My Bloody Talk. Dr Ben Turner MBBS, FANZCA, FCICM The Royal Children s Hospital, Melbourne
|
|
|
- Eric Hunt
- 5 years ago
- Views:
Transcription
1 My Bloody Talk Dr Ben Turner MBBS, FANZCA, FCICM The Royal Children s Hospital, Melbourne

2 Disclosures No conflicts of interest Interest in conflict
3 Blood transfusion Massive transfusion definitions Transfusion triggers Massive blood loss complications Massive transfusion protocols Complications of transfusion
4 Massive Transfusion Trauma Major surgery GI bleeding Birth trauma Bleeding diatheses Vascular malformations Feto-maternal haemorrhage
5 Signs that you may need to Transfuse How s it going up your end? Has this patient got a crossmatch? If you can no longer hear the music over the suckers Shit shit shit..
6 Transfusion Triggers Lower limit of Hb at which D02 becomes critical is not defined Theoretical level in adults is 2.5g/dL Validated in animals Healthy volunteers diluted to 4-5g/dL In Jehovah s Witness adults morbidity and mortality increase with anaemia but patients can survive with Hb 3g/dL. (Carson, 2002) Odds of death increase 2.5 times for every 1g/dL Hb is <8g/dL (Carson, 2002)
7 Massive Transfusion definition Paediatrics is different from adult medicine Both absolute and relative blood volumes differ in different sized and aged children ml/kg in preterm infant 60 ml/kg in female adolescent
8 Massive Transfusion definition Yaser et al, 2013 >50% TBV in <3hrs >100% TBV in 24hrs Transfusion for ongoing bleeding of >10% TBV in 10min
9 Massive Transfusion definition Does it matter? When you have to give enough blood that the transfusion may have physiologic consequences. STOP, LOOK, LISTEN, THINK
10 Physiologic complications of massive haemorrhage CVS Neurological Renal
11 Critical Triad Hypothermia Acidosis Coagulopathy
12 Assessment Temperature Haemoglobin Platelet count Coagulation screen INR/PT APTT Fibrinogen Acid-base status Ionised Ca++
13 Assessment Values indicative of critical physiological derangement T<35 C ph<7.2, base excess>-6, lactate >4mmol/l Ionised Ca++ <1.1mmol/l INR>1.5 APTT>1.5 x normal Fibrinogen <1.0g/l
14 Hypothermia Aetiology is multifactorial Trauma patients are frequently hypothermic on arrival at hospital and are exposed during assessment Surgical patients suffer exposure and effects of anaesthesia Most blood products are stored between 1-6 C Room temperature fluids are hypothermic
15 Hypothermia For each 1 C drop in temperature coagulation factor activity decreases by 10% Patients <34 C will be clinically coagulopathic Hypothermia causes platelet pooling in spleen <34 C platelet adhesion and aggregation is impaired
16 Acidosis Tissue hypoperfusion Decreased haemoglobin and O2 carriage Reduced cardiac output due to reduced pre-load Prolongs clotting time by impairing enzyme activity Reduces fibrinogen levels Reduces platelet count
17 Acidosis Treat the cause unless ph<7.2 NaHCO3 1ml/kg
18 Coagulopathy 25% of trauma patients are coagulopathic on arrival to hospital Systemic hypoperfusion has a dose dependent association with coagulopathy as measured by PT/APTT
19 Coagulopathy Shock increases thrombomodulin results in reduced thrombin, factors Va and VIIIa deactivates PAI-1, promoting fibrinolysis Complement cascade activation affects coagulation ñ tissue plasminogen activator and ò thrombin activatable fibrinolysis inhibitor lead to an increase in fibrinolysis
20 Management Most information comes from adult trauma studies Trauma differs in paediatrics Less penetrating trauma and more crush injuries
21 Guidelines 2012 National Blood Authority released: Patient Blood Guidelines:Module 1 Critical Bleeding/Massive Transfusion Endorsed by all major medical colleges in Australia Evidence based review of the literature using NHMRC grades A-D
22 Patient Blood Guidelines:Module 1 Critical Bleeding/Massive Transfusion Recommendations 2 Practice points 10 MTP protocol template
23 Recommendations Recommendation 1 Institutions develop an MTP that includes the dose, timing, and ratio of blood component therapy for use in trauma patients with, or at risk of, critical bleeding requiring massive transfusion (Grade C) Grade C body of evidence provides some support
24 Recommendations Recommendation 2 The routine use of rfviia in trauma patients with critical bleeding requiring massive transfusion is not recommended because of its lack of effect on mortality (grade B) and variable effect on morbidity (grade C) Grade B body of evidence can be trusted to guide practice in most situations
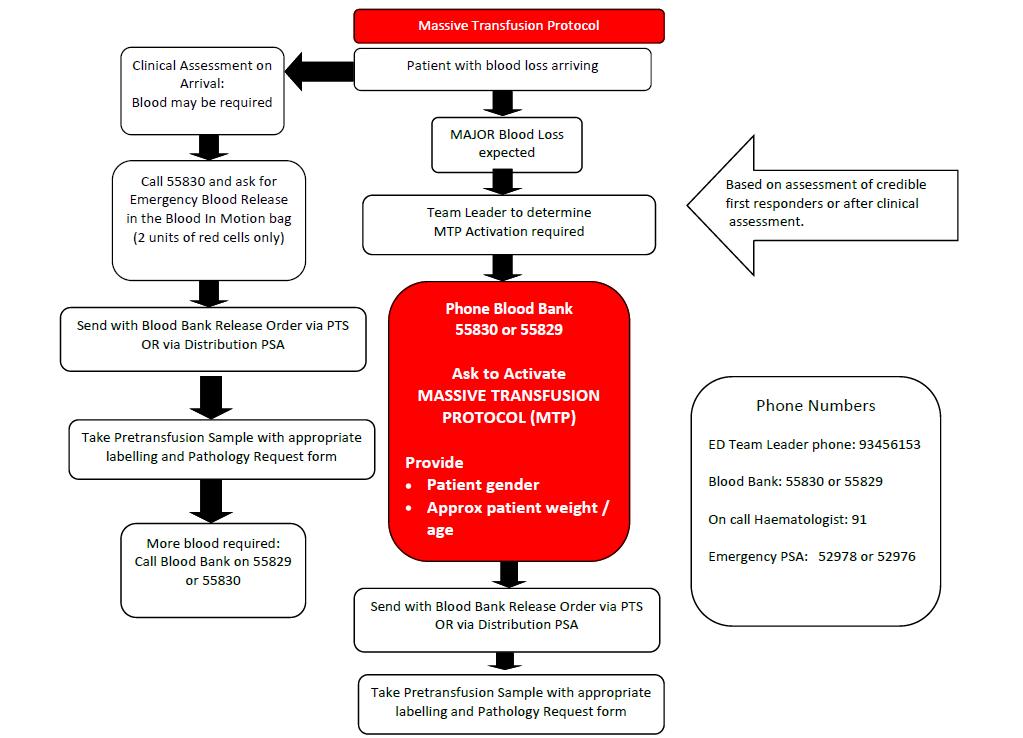
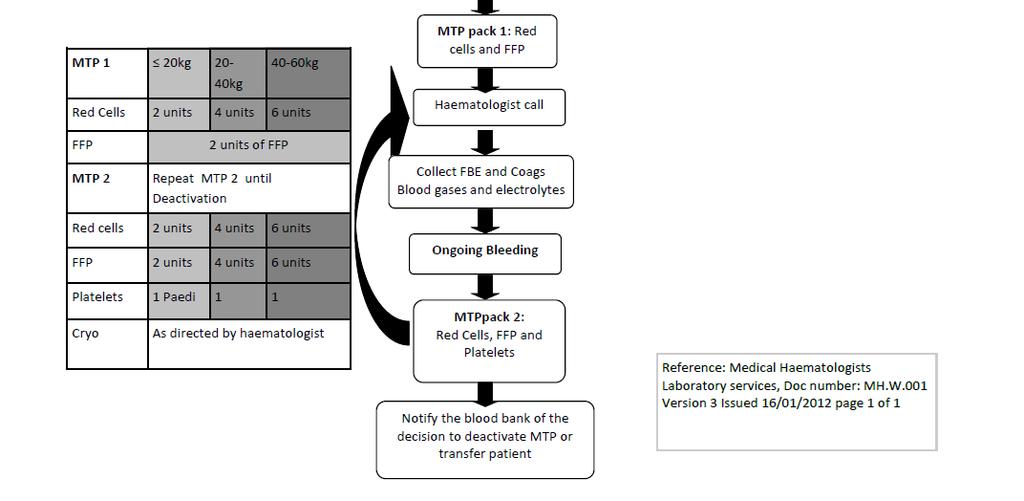
25 Massive Transfusion Protocol A system to streamline the availability and limit complications of massive transfusion in a critically bleeding child Provides clear guidelines for Trauma doctors Trauma nurses Haemotologist Laboratory staff Distribution orderlies
26 Massive Transfusion Protocol Activates a response in the blood bank Increase staff numbers Commence thawing frozen components Order urgent blood from the Blood Service
27

28
29 Massive Transfusion Protocol - template Local adaptation Multidisciplinary Incorporate recommendations and practice points Take into account local resources Provide details on how components will be delivered to the correct patient and location
