the bleeding won t stop? Liane Manz RN, BScN, CNCC(c) Royal Alexandra Hospital
|
|
|
- Oswald Turner
- 5 years ago
- Views:
Transcription
1 What do you do when the bleeding won t stop? Teddie Tanguay RN, MN, NP, CNCC(c) Teddie Tanguay RN, MN, NP, CNCC(c) Liane Manz RN, BScN, CNCC(c) Royal Alexandra Hospital
2 Outline Case study Normal coagulation Hemorrhagic shock Lethal Triad Massive transfusion Treatment and Complications
3 Case Study Mrs. P 26 yr old female Called EMS after 1 hour of vaginal bleeding PMHx: Nothing significant P5G4 Recent miscarriage with D&C for retain POC
4 Mrs. P cont.. At Rural hospital D&C performed Unable to achieve hemostasis RAH called for consultation STARS unable to fly Sent to Edmonton by ground Stop in Stony Plain due to instability

5 At the RAH PEA VF ST VT Asystole PEA VF ST
6 Blood Products in ED 32 U PRBC 10 U Cryo 6L Ringers 6U FFP 1 pooled platelets
7 In the OR 34 U PRBC 4 Pooled platelets 45L 4.5L Cell Saver 37 U 8U FFP Cryo
8 ICU 1255 HR =138 BP = 108/45 O2 Sat = 83% RR = 20 Temp = would not register U/O = 130 Vent Settings = AC % TV=700
9 ICU 1317 HR = 150 BP = 69/41 Levophed started at 20mcg/min O2 sat = 69% Temp = 34 C No changes to vent settings nitric oxide and steroids added
10 ICU Labs Hgb = 102 ABG = 7.24/40/39/16.3 INR =1.1 PTT = 41 Fibrinogen = 1.1 Electrolytes = K 4.0 Cl 115 ica 0.78 Lactate = 11.6
11 More Blood Products 11 U 8U PRBC Cryo 1000 mg Tranexamic Acid 8 U FFP 2mg Factor VII
12 No More 4U PRBC 4 1 Pooled Platelets 3U 3 U FFP
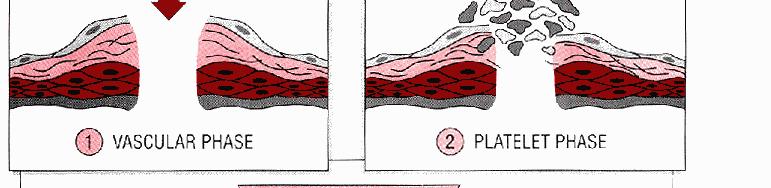
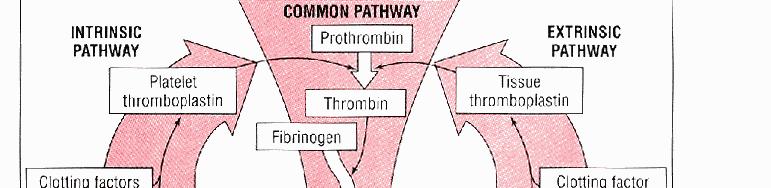
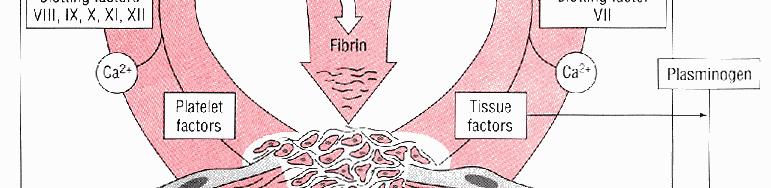
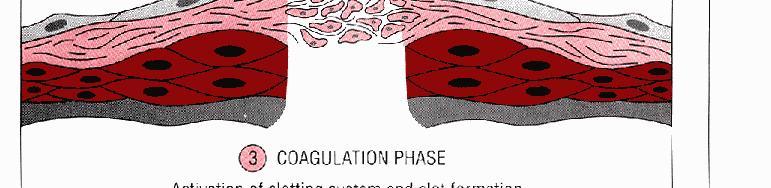
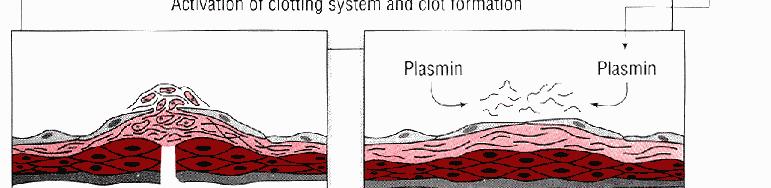
13 Normal Coagulation Hemostatsis Is the process of blood clot formation at the site of vessel linjury to stop bleeding 4 Phases of clotting process: Platelet plug Coagulation Cascade Termination of Clotting Fibrinolysis Rice, Wheeler, Chest, 2009
14
15 4 Classes of Hemorrhage Class I Class II» Blood loss of 15%» Vital signs no change» Blood loss 15 to 30%» Tachycardia, tachypnea and decreased pulse pressure» Skin cool and clammy Advanced Trauma Life Support
16 Hemorrhage Class III Class IV» Involves 30 to 40 % blood volume loss» SBP < 90 mmhg, HR > 120 and tachypnea» Decreased urine output and delayed capillary refill» changes in mental status» Involves 40 % or more blood volume loss» SBP < 90 mmhg, narrow pulse pressure, HR> 120» Urine output absent, skin cold and pale»capillary refill is delayed Advanced Trauma Life Support
17 Hemorrhage Intraoperative hemorrhage Blood loss exceeding 1000 mls or requiring a transfusion Massive hemorrhage Acute blood loss of more than 25% of patient s blood volume Patients with severe hemorrhage may develop acute coagulopathy on admission that worsens with transfusion Mortality is related to severity of hemorrhagic h shock and total number of packed cells transfused Sihler & Napolitano, Chest, 2009
18 Lethal Triad Hypothermia Increased loss of heat decreased d production of heat Effects platelet activation Acidosis Activity of intrinsic and extrinsic pathways reduced Increased fibrinogen degradation rate Coagulopathy O l ft i j i f ti Occurs early after injury in presence of tissue hypoperfusion Engels et al, Trauma, 2011







19 Sihler & Napolitano, Chest, 2009
20 Treatment Aim of Treatment Restoration of vascular and tissue integrity by surgery or embolization Blood transfusion to restore adequate blood volume to maximize tissue oxygen delivery Goal is to maintain hemostasis with blood products Sihler & Napolitano, Chest, 2009
21 Massive Transfusion Massive transfusion is the administration of > 10 units of PRBC s in 24 hours Goal is to achieve hemostasis without DVT s, Thrombosis, CVA or MI Selection of appropriate amount and types of blood components Engels et al., Trauma, 2011
22
23 Prevention of Lethal Triad Early control of Hemorrhage Hemostatic Resuscitation Hypotensive resuscitation Aggressive treatment of Coagulopathy Engels et al., Trauma, 2011
24 Hemostatic Resuscitation Expedite control of hemorrhage Prevent dilutional coagulopathy and thrombocytopenia Hypotensive resuscitation Transfuse blood products 1:1:1 ratio Frequent lab monitoring i Silher & Napolitano, Chest 2009
25 Dilutional Coagulopathy Infusion of RBC and Crystalloid dilute clotting proteins Increased PT, PTT Decreased Platelets and Fibrinogen Ratio of 1:1:1 for FFP, Platelets and red cells Cryoprecipitate when fibrinogen decreased UptoDate, 2012
26 Hypotensive Resuscitation Prehospital minimize i i fluid resuscitation ti Trauma Practice Guidelines Withhold IV fluids in patients with penetrating injuries Withhold IV fluids until active bleeding is addressed Titrate IV fluid administration to palpable radial pulse Small fixed boluses rather than continuous administration of IV fluids Engels et al., Trauma 2011
