Burn Resuscitation Formulas. John P. Sabra, MD Seton Surgical Group Department of Surgery Dell Medical School Austin, TX
|
|
|
- Cora Matthews
- 5 years ago
- Views:
Transcription


1 Burn Resuscitation Formulas John P. Sabra, MD Seton Surgical Group Department of Surgery Dell Medical School Austin, TX
2



3
4
5

6
7
8 BURN INJURY % Physiologic Change % TBSA burn
9 Stasis
 VOLUME PERIPHERAL RESISTANCE CARDIAC")
10 BURN VASCULAR PERMEABILITY EDEMA HEMATOCRIT BLOOD (PLASMA & VISCOSITY ECF) VOLUME PERIPHERAL RESISTANCE CARDIAC OUTPUT
11 PATHOPHYSIOLOGY OF BURN EDEMA Plasma-interstitial oncotic pr Pressure Gradient Interstitial Protein Hypoproteinemia EDEMA
12 Systemic Effects of Burn Injury Magnitude & duration of response proportional to extent of surface burned Hypovolemia Decreased perfusion & oxygen delivery Corrected with adequate fluid resuscitation Prevent shock & organ failure
13 Shock & Fluid Resuscitation Goal To maintain vital organ function while avoiding the complications of inadequate or excessive therapy

14 Under Resuscitation Shock Organ failure Death

15 Over-Resuscitation Compartment syndromes Cerebral edema Pulmonary edema
16



17

18
19 Resuscitation Volume HOW MUCH IS TOO MUCH? LIKE MANY ARGUMENTS THE TRUTH IS SOMEWHERE IN THE MIDDLE
20

21 Dr. Haldor Sneve 1905 patient is exposed to death first from shock. Oral and IV salt solutions recommended

22



23

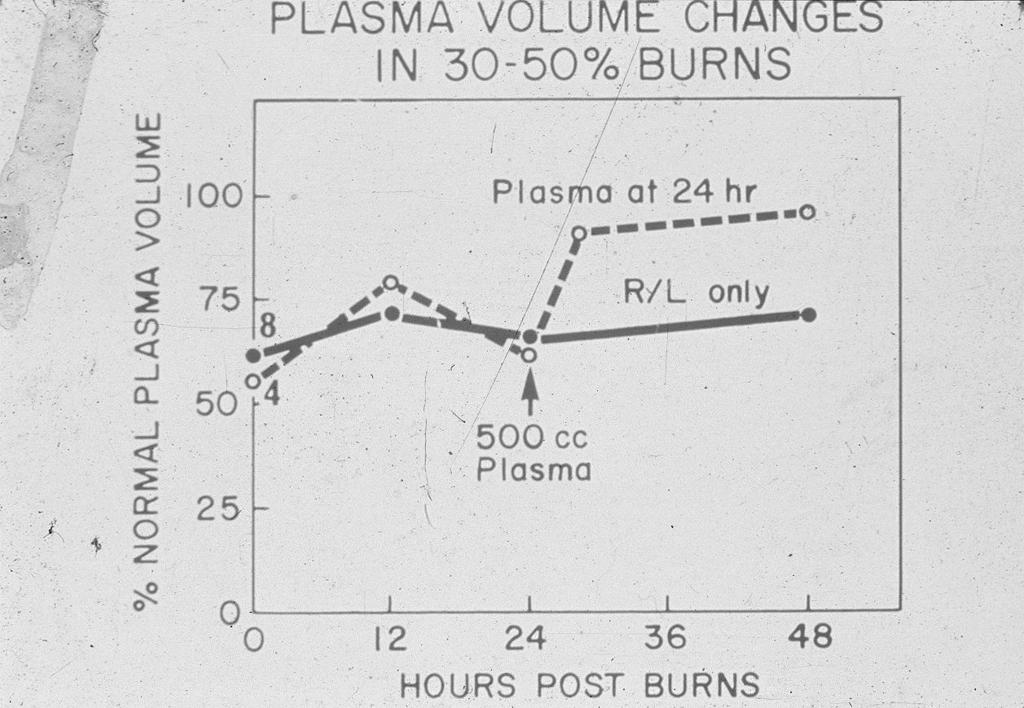
24 Cope O, Moore FD. The redistribution of body water and the fluid therapy of the burned patient. Ann Surg 1947; 126: Confirmed relationship between edema and shock in humans First to suggest that resuscitation should be both TBSA% AND weight

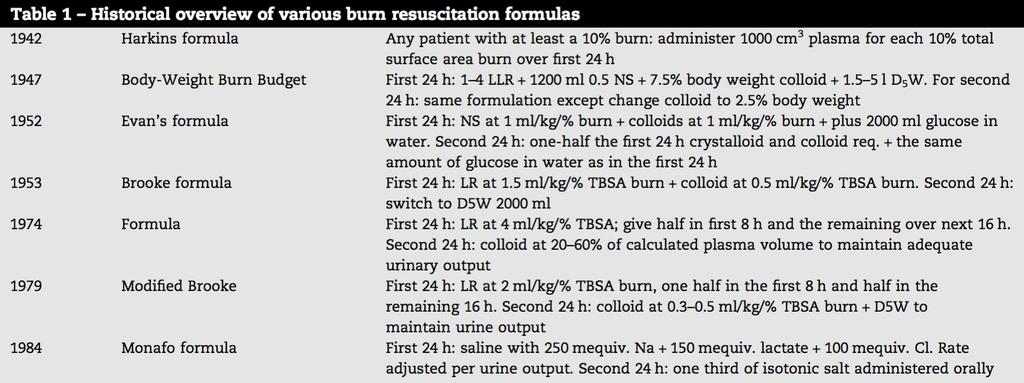
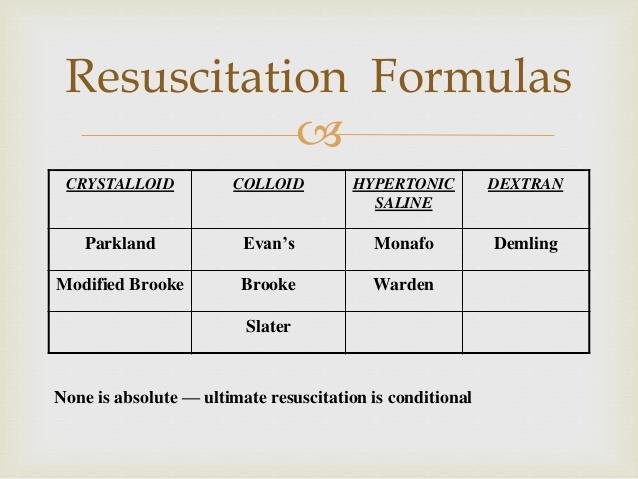
25 DR. CP Artz (San Antonio) Brooke formula 1.5 cc + colloid


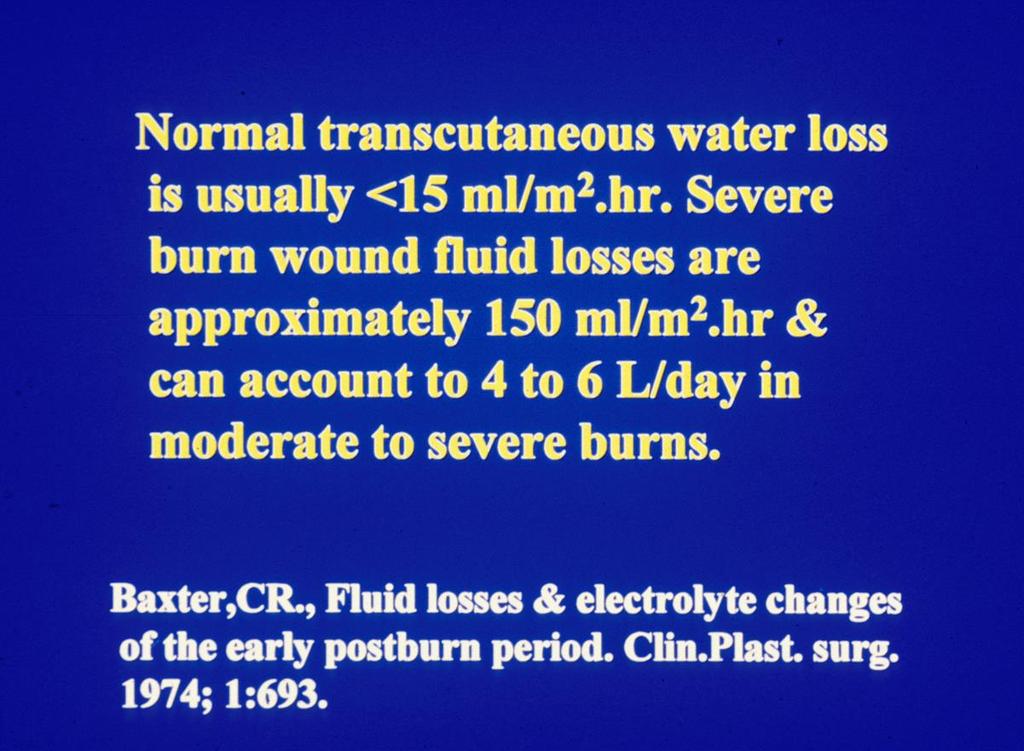
26 Dr Charles Baxter Research- Parkland 1960s Baxter, C. Clin. Plastic Surg. 1974
27
28
29

