Managing Coagulopathy in Intensive Care Setting
|
|
|
- Kathleen Patterson
- 5 years ago
- Views:
Transcription
1 Managing Coagulopathy in Intensive Care Setting Dr Rock LEUNG Associate Consultant Division of Haematology, Department of Pathology & Clinical Biochemistry Queen Mary Hospital
2 Normal Haemostasis Primary Haemostasis Vessels Platelets Von Willebrand Factos Coagulation Clotting factors In vivo vs In vitro
3 When Problem Occurs Quantitative more than qualitative For examples, thrombocytopenia more common than platelets dysfunction Acquired more than congenital
4 Quantitative Problem Productive defect Increased consumption Loss Dilution Lysis Pool
5 Qualitative Problems Inhibitory Inactivation Functional
6
7 IDEAL laboratory findings (only what is expected to see), patterns not always reproducible
8 Principles The first principle of the management of coagulopathies in critical care is to avoid the correction of laboratory abnormalities with blood components / products unless there is a clinical bleeding problem, a surgical procedure is required or both. If bleeding occurs, identify local factors; if bleeding general, identify underlying coagulation abnormalities. Don t let the vicious cycle of coagulopathy set in.
9 Common Scenarios Current State-of-the-Art Major bleeding Haemostatic support for invasive procedures Disseminated Intravascular Coagulation Thrombocytopenia Bleeding associated with antithrombotic drug ECMO related coagulopathy
10 Major bleeding Massive transfusion Replacement of one blood volume in 24 hours Transfusion of > 4 RBC units within 1 hour when ongoing need is foreseeable Replacement of 50% of total blood volume within 3 hours
11 Pathophysiology of Major Bleeding Cellular components in blood RBC s Rheological effect of RBC s on margination of platelets RBC s modulates biochemical & functional responsiveness of activated platelets. Platelets Dilutional thrombocytopenia Consumption Acquired platelet dysfunction No functional platelets in transfused RBC s Coagulation factors Dilutional Consumption Disseminated intravascular coagulation (D.I.C.)
12 Pathophysiology of Major Bleeding Haemodilution Crystalloids & colloids Dilutional effect Some colloids may influence primary haemostasis & coagulation Hypothermia Body temperature <35 C Affects platelet function Slows coagulation Increases fibrinolysis
13 Trauma Transfusion Initial data from military setting; automatically related to hospital trauma setting, & even non-trauma setting (e.g., obstetric). Promulgation of early plasma / platelets transfusion at a higher ratios with with reference to red cells to prevent the vicious cycle. Supported by clinical observational study (PROMMTT study) Favored by randomized clinical trials (PROPPR study) Time-varying ratios observed with greater ratio in the first 6 hours after injury associated with lower patient mortality (Efficient transfusion in the first few hours is important). Use of tranexamic acid as soon as possible (within 3 hours after injury) for trauma patients with bleeding or at risk for major bleedings (CRASH-2 trial).




 Effective communication Central Porter Center")
14 QMH Trauma Transfusion Protocol: More than a ratio No enforcement in 1:1: 1 package Provide alternative activation pathway, i.e., by clinical decision Protocolized approach Efficiency of delivery of blood component 1. Portering system Designated porter (They are really fast!) Lift-holding by security 2. Special blood bank service pledges (We are committed!) Effective communication Central Porter Center designated phoneline: 6666 Documenting the handover Porter keep updated of the patient s transfer status
15 Activation-to-Type & Screen Completion time T&S completion time from TTP activation (minutes) T&S completion time (Mean 38 min, range min) Pledge of T&S completion: min Case number Case 1 & 8: T&S sample arrived before activation Case 11: Failed resuscitation at A&E Case 12: Step down 2 minutes after activation (All four cases were excluded for time study)
16 Activation-to-FFP Thawing Completion Time & Activation-to-FFP Issue Time Time from TTP activation (minutes) Activation-to-FFP thawing completion time (mean 22 min, range min) Activation-to-FFP issue time (mean 25 min, range 5-49 min) Pledge of FFP thawing is 30 min B NC B B NC Case number (batch number) ID NC ID C ID NC FFP thawed FFP collection B = thawed component already available C = cancel request NC = not collected ID = improper documentation
17 Restricted Transfusion for Acute GI Bleeding Patients with acute upper gastrointestinal bleeding who were treated with restrictive strategy (<7g/dl) had longer survival (6 weeks) and a lower rate of rebleeding than did those who were treated with liberal strategy (<9 g/dl) Transfusion may counteract the splanchnic vasoconstrictive response due to hypovolaemia, increase the splanchnic blood flow and pressure and impair the formation of blood clot. Transfusion Strategies for Acute Upper Gastrointestinal Bleeding N Engl J Med 2013; 368:11-21 Trials on tranexamic acid in progress (HALT-IT)
18 Before Invasive Procedures There is no supportive evidence for the prophylactic use if FFP to correct abnormal results on coagulation screening Coagulation screening has no predictive value for later bleeding Generally, INR below 1.5 is considered safe Vitamin K deficiency should not be undertreated
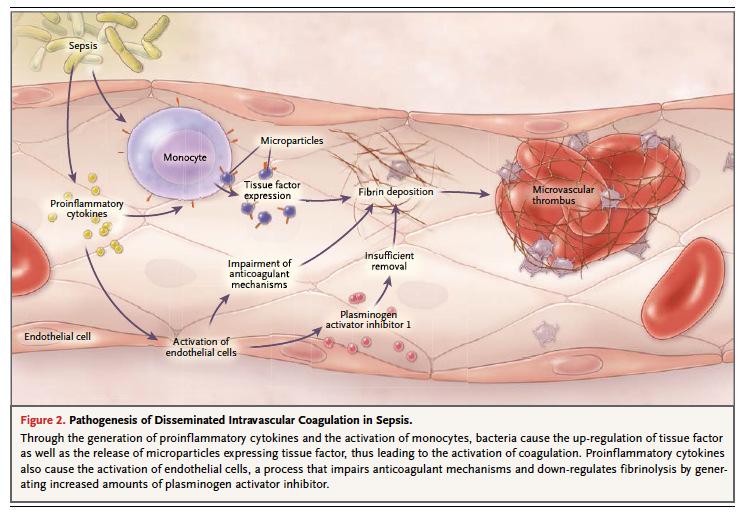
19 DIC
20 To score or not to score Diagnosis of DIC should only be made in the right clinical context Its diagnosis makes little difference to the management strategy unless patient bleeds & transfusion support is the only option based on current evidence RCT on pharmacological doses of protein C, antithrombin & tissue pathway inhibitor showed discouraging results Antifibrinolytic contraindicated and heparin risky
21 Thrombocytopenia Rule out pseudothrombocytopenia. Often multifactorial in ICU setting. Urgent & life-threatening causes: HIT, TTP. Platelet refractoriness in patients at risk: CCI (corrected count increment) for diagnosis, HLA-matched platelets as treatment. Platelet transfusion trigger Prophylactic vs Therapeutic Lowest threshold for prophylactic transfusion (mostly taken as 10 x 10^/L), limited by the precision of platelet count generated by automated haematology analyzers. Autoimmune thrombocytopenic pupura is no longer a diagnosis of exclusion.