30 Special circumstances Warfarin Add vit K, prothrombinex/ffp Head injury Platelet count >100 x 10 9 /L
31 Practice Point 4 In patients with critical bleeding requiring massive transfusion insufficient evidence was identified to support or refute the use of specific ratios of RBCs to blood components
32 Practice Point 10 Suggested doses of blood components are: FFP15ml/kg Platelets 1 adult therapeutic dose Cryoprecipitate 3-4g
33 Practice Point 8&9 rfviia MTP should include advice on the administration of rfviia May be considered if: Patient is salvagable Failed surgical or radiological measures Adequate blood component replacement ph>7.2, Temperature > 34 o C Initial dose 90mcg/kg is reasonable
34 Tranexamic acid CRASH II The Lancet, ,000 trauma patients with significant haemorrhage 274 hospitals, 40 countries Treated within 8 hrs of injury Tranexamic acid 1g over 10min, 1g over 8hrs
35 Tranexamic acid Significant reduction in all cause mortality RR % CI Lower risk of death secondary to bleeding RR % CI No increase in vaso occlusive disease in TXA group More effective if given within 3 hours
36 Transfusion Associated Complications Transfusion reactions AHTR, FNHTR (allergic) Immunological complications TRALI, TRIM, TA-GVHD, PTP
37 Transfusion Associated Complications Metabolic complications ê Ca ++, ê Mg ++, é K +, ê K +, metabolic alkalosis, impaired glucose homeostasis, Acidosis, Hypothermia Coagulopathy Infections TACO TANEC Air embolism
38 Conclusion Patients requiring massive transfusion may have significant metabolic derangement Prevent and treat the triad Acidosis Hypothermia Coagulopathy Develop MTP Remember blood transfusion has its own complications
Transfusion Requirements and Management in Trauma RACHEL JACK
 Transfusion Requirements and Management in Trauma RACHEL JACK Overview Haemostatic resuscitation Massive Transfusion Protocol Overview of NBA research guidelines Haemostatic resuscitation Permissive hypotension
Transfusion Requirements and Management in Trauma RACHEL JACK Overview Haemostatic resuscitation Massive Transfusion Protocol Overview of NBA research guidelines Haemostatic resuscitation Permissive hypotension
MANAGEMENT OF COAGULOPATHY AFTER TRAUMA OR MAJOR SURGERY
 MANAGEMENT OF COAGULOPATHY AFTER TRAUMA OR MAJOR SURGERY 19th ANNUAL CONTROVERSIES AND PROBLEMS IN SURGERY Thabo Mothabeng General Surgery: 1 Military Hospital HH Stone et al. Ann Surg. May 1983; 197(5):
MANAGEMENT OF COAGULOPATHY AFTER TRAUMA OR MAJOR SURGERY 19th ANNUAL CONTROVERSIES AND PROBLEMS IN SURGERY Thabo Mothabeng General Surgery: 1 Military Hospital HH Stone et al. Ann Surg. May 1983; 197(5):
MASSIVE TRANSFUSION DR.K.HITESH KUMAR FINAL YEAR PG DEPT. OF TRANSFUSION MEDICINE
 MASSIVE TRANSFUSION DR.K.HITESH KUMAR FINAL YEAR PG DEPT. OF TRANSFUSION MEDICINE CONTENTS Definition Indications Transfusion trigger Massive transfusion protocol Complications DEFINITION Massive transfusion:
MASSIVE TRANSFUSION DR.K.HITESH KUMAR FINAL YEAR PG DEPT. OF TRANSFUSION MEDICINE CONTENTS Definition Indications Transfusion trigger Massive transfusion protocol Complications DEFINITION Massive transfusion:
Bleeding, Coagulopathy, and Thrombosis in the Injured Patient
 Bleeding, Coagulopathy, and Thrombosis in the Injured Patient June 7, 2008 Kristan Staudenmayer, MD Trauma Fellow UCSF/SFGH Trauma deaths Sauaia A, et al. J Trauma. Feb 1995;38(2):185 Coagulopathy is Multi-factorial
Bleeding, Coagulopathy, and Thrombosis in the Injured Patient June 7, 2008 Kristan Staudenmayer, MD Trauma Fellow UCSF/SFGH Trauma deaths Sauaia A, et al. J Trauma. Feb 1995;38(2):185 Coagulopathy is Multi-factorial
Transfusion in major bleeding: new insights. Gert Poortmans
 Transfusion in major bleeding: new insights Gert Poortmans Trauma Cardiac Surgery Major Surgery with ongoing blood loss Burn Surgery Lethal Triad Polytransfusion: definitions Coagulation Coagulopathy of
Transfusion in major bleeding: new insights Gert Poortmans Trauma Cardiac Surgery Major Surgery with ongoing blood loss Burn Surgery Lethal Triad Polytransfusion: definitions Coagulation Coagulopathy of
Pre-hospital Administration of Blood Products (PHBP) and Tranexamic acid (TXA): Is the Jury Still Out?
 and Tranexamic acid (TXA): Is the Jury Still Out?") Pre-hospital Administration of Blood Products (PHBP) and Tranexamic acid (TXA): Is the Jury Still Out? Jessica K. Reynolds, MD Assistant Professor of Surgery University of Kentucky, Department of Trauma
Pre-hospital Administration of Blood Products (PHBP) and Tranexamic acid (TXA): Is the Jury Still Out? Jessica K. Reynolds, MD Assistant Professor of Surgery University of Kentucky, Department of Trauma
TRANSFUSION GUIDELINES FOR CARDIOTHORACIC UNIT 2006
 TRANSFUSION GUIDELINES FOR CARDIOTHORACIC UNIT 2006 CTU blood product transfusion guidelines 2006 1 Summary of guidelines RED CELLS (10-15ml/kg) This applies to ward patients / icu patients who are stable.
TRANSFUSION GUIDELINES FOR CARDIOTHORACIC UNIT 2006 CTU blood product transfusion guidelines 2006 1 Summary of guidelines RED CELLS (10-15ml/kg) This applies to ward patients / icu patients who are stable.