30 Any formula is only an estimate of fluid needs
31
32
33 Resuscitation Fluid Needs Related to: extent of burn (rule of nines) body size (pre-injury weight estimate) Delivered through large bore peripheral IV Attempt to avoid overlying burned skin Can use venous cut down or central line
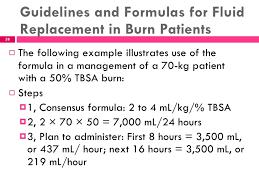
34 Resuscitation Fluid Needs: First 24 Hours Parkland Formula: Adults: 2-4 ml RL x Kg body weight x % burn Children: 3-4 ml RL x Kg body weight x % burn First half of volume over first 8 hours, second half over following 16 hours Hypovolemia, decreased CO Increased capillary permeability Crystalloid fluid is keystone, colloid not useful
35 Resuscitation Fluid Needs: Second 24 Hours Capillary permeability gradually returns to normal Colloid fluids started to minimize volume Only necessary in patients with large burns (greater than 30% TBSA) 0.5 ml of 5% albumin x Kg body weight x % burn
36 Monitoring of Resuscitation Actual volume infused will vary from calculates according to physiologic monitoring Optimal regimen: minimizes volume & salt loading prevents acute renal failure low incidence of pulmonary & cerebral edema
37 Monitoring of Resuscitation Urinary output is a reliable guide to end organ perfusion Adults: ml per hour Children (less than 30 Kg): 1 ml/kg per hour Infusion rate should be increased or decreased by 1/3 if u/o falls or exceeds limits by more than 1/3
38 Monitoring Resuscitation Blood pressure: Can be misleading due to progressive edema & vasoconstriction Heart Rate: Tachycardia commonly observed Hemaglobin & hematocrit: Not a reliable guide Transfusion not to be used for resuscitation

39 Fluid Resuscitation in the Pediatric Patient Require greater amounts of fluid Greater surface area per unit body mass More sensitive to fluid overload Lesser intravascular volume per unit surface area burned
40 MASSIVE SODIUM ADMINISTRATION IS THE COMMON DENOMINATOR IN ALL RESUSCITATION FORMULAE Example: 70 kg, 40% TBSA burn total fluid in 48 hrs Evans formula 12,400cc Brooke 12,400cc PMH 13,200cc
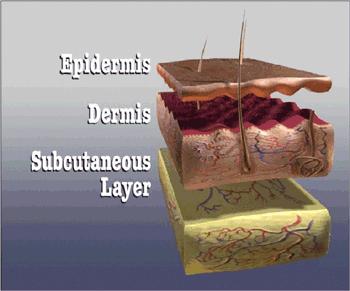
41 EVAPORATIVE WATER LOSSES Area Water Loss (gm/m 2 /24 hr) Normal Skin st degree burn nd degree burn rd degree burn 3436 Granulating wound 5138 Donor site 3590
42
43 Resuscitation Fluid Needs: Second 24 Hours Capillary permeability gradually returns to normal Colloid fluids started to minimize volume Only necessary in patients with large burns (greater than 30% TBSA) 0.5 ml of 5% albumin x Kg body weight x % burn
44 FORMULAS USED TO ESTIMATE RESUSCTATION FLUID FOR ACUTE BURNS Formula Electrolyte Colloid D5W Evans NS 1ml/kg/% 1ml/kg/% 2L Brooke LR 1.5L/kg/%.5ml/kg/% 2L PMH LR 4ml/kg/% 0 0 Shrine Galveston 5L/m 2 TBSA RL + 2L RL/ m 2 BSA 12.5gm albumin in 1 st 8 hrs Cincinnati 4ml RL/kg/% burn + 1.5L/m 2 BSA 50 meq NaHCO 3 for 8 hrs gms albumin

45 BODY MASS INDEX
46 RESUSCITATION Pearls URINE OUTPUT: Adult cc/kg/hr Pedi 1cc/kg/hr Colloid: 25% Albumin- COP of 70 mmhg vol expansion- 100cc-500cc 5%- COP of 20 mmhg vol. expan. about cc/cc Cochrane Report: human albumin no value. Provided no compelling neg. evidence in burn resus. Base deficit: at 24 hrs pb, a BD ±2 reflects adequate fluid resuscitation.

47 ABA 2008 consensus statement: Maximum: Parkland formula 4 cc Minimum: Modified Brooke formula 2cc
48
49
50 The problems of burn resuscitation formulae: a need for a simplified guideline. Bhat, S., Humphries, Y.M., Gulati, S., Rylah, B., Olson, W.E., Twomey, J. et al, Journal of Burns and Wounds. 2004;3: ED physicians (US & UK) Recall and apply a standard formula 33% and 4% successful recall
51 Rule of Ten (USAIR San Antonio) %TBSA x 10 = initial fluid rate in cc s >80kg add 100cc/10kg

