The Myths of Heart Failure with Preserved Ejection Fraction:
|
|
|
- Pauline Hart
- 6 years ago
- Views:
Transcription
1 The Myths of Heart Failure with Preserved Ejection Fraction: A misunderstood disease in search of a therapy Scott D. Solomon, MD The Edward D. Frohlich Distinguished Chair Professor of Medicine Harvard University Director, Noninvasive Cardiology Brigham and Women s Hospital

2 DISCLOSURES Dr. Solomon has received research Support from Abbott, Amgen, Bayer, Boston Scientific, Daichi- Sankyo, Novartis, NHLBI, NCI, and has consulted for Novartis, Bayer


3 The Two Faces of Heart Failure HFrEF HFpEF
4 Heart Failure Definition The inability to provide adequate cardiac output to the body at rest or with exertion, or to do so only in the setting of elevated cardiac filling pressures. -E. Braunwald modified by B. Borlaug and M. Redfield Clinically: A clinical syndrome characterized by breathlessness, fatigue and edema caused by an abnormality of the heart

5 Distribution of EF in Hospitalized Patients With Heart Failure OPTIMIZE-HF Registry, N=41,267 EF 40 % EF % EF 50 % Fonarow G et al. JACC. 2007; 50:
6 % Similar Signs and Symptoms in Patients with HFpEF and HFrEF HFrEF HFpEF Edema Orthop- nea PND Rest dyspnea S 3 Crackles JVP >6 cm Cardio- megaly CHARM Investigators
7 MYTH #1 HFpEF is very benign compared with HFrEF
8 Bello et al. CHARM. Circ HF 2014
9 Survival rates have improved for HFrEF, but not for HFpE F The survival rate among patients with a discharge diagnosis of HFpEF has not changed significantly over time 1 Among patients with HFrEF, the likelihood of survival increased from 1987 to Patients with reduced ejection fraction Patients with preserved ejection fraction Survival Survival p= Year 0.2 p= Year Advances in the management of patients with HFrEF have resulted in a significant extension of life expectancy, but this is not the case for patients with HFpEF Owan et al. N Engl J Med 2006;355:251 9; 2. Blanche et al. Swiss Med Wkly 2010;140:66 72

10 Myth # 2: HFpEF is a Collection of Comorbidities and NOT a Disease! HFrEF HFpEF P-value Age 71.8 ± 75.4 ± 11.5 < Hypertension % 55.1% Atrial Fibrillation 23.6% 31.8% < COPD 13.2% 17.7% Anemia 9.9% 21.1% < Bhatia et al. NEJM 2006
11 HF Hospitalization and Mortality Higher in HFpEF than in Studies of Similar Comorbidity 70 52,5 Mortality HF Hosp 35 17,5 0 ACCORD ACTION PEACE HOPE ALLHAT CHARM-P
12 MYTH #3 HFpEF is Caused by Diastolic Dysfunction
13 Age Dependence of Myocardial Relaxation Velocity in Normals Lateral E' (cm/sec) Age (Years) Henein et al. EHJ. 2002;23:
14 High Prevalence of Diastolic Dysfunction Regardless of Clinical Status 50 E = 7.5 ± 1.9, E/E = 9.1 ± 3.0 NT-proBNP = 90 (83,97) E = 6.9 ± 1.9, E/E = 10.2 ± 3.8 NT-proBNP = 120 (116, 123) E = 6.7 ± 1.9, E/E = 11.2 ± 4.7 NT-proBNP = 209 (188, 232) , , ,5 1,6 2,3 Healthy n = 371 Co-Morbid n = 4,555 HFpEF n = 474 No DM, HTN, CHD, HF Normal Mild DD Moderate DD Shah et al AHA 2012
15 Diastolic Dysfunction is Ubiquitous with Aging and Cannot Account for HFpEF




16 Myth # 5: Systolic Function is Normal in HFpEF Longitudinal Strain most likely represents Function of subendocardial myofiber bands Shah A. & Solomon SD. Myocardial Deformation Imaging. Circulation 2012
17 Myocardial Strain in Normals, HTN, HFpEF and HFrEF Myocardial Strain (%) Normal (n=50) Hypertension and Diastolic dysfunction (n=300) 1 Kraigher-Krainer E, JACC Knappe D, Circ HF TOPCAT Unpublished No HF HFpEF HFrEF PARAMOUNT 1 (n=~200) TOPCAT 3 (n=~438) Longitudinal Strain Circumferential Strain MADIT-CRT 2 (n=1077)
18 GLS was the BEST Predictor of Outcome in HFpEF in TOPCAT Trial Univariate Multivariate Age P < P = E/E' P < P = LV Mass P < P = Global Longitudinal Strain P < P = Left Atrial Volume P = P = LVEF P = P = Hazard Ratio for Primary Outcome (per 1 SD) TOPCAT Unpublished Data
19 MYTH #5 There is no Evidenced Based Treatment for HFpEF

20 THIS ONE IS TRUE!

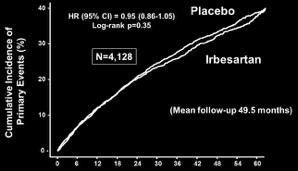
21 Outcomes Trials in HFpEF CHARM-Preserved PEP-CHF I-PRESERVE TOPCAT
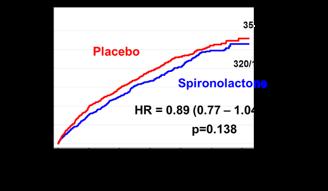
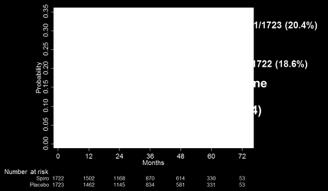
 Placebo Spironolactone HR = 0.89 (0.77 1.04) p=0.138 320/1722 (18.6%) Pfeffer et al.")
22 TOPCAT: 1 Outcome (CV Death, HF Hosp, or Resuscitated Cardiac Arrest) 351/1723 (20.4%) Placebo Spironolactone HR = 0.89 ( ) p= /1722 (18.6%) Pfeffer et al. NEJM 2014;370(15):
 Russia, Rep Georgia HR=1.10 (0.79-1.51) Pfeffer MA et al. Circulation.")
23 TOPCAT: Results by Region US, Canada, Argentina, Brazil HR=0.82 ( ) Placebo: 280/881 (31.8%) Interaction p=0.122 Placebo: 71/842 (8.4%) Russia, Rep Georgia HR=1.10 ( ) Pfeffer MA et al. Circulation Jan 6;131(1):34-42

24 TOPCAT: Benefit of Spironolactone Diminishes with Increasing Ejection Fraction Primary Outcome HF Hospitalization Solomon SD et al. Eur Heart J. 2015

25 2012 ESC Guidelines for Heart Failure Treatment No treatment has yet been shown, convincingly, to reduce morbidity and mortality in patients with HF-PEF. Diuretics are used to control sodium and water retention and relieve breathlessness and oedema as in HF-REF. Adequate treatment of hypertension and myocardial ischaemia is also considered to be important, as is control of the ventricular rate in patients with AF (see Section
26 Current Treatment of HFpEF Symptomatic Treatment with Diuretics Treatment of Hypertension Rate control in Atrial Fibrillation (? Maintain SR) Treat Ischemia? Spironolactone
27 Soluble Guanylate Cyclase stimulator Heart Failure Studies: The SOCRATES Program Design SOCRATES-REDUCED SOCRATES-PRESERVED 2 Phase II, randomized, parallel-group, placebo-controlled, doubleblind, dose finding phase IIb studies of 4 dose regimens of the oral sgc stimulator vericiguat over 12 weeks Inclusion Criteria Primary Outcome Worsening chronic heart failure requiring hospitalization (or IV diuretic for HF) with initiation after clinical stabilization LVEF <45% NT-proBNP at 12 weeks LVEF 45% Left atrial (LA) enlargement NT-proBNP / LA vol. at 12 weeks (split α: each p<0.025) Enrollment 410 patients in 5 arms 470 patients in 5 arms Study status FPFV Nov 29, 2013 FPFV Nov 6, 2013 CT.gov ID NCT NCT


28 SOCRATES-Preserved: Primary Results No reduction in log-nt-probnp or in LAV at week 12 compared with placebo Placebo 1.25 mg 2.5 mg 2.5 to 5 mg 2.5 to 10 mg Pooled 2.5/5/10 mg Change in left atrial volume (ml) Placebo 1.25 mg 2.5 mg 2.5 to 5 mg 2.5 to 10 mg Pooled 2.5/5/10 mg 0.20 Placebo 1.25 mg 2.5 mg 2.5 to 5 mg 2.5 to 10 mg Pooled dose groups 6 Data are mean ± standard error for the per-protocol analysis sets
 vs.")