Massive transfusion: Recent advances, guidelines & strategies. Dr.A.Surekha Devi Head, Dept. of Transfusion Medicine Global Hospital Hyderabad
 Massive transfusion: Recent advances, guidelines & strategies Dr.A.Surekha Devi Head, Dept. of Transfusion Medicine Global Hospital Hyderabad Massive Hemorrhage Introduction Hemorrhage is a major cause
Massive transfusion: Recent advances, guidelines & strategies Dr.A.Surekha Devi Head, Dept. of Transfusion Medicine Global Hospital Hyderabad Massive Hemorrhage Introduction Hemorrhage is a major cause
Patient Blood Management Guidelines: Module 1. Critical Bleeding Massive Transfusion
 Patient Blood Management Guidelines: Module 1 Critical Bleeding Massive Transfusion National Blood Authority, 2011. With the exception of any logos and registered trademarks, and where otherwise noted,
Patient Blood Management Guidelines: Module 1 Critical Bleeding Massive Transfusion National Blood Authority, 2011. With the exception of any logos and registered trademarks, and where otherwise noted,
Major Haemorrhage Transfusion Pathway
 Major Haemorrhage Transfusion Pathway SENIOR CLINICIAN ASSESSMENT: DECLARES MAJOR HAEMORRHAGE ( Call for help ( Telephone via switchboard: Consultant or Senior Clinician Duty Anaesthetist Porters (if will
Major Haemorrhage Transfusion Pathway SENIOR CLINICIAN ASSESSMENT: DECLARES MAJOR HAEMORRHAGE ( Call for help ( Telephone via switchboard: Consultant or Senior Clinician Duty Anaesthetist Porters (if will
Major Haemorrhage Protocol. Commentary
 Hairmyres Hospital Monklands Hospital Wishaw General Hospital Major Haemorrhage Protocol Commentary N.B. There is a separate NHSL protocol for the Management of Obstetric Haemorrhage Authors Dr Tracey
Hairmyres Hospital Monklands Hospital Wishaw General Hospital Major Haemorrhage Protocol Commentary N.B. There is a separate NHSL protocol for the Management of Obstetric Haemorrhage Authors Dr Tracey
Coagulation, Haemostasis and interpretation of Coagulation tests
 Coagulation, Haemostasis and interpretation of Coagulation tests Learning Outcomes Indicate the normal ranges for routine clotting screen and explain what each measurement means Recognise how to detect
Coagulation, Haemostasis and interpretation of Coagulation tests Learning Outcomes Indicate the normal ranges for routine clotting screen and explain what each measurement means Recognise how to detect
The principle of 1:1:1 blood product use in the resuscitation of trauma victims. K. D. Boffard
 The principle of 1:1:1 blood product use in the resuscitation of trauma victims K. D. Boffard Milpark Hospital Department of Surgery University of the Witwatersrand Johannesburg, South Africa Annual Controversies
The principle of 1:1:1 blood product use in the resuscitation of trauma victims K. D. Boffard Milpark Hospital Department of Surgery University of the Witwatersrand Johannesburg, South Africa Annual Controversies
TRANSFUSIONS FIRST, DO NO HARM
 TRANSFUSIONS FIRST, DO NO HARM BECAUSE BLOOD CAN KILL 7 TRALI DEATHS SINCE 2002 WMC 5 women BECAUSE In OB you are transfusing 2 instead of 1 BECAUSE BLOOD IS A LIQUID TRANSPLANT RISKS versus BENEFITS versus
TRANSFUSIONS FIRST, DO NO HARM BECAUSE BLOOD CAN KILL 7 TRALI DEATHS SINCE 2002 WMC 5 women BECAUSE In OB you are transfusing 2 instead of 1 BECAUSE BLOOD IS A LIQUID TRANSPLANT RISKS versus BENEFITS versus
EMSS17: Bleeding patients course material
 EMSS17: Bleeding patients course material Introduction During the bleeding patients workshop at the Emergency Medicine Summer School 2017 (EMSS17) you will learn how to assess and treat bleeding patients
EMSS17: Bleeding patients course material Introduction During the bleeding patients workshop at the Emergency Medicine Summer School 2017 (EMSS17) you will learn how to assess and treat bleeding patients
Blood Management and Protocol Use in Active Bleeding
 Blood Management and Protocol Use in Active Bleeding John A. Norton, DO Assistant Professor Clinical Department of Anesthesiology The Ohio State University Wexner Medical Center Acknowledgements Stephanie
Blood Management and Protocol Use in Active Bleeding John A. Norton, DO Assistant Professor Clinical Department of Anesthesiology The Ohio State University Wexner Medical Center Acknowledgements Stephanie
the bleeding won t stop? Liane Manz RN, BScN, CNCC(c) Royal Alexandra Hospital
 Royal Alexandra Hospital") What do you do when the bleeding won t stop? Teddie Tanguay RN, MN, NP, CNCC(c) Teddie Tanguay RN, MN, NP, CNCC(c) Liane Manz RN, BScN, CNCC(c) Royal Alexandra Hospital Outline Case study Normal coagulation
What do you do when the bleeding won t stop? Teddie Tanguay RN, MN, NP, CNCC(c) Teddie Tanguay RN, MN, NP, CNCC(c) Liane Manz RN, BScN, CNCC(c) Royal Alexandra Hospital Outline Case study Normal coagulation
Financial Disclosure. Objectives 9/24/2018
 Hemorrhage and Transfusion Adjuncts in the Setting of Damage Control Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Adjunct Professor of Orthopedics and Neurosurgery, University
Hemorrhage and Transfusion Adjuncts in the Setting of Damage Control Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Adjunct Professor of Orthopedics and Neurosurgery, University
Coagulopathy: Measuring and Management. Nina A. Guzzetta, M.D. Children s Healthcare of Atlanta Emory University School of Medicine
 Coagulopathy: Measuring and Management Nina A. Guzzetta, M.D. Children s Healthcare of Atlanta Emory University School of Medicine No Financial Disclosures Objectives Define coagulopathy of trauma Define
Coagulopathy: Measuring and Management Nina A. Guzzetta, M.D. Children s Healthcare of Atlanta Emory University School of Medicine No Financial Disclosures Objectives Define coagulopathy of trauma Define
Managing Coagulopathy in Intensive Care Setting
 Managing Coagulopathy in Intensive Care Setting Dr Rock LEUNG Associate Consultant Division of Haematology, Department of Pathology & Clinical Biochemistry Queen Mary Hospital Normal Haemostasis Primary
Managing Coagulopathy in Intensive Care Setting Dr Rock LEUNG Associate Consultant Division of Haematology, Department of Pathology & Clinical Biochemistry Queen Mary Hospital Normal Haemostasis Primary
Mechanisms of Trauma Coagulopathy. Dr B M Schyma Changi General Hospital Singapore
 Mechanisms of Trauma Coagulopathy Dr B M Schyma Changi General Hospital Singapore HAEMORRHAGE A continued cause of PREVENTABLE death. 24% of trauma patients are coagulopathic on arrival 1 56% of severe
Mechanisms of Trauma Coagulopathy Dr B M Schyma Changi General Hospital Singapore HAEMORRHAGE A continued cause of PREVENTABLE death. 24% of trauma patients are coagulopathic on arrival 1 56% of severe
Blood is serious business
 Transfusion at RCH BLOOD TRANSFUSION Anthea Greenway Dept of Clinical Haematology >10000 fresh blood products per year Supports craniofacial and cardiac surgery Support bone marrow, liver transplant and
Transfusion at RCH BLOOD TRANSFUSION Anthea Greenway Dept of Clinical Haematology >10000 fresh blood products per year Supports craniofacial and cardiac surgery Support bone marrow, liver transplant and
Damage Control Resuscitation
 Damage Control Resuscitation H M Cassimjee Critical Care Specialist Department of Critical Care & Level 1 Trauma Unit Inkosi Albert Luthuli Central Hospital Damage Control Resuscitation only for DAMAGED
Damage Control Resuscitation H M Cassimjee Critical Care Specialist Department of Critical Care & Level 1 Trauma Unit Inkosi Albert Luthuli Central Hospital Damage Control Resuscitation only for DAMAGED
PEDIATRIC MASSIVE TRANSFUSION
 PEDIATRIC MASSIVE TRANSFUSION CHELSEA RUNKLE RN, BSN, CCRN, SRNA CROZER-CHESTER MEDICAL CENTER/VILLANOVA UNIVERSITY NURSE ANESTHESIA PROGRAM LEADING CAUSE OF DEATH Trauma Motor vehicle accidents, nonaccidental
PEDIATRIC MASSIVE TRANSFUSION CHELSEA RUNKLE RN, BSN, CCRN, SRNA CROZER-CHESTER MEDICAL CENTER/VILLANOVA UNIVERSITY NURSE ANESTHESIA PROGRAM LEADING CAUSE OF DEATH Trauma Motor vehicle accidents, nonaccidental
Hemostatic Resuscitation
 Hemostatic Resuscitation 30 th David Miller Trauma Symposium Bill Beck, MD Assistant Professor of Surgery Trauma, Emergency General Surgery, Critical Care Disclosures None Again. Mac user. Why I Like Trauma?
