Syncope and Cardiovascular Causes of Falls in Older People. Professor T. Masud Nottingham University Hospitals NHS Trust
|
|
|
- Justina Jordan
- 6 years ago
- Views:
Transcription
1 Syncope and Cardiovascular Causes of Falls in Older People Professor T. Masud Nottingham University Hospitals NHS Trust
2 Faller 1 75 male, smoker, moderate alcohol intake Retired driving instructor At least 3 falls in 5 months One episode of falls with loss of consciousness No warning signs No palpitations/ chest pain
3 Faller 1 Investigations FBC/ U&ES/ LFTS/blood sugar normal ECG- sinus rhythm, rate = 86/mt, normal CXR - no abnormality 24-hour tape normal
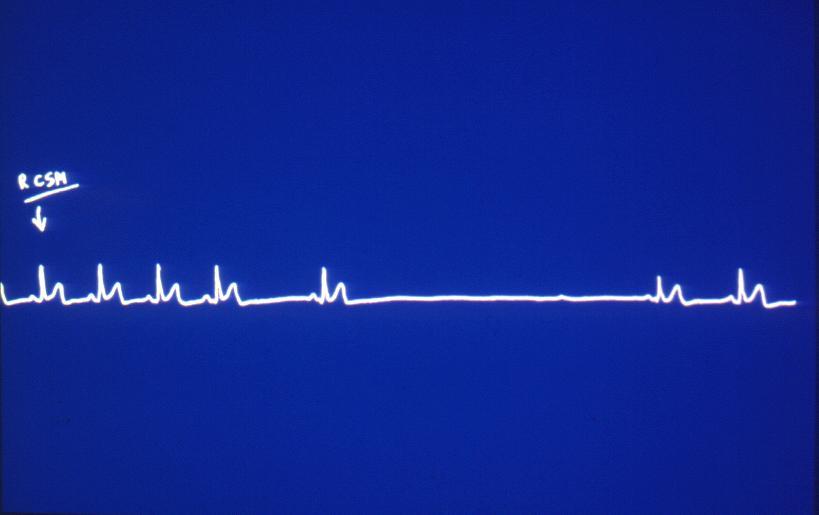
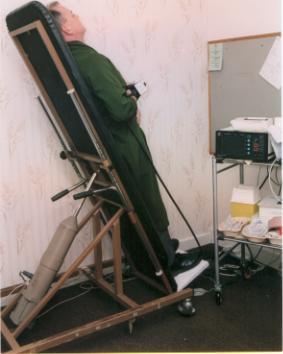
4 Faller 1 Tilt test Right Carotid sinus massage 5 second pause ( symptomatic ) No orthostatic hypotension No delayed vasodepressor effects
5
6 Faller 1 Carotid sinus syndrome (cardio-inhibitory type) Treatment : Dual chamber pacemaker F/u at one year no further falls
7 Faller 2 Mr. N 65 male Asian Collapse preceded by dizziness and loss of consciousness No chest pain/ palpitations Light-headedness and feeling of about to pass out during prayer on most occasions
8 Faller 2 O/E Sinus rhythm BP 132/74 mm Hg No postural hypotension No murmurs No carotid bruits Evidence of peripheral neuropathy
9 Faller 2 Tilt test response CSM >50 mm Hg systolic drop in BP (symptoms) Certain neck movements precipitated presyncope No orthostatic hypotension No delayed vasodepressor response
10 Faller 2 Carotid sinus syndrome (Vasodepressor Type ) Management : Life style modifications
11 Faller 3 EW 75 yrs. Female Falls at least 4 times in 12 months Mainly outdoors twice while shopping in the supermarket Dizzy, sweaty, looses consciousness for a few seconds Witness account pale and sweaty
12 Faller 3 Haematological & biochemical investigations normal 24 hour Holter monitoring X 2 - NAD ECG Sinus rhythm What next?
13 Faller 3 CSM no response Prolonged head-up tilt
14

15 ROMorris 2000
16 Results Time (minutes) Blood Pressure Heart rate 0 (Supine) 151/ (Upright) 138/ / / / / / / unrecordable 48




17 Faller 3 Neurocardiogenic (vasovagal) syncope Management General advice TED Stockings Fludrocortisone Follow up at 3 & 6 months no syncope
18 The overlap between falls, dizziness and syncope Falls Dizziness Syncope
19 Overlap of Falls and Syncope in Older People 30% of cognitively intact older people are unable to recall documented falls 3 months after the event Eye witness accounts of falls are often unavailable Amnesia for a loss of consciousness is present in up to 50% of patients with syncope
20 Definition of Syncope A transient loss of consciousness, due to a temporary impairment of cerebral perfusion, characterised by unresponsiveness and loss of postural tone with spontaneous recovery
21 Syncope: Reported Frequency Individuals <18 yrs Military Population yrs Individuals yrs* 15% 20-25% 16-19% Individuals >70 yrs* *during a 10-year period 23%
22 Causes of Syncope (CORN) Cardiac Arrhythmia (eg. sinus node disease) Outflow obstruction (eg. Aortic stenosis, HOCM) Circulatory failure (eg. pulmonary embolism) Orthostatic Hypotension (including postprandial) Reflex syncope Vasovagal (neurocardiogenic, neurally mediated, vasodepressor) Carotid sinus syndrome (cardioinhibitory, vasodepressor, mixed) Glossopharyngeal syncope (associated with glossopharyngeal neuralgia) Post-prandial hypotension Neurological Disease Vertebrobasilar TIA (other neuro signs/symptoms usually present) Subclavian steal syndrome Basilar migraine (rare) Conditions Mimicking Syncope ( but no reduction in cerebral perfusion) Epilepsy Metabolic disorders (eg. hypoglycaemia) Psychiatric (less common in elderly than younger syncope patients
23 The Commoner Cardiovascular Causes of Falls in the elderly (same causes for Syncope) Orthostatic Hypotension (OH) Arrhythmias (eg AV block, sick sinus) Structural Heart Disease (eg aortic stenosis) Carotid Sinus Syndrome Neurocardiogenic Syncope Postprandial Hypotension
24 Orthostatic Hypotension Defined as >20 mmhg fall in systolic blood pressure and/or a >10 mmhg fall in diastolic blood pressure within 3 minutes of standing WITH symptoms
25 Orthostatic Hypotension- Symptoms Dizziness Syncope/pre-syncope Circadian pattern Occipital or Coat Hanger Headache
26 Orthostatic Hypotension- Prevalence Varies on the population studied Community dwelling Institutionalised Acute in-patients Hypertension trials
27 Orthostatic Hypotension- Prevalence Investigator Number Type of patients Prevalence Rodstein et Zeman 250 Nursing Home 8% (1957) Johnson et al(1965) 100 In patients 17% Lennox et Williams 272 In patients 10% (1980) Robinson et al (1994) 106 Clinic 27.4% Alli et al (1992) 858 G.P.clinic 13.8% Mader et al (1987) 300 Health screening 13.7% Caird et al (1973) 294 Community dwelling 24% Rutan et al (1992) 5,201 Community dwelling 16.2%
28 Orthostatic Hypotension- Aetiology Circulatory Volume loss /Dehydration Medication Autonomic Failure (eg Diabetes ) Parkinson s Disease / MSA (Shy-Drager) Hypertension
29 Orthostatic Hypotension - Diagnosis Fulfil diagnostic criteria Monitor BP changes at different times of the day Consider Ambulatory BP Monitoring
30 Orthostatic Hypotension - Treatment Treat any acute conditions Review medication Postural training Head of bed raised Compression hosiery (careful of PVD) Fludrocortisone (can worsen heart failure) Midodrine - alpha 1 receptor agonist (careful of IHD) - causes peripheral vasoconstriction - can cause supine hypertension & piloerection
 Males > Females Associated with IHD and hypertension Associated with neurocardiogenic syncope and orthostatic hypotension Appreciable morbidity (injuries 50%).")