22
23 When is laboratory monitoring for Target- Specific Oral Anticoagulant (TACO) indicated? To identify the mechanism of bleeding To detect overdose or drug accumulation Renal impairment Liver impairment Elderly To determine the offset of activity Pre-operative Before thrombolysis for ischaemic stroke To monitor adherence To distinguish treatment failure from non-adherence Clot-based assays for drug levels available for dibigatran & rivaroxaban

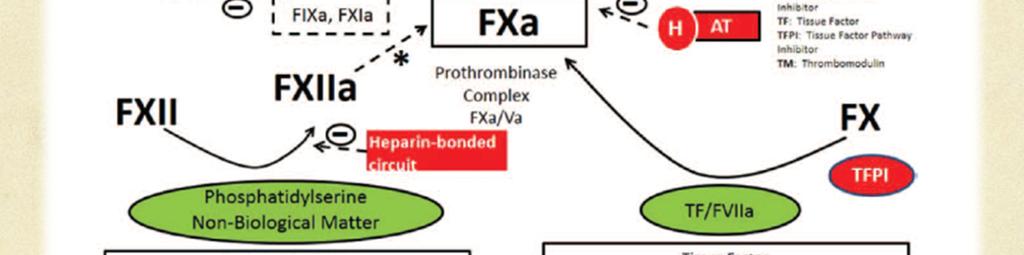
24 ECMO related coagulopathy

25
26 Monitoring of anticoagulation ACT sec Affected by hypothermia & haemodilution Closest to in vivo state, including other non-plasma components APTT may be off scale at the therapeutic range, depending on sensitivity of APTT reagent Anti-Xa assay So called therapeutic range (intercenter variation) Affected by plasma colorimetric When high in face of a normal ACT, suspicious of heparin resistance > check AT level Not practical for continuous monitoring
27 Haemoglobin Platelet count Laboratory tests Coagulation screening Prothrombin time (PT) Activated partial thromboplastin time (APTT) Fibrinogen D-dimers Other laboratory tests: ABG/RFT/LFT
28 Limitations of laboratory tests Haemoglobin may not reflect the extent of blood loss & the effect of haemodilution. Platelet count does not reflect platelet dysfunction acquired during tissue trauma & hypothermia. PT/APTT may not reflect in vivo function of the clotting factors during hypothermia. Increased D-dimers may or may not reflect disseminated intravascular coagulation (D.I.C.). Limitation of conventional laboratory parameters to guide transfusion therapy
29 Idealistic Guide for Transfusion Therapy Fast TAT Certainly NOT PT/APTT Assay better reflect in vivo coagulation state Protocolized (Standardized), with proven benefit by clinical trials, preferably RCT
30 Coagulation screen predicts poorly levels of coagulation factors Retrospective analysis of the individual coagulation factor levels of patients (using the threshold of 30 IU/dl and 1 g/l for fibrinogen) showed that 10 of the 22 patients had not required FFP replacement (nine patients had no coagulation factor levels below 30 IU/dl and one patient had only a decreased level of factor XII). British Journal of Haematology, 125, d
31 Exploring the Global Assay
32 TEG/ROTEM TEG: Cup rotates/rotem: Pin rotates Movement transmitted to tracing recorded as curves & pre-defined parameters A real time continuous assessment Standardization Reference range Validation of protocol for guided transfusion
33 Summary of evidence for TEguided transfusion therapy Supportive evidence Reduction of incidence and volume of FFP transfusion in cardiac surgery* Reduction of incidence of platelet transfusion in cardiac surgery* Reduce the amount of bleeding in massive transfusion** Uncertain evidence** Effect on mortality Effect on morbidity Effect on length of hospital / ICU stay **Cochrane Database Syst Rev Mar 16;(3) * Patient Blood Management: Module 2: Perioperative, National Blood Authority, 2012
34 How Accurate

35 Role of POC assay in perioperative bleeding Management of severe perioperative bleeding: Guideline from European Society of Anesthesiology European Journal of Anaesthesiology :
36 Cont d
37 Future Laboratory Service Development Efficiency Satellite blood bank (Operating Theatre Blood Transaction System) Pre-thawed plasma Just next door (Hot Floor & Rapid Response Lab Concept) Expansion of test repertoire: Global assay, POCT T&S turnaround time Safety Transfusion safety: Patient identification (Policies in place) Pre-operative optimization of haemostatsis Post-operative monitoring to identify patients at risk
38 Conclusion Coagulopathy in ICU setting is complex and often multifactorial. Always consider the clinical context. Conventional laboratory tests are valuable to guide subsequent investigations. Limitations of conventional laboratory tests should be acknowledged. Absence of robust evidence from clinical trials to guide the management of acquired bleeding disorders is very striking & the need of studies to address gaps that currently exists. Emerging role of global assay to guide transfusion therapy.
Transfusion Requirements and Management in Trauma RACHEL JACK
 Transfusion Requirements and Management in Trauma RACHEL JACK Overview Haemostatic resuscitation Massive Transfusion Protocol Overview of NBA research guidelines Haemostatic resuscitation Permissive hypotension
Transfusion Requirements and Management in Trauma RACHEL JACK Overview Haemostatic resuscitation Massive Transfusion Protocol Overview of NBA research guidelines Haemostatic resuscitation Permissive hypotension
Coagulation, Haemostasis and interpretation of Coagulation tests
 Coagulation, Haemostasis and interpretation of Coagulation tests Learning Outcomes Indicate the normal ranges for routine clotting screen and explain what each measurement means Recognise how to detect
Coagulation, Haemostasis and interpretation of Coagulation tests Learning Outcomes Indicate the normal ranges for routine clotting screen and explain what each measurement means Recognise how to detect
Heme (Bleeding and Coagulopathies) in the ICU
 in the ICU") Heme (Bleeding and Coagulopathies) in the ICU General Topics To Discuss Transfusions DIC Thrombocytopenia Liver and renal disease related bleeding Lack of evidence in managing critical illness related
Heme (Bleeding and Coagulopathies) in the ICU General Topics To Discuss Transfusions DIC Thrombocytopenia Liver and renal disease related bleeding Lack of evidence in managing critical illness related
TRANSFUSION GUIDELINES FOR CARDIOTHORACIC UNIT 2006
 TRANSFUSION GUIDELINES FOR CARDIOTHORACIC UNIT 2006 CTU blood product transfusion guidelines 2006 1 Summary of guidelines RED CELLS (10-15ml/kg) This applies to ward patients / icu patients who are stable.
TRANSFUSION GUIDELINES FOR CARDIOTHORACIC UNIT 2006 CTU blood product transfusion guidelines 2006 1 Summary of guidelines RED CELLS (10-15ml/kg) This applies to ward patients / icu patients who are stable.
MANAGEMENT OF COAGULOPATHY AFTER TRAUMA OR MAJOR SURGERY
 MANAGEMENT OF COAGULOPATHY AFTER TRAUMA OR MAJOR SURGERY 19th ANNUAL CONTROVERSIES AND PROBLEMS IN SURGERY Thabo Mothabeng General Surgery: 1 Military Hospital HH Stone et al. Ann Surg. May 1983; 197(5):
MANAGEMENT OF COAGULOPATHY AFTER TRAUMA OR MAJOR SURGERY 19th ANNUAL CONTROVERSIES AND PROBLEMS IN SURGERY Thabo Mothabeng General Surgery: 1 Military Hospital HH Stone et al. Ann Surg. May 1983; 197(5):
Massive Transfusion. MPQC Spring Summit April 29, Roger Belizaire MD PhD
 Massive Transfusion MPQC Spring Summit April 29, 2015 Roger Belizaire MD PhD Take home points 1. Blood is always available. Requests for massive transfusion or emergency release typically only require
Massive Transfusion MPQC Spring Summit April 29, 2015 Roger Belizaire MD PhD Take home points 1. Blood is always available. Requests for massive transfusion or emergency release typically only require
Major Haemorrhage Protocol. Commentary
 Hairmyres Hospital Monklands Hospital Wishaw General Hospital Major Haemorrhage Protocol Commentary N.B. There is a separate NHSL protocol for the Management of Obstetric Haemorrhage Authors Dr Tracey
Hairmyres Hospital Monklands Hospital Wishaw General Hospital Major Haemorrhage Protocol Commentary N.B. There is a separate NHSL protocol for the Management of Obstetric Haemorrhage Authors Dr Tracey
John Davidson Consultant in Intensive Care Medicine Freeman Hospital, Newcastle upon Tyne
 John Davidson Consultant in Intensive Care Medicine Freeman Hospital, Newcastle upon Tyne Overview of coagulation Testing coagulation Coagulopathy in ICU Incidence Causes Evaluation Management Coagulation
John Davidson Consultant in Intensive Care Medicine Freeman Hospital, Newcastle upon Tyne Overview of coagulation Testing coagulation Coagulopathy in ICU Incidence Causes Evaluation Management Coagulation
When should I transfuse platelets and plasma for children? Dr Liz Chalmers. Consultant Paediatric Haematologist Royal Hospital for Children Glasgow
 When should I transfuse platelets and plasma for children? Dr Liz Chalmers Consultant Paediatric Haematologist Royal Hospital for Children Glasgow When should I transfuse platelets and plasma in children?
When should I transfuse platelets and plasma for children? Dr Liz Chalmers Consultant Paediatric Haematologist Royal Hospital for Children Glasgow When should I transfuse platelets and plasma in children?
