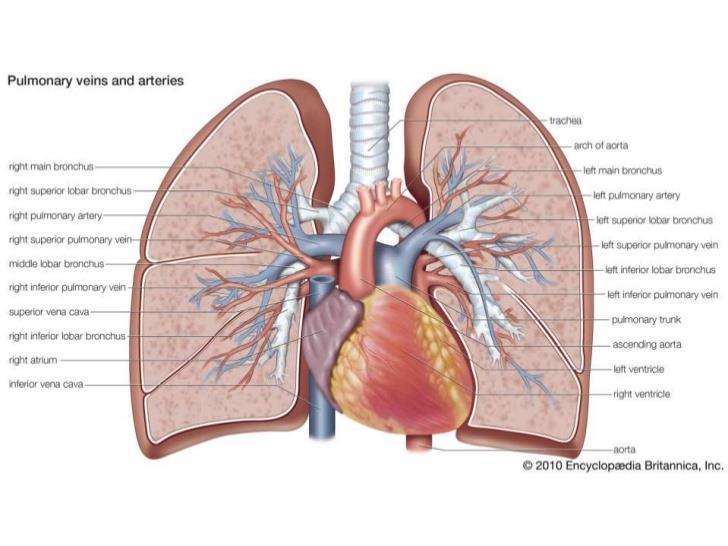
Pulmonary embolism - the great masquerader
|
|
|
- Jewel George
- 6 years ago
- Views:
Transcription

1 Pulmonary embolism - the great masquerader V.N. Karazin Kharkov National University Department of Internal Medicine Associate professor Makharynska О.S., MD, PhD 2016
2
 that breaks off and migrates to the lung, a process termed venous thromboembolism (VTE).")
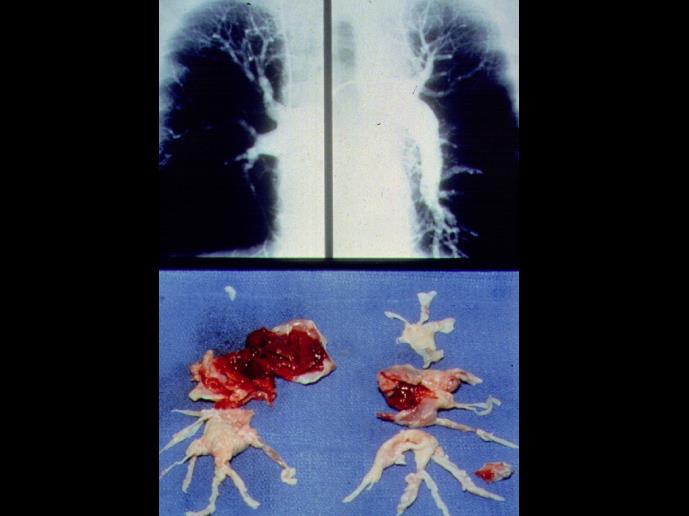
3 Pulmonary embolism (PE) is a blockage of the main artery of the lung or one of its branches by a substance that has travelled from elsewhere in the body through the bloodstream (embolism). PE most commonly results from deep vein thrombosis (a blood clot in the deep veins of the legs or pelvis) that breaks off and migrates to the lung, a process termed venous thromboembolism (VTE).

4
 despite normal systemic arterial pressure.")
5 CLASSIFICATION OF PULMONARY EMBOLISM Massive PE accounts for 5-10% of cases Submassive PE accounts for 20-25% of patients Low-risk constitutes about 70-75% of cases dyspnea, syncope, hypotension, cyanosis RV dysfunction (right heart failure) despite normal systemic arterial pressure. CLASSIFICATION OF PULMONARY EMBOLISM Acute situated centrally within the vascular lumen or if it occludes a vessel (vessel cut - off sign) Chronic it is eccentric and contiguous with the vessel wall, it reduces the arterial diameter by more than 50%, evidence of recanalization within the thrombus is present, and an arterial web is present. Central main pulmonary artery, the left and right main pulmonary arteries, the anterior trunk, the right and left interlobar arteries, the left upper lobe trunk, the right middle lobe artery, and the right and left lower lobe arteries Peripheral segmental and subsegmental arteries of the right upper lobe, the right middle lobe, the right lower lobe, the left upper lobe, the lingula, and the left lower lobe Management-of
6

 Central")

 Acute medical illness (AIDS (lupus anticoagulant),")

7 Predisposing factors of Venous stasis PULMONARY EMBOLISM Hypercoagulable states Immobilization Surgery and trauma Pregnancy Oral contraceptives and estrogen replacement Malignancy Warfarin (first few days of therapy) Central venous instrumentation - past 3 months Hereditary factors (Protein C deficiency, factor V Leiden, plasminogen activator abnormality etc.) Acute medical illness (AIDS (lupus anticoagulant), Behçet disease, myocardial infarction, systemic lupus erythematosus, polycythemia, ulcerative colitis etc.)

8 Virchow
9
10



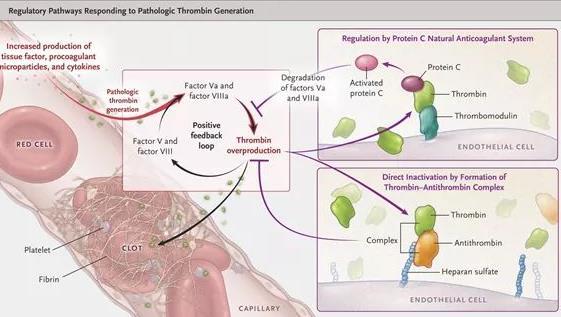
11 PULMONARY EMBOLISM: Pathophysiology N thrombus embolus ESC Guidelines 2014
 http://www.escardio.")
12 PULMONARY EMBOLISM: clinical picture Abrupt onset of pleuritic chest pain Shortness of breath Hypoxia Seizures Syncope Abdominal pain Fever Productive cough Wheezing Decreasing level of consciousness New onset of atrial fibrillation Hemoptysis Flank pain Delirium (in elderly patients) ESC Guidelines 2014
 -")

 - 43% Diaphoresis - 36% S 3 or S 4")


13 PULMONARY EMBOLISM: Physical Examination Physical signs: Tachypnea (RR>16/min) - 96% Rales - 58% Accentuated second heart sound - 53% Tachycardia (heart rate >100/min) - 44% Fever (temperature >37.8 C) - 43% Diaphoresis - 36% S 3 or S 4 gallop - 34% Clinical signs and symptoms of thrombophlebitis - 32% Lower extremity edema - 24% Cardiac murmur - 23% Cyanosis - 19%
14 PULMONARY EMBOLISM: Physical Examination may be grouped into 4 categories as follows: Massive pulmonary infarction Acute pulmonary infarction Acute embolism without infarction Multiple pulmonary emboli or thrombi


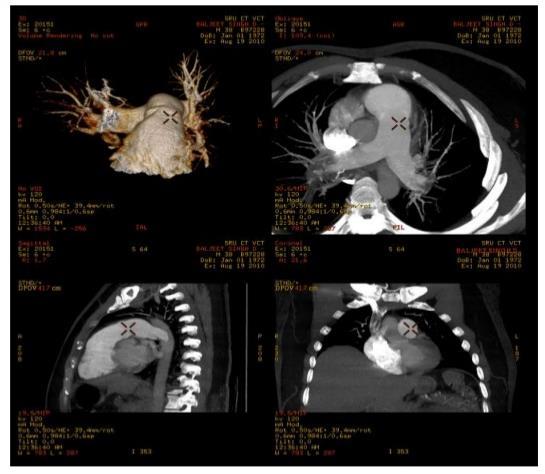
15 PULMONARY EMBOLISM: massive heart thrombus thrombus thrombus heart


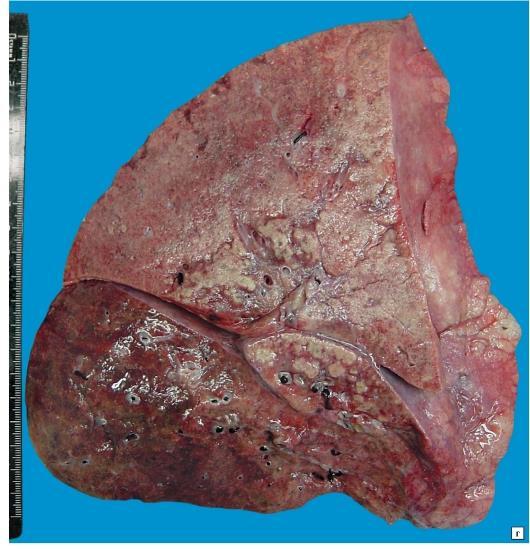
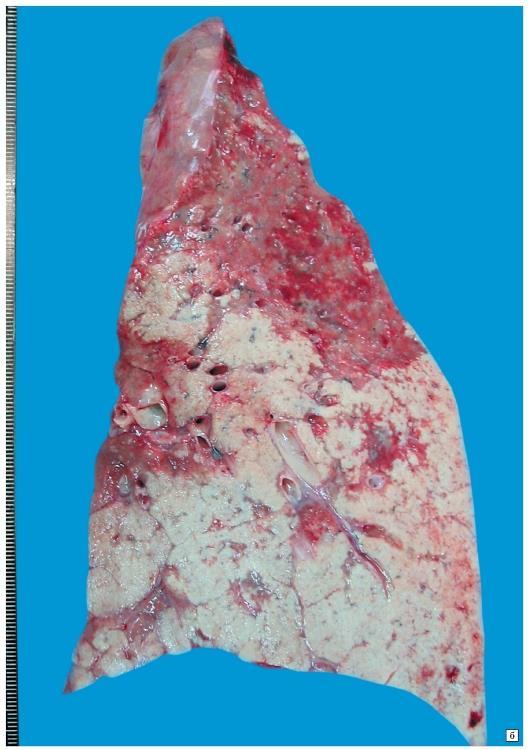
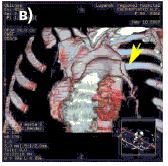
16 PULMONARY EMBOLISM: acute pulmonary infarction thrombus Lung infarction

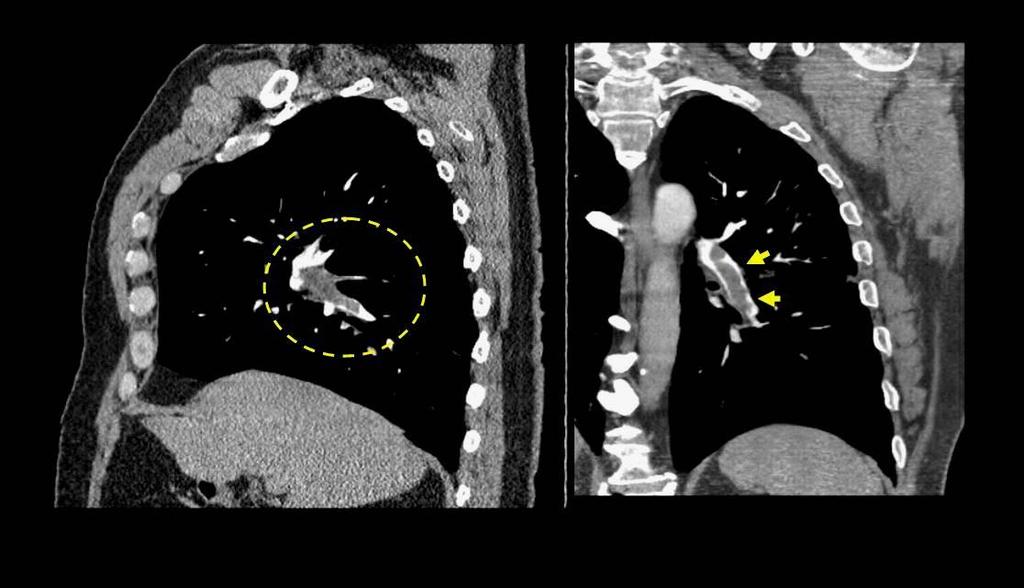
17 PULMONARY EMBOLISM: acute embolism without infarction
 as was suspected by clinical observations.")
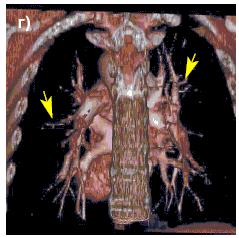
18 PULMONARY EMBOLISM: multiple pulmonary emboli or thrombi These two coronal CT images are of the same patient who presented with dyspnea, chest pain, and mild core pulmonale. The chest CT angiogram reveals multiple PE (arrows) as was suspected by clinical observations. Pulmonary emboli were found in several secondary, tertiary, and distal branches of the pulmonary arteries.
 and the American College of Physicians (ACP)")
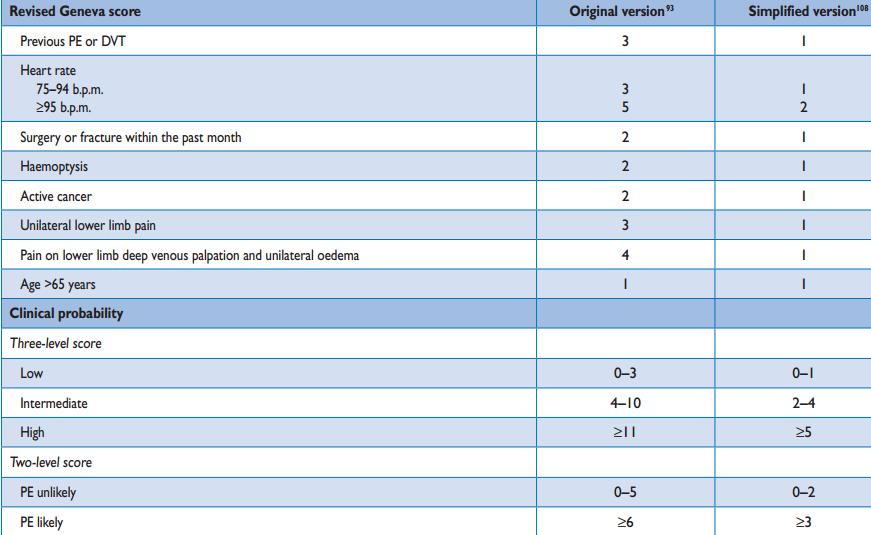
19 PULMONARY EMBOLISM: Assessment of clinical probability American Academy of Family Physicians (AAFP) and the American College of Physicians (ACP) (Canadian Pulmonary Embolism Score)