52 Future Continously monitored feedback
53
HYPOVOLEMIA AND HEMORRHAGE UPDATE ON VOLUME RESUSCITATION HEMORRHAGE AND HYPOVOLEMIA DISTRIBUTION OF BODY FLUIDS 11/7/2015
 UPDATE ON VOLUME RESUSCITATION HYPOVOLEMIA AND HEMORRHAGE HUMAN CIRCULATORY SYSTEM OPERATES WITH A SMALL VOLUME AND A VERY EFFICIENT VOLUME RESPONSIVE PUMP. HOWEVER THIS PUMP FAILS QUICKLY WITH VOLUME
UPDATE ON VOLUME RESUSCITATION HYPOVOLEMIA AND HEMORRHAGE HUMAN CIRCULATORY SYSTEM OPERATES WITH A SMALL VOLUME AND A VERY EFFICIENT VOLUME RESPONSIVE PUMP. HOWEVER THIS PUMP FAILS QUICKLY WITH VOLUME
Presented by: Indah Dwi Pratiwi
 Presented by: Indah Dwi Pratiwi Normal Fluid Requirements Resuscitation Fluids Goals of Resuscitation Maintain normal body temperature In most cases, elevate the feet and legs above the level of the heart
Presented by: Indah Dwi Pratiwi Normal Fluid Requirements Resuscitation Fluids Goals of Resuscitation Maintain normal body temperature In most cases, elevate the feet and legs above the level of the heart
Maria B. ALBUJA-CRUZ, MD ALBUMIN: OVERRATED. Surgical Grand Rounds
 Maria B. ALBUJA-CRUZ, MD ALBUMIN: OVERRATED Surgical Grand Rounds ALBUMIN Most abundant plasma protein 1/3 intravascular 50% of interstitial SKIN Synthesized in hepatocytes Transcapillary escape rate COP
Maria B. ALBUJA-CRUZ, MD ALBUMIN: OVERRATED Surgical Grand Rounds ALBUMIN Most abundant plasma protein 1/3 intravascular 50% of interstitial SKIN Synthesized in hepatocytes Transcapillary escape rate COP
Burn shock ( 燒燙傷休克 ) 馬偕紀念醫院整形重建外科 姚文騰醫師 2015/10/22
 馬偕紀念醫院整形重建外科 姚文騰醫師 2015/10/22") Burn shock ( 燒燙傷休克 ) 馬偕紀念醫院整形重建外科 姚文騰醫師 2015/10/22 重建階梯 Sheet STSG FTSG Mesh Meek Stamp Meek Introduction Cutaneous thermal injury involving more than one-third of the total body surface area (TBSA)
Burn shock ( 燒燙傷休克 ) 馬偕紀念醫院整形重建外科 姚文騰醫師 2015/10/22 重建階梯 Sheet STSG FTSG Mesh Meek Stamp Meek Introduction Cutaneous thermal injury involving more than one-third of the total body surface area (TBSA)
IV Fluids. I.V. Fluid Osmolarity Composition 0.9% NaCL (Normal Saline Solution, NSS) Uses/Clinical Considerations
 Uses/Clinical Considerations") IV Fluids When administering IV fluids, the type and amount of fluid may influence patient outcomes. Make sure to understand the differences between fluid products and their effects. Crystalloids Crystalloid
IV Fluids When administering IV fluids, the type and amount of fluid may influence patient outcomes. Make sure to understand the differences between fluid products and their effects. Crystalloids Crystalloid
COBIS. Fluid Resuscitation in Adults ADULT GUIDELINE
 COBIS Fluid Resuscitation in Adults ADULT GUIDELINE Page 1 of 6 Fluid resuscitation in adults Summary Fluid resuscitation for adults with burns is indicated for patients with greater than 15% burns. Patients
COBIS Fluid Resuscitation in Adults ADULT GUIDELINE Page 1 of 6 Fluid resuscitation in adults Summary Fluid resuscitation for adults with burns is indicated for patients with greater than 15% burns. Patients
INTRAVENOUS FLUIDS. Ahmad AL-zu bi
 INTRAVENOUS FLUIDS Ahmad AL-zu bi Types of IV fluids Crystalloids colloids Crystalloids Crystalloids are aqueous solutions of low molecular weight ions,with or without glucose. Isotonic, Hypotonic, & Hypertonic
INTRAVENOUS FLUIDS Ahmad AL-zu bi Types of IV fluids Crystalloids colloids Crystalloids Crystalloids are aqueous solutions of low molecular weight ions,with or without glucose. Isotonic, Hypotonic, & Hypertonic
Albumina nel paziente critico. Savona 18 aprile 2007
 Albumina nel paziente critico Savona 18 aprile 2007 What Is Unique About Critical Care RCTs patients eligibility is primarily defined by location of care in the ICU rather than by the presence of a specific
Albumina nel paziente critico Savona 18 aprile 2007 What Is Unique About Critical Care RCTs patients eligibility is primarily defined by location of care in the ICU rather than by the presence of a specific
Principles of Infusion Therapy: Fluids
 Principles of Infusion Therapy: Fluids Christie Heinzman, MSN, APRN-CNP Acute Care Pediatric Nurse Practitioner Cincinnati Children s Hospital Medical Center May 22, 2018 Conflict of Interest Disclosure
Principles of Infusion Therapy: Fluids Christie Heinzman, MSN, APRN-CNP Acute Care Pediatric Nurse Practitioner Cincinnati Children s Hospital Medical Center May 22, 2018 Conflict of Interest Disclosure
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE
 Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Fluids and electrolytes: the basics
 Fluids and electrolytes: the basics This document is based on the handout from the Surgery for Finals course. The notes provided here summarise key aspects, focusing on areas that are popular in clinical
Fluids and electrolytes: the basics This document is based on the handout from the Surgery for Finals course. The notes provided here summarise key aspects, focusing on areas that are popular in clinical
FLUID MANAGEMENT AND BLOOD COMPONENT THERAPY
 Manual: Section: Protocol #: Approval Date: Effective Date: Revision Due Date: 10/2019 LifeLine Patient Care Protocols Adult/Pediatrics AP1-011 10/2018 10/2018 FLUID MANAGEMENT AND BLOOD COMPONENT THERAPY
Manual: Section: Protocol #: Approval Date: Effective Date: Revision Due Date: 10/2019 LifeLine Patient Care Protocols Adult/Pediatrics AP1-011 10/2018 10/2018 FLUID MANAGEMENT AND BLOOD COMPONENT THERAPY
Reverse (fluid) resuscitation Should we be doing it? NAHLA IRTIZA ISMAIL
 resuscitation Should we be doing it? NAHLA IRTIZA ISMAIL") Reverse (fluid) resuscitation Should we be doing it? NAHLA IRTIZA ISMAIL 65 Male, 60 kg D1 in ICU Admitted from OT intubated Diagnosis : septic shock secondary to necrotising fasciitis of the R lower limb
Reverse (fluid) resuscitation Should we be doing it? NAHLA IRTIZA ISMAIL 65 Male, 60 kg D1 in ICU Admitted from OT intubated Diagnosis : septic shock secondary to necrotising fasciitis of the R lower limb
Amjad Bani Hani Ass.Prof. of Cardiac Surgery & Intensive Care FLUIDS AND ELECTROLYTES
 Amjad Bani Hani Ass.Prof. of Cardiac Surgery & Intensive Care FLUIDS AND ELECTROLYTES Body Water Content Water Balance: Normal 2500 2000 1500 1000 500 Metab Food Fluids Stool Breath Sweat Urine
Amjad Bani Hani Ass.Prof. of Cardiac Surgery & Intensive Care FLUIDS AND ELECTROLYTES Body Water Content Water Balance: Normal 2500 2000 1500 1000 500 Metab Food Fluids Stool Breath Sweat Urine
How and why I give IV fluid Disclosures SCA Fluids and public health 4/1/15. Andrew Shaw MB FRCA FCCM FFICM
 How and why I give IV fluid Andrew Shaw MB FRCA FCCM FFICM Professor and Chief Cardiothoracic Anesthesiology Vanderbilt University Medical Center 2015 Disclosures Consultant for Grifols manufacturer of
How and why I give IV fluid Andrew Shaw MB FRCA FCCM FFICM Professor and Chief Cardiothoracic Anesthesiology Vanderbilt University Medical Center 2015 Disclosures Consultant for Grifols manufacturer of
Dr. Nai Shun Tsoi Department of Paediatric and Adolescent Medicine Queen Mary Hospital Hong Kong SAR
 Dr. Nai Shun Tsoi Department of Paediatric and Adolescent Medicine Queen Mary Hospital Hong Kong SAR A very important aspect in paediatric intensive care and deserve more attention Basic principle is to
Dr. Nai Shun Tsoi Department of Paediatric and Adolescent Medicine Queen Mary Hospital Hong Kong SAR A very important aspect in paediatric intensive care and deserve more attention Basic principle is to
SHOCK. Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital
 SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
-Cardiogenic: shock state resulting from impairment or failure of myocardium
 Shock chapter Shock -Condition in which tissue perfusion is inadequate to deliver oxygen, nutrients to support vital organs, cellular function -Affects all body systems -Classic signs of early shock: Tachycardia,tachypnea,restlessness,anxiety,
