TAVI SURVEY. Performed by the ESC Council for Cardiology Practice
|
|
|
- Dana Lambert
- 5 years ago
- Views:
Transcription
1 TAVI SURVEY Performed by the ESC Council for Cardiology Practice BACKGROUND To evaluate the knowledge and the behaviour of a large community of cardiologists working in different settings, both in hospital and in out of hospital practice, the Council for Cardiology Practice developed a survey based on a questionnaire to submit to cardiologists who have subscribed to the Council s Newsletter and to the Council s E-Journal of Cardiology Practice. The aims of the survey were: To analyse the knowledge and the application of current knowledge about TAVI methodology for aortic valve replacement To analyse the behaviour of Cardiologists in Practice on this specific topic To understand how cardiologists are seeing the future of TAVI procedures To study possible implementation problems and solutions in the application of guidelines on Valvular Heart Disease of the European Society of Cardiology and of suggestions of scientific literature about the topic To verify in the future the modification of behaviour with a similar survey in the next years. METHOD The questionnaire was sent to 50,840 cardiologists who have subscribed to the E-journal and/or electronic Newsletter of the Council for Cardiology Practice, with a link to the website hosting the questionnaire. Data collected were anonymous. After the questions regarding the demographic characteristics, data regarding the answers about the scientific contents of the survey from N 6 to N 18, were matched by groups of: Age (Under 40 years / From 40 to 50 years / Over 50 years Groups 1, 2 and 3) Professional status (In University or normal hospital / Cardiologist in practice Groups 4 and 5) World region (Africa / Asia + Oceania / Europe / North America + South & Central America Groups 6, 7, 8 and 9) to verify possible differences among the answers by these groups and the possible statistic differences. The data regarding Age and World Regions groups were analyzed versus their complement in the sample. For the professional status, General Practitioners and other activities were excluded from the statistical analysis: Cardiologist in University and Cardiologist in Hospital group data were compared with the data from Cardiologist in Practice group. The profile of each group was determined by highlighting significant differences in the answers to questions Page 1
2 Significant differences => 99% => p-value 0, Significant differences => 95% => 0,01 < p-value 0, Significant differences => 90% => 0,05 < p-value 0,1 RESULTS AND DESCRIPTIVE ANALYSIS were the respondents to questions 1-5 (Q1-Q5). The data about the scientific contents were obtained from respondents that fully answered to questions 6-18 (Q8-Q18). The statistical analysis concentrated on the sample of these questionnaires. The responders of the Syncope Survey of the Council for Cardiology Practice were and of the Atrial Fibrillation Survey were DEMOGRAPHICS CHARACTERISTICS: In tables and in graphs 1, 2, 3 and 5 are summarized the demographic characteristics of the sample, with both data about the whole group of responders and the group of responders who completed the answers from Q6 to Q Gender Total % Respondent Q6 to Q18 % Female ,6% ,9% Male ,4% ,1% answered question ,0% ,0% skipped question 0 / 0 / Page 2


3 2. Age Total % Respondent Q6 to Q18 % Under 30 years 103 7,2% 81 6,5% From 30 to 40 years ,7% ,3% 35,8% Group 1 From 41 to 50 years ,5% ,7% 22,7% Group 2 From 51 to 60 years ,2% ,3% From 61 to 70 years ,5% ,3% 41,5% Group 3 Over 71 years 26 1,8% 25 2,0% answered question ,0% ,0% skipped question 0 / 0 / Page 3
4 3. Activity Total % Respondent Q6 to Q18 % General Practitioner 55 3,9% 46 3,7% Cardiologist in University Cardiologist in Hospital ,9% ,7% ,7% ,7% 57,4% Group 4 Cardiologist in Practice ,9% ,8% 28,8% Group 5 Other ,5% ,1% answered question ,0% ,0% skipped question 0 / 0 / Page 4

5 5. Region Total % Respondent Q6 to Q18 % Africa 49 3,4% 42 3,4% 3,4% Group 6 Asia ,1% ,4% Oceania 18 1,3% 14 1,1% 11,6% Group 7 Europe ,3% ,5% 77,5% Group 8 North America 15 1,1% 13 1,0% South & Central America 84 5,9% 81 6,5% 7,6% Group 9 answered question ,0% ,0% skipped question 0 / 0 / The number of responders to the survey was similar to that of the surveys performed by the Council for Cardiology Practice about Cardiology Practice and about Syncope Guidelines, while a higher number of respondents was observed for the survey about antithrombotic treatment in Atrial Fibrillation. The distribution of the responders for: Sex Age Hospital vs non-hospital Country was similar to that of the previous surveys of the Council for Cardiology Practice. Page 5
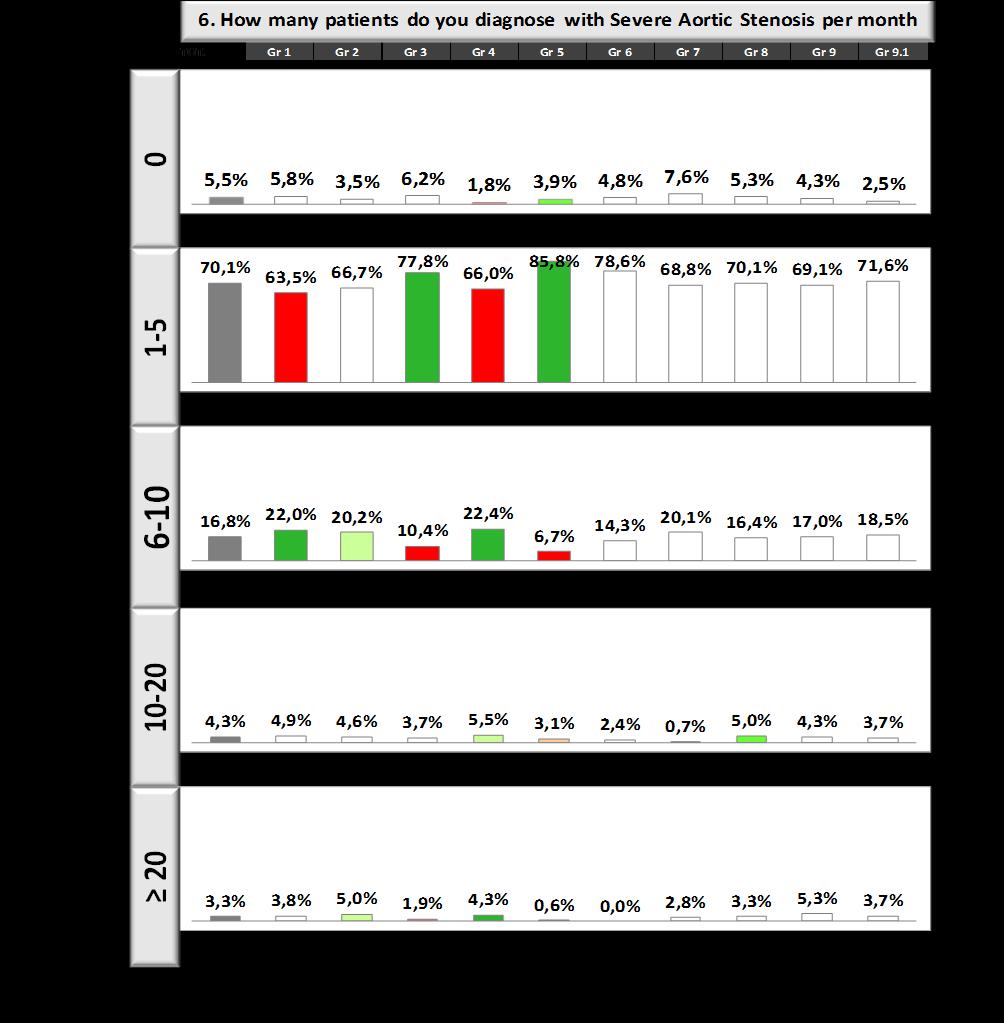
6 RESULTS TO THE SCIENTIFIC QUESTIONS FROM 6 TO 18 The respondents answering completely to these questions were and on these answers is concentrated the analysis. Here are summarized the results considering the answers to the single questions from 6 to 18 both regarding the total of the answers and the subgroups. The tables and graphs showing the subgroups data report the total data of the answers to the specific question and the data divided according to the pre-specified subgroups shown in red if the result of that group is significantly under the mean data or in green if the result of that group is significantly higher than the mean data. Please note that sometimes the red or green color does not necessarily correspond to a good or bad result it has only a mathematic meaning. 6. How many patients do you diagnose with Severe Aortic Stenosis per month approximately? Total % ,5% ,1% ,8% ,3% > ,3% answered question ,0% skipped question 0 / Page 6
7 6. How many patients do you diagnose with Severe Aortic Stenosis per month approximately? 70,1% 5,5% 16,8% 4,3% 3,3% >20 The large majority of the responders are facing a number of patients with severe aortic stenosis per month variable from 1 to 10. Consequently this is a high number of patients who have undergone cardiologic evaluation, who have been diagnosed and who have possible indication to aortic valve replacement and to TAVI procedure, By the groups analysis it seems that young cardiologists and hospital cardiologists have a larger opportunity to diagnose severe aortic stenosis than oldest cardiologists and non-hospital cardiologists, while non significant differences were observed according to the world regions. Page 7
8 Page 8
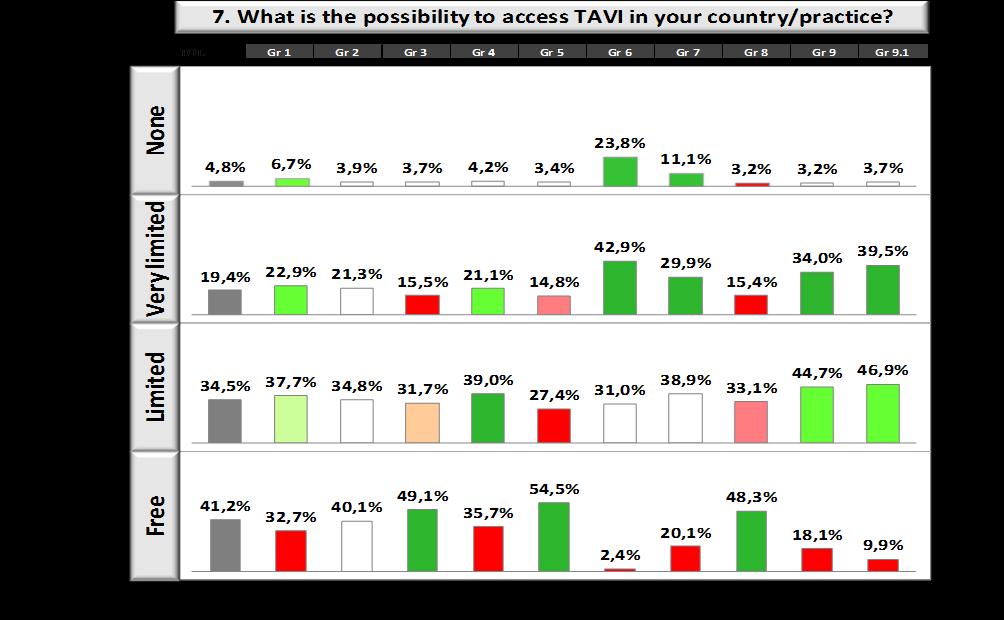
9 7. What is the possibility to access TAVI in your country/practice? Total % Free ,2% Limited ,5% Very limited ,4% None 60 4,8% answered question ,0% skipped question 0 / 7. What is the possibility to access TAVI in your country/practice? 41,2% 34,5% 19,4% 4,8% Free Limited Very limited None More than 40% of responders have free access to TAVI. It seems a very good result. But the groups analysis shows some expected and some non-expected data: youngest cardiologists and hospital cardiologists seem to have less free access to TAVI than their oldest and non-hospital colleagues. Cardiologists from Africa and Asian countries have less free access than European cardiologists to TAVI. Page 9
10 Page 10
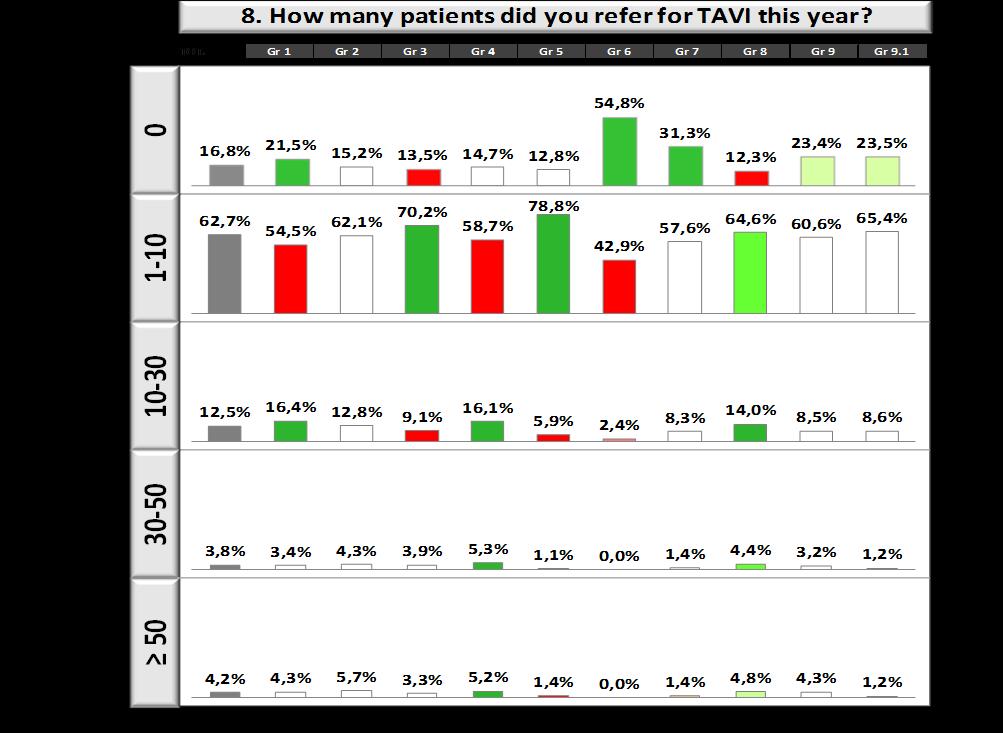
11 8. How many patients did you refer for TAVI this year? Total % ,8% ,7% ,5% ,8% > ,2% answered question ,0% skipped question 0 / 9. If you replied 0 to question 8: please give the main reason? If you did not reply 0 to question 8, please go directly to question 10. Total % I don't believe in TAVI 5 2,6% Long waiting list 18 9,5% No patients eligible 71 37,4% TAVI unavailable 96 50,5% answered question ,0% skipped question 19 / Page 11