29 NEAT-HFpEF: No Difference in Primary or Secondary Endpoints (including 6 min walk, QOL, NT-proBNP) Isosorbide Mononitrate with dose up-titration (30 to 120 mg/day over 4 weeks) vs. placebo in crossover design
 ANP BNP CNP Adrenomedullin Bradykinin Substance P (angiotensin II) Vasodilation! blood pressure! sympathetic tone!aldosterone levels! fibrosis!")
30 LCZ696 A first-in-class Angiotensin Receptor Neprilysin Inhibitor Simultaneously Inhibits NEP and the RAS Vasoactive Peptide System pro-bnp LCZ696 Heart Failure Renin Angiotensin System Angiotensinogen (liver secretion) ANP BNP CNP Adrenomedullin Bradykinin Substance P (angiotensin II) Vasodilation! blood pressure! sympathetic tone!aldosterone levels! fibrosis! hypertrophy Natriuresis/Diuresis NT-pro BNP Neprilysin X Inactive fragments Sacubitril (AHU377) LBQ657 O HO HN O OH O LCZ696 is a novel crystalline complex consisting of the molecular moieties of valsartan and sacubitril in an equimolar ratio Valsartan O N N N N O OH NH X Angiotensin I Angiotensin II AT 1 receptor Vasoconstriction " blood pressure " sympathetic tone " aldosterone " fibrosis " hypertrophy
31 PARAMOUNT: Study Design Placebo run-in Discontinue ACEI or ARB therapy one day prior to randomization LCZ mg BID Valsartan 40 mg BID LCZ mg BID Valsartan 80 mg BID 301 patients randomized LCZ mg BID Valsartan 160 mg BID Prior ACEi/ARB use discontinued Week Visit weeks week 1 week 10 weeks month extension Primary objective NT pro-bnp reduction from baseline at 12 weeks Secondary objectives Echocardiographic measures of diastolic function, left atrial size, LV size and function, PASP HF symptoms, Clinical composite assessment and Quality of life (KCCQ) Safety and tolerability Baseline randomization visit and visit at end of 12 weeks of core study Clinicaltrials.gov NCT Solomon et al. ESC Hotline 2012 Lancet 2012
32 PARAMOUNT: Significant Improvement in Several Domains Improvement in NT-proBNP Improvement in Left Atrial Size NTproBNP (pg/ml) (733,1012) 835 (710, 981) 783 (670,914) p = Valsartan LCZ696 LCZ696/Valsartan: 0.77 (0.64, 0.92) P = (512, 714) Change in Left Atrial Volume (ml) Weeks 36 Weeks P = 0.18 P = Weeks Post Randomization Improvement in NYHA Class W U LCZ696 Valsartan Solomon et al. Lancet 2012
33 Target patient population: 4,600 patients with symptomatic HF (NYHA Class II IV) and LVEF 45% Randomization 1:1 Double-blind treatment period Screening Active run-in period Valsartan 80 mg BID* LCZ mg BID LCZ mg BID Valsartan 160 mg BID On top of optimal background medications for co-morbidities (excluding ACEIs and ARBs) up to 2 weeks 3 8 weeks ~240 weeks Primary outcome: CV death and total (first and recurrent) HF hospitalizations (anticipated ~1,721 primary events) Steering Cmt: S. Solomon, co-chair, J. McMurray, Co-Chair, I. Anand, F. Zannad, A. Maggioni, M. Packer, M. Zile, B. Pieske, J. Rouleau, M. Redfield, C. Lam, D. Van Veldhuisen, F. Martinez, J. Ge, H. Krum, M. Pfeffer
34 SPRINT: BP Lowering Reduces Adverse Outcomes HF Hospitalization Reduced 38% SPRINT Investigators. N Engl J Med 2015
35 Heart Failure Hospitalizations Reduced Substantial with the SGLT-2 Inhibitor Empaglifozin Fitchett et al. Eur Heart J 2016

36 Effect of Exercise Training on Measures of Diastolic Function Edelmann F. Pieske B JACC 2011
37
38 FAIR-HFpEF Design Design: Multicentre, randomized (1:1), double-blind, placebo-controlled Main inclusion criteria: NYHA class II / III, LVEF 45% SR: BNP/NT-proBNP >100/>300 pg/ml or MRproANP>120 mmol/l (if in AF, twice) 6MWT < 450m Iron deficiency: serum ferritin <100 µg/l or TSAT <20% Hb: g/dL FCM up to 2000mg (2x1000mg) Treatment continues if ID is not corrected Screening R n=200 1 EP: 6MWT Placebo D0 W4 W12 W20 W24 Primary endpoint Change in 6MWT at week 24 Secondary endpoints Change in biomarkers for iron deficiency, renal function, cardiac function, NYHA functional class, PGA and QoL Overall safety over the treatment period
39 Inter-Atrial Shunt Device - Concept Abnormal LV relaxation results in elevated Left Atrial Pressure (LAP) and pulmonary edema Transcatheter implant to create a small 1 permanent interatrial shunt Shunt allows blood to move from the higher pressure LA to the lower pressure more compliant right side, reducing LAP without compromising LV cardiac output 1 Qp:Qs ratio (Pulmonary to Systemic flow ratio):
 Pulmonary edema, Dyspnea at rest/exercise 1 PCWP at rest is predictor of mortality")
40 Inter-Atrial Shunt Device 1 - MOA Hypothesis Elevated LV filling pressures (Elevated LAP) X Pulmonary Venous hypertension (Elevated PCWP 1 ) Pulmonary edema, Dyspnea at rest/exercise 1 PCWP at rest is predictor of mortality (Dorfs, EHJ 2014)
41 6 months Effectiveness endpoints 41 Hasenfuβ, et al The Lancet Vol 387 March 26, 2016

42 6 months Efficacy Endpoints 42 Hasenfuβ, et al The Lancet Vol 387 March 26, 2016
43
44 Conclusions HFpEF is alive, and not well. It is a heterogeneous disorder, associated with comborbidities but accounts for half of heart failure The cardiac phenotype is broader than we previously thought Diastolic dysfunction CANNOT account for the disorder and abnormalities of systole are becoming more recognized There is no evidenced-based therapy currently, but there are promising potential therapies being tested
LCZ696 A First-in-Class Angiotensin Receptor Neprilysin Inhibitor
 The Angiotensin Receptor Neprilysin Inhibitor LCZ696 in Heart Failure with Preserved Ejection Fraction The Prospective comparison of ARNI with ARB on Management Of heart failure with preserved ejection
The Angiotensin Receptor Neprilysin Inhibitor LCZ696 in Heart Failure with Preserved Ejection Fraction The Prospective comparison of ARNI with ARB on Management Of heart failure with preserved ejection
HFpEF 2016 : Comorbidities and Outcomes
 HFpEF 2016 : Comorbidities and Outcomes Christopher M. O Connor, MD, FACC CEO and Executive Director, Inova Heart and Vascular Institute Professor of Medicine, Duke University Editor in Chief, JACC: Heart
HFpEF 2016 : Comorbidities and Outcomes Christopher M. O Connor, MD, FACC CEO and Executive Director, Inova Heart and Vascular Institute Professor of Medicine, Duke University Editor in Chief, JACC: Heart
Heart Failure with Preserved EF (HFPEF) Epidemiology and management
 Epidemiology and management") Heart Failure with Preserved EF (HFPEF) Epidemiology and management Karl Swedberg Senior Professor of Medicine Sahlgrenska Academy University of Gothenburg Gothenburg, Sweden e-mail: karl.swedberg@gu.se
Heart Failure with Preserved EF (HFPEF) Epidemiology and management Karl Swedberg Senior Professor of Medicine Sahlgrenska Academy University of Gothenburg Gothenburg, Sweden e-mail: karl.swedberg@gu.se
Entresto Development of sacubitril/valsartan (LCZ696) for the treatment of heart failure with reduced ejection fraction
 for the treatment of heart failure with reduced ejection fraction") Cardio-Metabolic Franchise Entresto Development of sacubitril/valsartan (LCZ696) for the treatment of heart failure with reduced ejection fraction Randy L Webb, PhD Rutgers Workshop October 21, 2016 Heart
Cardio-Metabolic Franchise Entresto Development of sacubitril/valsartan (LCZ696) for the treatment of heart failure with reduced ejection fraction Randy L Webb, PhD Rutgers Workshop October 21, 2016 Heart
