIEL RNZN, MD, ND NDREJ SCHMIDT,
How to Determine Tolerance for Branch Vessel Coverage
 How to Determine Tolerance for Branch Vessel Coverage Venita Chandra, MD Clinical Assistant Professor of Surgery Division of Stanford Medical School, Stanford, CA PNEC May 25 th, 2017 DISCLOSURES Venita
How to Determine Tolerance for Branch Vessel Coverage Venita Chandra, MD Clinical Assistant Professor of Surgery Division of Stanford Medical School, Stanford, CA PNEC May 25 th, 2017 DISCLOSURES Venita
Taming The Aorta. David Minion, MD Program Director, Vascular Surgery University of Kentucky Medical Center Lexington, Kentucky, USA
 Taming The Aorta David Minion, MD Program Director, Vascular Surgery University of Kentucky Medical Center Lexington, Kentucky, USA Faculty Disclosure Consulting: Endologix, Cook 1 Objectives Review the
Taming The Aorta David Minion, MD Program Director, Vascular Surgery University of Kentucky Medical Center Lexington, Kentucky, USA Faculty Disclosure Consulting: Endologix, Cook 1 Objectives Review the
Popliteal Aneurysm: When is surgical therapy indicated? PROF. GRZEGORZ OSZKINIS
 Popliteal Aneurysm: When is surgical therapy indicated? PROF. GRZEGORZ OSZKINIS Asymptomatic mass - 38-40%will develop symptoms at a rate of 14%/yr Intermittent claudic ation (chronic ischemia) - 25%-40%
Popliteal Aneurysm: When is surgical therapy indicated? PROF. GRZEGORZ OSZKINIS Asymptomatic mass - 38-40%will develop symptoms at a rate of 14%/yr Intermittent claudic ation (chronic ischemia) - 25%-40%
Chimney endovascular aneurysm sealing (ch-evas) for ruptured abdominal aortic aneurysms (AAA) due to type Ia endoleak following failed EVAS
 for ruptured abdominal aortic aneurysms (AAA) due to type Ia endoleak following failed EVAS") Chimney endovascular aneurysm sealing (ch-evas) for ruptured abdominal aortic aneurysms (AAA) due to type Ia endoleak following failed EVAS Saritphat Orrapin MD FRCS (Thailand), Thoetphum Benyakorn, Tunyarat
Chimney endovascular aneurysm sealing (ch-evas) for ruptured abdominal aortic aneurysms (AAA) due to type Ia endoleak following failed EVAS Saritphat Orrapin MD FRCS (Thailand), Thoetphum Benyakorn, Tunyarat
Analysis of Type IIIb Endoleaks Encountered with Endologix Endografts
 Analysis of Type IIIb Endoleaks Encountered with Endologix Endografts Alan R. Wladis, MD, FACS, David Varnagy, MD, FACS, Manuel R. Perez-Izquierdo, MD, Mark Ranson, MD FACS, Delos Clift, MD FACS, Rebecca
Analysis of Type IIIb Endoleaks Encountered with Endologix Endografts Alan R. Wladis, MD, FACS, David Varnagy, MD, FACS, Manuel R. Perez-Izquierdo, MD, Mark Ranson, MD FACS, Delos Clift, MD FACS, Rebecca
Ovation. Sean Lyden, MD Department Chair, Vascular Surgery Cleveland Clinic
 Ovation Sean Lyden, MD Department Chair, Vascular Surgery Cleveland Clinic Disclosure Statement of Financial Interest Within the past 12 months, I or my spouse/partner have had a financial interest/arrangement
Ovation Sean Lyden, MD Department Chair, Vascular Surgery Cleveland Clinic Disclosure Statement of Financial Interest Within the past 12 months, I or my spouse/partner have had a financial interest/arrangement
How to Categorize the Infrarenal Neck Properly? I Van Herzeele Dept. Thoracic and Vascular Surgery, Ghent University, Belgium