20 PULMONARY EMBOLISM: D-dimer testing D-dimer testing is most reliable for excluding pulmonary embolism in younger patients who have no associated comorbidity or history of venous thromboembolism and whose symptoms are of short duration it is of questionable value in patients who are older than 80 years, who are hospitalized, who have cancer, or who are pregnant, because nonspecific elevation of D-dimer concentrations is common in such patients D-dimer testing should not be used when the clinical probability of pulmonary embolism is high
21 Potentially useful laboratory tests in patients with suspected pulmonary embolism include: D-dimer testing Ischemia-modified albumin level White blood cell count Arterial blood gases Markers of myocardial injury - serum troponin and liptin levels Markers of right ventricular dysfunction - brain natriuretic peptide
22 Laboratory tests and biomarkers Markers of right ventricular dysfunction In normotensive patients with PE, the positive predictive value of elevated BNP or NT-proBNP concentrations for early mortality is low. Haemodynamically stable patients with low NT-proBNP levels may be candidates for early discharge and outpatient treatment Markers of myocardial injury Elevated plasma troponin concentrations on admission have been reported in connection with PE and were associated with worse prognosis (troponin T concentrations >14 pg/ml). Elevated serum creatinine levels and a decreased (calculated) glomerular filtration rate are related to 30-day allcause mortality in acute PE.



23 Imaging studies that aid in the diagnosis of pulmonary embolism




24 PULMONARY EMBOLISM: computed tomographic pulmonary angiography is the initial imaging modality of choice for stable patients with suspected pulmonary embolism.
 The")
 segmental perfusion defects without corresponding ventilation or radiographic abnormalities Four moderate segmental perfusion defects without corresponding")
25 PULMONARY EMBOLISM: Lung scintigraphy with multiple tracers such as xenon-133 gas, Tc-99m-labelled aerosols, or Tc-99m-labelled carbon microparticles (Technegas) The high-probability criteria are as follows: Two large (>75% of a segment) segmental perfusion defects without corresponding ventilation or chest radiographic abnormalities One large segmental perfusion defect and 2 moderate (25-75% of a segment) segmental perfusion defects without corresponding ventilation or radiographic abnormalities Four moderate segmental perfusion defects without corresponding ventilation or chest radiographic abnormalities The intermediate-probability criteria are as follows: One moderate to fewer than 2 large segmental perfusion defects without corresponding ventilation or chest radiographic abnormalities Corresponding V/Q defects and radiographic parenchymal opacity in lower lung zone Single moderate matched V/Q defects with normal chest radiographic findings Corresponding V/Q and chest radiography small pleural effusion Difficult to categorize as normal, low, or high probability



26



27 PULMONARY EMBOLISM: pulmonary angiography This angiograph is a localization image that shows placement of the pigtail catheter in the pulmonary artery for selective angiography. The radiograph on the left is the positive image and on the right the negative image. On the right is a magnified portion of the radiograph showing a large filling defect in a branch of the pulmonary artery, which is a pulmonary embolus (arrows). This patient presented with ah clinical history of chest pain, advanced peripheral vascular disease, diabetic, smoker, and hypertension.
28 PULMONARY EMBOLISM: magnetic resonance angiography Magnetic resonance angiography is performed following intravenous administration of gadolinium. Emboli in the left and right main pulmonary arteries Embolus in the left main pulmonary artery А large pulmonary embolus in the left main branch of the pulmonary artery

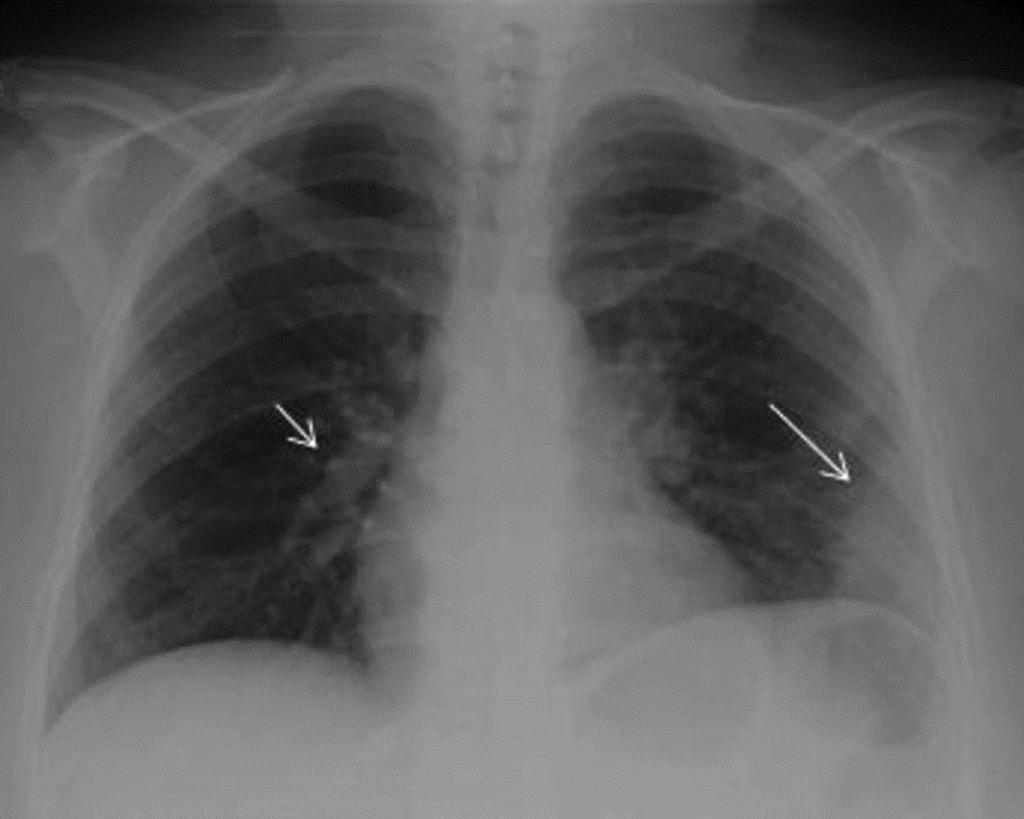

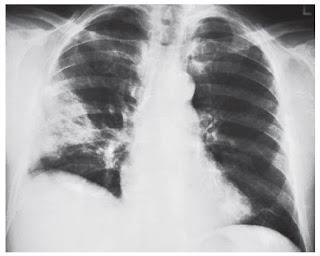
29 PULMONARY EMBOLISM: X- ray thrombus Palla s sign Hampton hump

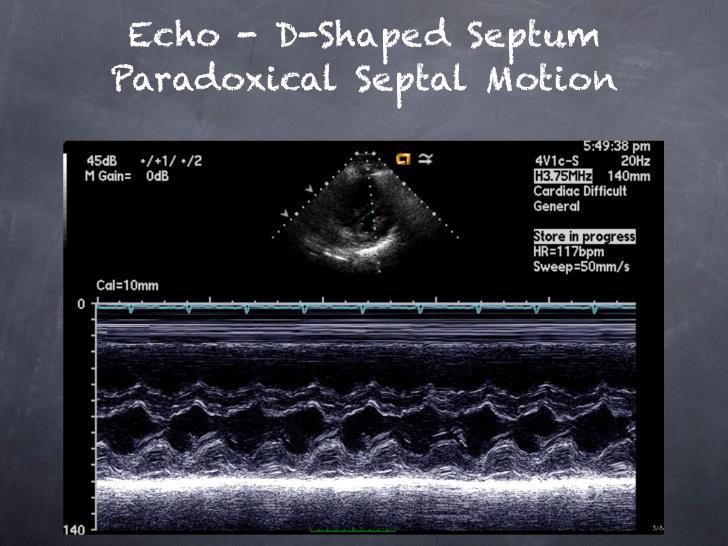
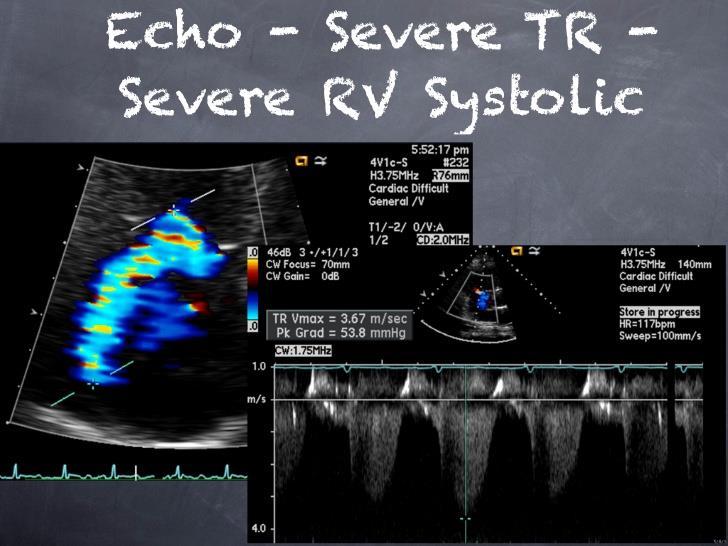
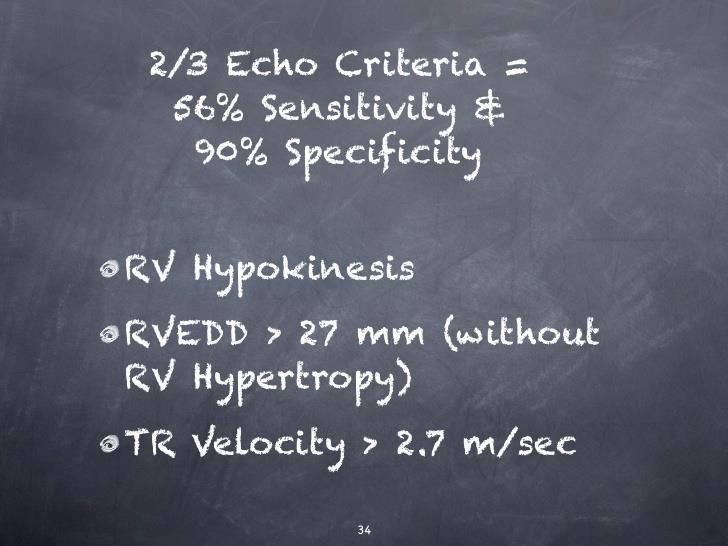
30 PULMONARY EMBOLISM: Echocardiography on depressed contractility of the RV free wall compared with the RV apex
 show a large")

