Moderator: Mitchell L. Schubert, MD, FACG Presenters: Sanjay Bangarulingam, MD and Pritesh Mutha, MD, MPH
|
|
|
- Noah Evans
- 6 years ago
- Views:
Transcription
1 Virginia Commonwealth University Fellow Presentations Moderator: Mitchell L. Schubert, MD, FACG Presenters: Sanjay Bangarulingam, MD and Pit Pritesh hm Mutha, MD, MPH Benign Esophageal Stricture Sanjay Bangarulingam, MD Mitchell Schubert, MD Virginia Commonwealth University McGuire VAMC Richmond, Virginia 1
: LA Grade D esophagitis Esophagram (01/2014): reflux; stricture EGD (02/2014): esophagitis; stricture PEG (02/2014): nausea, vomiting, dysphagia, weight loss")
2 Case 54 year old schizophrenic male with longstanding GERD c/o: Progressive dysphagia for solids and liquids, beginning Jan 2014 Inability to swallow secretions 30 lbs weight loss over 3 months History EGD (2010): LA Grade D esophagitis Esophagram (01/2014): reflux; stricture EGD (02/2014): esophagitis; stricture PEG (02/2014): nausea, vomiting, dysphagia, weight loss 2
3 Past Medical History Paranoid schizophrenia Esophagitis (LA Grade D) n Social History Resides in assisted living i facility. n Smokes 1 ppd X 10 years. n Alcohol abuse Medications Pantoprazole 40 mg bid Calcium 600 mg qd Clonazepam 1 mg Olanzapine 15 mg 3


4 Vitals stable Cachectic Physical Exam Otherwise normal exam with PEG tube in place EGD (April 2014) Unable to pass guidewire for dilation 4





5 Fluoroscopy Esophageal Scope PEG Scope Retrograde Wire 5




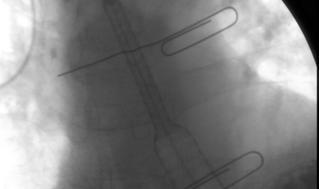


6 TTS Balloon Unable to open stricture Stent Deployment 6






7 Fully Deployed Stent Alimax Fully Covered Metal Stent Stent Removed After 4 Weeks 7


8 Stent Upsized to 18mm Stents for Benign Esophageal Strictures Ideal Stent Characteristics Easily placed Easily retrieved, repositioned, & removed Small-caliber delivery device Minimal shortening on deployment Low migration rates 8
9 Esophageal Stents for Benign Stricture Self Expandable Metal Stents(SEMS): Fully Covered Self Expandable Plastic Stents (SEPS): Biodegradable Stents Self Expanding Plastic Stents SEPS Only FDA approved stent for benign ES Relatively low cost Minimal tissue injury Easily repositionable and retrievable Clinical success: <50% High stent migration rates 9
10 Self Expanding Metal Stents SEMS Increasingly gy used for refractory benign esophageal strictures Not FDA approved No long-term prospective controlled trials Small studies suggest benefit SEP vs FC-SEM vs BDS Prospective 12-week stent treatment trial 32wk f/u patency, migration, relief of dysphagia n = 10 each Canena JM et al BMC Gastroenterol Jun 12;12:70 10

11 FC-SEP vs FC-SEM vs BDS Prospective 12-week study patency, migration, relief of dysphagia n = 10 each Canena JM et al BMC Gastroenterol Jun 12;12:70 FC-SEP vs FC-SEM vs BDS Prospective 12-week study patency, migration, relief of dysphagia n = 10 each FC-SEP FC-SEM BIODEGRAD MIGRATION 60% 30% 20% DYSPHAGIA RESOLVED 10% 40% 30% 11
12 Stents for Benign Esophageal Strictures Indications Refractory/recurrent or Complex stricture Weight Loss Aspiration Pain Decreased quality of life Stents for Benign Esophageal Strictures Complications: Immediate Aspiration Delivery system malfunction Malposition Dislodgement Perforation 12
13 Stents for Benign Esophageal Strictures Complications: Early (<1 wk) Chest pain Nausea Bleeding Stents for Benign Esophageal Strictures Complications: Late Recurrent dysphagia due to food impaction or migration Perforation (T-E fistula) Bleeding GERD (aspiration) 13
14 Conclusion Esophageal stenting is an effective option in refractory benign esophageal strictures Efficacy is modest, at the present time, due to migration and complications; expertise required Although no firm data, FC-SEMS are currently preferred over FC-SEPS due to ease of deployment, decreased migration, and efficacy Virginia Gastroenterology Symposium 2014 Clinical Vignette Pritesh Mutha, MD, MPH Chief Fellow Gastroenterology, Hepatology & Nutrition Virginia Commonwealth University McGuire VAMC 14
15 History 54 y/o AAM w/ PMH of chronic HCV GT1a presents to the ED with one day h/o chest pain, nausea, and vomiting 6 days post-liver biopsy No melena or hematochezia Cardiac enzymes negative. Hgb at baseline (14), lipase nl Discharged home after symptomatic treatment History Patient returns the very next day c/o sharp epigastric pain and is admitted to the hospital No other symptoms 15
16 Past Medical History Perforated duodenal ulcer s/p ex lap: 1995 Cholecystectomy: 2002 Polysubstance abuse Chronic HCV GT1a, treatment-naïve naïve History/Exam Medications Omeprazole Methadone Senna Gabapentin Aspirin Cyclobenzaprine Family history: No GI/liver disease in 1st degree family members Social History: Remote IVDU Tobacco 1ppd Alcohol quit 20 years ago Physical exam: VSS, Icteric No peritoneal/pleuritic signs 16
17 Labs CBC: Hgb 13.9; wbc 4.1; plt 234 LYTES: 135/4.1/96/27; 13/1.2; 138 HEART: Cpk/troponins normal PANCREAS: lipase/amylase normal LIVER: inr 1.0; alb 4.3; ast 151 (baseline 42); alt 208 (baseline 40); ap 221 (baseline 84); TB 4.2 (baseline 0.4) URINE: + methadone Differential diagnosis? 17
18 Differential diagnosis? Exacerbation of viral hepatitis Liver infection (related to biopsy) Bile peritonitis Subcapsular hematoma Intrahepatic bleed Choledocholithiasis (post cholecystectomy) Differential diagnosis? Exacerbation of viral hepatitis Liver infection (related to biopsy) Bile peritonitis Subcapsular hematoma Intrahepatic bleed Choledocholithiasis (post cholecystectomy) 18
19 CT abdomen with contrast New 12 mm lesion in right hepatic lobe Normal pancreas & bile ducts CT abdomen with contrast New 12 mm lesion in right hepatic lobe Normal pancreas & bile ducts Not explain symptoms/labs 19
20 Hospital course The very next day, the epigastric pain worsened and now radiated to the back. In addition, two dark-red red jelly-like like bowel movements. Hgb decreased from Transaminases remained elevated (ast 151, alt 208, Ap 221) Bili increased (direct 4.9) Lipase now elevated to 4500!!! Suspected Diagnosis Hemorrhagic pancreatitis from CBD stone 20
21 Suspected Diagnosis Hemorrhagic pancreatitis from CBD stone Unrelated to liver biopsy Unlikely to cause bloody bowel movements Suspected Diagnosis Hemorrhagic pancreatitis from CBD stone Hemobilia: GI bleeding; clot in CBD causing obstruction and pancreatitis Related to liver biopsy 21
22 Suspected Diagnosis Hemorrhagic pancreatitis from CBD stone Hemobilia: GI bleeding; clot in CBD causing obstruction and pancreatitis Related to liver biopsy What diagnostic test to perform? Day 3: EGD EGD : blood at ampulla 22





23 Day 3: EGD EGD : blood at ampulla What next???? ERCP Blood draining from major papilla No blood cast/ filling defects on balloon sweep of the CBD 23
24 GOOD NEWS: Hospital Course Lipase returned to normal Pain improved BAD NEWS Bleeding continued Hypotensive Hgb drops to 7.6 GOOD NEWS: Hospital Course Lipase returned to normal Pain improved BAD NEWS Bleeding continued Hypotensive Hgb drops to 7.6 WHAT NEXT??? Transfer to MICU Angiography 24



 cannulated")
25 CT Angiogram Pseudoaneurysm right hepatic lobe Mesenteric Arteriogram with Coil Embolization of Pseudoaneursym Right hepatic artery (4 th order branch) cannulated and embolized with microcoils 25