12 8. How many patients did you refer for TAVI this year? 62,7% 16,8% 12,5% 3,8% 4,2% >50 9. If you replied 0 to question 8: please give the main reason? 37,4% 50,5% 2,6% 9,5% I don't believe Long waiting No patients TAVI More than 60% of responders referred from 1 to 10 patients for TAVI in the last year. Among the responders the youngest cardiologists were prevalent for the answer no patients or 10 to 30 patients referred for TAVI / year, while responders 1 to 10 patients were the oldest and the nonhospital cardiologists. Africa and Asian regions have the largest percentage of responders no patients referred for TAVI, while the majority of cardiologists responders 1 to 10 and more patients referred are coming from Europe. If a cardiologist answered to have no referred patient for TAVI, the reason was not availability of TAVI for youngest and for hospital cardiologists, without clear differences for world regions. Page 12
13 Page 13

14 10. What is for you the main reason to indicate a TAVI vs. an AV replacement? Total % Age 117 9,4% Comorbidities ,8% Patients choice 24 1,9% Surgical Risk Score ,9% answered question ,0% skipped question 0 / Page 14


15 10. What is for you the main reason to indicate a TAVI vs. an AV replacement? 31,8% 56,9% 9,4% 1,9% Age Comorbidities Patients choice Surgical Risk Score The surgical risk score is the main reason for the indication of a TAVI procedure. Youngest cardiologists seems to prefer TAVI in patients with comorbidities, while for the other reasons there are no significant differences for age and world regions. Page 15
16 11. What is the main reason for not referring a patient for valve replacement? Total % Patient uncomfortable with the procedure ,0% Personal assessment of high-risk or not operable patient ,5% Prefer medical treatment 50 4,0% Short life-expectancy ,5% answered question ,0% skipped question 0 / 11. What is the main reason for not referring a patient for valve replacement? 55,5% 10,0% 4,0% 30,5% Patient Personal assessment Prefer Short A high surgical risk and/or a short life expectancy are the main reasons leading the responders to avoid a valve replacement. No differences according to ages were shown, while non-hospital cardiologists slightly indicate that patients may be uncomfortable with TAVI. The analysis for world regions indicates a significant difference for Asia group, where respondents prefer medical therapy and are thinking that patients may be uncomfortable with TAVI. European cardiologists are significantly less indicating medical treatment. Page 16

17 12. What is in your opinion the main possible complication of TAVI? Total % Aortic regurgitation ,4% Conduction defects ,5% Stroke ,9% Vascular complication ,1% answered question ,0% skipped question 0 / 12. What is in your opinion the main possible complication of TAVI? 22,4% 23,5% 28,9% 25,1% Aortic Conduction Stroke Vascular The believed main complications of TAVI are equally distributed among aortic regurgitation, conduction defects, stroke and vascular complication. This last possibility seems to be an occurrence of the past years and not common with the new materials and procedures. Aortic regurgitation Page 17

18 seems to be under-evaluated as possible complication. Youngest and hospital cardiologists are significantly more worried by conduction defects, while oldest and non hospital cardiologists by stroke. No significant differences were shown by region groups, except for American cardiologists indicating mainly vascular complications as main complication of TAVI. Page 18
19 13. What is in your opinion the main benefit of patients with TAVI? Total % Faster recovery time ,7% Improving quality of life ,2% Less operative pain 20 1,6% Minimal-invasive surgery ,6% answered question ,0% skipped question 0 / 13. What is in your opinion the main benefit of patients with TAVI? 33,7% 37,2% 27,6% 1,6% Faster Improving Less operative Minimal-invasive If the surgical risk is the main reason to prefer TAVI, however the main benefit that cardiologists are expecting is regarding the quality of life and a faster recovery time. These answers were indicated by all age groups and by cardiologists working in or out of hospital. European cardiologists indicate a faster recovery time while American cardiologists a quality of life improvement as main objectives of TAVI. Page 19

20 14. Who follows up TAVI patients in your experience? Total % Cardiac Surgeon 76 6,1% Haemodinamist ,6% Heart Team ,8% You directly ,8% answered question ,0% skipped question 0 / 14. Who follows up TAVI patients in your experience? 49,8% 41,8% 6,1% 12,6% Cardiac Surgeon Haemodinamist Heart Team You directly The majority of responders indicate in the Heart Team as responsible for the follow up of a TAVI patient. However some significant differences were shown for every analysis group. Younger Page 20
 by a Heart Team.")
21 cardiologists and hospital cardiologists seems to follow directly TAVI patients significantly less than their oldest and non-hospital colleagues and to let the patients be followed-up by haemodinamists, and (in hospital) by a Heart Team. This solution is significantly more frequent in Africa and Asian countries, while in Europe cardiologists are choosing more the you directly option and less frequently the Heart Team option. Page 21
22 15. What is in your opinion the most important issue in TAVI patients follow-up? Total % Compliance to medication and control ,0% Echocardiographic findings ,3% NYHA class ,7% Treatment of complications ,9% answered question ,0% skipped question 0 / 15. What is in your opinion the most important issue in TAVI patients follow-up? 15,0% 26,3% 40,7% 17,9% Compliance to Echocardiographic NYHA class Treatment of Most responders indicate NYHA class as the most important issue of TAVI follow-up, without great differences per age, professional status and world regions. Page 22


23 16. In your opinion, could TAVI be now or in the future a first option for AV replacement not only reserved to high risk patients? Total % Yes ,5% No ,5% answered question ,0% skipped question 0 / 16. In your opinion, could TAVI be now or in the future a first option for AV replacement not only reserved to high risk patients? 82,5% 17,5% Yes No Eight responders in ten are thinking that TAVI procedures may be not only a procedure reserved for high risk patients and will be used more diffusely as first option for aortic replacement. No Page 23


24 statistically relevant differences were found for any analysis group. Page 24
25 17. What is the maximum age you consider for a TAVI patients? Total % ,9% ,6% ,9% > ,3% answered question ,0% skipped question 4 / 17. What is the maximum age you consider for a TAVI patients? 5,9% 14,7% 31,0% 48,4% > 90 Nearly fifty percent of responders are indicating a very high age as limit for TAVI indication, but a larger percentage of the young cardiologists are considering 80 years as upper limit of age, and this limit is more indicated by African and Asian cardiologists. Page 25

26 18. How do you proceed with elderly patients (age > 75) who are affected by severe aortic stenosis? Total % Medication 58 4,7% No treatment 6 0,5% Referring to a heart-clinic for aortic replacement with a prosthetic valve ,2% Referring to a heart-clinic for TAVI ,7% answered question ,0% skipped question 0 / 18. How do you proceed with elderly patients (age > 75) who are affected by severe aortic stenosis? 49,2% 45,7% 4,7% 0,5% Medication No treatment Referring to a Referring to a Most responders are sending patients with aortic stenosis in similar percentages to a surgical Page 26

