Inherited Cardiomyopathies Molecular genetics and Clinical genetic testing
|
|
|
- Noah Brice Fox
- 5 years ago
- Views:
Transcription
1 Inherited Cardiomyopathies Molecular genetics and Clinical genetic testing Dr Shagun Aggarwal Associate Professor, Department of Medical Genetics Nizam s Institute of Medical Sciences Adjunct Scientist, Centre for DNA Fingerprinting & Diagnostics Hyderabad
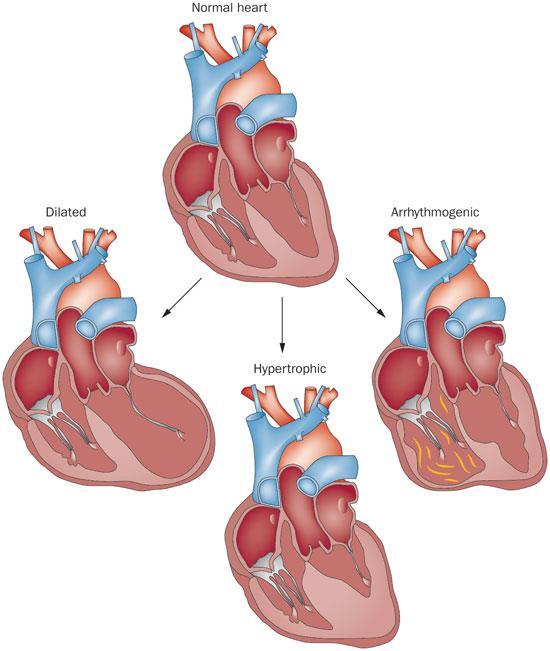
2 Cardiomyopathies The cardiomyopathies is a collection of myocardial disorders in which the heart muscle is structurally and functionally abnormal in the absence of coronary artery disease, hypertension, valvular or congenital heart disease sufficient to cause the observed myocardial abnormality.
3 Classification Morphofunctional phenotype (M) Organ(s) involvement (O) Genetic inheritance pattern (G) Etiological annotation (E) including genetic defect or underlying disease/substrate The functional status (S) of the disease using both the American College of Cardiology/American Heart Association stage and New York Heart Association functional class.


4 Rhythm disorders Cardiomyopathies Monogenic cardiac malformations Cardiac malformations Ischemic heart disease Heart failure Peripheral arterial disease

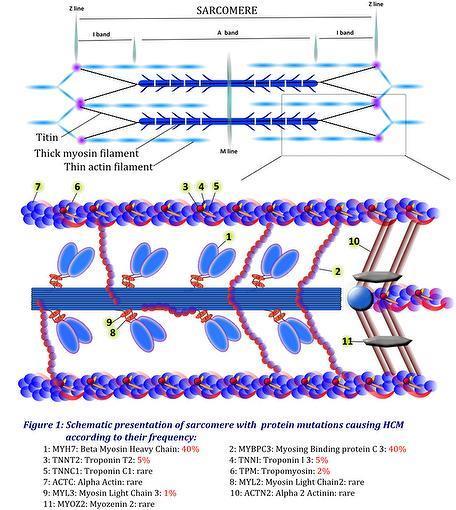
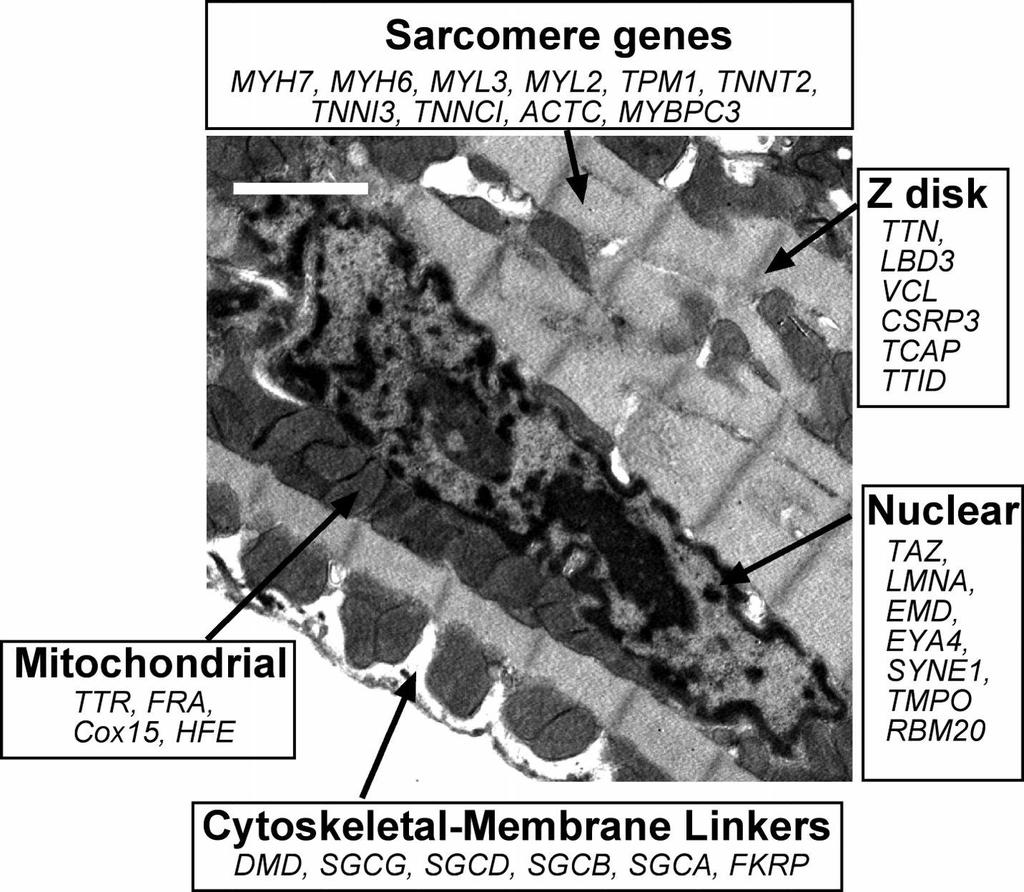
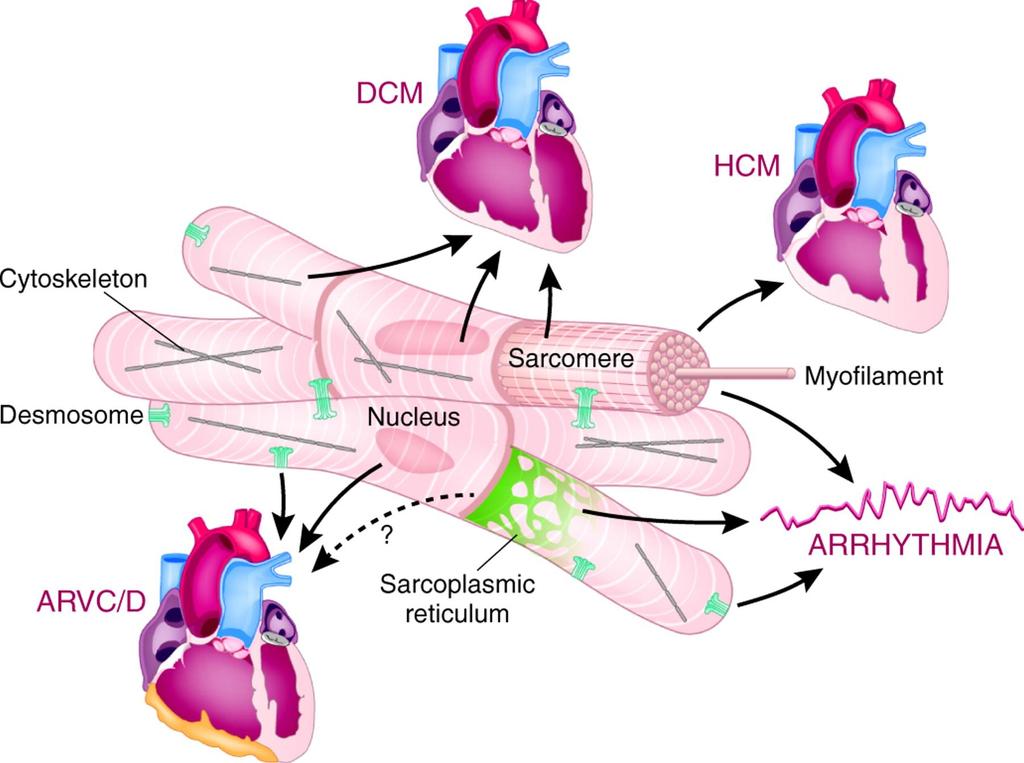
5 Ultrastructure of cardiac muscle
6
7

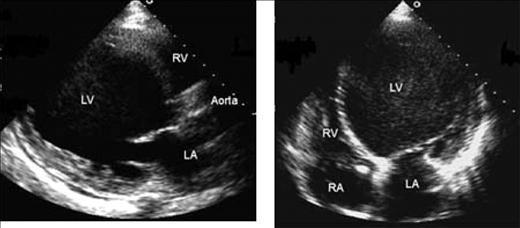
8 CASE 1- HOCM
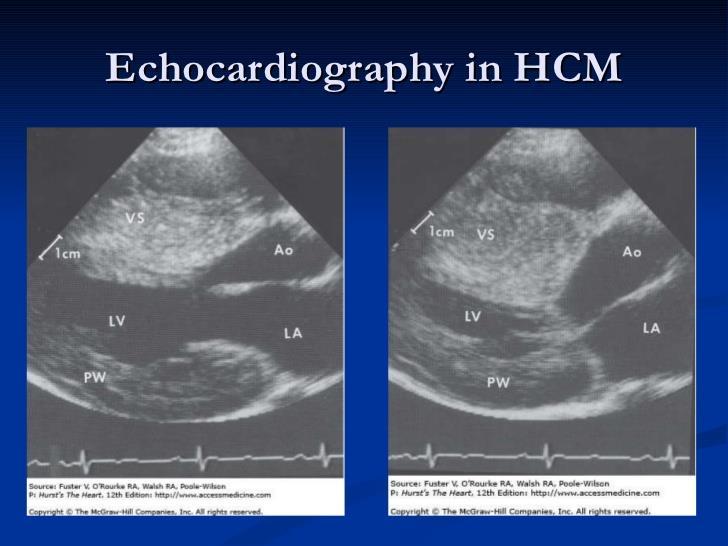
9
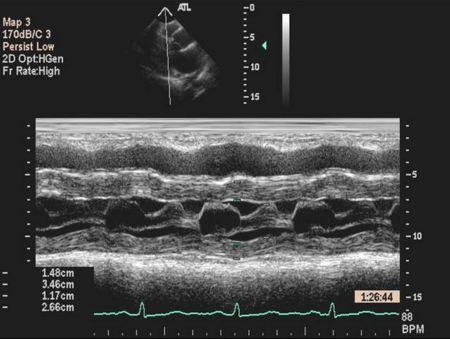
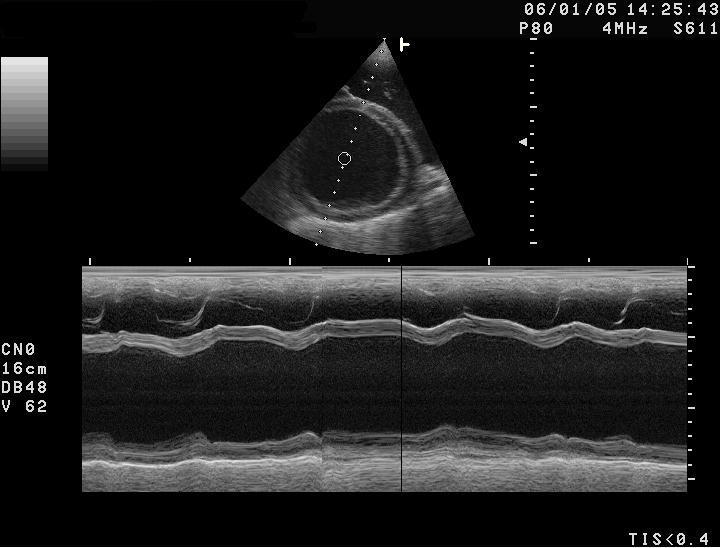
10 SAM