26 Post Embolization Bleeding ceased Discharged 2 days later Hgb 11 ALT 93/AST 72/TB 1.0 Lipase 206 Hemobilia Bleeding into the biliary tree due to abnormal communication between a vessel of the splanchnic circulation and the biliary system May occur days to months after injury to liver Etiology: Trauma; Iatrogenic Curr Gastroenterol Rep 12:121-9,
27 Diagnosis Quincke s triad (22%-37.9%) Upper abdominal pain (52%) Upper gastrointestinal bleed (73%) Jaundice (30%) Br J Surg Jun;88(6): Diagnosis EGD or side-viewing duodenoscopy ERCP MRCP CT hepatic angiography Conventional angiography Am J Gastroenterol 1994, 89:
28 Management Hemodynamic resuscitation Control hemorrhage/treat underlying etiology Angiography Surgery Maintain biliary patency ERCP Hemobilia-induced induced pancreatitis Eleven case reports of hemobilia-induced induced acute pancreatitis following percutaneous liver biopsy Management: Observation ERCP with sphincterotomy (clot in CBD) Surgical removal of blood clot 28
29 CONCLUSION Hemobilia Post Liver Biopsy Should be suspected when patient presents with the classic triad: GI bleeding Biliary/abdominal pain Jaundice Most commonly occurs in a delayed fashion (mean: 5 days) due to gradual erosion of a biopsy- induced hematoma or pseudoaneurysm sm into the bile duct. Diagnosis: EGD; ERCP; MRCP; CT; Angiography Treatment: Conservative Embolization Surgery 29
A patient with an unusual congenital anomaly of the pancreaticobiliary tree
 A patient with an unusual congenital anomaly of the pancreaticobiliary tree Thomas Hocker, HMS IV BIDMC Core Radiology Case Presentation September 17, 2007 Review of Normal Pancreaticobiliary Tract Anatomy
A patient with an unusual congenital anomaly of the pancreaticobiliary tree Thomas Hocker, HMS IV BIDMC Core Radiology Case Presentation September 17, 2007 Review of Normal Pancreaticobiliary Tract Anatomy
Management of Gastroenterology Emergencies Tim Gardner, MD Director, Pancreatic Disorders Section of Gastroenterology and Hepatology
 Management of Gastroenterology Emergencies Tim Gardner, MD Director, Pancreatic Disorders Section of Gastroenterology and Hepatology DHMC CREST Symposium November 7, 2008 There are no financial disclosures
Management of Gastroenterology Emergencies Tim Gardner, MD Director, Pancreatic Disorders Section of Gastroenterology and Hepatology DHMC CREST Symposium November 7, 2008 There are no financial disclosures
Management of Gallbladder Disease
 Management of Gallbladder Disease Steven B. Johnson, MD, FACS, FCCM Professor and Chairman, Department of Surgery Program Director, Phoenix Integrated Surgical Residency University of Arizona College of
Management of Gallbladder Disease Steven B. Johnson, MD, FACS, FCCM Professor and Chairman, Department of Surgery Program Director, Phoenix Integrated Surgical Residency University of Arizona College of
The role of ERCP in chronic pancreatitis
 The role of ERCP in chronic pancreatitis Marianna Arvanitakis Erasme University Hospital, ULB, Brussels, Belgium 10 th Nottingham Endoscopy Masterclass SPEAKER DECLARATIONS This presenter has the following
The role of ERCP in chronic pancreatitis Marianna Arvanitakis Erasme University Hospital, ULB, Brussels, Belgium 10 th Nottingham Endoscopy Masterclass SPEAKER DECLARATIONS This presenter has the following
Does Sphincter of Oddi Dysfunction Even Exist Anymore?
 Does Sphincter of Oddi Dysfunction Even Exist Anymore? Grace H. Elta, MD, FACG Professor of Medicine University of Michigan Sphincter of Oddi Dysfunction Best studied clinical association: Biliary pain
Does Sphincter of Oddi Dysfunction Even Exist Anymore? Grace H. Elta, MD, FACG Professor of Medicine University of Michigan Sphincter of Oddi Dysfunction Best studied clinical association: Biliary pain
ERCP complications and challenges in their diagnosis and management.
 ERCP complications and challenges in their diagnosis and management. Sandie R Thomson Chair of the Division of Gastroenterology, University of Cape Town ERCP Do I have a good Indication? . Algorithm for
ERCP complications and challenges in their diagnosis and management. Sandie R Thomson Chair of the Division of Gastroenterology, University of Cape Town ERCP Do I have a good Indication? . Algorithm for
PANCREATIC PSEUDOCYST DRAINAGE: ENDOSCOPIC APPROACHES & THE NURSING ROLE. PRESENTED BY: Susan DePasquale, CGRN, MSN
 PANCREATIC PSEUDOCYST DRAINAGE: ENDOSCOPIC APPROACHES & THE NURSING ROLE PRESENTED BY: Susan DePasquale, CGRN, MSN Pancreatic Fluid Collection (PFC) A result of pancreatic duct (PD) and side branch disruption,
PANCREATIC PSEUDOCYST DRAINAGE: ENDOSCOPIC APPROACHES & THE NURSING ROLE PRESENTED BY: Susan DePasquale, CGRN, MSN Pancreatic Fluid Collection (PFC) A result of pancreatic duct (PD) and side branch disruption,
Resident Teaching Conference 10/16/09 Rondi Kauffmann Resident presenter William Nealon Faculty presenter
 Resident Teaching Conference 10/16/09 Rondi Kauffmann Resident presenter William Nealon Faculty presenter KC 59 year old male Referred to Surgery clinic for incidentally discovered 5cm x 3cm pancreatic
Resident Teaching Conference 10/16/09 Rondi Kauffmann Resident presenter William Nealon Faculty presenter KC 59 year old male Referred to Surgery clinic for incidentally discovered 5cm x 3cm pancreatic
7/11/2017. We re gonna help a lot of people today. Biliary/Pancreatic Endoscopy. AGS July 1-2, Kenneth M. Sigman, MD
 Biliary/Pancreatic Endoscopy AGS July 1-2, 2017 Kenneth M. Sigman, MD We re gonna help a lot of people today 1 2 3 4 Cannulation It all starts with cannulation Double Wire Cannulation Difficult cannulations
Biliary/Pancreatic Endoscopy AGS July 1-2, 2017 Kenneth M. Sigman, MD We re gonna help a lot of people today 1 2 3 4 Cannulation It all starts with cannulation Double Wire Cannulation Difficult cannulations
Management of Gallbladder Disease. Cory Buschmann, MD PGY-5 11/28/2017
 Management of Gallbladder Disease Cory Buschmann, MD PGY-5 11/28/2017 Financial disclosures None Content Scope of gallbladder diseases Evaluation H&P Labs Imaging Cholecystectomy vs cholecystostomy Ancillary
Management of Gallbladder Disease Cory Buschmann, MD PGY-5 11/28/2017 Financial disclosures None Content Scope of gallbladder diseases Evaluation H&P Labs Imaging Cholecystectomy vs cholecystostomy Ancillary
Correspondence should be addressed to Justin Cochrane;
 Case Reports in Gastrointestinal Medicine Volume 2015, Article ID 794282, 4 pages http://dx.doi.org/10.1155/2015/794282 Case Report Acute on Chronic Pancreatitis Causing a Highway to the Colon with Subsequent
Case Reports in Gastrointestinal Medicine Volume 2015, Article ID 794282, 4 pages http://dx.doi.org/10.1155/2015/794282 Case Report Acute on Chronic Pancreatitis Causing a Highway to the Colon with Subsequent
Stenting for Esophageal Cancer Technical Issues and Outcomes
 Stenting for Esophageal Cancer Technical Issues and Outcomes Moishe Liberman Director C.E.T.O.C. Division of Thoracic Surgery Centre Hospitalier de l Université de Montréal Disclosures Research and Educational
Stenting for Esophageal Cancer Technical Issues and Outcomes Moishe Liberman Director C.E.T.O.C. Division of Thoracic Surgery Centre Hospitalier de l Université de Montréal Disclosures Research and Educational
Case 1- B.N. 66 yr old F with PMHx of breast cancer s/ p mastectomy, HTN, DM presented with dysphagia to solids and liquids.
