Bệnh viện trung ương Quân đội 108 Viện tim mạch Triệt phá đường dẫn truyền phụ vùng dưới vách bằng sóng RF (Ablation of Posteroseptal AP)
|
|
|
- Matthew Patterson
- 5 years ago
- Views:
Transcription
1 Bệnh viện trung ương Quân đội 108 Viện tim mạch Triệt phá đường dẫn truyền phụ vùng dưới vách bằng sóng RF (Ablation of Posteroseptal AP) Bs. Phạm Trường Sơn

2 Posteroseptal AP :Inferoseptal AP (inferior to the true septal)

 Left to left, CS to left, CS to Diverticulum Ablated at: the MV ring, TV")
3 The most complex: Pyramid space, confluence of 4 chamber - Superior: Central fibrous - Anterior:Ventricular septum - Posterior: left and Right Atria - TV is 5 mm to MV: + right atrium- left Ventricle space (thin tissue: AP inside) + CS os: at the superior (ablation site) 4 courses: Right to right, Right to left (common) Left to left, CS to left, CS to Diverticulum Ablated at: the MV ring, TV ring, inside CS
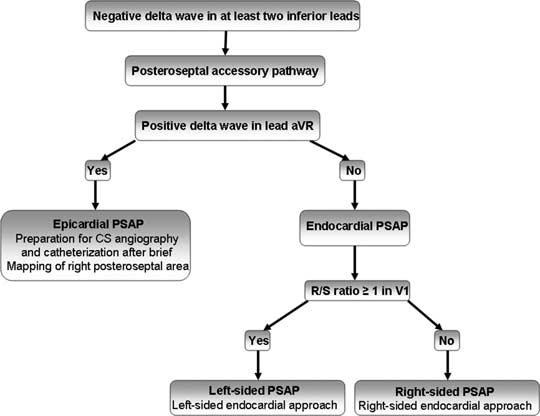
4 ECG characteristic 1/ Negative delta waves in leads III, avf (less common) positive delta waves in I and avl
5 2/Retrograde P waves : - Negative in the leads II, III, avf - Positive in AVR,AVL 3/ Slow and decremental retrograde conduction: incessant tachycardia. - Permanent junctional reciprocating tachycardia(pjrt)
6 EP Studying: 1. During AV reentrant tachycardia, the earliest atrial activation usually is recorded from + The ostium of the coronary sinus + The proximal coronary sinus within 2 cm (those beyond 1 2 cm are considered as left free-wall pathways: leftsided endocardial approach) 2. Functional left bundle branch block during tachycardia results in either no change or only a nominal prolongation of the VA interval (10 to 30 msec) - Functional right bundle branch block usually does not affect the VA interval.
7 Differentiation with SS-AVNRT (long VA time) - Advanced A during His refractoriness - Terminate tachy by PVC not conduct to A - Parahisian pacing: No change Stim to A - VA (V pacing and Tachy)< 85ms - VOD (PPI CL) <115 ms - VA pacing(at V base)<(at V apex)
8 Left sided aproach ECG 1/ Positive delta wave at V1, some study show no role 2/ R/S ratio 1 in lead V1 is the most predictive location 3/ If QRS transition between V1 and V2, the R-wave ( lead I) < S- wave mv is indicative of left-sided AP.

9 The 12-lead electrocardiogram of a patient with manifest right posteroseptal accessory pathway. R/S ratio < 1 in lead V1

10 The 12-lead electrocardiogram of a patient with manifest left posteroseptal. R/S ratio 1 in lead V1
11 EPS 1. Earliest atrial activation during AVRT was in the middle CS:
12 2. The prolongation (10 30ms increase) of the VA interval in response to the development of left bundle-branch block during orthodromic AVRT : 3. Long-RP AVRT defining a right endocardial AP.

13 4. The difference of VA intervals during AVRT, measured at the His catheter and the site of earliest atrial activation in the CS: -If 25 ms: a left endocardial AP in 89% of patients -If <25 ms in 95% of patients with a right endocardial or epicardial AP.
14 - These mapping criteria above are not necessarily predictive of where the effective ablation site is located. - Dhala et al: Overall success rate for the right-sided approach alone was 94% regardless of the above-mentioned electrophysiologic criteria + The right posteroseptum or the proximal coronary sinus: 50 % + The posteroseptal region of the tricuspid valve : 30% + Within the terminal 1 cm of the coronary sinus including its ostium: 16 % - Explained : many posteroseptal APs are right atrio-left ventricular fibers : right atrial approach
15 The most common reasons for prolonged or failed attempts at ablation: -Difficulties with catheter manipulation :48% +Inability to reach the appropriate AP site +Catheter instability + Inadequate tissue contact -Inaccurate mapping: 26% +AP at a site away from the mapped Area -The presence of epicardial APs

16 -40% of all patients referred after an unsuccessful ablation procedure - The CS method used as a primary method had an efficacy rate of 56% -The prevalence of an epicardial AP was 4%-25%. The largest series by Sun et al.: + CS-associated AP in 171 pt (36%) - Arruda et al :24% of the patients with posteroseptal APs required RF application in a venous branch or anomaly of the CS +(22%) in CS diverticulum and (70%) in the middle cardiac vein - Require: longer procedure times, longer radiation exposure, more RF, complication

17 - Embryologically, the CS develops: + As a remnant of sinus venosus musculature and as a continuation of RA + 40 mm of the CS is surrounded: striated muscle, with connections to LA - When connected with the epicardial surface of the ventricle: epicardial AP -Multiple left atrial myocardium connections to V: +Ablation at the Atrial site often produces : change in the activation sequence, should target at single V insertion. - Extensions of the CS myocardial coat to the : 5-20 mm deep into the vein +The middle cardiac vein (MCV): 82% + Posterior coronary vein (PCV):11% +Both vein: 5% -Requires ablation of the ventricular end at the insertion of the MCV or PCV into the CS
18 Diagnosis -Negative delta wave in lead II : highly specific finding for epicardial +Highest sensitivity (87%) +Low specificity (20-70%) -Positive delta in avr + Highest specificity (99%) + Moderate sensitivity (70%) -Deep S in V6 + Se: 70% + Sp:87% - Combination of 2 mentioned criteria: Highly accurate predictor -The differentiation between epicardial and left endocardial Ap: difficult.
19

20 -The delta wave is negative in III, and AVF: posteroseptal region. - Delta wave is negative in lead II and positive in AVR. -AP can be localized to CS

21 The 12-lead electrocardiogram of a patient with manifest epicardial posteroseptal accessory pathway. Positive delta wave in lead avr, and deep S-wave in V6.
22 Target 1. Earliest ventricular activation during atrial pacing or earliest atrial activation during ventricular pacing/orthodromic reciprocating tachycardia. -Not ideal. For example, downward slanted posteroseptal pathway, the earliest atrial activation may be close to the compact AV node. 2. Fragmented or double potentials at the site of earliest atrial activation in the CS: during retrograde conduction -While further away from this site the potentials frequently fused producing a single patter - Antz clarify the double potential at CS. +One is sharp potential representing CS musculature +The other is rouded, recorded along the floor of the CS and usually ( leftward activation of the CS musculature).
23 3. The ideal site for successful ablation: at a site where the accessory pathway courses epicardially (accessory pathway potentials) -A strong relation between AP potential amplitude and success +The large amplitude of AP potential indicates close proximity to the AP -Differentiate with the other signal from: the atrial electrogram, ventricular electrogram, His bundle electrogram.

24 - Pacing at a more rapid rate causes block in the accessory pathway and subsequently block in the AV node, as well. -The A and V electrogram is seen to be easily dissociated from the accessory pathway potential (Ap)
25 - Power <30 W, irrigated <15 w RF delivery inside CS -Avoided in distal small branches of CS: -Slow flow Lack of cooling high temperature low power delivery, venous occlusion. -Intramural thrombosis of the CS has been reported. - Solution : + Larger catheter electrodes or fluid irrigation can be used
26 Outcomes of posteroseptal ablation - Successful rate: 93%-98% - Complication: +CS branch: venous perforation, tamponade, venous occlusion -Damage to the RCA - Heart block: rare, AV nodal artery -Recurrence: 6-50%.
27 Coronary Artery Injury - Extremely low (0.06% - 0.1% ) - Within 2 mm of the ablation site - Acutely or several weeks after ablation - The acute injury due to : + Vasospasm from thermal energy: reversible ST segment elevation, normal angiography + RF energy directly on a coronary artery: acute edema with wall thickening and luminal narrowing, thrombosis with complete obstruction -Delayed coronary injury: Intimal hyperplasia, damages to the arterial wall and endothelium, which provides a nidus for progressive thrombus formation weeks later

28 LAO: + Ablation catheter placed near the ostium of the middle cardiac vein. + A guiding sheath has engaged the right coronary artery