27 prosthetic replacement and to a TAVI replacement. A significant percentage of young cardiologists however is choosing medication as possible treatment, while the oldest and non-hospital colleagues seems still prefer the surgical replacement. In the following pictures the data are shown in a different way that summarizes the most important findings of every subgroup, underlining the differences in respect to the mean result of the whole number of respondents. Page 27
28 The younger cardiologists seem to have less availability of TAVI, are thinking that the conduction defects are the most important issue of TAVI implant, seem to diagnose an higher number of aortic stenosis, but are referring less patients for TAVI and are using an higher level of medication treatment. Moreover they seem less prone to TAVI in patients with an age over 80 years and after a TAVI less frequently are following directly the patients but are referring them to the haemodinamist or to the surgeon Page 28

29 The group age from 41 to 50 years offers a level of answers more similar to the mean value of every answer. This group seems to prefer that the follow-up of a TAVI patient will be supervised by the Heart Team. The group of cardiologists of older age (> 50 years) diagnose less aortic stenosis (1-5 cases monthly), but are referring a higher number of patients/year for TAVI. However in an old patient Page 29

30 with severe aortic stenosis they seem to prefer to referral to the heart-clinic for aortic replacement. Regarding TAVI, they seem to have more free access than younger colleagues, they are following directly the patients during the follow-up, and during it they are consider stroke as the main issue of complication of TAVI. Hospital cardiologists are diagnosing more patients with aortic stenosis than their colleagues, but surprisingly they seem to have less free access to TAVI; at the other end they are referring a higher number of patients for TAVI, considering comorbidities the main reason for this indication and conduction defects as main issues among the possible complications of follow-up. The Heart Team is preferred in this group as responsible for the follow-up of the patients. Page 30
31 Cardiologists working in out of hospital settings are diagnosing a mean of 1 to 5 patients with aortic stenosis for month and are referring for TAVI from 1 to 10 patients per year; as a paradox they declare to have freer access than their hospital colleagues to TAVI and they feel freer to follow-up directly the patient after a TAVI implant. They are considering stroke as the main complication of TAVI procedure. Page 31

32 Cardiologists working in Africa, as expected have no or very limited access to TAVI, and frequently have not referred patients for this procedure. They are considering an age of more than 80 years for TAVI and they are considering the Heart Team the most appropriate choice for patient follow-up. Page 32
33 Cardiologists working in the Asia-Oceania area give results similar to that of Africa regarding availability of TAVI and number of patients referred for TAVI; moreover they are still using a medical approach in aortic stenosis and they are considering a very low age (70 years) for the indication of TAVI. Also in this group is preferred the Heart Team for the follow up of the patient after TAVI. European colleagues seem to have a more free access to TAVI, are following directly or are referring the patient to the heamodinamist after the procedure, are considering TAVI for very old patients for (> 90 years), but in old patients with severe aortic stenosis they prefer to send the patient to an aortic valve replacement. Page 33