 Case 1- B.N 66 yr old F with PMHx of breast cancer s/ p mastectomy, HTN, DM presented with dysphagia to solids and liquids. Reports retching to clear esophagus. Case 1- B.N EGD: Stricture in the distal
Case 1- B.N 66 yr old F with PMHx of breast cancer s/ p mastectomy, HTN, DM presented with dysphagia to solids and liquids. Reports retching to clear esophagus. Case 1- B.N EGD: Stricture in the distal
Chapter 32 Gastroenterology General Pathophysiology General Risk Factors for GI emergencies: Excessive Consumption Excessive Smoking Increased
 1 2 3 4 5 6 7 Chapter 32 Gastroenterology General Pathophysiology General Risk Factors for GI emergencies: Excessive Consumption Excessive Smoking Increased Ingestion of Caustic Substances Poor Bowel Habits
1 2 3 4 5 6 7 Chapter 32 Gastroenterology General Pathophysiology General Risk Factors for GI emergencies: Excessive Consumption Excessive Smoking Increased Ingestion of Caustic Substances Poor Bowel Habits
Vascular complications in percutaneous biliary interventions: A series of 111 procedures
 Vascular complications in percutaneous biliary interventions: A series of 111 procedures Poster No.: C-0744 Congress: ECR 2013 Type: Educational Exhibit Authors: A. BHARADWAZ; AARHUS, Re/DK Keywords: Obstruction
Vascular complications in percutaneous biliary interventions: A series of 111 procedures Poster No.: C-0744 Congress: ECR 2013 Type: Educational Exhibit Authors: A. BHARADWAZ; AARHUS, Re/DK Keywords: Obstruction
MAKING CONNECTIONS. Los Angeles Medical Center
 MAKING CONNECTIONS Los Angeles Medical Center Resident: Chris Molloy, MD Fellow: Christian Coroian, MD, MBA Attending: Tina Hardley, MD Program/Dept(s): Los Angeles Medical Center CHIEF COMPLAINT & HPI
MAKING CONNECTIONS Los Angeles Medical Center Resident: Chris Molloy, MD Fellow: Christian Coroian, MD, MBA Attending: Tina Hardley, MD Program/Dept(s): Los Angeles Medical Center CHIEF COMPLAINT & HPI
WallFlex Stents Technique Spotlights
 WallFlex Stents Technique Spotlights OPEN TO THE POSSIBILITIES SEAN E. McGarr, do Kennebec Gastrointestinal Associates Maine General Medical Center, Augusta, ME 04330, United States Director of Gastrointestinal
WallFlex Stents Technique Spotlights OPEN TO THE POSSIBILITIES SEAN E. McGarr, do Kennebec Gastrointestinal Associates Maine General Medical Center, Augusta, ME 04330, United States Director of Gastrointestinal
Principles of ERCP: papilla cannulation, indications/contraindications and risks. Dr. med. Henrik Csaba Horváth PhD
 Principles of ERCP: papilla cannulation, indications/contraindications and risks Dr. med. Henrik Csaba Horváth PhD Evolution of ERCP 1968. 1970s ECPG Endoscopic CholangioPancreatoGraphy Japan 1974 Biliary
Principles of ERCP: papilla cannulation, indications/contraindications and risks Dr. med. Henrik Csaba Horváth PhD Evolution of ERCP 1968. 1970s ECPG Endoscopic CholangioPancreatoGraphy Japan 1974 Biliary
Together, putting patients first
 The Role of a Gastroenterologist in the Diagnosis and Management of Pancreatic Cancer Sarah Jowett, Consultant Gastroenterologist Bradford Teaching Hospitals Trust Leeds Regional Study Day, 12 September
The Role of a Gastroenterologist in the Diagnosis and Management of Pancreatic Cancer Sarah Jowett, Consultant Gastroenterologist Bradford Teaching Hospitals Trust Leeds Regional Study Day, 12 September
Figure 2: Post-cholecystectomy biliary-like pain
 Figure 2: Post-cholecystectomy biliary-like pain 1 patient with recurrent episodes of pain (not daily), in the epigastrium/right upper quadrant, lasting >30 mins, building to a steady level, interrupting
Figure 2: Post-cholecystectomy biliary-like pain 1 patient with recurrent episodes of pain (not daily), in the epigastrium/right upper quadrant, lasting >30 mins, building to a steady level, interrupting
Lutheran Medical Center. Daniel H. Hunt, M.D. June 10 th, 2005
 Lutheran Medical Center Daniel H. Hunt, M.D. June 10 th, 2005 History xx y.o. pt with primary CBD stones s/p ERCP xx months earlier for attempted stone extraction resulting in post ERCP pancreatitis. Patient
Lutheran Medical Center Daniel H. Hunt, M.D. June 10 th, 2005 History xx y.o. pt with primary CBD stones s/p ERCP xx months earlier for attempted stone extraction resulting in post ERCP pancreatitis. Patient
Sreeni Jonnalagadda, MD., FASGE Professor of Medicine, UMKC Director of Interventional Endoscopy Saint Luke s Hospital, Kansas City
 Sreeni Jonnalagadda, MD., FASGE Professor of Medicine, UMKC Director of Interventional Endoscopy Saint Luke s Hospital, Kansas City Peptic stricture Shtki Schatzki s ring Esophageal cancer Radiation therapy
Sreeni Jonnalagadda, MD., FASGE Professor of Medicine, UMKC Director of Interventional Endoscopy Saint Luke s Hospital, Kansas City Peptic stricture Shtki Schatzki s ring Esophageal cancer Radiation therapy
Endoscopic Treatment of Luminal Perforations and Leaks
 Endoscopic Treatment of Luminal Perforations and Leaks Ali A. Siddiqui, MD Professor of Medicine Director of Interventional Endoscopy Jefferson Medical College Philadelphia, PA When Do You Suspect a Luminal
Endoscopic Treatment of Luminal Perforations and Leaks Ali A. Siddiqui, MD Professor of Medicine Director of Interventional Endoscopy Jefferson Medical College Philadelphia, PA When Do You Suspect a Luminal
COPYRIGHTED MATERIAL. 1 Approach to the patient with gross gastrointestinal bleeding. Grace H. Elta, Mimi Takami
 1 Approach to the patient with gross gastrointestinal bleeding Grace H. Elta, Mimi Takami Gastrointestinal (GI) bleeding is a common clinical problem that requires more than 300 000 hospitalizations annually
1 Approach to the patient with gross gastrointestinal bleeding Grace H. Elta, Mimi Takami Gastrointestinal (GI) bleeding is a common clinical problem that requires more than 300 000 hospitalizations annually
The first stents designed for use in the biliary tree and
 Imaging and Advanced Technology Michael B. Wallace, Section Editor Expandable Gastrointestinal Stents TODD H. BARON Department of Medicine, Division of Gastroenterology & Hepatology, Mayo Clinic, Rochester,
Imaging and Advanced Technology Michael B. Wallace, Section Editor Expandable Gastrointestinal Stents TODD H. BARON Department of Medicine, Division of Gastroenterology & Hepatology, Mayo Clinic, Rochester,
Imaging of liver and pancreas
 Imaging of liver and pancreas.. Disease of the liver Focal liver disease Diffusion liver disease Focal liver disease Benign Cyst Abscess Hemangioma FNH Hepatic adenoma HCC Malignant Fibrolamellar carcinoma
Imaging of liver and pancreas.. Disease of the liver Focal liver disease Diffusion liver disease Focal liver disease Benign Cyst Abscess Hemangioma FNH Hepatic adenoma HCC Malignant Fibrolamellar carcinoma
Primary Sclerosing Cholangitis and Cholestatic liver diseases. Ahsan M Bhatti MD, FACP Bhatti Gastroenterology Consultants
 Primary Sclerosing Cholangitis and Cholestatic liver diseases Ahsan M Bhatti MD, FACP Bhatti Gastroenterology Consultants I have nothing to disclose Educational Objectives What is PSC? Understand the cholestatic
Primary Sclerosing Cholangitis and Cholestatic liver diseases Ahsan M Bhatti MD, FACP Bhatti Gastroenterology Consultants I have nothing to disclose Educational Objectives What is PSC? Understand the cholestatic
Original Policy Date 12:2013
 MP 6.01.30 Magnetic Resonance Cholangiopancreatography Medical Policy Section Radiology Is12:2013sue 3:2005 Original Policy Date 12:2013 Last Review Status/Date 12:2013 Return to Medical Policy Index Disclaimer
MP 6.01.30 Magnetic Resonance Cholangiopancreatography Medical Policy Section Radiology Is12:2013sue 3:2005 Original Policy Date 12:2013 Last Review Status/Date 12:2013 Return to Medical Policy Index Disclaimer
ERCP and EUS: What s New and What Should We Do?