31 Carotid Sinus Syndrome (CSS) A cause of falls, dizziness and syncope in the elderly Not uncommon but rarely diagnosed Exaggerated baroreflex activity episodic bradycardia ± hypotension Disorder of the elderly (virtually unknown < 50yrs) Males > Females Associated with IHD and hypertension Associated with neurocardiogenic syncope and orthostatic hypotension Appreciable morbidity (injuries 50%). Low mortality

32 Carotid Sinus Syndrome (CSS) occurs in 0.5%-9.9% of patients with recurrent syncope in up to 14% of older people in nursing homes in up to 30% of older people with unexplained syncope and drop attacks associated with digoxin, b blockers, methyldopa association described with Alzheimers, Parkinsonism, Lewy Body disease

33 Carotid Sinus Syndrome (CSS) Precipitants: Head turning (tight neckwear) Looking up Vagal manoeuvres Micturition Defecation Coughing Swallowing Prolonged standing Exertion Meals

 - 50mmHg systolic drop (vasodepressor CSS) -")
34 How to perform Carotid Sinus Massage Exclude carotid bruits Longitudinal massage repeated both sides: 5-10 s Supine and at 70 head-upright tilt Resuscitation equipment C/I if CVA, TIA, MI within 3 months Relative C/Is- h/o VT, VF, carotid bruit (consider US) Positive response : - 3 s asystole (cardioinhibitory CSS) - 50mmHg systolic drop (vasodepressor CSS) - Mixed response
 General advice (avoid tight collars, sudden")

35 Carotid Sinus Syndrome (CSS) Management Treat only if symptomatic (2 syncopal episodes) General advice (avoid tight collars, sudden neck turning) Cardioinhibitory type Vasodepressor type Dual chamber pacing Anticholinergics Increase salt & fluids Fludrocortisone Midodrine

36 The Carotid Sinus Dilated portion of ICA Thin tunica media Abundant elastic tissue Rich sensory supply Nerve of Herring Glossopharngeal Nerve
37 Carotid Sinus Syndrome (CSS) Proposed mechanism Central processing Alpha 2, 5HT receptors Aortic arch & Heart Baroreceptors X Sympathetic Outflow + Vagus Heart rate Contractility Afferent Pathways Efferent Pathways Arteriolar tone IX Brainstem- medulla + pons Carotid sinus IX nucleus tractus solitarus Baroreceptors X Paramedian nucleus
 Witness - pallor, ashen colour, cold and clammy - dilated pupils - convulsive syncope - rapid recovery in mental")
38 Neurocardiogenic syncope (NCS) (Vasovagal, delayed vasopressor, neurally mediated) Features Upright posture Prodrome, LOC Post-syncopal nausea, headache, malaise (often no warning in the elderly + amnesia) Witness - pallor, ashen colour, cold and clammy - dilated pupils - convulsive syncope - rapid recovery in mental state

39 Neurocardiogenic syncope (NCS) Triggers Prolonged standing emotional stress, anxiety pain, pain anticipation, venepuncture accident, sight of blood situational e.g. - defecation, micturition, cough food, alcohol (esp. in the elderly)
40 Neurocardiogenic syncope (NCS)-one proposed mechanism Upright posture Downward displacement of blood Increased venous pooling Decreased ventricular filling Overstimulation of hypersensitive baroreceptors in LV wall Mechanoreceptor stimulation Increased afferent flow to brain stem vasodilatation bradycardia hypotension SYNCOPE
 Isoprenaline Venous")
41 Neurocardiogenic syncope (NCS) Diagnosis History Prolonged head-upright tilt with symptom reproduction Provocative tests: GTN (s/l or i/v) Isoprenaline Venous cannulation


42 How to perform Head-up Tilt test Tilt table 70 head up for 40 mins After 20 mins give GTN spray 400mcg Continuous BP and ECG monitoring Diagnoses Neurocardiogenic (vasovagal) syndrome Orthostatic hypotension Hyperventilation Central dizziness (symptoms only)

43 Cardiovascular Causes of Falls
 Compression Stockings")
![Fludrocortisone Midodrine (pre-synaptic alpha 1 agonist [sympathomimetic]) SSRIs (ß Blockers)](/docs-images/74/70136134/images/44-3.jpg "(Disopyramide) (Dual chamber pacing consider only if prolonged asystole - controversial")
44 Neurocardiogenic syncope (NCS) Management: (difficult) General advice (avoid prolonged standing, heat, dehydration, large meals, alcohol; increase water intake) Compression Stockings Fludrocortisone Midodrine (pre-synaptic alpha 1 agonist [sympathomimetic]) SSRIs (ß Blockers) (Disopyramide) (Dual chamber pacing consider only if prolonged asystole - controversial especially in the young)

45 Post Prandial Hypotension
46 Postprandial Hypotension Definition: A fall of 20 mmhg in Systolic blood pressure after the ingestion of a meal Can have effect for up to 90 minutes
47 Postprandial Hypotension Symptoms Similar to those of orthostatic hypotension though related temporally to meal times
48 Postprandial Hypotension Increased incidence of postprandial hypotension in patients with falls and syncope Worse after breakfast Associated with diabetes and number of prescribed drugs
49 Postprandial Hypotension Advise to eat smaller meals more frequently Rest after meals Water drinking Avoid alcohol
50 Overlap of Vasodepressor syndromes Orthostatic Hypotension Neurocardiogenic Syndrome Postprandial Hypotension Carotid Sinus Syndrome
 3. FBC, U&Es, LFTs, TFTs, glucose 4. Urinalysis 5. Specific tests as directed by 1 & 2 6. ECG 7. CXR")
51 Cardiovascular Causes and Falls Basic medical assessment of falls 1. Careful history 2. Thorough examination (inc.postural BP) 3. FBC, U&Es, LFTs, TFTs, glucose 4. Urinalysis 5. Specific tests as directed by 1 & 2 6. ECG 7. CXR
52 Further investigations to consider if appropriate: Holter monitoring (24 hour- 7day tapes) Echocardiography Carotid Sinus Massage Head-up Tilt Testing Ambulatory BP monitoring Implantable loop recorder Electrophysiological studies CT, EEG, Carotid Ultrasound
53 Suggested Protocol for the investigation of Syncope History Examination (including Lying/Standing Blood Pressure and 12 lead ECG) Orthostatic Hypotension Normal ECG No Orthostatic Hypotension Normal ECG No Orthostatic Hypotension Abnormal ECG Review medication Consider 24 hour ABPM TED stockings/lifestyle advice Referral for Tilt Table Testing with carotid sinus massage 24 hour monitor/echocardiogram If symptoms persist consider referral If normal Referral for Tilt Table Testing with carotid sinus massage

54 Testing (combines Carotid Sinus Massage and Prolonged Head Up Tilt Test) Carotid sinus massage R/L Supine and Tilted Supine Rest for 10 mins Head-Up tilt to 70 degress for mins Terminate if symptomatic or systolic blood pressure < 80 mmhg GTN Provocation Terminate if symptomatic or systolic blood pressure < 80 mmhg Supine rest for mins
55 Important Messages Always consider a cardiovascular aetiology if the cause of recurrent falls remains unexplained Carotid sinus syndrome and neurocardiogenic causes of unexplained syncope and unexplained falls are not uncommon Tilt Testing (including carotid sinus massage) can be a useful diagnostic aid in these patients
56
57 Fitting syncope investigations into a Falls Service Uncertainty over who to target High risk patients (such as those who have presented to A&E with an injury after falling) Patients with a clear syncope history History of drop attacks Recurrent or unexplained fallers
58 Who not to investigate for underlying syncope Dementia (Folstein MMSE<20) One off fallers Patients with obvious mechanical source for falls, e.g. impaired vision, aortic stenosis
Medicine Dr. Aso Lecture 9 Syncope and Pre-syncope
 Medicine Dr. Aso Lecture 9 Syncope and Pre-syncope SYNCOPE AND PRE-SYNCOPE Syncope:- sudden, transient loss of consciousness, due to reduced cerebral perfusion. The patient is unresponsive with loss of
Medicine Dr. Aso Lecture 9 Syncope and Pre-syncope SYNCOPE AND PRE-SYNCOPE Syncope:- sudden, transient loss of consciousness, due to reduced cerebral perfusion. The patient is unresponsive with loss of
Neurocardiogenic syncope
 Neurocardiogenic syncope Syncope Definition Collapse,Blackout A sudden, transient loss of consciousness and postural tone, with spontaneous recovery Very common Syncope Prevalence All age groups (particularly
Neurocardiogenic syncope Syncope Definition Collapse,Blackout A sudden, transient loss of consciousness and postural tone, with spontaneous recovery Very common Syncope Prevalence All age groups (particularly
Syncope: Evaluation of the Weak and Dizzy
 Syncope: Evaluation of the Weak and Dizzy William M. Miles, MD, FACC, FHRS Professor of Medicine Silverstein Chair for Cardiovascular Education University of Florida College of Medicine Disclosures Medtronic,
Syncope: Evaluation of the Weak and Dizzy William M. Miles, MD, FACC, FHRS Professor of Medicine Silverstein Chair for Cardiovascular Education University of Florida College of Medicine Disclosures Medtronic,
Rapid Access Clinics for Transient Loss of Consciousness
 Rapid Access Clinics for Transient Loss of Consciousness Michael Gammage Department of Cardiovascular Medicine University of Birmingham and University Hospital Birmingham NHS Foundation Trust Those who
Rapid Access Clinics for Transient Loss of Consciousness Michael Gammage Department of Cardiovascular Medicine University of Birmingham and University Hospital Birmingham NHS Foundation Trust Those who
Syncope: Evaluation of the Weak and Dizzy
 Syncope: Evaluation of the Weak and Dizzy William M. Miles, MD, FACC, FHRS Professor of Medicine Silverstein Chair for Cardiovascular Education University of Florida College of Medicine Disclosures Medtronic,
Syncope: Evaluation of the Weak and Dizzy William M. Miles, MD, FACC, FHRS Professor of Medicine Silverstein Chair for Cardiovascular Education University of Florida College of Medicine Disclosures Medtronic,
DECLARATION OF CONFLICT OF INTEREST
 DECLARATION OF CONFLICT OF INTEREST The Management of Syncope remains a challenge: Clues from the History Richard Sutton, DSc Emeritus Professor of Cardiology Imperial College, St Mary s Hospital, London,
DECLARATION OF CONFLICT OF INTEREST The Management of Syncope remains a challenge: Clues from the History Richard Sutton, DSc Emeritus Professor of Cardiology Imperial College, St Mary s Hospital, London,
Syncope Update Dr Matthew Lovell, Consultant in Cardiology
 Syncope Update Dr Matthew Lovell, Consultant in Cardiology Definition of Syncope Syncope is defined as TLOC due to cerebral hypoperfusion Characterized by a rapid onset, short duration, and spontaneous
Syncope Update Dr Matthew Lovell, Consultant in Cardiology Definition of Syncope Syncope is defined as TLOC due to cerebral hypoperfusion Characterized by a rapid onset, short duration, and spontaneous
Syncope Guidelines: What s New?