29 Ng.Th.T I II III AVR AVL AVF V1 V2 V3 V4 V5

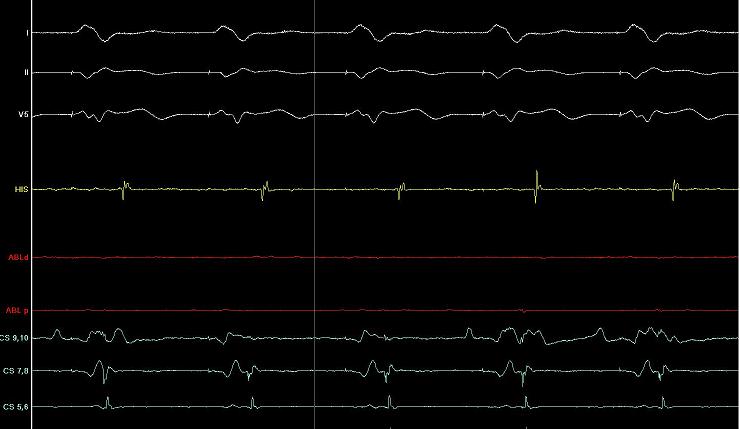
30 Erliest at CS 9-10 during SVT

31 Intermitent AP after Abl
32 AP gone

33 Tr.Q.H

34 VA during tachy

35 AP potential

36 VA block after ablation
37
38
39
40
41

42
43
44 CS aneurysm - The prevalence of CS aneurysms in patients with left posteroseptal AP: 2% to 26%. -If presented in postero AP, usually as connection.
 - 25% of the cases, aneurysm extends from the medial cardiac vein rather than from the CS itself -It Result from incomplete regression of the sinus venosus -Postmortem:")
45 - The majority of CS aneurysms are located along the inferoseptal aspect of the CS (usually within1.5 cm of the CS ostium) - 25% of the cases, aneurysm extends from the medial cardiac vein rather than from the CS itself -It Result from incomplete regression of the sinus venosus -Postmortem: muscular bundle within the wall of diverticulum, a continuation of the usual fibers found in the proximal coronary sinus. - When these fibers connect the atrial myocardium to ventricular myocardium, a complex epicardial accessory pathway is created.
46 -The aneurysm connects with the CS by either a narrow, intermediate, or broad neck. -These diverticulum all occurred in manifest AP due to bidirectional conduction. +A case reported by kivotaka (jpn circ J 2000) one pt with concealed AP successfully ablated at the neck of diverticulum. -The effective ablation was at the neck. At this site, a relative longer retrograde conduction, a larger potential AP - One approach to ablation: Circumferential ablation at the mouth of the diverticulum

47 -Extensive mapping in the right atrium, the coronary sinus (CS) and its branches, and the left atrium: was performed. No result - A CS: angiogram showed the presence of a diverticulum. The earliest ventricular activation was localized to the posteroregion -RF in this area failed to eliminate. -Subxiphoid percutaneous epicardial access, extensive endocardial and epicardial mapping was performed. - The earliest ventricular activation was mapped to the epicardial surface in the posteroseptal region).

48 - A coronary angiogram was performed to ensure that the ablation catheter was not in close proximity to one of the epicardial coronary arteries -The accessory pathway was eliminated after 6.5 seconds - Because of the thickness of the myocardium in this area, energy delivered from endocardial ablation often may not reach the epicardial location of the accessory pathway. - The epicardial ablation lesions were clearly at a distance away from the sites of attempted endocardial ablation. - Epicardial approach should be considered when repeated attempts of endocardial ablation fail
 -Three previous unsuccessful ablations -Large coronary sinus diverticulum: no electrogram recorded endocardially or within the CS diverticulum preceded the delta wave")

49 Cleveland, Ohio (PACE 2002; SAAD, E.B., ET AL.) -Three previous unsuccessful ablations -Large coronary sinus diverticulum: no electrogram recorded endocardially or within the CS diverticulum preceded the delta wave -Epicardial mapping through the pericardial approach: the earliest recorded activation, indicating an epicardial location. -However, RF at this site was not possible due to high impedances. +Reason: the presence of a relatively thick overlying epicardial fat pad located above the AP that impeded the delivery of energy -Intravascular linear lesions transecting the neck of the large coronary sinus diverticulum using the pericardial catheter: successful ablation
, and left anterior oblique (right panel)")
50 Monther Boulos report a case: -Two previous attempts had failed to ablate the posteroseptal AP - The presence of a large bilobar CS aneurysm with a relatively narrow connection between the two lobes AP (left panel), and left anterior oblique (right panel) views.
51 Use the antegrade approach for ablation because + The previous failed attempts +The possible presence of multiple connection sites between the CS musculature and the left atrium - This very low ventricular insertion site may also be one of the reasons for the absence of a deep S wave in lead V6 during sinus rhythm in this patient.

52 Carto was used: - Mapping within the CS aneurysm: delineated its geometry + The earliest ventricular site at the lowest portion (4-5 cm beneath the CS ostium) of the aneurysm. +Preceded the delta wave by 51 ms -A single RF application delivered at this site was sufficient to terminate conduction via this accessory pathway.
53 -The fusion of the local CS aneurysm-related potential with the earliest ventricular electrogram prior to RF ablation. - The dissociation between the two potentials following successful ablation
 39-year-old woman presented with atrial fibrillation, -Accessory pathway conduction was abolished surgically - Follow-up electrophysiological study demonstrated a residual accessory")
54 Neil C. Davidson, (Circulation. 2001;104: ) 39-year-old woman presented with atrial fibrillation, -Accessory pathway conduction was abolished surgically - Follow-up electrophysiological study demonstrated a residual accessory ventriculoatria connection. coronary sinus angiography was performed. Large saccular diverticulum at the coronary sinus os in the posterior septum and a smaller diverticulum next to the posterior cardiac vein which are labeled D1 and D2. PCV indicates posterior cardiac vein.
55 - Orthodromic tachycardia was easily inducible, with the accessory pathway as the retrograde limb. - During ventricular pacing, the earliest atrial activation was in the smaller diverticulum -Radiofrequency ablation resulted in loss of retrograde conduction after 3 seconds
56 Practical Approach -Begin at right sided, except strongly suggest left-sided ( R/S ratio in lead V1 1) -CS and its branches is recommended: after a brief mapping of the right posteroseptal area - CS venography done if no site found (esp: AVR (+), deep S at V6): The presence of venous anomaly identify the site of AP - If no, left sided tried, Epicardial approach - Electroanatomical mapping: more complex CS anomalies, multiple accessory pathway