 How to Categorize the Infrarenal Neck Properly? I Van Herzeele Dept. Thoracic and Vascular Surgery, Ghent University, Belgium Disclosure Speaker name: Isabelle Van Herzeele I have the following potential
How to Categorize the Infrarenal Neck Properly? I Van Herzeele Dept. Thoracic and Vascular Surgery, Ghent University, Belgium Disclosure Speaker name: Isabelle Van Herzeele I have the following potential
From 1996 to 1999, a total of 1,193 patients with
 THE ANEURX CLINICAL TRIAL AT 8 YEARS Lessons learned following the US AneuRx clinical trial from 1996 to 2004. BY CHRISTOPHER K. ZARINS, MD From 1996 to 1999, a total of 1,193 patients with infrarenal
THE ANEURX CLINICAL TRIAL AT 8 YEARS Lessons learned following the US AneuRx clinical trial from 1996 to 2004. BY CHRISTOPHER K. ZARINS, MD From 1996 to 1999, a total of 1,193 patients with infrarenal
Toward Total Endovascular Therapy of the Aorta. Adam W. Beck, MD. Associate Professor of Surgery Division of Vascular Surgery and Endovascular Therapy
 Toward Total Endovascular Therapy of the Aorta Adam W. Beck, MD Associate Professor of Surgery Division of Vascular Surgery and Endovascular Therapy University of Alabama at Birmingham Disclosures Grant
Toward Total Endovascular Therapy of the Aorta Adam W. Beck, MD Associate Professor of Surgery Division of Vascular Surgery and Endovascular Therapy University of Alabama at Birmingham Disclosures Grant
Animesh Rathore, MD, RPVI Sentara Vascular Specialists. Debate 4: Complex endovascular aortic repair will make open surgery obsolete
 Animesh Rathore, MD, RPVI Sentara Vascular Specialists Debate 4: Complex endovascular aortic repair will make open surgery obsolete Definition Complex aortic pathology (aneurysms/dissection) Involvement
Animesh Rathore, MD, RPVI Sentara Vascular Specialists Debate 4: Complex endovascular aortic repair will make open surgery obsolete Definition Complex aortic pathology (aneurysms/dissection) Involvement
Predictors of abdominal aortic aneurysm sac enlargement after EVAR Longterm results from the ENGAGE Registry
 Predictors of abdominal aortic aneurysm sac enlargement after EVAR Longterm results from the ENGAGE Registry D. Böckler Department of Vascular and Endovascular Surgery University Hospital Heidelberg Disclosure
Predictors of abdominal aortic aneurysm sac enlargement after EVAR Longterm results from the ENGAGE Registry D. Böckler Department of Vascular and Endovascular Surgery University Hospital Heidelberg Disclosure
Right Choice for Right Angles
 Right Choice for Right Angles The Anatomy of Technology Aorfix gives you technology that conforms to patient anatomy, optimising both procedure and post-operative performance. Fishmouth for optimum neck
Right Choice for Right Angles The Anatomy of Technology Aorfix gives you technology that conforms to patient anatomy, optimising both procedure and post-operative performance. Fishmouth for optimum neck
Residual Dissection and False Lumen Aneurysm After TEVAR
 WHAT WOULD YOU DO? Residual Dissection and False Lumen Aneurysm After MODERATOR: MARK FARBER, MD PANEL: YAZAN DUWAYRI, MD; MATTHEW J. EAGLETON, MD; WILLIAM D. JORDAN Jr, MD; TILO KÖLBEL, MD, PhD; AND ERIC
WHAT WOULD YOU DO? Residual Dissection and False Lumen Aneurysm After MODERATOR: MARK FARBER, MD PANEL: YAZAN DUWAYRI, MD; MATTHEW J. EAGLETON, MD; WILLIAM D. JORDAN Jr, MD; TILO KÖLBEL, MD, PhD; AND ERIC
How effective is preservation when viewed through a clinical and economic lens?