Therapeutic Targets and Interventions
 Therapeutic Targets and Interventions Ali Valika, MD, FACC Advanced Heart Failure and Pulmonary Hypertension Advocate Medical Group Midwest Heart Foundation Disclosures: 1. Novartis: Speaker Honorarium
Therapeutic Targets and Interventions Ali Valika, MD, FACC Advanced Heart Failure and Pulmonary Hypertension Advocate Medical Group Midwest Heart Foundation Disclosures: 1. Novartis: Speaker Honorarium
Disclosures. Overview. Goal statement. Advances in Chronic Heart Failure Management 5/22/17
 Disclosures Advances in Chronic Heart Failure Management I have nothing to disclose Van N Selby, MD UCSF Advanced Heart Failure Program May 22, 2017 Goal statement To review recently-approved therapies
Disclosures Advances in Chronic Heart Failure Management I have nothing to disclose Van N Selby, MD UCSF Advanced Heart Failure Program May 22, 2017 Goal statement To review recently-approved therapies
Disclosure of Relationships
 Disclosure of Relationships Over the past 12 months Dr Ruilope has served as Consultant and Speakers Bureau member of Astra-Zeneca, Bayer, Daiichi-Sankyo, Menarini, Novartis, Otsuka, Pfizer, Relypsa, Servier
Disclosure of Relationships Over the past 12 months Dr Ruilope has served as Consultant and Speakers Bureau member of Astra-Zeneca, Bayer, Daiichi-Sankyo, Menarini, Novartis, Otsuka, Pfizer, Relypsa, Servier
Drugs acting on the reninangiotensin-aldosterone
 Drugs acting on the reninangiotensin-aldosterone system John McMurray Eugene Braunwald Scholar in Cardiovascular Diseases, Brigham and Women s Hospital, Boston & Visiting Professor, Harvard Medical School
Drugs acting on the reninangiotensin-aldosterone system John McMurray Eugene Braunwald Scholar in Cardiovascular Diseases, Brigham and Women s Hospital, Boston & Visiting Professor, Harvard Medical School
Heart Failure with preserved ejection fraction (HFpEF)
") Heart Failure with preserved ejection fraction (HFpEF) Dr. Pierpaolo Pellicori Hull York Medical School Kingston-upon-Hull United Kingdom Conflict of interest: none Heart failure is a contemporary problem
Heart Failure with preserved ejection fraction (HFpEF) Dr. Pierpaolo Pellicori Hull York Medical School Kingston-upon-Hull United Kingdom Conflict of interest: none Heart failure is a contemporary problem
Disclosures. Advances in Chronic Heart Failure Management 6/12/2017. Van N Selby, MD UCSF Advanced Heart Failure Program June 19, 2017
 Advances in Chronic Heart Failure Management Van N Selby, MD UCSF Advanced Heart Failure Program June 19, 2017 I have nothing to disclose Disclosures 1 Goal statement To review recently-approved therapies
Advances in Chronic Heart Failure Management Van N Selby, MD UCSF Advanced Heart Failure Program June 19, 2017 I have nothing to disclose Disclosures 1 Goal statement To review recently-approved therapies
Outline. Classification by LVEF Conventional Therapy New Therapies. Ivabradine Sacubitril/valsartan
 New Pharmacological Therapies for Heart Failure Mark Drazner, MD, MSc Clinical Chief of Cardiology Medical Director, CHF/VAD/Transplant James M. Wooten Chair in Cardiology UT Southwestern Medical Center
New Pharmacological Therapies for Heart Failure Mark Drazner, MD, MSc Clinical Chief of Cardiology Medical Director, CHF/VAD/Transplant James M. Wooten Chair in Cardiology UT Southwestern Medical Center
Satish K Surabhi, MD.FACC,FSCAI,RPVI Medical Director, Cardiac Cath Labs AnMed Health Heart & Vascular Care
 Satish K Surabhi, MD.FACC,FSCAI,RPVI Medical Director, Cardiac Cath Labs AnMed Health Heart & Vascular Care None Fig. 1. Progression of Heart Failure.With each hospitalization for acute heart failure,
Satish K Surabhi, MD.FACC,FSCAI,RPVI Medical Director, Cardiac Cath Labs AnMed Health Heart & Vascular Care None Fig. 1. Progression of Heart Failure.With each hospitalization for acute heart failure,
HFpEF, Mito or Realidad?
 HFpEF, Mito or Realidad? Ileana L. Piña, MD, MPH Professor of Medicine and Epidemiology/Population Health Associate Chief for Academic Affairs -- Cardiology Montefiore-Einstein Medical Center Bronx, NY
HFpEF, Mito or Realidad? Ileana L. Piña, MD, MPH Professor of Medicine and Epidemiology/Population Health Associate Chief for Academic Affairs -- Cardiology Montefiore-Einstein Medical Center Bronx, NY
HF-Preserved Ejection Fraction
 HF-Preserved Ejection Fraction Justin A. Ezekowitz, MBBCh MSc FRCPC FACC FESC FAHA Associate Professor, University of Alberta Co-Director, Canadian VIGOUR Centre Cardiologist, Mazankowski Alberta Heart
HF-Preserved Ejection Fraction Justin A. Ezekowitz, MBBCh MSc FRCPC FACC FESC FAHA Associate Professor, University of Alberta Co-Director, Canadian VIGOUR Centre Cardiologist, Mazankowski Alberta Heart
Disclosures for Presenter
 A Comparison of Angiotensin Receptor- Neprilysin Inhibition (ARNI) With ACE Inhibition in the Long-Term Treatment of Chronic Heart Failure With a Reduced Ejection Fraction Milton Packer, John J.V. McMurray,
A Comparison of Angiotensin Receptor- Neprilysin Inhibition (ARNI) With ACE Inhibition in the Long-Term Treatment of Chronic Heart Failure With a Reduced Ejection Fraction Milton Packer, John J.V. McMurray,
Overview & Update on the Utilization of the Natriuretic Peptides in Heart Failure
 June 28, 2016 Overview & Update on the Utilization of the Natriuretic Peptides in Heart Failure Linda C. Rogers, PhD, DABCC, FACB. Agenda Overview of the Natriuretic Peptides and Efficacy studies Similarities
June 28, 2016 Overview & Update on the Utilization of the Natriuretic Peptides in Heart Failure Linda C. Rogers, PhD, DABCC, FACB. Agenda Overview of the Natriuretic Peptides and Efficacy studies Similarities
ACE inhibitors: still the gold standard?
 ACE inhibitors: still the gold standard? Session: Twenty-five years after CONSENSUS What have we learnt about the RAAS in heart failure? Lars Køber, MD, D.Sci Department of Cardiology Rigshospitalet University
ACE inhibitors: still the gold standard? Session: Twenty-five years after CONSENSUS What have we learnt about the RAAS in heart failure? Lars Køber, MD, D.Sci Department of Cardiology Rigshospitalet University
From PARADIGM-HF to Clinical Practice. Waleed AlHabeeb, MD, MHA Associate Professor of Medicine President of the Saudi Heart Failure Group
 From PARADIGM-HF to Clinical Practice Waleed AlHabeeb, MD, MHA Associate Professor of Medicine President of the Saudi Heart Failure Group PARADIGM-HF: Inclusion Criteria Chronic HF NYHA FC II IV with LVEF
From PARADIGM-HF to Clinical Practice Waleed AlHabeeb, MD, MHA Associate Professor of Medicine President of the Saudi Heart Failure Group PARADIGM-HF: Inclusion Criteria Chronic HF NYHA FC II IV with LVEF
Ejection Fraction in Patients With Chronic Heart Failure. Diastolic Heart Failure or Heart Failure with Preserved Ejection Fraction
 Diastolic Heart Failure or Heart Failure with Preserved Ejection Fraction Keith Miller MD Diastolic Heart Failure Risk Factors Common Risk Factors Aging Female gender Obesity Hypertension Diabetes mellitus
Diastolic Heart Failure or Heart Failure with Preserved Ejection Fraction Keith Miller MD Diastolic Heart Failure Risk Factors Common Risk Factors Aging Female gender Obesity Hypertension Diabetes mellitus
Diagnosis is it really Heart Failure?
