HFpEF in the Future: New Diagnostic Techniques and Treatments in the Pipeline
|
|
|
- Edward McKenzie
- 6 years ago
- Views:
Transcription



1 HFpEF in the Future: New Diagnostic Techniques and Treatments in the Pipeline Scott D. Solomon, MD Brigham and Women s Hospital Harvard University Boston, MA
2 Disclosures Dr. Solomon has received research support from Novartis, Daichi-Sankyo, Amgen, Boston Scientific, Forest, Biogen, the National Heart Lung and Blood Institute, NIDDK, NCI, and has consulted for Novartis and Sanofi-Aventis
3 It s tough to make predictions, especially about the future. Yogi Berra
4 The Current State of Heart Failure Therapy Systolic Heart Failure Diastolic/PSF Heart Failure Multiple randomized controlled double -blind clinical trials Therapies based on outcomes General HF community consensus The randomized controlled trial has even refuted previous held dictum Evidenced-based medicine Mechanistic studies and small, non-definitive trials Empiric symptom-based therapy Limited consensus Disconnect between randomized trials and observational data Anectode-based medicine
5 Challenges to Finding Effective Treatments in Diastolic/PSF Heart Failure Lack of appreciation Lack of agreement Marked heterogeneity Difficult diagnosis Lack of noninvasive methods Opposing mechanisms Theoretic benefits don t always translate to outcomes
6 Two Potential Reasons why the trials have Not been successful Wrong Patients Wrong Therapies
7 Diagnosis of HFpEF Diagnosis of Heart Failure in HFpEF Echocardiographic Diagnosis in HFpEF Stress Testing in HFpEF Novel Methods to Assess Cardiac Function in HFpEF Biomarkers beyond BNP
8 Diagnosis of HFpEF Diagnosis of Heart Failure in HFpEF Echocardiographic Diagnosis in HFpEF Stress Testing in HFpEF Novel Methods to Assess Cardiac Function in HFpEF Biomarkers beyond BNP
9 BNP Important in Prognosis: Should we make this a critical component of the diagnosis? Most New HFpEF Trials are requiring elevated BNP/NT-proBNP for Entry! Cleland et al. NEJM Letter 2007
10 False positives BNP Caveats BNP increases with age BNP higher in women than in men BNP higher in atrial fibrillation False negatives Obesity decreases BNP levels Intermittent or rapid increases in pressures
11 Diagnosis of HFpEF Diagnosis of Heart Failure in HFpEF Echocardiographic Diagnosis in HFpEF Stress Testing in HFpEF Novel Methods to Assess Cardiac Function in HFpEF Biomarkers beyond BNP
12 Use of Echocardiography in HFpEF 1. Establish that LV systolic function is normal 2. Exclude other possible causes of the patients symptoms and signs 3. Evaluate diastolic function

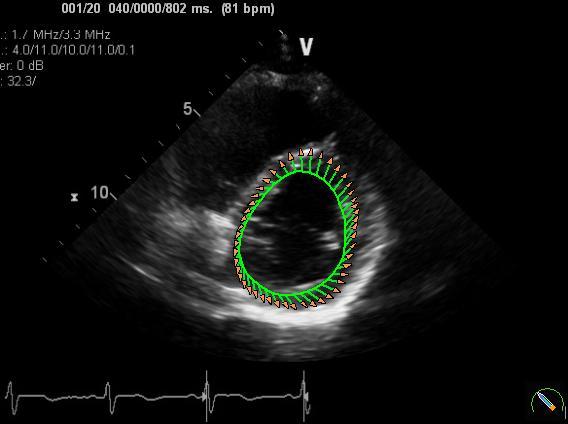
13 The GOLD Standard for Assessment of Diastolic Function



14 Traditional Doppler Approaches to Diastolic Function

15 Standard Doppler can be Diagnostically Misleading and Response to Therapy can be Impossible to Interpret Worsening of Diastolic Function


16 Doppler Tissue Imaging Measures Myocardial Relaxation Velocity Normal S E E = 17 cm/s A Ho C, Solomon SD. A Clinician s Guide to DTI. Circulation 2006

17 DTI more immune to changes in Preload
18 Is E/E an accurate measure of filling pressure? PCWP = 1.24 ( E/Em ) +1.9 LAP = E/Em 15 E inversely related to Tau, E/E surrogate for filling pressure Mitral inflow velocity (E wave) is a measure of the LA - > LV pressure gradient and is thus dependent on left atrial pressure AND ventricular relaxation. Dividing the E wave by E, itself a measure of ventricular relaxation, thus yields an estimate of LA pressure (which is itself related to LV EDP)

19 Circulation. 2009
20 Pulmonary Hypertension May be a Critical Component of HFpEF Lam C.S. et al J Am Coll Cardiol. 2009;53:
21 Prognostic impact of PH in HFpEF Lam C.S. et al J Am Coll Cardiol. 2009;53:
22 Diagnosis of HFpEF Diagnosis of Heart Failure in HFpEF Echocardiographic Diagnosis in HFpEF Stress Testing in HFpEF Novel Methods to Assess Cardiac Function in HFpEF Biomarkers beyond BNP
23 Elderly HFPEF Patients Have Severe Exercise Intolerance Peak VO2 (ml/kg/min) Healthy NO HFREF SD DDHFPEF p vs healthy age-matched normal subjects Kitzman et al, JAMA 2002
24 Exercise Capacity Correlates with LV-stiffness 27 patients with DHF, 12 patients with no DHF (according to end-diastolic pressure volume relationship): Cardiopulmonary exercise testing + PV measurements by conductance catheter method Sinning et al.; Cardiology Research and Practice 2011


25 In patients with diastolic dysfunction, the abnormal relaxation prevents augmentation of relaxation as heart rate increases during exercise. Quantifying the response of diastolic functional indices to dynamic exercise is therefore a way to assess diastolic functional reserve in patients with exertional dyspnea and normal resting ventricular systolic and diastolic function
26 Stress Testing in HFpEF Rule out ischemia Heart rate reserve (unmask chronotropic Incompetence) Unmask abnormalities of diastolic function that are less obvious at rest Unmask reactive pulmonary hypertension
27 Diagnosis of HFpEF Diagnosis of Heart Failure in HFpEF Echocardiographic Diagnosis in HFpEF Stress Testing in HFpEF Novel Methods to Assess Cardiac Function in HFpEF Biomarkers beyond BNP




28 Normal Strain and Torsion P S A L Contraction Counter-clockwise Apical Rotation as viewed from apex Contraction Basal Time Clockwise Systole Diastole Notomi et al. Circulation March, 2005

29 Comprehensive assessment of 39 women with HFpEF and 27 age-matched controls with rest and exercise echocardiography At rest, systolic longitudinal and radial strain, systolic mitral annular velocities, and apical rotation were lower in patients, and all failed to rise normally with exercise In diastole, patients had reduced and delayed untwisting, reduced LV sction at rest and with exericse, and higher EDP. Mitral annular systolic and diastolic velocities, systolic rotation and diastolic untwist on exercise correlated with peak VO2 max.


30
31 LV Untwisting Reflects IVPG 7.5 y = -0.44x r = 0.72 IVPG, mmhg Peak LV untwisting, rad/s Notomi et al. Circ 2006; 113:


32 Systolic torsion and diastolic untwisting are significantly increased in patients with mild diastolic dysfunction In patients with advanced diastolic dysfunction with increased filling pressure, they are normalized or reduced Not Yet Ready for Prime Time! Park et al. JASE 2008
33 Insights into HFpEF Mechanics Despite normal ejection fraction, systolic contractile function in HFpEF is not normal S, longitudinal strain, strain rate and rotational mechanics are all abnormal These measures are not ready to be used in diagnosis yet, but stay tuned
34 Diagnosis of HFpEF Diagnosis of Heart Failure in HFpEF Echocardiographic Diagnosis in HFpEF Stress Testing in HFpEF Novel Methods to Assess Cardiac Function in HFpEF Biomarkers beyond BNP



35 ST2 is a member of the interleukin-1 receptor family; the ligand for ST2 was recently identified to be IL-33 IL-33 is a fibroblast product, induced by cellular stretch Provides protection against myocardial fibrosis and hypertrophy in the context of pressure overload The effects of IL-33 may be blunted or blocked by high concentrations of ST2 or by knocking out the ST2 gene

36 Galectin-3 is a marker of fibrosis that may be important both for prognosis and as a marker of response to therapy Ann Med 2010
37 Diagnosics in HFpEF: Summary Flow-based Doppler methods (E/A), DT unreliable E/E good at extremes, but may be less useful at the margins Pulmonary pressures may be essential component Strain and torsion worth watching as potential diagnostic measures still lacking reliable outcomes data Biomarkers other than BNP may point to increased wall stress and fibrosis and may prove useful for both diagnosis, prognosis and response to therapy We need larger studies to confirm the relationship between measured abnormalities and outcomes
38 Future of Diagnosis in HFpEF Enormous heterogeneity in this disorder Diagnosis of a Disease or Phenotyping a Syndrome?