57 XIN CHÂN THÀNH CẢM ƠN
LONG RP TACHYCARDIA MAPPING AND RF ABLATION
 LONG RP TACHYCARDIA MAPPING AND RF ABLATION Dr. Hayam Eldamanhoury Ain shams univeristy Arrhythmia is a too broad topic SVT is broadly defined as narrow complex ( unless aberrant conduction ) Requires
LONG RP TACHYCARDIA MAPPING AND RF ABLATION Dr. Hayam Eldamanhoury Ain shams univeristy Arrhythmia is a too broad topic SVT is broadly defined as narrow complex ( unless aberrant conduction ) Requires
Differential diagnosis and pacing in maneuvers narrow QRS tachycardia. Richard Schilling
 Differential diagnosis and pacing in maneuvers narrow QRS tachycardia Richard Schilling Differential diagnosis of narrow complex QRS tachycardia Anything that activates the ventricle normally via the His
Differential diagnosis and pacing in maneuvers narrow QRS tachycardia Richard Schilling Differential diagnosis of narrow complex QRS tachycardia Anything that activates the ventricle normally via the His
ACCESSORY PATHWAYS AND SVT. Neil Grubb Royal Infirmary of Edinburgh
 ACCESSORY PATHWAYS AND SVT Neil Grubb Royal Infirmary of Edinburgh Bypass tracts - properties accessory AV connections usually endocardial may exhibit unidirectional conduction conduction properties similar
ACCESSORY PATHWAYS AND SVT Neil Grubb Royal Infirmary of Edinburgh Bypass tracts - properties accessory AV connections usually endocardial may exhibit unidirectional conduction conduction properties similar
EHRA Accreditation Exam - Sample MCQs Invasive cardiac electrophysiology
 EHRA Accreditation Exam - Sample MCQs Invasive cardiac electrophysiology Dear EHRA Member, Dear Colleague, As you know, the EHRA Accreditation Process is becoming increasingly recognised as an important
EHRA Accreditation Exam - Sample MCQs Invasive cardiac electrophysiology Dear EHRA Member, Dear Colleague, As you know, the EHRA Accreditation Process is becoming increasingly recognised as an important
A Narrow QRS Complex Tachycardia With An Apparently Concentric Retrograde Atrial Activation Sequence
 www.ipej.org 125 Case Report A Narrow QRS Complex Tachycardia With An Apparently Concentric Retrograde Atrial Activation Sequence Miguel A. Arias MD, PhD; Eduardo Castellanos MD, PhD; Alberto Puchol MD;
www.ipej.org 125 Case Report A Narrow QRS Complex Tachycardia With An Apparently Concentric Retrograde Atrial Activation Sequence Miguel A. Arias MD, PhD; Eduardo Castellanos MD, PhD; Alberto Puchol MD;
Basic Electrophysiology Protocols
 Indian Journal of Cardiology ISSN-0972-1622 2012 by the Indian Society of Cardiology Vol. 15, (3-4), 27-37 [ 27 Review Article Shomu Bohora Assistant Professor, Deptt. of Cardiology, U.N. Mehta Institute
Indian Journal of Cardiology ISSN-0972-1622 2012 by the Indian Society of Cardiology Vol. 15, (3-4), 27-37 [ 27 Review Article Shomu Bohora Assistant Professor, Deptt. of Cardiology, U.N. Mehta Institute
Tachy. Induction tachycardia lead ECG during Tachy /25/2009. Sinus Rhythm Single His
 12-lead ECG during Tachy 10.30.31 Sinus Rhythm Single His 11.20.02 Induction tachycardia 11.23.23 Tachy 11.25.23 1 I This finding excludes: (a) AVNRT (either typical or atypical) Tachy: Alternating cycle
12-lead ECG during Tachy 10.30.31 Sinus Rhythm Single His 11.20.02 Induction tachycardia 11.23.23 Tachy 11.25.23 1 I This finding excludes: (a) AVNRT (either typical or atypical) Tachy: Alternating cycle
Uncommon forms of AV reentry: atrio and fasciculo-ventricular fibers, slow conducting fibers. Jesus Almendral, Madrid, Spain
 Uncommon forms of AV reentry: atrio and fasciculo-ventricular fibers, slow conducting fibers Jesus Almendral, Madrid, Spain Common forms of AV reentry Accessory pathways: Upper insertion: atrium Lower
Uncommon forms of AV reentry: atrio and fasciculo-ventricular fibers, slow conducting fibers Jesus Almendral, Madrid, Spain Common forms of AV reentry Accessory pathways: Upper insertion: atrium Lower
Case 1 Left Atrial Tachycardia
 Case 1 Left Atrial Tachycardia A 16 years old woman was referred to our institution because of recurrent episodes of palpitations and dizziness despite previous ablation procedure( 13 years ago) of postero-septal
Case 1 Left Atrial Tachycardia A 16 years old woman was referred to our institution because of recurrent episodes of palpitations and dizziness despite previous ablation procedure( 13 years ago) of postero-septal
Supraventricular Tachycardia (SVT)
") Supraventricular Tachycardia (SVT) Bruce Stambler, MD Piedmont Heart Atlanta, GA Supraventricular Tachycardia Objectives Types and mechanisms AV nodal reentrant tachycardia (AVNRT) AV reciprocating tachycardia
Supraventricular Tachycardia (SVT) Bruce Stambler, MD Piedmont Heart Atlanta, GA Supraventricular Tachycardia Objectives Types and mechanisms AV nodal reentrant tachycardia (AVNRT) AV reciprocating tachycardia
Declaration of conflict of interest NONE
 Declaration of conflict of interest NONE Transatlantic Electrophysiology Lessons for and from Iberoamerica European Society of Cardiology Mexican Society of Cardiology Wolff-Parkinson-White Syndrome in
Declaration of conflict of interest NONE Transatlantic Electrophysiology Lessons for and from Iberoamerica European Society of Cardiology Mexican Society of Cardiology Wolff-Parkinson-White Syndrome in
WPW syndrome and AVRT
 WPW syndrome and AVRT Myung-Yong Lee, MD, PhD Division of Cardiology Department of Internal Medicine School of Medicine Dankook University, Cheonan, Korea Supraventricular tachycardia (SVT) Paroxysmal
WPW syndrome and AVRT Myung-Yong Lee, MD, PhD Division of Cardiology Department of Internal Medicine School of Medicine Dankook University, Cheonan, Korea Supraventricular tachycardia (SVT) Paroxysmal
Case Report Wide-QRS Tachycardia Inducible by Both Atrial and Ventricular Pacing
 Hellenic J Cardiol 2008; 49: 446-450 Case Report Wide-QRS Tachycardia Inducible by Both Atrial and Ventricular Pacing ELEFTHERIOS GIAZITZOGLOU, DEMOSTHENES G. KATRITSIS Department of Cardiology, Athens
Hellenic J Cardiol 2008; 49: 446-450 Case Report Wide-QRS Tachycardia Inducible by Both Atrial and Ventricular Pacing ELEFTHERIOS GIAZITZOGLOU, DEMOSTHENES G. KATRITSIS Department of Cardiology, Athens
Coronary sinus (CS) diverticula 1 5 have been associated
 diverticula 1 5 have been associated") Coronary Sinus-Ventricular Accessory Connections Producing Posteroseptal and Left Posterior Accessory Pathways Incidence and Electrophysiological Identification Yingxian Sun, MD; Mauricio Arruda, MD; Kenichiro
Coronary Sinus-Ventricular Accessory Connections Producing Posteroseptal and Left Posterior Accessory Pathways Incidence and Electrophysiological Identification Yingxian Sun, MD; Mauricio Arruda, MD; Kenichiro
Circulation: Arrhythmia and Electrophysiology CHALLENGE OF THE WEEK
 A 14-year-old girl with Wolff-Parkinson-White syndrome and recurrent paroxysmal palpitations due to atrioventricular reentry tachycardia had undergone two prior failed left lateral accessory pathway ablations
A 14-year-old girl with Wolff-Parkinson-White syndrome and recurrent paroxysmal palpitations due to atrioventricular reentry tachycardia had undergone two prior failed left lateral accessory pathway ablations
COMPLEX CASE STUDY INNOVATIVE COLLECTIONS. Case presentation
 The Journal of Innovations in Cardiac Rhythm Management, 3 (2012), 939 943 INNOVATIVE COLLECTIONS COMPLEX CASE STUDY Subtle Changes in Electrogram Morphology During Para-Hisian Pacing Performed on IV Adenosine:
The Journal of Innovations in Cardiac Rhythm Management, 3 (2012), 939 943 INNOVATIVE COLLECTIONS COMPLEX CASE STUDY Subtle Changes in Electrogram Morphology During Para-Hisian Pacing Performed on IV Adenosine:
AV Node Dependent SVT:Substrates, Mechanisms, and Recognition
 AV Node Dependent SVT:Substrates, Mechanisms, and Recognition Ching-Tai Tai Taipei Veterans General Hospital National Yang-Ming University AV Node Reentry Anatomy Physiology Anatomic-Physiologic Relation
AV Node Dependent SVT:Substrates, Mechanisms, and Recognition Ching-Tai Tai Taipei Veterans General Hospital National Yang-Ming University AV Node Reentry Anatomy Physiology Anatomic-Physiologic Relation