11 DAGGER SHAPED LVOT DOPLLER SPECTRUM

12 CASE 2 - APICAL HCM

13 CASE 3- MID CAVITORY HCM
14 HCM 1 in 500 Left ventricular hypertrophy in absence of systemic condition or other cardiac disease Onset : infancy to old age Usual: post adolescence Leading cause of sudden cardiac death in young Asymptomatic- range of symptoms 5-10% progress to heart failure
15 Common symptoms Shortness of breath (exacerbated by exertion) Chest pain Palpitations Orthostasis (low blood pressure when standing) Presyncope and syncope Diagnostic criteria Left ventricular hypertrophy (LVH) in non-dilated ventricle (in the absence of other known causes e.g. hypertension aortic stenosis athlete's heart) Most commonly asymmetric septal ( 15 mm; mm=borderline) Less frequently concentric and apical Characteristic echocardiographic findings Systolic anterior motion (SAM) of the mitral valve with associated left ventricular outflow tract obstruction and mitral regurgitation Midventricular obstruction as a result of systolic cavity obliteration Diastolic dysfunction including restrictive physiology Pathognomonic histopathology Myocyte disarray Myocyte hypertrophy Increased myocardial fibrosis Other findings suggestive of HCM Fourth heart sound Prominent left ventricular apical impulse/lift Brisk carotid upstroke Left ventricular outflow tract/intracavitary obstruction Abnormal ECG: Pattern consistent with LVH Pattern consistent with left atrial enlargement Prominent Q-waves in inferior and lateral leads Diffuse T-wave inversions
16 Genetics of HCM Strong genetic basis Autosomal dominant inheritance Incomplete penetrance- age dependent Variable expressivity
17 Pedigree showing autosomal dominant inheritance

18 50% recurrence risk in offspring
19 Genetics of HCM Strong genetic basis Autosomal dominant inheritance Incomplete penetrance- age dependent Variable expressivity Sarcomere genes most commonly involved 50-60% FHCM found to have mutations 20-30% of sporadic HCM
20
21 Gene % of established mutations Genes with established pathogenicity for HCM Location Name (HGNC) Phenotype OMIM Muscular component MYH q11.2 Myosin, heavy chain, cardiac muscle, Beta CMH1 (192600) Sarcomere, thick filament MYBPC p11.2 Myosin binding protein, cardiac CMH4 (115197) Sarcomere, intermediate filament TNNT2 5 1q32.1 Troponin T type 2 (cardiac) CMH2 (115195) Sarcomere, thin filament TNNI3 5 19q13.42 Troponin I, type 3 CMH3 (613690) Sarcomere, thin filament TPM1 2 15q22.2 Tropomyosin 1 (α) CMH 3 (115196) Sarcomere, thin filament MYL2? 12q24.11 Myosin, light chain 2, regulatory, cardiac, slow CMH 10 (608758) Sarcomere, thick filament MYL3 1 3p21.31 Myosin, light chain 3, alkali, ventricular, skeletal slow CMH 8 (608751) Sarcomere, thick filament ACTC1? 15q14 Actin, alpha, cardiac muscle 1 CMH 11 (612098) ACTN2? 1q43 Actinin, α Z-disc Sarcomere, thin filament TNNC1? 3p21.1 Troponin C type1 (slow) CMH 8 (613243) Sarcomere, thin filament MYOZ2? 4q26 Myozenin 2 CMH 16 (613838) Z-disc
22 Case 8 month old female Consanguineous parents Recurrent respiratory tract infections and labored breathing since 3 months age Predominant motor delay- partial neck holding, unable to sit with support Generalised hypotonia Hepatomegaly 2 cm

23 Serum CPK: 733 IU/l 2 D echo: Left ventricular hypertrophy and dilatation Global hypokinesia of LV
24 Diagnosis Pompe disease (Glycogen storage disorder type 2) Poor prognosis in absence of therapy ERT available Autosomal recessive disorder 25% recurrence risk


25 Noonan syndrome

26 RAS-MAPK pathway disorders 1 in %
27 Other syndromic hypertrophic cardiomyopathies Gene mutation Protein mutation Inheritance Gene Clinical features PRKAG2 Gamma subunit of AMP-dependant protein kinase 2 Autosomic recessive 7q36.1 Hypotonia; failure to thrive Hypoglycemia; Hepatomegaly; growth retardation GLA Alpha galactosidase X linked Xq22.1 Fabry disease Fatigue; acroparesthesia; proteinuria; renal failure, corneal opacity, anhidrosis; angiokeratoma; neuropathy LAMP2 Lysosome associated membrane protein 2 X linked Xq24 Danon disease Proximal myopathy; raised CPK; cognitive impairment, visual impairment; WPW


28 Fabry disease 3-10% males with HOCM have Fabry disease ERT available
29 AS A GENETICIST HOW DO YOU APPROACH A CASE OF HCM.
30 Approach to patient with HOCM History and examination Dysmorphic assessment and systemic evaluation Echocardiography and Ancillary testing Three generation family history with attention to sudden cardiac deaths esp. young age, heart failure, syncopal attacks Cardiac evaluation of family members- first degree relative
31
32
33
34 Relevance of genetic testing Identification of true positive and negative family members Prenatal diagnosis: 50% recurrence risk Optimise M/m using knowledge of genotypephenotype correlation 23 bp deletion in intron of MYBPC3 gene has increased risk of heart failure(or 7) TNNT2 mutations-less hypertrophy, more arrhythmia MYH7 mutations- LVH by 2 nd decade, increase risk of sudden death & heart failure Identification of systemic disease with specific Rx?Prophylactic pharmacotherapy in presymptomatic mutation +: Diltiazem, ACE/ARBs

35 CASE 5 - DILATED CARDIOMYOPATHY
36
37
38 DCM DCM is defined by LV dilatation and systolic dysfunction i.e. a reduction in myocardial force generation characterized by an ejection fraction of <50% 1 in % have family history Heart failure, thromboembolism and SCD
39 Genetically heterogeneous >50 genes known AD/AR/XL Incomplete penetrance Acquired etiologies also common Occurs as part of clinical spectrum of various genetic neuromuscular disorders
40

41 25 % Sarcomere 10-25% 5-8% Sequencing of 20 genes in DCM has a diagnostic yield of 17-30% only
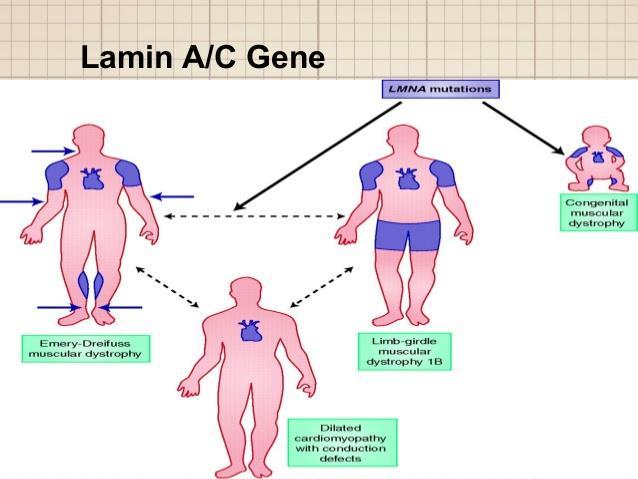
42 Common clinical conditions associated with DCM Duchenne & Becker s muscular dystrophyprobands as well as carrier mothers Limb girdle muscular dystrophy Emery-Dreifuss muscular dystrophy Mitochondrial myopathy Peripartum cardiomyopathy
43 Approach to a patient with DCM History (with special attention to heart failure symptoms, arrhythmias, presyncope and syncope) Three generation family history- special attention to X linked inheritance pattern Physical examination (with special attention to the cardiac and skeletal muscle systems) Electrocardiogram Echocardiogram CK-MM (at initial evaluation only)
44 Genetic testing Complicated by multiple genes No single gene contributes significantly except Titin Genotype-phenotype is important LMNA mutations: SCD frequency as high as 46% due to conduction system defects ICD should be considered SCN5A mutations also predispose to arrhythmia
45
46 Relevance of genetic testing Identification of true positive and negative family members Identification of asymptomatic female carriers in X linked inheritance Prenatal diagnosis Optimise M/m using knowledge of genotypephenotype correlation ICD in LMNA mutations Identification of systemic disease with M/m of comorbidities
47 Arrhythmogenic RVCM ARVC is defined by myocyte loss and fibrofatty infiltration of the myocardium and is associated with an increased susceptibility to arrhythmias and sudden death Involvement of LV also reported Male predominance Onset around 40 years T wave inversion in precordial leads 1 in Leading cause of SCD <35 years age
48 Early, concealed phase is characterized by propensity toward ventricular arrhythmia in the setting of preserved morphology, histology, and ventricular function Later stages: myocyte loss, inflammation, and fibroadiposis become evident Morphologically DCM Ventricular arrhythmia mc presentation Late stages: heart failure

49 Genetics of ARVCM Upto 60% have identifiable genetic mutations Majority involve components of the desmosome AD/AR forms