Hemostatic Resuscitation 30 th David Miller Trauma Symposium Bill Beck, MD Assistant Professor of Surgery Trauma, Emergency General Surgery, Critical Care Disclosures None Again. Mac user. Why I Like Trauma?
Intraoperative haemorrhage and haemostasis. Dr. med. Christian Quadri Capoclinica Anestesia, ORL
 Intraoperative haemorrhage and haemostasis Dr. med. Christian Quadri Capoclinica Anestesia, ORL Haemostasis is like love. Everybody talks about it, nobody understands it. JH Levy 2000 Intraoperative Haemorrhage
Intraoperative haemorrhage and haemostasis Dr. med. Christian Quadri Capoclinica Anestesia, ORL Haemostasis is like love. Everybody talks about it, nobody understands it. JH Levy 2000 Intraoperative Haemorrhage
Crossmatching and Issuing Blood Components; Indications and Effects.
 Crossmatching and Issuing Blood Components; Indications and Effects. Alison Muir Blood Transfusion, Blood Sciences, Newcastle Trust Topics Covered Taking the blood sample ABO Group Antibody Screening Compatibility
Crossmatching and Issuing Blood Components; Indications and Effects. Alison Muir Blood Transfusion, Blood Sciences, Newcastle Trust Topics Covered Taking the blood sample ABO Group Antibody Screening Compatibility
Massive Transfusion. MPQC Spring Summit April 29, Roger Belizaire MD PhD
 Massive Transfusion MPQC Spring Summit April 29, 2015 Roger Belizaire MD PhD Take home points 1. Blood is always available. Requests for massive transfusion or emergency release typically only require
Massive Transfusion MPQC Spring Summit April 29, 2015 Roger Belizaire MD PhD Take home points 1. Blood is always available. Requests for massive transfusion or emergency release typically only require
Pathophysiologie und Therapie bei Massenblutung
 Swisstransfusion Bern, 7. September 2012 Pathophysiologie und Therapie bei Massenblutung Lorenzo ALBERIO Universitätsklinik für Hämatologie und Hämatologisches Zentrallabor Coagulopathy of Trauma Haemorrhage
Swisstransfusion Bern, 7. September 2012 Pathophysiologie und Therapie bei Massenblutung Lorenzo ALBERIO Universitätsklinik für Hämatologie und Hämatologisches Zentrallabor Coagulopathy of Trauma Haemorrhage
*Corresponding author: Key words: neurotrauma, coagulopathy
 COAGULOPATHY IN NEURO TRAUMA A PROSPECTIVE ANALYSIS OF THE INCIDENCE AND CAUSES OF COAGULOPATHY IN PATIENTS WITH PURE NEURO TRAUMA AND MIXED TRAUMA ADMITTED TO THE NATIONAL HOSPITAL SRI LANKA *Jayawickrama
COAGULOPATHY IN NEURO TRAUMA A PROSPECTIVE ANALYSIS OF THE INCIDENCE AND CAUSES OF COAGULOPATHY IN PATIENTS WITH PURE NEURO TRAUMA AND MIXED TRAUMA ADMITTED TO THE NATIONAL HOSPITAL SRI LANKA *Jayawickrama
Administration of blood components. Tina Parker - Transfusion Practitioner
 . Administration of blood components Tina Parker - Transfusion Practitioner Red Cells Each unit contains 250-350mls Preserved with glucose and Mannitol to keep the correct tension Lasts 35 days from midnight
. Administration of blood components Tina Parker - Transfusion Practitioner Red Cells Each unit contains 250-350mls Preserved with glucose and Mannitol to keep the correct tension Lasts 35 days from midnight
TRANSFUSION SUPPORT IN HEPATOBILIARY AND PANCREATIC SURGERIES
 TRANSFUSION SUPPORT IN HEPATOBILIARY AND PANCREATIC SURGERIES Dr.K.C.Usha Professor & Head Dept: Of Transfusion Medicine & Director, Model Blood Bank Government Medical College Trivandrum,Kerala INTRODUCTION
TRANSFUSION SUPPORT IN HEPATOBILIARY AND PANCREATIC SURGERIES Dr.K.C.Usha Professor & Head Dept: Of Transfusion Medicine & Director, Model Blood Bank Government Medical College Trivandrum,Kerala INTRODUCTION
Guidelines for the management of warfarin reversal in adults
 SharePoint Location Clinical Policies and Guidelines SharePoint Index Directory General Policies and Guidelines Sub Area Haematology and Transfusion Key words (for search purposes) Warfarin, Bleeding Central
SharePoint Location Clinical Policies and Guidelines SharePoint Index Directory General Policies and Guidelines Sub Area Haematology and Transfusion Key words (for search purposes) Warfarin, Bleeding Central
Prothrombin Complex Concentrate- Octaplex. Octaplex
 Prothrombin Complex Concentrate- Concentrated Factors Prothrombin Complex Concentrate (PCC) 3- factor (factor II, IX, X) 4-factor (factors II, VII, IX, X) Activated 4-factor (factors II, VIIa, IX, X) Coagulation
Prothrombin Complex Concentrate- Concentrated Factors Prothrombin Complex Concentrate (PCC) 3- factor (factor II, IX, X) 4-factor (factors II, VII, IX, X) Activated 4-factor (factors II, VIIa, IX, X) Coagulation
Non-Medical Authorisation Course TRANSFUSION ALTERNATIVES. East Midlands Regional Transfusion Committee
 Non-Medical Authorisation Course TRANSFUSION ALTERNATIVES Janice Smith Matron Transfusion Specialist (Slides Leanne Hostler & Ant Jackson!) Aims Why we need to consider alternatives? What alternatives
Non-Medical Authorisation Course TRANSFUSION ALTERNATIVES Janice Smith Matron Transfusion Specialist (Slides Leanne Hostler & Ant Jackson!) Aims Why we need to consider alternatives? What alternatives
MASSIVE HAEMORRHAGE POLICY. ABMU HB Transfusion Team
 MASSIVE HAEMORRHAGE POLICY ABMU HB Transfusion Team Objec@ves To define the responsibili@es and roles of the Clinical team and the Haematology Department in the management of MASSIVE HAEMORRHAGE To describe
MASSIVE HAEMORRHAGE POLICY ABMU HB Transfusion Team Objec@ves To define the responsibili@es and roles of the Clinical team and the Haematology Department in the management of MASSIVE HAEMORRHAGE To describe
TXA. Things Change. Tranexamic Acid TXA. Resuscitation 2017 TXA In The ED March 31, MAST Trousers. High Flow IV Fluids.