How to ablate typical slow/fast AV nodal reentry tachycardia
 Europace (2000) 2, 15 19 Article No. eupc.1999.0070, available online at http://www.idealibrary.com on OW TO... SERIES ow to ablate typical slow/fast AV nodal reentry tachycardia. eidbüchel Department
Europace (2000) 2, 15 19 Article No. eupc.1999.0070, available online at http://www.idealibrary.com on OW TO... SERIES ow to ablate typical slow/fast AV nodal reentry tachycardia. eidbüchel Department
Anatomical Problems with Identification and Interruption of Posterior Septa1 Kent Bundles
 Anatomical Problems with Identification and Interruption of Posterior Septa1 Kent Bundles Will C. Sealy, M.D., and Eileen M. Mikat, Ph.D. ABSTRACT To gain insight into the cause of the complex anatomical
Anatomical Problems with Identification and Interruption of Posterior Septa1 Kent Bundles Will C. Sealy, M.D., and Eileen M. Mikat, Ph.D. ABSTRACT To gain insight into the cause of the complex anatomical
Conventional Mapping. Introduction
 Conventional Mapping Haitham Badran Ain Shams University it Introduction The mapping approach used to guide ablation depends on the type of arrhythmia being assessed. Simple fluoroscopic anatomy is essential
Conventional Mapping Haitham Badran Ain Shams University it Introduction The mapping approach used to guide ablation depends on the type of arrhythmia being assessed. Simple fluoroscopic anatomy is essential
II V 1 HRA 3 4 HB 5 6 HB 3 4 HB 1 2 CS 7 8 CS 5 6 CS 3 4 CS 1 2 ABL 3 4 ABL 1 2 RVA 3 4. T. Suga et al.
 Table 1. The distance between the positions of the catheter tip Patient Location Before elimination of After elimination of Number of the the accessory pathway the accessory pathway accessory pathway RAO
Table 1. The distance between the positions of the catheter tip Patient Location Before elimination of After elimination of Number of the the accessory pathway the accessory pathway accessory pathway RAO
A request for a log book extension must be put in writing and sent to BHRS, Unit 6B, Essex House, Cromwell Business Park, Chipping Norton,
 7 7. A request for a log book extension must be put in writing and sent to BHRS, Unit 6B, Essex House, Cromwell Business Park, Chipping Norton, Oxfordshire OX7 5SR. E-mail: admin@bhrs.com. Tel: 01789 867
7 7. A request for a log book extension must be put in writing and sent to BHRS, Unit 6B, Essex House, Cromwell Business Park, Chipping Norton, Oxfordshire OX7 5SR. E-mail: admin@bhrs.com. Tel: 01789 867
PARA-HISSIAN CONCEALED ACCESSORY PATHWAY
 PARA-HISSIAN CONCEALED ACCESSORY PATHWAY Anamnestic Findings 41 y.o. man with normal cardiac findings on echocardiography, suffering for paroxysmal supra-ventricular tachycardia since 1982 with rapid onset
PARA-HISSIAN CONCEALED ACCESSORY PATHWAY Anamnestic Findings 41 y.o. man with normal cardiac findings on echocardiography, suffering for paroxysmal supra-ventricular tachycardia since 1982 with rapid onset
Catheter Ablation of VT Without Structural Heart Disease 성균관의대 온영근
 Catheter Ablation of VT Without Structural Heart Disease 성균관의대 온영근 Idiopathic Monomorphic Ventricular Tachycardia Adenosine-sensitive Verapamil-sensitive Propranolol-sensitive Mech (Triggered activity)
Catheter Ablation of VT Without Structural Heart Disease 성균관의대 온영근 Idiopathic Monomorphic Ventricular Tachycardia Adenosine-sensitive Verapamil-sensitive Propranolol-sensitive Mech (Triggered activity)
Case Report Simultaneous Accessory Pathway and AV Node Mechanical Block
 185 Case Report Simultaneous Accessory Pathway and AV Node Mechanical Block Daniel Garofalo, MD, FRACP, Alfonso Gomez Gallanti, MD, David Filgueiras Rama, MD, Rafael Peinado Peinado, PhD, FESC Unidad de
185 Case Report Simultaneous Accessory Pathway and AV Node Mechanical Block Daniel Garofalo, MD, FRACP, Alfonso Gomez Gallanti, MD, David Filgueiras Rama, MD, Rafael Peinado Peinado, PhD, FESC Unidad de
Incessant Tachycardia Using a Concealed Atrionodal Bypass Tract
 191 Incessant Tachycardia Using a Concealed Atrionodal Bypass Tract ADAM ZIVIN, M.D., atid FRED MORADY, M.D. From the Division of Cardiology. Department of Internal Medicine, University of Michigan Medical
191 Incessant Tachycardia Using a Concealed Atrionodal Bypass Tract ADAM ZIVIN, M.D., atid FRED MORADY, M.D. From the Division of Cardiology. Department of Internal Medicine, University of Michigan Medical
Ventricular Preexcitation (Wolff-Parkinson-White Syndrome and Its Variants) 柯文欽醫師 國泰綜合醫院心臟內科主治醫師 臺北醫學大學講師
 柯文欽醫師 國泰綜合醫院心臟內科主治醫師 臺北醫學大學講師") Ventricular Preexcitation (Wolff-Parkinson-White Syndrome and Its Variants) 柯文欽醫師 國泰綜合醫院心臟內科主治醫師 臺北醫學大學講師 The Nobel Prize in Physiology or Medicine 1924 "for his discovery of the mechanism of the electrocardiogram"
Ventricular Preexcitation (Wolff-Parkinson-White Syndrome and Its Variants) 柯文欽醫師 國泰綜合醫院心臟內科主治醫師 臺北醫學大學講師 The Nobel Prize in Physiology or Medicine 1924 "for his discovery of the mechanism of the electrocardiogram"
Advances in Ablation Therapy for Ventricular Tachycardia
 Advances in Ablation Therapy for Ventricular Tachycardia Nitish Badhwar, MD, FACC, FHRS Director, Cardiac Electrophysiology Training Program University of California, San Francisco For those of you who
Advances in Ablation Therapy for Ventricular Tachycardia Nitish Badhwar, MD, FACC, FHRS Director, Cardiac Electrophysiology Training Program University of California, San Francisco For those of you who
ECG Interpretation Made Easy
 ECG Interpretation Made Easy Dr. A Tageldien Abdellah, MSc MD EBSC Lecturer of Cardiology- Hull University Hull York Medical School 2007-2008 ECG Interpretation Made Easy Synopsis Benefits Objectives Process
ECG Interpretation Made Easy Dr. A Tageldien Abdellah, MSc MD EBSC Lecturer of Cardiology- Hull University Hull York Medical School 2007-2008 ECG Interpretation Made Easy Synopsis Benefits Objectives Process
Medicine. Dynamic Changes of QRS Morphology of Premature Ventricular Contractions During Ablation in the Right Ventricular Outflow Tract
 Medicine CLINICAL CASE REPORT Dynamic Changes of QRS Morphology of Premature Ventricular Contractions During Ablation in the Right Ventricular Outflow Tract A Case Report Li Yue-Chun, MD, Lin Jia-Feng,
Medicine CLINICAL CASE REPORT Dynamic Changes of QRS Morphology of Premature Ventricular Contractions During Ablation in the Right Ventricular Outflow Tract A Case Report Li Yue-Chun, MD, Lin Jia-Feng,
Title. CitationJournal of Electrocardiology, 39(4): Issue Date Doc URL. Type. File Information. coronary sinus ostium
: Issue Date Doc URL. Type. File Information. coronary sinus ostium") Title Nonreentrant atrioventricular nodal tachycardia due coronary sinus ostium Author(s)Yokoshiki, Hisashi; Sasaki, Koji; Shimokawa, Junichi CitationJournal of Electrocardiology, 39(4): 395-399 Issue
Title Nonreentrant atrioventricular nodal tachycardia due coronary sinus ostium Author(s)Yokoshiki, Hisashi; Sasaki, Koji; Shimokawa, Junichi CitationJournal of Electrocardiology, 39(4): 395-399 Issue
Ankara, Turkey 2 Department of Cardiology, Division of Arrhythmia and Electrophysiology, Yuksek Ihtisas
 258 Case Report Electroanatomic Mapping-Guided Radiofrequency Ablation of Adenosine Sensitive Incessant Focal Atrial Tachycardia Originating from the Non-Coronary Aortic Cusp in a Child Serhat Koca, MD
258 Case Report Electroanatomic Mapping-Guided Radiofrequency Ablation of Adenosine Sensitive Incessant Focal Atrial Tachycardia Originating from the Non-Coronary Aortic Cusp in a Child Serhat Koca, MD
Case Report Left Ventricular Dysfunction Caused by Unrecognized Surgical AV block in a Patient with a Manifest Right Free Wall Accessory Pathway
 109 Case Report Left Ventricular Dysfunction Caused by Unrecognized Surgical AV block in a Patient with a Manifest Right Free Wall Accessory Pathway Rakesh Gopinathannair, MD, MA 1, Dwayne N Campbell,
109 Case Report Left Ventricular Dysfunction Caused by Unrecognized Surgical AV block in a Patient with a Manifest Right Free Wall Accessory Pathway Rakesh Gopinathannair, MD, MA 1, Dwayne N Campbell,