 Syncope Guidelines: What s New? Dr. Samuel Asirvatham Professor of Medicine and Pediatrics Mayo Clinic College of Medicine Medical Director, Electrophysiology Laboratory Program Director, EP Fellowship
Syncope Guidelines: What s New? Dr. Samuel Asirvatham Professor of Medicine and Pediatrics Mayo Clinic College of Medicine Medical Director, Electrophysiology Laboratory Program Director, EP Fellowship
Syncope By Remus Popa
 Syncope By Remus Popa A 66 years old male is brought to the ED from a restaurant where he fainted while dining out with his family. He complained of nausea and stood up to go to the restroom but immediately
Syncope By Remus Popa A 66 years old male is brought to the ED from a restaurant where he fainted while dining out with his family. He complained of nausea and stood up to go to the restroom but immediately
Valutazione iniziale e stratificazione del rischio
 Valutazione iniziale e stratificazione del rischio Paolo Alboni Sezione di Cardiologia Ospedale Privato Quisisana Ferrara DEFINITION OF SYNCOPE Syncope is a transient loss of consciousness due to global
Valutazione iniziale e stratificazione del rischio Paolo Alboni Sezione di Cardiologia Ospedale Privato Quisisana Ferrara DEFINITION OF SYNCOPE Syncope is a transient loss of consciousness due to global
Lee Chee Wan. Senior Consultant Pacing and Cardiac Electrophysiology. GP Symposium 2 nd April 2016
 Lee Chee Wan Senior Consultant Pacing and Cardiac Electrophysiology GP Symposium 2 nd April 2016 Objectives Definition of syncope Common causes of syncope & impacts How to clinically assess patient with
Lee Chee Wan Senior Consultant Pacing and Cardiac Electrophysiology GP Symposium 2 nd April 2016 Objectives Definition of syncope Common causes of syncope & impacts How to clinically assess patient with
Department of Paediatrics Clinical Guideline. Syncope Guideline
 Department of Paediatrics Clinical Guideline Syncope Guideline Definition Transient, self-limited loss of consciousness (TLOC), usually leading to falling. Onset is relatively rapid. Recovery is spontaneous,
Department of Paediatrics Clinical Guideline Syncope Guideline Definition Transient, self-limited loss of consciousness (TLOC), usually leading to falling. Onset is relatively rapid. Recovery is spontaneous,
An Approach to the Patient with Syncope. Guy Amit MD, MPH Soroka University Medical Center Beer-Sheva
 An Approach to the Patient with Syncope Guy Amit MD, MPH Soroka University Medical Center Beer-Sheva Case presentation A 23 y.o. man presented with 2 episodes of syncope One during exercise,one at rest
An Approach to the Patient with Syncope Guy Amit MD, MPH Soroka University Medical Center Beer-Sheva Case presentation A 23 y.o. man presented with 2 episodes of syncope One during exercise,one at rest
SYNCOPE. Sanjay P. Singh, MD Chairman & Professor, Department of Neurology. Syncope
 SYNCOPE Sanjay P. Singh, MD Chairman & Professor, Department of Neurology. Syncope Syncope is a clinical syndrome characterized by transient loss of consciousness (TLOC) and postural tone that is most
SYNCOPE Sanjay P. Singh, MD Chairman & Professor, Department of Neurology. Syncope Syncope is a clinical syndrome characterized by transient loss of consciousness (TLOC) and postural tone that is most
Syncope in ED-Risk Stratification Ger McMahon
 Syncope in ED-Risk Stratification Ger McMahon 3-8% of ED presentations increasing with advancing age ED physicians ranked syncope as the 2 nd most common decision making dilemma >50% are admitted @ 75%
Syncope in ED-Risk Stratification Ger McMahon 3-8% of ED presentations increasing with advancing age ED physicians ranked syncope as the 2 nd most common decision making dilemma >50% are admitted @ 75%
Syncope as we age: Frequency of causes and cost of care
 Syncope as we age: Frequency of causes and cost of care Dr Steve W Parry Clinical Senior Lecturer and Honorary Consultant Physician Clinical Director, Medicine Falls and Syncope Service, Royal Victoria
Syncope as we age: Frequency of causes and cost of care Dr Steve W Parry Clinical Senior Lecturer and Honorary Consultant Physician Clinical Director, Medicine Falls and Syncope Service, Royal Victoria
Sequoia Heart Symposium 2018: Syncope. Gregory Engel, MD
 Sequoia Heart Symposium 2018: Syncope Gregory Engel, MD Silicon Valley Cardiology Palo Alto Medical Foundation Sutter Health Palo Alto, Redwood City, and San Carlos, CA Chief, Cardiovascular Division Sequoia
Sequoia Heart Symposium 2018: Syncope Gregory Engel, MD Silicon Valley Cardiology Palo Alto Medical Foundation Sutter Health Palo Alto, Redwood City, and San Carlos, CA Chief, Cardiovascular Division Sequoia
Syncope. Charles DeBerardinis, DO Iredell Health Systems
 Syncope Charles DeBerardinis, DO Iredell Health Systems Syncope Syncope loss of consciousness Vertigo sensation of motion Drop attacks fall without loss of consciousness seizure Syncope Constatino n=670
Syncope Charles DeBerardinis, DO Iredell Health Systems Syncope Syncope loss of consciousness Vertigo sensation of motion Drop attacks fall without loss of consciousness seizure Syncope Constatino n=670
Death after Syncope: Can we predict it? Daniel Zamarripa, MD Senior Medical Director December 2013
 Death after Syncope: Can we predict it? Daniel Zamarripa, MD Senior Medical Director December 2013 Death after Syncope: Can we predict it? Those who suffer from frequent and severe fainting often die suddenly
Death after Syncope: Can we predict it? Daniel Zamarripa, MD Senior Medical Director December 2013 Death after Syncope: Can we predict it? Those who suffer from frequent and severe fainting often die suddenly
UNIVERSITY HOSPITALS OF LEICESTER NHS TRUST CARDIAC INVESTIGATIONS PAEDIATRIC & CONGENITAL SYNCOPE INVESTIGATIONS/QUESTIONNAIRE PROTOCOL
 UNIVERSITY HOSPITALS OF LEICESTER NHS TRUST CARDIAC INVESTIGATIONS PAEDIATRIC & CONGENITAL SYNCOPE INVESTIGATIONS/QUESTIONNAIRE PROTOCOL Written Date: 2009 by Dr Duke, then updated by Dr Sarita Makam 12/4/2016
UNIVERSITY HOSPITALS OF LEICESTER NHS TRUST CARDIAC INVESTIGATIONS PAEDIATRIC & CONGENITAL SYNCOPE INVESTIGATIONS/QUESTIONNAIRE PROTOCOL Written Date: 2009 by Dr Duke, then updated by Dr Sarita Makam 12/4/2016
Clinical Case 1 A patient with a syncope Panos E. Vardas President Elect of the ESC, Prof of Cardiology, University Hospital of Crete
 Clinical Case 1 A patient with a syncope Panos E. Vardas President Elect of the ESC, Prof. of Cardiology, University Hospital of Crete Case presentation A 64-year-old male smoker, with arterial hypertension