50 6-16% 11-43% 12-40% 2-7%
51 Approach Similar to HCM & DCM Signal Averaged ECG (SAECG) in ARVD only Holter monitoring Magnetic resonance imaging in ARVD Genetic testing may contribute to diagnosis in early stages
52 Compound heterozygosity and double heterozygosity common Significance of some previously reported mutations not known S358L mutation in TMEM43 in the Newfoundland founder population : fully penetrant, nonclassic form, high incidence of SCD and heart failure Cardiac ryanodine receptor (RyR2): distinct clinical entity, ARVC2, Characterized by juvenile SCD and effort-induced polymorphic ventricular tachycardia Definite Genotype phenotype information not available at present
53 No definite guidelines on mutation specific m/m Animal studies and anecdotal clinical reports suggest that prolonged and intense physical activity, particularly endurance training, may accelerate disease progression:? M/m of presymptomatic individuals
54 Left ventricular Non compaction Trabeculated/Spongy left ventricular wall May involve right ventricle Early onset disease Progressive poor cardiac outcome Ventricular hypertrophy Sudden Cardiac death Thromboembolism Asymptomatic % prevalence
55 CASE 6 - LV noncompaction
56
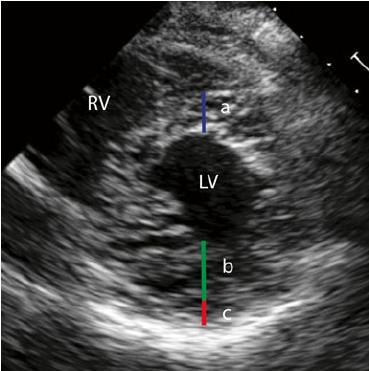
57

58 DEEP RECESSES NEAR APEX
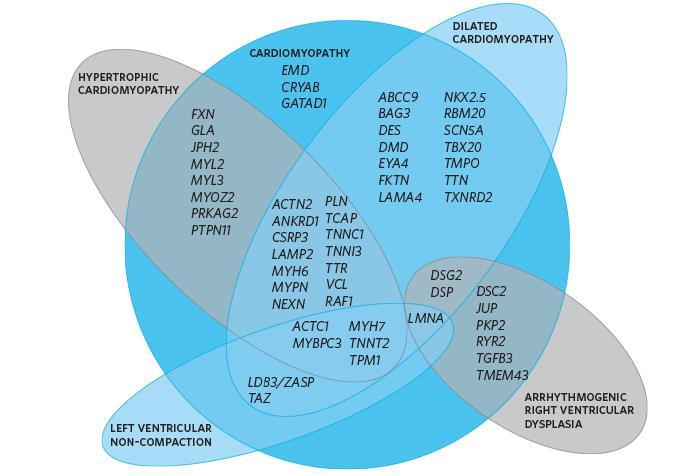
59 Genetics Mutation in upto 25%(17-40%) individuals Syndromic associations 1. Barth syndrome 2. Mitochondriopathies LDB3(5%), ACTC1, MYH7, MYBPC3, TNNT2, LMNA,DTNA mutations in isolated cases Overlap with HCM & DCM Relative contributions unknown No definite guidelines for M/m based on mutation
60 Restrictive cardiomyopathy RCM is characterized by increased stiffness of the ventricular chambers Progresses to heart failure and death in few years Upto 35% have genetic mutation TNNI3 (18%), MYH7(14%), and MYBPC3 (2%), TNNT2,ACTC1 Syndromic associations: Gaucher disease, Fabry disease, Glycogen storage disease, amyloidosis
61
62
63 HFSA Guideline Approach to Medical Evidence for Genetic Evaluation of Cardiomyopathy 1. A careful family history for 3 generations is recommended for all patients with cardiomyopathy Is it familial? Identify individuals at risk Inheritance pattern May suggest the age of onset, penetrance, lethality, response to treatment
64 2. Clinical screening for cardiomyopathy in asymptomatic first-degree relatives is recommended Asymptomatic at-risk relatives who are known to carry the disease-causing mutation(s) Asymptomatic at-risk first-degree relatives when genetic testing has not been performed or has not identified a disease-causing mutation
65 History (with special attention to heart failure symptoms, arrhythmias, presyncope and syncope) Physical examination (with special attention to the cardiac and skeletal muscle systems) Electrocardiogram Echocardiogram CK-MM (at initial evaluation only) Signal Averaged ECG (SAECG) in ARVD only Holter monitoring in HCM, ARVD Exercise treadmill testing in HCM Magnetic resonance imaging in ARVD
66 At-risk first-degree relatives with any abnormal clinical screening tests (regardless of genotype) should be considered for repeat clinical screening at one year
67 Rationale Early detection may delay disease presentation and progression, or averting lifethreatening events, such as sudden cardiac death Variable age of onset and incomplete penetrance, adult onset: basis for screening age & interval At risk family members: caution about presyncope, syncope, other S/S
68 3. Evaluation, genetic counseling, and genetic testing of cardiomyopathy patients are complex processes. Referral to centers expert in genetic evaluation and family-based management should be considered. Challenges Genetic heterogeneity Mutation heterogeneity Incomplete penetrance Variable expressivity Incomplete knowledge regarding genes involved & genotype-phenotype correlations
69 Challenges and limitations Deceased proband Incomplete information of clinical phenotypes Unavailable family members No definite therapeutic implications except LMNA mutations No definite prognostic implications No diagnostic utility in the affected person
70 4. Genetic testing should be considered for the most clearly affected person in a family DNA from tissue of deceased person if available Testing for unaffected at risk person likely to be negative Choice of test: 1. Specific genetic panel 2. Targeted testing depending on phenotype 3. NGS based multigene panel
71 HRS/EHRA consensus statement 2011 HCM: Recommended testing for MHY7,MYBPC3,TNNI3,TNNT2,TPM1 for all patients DCM-CCD: Recommended LMNA, SCN5A teating For all other cardiomyopathies: Can be useful but not recommended in index case Family targeted mutation testing recommended for all once index case mutation known Main limitation: Genetic heterogeneity, poor yield