39 202 Trials of Diastolic HF or HFpEF Clinicaltrials.gov

40 Aurigemma G & Gasch W. N Engl J Med
41 Pathophysiologic Approaches to Diastolic Heart Failure Cardiac Physiology Improve diastolic relaxation Slow HR > improve filling Improve myocardial oxygen supply/demand balance Reduce congestion Renal Function Improve Na and H20 handling Pulmonary Function Pulmonary Vasodilator? Peripheral Physiology Lower BP decrease afterload Improve conduit vessel function Cardiac Structure Regression of cardiac hypertrophy Reduce fibrosis
42 Pharmacologic Rx for HFpEF ACE/ARB PEP-CHF CHARM- Preserved I-PRESERVE AGE-Breaker Alegebrium Aldosterone Antagonists TOPCAT Aldo-DHF Beta-Blockers Seniors (±) CHINESE EPO ARNI PARAMOUNT PDE-5 RELAX Anemia in Heart Failure With a Preserved Ejection Fraction (HFPEF)
 Sex, n (%) Male 231 (23.5) 250 (25.2) 0.11* Female 101 (15.5) 125 (21.8) Age, n (%) <75 y 148 (16.6) 176 (21.4) 0.51* 75 y 184 (24.6) 199 (26.7) Total 332 (31.1) 375 (35.3) 0.039 0.5 0.6 0.7 0.8 0.")
43 SENIORS: Death or CV Hospitalization by Subgroup Favors Favors Nebivolol Placebo Nebivolol Placebo P value LVEF, n (%) 35% 219 (21.7) 249 (25.1) 0.42* >35% 110 (17.6) 125 (21.9) Sex, n (%) Male 231 (23.5) 250 (25.2) 0.11* Female 101 (15.5) 125 (21.8) Age, n (%) <75 y 148 (16.6) 176 (21.4) 0.51* 75 y 184 (24.6) 199 (26.7) Total 332 (31.1) 375 (35.3) Hazard ratio and 95% CI *P value for interaction between groups; P value vs placebo. The official status of nebivolol in the US is preregistration (awaiting FDA approval). LVEF, left ventricular ejection fraction; SENIORS, Study of the Effects of Nebivolol Intervention on Outcomes and Rehospitalization in Seniors with Heart Failure. Flather MD et al. Eur Heart J. 2005;26(3):
 or control Primary endpoint is a composite of hospitalization for heart failure and cardiovascular death Secondary endpoints:")
44 Multicentre, prospective, randomized, open-label, blinded endpoint (PROBE) trial. N = 1200 Randomized to either b-blocker (metoprolol succinate) or control Primary endpoint is a composite of hospitalization for heart failure and cardiovascular death Secondary endpoints: cardiovascular death, heart failure mortality or hospitalization, all-cause mortality, change in New York Heart Association class, change in left ventricular ejection fraction, increase in NT-proBNP (by 50% of the value at randomization), b-blocker tolerance, and premature termination of b-blocker therapy due to adverse events Follow-up period minimum of 2 years
45 TM A.G.E.s Stimulate Multiple Inflammatory and Metabolic Pathways AGEs AGE CROSSLINKS Multispecific AGE-receptors Receptors RAGE AGE R-1 AGE R-2 AGE R-3 (Galectin 3) MSRA Sources: Adapted from Raj, AJKD, 2000 Schmidt AM, et al, The Journal of Clinical Investigation, October 2001 Aronson, D and Rayfield E, Cardiovascular Diabetology 2002 Macrophages Epithelial Mesangial Endothelium Stimulation of Inflammatory & Metabolic Pathways Cytokines (TNF, IL-1, IL-6) Extracellular Matrix Production (CTGF, TGF ) Metabolic Pathway Activation (PKC ) Growth Factors (TGF, CTGF, PDGF, VEGF, IGF-1) Adhesion Molecules (VCAM-1, ICAM) Gene Expression (NF, ERK, 1, 2, JNK) Oxidative Stress (NADPH Oxidase)
46 End-Diastolic Pressure (mm Hg) Short-Term Dosing With Alagebrium Restores Flexibility In The Left Ventricle In Aged Dogs Low Volume, High Pressure Untreated Aged Dogs (volume loaded) * * * p < Treated Aged Dogs Control * Young Dogs End-Diastolic Volume Index (ml/m 2 ) High Volume, Low Pressure Male mongrel dogs. ALT-711: 1 mg/kg, oral, 4 weeks Adapted from Asif et al, PNAS 2000
 125 ± 35 Baseline Early mitral annulus diastolic velocity: 6.3 cm \ s 119 ± 34, p=0.")

47 23 Patients with Diastolic HF Open Label Alagebrium for 16 Weeks Baseline Treatment LV Mass (MRI) Annular E (TDI) 125 ± 35 Baseline Early mitral annulus diastolic velocity: 6.3 cm \ s 119 ± 34, p=0.036 Post - Treatment Post - Treatment Early Early mitral mitral annulus annulus diastolic diastolic velocity: equals 9.3 cm \ s 9.3 cm \ s 5 cm/s 5 cm/s 7.3 ± ± 1.7, p=0.045 Little, J Card Failure 2005
 receptor blockade (ARB) Ingestion of LCZ696 results in systemic exposure of the")
48 LCZ696: first in class, Angiotensin Receptor Neprilysin Inhibitor (ARNI) rapidly converted to NEPi and valsartan LCZ696 PLASMA AHU377 pro-drug LBQ657 active NEPi H N O H N O O N a O O Esterase O H O O H O O LCZ696 is a novel, dual-acting agent which delivers concomitant neprilysin inhibition and angiotensin (AT1) receptor blockade (ARB) Ingestion of LCZ696 results in systemic exposure of the neprilysin inhibitor (NEPi) pro-drug AHU377 (which is further metabolized to LBQ657) and valsartan (AT-1 receptor blocker) O Valsartan ARB N N O OH Highly selective NEP inhibitor: IC 50 for human NEP = 7.3 nm ACE >100 mm APP > 1 mm N N NH
49 PARAMOUNT: Therapeutic Validation Study (CLCZ696B2214) Placebo run-in LCZ mg BID LCZ mg BID LCZ mg BID Discontinue ACEI or ARB therapy one day prior to randomization Design 2 weeks wks, randomized, double-blind, active controlled study evaluating LCZ 200 mg bid compared to valsartan 160 mg bid followed by 6 month extension LCZ 696 and valsartan will be progressively up-titrated to the target doses Population Approximately 300 pts with chronic HF (NYHA class II-IV), LVEF 45%, and elevated NT-proBNP > 400 pg/ml Primary objective Secondary objectives Sample size Valsartan 40 mg BID Valsartan 80 mg BID Valsartan 160 mg BID 1 week 1 week 10 weeks Prior ACEi/ARB use discontinued NT-proBNP reduction from baseline at 12 weeks (core study) with 6 month extension HF symptoms and QoL Kansas City Cardiomyopathy Questionnaire & global assessment Echocardiographic parameters of diastolic function, cardiac filling pressures (LVDP using E/E as surrogate) and PASP Evaluate the effects on BNP, ANP, and cgmp as well as collagen markers (PIIP and TMP) Renal function and safety and tolerability Arterial stiffness (PWV, AI, central BPs) in sub-population 80% power to detect a 25% reduction in NT-proBNP vs comparator 6 month extension
 n=22 4.8 ± 0.8 4.7 ± 0.8 4.7 ± 0.8 E Sildenafil (cm/s) n=23 4.")

50 Improvement in Measures of Structure and Function with Sildenafil in HFpEF Baseline 6 months 1 Year E placebo (cm/s) n= ± ± ± 0.8 E Sildenafil (cm/s) n= ± ± ± 0.9 E/E Placebo n= ± ± ± 5 E/E Sildenafil n= ± ± ± 5 P < 0.01 P < 0.01 Guazzi et al. Circ HF 2011
51 RELAX Study Design: Randomized (1:1), double-blind, placebo controlled treatment study Intervention: PDE-5 inhibition with sildenafil (20 mg tid for 12 weeks followed by 60 mg tid for 12 weeks) or placebo for 24 weeks Study population: 190 patients with a clinical diagnosis of HF and normal EF ( 50%) enrolled over a planned 3.25 year enrollment period. Primary outcome: The primary endpoint will be exercise capacity as assessed by the change in peak peak VO2 at 24 weeks of double blinded therapy compared to the baseline peak VO2. Secondary outcomes: 1. Change in a composite score reflective of clinical status after 24 weeks of double-blinded treatment with PDE-5 inhibitor or placebo. 2. Change in submaximal exercise capacity at 12 and 24 weeks as assessed by 6 minute walk test 3. Change in peak VO2 at 12 weeks


52 Myocardial Fibrosis in Hypertension and CHF: The Aldosterone Hypothesis Aldosterone Cardiac fibroblasts Collagen synthesis Collagen deposition Myocardial fibrosis LV stiffness LVD Aldosterone Receptor Antagonists Aldosterone promotes myocardial fibrosis, enhances ventricular stiffness, and worsens diastolic function Hypertension potentiates diastolic dysfunction by enhancing myocyte hypertrophy and interstitial fibrosis Aldosterone receptor antagonists may have a therapeutic role CHF Adapted from Hameedi and Chadow. Curr Hypertens Rep. 2000;2:

 * Optional Titration to 45 mg at 4 mos")
53 TOPCAT: Trial Design AGE 50 YRS EF 45% WITHIN 6 MONTHS HEART FAILURE SYMPTOMS AND SIGNS CONTROLLED SYSTOLIC BP (< 140 mm Hg) * SERUM K MMOL/L PLUS ONE OF THE FOLLOWING: HF HOSPITALIZATION WITHIN 12 MONTHS BNP 100 PG/ML N-TERMINAL PRO-BNP 360 PG/ML N=3500 RANDOMIZE PLACEBO 15 MG SPIRONOLACTONE 15 MG Week 0 DOSE TITRATION (TARGET 30 MG) * Optional Titration to 45 mg at 4 mos Week 4 COMPOSITE PRIMARY ENDPOINT CV death, Aborted cardiac arrest, Hospitalization for management of HF ~ 3.25 yrs