Approach to disseminated intravascular coagulation
 Approach to disseminated intravascular coagulation Khaire Ananta Shankarrao 1, Anil Burley 2, Deshmukh 3 1.MD Scholar, [kayachikitsa] 2.Professor,MD kayachikitsa. 3.Professor and HOD,Kayachikitsa. CSMSS
Approach to disseminated intravascular coagulation Khaire Ananta Shankarrao 1, Anil Burley 2, Deshmukh 3 1.MD Scholar, [kayachikitsa] 2.Professor,MD kayachikitsa. 3.Professor and HOD,Kayachikitsa. CSMSS
Bleeding, Coagulopathy, and Thrombosis in the Injured Patient
 Bleeding, Coagulopathy, and Thrombosis in the Injured Patient June 7, 2008 Kristan Staudenmayer, MD Trauma Fellow UCSF/SFGH Trauma deaths Sauaia A, et al. J Trauma. Feb 1995;38(2):185 Coagulopathy is Multi-factorial
Bleeding, Coagulopathy, and Thrombosis in the Injured Patient June 7, 2008 Kristan Staudenmayer, MD Trauma Fellow UCSF/SFGH Trauma deaths Sauaia A, et al. J Trauma. Feb 1995;38(2):185 Coagulopathy is Multi-factorial
Pathophysiologie und Therapie bei Massenblutung
 Swisstransfusion Bern, 7. September 2012 Pathophysiologie und Therapie bei Massenblutung Lorenzo ALBERIO Universitätsklinik für Hämatologie und Hämatologisches Zentrallabor Coagulopathy of Trauma Haemorrhage
Swisstransfusion Bern, 7. September 2012 Pathophysiologie und Therapie bei Massenblutung Lorenzo ALBERIO Universitätsklinik für Hämatologie und Hämatologisches Zentrallabor Coagulopathy of Trauma Haemorrhage
MASSIVE TRANSFUSION DR.K.HITESH KUMAR FINAL YEAR PG DEPT. OF TRANSFUSION MEDICINE
 MASSIVE TRANSFUSION DR.K.HITESH KUMAR FINAL YEAR PG DEPT. OF TRANSFUSION MEDICINE CONTENTS Definition Indications Transfusion trigger Massive transfusion protocol Complications DEFINITION Massive transfusion:
MASSIVE TRANSFUSION DR.K.HITESH KUMAR FINAL YEAR PG DEPT. OF TRANSFUSION MEDICINE CONTENTS Definition Indications Transfusion trigger Massive transfusion protocol Complications DEFINITION Massive transfusion:
Blood Transfusion Guidelines in Clinical Practice
 Blood Transfusion Guidelines in Clinical Practice Salwa Hindawi Director of Blood Transfusion Services Associate Professor in Haematology and Transfusion Medicine King Abdalaziz University, Jeddah Saudi
Blood Transfusion Guidelines in Clinical Practice Salwa Hindawi Director of Blood Transfusion Services Associate Professor in Haematology and Transfusion Medicine King Abdalaziz University, Jeddah Saudi
EMSS17: Bleeding patients course material
 EMSS17: Bleeding patients course material Introduction During the bleeding patients workshop at the Emergency Medicine Summer School 2017 (EMSS17) you will learn how to assess and treat bleeding patients
EMSS17: Bleeding patients course material Introduction During the bleeding patients workshop at the Emergency Medicine Summer School 2017 (EMSS17) you will learn how to assess and treat bleeding patients
PBM: The Future of Transfusion December 6 th 2012 East of England RTC. Sue Mallett Royal Free London NHS Foundation Trust
 PBM: The Future of Transfusion December 6 th 2012 East of England RTC Sue Mallett Royal Free London NHS Foundation Trust Patient Blood Management The 3 Pillars Pre-operative optimization of anaemia Minimizing
PBM: The Future of Transfusion December 6 th 2012 East of England RTC Sue Mallett Royal Free London NHS Foundation Trust Patient Blood Management The 3 Pillars Pre-operative optimization of anaemia Minimizing
Massive transfusion: Recent advances, guidelines & strategies. Dr.A.Surekha Devi Head, Dept. of Transfusion Medicine Global Hospital Hyderabad
 Massive transfusion: Recent advances, guidelines & strategies Dr.A.Surekha Devi Head, Dept. of Transfusion Medicine Global Hospital Hyderabad Massive Hemorrhage Introduction Hemorrhage is a major cause
Massive transfusion: Recent advances, guidelines & strategies Dr.A.Surekha Devi Head, Dept. of Transfusion Medicine Global Hospital Hyderabad Massive Hemorrhage Introduction Hemorrhage is a major cause
British Society of Gastroenterology. St. Elsewhere's Hospital. National Comparative Audit of Blood Transfusion
 British Society of Gastroenterology UK Com parat ive Audit of Upper Gast roint est inal Bleeding and t he Use of Blood Transfusion Extract December 2007 St. Elsewhere's Hospital National Comparative Audit
British Society of Gastroenterology UK Com parat ive Audit of Upper Gast roint est inal Bleeding and t he Use of Blood Transfusion Extract December 2007 St. Elsewhere's Hospital National Comparative Audit
Guidance for management of bleeding in patients taking the new oral anticoagulant drugs: rivaroxaban, dabigatran or apixaban
 Guidance for management of bleeding in patients taking the new oral anticoagulant drugs: rivaroxaban, dabigatran or apixaban Purpose The aim of this guidance is to outline the management of patients presenting
Guidance for management of bleeding in patients taking the new oral anticoagulant drugs: rivaroxaban, dabigatran or apixaban Purpose The aim of this guidance is to outline the management of patients presenting
My Bloody Talk. Dr Ben Turner MBBS, FANZCA, FCICM The Royal Children s Hospital, Melbourne
 My Bloody Talk Dr Ben Turner MBBS, FANZCA, FCICM The Royal Children s Hospital, Melbourne Disclosures No conflicts of interest Interest in conflict Blood transfusion Massive transfusion definitions Transfusion
My Bloody Talk Dr Ben Turner MBBS, FANZCA, FCICM The Royal Children s Hospital, Melbourne Disclosures No conflicts of interest Interest in conflict Blood transfusion Massive transfusion definitions Transfusion
Appendix 3 PCC Warfarin Reversal
 Appendix 3 PCC Warfarin Reversal Reversal of Warfarin and Analogues 1. Principle of Procedure Guidelines for the Reversal of Oral-anticoagulation in the Event of Life Threatening Haemorrhage Prothrombin
Appendix 3 PCC Warfarin Reversal Reversal of Warfarin and Analogues 1. Principle of Procedure Guidelines for the Reversal of Oral-anticoagulation in the Event of Life Threatening Haemorrhage Prothrombin
ACQUIRED COAGULATION ABNORMALITIES
 ACQUIRED COAGULATION ABNORMALITIES ACQUIRED COAGULATION ABNORMALITIES - causes 1. Liver disease 2. Vitamin K deficiency 3. Increased consumption of the clotting factors (disseminated intravascular coagulation
ACQUIRED COAGULATION ABNORMALITIES ACQUIRED COAGULATION ABNORMALITIES - causes 1. Liver disease 2. Vitamin K deficiency 3. Increased consumption of the clotting factors (disseminated intravascular coagulation
How can ROTEM testing help you in trauma?