 ERCP and EUS: What s New and What Should We Do? Rajesh N. Keswani, MD Associate Professor of Medicine Division of Gastroenterology Northwestern University Feinberg School of Medicine EUS/ERCP in 2015 THE
ERCP and EUS: What s New and What Should We Do? Rajesh N. Keswani, MD Associate Professor of Medicine Division of Gastroenterology Northwestern University Feinberg School of Medicine EUS/ERCP in 2015 THE
Evaluation and Management of Refractory Biliary Stricture. J. David Horwhat, MD, FACG Director of Endoscopy Lancaster Gastroenterology, Inc.
 Evaluation and Management of Refractory Biliary Stricture J. David Horwhat, MD, FACG Director of Endoscopy Lancaster Gastroenterology, Inc Outline What defines a refractory biliary stricture Endoscopic
Evaluation and Management of Refractory Biliary Stricture J. David Horwhat, MD, FACG Director of Endoscopy Lancaster Gastroenterology, Inc Outline What defines a refractory biliary stricture Endoscopic
GASTROENTEROLOGY ESSENTIALS
 GASTROENTEROLOGY ESSENTIALS Practical Gastroenterology 8/25/2018 Jahnavi Koppala, MBBS Abdullah Abdussalam, MD A 48-year-old male was evaluated for noncardiac chest pain. Treatment with PPI twice daily
GASTROENTEROLOGY ESSENTIALS Practical Gastroenterology 8/25/2018 Jahnavi Koppala, MBBS Abdullah Abdussalam, MD A 48-year-old male was evaluated for noncardiac chest pain. Treatment with PPI twice daily
ACG Clinical Guideline: Management of Acute Pancreatitis
 ACG Clinical Guideline: Management of Acute Pancreatitis Scott Tenner, MD, MPH, FACG 1, John Baillie, MB, ChB, FRCP, FACG 2, John DeWitt, MD, FACG 3 and Santhi Swaroop Vege, MD, FACG 4 1 State University
ACG Clinical Guideline: Management of Acute Pancreatitis Scott Tenner, MD, MPH, FACG 1, John Baillie, MB, ChB, FRCP, FACG 2, John DeWitt, MD, FACG 3 and Santhi Swaroop Vege, MD, FACG 4 1 State University
Delayed Severe Hemobilia after Endoscopic Biliary Plastic Stent Insertion
 CASE REPORT Clin Endosc 2016;49:303-307 http://dx.doi.org/10.5946/ce.2015.081 Print ISSN 2234-2400 On-line ISSN 2234-2443 Open Access Delayed Severe Hemobilia after Endoscopic Biliary Plastic Stent Insertion
CASE REPORT Clin Endosc 2016;49:303-307 http://dx.doi.org/10.5946/ce.2015.081 Print ISSN 2234-2400 On-line ISSN 2234-2443 Open Access Delayed Severe Hemobilia after Endoscopic Biliary Plastic Stent Insertion
Douglas G. Adler MD. ACG Regional Postgraduate Course - Nashville, TN Copyright 2013 American College of Gastroenterology
 Enteral Stents 2013: State of the Art Douglas G. Adler MD Associate Professor of Medicine Director of Therapeutic Endoscopy University of Utah School of Medicine Huntsman Cancer Center Esophageal Stents
Enteral Stents 2013: State of the Art Douglas G. Adler MD Associate Professor of Medicine Director of Therapeutic Endoscopy University of Utah School of Medicine Huntsman Cancer Center Esophageal Stents
Tools of the Gastroenterologist: Introduction to GI Endoscopy
 Tools of the Gastroenterologist: Introduction to GI Endoscopy Objectives Endoscopy Upper endoscopy Colonoscopy Endoscopic retrograde cholangiopancreatography (ERCP) Endoscopic ultrasound (EUS) Endoscopic
Tools of the Gastroenterologist: Introduction to GI Endoscopy Objectives Endoscopy Upper endoscopy Colonoscopy Endoscopic retrograde cholangiopancreatography (ERCP) Endoscopic ultrasound (EUS) Endoscopic
Lahey Clinic Internal Medicine Residency Program: Curriculum for Gastroenterology
 Lahey Clinic Internal Medicine Residency Program: Curriculum for Gastroenterology Faculty representative: David L. Burns, MD, CNSP Resident representative: Tom Castiglione, MD Revision date: March 6, 2006
Lahey Clinic Internal Medicine Residency Program: Curriculum for Gastroenterology Faculty representative: David L. Burns, MD, CNSP Resident representative: Tom Castiglione, MD Revision date: March 6, 2006
Making ERCP Easy: Tips From A Master
 Making ERCP Easy: Tips From A Master Raj J. Shah, M.D., FASGE Associate Professor of Medicine University of Colorado School of Medicine Co-Director, Endoscopy Director, Pancreaticobiliary Endoscopy Services
Making ERCP Easy: Tips From A Master Raj J. Shah, M.D., FASGE Associate Professor of Medicine University of Colorado School of Medicine Co-Director, Endoscopy Director, Pancreaticobiliary Endoscopy Services
The campaign on laboratory: focus on Gallstone Disease and ERCP
 The campaign on laboratory: focus on Gallstone Disease and ERCP Mauro Giuliani, MD, Specialist in Visceral Surgery, Vice Head Physician, Surgical Ward, Ospedale Regionale di Locarno Alberto Fasoli, MD,
The campaign on laboratory: focus on Gallstone Disease and ERCP Mauro Giuliani, MD, Specialist in Visceral Surgery, Vice Head Physician, Surgical Ward, Ospedale Regionale di Locarno Alberto Fasoli, MD,
Definitive Surgical Treatment When Endoscopy Fails. Erik Peltz D.O. Resident Debate February 26 th 2007 University of Colorado Dept.