Shock chapter Shock -Condition in which tissue perfusion is inadequate to deliver oxygen, nutrients to support vital organs, cellular function -Affects all body systems -Classic signs of early shock: Tachycardia,tachypnea,restlessness,anxiety,
What would be the response of the sympathetic system to this patient s decrease in arterial pressure?
 CASE 51 A 62-year-old man undergoes surgery to correct a herniated disc in his spine. The patient is thought to have an uncomplicated surgery until he complains of extreme abdominal distention and pain
CASE 51 A 62-year-old man undergoes surgery to correct a herniated disc in his spine. The patient is thought to have an uncomplicated surgery until he complains of extreme abdominal distention and pain
Applicable to. Team Members Performing MD House Staff APRN/PA RN LPN
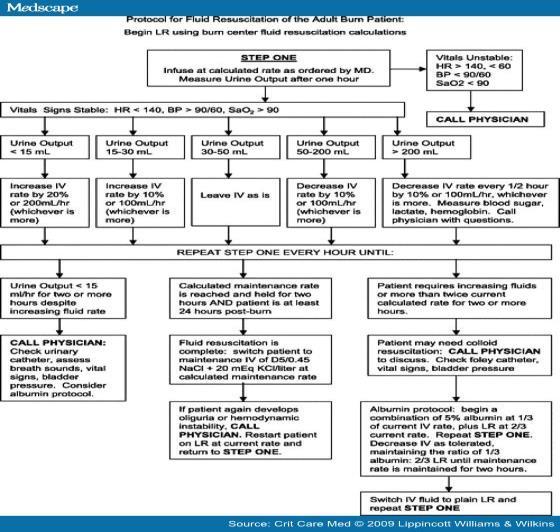
 Protocol: Adult Burn Fluid Resuscitation Category Clinical Practice Protocol Number Approval Date vember 1, 2016 Due for review vember 1, 2018 Applicable to VUH Children s DOT VMG Off-site locations VMG
Protocol: Adult Burn Fluid Resuscitation Category Clinical Practice Protocol Number Approval Date vember 1, 2016 Due for review vember 1, 2018 Applicable to VUH Children s DOT VMG Off-site locations VMG
Vasoactive Medications. Matthew J. Korobey Pharm.D., BCCCP Critical Care Clinical Specialist Mercy St. Louis
 Vasoactive Medications Matthew J. Korobey Pharm.D., BCCCP Critical Care Clinical Specialist Mercy St. Louis Objectives List components of physiology involved in blood pressure Review terminology related
Vasoactive Medications Matthew J. Korobey Pharm.D., BCCCP Critical Care Clinical Specialist Mercy St. Louis Objectives List components of physiology involved in blood pressure Review terminology related
Objectives. Initial Burn Care and Fluid Resuscitation 6/5/2015 INITIAL MANAGEMENT
 Initial Burn Care and Fluid Resuscitation Sarah Taylor MSN, RN, ACNS-BC Clinical Nurse Specialist Trauma Burn Center University of Michigan Health System Ann Arbor, MI Objectives Discuss the initial assessment
Initial Burn Care and Fluid Resuscitation Sarah Taylor MSN, RN, ACNS-BC Clinical Nurse Specialist Trauma Burn Center University of Michigan Health System Ann Arbor, MI Objectives Discuss the initial assessment
Department of Pediatrics, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok 10700, Thailand.
 SIRIRAJ MEDICAL LIBRARY SpecialIssue Clinical Practice Guide for the Management of Dengue Hemorrhagic Fever (DHF), Siriraj Hospital Kulkanya Chokephaibulkit, M.D., Wanee Wisuthsarewong, M.D., Gavivann
SIRIRAJ MEDICAL LIBRARY SpecialIssue Clinical Practice Guide for the Management of Dengue Hemorrhagic Fever (DHF), Siriraj Hospital Kulkanya Chokephaibulkit, M.D., Wanee Wisuthsarewong, M.D., Gavivann
Dr. Dafalla Ahmed Babiker Jazan University
 Dr. Dafalla Ahmed Babiker Jazan University objectives Overview Definition of dehydration Causes of dehydration Types of dehydration Diagnosis, signs and symptoms Management of dehydration Complications
Dr. Dafalla Ahmed Babiker Jazan University objectives Overview Definition of dehydration Causes of dehydration Types of dehydration Diagnosis, signs and symptoms Management of dehydration Complications
INTRODUCTION. Dengue is one of the ten leading. Globally 20 million cases/yr. 24,000 deaths/yr. It is important to know the typical and atypical
 DENGUE IN CHILDREN INTRODUCTION Dengue is one of the ten leading causes of hospitalization and death in children. Globally 20 million cases/yr. 24,000 deaths/yr. It is important to know the typical and
DENGUE IN CHILDREN INTRODUCTION Dengue is one of the ten leading causes of hospitalization and death in children. Globally 20 million cases/yr. 24,000 deaths/yr. It is important to know the typical and
Body fluid compartments Fluid Pharmacology Phases of fluid therapy. Fluid therapy during anesthesia Subcutaneous fluids
 Edward Cooper, VMD, MS, DACVECC Professor, Emergency and Critical Care The Ohio State University Body fluid compartments Fluid Pharmacology Phases of fluid therapy Resuscitation Replacement Maintenance
Edward Cooper, VMD, MS, DACVECC Professor, Emergency and Critical Care The Ohio State University Body fluid compartments Fluid Pharmacology Phases of fluid therapy Resuscitation Replacement Maintenance
L : Line and Tube อ นตรายป องก นได จากการให สารน า
 L : Line and Tube อ นตรายป องก นได จากการให สารน า รศ.นพ.กว ศ กด จ ตตว ฒนร ตน ภาคว ชาศ ลยศาสตร คณะแพทยศาสตร มหาว ทยาล ยเช ยงใหม 3 rd Mini Conference: ความปลอดภ ยในผ ป วย ร วมด วย ช วยได ท กคน ว นท 13-14
L : Line and Tube อ นตรายป องก นได จากการให สารน า รศ.นพ.กว ศ กด จ ตตว ฒนร ตน ภาคว ชาศ ลยศาสตร คณะแพทยศาสตร มหาว ทยาล ยเช ยงใหม 3 rd Mini Conference: ความปลอดภ ยในผ ป วย ร วมด วย ช วยได ท กคน ว นท 13-14
Body fluids. Lecture 13:
 Lecture 13: Body fluids Body fluids are distributed in compartments: A. Intracellular compartment: inside the cells of the body (two thirds) B. Extracellular compartment: (one third) it is divided into
Lecture 13: Body fluids Body fluids are distributed in compartments: A. Intracellular compartment: inside the cells of the body (two thirds) B. Extracellular compartment: (one third) it is divided into
KASHVET VETERINARIAN RESOURCES FLUID THERAPY AND SELECTION OF FLUIDS
 KASHVET VETERINARIAN RESOURCES FLUID THERAPY AND SELECTION OF FLUIDS INTRODUCTION Formulating a fluid therapy plan for the critical small animal patient requires careful determination of the current volume
KASHVET VETERINARIAN RESOURCES FLUID THERAPY AND SELECTION OF FLUIDS INTRODUCTION Formulating a fluid therapy plan for the critical small animal patient requires careful determination of the current volume
12/1/2009. Chapter 19: Hemorrhage. Hemorrhage and Shock Occurs when there is a disruption or leak in the vascular system Internal hemorrhage
 Chapter 19: Hemorrhage Hemorrhage and Shock Occurs when there is a disruption or leak in the vascular system External hemorrhage Internal hemorrhage Associated with higher morbidity and mortality than
Chapter 19: Hemorrhage Hemorrhage and Shock Occurs when there is a disruption or leak in the vascular system External hemorrhage Internal hemorrhage Associated with higher morbidity and mortality than
Kristan Staudenmayer, MD Stanford University, Stanford, CA
 Kristan Staudenmayer, MD Stanford University, Stanford, CA Fluid resuscitation Variety of fluids How to administer What you do DOES matter WWII 1942 North Africa high mortality from hemorrhaghic shock
Kristan Staudenmayer, MD Stanford University, Stanford, CA Fluid resuscitation Variety of fluids How to administer What you do DOES matter WWII 1942 North Africa high mortality from hemorrhaghic shock
Staging Sepsis for the Emergency Department: Physician
 Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Implementing therapy-delivery, dose adjustments and fluid balance. Eileen Lischer MA, BSN, RN, CNN University of California San Diego March 6, 2018
 Implementing therapy-delivery, dose adjustments and fluid balance. Eileen Lischer MA, BSN, RN, CNN University of California San Diego March 6, 2018 Objectives By the end of this session the learner will
Implementing therapy-delivery, dose adjustments and fluid balance. Eileen Lischer MA, BSN, RN, CNN University of California San Diego March 6, 2018 Objectives By the end of this session the learner will
Causes of Edema That Result From an Increased Capillary Pressure. Student Name. Institution Affiliation
 Running Head: CAUSES OF EDEMA 1 Causes of Edema That Result From an Increased Capillary Pressure Student Name Institution Affiliation CAUSES OF EDEMA 2 Causes of Edema That Result From an Increased Capillary