31 PULMONARY EMBOLISM: compression venous ultrasonography ession two crossection ultrasound images through the right common femoral vein (CFV) show a large nonocclusive thrombus in the vessel lumen (yellow arrow). The image on the left shows the common femoral vein prior to compression being applied with a large clot within it

32 PULMONARY EMBOLISM: ECG 50 MM/S S1Q3T3 pattern (McGinn-White sign) Uncompleted RBBB R Q QR pattern in V1 inversion of T waves in leads V1 V4

33 PULMONARY EMBOLISM: differential diagnoses Musculoskeletal pain Pleuritis Pericarditis Salicylate intoxication Hyperventilation Silicone pulmonary embolism Lung trauma Mediastinitis, acute Sickle cell disease
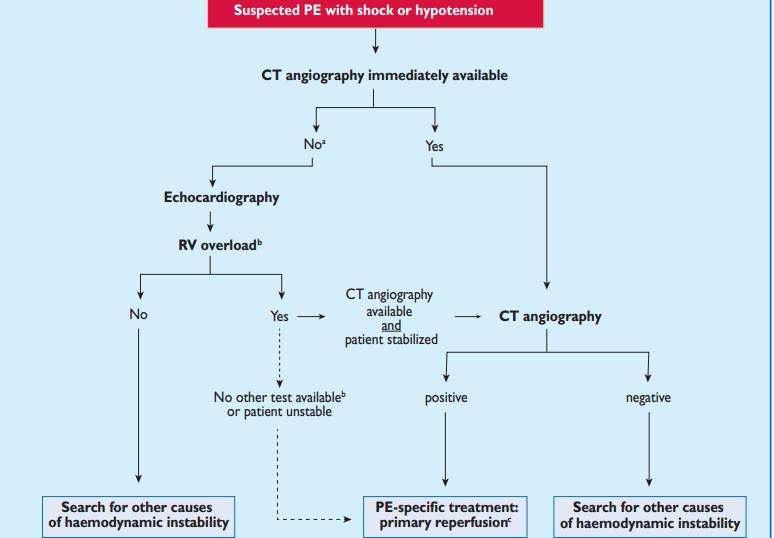
34 ESC Guidelines, 2014
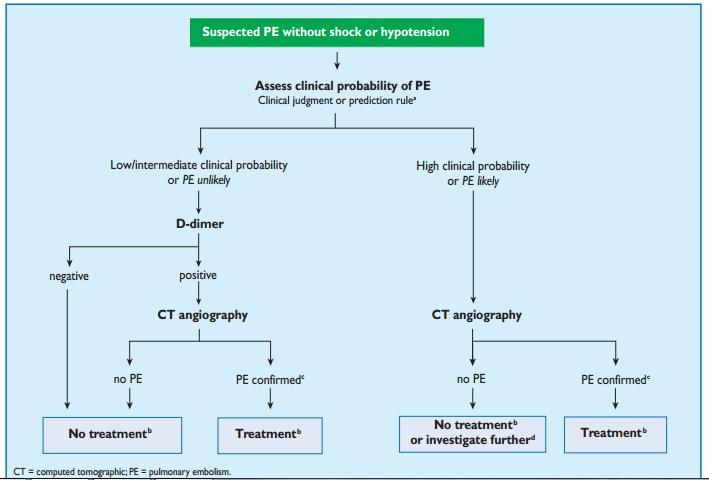
35 ESC Guidelines, 2014

36 PULMONARY EMBOLISM: Treatment in the acute phase Haemodynamic and respiratory support Anticoagulation Thrombolytic treatment Surgical embolectomy Percutaneous catheter-directed treatment Venous filters Early discharge and home treatment
37 Haemodynamic and respiratory support Acute RV failure with resulting low systemic output is the leading cause of death in patients with high-risk PE. Use of vasopressors is often necessary, in parallel with (or while waiting for) pharmacological, surgical, or interventional reperfusion treatment. Norepinephrine appears to improve RV function via a direct positive inotropic effect, while also improving RV coronary perfusion by peripheral vascular alpha-receptor stimulation and the increase in systemic BP. Vasodilators decrease pulmonary arterial pressure and pulmonary vascular resistance, but the main concern is the lack of specificity of these drugs for the pulmonary vasculature after systemic (intravenous) administration. Hypoxaemia is usually reversed with administration of oxygen. When mechanical ventilation is required, care should be taken to limit its adverse haemodynamic effects. In particular, the positive intrathoracic pressure induced by mechanical ventilation may reduce venous return and worsen RV failure in patients with massive PE. Low tidal volumes (approximately 6 ml/kg lean body weight) should be used in an attempt to keep the end-inspiratory plateau pressure <30 cm H2O.
38 Anticoagulation In patients with acute PE, anticoagulation is recommended, with the objective of preventing both early death and recurrent symptomatic or fatal VTE. The standard duration of anticoagulation should cover at least 3 months. Diagnostic investigations should not delay empirical anticoagulant therapy. Thrombolytic therapy should be used in patients with acute pulmonary embolism who have hypotension (systolic blood pressure< 90 mm Hg) who do not have a high bleeding risk and in selected patients with acute pulmonary embolism not associated with hypotension who have a low bleeding risk and whose initial clinical presentation or clinical course suggests a high risk of developing hypotension. Long-term anticoagulation is critical to the prevention of recurrence of DVT or pulmonary embolism, because even in patients who are fully anticoagulated, DVT and pulmonary embolism can and often do recur. Anticoagulation medications include the following: Unfractionated heparin Low-molecular-weight heparin Factor Xa Inhibitors Fondaparinux Warfarin Thrombolytic agents used in managing pulmonary embolism include the following: Alteplase Reteplase Urokinase Streptokinase
39 The first is systemic thrombolysis followed by anticoagulation (shock). The second is catheter-directed thrombolysis. Thrombolytic therapy should be used in patients with acute PE associated with hypotension (systolic BP < 90 mm HG), who do not have a high bleeding risk Thrombolytic therapy is suggested in select patients with acute PE not associated with hypotension and with a low bleeding risk whose initial clinical presentation or clinical course after starting anticoagulation suggests a high risk of developing hypotension Assessment of PE severity, prognosis, and risk of bleeding dictate whether thrombolytic therapy should be started. Thrombolytic therapy is not recommended for most patients with acute PE not associated with hypotension

40 Thrombolytics Thrombolysis is indicated for hemodynamically unstable patients with pulmonary embolism. Thrombolysis dramatically improves acute cor pulmonale. Thrombolytic therapy has replaced surgical embolectomy as the treatment for hemodynamically unstable patients with massive pulmonary embolism. Fibrinolytic regimens currently in common use for pulmonary embolism include 2 forms of recombinant tpa, alteplase and reteplase, along with urokinase and streptokinase. Alteplase usually is given as a front-loaded infusion over 90 or 120 minutes. Urokinase and streptokinase usually are given as infusions over 24 hours or more. Reteplase is a new-generation thrombolytic with a longer half-life; it is given as a single bolus or as 2 boluses administered 30 minutes apart. Reteplase and alteplase are preferred for patients with pulmonary embolism Streptokinase is least desirable of all the fibrinolytic agents because antigenic problems and other adverse reactions
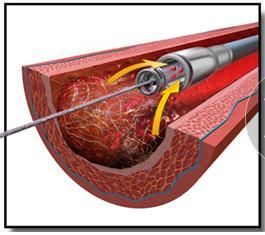
 rheolytic thrombectomy with hydrodynamic catheter devices, (iii) suction thrombectomy with aspiration catheters and (iv) rotational thrombectomy.")
41 Percutaneous catheter-directed treatment For patients with absolute contraindications to thrombolysis, interventional options include: (i) thrombus fragmentation with pigtail or balloon catheter, (ii) rheolytic thrombectomy with hydrodynamic catheter devices, (iii) suction thrombectomy with aspiration catheters and (iv) rotational thrombectomy. On the other hand, for patients without absolute contraindications to thrombolysis, catheter-directed thrombolysis or pharmacomechanical thrombolysis are preferred approaches.

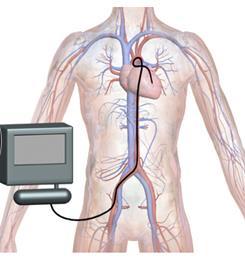
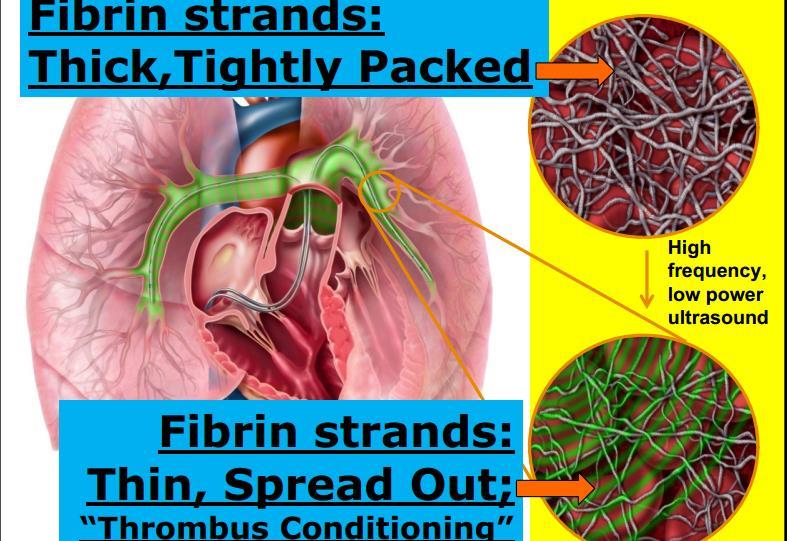
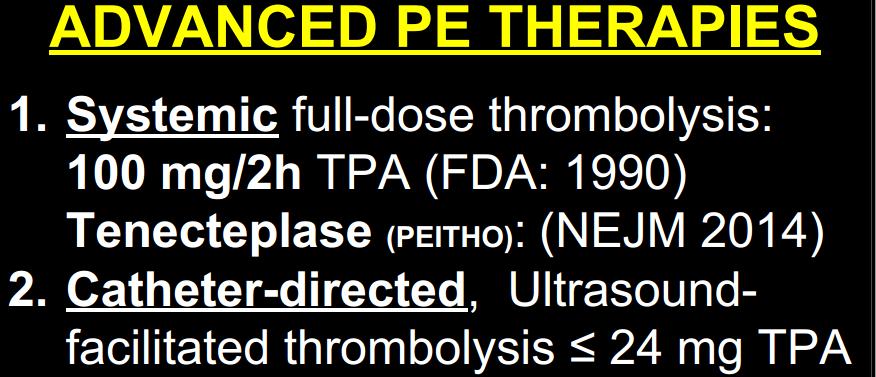
42 Catheter-directed, Ultrasound-facilitated thrombolysis
43


44 Surgical embolectomy The first successful surgical pulmonary embolectomy was performed in 1924, several decades before the introduction of medical treatment for PE. Following rapid transfer to the operating room and induction of anaesthesia and median sternotomy, normothermic cardiopulmonary bypass should be instituted. Aortic cross-clamping and cardioplegic cardiac arrest should be avoided. With bilateral PA incisions, clots can be removed from both pulmonary arteries down to the segmental level under direct vision. Prolonged periods of post-operative cardiopulmonary bypass and weaning may be necessary for recovery of RV function.


45 Parenteral anticoagulation In patients with high or intermediate clinical probability for PE, parenteral anticoagulation should be initiated whilst awaiting the results of diagnostic tests. Immediate anticoagulation can be achieved with parenteral anticoagulants such as intravenous UFH, subcutaneous lowmolecular-weight heparin (LMWH),or subcutaneous fondaparinux. UFH is recommended for patients in whom primary reperfusion is considered, as well as for those with serious renal impairment (creatinine clearance < 30 ml/min), or severe obesity. LMWH or fondaparinux are preferred over UFH for initial anticoagulation in PE.