 How can ROTEM testing help you in trauma? Complicated bleeding situations can appear intra and post operatively. They can be life-threatening and always require immediate action. A fast differential diagnosis
How can ROTEM testing help you in trauma? Complicated bleeding situations can appear intra and post operatively. They can be life-threatening and always require immediate action. A fast differential diagnosis
Effective Date: Approved by: Laboratory Director, Jerry Barker (electronic signature)
") 1 of 5 Policy #: 702 (PHL-702-05) Effective Date: 9/30/2004 Reviewed Date: 8/1/2016 Subject: TRANSFUSION GUIDELINES Approved by: Laboratory Director, Jerry Barker (electronic signature) Approved by: Laboratory
1 of 5 Policy #: 702 (PHL-702-05) Effective Date: 9/30/2004 Reviewed Date: 8/1/2016 Subject: TRANSFUSION GUIDELINES Approved by: Laboratory Director, Jerry Barker (electronic signature) Approved by: Laboratory
GUIDELINES FOR MANAGEMENT OF BLEEDING AND EXCESSIVE ANTICOAGULATION WITH ORAL ANTICOAGULANTS
 GUIDELINES FOR MANAGEMENT OF BLEEDING AND EXCESSIVE ANTICOAGULATION WITH ORAL ANTICOAGULANTS This guideline covers the management of patients being treated with Vitamin K antagonists (VKA): Warfarin Acenocoumarol
GUIDELINES FOR MANAGEMENT OF BLEEDING AND EXCESSIVE ANTICOAGULATION WITH ORAL ANTICOAGULANTS This guideline covers the management of patients being treated with Vitamin K antagonists (VKA): Warfarin Acenocoumarol
Dubbi e certezze nella gestione delle emorragie con metodiche point-of-care
 Sessione Educazionale 4 : Gestione del paziente emorragico Dubbi e certezze nella gestione delle emorragie con metodiche point-of-care P. Simioni Università di Padova hemostasis Vascular phase Platelet
Sessione Educazionale 4 : Gestione del paziente emorragico Dubbi e certezze nella gestione delle emorragie con metodiche point-of-care P. Simioni Università di Padova hemostasis Vascular phase Platelet
Transfusion in major bleeding: new insights. Gert Poortmans
 Transfusion in major bleeding: new insights Gert Poortmans Trauma Cardiac Surgery Major Surgery with ongoing blood loss Burn Surgery Lethal Triad Polytransfusion: definitions Coagulation Coagulopathy of
Transfusion in major bleeding: new insights Gert Poortmans Trauma Cardiac Surgery Major Surgery with ongoing blood loss Burn Surgery Lethal Triad Polytransfusion: definitions Coagulation Coagulopathy of
PREDLOG SMERNIC ZA KLINIČNO UPORABE SVEŽE ZMRZNJENE PLAZME Guidelines for clinical use of FFP proposal
 PREDLOG SMERNIC ZA KLINIČNO UPORABE SVEŽE ZMRZNJENE PLAZME Guidelines for clinical use of FFP proposal Dragoslav Domanovič, MD. PhD. Blood transfusion centre of Slovenia, Ljubljana FFP - definition Fresh
PREDLOG SMERNIC ZA KLINIČNO UPORABE SVEŽE ZMRZNJENE PLAZME Guidelines for clinical use of FFP proposal Dragoslav Domanovič, MD. PhD. Blood transfusion centre of Slovenia, Ljubljana FFP - definition Fresh
Management of Challenging Bleeding: Patients with Coagulopathy
 Management of Challenging Bleeding: Patients with Coagulopathy Joanne E Joseph Department of Haematology, SydPath St Vincent s Hospital University of NSW Sydney First and foremost.. It helps to know which
Management of Challenging Bleeding: Patients with Coagulopathy Joanne E Joseph Department of Haematology, SydPath St Vincent s Hospital University of NSW Sydney First and foremost.. It helps to know which
What s in the Massive Transfusion Protocol (MTP) Package?
 Package?") What s in the Massive Transfusion Protocol (MTP) Package? The Massive Transfusion Protocol Package is a set of documents intended to improve the coordination of a Massive Transfusion Protocol. The kit
What s in the Massive Transfusion Protocol (MTP) Package? The Massive Transfusion Protocol Package is a set of documents intended to improve the coordination of a Massive Transfusion Protocol. The kit
*Corresponding author: Key words: neurotrauma, coagulopathy
 COAGULOPATHY IN NEURO TRAUMA A PROSPECTIVE ANALYSIS OF THE INCIDENCE AND CAUSES OF COAGULOPATHY IN PATIENTS WITH PURE NEURO TRAUMA AND MIXED TRAUMA ADMITTED TO THE NATIONAL HOSPITAL SRI LANKA *Jayawickrama
COAGULOPATHY IN NEURO TRAUMA A PROSPECTIVE ANALYSIS OF THE INCIDENCE AND CAUSES OF COAGULOPATHY IN PATIENTS WITH PURE NEURO TRAUMA AND MIXED TRAUMA ADMITTED TO THE NATIONAL HOSPITAL SRI LANKA *Jayawickrama
Disseminated Intravascular Coagulation. M.Bahmanpour MD Assistant professor IUMS
 به نام خدا Disseminated Intravascular Coagulation M.Bahmanpour MD Assistant professor IUMS Algorithm for Diagnosis of DIC DIC Score factor score Presence of known underlying disorder No= 0 yes=2 Coagolation
به نام خدا Disseminated Intravascular Coagulation M.Bahmanpour MD Assistant professor IUMS Algorithm for Diagnosis of DIC DIC Score factor score Presence of known underlying disorder No= 0 yes=2 Coagolation
Intraoperative haemorrhage and haemostasis. Dr. med. Christian Quadri Capoclinica Anestesia, ORL
 Intraoperative haemorrhage and haemostasis Dr. med. Christian Quadri Capoclinica Anestesia, ORL Haemostasis is like love. Everybody talks about it, nobody understands it. JH Levy 2000 Intraoperative Haemorrhage
Intraoperative haemorrhage and haemostasis Dr. med. Christian Quadri Capoclinica Anestesia, ORL Haemostasis is like love. Everybody talks about it, nobody understands it. JH Levy 2000 Intraoperative Haemorrhage
2 Liters. Goal: Basic Algorithm Volume Resuscitation in Trauma. Initial Fluids. Blood. Where do Blood Products Come From?
 Goal: Basic Algorithm Volume Resuscitation in Trauma Sanjay Arora MD Associate Professor of Emergency Medicine Keck School of Medicine at USC Los Angeles County + USC Medical Center May 23, 2012 Initial
Goal: Basic Algorithm Volume Resuscitation in Trauma Sanjay Arora MD Associate Professor of Emergency Medicine Keck School of Medicine at USC Los Angeles County + USC Medical Center May 23, 2012 Initial
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Acute lung injury (ALI) transfusion-related, 363 372. See also Transfusion-related acute lung injury (TRALI) ALI. See Acute lung injury
Index Note: Page numbers of article titles are in boldface type. A Acute lung injury (ALI) transfusion-related, 363 372. See also Transfusion-related acute lung injury (TRALI) ALI. See Acute lung injury
Pre-hospital Administration of Blood Products (PHBP) and Tranexamic acid (TXA): Is the Jury Still Out?