34 And colleagues from gave answers generally not very different from the mean of the responders, except for the very limited option for TAVI availability and for the confidence in a better quality of life of TAVI patients. Page 34
35 DISCUSSION The European Society of Cardiology organized in the past leading surveys about different topics in different settings, for example on prevention like the series of EUROASPIRE or the surveys on heart failure and on atrial fibrillation. These surveys are generally multi-centre retrospective analysis of the management of a specific aspect of cardiology, realized using data-bases of patients followed in a specific time in selected hospital settings. The surveys proposed by the Council for Cardiology Practice, unlike the commonly published surveys, are based on the direct interview of a population of cardiologists with a wide dissemination of geographic and professional conditions (mainly hospital setting) and not on data derived from patient databases. This way of collecting information about a clinic topic is somewhat different and in our thinking represents a sort of intention to treat questionnaire. Although with many limitations, due to the characteristics of our sample, not randomized and with many selection bias, but that however is fully obtained on a volunteer basis and can be considered honest and representative of a large general population of cardiologists, working both in hospital (the majority) or in an out-of-hospital setting, the data derived from the TAVI patients survey of the ESC Council for Cardiology Practice gives, in the view of the authors, some interesting information on the knowledge of this topic. The surveys are intended to offer a snapshot of the current clinical practice about a specific topic and their importance will be increasing over time. The rate of adherence to this survey on TAVI treatment (<3%) is still low, less than the survey for atrial fibrillation, though in line with surveys on other important topics (i.e. syncope) previously conducted by the Council for Cardiology Practice. Similarly, the distribution of the responders by gender, age, hospital vs non-hospital activity and Countries was similar to that of the previous surveys. This survey mostly included European cardiologists. Answers were divided by groups based on: Age (Under 40 years / From 40 to 50 years / Over 50 years Groups 1, 2 and 3) Professional status (In University or normal hospital / Cardiologist in practice Groups 4 and 5) World region (Africa / Asia + Oceania / Europe / North America + South & Central America Groups 6, 7, 8 and 9). The scientific questions numbered 6 to 18 of the questionnaire explored how TAVI issues are felt by the cardiology community and were: 6. How many patients do you diagnose with Severe Aortic Stenosis per month approximately? 7. What is the possibility to access TAVI in your country/practice? 8. How many patients did you refer for TAVI this year? 9. If you replied 0 to question 8: please give the main reason? If you did not reply 0 to question 8, please go directly to question What is for you the main reason to indicate a TAVI vs. an AV replacement? 11. What is the main reason for not referring a patient for valve replacement? Page 35
36 12. What is in your opinion the main possible complication of TAVI? 13. What is in your opinion the main benefit of patients with TAVI? 14. Who follows up TAVI patients in your experience? 15. What is in your opinion the most important issue in TAVI patients follow-up? 16. In your opinion, could TAVI be now or in the future a first option for AV replacement not only reserved to high risk patients? 17. What is the maximum age you consider for a TAVI patients? 18. How do you proceed with elderly patients (age > 75) who are affected by severe aortic stenosis? The answers to these questions showed expected results, but also some results that may be debatable and partially unexpected or disappointing and may be summarized as follows: Question 6. Most cardiologists (87% - especially young and hospital cardiologists) diagnose 1-10 patients/ month with severe aortic stenosis. Do you diagnose means a new diagnosis per month and highlights the large population of patients with aortic stenosis and possible indication to aortic valve replacement or TAVI seen by the cardiologist population, working both in hospital or in an out-of-hospital setting. Question 7. Due to the limited economic resources, we are used to believe that the main limit to TAVI is the restricted access to the procedure. Unexpectedly, more than 40% of responders reported a free access to TAVI. However, this free access mainly involves the oldest cardiologists (and this could be related to a better established and functioning network with TAVI hospitals) and non-hospital colleagues. The latter findings are quite unexpected. A possible explanation is that non-hospital colleagues may refer their TAVI patients to private structures or they have, according to their freedom from a specific hospital, a larger network than their hospital colleagues with a larger availability of different public structures. Questions 8/9. While 4% of cardiologists referred more than 50 patients to TAVI, still a percentage of almost 17% did not refer any patient to TAVI in the current year. The main reason was unavailability of TAVI (50.5%). Still a 2.6% of cardiologists do not believe in TAVI, despite the striking results of large randomized trials. Spreading of a state-of-the-art TAVI culture has a critical role, especially for the youngest and non-hospital cardiologists, and contributes to extend the eligibility criteria. Cardiologists from Africa and Asian Countries, as expected, have less access and referral to TAVI than European cardiologists. Question 10. The main reason for TAVI preference over aortic valve replacement (AVR) was considered the surgical risk score, then comorbidities, age and lastly patient s choice. This sounds evidence-based, though it is important to remember that risk scores often do not include patient s frailty. Also, results from large trials in intermediate risk patients favour TAVI over AVR, and there is a current debate on extending TAVI to low risk patients also. Question 11. An unexpected surprising data was the still present, though limited (4%), percentage Page 36
37 of cardiologists who would prefer medical treatment over AVR, against all the evidence and against the common indications of Guidelines. This result is mainly coming from the Asian and African regions, and probably related to the poor situation of the National Health Systems of those countries. Only a very short life-expectancy and/or a prohibitive risk should be criteria for not referring a patient with severe aortic stenosis to either AVR or TAVI. Question 12. Disappointingly, although stroke is not a frequently reported complication after TAVI, and all trials have shown a lower risk with TAVI as compared to AVR, still 28.9% of cardiologists reported it as the main possible complication of TAVI. Vascular complications decrease with the learning curve and prosthesis profile. Conduction defects are prosthesis related. Aortic regurgitation, though common, is often mild, especially with modern prostheses. Question 13. The most important benefit felt after TAVI is considered to be the improvement of quality of life. The bibliography about TAVI seems to show that both AVR and TAVI have a similar impact on quality of life, while the main TAVI benefits are considered to be inferior invasiveness, less pain and faster recovery. Question 14. The heart team should take in charge post TAVI patients for almost 50% of the responders. This is a good sign, but a centralized follow-up may be difficult for all TAVI patients and should coexist with the possibility for the cardiologist to directly follow those patients. Hopefully, more than 40% of cardiologists directly follow the patients after TAVI. This happens especially in Europe, maybe as a consequence of a more extensive culture regarding TAVI aspects. Question 15. Low emphasis was put on compliance to medication and controls in post TAVI patients, while the majority of focus was on NYHA class. This may highlight an under-treatment of post TAVI patients, while this should be mandatory considering their complexity. Question 16. It is encouraging to note the high percentage of cardiologists for which TAVI may become an option also for mean or low risk patients in the treatment of aortic stenosis. In the near future TAVI will be offered more extensively, and there is great concordance on this opinion also in the literature. Question 17. Results of TAVI are also good in patients >90 years old, but not all responders believe an high age compatible with TAVI (oddly for younger cardiologists). Actually, more than age, life expectancy > 1 year should be the real limit for the indication to TAVI. Question 18. An almost equal percentage of cardiologists would refer a patient on the sole basis of his age to AVR or TAVI. This means that there is not a definite approach and the indications of treatment are not clear if age category is considered the main issue and when surgical risk or comorbidities are not the decisive issues. Probably TAVI will be considered as the standard approach following current trials results. Unfortunately there is still a ~5% who would propose medical treatment (or nothing!). Page 37
38 CONCLUSIONS The findings of the survey highlight several important issues: The population of patients of aortic stenosis is important and increasing. The main strategy to increase TAVI access may be the creation of functional networks involving single out-of-hospital cardiologists, hospitals with and without TAVI, eventually including private for those patients with private insurances or with some reimbursement possibility. Strategies to increase TAVI referral are important, since the main reason of missed access to TAVI was still its unavailability (50.5%). However the diffusion of knowledge regarding TAVI (trial results, technical aspects) plays a pivotal role. TAVI indication should be guided not only by surgical risk scores There is no evidence of any benefit of medical treatment for aortic stenosis patients and TAVI is a comfortable procedure even in elderly patients. Still the knowledge of TAVI features should play a pivotal role for the right choice of treatment of these patients. The most frequent complication after TAVI is different from the most feared one. There is still some confusion regarding the occurrence of stroke and vascular complications after TAVI, and scientific societies should improve the knowledge about this issue among cardiologists. AVR and TAVI have a similar impact on quality of life. The main TAVI benefits (thus the preference criterion) regard less invasiveness and pain and faster recovery Post TAVI follow-up by the heart team seems to be the favourite choice, however a widespread knowledge of post TAVI issues may extend the portion of cardiologists who will directly follow post TAVI patients in the future. Clinical status post TAVI should be monitored and periodically re-assessed to prevent worsening of the NYHA class: NYHA class is not the target but the expected result of a good follow-up. The main opinion is that TAVI will become a first option therapy in the near future and is already considered as a therapeutic option even in patients aged > 90 years old; this is an encouraging finding about the correct treatment of aortic stenosis. Further trials will better clarify the correct approach in patients > 75 years with no other preferential policy for TAVI or AVR. TAVI is perceived to become a first option therapy in the near future. However, despite results from large randomized and observational trials, there are still some problems regarding a correct Page 38
39 knowledge of the feasibility and safety of the TAVI procedure, and of its complications. Page 39
VASCULAR DISEASE MANAGEMENT SURVEY FROM THE ESC COUNCIL FOR CARDIOLOGY PRACTICE AND THE ESC WORKING GROUP ON AORTA AND PERIPHERAL VASCULAR DISEASES