46 Heparin action Heparin major anticoagulant effect by inactivating thrombin and activated factor X (factor Xa) through an antithrombin (AT)- dependent mechanism. Heparin binds to AT through a highaffinity pentasaccharide, which is present on about a third of heparin molecules. For inhibition of thrombin, heparin must bind to both the coagulation enzyme and AT, whereas binding to the enzyme is not required for inhibition of factor Xa. Unfractionated heparin infusion should be stopped during administration of streptokinase or urokinase

47 Available oral anticoagulants include: vitamin K antagonists (warfarin), direct thrombin inhibitors (dabigatran), direct factor Xa inhibitors (rivaroxaban) Oral anticoagulants should be initiated as soon as possible, and preferably on the same day as the parenteral anticoagulant. VKAs have been the gold standard in oral anticoagulation for more than 50 years. (The image shows red blood cells enmeshed in a fibrinous matrix in the process of clot formation.)
48 vitamin K antagonists (warfarin) The anticoagulant effect of warfarin is mediated by the inhibition of vitamin K dependent factors, which are II, VII, IX, and X. The peak effect does not occur until hours after drug administration, and the dosage is difficult to titrate. A prothrombin time ratio is expressed as an INR and is monitored to assess the adequacy of warfarin therapy. The recommended therapeutic range for venous thromboembolism is an INR of 2-3. This level of anticoagulation markedly reduces the risk of bleeding without the loss of effectiveness. Warfarin can be started at a dose of 10 mg in younger (e.g.,60 years of age), otherwise healthy outpatients, and at a dose of 5 mg in older patients and in those who are hospitalized. The daily dose is adjusted according to the INR over the next 5 7 days, aiming for an INR level of
49 Direct thrombin inhibitors (dabigatran) Dabigatran etexilate is a competitive reversible non-peptide antagonist of thrombin. Thrombin is a multifunctional enzyme which converts fibrinogen to fibrin, cross-linking fibrin monomers via activation of factor XIII and augmenting further thrombin production via the activation of factors V and VIII. It also activates platelets, generates anticoagulant activity via activation of protein C and initiates numerous cellular processes including wound healing. Indicated for treatment of deep vein thrombosis (DVT) and pulmonary embolus (PE) in patients who have been treated with a parenteral anticoagulant for 5-10 days Also indicated to reduce the risk of recurrence of DVT and PE in patients who have been previously treated CrCl >30 ml/min: 150 mg PO BID CrCl 30 ml/min or on dialysis: Dosage recommendations cannot be provided CrCl <50 ml/min with concomitant use of P-gp inhibitors: Avoid co-administration
.")
 to thrombin (factor IIa).")
50 Direct factor Xa inhibitors (rivaroxaban) Rivaroxaban is a competitive reversible antagonist of activated factor X (Xa). Factor Xa is the active component of the prothrombinase complex that catalyses conversion of prothrombin (factor II) to thrombin (factor IIa). CONTRAINDICATIONS: Active pathological bleeding Severe hypersensitivity reaction

51
52
53

 Patients with massive PE who survived but in whom recurrent embolism invariably will be fatal Patients who have objectively documented recurrent venous thromboembolism, adequate")
54 Vena Cava Filters The current grade 1B recommendation is that patients with acute PE should not routinely receive vena cava filters in addition to anticoagulants. An ideal IVC filter should be easily and safely placed using a percutaneous technique, biocompatible and mechanically stable, and able to trap emboli without causing occlusion of the vena cava INDICATED FOR: Patients with acute venous thromboembolism who have an absolute contraindication to anticoagulant therapy (eg, recent surgery, hemorrhagic stroke, significant active or recent bleeding) Patients with massive PE who survived but in whom recurrent embolism invariably will be fatal Patients who have objectively documented recurrent venous thromboembolism, adequate anticoagulant therapy notwithstanding
 to reduce the risk of postphlebitic syndrome.")
55 Supportive Care Compression stockings For patients who have had a proximal DVT, the use of elastic compression stockings provides a safe and effective adjunctive treatment that can limit postphlebitic syndrome. Stockings with a pressure of mm Hg at the ankle, worn for 2 years following diagnosis, are recommended (grade 2B) to reduce the risk of postphlebitic syndrome % 100% Additional support therapies Dopamine and dobutamine are the usual inotropic agents. Mechanical ventilation may be necessary to provide respiratory support and as adjunctive therapy for a failing circulatory system. Transfusion with packed red blood cells (either simple or exchange) improves oxygenation immediately. IV fluids may help or may hurt the patient who is hypotensive.

56 Pulmonary Embolism in Pregnancy The risk of venous thromboembolism is increased during pregnancy and the postpartum period. Pulmonary embolism is the leading cause of death in pregnancy. DVT and pulmonary embolism are common during all trimesters of pregnancy and for 6-12 weeks after delivery. The diagnostic approach to patients with pulmonary embolism should be exactly the same in a pregnant patient as in a nonpregnant one. A nuclear perfusion lung scan is safe in pregnancy, as is a chest CT scan. If the patient has a low pretest probability for pulmonary embolism and a normal D-dimer test result, clinical exclusion from further investigations is recommended. When the suspicion is high, the patients should have bilateral leg Doppler assessment. If the results are negative, CT pulmonary angiography is the next step. Heparin and fibrinolysis are safe in pregnancy. Warfarin is contraindicated, because it crosses the placental barrier. Therapeutic treatment with unfractionated heparin or LMWH during pregnancy, with anticoagulation continuing for 4-6 weeks postpartum and for a total of at least 6 months. Pregnant women who are in a hypercoagulable state or who have had previous venous thromboembolism -prophylactic anticoagulation during pregnancy.
57 Complications of PE Sudden cardiac death Obstructive shock Pulseless electrical activity Atrial or ventricular arrhythmias Secondary pulmonary arterial hypertension Cor pulmonale Severe hypoxemia Right-to-left intracardiac shunt Lung infarction Pleural effusion Paradoxical embolism Heparin-induced thrombocytopenia Thrombophlebitis
58 Chronic thromboembolic pulmonary hypertension Chronic thromboembolic pulmonary hypertension has been reported to be a long-term complication of PE, with a reported cumulative incidence of % within the first two years after a symptomatic PE event Inadequate anticoagulation, large thrombus mass, residual thrombi, and recurrence of VTE a pulmonary vascular remodelling process modified by infection, inflammation, circulating and vascular-resident progenitor cells, thyroid hormone replacement, or malignancy Hypercoagulation, sticky red blood cells, high platelet counts, and uncleavable fibrinogen, pulmonary microvascular disease development of CTEPH
 perfusion defect detected by perfusion lung scan, or")
59 The diagnosis of CTEPH is based on findings obtained after at least 3 months of effective anticoagulation, in order to discriminate this condition from sub-acute PE. These findings are: mean pulmonary arterial pressure 25 mm Hg, with pulmonary arterial wedge pressure 15 mm Hg; at least one (segmental) perfusion defect detected by perfusion lung scan, or pulmonaryarteryobstruction seen by MDCT angiography or conventional pulmonary cineangiography.

60 Pulmonary endarterectomy (PEA) is the treatment of choice for the disease. Patients who do not undergo surgery, or suffer from persistent or residual pulmonary hypertension after PEA, face a poor prognosis. Advances in balloon pulmonary angioplasty are continuing in an attempt to make this technique a therapeutic alternative for selected patients with non-operable CTEPH
61 CLINICAL CASE


62 In the ECG shown in the slide, what are the findings on leads I and III, and what is their relevance to PE?


63 QR pattern in V1
 in the right leg.")

64 CT venography reveals the presence of deep vein thrombosis (DVT) in the right leg. The patient's BP declines again to 89/62 mm Hg, and her heart rate is now 110 beats/min. Her oxygen saturation is 92%.
65 DIAGNOSIS? Acute massive unstable Pulmonary Embolism (unstable when systolic BP remains below 90 mm Hg for more than 15 minutes or when vasopressors are required) TREATMENT OPTIONS? The treatment options for hemodynamically unstable PE consist of thrombolysis and thrombectomy.