Clinical Case 1 A patient with a syncope Panos E. Vardas President Elect of the ESC, Prof. of Cardiology, University Hospital of Crete Case presentation A 64-year-old male smoker, with arterial hypertension
Presentation of transient loss of consciousness
 Presentation of transient loss of consciousness Definition of transient loss of consciousness Transient loss of consciousness: sudden onset, complete loss of consciousness of brief duration with relatively
Presentation of transient loss of consciousness Definition of transient loss of consciousness Transient loss of consciousness: sudden onset, complete loss of consciousness of brief duration with relatively
Syncope Guidelines Update. Bernard Harbieh, FHRS AUBMC-KMC Beirut-Lebanon
 Syncope Guidelines Update Bernard Harbieh, FHRS AUBMC-KMC Beirut-Lebanon New Syncope Guidelines Increase the volume of information on diagnosis and management Incorporation of emergency specialists, neurologists,
Syncope Guidelines Update Bernard Harbieh, FHRS AUBMC-KMC Beirut-Lebanon New Syncope Guidelines Increase the volume of information on diagnosis and management Incorporation of emergency specialists, neurologists,
Diagnostic and therapeutic management of the patient with syncope M. Brignole Arrhythmologic Centre and Syncope Unit Lavagna, Italy
 Diagnostic and therapeutic management of the patient with syncope M. Brignole Arrhythmologic Centre and Syncope Unit Lavagna, Italy Eur Heart J. 2009 Nov;30(21):2631-71 Available on www.escardio.org/guidelines
Diagnostic and therapeutic management of the patient with syncope M. Brignole Arrhythmologic Centre and Syncope Unit Lavagna, Italy Eur Heart J. 2009 Nov;30(21):2631-71 Available on www.escardio.org/guidelines
:{ic0fp'16. Geriatric Medicine: Blood Pressure Monitoring in the Elderly. Terrie Ginsberg, DO, FACOI
 :{ic0fp'16 ACOFP 53 rd Annual Convention & Scientific Seminars Geriatric Medicine: Blood Pressure Monitoring in the Elderly Terrie Ginsberg, DO, FACOI Blood Pressure Management in the Elderly Terrie B.
:{ic0fp'16 ACOFP 53 rd Annual Convention & Scientific Seminars Geriatric Medicine: Blood Pressure Monitoring in the Elderly Terrie Ginsberg, DO, FACOI Blood Pressure Management in the Elderly Terrie B.
SYNCOPE. DEFINITION Syncope is defined as sudden and transient loss of consciousness which is secondary to period of cerebral ischemia CAUSES
 SYNCOPE INTRODUCTION Syncope is a symptom not a disease Syncope is the abrupt and transient loss of consciousness associated with absence of postural tone, followed by complete and usually rapid spontaneous
SYNCOPE INTRODUCTION Syncope is a symptom not a disease Syncope is the abrupt and transient loss of consciousness associated with absence of postural tone, followed by complete and usually rapid spontaneous
Syncope Guidelines What s new? October 19 th 2017 Mohamed Aljaabari MBBCh, FACC, FHRS Consultant Electrophysiologist - Mafraq Hospital
 Syncope Guidelines What s new? October 19 th 2017 Mohamed Aljaabari MBBCh, FACC, FHRS Consultant Electrophysiologist - Mafraq Hospital Case Presentation 35 Male presented with sudden loss of consciousness
Syncope Guidelines What s new? October 19 th 2017 Mohamed Aljaabari MBBCh, FACC, FHRS Consultant Electrophysiologist - Mafraq Hospital Case Presentation 35 Male presented with sudden loss of consciousness
Faculty Disclosure. Sanjay P. Singh, MD, FAAN. Dr. Singh has listed an affiliation with: Consultant Sun Pharma Speaker s Bureau Lundbeck, Sunovion
 Faculty Disclosure Sanjay P. Singh, MD, FAAN Dr. Singh has listed an affiliation with: Consultant Sun Pharma Speaker s Bureau Lundbeck, Sunovion however, no conflict of interest exists for this conference.
Faculty Disclosure Sanjay P. Singh, MD, FAAN Dr. Singh has listed an affiliation with: Consultant Sun Pharma Speaker s Bureau Lundbeck, Sunovion however, no conflict of interest exists for this conference.
Wednesday September 20 th CMT Regional Study Day. Dr Colin Mason, Consultant DME, Addenbrooke s Hospital
 Wednesday September 20 th CMT Regional Study Day Dr Colin Mason, Consultant DME, Addenbrooke s Hospital Develop a structured approach to a patient presenting with a fall Risk stratify who can go home and
Wednesday September 20 th CMT Regional Study Day Dr Colin Mason, Consultant DME, Addenbrooke s Hospital Develop a structured approach to a patient presenting with a fall Risk stratify who can go home and
June 8, 2018, London UK TREATMENT OF VASOVAGAL SYNCOPE
 June 8, 2018, London UK TREATMENT OF VASOVAGAL SYNCOPE Where to go for help Syncope: HRS Definition Syncope is defined as: a transient loss of consciousness, associated with an inability to maintain postural
June 8, 2018, London UK TREATMENT OF VASOVAGAL SYNCOPE Where to go for help Syncope: HRS Definition Syncope is defined as: a transient loss of consciousness, associated with an inability to maintain postural
POSTURAL ORTHOSTATIC TACHYCARDIA SYNDROME (POTS) IT S NOT THAT SIMPLE
 IT S NOT THAT SIMPLE") POSTURAL ORTHOSTATIC TACHYCARDIA SYNDROME (POTS) IT S NOT THAT SIMPLE POTS Irritable heart syndrome. Soldier s heart. Effort syndrome. Vasoregulatory asthenia. Neurocirculatory asthenia. Anxiety neurosis.
POSTURAL ORTHOSTATIC TACHYCARDIA SYNDROME (POTS) IT S NOT THAT SIMPLE POTS Irritable heart syndrome. Soldier s heart. Effort syndrome. Vasoregulatory asthenia. Neurocirculatory asthenia. Anxiety neurosis.
Medicine in the elderly
 Postgrad Med J7 1997; 73: 635-639 ( The Fellowship of Postgraduate Medicine, 1997 Medicine in the elderly Summary Syncope and falls are often considered to be two separate diagnoses with two separate sets
Postgrad Med J7 1997; 73: 635-639 ( The Fellowship of Postgraduate Medicine, 1997 Medicine in the elderly Summary Syncope and falls are often considered to be two separate diagnoses with two separate sets
Vasovagal Syncope and Bradyarrhythmias Mechanisms, distinguishing cause and effect
 Vasovagal Syncope and Bradyarrhythmias Mechanisms, distinguishing cause and effect Walid Saliba, MD, FHRS, FACC Director EP lab Director Atrial Fibrillation Center Department of Cardiovascular Medicine
Vasovagal Syncope and Bradyarrhythmias Mechanisms, distinguishing cause and effect Walid Saliba, MD, FHRS, FACC Director EP lab Director Atrial Fibrillation Center Department of Cardiovascular Medicine
Syncope: Causes and Treatment
 March 01, 2006 By Avery Hayes, MD [1] and Mahendr S. Kochar, MD, MS [2] Because the causes of syncope are numerous and the diagnostic tests have low yield, this disorder is often difficult to evaluate.
March 01, 2006 By Avery Hayes, MD [1] and Mahendr S. Kochar, MD, MS [2] Because the causes of syncope are numerous and the diagnostic tests have low yield, this disorder is often difficult to evaluate.