 and Tranexamic acid (TXA): Is the Jury Still Out?") Pre-hospital Administration of Blood Products (PHBP) and Tranexamic acid (TXA): Is the Jury Still Out? Jessica K. Reynolds, MD Assistant Professor of Surgery University of Kentucky, Department of Trauma
Pre-hospital Administration of Blood Products (PHBP) and Tranexamic acid (TXA): Is the Jury Still Out? Jessica K. Reynolds, MD Assistant Professor of Surgery University of Kentucky, Department of Trauma
Major Haemorrhage Transfusion Pathway
 Major Haemorrhage Transfusion Pathway SENIOR CLINICIAN ASSESSMENT: DECLARES MAJOR HAEMORRHAGE ( Call for help ( Telephone via switchboard: Consultant or Senior Clinician Duty Anaesthetist Porters (if will
Major Haemorrhage Transfusion Pathway SENIOR CLINICIAN ASSESSMENT: DECLARES MAJOR HAEMORRHAGE ( Call for help ( Telephone via switchboard: Consultant or Senior Clinician Duty Anaesthetist Porters (if will
DIC. Bert Vandewiele Fellow Critical Care 23 May 2011
 DIC Bert Vandewiele Fellow Critical Care 23 May 2011 Dissiminated Intravascular Coagulopathie 11/3/2011 Dr. Bert Vandewiele 2 Dissiminated Intravascular Coagulopathie = Consumption coagulopathie = Defibrination
DIC Bert Vandewiele Fellow Critical Care 23 May 2011 Dissiminated Intravascular Coagulopathie 11/3/2011 Dr. Bert Vandewiele 2 Dissiminated Intravascular Coagulopathie = Consumption coagulopathie = Defibrination
Effect of under filling tube
 Effect of under filling tube 2 What constitutes underfilling? A 4.5ml vacutainer collection tube should contain at least 4ml of blood Less than that could give falsely prolonged clotting times ALSO be
Effect of under filling tube 2 What constitutes underfilling? A 4.5ml vacutainer collection tube should contain at least 4ml of blood Less than that could give falsely prolonged clotting times ALSO be
New Age Anticoagulants: Bleeding Considerations
 Ontario Regional Blood Coordinating Network March 23, 2012 New Age Anticoagulants: Bleeding Considerations Bill Geerts, MD, FRCPC Thromboembolism Specialist, Sunnybrook HSC Professor of Medicine, University
Ontario Regional Blood Coordinating Network March 23, 2012 New Age Anticoagulants: Bleeding Considerations Bill Geerts, MD, FRCPC Thromboembolism Specialist, Sunnybrook HSC Professor of Medicine, University
The principle of 1:1:1 blood product use in the resuscitation of trauma victims. K. D. Boffard
 The principle of 1:1:1 blood product use in the resuscitation of trauma victims K. D. Boffard Milpark Hospital Department of Surgery University of the Witwatersrand Johannesburg, South Africa Annual Controversies
The principle of 1:1:1 blood product use in the resuscitation of trauma victims K. D. Boffard Milpark Hospital Department of Surgery University of the Witwatersrand Johannesburg, South Africa Annual Controversies
Blood transfusion. Dr. J. Potgieter Dept. of Haematology NHLS - TAD
 Blood transfusion Dr. J. Potgieter Dept. of Haematology NHLS - TAD General Blood is collected from volunteer donors >90% is separated into individual components and plasma Donors should be: healthy, have
Blood transfusion Dr. J. Potgieter Dept. of Haematology NHLS - TAD General Blood is collected from volunteer donors >90% is separated into individual components and plasma Donors should be: healthy, have
MANAGEMENT OF OVERANTICOAGULATION AND PREOPERATIVE MANAGEMENT OF WARFARIN DOSE 1. GUIDELINES FOR THE MANAGEMENT OF AN ELEVATED INR
 MANAGEMENT OF OVERANTICOAGULATION AND PREOPERATIVE MANAGEMENT OF WARFARIN DOSE 1. GUIDELINES FOR THE MANAGEMENT OF AN ELEVATED INR 1.1 Time to lower INR Prothrombinex-VF - 15 minutes Fresh Frozen Plasma
MANAGEMENT OF OVERANTICOAGULATION AND PREOPERATIVE MANAGEMENT OF WARFARIN DOSE 1. GUIDELINES FOR THE MANAGEMENT OF AN ELEVATED INR 1.1 Time to lower INR Prothrombinex-VF - 15 minutes Fresh Frozen Plasma
Introduction to coagulation and laboratory tests
 Introduction to coagulation and laboratory tests Marc Jacquemin Special Haemostasis Laboratory Center for Molecular and Vascular Biology University of Leuven Coagulation in a blood vessel: fibrin stabilises
Introduction to coagulation and laboratory tests Marc Jacquemin Special Haemostasis Laboratory Center for Molecular and Vascular Biology University of Leuven Coagulation in a blood vessel: fibrin stabilises
Blood Component Therapy
 Blood Component Therapy Dr Anupam Chhabra Incharge-Transfusion Medicine Pushpanjali Crosslay Hopital NCR-Delhi Introduction Blood a blood components are considered drugs because of their use in treating
Blood Component Therapy Dr Anupam Chhabra Incharge-Transfusion Medicine Pushpanjali Crosslay Hopital NCR-Delhi Introduction Blood a blood components are considered drugs because of their use in treating
DOAC and NOAC are terms for a novel class of directly acting oral anticoagulant drugs including Rivaroxaban, Apixaban, Edoxaban, and Dabigatran.
 Guideline for Patients on Direct Oral Anticoagulant Therapy Requiring Urgent Surgery for Hip Fracture Trust Ref:C10/2017 1. Introduction This guideline is for the clinical management of patients on direct
Guideline for Patients on Direct Oral Anticoagulant Therapy Requiring Urgent Surgery for Hip Fracture Trust Ref:C10/2017 1. Introduction This guideline is for the clinical management of patients on direct
Management of the Trauma Patient. Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015
 Management of the Trauma Patient Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015 Saturday Night 25 yo M s/p high speed MVC Hypotensive in the ED, altered
Management of the Trauma Patient Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015 Saturday Night 25 yo M s/p high speed MVC Hypotensive in the ED, altered
MANAGEMENT OF COMMON BLEEDING DISORDERS. Auro Viswabandya Department of Haematology, CMC, Vellore
 MANAGEMENT OF COMMON BLEEDING DISORDERS Auro Viswabandya Department of Haematology, CMC, Vellore BLOOD CLOT : PRIMARY HAEMOSTASIS (Platelets) + SECONDARY HAEMOSTASIS (Coagulation Factors) HAEMOSTATIC DISORDERS
MANAGEMENT OF COMMON BLEEDING DISORDERS Auro Viswabandya Department of Haematology, CMC, Vellore BLOOD CLOT : PRIMARY HAEMOSTASIS (Platelets) + SECONDARY HAEMOSTASIS (Coagulation Factors) HAEMOSTATIC DISORDERS
Prothrombin Complex Concentrate- Octaplex. Octaplex
 Prothrombin Complex Concentrate- Concentrated Factors Prothrombin Complex Concentrate (PCC) 3- factor (factor II, IX, X) 4-factor (factors II, VII, IX, X) Activated 4-factor (factors II, VIIa, IX, X) Coagulation
Prothrombin Complex Concentrate- Concentrated Factors Prothrombin Complex Concentrate (PCC) 3- factor (factor II, IX, X) 4-factor (factors II, VII, IX, X) Activated 4-factor (factors II, VIIa, IX, X) Coagulation
Active date July Ratification date: Review date January 2014 Applies to: Staff managing patients on warfarin. Exclusions:
 Guideline Title: Guidelines for the management of warfarin reversal [key words : Beriplex, Octaplex, PCC, vitamin K, anticoagulant, anticoagulation] Authors: Dr Sarah Allford, Consultant Haematologist
Guideline Title: Guidelines for the management of warfarin reversal [key words : Beriplex, Octaplex, PCC, vitamin K, anticoagulant, anticoagulation] Authors: Dr Sarah Allford, Consultant Haematologist
CLINICAL FELLOWSHIP PROGRAM IN COAGULATION