Running Head: CAUSES OF EDEMA 1 Causes of Edema That Result From an Increased Capillary Pressure Student Name Institution Affiliation CAUSES OF EDEMA 2 Causes of Edema That Result From an Increased Capillary
How Well Does The Parkland Formula Estimate Actual Fluid Resuscitation Volumes?
 How Well Does The Parkland Formula Estimate Actual Fluid Resuscitation Volumes? Robert C. Cartotto, MD, FRCS(C), Marilyn Innes, BA, Melinda A. Musgrave, PhD, MD, Manuel Gomez, MD, Andrew B. Cooper, MD,
How Well Does The Parkland Formula Estimate Actual Fluid Resuscitation Volumes? Robert C. Cartotto, MD, FRCS(C), Marilyn Innes, BA, Melinda A. Musgrave, PhD, MD, Manuel Gomez, MD, Andrew B. Cooper, MD,
HIGH-DOSE ASCORBIC ACID AND FLUID RESUSCITATION REQUIREMENTS IN MASSIVE BURN INJURY A REAL IMPACT?
 HIGH-DOSE ASCORBIC ACID AND FLUID RESUSCITATION REQUIREMENTS IN MASSIVE BURN INJURY A REAL IMPACT? P. Stoecklin, Y.A. Que, P. Voirol, H. Engel, M.M. Berger Service de Médecine Intensive Adulte et Centre
HIGH-DOSE ASCORBIC ACID AND FLUID RESUSCITATION REQUIREMENTS IN MASSIVE BURN INJURY A REAL IMPACT? P. Stoecklin, Y.A. Que, P. Voirol, H. Engel, M.M. Berger Service de Médecine Intensive Adulte et Centre
Categories & Complications
 Shock, Fluid & Therapy Arthur Jones, EdD, RRT Learning Objectives: Explain the etiologies, manifestations and management of shock. Describe specific agents used to maintain blood pressure, fluid balance
Shock, Fluid & Therapy Arthur Jones, EdD, RRT Learning Objectives: Explain the etiologies, manifestations and management of shock. Describe specific agents used to maintain blood pressure, fluid balance
Salty Solutions or Salty Problems? Outline. Outline 29/04/2013
 Salty Solutions or Salty Problems? 18 th October 2012 Richard Seigne Anaesthetist 1 - Non fluid 40% T o t a l b o d y f l u i d 60% NaCl NaCl Intra-cellular fluid 2/3 KCl Interstitial fluid 3/4 of ECF
Salty Solutions or Salty Problems? 18 th October 2012 Richard Seigne Anaesthetist 1 - Non fluid 40% T o t a l b o d y f l u i d 60% NaCl NaCl Intra-cellular fluid 2/3 KCl Interstitial fluid 3/4 of ECF
Basic Fluid and Electrolytes
 Basic Fluid and Electrolytes Chapter 22 Basic Fluid and Electrolytes Introduction Infants and young children have a greater need for water and are more vulnerable to alterations in fluid and electrolyte
Basic Fluid and Electrolytes Chapter 22 Basic Fluid and Electrolytes Introduction Infants and young children have a greater need for water and are more vulnerable to alterations in fluid and electrolyte
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal compartment syndrome, as complication of fluid resuscitation, 331 338 abdominal perfusion pressure, 332 fluid restriction practice
Index Note: Page numbers of article titles are in boldface type. A Abdominal compartment syndrome, as complication of fluid resuscitation, 331 338 abdominal perfusion pressure, 332 fluid restriction practice
Surgical Resuscitation Management in Poly-Trauma Patients
 Surgical Resuscitation Management in Poly-Trauma Patients Andrew Bernard, MD FACS Paul Kearney MD Chair of Trauma Surgery Associate Professor Medical Director of Trauma and Acute Care Surgery UK Healthcare
Surgical Resuscitation Management in Poly-Trauma Patients Andrew Bernard, MD FACS Paul Kearney MD Chair of Trauma Surgery Associate Professor Medical Director of Trauma and Acute Care Surgery UK Healthcare
Faith Borunda, MSN-RN, CCRN, CPTC Senior Director of Regional Operations Southwest Transplant Alliance
 Faith Borunda, MSN-RN, CCRN, CPTC Senior Director of Regional Operations Southwest Transplant Alliance The Never -Ending Need 114,401 in the U.S. wait for a lifesaving transplant * United Network for Organ
Faith Borunda, MSN-RN, CCRN, CPTC Senior Director of Regional Operations Southwest Transplant Alliance The Never -Ending Need 114,401 in the U.S. wait for a lifesaving transplant * United Network for Organ
How Normal Body Processes Are Altered By Disease and Injury
 1 Chapter 4, GENERAL PRINCIPLES OF PATHOPHYSIOLOGY. Part 1 How Normal Body Processes Are Altered By Disease and Injury 2 How Cells Respond to Change and Injury 3 Pathology & Pathophysiology : the study
1 Chapter 4, GENERAL PRINCIPLES OF PATHOPHYSIOLOGY. Part 1 How Normal Body Processes Are Altered By Disease and Injury 2 How Cells Respond to Change and Injury 3 Pathology & Pathophysiology : the study
Written 01/09/17 Rewritten 3/29/17 for Interior Regional EMS Symposium
 Written 01/09/17 Rewritten 3/29/17 for Interior Regional EMS Symposium MARIA E. MANDICH MD Fairbanks Memorial Hospital Emergency Department Attending Physician Interior Region EMS Council Medical Director
Written 01/09/17 Rewritten 3/29/17 for Interior Regional EMS Symposium MARIA E. MANDICH MD Fairbanks Memorial Hospital Emergency Department Attending Physician Interior Region EMS Council Medical Director
Shock and hemodynamic monitorization. Nilüfer Yalındağ Öztürk Marmara University Pendik Research and Training Hospital
 Shock and hemodynamic monitorization Nilüfer Yalındağ Öztürk Marmara University Pendik Research and Training Hospital Shock Leading cause of morbidity and mortality Worldwide: dehydration and hypovolemic
Shock and hemodynamic monitorization Nilüfer Yalındağ Öztürk Marmara University Pendik Research and Training Hospital Shock Leading cause of morbidity and mortality Worldwide: dehydration and hypovolemic
Blood Vessels. Chapter 20
 Blood Vessels Chapter 20 Summary of the Characteristics of Arteries and Veins Characteristic Artery Vein Wall thickness thick thin Shape in cross section round flattened Thickest tunic media externa Collagen
Blood Vessels Chapter 20 Summary of the Characteristics of Arteries and Veins Characteristic Artery Vein Wall thickness thick thin Shape in cross section round flattened Thickest tunic media externa Collagen
How to maintain optimal perfusion during Cardiopulmonary By-pass. Herdono Poernomo, MD
 How to maintain optimal perfusion during Cardiopulmonary By-pass Herdono Poernomo, MD Cardiopulmonary By-pass Target Physiologic condition as a healthy person Everything is in Normal Limit How to maintain
How to maintain optimal perfusion during Cardiopulmonary By-pass Herdono Poernomo, MD Cardiopulmonary By-pass Target Physiologic condition as a healthy person Everything is in Normal Limit How to maintain
Going on Bypass. What happens before, during and after CPB. Perfusion Dept. Royal Children s Hospital Melbourne, Australia
 Going on Bypass What happens before, during and after CPB. Perfusion Dept. Royal Children s Hospital Melbourne, Australia Circulation Brain Liver Kidneys Viscera Muscle Skin IVC, SVC Pump Lungs R.A. L.V.
Going on Bypass What happens before, during and after CPB. Perfusion Dept. Royal Children s Hospital Melbourne, Australia Circulation Brain Liver Kidneys Viscera Muscle Skin IVC, SVC Pump Lungs R.A. L.V.
SLCOA National Guidelines
 SLCOA National Guidelines Peri - operative Fluid & Electrolyte Management SLCOA National Guidelines Contents List of Contributors 92 Paediatric fasting guidelines for elective procedures 93 Guidelines
SLCOA National Guidelines Peri - operative Fluid & Electrolyte Management SLCOA National Guidelines Contents List of Contributors 92 Paediatric fasting guidelines for elective procedures 93 Guidelines
The Parkland Formula Under Fire: Is the Criticism Justified?
 The Parkland Formula Under Fire: Is the Criticism Justified? Jennifer Blumetti, MD, John L. Hunt, MD, Brett D. Arnoldo, MD, Jennifer K. Parks, MPH, Gary F. Purdue, MD Controversy has continued regarding
The Parkland Formula Under Fire: Is the Criticism Justified? Jennifer Blumetti, MD, John L. Hunt, MD, Brett D. Arnoldo, MD, Jennifer K. Parks, MPH, Gary F. Purdue, MD Controversy has continued regarding