 Resuscitation 2017 In The ED March 31, 2017 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN SECURE THE ABC S MAST
Resuscitation 2017 In The ED March 31, 2017 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN SECURE THE ABC S MAST
Balanced Transfusion Resuscitation
 Transparency in Transfusion Medicine 2013 Balanced Transfusion Resuscitation HGD Hendriks MD, PhD University Medical Center Groningen Balancing 1 2 3 Preoperative Peroperative Postoperative Balanced Coagulation
Transparency in Transfusion Medicine 2013 Balanced Transfusion Resuscitation HGD Hendriks MD, PhD University Medical Center Groningen Balancing 1 2 3 Preoperative Peroperative Postoperative Balanced Coagulation
GUIDELINES FOR MANAGEMENT OF BLEEDING AND EXCESSIVE ANTICOAGULATION WITH ORAL ANTICOAGULANTS
 GUIDELINES FOR MANAGEMENT OF BLEEDING AND EXCESSIVE ANTICOAGULATION WITH ORAL ANTICOAGULANTS This guideline covers the management of patients being treated with Vitamin K antagonists (VKA): Warfarin Acenocoumarol
GUIDELINES FOR MANAGEMENT OF BLEEDING AND EXCESSIVE ANTICOAGULATION WITH ORAL ANTICOAGULANTS This guideline covers the management of patients being treated with Vitamin K antagonists (VKA): Warfarin Acenocoumarol
When Should I Use Tranexamic Acid for Children? Dr Andrea Kelleher Consultant Adult and Paediatric Cardiac Anaesthetist
 When Should I Use Tranexamic Acid for Children? Dr Andrea Kelleher Consultant Adult and Paediatric Cardiac Anaesthetist When? When a drug is licenced for (the proposed) use When its use is supported by
When Should I Use Tranexamic Acid for Children? Dr Andrea Kelleher Consultant Adult and Paediatric Cardiac Anaesthetist When? When a drug is licenced for (the proposed) use When its use is supported by
TRAUMA RESUSCITATION. Dr. Carlos Palisi Dr. Nicholas Smith Liverpool Hospital
 TRAUMA RESUSCITATION Dr. Carlos Palisi Dr. Nicholas Smith Liverpool Hospital First Principles.ATLS/EMST A- Airway and C-spine B- Breathing C- Circulation and Access D- Neurological deficit E- adequate
TRAUMA RESUSCITATION Dr. Carlos Palisi Dr. Nicholas Smith Liverpool Hospital First Principles.ATLS/EMST A- Airway and C-spine B- Breathing C- Circulation and Access D- Neurological deficit E- adequate
Sign up to receive ATOTW weekly
 MANAGEMENT OF MAJOR HAEMORRHAGE PART ONE: INITIAL RESPONSE ANAESTHESIA TUTORIAL OF THE WEEK 136 1 ST JUNE 2009 Katrina Webster (Senior Registrar in Anaesthesia) Royal Hobart Hospital, Tasmania, Australia.
MANAGEMENT OF MAJOR HAEMORRHAGE PART ONE: INITIAL RESPONSE ANAESTHESIA TUTORIAL OF THE WEEK 136 1 ST JUNE 2009 Katrina Webster (Senior Registrar in Anaesthesia) Royal Hobart Hospital, Tasmania, Australia.
Shock and Resuscitation: Part II. Patrick M Reilly MD FACS Professor of Surgery
 Shock and Resuscitation: Part II Patrick M Reilly MD FACS Professor of Surgery Trauma Patient 1823 / 18 Police Dropoff Torso GSW Lower Midline / Right Buttock Shock This Monday Trauma Patient 1823 / 18
Shock and Resuscitation: Part II Patrick M Reilly MD FACS Professor of Surgery Trauma Patient 1823 / 18 Police Dropoff Torso GSW Lower Midline / Right Buttock Shock This Monday Trauma Patient 1823 / 18
Heme (Bleeding and Coagulopathies) in the ICU
 in the ICU") Heme (Bleeding and Coagulopathies) in the ICU General Topics To Discuss Transfusions DIC Thrombocytopenia Liver and renal disease related bleeding Lack of evidence in managing critical illness related
Heme (Bleeding and Coagulopathies) in the ICU General Topics To Discuss Transfusions DIC Thrombocytopenia Liver and renal disease related bleeding Lack of evidence in managing critical illness related
Pediatric massive transfusion protocols
 University of New Mexico UNM Digital Repository Emergency Medicine Research and Scholarship Emergency Medicine 2014 Pediatric massive transfusion protocols Ramsey Tate Follow this and additional works
University of New Mexico UNM Digital Repository Emergency Medicine Research and Scholarship Emergency Medicine 2014 Pediatric massive transfusion protocols Ramsey Tate Follow this and additional works
Transfusion 2004: Current Practice Standards. Kay Elliott, MT (ASCP) SBB SWMC Transfusion Service
 SBB SWMC Transfusion Service") Transfusion 2004: Current Practice Standards Kay Elliott, MT (ASCP) SBB SWMC Transfusion Service Massive Transfusion Protocol (MTP) When should it be activated? Massive bleeding i.e. loss of one blood
Transfusion 2004: Current Practice Standards Kay Elliott, MT (ASCP) SBB SWMC Transfusion Service Massive Transfusion Protocol (MTP) When should it be activated? Massive bleeding i.e. loss of one blood
British Society of Gastroenterology. St. Elsewhere's Hospital. National Comparative Audit of Blood Transfusion
 British Society of Gastroenterology UK Com parat ive Audit of Upper Gast roint est inal Bleeding and t he Use of Blood Transfusion Extract December 2007 St. Elsewhere's Hospital National Comparative Audit
British Society of Gastroenterology UK Com parat ive Audit of Upper Gast roint est inal Bleeding and t he Use of Blood Transfusion Extract December 2007 St. Elsewhere's Hospital National Comparative Audit
Thicker than Water. Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago
 Thicker than Water Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago I have no relevant financial relationships to disclose. Who is bleeding? How much and what kind
Thicker than Water Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago I have no relevant financial relationships to disclose. Who is bleeding? How much and what kind
Unless this copy has been taken directly from the Trust intranet site (Pandora) there is no assurance that this is the most up to date version
 there is no assurance that this is the most up to date version") Policy No: RM57 Version: 5.0 Name of Policy: Management of Massive Blood Transfusion Effective From: 02/03/2018 Date Ratified 11/10/2017 Ratified Hospital Transfusion Committee Review Date 01/10/2019 Sponsor
Policy No: RM57 Version: 5.0 Name of Policy: Management of Massive Blood Transfusion Effective From: 02/03/2018 Date Ratified 11/10/2017 Ratified Hospital Transfusion Committee Review Date 01/10/2019 Sponsor
The Bleeding Jehovah s Witness: A Nightmare Scenario?
 The Bleeding Jehovah s Witness: A Nightmare Scenario? David Smith, Bristol Hospital Liaison Committee for Jehovah s Witnesses SW RTC: Bleeding in the Medical Patient - 21 February 2018 Jehovah s Witnesses
The Bleeding Jehovah s Witness: A Nightmare Scenario? David Smith, Bristol Hospital Liaison Committee for Jehovah s Witnesses SW RTC: Bleeding in the Medical Patient - 21 February 2018 Jehovah s Witnesses
When should I transfuse platelets and plasma for children? Dr Liz Chalmers. Consultant Paediatric Haematologist Royal Hospital for Children Glasgow
 When should I transfuse platelets and plasma for children? Dr Liz Chalmers Consultant Paediatric Haematologist Royal Hospital for Children Glasgow When should I transfuse platelets and plasma in children?
When should I transfuse platelets and plasma for children? Dr Liz Chalmers Consultant Paediatric Haematologist Royal Hospital for Children Glasgow When should I transfuse platelets and plasma in children?
Management of the Trauma Patient. Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015
 Management of the Trauma Patient Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015 Saturday Night 25 yo M s/p high speed MVC Hypotensive in the ED, altered
Management of the Trauma Patient Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015 Saturday Night 25 yo M s/p high speed MVC Hypotensive in the ED, altered
Blood and blood component therapy in the critically ill patient
 Blood and blood component therapy in the critically ill patient Dr Liesel Bösenberg Specialist Physician and Fellow in Critical Care Kalafong Hospital Points that we shall ponder Transfusion triggers EGDT
Blood and blood component therapy in the critically ill patient Dr Liesel Bösenberg Specialist Physician and Fellow in Critical Care Kalafong Hospital Points that we shall ponder Transfusion triggers EGDT
John Davidson Consultant in Intensive Care Medicine Freeman Hospital, Newcastle upon Tyne
 John Davidson Consultant in Intensive Care Medicine Freeman Hospital, Newcastle upon Tyne Overview of coagulation Testing coagulation Coagulopathy in ICU Incidence Causes Evaluation Management Coagulation
John Davidson Consultant in Intensive Care Medicine Freeman Hospital, Newcastle upon Tyne Overview of coagulation Testing coagulation Coagulopathy in ICU Incidence Causes Evaluation Management Coagulation
What s in the Massive Transfusion Protocol (MTP) Package?