 VASCULAR DISEASE MANAGEMENT SURVEY FROM THE ESC COUNCIL FOR CARDIOLOGY PRACTICE AND THE ESC WORKING GROUP ON AORTA AND PERIPHERAL VASCULAR DISEASES RICCARDO ASTEGGIANO MD, FESC VICTOR ABOYANS MD, PhD,
VASCULAR DISEASE MANAGEMENT SURVEY FROM THE ESC COUNCIL FOR CARDIOLOGY PRACTICE AND THE ESC WORKING GROUP ON AORTA AND PERIPHERAL VASCULAR DISEASES RICCARDO ASTEGGIANO MD, FESC VICTOR ABOYANS MD, PhD,
Survey on the Management of Syncope Patients performed by the ESC Council for Cardiology Practice
 Survey on the Management of Syncope Patients performed by the ESC Council for Cardiology Practice A survey on the use of ESC Guidelines on Syncope by Cardiologists Report from: Riccardo Asteggiano, Maxime
Survey on the Management of Syncope Patients performed by the ESC Council for Cardiology Practice A survey on the use of ESC Guidelines on Syncope by Cardiologists Report from: Riccardo Asteggiano, Maxime
Hypertension in Aortic Valve Disease
 Hypertension in Aortic Valve Disease Hanna M. Nosseir MRCP, FRCP Head of Cardiology department Galaa Military Medical Complex Aortic stenosis: Introduction Arterial hypertension and aortic stenosis are
Hypertension in Aortic Valve Disease Hanna M. Nosseir MRCP, FRCP Head of Cardiology department Galaa Military Medical Complex Aortic stenosis: Introduction Arterial hypertension and aortic stenosis are
Centers for Medicare and Medicaid Services. National Coverage of Transcatheter Valve Technologies December 2015
 Centers for Medicare and Medicaid Services National Coverage of Transcatheter Valve Technologies December 2015 National Coverage Determination (NCD) for Transcatheter Aortic Valve Replacement (TAVR) (20.32)
Centers for Medicare and Medicaid Services National Coverage of Transcatheter Valve Technologies December 2015 National Coverage Determination (NCD) for Transcatheter Aortic Valve Replacement (TAVR) (20.32)
Summary Transcatheter aortic valve implantation: Evaluation of the evidence and synthesis of organizational issues
 ETMIS 2012 ; Vol. 8 : N 0 8 Summary Transcatheter aortic valve implantation: Evaluation of the evidence and synthesis of organizational issues May 2012 A production of the Institut national d excellence
ETMIS 2012 ; Vol. 8 : N 0 8 Summary Transcatheter aortic valve implantation: Evaluation of the evidence and synthesis of organizational issues May 2012 A production of the Institut national d excellence
Igor Palacios, MD Director of Interventional Cardiology Massachusetts General Hospital Professor of Medicine Harvard Medical School
 Aortic Stenosis: Current State of Percutaneous Therapies, Emerging Technologies and Future Directions Igor Palacios, MD Director of Interventional Cardiology Massachusetts General Hospital Professor of
Aortic Stenosis: Current State of Percutaneous Therapies, Emerging Technologies and Future Directions Igor Palacios, MD Director of Interventional Cardiology Massachusetts General Hospital Professor of
The more we listen, the more lives we save. Heart Valve V O I C E. Heart Valve Disease. A Practical Guide for Primary Care
 Heart Valve V O I C E The more we listen, the more lives we save. Heart Valve Disease A Practical Guide for Primary Care About Heart Valve Voice Heart Valve Voice is a charity run by a group of multi-disciplinary
Heart Valve V O I C E The more we listen, the more lives we save. Heart Valve Disease A Practical Guide for Primary Care About Heart Valve Voice Heart Valve Voice is a charity run by a group of multi-disciplinary
Valvular Intervention
 Valvular Intervention Outline Introduction Aortic Stenosis Mitral Regurgitation Conclusion Calcific Aortic Stenosis Deformed Eccentric Calcified Nodular Rigid HOSTILE TARGET difficult to displace prone
Valvular Intervention Outline Introduction Aortic Stenosis Mitral Regurgitation Conclusion Calcific Aortic Stenosis Deformed Eccentric Calcified Nodular Rigid HOSTILE TARGET difficult to displace prone
SAMPLE PATIENT SURVEY QUESTIONNAIRE
 This document includes questions you could use- either as a stand alone document or as part of a larger survey- to assess a patient s satisfaction with their contraceptive care experience. --- Patient
This document includes questions you could use- either as a stand alone document or as part of a larger survey- to assess a patient s satisfaction with their contraceptive care experience. --- Patient
Indication, Timing, Assessment and Update on TAVI
 Indication, Timing, Assessment and Update on TAVI Swedish Heart and Vascular Institute Ming Zhang MD PhD Interventional Cardiology Structure Heart Disease Conflict of Interest None Starr- Edwards Mechanical
Indication, Timing, Assessment and Update on TAVI Swedish Heart and Vascular Institute Ming Zhang MD PhD Interventional Cardiology Structure Heart Disease Conflict of Interest None Starr- Edwards Mechanical
Title:Relation Between E/e' ratio and NT-proBNP Levels in Elderly Patients with Symptomatic Severe Aortic Stenosis
 Author's response to reviews Title:Relation Between E/e' ratio and NT-proBNP Levels in Elderly Patients with Symptomatic Severe Aortic Stenosis Authors: Mihai Strachinaru (m.strachinaru@erasmusmc.nl) Bas
Author's response to reviews Title:Relation Between E/e' ratio and NT-proBNP Levels in Elderly Patients with Symptomatic Severe Aortic Stenosis Authors: Mihai Strachinaru (m.strachinaru@erasmusmc.nl) Bas
Optimal care for your patient before and after TAVR
 Optimal care for your patient before and after TAVR Martin Leon MD: Hello. My name is Martin Leon from Columbia University Medical Center and the New York Presbyterian Hospital in New York City. It s my
Optimal care for your patient before and after TAVR Martin Leon MD: Hello. My name is Martin Leon from Columbia University Medical Center and the New York Presbyterian Hospital in New York City. It s my
IPAC date: May of 13
 National Institute for Health and Care Excellence IP685/3 Transcatheter aortic valve implantation (transcatheter aortic valve replacement) for aortic stenosis Consultation Comments table IPAC date: May
National Institute for Health and Care Excellence IP685/3 Transcatheter aortic valve implantation (transcatheter aortic valve replacement) for aortic stenosis Consultation Comments table IPAC date: May
Establishing a New Path Forward for Patients With Severe Symptomatic Aortic Stenosis THE PARTNER TRIAL CLINICAL RESULTS
 Establishing a New Path Forward for Patients With Severe Symptomatic Aortic Stenosis THE PARTNER TRIAL CLINICAL RESULTS E D W A R D S T R A N S C A T H E T E R H E A R T V A L V E P R O G R A M T h e Pa
Establishing a New Path Forward for Patients With Severe Symptomatic Aortic Stenosis THE PARTNER TRIAL CLINICAL RESULTS E D W A R D S T R A N S C A T H E T E R H E A R T V A L V E P R O G R A M T h e Pa
Valve Disease in Patients With Heart Failure TAVI or Surgery? Miguel Sousa Uva Hospital Cruz Vermelha Lisbon, Portugal
 Valve Disease in Patients With Heart Failure TAVI or Surgery? Miguel Sousa Uva Hospital Cruz Vermelha Lisbon, Portugal I have nothing to disclose. Wide Spectrum Stable vs Decompensated NYHA II IV? Ejection
Valve Disease in Patients With Heart Failure TAVI or Surgery? Miguel Sousa Uva Hospital Cruz Vermelha Lisbon, Portugal I have nothing to disclose. Wide Spectrum Stable vs Decompensated NYHA II IV? Ejection
RANDOMISED TRIALS TAVI WITH SAVR STEPHAN WINDECKER AORTIC VALVE DISEASE COMPARING
 AORTIC VALVE DISEASE RANDOMISED TRIALS COMPARING TAVI WITH SAVR STEPHAN WINDECKER DEPARTMENT OF CARDIOLOGY SWISS CARDIOVASCULAR CENTER AND CLINICAL TRIALS UNIT BERN BERN UNIVERSITY HOSPITAL, SWITZERLAND
AORTIC VALVE DISEASE RANDOMISED TRIALS COMPARING TAVI WITH SAVR STEPHAN WINDECKER DEPARTMENT OF CARDIOLOGY SWISS CARDIOVASCULAR CENTER AND CLINICAL TRIALS UNIT BERN BERN UNIVERSITY HOSPITAL, SWITZERLAND
Bicuspid aortic root spared during ascending aorta surgery: an update of long-term results
 Short Communication Bicuspid aortic root spared during ascending aorta surgery: an update of long-term results Marco Russo, Guglielmo Saitto, Paolo Nardi, Fabio Bertoldo, Carlo Bassano, Antonio Scafuri,
Short Communication Bicuspid aortic root spared during ascending aorta surgery: an update of long-term results Marco Russo, Guglielmo Saitto, Paolo Nardi, Fabio Bertoldo, Carlo Bassano, Antonio Scafuri,
TAVR IN INTERMEDIATE-RISK PATIENTS
 TAVR IN INTERMEDIATE-RISK PATIENTS K. Lampropoulos MD, PhD, FESC, MEAPCI Interventional Cardiologist Evangelismos General Hospital The Burden of Valve Disease Prevalence Survival NATURAL HISTORY OF AS
TAVR IN INTERMEDIATE-RISK PATIENTS K. Lampropoulos MD, PhD, FESC, MEAPCI Interventional Cardiologist Evangelismos General Hospital The Burden of Valve Disease Prevalence Survival NATURAL HISTORY OF AS
TAVI- Is Stroke Risk the Achilles Heel of Percutaneous Aortic Valve Repair?
 TAVI- Is Stroke Risk the Achilles Heel of Percutaneous Aortic Valve Repair? Elaine E. Tseng, MD and Marlene Grenon, MD Department of Surgery Divisions of Adult Cardiothoracic and Vascular and Endovascular
TAVI- Is Stroke Risk the Achilles Heel of Percutaneous Aortic Valve Repair? Elaine E. Tseng, MD and Marlene Grenon, MD Department of Surgery Divisions of Adult Cardiothoracic and Vascular and Endovascular
Assessment and Preparation of Patients with TAVI. Rob Tanzola Associate Professor, Queen s University
 Assessment and Preparation of Patients with TAVI Rob Tanzola Associate Professor, Queen s University My patient has aortic stenosis and needs non-cardiac surgery Should (s)he get a TAVI? Rob Tanzola Associate
Assessment and Preparation of Patients with TAVI Rob Tanzola Associate Professor, Queen s University My patient has aortic stenosis and needs non-cardiac surgery Should (s)he get a TAVI? Rob Tanzola Associate
The Impact of TAVI Nurse Coordinator on patient management of Transcatheter Aortic Valve Implantation (TAVI) program in QEH
 program in QEH") HA Convention 18-19 May 2015 The Impact of TAVI Nurse Coordinator on patient management of Transcatheter Aortic Valve Implantation (TAVI) program in QEH Division of Cardiology Department of Medicine Queen
HA Convention 18-19 May 2015 The Impact of TAVI Nurse Coordinator on patient management of Transcatheter Aortic Valve Implantation (TAVI) program in QEH Division of Cardiology Department of Medicine Queen
TAVI After PARTNER-2 : The Hamilton Approach
 TAVI After PARTNER-2 : The Hamilton Approach James L. Velianou MD FRCPC Interventional Cardiology Hamilton General Hospital St Catharines General Hospital Associate Professor of Medicine McMaster University
TAVI After PARTNER-2 : The Hamilton Approach James L. Velianou MD FRCPC Interventional Cardiology Hamilton General Hospital St Catharines General Hospital Associate Professor of Medicine McMaster University
Policy Specific Section: March 30, 2012 March 7, 2013
 Medical Policy Transcatheter Aortic Valve Replacement for Aortic Stenosis Type: Medical Necessity and Investigational / Experimental Policy Specific Section: Surgery Original Policy Date: Effective Date:
Medical Policy Transcatheter Aortic Valve Replacement for Aortic Stenosis Type: Medical Necessity and Investigational / Experimental Policy Specific Section: Surgery Original Policy Date: Effective Date:
TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central
 TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University 1 Disclosure Chiesi Pharma- Consultant
TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University 1 Disclosure Chiesi Pharma- Consultant
Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know
 Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know James F. Burke, MD Program Director Cardiovascular Disease Fellowship Lankenau Medical Center Disclosure Dr. Burke has no conflicts
Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know James F. Burke, MD Program Director Cardiovascular Disease Fellowship Lankenau Medical Center Disclosure Dr. Burke has no conflicts
Percutaneous Management of Severe AS in Octagenarians. Phillip Matsis FRACP FCSANZ Interventional Cardiologist Wakefield Heart Centre Wellington