 CLINICAL FELLOWSHIP PROGRAM IN COAGULATION The Department of Pathology and Laboratory Medicine University of Alberta, Faculty of Medicine and Dentistry and Alberta Health Services CLINICAL FELLOWSHIP IN
CLINICAL FELLOWSHIP PROGRAM IN COAGULATION The Department of Pathology and Laboratory Medicine University of Alberta, Faculty of Medicine and Dentistry and Alberta Health Services CLINICAL FELLOWSHIP IN
HEME 10 Bleeding Disorders
 HEME 10 Bleeding Disorders When injury occurs, three mechanisms occur Blood vessels Primary hemostasis Secondary hemostasis Diseases of the blood vessels Platelet disorders Thrombocytopenia Functional
HEME 10 Bleeding Disorders When injury occurs, three mechanisms occur Blood vessels Primary hemostasis Secondary hemostasis Diseases of the blood vessels Platelet disorders Thrombocytopenia Functional
Coagulopathy: Measuring and Management. Nina A. Guzzetta, M.D. Children s Healthcare of Atlanta Emory University School of Medicine
 Coagulopathy: Measuring and Management Nina A. Guzzetta, M.D. Children s Healthcare of Atlanta Emory University School of Medicine No Financial Disclosures Objectives Define coagulopathy of trauma Define
Coagulopathy: Measuring and Management Nina A. Guzzetta, M.D. Children s Healthcare of Atlanta Emory University School of Medicine No Financial Disclosures Objectives Define coagulopathy of trauma Define
UPDATE OF NEUROCRITICAL CARE PHARMACOTHERAPY. Vera Wilson, PharmD, BCPS Emergency Services Clinical Pharmacy Specialist Johnson City Medical Center
 UPDATE OF NEUROCRITICAL CARE PHARMACOTHERAPY Vera Wilson, PharmD, BCPS Emergency Services Clinical Pharmacy Specialist Johnson City Medical Center DISCLOSURE STATEMENT OF FINANCIAL INTEREST I, Vera Wilson,
UPDATE OF NEUROCRITICAL CARE PHARMACOTHERAPY Vera Wilson, PharmD, BCPS Emergency Services Clinical Pharmacy Specialist Johnson City Medical Center DISCLOSURE STATEMENT OF FINANCIAL INTEREST I, Vera Wilson,
Platelet Disorders. By : Saja Al-Oran
 Platelet Disorders By : Saja Al-Oran Introduction The platelet arise from the fragmentation of the cytoplasm of megakaryocyte in the bone marrow. circulate in the blood as disc-shaped anucleate particles
Platelet Disorders By : Saja Al-Oran Introduction The platelet arise from the fragmentation of the cytoplasm of megakaryocyte in the bone marrow. circulate in the blood as disc-shaped anucleate particles
TRANSFUSIONS FIRST, DO NO HARM
 TRANSFUSIONS FIRST, DO NO HARM BECAUSE BLOOD CAN KILL 7 TRALI DEATHS SINCE 2002 WMC 5 women BECAUSE In OB you are transfusing 2 instead of 1 BECAUSE BLOOD IS A LIQUID TRANSPLANT RISKS versus BENEFITS versus
TRANSFUSIONS FIRST, DO NO HARM BECAUSE BLOOD CAN KILL 7 TRALI DEATHS SINCE 2002 WMC 5 women BECAUSE In OB you are transfusing 2 instead of 1 BECAUSE BLOOD IS A LIQUID TRANSPLANT RISKS versus BENEFITS versus
Topics of today lectures: Hemostasis
 Topics of today lectures: Hemostasis Meaning of hemostasis Mechanisms of hemostasis - Vascular contraction - Platelets plug - Blood coagulation (clotting) - Structure and functions of platelets - Blood
Topics of today lectures: Hemostasis Meaning of hemostasis Mechanisms of hemostasis - Vascular contraction - Platelets plug - Blood coagulation (clotting) - Structure and functions of platelets - Blood
Shock and Resuscitation: Part II. Patrick M Reilly MD FACS Professor of Surgery
 Shock and Resuscitation: Part II Patrick M Reilly MD FACS Professor of Surgery Trauma Patient 1823 / 18 Police Dropoff Torso GSW Lower Midline / Right Buttock Shock This Monday Trauma Patient 1823 / 18
Shock and Resuscitation: Part II Patrick M Reilly MD FACS Professor of Surgery Trauma Patient 1823 / 18 Police Dropoff Torso GSW Lower Midline / Right Buttock Shock This Monday Trauma Patient 1823 / 18
Guidelines for the management of warfarin reversal in adults
 SharePoint Location Clinical Policies and Guidelines SharePoint Index Directory General Policies and Guidelines Sub Area Haematology and Transfusion Key words (for search purposes) Warfarin, Bleeding Central
SharePoint Location Clinical Policies and Guidelines SharePoint Index Directory General Policies and Guidelines Sub Area Haematology and Transfusion Key words (for search purposes) Warfarin, Bleeding Central
Dr Shikha Chattree Haematology Consultant Sunderland Royal infirmary
 Dr Shikha Chattree Haematology Consultant Sunderland Royal infirmary Increasing use of Novel Oral Anticoagulants (NOACs) in the management of prophylaxis and management of venous thromboembolism and in
Dr Shikha Chattree Haematology Consultant Sunderland Royal infirmary Increasing use of Novel Oral Anticoagulants (NOACs) in the management of prophylaxis and management of venous thromboembolism and in
Blood Management and Protocol Use in Active Bleeding
 Blood Management and Protocol Use in Active Bleeding John A. Norton, DO Assistant Professor Clinical Department of Anesthesiology The Ohio State University Wexner Medical Center Acknowledgements Stephanie
Blood Management and Protocol Use in Active Bleeding John A. Norton, DO Assistant Professor Clinical Department of Anesthesiology The Ohio State University Wexner Medical Center Acknowledgements Stephanie
3/16/15. Management of the Bleeding Trauma Patient: Concepts in Damage Control Resuscitation. Obligatory Traumatologist Slide
 Management of the Bleeding Trauma Patient: Concepts in Damage Control Resuscitation Courtney Sommer, MD MPH Duke Trauma Symposium March 12, 2015 Obligatory Traumatologist Slide In 2010 trauma was leading
Management of the Bleeding Trauma Patient: Concepts in Damage Control Resuscitation Courtney Sommer, MD MPH Duke Trauma Symposium March 12, 2015 Obligatory Traumatologist Slide In 2010 trauma was leading
Clinical Overview of Coagulation Testing Issues
 Clinical Overview of Coagulation Testing Issues Adam M. Vogel, MD Assistant Professor, Division of Pediatric Surgery Washington University in St. Louis School of Medicine September 19, 2014 Disclosure
Clinical Overview of Coagulation Testing Issues Adam M. Vogel, MD Assistant Professor, Division of Pediatric Surgery Washington University in St. Louis School of Medicine September 19, 2014 Disclosure
Disseminated intravascular coagulation (DIC) Dr. Klara Vezendi Szeged University Transfusiology Department
 Dr. Klara Vezendi Szeged University Transfusiology Department") Disseminated intravascular coagulation (DIC) Dr. Klara Vezendi Szeged University Transfusiology Department Disseminated intravascular coagulation (DIC, consumptive coagulopathy) is a clinicopathologic
Disseminated intravascular coagulation (DIC) Dr. Klara Vezendi Szeged University Transfusiology Department Disseminated intravascular coagulation (DIC, consumptive coagulopathy) is a clinicopathologic
Hemostatic Resuscitation
 Hemostatic Resuscitation 30 th David Miller Trauma Symposium Bill Beck, MD Assistant Professor of Surgery Trauma, Emergency General Surgery, Critical Care Disclosures None Again. Mac user. Why I Like Trauma?
Hemostatic Resuscitation 30 th David Miller Trauma Symposium Bill Beck, MD Assistant Professor of Surgery Trauma, Emergency General Surgery, Critical Care Disclosures None Again. Mac user. Why I Like Trauma?
UNIT VI. Chapter 37: Platelets Hemostasis and Blood Coagulation Presented by Dr. Diksha Yadav. Copyright 2011 by Saunders, an imprint of Elsevier Inc.