 Nonvariceal Gastrointestinal Hemorrhage: Definitive Surgical Treatment When Endoscopy Fails Erik Peltz D.O. Resident Debate February 26 th 2007 University of Colorado Dept. Surgery Non-Variceal Upper GI
Nonvariceal Gastrointestinal Hemorrhage: Definitive Surgical Treatment When Endoscopy Fails Erik Peltz D.O. Resident Debate February 26 th 2007 University of Colorado Dept. Surgery Non-Variceal Upper GI
ACUTE CHOLANGITIS AS a result of an occluded
 Digestive Endoscopy 2017; 29 (Suppl. 2): 88 93 doi: 10.1111/den.12836 Current status of biliary drainage strategy for acute cholangitis Endoscopic treatment for acute cholangitis with common bile duct
Digestive Endoscopy 2017; 29 (Suppl. 2): 88 93 doi: 10.1111/den.12836 Current status of biliary drainage strategy for acute cholangitis Endoscopic treatment for acute cholangitis with common bile duct
Abdominal Pain. Luke Donnelly, MD Emergency Medicine
 Abdominal Pain Luke Donnelly, MD Emergency Medicine Objectives Approach to abdominal pain Evaluation Critical diagnoses and treatments Abdominal Pain Most Common ER Complaint Broad Differential Can often
Abdominal Pain Luke Donnelly, MD Emergency Medicine Objectives Approach to abdominal pain Evaluation Critical diagnoses and treatments Abdominal Pain Most Common ER Complaint Broad Differential Can often
Long Term Follow-up. 6 Month 1 Year Annual enter year #: What is the assessment date: / / Unknown. Is the patient alive? Yes No
 Long Term Follow-up 6 Month 1 Year Annual enter year #: What is the assessment date: / / Unknown Is the patient alive? Yes No Was an exam performed by a bariatric physician or PA/NP? Yes No Was the patient
Long Term Follow-up 6 Month 1 Year Annual enter year #: What is the assessment date: / / Unknown Is the patient alive? Yes No Was an exam performed by a bariatric physician or PA/NP? Yes No Was the patient
Overview. Doumit S. BouHaidar, MD ACG/VGS/ODSGNA Regional Postgraduate Course Copyright American College of Gastroenterology 1
 Doumit S. BouHaidar, MD Associate Professor of Medicine Director, Advanced Therapeutic Endoscopy Virginia Commonwealth University Overview Copyright American College of Gastroenterology 1 Incidence: 4
Doumit S. BouHaidar, MD Associate Professor of Medicine Director, Advanced Therapeutic Endoscopy Virginia Commonwealth University Overview Copyright American College of Gastroenterology 1 Incidence: 4
ESPEN Congress Brussels Stenting of the esophagus and small bowel. Jean-Marc Dumonceau
 ESPEN Congress Brussels 2005 Stenting of the esophagus and small bowel Jean-Marc Dumonceau Stenting of the esophagus and small bowel Jean-Marc Dumonceau, Div. of Gastroenterology Geneva, Switzerland Indication:
ESPEN Congress Brussels 2005 Stenting of the esophagus and small bowel Jean-Marc Dumonceau Stenting of the esophagus and small bowel Jean-Marc Dumonceau, Div. of Gastroenterology Geneva, Switzerland Indication:
ERCP / PTC Surgical Laparoscopic vs open Timing and order of approach
 Choledocholithiasis Which Approach and When? Lygia Stewart, MD University of California, San Francisco 2010 Naffziger Post-Graduate Course Clinical Manifestations of Choledocholithiasis Asymptomatic (no
Choledocholithiasis Which Approach and When? Lygia Stewart, MD University of California, San Francisco 2010 Naffziger Post-Graduate Course Clinical Manifestations of Choledocholithiasis Asymptomatic (no
Expandable stents in digestive pathology present use in an emergency hospital
 ORIGINAL ARTICLES Article received on November30, 2015 and accepted for publishing on December15, 2015. Expandable stents in digestive pathology present use in an emergency hospital Mădălina Ilie 1, Vasile
ORIGINAL ARTICLES Article received on November30, 2015 and accepted for publishing on December15, 2015. Expandable stents in digestive pathology present use in an emergency hospital Mădălina Ilie 1, Vasile
Visceral Artery Aneurysms Endovascular vs. Open?
 Disclosures Visceral Artery Aneurysms Endovascular vs. Open? John S. Lane III, MD Professor and Acting Chief of Vascular Surgery UC San Diego, Department of Surgery None relevant UCSF Vascular Symposium,
Disclosures Visceral Artery Aneurysms Endovascular vs. Open? John S. Lane III, MD Professor and Acting Chief of Vascular Surgery UC San Diego, Department of Surgery None relevant UCSF Vascular Symposium,
Surgical Management of Chronic Pancreatitis VERENA LIU, MD KINGS COUNTY HOSPITAL CENTER SURGERY GRAND ROUNDS 4/1/2013
 Surgical Management of Chronic Pancreatitis VERENA LIU, MD KINGS COUNTY HOSPITAL CENTER SURGERY GRAND ROUNDS 4/1/2013 Case Report 42F with h/o chronic pancreatitis due to alcohol use with chronic upper
Surgical Management of Chronic Pancreatitis VERENA LIU, MD KINGS COUNTY HOSPITAL CENTER SURGERY GRAND ROUNDS 4/1/2013 Case Report 42F with h/o chronic pancreatitis due to alcohol use with chronic upper
Navigating the Biliary Tract with CT & MR: An Imaging Approach to Bile Duct Obstruction
 Navigating the Biliary Tract with CT & MR: An Imaging Approach to Bile Duct Obstruction Ann S. Fulcher, MD Medical College of Virginia Virginia Commonwealth University Richmond, Virginia Objectives To
Navigating the Biliary Tract with CT & MR: An Imaging Approach to Bile Duct Obstruction Ann S. Fulcher, MD Medical College of Virginia Virginia Commonwealth University Richmond, Virginia Objectives To
Jaundice. Agnieszka Dobrowolska- Zachwieja, MD, PhD
 Jaundice Agnieszka Dobrowolska- Zachwieja, MD, PhD Jaundice definition Jaundice, as in the French jaune, refers to the yellow discoloration of the skin. It arises from the abnormal accumulation of bilirubin
Jaundice Agnieszka Dobrowolska- Zachwieja, MD, PhD Jaundice definition Jaundice, as in the French jaune, refers to the yellow discoloration of the skin. It arises from the abnormal accumulation of bilirubin
Cholangiocarcinoma: Radiologic evaluation and interventions
 November 2014 Cholangiocarcinoma: Radiologic evaluation and interventions Colin Nevins, Harvard Medical School Year III Agenda Initial course and work-up Endoscopic retrograde cholangiopancreatography
November 2014 Cholangiocarcinoma: Radiologic evaluation and interventions Colin Nevins, Harvard Medical School Year III Agenda Initial course and work-up Endoscopic retrograde cholangiopancreatography
Slide 1. Slide 2. Slide 3 Pancreatic Cancer- Case #1. Endoscopic management of GI malignancy. Endoscopic approaches in GI malignancy- Agenda
 Slide 1 A teaching hospital of Harvard Medical School Endoscopic management of GI malignancy Tyler Berzin MD, MS Center for Advanced Endoscopy Division of Gastroenterology Beth Israel Deaconess Medical
Slide 1 A teaching hospital of Harvard Medical School Endoscopic management of GI malignancy Tyler Berzin MD, MS Center for Advanced Endoscopy Division of Gastroenterology Beth Israel Deaconess Medical
WallFlex Biliary RX Fully Covered Stent System Prescriptive Information
 Caution/Rx Only: Federal Law (USA) restricts this device to sale by or on the order of a physician. Warning Contents supplied STERILE using an ethylene oxide (EO) process. Do not use if sterile barrier
Caution/Rx Only: Federal Law (USA) restricts this device to sale by or on the order of a physician. Warning Contents supplied STERILE using an ethylene oxide (EO) process. Do not use if sterile barrier
Perforation of a Duodenal Diverticulum. Elective Student S. C.