Il massaggio del seno carotideo Roberto Maggi Centro Aritmologico e Syncope Unit Lavagna, Italia
 Il massaggio del seno carotideo Roberto Maggi Centro Aritmologico e Syncope Unit Lavagna, Italia Tigullio Cardiologia, 7 aprile 2016 Carotid sinus hypersensitivity Vagus nerve Glossopharyngeal nerve Carotid
Il massaggio del seno carotideo Roberto Maggi Centro Aritmologico e Syncope Unit Lavagna, Italia Tigullio Cardiologia, 7 aprile 2016 Carotid sinus hypersensitivity Vagus nerve Glossopharyngeal nerve Carotid
12 Syncope WISHWA N. KAPOOR. Definition
 12 Syncope WISHWA N. KAPOOR Definition Syncope is a sudden transient loss of consciousness associated with loss of postural tone. "Blackout spells," "passing out," or "fainting" are terms occasionally
12 Syncope WISHWA N. KAPOOR Definition Syncope is a sudden transient loss of consciousness associated with loss of postural tone. "Blackout spells," "passing out," or "fainting" are terms occasionally
European Society of Cardiology Task Force Report
 European Society of Cardiology Task Force Report Guidelines on Management (Diagnosis and Treatment) of Syncope Eur Heart J 2001; 22: 1256-1306 European Society of Cardiology Task Force Report Guidelines
European Society of Cardiology Task Force Report Guidelines on Management (Diagnosis and Treatment) of Syncope Eur Heart J 2001; 22: 1256-1306 European Society of Cardiology Task Force Report Guidelines
Autonomic Mediated (Neurocardiogenic) Syncope
 Syncope") Autonomic Mediated (Neurocardiogenic) Syncope Introduction Syncope is brief loss of consciousness causing collapse with spontaneous recovery. Other terms used to describe syncope include blackout, faint,
Autonomic Mediated (Neurocardiogenic) Syncope Introduction Syncope is brief loss of consciousness causing collapse with spontaneous recovery. Other terms used to describe syncope include blackout, faint,
Index. cardiology.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Adenosine in idiopathic AV block, 445 446 Adolescent(s) syncope in, 397 409. See also Syncope, in children and adolescents AECG monitoring.
Index Note: Page numbers of article titles are in boldface type. A Adenosine in idiopathic AV block, 445 446 Adolescent(s) syncope in, 397 409. See also Syncope, in children and adolescents AECG monitoring.
C1: Medical Standards for Safety Critical Workers with Cardiovascular Disorders
 C1: Medical Standards for Safety Critical Workers with Cardiovascular Disorders GENERAL ISSUES REGARDING MEDICAL FITNESS-FOR-DUTY 1. These medical standards apply to Union Pacific Railroad (UPRR) employees
C1: Medical Standards for Safety Critical Workers with Cardiovascular Disorders GENERAL ISSUES REGARDING MEDICAL FITNESS-FOR-DUTY 1. These medical standards apply to Union Pacific Railroad (UPRR) employees
Tilt training EM R1 송진우
 Tilt training 2006.7.15. EM R1 송진우 Introduction North American Vasovagal Pacemaker Study Randomized, controlled trial Reduction in the likelihood of syncope by dual chamber pacing with rate drop response
Tilt training 2006.7.15. EM R1 송진우 Introduction North American Vasovagal Pacemaker Study Randomized, controlled trial Reduction in the likelihood of syncope by dual chamber pacing with rate drop response
Clinical Evaluation & Management of Syncope:UPDATE
 Clinical Evaluation & Management of Syncope:UPDATE 2017 ACC/AHA/HRS Guideline for the Evaluation and Management of Patients With Syncope Developed in Collaboration with the American College of Emergency
Clinical Evaluation & Management of Syncope:UPDATE 2017 ACC/AHA/HRS Guideline for the Evaluation and Management of Patients With Syncope Developed in Collaboration with the American College of Emergency
Emergency Department Guidelines COLLAPSE? CAUSE / SYNCOPE. Version x (x 201x) Review date: x 2014 Page 1 of 5
 Review date: x 2014 Page 1 of 5") COLLAPSE? CAUSE / SYNCOPE Review date: x 2014 Page 1 of 5 KEY POINTS: Do not use this guideline for mechanical falls Definition: Syncope is a transient loss of consciousness with an inability to maintain
COLLAPSE? CAUSE / SYNCOPE Review date: x 2014 Page 1 of 5 KEY POINTS: Do not use this guideline for mechanical falls Definition: Syncope is a transient loss of consciousness with an inability to maintain
Orthostatic instability is an important co-factor and trigger of reflex syncope
 Orthostatic instability is an important co-factor and trigger of reflex syncope Artur Fedorowski 1,2, Philippe Burri 2, Steen Juul-Möller 2, and Olle Melander 1,2 1 Lund University, Sweden 2 Skåne University
Orthostatic instability is an important co-factor and trigger of reflex syncope Artur Fedorowski 1,2, Philippe Burri 2, Steen Juul-Möller 2, and Olle Melander 1,2 1 Lund University, Sweden 2 Skåne University
Difficult Diagnosis: An Interactive Session
 Difficult Diagnosis: An Interactive Session W A D E S M I T H, M. D. D E P T. O F N E U R O L O G Y, U C S F F E B R U A R Y 1 5, 2 0 1 3 58-year-old man with HTN and HLD Recurrent episodes of dizziness
Difficult Diagnosis: An Interactive Session W A D E S M I T H, M. D. D E P T. O F N E U R O L O G Y, U C S F F E B R U A R Y 1 5, 2 0 1 3 58-year-old man with HTN and HLD Recurrent episodes of dizziness
Case Discussion. Date: 2011/03/12 Reporter: FM R1 宋泓逸 Supervisor: F1 許瓅文
 Case Discussion Date: 2011/03/12 Reporter: FM R1 宋泓逸 Supervisor: F1 許瓅文 Discussion Syncope: in the emergency department References Articles from UpToDate, keyword as syncope Harrison s internal medicine,
Case Discussion Date: 2011/03/12 Reporter: FM R1 宋泓逸 Supervisor: F1 許瓅文 Discussion Syncope: in the emergency department References Articles from UpToDate, keyword as syncope Harrison s internal medicine,
Tilt Table Testing. Dr. Prateek Suri
 Tilt Table Testing Dr. Prateek Suri Background Syncope is very commonly seen in the population Among the various causes of syncope vasovagal syncope is the most common cause There is an absence of a gold
Tilt Table Testing Dr. Prateek Suri Background Syncope is very commonly seen in the population Among the various causes of syncope vasovagal syncope is the most common cause There is an absence of a gold
Transient loss of consciousness
 Issue date: August 2010 Transient loss of consciousness Transient loss of consciousness ( blackouts ) management in adults and young people Developed by the National Clinical Guideline Centre Transient
Issue date: August 2010 Transient loss of consciousness Transient loss of consciousness ( blackouts ) management in adults and young people Developed by the National Clinical Guideline Centre Transient
"Non-Epileptic Paroxysmal Events (NEPE) Erick Sell, M.D Neurology Division Children s Hospital of Eastern Ontario
 Erick Sell, M.D Neurology Division Children s Hospital of Eastern Ontario") "Non-Epileptic Paroxysmal Events (NEPE) Erick Sell, M.D Neurology Division Children s Hospital of Eastern Ontario Objectives Learn the clinical presentation of some examples of non-epileptic paroxysmal
"Non-Epileptic Paroxysmal Events (NEPE) Erick Sell, M.D Neurology Division Children s Hospital of Eastern Ontario Objectives Learn the clinical presentation of some examples of non-epileptic paroxysmal
Dizziness, postural hypotension and postural blackouts: Two cases suggesting multiple system atrophy
 Dizziness, postural hypotension and postural blackouts: Two cases suggesting multiple system atrophy Dr Rahul Chakor, Associate Prof and Head Dept of Neurology, Dr Anand Soni, Senior Resident, T N Medical
Dizziness, postural hypotension and postural blackouts: Two cases suggesting multiple system atrophy Dr Rahul Chakor, Associate Prof and Head Dept of Neurology, Dr Anand Soni, Senior Resident, T N Medical
Guidelines Pediatric Congenital Heart Disease SYNCOPE
 Guidelines Pediatric Congenital Heart Disease SYNCOPE www.kinderkardiologie.org/dgpkleitlinien.shtm Definition and Characteristics of Syncope temporary loss of consciousness and tonicity due to inadequate
Guidelines Pediatric Congenital Heart Disease SYNCOPE www.kinderkardiologie.org/dgpkleitlinien.shtm Definition and Characteristics of Syncope temporary loss of consciousness and tonicity due to inadequate