72 Next Generation sequencing High throughput sequencing techniques Generate millions of base pair Clinical exome panel: sequences all OMIM genes with known Mendelian phenotypes Challenge: VUS
73 5. Genetic and family counseling is recommended for all patients and families with cardiomyopathy Pretest Postest Preconceptional & Prenatal A negative genetic test does not exclude genetic etiology/inherited cardiomyopathies
74 Approach to genetic testing for Cardiomyopathies
75 Advantages of genetic testing Presymptomatic testing of relatives Prenatal diagnosis in at risk pregnancy Rarely diagnosis in some patients with nondefinitive findings Identifies genetic vs acquired eg. in DCM Identification of underlying systemic condition or syndrome : surveillance of other findings Management in storage disorders: ERT
76 Take home messages Large majority of cardiomyopathies are of genetic etiology and show autosomal dominant inheritance Clinical presentations vary and SCD may be the first presentation Screening of first degree relatives is important Genetic testing helps in presymptomatic diagnosis and targeting surveillance Testing is difficult in view of genetic heterogeneity and missing genotype-phenotype correlations Next generation sequencing enables overcoming some of these drawbacks
77 Thank you
Hypertrophic Cardiomyopathy
 Hypertrophic Cardiomyopathy From Genetics to ECHO Alexandra A Frogoudaki Second Cardiology Department ATTIKON University Hospital Athens University Athens, Greece EUROECHO 2010, Copenhagen, 11/12/2010
Hypertrophic Cardiomyopathy From Genetics to ECHO Alexandra A Frogoudaki Second Cardiology Department ATTIKON University Hospital Athens University Athens, Greece EUROECHO 2010, Copenhagen, 11/12/2010
Genetic Cardiomyopathies
 2017 HFCT Annual Scientific Meeting The Heart Failure Crosstalk Genetic Cardiomyopathies Teerapat Yingchoncharoen M.D. Ramathibodi Hospital Cardiomyopathy Group of diseases of the myocardium associated
2017 HFCT Annual Scientific Meeting The Heart Failure Crosstalk Genetic Cardiomyopathies Teerapat Yingchoncharoen M.D. Ramathibodi Hospital Cardiomyopathy Group of diseases of the myocardium associated
Clinical Genetics in Cardiomyopathies
 Clinical Genetics in Cardiomyopathies Γεώργιος Κ Ευθυμιάδης Αναπληρωτής Καθηγητής Καρδιολογίας ΑΠΘ No conflict of interest Genetic terms Proband: The first individual diagnosed in a family Mutation: A
Clinical Genetics in Cardiomyopathies Γεώργιος Κ Ευθυμιάδης Αναπληρωτής Καθηγητής Καρδιολογίας ΑΠΘ No conflict of interest Genetic terms Proband: The first individual diagnosed in a family Mutation: A
Preventing Sudden Death in Young Athletes. Outline. Scope of the Problem. Causes of SCD in Young Athletes. Sudden death in the young athlete
 Preventing Sudden Death in Young Athletes Ronn E. Tanel, MD Director, Pediatric Arrhythmia Service UCSF Children s Hospital Associate Professor of Pediatrics UCSF School of Medicine Outline Sudden death
Preventing Sudden Death in Young Athletes Ronn E. Tanel, MD Director, Pediatric Arrhythmia Service UCSF Children s Hospital Associate Professor of Pediatrics UCSF School of Medicine Outline Sudden death
Corporate Medical Policy
 Corporate Medical Policy Genetic Testing for Predisposition to Inherited Hypertrophic File Name: Origination: Last CAP Review: Next CAP Review: Last Review: genetic_testing_for_predisposition_to_inherited_hypertrophic_cardiomyopathy
Corporate Medical Policy Genetic Testing for Predisposition to Inherited Hypertrophic File Name: Origination: Last CAP Review: Next CAP Review: Last Review: genetic_testing_for_predisposition_to_inherited_hypertrophic_cardiomyopathy
Familial DilatedCardiomyopathy Georgios K Efthimiadis, MD
 Familial DilatedCardiomyopathy Georgios K Efthimiadis, MD Dilated Cardiomyopathy Dilated LV/RV, reduced EF, in the absence of CAD valvulopathy pericardial disease Prevalence:40/100.000 persons Natural
Familial DilatedCardiomyopathy Georgios K Efthimiadis, MD Dilated Cardiomyopathy Dilated LV/RV, reduced EF, in the absence of CAD valvulopathy pericardial disease Prevalence:40/100.000 persons Natural
Hypertrophic Cardiomyopathy: beyond gradient and wall thickness
 Hypertrophic Cardiomyopathy: beyond gradient and wall thickness Michael H. Picard, M.D. Massachusetts General Hospital Harvard Medical School no disclosures special thanks to A. Baggish 1 Hypertrophic
Hypertrophic Cardiomyopathy: beyond gradient and wall thickness Michael H. Picard, M.D. Massachusetts General Hospital Harvard Medical School no disclosures special thanks to A. Baggish 1 Hypertrophic
Managing Hypertrophic Cardiomyopathy with Imaging. Gisela C. Mueller University of Michigan Department of Radiology
 Managing Hypertrophic Cardiomyopathy with Imaging Gisela C. Mueller University of Michigan Department of Radiology Disclosures Gadolinium contrast material for cardiac MRI Acronyms Afib CAD Atrial fibrillation
Managing Hypertrophic Cardiomyopathy with Imaging Gisela C. Mueller University of Michigan Department of Radiology Disclosures Gadolinium contrast material for cardiac MRI Acronyms Afib CAD Atrial fibrillation
2011 HCM Guideline Data Supplements
 Data Supplement 1. Genetics Table Study Name/Author (Citation) Aim of Study Quality of life and psychological distress quality of life and in mutation psychological carriers: a crosssectional distress
Data Supplement 1. Genetics Table Study Name/Author (Citation) Aim of Study Quality of life and psychological distress quality of life and in mutation psychological carriers: a crosssectional distress
Echocardiographic Evaluation of the Cardiomyopathies. Stephanie Coulter, MD, FACC, FASE April, 2016
 Echocardiographic Evaluation of the Cardiomyopathies Stephanie Coulter, MD, FACC, FASE April, 2016 Cardiomyopathies (CMP) primary disease intrinsic to cardiac muscle Dilated CMP Hypertrophic CMP Infiltrative
Echocardiographic Evaluation of the Cardiomyopathies Stephanie Coulter, MD, FACC, FASE April, 2016 Cardiomyopathies (CMP) primary disease intrinsic to cardiac muscle Dilated CMP Hypertrophic CMP Infiltrative
Cardiac Considerations and Care in Children with Neuromuscular Disorders
 Cardiac Considerations and Care in Children with Neuromuscular Disorders - importance of early and ongoing treatment, management and available able medications. Dr Bo Remenyi Department of Cardiology The
Cardiac Considerations and Care in Children with Neuromuscular Disorders - importance of early and ongoing treatment, management and available able medications. Dr Bo Remenyi Department of Cardiology The
Cardiomyopathy in Fabry s disease
 Cardiomyopathy in Fabry s disease Herzinsuffizienzlunch Basel, 11.09.2018 Christiane Gruner Kardiologie, UniversitätsSpital Zürich Content Background / epidemiology Differential diagnosis Clinical presentations
Cardiomyopathy in Fabry s disease Herzinsuffizienzlunch Basel, 11.09.2018 Christiane Gruner Kardiologie, UniversitätsSpital Zürich Content Background / epidemiology Differential diagnosis Clinical presentations
Hypertrophic Cardiomyopathy
 Hypertrophic Cardiomyopathy A Presentation for the MUD meeting January, 2018 Reviewed by Bill Rooney MD VP/Medical Director 1 https://commons.wikimedia.org/wiki/file:blausen_0166_cardiomyopathy_hypertrophic.p
Hypertrophic Cardiomyopathy A Presentation for the MUD meeting January, 2018 Reviewed by Bill Rooney MD VP/Medical Director 1 https://commons.wikimedia.org/wiki/file:blausen_0166_cardiomyopathy_hypertrophic.p
How NOT to miss Hypertrophic Cardiomyopathy? Adaya Weissler-Snir, MD University Health Network, University of Toronto
 How NOT to miss Hypertrophic Cardiomyopathy? Adaya Weissler-Snir, MD University Health Network, University of Toronto Introduction Hypertrophic cardiomyopathy is the most common genetic cardiomyopathy,
How NOT to miss Hypertrophic Cardiomyopathy? Adaya Weissler-Snir, MD University Health Network, University of Toronto Introduction Hypertrophic cardiomyopathy is the most common genetic cardiomyopathy,
Inherited Arrhythmia Syndromes
 Inherited Arrhythmia Syndromes When to perform Genetic testing? Arthur AM Wilde February 4, 2017 Which pts should undergo genetic testing? SCD victims with a likely diagnosis Pts diagnosed with an inherited
Inherited Arrhythmia Syndromes When to perform Genetic testing? Arthur AM Wilde February 4, 2017 Which pts should undergo genetic testing? SCD victims with a likely diagnosis Pts diagnosed with an inherited
Definition and classification of the cardiomyopathies. Georgios K Efthimiadis Ass Prof of Cardiology
 Definition and classification of the cardiomyopathies Georgios K Efthimiadis Ass Prof of Cardiology Historical Context WHO: 1980 classification "heart muscle diseases of unknown cause" WHO 1995 classification
Definition and classification of the cardiomyopathies Georgios K Efthimiadis Ass Prof of Cardiology Historical Context WHO: 1980 classification "heart muscle diseases of unknown cause" WHO 1995 classification
Cardiac Conditions in Sport & Exercise. Cardiac Conditions in Sport. USA - Sudden Cardiac Death (SCD) Dr Anita Green. Sudden Cardiac Death
 Dr Anita Green. Sudden Cardiac Death") Cardiac Conditions in Sport & Exercise Dr Anita Green Cardiac Conditions in Sport Sudden Cardiac Death USA - Sudden Cardiac Death (SCD)
Cardiac Conditions in Sport & Exercise Dr Anita Green Cardiac Conditions in Sport Sudden Cardiac Death USA - Sudden Cardiac Death (SCD)
Cardiomyopathy. Jeff Grubbe MD FACP, Chief Medical Director, Allstate Life & Retirement
 Cardiomyopathy Jeff Grubbe MD FACP, Chief Medical Director, Allstate Life & Retirement Nebraska Home Office Life Underwriters Association March 20, 2018 1 Cardiomyopathy A myocardial disorder in which
Cardiomyopathy Jeff Grubbe MD FACP, Chief Medical Director, Allstate Life & Retirement Nebraska Home Office Life Underwriters Association March 20, 2018 1 Cardiomyopathy A myocardial disorder in which
Treatment of Hypertrophic Cardiomyopathy in Bruce B. Reid, MD