27 Factor VIIa Tranexamic Mechanism of Action Increased tissue factor binding Increased binding to activated t platelets l t Activation of factor X Correction of early coagulopathy Mechanism of Action Inhibits the breakdown of the clot Antifibrinolytics Crash 2 study Shiler & Napolitano, Chest, 2009
28 Complications of MT Metabolic Alkalosisl Due to citrate accumulation Hypokalemia due to exchange of H ions Hypocalcaemia Citrate binding Hypokalemia K reenter the red cells Aldosterone, ADH, Catecholamine release Hyperkalemia From K leakage from blood (renal failure) Rice, Wheeler, Chest 2009
29 Complications of MT Hypothermia Decreased clotting, metabolic acidosis Dilutional Thrombocytopenia TRALI TACO Loss and consumption Shiler & Napolitano, Chest, 2009
30 Nursing Care Prevent Hypothermia Increase room temperature Heating blankets Warm ALL FLUIDS Increase temp on ventilator humidifiers Follow Massive Transfusion Protocol 1:1:1 ratio Treat acidemia R/L instead of NS
31 Back to Mrs. P Temp = 36 C Hgb = 90 ABG = 7.24/40/40 INR = 1.0 PTT = 44 GCS = 3 No sedation/analgesic since the OR Lactate = 8.4
32 ICU Assessment 2000h VS began to stabilize Requiring i less inotropic i support Temp 38 C Improved LOC
33 Outcome Discharged home in less than 1 month No deficits Returned to the ICU to visit and thank the staff 6 months post discharge
34
35 References Engels, P.T., et al. (2011). The natural history of trauma-related related coagulopathy: Implications for treatment. The Journal of Trauma Injury, Infection and Critical Care. 71 (5), Rice, T.W &.Wheeler,A.P.,,(2009). Coagulopathy in critically ill patients. Part 1: platelet disorders. Chest, 136, Riha, G.M., & Schreiber, M.A., (2010). Update and new developments in the management of the exsanguinating patient. Journal of Intensive Care Medicine. i Online DOI: / / Sihler, K.C., & Napolitano, L.M. (2010). Complications of massive transfusion. Chest, 137, Sihler, K.C., & Napolitano, L.M. (2009). Massive transfusion new insight. Chest, 136, Wheeler,A.P., & Rice, T.W. (2010). Coagulopathy in critically ill patients? Part 2- soluble clotting factors and hemostatic testing. Chest, 137 (1),
36 Contact Information ca
TRAUMA RESUSCITATION. Dr. Carlos Palisi Dr. Nicholas Smith Liverpool Hospital
 TRAUMA RESUSCITATION Dr. Carlos Palisi Dr. Nicholas Smith Liverpool Hospital First Principles.ATLS/EMST A- Airway and C-spine B- Breathing C- Circulation and Access D- Neurological deficit E- adequate
TRAUMA RESUSCITATION Dr. Carlos Palisi Dr. Nicholas Smith Liverpool Hospital First Principles.ATLS/EMST A- Airway and C-spine B- Breathing C- Circulation and Access D- Neurological deficit E- adequate
MANAGEMENT OF COAGULOPATHY AFTER TRAUMA OR MAJOR SURGERY
 MANAGEMENT OF COAGULOPATHY AFTER TRAUMA OR MAJOR SURGERY 19th ANNUAL CONTROVERSIES AND PROBLEMS IN SURGERY Thabo Mothabeng General Surgery: 1 Military Hospital HH Stone et al. Ann Surg. May 1983; 197(5):
MANAGEMENT OF COAGULOPATHY AFTER TRAUMA OR MAJOR SURGERY 19th ANNUAL CONTROVERSIES AND PROBLEMS IN SURGERY Thabo Mothabeng General Surgery: 1 Military Hospital HH Stone et al. Ann Surg. May 1983; 197(5):
Transfusion Requirements and Management in Trauma RACHEL JACK
 Transfusion Requirements and Management in Trauma RACHEL JACK Overview Haemostatic resuscitation Massive Transfusion Protocol Overview of NBA research guidelines Haemostatic resuscitation Permissive hypotension
Transfusion Requirements and Management in Trauma RACHEL JACK Overview Haemostatic resuscitation Massive Transfusion Protocol Overview of NBA research guidelines Haemostatic resuscitation Permissive hypotension
Pediatric massive transfusion protocols
 University of New Mexico UNM Digital Repository Emergency Medicine Research and Scholarship Emergency Medicine 2014 Pediatric massive transfusion protocols Ramsey Tate Follow this and additional works
University of New Mexico UNM Digital Repository Emergency Medicine Research and Scholarship Emergency Medicine 2014 Pediatric massive transfusion protocols Ramsey Tate Follow this and additional works
Damage Control Resuscitation. VGH Trauma Rounds 2018 Harvey Hawes
 Damage Control Resuscitation VGH Trauma Rounds 2018 Harvey Hawes Example Case 25yo F in motor vehicle collision at high speed Picked up at scene by Helicopter EMS unit Initial vital signs: HR 134 BP 88/42
Damage Control Resuscitation VGH Trauma Rounds 2018 Harvey Hawes Example Case 25yo F in motor vehicle collision at high speed Picked up at scene by Helicopter EMS unit Initial vital signs: HR 134 BP 88/42
2 Liters. Goal: Basic Algorithm Volume Resuscitation in Trauma. Initial Fluids. Blood. Where do Blood Products Come From?