Ablative Therapy for Ventricular Tachycardia
 Ablative Therapy for Ventricular Tachycardia Nitish Badhwar, MD, FACC, FHRS 2 nd Annual UC Davis Heart and Vascular Center Cardiovascular Nurse / Technologist Symposium May 5, 2012 Disclosures Research
Ablative Therapy for Ventricular Tachycardia Nitish Badhwar, MD, FACC, FHRS 2 nd Annual UC Davis Heart and Vascular Center Cardiovascular Nurse / Technologist Symposium May 5, 2012 Disclosures Research
Goals 2/10/2016. Voltage Gradient Mapping: A Novel Approach for Successful Ablation of AV Nodal Reentry Tachycardia
 Voltage Gradient Mapping: A Novel Approach for Successful Ablation of AV Nodal Reentry Tachycardia Steven J. Bailin*, MD ; FACC, FHRS Iowa Heart Center, Des Moines, IA University of Iowa Hospital and Clinics,
Voltage Gradient Mapping: A Novel Approach for Successful Ablation of AV Nodal Reentry Tachycardia Steven J. Bailin*, MD ; FACC, FHRS Iowa Heart Center, Des Moines, IA University of Iowa Hospital and Clinics,
Chapter 16: Arrhythmias and Conduction Disturbances
 Complete the following. Chapter 16: Arrhythmias and Conduction Disturbances 1. Cardiac arrhythmias result from abnormal impulse, abnormal impulse, or both mechanisms together. 2. is the ability of certain
Complete the following. Chapter 16: Arrhythmias and Conduction Disturbances 1. Cardiac arrhythmias result from abnormal impulse, abnormal impulse, or both mechanisms together. 2. is the ability of certain
Supraventricular Tachycardia: From Fetus to Adult. Mohamed Hamdan, MD
 Supraventricular Tachycardia: From Fetus to Adult Mohamed Hamdan, MD Learning Objectives Define type of SVT by age Describe clinical approach Describe prenatal and postnatal management of SVT 2 SVT Across
Supraventricular Tachycardia: From Fetus to Adult Mohamed Hamdan, MD Learning Objectives Define type of SVT by age Describe clinical approach Describe prenatal and postnatal management of SVT 2 SVT Across
The Efficient and Smart Methods for Diagnosis of SVT 대구파티마병원순환기내과정병천
 The Efficient and Smart Methods for Diagnosis of SVT 대구파티마병원순환기내과정병천 Differentiation Supraventricular Origin from Ventricular Origin on ECG. QRS-Complex Width. 1. Narrow QRS-Complex Tachycardia (
The Efficient and Smart Methods for Diagnosis of SVT 대구파티마병원순환기내과정병천 Differentiation Supraventricular Origin from Ventricular Origin on ECG. QRS-Complex Width. 1. Narrow QRS-Complex Tachycardia (
Interventional Cardiology. Research Article
 Interventional Cardiology Accuracy of the new electrocardiogram algorithm in predicting localization of accessory pathways in patients with typical Wolff-Parkinson- White syndrome Objective: This study
Interventional Cardiology Accuracy of the new electrocardiogram algorithm in predicting localization of accessory pathways in patients with typical Wolff-Parkinson- White syndrome Objective: This study
CATHETER ABLATION FOR TACHYCARDIAS
 190 CATHETER ABLATION FOR TACHYCARDIAS MASOOD AKHTAR, M.D. T ACHY ARRHYTHMIAS constitute a major cause of mortality and morbidity. The most serious manifestation of cardiac arrhythmia is sudden cardiac
190 CATHETER ABLATION FOR TACHYCARDIAS MASOOD AKHTAR, M.D. T ACHY ARRHYTHMIAS constitute a major cause of mortality and morbidity. The most serious manifestation of cardiac arrhythmia is sudden cardiac
In certain cases of supraventricular
 Case Report Hellenic J Cardiol 2013; 54: 469-473 A Tachycardia with Varying QRS Morphology and RP Intervals: Differential Diagnosis and Therapy Socrates Korovesis, Eleftherios Giazitzoglou, Demosthenes
Case Report Hellenic J Cardiol 2013; 54: 469-473 A Tachycardia with Varying QRS Morphology and RP Intervals: Differential Diagnosis and Therapy Socrates Korovesis, Eleftherios Giazitzoglou, Demosthenes
Case Report Mahaim Fiber Accelerated Automaticity and Clues to a Mahaim Fiber Being Morphologically an Ectopic or a Split AV Node
 www.ipej.org 62 Case Report Mahaim Fiber Accelerated Automaticity and Clues to a Mahaim Fiber Being Morphologically an Ectopic or a Split AV Node Shomu Bohora, Narayanan Namboodiri, Santosh Dora, VK Ajit
www.ipej.org 62 Case Report Mahaim Fiber Accelerated Automaticity and Clues to a Mahaim Fiber Being Morphologically an Ectopic or a Split AV Node Shomu Bohora, Narayanan Namboodiri, Santosh Dora, VK Ajit
Mapping and Ablation of Challenging Outflow Tract VTs: Pulmonary Artery, LVOT, Epicardial
 Mapping and Ablation of Challenging Outflow Tract VTs: Pulmonary Artery, LVOT, Epicardial Samuel J. Asirvatham, MD Mayo Clinic Rochester California Heart Rhythm Symposium San Francisco, CA September 8,
Mapping and Ablation of Challenging Outflow Tract VTs: Pulmonary Artery, LVOT, Epicardial Samuel J. Asirvatham, MD Mayo Clinic Rochester California Heart Rhythm Symposium San Francisco, CA September 8,
Electrocardiography Normal 5. Faisal I. Mohammed, MD, PhD
 Electrocardiography Normal 5 Faisal I. Mohammed, MD, PhD 1 Objectives 2 1. Describe the different waves in a normal electrocardiogram. 2. Recall the normal P-R and Q-T interval time of the QRS wave. 3.
Electrocardiography Normal 5 Faisal I. Mohammed, MD, PhD 1 Objectives 2 1. Describe the different waves in a normal electrocardiogram. 2. Recall the normal P-R and Q-T interval time of the QRS wave. 3.
Looks Like VT But Isn't - Successful Ablation Of A Left Free Wall Accessory Pathway With Mahaim-like Properties
 www.ipej.org 112 Case Report Looks Like VT But Isn't - Successful Ablation Of A Left Free Wall Accessory Pathway With Mahaim-like Properties Faizel Osman MD MRCP 1, Peter J Stafford BSc MD FRCP 2, G Andre
www.ipej.org 112 Case Report Looks Like VT But Isn't - Successful Ablation Of A Left Free Wall Accessory Pathway With Mahaim-like Properties Faizel Osman MD MRCP 1, Peter J Stafford BSc MD FRCP 2, G Andre
VENTRICULAR TACHYCARDIA IN THE ABSENCE OF STRUCTURAL HEART DISEASE
 VENTRICULAR TACHYCARDIA IN THE ABSENCE OF STRUCTURAL HEART DISEASE Dimosthenis Avramidis, MD. Consultant Mitera Children s Hospital Athens Greece Scientific Associate 1st Cardiology Dpt Evangelismos Hospital
VENTRICULAR TACHYCARDIA IN THE ABSENCE OF STRUCTURAL HEART DISEASE Dimosthenis Avramidis, MD. Consultant Mitera Children s Hospital Athens Greece Scientific Associate 1st Cardiology Dpt Evangelismos Hospital
This presentation will deal with the basics of ECG description as well as the physiological basics of
 Snímka 1 Electrocardiography basics This presentation will deal with the basics of ECG description as well as the physiological basics of Snímka 2 Lecture overview 1. Cardiac conduction system functional
Snímka 1 Electrocardiography basics This presentation will deal with the basics of ECG description as well as the physiological basics of Snímka 2 Lecture overview 1. Cardiac conduction system functional
Catheter Ablation of Supraventricular Arrhythmias: State of the Art
 124 NASPE 25TH ANNIVERSARY SERIES Catheter Ablation of Supraventricular Arrhythmias: State of the Art FRED MORADY, M.D. From the Division of Cardiology, Department of Medicine, University of Michigan,
124 NASPE 25TH ANNIVERSARY SERIES Catheter Ablation of Supraventricular Arrhythmias: State of the Art FRED MORADY, M.D. From the Division of Cardiology, Department of Medicine, University of Michigan,
human anatomy 2016 lecture thirteen Dr meethak ali ahmed neurosurgeon
 Heart The heart is a hollow muscular organ that is somewhat pyramid shaped and lies within the pericardium in the mediastinum. It is connected at its base to the great blood vessels but otherwise lies
Heart The heart is a hollow muscular organ that is somewhat pyramid shaped and lies within the pericardium in the mediastinum. It is connected at its base to the great blood vessels but otherwise lies
Case-Based Practical ECG Interpretation for the Generalist
 Case-Based Practical ECG Interpretation for the Generalist Paul D. Varosy, MD, FACC, FAHA, FHRS Director of Cardiac Electrophysiology VA Eastern Colorado Health Care System Associate Professor of Medicine
Case-Based Practical ECG Interpretation for the Generalist Paul D. Varosy, MD, FACC, FAHA, FHRS Director of Cardiac Electrophysiology VA Eastern Colorado Health Care System Associate Professor of Medicine