Syncope. A Symptom not a Diagnosis. Vijay Duggirala, MD
 Syncope A Symptom not a Diagnosis Vijay Duggirala, MD Assistant Professor-Clinical Department of Internal Medicine Division of Hospital Medicine The Ohio State University Wexner Medical Center Objectives
Syncope A Symptom not a Diagnosis Vijay Duggirala, MD Assistant Professor-Clinical Department of Internal Medicine Division of Hospital Medicine The Ohio State University Wexner Medical Center Objectives
Syncope and Sudden Death: Back to Titanic. Ric Samson, MD Childrens Heart Center Nevada
 Syncope and Sudden Death: Back to Titanic Ric Samson, MD Childrens Heart Center Nevada The Titanic Syncope vs. Sudden Death The Dilemma syncope sudden death Syncope vs. Sudden Death syncope sudden death
Syncope and Sudden Death: Back to Titanic Ric Samson, MD Childrens Heart Center Nevada The Titanic Syncope vs. Sudden Death The Dilemma syncope sudden death Syncope vs. Sudden Death syncope sudden death
Adult with transient loss of consciousness faints, fits and funny turns
 Adult with transient loss of consciousness faints, fits and funny turns Introduction Problem-specific video guides to diagnosing patients and helping them with management and prevention to transient loss
Adult with transient loss of consciousness faints, fits and funny turns Introduction Problem-specific video guides to diagnosing patients and helping them with management and prevention to transient loss
APPENDIX D1 - CHARACTERISTICS OF INCLUDED STUDIES
 APPENDIX D1 - CHARACTERISTICS OF INCLUDED STUDIES 1 Initial Assessment included studies table... 3 1.1 Initial symptoms for diagnosis review... 3 1.2 Decision rules for diagnosis review... 8 1.3 Initial
APPENDIX D1 - CHARACTERISTICS OF INCLUDED STUDIES 1 Initial Assessment included studies table... 3 1.1 Initial symptoms for diagnosis review... 3 1.2 Decision rules for diagnosis review... 8 1.3 Initial
Syncope evaluation: the role of syncope clinics Michele Brignole Arrhythmologic Centre, Lavagna, Italy
 Syncope evaluation: the role of syncope clinics Michele Brignole Arrhythmologic Centre, Lavagna, Italy Why should we need a Syncope Management Unit? We are not happy with current strategies: - not standardized
Syncope evaluation: the role of syncope clinics Michele Brignole Arrhythmologic Centre, Lavagna, Italy Why should we need a Syncope Management Unit? We are not happy with current strategies: - not standardized
Applying Syncope Guidelines to Clinical Practice
 Applying Syncope Guidelines to Clinical Practice ACC Rockies February 27, 2018 Roopinder K Sandhu Associate Professor of Medicine U of A Director of Edmonton Cardiac Arrhythmia Trials Research Group Visiting
Applying Syncope Guidelines to Clinical Practice ACC Rockies February 27, 2018 Roopinder K Sandhu Associate Professor of Medicine U of A Director of Edmonton Cardiac Arrhythmia Trials Research Group Visiting
13/09/2018. Reflex syncope Diagnosis and treatment. Classification. ficat Reflex (neurally
 Classification TLOC Diagnosis and treatment Jean-Claude Deharo Aix-Marseille Université, France Nontraumatic TLOC Syncope Epileptic seizures TLOC due to head trauma Psychogenic Tonic-clonic seizures Psychogenic
Classification TLOC Diagnosis and treatment Jean-Claude Deharo Aix-Marseille Université, France Nontraumatic TLOC Syncope Epileptic seizures TLOC due to head trauma Psychogenic Tonic-clonic seizures Psychogenic
Syncope. A Symptom not a Diagnosis
 A Symptom not a Diagnosis Vijay Duggirala, MD Assistant Professor-Clinical Department of Internal Medicine Division of Hospital Medicine The Ohio State University Wexner Medical Center Objectives Define
A Symptom not a Diagnosis Vijay Duggirala, MD Assistant Professor-Clinical Department of Internal Medicine Division of Hospital Medicine The Ohio State University Wexner Medical Center Objectives Define
Syncope. Erica Flores, PGY-5
 Syncope Erica Flores, PGY-5 Learning Objectives Recognize the different etiologies of patients presenting with syncope Describe appropriate testing and management of patients presenting with syncope Syncope
Syncope Erica Flores, PGY-5 Learning Objectives Recognize the different etiologies of patients presenting with syncope Describe appropriate testing and management of patients presenting with syncope Syncope
FLORIDA SOUTHERN COLLEGE. Syncope in Athletes. Samantha Sabatino
 Sabatino 1 FLORIDA SOUTHERN COLLEGE Syncope in Athletes Samantha Sabatino 86 Argon Place New Hyde Park, NY 11040 Cell: 516-805-5086 House: 516-248-6631 Email: SSabatino@flsouthern.edu 2010 Winner, Literature
Sabatino 1 FLORIDA SOUTHERN COLLEGE Syncope in Athletes Samantha Sabatino 86 Argon Place New Hyde Park, NY 11040 Cell: 516-805-5086 House: 516-248-6631 Email: SSabatino@flsouthern.edu 2010 Winner, Literature
Syncope (From a Cardiologist s Perspective) Patrick Henderson, DO 118 th OOA Annual Convention Internal Medicine Specialty Track April 28 th, 2018
 Patrick Henderson, DO 118 th OOA Annual Convention Internal Medicine Specialty Track April 28 th, 2018") Syncope (From a Cardiologist s Perspective) Patrick Henderson, DO 118 th OOA Annual Convention Internal Medicine Specialty Track April 28 th, 2018 No financial disclosures to report Goals Formally define
Syncope (From a Cardiologist s Perspective) Patrick Henderson, DO 118 th OOA Annual Convention Internal Medicine Specialty Track April 28 th, 2018 No financial disclosures to report Goals Formally define
2018 ESC SYNCOPE GUIDELINES SUMMARY
 208 ESC SYNCOPE GUIDELINES SUMMARY NEW GUIDELINES OVERVIEW OF UPDATED RECOMMENDATIONS SINCE 2009 208 EUROPEAN SOCIETY OF CARDIOLOGY SYNCOPE GUIDELINES Goals of 208 Task Force Reducing Cost & Admissions:
208 ESC SYNCOPE GUIDELINES SUMMARY NEW GUIDELINES OVERVIEW OF UPDATED RECOMMENDATIONS SINCE 2009 208 EUROPEAN SOCIETY OF CARDIOLOGY SYNCOPE GUIDELINES Goals of 208 Task Force Reducing Cost & Admissions:
Integrated Bone Health and Falls Pathway
 Integrated Bone Health and Falls Pathway Start 1: Presents with a fall 2: Opportunistic case finding 4: Initial falls /osteoporosis screen 3: Health and wellbeing advice Medical problem/ unexplained fall
Integrated Bone Health and Falls Pathway Start 1: Presents with a fall 2: Opportunistic case finding 4: Initial falls /osteoporosis screen 3: Health and wellbeing advice Medical problem/ unexplained fall
Sincopi ricorrenti: diagnosi differenziale e management. Alessandro Proclemer SOC Cardiologia Az. Osp.-Univ. Udine
 Sincopi ricorrenti: diagnosi differenziale e management Alessandro Proclemer SOC Cardiologia Az. Osp.-Univ. Udine DISCLOSURE INFORMATION Dr. Alessandro Proclemer negli ultimi due anni ho avuto i seguenti
Sincopi ricorrenti: diagnosi differenziale e management Alessandro Proclemer SOC Cardiologia Az. Osp.-Univ. Udine DISCLOSURE INFORMATION Dr. Alessandro Proclemer negli ultimi due anni ho avuto i seguenti
2018 ESC Guidelines for the diagnosis and management of syncope
 2018 ESC Guidelines for the diagnosis and management of syncope Michele Brignole (Chairperson) (Italy); Angel Moya (Co-chairperson) (Spain); Jean-Claude Deharo (France); Frederik de Lange (The Netherlands);
2018 ESC Guidelines for the diagnosis and management of syncope Michele Brignole (Chairperson) (Italy); Angel Moya (Co-chairperson) (Spain); Jean-Claude Deharo (France); Frederik de Lange (The Netherlands);
Evaluation of Dizziness and Fainting in Children and Adolescents
 Evaluation of Dizziness and Fainting in Children and Adolescents Collin Cowley, MD - Pediatric Cardiology Lynne Kerr, MD, PhD Pediatric Neurology Chuck Norlin, MD General Pediatrics Bettina Smith Edmondson,
Evaluation of Dizziness and Fainting in Children and Adolescents Collin Cowley, MD - Pediatric Cardiology Lynne Kerr, MD, PhD Pediatric Neurology Chuck Norlin, MD General Pediatrics Bettina Smith Edmondson,
Distinguishing Cardiac from Non- Cardiac Syncope
 10 th Annual International SADS Foundation Conference Toronto Distinguishing Cardiac from Non- Cardiac Syncope Shubhayan Sanatani, MD, FRCPC Head, Division of Cardiology, BC Children s Hospital Director,