 Goal: Basic Algorithm Volume Resuscitation in Trauma Sanjay Arora MD Associate Professor of Emergency Medicine Keck School of Medicine at USC Los Angeles County + USC Medical Center May 23, 2012 Initial
Goal: Basic Algorithm Volume Resuscitation in Trauma Sanjay Arora MD Associate Professor of Emergency Medicine Keck School of Medicine at USC Los Angeles County + USC Medical Center May 23, 2012 Initial
Bleeding, Coagulopathy, and Thrombosis in the Injured Patient
 Bleeding, Coagulopathy, and Thrombosis in the Injured Patient June 7, 2008 Kristan Staudenmayer, MD Trauma Fellow UCSF/SFGH Trauma deaths Sauaia A, et al. J Trauma. Feb 1995;38(2):185 Coagulopathy is Multi-factorial
Bleeding, Coagulopathy, and Thrombosis in the Injured Patient June 7, 2008 Kristan Staudenmayer, MD Trauma Fellow UCSF/SFGH Trauma deaths Sauaia A, et al. J Trauma. Feb 1995;38(2):185 Coagulopathy is Multi-factorial
Massive transfusion: Recent advances, guidelines & strategies. Dr.A.Surekha Devi Head, Dept. of Transfusion Medicine Global Hospital Hyderabad
 Massive transfusion: Recent advances, guidelines & strategies Dr.A.Surekha Devi Head, Dept. of Transfusion Medicine Global Hospital Hyderabad Massive Hemorrhage Introduction Hemorrhage is a major cause
Massive transfusion: Recent advances, guidelines & strategies Dr.A.Surekha Devi Head, Dept. of Transfusion Medicine Global Hospital Hyderabad Massive Hemorrhage Introduction Hemorrhage is a major cause
Remote Damage Control Resuscitation: An Overview for Medical Directors and Supervisors. THOR Collaboration
 Remote Damage Control Resuscitation: An Overview for Medical Directors and Supervisors THOR Collaboration Agenda What is Remote Damage Control Resuscitation? Putting RDCR into Practice Control Hemorrhage
Remote Damage Control Resuscitation: An Overview for Medical Directors and Supervisors THOR Collaboration Agenda What is Remote Damage Control Resuscitation? Putting RDCR into Practice Control Hemorrhage
Financial Disclosure. Objectives 9/24/2018
 Hemorrhage and Transfusion Adjuncts in the Setting of Damage Control Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Adjunct Professor of Orthopedics and Neurosurgery, University
Hemorrhage and Transfusion Adjuncts in the Setting of Damage Control Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Adjunct Professor of Orthopedics and Neurosurgery, University
MASSIVE TRANSFUSION DR.K.HITESH KUMAR FINAL YEAR PG DEPT. OF TRANSFUSION MEDICINE
 MASSIVE TRANSFUSION DR.K.HITESH KUMAR FINAL YEAR PG DEPT. OF TRANSFUSION MEDICINE CONTENTS Definition Indications Transfusion trigger Massive transfusion protocol Complications DEFINITION Massive transfusion:
MASSIVE TRANSFUSION DR.K.HITESH KUMAR FINAL YEAR PG DEPT. OF TRANSFUSION MEDICINE CONTENTS Definition Indications Transfusion trigger Massive transfusion protocol Complications DEFINITION Massive transfusion:
Implementation and execution of civilian RDCR programs Minnesota RDCR
 Implementation and execution of civilian RDCR programs Minnesota RDCR Donald H Jenkins, MD FACS Associate Professor of Surgery and Director of Trauma Division of Trauma, Critical Care and Emergency General
Implementation and execution of civilian RDCR programs Minnesota RDCR Donald H Jenkins, MD FACS Associate Professor of Surgery and Director of Trauma Division of Trauma, Critical Care and Emergency General
3/16/15. Management of the Bleeding Trauma Patient: Concepts in Damage Control Resuscitation. Obligatory Traumatologist Slide
 Management of the Bleeding Trauma Patient: Concepts in Damage Control Resuscitation Courtney Sommer, MD MPH Duke Trauma Symposium March 12, 2015 Obligatory Traumatologist Slide In 2010 trauma was leading
Management of the Bleeding Trauma Patient: Concepts in Damage Control Resuscitation Courtney Sommer, MD MPH Duke Trauma Symposium March 12, 2015 Obligatory Traumatologist Slide In 2010 trauma was leading
Printed copies of this document may not be up to date, obtain the most recent version from
 Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Claire Fraser P.Ramnarayan Author Position tanp CATS Consultant Document Owner E. Polke Document
Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Claire Fraser P.Ramnarayan Author Position tanp CATS Consultant Document Owner E. Polke Document
Surgical Resuscitation Management in Poly-Trauma Patients
 Surgical Resuscitation Management in Poly-Trauma Patients Andrew Bernard, MD FACS Paul Kearney MD Chair of Trauma Surgery Associate Professor Medical Director of Trauma and Acute Care Surgery UK Healthcare
Surgical Resuscitation Management in Poly-Trauma Patients Andrew Bernard, MD FACS Paul Kearney MD Chair of Trauma Surgery Associate Professor Medical Director of Trauma and Acute Care Surgery UK Healthcare
Management of the Trauma Patient. Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015
 Management of the Trauma Patient Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015 Saturday Night 25 yo M s/p high speed MVC Hypotensive in the ED, altered
Management of the Trauma Patient Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015 Saturday Night 25 yo M s/p high speed MVC Hypotensive in the ED, altered
HYPOTHERMIA IN TRAUMA. Kevin Palmer EMT-P, DiMM
 HYPOTHERMIA IN TRAUMA Kevin Palmer EMT-P, DiMM DISCLOSURE No Financial conflicts of interest Member of the Wilderness Medical Society Diploma in Mountain Medicine Fellowship in the Academy of Wilderness
HYPOTHERMIA IN TRAUMA Kevin Palmer EMT-P, DiMM DISCLOSURE No Financial conflicts of interest Member of the Wilderness Medical Society Diploma in Mountain Medicine Fellowship in the Academy of Wilderness
Transfusion in major bleeding: new insights. Gert Poortmans
 Transfusion in major bleeding: new insights Gert Poortmans Trauma Cardiac Surgery Major Surgery with ongoing blood loss Burn Surgery Lethal Triad Polytransfusion: definitions Coagulation Coagulopathy of
Transfusion in major bleeding: new insights Gert Poortmans Trauma Cardiac Surgery Major Surgery with ongoing blood loss Burn Surgery Lethal Triad Polytransfusion: definitions Coagulation Coagulopathy of
PEDIATRIC MASSIVE TRANSFUSION
 PEDIATRIC MASSIVE TRANSFUSION CHELSEA RUNKLE RN, BSN, CCRN, SRNA CROZER-CHESTER MEDICAL CENTER/VILLANOVA UNIVERSITY NURSE ANESTHESIA PROGRAM LEADING CAUSE OF DEATH Trauma Motor vehicle accidents, nonaccidental
PEDIATRIC MASSIVE TRANSFUSION CHELSEA RUNKLE RN, BSN, CCRN, SRNA CROZER-CHESTER MEDICAL CENTER/VILLANOVA UNIVERSITY NURSE ANESTHESIA PROGRAM LEADING CAUSE OF DEATH Trauma Motor vehicle accidents, nonaccidental
Hemostatic Resuscitation in Trauma. Joanna Davidson, MD 6/6/2012
 Hemostatic Resuscitation in Trauma { Joanna Davidson, MD 6/6/2012 Case of HM 28 yo M arrives CCH trauma bay 5/27/12 at 241 AM Restrained driver in low speed MVC after getting shot in the chest Arrived
Hemostatic Resuscitation in Trauma { Joanna Davidson, MD 6/6/2012 Case of HM 28 yo M arrives CCH trauma bay 5/27/12 at 241 AM Restrained driver in low speed MVC after getting shot in the chest Arrived
Pre-hospital Administration of Blood Products (PHBP) and Tranexamic acid (TXA): Is the Jury Still Out?