 Percutaneous Management of Severe AS in Octagenarians Phillip Matsis FRACP FCSANZ Interventional Cardiologist Wakefield Heart Centre Wellington May 2017 Outline Aetiology of AS Natural History of AS Assessment
Percutaneous Management of Severe AS in Octagenarians Phillip Matsis FRACP FCSANZ Interventional Cardiologist Wakefield Heart Centre Wellington May 2017 Outline Aetiology of AS Natural History of AS Assessment
Transcatheter Aortic Valve Implantation (TAVI) Overview for Wales. Dr Richard Anderson University Hospital of Wales, Cardiff, UK
 Overview for Wales. Dr Richard Anderson University Hospital of Wales, Cardiff, UK") Transcatheter Aortic Valve Implantation (TAVI) Overview for Wales Dr Richard Anderson University Hospital of Wales, Cardiff, UK Aortic stenosis is a disease of old age Age demographics in Wales % Wales
Transcatheter Aortic Valve Implantation (TAVI) Overview for Wales Dr Richard Anderson University Hospital of Wales, Cardiff, UK Aortic stenosis is a disease of old age Age demographics in Wales % Wales
1-YEAR OUTCOMES FROM JOHN WEBB, MD
 1-YEAR OUTCOMES FROM JOHN WEBB, MD ON BEHALF OF THE SAPIEN 3 INVESTIGATORS UNIVERSITY OF BRITISH COLUMBIA VANCOUVER, CANADA Potential conflicts of interest Speaker's name: John Webb I have the following
1-YEAR OUTCOMES FROM JOHN WEBB, MD ON BEHALF OF THE SAPIEN 3 INVESTIGATORS UNIVERSITY OF BRITISH COLUMBIA VANCOUVER, CANADA Potential conflicts of interest Speaker's name: John Webb I have the following
A new option for the Diagnosis and Management of Valvular Heart Disease. Oregon Comprehensive Valve Center
 A new option for the Diagnosis and Management of Valvular Heart Disease Oregon Comprehensive Valve Center I have no disclosures Oregon Comprehensive Valve Center Weekly multidisciplinary case conferences
A new option for the Diagnosis and Management of Valvular Heart Disease Oregon Comprehensive Valve Center I have no disclosures Oregon Comprehensive Valve Center Weekly multidisciplinary case conferences
Improving Quality of Care for Patients with Heart Valve Disease
 Improving Quality of Care for Patients with Heart Valve Disease The Heart Team The Heart Valve Clinic Raphael Rosenhek Department of Cardiology Medical University of Vienna Eurovalve 2016 Brussels, March
Improving Quality of Care for Patients with Heart Valve Disease The Heart Team The Heart Valve Clinic Raphael Rosenhek Department of Cardiology Medical University of Vienna Eurovalve 2016 Brussels, March
Extension to medium and low risk patients? Friedrich Eckstein University Hospital Basel
 TAVI CON Extension to medium and low risk patients? Friedrich Eckstein University Hospital Basel Extension to medium and low risk patients? In octogenerians already reality in most of the swiss clinics!?
TAVI CON Extension to medium and low risk patients? Friedrich Eckstein University Hospital Basel Extension to medium and low risk patients? In octogenerians already reality in most of the swiss clinics!?
TAVR 2018: TAVR has high clinical efficacy according to baseline patient risk! ii. Con
 TAVR 2018: TAVR has high clinical efficacy according to baseline patient risk! ii. Con Dimitrios C. Angouras, MD, FETCS Associate Professor of Cardiac Surgery National and Kapodistrian University of Athens,
TAVR 2018: TAVR has high clinical efficacy according to baseline patient risk! ii. Con Dimitrios C. Angouras, MD, FETCS Associate Professor of Cardiac Surgery National and Kapodistrian University of Athens,
Incorporating the intermediate risk in Transcatheter Aortic Valve Implantation (TAVI)
") Incorporating the intermediate risk in Transcatheter Aortic Valve Implantation (TAVI) Larry S. Dean, MD, MSCAI Past President SCAI Professor of Medicine and Surgery University of Washington School of Medicine
Incorporating the intermediate risk in Transcatheter Aortic Valve Implantation (TAVI) Larry S. Dean, MD, MSCAI Past President SCAI Professor of Medicine and Surgery University of Washington School of Medicine
A More Definitive Ablation Procedure for Atrial Fibrillation
 Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/heart-matters/a-more-definitive-ablation-procedure-for-atrialfibrillation/3982/
Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/heart-matters/a-more-definitive-ablation-procedure-for-atrialfibrillation/3982/
Are Heart Valve Referral Centers Feasible in Latin America?
 Are Heart Valve Referral Centers Feasible in Latin America? Vadim Kotowicz, MD Chief of Cardiovascular Surgery Department Italian Hospital of Buenos Aires Disclosure Medtronic inc. Consultanting Johnson
Are Heart Valve Referral Centers Feasible in Latin America? Vadim Kotowicz, MD Chief of Cardiovascular Surgery Department Italian Hospital of Buenos Aires Disclosure Medtronic inc. Consultanting Johnson
TAVR in 2017 What we know? What to expect?
 Journal of Geriatric Cardiology (2018) 15: 55 60 2018 JGC All rights reserved; www.jgc301.com Perspective Open Access TAVR in 2017 What we know? What to expect? Panagiota Kourkoveli 1,*, Konstantinos Spargias
Journal of Geriatric Cardiology (2018) 15: 55 60 2018 JGC All rights reserved; www.jgc301.com Perspective Open Access TAVR in 2017 What we know? What to expect? Panagiota Kourkoveli 1,*, Konstantinos Spargias
HIV Pre- Exposure Prophylaxis
 HIV Pre- Exposure Prophylaxis KNOWLEDGE AND ATTITUDES IN NORTH QUEENSLAND GENERAL PRACTITIONERS Principle Investigator: William Lane Co-Supervisor 1: Professor Clare Heal Co-Supervisor 2: Dr Jennifer Banks
HIV Pre- Exposure Prophylaxis KNOWLEDGE AND ATTITUDES IN NORTH QUEENSLAND GENERAL PRACTITIONERS Principle Investigator: William Lane Co-Supervisor 1: Professor Clare Heal Co-Supervisor 2: Dr Jennifer Banks
ORGAN DONATION AND TRANSPLANTS between an ideal situation and a coherent programme
 http://www.viata-medicala.ro/*articleid_2653-dart.html ORGAN DONATION AND TRANSPLANTS between an ideal situation and a coherent programme Author: Dr. Aurel F. Marin, 7 January 2011 According to data provided
http://www.viata-medicala.ro/*articleid_2653-dart.html ORGAN DONATION AND TRANSPLANTS between an ideal situation and a coherent programme Author: Dr. Aurel F. Marin, 7 January 2011 According to data provided
Incidence And Predictors Of Left Bundle Branch Block After Transcatheter Aortic Valve Implantation
 Incidence And Predictors Of Left Bundle Branch Block After Transcatheter Aortic Valve Implantation Ömer Aktug 1, MD; Guido Dohmen 2, MD; Kathrin Brehmer 1, MD; Verena Deserno 1 ; Ralf Herpertz 1 ; Rüdiger
Incidence And Predictors Of Left Bundle Branch Block After Transcatheter Aortic Valve Implantation Ömer Aktug 1, MD; Guido Dohmen 2, MD; Kathrin Brehmer 1, MD; Verena Deserno 1 ; Ralf Herpertz 1 ; Rüdiger
DHS COMPARATIVE STUDIES
 DHS COMPARATIVE STUDIES DHS DEMOGRAPHIC AND HEALTH SURVEYS The Demographic and Health Surveys (DHS) is a 13-year project to assist government and private agencies in developing countries to conduct nationa!
DHS COMPARATIVE STUDIES DHS DEMOGRAPHIC AND HEALTH SURVEYS The Demographic and Health Surveys (DHS) is a 13-year project to assist government and private agencies in developing countries to conduct nationa!
Aortic Stenosis in the Elderly: Difficulties for the Clinician. Are Symptoms Due to Aortic Stenosis?
 Aortic Stenosis in the Elderly: Difficulties for the Clinician Are Symptoms Due to Aortic Stenosis? Raphael Rosenhek Department of Cardiology Medical University of Vienna No disclosure European Society
Aortic Stenosis in the Elderly: Difficulties for the Clinician Are Symptoms Due to Aortic Stenosis? Raphael Rosenhek Department of Cardiology Medical University of Vienna No disclosure European Society
Sotirios N. Prapas, M.D., Ph.D, F.E.C.T.S.
 CORONARY ARTERY REVASCULARIZATION WITH MILD AORTIC STENOSIS: STRATEGIES OF TREATMENT 9 th ANNUAL MEETING OF THE EAB SOCIETY, Pravets, Bulgaria, 2012 Sotirios N. Prapas, M.D., Ph.D, F.E.C.T.S. Director
CORONARY ARTERY REVASCULARIZATION WITH MILD AORTIC STENOSIS: STRATEGIES OF TREATMENT 9 th ANNUAL MEETING OF THE EAB SOCIETY, Pravets, Bulgaria, 2012 Sotirios N. Prapas, M.D., Ph.D, F.E.C.T.S. Director
TAVR in Intermediate Risk Populations /Optimizing Systems for TAVR
 TAVR in Intermediate Risk Populations /Optimizing Systems for TAVR Saibal Kar, MD, FACC, FAHA, FSCAI Professor of Medicine Director of Interventional Cardiac Research Smidt Heart Institute, Cedars-Sinai
TAVR in Intermediate Risk Populations /Optimizing Systems for TAVR Saibal Kar, MD, FACC, FAHA, FSCAI Professor of Medicine Director of Interventional Cardiac Research Smidt Heart Institute, Cedars-Sinai
Lewis & Clark National Estimation and Awareness Study
 Lewis & Clark National Estimation and Awareness Study Prepared by for the Institute for Tourism and Recreation Research and Montana's Tourism Advisory Council Institute for Tourism and Recreation Research
Lewis & Clark National Estimation and Awareness Study Prepared by for the Institute for Tourism and Recreation Research and Montana's Tourism Advisory Council Institute for Tourism and Recreation Research
Annotated bibliographies:
 Annotated bibliographies: California Immunization Handbook: School and Child Care Immunization Requirements for Schools and Child Care Programs. Seventh Edition. July 2003. Web. 10 Oct. 2010. This handbook
Annotated bibliographies: California Immunization Handbook: School and Child Care Immunization Requirements for Schools and Child Care Programs. Seventh Edition. July 2003. Web. 10 Oct. 2010. This handbook
Heart Valve disease: MR. AS tough patient When to echo, When to refer, What s new
 Heart Valve disease: MR. AS tough patient When to echo, When to refer, What s new B. Sonnenberg UAH Cardiology CME Day 5 May 2015 Disclosures Speaker s or Advisory Boards: none Research grants: none (co-investigator
Heart Valve disease: MR. AS tough patient When to echo, When to refer, What s new B. Sonnenberg UAH Cardiology CME Day 5 May 2015 Disclosures Speaker s or Advisory Boards: none Research grants: none (co-investigator
Transcatheter Mitral Valve Repair: today and tomorrow Sponsored by Abbott. Chairperson: M. Haude Panellists: A. Al Nooryani, M.
 Transcatheter Mitral Valve Repair: today and tomorrow Sponsored by Abbott Chairperson: M. Haude Panellists: A. Al Nooryani, M. Al Otaiby Session objectives To learn about the clinical patient profile for
Transcatheter Mitral Valve Repair: today and tomorrow Sponsored by Abbott Chairperson: M. Haude Panellists: A. Al Nooryani, M. Al Otaiby Session objectives To learn about the clinical patient profile for
In Process, Unpublished STS/ACC TVT Registry Manuscripts
 In Process, Unpublished STS/ACC TVT Registry Manuscripts The following pages list current research and publications proposals that have been recently approved, are under analysis, are under manuscript
In Process, Unpublished STS/ACC TVT Registry Manuscripts The following pages list current research and publications proposals that have been recently approved, are under analysis, are under manuscript
Welcome Number 6. The background of the Cardiac Sonographer Network News masthead is a diagnostic image:
 Number 6 Welcome Number 6 Welcome to the newsletter created just for you: sonographers who perform pediatric echocardiograms in primarily adult echo labs. Each issue features tips on echocardiography of
Number 6 Welcome Number 6 Welcome to the newsletter created just for you: sonographers who perform pediatric echocardiograms in primarily adult echo labs. Each issue features tips on echocardiography of
Low Gradient Severe AS: Who Qualifies for TAVR? Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor
 Low Gradient Severe AS: Who Qualifies for TAVR? Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University
Low Gradient Severe AS: Who Qualifies for TAVR? Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University
Understanding the guidelines for Interventions in MR. Ali AlMasood
 Understanding the guidelines for Interventions in MR Ali AlMasood Mitral regurgitation The most diverse from all acquired valve diseases About 50% of patients with an LVEF 35 percent had moderate to severe