 How effective is preservation when viewed through a clinical and economic lens? Nilo J Mosquera, MD. Head of Department Angiology and Vascular Surgery Department. Complexo Hospitalario Universitario de
How effective is preservation when viewed through a clinical and economic lens? Nilo J Mosquera, MD. Head of Department Angiology and Vascular Surgery Department. Complexo Hospitalario Universitario de
Fenestrated Implantation: How I do it. Tara M Mastracci, FRCSC, FACS, FRCS, MSc Royal Free London
 Fenestrated Implantation: How I do it. Tara M Mastracci, FRCSC, FACS, FRCS, MSc Royal Free London Disclosures Cook Medical Inc -- Proctorship and Consultation All speaking and consultation fees are donated
Fenestrated Implantation: How I do it. Tara M Mastracci, FRCSC, FACS, FRCS, MSc Royal Free London Disclosures Cook Medical Inc -- Proctorship and Consultation All speaking and consultation fees are donated
Treating very short necks ( 4mm <10mm) using the Endurant stent graft + EndoAnchors: 1-year results and current insights
 using the Endurant stent graft + EndoAnchors: 1-year results and current insights") Treating very short necks ( 4mm
Treating very short necks ( 4mm
Endovascular Management of Thoracic Aortic Pathology Stéphan Haulon, J Sobocinski, B Maurel, T Martin-Gonzalez, R Spear, A Hertault, R Azzaoui
 Endovascular Management of Thoracic Aortic Pathology Stéphan Haulon, J Sobocinski, B Maurel, T Martin-Gonzalez, R Spear, A Hertault, R Azzaoui Aortic Center, Lille University Hospital, France Disclosures
Endovascular Management of Thoracic Aortic Pathology Stéphan Haulon, J Sobocinski, B Maurel, T Martin-Gonzalez, R Spear, A Hertault, R Azzaoui Aortic Center, Lille University Hospital, France Disclosures
Type 1a Endoleak in hostile neck anatomies: Endoanchor can fix it! D. Böckler University Hospital Heidelberg, Germany
 Type 1a Endoleak in hostile neck anatomies: Endoanchor can fix it! D. Böckler University Hospital Heidelberg, Germany Disclosures Speaker name: Dittmar Böckler I have the following potential conflicts
Type 1a Endoleak in hostile neck anatomies: Endoanchor can fix it! D. Böckler University Hospital Heidelberg, Germany Disclosures Speaker name: Dittmar Böckler I have the following potential conflicts
Dr Peter Bungay Derbyshire Vascular Services Royal Derby Hospital Derby UK
 Dr Peter Bungay Derbyshire Vascular Services Royal Derby Hospital Derby UK Disclosure I have the following potential conflicts of interest to report Consultant, proctor and paid speaker for Vascutek UK
Dr Peter Bungay Derbyshire Vascular Services Royal Derby Hospital Derby UK Disclosure I have the following potential conflicts of interest to report Consultant, proctor and paid speaker for Vascutek UK
Conflicts of Interest. Endovascular Repair of Thoracoabdominal Aneurysm. Overview PLANNING ANATOMIC CONSIDERATIONS FOR COMPLEX AORTIC REPAIR
 Endovascular Repair of Thoracoabdominal Aneurysm Tim Resch MD Björn Sonesson MD, Nuno Dias MD Vascular Center Skane University Hospital Conflicts of Interest COOK Medical - Consulting, Speakers Bureau,
Endovascular Repair of Thoracoabdominal Aneurysm Tim Resch MD Björn Sonesson MD, Nuno Dias MD Vascular Center Skane University Hospital Conflicts of Interest COOK Medical - Consulting, Speakers Bureau,
Young-Guk Ko, M.D. Severance Cardiovascular Hospital, Yonsei University Health System,
 Young-Guk Ko, M.D., Dangas G, J Am Coll Cardiol Intv 2012;5:1071 All-cause Mortality Dangas Severance G, J Am Coll Cardiovascular Cardiol Intv Hospital, 2012;5:1071 Yonsei University Health System Aneurysm-related
Young-Guk Ko, M.D., Dangas G, J Am Coll Cardiol Intv 2012;5:1071 All-cause Mortality Dangas Severance G, J Am Coll Cardiovascular Cardiol Intv Hospital, 2012;5:1071 Yonsei University Health System Aneurysm-related
symptomatic aneurysms or aneurysms that grow >1cm/yr
 1. Elective repair for aneurysm >5.5 cm, symptomatic aneurysms or aneurysms that grow >1cm/yr 2. Ruptured AAA Aneurysm Detection and Management Study (ADAM) and UK Small Aneurysm Trial early open surgery
1. Elective repair for aneurysm >5.5 cm, symptomatic aneurysms or aneurysms that grow >1cm/yr 2. Ruptured AAA Aneurysm Detection and Management Study (ADAM) and UK Small Aneurysm Trial early open surgery
EVAR replaced standard repair in most cases. Why?