 ESC Congress Munich - 25-29 August 2012 Heart Failure with Preserved Ejection Fraction From Bench to Bedside Diagnosis is it really Heart Failure? Prof. Burkert Pieske Department of Cardiology Med.University
ESC Congress Munich - 25-29 August 2012 Heart Failure with Preserved Ejection Fraction From Bench to Bedside Diagnosis is it really Heart Failure? Prof. Burkert Pieske Department of Cardiology Med.University
Highlight Session Heart failure and cardiomyopathies Michel KOMAJDA Paris France
 Highlight Session 2014 Heart failure and cardiomyopathies Michel KOMAJDA Paris France # esccongress www.escardio.org/esc2014 HEART FAILURE AND CARDIOMYOPATHIES TOPIC 1 Drug Therapy TOPIC 2 Device Therapy
Highlight Session 2014 Heart failure and cardiomyopathies Michel KOMAJDA Paris France # esccongress www.escardio.org/esc2014 HEART FAILURE AND CARDIOMYOPATHIES TOPIC 1 Drug Therapy TOPIC 2 Device Therapy
2/15/2017. Disclosures. Heart Failure = Big Problem. Heart Failure Update Reducing Hospitalizations and Improving Patient Outcomes 02/18/2017
 Heart Failure Update Reducing Hospitalizations and Improving Patient Outcomes 02/18/2017 Julio A. Barcena, M.D. South Miami Heart Specialists Disclosures I have no relevant commercial relationships to
Heart Failure Update Reducing Hospitalizations and Improving Patient Outcomes 02/18/2017 Julio A. Barcena, M.D. South Miami Heart Specialists Disclosures I have no relevant commercial relationships to
Updates in Congestive Heart Failure
 Updates in Congestive Heart Failure GREGORY YOST, DO JOHNSTOWN CARDIOVASCULAR ASSOCIATES 1/28/2018 Disclosures Edwards speaker on Sapien3 valves (TAVR) Stages A-D and NYHA Classes I-IV Stage A: High risk
Updates in Congestive Heart Failure GREGORY YOST, DO JOHNSTOWN CARDIOVASCULAR ASSOCIATES 1/28/2018 Disclosures Edwards speaker on Sapien3 valves (TAVR) Stages A-D and NYHA Classes I-IV Stage A: High risk
HFpEF: How to optimise management
 HFpEF: How to optimise management Burkert Pieske M.D. Berlin, Germany Department of Internal Medicine and Cardiology, Campus Virchow Klinikum, Charité University Medicine Berlin, and Department of Internal
HFpEF: How to optimise management Burkert Pieske M.D. Berlin, Germany Department of Internal Medicine and Cardiology, Campus Virchow Klinikum, Charité University Medicine Berlin, and Department of Internal
THE PROPER APPROACH TO DIAGNOSING HEART FAILURE WITH PRESERVED EJECTION FRACTION
 THE PROPER APPROACH TO DIAGNOSING HEART FAILURE WITH PRESERVED EJECTION FRACTION James C. Fang, MD, FACC Professor and Chief Cardiovascular Division University of Utah School of Medicine Disclosures Data
THE PROPER APPROACH TO DIAGNOSING HEART FAILURE WITH PRESERVED EJECTION FRACTION James C. Fang, MD, FACC Professor and Chief Cardiovascular Division University of Utah School of Medicine Disclosures Data
HF-PEF: Symptoms, quality of life and mortality/morbidity
 HF-PEF: Symptoms, quality of life and mortality/morbidity May 21, 2011 John McMurray, MD Eugene Braunwald Scholar in Cardiovascular Diseases, Brigham & Women s Hospital Boston; Visiting Professor of Medicine,
HF-PEF: Symptoms, quality of life and mortality/morbidity May 21, 2011 John McMurray, MD Eugene Braunwald Scholar in Cardiovascular Diseases, Brigham & Women s Hospital Boston; Visiting Professor of Medicine,
New horizons in HF: potential of new drugs
 New horizons in HF: potential of new drugs Marc A. Pfeffer, MD, PhD Dzau Professor of Medicine, Harvard Medical School Cardiovascular Division, Brigham & Women s Hospital Boston, Massachusetts FINANCIAL
New horizons in HF: potential of new drugs Marc A. Pfeffer, MD, PhD Dzau Professor of Medicine, Harvard Medical School Cardiovascular Division, Brigham & Women s Hospital Boston, Massachusetts FINANCIAL
HeFSSA Practitioners Program 2017 Theme The Patient Journey: Feel Good and Live Long. Case Study 2
 HeFSSA Practitioners Program 2017 Theme The Patient Journey: Feel Good and Live Long Case Study 2 HEART FAILURE WITH MID-RANGE EJECTION FRACTION TREATMENT OPTIONS CLINICAL CASE MEDICAL HISTORY 59-year-old
HeFSSA Practitioners Program 2017 Theme The Patient Journey: Feel Good and Live Long Case Study 2 HEART FAILURE WITH MID-RANGE EJECTION FRACTION TREATMENT OPTIONS CLINICAL CASE MEDICAL HISTORY 59-year-old
Learning Objectives. Heart Failure (HF): Scope of the Problem. Temporal Trends in Age-Adjusted Survival After HF Diagnosis
: Scope of the Problem. Temporal Trends in Age-Adjusted Survival After HF Diagnosis") 7:5 :5 am Update in Heart Failure SPEAKER Orly Vardeny, PharmD, MS Presenter Disclosure Information The following relationships exist related to this presentation: Orly Vardeny, PharmD, MS: Advisory Board
7:5 :5 am Update in Heart Failure SPEAKER Orly Vardeny, PharmD, MS Presenter Disclosure Information The following relationships exist related to this presentation: Orly Vardeny, PharmD, MS: Advisory Board
Treating HF Patients with ARNI s Why, When and How?
 Treating HF Patients with ARNI s Why, When and How? 19 th Annual San Diego Heart Failure Symposium for Primary Care Physicians January 11-12, 2019 La Jolla, CA Barry Greenberg M.D. Distinguished Professor
Treating HF Patients with ARNI s Why, When and How? 19 th Annual San Diego Heart Failure Symposium for Primary Care Physicians January 11-12, 2019 La Jolla, CA Barry Greenberg M.D. Distinguished Professor
Management of chronic heart failure: update J. Parissis Attikon University Hospital
 Management of chronic heart failure: update 2015 J. Parissis Attikon University Hospital Disclosures: received honoraria for lectures from Servier, Pfizer, Novartis Discharges in Thousands Heart Failure
Management of chronic heart failure: update 2015 J. Parissis Attikon University Hospital Disclosures: received honoraria for lectures from Servier, Pfizer, Novartis Discharges in Thousands Heart Failure
UPDATES IN MANAGEMENT OF HF
 UPDATES IN MANAGEMENT OF HF Jennifer R Brown MD, MS Heart Failure Specialist Medstar Cardiology Associates DC ACP Meeting Fall 2017 Disclosures: speaker bureau for novartis speaker bureau for actelion
UPDATES IN MANAGEMENT OF HF Jennifer R Brown MD, MS Heart Failure Specialist Medstar Cardiology Associates DC ACP Meeting Fall 2017 Disclosures: speaker bureau for novartis speaker bureau for actelion
Heart Failure (HF): Scope of the Problem. Temporal Trends in Age-Adjusted Survival After HF Diagnosis. More malignant than cancer
: Scope of the Problem. Temporal Trends in Age-Adjusted Survival After HF Diagnosis. More malignant than cancer") Patients in US (millions) Heart Failure (HF): Scope of the Problem 1 8 6 4 2 3.5 4.8 1. 1991 21 237 US prevalence*: 5.8 million US annual incidence: 67, Annual mortality: 282,754 5-1% depending on severity
Patients in US (millions) Heart Failure (HF): Scope of the Problem 1 8 6 4 2 3.5 4.8 1. 1991 21 237 US prevalence*: 5.8 million US annual incidence: 67, Annual mortality: 282,754 5-1% depending on severity
Treatment Of Preserved Cardiac Function Heart Failure with an Aldosterone antagonist (TOPCAT) AHA Nov 18, 2014 Update on Randomized Trials
 AHA Nov 18, 2014 Update on Randomized Trials") Treatment Of Preserved Cardiac Function Heart Failure with an Aldosterone antagonist (TOPCAT) AHA Nov 18, 2014 Update on Randomized Trials Marc A. Pfeffer, MD, PhD; Brian Claggett, PhD; Susan F. Assmann,
Treatment Of Preserved Cardiac Function Heart Failure with an Aldosterone antagonist (TOPCAT) AHA Nov 18, 2014 Update on Randomized Trials Marc A. Pfeffer, MD, PhD; Brian Claggett, PhD; Susan F. Assmann,
Update on pharmacological treatment of heart failure. Aldo Pietro Maggioni, MD, FESC ANMCO Research Center Firenze, Italy
 Update on pharmacological treatment of heart failure Aldo Pietro Maggioni, MD, FESC ANMCO Research Center Firenze, Italy Presenter Disclosures Dr. Maggioni : Serving in Committees of studies sponsored
Update on pharmacological treatment of heart failure Aldo Pietro Maggioni, MD, FESC ANMCO Research Center Firenze, Italy Presenter Disclosures Dr. Maggioni : Serving in Committees of studies sponsored
INIBITORI NEPRILISINA
 INIBITORI NEPRILISINA Marco Canepa, MD, PhD Università degli Studi di Genova Cardiologia, Ospedale Policlinico San Martino IRCCS marco.canepa@unige.it ARNI: ANGIOTENSIN RECEPTOR NEPRILYSIN INHIBITORS
INIBITORI NEPRILISINA Marco Canepa, MD, PhD Università degli Studi di Genova Cardiologia, Ospedale Policlinico San Martino IRCCS marco.canepa@unige.it ARNI: ANGIOTENSIN RECEPTOR NEPRILYSIN INHIBITORS
Mihai Gheorghiade MD
 Mihai Gheorghiade MD Center for Cardiovascular Innovation, Northwestern University Feinberg School of Medicine, Chicago, Illinois On behalf of: Stephen J Greene MD; Javed Butler MD MPH MBA; Gerasimos Filippatos
Mihai Gheorghiade MD Center for Cardiovascular Innovation, Northwestern University Feinberg School of Medicine, Chicago, Illinois On behalf of: Stephen J Greene MD; Javed Butler MD MPH MBA; Gerasimos Filippatos
Pravin Manga Division of Cardiology Department of Medicine University of Witwatersrand