 Perforation of a Duodenal Diverticulum 2008 4 Elective Student S. C. Case History An elderly male presented to the Emergency Department with abdominal pain. Chief Complaint: Worsening, diffuse abdominal
Perforation of a Duodenal Diverticulum 2008 4 Elective Student S. C. Case History An elderly male presented to the Emergency Department with abdominal pain. Chief Complaint: Worsening, diffuse abdominal
PANCREATIC PSEUDOCYSTS. Madhuri Rao MD PGY-5 Kings County Hospital Center
 PANCREATIC PSEUDOCYSTS Madhuri Rao MD PGY-5 Kings County Hospital Center 34 yo M Case Presentation PMH: Chronic pancreatitis (ETOH related) PSH: Nil Meds: Nil NKDA www.downstatesurgery.org Symptoms o Chronic
PANCREATIC PSEUDOCYSTS Madhuri Rao MD PGY-5 Kings County Hospital Center 34 yo M Case Presentation PMH: Chronic pancreatitis (ETOH related) PSH: Nil Meds: Nil NKDA www.downstatesurgery.org Symptoms o Chronic
Approach to the Biliary Stricture
 Approach to the Biliary Stricture ACG Eastern Postgraduate Course Washington DC June 8, 2014 Steven A. Edmundowicz MD FASGE Chief of Endoscopy Division of Gastroenterology Professor of Medicine Disclosures
Approach to the Biliary Stricture ACG Eastern Postgraduate Course Washington DC June 8, 2014 Steven A. Edmundowicz MD FASGE Chief of Endoscopy Division of Gastroenterology Professor of Medicine Disclosures
Managing Complications of Bariatric Surgery. Objectives
 Managing Complications of Bariatric Surgery John J. Vargo, II, MD, MPH, FACG Chair, Department of Gastroenterology and Hepatology Digestive Disease and Surgery Institute Cleveland Clinic Cleveland, OH
Managing Complications of Bariatric Surgery John J. Vargo, II, MD, MPH, FACG Chair, Department of Gastroenterology and Hepatology Digestive Disease and Surgery Institute Cleveland Clinic Cleveland, OH
Morning Report. Allison Haden, MD October 1, 2002
 Morning Report Allison Haden, MD October 1, 2002 68 yo WM with N/V and abdominal pain Became ill about 2 weeks ago, per pt. intermittent nausea: worse w/eating vomiting within 30min of eating, nonbilious,
Morning Report Allison Haden, MD October 1, 2002 68 yo WM with N/V and abdominal pain Became ill about 2 weeks ago, per pt. intermittent nausea: worse w/eating vomiting within 30min of eating, nonbilious,
Endoscopic Management of the Iatrogenic CBD Injury
 The Liver Week 2014, Jeju, Korea Endoscopic Management of the Iatrogenic CBD Injury Jong Ho Moon, MD, PhD Department of Internal Medicine Soon Chun Hyang University School of Medicine Bucheon/Seoul, KOREA
The Liver Week 2014, Jeju, Korea Endoscopic Management of the Iatrogenic CBD Injury Jong Ho Moon, MD, PhD Department of Internal Medicine Soon Chun Hyang University School of Medicine Bucheon/Seoul, KOREA
What can you expect after your ERCP?
 ERCP Explained and respond to bed rest, pain relief and fasting to rest the gut with the patient needing to stay in hospital for only a few days. Some patients develop severe pancreatitis and may require
ERCP Explained and respond to bed rest, pain relief and fasting to rest the gut with the patient needing to stay in hospital for only a few days. Some patients develop severe pancreatitis and may require
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A ACLF. See Acute-on-chronic liver failure (ACLF) Acute kidney injury (AKI) in ACLF patients, 967 Acute liver failure (ALF), 957 964 causes
Index Note: Page numbers of article titles are in boldface type. A ACLF. See Acute-on-chronic liver failure (ACLF) Acute kidney injury (AKI) in ACLF patients, 967 Acute liver failure (ALF), 957 964 causes
Sphincter of Oddi dysfunction: SOD after EPISOD, Now what do we do?
 Sphincter of Oddi dysfunction: SOD after EPISOD, Now what do we do? Priya A. Jamidar, M.D., FASGE Professor of Medicine, Director of Endoscopy Yale School Y A L E S CH OO L O F MEDIC IN E February in Connecticut
Sphincter of Oddi dysfunction: SOD after EPISOD, Now what do we do? Priya A. Jamidar, M.D., FASGE Professor of Medicine, Director of Endoscopy Yale School Y A L E S CH OO L O F MEDIC IN E February in Connecticut
Management of biliary injury after laparoscopic cholecystectomy N. Dayes Kings County Hospital Center & Long Island College Hospital 8/19/2010
 Management of biliary injury after laparoscopic cholecystectomy N. Dayes Kings County Hospital Center & Long Island College Hospital 8/19/2010 Case Presentation 30 y.o. woman with 2 weeks of RUQ abdominal
Management of biliary injury after laparoscopic cholecystectomy N. Dayes Kings County Hospital Center & Long Island College Hospital 8/19/2010 Case Presentation 30 y.o. woman with 2 weeks of RUQ abdominal
A Guide for Patients Living with a Biliary Metal Stent
 A Guide for Patients Living with a Biliary Metal Stent What is a biliary metal stent? A biliary metal stent (also known as a bile duct stent ) is a flexible metallic tube specially designed to hold your
A Guide for Patients Living with a Biliary Metal Stent What is a biliary metal stent? A biliary metal stent (also known as a bile duct stent ) is a flexible metallic tube specially designed to hold your
Visceral aneurysm. Diagnosis and Interventions M.NEDEVSKA
 Visceral aneurysm Diagnosis and Interventions M.NEDEVSKA History 1953 De Bakeyand Cooley Visceral aneurysm VAAs rare, reported incidence of 0.01 to 0.2% on routine autopsies. Clinically important Potentially
Visceral aneurysm Diagnosis and Interventions M.NEDEVSKA History 1953 De Bakeyand Cooley Visceral aneurysm VAAs rare, reported incidence of 0.01 to 0.2% on routine autopsies. Clinically important Potentially
A tale of two LAMS: a report of benign tissue ingrowth resulting in recurrent gastric outlet obstruction
 A tale of two LAMS: a report of benign tissue ingrowth resulting in recurrent gastric outlet obstruction Authors Parth J. Parekh, Mohammad H. Shakhatreh, Paul Yeaton Institution Department of Internal
A tale of two LAMS: a report of benign tissue ingrowth resulting in recurrent gastric outlet obstruction Authors Parth J. Parekh, Mohammad H. Shakhatreh, Paul Yeaton Institution Department of Internal
Gary M. Annunziata, D.O., F.A.C.P. / Anh T. Duong, M.D. / Jonathan C. Lin, M.D., MPH Phone- (760) Fax- (760) Preparation for ERCP
 Fax- (760) Preparation for ERCP") Gary M. Annunziata, D.O., F.A.C.P. / Anh T. Duong, M.D. / Jonathan C. Lin, M.D., MPH Phone- (760) 321-2500 Fax- (760) 321-5720 Preparation for ERCP Patient Name- Procedure Date and Time- Please do not
Gary M. Annunziata, D.O., F.A.C.P. / Anh T. Duong, M.D. / Jonathan C. Lin, M.D., MPH Phone- (760) 321-2500 Fax- (760) 321-5720 Preparation for ERCP Patient Name- Procedure Date and Time- Please do not
Pictorial review of Benign Biliary tract abnormality on MRCP/MRI Liver with Endoscopic (including splyglass) and Endoscopic Ultrasound correlation
 and Endoscopic Ultrasound correlation") Pictorial review of Benign Biliary tract abnormality on MRCP/MRI Liver with Endoscopic (including splyglass) and Endoscopic Ultrasound correlation Poster No.: C-2617 Congress: ECR 2015 Type: Educational
Pictorial review of Benign Biliary tract abnormality on MRCP/MRI Liver with Endoscopic (including splyglass) and Endoscopic Ultrasound correlation Poster No.: C-2617 Congress: ECR 2015 Type: Educational
THE CRITICAL COMPLCATIONS AND MANAGEMENTS AFTER PANCREATIC SURGERY 2013/12/21