 EVAR replaced standard repair in most cases. Why? Initial major steps in endograft evolution Papazoglou O. Konstantinos M.D. The story of a major breakthrough in vascular surgery 1991 Parodi introduces
EVAR replaced standard repair in most cases. Why? Initial major steps in endograft evolution Papazoglou O. Konstantinos M.D. The story of a major breakthrough in vascular surgery 1991 Parodi introduces
CHALLENGING ILIAC ACCESSES AND THROMBOSIS PREVENTION
 CHALLENGING ILIAC ACCESSES AND THROMBOSIS PREVENTION ARMANDO MANSILHA MD, PhD, FEBVS UNIVERSITY HOSPITAL - PORTO Disclosure of Interest Speaker name: ARMANDO MANSILHA I have the following potential conflicts
CHALLENGING ILIAC ACCESSES AND THROMBOSIS PREVENTION ARMANDO MANSILHA MD, PhD, FEBVS UNIVERSITY HOSPITAL - PORTO Disclosure of Interest Speaker name: ARMANDO MANSILHA I have the following potential conflicts
What is the benefit. of MEP s in BEVAR for TAAA. in preventing paraplegia?
 What is the benefit of MEP s in BEVAR for TAAA in preventing paraplegia? P M Kasprzak Department of Vascular Surgery, Endovascular Surgery University Hospital Regensburg, Germany Disclosures Dr. Kasprzak
What is the benefit of MEP s in BEVAR for TAAA in preventing paraplegia? P M Kasprzak Department of Vascular Surgery, Endovascular Surgery University Hospital Regensburg, Germany Disclosures Dr. Kasprzak
Challenges. 1. Sizing. 2. Proximal landing zone 3. Distal landing zone 4. Access vessels 5. Spinal cord ischemia 6. Endoleak
 Disclosure I have the following potential conflicts of interest to report: Consulting: Medtronic, Gore Employment in industry Stockholder of a healthcare company Owner of a healthcare company Other(s)
Disclosure I have the following potential conflicts of interest to report: Consulting: Medtronic, Gore Employment in industry Stockholder of a healthcare company Owner of a healthcare company Other(s)
Mid-term results of 300+ patients treated by endovascular aortic sealing (EVAS)
") Mid-term results of 300+ patients treated by endovascular aortic sealing (EVAS) Jean-Paul P.M. de Vries Dept Vascular Surgery St. Antonius Hospital, Nieuwegein,The Netherlands On behalf of the DEVASS study
Mid-term results of 300+ patients treated by endovascular aortic sealing (EVAS) Jean-Paul P.M. de Vries Dept Vascular Surgery St. Antonius Hospital, Nieuwegein,The Netherlands On behalf of the DEVASS study
MODERN METHODS FOR TREATING ABDOMINAL ANEURYSMS AND THORACIC AORTIC DISEASE
 MODERN METHODS FOR TREATING ABDOMINAL ANEURYSMS AND THORACIC AORTIC DISEASE AAA FACTS 200,000 New Cases Each Year Ruptured AAA = 15,000 Deaths per Year in U.S. 13th Leading Cause of Death 80% Chance of
MODERN METHODS FOR TREATING ABDOMINAL ANEURYSMS AND THORACIC AORTIC DISEASE AAA FACTS 200,000 New Cases Each Year Ruptured AAA = 15,000 Deaths per Year in U.S. 13th Leading Cause of Death 80% Chance of
Three year experience with multilayer stent in the treatment of thoracoabdominal aneurysms no evidence for aneurysm stabilization
 Three year experience with multilayer stent in the treatment of thoracoabdominal aneurysms no evidence for aneurysm stabilization Thomas Larzon, MD, PhD Head of Vascular Surgery Dept of Cardiothoracic
Three year experience with multilayer stent in the treatment of thoracoabdominal aneurysms no evidence for aneurysm stabilization Thomas Larzon, MD, PhD Head of Vascular Surgery Dept of Cardiothoracic
Bifurcated system Proximal suprarenal stent Modular (aortic main body and two iliac legs) Full thickness woven polyester graft material Fully