 and Tranexamic acid (TXA): Is the Jury Still Out?") Pre-hospital Administration of Blood Products (PHBP) and Tranexamic acid (TXA): Is the Jury Still Out? Jessica K. Reynolds, MD Assistant Professor of Surgery University of Kentucky, Department of Trauma
Pre-hospital Administration of Blood Products (PHBP) and Tranexamic acid (TXA): Is the Jury Still Out? Jessica K. Reynolds, MD Assistant Professor of Surgery University of Kentucky, Department of Trauma
PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT
 PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT Melanie Sanchez, RN, MSNE, OCN, CCRN Clinical Nurse III City of Hope National Medical Center HOW THE EXPERTS TREAT HEMATOLOGIC MALIGNANCIES LAS VEGAS, NV
PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT Melanie Sanchez, RN, MSNE, OCN, CCRN Clinical Nurse III City of Hope National Medical Center HOW THE EXPERTS TREAT HEMATOLOGIC MALIGNANCIES LAS VEGAS, NV
Shock and Resuscitation: Part II. Patrick M Reilly MD FACS Professor of Surgery
 Shock and Resuscitation: Part II Patrick M Reilly MD FACS Professor of Surgery Trauma Patient 1823 / 18 Police Dropoff Torso GSW Lower Midline / Right Buttock Shock This Monday Trauma Patient 1823 / 18
Shock and Resuscitation: Part II Patrick M Reilly MD FACS Professor of Surgery Trauma Patient 1823 / 18 Police Dropoff Torso GSW Lower Midline / Right Buttock Shock This Monday Trauma Patient 1823 / 18
Staging Sepsis for the Emergency Department: Physician
 Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Shock and Trauma Resuscitation
 Shock and Trauma Resuscitation Bonjo Batoon, MS, CRNA Bbatoon@som.umaryland.edu Disclaimer Resuscitation is continuously evolving There is no one right way Knowing is half the battle G.I. Joe Having to
Shock and Trauma Resuscitation Bonjo Batoon, MS, CRNA Bbatoon@som.umaryland.edu Disclaimer Resuscitation is continuously evolving There is no one right way Knowing is half the battle G.I. Joe Having to
Unrestricted. Dr ppooransari fellowship of perenatalogy
 Unrestricted Dr ppooransari fellowship of perenatalogy Assessment of severity of hemorrhage Significant drops in blood pressure are generally not manifested until substantial bleeding has occurred, and
Unrestricted Dr ppooransari fellowship of perenatalogy Assessment of severity of hemorrhage Significant drops in blood pressure are generally not manifested until substantial bleeding has occurred, and
Coagulopathy: Measuring and Management. Nina A. Guzzetta, M.D. Children s Healthcare of Atlanta Emory University School of Medicine
 Coagulopathy: Measuring and Management Nina A. Guzzetta, M.D. Children s Healthcare of Atlanta Emory University School of Medicine No Financial Disclosures Objectives Define coagulopathy of trauma Define
Coagulopathy: Measuring and Management Nina A. Guzzetta, M.D. Children s Healthcare of Atlanta Emory University School of Medicine No Financial Disclosures Objectives Define coagulopathy of trauma Define
Transfusion 2004: Current Practice Standards. Kay Elliott, MT (ASCP) SBB SWMC Transfusion Service
 SBB SWMC Transfusion Service") Transfusion 2004: Current Practice Standards Kay Elliott, MT (ASCP) SBB SWMC Transfusion Service Massive Transfusion Protocol (MTP) When should it be activated? Massive bleeding i.e. loss of one blood
Transfusion 2004: Current Practice Standards Kay Elliott, MT (ASCP) SBB SWMC Transfusion Service Massive Transfusion Protocol (MTP) When should it be activated? Massive bleeding i.e. loss of one blood
SHOCK Susanna Hilda Hutajulu, MD, PhD
 SHOCK Susanna Hilda Hutajulu, MD, PhD Div Hematology and Medical Oncology Department of Internal Medicine Universitas Gadjah Mada Yogyakarta Outline Definition Epidemiology Physiology Classes of Shock
SHOCK Susanna Hilda Hutajulu, MD, PhD Div Hematology and Medical Oncology Department of Internal Medicine Universitas Gadjah Mada Yogyakarta Outline Definition Epidemiology Physiology Classes of Shock
Epidemiology. Case. Pre-Hospital SI and Massive Transfusion
 Epidemiology Preston Maxim, MD Assoc. Professor of Emergency Medicine San Francisco General Hospital ~180,000 deaths 2007 due to trauma 25% trauma patients require 1 unit of PRBC and only 25% of those
Epidemiology Preston Maxim, MD Assoc. Professor of Emergency Medicine San Francisco General Hospital ~180,000 deaths 2007 due to trauma 25% trauma patients require 1 unit of PRBC and only 25% of those
Hemostatic Resuscitation
 Hemostatic Resuscitation 30 th David Miller Trauma Symposium Bill Beck, MD Assistant Professor of Surgery Trauma, Emergency General Surgery, Critical Care Disclosures None Again. Mac user. Why I Like Trauma?
Hemostatic Resuscitation 30 th David Miller Trauma Symposium Bill Beck, MD Assistant Professor of Surgery Trauma, Emergency General Surgery, Critical Care Disclosures None Again. Mac user. Why I Like Trauma?
Recombinant Activated Factor VII: Useful. Department of Surgery Grand Rounds 11/8/10 David Mauchley MD
 Recombinant Activated Factor VII: Useful Department of Surgery Grand Rounds 11/8/10 David Mauchley MD Hemostasis and Coagulation Traditional cascade model Two convergent pathways Series of proteolytic
Recombinant Activated Factor VII: Useful Department of Surgery Grand Rounds 11/8/10 David Mauchley MD Hemostasis and Coagulation Traditional cascade model Two convergent pathways Series of proteolytic
FLUID MANAGEMENT AND BLOOD COMPONENT THERAPY
 Manual: Section: Protocol #: Approval Date: Effective Date: Revision Due Date: 10/2019 LifeLine Patient Care Protocols Adult/Pediatrics AP1-011 10/2018 10/2018 FLUID MANAGEMENT AND BLOOD COMPONENT THERAPY
Manual: Section: Protocol #: Approval Date: Effective Date: Revision Due Date: 10/2019 LifeLine Patient Care Protocols Adult/Pediatrics AP1-011 10/2018 10/2018 FLUID MANAGEMENT AND BLOOD COMPONENT THERAPY
RENAL & HEMATOLOGY EMERGENCIES JEFF SIMONS B.S. F-PC
 RENAL & HEMATOLOGY EMERGENCIES JEFF SIMONS B.S. F-PC GOALS Overview of renal system anatomy / physiology Discuss common medical / trauma renal issues Identify associated assessment keys GOALS Introduction
RENAL & HEMATOLOGY EMERGENCIES JEFF SIMONS B.S. F-PC GOALS Overview of renal system anatomy / physiology Discuss common medical / trauma renal issues Identify associated assessment keys GOALS Introduction
My Bloody Talk. Dr Ben Turner MBBS, FANZCA, FCICM The Royal Children s Hospital, Melbourne
 My Bloody Talk Dr Ben Turner MBBS, FANZCA, FCICM The Royal Children s Hospital, Melbourne Disclosures No conflicts of interest Interest in conflict Blood transfusion Massive transfusion definitions Transfusion
My Bloody Talk Dr Ben Turner MBBS, FANZCA, FCICM The Royal Children s Hospital, Melbourne Disclosures No conflicts of interest Interest in conflict Blood transfusion Massive transfusion definitions Transfusion
TXA. Things Change. Tranexamic Acid TXA. Resuscitation 2017 TXA In The ED March 31, MAST Trousers. High Flow IV Fluids.
 Resuscitation 2017 In The ED March 31, 2017 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN SECURE THE ABC S MAST
Resuscitation 2017 In The ED March 31, 2017 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN SECURE THE ABC S MAST
Massive Transfusion Initiation & Implication
 Massive Transfusion Initiation & Implication Katayoun Fayaz MD Blood Bank Medical Director Northwell Health April 2017 Trauma Statistics/Facts Each year trauma accounts for 41 million emergency department
Massive Transfusion Initiation & Implication Katayoun Fayaz MD Blood Bank Medical Director Northwell Health April 2017 Trauma Statistics/Facts Each year trauma accounts for 41 million emergency department
Michael Avant, M.D. The Children s Hospital of GHS
 Michael Avant, M.D. The Children s Hospital of GHS OVERVIEW ER to ICU Transition Early Management Priorities the First 48 hours Organ System Support Complications THE FIRST 48 HOURS Communication Damage
Michael Avant, M.D. The Children s Hospital of GHS OVERVIEW ER to ICU Transition Early Management Priorities the First 48 hours Organ System Support Complications THE FIRST 48 HOURS Communication Damage
Major Haemorrhage Protocol. Commentary
 Hairmyres Hospital Monklands Hospital Wishaw General Hospital Major Haemorrhage Protocol Commentary N.B. There is a separate NHSL protocol for the Management of Obstetric Haemorrhage Authors Dr Tracey
Hairmyres Hospital Monklands Hospital Wishaw General Hospital Major Haemorrhage Protocol Commentary N.B. There is a separate NHSL protocol for the Management of Obstetric Haemorrhage Authors Dr Tracey
Transfusion Pitfalls. Objectives. Packed Red Blood Cells. TRICC trial (subgroups): Is transfusion always good? Components
: Is transfusion always good? Components") Objectives Transfusion Pitfalls Gregory W. Hendey, MD, FACEP Professor and Chief UCSF Fresno, Emergency Medicine To list risks and benefits of various blood products To discuss controversy over liberal
Objectives Transfusion Pitfalls Gregory W. Hendey, MD, FACEP Professor and Chief UCSF Fresno, Emergency Medicine To list risks and benefits of various blood products To discuss controversy over liberal
PUZZLE. EARLY IMPACT ALS Jamie Syrett, MD Director of Prehospital Care Rochester General Health System PUZZLE THINKING OUTSIDE THE BOX! EARLY IMPACT?