54 Ongoing: Aldo-DHF Aldosterone Receptor Blockade in Diastolic Heart Failure Funded by BMBF/DLR (Clinical Trial Program) Double-blind, randomised, placebo-controlled, parallel group 420 patients 1:1 spironolactone 25 mg vs. Placebo, Follow-up 18 months 50 years with heart failure NYHA II LV EF 50% Echocardiographic evidence of diastolic dysfunction ASE I Peak VO2 <20 ml/min/kg Primary Endpoints: 1. Change in maximum exercise capacity (peak VO2) on spiroergometry at 12 months compared to baseline 2. Change in E/é as indicator of diastolic function at 12 months compared to baseline ISRCTN (
55 Efficacy of Treating Anemia in Heart Failure With a Normal Ejection Fraction (HFNEF) on Ventricular Function, Exercise Capacity and Health Status NCT , Funded by NIH (NIA) Study Design: Treatment, Randomized, Single-Blind, Placebo Control, Expanded Access Assignment, Safety/Efficacy Study Intervention: Epoetin alfa versus placebo Primary Outcomes: Left Ventricular End Diastolic Volume (by Three Dimensional Echocardiography) Secondary Outcomes: Peak Oxygen Consumption by Cardiopulmonary Exercise Testing; 6 - minute walk duration; Health Status (Kansas City Cardiomyopathy Questionnaire); Left ventricular structure (volumes and mass) and function (stroke volume, cardiac output); Hospitalization Expected Total Enrollment: 60



56 The Baroreflex as a Therapeutic Target in Hypertension and Heart Failure Carotid Baroreceptor Stimulation Brain Autonomic Nervous System Inhibited sympathetic activity and enhanced parasympathetic activity Heart Vessels Kidneys HR Vasodilation Stiffness Diuresis Renin secretion Reduced excessive blood pressure Reduced afterload, wave reflections and augmentation Reduced myocardial work and oxygen consumption Reduced neurohormonal stimulus Increased venous capacitance
57 Change in mmhg Sustainable Reduction of SBP over 4 years 0 Systolic (Baseline = 193 ± 36 mmhg) Diastolic (Baseline= 111 ± 20 mmhg) Anti-hypertensive Medications Changes Baseline year years years years N=18 1 year 2 years 3 years 4 years 7. The response is sustainable 8. The response has a large magnitude Kroon et al, J Hypertension 2010
 108 Baseline 3 Months 12 Months (N=21) Severely Abnormal Mildly or Moderately Abnormal Reference Range * Based on current ASE guidelines and")
58 Reduction in Left Ventricular Mass Index at 3 and 12 Months 100% 80% % 40% % 0% P < 0.01 P < 0.01 (N=21) 108 Baseline 3 Months 12 Months (N=21) Severely Abnormal Mildly or Moderately Abnormal Reference Range * Based on current ASE guidelines and classifications Bisognano et al, J Clinical Hypertension 2009
59 HOPE4HF Trial Randomized open-label study of Rheos baroreflex activation therapy system in patients with HF, EF >= 40%, elevated BP, elevated BNP N = 540 Primary outcome: CV Death or HF Event Secondary Outcomes: LV Mass, QOL
 1900 1700 1500 1300 1100 900 700 500 Exercise Peak")

60 Effect of Exercise Training on Exercise Capacity in Elderly Patients with HFPEF Peak VO2 (ml/min) Exercise Peak VO 2 (ml/min) Control Baseline Followup Baseline Follow-up p < Kitzman et al, Circulation HF, 2010 In Press
61 Ex-DHF Pilot Study Prospective, randomised, controlled, multicenter trial in patients with mild DHF Screening for eligibility (n=71) Inclusion criteria: Age 45, NHHA II-III, preserved EF, echo signs of DDys, at least 1 RF Randomisation 2:1 Training (n= 46) Supervised, facility based endurance / resistance training (32 sessions) Controls (n= 21) Usual care / activity alone 3 months follow up 3 months follow up Primary endpoint: change in peak VO 2 Secondary endpoints: echocardiographic parameters, exercise capacity, QOL, serum biomarkers Edelmann, Pieske et al. unpublished
62 Effect of Exercise Training on Measures of Diastolic Function Echo: E/é LAVI Edelmann F Pieske B. Unpublished