10 th Annual International SADS Foundation Conference Toronto Distinguishing Cardiac from Non- Cardiac Syncope Shubhayan Sanatani, MD, FRCPC Head, Division of Cardiology, BC Children s Hospital Director,
Bradycardia and Syncope. P Boon Lim, MB BChir PhD Imperial College Healthcare London, UK
 Bradycardia and Syncope P Boon Lim, MB BChir PhD Imperial College Healthcare London, UK Disclosures Medtronic: Research Grant Boston Scientific: Consulting Fee, Research Grant Biosense Webster: Consulting
Bradycardia and Syncope P Boon Lim, MB BChir PhD Imperial College Healthcare London, UK Disclosures Medtronic: Research Grant Boston Scientific: Consulting Fee, Research Grant Biosense Webster: Consulting
Section Editor Leonard I Ganz, MD, FHRS, FACC
 1 of 12 9/29/2013 6:53 PM Official reprint from UpToDate www.uptodate.com 2013 UpToDate The content on the UpToDate website is not intended nor recommended as a substitute for medical advice, diagnosis,
1 of 12 9/29/2013 6:53 PM Official reprint from UpToDate www.uptodate.com 2013 UpToDate The content on the UpToDate website is not intended nor recommended as a substitute for medical advice, diagnosis,
APPENDIX D1 - CHARACTERISTICS OF INCLUDED STUDIES APPENDIX D1 - CHARACTERISTICS OF INCLUDED STUDIES... 1
 APPENDIX D1 - CHARACTERISTICS OF INCLUDED STUDIES APPENDIX D1 - CHARACTERISTICS OF INCLUDED STUDIES... 1 1 Initial Assessment included studies table... 3 1.1 Initial symptoms for diagnosis review... 3
APPENDIX D1 - CHARACTERISTICS OF INCLUDED STUDIES APPENDIX D1 - CHARACTERISTICS OF INCLUDED STUDIES... 1 1 Initial Assessment included studies table... 3 1.1 Initial symptoms for diagnosis review... 3
Falls Assessment and Medication
 Falls Assessment and Medication Professor T.Masud President-Elect British Geriatrics Society Nottingham University Hospitals NHS Trust, UK Visiting Professor University of Southern Denmark Mrs GH is a
Falls Assessment and Medication Professor T.Masud President-Elect British Geriatrics Society Nottingham University Hospitals NHS Trust, UK Visiting Professor University of Southern Denmark Mrs GH is a
SYNCOPE SYNCOPE 5/1/2013. J. Scott Neumeister M. D. Nebraska Medical Center
 SYNCOPE J. Scott Neumeister M. D. Nebraska Medical Center SYNCOPE Transient loss of consciousness Altered blood flow to the brain Quality Quantity Postural collapse European society of Cardiology. Guidelines
SYNCOPE J. Scott Neumeister M. D. Nebraska Medical Center SYNCOPE Transient loss of consciousness Altered blood flow to the brain Quality Quantity Postural collapse European society of Cardiology. Guidelines
All that blacks out is not syncope: a neurological view of transient loss of consciousness
 All that blacks out is not syncope: a neurological view of transient loss of consciousness Dr Simon Taggart Consultant Clinical Neurophysiologist. JCUH, Middlesbrough. Misdiagnosis of Blackouts Sutula
All that blacks out is not syncope: a neurological view of transient loss of consciousness Dr Simon Taggart Consultant Clinical Neurophysiologist. JCUH, Middlesbrough. Misdiagnosis of Blackouts Sutula
Incidence, Clinical Presentation. and Outcome in Patients with Long. Asystole Induced by Head-up Tilt Test
 2005 16 134-138 Incidence, Clinical Presentation and Outcome in Patients with Long Asystole Induced by Head-up Tilt Test Ming-Ting Chou, Chen-Chuan Cheng, Wen-Shiann Wu, and Tseui-Yuen Huang Division of
2005 16 134-138 Incidence, Clinical Presentation and Outcome in Patients with Long Asystole Induced by Head-up Tilt Test Ming-Ting Chou, Chen-Chuan Cheng, Wen-Shiann Wu, and Tseui-Yuen Huang Division of
By definition, syncope is a
 Approach to the Patient with Syncope: History and Physical Examination Are Key Nora Goldschlager, MD CARDIOLOGY ABSTRACT Syncope, the transient loss of consciousness that occurs due to inadequate cerebral
Approach to the Patient with Syncope: History and Physical Examination Are Key Nora Goldschlager, MD CARDIOLOGY ABSTRACT Syncope, the transient loss of consciousness that occurs due to inadequate cerebral
Cardiology Services Bon Secours Hospital. Mary Buckley Staff Nurse Cardiology
 Cardiology Services Bon Secours Hospital Mary Buckley Staff Nurse Cardiology Overview Philosophy Cardiology Team Referral Criteria Electrocardiograph (ECG) 24/48 Hour Holter Monitor Event Monitors 24 Hour
Cardiology Services Bon Secours Hospital Mary Buckley Staff Nurse Cardiology Overview Philosophy Cardiology Team Referral Criteria Electrocardiograph (ECG) 24/48 Hour Holter Monitor Event Monitors 24 Hour
Systemic Hypertension Dr ahmed almutairi Assistant professor Internal medicine dept
 Systemic Hypertension Dr ahmed almutairi Assistant professor Internal medicine dept Continents 1- introduction 2- classification/definition 3- classification/etiology 4-etiology in both categories 5- complications
Systemic Hypertension Dr ahmed almutairi Assistant professor Internal medicine dept Continents 1- introduction 2- classification/definition 3- classification/etiology 4-etiology in both categories 5- complications
Tilt Table Testing MM /01/2015. HMO; PPO; QUEST Integration 09/22/2017 Section: Medicine Place(s) of Service: Office, Outpatient
 of Service: Office, Outpatient") Tilt Table Testing Policy Number: Original Effective Date: MM.02.024 01/01/2015 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 09/22/2017 Section: Medicine Place(s) of Service:
Tilt Table Testing Policy Number: Original Effective Date: MM.02.024 01/01/2015 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 09/22/2017 Section: Medicine Place(s) of Service:
HEART CONDITIONS IN SPORT
 HEART CONDITIONS IN SPORT Dr. Anita Green CHD Risk Factors Smoking Hyperlipidaemia Hypertension Obesity Physical Inactivity Diabetes Risks are cumulative (multiplicative) Lifestyles predispose to RF One
HEART CONDITIONS IN SPORT Dr. Anita Green CHD Risk Factors Smoking Hyperlipidaemia Hypertension Obesity Physical Inactivity Diabetes Risks are cumulative (multiplicative) Lifestyles predispose to RF One
Management Of Medical Emergencies
 Management Of Medical Emergencies U.S. Aging Population 35 million people (12%) 65 years or older Number will increase by nearly 75% by year 2030 The number of people more than 85 years old will approach
Management Of Medical Emergencies U.S. Aging Population 35 million people (12%) 65 years or older Number will increase by nearly 75% by year 2030 The number of people more than 85 years old will approach
Paediatric Syncope. IAEM Clinical Guideline 10. Version 1 August, Author: Laura Heffernan
 IAEM Clinical Guideline 10 Paediatric Syncope Version 1 August, 2018 Author: Laura Heffernan Guideline lead: Dr Carol Blackburn, in collaboration with the IAEM Guideline Development Committee and Our Lady
IAEM Clinical Guideline 10 Paediatric Syncope Version 1 August, 2018 Author: Laura Heffernan Guideline lead: Dr Carol Blackburn, in collaboration with the IAEM Guideline Development Committee and Our Lady
Hypotensive susceptibility and antihypertensive drugs Diana Solari Santa Margherita Ligure, 7 aprile 2016
 Hypotensive susceptibility and antihypertensive drugs Diana Solari Santa Margherita Ligure, 7 aprile 2016 Arrhythmologic Center, Department of Cardiology, Lavagna SYNCOPE AND ANTIHYPERTENSIVE DRUGS Many
Hypotensive susceptibility and antihypertensive drugs Diana Solari Santa Margherita Ligure, 7 aprile 2016 Arrhythmologic Center, Department of Cardiology, Lavagna SYNCOPE AND ANTIHYPERTENSIVE DRUGS Many
Clinical guideline Published: 25 August 2010 nice.org.uk/guidance/cg109
 Transient loss of consciousness ('blackouts') in over 16s Clinical guideline Published: 25 August 2010 nice.org.uk/guidance/cg109 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Transient loss of consciousness ('blackouts') in over 16s Clinical guideline Published: 25 August 2010 nice.org.uk/guidance/cg109 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Note: At the end of the instructions, you will find a table which must be filled in to complete the exercise.