 Pravin Manga Division of Cardiology Department of Medicine University of Witwatersrand Overview Definition Epidemiology Biomarkers Treatment Clinical Heart Failure: Syndrome in which patients have typical
Pravin Manga Division of Cardiology Department of Medicine University of Witwatersrand Overview Definition Epidemiology Biomarkers Treatment Clinical Heart Failure: Syndrome in which patients have typical
AHA Nov 18, 2013 Late Breaking Session
 Treatment Of Preserved Cardiac Function Heart Failure with an Aldosterone antagonist (TOPCAT) AHA Nov 18, 2013 Late Breaking Session Marc A. Pfeffer MD, PhD, on behalf of the TOPCAT Investigators TOPCAT
Treatment Of Preserved Cardiac Function Heart Failure with an Aldosterone antagonist (TOPCAT) AHA Nov 18, 2013 Late Breaking Session Marc A. Pfeffer MD, PhD, on behalf of the TOPCAT Investigators TOPCAT
ESC Guidelines for the Diagnosis and Treatment of Chronic Heart Failure
 ESC Guidelines for the Diagnosis and Treatment of Chronic Heart Failure - 2005 Karl Swedberg Professor of Medicine Department of Medicine Sahlgrenska University Hospital/Östra Göteborg University Göteborg
ESC Guidelines for the Diagnosis and Treatment of Chronic Heart Failure - 2005 Karl Swedberg Professor of Medicine Department of Medicine Sahlgrenska University Hospital/Östra Göteborg University Göteborg
ANGIOTENSIN RECEPTOR-NEPRILYSIN INHIBITORS IN HEART FAILURE FROM CHD
 ANGIOTENSIN RECEPTOR-NEPRILYSIN INHIBITORS IN HEART FAILURE FROM CHD Karen Stout, MD FACC Professor, Medicine/Pediatrics University of Washington Seattle, WA USA No disclosures Case 35 year old man with
ANGIOTENSIN RECEPTOR-NEPRILYSIN INHIBITORS IN HEART FAILURE FROM CHD Karen Stout, MD FACC Professor, Medicine/Pediatrics University of Washington Seattle, WA USA No disclosures Case 35 year old man with
2017 Summer MAOFP Update
 2017 Summer MAOFP Update. Cardiology Update 2017 Landmark Trials Change Practice Guidelines David J. Strobl, DO, FNLA Heart Failure: Epidemiology More than 4 million patients affected 400,000 new cases
2017 Summer MAOFP Update. Cardiology Update 2017 Landmark Trials Change Practice Guidelines David J. Strobl, DO, FNLA Heart Failure: Epidemiology More than 4 million patients affected 400,000 new cases
Systolic and Diastolic Dysfunction: Four Upcoming Challenges
 Systolic and Diastolic Dysfunction: Four Upcoming Challenges Promoting Early Detection HFrEF: Beyond Neprilysin/Enalapril HFmrEF: What Is It and How Does One Manage It? HFpEF: Etiopathogenetic Role and
Systolic and Diastolic Dysfunction: Four Upcoming Challenges Promoting Early Detection HFrEF: Beyond Neprilysin/Enalapril HFmrEF: What Is It and How Does One Manage It? HFpEF: Etiopathogenetic Role and
LCZ696: LA NUOVA RIVOLUZIONE NELLA TERAPIA DELLO SCOMPENSO CARDIACO. Dario Leosco Università di Napoli Federico II
 LCZ696: LA NUOVA RIVOLUZIONE NELLA TERAPIA DELLO SCOMPENSO CARDIACO Dario Leosco Università di Napoli Federico II Projected changes in cardiovascular diseases CVD Deaths Increase 33% CVD DALYS 22% CAD
LCZ696: LA NUOVA RIVOLUZIONE NELLA TERAPIA DELLO SCOMPENSO CARDIACO Dario Leosco Università di Napoli Federico II Projected changes in cardiovascular diseases CVD Deaths Increase 33% CVD DALYS 22% CAD
Behandeling van Hartfalen: over 5 jaar
 Behandeling van Hartfalen: over 5 jaar Adriaan Voors, cardioloog UMCG Over 5 jaar Heart Failure Treatment in 5 Years HFrEF: best evidence, biggest pipeline Entresto Omcamtiv LVAD: destination therapy HFrEF:
Behandeling van Hartfalen: over 5 jaar Adriaan Voors, cardioloog UMCG Over 5 jaar Heart Failure Treatment in 5 Years HFrEF: best evidence, biggest pipeline Entresto Omcamtiv LVAD: destination therapy HFrEF:
WHAT S NEW IN HEART FAILURE
 WHAT S NEW IN HEART FAILURE Drugs, Devices and Diagnostics John M. Herre, MD, FACC, FACP Director, Advanced Heart Failure Program Sentara Helathcare Professor of Medicine Eastern Virginia Medical School
WHAT S NEW IN HEART FAILURE Drugs, Devices and Diagnostics John M. Herre, MD, FACC, FACP Director, Advanced Heart Failure Program Sentara Helathcare Professor of Medicine Eastern Virginia Medical School
ECG in CRT patients & novel HF therapies. Δημήτριος M. Κωνσταντίνου Ειδικός Καρδιολόγος, MD, MSc, PhD, CCDS Πανεπιστημιακός Υπότροφος
 ECG in CRT patients & novel HF therapies Δημήτριος M. Κωνσταντίνου Ειδικός Καρδιολόγος, MD, MSc, PhD, CCDS Πανεπιστημιακός Υπότροφος Dr. Konstantinou has received grants from Medtronic Is identification
ECG in CRT patients & novel HF therapies Δημήτριος M. Κωνσταντίνου Ειδικός Καρδιολόγος, MD, MSc, PhD, CCDS Πανεπιστημιακός Υπότροφος Dr. Konstantinou has received grants from Medtronic Is identification
Heart Failure Update. Bibiana Cujec MD May 2015
 Heart Failure Update Bibiana Cujec MD May 2015 Disclosures Participation in clinical trial GUIDE IT (BNP in management of HF) Plan Review of new trials/ccs guidelines Management of heart failure: cases
Heart Failure Update Bibiana Cujec MD May 2015 Disclosures Participation in clinical trial GUIDE IT (BNP in management of HF) Plan Review of new trials/ccs guidelines Management of heart failure: cases
The ACC Heart Failure Guidelines
 The ACC Heart Failure Guidelines Fakhr Alayoubi, Msc,R Ph President of SCCP Cardiology Clinical Pharmacist Assistant Professor At King Saud University King Khalid University Hospital Riyadh-KSA 2017 ACC/AHA/HFSA
The ACC Heart Failure Guidelines Fakhr Alayoubi, Msc,R Ph President of SCCP Cardiology Clinical Pharmacist Assistant Professor At King Saud University King Khalid University Hospital Riyadh-KSA 2017 ACC/AHA/HFSA
ARxCH. Annual Review of Changes in Healthcare. Entresto: An Overview for Pharmacists
 Entresto: An Overview for Pharmacists David Comshaw, PharmD Candidate 2019 1 Gyen Musgrave, PharmD Candidate 2019 1 Suzanne Surowiec, PharmD, BCACP 1 Jason Guy, PharmD 1 1 University of Findlay College
Entresto: An Overview for Pharmacists David Comshaw, PharmD Candidate 2019 1 Gyen Musgrave, PharmD Candidate 2019 1 Suzanne Surowiec, PharmD, BCACP 1 Jason Guy, PharmD 1 1 University of Findlay College
The Approach to Patients with Heart Failure and Mid-Range (40-50%) Ejection Fraction (HFmrEF)
 Ejection Fraction (HFmrEF)") The Approach to Patients with Heart Failure and Mid-Range (40-50%) Ejection Fraction (HFmrEF) 22 nd Annual Heart Failure 2018 an Update on Therapy April 21, 2018 Los Angeles, CA Barry Greenberg, M.D. Distinguished
The Approach to Patients with Heart Failure and Mid-Range (40-50%) Ejection Fraction (HFmrEF) 22 nd Annual Heart Failure 2018 an Update on Therapy April 21, 2018 Los Angeles, CA Barry Greenberg, M.D. Distinguished
Heart Failure in Women: Dr Goh Ping Ping Cardiologist Asian Heart & Vascular Centre
 Heart Failure in Women: More than EF? Dr Goh Ping Ping Cardiologist Asian Heart & Vascular Centre Overview Review pathophysiology as it relates to diagnosis and management Rational approach to workup:
Heart Failure in Women: More than EF? Dr Goh Ping Ping Cardiologist Asian Heart & Vascular Centre Overview Review pathophysiology as it relates to diagnosis and management Rational approach to workup:
Heart Failure (HF): Scope of the Problem. Temporal Trends in Age-Adjusted Survival After HF Diagnosis. More malignant than most cancers
: Scope of the Problem. Temporal Trends in Age-Adjusted Survival After HF Diagnosis. More malignant than most cancers") Patients in US (millions) Heart Failure (HF): Scope of the Problem 1 4 2 3.5 4. 1. 1991 21 237 US prevalence*: 5. million US annual incidence: 7, Annual mortality: 22,754 5-1% depending on severity Cost:
Patients in US (millions) Heart Failure (HF): Scope of the Problem 1 4 2 3.5 4. 1. 1991 21 237 US prevalence*: 5. million US annual incidence: 7, Annual mortality: 22,754 5-1% depending on severity Cost:
Diastolic Heart Failure Uri Elkayam, MD
 Diastolic Heart Failure Uri Elkayam, MD Professor of Medicine University of Southern California School of Medicine Los Angeles, California elkayam@usc.edu Diastolic Heart Failure Clinical Definition A
Diastolic Heart Failure Uri Elkayam, MD Professor of Medicine University of Southern California School of Medicine Los Angeles, California elkayam@usc.edu Diastolic Heart Failure Clinical Definition A
Heart Failure Update. Chim Lang
 Heart Failure Update Chim Lang Heart Failure Patient s Journey Acute Treat and stabilize Initiate monitoring Plan interventions Chronic Optimize drug and device therapy Manage Co-morbidities Subacute
Heart Failure Update Chim Lang Heart Failure Patient s Journey Acute Treat and stabilize Initiate monitoring Plan interventions Chronic Optimize drug and device therapy Manage Co-morbidities Subacute
Iron Deficiency: New Therapeutic Target in Heart Failure. Stefan D. Anker, MD PhD
 Iron Deficiency: New Therapeutic Target in Heart Failure Stefan D. Anker, MD PhD Department of Cardiology, Applied Cachexia Research, Charité Campus Virchow-Klinikum, Universitätsmedizin Berlin, Germany.