63

64
65 Summary One size may not fit all in HFpEF (which may explain why trials have failed) As we get better at phenotyping in HFpEF, we should aim for more directed therapies There are potential roles for pharmacologic therapy, device therapy, and lifestyle intervention
66 The Future of HFpEF The future ain t what it used to be Yogi Berra The future is much like the present, only longer Dan Quisenberry The future will be better tomorrow Dan Quayle
LCZ696 A First-in-Class Angiotensin Receptor Neprilysin Inhibitor
 The Angiotensin Receptor Neprilysin Inhibitor LCZ696 in Heart Failure with Preserved Ejection Fraction The Prospective comparison of ARNI with ARB on Management Of heart failure with preserved ejection
The Angiotensin Receptor Neprilysin Inhibitor LCZ696 in Heart Failure with Preserved Ejection Fraction The Prospective comparison of ARNI with ARB on Management Of heart failure with preserved ejection
Therapeutic Targets and Interventions
 Therapeutic Targets and Interventions Ali Valika, MD, FACC Advanced Heart Failure and Pulmonary Hypertension Advocate Medical Group Midwest Heart Foundation Disclosures: 1. Novartis: Speaker Honorarium
Therapeutic Targets and Interventions Ali Valika, MD, FACC Advanced Heart Failure and Pulmonary Hypertension Advocate Medical Group Midwest Heart Foundation Disclosures: 1. Novartis: Speaker Honorarium
Diagnosis is it really Heart Failure?
 ESC Congress Munich - 25-29 August 2012 Heart Failure with Preserved Ejection Fraction From Bench to Bedside Diagnosis is it really Heart Failure? Prof. Burkert Pieske Department of Cardiology Med.University
ESC Congress Munich - 25-29 August 2012 Heart Failure with Preserved Ejection Fraction From Bench to Bedside Diagnosis is it really Heart Failure? Prof. Burkert Pieske Department of Cardiology Med.University
Disclosure of Relationships
 Disclosure of Relationships Over the past 12 months Dr Ruilope has served as Consultant and Speakers Bureau member of Astra-Zeneca, Bayer, Daiichi-Sankyo, Menarini, Novartis, Otsuka, Pfizer, Relypsa, Servier
Disclosure of Relationships Over the past 12 months Dr Ruilope has served as Consultant and Speakers Bureau member of Astra-Zeneca, Bayer, Daiichi-Sankyo, Menarini, Novartis, Otsuka, Pfizer, Relypsa, Servier
Diastolic Heart Failure Uri Elkayam, MD
 Diastolic Heart Failure Uri Elkayam, MD Professor of Medicine University of Southern California School of Medicine Los Angeles, California elkayam@usc.edu Diastolic Heart Failure Clinical Definition A
Diastolic Heart Failure Uri Elkayam, MD Professor of Medicine University of Southern California School of Medicine Los Angeles, California elkayam@usc.edu Diastolic Heart Failure Clinical Definition A
Heart Failure in Women: Dr Goh Ping Ping Cardiologist Asian Heart & Vascular Centre
 Heart Failure in Women: More than EF? Dr Goh Ping Ping Cardiologist Asian Heart & Vascular Centre Overview Review pathophysiology as it relates to diagnosis and management Rational approach to workup:
Heart Failure in Women: More than EF? Dr Goh Ping Ping Cardiologist Asian Heart & Vascular Centre Overview Review pathophysiology as it relates to diagnosis and management Rational approach to workup:
Drugs acting on the reninangiotensin-aldosterone
 Drugs acting on the reninangiotensin-aldosterone system John McMurray Eugene Braunwald Scholar in Cardiovascular Diseases, Brigham and Women s Hospital, Boston & Visiting Professor, Harvard Medical School
Drugs acting on the reninangiotensin-aldosterone system John McMurray Eugene Braunwald Scholar in Cardiovascular Diseases, Brigham and Women s Hospital, Boston & Visiting Professor, Harvard Medical School
Updates in Congestive Heart Failure
 Updates in Congestive Heart Failure GREGORY YOST, DO JOHNSTOWN CARDIOVASCULAR ASSOCIATES 1/28/2018 Disclosures Edwards speaker on Sapien3 valves (TAVR) Stages A-D and NYHA Classes I-IV Stage A: High risk
Updates in Congestive Heart Failure GREGORY YOST, DO JOHNSTOWN CARDIOVASCULAR ASSOCIATES 1/28/2018 Disclosures Edwards speaker on Sapien3 valves (TAVR) Stages A-D and NYHA Classes I-IV Stage A: High risk
Disclosures. Advances in Chronic Heart Failure Management 6/12/2017. Van N Selby, MD UCSF Advanced Heart Failure Program June 19, 2017
 Advances in Chronic Heart Failure Management Van N Selby, MD UCSF Advanced Heart Failure Program June 19, 2017 I have nothing to disclose Disclosures 1 Goal statement To review recently-approved therapies
Advances in Chronic Heart Failure Management Van N Selby, MD UCSF Advanced Heart Failure Program June 19, 2017 I have nothing to disclose Disclosures 1 Goal statement To review recently-approved therapies
Disclosures. Overview. Goal statement. Advances in Chronic Heart Failure Management 5/22/17
 Disclosures Advances in Chronic Heart Failure Management I have nothing to disclose Van N Selby, MD UCSF Advanced Heart Failure Program May 22, 2017 Goal statement To review recently-approved therapies
Disclosures Advances in Chronic Heart Failure Management I have nothing to disclose Van N Selby, MD UCSF Advanced Heart Failure Program May 22, 2017 Goal statement To review recently-approved therapies
Μαρία Μπόνου Διευθύντρια ΕΣΥ, ΓΝΑ Λαϊκό
 Μαρία Μπόνου Διευθύντρια ΕΣΥ, ΓΝΑ Λαϊκό Diastolic HF DD: Diastolic Dysfunction DHF: Diastolic HF HFpEF: HF with preserved EF DD Pathophysiologic condition: impaired relaxation, LV compliance, LV filling
Μαρία Μπόνου Διευθύντρια ΕΣΥ, ΓΝΑ Λαϊκό Diastolic HF DD: Diastolic Dysfunction DHF: Diastolic HF HFpEF: HF with preserved EF DD Pathophysiologic condition: impaired relaxation, LV compliance, LV filling
Ejection Fraction in Patients With Chronic Heart Failure. Diastolic Heart Failure or Heart Failure with Preserved Ejection Fraction
 Diastolic Heart Failure or Heart Failure with Preserved Ejection Fraction Keith Miller MD Diastolic Heart Failure Risk Factors Common Risk Factors Aging Female gender Obesity Hypertension Diabetes mellitus
Diastolic Heart Failure or Heart Failure with Preserved Ejection Fraction Keith Miller MD Diastolic Heart Failure Risk Factors Common Risk Factors Aging Female gender Obesity Hypertension Diabetes mellitus
Dr.Fayez EL Shaer Consultant cardiologist Assistant professor of cardiology KKUH
 Pulmonary Hypertension in patients with Heart Failure with Preserved Ejection Fraction Dr.Fayez EL Shaer Consultant cardiologist Assistant professor of cardiology KKUH Recent evaluation of available data
Pulmonary Hypertension in patients with Heart Failure with Preserved Ejection Fraction Dr.Fayez EL Shaer Consultant cardiologist Assistant professor of cardiology KKUH Recent evaluation of available data
Diastolic Function. Rick Nishimura Leighton Professor of CV Diseases Mayo Clinic No Disclosures
 Diastolic Function Rick Nishimura Leighton Professor of CV Diseases Mayo Clinic No Disclosures Heart = Pump Heart Failure Systolic Dysfunction Diastolic Dysfunction Diastole is a complex sequence of multiple
Diastolic Function Rick Nishimura Leighton Professor of CV Diseases Mayo Clinic No Disclosures Heart = Pump Heart Failure Systolic Dysfunction Diastolic Dysfunction Diastole is a complex sequence of multiple
Is normal ejection fraction equivalent to normal systolic function?
 Is normal ejection fraction equivalent to normal systolic function? D. Vinereanu University of Medicine, Bucharest, Romania EAE course, Bucharest No 2 nd criterion (out of 3) for the diagnosis of HFNEF:
Is normal ejection fraction equivalent to normal systolic function? D. Vinereanu University of Medicine, Bucharest, Romania EAE course, Bucharest No 2 nd criterion (out of 3) for the diagnosis of HFNEF:
UPDATES IN MANAGEMENT OF HF
 UPDATES IN MANAGEMENT OF HF Jennifer R Brown MD, MS Heart Failure Specialist Medstar Cardiology Associates DC ACP Meeting Fall 2017 Disclosures: speaker bureau for novartis speaker bureau for actelion
UPDATES IN MANAGEMENT OF HF Jennifer R Brown MD, MS Heart Failure Specialist Medstar Cardiology Associates DC ACP Meeting Fall 2017 Disclosures: speaker bureau for novartis speaker bureau for actelion
ACE inhibitors: still the gold standard?
 ACE inhibitors: still the gold standard? Session: Twenty-five years after CONSENSUS What have we learnt about the RAAS in heart failure? Lars Køber, MD, D.Sci Department of Cardiology Rigshospitalet University
ACE inhibitors: still the gold standard? Session: Twenty-five years after CONSENSUS What have we learnt about the RAAS in heart failure? Lars Køber, MD, D.Sci Department of Cardiology Rigshospitalet University
HFpEF, Mito or Realidad?
 HFpEF, Mito or Realidad? Ileana L. Piña, MD, MPH Professor of Medicine and Epidemiology/Population Health Associate Chief for Academic Affairs -- Cardiology Montefiore-Einstein Medical Center Bronx, NY
HFpEF, Mito or Realidad? Ileana L. Piña, MD, MPH Professor of Medicine and Epidemiology/Population Health Associate Chief for Academic Affairs -- Cardiology Montefiore-Einstein Medical Center Bronx, NY
The Myths of Heart Failure with Preserved Ejection Fraction:
 The Myths of Heart Failure with Preserved Ejection Fraction: A misunderstood disease in search of a therapy Scott D. Solomon, MD The Edward D. Frohlich Distinguished Chair Professor of Medicine Harvard
The Myths of Heart Failure with Preserved Ejection Fraction: A misunderstood disease in search of a therapy Scott D. Solomon, MD The Edward D. Frohlich Distinguished Chair Professor of Medicine Harvard
Vitals HR 90 BP 125/58 Tmax 98.7F O2 Sat 97% on NC 2L/min BMP SCr 1.78 K 3.9 Gluc 194 A1c 7.5 Cardiac LVEF 55% NTproBNP 9,200 Troponin 0.