66 Thrombectomy was performed

67
PULMONARY EMBOLISM (PE): DIAGNOSIS AND TREATMENT
: DIAGNOSIS AND TREATMENT") PULMONARY EMBOLISM (PE): DIAGNOSIS AND TREATMENT OBJECTIVE: To provide a diagnostic algorithm and treatment options for patients with acute pulmonary embolism (PE). BACKGROUND: Venous thromboembolism (VTE)
PULMONARY EMBOLISM (PE): DIAGNOSIS AND TREATMENT OBJECTIVE: To provide a diagnostic algorithm and treatment options for patients with acute pulmonary embolism (PE). BACKGROUND: Venous thromboembolism (VTE)
Dr. Rami M. Adil Al-Hayali Assistant Professor in Medicine
 Dr. Rami M. Adil Al-Hayali Assistant Professor in Medicine Venous thromboembolism: pulmonary embolism (PE) deep vein thrombosis (DVT) 1% of all patients admitted to hospital 5% of in-hospital mortality
Dr. Rami M. Adil Al-Hayali Assistant Professor in Medicine Venous thromboembolism: pulmonary embolism (PE) deep vein thrombosis (DVT) 1% of all patients admitted to hospital 5% of in-hospital mortality
Venous Thrombosis. Magnitude of the Problem. DVT 2 Million PE 600,000. Death 60,000. Estimated Cost of VTE Care $1.5 Billion/year.
 Venous Thrombosis Magnitude of the Problem DVT 2 Million Postthrombotic Syndrome 800,000 PE 600,000 Death 60,000 Silent PE 1 Million Pulmonary Hypertension 30,000 Estimated Cost of VTE Care $1.5 Billion/year
Venous Thrombosis Magnitude of the Problem DVT 2 Million Postthrombotic Syndrome 800,000 PE 600,000 Death 60,000 Silent PE 1 Million Pulmonary Hypertension 30,000 Estimated Cost of VTE Care $1.5 Billion/year
October 2017 Pulmonary Embolism
 October 2017 Pulmonary Embolism Prof. Ahmed BaHammam, FRCP, FCCP Professor of Medicine College of Medicine King Saud University 1 Objectives Epidemiology Pathophysiology Diagnosis Massive PE Treatment
October 2017 Pulmonary Embolism Prof. Ahmed BaHammam, FRCP, FCCP Professor of Medicine College of Medicine King Saud University 1 Objectives Epidemiology Pathophysiology Diagnosis Massive PE Treatment
Pulmonary Thromboembolism
 Pulmonary Thromboembolism James Allen, MD Epidemiology of Pulmonary Embolism 1,500,000 new cases per year in the United States Often asymptomatic 300,000 deaths per year DVT or PE present in 10% of ICU
Pulmonary Thromboembolism James Allen, MD Epidemiology of Pulmonary Embolism 1,500,000 new cases per year in the United States Often asymptomatic 300,000 deaths per year DVT or PE present in 10% of ICU
What is New in Acute Pulmonary Embolism? Interventional Treatment. Prof. Nils Kucher University Hospital Bern Switzerland
 What is New in Acute Pulmonary Embolism? Interventional Treatment Prof. Nils Kucher University Hospital Bern Switzerland nils.kucher@insel.ch Disclosure of Interest Dr. Kucher received research grants
What is New in Acute Pulmonary Embolism? Interventional Treatment Prof. Nils Kucher University Hospital Bern Switzerland nils.kucher@insel.ch Disclosure of Interest Dr. Kucher received research grants
Pulmonary Embolism. Pulmonary Embolism. Pulmonary Embolism. PE - Clinical
 Pulmonary embolus - a practical approach to investigation and treatment Sam Janes Wellcome Senior Fellow and Respiratory Physician, University College London Background Diagnosis Treatment Common: 50 cases
Pulmonary embolus - a practical approach to investigation and treatment Sam Janes Wellcome Senior Fellow and Respiratory Physician, University College London Background Diagnosis Treatment Common: 50 cases
Pulmonary embolism. Paweł Balsam MD, PhD
 Pulmonary embolism Paweł Balsam MD, PhD Venous thromboembolism (VTE) Pulmonary embolism (PE) and deep vein thrombosis (DVT) are two clinical presentations of veonus thromboembolism Pulmonary embolism A
Pulmonary embolism Paweł Balsam MD, PhD Venous thromboembolism (VTE) Pulmonary embolism (PE) and deep vein thrombosis (DVT) are two clinical presentations of veonus thromboembolism Pulmonary embolism A
Acute Pulmonary Embolism and Deep Vein Thrombosis. Barbara LeVarge MD Beth Israel Deaconess Medical Center Pulmonary Hypertension Center COPYRIGHT
 Acute Pulmonary Embolism and Deep Vein Thrombosis Barbara LeVarge MD Beth Israel Deaconess Medical Center Pulmonary Hypertension Center Acute PE and DVT No disclosures. Acute PE and DVT Learning objectives
Acute Pulmonary Embolism and Deep Vein Thrombosis Barbara LeVarge MD Beth Israel Deaconess Medical Center Pulmonary Hypertension Center Acute PE and DVT No disclosures. Acute PE and DVT Learning objectives
Thrombolysis in PE. Outline. Disclosure. Overview on Pulmonary Embolism. Hot Topics in Emergency Medicine 2012 Midyear Clinical Meeting
 Disclosure Thrombolysis in PE Daniel P. Hays, PharmD, BCPS, FASHP reports no relevant financial relationships. Daniel P. Hays, PharmD, BCPS, FASHP Outline 55 YOF presents to ED with SOB PMH of DVT + noncompliance
Disclosure Thrombolysis in PE Daniel P. Hays, PharmD, BCPS, FASHP reports no relevant financial relationships. Daniel P. Hays, PharmD, BCPS, FASHP Outline 55 YOF presents to ED with SOB PMH of DVT + noncompliance
Pulmonary embolism. Paweł Balsam
 Pulmonary embolism Paweł Balsam Venous thromboembolism (VTE) Pulmonary embolism (PE) and deep vein thrombosis (DVT) are two clinical presentations of veonus thromboembolism Pulmonary embolism A pulmonary
Pulmonary embolism Paweł Balsam Venous thromboembolism (VTE) Pulmonary embolism (PE) and deep vein thrombosis (DVT) are two clinical presentations of veonus thromboembolism Pulmonary embolism A pulmonary
Venous thrombosis is common and often occurs spontaneously, but it also frequently accompanies medical and surgical conditions, both in the community
 Venous Thrombosis Venous Thrombosis It occurs mainly in the deep veins of the leg (deep vein thrombosis, DVT), from which parts of the clot frequently embolize to the lungs (pulmonary embolism, PE). Fewer
Venous Thrombosis Venous Thrombosis It occurs mainly in the deep veins of the leg (deep vein thrombosis, DVT), from which parts of the clot frequently embolize to the lungs (pulmonary embolism, PE). Fewer
PE and DVT. Dr Anzo William Adiga WatsApp or Call Medical Officer/RHEMA MEDICAL GROUP
 PE and DVT Dr Anzo William Adiga WatsApp or Call +256777363201 Medical Officer/RHEMA MEDICAL GROUP OBJECTIVES DEFINE DVT AND P.E PATHOPHYSIOLOGY OF DVT CLINICAL PRESENTATION OF DVT/PE INVESTIGATE DVT MANAGEMENT
PE and DVT Dr Anzo William Adiga WatsApp or Call +256777363201 Medical Officer/RHEMA MEDICAL GROUP OBJECTIVES DEFINE DVT AND P.E PATHOPHYSIOLOGY OF DVT CLINICAL PRESENTATION OF DVT/PE INVESTIGATE DVT MANAGEMENT
Mabel Labrada, MD Miami VA Medical Center
 Mabel Labrada, MD Miami VA Medical Center *1-Treatment for acute DVT with underlying malignancy is for 3 months. *2-Treatment of provoked acute proximal DVT can be stopped after 3months of treatment and
Mabel Labrada, MD Miami VA Medical Center *1-Treatment for acute DVT with underlying malignancy is for 3 months. *2-Treatment of provoked acute proximal DVT can be stopped after 3months of treatment and
PULMONARY EMBOLISM -CASE REPORT-
 University Goce Delcev, Faculty of Medical sciences, Stip University Clinic of Cardiology, Skopje R. Of Macedonia PULMONARY EMBOLISM -CASE REPORT- Gordana Kamceva MD mr.sci Acknowledgment Marija Vavlukis
University Goce Delcev, Faculty of Medical sciences, Stip University Clinic of Cardiology, Skopje R. Of Macedonia PULMONARY EMBOLISM -CASE REPORT- Gordana Kamceva MD mr.sci Acknowledgment Marija Vavlukis
DEEP VEIN THROMBOSIS (DVT): TREATMENT
: TREATMENT") DEEP VEIN THROMBOSIS (DVT): TREATMENT OBJECTIVE: To provide an evidence-based approach to treatment of patients presenting with deep vein thrombosis (DVT). BACKGROUND: An estimated 45,000 patients in Canada
DEEP VEIN THROMBOSIS (DVT): TREATMENT OBJECTIVE: To provide an evidence-based approach to treatment of patients presenting with deep vein thrombosis (DVT). BACKGROUND: An estimated 45,000 patients in Canada
Jessica Bryan, Natalia Evans, Karlyn Henderson, & Whitney Parks
 Jessica Bryan, Natalia Evans, Karlyn Henderson, & Whitney Parks 1. What is the most common cause of death in hospitalized patients? 1. Hospital-acquired infection 2. Pulmonary embolism 3. Myocardial infarction
Jessica Bryan, Natalia Evans, Karlyn Henderson, & Whitney Parks 1. What is the most common cause of death in hospitalized patients? 1. Hospital-acquired infection 2. Pulmonary embolism 3. Myocardial infarction
Venous thromboembolic diseases: diagnosis, management and thrombophilia testing (2012) NICE guideline CG144
 NICE guideline CG144") Venous thromboembolic diseases: diagnosis, management and thrombophilia testing (2012) NICE guideline CG144 Appendix A: Summary of new evidence from Summary of evidence from previous year Diagnosis Diagnostic
Venous thromboembolic diseases: diagnosis, management and thrombophilia testing (2012) NICE guideline CG144 Appendix A: Summary of new evidence from Summary of evidence from previous year Diagnosis Diagnostic
Single Center 4 year series of 114 consecutive patients treated for massive and submassive PE. Mark Goodwin, MD
 Single Center 4 year series of 114 consecutive patients treated for massive and submassive PE Mark Goodwin, MD Disclosure Speaker name:... I have the following potential conflicts of interest to report:
Single Center 4 year series of 114 consecutive patients treated for massive and submassive PE Mark Goodwin, MD Disclosure Speaker name:... I have the following potential conflicts of interest to report:
CURRENT & FUTURE THERAPEUTIC MANAGEMENT OF VENOUS THROMBOEMBOLISM. Gordon Lowe Professor of Vascular Medicine University of Glasgow
 CURRENT & FUTURE THERAPEUTIC MANAGEMENT OF VENOUS THROMBOEMBOLISM Gordon Lowe Professor of Vascular Medicine University of Glasgow VENOUS THROMBOEMBOLISM Common cause of death and disability 50% hospital-acquired
CURRENT & FUTURE THERAPEUTIC MANAGEMENT OF VENOUS THROMBOEMBOLISM Gordon Lowe Professor of Vascular Medicine University of Glasgow VENOUS THROMBOEMBOLISM Common cause of death and disability 50% hospital-acquired
A 50-year-old woman with syncope
 Hira Shahzad 1, Ali Bin Sarwar Zubairi 2 1 Medical College, Aga Khan University Hospital, Karachi 2 Department of Medicine, Aga Khan University Hospital, Karachi, Pakistan Ali Bin Sarwar Zubairi Associate
Hira Shahzad 1, Ali Bin Sarwar Zubairi 2 1 Medical College, Aga Khan University Hospital, Karachi 2 Department of Medicine, Aga Khan University Hospital, Karachi, Pakistan Ali Bin Sarwar Zubairi Associate
Diagnosis and Treatment of Pulmonary Embolism. Farzin Ghiasi, MD Pulmonologist August, 2016
 Diagnosis and Treatment of Pulmonary Embolism Farzin Ghiasi, MD Pulmonologist August, 2016 DVT & PE Hypercoagulable state is characteristic of pregnancy, and DVT occurs in about 1 in 500 pregnancies. In
Diagnosis and Treatment of Pulmonary Embolism Farzin Ghiasi, MD Pulmonologist August, 2016 DVT & PE Hypercoagulable state is characteristic of pregnancy, and DVT occurs in about 1 in 500 pregnancies. In
Handbook for Venous Thromboembolism
 Handbook for Venous Thromboembolism Gregory Piazza Benjamin Hohlfelder Samuel Z. Goldhaber Handbook for Venous Thromboembolism Gregory Piazza Cardiovascular Division Harvard Medical School Brigham and
Handbook for Venous Thromboembolism Gregory Piazza Benjamin Hohlfelder Samuel Z. Goldhaber Handbook for Venous Thromboembolism Gregory Piazza Cardiovascular Division Harvard Medical School Brigham and
Severe pulmonary embolism: surgical aspects. Oliver Reuthebuch Clinic for Cardiac Surgery University Hospital Basel Switzerland
 Severe pulmonary embolism: surgical aspects Oliver Reuthebuch Clinic for Cardiac Surgery University Hospital Basel Switzerland Severe pulmonary embolism Acute pulmonary embolism Chronic pulmonary thromboembolism
Severe pulmonary embolism: surgical aspects Oliver Reuthebuch Clinic for Cardiac Surgery University Hospital Basel Switzerland Severe pulmonary embolism Acute pulmonary embolism Chronic pulmonary thromboembolism
Diagnosis and management of acute pulmonary embolism Bobbie Morici, MSPAS, PA-C