Iron Deficiency: New Therapeutic Target in Heart Failure Stefan D. Anker, MD PhD Department of Cardiology, Applied Cachexia Research, Charité Campus Virchow-Klinikum, Universitätsmedizin Berlin, Germany.
SGK 2016 Session: Postgraduate Course in Heart Failure Lausanne, 15. June 2016 Heart Failure Guidelines 2016
 SGK 2016 Session: Postgraduate Course in Heart Failure Lausanne, 15. June 2016 Heart Failure Guidelines 2016 Matthias Nägele, MD University Hospital Zurich Disclosures I have nothing to disclose. The new
SGK 2016 Session: Postgraduate Course in Heart Failure Lausanne, 15. June 2016 Heart Failure Guidelines 2016 Matthias Nägele, MD University Hospital Zurich Disclosures I have nothing to disclose. The new
HFpEF. April 26, 2018
 HFpEF April 26, 2018 (J Am Coll Cardiol 2017;70:2476 86) HFpEF 50% or more (40-71%) of patients with CHF have preserved LV systolic function. HFpEF is an increasingly frequent hospital discharge. Outcomes
HFpEF April 26, 2018 (J Am Coll Cardiol 2017;70:2476 86) HFpEF 50% or more (40-71%) of patients with CHF have preserved LV systolic function. HFpEF is an increasingly frequent hospital discharge. Outcomes
The REDUCE LAP Heart Failure Trial. David M Kaye MD, PhD on behalf of the REDUCE LAP HF Investigators
 Transcatheter Intracardiac Shunt Device Provides Sustained Clinical Benefit at One Year in Heart Failure with Preserved or Mildly Reduced Ejection Fraction: The REDUCE LAP Heart Failure Trial David M Kaye
Transcatheter Intracardiac Shunt Device Provides Sustained Clinical Benefit at One Year in Heart Failure with Preserved or Mildly Reduced Ejection Fraction: The REDUCE LAP Heart Failure Trial David M Kaye
Combination of renin-angiotensinaldosterone. how to choose?
 Combination of renin-angiotensinaldosterone system inhibitors how to choose? Karl Swedberg Professor of Medicine Sahlgrenska Academy University of Gothenburg karl.swedberg@gu.se Disclosures Research grants
Combination of renin-angiotensinaldosterone system inhibitors how to choose? Karl Swedberg Professor of Medicine Sahlgrenska Academy University of Gothenburg karl.swedberg@gu.se Disclosures Research grants
The Therapeutic Potential of Novel Approaches to RAAS. Professor of Medicine University of California, San Diego
 The Therapeutic Potential of Novel Approaches to RAAS Inhibition in Heart Failure Barry Greenberg, M.D. Professor of Medicine University of California, San Diego Chain of Events Leading to End-Stage Heart
The Therapeutic Potential of Novel Approaches to RAAS Inhibition in Heart Failure Barry Greenberg, M.D. Professor of Medicine University of California, San Diego Chain of Events Leading to End-Stage Heart
ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure
 Patients t with acute heart failure frequently develop chronic heart failure Patients with chronic heart failure frequently decompensate acutely ESC Guidelines for the Diagnosis and A clinical response
Patients t with acute heart failure frequently develop chronic heart failure Patients with chronic heart failure frequently decompensate acutely ESC Guidelines for the Diagnosis and A clinical response
New Trials. Iain Squire. Professor of Cardiovascular Medicine University of Leicester. Chair, BSH
 New Trials Iain Squire Professor of Cardiovascular Medicine University of Leicester Chair, BSH BSH Heart Failure Day for Revalidation and Training 2017 Presentation title: New Trials Speaker: Iain Squire
New Trials Iain Squire Professor of Cardiovascular Medicine University of Leicester Chair, BSH BSH Heart Failure Day for Revalidation and Training 2017 Presentation title: New Trials Speaker: Iain Squire
Systolic Dysfunction Clinical /Hemodynamic Guide for Management From Neprilysin Inhibitors to Ivabradine
 Systolic Dysfunction Clinical /Hemodynamic Guide for Management From Neprilysin Inhibitors to Ivabradine Donna Mancini MD Choudhrie Professor of Cardiology Columbia University Speaker Disclosure Amgen
Systolic Dysfunction Clinical /Hemodynamic Guide for Management From Neprilysin Inhibitors to Ivabradine Donna Mancini MD Choudhrie Professor of Cardiology Columbia University Speaker Disclosure Amgen
HFpEF: Pathophysiology & Treatment
 HFpEF: Pathophysiology & Treatment Barry A. Borlaug, MD Mayo Clinic, Rochester, MN borlaug.barry@mayo.edu Disclosure Financial Relationships Research Support: Aires Pharmaceuticals, Medtronic, GSK Consulting/Advisory
HFpEF: Pathophysiology & Treatment Barry A. Borlaug, MD Mayo Clinic, Rochester, MN borlaug.barry@mayo.edu Disclosure Financial Relationships Research Support: Aires Pharmaceuticals, Medtronic, GSK Consulting/Advisory
Heart Failure Medical and Surgical Treatment
 Heart Failure Medical and Surgical Treatment Daniel S. Yip, M.D. Medical Director, Heart Failure and Transplantation Mayo Clinic Second Annual Lakeland Regional Health Cardiovascular Symposium February
Heart Failure Medical and Surgical Treatment Daniel S. Yip, M.D. Medical Director, Heart Failure and Transplantation Mayo Clinic Second Annual Lakeland Regional Health Cardiovascular Symposium February
HEART FAILURE: PHARMACOTHERAPY UPDATE
 HEART FAILURE: PHARMACOTHERAPY UPDATE 3 HEART FAILURE REVIEW 1 5.1 million x1.25 = 6.375 million 40 years old = MICHAEL F. AKERS, PHARM.D. CLINICAL PHARMACIST CENTRACARE HEALTH, ST. CLOUD HOSPITAL HF Diagnosis
HEART FAILURE: PHARMACOTHERAPY UPDATE 3 HEART FAILURE REVIEW 1 5.1 million x1.25 = 6.375 million 40 years old = MICHAEL F. AKERS, PHARM.D. CLINICAL PHARMACIST CENTRACARE HEALTH, ST. CLOUD HOSPITAL HF Diagnosis
Effect of ferric carboxymaltose on functional capacity in patients with heart failure and iron deficiency (CONFIRM-HF)
") Effect of ferric carboxymaltose on functional capacity in patients with heart failure and iron deficiency (CONFIRM-HF) Piotr Ponikowski, Dirk J. van Veldhuisen, Josep Comin-Colet Georg Ertl, Michel Komajda,
Effect of ferric carboxymaltose on functional capacity in patients with heart failure and iron deficiency (CONFIRM-HF) Piotr Ponikowski, Dirk J. van Veldhuisen, Josep Comin-Colet Georg Ertl, Michel Komajda,
Optimal blockade of the Renin- Angiotensin-Aldosterone. in chronic heart failure
 Optimal blockade of the Renin- Angiotensin-Aldosterone Aldosterone- (RAA)-System in chronic heart failure Jan Östergren Department of Medicine Karolinska University Hospital Stockholm, Sweden Key Issues
Optimal blockade of the Renin- Angiotensin-Aldosterone Aldosterone- (RAA)-System in chronic heart failure Jan Östergren Department of Medicine Karolinska University Hospital Stockholm, Sweden Key Issues
Beyond ACE-inhibitors for Heart Failure. Jacob Townsend, MD NCVH Birmingham 2015
 Beyond ACE-inhibitors for Heart Failure Jacob Townsend, MD NCVH Birmingham 2015 % Decrease in Mortality Current Therapy HFrEF 0% Angiotensin receptor blocker ACE inhibitor Beta blocker Mineralocorticoid
Beyond ACE-inhibitors for Heart Failure Jacob Townsend, MD NCVH Birmingham 2015 % Decrease in Mortality Current Therapy HFrEF 0% Angiotensin receptor blocker ACE inhibitor Beta blocker Mineralocorticoid
Guideline Management of Chronic Heart Failure
 Guideline Management of Chronic Heart Failure 2013 ACC/AHA Guideline Mgmt HF 2016 ACC/AHA/HFSA Focused Update 2017 ACCAHA/HFSA Focused Update October 17 th, 2017 Dawn Lombardo DO, MSc Professor of Medicine/Clinical
Guideline Management of Chronic Heart Failure 2013 ACC/AHA Guideline Mgmt HF 2016 ACC/AHA/HFSA Focused Update 2017 ACCAHA/HFSA Focused Update October 17 th, 2017 Dawn Lombardo DO, MSc Professor of Medicine/Clinical
Systolic Dysfunction Clinical/Hemodynamic Guide for Management; New Medical and Interventional Therapeutic Challenges
 Systolic Dysfunction Clinical/Hemodynamic Guide for Management; New Medical and Interventional Therapeutic Challenges Clyde W. Yancy, MD, MSc, FACC, FAHA, MACP Magerstadt Professor of Medicine Professor,
Systolic Dysfunction Clinical/Hemodynamic Guide for Management; New Medical and Interventional Therapeutic Challenges Clyde W. Yancy, MD, MSc, FACC, FAHA, MACP Magerstadt Professor of Medicine Professor,