Wet Lungs Dry lungs Impact on Outcome in ARDS. Charlie Phillips MD Division of PCCM OHSU 2009
 Wet Lungs Dry lungs Impact on Outcome in ARDS Charlie Phillips MD Division of PCCM OHSU 2009 Today s talk Pathophysiology of ARDS The case for dry Targeting EVLW Disclosures Advisor for Pulsion Medical
Wet Lungs Dry lungs Impact on Outcome in ARDS Charlie Phillips MD Division of PCCM OHSU 2009 Today s talk Pathophysiology of ARDS The case for dry Targeting EVLW Disclosures Advisor for Pulsion Medical
Rq : Serum = plasma w/ fibrinogen and other other proteins involved in clotting removed.
 Functions of the blood Transport Nutritive Respiratory Excretory Hormone transport Temperature regulation Acid base balance ph (7.30 7.45) Protective (immunology) Rq : It comprises both ECF (plasma) &
Functions of the blood Transport Nutritive Respiratory Excretory Hormone transport Temperature regulation Acid base balance ph (7.30 7.45) Protective (immunology) Rq : It comprises both ECF (plasma) &
Sepsis: Identification and Management in an Acute Care Setting
 Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
Conflicts of Interest
 Anesthesia for Major Abdominal Cancer Resection John E. Ellis MD Adjunct Professor University of Pennsylvania johnellis1700@gmail.com Conflicts of Interest 1 Upper Abdominal Surgery Focus on oncologic
Anesthesia for Major Abdominal Cancer Resection John E. Ellis MD Adjunct Professor University of Pennsylvania johnellis1700@gmail.com Conflicts of Interest 1 Upper Abdominal Surgery Focus on oncologic
"Small Volume" Resuscitation for Trauma Cases : PRO Aspects
 "Small Volume" Resuscitation for Trauma Cases : PRO Aspects Jim Holliman, M.D., F.A.C.E.P. Program Manager, Afghanistan Health Care Sector Reconstruction Project Center for Disaster and Humanitarian Assistance
"Small Volume" Resuscitation for Trauma Cases : PRO Aspects Jim Holliman, M.D., F.A.C.E.P. Program Manager, Afghanistan Health Care Sector Reconstruction Project Center for Disaster and Humanitarian Assistance
Cardiovascular Module
 Cardiovascular Module Cardiovascular Physiology Lect. Six Microcirculation & Lymphatics (Edema formation) Prof. Dr. Najeeb Hassan Mohammed The microcirculation and the lymphatic system The microcirculation
Cardiovascular Module Cardiovascular Physiology Lect. Six Microcirculation & Lymphatics (Edema formation) Prof. Dr. Najeeb Hassan Mohammed The microcirculation and the lymphatic system The microcirculation
Fluids in ICU. JMO teaching 5th July 2016
 Fluids in ICU JMO teaching 5th July 2016 Objectives Physiology of fluid infusion History of fluid resuscitation Physiology of fluid resuscitation Types of resuscitation fluid The ideal resuscitation fluid
Fluids in ICU JMO teaching 5th July 2016 Objectives Physiology of fluid infusion History of fluid resuscitation Physiology of fluid resuscitation Types of resuscitation fluid The ideal resuscitation fluid
Burn injury. A : patent airway with smoking inhalation, stridor. D: E4V5M6,pupil 2mm RTLBE
 Burn injury Pinyong Uthaitas Emergency Department Faculty of Medicine, Ramathibodi Hospital A Thai man 52 year old came to the hospital due to flam burn ½ hr ago at his house. He gain conscious but hoarseness
Burn injury Pinyong Uthaitas Emergency Department Faculty of Medicine, Ramathibodi Hospital A Thai man 52 year old came to the hospital due to flam burn ½ hr ago at his house. He gain conscious but hoarseness
3/14/2017. Pediatric Sepsis: From Goal Directed Therapy to Protocolized Care. Objectives. Developmental Response to Sepsis
 Pediatric Sepsis: From Goal Directed Therapy to Protocolized Care March 20, 2017 Reid WD Farris, MS MD Objectives Review the evolution & current state of the pediatric septic shock treatment guidelines
Pediatric Sepsis: From Goal Directed Therapy to Protocolized Care March 20, 2017 Reid WD Farris, MS MD Objectives Review the evolution & current state of the pediatric septic shock treatment guidelines
Hypo/Hypernatremia. Stuart L. Goldstein MD. Director, Center for Acute Care Nephrology Cincinnati Children s Hospital
 Hypo/Hypernatremia Stuart L. Goldstein MD Director, Center for Acute Care Nephrology Cincinnati Children s Hospital Objectives Understand Fluid cellular shifts Understand maintenance fluid and calculations
Hypo/Hypernatremia Stuart L. Goldstein MD Director, Center for Acute Care Nephrology Cincinnati Children s Hospital Objectives Understand Fluid cellular shifts Understand maintenance fluid and calculations
Dr. Carlos Fernando Estrada Garzona. Departamento de Farmacología Universidad de Costa Rica
 Dr. Carlos Fernando Estrada Garzona Departamento de Farmacología Universidad de Costa Rica OBJETIVOS FISIOLOGIA LIQUIDOS CORPORALES SOLUCIONES PARENTERALES PRINCIPIOS DE FLUIDOTERAPIA CRISTALOIDE VS COLOIDE
Dr. Carlos Fernando Estrada Garzona Departamento de Farmacología Universidad de Costa Rica OBJETIVOS FISIOLOGIA LIQUIDOS CORPORALES SOLUCIONES PARENTERALES PRINCIPIOS DE FLUIDOTERAPIA CRISTALOIDE VS COLOIDE
COBIS Fluid Resuscitation of Childhood Burns PAEDIATRIC
 COBIS Fluid Resuscitation of Childhood Burns PAEDIATRIC Aim To promote a unified approach to fluid resuscitation of children with thermal injuries in Scotland, including the immediate resuscitation in
COBIS Fluid Resuscitation of Childhood Burns PAEDIATRIC Aim To promote a unified approach to fluid resuscitation of children with thermal injuries in Scotland, including the immediate resuscitation in
Principles of Fluid Balance
 Principles of Fluid Balance I. The Cellular Environment: Fluids and Electrolytes A. Water 1. Total body water (TBW) = 60% of total body weight 2. Fluid Compartments in the Body a. Intracellular Compartment
Principles of Fluid Balance I. The Cellular Environment: Fluids and Electrolytes A. Water 1. Total body water (TBW) = 60% of total body weight 2. Fluid Compartments in the Body a. Intracellular Compartment
12/29/2014. IV/IO Therapy & Fluid Administration. Objectives. Cleansing of the soul
 IV/IO Therapy & Fluid Administration Gary Hoertz, EMT-P Spokane County EMS Indications for IV Access Types of Intravenous Access IV fluids Flow Rates Fluid resuscitation Objectives Cleansing of the soul
IV/IO Therapy & Fluid Administration Gary Hoertz, EMT-P Spokane County EMS Indications for IV Access Types of Intravenous Access IV fluids Flow Rates Fluid resuscitation Objectives Cleansing of the soul
THe Story of salty Sam
 THe Story of salty Sam Understanding fluids, urea and electrolyte balance; a quantitative approach. A self-directed learning activity. Part One. meet salty sam Salty Sam is a pretty average 70 kg bloke,
THe Story of salty Sam Understanding fluids, urea and electrolyte balance; a quantitative approach. A self-directed learning activity. Part One. meet salty sam Salty Sam is a pretty average 70 kg bloke,
Over- and underfill: not all nephrotic states are equal. Detlef Bockenhauer
 Over- and underfill: not all nephrotic states are equal Detlef Bockenhauer Objectives Review pathophysiology of oedema: undervs overfill Treatment options The clinical setting: case 1 A6-y old girl with
Over- and underfill: not all nephrotic states are equal Detlef Bockenhauer Objectives Review pathophysiology of oedema: undervs overfill Treatment options The clinical setting: case 1 A6-y old girl with
Purist? or Pragmatist? Assessment & Management of ICU Volume Status
 Assessment & Management of ICU Volume Status 9 th Annual Rocky Mountain Hospital Medicine Symposium Denver, Colorado Paula Dennen, MD Assistant Professor of Medicine Nephrology and Critical Care Medicine
Assessment & Management of ICU Volume Status 9 th Annual Rocky Mountain Hospital Medicine Symposium Denver, Colorado Paula Dennen, MD Assistant Professor of Medicine Nephrology and Critical Care Medicine