 Full thickness woven polyester graft material Fully") Physician Training Bifurcated system Proximal suprarenal stent Modular (aortic main body and two iliac legs) Full thickness woven polyester graft material Fully supported by self-expanding z-stents H&L-B
Physician Training Bifurcated system Proximal suprarenal stent Modular (aortic main body and two iliac legs) Full thickness woven polyester graft material Fully supported by self-expanding z-stents H&L-B
The Petticoat Technique Managing Type B Dissection with both Early and Long Term Considerations
 The Petticoat Technique Managing Type B Dissection with both Early and Long Term Considerations Joseph V. Lombardi, MD Professor & Chief, Division of Vascular & Endovascular Surgery Department of Surgery,
The Petticoat Technique Managing Type B Dissection with both Early and Long Term Considerations Joseph V. Lombardi, MD Professor & Chief, Division of Vascular & Endovascular Surgery Department of Surgery,
Alma Mater Studiorum Bologna University. S.Orsola-Malpighi, Bologna, Italy Vascular Surgery
 Alma Mater Studiorum Bologna University S.Orsola-Malpighi, Bologna, Italy Vascular Surgery L orientamento dell arteria renale influenza gli outcomes renali nel trattamento endovascolare degli aneurismi
Alma Mater Studiorum Bologna University S.Orsola-Malpighi, Bologna, Italy Vascular Surgery L orientamento dell arteria renale influenza gli outcomes renali nel trattamento endovascolare degli aneurismi
Hostile Neck During EVAR, The Role Of Endoanchores
 Hostile Neck During EVAR, The Role Of Endoanchores Samer Koussayer, MD, FACS, RVT Prof, Al Faisal University Section Head and consultant Vascular & Endovascular Surgery Division King Faisal Specialist
Hostile Neck During EVAR, The Role Of Endoanchores Samer Koussayer, MD, FACS, RVT Prof, Al Faisal University Section Head and consultant Vascular & Endovascular Surgery Division King Faisal Specialist
NEW INNOVATIONS IN ENDOLEAK MANAGEMENT
 DISCLOSURES NEW INNOVATIONS IN ENDOLEAK MANAGEMENT Kelley HodgkissHarlow, MD, RPVI, FACS Vascular and Endovascular Surgery Kaiser Permanente, San Diego Nothing to disclose GOALS BACKGROUND Background Surveillance
DISCLOSURES NEW INNOVATIONS IN ENDOLEAK MANAGEMENT Kelley HodgkissHarlow, MD, RPVI, FACS Vascular and Endovascular Surgery Kaiser Permanente, San Diego Nothing to disclose GOALS BACKGROUND Background Surveillance
14F OD Ovation Abdominal Stent Graft System
 14F OD Ovation Abdominal Stent Graft System 2 Year Results from the European Study Dierk Scheinert, MD Center for Vascular Medicine Angiology and Vascular Surgery Park Hospital Leipzig, Germany Disclosure
14F OD Ovation Abdominal Stent Graft System 2 Year Results from the European Study Dierk Scheinert, MD Center for Vascular Medicine Angiology and Vascular Surgery Park Hospital Leipzig, Germany Disclosure
Is EVAS a proper choice in women?
 Is EVAS a proper choice in women? CACVS 2018 Jan MM Heyligers, PhD, FEBVS Consultant Vascular Surgeon Elisabeth TweeSteden Hospital Tilburg The Netherlands Disclosures Consultant for Endologix DEVASS =Dutch
Is EVAS a proper choice in women? CACVS 2018 Jan MM Heyligers, PhD, FEBVS Consultant Vascular Surgeon Elisabeth TweeSteden Hospital Tilburg The Netherlands Disclosures Consultant for Endologix DEVASS =Dutch
Open fenestration for complicated acute aortic B dissection
 Art of Operative Techniques Open fenestration for complicated acute aortic B dissection Santi Trimarchi 1, Sara Segreti 1, Viviana Grassi 1, Chiara Lomazzi 1, Marta Cova 1, Gabriele Piffaretti 2, Vincenzo
Art of Operative Techniques Open fenestration for complicated acute aortic B dissection Santi Trimarchi 1, Sara Segreti 1, Viviana Grassi 1, Chiara Lomazzi 1, Marta Cova 1, Gabriele Piffaretti 2, Vincenzo