 UNIT VI Chapter 37: Platelets Hemostasis and Blood Coagulation Presented by Dr. Diksha Yadav Hemostasis: Prevention of Blood Loss Vascular constriction Formation of a platelet plug Formation of a blood
UNIT VI Chapter 37: Platelets Hemostasis and Blood Coagulation Presented by Dr. Diksha Yadav Hemostasis: Prevention of Blood Loss Vascular constriction Formation of a platelet plug Formation of a blood
the bleeding won t stop? Liane Manz RN, BScN, CNCC(c) Royal Alexandra Hospital
 Royal Alexandra Hospital") What do you do when the bleeding won t stop? Teddie Tanguay RN, MN, NP, CNCC(c) Teddie Tanguay RN, MN, NP, CNCC(c) Liane Manz RN, BScN, CNCC(c) Royal Alexandra Hospital Outline Case study Normal coagulation
What do you do when the bleeding won t stop? Teddie Tanguay RN, MN, NP, CNCC(c) Teddie Tanguay RN, MN, NP, CNCC(c) Liane Manz RN, BScN, CNCC(c) Royal Alexandra Hospital Outline Case study Normal coagulation
Groupe d Intérêt en Hémostase Périopératoire
 How do I treat massive bleeding? Red blood cell / plasma / platelet ratio and massive transfusion protocols Anne GODIER Service d Anesthésie-Réanimation Hopital Cochin Paris Groupe d Intérêt en Hémostase
How do I treat massive bleeding? Red blood cell / plasma / platelet ratio and massive transfusion protocols Anne GODIER Service d Anesthésie-Réanimation Hopital Cochin Paris Groupe d Intérêt en Hémostase
PEDIATRIC MASSIVE TRANSFUSION
 PEDIATRIC MASSIVE TRANSFUSION CHELSEA RUNKLE RN, BSN, CCRN, SRNA CROZER-CHESTER MEDICAL CENTER/VILLANOVA UNIVERSITY NURSE ANESTHESIA PROGRAM LEADING CAUSE OF DEATH Trauma Motor vehicle accidents, nonaccidental
PEDIATRIC MASSIVE TRANSFUSION CHELSEA RUNKLE RN, BSN, CCRN, SRNA CROZER-CHESTER MEDICAL CENTER/VILLANOVA UNIVERSITY NURSE ANESTHESIA PROGRAM LEADING CAUSE OF DEATH Trauma Motor vehicle accidents, nonaccidental
2012, Görlinger Klaus
 Gerinnungsmanagement der Gegenwart - wie gehen wir heute vor? 25. Allander Gerinnungsrunde am 15. März 2012 Klaus Görlinger Universitätsklinikum Essen klaus@goerlinger.net CSL Behring GmbH Octapharma AG
Gerinnungsmanagement der Gegenwart - wie gehen wir heute vor? 25. Allander Gerinnungsrunde am 15. März 2012 Klaus Görlinger Universitätsklinikum Essen klaus@goerlinger.net CSL Behring GmbH Octapharma AG
New Advances in Transfusion EM I LY CO BERLY, M D
 New Advances in Transfusion EM I LY CO BERLY, M D TRANSFUSI ON M EDI CI NE FELLO W VANDERBI LT UNI VERSITY Objectives To discuss the terminology, components, transfusion risks, and dosing guidelines for
New Advances in Transfusion EM I LY CO BERLY, M D TRANSFUSI ON M EDI CI NE FELLO W VANDERBI LT UNI VERSITY Objectives To discuss the terminology, components, transfusion risks, and dosing guidelines for
Emergency Management of Patients on Direct Oral Anticoagulants (DOACs)
") Emergency Management of Patients on Direct Oral Anticoagulants (DOACs) Dr Tina Biss Consultant Haematologist Newcastle upon Tyne Hospitals NHS Foundation Trust NE RTC Annual Education Symposium 11 th October
Emergency Management of Patients on Direct Oral Anticoagulants (DOACs) Dr Tina Biss Consultant Haematologist Newcastle upon Tyne Hospitals NHS Foundation Trust NE RTC Annual Education Symposium 11 th October
EDUCATIONAL COMMENTARY DISSEMINATED INTRAVASCULAR COAGULATION
 EDUCATIONAL COMMENTARY DISSEMINATED INTRAVASCULAR COAGULATION Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE
EDUCATIONAL COMMENTARY DISSEMINATED INTRAVASCULAR COAGULATION Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE
Patient Blood Management Are you providing this? Jeannie Callum, BA, MD, FRCPC Associate Professor, University of Toronto
 Patient Blood Management Are you providing this? Jeannie Callum, BA, MD, FRCPC Associate Professor, University of Toronto Disclosures Relevant relationships with commercial entities: Octapharma, CSL Behring
Patient Blood Management Are you providing this? Jeannie Callum, BA, MD, FRCPC Associate Professor, University of Toronto Disclosures Relevant relationships with commercial entities: Octapharma, CSL Behring
DISSEMINATED INTRAVASCULAR COAGULATION (DIC) Pichika Chantrathammachart MD Division of Hematology, Department of Medicine Ramathibodi Hospital
 Pichika Chantrathammachart MD Division of Hematology, Department of Medicine Ramathibodi Hospital") DISSEMINATED INTRAVASCULAR COAGULATION (DIC) Pichika Chantrathammachart MD Division of Hematology, Department of Medicine Ramathibodi Hospital Disseminated intravascular coagulation (DIC) Disseminated
DISSEMINATED INTRAVASCULAR COAGULATION (DIC) Pichika Chantrathammachart MD Division of Hematology, Department of Medicine Ramathibodi Hospital Disseminated intravascular coagulation (DIC) Disseminated
ADMINISTRATIVE CLINICAL Page 1 of 6
 ADMINISTRATIVE CLINICAL Page 1 of 6 Anticoagulant Guidelines #2: REVERSAL OF OR MANAGEMENT OF BLEEDING WITH ANTICOAGULANTS Origination Date: Revision Date: Reviewed Date: 09/12 09/12, 01/13, 11/13, 11/15
ADMINISTRATIVE CLINICAL Page 1 of 6 Anticoagulant Guidelines #2: REVERSAL OF OR MANAGEMENT OF BLEEDING WITH ANTICOAGULANTS Origination Date: Revision Date: Reviewed Date: 09/12 09/12, 01/13, 11/13, 11/15
Haemostasis & Coagulation disorders Objectives:
 Haematology Lec. 1 د.ميسم مؤيد علوش Haemostasis & Coagulation disorders Objectives: - Define haemostasis and what are the major components involved in haemostasis? - How to assess the coagulation status?
Haematology Lec. 1 د.ميسم مؤيد علوش Haemostasis & Coagulation disorders Objectives: - Define haemostasis and what are the major components involved in haemostasis? - How to assess the coagulation status?
Routine preoperative coagulation tests: are they necessary?
 Routine preoperative coagulation tests: are they necessary? Dr Azzah Alzahrani MD Pediatrics Hematology /Oncology PSMMS Outline Introduction. Brief review of hemostatic mechanisms. A clinical aspect of
Routine preoperative coagulation tests: are they necessary? Dr Azzah Alzahrani MD Pediatrics Hematology /Oncology PSMMS Outline Introduction. Brief review of hemostatic mechanisms. A clinical aspect of
Assessing thrombocytopenia in the intensive care unit: The past, present, and future
 Assessing thrombocytopenia in the intensive care unit: The past, present, and future Ryan Zarychanski MD MSc FRCPC Sections of Critical Care and of Hematology, University of Manitoba Disclosures FINANCIAL
Assessing thrombocytopenia in the intensive care unit: The past, present, and future Ryan Zarychanski MD MSc FRCPC Sections of Critical Care and of Hematology, University of Manitoba Disclosures FINANCIAL
Balanced Transfusion Resuscitation
 Transparency in Transfusion Medicine 2013 Balanced Transfusion Resuscitation HGD Hendriks MD, PhD University Medical Center Groningen Balancing 1 2 3 Preoperative Peroperative Postoperative Balanced Coagulation
Transparency in Transfusion Medicine 2013 Balanced Transfusion Resuscitation HGD Hendriks MD, PhD University Medical Center Groningen Balancing 1 2 3 Preoperative Peroperative Postoperative Balanced Coagulation
Guidelines for testing and perioperative management of dabigatran and rivaroxaban
 Guidelines for testing and perioperative management of dabigatran and rivaroxaban: for possible use in local management protocols These guidelines have been produced by PHARMAC in conjunction with bpac
Guidelines for testing and perioperative management of dabigatran and rivaroxaban: for possible use in local management protocols These guidelines have been produced by PHARMAC in conjunction with bpac
NICE guideline Published: 18 November 2015 nice.org.uk/guidance/ng24
 Blood transfusion NICE guideline Published: 18 November 2015 nice.org.uk/guidance/ng24 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Blood transfusion NICE guideline Published: 18 November 2015 nice.org.uk/guidance/ng24 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
10/24/2013. Heparin-Induced Thrombocytopenia (HIT) Anticoagulation Management in ECMO Therapy:
 Anticoagulation Management in ECMO Therapy:") Anticoagulation Management in ECMO Therapy: Heparin-Induced (HIT) Michael H. Creer, MD Professor of Pathology Director, Clinical Laboratories, Medical Co- Director, Hematopathology and Chief, Division
Anticoagulation Management in ECMO Therapy: Heparin-Induced (HIT) Michael H. Creer, MD Professor of Pathology Director, Clinical Laboratories, Medical Co- Director, Hematopathology and Chief, Division
TRAUMA RESUSCITATION. Dr. Carlos Palisi Dr. Nicholas Smith Liverpool Hospital
 TRAUMA RESUSCITATION Dr. Carlos Palisi Dr. Nicholas Smith Liverpool Hospital First Principles.ATLS/EMST A- Airway and C-spine B- Breathing C- Circulation and Access D- Neurological deficit E- adequate
TRAUMA RESUSCITATION Dr. Carlos Palisi Dr. Nicholas Smith Liverpool Hospital First Principles.ATLS/EMST A- Airway and C-spine B- Breathing C- Circulation and Access D- Neurological deficit E- adequate
TRANSFUSION SUPPORT IN HEPATOBILIARY AND PANCREATIC SURGERIES
 TRANSFUSION SUPPORT IN HEPATOBILIARY AND PANCREATIC SURGERIES Dr.K.C.Usha Professor & Head Dept: Of Transfusion Medicine & Director, Model Blood Bank Government Medical College Trivandrum,Kerala INTRODUCTION
TRANSFUSION SUPPORT IN HEPATOBILIARY AND PANCREATIC SURGERIES Dr.K.C.Usha Professor & Head Dept: Of Transfusion Medicine & Director, Model Blood Bank Government Medical College Trivandrum,Kerala INTRODUCTION
International Journal of Health Sciences and Research ISSN:
 International Journal of Health Sciences and Research www.ijhsr.org ISSN: 2249-9571 Original Research Article Appropriate and Inappropriate Use of Fresh Frozen Plasma (FFP) and Packed Cell Volume (PCV)
International Journal of Health Sciences and Research www.ijhsr.org ISSN: 2249-9571 Original Research Article Appropriate and Inappropriate Use of Fresh Frozen Plasma (FFP) and Packed Cell Volume (PCV)
MANAGEMENT OF BLEEDING AND EXCESSIVE ANTICOAGULATION IN ADULTS RECEIVING ANTI-COAGULANTS
 Hairmyres Hospital MANAGEMENT OF BLEEDING AND EXCESSIVE ANTICOAGULATION IN ADULTS RECEIVING ANTI-COAGULANTS Bleeding in patients on anticoagulants, even in the absence of over-anticoagulation, can be life-threatening
Hairmyres Hospital MANAGEMENT OF BLEEDING AND EXCESSIVE ANTICOAGULATION IN ADULTS RECEIVING ANTI-COAGULANTS Bleeding in patients on anticoagulants, even in the absence of over-anticoagulation, can be life-threatening
Unrestricted. Dr ppooransari fellowship of perenatalogy
 Unrestricted Dr ppooransari fellowship of perenatalogy Assessment of severity of hemorrhage Significant drops in blood pressure are generally not manifested until substantial bleeding has occurred, and
Unrestricted Dr ppooransari fellowship of perenatalogy Assessment of severity of hemorrhage Significant drops in blood pressure are generally not manifested until substantial bleeding has occurred, and
Audit of Platelet Use
 South West Regional Transfusion Committee Audit of Platelet Use Report by Regional Transfusion Team Acknowledgements Thanks to all transfusion laboratory staff who provided the data for this audit report.