 ALDOSTERONE ANTAGONIST IN HEART FAILURE WITH PRESERVED EJECTION FRACTION ABBREVIATIONS BMP: basic metabolic panel HPI: history of present illness CAD: coronary artery disease HR: heart rate PINHUI (JUDY)
ALDOSTERONE ANTAGONIST IN HEART FAILURE WITH PRESERVED EJECTION FRACTION ABBREVIATIONS BMP: basic metabolic panel HPI: history of present illness CAD: coronary artery disease HR: heart rate PINHUI (JUDY)
Heart Failure with preserved ejection fraction (HFpEF)
") Heart Failure with preserved ejection fraction (HFpEF) Dr. Pierpaolo Pellicori Hull York Medical School Kingston-upon-Hull United Kingdom Conflict of interest: none Heart failure is a contemporary problem
Heart Failure with preserved ejection fraction (HFpEF) Dr. Pierpaolo Pellicori Hull York Medical School Kingston-upon-Hull United Kingdom Conflict of interest: none Heart failure is a contemporary problem
E/Ea is NOT an essential estimator of LV filling pressures
 Euroecho Kopenhagen Echo in Resynchronization in 2010 E/Ea is NOT an essential estimator of LV filling pressures Wilfried Mullens, MD, PhD December 10, 2010 Ziekenhuis Oost Limburg Genk University Hasselt
Euroecho Kopenhagen Echo in Resynchronization in 2010 E/Ea is NOT an essential estimator of LV filling pressures Wilfried Mullens, MD, PhD December 10, 2010 Ziekenhuis Oost Limburg Genk University Hasselt
Treating HF Patients with ARNI s Why, When and How?
 Treating HF Patients with ARNI s Why, When and How? 19 th Annual San Diego Heart Failure Symposium for Primary Care Physicians January 11-12, 2019 La Jolla, CA Barry Greenberg M.D. Distinguished Professor
Treating HF Patients with ARNI s Why, When and How? 19 th Annual San Diego Heart Failure Symposium for Primary Care Physicians January 11-12, 2019 La Jolla, CA Barry Greenberg M.D. Distinguished Professor
THE PROPER APPROACH TO DIAGNOSING HEART FAILURE WITH PRESERVED EJECTION FRACTION
 THE PROPER APPROACH TO DIAGNOSING HEART FAILURE WITH PRESERVED EJECTION FRACTION James C. Fang, MD, FACC Professor and Chief Cardiovascular Division University of Utah School of Medicine Disclosures Data
THE PROPER APPROACH TO DIAGNOSING HEART FAILURE WITH PRESERVED EJECTION FRACTION James C. Fang, MD, FACC Professor and Chief Cardiovascular Division University of Utah School of Medicine Disclosures Data
HFpEF: How to optimise management
 HFpEF: How to optimise management Burkert Pieske M.D. Berlin, Germany Department of Internal Medicine and Cardiology, Campus Virchow Klinikum, Charité University Medicine Berlin, and Department of Internal
HFpEF: How to optimise management Burkert Pieske M.D. Berlin, Germany Department of Internal Medicine and Cardiology, Campus Virchow Klinikum, Charité University Medicine Berlin, and Department of Internal
DECLARATION OF CONFLICT OF INTEREST
 DECLARATION OF CONFLICT OF INTEREST ESC Congress 2011 Pathophysiology of HFPEF Vascular Remodeling & Pulmonary Hypertension Carolyn S.P. Lam MBBS, MRCP, MS Case Presentation 81 yo woman with dyspnoea &
DECLARATION OF CONFLICT OF INTEREST ESC Congress 2011 Pathophysiology of HFPEF Vascular Remodeling & Pulmonary Hypertension Carolyn S.P. Lam MBBS, MRCP, MS Case Presentation 81 yo woman with dyspnoea &
Aldosterone Antagonism in Heart Failure: Now for all Patients?
 Aldosterone Antagonism in Heart Failure: Now for all Patients? Inder Anand, MD, FRCP, D Phil (Oxon.) Professor of Medicine, University of Minnesota, Director Heart Failure Program, VA Medical Center 111C
Aldosterone Antagonism in Heart Failure: Now for all Patients? Inder Anand, MD, FRCP, D Phil (Oxon.) Professor of Medicine, University of Minnesota, Director Heart Failure Program, VA Medical Center 111C
Strain/Untwisting/Diastolic Suction
 What Is Diastole and How to Assess It? Strain/Untwisting/Diastolic Suction James D. Thomas, M.D., F.A.C.C. Cardiovascular Imaging Center Department of Cardiology Cleveland Clinic Foundation Cleveland,
What Is Diastole and How to Assess It? Strain/Untwisting/Diastolic Suction James D. Thomas, M.D., F.A.C.C. Cardiovascular Imaging Center Department of Cardiology Cleveland Clinic Foundation Cleveland,
Overview & Update on the Utilization of the Natriuretic Peptides in Heart Failure
 June 28, 2016 Overview & Update on the Utilization of the Natriuretic Peptides in Heart Failure Linda C. Rogers, PhD, DABCC, FACB. Agenda Overview of the Natriuretic Peptides and Efficacy studies Similarities
June 28, 2016 Overview & Update on the Utilization of the Natriuretic Peptides in Heart Failure Linda C. Rogers, PhD, DABCC, FACB. Agenda Overview of the Natriuretic Peptides and Efficacy studies Similarities
Evidence of Baroreflex Activation Therapy s Mechanism of Action
 Evidence of Baroreflex Activation Therapy s Mechanism of Action Edoardo Gronda, MD, FESC Heart Failure Research Center IRCCS MultiMedica Cardiovascular Department Sesto S. Giovanni (Milano) Italy Agenda
Evidence of Baroreflex Activation Therapy s Mechanism of Action Edoardo Gronda, MD, FESC Heart Failure Research Center IRCCS MultiMedica Cardiovascular Department Sesto S. Giovanni (Milano) Italy Agenda
From PARADIGM-HF to Clinical Practice. Waleed AlHabeeb, MD, MHA Associate Professor of Medicine President of the Saudi Heart Failure Group
 From PARADIGM-HF to Clinical Practice Waleed AlHabeeb, MD, MHA Associate Professor of Medicine President of the Saudi Heart Failure Group PARADIGM-HF: Inclusion Criteria Chronic HF NYHA FC II IV with LVEF
From PARADIGM-HF to Clinical Practice Waleed AlHabeeb, MD, MHA Associate Professor of Medicine President of the Saudi Heart Failure Group PARADIGM-HF: Inclusion Criteria Chronic HF NYHA FC II IV with LVEF
Diastology Disclosures: None. Dias2011:1
 Diastology 2011 James D. Thomas, M.D., F.A.C.C. Cardiovascular Imaging Center Department of Cardiology Cleveland Clinic Foundation Cleveland, Ohio, USA Disclosures: None Dias2011:1 Is EVERYBODY a member!?!
Diastology 2011 James D. Thomas, M.D., F.A.C.C. Cardiovascular Imaging Center Department of Cardiology Cleveland Clinic Foundation Cleveland, Ohio, USA Disclosures: None Dias2011:1 Is EVERYBODY a member!?!
HF-Preserved Ejection Fraction
 HF-Preserved Ejection Fraction Justin A. Ezekowitz, MBBCh MSc FRCPC FACC FESC FAHA Associate Professor, University of Alberta Co-Director, Canadian VIGOUR Centre Cardiologist, Mazankowski Alberta Heart
HF-Preserved Ejection Fraction Justin A. Ezekowitz, MBBCh MSc FRCPC FACC FESC FAHA Associate Professor, University of Alberta Co-Director, Canadian VIGOUR Centre Cardiologist, Mazankowski Alberta Heart
HFpEF: Pathophysiology & Treatment
 HFpEF: Pathophysiology & Treatment Barry A. Borlaug, MD Mayo Clinic, Rochester, MN borlaug.barry@mayo.edu Disclosure Financial Relationships Research Support: Aires Pharmaceuticals, Medtronic, GSK Consulting/Advisory
HFpEF: Pathophysiology & Treatment Barry A. Borlaug, MD Mayo Clinic, Rochester, MN borlaug.barry@mayo.edu Disclosure Financial Relationships Research Support: Aires Pharmaceuticals, Medtronic, GSK Consulting/Advisory
Disclosures for Presenter
 A Comparison of Angiotensin Receptor- Neprilysin Inhibition (ARNI) With ACE Inhibition in the Long-Term Treatment of Chronic Heart Failure With a Reduced Ejection Fraction Milton Packer, John J.V. McMurray,
A Comparison of Angiotensin Receptor- Neprilysin Inhibition (ARNI) With ACE Inhibition in the Long-Term Treatment of Chronic Heart Failure With a Reduced Ejection Fraction Milton Packer, John J.V. McMurray,
DIASTOLIC HEART FAILURE
 DIASTOLIC HEART FAILURE M Mohsen Ibrahim, MD Alexandria, Proposed Criteria for Diastolic Heart Failure ESC Working Group (EHJ 1998) CHF signs/symptoms EF 45% Hemodynamic or echo evidence of diastolic dysfunction
DIASTOLIC HEART FAILURE M Mohsen Ibrahim, MD Alexandria, Proposed Criteria for Diastolic Heart Failure ESC Working Group (EHJ 1998) CHF signs/symptoms EF 45% Hemodynamic or echo evidence of diastolic dysfunction
Satish K Surabhi, MD.FACC,FSCAI,RPVI Medical Director, Cardiac Cath Labs AnMed Health Heart & Vascular Care
 Satish K Surabhi, MD.FACC,FSCAI,RPVI Medical Director, Cardiac Cath Labs AnMed Health Heart & Vascular Care None Fig. 1. Progression of Heart Failure.With each hospitalization for acute heart failure,
Satish K Surabhi, MD.FACC,FSCAI,RPVI Medical Director, Cardiac Cath Labs AnMed Health Heart & Vascular Care None Fig. 1. Progression of Heart Failure.With each hospitalization for acute heart failure,
Akash Ghai MD, FACC February 27, No Disclosures
 Akash Ghai MD, FACC February 27, 2015 No Disclosures Epidemiology Lifetime risk is > 20% for American s older than 40 years old. > 650,000 new cases diagnosed each year. Incidence increases with age: 2%
Akash Ghai MD, FACC February 27, 2015 No Disclosures Epidemiology Lifetime risk is > 20% for American s older than 40 years old. > 650,000 new cases diagnosed each year. Incidence increases with age: 2%
ANGIOTENSIN RECEPTOR-NEPRILYSIN INHIBITORS IN HEART FAILURE FROM CHD
 ANGIOTENSIN RECEPTOR-NEPRILYSIN INHIBITORS IN HEART FAILURE FROM CHD Karen Stout, MD FACC Professor, Medicine/Pediatrics University of Washington Seattle, WA USA No disclosures Case 35 year old man with
ANGIOTENSIN RECEPTOR-NEPRILYSIN INHIBITORS IN HEART FAILURE FROM CHD Karen Stout, MD FACC Professor, Medicine/Pediatrics University of Washington Seattle, WA USA No disclosures Case 35 year old man with
An Integrated Approach to Study LV Diastolic Function
 An Integrated Approach to Study LV Diastolic Function Assoc. Prof. Adriana Ilieşiu, FESC University of Medicine Carol Davila Bucharest, Romania LV Diastolic Dysfunction impaired relaxation (early diastole)