 Diagnosis and management of acute pulmonary embolism Bobbie Morici, MSPAS, PA-C ABSTRACT Acute pulmonary embolism is a life-threatening diagnosis that can present with a multitude of nonspecific symptoms.
Diagnosis and management of acute pulmonary embolism Bobbie Morici, MSPAS, PA-C ABSTRACT Acute pulmonary embolism is a life-threatening diagnosis that can present with a multitude of nonspecific symptoms.
Ultrasound-enhanced, catheter-directed thrombolysis for pulmonary embolism
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Interventional procedure consultation document Ultrasound-enhanced, catheter-directed thrombolysis for pulmonary embolism A pulmonary embolism (PE) is
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Interventional procedure consultation document Ultrasound-enhanced, catheter-directed thrombolysis for pulmonary embolism A pulmonary embolism (PE) is
Pulmonary Embolism. Supportive module 3 "Basics of diagnosis, treatment and prevention of major pulmonary diseases "
 Supportive module 3 "Basics of diagnosis, treatment and prevention of major pulmonary diseases " Pulmonary Embolism LECTURE IN INTERNAL MEDICINE FOR IV COURSE STUDENTS M. Yabluchansky, L. Bogun, L. Martymianova,
Supportive module 3 "Basics of diagnosis, treatment and prevention of major pulmonary diseases " Pulmonary Embolism LECTURE IN INTERNAL MEDICINE FOR IV COURSE STUDENTS M. Yabluchansky, L. Bogun, L. Martymianova,
Innovative Endovascular Approach to Pulmonary Embolism by Ultrasound Enhanced Thrombolysis. Prof. Ralf R.Kolvenbach MD,PhD,FEBVS
 Innovative Endovascular Approach to Pulmonary Embolism by Ultrasound Enhanced Thrombolysis Prof. Ralf R.Kolvenbach MD,PhD,FEBVS Catheter-based thrombolysis Local administration of lytic agent Higher local
Innovative Endovascular Approach to Pulmonary Embolism by Ultrasound Enhanced Thrombolysis Prof. Ralf R.Kolvenbach MD,PhD,FEBVS Catheter-based thrombolysis Local administration of lytic agent Higher local
Cover Page. The handle holds various files of this Leiden University dissertation.
 Cover Page The handle http://hdl.handle.net/1887/21764 holds various files of this Leiden University dissertation. Author: Mos, Inge Christina Maria Title: A more granular view on pulmonary embolism Issue
Cover Page The handle http://hdl.handle.net/1887/21764 holds various files of this Leiden University dissertation. Author: Mos, Inge Christina Maria Title: A more granular view on pulmonary embolism Issue
Epidemiology: Incidence VTE: Mortality Morbidity Risk Factors: Acute Chronic : Genetic
 Submassive PE Pulmonary Embolism Epidemiology: Incidence VTE: 100-200/100,000 = 3rd most frequent cardiovascular disease Symptomatic DVT complicated by PE = 40-50% Sudden fatal PE = 34% Intermediate-risk
Submassive PE Pulmonary Embolism Epidemiology: Incidence VTE: 100-200/100,000 = 3rd most frequent cardiovascular disease Symptomatic DVT complicated by PE = 40-50% Sudden fatal PE = 34% Intermediate-risk
REVIEW ON PULMONARY EMBOLISM
 REVIEW ON PULMONARY EMBOLISM * Shashi Kumar Yadav, Prof. Xiao Wei, Roshan Kumar Yadav, Sanjay Kumar Verma and Deepika Dhakal * Department of Medicine, Clinical College of Yangtze University, The first
REVIEW ON PULMONARY EMBOLISM * Shashi Kumar Yadav, Prof. Xiao Wei, Roshan Kumar Yadav, Sanjay Kumar Verma and Deepika Dhakal * Department of Medicine, Clinical College of Yangtze University, The first
Pulmonary Thromboembolism
 Pulmonary Thromboembolism Jing ZHANG ( 张静 ), MD, PhD zhang.jing@zs-hospital.sh.cn Department of Pulmonary Medicine Zhongshan Hospital Fudan University OUTLINE Understand the historical context of pulmonary
Pulmonary Thromboembolism Jing ZHANG ( 张静 ), MD, PhD zhang.jing@zs-hospital.sh.cn Department of Pulmonary Medicine Zhongshan Hospital Fudan University OUTLINE Understand the historical context of pulmonary
Diagnosis and Treatment of Deep Venous Thrombosis and Pulmonary Embolism
 Agency for Healthcare Research and Quality Evidence Report/Technology Assessment Diagnosis and Treatment of Deep Venous Thrombosis and Pulmonary Embolism Summary Number 68 Overview Venous thromboembolism
Agency for Healthcare Research and Quality Evidence Report/Technology Assessment Diagnosis and Treatment of Deep Venous Thrombosis and Pulmonary Embolism Summary Number 68 Overview Venous thromboembolism
Epidemiology. Update on Pulmonary Embolism. Keys to PE Management 5/5/2014. Diagnosis. Risk stratification. Treatment
 Update on Pulmonary Embolism Steven M. Dean, DO, FACP, RPVI Program Director- Vascular Medicine Associate Professor of Internal Medicine Division of Cardiovascular Medicine The Ohio State University Keys
Update on Pulmonary Embolism Steven M. Dean, DO, FACP, RPVI Program Director- Vascular Medicine Associate Professor of Internal Medicine Division of Cardiovascular Medicine The Ohio State University Keys
Pulmonary Embolism. Dr.V.Maruthi Rama Krishna Rao
 Pulmonary Embolism Dr.V.Maruthi Rama Krishna Rao Assistant prof EMD Pulmonary embolism (PE) refers to the lodging of a embolic material from a distant site in the pulmonary circulation The term embolus
Pulmonary Embolism Dr.V.Maruthi Rama Krishna Rao Assistant prof EMD Pulmonary embolism (PE) refers to the lodging of a embolic material from a distant site in the pulmonary circulation The term embolus
Pulmonary Embolism. Thoracic radiologist Helena Lauri
 Pulmonary Embolism Thoracic radiologist Helena Lauri 8.5.2017 Statistics 1-2 out of 1000 adults annually are diagnosed with deep vein thrombosis (DVT) and/or pulmonary embolism (PE) About half of patients
Pulmonary Embolism Thoracic radiologist Helena Lauri 8.5.2017 Statistics 1-2 out of 1000 adults annually are diagnosed with deep vein thrombosis (DVT) and/or pulmonary embolism (PE) About half of patients
University Journal of Medicine and Medical Specialities
 University Journal of Medicine and Medical Specialities Volume 1 Issue 1 2015 An unusual case of SADDLE Pulmonary Thrombo Embolism Boopathirajan P Jayanthi R Stanley Medical College Abstract: Pulmonary
University Journal of Medicine and Medical Specialities Volume 1 Issue 1 2015 An unusual case of SADDLE Pulmonary Thrombo Embolism Boopathirajan P Jayanthi R Stanley Medical College Abstract: Pulmonary
CARDIAC PROBLEMS IN PREGNANCY
 CARDIAC PROBLEMS IN PREGNANCY LAS VEGAS, NEVADA, USA 27 February 1 March 2016 SUCCESSFUL TREATMENT WITH RECOMBINANT TISSUE PLASMINOGEN ACTIVATOR OF MASSIVE PULMONARY EMBOLISM IN THE 16 TH WEEK OF PREGNANCY
CARDIAC PROBLEMS IN PREGNANCY LAS VEGAS, NEVADA, USA 27 February 1 March 2016 SUCCESSFUL TREATMENT WITH RECOMBINANT TISSUE PLASMINOGEN ACTIVATOR OF MASSIVE PULMONARY EMBOLISM IN THE 16 TH WEEK OF PREGNANCY
VENOUS THROMBOEMBOLISM DR. AMITESH AGGARWAL
 VENOUS THROMBOEMBOLISM DR. AMITESH AGGARWAL Pulmonary embolism and deep venous thrombosis spectrum of one disease venous thromboembolism PE is not a disease it is a complication of DVT 79% PE DVT LL 50%
VENOUS THROMBOEMBOLISM DR. AMITESH AGGARWAL Pulmonary embolism and deep venous thrombosis spectrum of one disease venous thromboembolism PE is not a disease it is a complication of DVT 79% PE DVT LL 50%
Is Thrombolysis Only for a Crisis?
 Is Thrombolysis Only for a Crisis? December 19, 2017 Is Thrombolysis Only for a Crisis? Indications for Thrombolytic Therapy in Patients with Acute Pulmonary Embolism Case Scenario A 28 year old woman
Is Thrombolysis Only for a Crisis? December 19, 2017 Is Thrombolysis Only for a Crisis? Indications for Thrombolytic Therapy in Patients with Acute Pulmonary Embolism Case Scenario A 28 year old woman
Diagnosis and management of pulmonary embolism
 Follow the link from the online version of this article to obtain certified continuing medical education credits bmj.com Respiratory Medicine updates from BMJ Group are at bmj.com/specialties/respiratory-medicine
Follow the link from the online version of this article to obtain certified continuing medical education credits bmj.com Respiratory Medicine updates from BMJ Group are at bmj.com/specialties/respiratory-medicine
Innovative Endovascular Approach to Pulmonary Embolism by Ultrasound Enhanced Thrombolysis. Prof. Ralf R.Kolvenbach MD,PhD,FEBVS
 Innovative Endovascular Approach to Pulmonary Embolism by Ultrasound Enhanced Thrombolysis Prof. Ralf R.Kolvenbach MD,PhD,FEBVS Conflict of Interest BTG Standard PE therapy ANTICOAGULATION (AC) HEPARIN
Innovative Endovascular Approach to Pulmonary Embolism by Ultrasound Enhanced Thrombolysis Prof. Ralf R.Kolvenbach MD,PhD,FEBVS Conflict of Interest BTG Standard PE therapy ANTICOAGULATION (AC) HEPARIN
8/16/2012. Pulmonary Embolism
 Pulmonary Embolism Rita M. Williams, NP-C, PA PeaceHealth Medical Group, Pulmonary & Critical Care Pulmonary Embolism Acute pulmonary embolism (PE) is a common and frequently fatal disease Clinical presentation
Pulmonary Embolism Rita M. Williams, NP-C, PA PeaceHealth Medical Group, Pulmonary & Critical Care Pulmonary Embolism Acute pulmonary embolism (PE) is a common and frequently fatal disease Clinical presentation
Pathology of pulmonary vascular disease. Dr.Ashraf Abdelfatah Deyab. Assistant Professor of Pathology Faculty of Medicine Almajma ah University
 Pathology of pulmonary vascular disease Dr.Ashraf Abdelfatah Deyab Assistant Professor of Pathology Faculty of Medicine Almajma ah University Pulmonary vascular disease Type of pulmonary circulation: Types
Pathology of pulmonary vascular disease Dr.Ashraf Abdelfatah Deyab Assistant Professor of Pathology Faculty of Medicine Almajma ah University Pulmonary vascular disease Type of pulmonary circulation: Types
Disclosures. Objectives
 BRIGHAM AND WOMEN S HOSPITAL Treatment of Massive and Submassive Pulmonary Embolism Gregory Piazza, MD, MS Assistant Professor of Medicine Harvard Medical School Staff Physician, Cardiovascular Division
BRIGHAM AND WOMEN S HOSPITAL Treatment of Massive and Submassive Pulmonary Embolism Gregory Piazza, MD, MS Assistant Professor of Medicine Harvard Medical School Staff Physician, Cardiovascular Division
Interventional Management of Acute Pulmonary Embolism
 Interventional Management of Acute Pulmonary Embolism Prof. Nils Kucher Angiology & Cardiology University Hospital Bern Inselspital nils.kucher@insel.ch DECLARATION OF CONFLICT OF INTEREST Consultant to
Interventional Management of Acute Pulmonary Embolism Prof. Nils Kucher Angiology & Cardiology University Hospital Bern Inselspital nils.kucher@insel.ch DECLARATION OF CONFLICT OF INTEREST Consultant to
Understanding Best Practices in Anticoagulation Therapy in Patients with Venous Thromboembolism. Rajat Deo, MD, MTR
 Understanding Best Practices in Anticoagulation Therapy in Patients with Venous Thromboembolism Rajat Deo, MD, MTR Director of Translational Research in Cardiac Arrhythmias Division of Cardiovascular Medicine
Understanding Best Practices in Anticoagulation Therapy in Patients with Venous Thromboembolism Rajat Deo, MD, MTR Director of Translational Research in Cardiac Arrhythmias Division of Cardiovascular Medicine
DVT - initial management NSCCG
 Background information Information resources for patients and carers Updates to this care map Synonyms Below knee DVT and bleeding risks Patient with confirmed DVT Scan confirms superficial thrombophlebitis
Background information Information resources for patients and carers Updates to this care map Synonyms Below knee DVT and bleeding risks Patient with confirmed DVT Scan confirms superficial thrombophlebitis
Clinical Guide - Suspected PE (Reviewed 2006)
") Clinical Guide - Suspected (Reviewed 2006) Principal Developer: B. Geerts Secondary Developers: C. Demers, C. Kearon Background Investigation of patients with suspected pulmonary emboli () remains problematic
Clinical Guide - Suspected (Reviewed 2006) Principal Developer: B. Geerts Secondary Developers: C. Demers, C. Kearon Background Investigation of patients with suspected pulmonary emboli () remains problematic
Heart Health ESC Guidelines on the diagnosis and management of acute pulmonary embolism
 Heart Health Open Access Received: Oct 22, 2014 Accepted: Dec 01, 2014 Published: Dec 05, 2014 http://dx.doi.org/10.14437/hhoa-1-105 Review Jiri Widimsky, Heart Health Open Access 2014, 1:1 2014 ESC Guidelines