Heart Failure Guidelines For your Daily Practice
 Heart Failure Guidelines For your Daily Practice Juan M. Aranda, Jr., MD, FACC, FHFSA Professor of Medicine Director of Heart Failure and Cardiac Transplantation University of Florida College of Medicine
Heart Failure Guidelines For your Daily Practice Juan M. Aranda, Jr., MD, FACC, FHFSA Professor of Medicine Director of Heart Failure and Cardiac Transplantation University of Florida College of Medicine
Heart Failure: Combination Treatment Strategies
 Heart Failure: Combination Treatment Strategies M. McDonald MD, FRCP State of the Heart Symposium May 28, 2011 None Disclosures Case 69 F, prior MIs (LV ejection fraction 25%), HTN No demonstrable ischemia
Heart Failure: Combination Treatment Strategies M. McDonald MD, FRCP State of the Heart Symposium May 28, 2011 None Disclosures Case 69 F, prior MIs (LV ejection fraction 25%), HTN No demonstrable ischemia
Heart Failure A Disease for the Internist?
 Heart Failure A Disease for the Internist? Dr Chris Davidson Sussex Cardiac Centre BRIGHTON UK Hot Topics in Heart Failure Drug treatments Valsartan / neprilysin inhib Investigations BNP and others Devices
Heart Failure A Disease for the Internist? Dr Chris Davidson Sussex Cardiac Centre BRIGHTON UK Hot Topics in Heart Failure Drug treatments Valsartan / neprilysin inhib Investigations BNP and others Devices
Heart Failure: Current Management Strategies
 Heart Failure: Current Management Strategies CSHP Fall Education Session- September 30th, 2017 Carolyn MacKinnon & Tamara Matchett BscPharm, ACPR Candidates Objectives 1. Describe the pathophysiology &
Heart Failure: Current Management Strategies CSHP Fall Education Session- September 30th, 2017 Carolyn MacKinnon & Tamara Matchett BscPharm, ACPR Candidates Objectives 1. Describe the pathophysiology &
8:30-10:30 WS #4: Cardiology :00-13:00 WS #11: Cardiology 101 (Repeated)
") Professor Ralph Stewart Cardiologist Auckland City Hospital Green Lane Cardiovascular Research Unit Auckland Heart Group Fiona Stewart Cardiologist Green Lane Hospital National Women's Hospital Professor
Professor Ralph Stewart Cardiologist Auckland City Hospital Green Lane Cardiovascular Research Unit Auckland Heart Group Fiona Stewart Cardiologist Green Lane Hospital National Women's Hospital Professor
The NEW Heart Failure Guidelines
 The NEW Heart Failure Guidelines Daily Practice HF scenario of the Case Presentations HF as a complex and heterogeneous syndrome Several proposed pathophysiological mechanisms involving the heart and the
The NEW Heart Failure Guidelines Daily Practice HF scenario of the Case Presentations HF as a complex and heterogeneous syndrome Several proposed pathophysiological mechanisms involving the heart and the
Nitrate s Effect on Activity Tolerance in Heart Failure with Preserved Ejection Fraction (NEAT) A Randomized Clinical Trial
 A Randomized Clinical Trial") Nitrate s Effect on Activity Tolerance in Heart Failure with Preserved Ejection Fraction (NEAT) A Randomized Clinical Trial Margaret M Redfield On behalf of the NHLBI Heart Failure Clinical Research Network
Nitrate s Effect on Activity Tolerance in Heart Failure with Preserved Ejection Fraction (NEAT) A Randomized Clinical Trial Margaret M Redfield On behalf of the NHLBI Heart Failure Clinical Research Network
Heart Failure Therapies State of the Art 2017
 Heart Failure Therapies State of the Art 2017 Andrew J. Sauer, MD Assistant Professor Director, Center for Heart Failure Medical Director, Heart Transplantation UNOS Primary Transplant Physician asauer@kumc.edu
Heart Failure Therapies State of the Art 2017 Andrew J. Sauer, MD Assistant Professor Director, Center for Heart Failure Medical Director, Heart Transplantation UNOS Primary Transplant Physician asauer@kumc.edu
Μαρία Μπόνου Διευθύντρια ΕΣΥ, ΓΝΑ Λαϊκό
 Μαρία Μπόνου Διευθύντρια ΕΣΥ, ΓΝΑ Λαϊκό Diastolic HF DD: Diastolic Dysfunction DHF: Diastolic HF HFpEF: HF with preserved EF DD Pathophysiologic condition: impaired relaxation, LV compliance, LV filling
Μαρία Μπόνου Διευθύντρια ΕΣΥ, ΓΝΑ Λαϊκό Diastolic HF DD: Diastolic Dysfunction DHF: Diastolic HF HFpEF: HF with preserved EF DD Pathophysiologic condition: impaired relaxation, LV compliance, LV filling
What s New in the Treatment of Heart Failure March 28, 2018 Ohio Chapter-ACC
 What s New in the Treatment of Heart Failure March 28, 2018 Ohio Chapter-ACC Randall C Starling MD MPH FACC FAHA FESC FHFSA Professor of Medicine Kaufman Center for Heart Failure Heart and Vascular Institute
What s New in the Treatment of Heart Failure March 28, 2018 Ohio Chapter-ACC Randall C Starling MD MPH FACC FAHA FESC FHFSA Professor of Medicine Kaufman Center for Heart Failure Heart and Vascular Institute
Faiez Zannad. Institut Lorrain du Coeur et des Vaisseaux. CIC - Inserm
 Faiez Zannad Institut Lorrain du Coeur et des Vaisseaux CIC - Inserm Disclosure Faiez Zannad Grants BG Medicine, Roche Diagnostics. Consultant/Steering committees/event committees/ Data safety Monitoring
Faiez Zannad Institut Lorrain du Coeur et des Vaisseaux CIC - Inserm Disclosure Faiez Zannad Grants BG Medicine, Roche Diagnostics. Consultant/Steering committees/event committees/ Data safety Monitoring
Updates in Heart Failure (HF) 2016: ACC / AHA and ESC
 2016: ACC / AHA and ESC") Updates in Heart Failure (HF) 2016: ACC / AHA and ESC Patrick McBride, MD, MPH Professor of Medicine & Family Medicine, UW School of Medicine and Public Health Special thanks to: Clyde W. Yancy, MD, MSc
Updates in Heart Failure (HF) 2016: ACC / AHA and ESC Patrick McBride, MD, MPH Professor of Medicine & Family Medicine, UW School of Medicine and Public Health Special thanks to: Clyde W. Yancy, MD, MSc
Anemia and Iron Deficiency: What Every Cardiologist Needs to Know
 6th Saudi HF Group Symposium Riyadh - December 8-9, 2017 Anemia and Iron Deficiency: What Every Cardiologist Needs to Know Ammar Chaudhary MBChB, FRCPC Consultant Cardiologist Advanced Heart Failure Department
6th Saudi HF Group Symposium Riyadh - December 8-9, 2017 Anemia and Iron Deficiency: What Every Cardiologist Needs to Know Ammar Chaudhary MBChB, FRCPC Consultant Cardiologist Advanced Heart Failure Department
Heart Failure with Preserved Ejection Fraction (HFpEF): Natural History and Contemporary Management
: Natural History and Contemporary Management") Heart Failure with Preserved Ejection Fraction (HFpEF): Natural History and Contemporary Management Jason L. Guichard, MD, PhD Greenville Health System Department of Medicine, Carolina Cardiology Consultants
Heart Failure with Preserved Ejection Fraction (HFpEF): Natural History and Contemporary Management Jason L. Guichard, MD, PhD Greenville Health System Department of Medicine, Carolina Cardiology Consultants
HFpEF in the Future: New Diagnostic Techniques and Treatments in the Pipeline
 HFpEF in the Future: New Diagnostic Techniques and Treatments in the Pipeline Scott D. Solomon, MD Brigham and Women s Hospital Harvard University Boston, MA Disclosures Dr. Solomon has received research
HFpEF in the Future: New Diagnostic Techniques and Treatments in the Pipeline Scott D. Solomon, MD Brigham and Women s Hospital Harvard University Boston, MA Disclosures Dr. Solomon has received research
TERAPIA DELLO SCOMPENSO DAI BETA- BLOCCANTI AGLI ARNI (ARNI SI ARNI NO) Iseo 10 Novembre 2018
 Iseo 10 Novembre 2018") TERAPIA DELLO SCOMPENSO DAI BETA- BLOCCANTI AGLI ARNI (ARNI SI ARNI NO) Iseo 10 Novembre 2018 Carlo Lombardi Cattedra di Cardiologia Università e Spedali Civili di Brescia All-cause mortality in the European
TERAPIA DELLO SCOMPENSO DAI BETA- BLOCCANTI AGLI ARNI (ARNI SI ARNI NO) Iseo 10 Novembre 2018 Carlo Lombardi Cattedra di Cardiologia Università e Spedali Civili di Brescia All-cause mortality in the European
HeFSSA Practitioners Program 2018 Back to basics on heart failure treatment?