An Integrated Approach to Study LV Diastolic Function Assoc. Prof. Adriana Ilieşiu, FESC University of Medicine Carol Davila Bucharest, Romania LV Diastolic Dysfunction impaired relaxation (early diastole)
Outline. Classification by LVEF Conventional Therapy New Therapies. Ivabradine Sacubitril/valsartan
 New Pharmacological Therapies for Heart Failure Mark Drazner, MD, MSc Clinical Chief of Cardiology Medical Director, CHF/VAD/Transplant James M. Wooten Chair in Cardiology UT Southwestern Medical Center
New Pharmacological Therapies for Heart Failure Mark Drazner, MD, MSc Clinical Chief of Cardiology Medical Director, CHF/VAD/Transplant James M. Wooten Chair in Cardiology UT Southwestern Medical Center
Diastolic Heart Failure. Edwin Tulloch-Reid MBBS FACC Consultant Cardiologist Heart Institute of the Caribbean December 2012
 Diastolic Heart Failure Edwin Tulloch-Reid MBBS FACC Consultant Cardiologist Heart Institute of the Caribbean December 2012 Disclosures Have spoken for Merck, Sharpe and Dohme Sat on a physician advisory
Diastolic Heart Failure Edwin Tulloch-Reid MBBS FACC Consultant Cardiologist Heart Institute of the Caribbean December 2012 Disclosures Have spoken for Merck, Sharpe and Dohme Sat on a physician advisory
2/15/2017. Disclosures. Heart Failure = Big Problem. Heart Failure Update Reducing Hospitalizations and Improving Patient Outcomes 02/18/2017
 Heart Failure Update Reducing Hospitalizations and Improving Patient Outcomes 02/18/2017 Julio A. Barcena, M.D. South Miami Heart Specialists Disclosures I have no relevant commercial relationships to
Heart Failure Update Reducing Hospitalizations and Improving Patient Outcomes 02/18/2017 Julio A. Barcena, M.D. South Miami Heart Specialists Disclosures I have no relevant commercial relationships to
HeFSSA Practitioners Program 2017 Theme The Patient Journey: Feel Good and Live Long. Case Study 2
 HeFSSA Practitioners Program 2017 Theme The Patient Journey: Feel Good and Live Long Case Study 2 HEART FAILURE WITH MID-RANGE EJECTION FRACTION TREATMENT OPTIONS CLINICAL CASE MEDICAL HISTORY 59-year-old
HeFSSA Practitioners Program 2017 Theme The Patient Journey: Feel Good and Live Long Case Study 2 HEART FAILURE WITH MID-RANGE EJECTION FRACTION TREATMENT OPTIONS CLINICAL CASE MEDICAL HISTORY 59-year-old
ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure
 Patients t with acute heart failure frequently develop chronic heart failure Patients with chronic heart failure frequently decompensate acutely ESC Guidelines for the Diagnosis and A clinical response
Patients t with acute heart failure frequently develop chronic heart failure Patients with chronic heart failure frequently decompensate acutely ESC Guidelines for the Diagnosis and A clinical response
Mechanisms of heart failure with normal EF Arterial stiffness and ventricular-arterial coupling. What is the pathophysiology at presentation?
 Mechanisms of heart failure with normal EF Arterial stiffness and ventricular-arterial coupling What is the pathophysiology at presentation? Ventricular-arterial coupling elastance Central arterial pressure
Mechanisms of heart failure with normal EF Arterial stiffness and ventricular-arterial coupling What is the pathophysiology at presentation? Ventricular-arterial coupling elastance Central arterial pressure
The Therapeutic Potential of Novel Approaches to RAAS. Professor of Medicine University of California, San Diego
 The Therapeutic Potential of Novel Approaches to RAAS Inhibition in Heart Failure Barry Greenberg, M.D. Professor of Medicine University of California, San Diego Chain of Events Leading to End-Stage Heart
The Therapeutic Potential of Novel Approaches to RAAS Inhibition in Heart Failure Barry Greenberg, M.D. Professor of Medicine University of California, San Diego Chain of Events Leading to End-Stage Heart
New horizons in HF: potential of new drugs
 New horizons in HF: potential of new drugs Marc A. Pfeffer, MD, PhD Dzau Professor of Medicine, Harvard Medical School Cardiovascular Division, Brigham & Women s Hospital Boston, Massachusetts FINANCIAL
New horizons in HF: potential of new drugs Marc A. Pfeffer, MD, PhD Dzau Professor of Medicine, Harvard Medical School Cardiovascular Division, Brigham & Women s Hospital Boston, Massachusetts FINANCIAL
Left ventricular diastolic function and filling pressure in patients with dilated cardiomyopathy
 Left ventricular diastolic function and filling pressure in patients with dilated cardiomyopathy Bogdan A. Popescu University of Medicine and Pharmacy Bucharest, Romania My conflicts of interest: I have
Left ventricular diastolic function and filling pressure in patients with dilated cardiomyopathy Bogdan A. Popescu University of Medicine and Pharmacy Bucharest, Romania My conflicts of interest: I have
HFpEF 2016 : Comorbidities and Outcomes
 HFpEF 2016 : Comorbidities and Outcomes Christopher M. O Connor, MD, FACC CEO and Executive Director, Inova Heart and Vascular Institute Professor of Medicine, Duke University Editor in Chief, JACC: Heart
HFpEF 2016 : Comorbidities and Outcomes Christopher M. O Connor, MD, FACC CEO and Executive Director, Inova Heart and Vascular Institute Professor of Medicine, Duke University Editor in Chief, JACC: Heart
Diastolic Heart Failure
 Chronic Heart Failure Prevalence overall = 2-3 % Diastolic Heart Failure Patrick Wouters University Hospital Ghent Belgium (Heart Failure + Asymptomatic Ventricular Dysfunction) Prevalence > 70 y = 10-20
Chronic Heart Failure Prevalence overall = 2-3 % Diastolic Heart Failure Patrick Wouters University Hospital Ghent Belgium (Heart Failure + Asymptomatic Ventricular Dysfunction) Prevalence > 70 y = 10-20
Entresto Development of sacubitril/valsartan (LCZ696) for the treatment of heart failure with reduced ejection fraction
 for the treatment of heart failure with reduced ejection fraction") Cardio-Metabolic Franchise Entresto Development of sacubitril/valsartan (LCZ696) for the treatment of heart failure with reduced ejection fraction Randy L Webb, PhD Rutgers Workshop October 21, 2016 Heart
Cardio-Metabolic Franchise Entresto Development of sacubitril/valsartan (LCZ696) for the treatment of heart failure with reduced ejection fraction Randy L Webb, PhD Rutgers Workshop October 21, 2016 Heart
Post Hoc Analysis of the PARADIGM Heart Failure Trial:
 Post Hoc Analysis of the PARADIGM Heart Failure Trial: Pulse Pressure and Outcomes in Heart Failure with Reduced Ejection Fraction Chen-Huan Chen, M.D. Professor, Department of Medicine, National Yang-Ming
Post Hoc Analysis of the PARADIGM Heart Failure Trial: Pulse Pressure and Outcomes in Heart Failure with Reduced Ejection Fraction Chen-Huan Chen, M.D. Professor, Department of Medicine, National Yang-Ming
ESC Guidelines for the Diagnosis and Treatment of Chronic Heart Failure
 ESC Guidelines for the Diagnosis and Treatment of Chronic Heart Failure - 2005 Karl Swedberg Professor of Medicine Department of Medicine Sahlgrenska University Hospital/Östra Göteborg University Göteborg
ESC Guidelines for the Diagnosis and Treatment of Chronic Heart Failure - 2005 Karl Swedberg Professor of Medicine Department of Medicine Sahlgrenska University Hospital/Östra Göteborg University Göteborg
Therapeutic Targets and Interventions. Ali Valika, MD, FACC Advocate Medical Group
 Therapeutic Targets and Interventions Ali Valika, MD, FACC Advocate Medical Group Disclosures: 1. Novartis: Speaker Honorarium Diastolic Heart Failure Diastolic heart failure (DHF) is a major cause of
Therapeutic Targets and Interventions Ali Valika, MD, FACC Advocate Medical Group Disclosures: 1. Novartis: Speaker Honorarium Diastolic Heart Failure Diastolic heart failure (DHF) is a major cause of
New in Heart Failure SGK autumn session 2012
 New in Heart Failure SGK autumn session 2012 Roger Hullin Cardiology Department of Internal Medicine Centre Universitaire Hospitaler Vaudois University of Lausanne ESC Heart Failure Guidelines 2012 Classes
New in Heart Failure SGK autumn session 2012 Roger Hullin Cardiology Department of Internal Medicine Centre Universitaire Hospitaler Vaudois University of Lausanne ESC Heart Failure Guidelines 2012 Classes
Βασιλική Κατσή. Καρδιολόγος ΓNA Ιπποκράτειο
 Βασιλική Κατσή Καρδιολόγος ΓNA Ιπποκράτειο 40 διαφάνειες ίσως Και πρέπει και δικαιούνται ΣΥΧΝΟΤΕΡΑ 76-96% 3343 men and 4199 women followed for 25 years, no HF at baseline BP (mm Hg)
Βασιλική Κατσή Καρδιολόγος ΓNA Ιπποκράτειο 40 διαφάνειες ίσως Και πρέπει και δικαιούνται ΣΥΧΝΟΤΕΡΑ 76-96% 3343 men and 4199 women followed for 25 years, no HF at baseline BP (mm Hg)
Objectives. Systolic Heart Failure: Definitions. Heart Failure: Historical Perspective 2/7/2009
 Objectives Diastolic Heart Failure and Indications for Echocardiography in the Asian Population Damon M. Kwan, MD UCSF Asian Heart & Vascular Symposium 02.07.09 Define diastolic heart failure and differentiate
Objectives Diastolic Heart Failure and Indications for Echocardiography in the Asian Population Damon M. Kwan, MD UCSF Asian Heart & Vascular Symposium 02.07.09 Define diastolic heart failure and differentiate
HFPEF Echo with Strain vs. MRI T1 Mapping
 HFPEF Echo with Strain vs. MRI T1 Mapping Erik Schelbert, MD MS Director, Cardiovascular Magnetic Resonance Assistant Professor of Medicine Heart & Vascular Institute University of Pittsburgh Disclosures
HFPEF Echo with Strain vs. MRI T1 Mapping Erik Schelbert, MD MS Director, Cardiovascular Magnetic Resonance Assistant Professor of Medicine Heart & Vascular Institute University of Pittsburgh Disclosures
Heart Failure. Subjective SOB (shortness of breath) Peripheral edema. Orthopnea (2-3 pillows) PND (paroxysmal nocturnal dyspnea)