ECG. Prepared by: Dr.Fatima Daoud Reference: Guyton and Hall Textbook of Medical Physiology,12 th edition Chapters: 11,12,13
 ECG Prepared by: Dr.Fatima Daoud Reference: Guyton and Hall Textbook of Medical Physiology,12 th edition Chapters: 11,12,13 The Concept When the cardiac impulse passes through the heart, electrical current
ECG Prepared by: Dr.Fatima Daoud Reference: Guyton and Hall Textbook of Medical Physiology,12 th edition Chapters: 11,12,13 The Concept When the cardiac impulse passes through the heart, electrical current
Title. CitationJournal of Electrocardiology, 43(5): Issue Date Doc URL. Type. File Information.
: Issue Date Doc URL. Type. File Information.") Title Pleomorphic ventricular tachycardia originating from Author(s)Yokoshiki, Hisashi; Mitsuyama, Hirofumi; Watanabe, M CitationJournal of Electrocardiology, 43(5): 452-458 Issue Date 2010-09 Doc URL
Title Pleomorphic ventricular tachycardia originating from Author(s)Yokoshiki, Hisashi; Mitsuyama, Hirofumi; Watanabe, M CitationJournal of Electrocardiology, 43(5): 452-458 Issue Date 2010-09 Doc URL
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,500 108,000 1.7 M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,500 108,000 1.7 M Open access books available International authors and editors Downloads Our
Ablation of Posteroseptal APs - Tips/Tricks
 blation of Posteroseptal Ps - Tips/Tricks California eart Rhythm Symposium San Francisco September 7,202 Warren (Sonny) Jackman eart Rhythm nstitute University of Oklahoma ealth Sciences Center Oklahoma
blation of Posteroseptal Ps - Tips/Tricks California eart Rhythm Symposium San Francisco September 7,202 Warren (Sonny) Jackman eart Rhythm nstitute University of Oklahoma ealth Sciences Center Oklahoma
Atrioventricular (AV) Nodal Reentry Associated with 2:1 Infra-His Conduction Block during Tachycardia in a Patient with AV Nodal Triple Pathways
 Nodal Reentry Associated with 2:1 Infra-His Conduction Block during Tachycardia in a Patient with AV Nodal Triple Pathways") Atrioventricular (AV) Nodal Reentry Associated with 2:1 Infra-His Conduction Block during Tachycardia in a Patient with AV Nodal Triple Pathways Haruhiko ABE, M.D., Takashi OHKITA, M.D., Masasuke FUJITA,
Atrioventricular (AV) Nodal Reentry Associated with 2:1 Infra-His Conduction Block during Tachycardia in a Patient with AV Nodal Triple Pathways Haruhiko ABE, M.D., Takashi OHKITA, M.D., Masasuke FUJITA,
THE HEART. A. The Pericardium - a double sac of serous membrane surrounding the heart
 THE HEART I. Size and Location: A. Fist-size weighing less than a pound (250 to 350 grams). B. Located in the mediastinum between the 2 nd rib and the 5 th intercostal space. 1. Tipped to the left, resting
THE HEART I. Size and Location: A. Fist-size weighing less than a pound (250 to 350 grams). B. Located in the mediastinum between the 2 nd rib and the 5 th intercostal space. 1. Tipped to the left, resting
Pre-excited tachycardia: Atrial tachycardia with a bystander left lateral accessory pathway
 Pre-excited tachycardia: Atrial tachycardia with a bystander left lateral accessory pathway Jeffrey Munro, DO, Win-Kuang Shen, MD, FHRS, Komandoor Srivathsan, MD From the Department of Cardiovascular Disease,
Pre-excited tachycardia: Atrial tachycardia with a bystander left lateral accessory pathway Jeffrey Munro, DO, Win-Kuang Shen, MD, FHRS, Komandoor Srivathsan, MD From the Department of Cardiovascular Disease,
Differentiating Slow Fast Atrioventricular Nodal Reentry Tachycardia From Atrioventrcular..
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 16, Issue 1 Ver. X (January. 2017), PP 69-77 www.iosrjournals.org Differentiating Slow Fast Atrioventricular
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 16, Issue 1 Ver. X (January. 2017), PP 69-77 www.iosrjournals.org Differentiating Slow Fast Atrioventricular
Electrical disconnection of pulmonary vein (PV) myocardium
 myocardium") Left Atrial Appendage Activity Masquerading as Pulmonary Vein Potentials Dipen Shah, MD; Michel Haissaguerre, MD; Pierre Jais, MD; Meleze Hocini, MD; Teiichi Yamane, MD; Laurent Macle, MD; Kee Joon Choi,
Left Atrial Appendage Activity Masquerading as Pulmonary Vein Potentials Dipen Shah, MD; Michel Haissaguerre, MD; Pierre Jais, MD; Meleze Hocini, MD; Teiichi Yamane, MD; Laurent Macle, MD; Kee Joon Choi,
By the end of this lecture, you will be able to: Understand the 12 lead ECG in relation to the coronary circulation and myocardium Perform an ECG
 By the end of this lecture, you will be able to: Understand the 12 lead ECG in relation to the coronary circulation and myocardium Perform an ECG recording Identify the ECG changes that occur in the presence
By the end of this lecture, you will be able to: Understand the 12 lead ECG in relation to the coronary circulation and myocardium Perform an ECG recording Identify the ECG changes that occur in the presence
EPS Case presentation Looks like VT but it isn t!
 EPS Case presentation Looks like VT but it isn t! E. Συμεωνίδου, MD, PhD Β Παν Καρδιολογική κλινική, Νοσ Aττικόν Σεμινάρια Ομάδων Εργασίας ΕΚΕ 2016 Ιωάννινα Disclosures I have no conflict of interest to
EPS Case presentation Looks like VT but it isn t! E. Συμεωνίδου, MD, PhD Β Παν Καρδιολογική κλινική, Νοσ Aττικόν Σεμινάρια Ομάδων Εργασίας ΕΚΕ 2016 Ιωάννινα Disclosures I have no conflict of interest to
CARDIOINSIGHT TM NONINVASIVE 3D MAPPING SYSTEM CLINICAL EVIDENCE SUMMARY
 CARDIOINSIGHT TM NONINVASIVE 3D MAPPING SYSTEM CLINICAL EVIDENCE SUMMARY April 2017 SUPPORTING EVIDENCE RHYTHM AF VT PUBLICATIONS Driver Domains in Persistent Atrial Fibrillation (Haissaiguerre, et al)
CARDIOINSIGHT TM NONINVASIVE 3D MAPPING SYSTEM CLINICAL EVIDENCE SUMMARY April 2017 SUPPORTING EVIDENCE RHYTHM AF VT PUBLICATIONS Driver Domains in Persistent Atrial Fibrillation (Haissaiguerre, et al)
How to ablate typical atrial flutter
 Europace (1999) 1, 151 155 HOW TO... SERIES How to ablate typical atrial flutter A. Takahashi, D. C. Shah, P. Jaïs and M. Haïssaguerre Electrophysiologie Cardiaque, Hopital Cardiologique du Haut-Lévêque,
Europace (1999) 1, 151 155 HOW TO... SERIES How to ablate typical atrial flutter A. Takahashi, D. C. Shah, P. Jaïs and M. Haïssaguerre Electrophysiologie Cardiaque, Hopital Cardiologique du Haut-Lévêque,
How to Ablate Atrial Tachycardia Mechanisms and Approach. DrJo Jo Hai
 How to Ablate Atrial Tachycardia Mechanisms and Approach DrJo Jo Hai Contents Mechanisms of focal atrial tachycardia Various mapping techniques Detailed discussion on activation sequence mapping and entrainment
How to Ablate Atrial Tachycardia Mechanisms and Approach DrJo Jo Hai Contents Mechanisms of focal atrial tachycardia Various mapping techniques Detailed discussion on activation sequence mapping and entrainment
Case Report What Next After Failed Septal Ventricular Tachycardia Ablation?
 www.ipej.org 180 Case Report What Next After Failed Septal Ventricular Tachycardia Ablation? Laurent Roten, MD 1, Nicolas Derval, MD 1, Patrizio Pascale, MD 1, Pierre Jais, MD 1, Pierre Coste, MD 2, Frederic
www.ipej.org 180 Case Report What Next After Failed Septal Ventricular Tachycardia Ablation? Laurent Roten, MD 1, Nicolas Derval, MD 1, Patrizio Pascale, MD 1, Pierre Jais, MD 1, Pierre Coste, MD 2, Frederic
Ji-Eun Ban, MD, Sang-Weon Park, MD, Hyun-Soo Lee, MPH, Jong-Il Choi, MD, and Young-Hoon Kim, MD
 Case Report Print SSN 1738-5520 On-line SSN 1738-5555 Korean Circulation Journal Swallowing-nduced Atrial Tachyarrhythmias Successfully Ablated at the Left Posterior nteratrial Septum in Patient with Wolff-Parkinson-White
Case Report Print SSN 1738-5520 On-line SSN 1738-5555 Korean Circulation Journal Swallowing-nduced Atrial Tachyarrhythmias Successfully Ablated at the Left Posterior nteratrial Septum in Patient with Wolff-Parkinson-White
Supraventricular Tachycardia (SVT)
") Supraventricular Tachycardia (SVT) Daniel Frisch, MD Cardiology Division, Electrophysiology Section Thomas Jefferson University Hospital daniel.frisch@jefferson.edu Short RP Are these the Mid same RP tachycardias?