Heart Health Open Access Received: Oct 22, 2014 Accepted: Dec 01, 2014 Published: Dec 05, 2014 http://dx.doi.org/10.14437/hhoa-1-105 Review Jiri Widimsky, Heart Health Open Access 2014, 1:1 2014 ESC Guidelines
Risk factors for DVT. Venous thrombosis & pulmonary embolism. Anticoagulation (cont d) Diagnosis 1/5/2018. Ahmed Mahmoud, MD
 Diagnosis 1/5/2018. Ahmed Mahmoud, MD") Risk factors for DVT Venous thrombosis & pulmonary embolism Ahmed Mahmoud, MD Surgery ; post op especially for long cases, pelvic operations (THR), Trauma ; long bone fractures, pelvic fractures (posterior
Risk factors for DVT Venous thrombosis & pulmonary embolism Ahmed Mahmoud, MD Surgery ; post op especially for long cases, pelvic operations (THR), Trauma ; long bone fractures, pelvic fractures (posterior
Venous thrombosis & pulmonary embolism. Ahmed Mahmoud, MD
 Venous thrombosis & pulmonary embolism Ahmed Mahmoud, MD Risk factors for DVT Surgery ; post op especially for long cases, pelvic operations (THR), Trauma ; long bone fractures, pelvic fractures (posterior
Venous thrombosis & pulmonary embolism Ahmed Mahmoud, MD Risk factors for DVT Surgery ; post op especially for long cases, pelvic operations (THR), Trauma ; long bone fractures, pelvic fractures (posterior
Disclosures. DVT: Diagnosis and Treatment. Questions To Ask. Dr. Susanna Shin - DVT: Diagnosis and Treatment. Acute Venous Thromboembolism (VTE) None
 None") Disclosures DVT: Diagnosis and Treatment None Susanna Shin, MD, FACS Assistant Professor University of Washington Acute Venous Thromboembolism (VTE) Deep Venous Thrombosis (DVT) Pulmonary Embolism (PE)
Disclosures DVT: Diagnosis and Treatment None Susanna Shin, MD, FACS Assistant Professor University of Washington Acute Venous Thromboembolism (VTE) Deep Venous Thrombosis (DVT) Pulmonary Embolism (PE)
Interventional Treatment VTE: Radiologic Approach
 Interventional Treatment VTE: Radiologic Approach Hae Giu Lee, MD Professor, Dept of Radiology Seoul St. Mary s Hospital The Catholic University of Korea Introduction Incidence High incidence: 250,000-1,000,000/year
Interventional Treatment VTE: Radiologic Approach Hae Giu Lee, MD Professor, Dept of Radiology Seoul St. Mary s Hospital The Catholic University of Korea Introduction Incidence High incidence: 250,000-1,000,000/year
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Acute coronary syndrome(s), anticoagulant therapy in, 706, 707 antiplatelet therapy in, 702 ß-blockers in, 703 cardiac biomarkers in,
Index Note: Page numbers of article titles are in boldface type. A Acute coronary syndrome(s), anticoagulant therapy in, 706, 707 antiplatelet therapy in, 702 ß-blockers in, 703 cardiac biomarkers in,
This chapter will describe the effectiveness of antithrombotic
 Antithrombotic Therapy for Venous Thromboembolic Disease The Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy Harry R. Büller, MD, Chair; Giancarlo Agnelli, MD; Russel D. Hull, MBBS,
Antithrombotic Therapy for Venous Thromboembolic Disease The Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy Harry R. Büller, MD, Chair; Giancarlo Agnelli, MD; Russel D. Hull, MBBS,
Surgical Management in Chronic Thromboembolic Pulmonary Hypertension. Michael Bates, MD, FACS Ochsner Health System, New Orleans, LA
 Surgical Management in Chronic Thromboembolic Pulmonary Hypertension Michael Bates, MD, FACS Ochsner Health System, New Orleans, LA Disclosures No industry conflicts I am a surgeon and always disclose
Surgical Management in Chronic Thromboembolic Pulmonary Hypertension Michael Bates, MD, FACS Ochsner Health System, New Orleans, LA Disclosures No industry conflicts I am a surgeon and always disclose
Intraoperative Pulmonary Embolus
 PBLD Table #5 Intraoperative Pulmonary Embolus Holly Richter, M.D. and Sean Benton, D.O. Objectives 1. Determine patients who are at risk for perioperative pulmonary embolism 2. Form a differential diagnosis
PBLD Table #5 Intraoperative Pulmonary Embolus Holly Richter, M.D. and Sean Benton, D.O. Objectives 1. Determine patients who are at risk for perioperative pulmonary embolism 2. Form a differential diagnosis
Blood Thinner Agent. Done by: Meznah Al-mutairi Pharm.D Candidate PNU Collage of Pharmacy
 Blood Thinner Agent Done by: Meznah Al-mutairi Pharm.D Candidate PNU Collage of Pharmacy Outline: Blood thinner agent definition. anticoagulants drugs. Thrombolytics. Blood thinner agent Therapeutic interference
Blood Thinner Agent Done by: Meznah Al-mutairi Pharm.D Candidate PNU Collage of Pharmacy Outline: Blood thinner agent definition. anticoagulants drugs. Thrombolytics. Blood thinner agent Therapeutic interference
Deep Vein Thrombosis
 Deep Vein Thrombosis from NHS (UK) guidelines Introduction Deep vein thrombosis (DVT) is a blood clot in one of the deep veins in the body. Blood clots that develop in a vein are also known as venous thrombosis.
Deep Vein Thrombosis from NHS (UK) guidelines Introduction Deep vein thrombosis (DVT) is a blood clot in one of the deep veins in the body. Blood clots that develop in a vein are also known as venous thrombosis.
Pulmonary Embolism. Supportive module 3 "Basics of diagnosis, treatment and prevention of major pulmonary diseases "
 2016/2017 Spring Semester Supportive module 3 "Basics of diagnosis, treatment and prevention of major pulmonary diseases " Pulmonary Embolism LECTURE IN INTERNAL MEDICINE FOR IV COURSE STUDENTS M. Yabluchansky,
2016/2017 Spring Semester Supportive module 3 "Basics of diagnosis, treatment and prevention of major pulmonary diseases " Pulmonary Embolism LECTURE IN INTERNAL MEDICINE FOR IV COURSE STUDENTS M. Yabluchansky,
Venous Thromboembolism Prophylaxis
 Approved by: Venous Thromboembolism Prophylaxis Vice President and Chief Medical Officer; and Vice President and Chief Operating Officer Corporate Policy & Procedures Manual Number: Date Approved January
Approved by: Venous Thromboembolism Prophylaxis Vice President and Chief Medical Officer; and Vice President and Chief Operating Officer Corporate Policy & Procedures Manual Number: Date Approved January
Radiologic Features of The Pulmonary Embolus
 January 2003 Radiologic Features of The Pulmonary Embolus Travis McGlothin HMSIII Mr. J is a 51 y.o. male who presented to the BIDMC ED w/ acute onset of: Lft. Hemiparesis slurred speech mild dyspnea mild
January 2003 Radiologic Features of The Pulmonary Embolus Travis McGlothin HMSIII Mr. J is a 51 y.o. male who presented to the BIDMC ED w/ acute onset of: Lft. Hemiparesis slurred speech mild dyspnea mild
Pulmonary Embolectomy:
 Pulmonary Embolectomy: Recommendation for early surgical intervention Tomas A. Salerno, M.D. Professor of Surgery, University of Miami Miller School of Medicine and Jackson Memorial Hospital Epidemiology
Pulmonary Embolectomy: Recommendation for early surgical intervention Tomas A. Salerno, M.D. Professor of Surgery, University of Miami Miller School of Medicine and Jackson Memorial Hospital Epidemiology
Approach to Thrombosis
 Approach to Thrombosis Theera Ruchutrakool, M.D. Division of Hematology Department of Medicine Siriraj Hospital Faculty of Medicine Mahidol University Approach to Thrombosis Thrombosis: thrombus formation
Approach to Thrombosis Theera Ruchutrakool, M.D. Division of Hematology Department of Medicine Siriraj Hospital Faculty of Medicine Mahidol University Approach to Thrombosis Thrombosis: thrombus formation
Pulmonary Embolism Is it the Greatest Danger in Deep Vein Thrombosis?
 Difficult issues in Deep Vein Thrombosis: Pulmonary Embolism Is it the Greatest Danger in Deep Vein Thrombosis? Raluca Dulgheru; C Gherghinescu; B Dorobat; H Muresan; R Darabont; M Cinteza; D Vinereanu
Difficult issues in Deep Vein Thrombosis: Pulmonary Embolism Is it the Greatest Danger in Deep Vein Thrombosis? Raluca Dulgheru; C Gherghinescu; B Dorobat; H Muresan; R Darabont; M Cinteza; D Vinereanu
Management of Acute Myocardial Infarction
 Management of Acute Myocardial Infarction Prof. Hossam Kandil Professor of Cardiology Cairo University ST Elevation Acute Myocardial Infarction Aims Of Management Emergency care (Pre-hospital) Early care
Management of Acute Myocardial Infarction Prof. Hossam Kandil Professor of Cardiology Cairo University ST Elevation Acute Myocardial Infarction Aims Of Management Emergency care (Pre-hospital) Early care
RISK STRATIFICATION OF PATIENTS WITH ACUTE SYMPTOMATIC PULMONARY EMBOLISM. David Jiménez, MD, PhD, FCCP Ramón y Cajal Hospital, IRYCIS Madrid, Spain
 RISK STRATIFICATION OF PATIENTS WITH ACUTE SYMPTOMATIC PULMONARY EMBOLISM David Jiménez, MD, PhD, FCCP Ramón y Cajal Hospital, IRYCIS Madrid, Spain Potential Conflicts of Interest Financial conflicts of
RISK STRATIFICATION OF PATIENTS WITH ACUTE SYMPTOMATIC PULMONARY EMBOLISM David Jiménez, MD, PhD, FCCP Ramón y Cajal Hospital, IRYCIS Madrid, Spain Potential Conflicts of Interest Financial conflicts of
Use of EKOS Catheter in the management of Venous Mr. Manoj Niverthi, Mr. Sarang Pujari, and Ms. Nupur Dandavate, The GTF Group
 Use of EKOS Catheter in the management of Venous Thromboembolism @ Mr. Manoj Niverthi, Mr. Sarang Pujari, and Ms. Nupur Dandavate, The GTF Group Introduction Georgia Thrombosis Forum (GTF, www.gtfonline.net)
Use of EKOS Catheter in the management of Venous Thromboembolism @ Mr. Manoj Niverthi, Mr. Sarang Pujari, and Ms. Nupur Dandavate, The GTF Group Introduction Georgia Thrombosis Forum (GTF, www.gtfonline.net)
Cardiovascular Images
 Cardiovascular Images Pulmonary Embolism Diagnosed From Right Heart Changes Seen After Exercise Stress Echocardiography Brian C. Case, MD; Micheas Zemedkun, MD; Amarin Sangkharat, MD; Allen J. Taylor,
Cardiovascular Images Pulmonary Embolism Diagnosed From Right Heart Changes Seen After Exercise Stress Echocardiography Brian C. Case, MD; Micheas Zemedkun, MD; Amarin Sangkharat, MD; Allen J. Taylor,
PE Pathway. The charts are listed as follows:
 PE Pathway This document comprises 6 simple flow charts to assist clinicians in the investigation and treatment of suspected or confirmed Acute Pulmonary Emboli. The pathway has been put together using
PE Pathway This document comprises 6 simple flow charts to assist clinicians in the investigation and treatment of suspected or confirmed Acute Pulmonary Emboli. The pathway has been put together using
Pulmonary Embolism in the mirror of the real clinical case (BMJ Case Reports 2013; doi: /bcr )
") Supportive module 3 "Basics of diagnosis, treatment and prevention of major pulmonary diseases " Pulmonary Embolism in the mirror of the real clinical case (BMJ Case Reports 2013; doi:10.1136/bcr-2012-008197)
Supportive module 3 "Basics of diagnosis, treatment and prevention of major pulmonary diseases " Pulmonary Embolism in the mirror of the real clinical case (BMJ Case Reports 2013; doi:10.1136/bcr-2012-008197)
Slide 1. Slide 2. Slide 3. Outline of This Presentation
 Slide 1 Current Approaches to Venous Thromboembolism Prevention in Orthopedic Patients Hujefa Vora, MD Maria Fox, RN June 9, 2017 Slide 2 Slide 3 Outline of This Presentation Pathophysiology of venous
Slide 1 Current Approaches to Venous Thromboembolism Prevention in Orthopedic Patients Hujefa Vora, MD Maria Fox, RN June 9, 2017 Slide 2 Slide 3 Outline of This Presentation Pathophysiology of venous
Pulmonary embolism. Team Members: Fatima AlTassan, Jawaher abanumy, Abdulrahman thekry, khalid aleidan
 Pulmonary embolism Objectives: Epidemiology Pathophysiology Diagnosis Massive PE Treatment Team Members: Fatima AlTassan, Jawaher abanumy, Abdulrahman thekry, khalid aleidan Team Leader: Nawaf Alkhudhayri
Pulmonary embolism Objectives: Epidemiology Pathophysiology Diagnosis Massive PE Treatment Team Members: Fatima AlTassan, Jawaher abanumy, Abdulrahman thekry, khalid aleidan Team Leader: Nawaf Alkhudhayri
Deep Vein Thrombosis and Pulmonary Embolism: Patient Information
 Deep Vein Thrombosis and Pulmonary Embolism: Patient Information A Deep Vein Thrombosis (DVT) and a Pulmonary Embolism (PE) are both disorders of unwanted blood clotting. Unwanted blood clots can occur