Understanding the guidelines for Interventions in MR Ali AlMasood Mitral regurgitation The most diverse from all acquired valve diseases About 50% of patients with an LVEF 35 percent had moderate to severe
Screening for CETPH after acute pulmonary embolism: is it needed? Menno V. Huisman Department of Vascular Medicine LUMC Leiden
 Screening for CETPH after acute pulmonary embolism: is it needed? Menno V. Huisman Department of Vascular Medicine LUMC Leiden m.v.huisman@lumc.nl Background CETPH Chronic Thrombo Embolic Pulmonary Hypertension
Screening for CETPH after acute pulmonary embolism: is it needed? Menno V. Huisman Department of Vascular Medicine LUMC Leiden m.v.huisman@lumc.nl Background CETPH Chronic Thrombo Embolic Pulmonary Hypertension
Percutaneous Mitral Valve Repair: What Can We Treat and What Should We Treat
 Percutaneous Mitral Valve Repair: What Can We Treat and What Should We Treat Innovative Procedures, Devices & State of the Art Care for Arrhythmias, Heart Failure & Structural Heart Disease October 8-10,
Percutaneous Mitral Valve Repair: What Can We Treat and What Should We Treat Innovative Procedures, Devices & State of the Art Care for Arrhythmias, Heart Failure & Structural Heart Disease October 8-10,
RISK PREDICTION IN TAVR. Beyond STS PROM and the Eyeball Assessment
 RISK PREDICTION IN TAVR Beyond STS PROM and the Eyeball Assessment SAVR VS TAVR BIOPROSHETIC OPEN SURGICAL VALVE (SAVR) BIOPROSTHETIC TRANSCATHETER VALVE (TAVR) This Photo by Unknown Author is licensed
RISK PREDICTION IN TAVR Beyond STS PROM and the Eyeball Assessment SAVR VS TAVR BIOPROSHETIC OPEN SURGICAL VALVE (SAVR) BIOPROSTHETIC TRANSCATHETER VALVE (TAVR) This Photo by Unknown Author is licensed
CARDIAC REHABILITATION AFTER TRANSCATHETER AORTIC VALVE IMPLANTATION: A SINGLE CENTRE EXPERIENCE
 ESC Congress 2011 27 Aug - 31 Aug 2011, Paris - France CARDIAC REHABILITATION AFTER TRANSCATHETER AORTIC VALVE IMPLANTATION: A SINGLE CENTRE EXPERIENCE N.Russo, L.Compostella, T.Setzu, M.Napodano, L.Testolin,
ESC Congress 2011 27 Aug - 31 Aug 2011, Paris - France CARDIAC REHABILITATION AFTER TRANSCATHETER AORTIC VALVE IMPLANTATION: A SINGLE CENTRE EXPERIENCE N.Russo, L.Compostella, T.Setzu, M.Napodano, L.Testolin,
TAVR in patients with. End-Stage CKD or in Renal Replacement Therapy:
 TAVR in patients with End-Stage CKD or in Renal Replacement Therapy: Special Considerations and Prevention of early Valve Failure Antonios Chalapas, MD, PhD, FESC THV & Hygeia Hospital Heart Team Athens,
TAVR in patients with End-Stage CKD or in Renal Replacement Therapy: Special Considerations and Prevention of early Valve Failure Antonios Chalapas, MD, PhD, FESC THV & Hygeia Hospital Heart Team Athens,
Define Objectives. Define Solution. Design Evaluation. Use Findings. Report Findings. Implement Program. Program. Conduct Evaluation
 Quality Assurance, Customer Satisfaction and Follow-Up: Definition and Practical Experience Micki Thompson 2-1-11 Tampa Bay Cares, Inc James B. Luther, Ph.D. Luther Consulting, LLC May, 2009 Overview Brief
Quality Assurance, Customer Satisfaction and Follow-Up: Definition and Practical Experience Micki Thompson 2-1-11 Tampa Bay Cares, Inc James B. Luther, Ph.D. Luther Consulting, LLC May, 2009 Overview Brief
CIPG Transcatheter Aortic Valve Replacement- When Is Less, More?
 CIPG 2013 Transcatheter Aortic Valve Replacement- When Is Less, More? James D. Rossen, M.D. Professor of Medicine and Neurosurgery Director, Cardiac Catheterization Laboratory and Interventional Cardiology
CIPG 2013 Transcatheter Aortic Valve Replacement- When Is Less, More? James D. Rossen, M.D. Professor of Medicine and Neurosurgery Director, Cardiac Catheterization Laboratory and Interventional Cardiology
Transcatheter Aortic-Valve Implantation for Aortic Stenosis
 Transcatheter Aortic-Valve Implantation for Aortic Stenosis Policy Number: 7.01.132 Last Review: 6/2018 Origination: 2/2012 Next Review: 2/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC)
Transcatheter Aortic-Valve Implantation for Aortic Stenosis Policy Number: 7.01.132 Last Review: 6/2018 Origination: 2/2012 Next Review: 2/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC)
Is it a business for the cardiac surgeon?
 TAVI FOR LOW RISK PATIENTS Is it a business for the cardiac surgeon? Augusto D Onofrio Gino Gerosa Department of Cardiac, Thoracic and Vascular Sciences, University of Padua, Italy T A V I Cardiac surgery
TAVI FOR LOW RISK PATIENTS Is it a business for the cardiac surgeon? Augusto D Onofrio Gino Gerosa Department of Cardiac, Thoracic and Vascular Sciences, University of Padua, Italy T A V I Cardiac surgery
GLORIA -AF REGISTRY PROGRAMME
 GLORIA -AF REGISTRY PROGRAMME EXECUTIVE SUMMARY The approval of novel oral anticoagulants has changed prescribing patterns for stroke prevention in atrial fibrillation (AF) worldwide. 1 There is a need
GLORIA -AF REGISTRY PROGRAMME EXECUTIVE SUMMARY The approval of novel oral anticoagulants has changed prescribing patterns for stroke prevention in atrial fibrillation (AF) worldwide. 1 There is a need
THE PERCUTANEOUS MANAGEMENT OF VALVULAR HEART DISEASE DR JOHN RAWLINS CONSULTANT INTERVENTIONAL CARDIOLOGIST UNIVERSITY HOSPITAL SOUTHAMPTON
 THE PERCUTANEOUS MANAGEMENT OF VALVULAR HEART DISEASE DR JOHN RAWLINS CONSULTANT INTERVENTIONAL CARDIOLOGIST UNIVERSITY HOSPITAL SOUTHAMPTON INTRODUCTION History of heart valve intervention Current indications
THE PERCUTANEOUS MANAGEMENT OF VALVULAR HEART DISEASE DR JOHN RAWLINS CONSULTANT INTERVENTIONAL CARDIOLOGIST UNIVERSITY HOSPITAL SOUTHAMPTON INTRODUCTION History of heart valve intervention Current indications
4 th IAS Conference on HIV Pathogenesis, Treatment and Prevention. 1. IAS 2007 Evaluation: Delegate Survey
 4 th IAS Conference on HIV Pathogenesis, Treatment and Prevention Appendices 1. IAS 2007 Evaluation: Delegate Survey 2. Report of the longer-term impact of the 3 rd IAS Conference on HIV Pathogenesis,
4 th IAS Conference on HIV Pathogenesis, Treatment and Prevention Appendices 1. IAS 2007 Evaluation: Delegate Survey 2. Report of the longer-term impact of the 3 rd IAS Conference on HIV Pathogenesis,
Slide 1: Perioperative Management of Anticoagulation
 Perioperative Management of Anticoagulation by Steven L. Cohn, MD, FACP Director, Medical Consultation Service, Kings County Hospital Center, Clinical Professor of Medicine, SUNY Downstate, Brooklyn, NY
Perioperative Management of Anticoagulation by Steven L. Cohn, MD, FACP Director, Medical Consultation Service, Kings County Hospital Center, Clinical Professor of Medicine, SUNY Downstate, Brooklyn, NY
Transcatheter Therapies For Aortic Valve Disease. March 2017 Brian Whisenant MD
 Transcatheter Therapies For Aortic Valve Disease March 2017 Brian Whisenant MD Introduction I got into this field to protect my turf. I must say, I have come full circle... - Kent W. Jones I got into this
Transcatheter Therapies For Aortic Valve Disease March 2017 Brian Whisenant MD Introduction I got into this field to protect my turf. I must say, I have come full circle... - Kent W. Jones I got into this
Five-Year Outcomes of Transcatheter Aortic Valve Replacement (TAVR) in Inoperable Patients With Severe Aortic Stenosis: The PARTNER Trial
 in Inoperable Patients With Severe Aortic Stenosis: The PARTNER Trial") Five-Year Outcomes of Transcatheter Aortic Valve Replacement (TAVR) in Inoperable Patients With Severe Aortic Stenosis: The PARTNER Trial Samir R. Kapadia, MD On behalf of The PARTNER Trial Investigators
Five-Year Outcomes of Transcatheter Aortic Valve Replacement (TAVR) in Inoperable Patients With Severe Aortic Stenosis: The PARTNER Trial Samir R. Kapadia, MD On behalf of The PARTNER Trial Investigators
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Transcatheter Aortic Valve Implantation for Aortic Stenosis Page 1 of 37 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Transcatheter Aortic Valve Implantation
Transcatheter Aortic Valve Implantation for Aortic Stenosis Page 1 of 37 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Transcatheter Aortic Valve Implantation
TAVR and Cardiac Surgeons
 TAVR and Cardiac Surgeons TAVR and Cardiac Surgeons Ragheb Hasan Consultant and Clinical Lead Cardiothoracic Surgeon Manchester Royal Infirmary, Oxford Road, Manchester UK Aortic Stenosis Is A Growing
TAVR and Cardiac Surgeons TAVR and Cardiac Surgeons Ragheb Hasan Consultant and Clinical Lead Cardiothoracic Surgeon Manchester Royal Infirmary, Oxford Road, Manchester UK Aortic Stenosis Is A Growing
Manuscript ID BMJ entitled "Benzodiazepines and the Risk of Allcause Mortality in Adults: A Cohort Study"
 12-Jan-2017 Dear Dr. Patorno Manuscript ID BMJ.2016.036319 entitled "Benzodiazepines and the Risk of Allcause Mortality in Adults: A Cohort Study" Thank you for sending us your paper. We sent it for external
12-Jan-2017 Dear Dr. Patorno Manuscript ID BMJ.2016.036319 entitled "Benzodiazepines and the Risk of Allcause Mortality in Adults: A Cohort Study" Thank you for sending us your paper. We sent it for external
Interventional procedures guidance Published: 26 September 2014 nice.org.uk/guidance/ipg504
 Transcatheter valve-in-valve e implantation for aortic bioprosthetic valve dysfunction Interventional procedures guidance Published: 26 September 2014 nice.org.uk/guidance/ipg504 Your responsibility This
Transcatheter valve-in-valve e implantation for aortic bioprosthetic valve dysfunction Interventional procedures guidance Published: 26 September 2014 nice.org.uk/guidance/ipg504 Your responsibility This
NATIONAL SURVEY OF ALL REGISTERED PSYCHOLOGY PRACTITIONERS
 Research report February 2017 NATIONAL SURVEY OF ALL REGISTERED PSYCHOLOGY PRACTITIONERS Prepared by: Quantify Research (Pty) Ltd https://www.quantifyresearch.co.za TABLE OF CONTENTS Survey Results (cont.):
Research report February 2017 NATIONAL SURVEY OF ALL REGISTERED PSYCHOLOGY PRACTITIONERS Prepared by: Quantify Research (Pty) Ltd https://www.quantifyresearch.co.za TABLE OF CONTENTS Survey Results (cont.):
Bleeding Management Strategies. Aiming for the best Outcomes August 27, Amit Gupta, MD FACC FSCAI Interventional Cardiologist CANM
 Bleeding Management Strategies Aiming for the best Outcomes August 27, 2016 Amit Gupta, MD FACC FSCAI Interventional Cardiologist CANM Learning Objectives Review the use of anti-coagulants in patients
Bleeding Management Strategies Aiming for the best Outcomes August 27, 2016 Amit Gupta, MD FACC FSCAI Interventional Cardiologist CANM Learning Objectives Review the use of anti-coagulants in patients
bpac better e m dicine
 INR Testing Quiz Feedback bpac nz better medicin e Contents INR Testing Quiz 2 Quiz Feedback: Responses from Colleagues, and Expert Review 4 bpac nz Review : Dr Janine Bailey, Motueka Dr Stephen Kuzmich,
INR Testing Quiz Feedback bpac nz better medicin e Contents INR Testing Quiz 2 Quiz Feedback: Responses from Colleagues, and Expert Review 4 bpac nz Review : Dr Janine Bailey, Motueka Dr Stephen Kuzmich,
Measuring the risk in valve patients Lessons learnt from the TAVI story? Bernard Iung Bichat Hospital, Paris, France
 Measuring the risk in valve patients Lessons learnt from the TAVI story? Bernard Iung Bichat Hospital, Paris, France Faculty disclosure Bernard Iung I disclose the following financial relationships: Consultant
Measuring the risk in valve patients Lessons learnt from the TAVI story? Bernard Iung Bichat Hospital, Paris, France Faculty disclosure Bernard Iung I disclose the following financial relationships: Consultant
BWGIC Activity report 2014
 BWGIC Activity report 2014 Quality control in percutaneous coronary intervention (PCI) and trans-catheter aortic valve implantation (TAVI) The project was to contribute to control and to improve the quality
BWGIC Activity report 2014 Quality control in percutaneous coronary intervention (PCI) and trans-catheter aortic valve implantation (TAVI) The project was to contribute to control and to improve the quality
Debate: SAVR for Low-Risk Patients in 2017 is Obsolete AVR vs TAVI
 Debate: SAVR for Low-Risk Patients in 2017 is Obsolete AVR vs TAVI Joseph E. Bavaria, MD Roberts-Measey Professor of Surgery Vice Chair, Division of Cardiovascular Surgery University of Pennsylvania Immediate