 Autonomic Nervous System Theoretical foundations and instructions for conducting practical exercises carried out during the course List of practical exercises 1. Deep (controlled) breath test 2. Cold pressor
Autonomic Nervous System Theoretical foundations and instructions for conducting practical exercises carried out during the course List of practical exercises 1. Deep (controlled) breath test 2. Cold pressor
Disclosures. I have no financial disclosures relevant to the talk
 Syncope Sachin S. Sule, MD, FACP Associate Professor of Integrated Medical Science Division of Medicine Director,Internal Medicine Residency Program Charles E. Schmidt College of Medicine, Florida Atlantic
Syncope Sachin S. Sule, MD, FACP Associate Professor of Integrated Medical Science Division of Medicine Director,Internal Medicine Residency Program Charles E. Schmidt College of Medicine, Florida Atlantic
Fainting (Syncope) Information for patients
 Information for patients") Fainting (Syncope) Information for patients 2 This leaflet is provided to help you recognise a simple faint from a more serious condition you might have (such as problems with your heart rhythm) and to
Fainting (Syncope) Information for patients 2 This leaflet is provided to help you recognise a simple faint from a more serious condition you might have (such as problems with your heart rhythm) and to
Le linee guida Sincope 2018 della Società Europea di Cardiologia La Syncope Unit Multidisciplinare. Andrea Ungar, MD, PhD, FESC
 Le linee guida Sincope 2018 della Società Europea di Cardiologia La Syncope Unit Multidisciplinare Andrea Ungar, MD, PhD, FESC Syncope Unit, Hypertension Centre Geriatric and Intensive care Medicine University
Le linee guida Sincope 2018 della Società Europea di Cardiologia La Syncope Unit Multidisciplinare Andrea Ungar, MD, PhD, FESC Syncope Unit, Hypertension Centre Geriatric and Intensive care Medicine University
What are you trying to achieve? Falls Prevention, Assessment and Management Strategies. Falls can be classified into four main groups:
 What are you trying to achieve? Falls Prevention, Assessment and Management Strategies Dr Adam Darowski Community: Falls risk assessment: Falls risk is 50% per year in 80yr population and higher in those
What are you trying to achieve? Falls Prevention, Assessment and Management Strategies Dr Adam Darowski Community: Falls risk assessment: Falls risk is 50% per year in 80yr population and higher in those
Research Article Recurrent Syncope in Patients with Carotid Sinus Hypersensitivity
 International Scholarly Research Network ISRN Cardiology Volume 2012, Article ID 216206, 5 pages doi:10.5402/2012/216206 Research Article Recurrent Syncope in Patients with Carotid Sinus Hypersensitivity
International Scholarly Research Network ISRN Cardiology Volume 2012, Article ID 216206, 5 pages doi:10.5402/2012/216206 Research Article Recurrent Syncope in Patients with Carotid Sinus Hypersensitivity
Management of Arrhythmias The General Practitioners role
 Management of Arrhythmias The General Practitioners role Rohan Gunawardena MD, FRCP, FCCP, FACC Consultant Cardiac Electrophysiologist National Hospital of Sri Lanka Arrhythmias not common Palpitations
Management of Arrhythmias The General Practitioners role Rohan Gunawardena MD, FRCP, FCCP, FACC Consultant Cardiac Electrophysiologist National Hospital of Sri Lanka Arrhythmias not common Palpitations
TLOC - What are the red flags? John Dean March 2018
 TLOC - What are the red flags? John Dean March 2018 What is TLOC? Transient loss of consciousness It is very common It accounts for 5% of ED attendances It accounts for 6% of hospital admissions It consumes
TLOC - What are the red flags? John Dean March 2018 What is TLOC? Transient loss of consciousness It is very common It accounts for 5% of ED attendances It accounts for 6% of hospital admissions It consumes
TAVR : Caring for your patients before and after TAVR
 TAVR : Caring for your patients before and after TAVR Zubair Ahmed MD FSCAI Interventional Cardiologist Washington Regional Medical Center / Walker Heart Institute What is Aortic Valve Stenosis? AVA ~4
TAVR : Caring for your patients before and after TAVR Zubair Ahmed MD FSCAI Interventional Cardiologist Washington Regional Medical Center / Walker Heart Institute What is Aortic Valve Stenosis? AVA ~4
Syncope: diagnosis and management according to the 2009 guidelines of the European Society of Cardiology
 REVIEW ARTICLE Syncope: diagnosis and management according to the 2009 guidelines of the European Society of Cardiology Richard Sutton 1, David Benditt 2, Michele Brignole 3, Angel Moya 4 1 Imperial College,
REVIEW ARTICLE Syncope: diagnosis and management according to the 2009 guidelines of the European Society of Cardiology Richard Sutton 1, David Benditt 2, Michele Brignole 3, Angel Moya 4 1 Imperial College,
Syncope : What tests should I do? Boon Lim Consultant Cardiologist Clinical Lead for Imperial Syncope Unit Hammersmith Hospital
 Syncope : What tests should I do? Boon Lim Consultant Cardiologist Clinical Lead for Imperial Syncope Unit Hammersmith Hospital The most important diagnostic test is History taking Why is history taking
Syncope : What tests should I do? Boon Lim Consultant Cardiologist Clinical Lead for Imperial Syncope Unit Hammersmith Hospital The most important diagnostic test is History taking Why is history taking
European Heart Journal (2001) 22, doi: /euhj , available online at on
 22, doi: /euhj , available online at on") European Heart Journal (2001) 22, 1256 1306 doi:10.1053/euhj.2001.2739, available online at http://www.idealibrary.com on Task Force Report Guidelines on management (diagnosis and treatment) of syncope*
European Heart Journal (2001) 22, 1256 1306 doi:10.1053/euhj.2001.2739, available online at http://www.idealibrary.com on Task Force Report Guidelines on management (diagnosis and treatment) of syncope*
The relevance of a junctional rhythm during neurocardiogenic reaction provoked by tilt testing
 The relevance of a junctional rhythm during neurocardiogenic reaction provoked by tilt testing Dorota Zyśko, Jacek Gajek Wroclaw Medical University, Wroclaw, Poland ESC STOCKHOLM 2010 Junctional rhythm
The relevance of a junctional rhythm during neurocardiogenic reaction provoked by tilt testing Dorota Zyśko, Jacek Gajek Wroclaw Medical University, Wroclaw, Poland ESC STOCKHOLM 2010 Junctional rhythm
NICE Action Plan 6/13 Transient loss of consciousness ('blackouts') management in adults and young people NICE CG 109 December 2013
 management in adults and young people NICE CG 109 December 2013") NICE Action Plan 6/13 Transient loss of consciousness ('blackouts') management in adults and young people NICE CG 109 December 2013 Title: Prepared by: Presented by: Main aim: Recommendations: Previous
NICE Action Plan 6/13 Transient loss of consciousness ('blackouts') management in adults and young people NICE CG 109 December 2013 Title: Prepared by: Presented by: Main aim: Recommendations: Previous
Responses to Changes in Posture QUESTIONS. Case PHYSIOLOGY CASES AND PROBLEMS
 64 PHYSIOLOGY CASES AND PROBLEMS Case 12 Responses to Changes in Posture Joslin Chambers is a 27-year-old assistant manager at a discount department store. One morning, she awakened from a deep sleep and
64 PHYSIOLOGY CASES AND PROBLEMS Case 12 Responses to Changes in Posture Joslin Chambers is a 27-year-old assistant manager at a discount department store. One morning, she awakened from a deep sleep and
13/09/2018. The ISSUE Studies. International (Italy & Spain) Study of Syncope of Uncertain Etiology. ISSUE study Pre-defined inclusion cathegories
 Study of Syncope of Uncertain Etiology. ISSUE study Pre-defined inclusion cathegories") The Studies Jean-Claude Deharo Aix-Marseille Université, France In Cardiac Electrophysiology Methods and Models Editors: Daniel C. Sigg, Paul A. Iaizzo, Yong-Fu Xiao, Bin He Springer 2010 study Pre-defined
The Studies Jean-Claude Deharo Aix-Marseille Université, France In Cardiac Electrophysiology Methods and Models Editors: Daniel C. Sigg, Paul A. Iaizzo, Yong-Fu Xiao, Bin He Springer 2010 study Pre-defined