 PUZZLE EARLY IMPACT ALS Jamie Syrett, MD Director of Prehospital Care Rochester General Health System PUZZLE THINKING OUTSIDE THE BOX! EARLY IMPACT? IV ACCESS? What things do we do that make a difference?
PUZZLE EARLY IMPACT ALS Jamie Syrett, MD Director of Prehospital Care Rochester General Health System PUZZLE THINKING OUTSIDE THE BOX! EARLY IMPACT? IV ACCESS? What things do we do that make a difference?
What is. InSpectra StO 2?
 What is InSpectra StO 2? www.htibiomeasurement.com What is InSpectra StO 2? Hemoglobin O 2 saturation is measured in three areas: 1) Arterial (SaO 2, SpO 2 ) Assesses how well oxygen is loading onto hemoglobin
What is InSpectra StO 2? www.htibiomeasurement.com What is InSpectra StO 2? Hemoglobin O 2 saturation is measured in three areas: 1) Arterial (SaO 2, SpO 2 ) Assesses how well oxygen is loading onto hemoglobin
VanderbiltEM.com. Prehospital STEMIs. EMS Today 2018 Research That Should Be On Your Radar Screen 3/1/2018
 EMS Today 2018 Research That Should Be On Your Radar Screen Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN VanderbiltEM.com
EMS Today 2018 Research That Should Be On Your Radar Screen Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN VanderbiltEM.com
HYPOVOLEMIA AND HEMORRHAGE UPDATE ON VOLUME RESUSCITATION HEMORRHAGE AND HYPOVOLEMIA DISTRIBUTION OF BODY FLUIDS 11/7/2015
 UPDATE ON VOLUME RESUSCITATION HYPOVOLEMIA AND HEMORRHAGE HUMAN CIRCULATORY SYSTEM OPERATES WITH A SMALL VOLUME AND A VERY EFFICIENT VOLUME RESPONSIVE PUMP. HOWEVER THIS PUMP FAILS QUICKLY WITH VOLUME
UPDATE ON VOLUME RESUSCITATION HYPOVOLEMIA AND HEMORRHAGE HUMAN CIRCULATORY SYSTEM OPERATES WITH A SMALL VOLUME AND A VERY EFFICIENT VOLUME RESPONSIVE PUMP. HOWEVER THIS PUMP FAILS QUICKLY WITH VOLUME
Thicker than Water. Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago
 Thicker than Water Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago I have no relevant financial relationships to disclose. Who is bleeding? How much and what kind
Thicker than Water Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago I have no relevant financial relationships to disclose. Who is bleeding? How much and what kind
anesthesia & mass casualty events
 anesthesia & mass casualty events marc p steurer, md, desa president, trauma anesthesiology society (www.tashq.org) director, trauma anesthesiology UCSF/ SFGH associate professor UCSF faculty disclosure
anesthesia & mass casualty events marc p steurer, md, desa president, trauma anesthesiology society (www.tashq.org) director, trauma anesthesiology UCSF/ SFGH associate professor UCSF faculty disclosure
Components of Blood. N26 Blood Administration 4/24/2012. Cabrillo College ADN/C. Madsen RN, MSN 1. Formed elements Cells. Plasma. What can we give?
 Components of Blood Formed elements Cells Erythrocytes (RBCs) Leukocytes (WBCs) Thrombocytes (platelets) Plasma 90% water 10% solutes Proteins, clotting factors 1 What can we give? Whole blood Packed RBC
Components of Blood Formed elements Cells Erythrocytes (RBCs) Leukocytes (WBCs) Thrombocytes (platelets) Plasma 90% water 10% solutes Proteins, clotting factors 1 What can we give? Whole blood Packed RBC
Sign up to receive ATOTW weekly
 MANAGEMENT OF MAJOR HAEMORRHAGE PART ONE: INITIAL RESPONSE ANAESTHESIA TUTORIAL OF THE WEEK 136 1 ST JUNE 2009 Katrina Webster (Senior Registrar in Anaesthesia) Royal Hobart Hospital, Tasmania, Australia.
MANAGEMENT OF MAJOR HAEMORRHAGE PART ONE: INITIAL RESPONSE ANAESTHESIA TUTORIAL OF THE WEEK 136 1 ST JUNE 2009 Katrina Webster (Senior Registrar in Anaesthesia) Royal Hobart Hospital, Tasmania, Australia.
WHAT S NEW-ISH IN ARDS MANAGEMENT AFTER TRAUMA?
 WHAT S NEW-ISH IN ARDS MANAGEMENT AFTER TRAUMA? Bryce Robinson MD, MS, FACS, FCCM Associate Professor of Surgery Associate Medical Director, Critical Care Harborview Medical Center Department of Surgery
WHAT S NEW-ISH IN ARDS MANAGEMENT AFTER TRAUMA? Bryce Robinson MD, MS, FACS, FCCM Associate Professor of Surgery Associate Medical Director, Critical Care Harborview Medical Center Department of Surgery
EMSS17: Bleeding patients course material
 EMSS17: Bleeding patients course material Introduction During the bleeding patients workshop at the Emergency Medicine Summer School 2017 (EMSS17) you will learn how to assess and treat bleeding patients
EMSS17: Bleeding patients course material Introduction During the bleeding patients workshop at the Emergency Medicine Summer School 2017 (EMSS17) you will learn how to assess and treat bleeding patients
Adult Trauma Advances in Pediatrics. (sometimes they are little adults) FAST examination. Who is bleeding? How much and what kind of TXA volume?
 FAST examination. Who is bleeding? How much and what kind of TXA volume?") Adult Trauma Advances in Pediatrics (sometimes they are little adults) Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago Alisa McQueen MD, FAAP, FACEP Associate
Adult Trauma Advances in Pediatrics (sometimes they are little adults) Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago Alisa McQueen MD, FAAP, FACEP Associate
High Risk + Challenging Trauma Cases. Hawaii. Topics 1/27/2014. David Thompson, MD, MPH. Head injury in the anticoagulated patient.
 High Risk + Challenging Trauma Cases David Thompson, MD, MPH Hawaii Topics Head injury in the anticoagulated patient Shock recognition Case 1: Head injury HPI: 57 yo male w/ PMH atrial fibrillation, on
High Risk + Challenging Trauma Cases David Thompson, MD, MPH Hawaii Topics Head injury in the anticoagulated patient Shock recognition Case 1: Head injury HPI: 57 yo male w/ PMH atrial fibrillation, on
DAMAGE CONTROL RESUSCITATION
 DAMAGE CONTROL RESUSCITATION Chapter 4 Contributing Authors Jeremy G. Perkins, MD, FACP, LTC, MC, US Army Alec C. Beekley, MD, FACS, LTC, MC, US Army All figures and tables included in this chapter have
DAMAGE CONTROL RESUSCITATION Chapter 4 Contributing Authors Jeremy G. Perkins, MD, FACP, LTC, MC, US Army Alec C. Beekley, MD, FACS, LTC, MC, US Army All figures and tables included in this chapter have
Department of Pediatrics, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok 10700, Thailand.