 THE CRITICAL COMPLCATIONS AND MANAGEMENTS AFTER PANCREATIC SURGERY Tsann-Long Hwang, MD, FACS Department of Surgery Chang Gung Memorial Hospital Chang Gung University Taipei, TAIWAN 2013/12/21 THE DIFFICULTY
THE CRITICAL COMPLCATIONS AND MANAGEMENTS AFTER PANCREATIC SURGERY Tsann-Long Hwang, MD, FACS Department of Surgery Chang Gung Memorial Hospital Chang Gung University Taipei, TAIWAN 2013/12/21 THE DIFFICULTY
Lumen Apposing Metal Stents: Expanding the Role of the Interventional Endoscopist. Alireza Sedarat, MD UCLA Division of Digestive Diseases
 Lumen Apposing Metal Stents: Expanding the Role of the Interventional Endoscopist Alireza Sedarat, MD UCLA Division of Digestive Diseases Disclosures Consultant for Boston Scientific and Olympus Corporation
Lumen Apposing Metal Stents: Expanding the Role of the Interventional Endoscopist Alireza Sedarat, MD UCLA Division of Digestive Diseases Disclosures Consultant for Boston Scientific and Olympus Corporation
Afternoon Session Cases
 Afternoon Session Cases Case 1 19 year old woman Presented with abdominal pain to community hospital Mild incr WBC a14, 000, Hg normal, lipase 100 (normal to 75) US 5.2 x 3.7 x 4 cm mass in porta hepatis
Afternoon Session Cases Case 1 19 year old woman Presented with abdominal pain to community hospital Mild incr WBC a14, 000, Hg normal, lipase 100 (normal to 75) US 5.2 x 3.7 x 4 cm mass in porta hepatis
AN UNCOMMON CAUSE OF MASSIVE HEMATURIA
 Originally Posted: August, 01, 2014 AN UNCOMMON CAUSE OF MASSIVE HEMATURIA Resident(s): Monzer Chehab, MD, Alexander Copelan MD Attending(s): Purushottam Dixit, MD Program/Dept(s): Oakland University William
Originally Posted: August, 01, 2014 AN UNCOMMON CAUSE OF MASSIVE HEMATURIA Resident(s): Monzer Chehab, MD, Alexander Copelan MD Attending(s): Purushottam Dixit, MD Program/Dept(s): Oakland University William
An unusual source of right upper quadrant pain
 Originally Posted: Month, 00, 20xx An unusual source of right upper quadrant pain Resident(s): Ashish R. Vyas MD (PGY-V), Dominic T. Semaan M.D., J.D. (PGY-V) Attending(s): Dr. Denis Lincoln Program/Dept(s):
Originally Posted: Month, 00, 20xx An unusual source of right upper quadrant pain Resident(s): Ashish R. Vyas MD (PGY-V), Dominic T. Semaan M.D., J.D. (PGY-V) Attending(s): Dr. Denis Lincoln Program/Dept(s):
A rare cause of upper gastrointestinal bleeding: Posttraumatic pseudoaneurysm
 www.edoriumjournals.com Case Report open ACCESS A rare cause of upper gastrointestinal bleeding: Posttraumatic pseudoaneurysm Negi RC, Brij Sharma, Bhupender, Gaurav Kapoor, Bal Beer Verma, Ashok Sharma
www.edoriumjournals.com Case Report open ACCESS A rare cause of upper gastrointestinal bleeding: Posttraumatic pseudoaneurysm Negi RC, Brij Sharma, Bhupender, Gaurav Kapoor, Bal Beer Verma, Ashok Sharma
Disclosures. Extra-hepatic Biliary Disease and the Pancreas. Objectives. Pancreatitis 10/3/2018. No relevant financial disclosures to report
 Extra-hepatic Biliary Disease and the Pancreas Disclosures No relevant financial disclosures to report Jeffrey Coughenour MD FACS Clinical Associate Professor of Surgery and Emergency Medicine Division
Extra-hepatic Biliary Disease and the Pancreas Disclosures No relevant financial disclosures to report Jeffrey Coughenour MD FACS Clinical Associate Professor of Surgery and Emergency Medicine Division
SUNY Downstate Medical Center Kings County Hospital
 Management of Choledocholithiasis SUNY Downstate Medical Center Kings County Hospital Department of Surgery Grand Rounds Kiyanda Baldwin October 22, 2009 Case Presentation 43 y/o F c/o jaundice x 3 days
Management of Choledocholithiasis SUNY Downstate Medical Center Kings County Hospital Department of Surgery Grand Rounds Kiyanda Baldwin October 22, 2009 Case Presentation 43 y/o F c/o jaundice x 3 days
STRICTURES OF THE BILE DUCTS Session No.: 5. Andrea Tringali Digestive Endoscopy Unit Catholic University Rome - Italy
 STRICTURES OF THE BILE DUCTS Session No.: 5 Andrea Tringali Digestive Endoscopy Unit Catholic University Rome - Italy Drainage of biliary strictures. The history before 1980 Surgical bypass Percutaneous
STRICTURES OF THE BILE DUCTS Session No.: 5 Andrea Tringali Digestive Endoscopy Unit Catholic University Rome - Italy Drainage of biliary strictures. The history before 1980 Surgical bypass Percutaneous
Case Scenario 1. Discharge Summary
 Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
Background. RUQ Ultrasound Normal, Recommend Clinical Correlation. Sohail R. Shah, MD, MSHA, FACS, FAAP Texas Children s Hosptial
 RUQ Ultrasound Normal, Recommend Clinical Correlation Sohail R. Shah, MD, MSHA, FACS, FAAP Texas Children s Hosptial Background Incidence of pediatric gallbladder disease continues to rise U.S. Pediatric
RUQ Ultrasound Normal, Recommend Clinical Correlation Sohail R. Shah, MD, MSHA, FACS, FAAP Texas Children s Hosptial Background Incidence of pediatric gallbladder disease continues to rise U.S. Pediatric
Radiological Tests: Which One is Most Appropriate for My Patient?
 Radiological Tests: Which One is Most Appropriate for My Patient? Robert Hartman, M.D. 2016 MFMER slide-1 Disclosures No Disclosures 2016 MFMER slide-2 Objectives Discuss tools to aid in the ordering of
Radiological Tests: Which One is Most Appropriate for My Patient? Robert Hartman, M.D. 2016 MFMER slide-1 Disclosures No Disclosures 2016 MFMER slide-2 Objectives Discuss tools to aid in the ordering of
Trimming of a Broken Migrated Biliary Metal Stent with the Nd:YAG Laser
 16 Trimming of a Broken Migrated Biliary Metal Stent with the Nd:YAG Laser I. Zuber-Jerger F. Kullmann Department of Internal Medicine I, University of Regensburg, Regensburg, Germany Key Words Broken
16 Trimming of a Broken Migrated Biliary Metal Stent with the Nd:YAG Laser I. Zuber-Jerger F. Kullmann Department of Internal Medicine I, University of Regensburg, Regensburg, Germany Key Words Broken
Owen Dickinson. Consultant in Endoscopy & Interventional Radiology. Upper GI Stenting. Rotherham Foundation Trust
 Owen Dickinson Consultant in Endoscopy & Interventional Radiology Upper GI Stenting Rotherham Foundation Trust Owen Dickinson Consultant in Endoscopy & Interventional Radiology Rotherham Foundation Trust
Owen Dickinson Consultant in Endoscopy & Interventional Radiology Upper GI Stenting Rotherham Foundation Trust Owen Dickinson Consultant in Endoscopy & Interventional Radiology Rotherham Foundation Trust
Disclosures. Overview. Case 1. Common Bile Duct Sizes 10/14/2016. General GI + Advanced Endoscopy: NAFLD/Stones/Pancreatitis
 Disclosures General GI + Advanced Endoscopy: NAFLD/Stones/Pancreatitis 123 Blank Blank, LLC Aldo Maspons, MD Assistant Professor Director of Endoscopy Department of Pediatrics Texas Tech University Health
Disclosures General GI + Advanced Endoscopy: NAFLD/Stones/Pancreatitis 123 Blank Blank, LLC Aldo Maspons, MD Assistant Professor Director of Endoscopy Department of Pediatrics Texas Tech University Health
Chapter 14: Training in Radiology. DDSEP Chapter 1: Question 12
 DDSEP Chapter 1: Question 12 A 52-year-old white male presents for evaluation of sudden onset of abdominal pain and shoulder pain. His past medical history is notable for a history of coronary artery disease,
DDSEP Chapter 1: Question 12 A 52-year-old white male presents for evaluation of sudden onset of abdominal pain and shoulder pain. His past medical history is notable for a history of coronary artery disease,