Supraventricular Tachycardia (SVT) Daniel Frisch, MD Cardiology Division, Electrophysiology Section Thomas Jefferson University Hospital daniel.frisch@jefferson.edu Short RP Are these the Mid same RP tachycardias?
Catheter Ablation of Atrial Tachycardia Originating from the Tip of Right Atrial Appendage
 Case Report Catheter Ablation of Atrial Tachycardia Originating from the Tip of Right Atrial Appendage Masaru Inoue MD, Takao Matsubara MD, Toshihiko Yasuda MD, Kenji Miwa MD, Tadatsugu Gamou MD, Hounin
Case Report Catheter Ablation of Atrial Tachycardia Originating from the Tip of Right Atrial Appendage Masaru Inoue MD, Takao Matsubara MD, Toshihiko Yasuda MD, Kenji Miwa MD, Tadatsugu Gamou MD, Hounin
ECG QUIZ Luc DE ROY Brussels Belgium Disclosure in relation to this topic: none
 ECG QUIZ Luc DE ROY Brussels Belgium Disclosure in relation to this topic: none TEST EXAMPLE What is the colour of this rectangle? 1. Blue? 2. Red? 3. Purple? 4. Green? 5. Yellow? 6. 1 and 3? 7. Any of
ECG QUIZ Luc DE ROY Brussels Belgium Disclosure in relation to this topic: none TEST EXAMPLE What is the colour of this rectangle? 1. Blue? 2. Red? 3. Purple? 4. Green? 5. Yellow? 6. 1 and 3? 7. Any of
The Electrocardiogram
 The Electrocardiogram Chapters 11 and 13 AUTUMN WEDAN AND NATASHA MCDOUGAL The Normal Electrocardiogram P-wave Generated when the atria depolarizes QRS-Complex Ventricles depolarizing before a contraction
The Electrocardiogram Chapters 11 and 13 AUTUMN WEDAN AND NATASHA MCDOUGAL The Normal Electrocardiogram P-wave Generated when the atria depolarizes QRS-Complex Ventricles depolarizing before a contraction
TACHYARRHYTHMIAs. Pawel Balsam, MD, PhD
 TACHYARRHYTHMIAs Pawel Balsam, MD, PhD SupraVentricular Tachycardia Atrial Extra Systole Sinus Tachycardia Focal A. Tachycardia AVRT AVNRT Atrial Flutter Atrial Fibrillation Ventricular Tachycardia Ventricular
TACHYARRHYTHMIAs Pawel Balsam, MD, PhD SupraVentricular Tachycardia Atrial Extra Systole Sinus Tachycardia Focal A. Tachycardia AVRT AVNRT Atrial Flutter Atrial Fibrillation Ventricular Tachycardia Ventricular
Blood supply of the Heart & Conduction System. Dr. Nabil Khouri
 Blood supply of the Heart & Conduction System Dr. Nabil Khouri Arterial supply of Heart Right coronary artery Left coronary artery 3 Introduction: Coronary arteries - VASAVASORUM arising from aortic sinuses
Blood supply of the Heart & Conduction System Dr. Nabil Khouri Arterial supply of Heart Right coronary artery Left coronary artery 3 Introduction: Coronary arteries - VASAVASORUM arising from aortic sinuses
Circulation. Circulation = is a process used for the transport of oxygen, carbon! dioxide, nutrients and wastes through-out the body
 Circulation Circulation = is a process used for the transport of oxygen, carbon! dioxide, nutrients and wastes through-out the body Heart = muscular organ about the size of your fist which pumps blood.
Circulation Circulation = is a process used for the transport of oxygen, carbon! dioxide, nutrients and wastes through-out the body Heart = muscular organ about the size of your fist which pumps blood.
ECG ABNORMALITIES D R. T AM A R A AL Q U D AH
 ECG ABNORMALITIES D R. T AM A R A AL Q U D AH When we interpret an ECG we compare it instantaneously with the normal ECG and normal variants stored in our memory; these memories are stored visually in
ECG ABNORMALITIES D R. T AM A R A AL Q U D AH When we interpret an ECG we compare it instantaneously with the normal ECG and normal variants stored in our memory; these memories are stored visually in
Catheter ablation of atrial macro re-entrant Tachycardia - How to use 3D entrainment mapping -
 Catheter ablation of atrial macro re-entrant Tachycardia - How to use 3D entrainment mapping - M. Esato, Y. Chun, G. Hindricks Kyoto Ijinkai Takeda Hosptial, Department of Arrhythmia, Japan Kyoto Koseikai
Catheter ablation of atrial macro re-entrant Tachycardia - How to use 3D entrainment mapping - M. Esato, Y. Chun, G. Hindricks Kyoto Ijinkai Takeda Hosptial, Department of Arrhythmia, Japan Kyoto Koseikai
The Heart. Happy Friday! #takeoutyournotes #testnotgradedyet
 The Heart Happy Friday! #takeoutyournotes #testnotgradedyet Introduction Cardiovascular system distributes blood Pump (heart) Distribution areas (capillaries) Heart has 4 compartments 2 receive blood (atria)
The Heart Happy Friday! #takeoutyournotes #testnotgradedyet Introduction Cardiovascular system distributes blood Pump (heart) Distribution areas (capillaries) Heart has 4 compartments 2 receive blood (atria)
Characteristics of systolic and diastolic potentials recorded in the left interventricular septum in verapamil-sensitive left ventricular tachycardia
 CASE REPORT Cardiology Journal 2012, Vol. 19, No. 4, pp. 418 423 10.5603/CJ.2012.0075 Copyright 2012 Via Medica ISSN 1897 5593 Characteristics of systolic and diastolic potentials recorded in the left
CASE REPORT Cardiology Journal 2012, Vol. 19, No. 4, pp. 418 423 10.5603/CJ.2012.0075 Copyright 2012 Via Medica ISSN 1897 5593 Characteristics of systolic and diastolic potentials recorded in the left
Adenosine-Sensitive Focal Reentrant Atrial Tachycardia Originating From the Mitral Annulus Aorta Junction
 Case Report Adenosine-Sensitive Focal Reentrant Atrial Tachycardia Originating From the Mitral Annulus Aorta Junction tsuro Morishima MD, Takahito Sone MD, Hideyuki Tsuboi MD, Hiroaki Mukawa MD, Michitaka
Case Report Adenosine-Sensitive Focal Reentrant Atrial Tachycardia Originating From the Mitral Annulus Aorta Junction tsuro Morishima MD, Takahito Sone MD, Hideyuki Tsuboi MD, Hiroaki Mukawa MD, Michitaka
ECG CONVENTIONS AND INTERVALS
 1 ECG Waveforms and Intervals ECG waveforms labeled alphabetically P wave== represents atrial depolarization QRS complex=ventricular depolarization ST-T-U complex (ST segment, T wave, and U wave)== V repolarization.
1 ECG Waveforms and Intervals ECG waveforms labeled alphabetically P wave== represents atrial depolarization QRS complex=ventricular depolarization ST-T-U complex (ST segment, T wave, and U wave)== V repolarization.
Case Report Coexistence of Atrioventricular Nodal Reentrant Tachycardia and Idiopathic Left Ventricular Outflow-Tract Tachycardia
 www.ipej.org 149 Case Report Coexistence of Atrioventricular Nodal Reentrant Tachycardia and Idiopathic Left Ventricular Outflow-Tract Tachycardia Majid Haghjoo, M.D, Arash Arya, M.D, Mohammadreza Dehghani,
www.ipej.org 149 Case Report Coexistence of Atrioventricular Nodal Reentrant Tachycardia and Idiopathic Left Ventricular Outflow-Tract Tachycardia Majid Haghjoo, M.D, Arash Arya, M.D, Mohammadreza Dehghani,
December 2018 Tracings
 Tracings Tracing 1 Tracing 4 Tracing 1 Answer Tracing 4 Answer Tracing 2 Tracing 5 Tracing 2 Answer Tracing 5 Answer Tracing 3 Tracing 6 Tracing 3 Answer Tracing 6 Answer Questions? Contact Dr. Nelson
Tracings Tracing 1 Tracing 4 Tracing 1 Answer Tracing 4 Answer Tracing 2 Tracing 5 Tracing 2 Answer Tracing 5 Answer Tracing 3 Tracing 6 Tracing 3 Answer Tracing 6 Answer Questions? Contact Dr. Nelson
Kent Bundles in the Anterior Septal Space Will C. Sealy, M.D.
 Kent Bundles in the Anterior Septal Space Will C. Sealy, M.D. ABSTRACT Kent bundles in the anterior septal area of the heart occupy a region of complex morphology. In this study, the anatomical characteristics
Kent Bundles in the Anterior Septal Space Will C. Sealy, M.D. ABSTRACT Kent bundles in the anterior septal area of the heart occupy a region of complex morphology. In this study, the anatomical characteristics
12 LEAD EKG BASICS. By: Steven Jones, NREMT P CLEMC
 12 LEAD EKG BASICS By: Steven Jones, NREMT P CLEMC ECG Review Waves and Intervals P wave: the sequential activation (depolarization) of the right and left atria QRS complex: right and left ventricular
12 LEAD EKG BASICS By: Steven Jones, NREMT P CLEMC ECG Review Waves and Intervals P wave: the sequential activation (depolarization) of the right and left atria QRS complex: right and left ventricular
Cardiovascular System