 Package?") What s in the Massive Transfusion Protocol (MTP) Package? The Massive Transfusion Protocol Package is a set of documents intended to improve the coordination of a Massive Transfusion Protocol. The kit
What s in the Massive Transfusion Protocol (MTP) Package? The Massive Transfusion Protocol Package is a set of documents intended to improve the coordination of a Massive Transfusion Protocol. The kit
Effective Date: Approved by: Laboratory Director, Jerry Barker (electronic signature)
") 1 of 5 Policy #: 702 (PHL-702-05) Effective Date: 9/30/2004 Reviewed Date: 8/1/2016 Subject: TRANSFUSION GUIDELINES Approved by: Laboratory Director, Jerry Barker (electronic signature) Approved by: Laboratory
1 of 5 Policy #: 702 (PHL-702-05) Effective Date: 9/30/2004 Reviewed Date: 8/1/2016 Subject: TRANSFUSION GUIDELINES Approved by: Laboratory Director, Jerry Barker (electronic signature) Approved by: Laboratory
23/10/2011. Case One: Mrs. B. Mrs. B., 36 year old, 30 weeks pregnant, 2 nd baby Blood type A negative Belted driver of minivan, struck a parked car
 GETTING IT BLOODY RIGHT: CHOOSING THE BEST PRODUCT Kathleen Eckert, ART, Transfusion Safety Officer, LHSC Brenda Morgan, RN BScN MSc, CNS, Critical Care, Victoria Hospital, LHSC http://www.transfusionontario.org/public-en/public.php
GETTING IT BLOODY RIGHT: CHOOSING THE BEST PRODUCT Kathleen Eckert, ART, Transfusion Safety Officer, LHSC Brenda Morgan, RN BScN MSc, CNS, Critical Care, Victoria Hospital, LHSC http://www.transfusionontario.org/public-en/public.php
Transfusion Triggers. Richard Soutar January 2012
 Transfusion Triggers Richard Soutar January 2012 1 Educational objectives: To understand the risks of transfusion - the known, the uncertain and unknown To understand the fear of the unknown in Transfusion
Transfusion Triggers Richard Soutar January 2012 1 Educational objectives: To understand the risks of transfusion - the known, the uncertain and unknown To understand the fear of the unknown in Transfusion
Massive Transfusion Initiation & Implication
 Massive Transfusion Initiation & Implication Katayoun Fayaz MD Blood Bank Medical Director Northwell Health April 2017 Trauma Statistics/Facts Each year trauma accounts for 41 million emergency department
Massive Transfusion Initiation & Implication Katayoun Fayaz MD Blood Bank Medical Director Northwell Health April 2017 Trauma Statistics/Facts Each year trauma accounts for 41 million emergency department
Kay Barrera MD. Surgery Grand Rounds June 19, 2014 SUNY Downstate
 Kay Barrera MD Surgery Grand Rounds June 19, 2014 SUNY Downstate Kay Barrera MD Surgery Grand Rounds June 19, 2014 SUNY Downstate Outline Why are we talking about this SCORE expectations When do we use
Kay Barrera MD Surgery Grand Rounds June 19, 2014 SUNY Downstate Kay Barrera MD Surgery Grand Rounds June 19, 2014 SUNY Downstate Outline Why are we talking about this SCORE expectations When do we use
Remote Damage Control Resuscitation: An Overview for Medical Directors and Supervisors. THOR Collaboration
 Remote Damage Control Resuscitation: An Overview for Medical Directors and Supervisors THOR Collaboration Agenda What is Remote Damage Control Resuscitation? Putting RDCR into Practice Control Hemorrhage
Remote Damage Control Resuscitation: An Overview for Medical Directors and Supervisors THOR Collaboration Agenda What is Remote Damage Control Resuscitation? Putting RDCR into Practice Control Hemorrhage
A Guide To Safe Blood Transfusion Practice
 A Guide To Safe Blood Transfusion Practice Marie Browett, Pavlina Sharp, Fiona Waller, Hafiz Qureshi, Malcolm Chambers (on behalf of the UHL Blood Transfusion Team) A Guide To Safe Blood Transfusion Practice
A Guide To Safe Blood Transfusion Practice Marie Browett, Pavlina Sharp, Fiona Waller, Hafiz Qureshi, Malcolm Chambers (on behalf of the UHL Blood Transfusion Team) A Guide To Safe Blood Transfusion Practice
VanderbiltEM.com. Prehospital STEMIs. EMS Today 2018 Research That Should Be On Your Radar Screen 3/1/2018
 EMS Today 2018 Research That Should Be On Your Radar Screen Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN VanderbiltEM.com
EMS Today 2018 Research That Should Be On Your Radar Screen Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN VanderbiltEM.com
Dr Shikha Chattree Haematology Consultant Sunderland Royal infirmary
 Dr Shikha Chattree Haematology Consultant Sunderland Royal infirmary Increasing use of Novel Oral Anticoagulants (NOACs) in the management of prophylaxis and management of venous thromboembolism and in
Dr Shikha Chattree Haematology Consultant Sunderland Royal infirmary Increasing use of Novel Oral Anticoagulants (NOACs) in the management of prophylaxis and management of venous thromboembolism and in
1 Transfusion Medicine and Blood Bank Department, H. São João, Centro
 Original Article Interventional Algorithms for the Control of Coagulopathic Bleeding in Surgical, Trauma, and Postpartum Settings: Recommendations From the Share Network Group Clinical and Applied Thrombosis/Hemostasis
Original Article Interventional Algorithms for the Control of Coagulopathic Bleeding in Surgical, Trauma, and Postpartum Settings: Recommendations From the Share Network Group Clinical and Applied Thrombosis/Hemostasis
Chapter 3 MAKING THE DECISION TO TRANSFUSE
 Chapter 3 MAKING THE DECISION TO TRANSFUSE PRACTICE POINTS Determine the best treatment for the patient which may include transfusion. Treat the cause of cytopenia (anaemia or thrombocytopenia) or plasma
Chapter 3 MAKING THE DECISION TO TRANSFUSE PRACTICE POINTS Determine the best treatment for the patient which may include transfusion. Treat the cause of cytopenia (anaemia or thrombocytopenia) or plasma
UPDATE IN TRAUMA ANESTHESIA ARANA Spring Meeting May 5th, 2017 Joe Romero CRNA, MS, CPT USAR
 UPDATE IN TRAUMA ANESTHESIA 2018 ARANA Spring Meeting May 5th, 2017 Joe Romero CRNA, MS, CPT USAR UPDATE IN TRAUMA ANESTHESIA 2018 - An overview of trauma demographics, mechanisms, and current literature
UPDATE IN TRAUMA ANESTHESIA 2018 ARANA Spring Meeting May 5th, 2017 Joe Romero CRNA, MS, CPT USAR UPDATE IN TRAUMA ANESTHESIA 2018 - An overview of trauma demographics, mechanisms, and current literature
Laboratory Empowerment. Debbie Asher Adrian Ebbs Transfusion Laboratory Managers, Eastern Pathology Alliance
 Laboratory Empowerment Debbie Asher Adrian Ebbs Transfusion Laboratory Managers, Eastern Pathology Alliance Why? Electronic ICE requesting was in use for requesting red cells NBTC Indication Codes were
Laboratory Empowerment Debbie Asher Adrian Ebbs Transfusion Laboratory Managers, Eastern Pathology Alliance Why? Electronic ICE requesting was in use for requesting red cells NBTC Indication Codes were
Blood Conservation. To introduce the learner to the basic concepts of blood conservation!! Learning Outcomes
 Section 4 Blood Conservation Aim To introduce the learner to the basic concepts of blood conservation Learning Outcomes Identify the principles of blood conservation Identify the areas where blood conservation
Section 4 Blood Conservation Aim To introduce the learner to the basic concepts of blood conservation Learning Outcomes Identify the principles of blood conservation Identify the areas where blood conservation
Clinical Overview of Coagulation Testing Issues
 Clinical Overview of Coagulation Testing Issues Adam M. Vogel, MD Assistant Professor, Division of Pediatric Surgery Washington University in St. Louis School of Medicine September 19, 2014 Disclosure
Clinical Overview of Coagulation Testing Issues Adam M. Vogel, MD Assistant Professor, Division of Pediatric Surgery Washington University in St. Louis School of Medicine September 19, 2014 Disclosure
Haematology and Transfusion
 Haematology and Transfusion dr.w.engelhardt@gmail.com Wolfram Engelhardt Offenburg, Germany James Blundell 1828 Diameter 6-8 µm Erythrocytes Women: Men: 4-5 x 10 6 /µl 5-6 x 10 6 /µl live 100-120 days
Haematology and Transfusion dr.w.engelhardt@gmail.com Wolfram Engelhardt Offenburg, Germany James Blundell 1828 Diameter 6-8 µm Erythrocytes Women: Men: 4-5 x 10 6 /µl 5-6 x 10 6 /µl live 100-120 days