 Peripheral edema. Orthopnea (2-3 pillows) PND (paroxysmal nocturnal dyspnea)") Pharmacology I. Definitions A. Heart Failure (HF) Heart Failure Ezra Levy, Pharm.D. HF Results when one or both ventricles are unable to pump sufficient blood to meet the body s needs There are 2 types
Pharmacology I. Definitions A. Heart Failure (HF) Heart Failure Ezra Levy, Pharm.D. HF Results when one or both ventricles are unable to pump sufficient blood to meet the body s needs There are 2 types
HFpEF. April 26, 2018
 HFpEF April 26, 2018 (J Am Coll Cardiol 2017;70:2476 86) HFpEF 50% or more (40-71%) of patients with CHF have preserved LV systolic function. HFpEF is an increasingly frequent hospital discharge. Outcomes
HFpEF April 26, 2018 (J Am Coll Cardiol 2017;70:2476 86) HFpEF 50% or more (40-71%) of patients with CHF have preserved LV systolic function. HFpEF is an increasingly frequent hospital discharge. Outcomes
Evalua&on)of)Le-)Ventricular)Diastolic) Dysfunc&on)by)Echocardiography:) Role)of)Ejec&on)Frac&on)
of)Le-)Ventricular)Diastolic) Dysfunc&on)by)Echocardiography:) Role)of)Ejec&on)Frac&on)") Evalua&on)of)Le-)Ventricular)Diastolic) Dysfunc&on)by)Echocardiography:) Role)of)Ejec&on)Frac&on) N.Koutsogiannis) Department)of)Cardiology) University)Hospital)of)Patras)! I have no conflicts of interest
Evalua&on)of)Le-)Ventricular)Diastolic) Dysfunc&on)by)Echocardiography:) Role)of)Ejec&on)Frac&on) N.Koutsogiannis) Department)of)Cardiology) University)Hospital)of)Patras)! I have no conflicts of interest
Comparing nebivolol and spironolactone in the treatment of heart failure with a preserved ejection fraction
 James Madison University JMU Scholarly Commons Physician Assistant Capstones The Graduate School 5-16-2017 Comparing nebivolol and spironolactone in the treatment of heart failure with a preserved ejection
James Madison University JMU Scholarly Commons Physician Assistant Capstones The Graduate School 5-16-2017 Comparing nebivolol and spironolactone in the treatment of heart failure with a preserved ejection
Baroreflex Activation Therapy: Integrated Autonomic Neuromodulation for Heart Failure and Hypertension
 Baroreflex Activation Therapy: Integrated Autonomic Neuromodulation for Heart Failure and Hypertension Robert S. Kieval, VMD, PhD Founder & Chief Technology Officer, CVRx, Inc. Financial Disclosure I,
Baroreflex Activation Therapy: Integrated Autonomic Neuromodulation for Heart Failure and Hypertension Robert S. Kieval, VMD, PhD Founder & Chief Technology Officer, CVRx, Inc. Financial Disclosure I,
Heart Failure with Preserved EF (HFPEF) Epidemiology and management
 Epidemiology and management") Heart Failure with Preserved EF (HFPEF) Epidemiology and management Karl Swedberg Senior Professor of Medicine Sahlgrenska Academy University of Gothenburg Gothenburg, Sweden e-mail: karl.swedberg@gu.se
Heart Failure with Preserved EF (HFPEF) Epidemiology and management Karl Swedberg Senior Professor of Medicine Sahlgrenska Academy University of Gothenburg Gothenburg, Sweden e-mail: karl.swedberg@gu.se
ABSTARCT...1 FREQUENTLY USED ABBREVIATIONS...2 INTRODUCTION...3. Overview...3. Systolic and diastolic heart failure...4
 TABLE OF CONTENTS ABSTARCT...1 FREQUENTLY USED ABBREVIATIONS...2 INTRODUCTION...3 Overview...3 Systolic and diastolic heart failure...4 Prevalence and incidence of heart failure...4 Prognosis...5 Etiology
TABLE OF CONTENTS ABSTARCT...1 FREQUENTLY USED ABBREVIATIONS...2 INTRODUCTION...3 Overview...3 Systolic and diastolic heart failure...4 Prevalence and incidence of heart failure...4 Prognosis...5 Etiology
Atrial dysfunction and chronotropic incompetence
 Pathophysiology of heart failure with preserved ejection fraction Atrial dysfunction and chronotropic incompetence Vojtech Melenovsky IKEM, Prague, Czech Republic DECLARATION OF CONFLICT OF INTEREST :
Pathophysiology of heart failure with preserved ejection fraction Atrial dysfunction and chronotropic incompetence Vojtech Melenovsky IKEM, Prague, Czech Republic DECLARATION OF CONFLICT OF INTEREST :
Diastolic Heart Failure (HFpEF) Felix J. Rogers, DO, FACOI April 29, 2018
 Felix J. Rogers, DO, FACOI April 29, 2018") Diastolic Heart Failure (HFpEF) Felix J. Rogers, DO, FACOI April 29, 2018 Case presentation MSO, an 81 year old woman was admitted to HFWH because of progressive dyspnea and difficult to control hypertension
Diastolic Heart Failure (HFpEF) Felix J. Rogers, DO, FACOI April 29, 2018 Case presentation MSO, an 81 year old woman was admitted to HFWH because of progressive dyspnea and difficult to control hypertension
Risk Stratification in Heart Failure: The Role of Emerging Biomarkers
 Risk Stratification in Heart Failure: The Role of Emerging Biomarkers David G. Grenache, PhD Associate Professor of Pathology, University of Utah Medical Director, ARUP Laboratories Salt Lake City, UT
Risk Stratification in Heart Failure: The Role of Emerging Biomarkers David G. Grenache, PhD Associate Professor of Pathology, University of Utah Medical Director, ARUP Laboratories Salt Lake City, UT
Nitrate s Effect on Activity Tolerance in Heart Failure with Preserved Ejection Fraction (NEAT) A Randomized Clinical Trial
 A Randomized Clinical Trial") Nitrate s Effect on Activity Tolerance in Heart Failure with Preserved Ejection Fraction (NEAT) A Randomized Clinical Trial Margaret M Redfield On behalf of the NHLBI Heart Failure Clinical Research Network
Nitrate s Effect on Activity Tolerance in Heart Failure with Preserved Ejection Fraction (NEAT) A Randomized Clinical Trial Margaret M Redfield On behalf of the NHLBI Heart Failure Clinical Research Network
Disclosure Statement. Heart Failure: Refreshers and Updates. Objectives. CHF: Chronic Heart Failure. Definitions. Definitions 2/19/2018
 Disclosure Statement Heart Failure: Refreshers and Updates Tracy K. Pettinger, PharmD Clinical Associate Professor College of Pharmacy The planners and presenter of this presentation have disclosed no
Disclosure Statement Heart Failure: Refreshers and Updates Tracy K. Pettinger, PharmD Clinical Associate Professor College of Pharmacy The planners and presenter of this presentation have disclosed no
Heart Failure: Combination Treatment Strategies
 Heart Failure: Combination Treatment Strategies M. McDonald MD, FRCP State of the Heart Symposium May 28, 2011 None Disclosures Case 69 F, prior MIs (LV ejection fraction 25%), HTN No demonstrable ischemia
Heart Failure: Combination Treatment Strategies M. McDonald MD, FRCP State of the Heart Symposium May 28, 2011 None Disclosures Case 69 F, prior MIs (LV ejection fraction 25%), HTN No demonstrable ischemia
Optimal blockade of the Renin- Angiotensin-Aldosterone. in chronic heart failure
 Optimal blockade of the Renin- Angiotensin-Aldosterone Aldosterone- (RAA)-System in chronic heart failure Jan Östergren Department of Medicine Karolinska University Hospital Stockholm, Sweden Key Issues
Optimal blockade of the Renin- Angiotensin-Aldosterone Aldosterone- (RAA)-System in chronic heart failure Jan Östergren Department of Medicine Karolinska University Hospital Stockholm, Sweden Key Issues
Heart Failure Update John Coyle, M.D.
 Heart Failure Update 2011 John Coyle, M.D. Causes of Heart Failure Anderson,B.Am Heart J 1993;126:632-40 It It is now well-established that at least one-half of the patients presenting with symptoms and
Heart Failure Update 2011 John Coyle, M.D. Causes of Heart Failure Anderson,B.Am Heart J 1993;126:632-40 It It is now well-established that at least one-half of the patients presenting with symptoms and
Heart Failure (HF) Treatment
 Treatment") Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
The ACC Heart Failure Guidelines
 The ACC Heart Failure Guidelines Fakhr Alayoubi, Msc,R Ph President of SCCP Cardiology Clinical Pharmacist Assistant Professor At King Saud University King Khalid University Hospital Riyadh-KSA 2017 ACC/AHA/HFSA
The ACC Heart Failure Guidelines Fakhr Alayoubi, Msc,R Ph President of SCCP Cardiology Clinical Pharmacist Assistant Professor At King Saud University King Khalid University Hospital Riyadh-KSA 2017 ACC/AHA/HFSA
Heart Failure with Preserved Ejection Fraction (HFpEF): Natural History and Contemporary Management
: Natural History and Contemporary Management") Heart Failure with Preserved Ejection Fraction (HFpEF): Natural History and Contemporary Management Jason L. Guichard, MD, PhD Greenville Health System Department of Medicine, Carolina Cardiology Consultants
Heart Failure with Preserved Ejection Fraction (HFpEF): Natural History and Contemporary Management Jason L. Guichard, MD, PhD Greenville Health System Department of Medicine, Carolina Cardiology Consultants
Diastolic Function Assessment Practical Ways to Incorporate into Every Echo
 Diastolic Function Assessment Practical Ways to Incorporate into Every Echo Jae K. Oh, MD Echo Hawaii 2018 2018 MFMER 3712003-1 Learning Objectives My presentation will help you to Appreciate the importance
Diastolic Function Assessment Practical Ways to Incorporate into Every Echo Jae K. Oh, MD Echo Hawaii 2018 2018 MFMER 3712003-1 Learning Objectives My presentation will help you to Appreciate the importance
Checklist for Treating Heart Failure. Alan M. Kaneshige MD, FACC, FASE Oklahoma Heart Institute
 Checklist for Treating Heart Failure Alan M. Kaneshige MD, FACC, FASE Oklahoma Heart Institute Novartis Disclosure Heart Failure (HF) a complex clinical syndrome that arises secondary to abnormalities
Checklist for Treating Heart Failure Alan M. Kaneshige MD, FACC, FASE Oklahoma Heart Institute Novartis Disclosure Heart Failure (HF) a complex clinical syndrome that arises secondary to abnormalities