 SIRIRAJ MEDICAL LIBRARY SpecialIssue Clinical Practice Guide for the Management of Dengue Hemorrhagic Fever (DHF), Siriraj Hospital Kulkanya Chokephaibulkit, M.D., Wanee Wisuthsarewong, M.D., Gavivann
SIRIRAJ MEDICAL LIBRARY SpecialIssue Clinical Practice Guide for the Management of Dengue Hemorrhagic Fever (DHF), Siriraj Hospital Kulkanya Chokephaibulkit, M.D., Wanee Wisuthsarewong, M.D., Gavivann
Heme (Bleeding and Coagulopathies) in the ICU
 in the ICU") Heme (Bleeding and Coagulopathies) in the ICU General Topics To Discuss Transfusions DIC Thrombocytopenia Liver and renal disease related bleeding Lack of evidence in managing critical illness related
Heme (Bleeding and Coagulopathies) in the ICU General Topics To Discuss Transfusions DIC Thrombocytopenia Liver and renal disease related bleeding Lack of evidence in managing critical illness related
Sepsis Awareness and Education
 Sepsis Awareness and Education Meets the updated New York State Department of Health (NYSDOH) requirements for Infection Control and Barrier Precautions coursework Element VII: Sepsis Awareness and Education
Sepsis Awareness and Education Meets the updated New York State Department of Health (NYSDOH) requirements for Infection Control and Barrier Precautions coursework Element VII: Sepsis Awareness and Education
10/4/2018. Nothing to Disclose. Liz Robertson, MD FACS October 5, 2018 Steven R. Hall Trauma Symposium Big Cedar Lodge, MO
 Nothing to Disclose Liz Robertson, MD FACS October 5, 2018 Steven R. Hall Trauma Symposium Big Cedar Lodge, MO History of IV Resuscitation Review of Data for Fluid Strategies Historical Examples of IV
Nothing to Disclose Liz Robertson, MD FACS October 5, 2018 Steven R. Hall Trauma Symposium Big Cedar Lodge, MO History of IV Resuscitation Review of Data for Fluid Strategies Historical Examples of IV
Shock and Trauma Resuscitation
 Shock and Trauma Resuscitation Bonjo Batoon, MS, CRNA Bbatoon@som.umaryland.edu Disclaimer Resuscitation is continuously evolving There is no one right way Knowing is half the battle G.I. Joe Having to
Shock and Trauma Resuscitation Bonjo Batoon, MS, CRNA Bbatoon@som.umaryland.edu Disclaimer Resuscitation is continuously evolving There is no one right way Knowing is half the battle G.I. Joe Having to
What s in the Massive Transfusion Protocol (MTP) Package?
 Package?") What s in the Massive Transfusion Protocol (MTP) Package? The Massive Transfusion Protocol Package is a set of documents intended to improve the coordination of a Massive Transfusion Protocol. The kit
What s in the Massive Transfusion Protocol (MTP) Package? The Massive Transfusion Protocol Package is a set of documents intended to improve the coordination of a Massive Transfusion Protocol. The kit
Major Haemorrhage Transfusion Pathway
 Major Haemorrhage Transfusion Pathway SENIOR CLINICIAN ASSESSMENT: DECLARES MAJOR HAEMORRHAGE ( Call for help ( Telephone via switchboard: Consultant or Senior Clinician Duty Anaesthetist Porters (if will
Major Haemorrhage Transfusion Pathway SENIOR CLINICIAN ASSESSMENT: DECLARES MAJOR HAEMORRHAGE ( Call for help ( Telephone via switchboard: Consultant or Senior Clinician Duty Anaesthetist Porters (if will
2012, Görlinger Klaus
 Gerinnungsmanagement der Gegenwart - wie gehen wir heute vor? 25. Allander Gerinnungsrunde am 15. März 2012 Klaus Görlinger Universitätsklinikum Essen klaus@goerlinger.net CSL Behring GmbH Octapharma AG
Gerinnungsmanagement der Gegenwart - wie gehen wir heute vor? 25. Allander Gerinnungsrunde am 15. März 2012 Klaus Görlinger Universitätsklinikum Essen klaus@goerlinger.net CSL Behring GmbH Octapharma AG
STORMY DENGUE with bloody problems. Anand M.Patil PICU MED/SURG TEAM Apollo Childrens Hospitals Chennai
 STORMY DENGUE with bloody problems Anand M.Patil PICU MED/SURG TEAM Apollo Childrens Hospitals Chennai 1 HISTORY 4 ½ years girl Day 1: Fever, Lethargy, Low urine output Hypotension, high PCV,low platelets
STORMY DENGUE with bloody problems Anand M.Patil PICU MED/SURG TEAM Apollo Childrens Hospitals Chennai 1 HISTORY 4 ½ years girl Day 1: Fever, Lethargy, Low urine output Hypotension, high PCV,low platelets
Disclosure Chair of ACS COT EMS Committee Authored Evidence Based Prehospital Guideline for External Hemorrhage Control
 Eileen M. Bulger, MD Professor of Surgery, Chief of Trauma Harborview Medical Center University of Washington Disclosure Chair of ACS COT EMS Committee Authored Evidence Based Prehospital Guideline for
Eileen M. Bulger, MD Professor of Surgery, Chief of Trauma Harborview Medical Center University of Washington Disclosure Chair of ACS COT EMS Committee Authored Evidence Based Prehospital Guideline for
CrackCast Episode 7 Blood and Blood Components
 CrackCast Episode 7 Blood and Blood Components Episode Overview: 1) Describe the 3 categories of blood antigens 2) Who is the universal donor and why? 3) Define massive transfusion 4) List 5 physiologic
CrackCast Episode 7 Blood and Blood Components Episode Overview: 1) Describe the 3 categories of blood antigens 2) Who is the universal donor and why? 3) Define massive transfusion 4) List 5 physiologic
Administration of blood components. Tina Parker - Transfusion Practitioner
 . Administration of blood components Tina Parker - Transfusion Practitioner Red Cells Each unit contains 250-350mls Preserved with glucose and Mannitol to keep the correct tension Lasts 35 days from midnight
. Administration of blood components Tina Parker - Transfusion Practitioner Red Cells Each unit contains 250-350mls Preserved with glucose and Mannitol to keep the correct tension Lasts 35 days from midnight
The Septic Patient. Dr Arunraj Navaratnarajah. Renal SpR Imperial College NHS Healthcare Trust
 The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
John Park, MD Assistant Professor of Medicine
 John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014
 December 17, 2014") Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014 Presenters Mark Blaney, RN Regional Nurse Educator CHI Franciscan Health Karen Lautermilch Director, Quality & Performance
Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014 Presenters Mark Blaney, RN Regional Nurse Educator CHI Franciscan Health Karen Lautermilch Director, Quality & Performance
Written 01/09/17 Rewritten 3/29/17 for Interior Regional EMS Symposium
 Written 01/09/17 Rewritten 3/29/17 for Interior Regional EMS Symposium MARIA E. MANDICH MD Fairbanks Memorial Hospital Emergency Department Attending Physician Interior Region EMS Council Medical Director
Written 01/09/17 Rewritten 3/29/17 for Interior Regional EMS Symposium MARIA E. MANDICH MD Fairbanks Memorial Hospital Emergency Department Attending Physician Interior Region EMS Council Medical Director
Kristan Staudenmayer, MD Stanford University, Stanford, CA
 Kristan Staudenmayer, MD Stanford University, Stanford, CA Fluid resuscitation Variety of fluids How to administer What you do DOES matter WWII 1942 North Africa high mortality from hemorrhaghic shock
Kristan Staudenmayer, MD Stanford University, Stanford, CA Fluid resuscitation Variety of fluids How to administer What you do DOES matter WWII 1942 North Africa high mortality from hemorrhaghic shock
Scenario #4A: Geriatric Trauma Resuscitation Version-5
 Scenario #4A: Geriatric Trauma Resuscitation Version-5 Goals & Objectives: 1. Discuss the principles of initial assessment of a geriatric trauma patient. 2. Recognize physiologic and anatomic changes that
Scenario #4A: Geriatric Trauma Resuscitation Version-5 Goals & Objectives: 1. Discuss the principles of initial assessment of a geriatric trauma patient. 2. Recognize physiologic and anatomic changes that
Effective Date: Approved by: Laboratory Director, Jerry Barker (electronic signature)
") 1 of 5 Policy #: 702 (PHL-702-05) Effective Date: 9/30/2004 Reviewed Date: 8/1/2016 Subject: TRANSFUSION GUIDELINES Approved by: Laboratory Director, Jerry Barker (electronic signature) Approved by: Laboratory
1 of 5 Policy #: 702 (PHL-702-05) Effective Date: 9/30/2004 Reviewed Date: 8/1/2016 Subject: TRANSFUSION GUIDELINES Approved by: Laboratory Director, Jerry Barker (electronic signature) Approved by: Laboratory
Prehospital Resuscitation for the 21 st Century Simulation Case. VF/Asystole
 Prehospital Resuscitation for the 21 st Century Simulation Case VF/Asystole Case History 1 (hypovolemic cardiac arrest secondary to massive upper GI bleed) 56 year-old male patient who fainted in the presence
Prehospital Resuscitation for the 21 st Century Simulation Case VF/Asystole Case History 1 (hypovolemic cardiac arrest secondary to massive upper GI bleed) 56 year-old male patient who fainted in the presence
APPROACH TO TRAUMA CARE
 APPROACH TO TRAUMA CARE Timothy Murray, RN, CFRN Jan 2017 OBJECTIVES Demonstrate Concepts of Primary and Secondary Patient Assessment Establish Management Priorities in Trauma Situations Initiating Interventions
APPROACH TO TRAUMA CARE Timothy Murray, RN, CFRN Jan 2017 OBJECTIVES Demonstrate Concepts of Primary and Secondary Patient Assessment Establish Management Priorities in Trauma Situations Initiating Interventions
2/2/2011. Blood Components and Transfusions. Why Blood Transfusion?