Chest diseases Hospital Laboratory Hematology Practice guidelines
 Chest diseases Hospital Laboratory Hematology Practice guidelines Title RBCs transfusion in Adults SOP Code Policy Owner Hematology Unit Section Hematology Prepared By Dr. Taher Ahmed Abdelhameed Issuing
Chest diseases Hospital Laboratory Hematology Practice guidelines Title RBCs transfusion in Adults SOP Code Policy Owner Hematology Unit Section Hematology Prepared By Dr. Taher Ahmed Abdelhameed Issuing
Blood Transfusion Guidelines in Clinical Practice
 Blood Transfusion Guidelines in Clinical Practice Salwa Hindawi Director of Blood Transfusion Services Associate Professor in Haematology and Transfusion Medicine King Abdalaziz University, Jeddah Saudi
Blood Transfusion Guidelines in Clinical Practice Salwa Hindawi Director of Blood Transfusion Services Associate Professor in Haematology and Transfusion Medicine King Abdalaziz University, Jeddah Saudi
LEEDS TEACHING HOSPITALS TRUST. Transfusion in massive haemorrhage in Neonates & Paediatrics (birth -16years) Guideline Detail
 Guideline Detail") LEEDS TEACHING HOSPITALS TRUST Transfusion in massive haemorrhage in Neonates & Paediatrics (birth -16years) Guideline Detail Ownership Fran Hartley, Transfusion Practitioner (contact for review) Dr Marina
LEEDS TEACHING HOSPITALS TRUST Transfusion in massive haemorrhage in Neonates & Paediatrics (birth -16years) Guideline Detail Ownership Fran Hartley, Transfusion Practitioner (contact for review) Dr Marina
PBM: The Future of Transfusion December 6 th 2012 East of England RTC. Sue Mallett Royal Free London NHS Foundation Trust
 PBM: The Future of Transfusion December 6 th 2012 East of England RTC Sue Mallett Royal Free London NHS Foundation Trust Patient Blood Management The 3 Pillars Pre-operative optimization of anaemia Minimizing
PBM: The Future of Transfusion December 6 th 2012 East of England RTC Sue Mallett Royal Free London NHS Foundation Trust Patient Blood Management The 3 Pillars Pre-operative optimization of anaemia Minimizing
Effect of under filling tube
 Effect of under filling tube 2 What constitutes underfilling? A 4.5ml vacutainer collection tube should contain at least 4ml of blood Less than that could give falsely prolonged clotting times ALSO be
Effect of under filling tube 2 What constitutes underfilling? A 4.5ml vacutainer collection tube should contain at least 4ml of blood Less than that could give falsely prolonged clotting times ALSO be
Adult Trauma Advances in Pediatrics. (sometimes they are little adults) FAST examination. Who is bleeding? How much and what kind of TXA volume?
 FAST examination. Who is bleeding? How much and what kind of TXA volume?") Adult Trauma Advances in Pediatrics (sometimes they are little adults) Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago Alisa McQueen MD, FAAP, FACEP Associate
Adult Trauma Advances in Pediatrics (sometimes they are little adults) Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago Alisa McQueen MD, FAAP, FACEP Associate
International Journal of Health Sciences and Research ISSN:
 International Journal of Health Sciences and Research www.ijhsr.org ISSN: 2249-9571 Original Research Article Appropriate and Inappropriate Use of Fresh Frozen Plasma (FFP) and Packed Cell Volume (PCV)
International Journal of Health Sciences and Research www.ijhsr.org ISSN: 2249-9571 Original Research Article Appropriate and Inappropriate Use of Fresh Frozen Plasma (FFP) and Packed Cell Volume (PCV)
Transfusion Pitfalls. Objectives. Packed Red Blood Cells. TRICC trial (subgroups): Is transfusion always good? Components
: Is transfusion always good? Components") Objectives Transfusion Pitfalls Gregory W. Hendey, MD, FACEP Professor and Chief UCSF Fresno, Emergency Medicine To list risks and benefits of various blood products To discuss controversy over liberal
Objectives Transfusion Pitfalls Gregory W. Hendey, MD, FACEP Professor and Chief UCSF Fresno, Emergency Medicine To list risks and benefits of various blood products To discuss controversy over liberal
Patient Blood Management Are you providing this? Jeannie Callum, BA, MD, FRCPC Associate Professor, University of Toronto
 Patient Blood Management Are you providing this? Jeannie Callum, BA, MD, FRCPC Associate Professor, University of Toronto Disclosures Relevant relationships with commercial entities: Octapharma, CSL Behring
Patient Blood Management Are you providing this? Jeannie Callum, BA, MD, FRCPC Associate Professor, University of Toronto Disclosures Relevant relationships with commercial entities: Octapharma, CSL Behring
Thursday, February 26, :00 am. Regulation of Coagulation/Disseminated Intravascular Coagulation HEMOSTASIS/THROMBOSIS III
 REGULATION OF COAGULATION Introduction HEMOSTASIS/THROMBOSIS III Regulation of Coagulation/Disseminated Coagulation necessary for maintenance of vascular integrity Enough fibrinogen to clot all vessels
REGULATION OF COAGULATION Introduction HEMOSTASIS/THROMBOSIS III Regulation of Coagulation/Disseminated Coagulation necessary for maintenance of vascular integrity Enough fibrinogen to clot all vessels
Massive Transfusion in Trauma
 Page 1 Massive Transfusion in Trauma Robert S. Harris, M.D. Atlanta, Georgia Definitions and Demographics Hemorrhage is the second most common cause of death following injury and trauma, and is responsible
Page 1 Massive Transfusion in Trauma Robert S. Harris, M.D. Atlanta, Georgia Definitions and Demographics Hemorrhage is the second most common cause of death following injury and trauma, and is responsible
Blood transfusions in sepsis, the elderly and patients with TBI
 Blood transfusions in sepsis, the elderly and patients with TBI Shabbir Alekar MICU, CH Baragwanath Academic Hospital & The University of the Witwatersrand CCSSA Congress 11 June 2015 Packed RBC - complications
Blood transfusions in sepsis, the elderly and patients with TBI Shabbir Alekar MICU, CH Baragwanath Academic Hospital & The University of the Witwatersrand CCSSA Congress 11 June 2015 Packed RBC - complications
Michael Avant, M.D. The Children s Hospital of GHS
 Michael Avant, M.D. The Children s Hospital of GHS OVERVIEW ER to ICU Transition Early Management Priorities the First 48 hours Organ System Support Complications THE FIRST 48 HOURS Communication Damage
Michael Avant, M.D. The Children s Hospital of GHS OVERVIEW ER to ICU Transition Early Management Priorities the First 48 hours Organ System Support Complications THE FIRST 48 HOURS Communication Damage
Where Blood Matters AIMS. National Scientific Meeting. Darwin Convention Centre September Morteza Mohajeri, MD, FRACS ( Cardiothoracic )
") Where Blood Matters AIMS National Scientific Meeting Darwin Convention Centre 24 27 September 2012 Morteza Mohajeri, MD, FRACS ( Cardiothoracic ) Senior Medical Advisor QBMP 1 National Blood Agreement
Where Blood Matters AIMS National Scientific Meeting Darwin Convention Centre 24 27 September 2012 Morteza Mohajeri, MD, FRACS ( Cardiothoracic ) Senior Medical Advisor QBMP 1 National Blood Agreement
JOURNAL CLUB INDICATIONS FOR AND ADVERSE EFFECTS OF RED CELL TRANSFUSION. Maggie Woods PGY-3
 JOURNAL CLUB INDICATIONS FOR AND ADVERSE EFFECTS OF RED CELL TRANSFUSION Maggie Woods PGY-3 BACKGROUND Objective: To describe evidence for current guidelines, review trends, examine the risks of transfusion
JOURNAL CLUB INDICATIONS FOR AND ADVERSE EFFECTS OF RED CELL TRANSFUSION Maggie Woods PGY-3 BACKGROUND Objective: To describe evidence for current guidelines, review trends, examine the risks of transfusion
The ABC s of Blood Components. Terry Downs, MT(ASCP)SBB Administrative Manager University of Michigan Hospitals Blood Bank and Transfusion Service
SBB Administrative Manager University of Michigan Hospitals Blood Bank and Transfusion Service") The ABC s of Blood Components Terry Downs, MT(ASCP)SBB Administrative Manager University of Michigan Hospitals Blood Bank and Transfusion Service Objectives Describe three additives used in blood components.