Shock. William Schecter, MD
 Shock William Schecter, MD The Cell as a furnace O 2 1 mole Glucose Cell C0 2 ATP 38 moles H 2 0 Shock = Inadequate Delivery of 02 and Glucose to the Cell 0 2 Cell ATP 2 moles Lactic Acid Treatment of
Shock William Schecter, MD The Cell as a furnace O 2 1 mole Glucose Cell C0 2 ATP 38 moles H 2 0 Shock = Inadequate Delivery of 02 and Glucose to the Cell 0 2 Cell ATP 2 moles Lactic Acid Treatment of
SHOCK AETIOLOGY OF SHOCK (1) Inadequate circulating blood volume ) Loss of Autonomic control of the vasculature (3) Impaired cardiac function
 Inadequate circulating blood volume ) Loss of Autonomic control of the vasculature (3) Impaired cardiac function") SHOCK Shock is a condition in which the metabolic needs of the body are not met because of an inadequate cardiac output. If tissue perfusion can be restored in an expeditious fashion, cellular injury may
SHOCK Shock is a condition in which the metabolic needs of the body are not met because of an inadequate cardiac output. If tissue perfusion can be restored in an expeditious fashion, cellular injury may
25. Fluid Management and Renal Function During a Laparoscopic Case Done Under CO 2 Pneumoperitoneum
 25. Fluid Management and Renal Function During a Laparoscopic Case Done Under CO 2 Pneumoperitoneum Gamal Mostafa, M.D. Frederick L. Greene, M.D. Minimally invasive surgery aims to attenuate the stress
25. Fluid Management and Renal Function During a Laparoscopic Case Done Under CO 2 Pneumoperitoneum Gamal Mostafa, M.D. Frederick L. Greene, M.D. Minimally invasive surgery aims to attenuate the stress
Paediatric Shock. Dr Andrew Pittaway Department of Anaesthesia Bristol Royal Hospital for Children Bristol, UK
 Paediatric Shock Dr Andrew Pittaway Department of Anaesthesia Bristol Royal Hospital for Children Bristol, UK Self-assessment: 1. What is the definition of shock? 2. List the different pathophysiological
Paediatric Shock Dr Andrew Pittaway Department of Anaesthesia Bristol Royal Hospital for Children Bristol, UK Self-assessment: 1. What is the definition of shock? 2. List the different pathophysiological
TBSA Burn Estimation Chart Adult Major Burn Clinical Practice Guideline
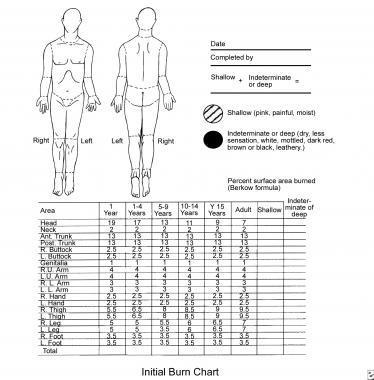
 TBSA Burn Estimation Chart Adult Major Burn Clinical Practice Guideline Patient Label Anatomical Subunit Percent Total Percent One Side Anterior Posterior Injury Subtotal 3.5% 2nd and 3rd degree burns
TBSA Burn Estimation Chart Adult Major Burn Clinical Practice Guideline Patient Label Anatomical Subunit Percent Total Percent One Side Anterior Posterior Injury Subtotal 3.5% 2nd and 3rd degree burns
What is. InSpectra StO 2?
 What is InSpectra StO 2? www.htibiomeasurement.com What is InSpectra StO 2? Hemoglobin O 2 saturation is measured in three areas: 1) Arterial (SaO 2, SpO 2 ) Assesses how well oxygen is loading onto hemoglobin
What is InSpectra StO 2? www.htibiomeasurement.com What is InSpectra StO 2? Hemoglobin O 2 saturation is measured in three areas: 1) Arterial (SaO 2, SpO 2 ) Assesses how well oxygen is loading onto hemoglobin
John Park, MD Assistant Professor of Medicine
 John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
Fundamentals of Pharmacology for Veterinary Technicians Chapter 19
 Figure 19-1 Figure 19-2A Figure 19-2B Figure 19-3 Figure 19-4A1 Figure 19-4A2 Figure 19-4B Figure 19-4C Figure 19-4D Figure 19-5 Figure 19-6A Figure 19-6B A Figure 19-7A B Figure 19-7B C Figure 19-7C D
Figure 19-1 Figure 19-2A Figure 19-2B Figure 19-3 Figure 19-4A1 Figure 19-4A2 Figure 19-4B Figure 19-4C Figure 19-4D Figure 19-5 Figure 19-6A Figure 19-6B A Figure 19-7A B Figure 19-7B C Figure 19-7C D
SHOCK. Pathophysiology
 SHOCK Dr. Ahmed Saleem FICMS TUCOM / 3rd Year / 2015 Shock is the most common and therefore the most important cause of death of surgical patients. Death may occur rapidly due to a profound state of shock,
SHOCK Dr. Ahmed Saleem FICMS TUCOM / 3rd Year / 2015 Shock is the most common and therefore the most important cause of death of surgical patients. Death may occur rapidly due to a profound state of shock,
ORIGINAL ARTICLE. Marc G. Jeschke, MD; Robert E. Barrow, PhD; Steven E. Wolf, MD; David N. Herndon, MD
 ORIGINAL ARTICLE Mortality in Burned Children With Acute Renal Failure Marc G. Jeschke, MD; Robert E. Barrow, PhD; Steven E. Wolf, MD; David N. Herndon, MD Background: During the past 13 years, mortality
ORIGINAL ARTICLE Mortality in Burned Children With Acute Renal Failure Marc G. Jeschke, MD; Robert E. Barrow, PhD; Steven E. Wolf, MD; David N. Herndon, MD Background: During the past 13 years, mortality
Renal Regulation of Sodium and Volume. Dr. Dave Johnson Associate Professor Dept. Physiology UNECOM
 Renal Regulation of Sodium and Volume Dr. Dave Johnson Associate Professor Dept. Physiology UNECOM Maintaining Volume Plasma water and sodium (Na + ) are regulated independently - you are already familiar
Renal Regulation of Sodium and Volume Dr. Dave Johnson Associate Professor Dept. Physiology UNECOM Maintaining Volume Plasma water and sodium (Na + ) are regulated independently - you are already familiar
Resuscitation targets in severe burns. ASMIC 2015 Dr Kamal Bashar Abu Bakar 14th August 2015
 Resuscitation targets in severe burns ASMIC 2015 Dr Kamal Bashar Abu Bakar 14th August 2015 Disclaimer Resuscitation targets in severe burns Resuscitation Aim of resuscitation 1. Re-expanding the intra
Resuscitation targets in severe burns ASMIC 2015 Dr Kamal Bashar Abu Bakar 14th August 2015 Disclaimer Resuscitation targets in severe burns Resuscitation Aim of resuscitation 1. Re-expanding the intra
FLUID THERAPY: IT S MORE THAN JUST LACTATED RINGERS
 FLUID THERAPY: IT S MORE THAN JUST LACTATED RINGERS Elisa M. Mazzaferro, MS, DVM, PhD, DACVECC Cornell University Veterinary Specialists, Stamford, CT, USA Total body water constitutes approximately 60%
FLUID THERAPY: IT S MORE THAN JUST LACTATED RINGERS Elisa M. Mazzaferro, MS, DVM, PhD, DACVECC Cornell University Veterinary Specialists, Stamford, CT, USA Total body water constitutes approximately 60%
Non-cardiogenic pulmonary oedema
 Zurich Open Repository and Archive University of Zurich Main Library Strickhofstrasse 39 CH-8057 Zurich www.zora.uzh.ch Year: 2012 Non-cardiogenic pulmonary oedema Glaus, T M Posted at the Zurich Open
Zurich Open Repository and Archive University of Zurich Main Library Strickhofstrasse 39 CH-8057 Zurich www.zora.uzh.ch Year: 2012 Non-cardiogenic pulmonary oedema Glaus, T M Posted at the Zurich Open
What is the Role of Albumin in Sepsis? An Evidenced Based Affair. Justin Belsky MD PGY3 2/6/14
 What is the Role of Albumin in Sepsis? An Evidenced Based Affair Justin Belsky MD PGY3 2/6/14 Microcirculation https://www.youtube.com/watch?v=xao1gsyur7q Capillary Leak in Sepsis Asking the RIGHT Question
What is the Role of Albumin in Sepsis? An Evidenced Based Affair Justin Belsky MD PGY3 2/6/14 Microcirculation https://www.youtube.com/watch?v=xao1gsyur7q Capillary Leak in Sepsis Asking the RIGHT Question
INTRAVENOUS FLUID THERAPY. Tom Heaps Consultant Acute Physician
 INTRAVENOUS FLUID THERAPY Tom Heaps Consultant Acute Physician LEARNING OBJECTIVES 1. Crystalloids vs colloids 2. Balanced vs non-balanced solutions 3. Composition of various IV fluids 4. What is normal
INTRAVENOUS FLUID THERAPY Tom Heaps Consultant Acute Physician LEARNING OBJECTIVES 1. Crystalloids vs colloids 2. Balanced vs non-balanced solutions 3. Composition of various IV fluids 4. What is normal
The Septic Patient. Dr Arunraj Navaratnarajah. Renal SpR Imperial College NHS Healthcare Trust
 The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
Fluids and Lactate. A/Prof Peter Morley