Cholangiocarcinoma (Bile Duct Cancer)
") Cholangiocarcinoma (Bile Duct Cancer) The Bile Duct System (Biliary Tract) A network of bile ducts (tubes) connects the liver and the gallbladder to the small intestine. This network begins in the liver
Cholangiocarcinoma (Bile Duct Cancer) The Bile Duct System (Biliary Tract) A network of bile ducts (tubes) connects the liver and the gallbladder to the small intestine. This network begins in the liver
INVESTIGATIONS OF GASTROINTESTINAL DISEAS
 INVESTIGATIONS OF GASTROINTESTINAL DISEAS Lecture 1 and 2 دز اسماعيل داود فرع الطب كلية طب الموصل Radiological tests of structure (imaging) Plain X-ray: May shows soft tissue outlines like liver, spleen,
INVESTIGATIONS OF GASTROINTESTINAL DISEAS Lecture 1 and 2 دز اسماعيل داود فرع الطب كلية طب الموصل Radiological tests of structure (imaging) Plain X-ray: May shows soft tissue outlines like liver, spleen,
Discharge Summary-Page 1
 Discharge Summary-Page 1 Admission diagnosis: 1. Gastritis. 2. Alcoholic cirrhosis, ascites, grade 1 esophageal varices. 3. Recent left knee arthroplasty. 4. Osteoporosis naqmq : 1. Three chest X-rays
Discharge Summary-Page 1 Admission diagnosis: 1. Gastritis. 2. Alcoholic cirrhosis, ascites, grade 1 esophageal varices. 3. Recent left knee arthroplasty. 4. Osteoporosis naqmq : 1. Three chest X-rays
Percutaneous Transarterial Embolization of Pseudoaneurysm Secondary to Pancreatitis: a case report
 Chin J Radiol 2003; 28: 347-351 347 Percutaneous Transarterial Embolization of Pseudoaneurysm Secondary to Pancreatitis: a case report HSIN-YI LAI YUNG-FANG CHEN HSEIN-JAR CHIANG WU-CHUNG SHEN Department
Chin J Radiol 2003; 28: 347-351 347 Percutaneous Transarterial Embolization of Pseudoaneurysm Secondary to Pancreatitis: a case report HSIN-YI LAI YUNG-FANG CHEN HSEIN-JAR CHIANG WU-CHUNG SHEN Department
General'Surgery'Service'
 General'Surgery'Service' Patient Care Goals and Objectives 1)! Stomach/Duodenum and Bariatric 2)! Interpret the results of clinical evaluations (history, physical examination) performed on patients being
General'Surgery'Service' Patient Care Goals and Objectives 1)! Stomach/Duodenum and Bariatric 2)! Interpret the results of clinical evaluations (history, physical examination) performed on patients being
ENDOSCOPIC TREATMENT OF A BILE DUCT
 HPB Surgery, 1990, Vol. 3, pp. 67-71 Reprints available directly from the publisher Photocopying permitted by license only 1990 Harwood Academic Publishers GmbH Printed in the United Kingdom CASE REPORT
HPB Surgery, 1990, Vol. 3, pp. 67-71 Reprints available directly from the publisher Photocopying permitted by license only 1990 Harwood Academic Publishers GmbH Printed in the United Kingdom CASE REPORT
Gastrointestinal Emergencies CEN REVIEW 2017 MARY RALEY, BSN, RN, CEN, TCRN, TNSCC
 Gastrointestinal Emergencies CEN REVIEW 2017 MARY RALEY, BSN, RN, CEN, TCRN, TNSCC Gastrointestinal Emergencies is 7% of the CEN A. Acute abdomen B. Bleeding C. Cholecystitis D. Cirrhosis E. Diverticulitis
Gastrointestinal Emergencies CEN REVIEW 2017 MARY RALEY, BSN, RN, CEN, TCRN, TNSCC Gastrointestinal Emergencies is 7% of the CEN A. Acute abdomen B. Bleeding C. Cholecystitis D. Cirrhosis E. Diverticulitis
The Bile Duct (and Pancreas) and the Physician
 and the Physician") The Bile Duct (and Pancreas) and the Physician Javaid Iqbal Consultant in Gastroenterology and Pancreato-biliary Medicine University Hospital South Manchester Not so common?! Two weeks 38 ERCP s 20 15
The Bile Duct (and Pancreas) and the Physician Javaid Iqbal Consultant in Gastroenterology and Pancreato-biliary Medicine University Hospital South Manchester Not so common?! Two weeks 38 ERCP s 20 15
Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds
 Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds Imaging in jaundice and 2ww pathway Image protocol Staging Limitations Pancreatic cancer 1.2.4 Refer people using a suspected
Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds Imaging in jaundice and 2ww pathway Image protocol Staging Limitations Pancreatic cancer 1.2.4 Refer people using a suspected
CHIEF COMPLAINT & HPI
 THE GREAT HOUDINI Resident: Marc Lim, MD Attending: Shekher Maddineni, MD Program/Department: Westchester Medical Center/New York Medical College/Department of Radiology CHIEF COMPLAINT & HPI Chief Complaint
THE GREAT HOUDINI Resident: Marc Lim, MD Attending: Shekher Maddineni, MD Program/Department: Westchester Medical Center/New York Medical College/Department of Radiology CHIEF COMPLAINT & HPI Chief Complaint
Pancreatic Benign April 27, 2016
 Department of Surgery Pancreatic Benign April 27, 2016 James Choi Dr. Hernandez Objectives Medical Expert: 1. Anatomy and congenital anomalies of the pancreas and pancreatic duct (divisum, annular pancreas
Department of Surgery Pancreatic Benign April 27, 2016 James Choi Dr. Hernandez Objectives Medical Expert: 1. Anatomy and congenital anomalies of the pancreas and pancreatic duct (divisum, annular pancreas
Case Report Post-ERCP multiple bleeding and related treatment. a decompensated cirrhotic patient with choledocholithiasis
 Int J Clin Exp Med 2018;11(8):8699-8703 www.ijcem.com /ISSN:1940-5901/IJCEM0068746 Case Report in a decompensated cirrhotic patient with choledocholithiasis: a case report Zhongcheng Zhou, Jing Chen, Faming
Int J Clin Exp Med 2018;11(8):8699-8703 www.ijcem.com /ISSN:1940-5901/IJCEM0068746 Case Report in a decompensated cirrhotic patient with choledocholithiasis: a case report Zhongcheng Zhou, Jing Chen, Faming
A CASE REPORT OF SPONTANEOUS BILOMA - AN ENIGMATIC SURGICAL PROBLEM
 A CASE REPORT OF SPONTANEOUS BILOMA - AN ENIGMATIC SURGICAL PROBLEM *Sumanta Kumar Ghosh and Biswajit Mukherjee ESIC Medical College, Joka, Kolkata, India *Author for Correspondence ABSTRACT Occurrence
A CASE REPORT OF SPONTANEOUS BILOMA - AN ENIGMATIC SURGICAL PROBLEM *Sumanta Kumar Ghosh and Biswajit Mukherjee ESIC Medical College, Joka, Kolkata, India *Author for Correspondence ABSTRACT Occurrence
GENERAL SURGERY FOR SMART PEOPLE JOE NOLD MD, FACS WICHITA SURGICAL SPECIALISTS
 GENERAL SURGERY FOR SMART PEOPLE JOE NOLD MD, FACS WICHITA SURGICAL SPECIALISTS CONFLICTS/DECLARATIONS I have no financial conflicts or declarations I AM always willing to see a consult for you TEXT TOPICS
GENERAL SURGERY FOR SMART PEOPLE JOE NOLD MD, FACS WICHITA SURGICAL SPECIALISTS CONFLICTS/DECLARATIONS I have no financial conflicts or declarations I AM always willing to see a consult for you TEXT TOPICS
A Review of Liver Function Tests. James Gray Gastroenterology Vancouver
 A Review of Liver Function Tests James Gray Gastroenterology Vancouver Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
A Review of Liver Function Tests James Gray Gastroenterology Vancouver Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
Last Revised: September 15 Last Reviewed: September EOSINOPHILIC ESOPHAGITIS (EOE)/PPI-RESPONSIVE ESOPHAGEAL EOSINOPHILIA (PPI-REE)
/PPI-RESPONSIVE ESOPHAGEAL EOSINOPHILIA (PPI-REE)") 7.0 GASTROENTEROLOGY Last Revised: September 5 Last Reviewed: September 5 7. EOSINOPHILIC ESOPHAGITIS (EOE)/PPI-RESPONSIVE ESOPHAGEAL EOSINOPHILIA (PPI-REE) Significant changes: ) Addition of PPI-REE as
7.0 GASTROENTEROLOGY Last Revised: September 5 Last Reviewed: September 5 7. EOSINOPHILIC ESOPHAGITIS (EOE)/PPI-RESPONSIVE ESOPHAGEAL EOSINOPHILIA (PPI-REE) Significant changes: ) Addition of PPI-REE as