The ABC s of Blood Components Terry Downs, MT(ASCP)SBB Administrative Manager University of Michigan Hospitals Blood Bank and Transfusion Service Objectives Describe three additives used in blood components.
Hemostatic Resuscitation in Trauma. Joanna Davidson, MD 6/6/2012
 Hemostatic Resuscitation in Trauma { Joanna Davidson, MD 6/6/2012 Case of HM 28 yo M arrives CCH trauma bay 5/27/12 at 241 AM Restrained driver in low speed MVC after getting shot in the chest Arrived
Hemostatic Resuscitation in Trauma { Joanna Davidson, MD 6/6/2012 Case of HM 28 yo M arrives CCH trauma bay 5/27/12 at 241 AM Restrained driver in low speed MVC after getting shot in the chest Arrived
Guidance for management of bleeding in patients taking the new oral anticoagulant drugs: rivaroxaban, dabigatran or apixaban
 Guidance for management of bleeding in patients taking the new oral anticoagulant drugs: rivaroxaban, dabigatran or apixaban Purpose The aim of this guidance is to outline the management of patients presenting
Guidance for management of bleeding in patients taking the new oral anticoagulant drugs: rivaroxaban, dabigatran or apixaban Purpose The aim of this guidance is to outline the management of patients presenting
Survey of Massive Blood Loss In the North East of England 2013
 Survey of Massive Blood Loss In the North East of England 2013 November 2014 Acknowledgements Dr Michelle Lannon ST6 Haematology The Newcastle upon Tyne Hospitals NHS Foundation Trust Dr Adil Iqbal Consultant
Survey of Massive Blood Loss In the North East of England 2013 November 2014 Acknowledgements Dr Michelle Lannon ST6 Haematology The Newcastle upon Tyne Hospitals NHS Foundation Trust Dr Adil Iqbal Consultant
Patient Blood Management and alternatives to transfusion
 Patient Blood Management and alternatives to transfusion Patient Blood Management and the alternatives to transfusion and when these should be used Learning Outcomes Explain techniques that can be used
Patient Blood Management and alternatives to transfusion Patient Blood Management and the alternatives to transfusion and when these should be used Learning Outcomes Explain techniques that can be used
TRANSFUSIONS WHY DO WE EVEN CARE?????
 TRANSFUSIONS WHY DO WE EVEN CARE????? BECAUSE BLOOD CAN KILL 7 TRALI DEATHS SINCE 2002 WMC 5 women Because in OB you are transfusing 2 instead of 1 BECAUSE BLOOD IS A LIQUID TRANSPLANT JOINT COMMISSION
TRANSFUSIONS WHY DO WE EVEN CARE????? BECAUSE BLOOD CAN KILL 7 TRALI DEATHS SINCE 2002 WMC 5 women Because in OB you are transfusing 2 instead of 1 BECAUSE BLOOD IS A LIQUID TRANSPLANT JOINT COMMISSION
Groupe d Intérêt en Hémostase Périopératoire
 How do I treat massive bleeding? Red blood cell / plasma / platelet ratio and massive transfusion protocols Anne GODIER Service d Anesthésie-Réanimation Hopital Cochin Paris Groupe d Intérêt en Hémostase
How do I treat massive bleeding? Red blood cell / plasma / platelet ratio and massive transfusion protocols Anne GODIER Service d Anesthésie-Réanimation Hopital Cochin Paris Groupe d Intérêt en Hémostase
Dr Charlie Baker Consultant Anaesthetist UHNM. Being a place our f amilies would choose
 Dr Charlie Baker Consultant Anaesthetist UHNM Being a place our f amilies would choose The story so far: Anaemia is associated with transfusion. The more anaemic you are pre op the more likely you are
Dr Charlie Baker Consultant Anaesthetist UHNM Being a place our f amilies would choose The story so far: Anaemia is associated with transfusion. The more anaemic you are pre op the more likely you are
2012, Görlinger Klaus
 Gerinnungsmanagement der Gegenwart - wie gehen wir heute vor? 25. Allander Gerinnungsrunde am 15. März 2012 Klaus Görlinger Universitätsklinikum Essen klaus@goerlinger.net CSL Behring GmbH Octapharma AG
Gerinnungsmanagement der Gegenwart - wie gehen wir heute vor? 25. Allander Gerinnungsrunde am 15. März 2012 Klaus Görlinger Universitätsklinikum Essen klaus@goerlinger.net CSL Behring GmbH Octapharma AG
Management of Massive Transfusion. Philippe Van der Linden MD, PhD CHU Brugmann-HUDERF, Free University of Brussels
 Management of Massive Transfusion Philippe Van der Linden MD, PhD CHU Brugmann-HUDERF, Free University of Brussels Massive Hemorrhage: definition? Replacement of one blood mass in less than 24 hours Dynamic
Management of Massive Transfusion Philippe Van der Linden MD, PhD CHU Brugmann-HUDERF, Free University of Brussels Massive Hemorrhage: definition? Replacement of one blood mass in less than 24 hours Dynamic
Kristan Staudenmayer, MD Stanford University, Stanford, CA
 Kristan Staudenmayer, MD Stanford University, Stanford, CA Fluid resuscitation Variety of fluids How to administer What you do DOES matter WWII 1942 North Africa high mortality from hemorrhaghic shock
Kristan Staudenmayer, MD Stanford University, Stanford, CA Fluid resuscitation Variety of fluids How to administer What you do DOES matter WWII 1942 North Africa high mortality from hemorrhaghic shock
New drugs for anticoagulation so much choice, how do they compare? Dr Patrick Kesteven Newcastle
 New drugs for anticoagulation so much choice, how do they compare? Dr Patrick Kesteven Newcastle CONCLUSIONS 1. Arrival of new anticoagulants is a Good Thing. CONCLUSIONS 1. Arrival of new anticoagulants
New drugs for anticoagulation so much choice, how do they compare? Dr Patrick Kesteven Newcastle CONCLUSIONS 1. Arrival of new anticoagulants is a Good Thing. CONCLUSIONS 1. Arrival of new anticoagulants
CrackCast Episode 7 Blood and Blood Components
 CrackCast Episode 7 Blood and Blood Components Episode Overview: 1) Describe the 3 categories of blood antigens 2) Who is the universal donor and why? 3) Define massive transfusion 4) List 5 physiologic
CrackCast Episode 7 Blood and Blood Components Episode Overview: 1) Describe the 3 categories of blood antigens 2) Who is the universal donor and why? 3) Define massive transfusion 4) List 5 physiologic
The changing face of
 The changing face of sepsis. @SepsisUK Dr Ron Daniels B.E.M. CEO, UK Sepsis Trust CEO, Global Sepsis Alliance Special Adviser (maternal sepsis) to WHO Breast cancer Cognitive impairment Mild 3.8 7.1
The changing face of sepsis. @SepsisUK Dr Ron Daniels B.E.M. CEO, UK Sepsis Trust CEO, Global Sepsis Alliance Special Adviser (maternal sepsis) to WHO Breast cancer Cognitive impairment Mild 3.8 7.1