 Fluids and Lactate A/Prof Peter Morley RCTs Other evidence 5 6 Plan Background information Crystalloids Which crystalloid? Colloids Crystalloids v colloids Once that s settled, how much fluid Plan Background
Fluids and Lactate A/Prof Peter Morley RCTs Other evidence 5 6 Plan Background information Crystalloids Which crystalloid? Colloids Crystalloids v colloids Once that s settled, how much fluid Plan Background
Burns Management in the Emergency Department
 Management in the Emergency Department (Referral Proforma) Time/Date of injury (24hr) Patient demographic data sticker Airway Please remember to protect C-spine until clinically cleared as stable Administer
Management in the Emergency Department (Referral Proforma) Time/Date of injury (24hr) Patient demographic data sticker Airway Please remember to protect C-spine until clinically cleared as stable Administer
Pediatric Burn Management Justin D. Klein, MD Associate Burn Director Lisa C. Vitale, RN Burn Program Coordinator
 Pediatric Burn Management Justin D. Klein, MD Associate Burn Director Lisa C. Vitale, RN Burn Program Coordinator Lecture Overview Burn statistics and etiologies Pre-hospital evaluation Anatomy of a burn
Pediatric Burn Management Justin D. Klein, MD Associate Burn Director Lisa C. Vitale, RN Burn Program Coordinator Lecture Overview Burn statistics and etiologies Pre-hospital evaluation Anatomy of a burn
Fluid Therapy What, when and how much? Michael Ethier DVM, DVSc, DACVECC Toronto Veterinary Emergency Hospital
 Fluid Therapy What, when and how much? Michael Ethier DVM, DVSc, DACVECC Toronto Veterinary Emergency Hospital Intravenous fluids are one of the most common therapies administered to hospitalized patients,
Fluid Therapy What, when and how much? Michael Ethier DVM, DVSc, DACVECC Toronto Veterinary Emergency Hospital Intravenous fluids are one of the most common therapies administered to hospitalized patients,
Intravenous Fluid Therapy in Critical Illness
 Intravenous Fluid Therapy in Critical Illness GINA HURST, MD DIVISION OF EMERGENCY CRITICAL CARE HENRY FORD HOSPITAL DETROIT, MI Objectives Establish goals of IV fluid therapy Review fluid types and availability
Intravenous Fluid Therapy in Critical Illness GINA HURST, MD DIVISION OF EMERGENCY CRITICAL CARE HENRY FORD HOSPITAL DETROIT, MI Objectives Establish goals of IV fluid therapy Review fluid types and availability
Nursing Process Focus: Patients Receiving Dextran 40 (Gentran 40)
") Assess for presence/history of hypovolemia, shock, venous thrombosis. Assess vital signs: Hypovolemic shock secondary to surgery, burns, hemorrhage, other serious condition PT and PTT abnormalities Venous
Assess for presence/history of hypovolemia, shock, venous thrombosis. Assess vital signs: Hypovolemic shock secondary to surgery, burns, hemorrhage, other serious condition PT and PTT abnormalities Venous
Wisecracks 1. What are the indications for an escharotomy 2. What are the primary considerations in mechanical ventilation of burn patients
 Chapter 63 Thermal Burns Episode Overview Questions 1. List zones of burns 2. List 6 indications for intubation in the burn patient 3. List and describe 2 formulas for fluid resuscitation 4. Describe depth
Chapter 63 Thermal Burns Episode Overview Questions 1. List zones of burns 2. List 6 indications for intubation in the burn patient 3. List and describe 2 formulas for fluid resuscitation 4. Describe depth
Fluid balance in the critically ill child with dengue Too much too little? Professor Lucy Lum Universiti Malaya ASMIC Sept
 Fluid balance in the critically ill child with dengue Too much too little? Professor Lucy Lum Universiti Malaya ASMIC 2018 21-23 Sept CFR 0.22 in 2017 0.15 in 2018 2 Lecture Contents: Dynamic disease Self-limiting
Fluid balance in the critically ill child with dengue Too much too little? Professor Lucy Lum Universiti Malaya ASMIC 2018 21-23 Sept CFR 0.22 in 2017 0.15 in 2018 2 Lecture Contents: Dynamic disease Self-limiting
Blood products and plasma substitutes
 Blood products and plasma substitutes Plasma substitutes Dextran 70 and polygeline are macromolecular substances which are metabolized slowly; they may be used to expand and maintain blood volume in shock
Blood products and plasma substitutes Plasma substitutes Dextran 70 and polygeline are macromolecular substances which are metabolized slowly; they may be used to expand and maintain blood volume in shock
CSL Behring LLC Albuminar -25 US Package Insert Albumin (Human) USP, 25% Revised: 01/2008 Page 1
 USP, 25% Revised: 01/2008 Page 1") Page 1 CSL Behring Albuminar -25 Albumin (Human) USP, 25% R x only DESCRIPTION Albuminar -25, Albumin (Human) 25%, is a sterile aqueous solution of albumin obtained from large pools of adult human venous
Page 1 CSL Behring Albuminar -25 Albumin (Human) USP, 25% R x only DESCRIPTION Albuminar -25, Albumin (Human) 25%, is a sterile aqueous solution of albumin obtained from large pools of adult human venous
Fluids: occult effects. S Magder Department of Critical Care, McGill University Health Centre
 Fluids: occult effects S Magder Department of Critical Care, McGill University Health Centre Why is volume important? 1. Water is essential to dissolve substances and allow them to diffuse 2. Necessary
Fluids: occult effects S Magder Department of Critical Care, McGill University Health Centre Why is volume important? 1. Water is essential to dissolve substances and allow them to diffuse 2. Necessary
Children's National Medical Center The Division of Trauma and Burn Burn Education Module Post-test
 Children's National Medical Center The Division of Trauma and Burn Burn Education Module Post-test Purpose: To provide nurses with on overview of burn injuries in pediatric patients. Learning Objectives:
Children's National Medical Center The Division of Trauma and Burn Burn Education Module Post-test Purpose: To provide nurses with on overview of burn injuries in pediatric patients. Learning Objectives:
How Normal Body Processes Are Altered By Disease and Injury
 1 Chapter 4, General Principles of Pathophysiology Part 1 How Normal Body Processes Are Altered By Disease and Injury 2 How Cells Respond to Change and Injury 3 Pathology & Pathophysiology : the study
1 Chapter 4, General Principles of Pathophysiology Part 1 How Normal Body Processes Are Altered By Disease and Injury 2 How Cells Respond to Change and Injury 3 Pathology & Pathophysiology : the study
Burn Injuries & Its Management M JARI.MD
 Burn Injuries & Its Management M JARI.MD 1 BURNS Wounds caused by exposure to: 1. excessive heat 2. Chemicals 3. fire/steam 4. radiation 5. electricity 2 BURNS Results in 10-20 thousand deaths annually
Burn Injuries & Its Management M JARI.MD 1 BURNS Wounds caused by exposure to: 1. excessive heat 2. Chemicals 3. fire/steam 4. radiation 5. electricity 2 BURNS Results in 10-20 thousand deaths annually
The Use of Dynamic Parameters in Perioperative Fluid Management
 The Use of Dynamic Parameters in Perioperative Fluid Management Gerard R. Manecke Jr., M.D. Chief, Cardiac Anesthesia UCSD Medical Center San Diego, CA, USA Thanks to Tom Higgins, M.D. 1 Goals of today
The Use of Dynamic Parameters in Perioperative Fluid Management Gerard R. Manecke Jr., M.D. Chief, Cardiac Anesthesia UCSD Medical Center San Diego, CA, USA Thanks to Tom Higgins, M.D. 1 Goals of today
Chapter 3 MAKING THE DECISION TO TRANSFUSE
 Chapter 3 MAKING THE DECISION TO TRANSFUSE PRACTICE POINTS Determine the best treatment for the patient which may include transfusion. Treat the cause of cytopenia (anaemia or thrombocytopenia) or plasma
Chapter 3 MAKING THE DECISION TO TRANSFUSE PRACTICE POINTS Determine the best treatment for the patient which may include transfusion. Treat the cause of cytopenia (anaemia or thrombocytopenia) or plasma