Deep Vein Thrombosis and Pulmonary Embolism: Patient Information A Deep Vein Thrombosis (DVT) and a Pulmonary Embolism (PE) are both disorders of unwanted blood clotting. Unwanted blood clots can occur
Acute and long-term treatment of VTE. Cecilia Becattini University of Perugia
 Acute and long-term treatment of VTE Cecilia Becattini University of Perugia Acute and long-term treatment of VTE The goals The acute PE phase After the acute phase Treatment for VTE Goals of acute treatment
Acute and long-term treatment of VTE Cecilia Becattini University of Perugia Acute and long-term treatment of VTE The goals The acute PE phase After the acute phase Treatment for VTE Goals of acute treatment
Comparison of Five Major Recent Endovascular Treatment Trials
 Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
THROMBOTIC DISORDERS: The Final Frontier
 THROMBOTIC DISORDERS: The Final Frontier Jeffrey I. Weitz, MD, FRCP(C), FACP Professor of Medicine and Biochemistry McMaster University Canada Research Chair in Thrombosis Heart & Stroke Foundation/ J.F.
THROMBOTIC DISORDERS: The Final Frontier Jeffrey I. Weitz, MD, FRCP(C), FACP Professor of Medicine and Biochemistry McMaster University Canada Research Chair in Thrombosis Heart & Stroke Foundation/ J.F.
ADULT TRANSCATHETER AORTIC VALVE REPLACEMENT (TAVR) TELEMETRY BED TRANSFER ORDERS 1 of 4
 TELEMETRY BED TRANSFER ORDERS 1 of 4") TELEMETRY BED TRANSFER 1 of 4 9 Actual 9 Estimated Patient ID Area Weight kg 9 Actual 9 Estimated Height cm ALLERGIES: REFER TO ALLERGY PROFILE/ POWERCHART Transfer to: 10 South Attending Physician: Diagnosis:
TELEMETRY BED TRANSFER 1 of 4 9 Actual 9 Estimated Patient ID Area Weight kg 9 Actual 9 Estimated Height cm ALLERGIES: REFER TO ALLERGY PROFILE/ POWERCHART Transfer to: 10 South Attending Physician: Diagnosis:
Diagnosis and Management of Acute Myocardial Infarction
 Diagnosis and Management of Acute Myocardial Infarction Acute Myocardial Infarction (AMI) occurs as a result of prolonged myocardial ischemia Atherosclerosis leads to endothelial rupture or erosion that
Diagnosis and Management of Acute Myocardial Infarction Acute Myocardial Infarction (AMI) occurs as a result of prolonged myocardial ischemia Atherosclerosis leads to endothelial rupture or erosion that
Deep Vein Thrombosis
 Deep Vein Thrombosis Introduction Deep vein thrombosis (DVT) is a blood clot in a vein. This condition can affect men and women of any age and race. DVT is a potentially serious condition. If not treated,
Deep Vein Thrombosis Introduction Deep vein thrombosis (DVT) is a blood clot in a vein. This condition can affect men and women of any age and race. DVT is a potentially serious condition. If not treated,
What are blood clots?
 What are blood clots? Dr Matthew Fay GP Principal The Willows Medical Practice- Queensbury GPwSI and Co-Founder Westcliffe Cardiology Service GP Partner Westcliffe Medical Group Created 5/31/18 Dr. Matthew
What are blood clots? Dr Matthew Fay GP Principal The Willows Medical Practice- Queensbury GPwSI and Co-Founder Westcliffe Cardiology Service GP Partner Westcliffe Medical Group Created 5/31/18 Dr. Matthew
Epidermiology Early pulmonary embolism
 Epidermiology Early pulmonary embolism Sitang Nirattisaikul Faculty of Medicine, Prince of Songkla University 3 rd most common cause of cardiovascular death in the United States, following ischemic heart
Epidermiology Early pulmonary embolism Sitang Nirattisaikul Faculty of Medicine, Prince of Songkla University 3 rd most common cause of cardiovascular death in the United States, following ischemic heart
Chapter 1. Introduction
 Chapter 1 Introduction Introduction 9 Even though the first reports on venous thromboembolism date back to the 13 th century and the mechanism of acute pulmonary embolism (PE) was unraveled almost 150
Chapter 1 Introduction Introduction 9 Even though the first reports on venous thromboembolism date back to the 13 th century and the mechanism of acute pulmonary embolism (PE) was unraveled almost 150
Pulmonary Embolism..Diagnostic Approach and Algorithm. Tolulope Adesiyun Harvard Medical School, Year III Gillian Lieberman, MD
 Pulmonary Embolism..Diagnostic Approach and Algorithm Tolulope Adesiyun Harvard Medical School, Year III Gillian Lieberman, MD Epidemiology of Pulmonary Embolism Pulmonary Embolus (PE): Thrombus originating
Pulmonary Embolism..Diagnostic Approach and Algorithm Tolulope Adesiyun Harvard Medical School, Year III Gillian Lieberman, MD Epidemiology of Pulmonary Embolism Pulmonary Embolus (PE): Thrombus originating
Cor pulmonale. Dr hamid reza javadi
 1 Cor pulmonale Dr hamid reza javadi 2 Definition Cor pulmonale ;pulmonary heart disease; is defined as dilation and hypertrophy of the right ventricle (RV) in response to diseases of the pulmonary vasculature
1 Cor pulmonale Dr hamid reza javadi 2 Definition Cor pulmonale ;pulmonary heart disease; is defined as dilation and hypertrophy of the right ventricle (RV) in response to diseases of the pulmonary vasculature
Acute Pulmonary Embolism SB Gupta
 Acute Pulmonary Embolism 2010 SB Gupta Pulmonary Embolism accounts for more than 650,000 cases each year and as many as 300,000 deaths annually in the US alone. PE is the 3rd most common cause acute cardiovascular
Acute Pulmonary Embolism 2010 SB Gupta Pulmonary Embolism accounts for more than 650,000 cases each year and as many as 300,000 deaths annually in the US alone. PE is the 3rd most common cause acute cardiovascular
Anticoagulants. Pathological formation of a haemostatic plug Arterial associated with atherosclerosis Venous blood stasis e.g. DVT
 Haemostasis Thrombosis Phases Endogenous anticoagulants Stopping blood loss Pathological formation of a haemostatic plug Arterial associated with atherosclerosis Venous blood stasis e.g. DVT Vascular Platelet
Haemostasis Thrombosis Phases Endogenous anticoagulants Stopping blood loss Pathological formation of a haemostatic plug Arterial associated with atherosclerosis Venous blood stasis e.g. DVT Vascular Platelet
Proper Diagnosis of Venous Thromboembolism (VTE)
") Proper Diagnosis of Venous Thromboembolism (VTE) Whal Lee, M.D. Seoul National University Hospital Department of Radiology 2 nd EFORT Asia Symposium, 3 rd November 2010, Taipei DVT - Risk Factors Previous
Proper Diagnosis of Venous Thromboembolism (VTE) Whal Lee, M.D. Seoul National University Hospital Department of Radiology 2 nd EFORT Asia Symposium, 3 rd November 2010, Taipei DVT - Risk Factors Previous
Updates in venous thromboembolism. Cecilia Becattini University of Perugia
 Updates in venous thromboembolism Cecilia Becattini University of Perugia News for VTE Diagnosis Treatment the acute phase the agents Pulmonary embolism: diagnosis Vein ultrasonography Meta-analysis 15
Updates in venous thromboembolism Cecilia Becattini University of Perugia News for VTE Diagnosis Treatment the acute phase the agents Pulmonary embolism: diagnosis Vein ultrasonography Meta-analysis 15
Venothrombotic Events: The Subtle Killer
 Venothrombotic Events: The Subtle Killer Disclosure Statement No financial or professional conflicts to report Learner Objectives Review risk factors, symptoms and subgroups of VTE Recognize medications
Venothrombotic Events: The Subtle Killer Disclosure Statement No financial or professional conflicts to report Learner Objectives Review risk factors, symptoms and subgroups of VTE Recognize medications
DVT and Pulmonary Embolus. Dr Piers Blombery BSc(Biomed), MBBS (Hons), FRACP, FRCPA Consultant Haematologist Peter MacCallum Cancer Centre
, MBBS (Hons), FRACP, FRCPA Consultant Haematologist Peter MacCallum Cancer Centre") DVT and Pulmonary Embolus Dr Piers Blombery BSc(Biomed), MBBS (Hons), FRACP, FRCPA Consultant Haematologist Peter MacCallum Cancer Centre Overview Structure of deep and superficial venous system of upper
DVT and Pulmonary Embolus Dr Piers Blombery BSc(Biomed), MBBS (Hons), FRACP, FRCPA Consultant Haematologist Peter MacCallum Cancer Centre Overview Structure of deep and superficial venous system of upper
How long to continue anticoagulation after DVT?
 How long to continue anticoagulation after DVT? Dr. Nihar Ranjan Pradhan M.S., DNB (Vascular Surgery), FVES(UK) Consultant Vascular Surgeon Apollo Hospital, Jubilee Hills, Hyderabad (Formerly Faculty in
How long to continue anticoagulation after DVT? Dr. Nihar Ranjan Pradhan M.S., DNB (Vascular Surgery), FVES(UK) Consultant Vascular Surgeon Apollo Hospital, Jubilee Hills, Hyderabad (Formerly Faculty in
Supplementary material 1. Definitions of study endpoints (extracted from the Endpoint Validation Committee Charter) 1.
 1.") Rationale, design, and baseline characteristics of the SIGNIFY trial: a randomized, double-blind, placebo-controlled trial of ivabradine in patients with stable coronary artery disease without clinical
Rationale, design, and baseline characteristics of the SIGNIFY trial: a randomized, double-blind, placebo-controlled trial of ivabradine in patients with stable coronary artery disease without clinical
Updates in Medical Management of Pulmonary Embolism and Deep Vein Thrombosis. By: Justin Youtsey, Elliott Reiff, William Montgomery, Grant Finlan
 Updates in Medical Management of Pulmonary Embolism and Deep Vein Thrombosis By: Justin Youtsey, Elliott Reiff, William Montgomery, Grant Finlan Objectives Describe the prevalence of PE and DVT as it relates
Updates in Medical Management of Pulmonary Embolism and Deep Vein Thrombosis By: Justin Youtsey, Elliott Reiff, William Montgomery, Grant Finlan Objectives Describe the prevalence of PE and DVT as it relates
THROMBOSIS AND BLEEDING
 THROMBOSIS AND BLEEDING Klara Gadó MD. PhD. Senior Professor of Internal Medicine Semmelweis University, Budapest What is thrombosis? formation of a blood clot in a blood vessel Blood can not flow Organ
THROMBOSIS AND BLEEDING Klara Gadó MD. PhD. Senior Professor of Internal Medicine Semmelweis University, Budapest What is thrombosis? formation of a blood clot in a blood vessel Blood can not flow Organ
Objectives DVT PE 5/11/2011. Venous Thromboembolism (VTE) Venous Thromboembolism (VTE) Virchow s Triad. VTE Incidence
 Venous Thromboembolism (VTE) Virchow s Triad. VTE Incidence") Objectives Current Concepts in the Diagnosis and Management of Venous Thromboembolism 1. Discuss antithrombotic treatment options for venous thromboembolism. 2. Describe the role of thrombolytic therapy
Objectives Current Concepts in the Diagnosis and Management of Venous Thromboembolism 1. Discuss antithrombotic treatment options for venous thromboembolism. 2. Describe the role of thrombolytic therapy
Venothrombotic Events: The Subtle Killer
 Venothrombotic Events: The Subtle Killer Disclosure Statement No financial or professional conflicts to report Learner Objectives Review risk factors, symptoms and subgroups of VTE Recognize medications
Venothrombotic Events: The Subtle Killer Disclosure Statement No financial or professional conflicts to report Learner Objectives Review risk factors, symptoms and subgroups of VTE Recognize medications
Diagnosis and initial treatment of patients with suspected pulmonary thromboembolism
 Diagnosis and initial treatment of patients with suspected pulmonary thromboembolism Pulmonary thromboembolism (PTE) remains a frequently occurring diagnostic problem, with an incidence of approximately
Diagnosis and initial treatment of patients with suspected pulmonary thromboembolism Pulmonary thromboembolism (PTE) remains a frequently occurring diagnostic problem, with an incidence of approximately
Deep Vein Thrombosis and Pulmonary Embolism in the Perioperative Patient
 ...PRESENTATIONS... Deep Vein Thrombosis and Pulmonary Embolism in the Perioperative Patient Based on a presentation by James E. Muntz, MD Presentation Summary Approximately 500,000 cases of deep vein
...PRESENTATIONS... Deep Vein Thrombosis and Pulmonary Embolism in the Perioperative Patient Based on a presentation by James E. Muntz, MD Presentation Summary Approximately 500,000 cases of deep vein