South West Regional Transfusion Committee Audit of Platelet Use Report by Regional Transfusion Team Acknowledgements Thanks to all transfusion laboratory staff who provided the data for this audit report.
L iter diagnostico di laboratorio nelle coagulopatie congenite emorragiche
 L iter diagnostico di laboratorio nelle coagulopatie congenite emorragiche Armando Tripodi Angelo Bianchi Bonomi Hemophilia and Thrombosis Center Dept. of Clinical Sciences and Community Health University
L iter diagnostico di laboratorio nelle coagulopatie congenite emorragiche Armando Tripodi Angelo Bianchi Bonomi Hemophilia and Thrombosis Center Dept. of Clinical Sciences and Community Health University
Chapter 3 MAKING THE DECISION TO TRANSFUSE
 Chapter 3 MAKING THE DECISION TO TRANSFUSE PRACTICE POINTS Determine the best treatment for the patient which may include transfusion. Treat the cause of cytopenia (anaemia or thrombocytopenia) or plasma
Chapter 3 MAKING THE DECISION TO TRANSFUSE PRACTICE POINTS Determine the best treatment for the patient which may include transfusion. Treat the cause of cytopenia (anaemia or thrombocytopenia) or plasma
Haematological Emergencies (Part 1) Ray Mun Koo Haematology Advanced Trainee Canberra Hospital
 Ray Mun Koo Haematology Advanced Trainee Canberra Hospital") Haematological Emergencies (Part 1) Ray Mun Koo Haematology Advanced Trainee Canberra Hospital Case Number 1 43 year old male presenting with fevers, abdominal distension and weight gain over 2 weeks.
Haematological Emergencies (Part 1) Ray Mun Koo Haematology Advanced Trainee Canberra Hospital Case Number 1 43 year old male presenting with fevers, abdominal distension and weight gain over 2 weeks.
Razvana Akbar Anticoagulation Pharmacist LTH
 Razvana Akbar Anticoagulation Pharmacist LTH Platelet function Drugs affecting Coagulation; Anti-platelet drugs Anticoagulants Oral anticoagulants Parenteral anticoagulants Drugs affecting Haemoglobin
Razvana Akbar Anticoagulation Pharmacist LTH Platelet function Drugs affecting Coagulation; Anti-platelet drugs Anticoagulants Oral anticoagulants Parenteral anticoagulants Drugs affecting Haemoglobin
Internal Quality Control in the Haemostasis laboratory. Dr Steve Kitchen Sheffield Haemophilia and Thrombosis centre & UK NEQAS Blood Coagulation
 Internal Quality Control in the Haemostasis laboratory Dr Steve Kitchen Sheffield Haemophilia and Thrombosis centre & UK NEQAS Blood Coagulation Why do we need Quality control? Philadelphia Enquirer Aug
Internal Quality Control in the Haemostasis laboratory Dr Steve Kitchen Sheffield Haemophilia and Thrombosis centre & UK NEQAS Blood Coagulation Why do we need Quality control? Philadelphia Enquirer Aug
GUIDELINES FOR THE TRANSFUSION OF BLOOD COMPONENTS
 CHILDREN S HOSPITALS AND CLINICS OF MINNESOTA Introduction: GUIDELINES FOR THE TRANSFUSION OF BLOOD COMPONENTS These guidelines have been developed in conjunction with the hospital Transfusion Committee.
CHILDREN S HOSPITALS AND CLINICS OF MINNESOTA Introduction: GUIDELINES FOR THE TRANSFUSION OF BLOOD COMPONENTS These guidelines have been developed in conjunction with the hospital Transfusion Committee.
Schematic Of Heparin Induced Thrombocytopenia Platelet Count
 Schematic Of Heparin Induced Thrombocytopenia Platelet Count Normal IgG and IgG2 differentially inhibit HIT antibody-dependent platelet activation that platelet counts were lower in FcγRIIA 131RR patients
Schematic Of Heparin Induced Thrombocytopenia Platelet Count Normal IgG and IgG2 differentially inhibit HIT antibody-dependent platelet activation that platelet counts were lower in FcγRIIA 131RR patients
General approach to the investigation of haemostasis. Jan Gert Nel Dept. of Haematology University of Pretoria 2013
 General approach to the investigation of haemostasis Jan Gert Nel Dept. of Haematology University of Pretoria 2013 Clinical reasons to investigate haemostasis Investigating a clinically suspected bleeding
General approach to the investigation of haemostasis Jan Gert Nel Dept. of Haematology University of Pretoria 2013 Clinical reasons to investigate haemostasis Investigating a clinically suspected bleeding
Laboratory Empowerment. Debbie Asher Adrian Ebbs Transfusion Laboratory Managers, Eastern Pathology Alliance
 Laboratory Empowerment Debbie Asher Adrian Ebbs Transfusion Laboratory Managers, Eastern Pathology Alliance Why? Electronic ICE requesting was in use for requesting red cells NBTC Indication Codes were
Laboratory Empowerment Debbie Asher Adrian Ebbs Transfusion Laboratory Managers, Eastern Pathology Alliance Why? Electronic ICE requesting was in use for requesting red cells NBTC Indication Codes were
NOACS/DOACS*: COAGULATION TESTS
 NOACS/DOACS*: COAGULATION TESTS OBJECTIVES: To describe the effect of the newer direct oral anticoagulants (DOACs) on laboratory coagulation tests which are widely available: prothrombin time (PT), international
NOACS/DOACS*: COAGULATION TESTS OBJECTIVES: To describe the effect of the newer direct oral anticoagulants (DOACs) on laboratory coagulation tests which are widely available: prothrombin time (PT), international
This slide belongs to iron lecture and it is to clarify the iron cycle in the body and the effect of hypoxia on erythropoitein secretion
 This slide belongs to iron lecture and it is to clarify the iron cycle in the body and the effect of hypoxia on erythropoitein secretion Topics of today lectures: Hemostasis Meaning of hemostasis Mechanisms
This slide belongs to iron lecture and it is to clarify the iron cycle in the body and the effect of hypoxia on erythropoitein secretion Topics of today lectures: Hemostasis Meaning of hemostasis Mechanisms