Debate: SAVR for Low-Risk Patients in 2017 is Obsolete AVR vs TAVI Joseph E. Bavaria, MD Roberts-Measey Professor of Surgery Vice Chair, Division of Cardiovascular Surgery University of Pennsylvania Immediate
Summary of the Dental Results from the GP Patient Survey; July to September 2014
 Introduction Summary of the Dental Results from the GP Patient Survey; July to September 2014 1. Dental questions were originally added to the GP Patient Survey in January to March 2010, as the Department
Introduction Summary of the Dental Results from the GP Patient Survey; July to September 2014 1. Dental questions were originally added to the GP Patient Survey in January to March 2010, as the Department
Transcatheter Aortic Valve Implantation (TAVI)
") Transcatheter Aortic Valve Implantation (TAVI) QEH Registry A Multidisciplinary Team Approach Michael KY Lee 1, LK Chan 1, KC Chan 1, KT Chan 1, SF Chui 1, HS Ma 1, CY Wong 1, CS Chiang 1, P Li 1, CB Lam
Transcatheter Aortic Valve Implantation (TAVI) QEH Registry A Multidisciplinary Team Approach Michael KY Lee 1, LK Chan 1, KC Chan 1, KT Chan 1, SF Chui 1, HS Ma 1, CY Wong 1, CS Chiang 1, P Li 1, CB Lam
Statistical Essentials in Interpreting Clinical Trials Stuart J. Pocock, PhD
 Statistical Essentials in Interpreting Clinical Trials Stuart J. Pocock, PhD June 03, 2016 www.medscape.com I'm Stuart Pocock, professor of medical statistics at London University. I am going to take you
Statistical Essentials in Interpreting Clinical Trials Stuart J. Pocock, PhD June 03, 2016 www.medscape.com I'm Stuart Pocock, professor of medical statistics at London University. I am going to take you
A survey of the UK maxillofacial laboratory service: Profiles of staff and work
 British Journal of Oral and Maxillofacial Surgery 44 (2006) 406 410 A survey of the UK maxillofacial laboratory service: Profiles of staff and work J. Watson a, G. Cannavina a,, C.W. Stokes a,g.kent b
British Journal of Oral and Maxillofacial Surgery 44 (2006) 406 410 A survey of the UK maxillofacial laboratory service: Profiles of staff and work J. Watson a, G. Cannavina a,, C.W. Stokes a,g.kent b
Itamar Medical. December Investors Presentation.
 Itamar Medical December 2017. Investors Presentation. Disclaimer Itamar Medical Ltd. (the "Company") is furnishing this presentation and any information given during this presentation, solely for the consideration
Itamar Medical December 2017. Investors Presentation. Disclaimer Itamar Medical Ltd. (the "Company") is furnishing this presentation and any information given during this presentation, solely for the consideration
Appropriate Patient Selection or Healthcare Rationing? Lessons from Surgical Aortic Valve Replacement in The PARTNER I Trial Wilson Y.
 Appropriate Patient Selection or Healthcare Rationing? Lessons from Surgical Aortic Valve Replacement in The PARTNER I Trial Wilson Y. Szeto, MD on behalf of The PARTNER Trial Investigators and The PARTNER
Appropriate Patient Selection or Healthcare Rationing? Lessons from Surgical Aortic Valve Replacement in The PARTNER I Trial Wilson Y. Szeto, MD on behalf of The PARTNER Trial Investigators and The PARTNER
A new era in cardiac valve surgery has begun...
 THE CENTER FOR VALVE SURGERY A new era in cardiac valve surgery has begun... Good Help to Those in Need Rawn Salenger, MD, FACS, Director, The Center for Valve Surgery Edward F. Lundy, MD, PhD, Chief of
THE CENTER FOR VALVE SURGERY A new era in cardiac valve surgery has begun... Good Help to Those in Need Rawn Salenger, MD, FACS, Director, The Center for Valve Surgery Edward F. Lundy, MD, PhD, Chief of
Aortic Stenosis: Interventional Choice for a 70-year old- SAVR, TAVR or BAV? Interventional Choice for a 90-year old- SAVR, TAVR or BAV?
 Aortic Stenosis: Interventional Choice for a 70-year old- SAVR, TAVR or BAV? Interventional Choice for a 90-year old- SAVR, TAVR or BAV? Samin K Sharma, MD, FACC, FSCAI Director Clinical & Interventional
Aortic Stenosis: Interventional Choice for a 70-year old- SAVR, TAVR or BAV? Interventional Choice for a 90-year old- SAVR, TAVR or BAV? Samin K Sharma, MD, FACC, FSCAI Director Clinical & Interventional
Spotlight on valvular heart disease guidelines. Prosthetic heart valves. Bernard Iung Bichat Hospital, Paris Diderot University Paris, France
 Spotlight on valvular heart disease guidelines. Prosthetic heart valves. Bernard Iung Bichat Hospital, Paris Diderot University Paris, France Faculty disclosure First name - last name I disclose the following
Spotlight on valvular heart disease guidelines. Prosthetic heart valves. Bernard Iung Bichat Hospital, Paris Diderot University Paris, France Faculty disclosure First name - last name I disclose the following
Clinical Commissioning Policy: Transcatheter Aortic Valve Implantation (TAVI) For Aortic Stenosis. December Reference : NHSCB/A10/a/1
 For Aortic Stenosis. December Reference : NHSCB/A10/a/1") Clinical Commissioning Policy: Transcatheter Aortic Valve Implantation (TAVI) For Aortic Stenosis December 2012 Reference : NHSCB/A10/a/1 NHS Commissioning Board Clinical Commissioning Policy: Transcatheter
Clinical Commissioning Policy: Transcatheter Aortic Valve Implantation (TAVI) For Aortic Stenosis December 2012 Reference : NHSCB/A10/a/1 NHS Commissioning Board Clinical Commissioning Policy: Transcatheter
21/06/2018. MEASURING PERFORMANCE (AUDIT AND QUALITY IMPROVEMENT) Towards Reducing Inequity. What should we be measuring?
 Towards Reducing Inequity. What should we be measuring?") MEASURING PERFORMANCE (AUDIT AND QUALITY IMPROVEMENT) Towards Reducing Inequity Dr Raewyn Fisher Cardiologist Director of Waikato Integrated Heart Failure Service What should we be measuring? At risk,
MEASURING PERFORMANCE (AUDIT AND QUALITY IMPROVEMENT) Towards Reducing Inequity Dr Raewyn Fisher Cardiologist Director of Waikato Integrated Heart Failure Service What should we be measuring? At risk,
TAVR (Transcatheter Aortic Valve Replacement).
.") HEART & VASCULAR Your guide to TAVR (Transcatheter Aortic Valve Replacement). An alternative to open heart valve replacement surgery. For many years, the only way to treat a heart valve condition was through
HEART & VASCULAR Your guide to TAVR (Transcatheter Aortic Valve Replacement). An alternative to open heart valve replacement surgery. For many years, the only way to treat a heart valve condition was through
6: Service considerations a report from the Adult Dental Health Survey 2009
 UK Data Archive Study Number - Adult Dental Health Survey, 009 6: Service considerations a report from the Adult Dental Health Survey 009 Copyright 0, The Health and Social Care Information Centre. All
UK Data Archive Study Number - Adult Dental Health Survey, 009 6: Service considerations a report from the Adult Dental Health Survey 009 Copyright 0, The Health and Social Care Information Centre. All
National Survey of Young Adults on HIV/AIDS
 REPORT National Survey of Young Adults on HIV/AIDS November 2017 Kaiser Family Foundation Introduction More than three and a half decades have passed since the first case of AIDS. An entire generation
REPORT National Survey of Young Adults on HIV/AIDS November 2017 Kaiser Family Foundation Introduction More than three and a half decades have passed since the first case of AIDS. An entire generation
Transcatheter Aortic-Valve Implantation for Aortic Stenosis
 Transcatheter Aortic-Valve Implantation for Aortic Stenosis Policy Number: 7.01.132 Last Review: 2/2019 Origination: 2/2012 Next Review: 2/2020 Policy Blue Cross and Blue Shield of Kansas City (Blue KC)
Transcatheter Aortic-Valve Implantation for Aortic Stenosis Policy Number: 7.01.132 Last Review: 2/2019 Origination: 2/2012 Next Review: 2/2020 Policy Blue Cross and Blue Shield of Kansas City (Blue KC)
Alzheimers New Zealand
 Alzheimers New Zealand Awareness and Understanding of Dementia in New Zealand Report Contents Introduction... 3 Summary of Main Findings... 5 Executive summary... 8 Section One: Understanding of Alzheimer
Alzheimers New Zealand Awareness and Understanding of Dementia in New Zealand Report Contents Introduction... 3 Summary of Main Findings... 5 Executive summary... 8 Section One: Understanding of Alzheimer
ARRHYTHMIAS AND DEVICE THERAPY
 Topic List A BASICS 1 History of Cardiology 2 Clinical Skills 2.1 History Taking 2.2 Physical Examination 2.3 Electrocardiography 2.99 Clinical Skills - Other B IMAGING 3 Imaging 3.1 Echocardiography 3.2
Topic List A BASICS 1 History of Cardiology 2 Clinical Skills 2.1 History Taking 2.2 Physical Examination 2.3 Electrocardiography 2.99 Clinical Skills - Other B IMAGING 3 Imaging 3.1 Echocardiography 3.2
Are you not responding to antidepressants?
 PATIENTS & RELATIVES Are you not responding to antidepressants? TMS therapy might be the solution for you. Does not affect cognitive function No anesthesia Covered by most private providers Outpatient
PATIENTS & RELATIVES Are you not responding to antidepressants? TMS therapy might be the solution for you. Does not affect cognitive function No anesthesia Covered by most private providers Outpatient
AS with reduced LV ejection fraction: Contractile reserve should be systematically assessed: PRO
 AS with reduced LV ejection fraction: Contractile reserve should be systematically assessed: PRO Jean-Luc MONIN, MD, PhD Henri Mondor University Hospital Créteil, FRANCE Potential conflicts of interest
AS with reduced LV ejection fraction: Contractile reserve should be systematically assessed: PRO Jean-Luc MONIN, MD, PhD Henri Mondor University Hospital Créteil, FRANCE Potential conflicts of interest
TAVI: The Real Deal? Marc Pelletier, MD Head, Department of Cardiac Surgery New Brunswick Heart Centre
 TAVI: The Real Deal? Marc Pelletier, MD Head, Department of Cardiac Surgery New Brunswick Heart Centre Disclosure St. Jude Medical: Consultant and Proctor Edwards Lifesciences: Proctor Medtronic: Research
TAVI: The Real Deal? Marc Pelletier, MD Head, Department of Cardiac Surgery New Brunswick Heart Centre Disclosure St. Jude Medical: Consultant and Proctor Edwards Lifesciences: Proctor Medtronic: Research
Interventional procedures guidance Published: 26 July 2017 nice.org.uk/guidance/ipg586
 Transcatheter aortic valve implantation for aortic stenosis Interventional procedures guidance Published: 26 July 17 nice.org.uk/guidance/ipg586 Your responsibility This guidance represents the view of
Transcatheter aortic valve implantation for aortic stenosis Interventional procedures guidance Published: 26 July 17 nice.org.uk/guidance/ipg586 Your responsibility This guidance represents the view of
Improving assessment process of health technologies: Towards a MCDA approach?
 Improving assessment process of health technologies: Towards a MCDA approach? François Meyer MD Advisor to the President, International Affairs ISPOR Amsterdam November 2014 Assessment of clinical added
Improving assessment process of health technologies: Towards a MCDA approach? François Meyer MD Advisor to the President, International Affairs ISPOR Amsterdam November 2014 Assessment of clinical added
NATIONAL SURVEY OF YOUNG ADULTS ON HIV/AIDS
 NATIONAL SURVEY OF YOUNG ADULTS ON HIV/AIDS Kaiser Family Foundation November 30, 2017 Introduction More than three and a half decades have passed since the first case of AIDS. An entire generation has
NATIONAL SURVEY OF YOUNG ADULTS ON HIV/AIDS Kaiser Family Foundation November 30, 2017 Introduction More than three and a half decades have passed since the first case of AIDS. An entire generation has
Awareness and understanding of dementia in New Zealand
 Awareness and understanding of dementia in New Zealand Alzheimers NZ Telephone survey May 2017 Contents Contents... 2 Key findings... 3 Executive summary... 5 1 Methodology... 8 1.1 Background and objectives...
Awareness and understanding of dementia in New Zealand Alzheimers NZ Telephone survey May 2017 Contents Contents... 2 Key findings... 3 Executive summary... 5 1 Methodology... 8 1.1 Background and objectives...