 Treatment of Hypertrophic Cardiomyopathy in 2017 Bruce B. Reid, MD Disclosures I have no conflicts of interest to disclose I will not be discussing any off label medications and/or devices Objectives 1)
Treatment of Hypertrophic Cardiomyopathy in 2017 Bruce B. Reid, MD Disclosures I have no conflicts of interest to disclose I will not be discussing any off label medications and/or devices Objectives 1)
Hereditary Cardiovascular Conditions. genetic testing for undiagnosed diseases
 Hereditary Cardiovascular Conditions genetic testing for undiagnosed diseases What is Hypertrophic Cardiomyopathy (HCM)? normal heart heart with hcm Extra or thick heart muscle Typically in the left ventricle
Hereditary Cardiovascular Conditions genetic testing for undiagnosed diseases What is Hypertrophic Cardiomyopathy (HCM)? normal heart heart with hcm Extra or thick heart muscle Typically in the left ventricle
What Clinicians Need to Know About Genetic Testing for Patients and Families with HCM
 What Clinicians Need to Know About Genetic Testing for Patients and Families with HCM Sharon Cresci, MD Assistant Professor of Medicine Assistant Professor of Genetics Cardiovascular Division Washington
What Clinicians Need to Know About Genetic Testing for Patients and Families with HCM Sharon Cresci, MD Assistant Professor of Medicine Assistant Professor of Genetics Cardiovascular Division Washington
ΜΥΟΚΑΡΔΙΟΠΑΘΕΙΕΣ. Ανεξήγητη βραδυκαρδία µε ή χωρίς διαταραχές κολποκοιλιακής αγωγής: τι µπορεί να κρύβει? ΕΦΗ Ι. ΠΡΑΠΠΑ Καρδιολόγος
 ΜΥΟΚΑΡΔΙΟΠΑΘΕΙΕΣ Ανεξήγητη βραδυκαρδία µε ή χωρίς διαταραχές κολποκοιλιακής αγωγής: τι µπορεί να κρύβει? ΕΦΗ Ι. ΠΡΑΠΠΑ Καρδιολόγος Β Καρδιολογική Κλινική, ΠΓΝΑ «Ο ΕΥΑΓΓΕΛΙΣΜΟΣ» CONFLICT of INTEREST : none
ΜΥΟΚΑΡΔΙΟΠΑΘΕΙΕΣ Ανεξήγητη βραδυκαρδία µε ή χωρίς διαταραχές κολποκοιλιακής αγωγής: τι µπορεί να κρύβει? ΕΦΗ Ι. ΠΡΑΠΠΑ Καρδιολόγος Β Καρδιολογική Κλινική, ΠΓΝΑ «Ο ΕΥΑΓΓΕΛΙΣΜΟΣ» CONFLICT of INTEREST : none
HYPERTROPHY: Behind the curtain. V. Yotova St. Radboud Medical University Center, Nijmegen
 HYPERTROPHY: Behind the curtain V. Yotova St. Radboud Medical University Center, Nijmegen Disclosure of interest: none Relative wall thickness (cm) M 0.22 0.42 0.43 0.47 0.48 0.52 0.53 F 0.24 0.42 0.43
HYPERTROPHY: Behind the curtain V. Yotova St. Radboud Medical University Center, Nijmegen Disclosure of interest: none Relative wall thickness (cm) M 0.22 0.42 0.43 0.47 0.48 0.52 0.53 F 0.24 0.42 0.43
CARDIOMYOPATHY IN CT. Hans- Christoph Becker Professor of Radiology
 CARDIOMYOPATHY IN CT Hans- Christoph Becker Professor of Radiology 1 Cardiomyopathy Heart muscle disease Deterioration of the heart function, heart failure Dyspnea, peripheral edema Risk of arrhythmia,
CARDIOMYOPATHY IN CT Hans- Christoph Becker Professor of Radiology 1 Cardiomyopathy Heart muscle disease Deterioration of the heart function, heart failure Dyspnea, peripheral edema Risk of arrhythmia,
Left ventricular non-compaction: the New Cardiomyopathy on the Block
 Left ventricular non-compaction: the New Cardiomyopathy on the Block Aamir Jeewa MB BCh, FAAP, FRCPC Section Head, Cardiomyopathy & Heart Function Program The Hospital for Sick Children Assistant Professor
Left ventricular non-compaction: the New Cardiomyopathy on the Block Aamir Jeewa MB BCh, FAAP, FRCPC Section Head, Cardiomyopathy & Heart Function Program The Hospital for Sick Children Assistant Professor
What s new in Hypertrophic Cardiomyopathy?
 What s new in Hypertrophic Cardiomyopathy? Dr Andris Ellims HCM Clinic @ The Alfred Hypertrophic Cardiomyopathy = otherwise unexplained LV hypertrophy* 1 in 500 prevalence most common inherited cardiovascular
What s new in Hypertrophic Cardiomyopathy? Dr Andris Ellims HCM Clinic @ The Alfred Hypertrophic Cardiomyopathy = otherwise unexplained LV hypertrophy* 1 in 500 prevalence most common inherited cardiovascular
Proceedings of the 34th World Small Animal Veterinary Congress WSAVA 2009
 www.ivis.org Proceedings of the 34th World Small Animal Veterinary Congress WSAVA 2009 São Paulo, Brazil - 2009 Next WSAVA Congress : Reprinted in IVIS with the permission of the Congress Organizers MANAGEMENT
www.ivis.org Proceedings of the 34th World Small Animal Veterinary Congress WSAVA 2009 São Paulo, Brazil - 2009 Next WSAVA Congress : Reprinted in IVIS with the permission of the Congress Organizers MANAGEMENT
Genetic testing in Cardiomyopathies
 Genetic testing in Cardiomyopathies Silvia Giuliana Priori Cardiovascular Genetics, Langone Medical Center, New York University School of Medicine, New York, USA and Molecular Cardiology, IRCCS Fondazione
Genetic testing in Cardiomyopathies Silvia Giuliana Priori Cardiovascular Genetics, Langone Medical Center, New York University School of Medicine, New York, USA and Molecular Cardiology, IRCCS Fondazione
Cardiomyopathy: The Good, the Bad.and the Insurable?
 Cardiomyopathy: The Good, the Bad.and the Insurable? WAHLU Spring Seminar 2014 Joy Geiger, RN, BSN, ALMI Medical Consultant The Northwestern Mutual Life Insurance Company Milwaukee, WI Objectives Overview
Cardiomyopathy: The Good, the Bad.and the Insurable? WAHLU Spring Seminar 2014 Joy Geiger, RN, BSN, ALMI Medical Consultant The Northwestern Mutual Life Insurance Company Milwaukee, WI Objectives Overview
HYPERTROPHIC CARDIOMYOPATHY RISK STRATIFICATION WHAT IS NEW?
 HYPERTROPHIC CARDIOMYOPATHY RISK STRATIFICATION WHAT IS NEW? Division of Inherited Cardiac Diseases Heart Center for the Young and Athletes A Dpt of Cardiology University of Athens LANCET 2013 ESC HCM
HYPERTROPHIC CARDIOMYOPATHY RISK STRATIFICATION WHAT IS NEW? Division of Inherited Cardiac Diseases Heart Center for the Young and Athletes A Dpt of Cardiology University of Athens LANCET 2013 ESC HCM
HEART CONDITIONS IN SPORT
 HEART CONDITIONS IN SPORT Dr. Anita Green CHD Risk Factors Smoking Hyperlipidaemia Hypertension Obesity Physical Inactivity Diabetes Risks are cumulative (multiplicative) Lifestyles predispose to RF One
HEART CONDITIONS IN SPORT Dr. Anita Green CHD Risk Factors Smoking Hyperlipidaemia Hypertension Obesity Physical Inactivity Diabetes Risks are cumulative (multiplicative) Lifestyles predispose to RF One
Utility of Echocardiography
 Hypertrophic Cardiomyopathy and Beyond- Echo Hawaii 2018 Lawrence Rudski MD FRCPC FACC FASE Professor of Medicine Director, Division of Cardiology and Azrieli Heart Center Jewish General Hospital, McGill
Hypertrophic Cardiomyopathy and Beyond- Echo Hawaii 2018 Lawrence Rudski MD FRCPC FACC FASE Professor of Medicine Director, Division of Cardiology and Azrieli Heart Center Jewish General Hospital, McGill
HYPERTROPHIC CARDIOMYOPATHY
 HYPERTROPHIC CARDIOMYOPATHY Most often diagnosed during infancy or adolescence, hypertrophic cardiomyopathy (HCM) is the second most common form of heart muscle disease, is usually genetically transmitted,
HYPERTROPHIC CARDIOMYOPATHY Most often diagnosed during infancy or adolescence, hypertrophic cardiomyopathy (HCM) is the second most common form of heart muscle disease, is usually genetically transmitted,
Cardiomyopathy. ACOI IM Board Review 2018 Martin C. Burke DO, FACOI
 Cardiomyopathy ACOI IM Board Review 2018 Martin C. Burke DO, FACOI No Disclosures Cardiomyopathies Definition: diseases of heart muscle 1980 WHO: unknown causes Not clinically relevant 1995 WHO: diseases
Cardiomyopathy ACOI IM Board Review 2018 Martin C. Burke DO, FACOI No Disclosures Cardiomyopathies Definition: diseases of heart muscle 1980 WHO: unknown causes Not clinically relevant 1995 WHO: diseases
Slide 1. Slide 2. Slide 3. Sudden Cardiac Death In Athletes. Epidemiology. Epidemiology. Shaun McMurtry, MD Primary Care Sports Medicine
 Slide 1 Sudden Cardiac Death In Athletes Shaun McMurtry, MD Primary Care Sports Medicine Slide 2 Epidemiology College and Professional Athletes 500,000 participants each year Competitive Athletics Estimated
Slide 1 Sudden Cardiac Death In Athletes Shaun McMurtry, MD Primary Care Sports Medicine Slide 2 Epidemiology College and Professional Athletes 500,000 participants each year Competitive Athletics Estimated
Sudden cardiac death: Primary and secondary prevention
 Sudden cardiac death: Primary and secondary prevention By Kai Chi Chan Penultimate Year Medical Student St George s University of London at UNic Sheba Medical Centre Definition Sudden cardiac arrest (SCA)
Sudden cardiac death: Primary and secondary prevention By Kai Chi Chan Penultimate Year Medical Student St George s University of London at UNic Sheba Medical Centre Definition Sudden cardiac arrest (SCA)
4/11/2017. Cardiomyopathy. John Steuter, MD Bryan Heart. Disclosures. No Conflicts. Cardiomyopathy. WHO Classification
 Cardiomyopathy John Steuter, MD Bryan Heart Disclosures No Conflicts Cardiomyopathy WHO Classification Anatomy & physiology of the LV 1. Dilated Enlarged Systolic dysfunction 2. Hypertrophic Thickened
Cardiomyopathy John Steuter, MD Bryan Heart Disclosures No Conflicts Cardiomyopathy WHO Classification Anatomy & physiology of the LV 1. Dilated Enlarged Systolic dysfunction 2. Hypertrophic Thickened
The Management of HOCM: What are the Surgical Options
 The Management of HOCM: What are the Surgical Options Konstadinos A Plestis, MD System Chief of Cardiac Thoracic and Vascular Surgery Main Line Health Care System Professor Sidney Kimmel Medical College
The Management of HOCM: What are the Surgical Options Konstadinos A Plestis, MD System Chief of Cardiac Thoracic and Vascular Surgery Main Line Health Care System Professor Sidney Kimmel Medical College
9/23/2011. Cardiac MRI Evaluation of Cardiomyopathy and Myocarditis. Primary Hypertrophic Cardiomyopathy. Cardiomyopathy.
 Cardiomyopathy Cardiac MRI Evaluation of Cardiomyopathy and Myocarditis Laureen Sena Children s Hospital Boston, MA NASCI 2011 Baltimore, Maryland Primary Hypertrophic ARVD Dilated Restrictive Unclassified
Cardiomyopathy Cardiac MRI Evaluation of Cardiomyopathy and Myocarditis Laureen Sena Children s Hospital Boston, MA NASCI 2011 Baltimore, Maryland Primary Hypertrophic ARVD Dilated Restrictive Unclassified