 HeFSSA Practitioners Program 2018 Back to basics on heart failure treatment? Co-morbidity in heart failure Arrhythmias in heart failure Special investigations in heart failure Heart failure with preserved
HeFSSA Practitioners Program 2018 Back to basics on heart failure treatment? Co-morbidity in heart failure Arrhythmias in heart failure Special investigations in heart failure Heart failure with preserved
Objectives. Systolic Heart Failure: Definitions. Heart Failure: Historical Perspective 2/7/2009
 Objectives Diastolic Heart Failure and Indications for Echocardiography in the Asian Population Damon M. Kwan, MD UCSF Asian Heart & Vascular Symposium 02.07.09 Define diastolic heart failure and differentiate
Objectives Diastolic Heart Failure and Indications for Echocardiography in the Asian Population Damon M. Kwan, MD UCSF Asian Heart & Vascular Symposium 02.07.09 Define diastolic heart failure and differentiate
Heart Failure Management. Waleed AlHabeeb, MD, MHA Assistant Professor of Medicine Consultant Heart Failure Cardiologist
 Heart Failure Management Waleed AlHabeeb, MD, MHA Assistant Professor of Medicine Consultant Heart Failure Cardiologist Heart failure prevalence is expected to continue to increase¹ 21 MILLION ADULTS WORLDWIDE
Heart Failure Management Waleed AlHabeeb, MD, MHA Assistant Professor of Medicine Consultant Heart Failure Cardiologist Heart failure prevalence is expected to continue to increase¹ 21 MILLION ADULTS WORLDWIDE
Diastolic Dysfunction: Hypertension to Hypertrophy to Heart Failure
 Diastolic Dysfunction: Hypertension to Hypertrophy to Heart Failure Dr. Shelley Zieroth FRCPC Assistant Professor, Cardiology, University of Manitoba Director of Cardiac Transplant and Heart Failure Clinics
Diastolic Dysfunction: Hypertension to Hypertrophy to Heart Failure Dr. Shelley Zieroth FRCPC Assistant Professor, Cardiology, University of Manitoba Director of Cardiac Transplant and Heart Failure Clinics
Sacubitril/Valsartan in HFrEF for All Protagonist View George Honos MD FRCPC FCCS FACC
 Sacubitril/Valsartan in HFrEF for All Protagonist View George Honos MD FRCPC FCCS FACC Head of Cardiology Medical Manager / CV Program CHUM Disclosure Statement Within the past two years: I have had an
Sacubitril/Valsartan in HFrEF for All Protagonist View George Honos MD FRCPC FCCS FACC Head of Cardiology Medical Manager / CV Program CHUM Disclosure Statement Within the past two years: I have had an
Comorbidities in Heart Failure: Iron Deficiency. Ammar Chaudhary, MBChB, FRCPC King Faisal Specialist Hospital and Research Centre - Jeddah
 Comorbidities in Heart Failure: Iron Deficiency Ammar Chaudhary, MBChB, FRCPC King Faisal Specialist Hospital and Research Centre - Jeddah ACC Middle East Conference 2018 Iron Deficiency in Heart Failure
Comorbidities in Heart Failure: Iron Deficiency Ammar Chaudhary, MBChB, FRCPC King Faisal Specialist Hospital and Research Centre - Jeddah ACC Middle East Conference 2018 Iron Deficiency in Heart Failure
Akash Ghai MD, FACC February 27, No Disclosures
 Akash Ghai MD, FACC February 27, 2015 No Disclosures Epidemiology Lifetime risk is > 20% for American s older than 40 years old. > 650,000 new cases diagnosed each year. Incidence increases with age: 2%
Akash Ghai MD, FACC February 27, 2015 No Disclosures Epidemiology Lifetime risk is > 20% for American s older than 40 years old. > 650,000 new cases diagnosed each year. Incidence increases with age: 2%
Heart Failure. Subjective SOB (shortness of breath) Peripheral edema. Orthopnea (2-3 pillows) PND (paroxysmal nocturnal dyspnea)
 Peripheral edema. Orthopnea (2-3 pillows) PND (paroxysmal nocturnal dyspnea)") Pharmacology I. Definitions A. Heart Failure (HF) Heart Failure Ezra Levy, Pharm.D. HF Results when one or both ventricles are unable to pump sufficient blood to meet the body s needs There are 2 types
Pharmacology I. Definitions A. Heart Failure (HF) Heart Failure Ezra Levy, Pharm.D. HF Results when one or both ventricles are unable to pump sufficient blood to meet the body s needs There are 2 types
Heart Failure (HF): Scope of the Problem. Temporal Trends in Age-Adjusted Survival After HF Diagnosis. More malignant than most cancers
: Scope of the Problem. Temporal Trends in Age-Adjusted Survival After HF Diagnosis. More malignant than most cancers") Evidence-Based Approaches to the Management of Heart Failure: Reducing Hospitalization and Improving Patient Outcomes Eldrin F. Lewis, MD, MPH Director of Cardiovascular Clerkship Brigham and Women s Hospital
Evidence-Based Approaches to the Management of Heart Failure: Reducing Hospitalization and Improving Patient Outcomes Eldrin F. Lewis, MD, MPH Director of Cardiovascular Clerkship Brigham and Women s Hospital
2016 ESC Heart Failure Guidelines: what is new? Piotr Ponikowski Wroclaw, Poland
 2016 ESC Heart Failure Guidelines: what is new? Piotr Ponikowski Wroclaw, Poland Disclosures Consultancy fees and speaker s honoraria from: Amgen, Servier, Novartis, Johnson & Johnson, Merck, Berlin Chemie,
2016 ESC Heart Failure Guidelines: what is new? Piotr Ponikowski Wroclaw, Poland Disclosures Consultancy fees and speaker s honoraria from: Amgen, Servier, Novartis, Johnson & Johnson, Merck, Berlin Chemie,
Aldosterone Antagonism in Heart Failure: Now for all Patients?
 Aldosterone Antagonism in Heart Failure: Now for all Patients? Inder Anand, MD, FRCP, D Phil (Oxon.) Professor of Medicine, University of Minnesota, Director Heart Failure Program, VA Medical Center 111C
Aldosterone Antagonism in Heart Failure: Now for all Patients? Inder Anand, MD, FRCP, D Phil (Oxon.) Professor of Medicine, University of Minnesota, Director Heart Failure Program, VA Medical Center 111C
Does My Patient Always Require Diuretics???
 Does My Patient Always Require Diuretics??? Shelley Zieroth, MD Associate Professor, Section of Cardiology Director, SBH Heart Failure and Transplant Clinics Head, Medical Heart Failure Program WRHA Cardiac
Does My Patient Always Require Diuretics??? Shelley Zieroth, MD Associate Professor, Section of Cardiology Director, SBH Heart Failure and Transplant Clinics Head, Medical Heart Failure Program WRHA Cardiac