Optimal Adrenergic Blockades in Heart Failure. Jae-Joong Kim MD, PhD Asan Medical Center, University of Ulsan, Seoul, Korea
 Optimal Adrenergic Blockades in Heart Failure Jae-Joong Kim MD, PhD Asan Medical Center, University of Ulsan, Seoul, Korea Contents Harmful effects of adrenergic system in heart failure Clinical studies
Optimal Adrenergic Blockades in Heart Failure Jae-Joong Kim MD, PhD Asan Medical Center, University of Ulsan, Seoul, Korea Contents Harmful effects of adrenergic system in heart failure Clinical studies
Highlight Session Heart failure and cardiomyopathies Michel KOMAJDA Paris France
 Highlight Session 2014 Heart failure and cardiomyopathies Michel KOMAJDA Paris France # esccongress www.escardio.org/esc2014 HEART FAILURE AND CARDIOMYOPATHIES TOPIC 1 Drug Therapy TOPIC 2 Device Therapy
Highlight Session 2014 Heart failure and cardiomyopathies Michel KOMAJDA Paris France # esccongress www.escardio.org/esc2014 HEART FAILURE AND CARDIOMYOPATHIES TOPIC 1 Drug Therapy TOPIC 2 Device Therapy
Heart Failure with Preserved Ejection Fraction: Mechanisms and Management
 Heart Failure with Preserved Ejection Fraction: Mechanisms and Management Jay N. Cohn, M.D. Professor of Medicine Director, Rasmussen Center for Cardiovascular Disease Prevention University of Minnesota
Heart Failure with Preserved Ejection Fraction: Mechanisms and Management Jay N. Cohn, M.D. Professor of Medicine Director, Rasmussen Center for Cardiovascular Disease Prevention University of Minnesota
HFNEF. Heart Failure is
 HFNEF Bijoy K. Khandheria, MD. FASE, FACP, FACC FESC Professor of Medicine University of Wisconsin Director. Echocardiography Services Aurora Health Care No conflicts or off label use CP1173868-1 Heart
HFNEF Bijoy K. Khandheria, MD. FASE, FACP, FACC FESC Professor of Medicine University of Wisconsin Director. Echocardiography Services Aurora Health Care No conflicts or off label use CP1173868-1 Heart
Heart Failure in Women
 Heart Failure in Women Disclosure Professor Sindone has received honoraria, speaker fees, consultancy fees, is a member of advisory boards or has appeared on expert panels for: Professor Andrew Sindone
Heart Failure in Women Disclosure Professor Sindone has received honoraria, speaker fees, consultancy fees, is a member of advisory boards or has appeared on expert panels for: Professor Andrew Sindone
THE DIASTOLIC STRESS TEST: A NEW CLINICAL TOOL? THE CONCEPT OF DIASTOLIC RESERVE
 Thierry C. Gillebert University of Ghent ESC Education Committee THE DIASTOLIC STRESS TEST: A NEW CLINICAL TOOL? THE CONCEPT OF DIASTOLIC RESERVE 1 Case: Ann, 63 years Suffered from metabolic syndrome
Thierry C. Gillebert University of Ghent ESC Education Committee THE DIASTOLIC STRESS TEST: A NEW CLINICAL TOOL? THE CONCEPT OF DIASTOLIC RESERVE 1 Case: Ann, 63 years Suffered from metabolic syndrome
Systolic Dysfunction Clinical /Hemodynamic Guide for Management From Neprilysin Inhibitors to Ivabradine
 Systolic Dysfunction Clinical /Hemodynamic Guide for Management From Neprilysin Inhibitors to Ivabradine Donna Mancini MD Choudhrie Professor of Cardiology Columbia University Speaker Disclosure Amgen
Systolic Dysfunction Clinical /Hemodynamic Guide for Management From Neprilysin Inhibitors to Ivabradine Donna Mancini MD Choudhrie Professor of Cardiology Columbia University Speaker Disclosure Amgen
Pulmonary Hypertension Due to Left Heart Disease
 ACC Middle East Conference 2018 Pulmonary Hypertension Due to Left Heart Disease Ammar Chaudhary, MBChB, FRCPC Advanced Heart Failure & Transplantation King Faisal Specialist Hospital and Research Center
ACC Middle East Conference 2018 Pulmonary Hypertension Due to Left Heart Disease Ammar Chaudhary, MBChB, FRCPC Advanced Heart Failure & Transplantation King Faisal Specialist Hospital and Research Center
What to do for the Patient with Heart Failure and Preserved Ejection Fraction: HFpEF
 What to do for the Patient with Heart Failure and Preserved Ejection Fraction: HFpEF Mariell Jessup MD, FAHA, FACC, FESC Professor of Medicine University of Pennsylvania Philadelphia, Pennsylvania Disclosure:
What to do for the Patient with Heart Failure and Preserved Ejection Fraction: HFpEF Mariell Jessup MD, FAHA, FACC, FESC Professor of Medicine University of Pennsylvania Philadelphia, Pennsylvania Disclosure:
Heart Failure with Reduced EF. Dino Recchia, MD, FACC, FHFSA
 Heart Failure with Reduced EF Dino Recchia, MD, FACC, FHFSA Heart Failure HF is the end phenotype of almost all CV disorders Complex clinical syndrome resulting from any structural or functional impairment
Heart Failure with Reduced EF Dino Recchia, MD, FACC, FHFSA Heart Failure HF is the end phenotype of almost all CV disorders Complex clinical syndrome resulting from any structural or functional impairment
ΚΑΡΔΙΑΚΗ ΑΝΕΠΑΡΚΕΙΑ ΜΕ ΔΙΑΤΗΡΗΜΕΝΟ ΚΛΑΣΜΑ ΕΞΩΘΗΣΗΣ
 ΚΑΡΔΙΑΚΗ ΑΝΕΠΑΡΚΕΙΑ ΜΕ ΔΙΑΤΗΡΗΜΕΝΟ ΚΛΑΣΜΑ ΕΞΩΘΗΣΗΣ ΙΓΝΑΤΙΟΣ ΟΙΚΟΝΟΜΙΔΗΣ MD, PHD, FESC ΑΝΑΠΛΗΡΩΤΗΣ ΚΑΘΗΓΗΤΗΣ ΚΑΡΔΙΟΛΟΓΙΑΣ Β ΚΑΡΔΙΟΛΟΓΙΚΗ ΚΛΙΝΙΚΗ, ΕΘΝΙΚΌ ΚΑΙ ΚΑΠΟΔΙΣΤΡΙΑΚΌ ΠΑΝΕΠΙΣΤΗΜΙΟ ΑΘΗΝΩΝ ΝΟΣΟΚΟΜΕΙΟ
ΚΑΡΔΙΑΚΗ ΑΝΕΠΑΡΚΕΙΑ ΜΕ ΔΙΑΤΗΡΗΜΕΝΟ ΚΛΑΣΜΑ ΕΞΩΘΗΣΗΣ ΙΓΝΑΤΙΟΣ ΟΙΚΟΝΟΜΙΔΗΣ MD, PHD, FESC ΑΝΑΠΛΗΡΩΤΗΣ ΚΑΘΗΓΗΤΗΣ ΚΑΡΔΙΟΛΟΓΙΑΣ Β ΚΑΡΔΙΟΛΟΓΙΚΗ ΚΛΙΝΙΚΗ, ΕΘΝΙΚΌ ΚΑΙ ΚΑΠΟΔΙΣΤΡΙΑΚΌ ΠΑΝΕΠΙΣΤΗΜΙΟ ΑΘΗΝΩΝ ΝΟΣΟΚΟΜΕΙΟ
Atrial dyssynchrony syndrome: An overlooked cause of heart failure with normal ejection fraction
 Atrial dyssynchrony syndrome: An overlooked cause of heart failure with normal ejection fraction JC Eicher, G Laurent, O Barthez, A Mathé, G Bertaux, JE Wolf Heart Failure Treatment Unit, Rhythmology and
Atrial dyssynchrony syndrome: An overlooked cause of heart failure with normal ejection fraction JC Eicher, G Laurent, O Barthez, A Mathé, G Bertaux, JE Wolf Heart Failure Treatment Unit, Rhythmology and
Impact of Nicorandil on Renal Function in Patients With Acute Heart Failure and Pre-Existing Renal Dysfunction
 Impact of Nicorandil on Renal Function in Patients With Acute Heart Failure and Pre-Existing Renal Dysfunction Masahito Shigekiyo, Kenji Harada, Ayumi Okada, Naho Terada, Hiroyoshi Yoshikawa, Akira Hirono,
Impact of Nicorandil on Renal Function in Patients With Acute Heart Failure and Pre-Existing Renal Dysfunction Masahito Shigekiyo, Kenji Harada, Ayumi Okada, Naho Terada, Hiroyoshi Yoshikawa, Akira Hirono,
2017 Summer MAOFP Update
 2017 Summer MAOFP Update. Cardiology Update 2017 Landmark Trials Change Practice Guidelines David J. Strobl, DO, FNLA Heart Failure: Epidemiology More than 4 million patients affected 400,000 new cases
2017 Summer MAOFP Update. Cardiology Update 2017 Landmark Trials Change Practice Guidelines David J. Strobl, DO, FNLA Heart Failure: Epidemiology More than 4 million patients affected 400,000 new cases
Management of chronic heart failure: update J. Parissis Attikon University Hospital
 Management of chronic heart failure: update 2015 J. Parissis Attikon University Hospital Disclosures: received honoraria for lectures from Servier, Pfizer, Novartis Discharges in Thousands Heart Failure
Management of chronic heart failure: update 2015 J. Parissis Attikon University Hospital Disclosures: received honoraria for lectures from Servier, Pfizer, Novartis Discharges in Thousands Heart Failure
WHAT S NEW IN HEART FAILURE
 WHAT S NEW IN HEART FAILURE Drugs, Devices and Diagnostics John M. Herre, MD, FACC, FACP Director, Advanced Heart Failure Program Sentara Helathcare Professor of Medicine Eastern Virginia Medical School
WHAT S NEW IN HEART FAILURE Drugs, Devices and Diagnostics John M. Herre, MD, FACC, FACP Director, Advanced Heart Failure Program Sentara Helathcare Professor of Medicine Eastern Virginia Medical School
Heart Failure Clinician Guide JANUARY 2018
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Value of echocardiography in chronic dyspnea
 Value of echocardiography in chronic dyspnea Jahrestagung Schweizerische Gesellschaft für /Schweizerische Gesellschaft für Pneumologie B. Kaufmann 16.06.2016 Chronic dyspnea Shortness of breath lasting
Value of echocardiography in chronic dyspnea Jahrestagung Schweizerische Gesellschaft für /Schweizerische Gesellschaft für Pneumologie B. Kaufmann 16.06.2016 Chronic dyspnea Shortness of breath lasting
Disclosure Information : No conflict of interest
 Intravenous nicorandil improves symptoms and left ventricular diastolic function immediately in patients with acute heart failure : a randomized, controlled trial M. Shigekiyo, K. Harada, A. Okada, N.
Intravenous nicorandil improves symptoms and left ventricular diastolic function immediately in patients with acute heart failure : a randomized, controlled trial M. Shigekiyo, K. Harada, A. Okada, N.
Heart Failure Medical and Surgical Treatment
 Heart Failure Medical and Surgical Treatment Daniel S. Yip, M.D. Medical Director, Heart Failure and Transplantation Mayo Clinic Second Annual Lakeland Regional Health Cardiovascular Symposium February
Heart Failure Medical and Surgical Treatment Daniel S. Yip, M.D. Medical Director, Heart Failure and Transplantation Mayo Clinic Second Annual Lakeland Regional Health Cardiovascular Symposium February
LCZ696: LA NUOVA RIVOLUZIONE NELLA TERAPIA DELLO SCOMPENSO CARDIACO. Dario Leosco Università di Napoli Federico II
 LCZ696: LA NUOVA RIVOLUZIONE NELLA TERAPIA DELLO SCOMPENSO CARDIACO Dario Leosco Università di Napoli Federico II Projected changes in cardiovascular diseases CVD Deaths Increase 33% CVD DALYS 22% CAD
LCZ696: LA NUOVA RIVOLUZIONE NELLA TERAPIA DELLO SCOMPENSO CARDIACO Dario Leosco Università di Napoli Federico II Projected changes in cardiovascular diseases CVD Deaths Increase 33% CVD DALYS 22% CAD