Anaesthesia for non-cardiac surgery in patients left ventricular outflow tract obstruction (LVOTO)
") Anaesthesia for non-cardiac surgery in patients left ventricular outflow tract obstruction (LVOTO) Dr. Siân Jaggar Consultant Anaesthetist Royal Brompton Hospital London UK Congenital Cardiac Services
Anaesthesia for non-cardiac surgery in patients left ventricular outflow tract obstruction (LVOTO) Dr. Siân Jaggar Consultant Anaesthetist Royal Brompton Hospital London UK Congenital Cardiac Services
Etiology, Classification & Management. Sheba Medical Center Cardiology Department Matthew Wright St. George s University of London
 Etiology, Classification & Management Sheba Medical Center Cardiology Department Matthew Wright St. George s University of London Introduction World Health Organization (1995): Diseases of myocardium (heart
Etiology, Classification & Management Sheba Medical Center Cardiology Department Matthew Wright St. George s University of London Introduction World Health Organization (1995): Diseases of myocardium (heart
Cardiac Issues in the Adolescent Athlete. Sean Levchuck, M.D. St. Francis Hospital- The Heart Center
 Cardiac Issues in the Adolescent Athlete Sean Levchuck, M.D. St. Francis Hospital- The Heart Center Sudden Cardiac Death Incidence is.6-6.2 % per 100,000 children in the US 20-25 % of the deaths occur
Cardiac Issues in the Adolescent Athlete Sean Levchuck, M.D. St. Francis Hospital- The Heart Center Sudden Cardiac Death Incidence is.6-6.2 % per 100,000 children in the US 20-25 % of the deaths occur
LVH GREY ZONE OF HYPERTROPHIED VENTRICLES
 LVH GREY ZONE OF HYPERTROPHIED VENTRICLES Unit of Inherited and Rare Cardiac Diseases Heart Center for the Young and Athletes Onassis Cardiac Surgery Centre Common phenotype different causes By Jacopo
LVH GREY ZONE OF HYPERTROPHIED VENTRICLES Unit of Inherited and Rare Cardiac Diseases Heart Center for the Young and Athletes Onassis Cardiac Surgery Centre Common phenotype different causes By Jacopo
YES NO UNKNOWN. Stage I: Rule-Out Dashboard Secondary Findings in Adults ACTIONABILITY PENETRANCE SIGNIFICANCE/BURDEN OF DISEASE NEXT STEPS
 Stage I: Rule-Out Dashboard HGNC ID: 11949, 6636, 2928 OMIM ID: 191045, 150330, 302045 ACTIONABILITY PENETRANCE 1. Is there a qualifying resource, such as a practice guideline or systematic review, for
Stage I: Rule-Out Dashboard HGNC ID: 11949, 6636, 2928 OMIM ID: 191045, 150330, 302045 ACTIONABILITY PENETRANCE 1. Is there a qualifying resource, such as a practice guideline or systematic review, for
Genotype Positive/ Phenotype Negative: Is It a Disease?
 Genotype Positive/ Phenotype Negative: Is It a Disease? Michelle Michels MD, PhD Center of Inherited Cardiovascular Diseases Erasmus MC, Rotterdam, the Netherlands No disclosures What is phenotype negative
Genotype Positive/ Phenotype Negative: Is It a Disease? Michelle Michels MD, PhD Center of Inherited Cardiovascular Diseases Erasmus MC, Rotterdam, the Netherlands No disclosures What is phenotype negative
Index of subjects. effect on ventricular tachycardia 30 treatment with 101, 116 boosterpump 80 Brockenbrough phenomenon 55, 125
 145 Index of subjects A accessory pathways 3 amiodarone 4, 5, 6, 23, 30, 97, 102 angina pectoris 4, 24, 1l0, 137, 139, 140 angulation, of cavity 73, 74 aorta aortic flow velocity 2 aortic insufficiency
145 Index of subjects A accessory pathways 3 amiodarone 4, 5, 6, 23, 30, 97, 102 angina pectoris 4, 24, 1l0, 137, 139, 140 angulation, of cavity 73, 74 aorta aortic flow velocity 2 aortic insufficiency
SEMINAIRES IRIS. Sudden cardiac death in the adult. Gian Battista Chierchia. Heart Rhythm Management Center, UZ Brussel. 20% 25% Cancers !
 Sudden cardiac death in the adult Gian Battista Chierchia. Heart Rhythm Management Center, UZ Brussel.! " # $ % Cancers National Vital Statistics Report, Vol 49 (11), Oct. 12, 2001. 20% 25% State-specific
Sudden cardiac death in the adult Gian Battista Chierchia. Heart Rhythm Management Center, UZ Brussel.! " # $ % Cancers National Vital Statistics Report, Vol 49 (11), Oct. 12, 2001. 20% 25% State-specific
INTRODUCTION. left ventricular non-compaction is a sporadic or familial cardiomyopathy characterized by
 A Rare Case of Arrhythmogenic Right Ventricular Cardiomyopathy Co-existing with Isolated Left Ventricular Non-compaction NS Yelgeç, AT Alper, Aİ Tekkeşin, C Türkkan INTRODUCTION Arrhythmogenic right ventricular
A Rare Case of Arrhythmogenic Right Ventricular Cardiomyopathy Co-existing with Isolated Left Ventricular Non-compaction NS Yelgeç, AT Alper, Aİ Tekkeşin, C Türkkan INTRODUCTION Arrhythmogenic right ventricular
Hypertrophic Cardiomyopathy
 019-CardioCase:019-CardioCase 4/16/07 1:39 PM Page 19 Hypertrophic Cardiomyopathy Abdullah Alshehri, MD; and Andrew Ignaszewski, MD, FRCPC CardioCase presentation Presley s check-up Presley, 37, discovered
019-CardioCase:019-CardioCase 4/16/07 1:39 PM Page 19 Hypertrophic Cardiomyopathy Abdullah Alshehri, MD; and Andrew Ignaszewski, MD, FRCPC CardioCase presentation Presley s check-up Presley, 37, discovered
Clinical Utilization and Function of Tissue Doppler Imaging in Detecting Congenital Cardiomyopathies
 618221JDMXXX10.1177/8756479315618221Journal of Diagnostic Medical SonographyAlexander research-article2015 Literature Review Clinical Utilization and Function of Tissue Doppler Imaging in Detecting Congenital
618221JDMXXX10.1177/8756479315618221Journal of Diagnostic Medical SonographyAlexander research-article2015 Literature Review Clinical Utilization and Function of Tissue Doppler Imaging in Detecting Congenital
ESC Guidelines on Hypertrophic Cardiomyopathy
 2014 version ES Guidelines on Hypertrophic ardiomyopathy Pr Michel KOMAJDA Dept of ardiology HU PTE SALPETRERE University Pierre et Marie urie PARS FRANE European Heart Journal (2014):doi:10.1093/eurheartj/ehu284
2014 version ES Guidelines on Hypertrophic ardiomyopathy Pr Michel KOMAJDA Dept of ardiology HU PTE SALPETRERE University Pierre et Marie urie PARS FRANE European Heart Journal (2014):doi:10.1093/eurheartj/ehu284
Εμφύτευση απινιδωτών για πρωτογενή πρόληψη σε ασθενείς που δεν περιλαμβάνονται στις κλινικές μελέτες
 Εμφύτευση απινιδωτών για πρωτογενή πρόληψη σε ασθενείς που δεν περιλαμβάνονται στις κλινικές μελέτες Δημήτριος M. Κωνσταντίνου Ειδικός Καρδιολόγος, MD, MSc, PhD, CCDS Πανεπιστημιακός Υπότροφος Dr. Konstantinou
Εμφύτευση απινιδωτών για πρωτογενή πρόληψη σε ασθενείς που δεν περιλαμβάνονται στις κλινικές μελέτες Δημήτριος M. Κωνσταντίνου Ειδικός Καρδιολόγος, MD, MSc, PhD, CCDS Πανεπιστημιακός Υπότροφος Dr. Konstantinou
Case based learning: CMR in Heart Failure
 Case based learning: CMR in Heart Failure Milind Y Desai, MD FACC FAHA FESC Associate Professor of Medicine Heart and Vascular Institute, Cleveland Clinic Cleveland, OH Disclosures: none Use of Gadolinium
Case based learning: CMR in Heart Failure Milind Y Desai, MD FACC FAHA FESC Associate Professor of Medicine Heart and Vascular Institute, Cleveland Clinic Cleveland, OH Disclosures: none Use of Gadolinium
ECG Workshop. Nezar Amir
 ECG Workshop Nezar Amir Myocardial Ischemia ECG Infarct ECG in STEMI is dynamic & evolving Common causes of ST shift Infarct Localisation Left main artery occlusion: o diffuse ST-depression with ST elevation
ECG Workshop Nezar Amir Myocardial Ischemia ECG Infarct ECG in STEMI is dynamic & evolving Common causes of ST shift Infarct Localisation Left main artery occlusion: o diffuse ST-depression with ST elevation
Cardiac MRI: Clinical Application to Disease
 Cardiac MRI: Clinical Application to Disease Jessi Smith, MD Cardiothoracic imaging, Indiana University Slides courtesy of Stacy Rissing, MD Outline Imaging planes Disease findings Pulse sequences used
Cardiac MRI: Clinical Application to Disease Jessi Smith, MD Cardiothoracic imaging, Indiana University Slides courtesy of Stacy Rissing, MD Outline Imaging planes Disease findings Pulse sequences used
Arrhythmogenic Cardiomyopathy cases. Δέσποινα Παρχαρίδου Καρδιολόγος Επιστημονικός Συνεργάτης Α Καρδιολογική κλινική ΑΧΕΠΑ
 Arrhythmogenic Cardiomyopathy cases Δέσποινα Παρχαρίδου Καρδιολόγος Επιστημονικός Συνεργάτης Α Καρδιολογική κλινική ΑΧΕΠΑ Definition ARVD (Arrhythmogenic Right Ventricular Dysplasia) Progressive loss of
Arrhythmogenic Cardiomyopathy cases Δέσποινα Παρχαρίδου Καρδιολόγος Επιστημονικός Συνεργάτης Α Καρδιολογική κλινική ΑΧΕΠΑ Definition ARVD (Arrhythmogenic Right Ventricular Dysplasia) Progressive loss of
EVALUATION OF THE ATHLETE. Karen Stout, MD Professor, Medicine and Pediatrics University of Washington
 EVALUATION OF THE 12 ATHLETE Karen Stout, MD Professor, Medicine and Pediatrics University of Washington NO DISCLOSURES OUTLINE Why evaluate athletes? What s the problem? What evaluation should be done?
EVALUATION OF THE 12 ATHLETE Karen Stout, MD Professor, Medicine and Pediatrics University of Washington NO DISCLOSURES OUTLINE Why evaluate athletes? What s the problem? What evaluation should be done?
Investigating the family after a sudden cardiac death. Dr Catherine Mercer Consultant Clinical Geneticist, Wessex
 Investigating the family after a sudden cardiac death Dr Catherine Mercer Consultant Clinical Geneticist, Wessex Sudden adult deaths subdivided Sudden Adult Death Sudden Cardiac Death Sudden Arrhythmic
Investigating the family after a sudden cardiac death Dr Catherine Mercer Consultant Clinical Geneticist, Wessex Sudden adult deaths subdivided Sudden Adult Death Sudden Cardiac Death Sudden Arrhythmic
HCM GUIDELINES ESC 2014 HYPERTROPHIC CARDIOMYOPATHY ASYMPTOMATIC PATIENT
 HCM GUIDELINES ESC 2014 HYPERTROPHIC CARDIOMYOPATHY ASYMPTOMATIC PATIENT Division of Inherited Cardiac Diseases Heart Center for the Young and Athletes A Dpt of Cardiology University of Athens ASYMPTOMATIC
HCM GUIDELINES ESC 2014 HYPERTROPHIC CARDIOMYOPATHY ASYMPTOMATIC PATIENT Division of Inherited Cardiac Diseases Heart Center for the Young and Athletes A Dpt of Cardiology University of Athens ASYMPTOMATIC
Steel vs Alcohol. Or Neither. Management of Hypertrophic Cardiomyopathy. Josh Doll, MD January 24, 2015