 Cardiovascular System The Heart Cardiovascular System The Heart Overview What does the heart do? By timed muscular contractions creates pressure gradients blood moves then from high pressure to low pressure
Cardiovascular System The Heart Cardiovascular System The Heart Overview What does the heart do? By timed muscular contractions creates pressure gradients blood moves then from high pressure to low pressure
Ventricular Arrhythmias
 Presenting your most challenging cases Venice Arrhythmias Ventricular Arrhythmias Gioia Turitto, MD Presenter Disclosure Information A questionable indication for CRT-D in a patient with VT after successful
Presenting your most challenging cases Venice Arrhythmias Ventricular Arrhythmias Gioia Turitto, MD Presenter Disclosure Information A questionable indication for CRT-D in a patient with VT after successful
PERMANENT PACEMAKERS AND IMPLANTABLE DEFIBRILLATORS Considerations for intensivists
 PERMANENT PACEMAKERS AND IMPLANTABLE DEFIBRILLATORS Considerations for intensivists Craig A. McPherson, MD, FACC Associate Professor of Medicine Constantine Manthous, MD, FACP, FCCP Associate Clinical
PERMANENT PACEMAKERS AND IMPLANTABLE DEFIBRILLATORS Considerations for intensivists Craig A. McPherson, MD, FACC Associate Professor of Medicine Constantine Manthous, MD, FACP, FCCP Associate Clinical
Basic electrocardiography reading. R3 lee wei-chieh
 Basic electrocardiography reading R3 lee wei-chieh The Normal Conduction System Lead Placement avf Limb Leads Precordial Leads Interpretation Rate Rhythm Interval Axis Chamber abnormality QRST change What
Basic electrocardiography reading R3 lee wei-chieh The Normal Conduction System Lead Placement avf Limb Leads Precordial Leads Interpretation Rate Rhythm Interval Axis Chamber abnormality QRST change What
Reentrant Ventricular Tachycardia Originating in the Right Ventricular Outflow Tract
 Circ J 2008; 72: 855 860 Reentrant Ventricular Tachycardia Originating in the Right Ventricular Outflow Tract Slow Conduction Identified by Right Coronary Artery Ostium Pacing Emi Nakano, MD; Tomoo Harada,
Circ J 2008; 72: 855 860 Reentrant Ventricular Tachycardia Originating in the Right Ventricular Outflow Tract Slow Conduction Identified by Right Coronary Artery Ostium Pacing Emi Nakano, MD; Tomoo Harada,
the Cardiovascular System I
 the Cardiovascular System I By: Dr. Nabil A Khouri MD, MsC, Ph.D MEDIASTINUM 1. Superior Mediastinum 2. inferior Mediastinum Anterior mediastinum. Middle mediastinum. Posterior mediastinum Anatomy of
the Cardiovascular System I By: Dr. Nabil A Khouri MD, MsC, Ph.D MEDIASTINUM 1. Superior Mediastinum 2. inferior Mediastinum Anterior mediastinum. Middle mediastinum. Posterior mediastinum Anatomy of
Asymptomatic patient with WPW
 Asymptomatic patient with WPW Dimosthenis Avramidis, MD. Arrythmiologist Mitera Children s Hospital Athens Greece Scientific Associate 1st Cardiology Dpt Evangelismos Hospital Athens Greece Preexcitation
Asymptomatic patient with WPW Dimosthenis Avramidis, MD. Arrythmiologist Mitera Children s Hospital Athens Greece Scientific Associate 1st Cardiology Dpt Evangelismos Hospital Athens Greece Preexcitation
ECG Basics Sonia Samtani 7/2017 UCI Resident Lecture Series
 ECG Basics Sonia Samtani 7/2017 UCI Resident Lecture Series Agenda I. Introduction II.The Conduction System III.ECG Basics IV.Cardiac Emergencies V.Summary The Conduction System Lead Placement avf Precordial
ECG Basics Sonia Samtani 7/2017 UCI Resident Lecture Series Agenda I. Introduction II.The Conduction System III.ECG Basics IV.Cardiac Emergencies V.Summary The Conduction System Lead Placement avf Precordial
Adenosine Mapping for Adenosine-Dependent Accessory Pathway Ablation
 Adenosine Mapping for Adenosine-Dependent Accessory Pathway Ablation MARTIN J. LAPAGE, M.D., M.S.,* MICHAEL J. WALSH, M.D., JOHN H. REED, M.D., M.P.H., and J. PHILIP SAUL, M.D. From the *Department of
Adenosine Mapping for Adenosine-Dependent Accessory Pathway Ablation MARTIN J. LAPAGE, M.D., M.S.,* MICHAEL J. WALSH, M.D., JOHN H. REED, M.D., M.P.H., and J. PHILIP SAUL, M.D. From the *Department of
Lab Activity 23. Cardiac Anatomy. Portland Community College BI 232
 Lab Activity 23 Cardiac Anatomy Portland Community College BI 232 Cardiac Muscle Histology Branching cells Intercalated disc: contains many gap junctions connecting the adjacent cell cytoplasm, creates
Lab Activity 23 Cardiac Anatomy Portland Community College BI 232 Cardiac Muscle Histology Branching cells Intercalated disc: contains many gap junctions connecting the adjacent cell cytoplasm, creates
Catheter Ablation of a Complex Atrial Tachycardia after Surgical Repair of Tetralogy of Fallot Guided by Combined Noncontact and Contact Mapping
 J Arrhythmia Vol 26 No 1 2010 Case Report Catheter Ablation of a Complex Atrial Tachycardia after Surgical Repair of Tetralogy of Fallot Guided by Combined Noncontact and Contact Mapping Eitaro Fujii MD,
J Arrhythmia Vol 26 No 1 2010 Case Report Catheter Ablation of a Complex Atrial Tachycardia after Surgical Repair of Tetralogy of Fallot Guided by Combined Noncontact and Contact Mapping Eitaro Fujii MD,
Emergency Medical Training Services Emergency Medical Technician Paramedic Program Outlines Outline Topic: WPW Revised: 11/2013
 Emergency Medical Training Services Emergency Medical Technician Paramedic Program Outlines Outline Topic: WPW Revised: 11/2013 Wolff-Parkinson-White syndrome (WPW) is a syndrome of pre-excitation of the
Emergency Medical Training Services Emergency Medical Technician Paramedic Program Outlines Outline Topic: WPW Revised: 11/2013 Wolff-Parkinson-White syndrome (WPW) is a syndrome of pre-excitation of the
Rakesh Yadav MD, DM, Sharad Chandra MD, DM, Nitish Naik MD, DM, Rajnish Juneja MD, DM
 www.ipej.org 278 Case Report Radiofrequency Catheter Ablation Of Atrioventricular Nodal Reentrant Tachycardia Associated With Anomalous Drainage Of Both Superior Vena Cava Into Coronary Sinus Rakesh Yadav
www.ipej.org 278 Case Report Radiofrequency Catheter Ablation Of Atrioventricular Nodal Reentrant Tachycardia Associated With Anomalous Drainage Of Both Superior Vena Cava Into Coronary Sinus Rakesh Yadav
Journal of the American College of Cardiology Vol. 45, No. 9, by the American College of Cardiology Foundation ISSN /05/$30.
 Journal of the American College of Cardiology Vol. 45, No. 9, 2005 2005 by the American College of Cardiology Foundation ISSN 0735-1097/05/$30.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2005.01.042
Journal of the American College of Cardiology Vol. 45, No. 9, 2005 2005 by the American College of Cardiology Foundation ISSN 0735-1097/05/$30.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2005.01.042
Kadlec Regional Medical Center Cardiac Electrophysiology
 Definition of electrophysiology study and ablation Kadlec Regional Medical Center Cardiac Electrophysiology Electrophysiology Study and Ablation An electrophysiology, or EP, study is a test of the heart
Definition of electrophysiology study and ablation Kadlec Regional Medical Center Cardiac Electrophysiology Electrophysiology Study and Ablation An electrophysiology, or EP, study is a test of the heart
Ablation Lesion Assessment
 HRC 2016 Ablation Lesion Assessment The creation of effective and permanent lesions Ian Wright Imperial College Healthcare Wed 09:00-09:30 Hall 11 Objective Examine the role of existing strategies and
HRC 2016 Ablation Lesion Assessment The creation of effective and permanent lesions Ian Wright Imperial College Healthcare Wed 09:00-09:30 Hall 11 Objective Examine the role of existing strategies and
Topographic Distribution of Focal Left Atrial Tachycardias Defined by Electrocardiographic and Electrophysiological Data
 Circ J 2005; 69: 205 210 Topographic Distribution of Focal Left Atrial Tachycardias Defined by Electrocardiographic and Electrophysiological Data Hitoshi Hachiya, MD; Sabine Ernst, MD; Feifan Ouyang, MD;
Circ J 2005; 69: 205 210 Topographic Distribution of Focal Left Atrial Tachycardias Defined by Electrocardiographic and Electrophysiological Data Hitoshi Hachiya, MD; Sabine Ernst, MD; Feifan Ouyang, MD;