 Blood Components and Transfusions Describe blood components Identify nursing responsibilities r/t blood transfusion Discuss factors r/t blood transfusion including blood typing, Rh factor, and cross matching
Blood Components and Transfusions Describe blood components Identify nursing responsibilities r/t blood transfusion Discuss factors r/t blood transfusion including blood typing, Rh factor, and cross matching
GUIDANCE DOCUMENT FOR MASSIVE HEMORRHAGE MANAGEMENT IN ADULTS
 GUIDANCE DOCUMENT FOR MASSIVE HEMORRHAGE MANAGEMENT IN ADULTS 1.0 Definitions & Acronyms 1.1 Massive Hemorrhage Event (MHE): Transfusion of a volume of blood components equivalent to a patient s estimated
GUIDANCE DOCUMENT FOR MASSIVE HEMORRHAGE MANAGEMENT IN ADULTS 1.0 Definitions & Acronyms 1.1 Massive Hemorrhage Event (MHE): Transfusion of a volume of blood components equivalent to a patient s estimated
Frank Sebat, MD - June 29, 2006
 Types of Shock Hypovolemic Shock Low blood volume decreasing cardiac output. AN INTEGRATED SYSTEM OF CARE FOR PATIENTS AT RISK SHOCK TEAM and RAPID RESPONSE TEAM Septic or Distributive Shock Decrease in
Types of Shock Hypovolemic Shock Low blood volume decreasing cardiac output. AN INTEGRATED SYSTEM OF CARE FOR PATIENTS AT RISK SHOCK TEAM and RAPID RESPONSE TEAM Septic or Distributive Shock Decrease in
No Disclosures OBJECTIVES. Damage Control Resuscitation Lessons Learned and the Way Forward After More Than a Decade of War
 Damage Control Resuscitation Lessons Learned and the Way Forward After More Than a Decade of War No Disclosures COL(ret) Michael M. Woll, MD, FACS Surgical Det. A, 249 th General Hospital 28 th Combat
Damage Control Resuscitation Lessons Learned and the Way Forward After More Than a Decade of War No Disclosures COL(ret) Michael M. Woll, MD, FACS Surgical Det. A, 249 th General Hospital 28 th Combat
Damage Control Resuscitation
 Damage Control Resuscitation H M Cassimjee Critical Care Specialist Department of Critical Care & Level 1 Trauma Unit Inkosi Albert Luthuli Central Hospital Damage Control Resuscitation only for DAMAGED
Damage Control Resuscitation H M Cassimjee Critical Care Specialist Department of Critical Care & Level 1 Trauma Unit Inkosi Albert Luthuli Central Hospital Damage Control Resuscitation only for DAMAGED
State of Florida Hypothermia Protocol. Michael D. Weiss, M.D. Associate Professor of Pediatrics Division of Neonatology
 State of Florida Hypothermia Protocol Michael D. Weiss, M.D. Associate Professor of Pediatrics Division of Neonatology I. Entry Criteria 1. Gestational Age greater than or equal to 35 weeks gestation
State of Florida Hypothermia Protocol Michael D. Weiss, M.D. Associate Professor of Pediatrics Division of Neonatology I. Entry Criteria 1. Gestational Age greater than or equal to 35 weeks gestation
Case year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50
 Case 1 65 year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50 Case 1 65 year old female nursing home resident with
Case 1 65 year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50 Case 1 65 year old female nursing home resident with
IDS. Pediatric Donor Management
 IDS Guidelines for Clinical Management of Organ Donors: Weight < 40 kg Organ Perfusion & Hormonal Replacement Guidelines: Normal HR, SBP: (see chart below) Urinary output of 1-3 cc/kg/hr CVP 6-10 mmhg
IDS Guidelines for Clinical Management of Organ Donors: Weight < 40 kg Organ Perfusion & Hormonal Replacement Guidelines: Normal HR, SBP: (see chart below) Urinary output of 1-3 cc/kg/hr CVP 6-10 mmhg
Sepsis and Shock States
 Sepsis and Shock States Presented By: Cynthia Webner BSN, RN, CCRN, CMC www.cardionursing.com CNEA 2009 1 INFECTION Inflammatory response to microorganisms, or Invasion of normally sterile tissues SYSTEMIC
Sepsis and Shock States Presented By: Cynthia Webner BSN, RN, CCRN, CMC www.cardionursing.com CNEA 2009 1 INFECTION Inflammatory response to microorganisms, or Invasion of normally sterile tissues SYSTEMIC
COUNTY OF SACRAMENTO EMERGENCY MEDICAL SERVICES AGENCY
 COUNTY OF SACRAMENTO EMERGENCY MEDICAL SERVICES AGENCY Document # 8024.31 PROGRAM DOCUMENT: Initial Date: 10/26/94 Cardiac Dysrhythmias Last Approval Date: 11/01/16 Effective Date: 11/01/18 Next Review
COUNTY OF SACRAMENTO EMERGENCY MEDICAL SERVICES AGENCY Document # 8024.31 PROGRAM DOCUMENT: Initial Date: 10/26/94 Cardiac Dysrhythmias Last Approval Date: 11/01/16 Effective Date: 11/01/18 Next Review
Does a Controlled Fluid Resuscitation Strategy Decrease Mortality in Trauma Patients?