 Steel vs Alcohol Or Neither Management of Hypertrophic Cardiomyopathy Josh Doll, MD January 24, 2015 47yo Male, Mr. L Severe progressive dyspnea on exertion and weight gain Previous avid Cross-Fit participant
Steel vs Alcohol Or Neither Management of Hypertrophic Cardiomyopathy Josh Doll, MD January 24, 2015 47yo Male, Mr. L Severe progressive dyspnea on exertion and weight gain Previous avid Cross-Fit participant
Clinical phenotypes associated with Desmosome gene mutations
 Clinical phenotypes associated with Desmosome gene mutations Serio A, Serafini E, Pilotto A, Pasotti M, Gambarin F, Grasso M, Disabella E, Diegoli M, Tagliani M, Arbustini E Centre for Inherited Cardiovascular
Clinical phenotypes associated with Desmosome gene mutations Serio A, Serafini E, Pilotto A, Pasotti M, Gambarin F, Grasso M, Disabella E, Diegoli M, Tagliani M, Arbustini E Centre for Inherited Cardiovascular
Risk Factors for Sudden cardiac Death
 Risk Factors for Sudden cardiac Death A. Arenal Arrhythmias in competitive sports Disclosure Conflict of interest Advisory board: Medtronic, Boston Scientific Research grants: Medtronic, Boston Scientific,
Risk Factors for Sudden cardiac Death A. Arenal Arrhythmias in competitive sports Disclosure Conflict of interest Advisory board: Medtronic, Boston Scientific Research grants: Medtronic, Boston Scientific,
ACTIONABILITY PENETRANCE SIGNIFICANCE/BURDEN OF DISEASE NEXT STEPS. YES ( 1 of above) YES (Proceed to Stage II)
 YES (Proceed to Stage II)") Stage I: Rule-Out Dashboard GENE/GENE PANEL: TNNT2, LMNA HGNC ID: 11949, 6636 ACTIONABILITY 1. Is there a qualifying resource, such as a practice guideline or systematic review, for the genetic condition?
Stage I: Rule-Out Dashboard GENE/GENE PANEL: TNNT2, LMNA HGNC ID: 11949, 6636 ACTIONABILITY 1. Is there a qualifying resource, such as a practice guideline or systematic review, for the genetic condition?
Sudden Death (SD) and hypertrophic cardiomyopathy (HCM) Attempt of risk stratification
 and hypertrophic cardiomyopathy (HCM) Attempt of risk stratification") Sudden Death (SD) and hypertrophic cardiomyopathy (HCM) Attempt of risk stratification 84th Annual Scientific Meeting of the Aerospace Medical Association May 12-16, 2013 Sheraton Chicago Hotel & Towers,
Sudden Death (SD) and hypertrophic cardiomyopathy (HCM) Attempt of risk stratification 84th Annual Scientific Meeting of the Aerospace Medical Association May 12-16, 2013 Sheraton Chicago Hotel & Towers,
Cardiomyopathy. Cardiomyopathies HOCM. Hypertrophic Obstructive Cardiomyopathy. Systolic Anterior Movement (SAM) of Mitral Valve (Venturi Effect) Cine
 of Mitral Valve (Venturi Effect) Cine") Jens Bremerich Radiology University Hospital Basel Hypertrophic Obstructive Cine VENC Cine (5m/s) Modified Bernoulli Equation: P (in mmhg) = 4 x (Vmax)2 Vmax= 4.2 m/s, P = 70mm Hg Hydrodynamica 738 HOCM
Jens Bremerich Radiology University Hospital Basel Hypertrophic Obstructive Cine VENC Cine (5m/s) Modified Bernoulli Equation: P (in mmhg) = 4 x (Vmax)2 Vmax= 4.2 m/s, P = 70mm Hg Hydrodynamica 738 HOCM
ISPUB.COM. Hypertrophic Cardiomyopathy. L Hull-Grommesh CLINICAL DESCRIPTION INCIDENCE/PREVALENCE
 ISPUB.COM The Internet Journal of Advanced Nursing Practice Volume 10 Number 2 L Hull-Grommesh Citation L Hull-Grommesh.. The Internet Journal of Advanced Nursing Practice. 2008 Volume 10 Number 2. Abstract
ISPUB.COM The Internet Journal of Advanced Nursing Practice Volume 10 Number 2 L Hull-Grommesh Citation L Hull-Grommesh.. The Internet Journal of Advanced Nursing Practice. 2008 Volume 10 Number 2. Abstract
6/12/2017. Isolated Noncompaction of the Left Ventricle. Objectives. Pathophysiology
 Isolated Noncompaction of the Left Ventricle Beth Davidson DNP, ACNP, CHFN, CCRN AAHFN June 23, 2017 Objectives 1. Describe the pathophysiology of LVNC 2. Identify the key clinical findings/manifestations
Isolated Noncompaction of the Left Ventricle Beth Davidson DNP, ACNP, CHFN, CCRN AAHFN June 23, 2017 Objectives 1. Describe the pathophysiology of LVNC 2. Identify the key clinical findings/manifestations
Cardiomyopathies. Andre Keren, MD
 Cardiomyopathies Andre Keren, MD Cardiomyopathies Heart muscle disease of unknown etiology Elliott P et al. Eur Heart J 2008;29:270-276 Definition of Cardiomyopathies Elliott P et al. Eur Heart J 2008;29:270-276
Cardiomyopathies Andre Keren, MD Cardiomyopathies Heart muscle disease of unknown etiology Elliott P et al. Eur Heart J 2008;29:270-276 Definition of Cardiomyopathies Elliott P et al. Eur Heart J 2008;29:270-276
Cardiac MRI: Clinical Application to Disease
 Cardiac MRI: Clinical Application to Disease Stacy Rissing, MD! Cardiothoracic imaging, Indiana University! Outline Imaging planes Disease findings Pulse sequences used for each indication Pathophysiology
Cardiac MRI: Clinical Application to Disease Stacy Rissing, MD! Cardiothoracic imaging, Indiana University! Outline Imaging planes Disease findings Pulse sequences used for each indication Pathophysiology
Apical Hypertrophic Cardiomyopathy With Hemodynamically Unstable Ventricular Arrhythmia Atypical Presentation
 Cronicon OPEN ACCESS Hemant Chaturvedi* Department of Cardiology, Non-Invasive Cardiology, Eternal Heart Care Center & research Institute, Rajasthan, India Received: September 15, 2015; Published: October
Cronicon OPEN ACCESS Hemant Chaturvedi* Department of Cardiology, Non-Invasive Cardiology, Eternal Heart Care Center & research Institute, Rajasthan, India Received: September 15, 2015; Published: October
In Vivo Animal Models of Heart Disease. Why Animal Models of Disease? Timothy A Hacker, PhD Department of Medicine University of Wisconsin-Madison
 In Vivo Animal Models of Heart Disease Timothy A Hacker, PhD Department of Medicine University of Wisconsin-Madison Why Animal Models of Disease? Heart Failure (HF) Leading cause of morbidity and mortality
In Vivo Animal Models of Heart Disease Timothy A Hacker, PhD Department of Medicine University of Wisconsin-Madison Why Animal Models of Disease? Heart Failure (HF) Leading cause of morbidity and mortality
Cardiac MRI: Cardiomyopathy
 Cardiac MRI: Cardiomyopathy Laura E. Heyneman, MD I do not have any relevant financial relationships with any commercial interests Cardiac MRI: Cardiomyopathy Laura E. Heyneman, MD Duke University Medical
Cardiac MRI: Cardiomyopathy Laura E. Heyneman, MD I do not have any relevant financial relationships with any commercial interests Cardiac MRI: Cardiomyopathy Laura E. Heyneman, MD Duke University Medical
Review of Cardiac Imaging Modalities in the Renal Patient. George Youssef
 Review of Cardiac Imaging Modalities in the Renal Patient George Youssef ECHO Left ventricular hypertrophy (LVH) assessment Diastolic dysfunction Stress ECHO Cardiac CT angiography Echocardiography - positives
Review of Cardiac Imaging Modalities in the Renal Patient George Youssef ECHO Left ventricular hypertrophy (LVH) assessment Diastolic dysfunction Stress ECHO Cardiac CT angiography Echocardiography - positives
CURRENT GENETIC TESTING TOOLS IN NEONATAL MEDICINE. Dr. Bahar Naghavi
 2 CURRENT GENETIC TESTING TOOLS IN NEONATAL MEDICINE Dr. Bahar Naghavi Assistant professor of Basic Science Department, Shahid Beheshti University of Medical Sciences, Tehran,Iran 3 Introduction Over 4000
2 CURRENT GENETIC TESTING TOOLS IN NEONATAL MEDICINE Dr. Bahar Naghavi Assistant professor of Basic Science Department, Shahid Beheshti University of Medical Sciences, Tehran,Iran 3 Introduction Over 4000
Appropriate Use Criteria for Initial Transthoracic Echocardiography in Outpatient Pediatric Cardiology (scores listed by Appropriate Use rating)
") Appropriate Use Criteria for Initial Transthoracic Echocardiography in Outpatient Pediatric Cardiology (scores listed by Appropriate Use rating) Table 1: Appropriate indications (median score 7-9) Indication
Appropriate Use Criteria for Initial Transthoracic Echocardiography in Outpatient Pediatric Cardiology (scores listed by Appropriate Use rating) Table 1: Appropriate indications (median score 7-9) Indication
Update in Cardiomyopathies: Their New Classifications and Importance of Mixed Phenotypes
 Update in Cardiomyopathies: Their New Classifications and Importance of Mixed Phenotypes Andre Keren MD Hadassah-Hebrew University Hospital, Jerusalem Cesarea, 2008 f o s r a es e y t hi 0 a 5 p t o rs
Update in Cardiomyopathies: Their New Classifications and Importance of Mixed Phenotypes Andre Keren MD Hadassah-Hebrew University Hospital, Jerusalem Cesarea, 2008 f o s r a es e y t hi 0 a 5 p t o rs
Implications of the new diagnostic criteria for ARVC
 EUROECHO 2010 Echocardiographic assessment of cardiomyopathies Implications of the new diagnostic criteria for ARVC Barbara Bauce, MD, PhD Department of Cardiac, Thoracic and Vascular Sciences University
EUROECHO 2010 Echocardiographic assessment of cardiomyopathies Implications of the new diagnostic criteria for ARVC Barbara Bauce, MD, PhD Department of Cardiac, Thoracic and Vascular Sciences University
HCM GENETIC OR CLINICAL FAMILY SCREENING?
 HCM GENETIC OR CLINICAL FAMILY SCREENING? Division of Inherited Cardiac Diseases Heart Center for the Young and Athletes A Dpt of Cardiology University of Athens GENETICS IN HCM DIAGNOSIS GENETIC RECOMFIRMATION
HCM GENETIC OR CLINICAL FAMILY SCREENING? Division of Inherited Cardiac Diseases Heart Center for the Young and Athletes A Dpt of Cardiology University of Athens GENETICS IN HCM DIAGNOSIS GENETIC RECOMFIRMATION
Dr Navin Chandra Clinical Research Fellow in Cardiology St George s University of London
 Dr Navin Chandra Clinical Research Fellow in Cardiology St George s University of London Cardiac Adaptation in Athletes Athletic training for prolonged periods may result in physiological adaptations of
Dr Navin Chandra Clinical Research Fellow in Cardiology St George s University of London Cardiac Adaptation in Athletes Athletic training for prolonged periods may result in physiological adaptations of
The Genetics and Prevention of Sudden Cardiac Death
 The Genetics and Prevention of Sudden Cardiac Death Sudden cardiac death (SCD), a serious public health problem Every day, between 1,600 and 2,000 people die worldwide from genetically caused SCD. 1 SCD
The Genetics and Prevention of Sudden Cardiac Death Sudden cardiac death (SCD), a serious public health problem Every day, between 1,600 and 2,000 people die worldwide from genetically caused SCD. 1 SCD
Medical Policy and and and and
 ARBenefits Approval: 10/12/2011 Effective Date: 01/01/2012 Revision Date: Code(s): 93799, Unlisted cardiovascular service or procedure Medical Policy Title: Percutaneous Transluminal Septal Myocardial
ARBenefits Approval: 10/12/2011 Effective Date: 01/01/2012 Revision Date: Code(s): 93799, Unlisted cardiovascular service or procedure Medical Policy Title: Percutaneous Transluminal Septal Myocardial
Why Cardiac MRI? Presented by:
 Why Cardiac MRI? Presented by: Lisa G. Carkner, MD, FACC 1 Disclosures I have no financial disclosures Objectives Review basic principles of Cardiac MRI. What patient characteristics do I need to consider
Why Cardiac MRI? Presented by: Lisa G. Carkner, MD, FACC 1 Disclosures I have no financial disclosures Objectives Review basic principles of Cardiac MRI. What patient characteristics do I need to consider
Το ΗΚΓ στις Μυοκαρδιοπάθειες και στην Περικαρδίτιδα
 4 ο ΠΑΝΕΛΛΗΝΙΟ ΑΡΡΥΘΜΙΟΛΟΓΙΚΟ ΣΥΝΕΔΡΙΟ Φροντιστηριακό Μάθημα ΗΚΓ Το ΗΚΓ στις Μυοκαρδιοπάθειες και στην Περικαρδίτιδα Γ.Ν.Α. «Ο Ευαγγελισμός» Ξυδώνας Σωτήριος, MD, PhD, FESC Εργαστήριο Ηλεκτροφυσιολογίας
4 ο ΠΑΝΕΛΛΗΝΙΟ ΑΡΡΥΘΜΙΟΛΟΓΙΚΟ ΣΥΝΕΔΡΙΟ Φροντιστηριακό Μάθημα ΗΚΓ Το ΗΚΓ στις Μυοκαρδιοπάθειες και στην Περικαρδίτιδα Γ.Ν.Α. «Ο Ευαγγελισμός» Ξυδώνας Σωτήριος, MD, PhD, FESC Εργαστήριο Ηλεκτροφυσιολογίας
Molecular Diagnostic Laboratory 18 Sequencing St, Gene Town, ZY Tel: Fax:
 Molecular Diagnostic Laboratory 18 Sequencing St, Gene Town, ZY 01234 Tel: 555-920-3333 Fax: 555-920-3334 www.moldxlaboratory.com Patient Name: Jane Doe Specimen type: Blood, peripheral DOB: 04/05/1990
Molecular Diagnostic Laboratory 18 Sequencing St, Gene Town, ZY 01234 Tel: 555-920-3333 Fax: 555-920-3334 www.moldxlaboratory.com Patient Name: Jane Doe Specimen type: Blood, peripheral DOB: 04/05/1990
7. Echocardiography Appropriate Use Criteria (by Indication)
") Criteria for Echocardiography 1133 7. Echocardiography Criteria (by ) Table 1. TTE for General Evaluation of Cardiac Structure and Function Suspected Cardiac Etiology General With TTE 1. Symptoms or conditions
Criteria for Echocardiography 1133 7. Echocardiography Criteria (by ) Table 1. TTE for General Evaluation of Cardiac Structure and Function Suspected Cardiac Etiology General With TTE 1. Symptoms or conditions
in Familial Dilated Cardiomyopathy
 Familial Dilated Cardiomyopathy y Clinical and Genetic et Issues in Familial Dilated Cardiomyopathy College of Medicine, Chungbuk National University Kyung-Kuk Hwang Contents Definition (criteria) Clinical
Familial Dilated Cardiomyopathy y Clinical and Genetic et Issues in Familial Dilated Cardiomyopathy College of Medicine, Chungbuk National University Kyung-Kuk Hwang Contents Definition (criteria) Clinical
27-year-old professionnal rugby player: asymptomatic
 27-year-old professionnal rugby player: asymptomatic Benefits and limits of cardiac MRI in the young athlete with a suspected heart disease. Philippe PAULE Service de Cardiologie, HIA Clermont Tonnerre,
27-year-old professionnal rugby player: asymptomatic Benefits and limits of cardiac MRI in the young athlete with a suspected heart disease. Philippe PAULE Service de Cardiologie, HIA Clermont Tonnerre,
DIAGNOSIS AND MANAGEMENT OF ARRHYTHMOGENIC CARDIOMYOPATHY. David SIU MD ( 蕭頌華醫生 ) Division of Cardiology The University of Hong Kong
 Division of Cardiology The University of Hong Kong") APHRS Summit 2018 in conjunction with HKCC Heart Rhythm Refresher Course DIAGNOSIS AND MANAGEMENT OF ARRHYTHMOGENIC CARDIOMYOPATHY David SIU MD ( 蕭頌華醫生 ) Division of Cardiology The University of Hong Kong
APHRS Summit 2018 in conjunction with HKCC Heart Rhythm Refresher Course DIAGNOSIS AND MANAGEMENT OF ARRHYTHMOGENIC CARDIOMYOPATHY David SIU MD ( 蕭頌華醫生 ) Division of Cardiology The University of Hong Kong
Dr Philippe Charron. ESC congress, Stockholm, 29 August 2010
 Inherited cardiomyopathies and and channelopathies: who is at risk for sudden cardiac death? Does genetic profiling predict risk in individual patients? Dr Philippe Charron Centre de Référence pour les
Inherited cardiomyopathies and and channelopathies: who is at risk for sudden cardiac death? Does genetic profiling predict risk in individual patients? Dr Philippe Charron Centre de Référence pour les
Heart Failure Compendium. Thomas J. Cahill, Houman Ashrafian, Hugh Watkins
 Heart Failure Compendium Circulation Research Compendium on Heart Failure Research Advances in Heart Failure: A Compendium Epidemiology of Heart Failure Genetic Cardiomyopathies Causing Heart Failure Non-coding
Heart Failure Compendium Circulation Research Compendium on Heart Failure Research Advances in Heart Failure: A Compendium Epidemiology of Heart Failure Genetic Cardiomyopathies Causing Heart Failure Non-coding
Presenter: Steven Brust, HCS-D, HCS-H Product Manager, Home Health Coding Center
 Presenter: Steven Brust, HCS-D, HCS-H Product Manager, Home Health Coding Center Pinpoint & properly assign the appropriate heart failure codes Left- vs. Right-sided Left ventricular failure (LVF) may
Presenter: Steven Brust, HCS-D, HCS-H Product Manager, Home Health Coding Center Pinpoint & properly assign the appropriate heart failure codes Left- vs. Right-sided Left ventricular failure (LVF) may
Familial Aggregation of Dilated Cardiomyopathy in Patients with Peripartum Cardiomyopathy
 Familial Aggregation of Dilated Cardiomyopathy in Patients with Peripartum Cardiomyopathy Tibazarwa K 1, Sliwa K 1, Wonkam A 2, Mayosi BM 1 1 Hatter Cardiovascular Research Institute, Department of Medicine,
Familial Aggregation of Dilated Cardiomyopathy in Patients with Peripartum Cardiomyopathy Tibazarwa K 1, Sliwa K 1, Wonkam A 2, Mayosi BM 1 1 Hatter Cardiovascular Research Institute, Department of Medicine,
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Genetic Testing for Predisposition to Page 1 of 19 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Genetic Testing for Predisposition to Inherited Hypertrophic Cardiomyopathy
Genetic Testing for Predisposition to Page 1 of 19 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Genetic Testing for Predisposition to Inherited Hypertrophic Cardiomyopathy
Sudden Cardiac Death in Sports: Causes and Current Screening Recommendations
 Sports Cardiology Sudden Cardiac Death in Sports: Causes and Current Screening Recommendations Domenico Corrado, MD, PhD Inherited Arrhytmogenic Cardiomyopathy Unit Department of Cardiac, Thoracic and
Sports Cardiology Sudden Cardiac Death in Sports: Causes and Current Screening Recommendations Domenico Corrado, MD, PhD Inherited Arrhytmogenic Cardiomyopathy Unit Department of Cardiac, Thoracic and
Highlights from EuroEcho 2009 Echo in cardiomyopathies
 Highlights from EuroEcho 2009 Echo in cardiomyopathies Bogdan A. Popescu University of Medicine and Pharmacy, Bucharest, Romania ESC Congress 2010 Hypertrophic cardiomyopathy To determine the differences
Highlights from EuroEcho 2009 Echo in cardiomyopathies Bogdan A. Popescu University of Medicine and Pharmacy, Bucharest, Romania ESC Congress 2010 Hypertrophic cardiomyopathy To determine the differences
Update on use of cardiac MRI in ARVC/D. Stefan L. Zimmerman, MD Johns Hopkins University Department of Radiology
 Update on use of cardiac MRI in ARVC/D Stefan L. Zimmerman, MD Johns Hopkins University Department of Radiology Outline Background Diagnosis Characteristic imaging findings Genetics of ARVC Genotype phenotype
Update on use of cardiac MRI in ARVC/D Stefan L. Zimmerman, MD Johns Hopkins University Department of Radiology Outline Background Diagnosis Characteristic imaging findings Genetics of ARVC Genotype phenotype
Clinical Policy: Holter Monitors Reference Number: CP.MP.113
 Clinical Policy: Reference Number: CP.MP.113 Effective Date: 05/18 Last Review Date: 04/18 Coding Implications Revision Log Description Ambulatory electrocardiogram (ECG) monitoring provides a view of
Clinical Policy: Reference Number: CP.MP.113 Effective Date: 05/18 Last Review Date: 04/18 Coding Implications Revision Log Description Ambulatory electrocardiogram (ECG) monitoring provides a view of
ASE 2011 Appropriate Use Criteria for Echocardiography
 ASE 2011 Appropriate Use Criteria for Echocardiography Table 1. TTE for General Evaluation of Cardiac Structure and Function 1 2 Suspected Cardiac Etiology General With TTE Symptoms or conditions potentially
ASE 2011 Appropriate Use Criteria for Echocardiography Table 1. TTE for General Evaluation of Cardiac Structure and Function 1 2 Suspected Cardiac Etiology General With TTE Symptoms or conditions potentially
Medical Policy An Independent Licensee of the Blue Cross and Blue Shield Association
 Genetic Testing for Predisposition to Page 1 of 12 Medical Policy An Independent Licensee of the Blue Cross and Blue Shield Association Title: Genetic Testing for Predisposition to Inherited Hypertrophic
Genetic Testing for Predisposition to Page 1 of 12 Medical Policy An Independent Licensee of the Blue Cross and Blue Shield Association Title: Genetic Testing for Predisposition to Inherited Hypertrophic
Family stories: to illustrate inheritance and the impact on families. Dr Claire Turner Consultant clinical geneticist
 Family stories: to illustrate inheritance and the impact on families Dr Claire Turner Consultant clinical geneticist Overview With respect to inherited cardiac conditions Simple modes of inheritance (Mendelian)
Family stories: to illustrate inheritance and the impact on families Dr Claire Turner Consultant clinical geneticist Overview With respect to inherited cardiac conditions Simple modes of inheritance (Mendelian)