 Does a Controlled Fluid Resuscitation Strategy Decrease Mortality in Trauma Patients? death Haemorrhage remains the biggest killer of major trauma patients Expected deaths will increase to 8 million/year
Does a Controlled Fluid Resuscitation Strategy Decrease Mortality in Trauma Patients? death Haemorrhage remains the biggest killer of major trauma patients Expected deaths will increase to 8 million/year
Emergency Blood and Massive Transfusion: The Surgeon s Perspective. Transfusion Medicine Update September 16 17, 2009
 Transfusion Medicine Update September 16 17, 2009 Mandip S. Atwal, D.O. FACOS Carl M. Pesta, D.O. FACOS Agenda History Hemorrhagic shock Transfusion is Bad Transfusion Prevention Transfusion The Red Chest
Transfusion Medicine Update September 16 17, 2009 Mandip S. Atwal, D.O. FACOS Carl M. Pesta, D.O. FACOS Agenda History Hemorrhagic shock Transfusion is Bad Transfusion Prevention Transfusion The Red Chest
Contents. Version 1.0: 01/02/2010 Protocol# ISRCTN Page 1 of 7
 Contents 1. INTRODUCTION... 2 2. STUDY SYNOPSIS... 2 3. STUDY OBJECTIVES... 2 3.1. Primary Objective... 2 3.2. Secondary Objectives... 2 3.3. Assessment of Objectives... 3 3.4. Change the Primary Objective
Contents 1. INTRODUCTION... 2 2. STUDY SYNOPSIS... 2 3. STUDY OBJECTIVES... 2 3.1. Primary Objective... 2 3.2. Secondary Objectives... 2 3.3. Assessment of Objectives... 3 3.4. Change the Primary Objective
CUTTING EDGE DECOMPRESSION. A new approach to thoracostomy, p. 26. DRUG WAR Medics p. 38 NECK Trauma p. 50 TRAUMA S Lethal Triad p.
 NITROUS Oxide p. 34 DRUG WAR Medics p. 38 NECK Trauma p. 50 TRAUMA S Lethal Triad p. 56 APRIL 2014 CUTTING EDGE DECOMPRESSION A new approach to thoracostomy, p. 26 Always En Route At Hypothermia, acidosis
NITROUS Oxide p. 34 DRUG WAR Medics p. 38 NECK Trauma p. 50 TRAUMA S Lethal Triad p. 56 APRIL 2014 CUTTING EDGE DECOMPRESSION A new approach to thoracostomy, p. 26 Always En Route At Hypothermia, acidosis
Printed copies of this document may not be up to date, obtain the most recent version from
 Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Shruti Dholakia L Chigaru Author Position Fellow CATS Consultant Document Owner E. Polke Document
Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Shruti Dholakia L Chigaru Author Position Fellow CATS Consultant Document Owner E. Polke Document
Damage Control in Abdominal and Pelvic Injuries
 Damage Control in Abdominal and Pelvic Injuries Raul Coimbra, MD, PhD, FACS The Monroe E. Trout Professor of Surgery Surgeon-in Chief UCSD Medical Center Hillcrest Campus Executive Vice-Chairman Department
Damage Control in Abdominal and Pelvic Injuries Raul Coimbra, MD, PhD, FACS The Monroe E. Trout Professor of Surgery Surgeon-in Chief UCSD Medical Center Hillcrest Campus Executive Vice-Chairman Department
Hematology Review. CCRN exam. The Coagulation Cascade. The Coagulation Cascade. Components include: Intrinsic pathway Extrinsic pathway Common pathway
 CCRN exam Hematology Review CCRN Review October 2013 Department of Critical Care Nursing Hematology is 2% of the exam Focus on coagulation cascade, DIC, and HIT Anatomy of the hematologic system Bone marrow
CCRN exam Hematology Review CCRN Review October 2013 Department of Critical Care Nursing Hematology is 2% of the exam Focus on coagulation cascade, DIC, and HIT Anatomy of the hematologic system Bone marrow
MASSIVE TRANSFUSION PROTOCOL
 MASSIVE TRANSFUSION PROTOCOL IF YOU ANTICIPATE EMERGENT NEED FOR LARGE AMOUNTS OF BLOOD IN A SHORT PERIOD OF TIME Call Blood Bank: 6622121 Tell them you have a patient who needs a Massive Transfusion and
MASSIVE TRANSFUSION PROTOCOL IF YOU ANTICIPATE EMERGENT NEED FOR LARGE AMOUNTS OF BLOOD IN A SHORT PERIOD OF TIME Call Blood Bank: 6622121 Tell them you have a patient who needs a Massive Transfusion and
Pediatric emergencies (SHOCK & COMA) Dr Mubarak Abdelrahman Assistant Professor Jazan University
 Dr Mubarak Abdelrahman Assistant Professor Jazan University") Pediatric emergencies (SHOCK & COMA) Dr Mubarak Abdelrahman Assistant Professor Jazan University SHOCK Definition: Shock is a syndrome = inability to provide sufficient oxygenated blood to tissues. Oxygen
Pediatric emergencies (SHOCK & COMA) Dr Mubarak Abdelrahman Assistant Professor Jazan University SHOCK Definition: Shock is a syndrome = inability to provide sufficient oxygenated blood to tissues. Oxygen
CHILL OUT! Induced Hypothermia: Challenges & Successes in the
 CHILL OUT! Induced Hypothermia: Challenges & Successes in the ICU Colleen Bell RN, BS, CCRN, Donna Brault RN, BSN, CCRN, Cathy Patnode RN, BSN, CCRN Champlain Valley Physician Hospital November 2012 Objectives
CHILL OUT! Induced Hypothermia: Challenges & Successes in the ICU Colleen Bell RN, BS, CCRN, Donna Brault RN, BSN, CCRN, Cathy Patnode RN, BSN, CCRN Champlain Valley Physician Hospital November 2012 Objectives
Case Scenario 3: Shock and Sepsis
 Name: Molly Boyle 1. Define the term shock (Lewis textbook): Shock is a syndrome characterized by decreased perfusion and impaired metabolism. Shock can have a number of causes that result in damage to
Name: Molly Boyle 1. Define the term shock (Lewis textbook): Shock is a syndrome characterized by decreased perfusion and impaired metabolism. Shock can have a number of causes that result in damage to
Massive Transfusion. MPQC Spring Summit April 29, Roger Belizaire MD PhD
 Massive Transfusion MPQC Spring Summit April 29, 2015 Roger Belizaire MD PhD Take home points 1. Blood is always available. Requests for massive transfusion or emergency release typically only require
Massive Transfusion MPQC Spring Summit April 29, 2015 Roger Belizaire MD PhD Take home points 1. Blood is always available. Requests for massive transfusion or emergency release typically only require
23/10/2011. Case One: Mrs. B. Mrs. B., 36 year old, 30 weeks pregnant, 2 nd baby Blood type A negative Belted driver of minivan, struck a parked car
 GETTING IT BLOODY RIGHT: CHOOSING THE BEST PRODUCT Kathleen Eckert, ART, Transfusion Safety Officer, LHSC Brenda Morgan, RN BScN MSc, CNS, Critical Care, Victoria Hospital, LHSC http://www.transfusionontario.org/public-en/public.php
GETTING IT BLOODY RIGHT: CHOOSING THE BEST PRODUCT Kathleen Eckert, ART, Transfusion Safety Officer, LHSC Brenda Morgan, RN BScN MSc, CNS, Critical Care, Victoria Hospital, LHSC http://www.transfusionontario.org/public-en/public.php
9/13/2015. Laboratory. HPI and PE
 Critical Care HPI and PE 74 yo male confused SBP 90/20 MAP50, P 122, RR 34 Ox1 w/o nuchal rigidity S1S2 wo m RLL reduced breath sounds Skin warm dry Laboratory» WBC 15,600 Hgb 8.4 HCt 23%, Plts 95000,
Critical Care HPI and PE 74 yo male confused SBP 90/20 MAP50, P 122, RR 34 Ox1 w/o nuchal rigidity S1S2 wo m RLL reduced breath sounds Skin warm dry Laboratory» WBC 15,600 Hgb 8.4 HCt 23%, Plts 95000,
Introduction. Invasive Hemodynamic Monitoring. Determinants of Cardiovascular Function. Cardiovascular System. Hemodynamic Monitoring
 Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained
Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained