Recombinant Factor VIIa for Intracerebral Hemorrhage
|
|
|
- Marlene Ramsey
- 5 years ago
- Views:
Transcription
1 Recombinant Factor VIIa for Intracerebral Hemorrhage January 24, 2006 Justin Lee Pharmacy Resident University Health Network
2 Outline 1. Introduction to patient case 2. Overview of intracerebral hemorrhage (ICH) a. Presentation b. Risk factors c. Medical management 3. Overview of recombinant Factor VIIa a. Efficacy b. Safety 4. Apply EBM principles to patient case
3 Overview of Patient Case
4 Mr. ICH 58 year old male of African descent HPI: Sudden onset of severe headache, nausea and left-sided weakness After wife called 911, patient began to have slurred speech,vomited and then collapsed On admission, BP 190/95, HR 52, GCS 7

5 At 3 h from onset, Mr. ICH head CT confirms ICH in the right putamen Mild hydrocephalus and slight left midline shift
6 PMH: Mr. ICH Hypertension Hyperlipidemia DVT (1 year ago) Type II Diabetes Smoker (1 pack per day)
7 BPMH: Mr. ICH Hydrochlorothiazide 25 mg po OD Ramipril 5 mg po OD Atorvastatin 40 mg po OD Metformin 1000 mg po BID
8 Clinical Question Is recombinant Factor VII (rfviia( rfviia) ) a reasonable therapeutic alternative in Mr. ICH? Will it improve his clinical outcome? Is it safe to use in the treatment of ICH given his past medical history?
9 Overview of Intracerebral Hemorrhage (ICH)

10 Clinical Presentation Bleeding due to a ruptured intracranial vessel Focal neurological deficit Sudden onset Progresses over minutes to hours Signs and Symptoms ± Headache ± Nausea / Vomiting ± LOC ± BP
11 Causes and Risk Factors Primary (80-85%) 85%) Sustained hypertension Cerebral amyloid angiopathy Secondary (15-20%) Trauma Aneurysms Arteriovenous malformations (AVMs) Coagulopathies Use of anticoagulants, antiplatelets or thrombolytics Illicit drug use Alcohol
12 Treatment Guidelines Lack of proven medical or surgical treatment!
13 Medical Management Airway and oxygenation Manage blood pressure Manage intracranial pressure Maintain euvolemia Prevent seizures Treat hyperthermia
14 Morbidity and Mortality Mortality at 1 month is 35-52% 52% Half of the deaths occur within first 2 days Only 20% of survivors regain functional independence Broderick JP et al. Stroke 1999; 30:
15 Hematoma Growth ICH is a dynamic phenomenon Result of ongoing bleeding or rebleeding 38% of ICH patients exhibit hematoma growth (volume increase >33%) within 24 hours Early hematoma growth is associated with neurological deterioration Hematoma volume is determinant of mortality and functional outcome Brott T et al. Stroke 1997; 28: 1-5 Davis SM et al. Neurology 2006; 66:
16 Hypothesis Risk of disability or death can be reduced by treatments that: promote clotting arrest bleeding minimize hematoma growth
17 Overview of Recombinant Factor VIIa (rfviia)
18 NovoSeven (rfviia( rfviia) rfviia induces hemostasis at site of injury Binds to exposed tissue factor (TF) Binds to activated platelets Result? Formation of thrombin Good safety profile in patients with hemophilia and other bleeding disorders Hemostatic benefits may be offset by thromboembolic adverse events
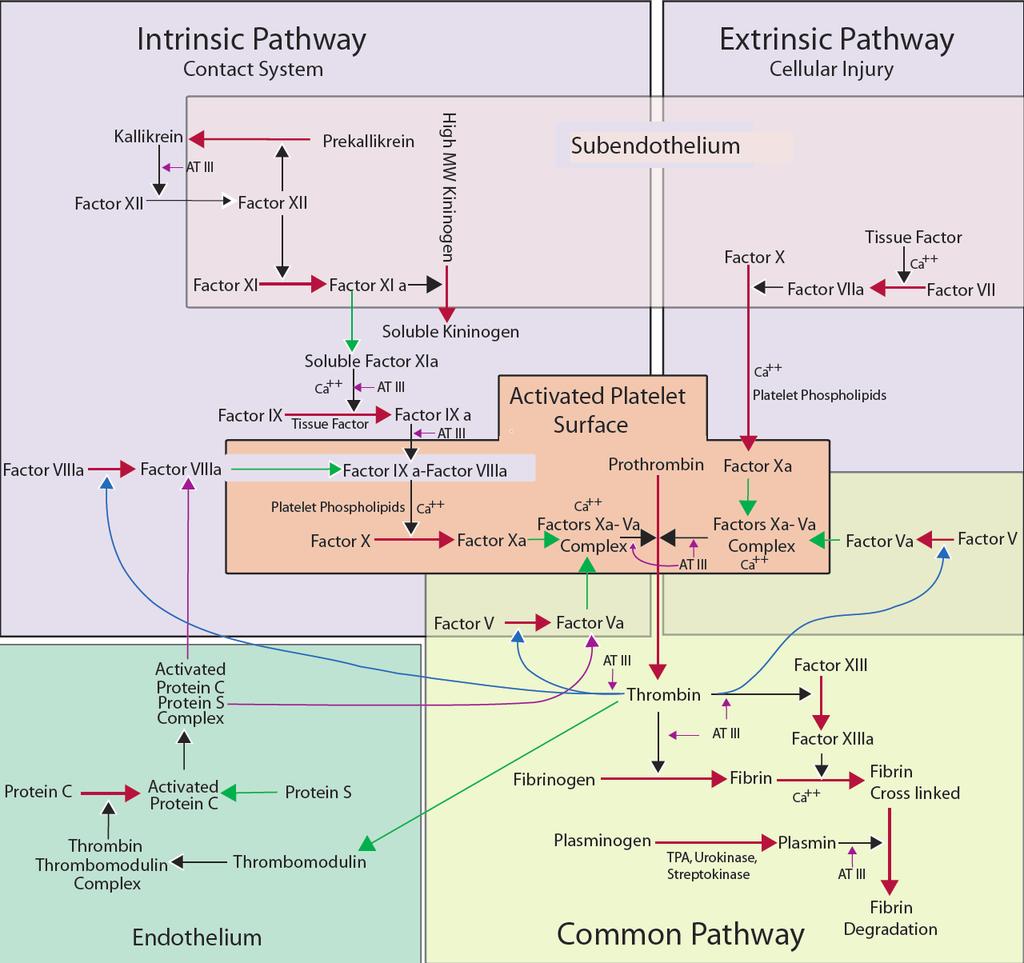
19 Coagulation Cascade
20 rfviia-tissue Factor Complex rfviia-tf complex activates Factor IX and Factor X

21 Direct Activation of Factor X Platelets are activated by initial thrombin generated by rfviia rfviia directly activates Factor X on the surface of an activated platelet
 to thrombiin (Factor")
22 Thrombin Burst Factor Xa, in complex with other factors, converts prothrombin (Factor II) to thrombiin (Factor IIa)

23 Formation of Fibrin Clot Thrombin leads to formation of a hemostatic plug by converting fibrinogen to fibrin
24 Literature Search Results 3 Phase II RCTs to date rfviia EurAsia IIA rfviia USA IIA rfviia IIB All compare various rfviia doses to placebo All studies funded by NovoNordisk
25 rfviia EurAsia IIA Stroke 2005; 36: 74-9
26 rfviia EurAsia IIA Dose escalation trial Multicenter,, randomized, double-blind, blind, placebo- controlled 48 patients rfviia 10, 20, 40, 80, 120 or 160 µg/kg vs. placebo Primary endpoint was frequency of AEs
27 rfviia EurAsia IIA rfviia was well tolerated 6 possible treatment-related related AEs 2 DVTs (in placebo and 20 µg/kg) No noticeable differences in types, frequency or severity of AEs Most common AEs included: Fever Headache UTI Hypertension Constipation
28 rfviia USA IIA Neurocrit Care 2006; 04:
29 rfviia USA IIA Dose-escalation escalation trial Multicenter,, randomized, double-blind, blind, placebo-controlled controlled 40 patients rfviia 5, 20, 40, or 80 µg/kg vs. placebo Primary endpoint was frequency of AEs
30 rfviia USA IIA rfviia was well tolerated 12 possible or probable treatment-related related AEs None were thromboembolic AEs No significant differences in types, frequency or severity of AEs Most common AEs included: UTI Fever Constipation Somnalence
31 rfviia IIB Trial N Engl J Med 2005; 352:
32 rfviia IIB Multicenter (73 hospitals, 20 countries) Double-blind, blind, placebo-controlled controlled 399 patients Intervention: Single IV dose of rfviia 40, 80 or 160 N= 108 (40 µg) N= 92 (80 µg) N= 103 (160 µg) N= 96 (placebo) Primary Endpoint: % change in volume of ICH at 24 hours Clinical outcomes at 90 days 40, 80 or 160 µg/kg vs. placebo
33 rfviia IIB Trial Inclusion Criteria 18 years of age CT confirmed ICH within 3 h of onset Exclusion Criteria GCS 3-53 Planned surgical evacuation with 24 h ICH secondary to aneurysm, AVM, trauma or other cause Use of oral anticoagulants Thrombocytopenia History of coagulopathy,, acute sepsis, crush injury or DIC Pregnancy Symptomatic thrombotic or vaso-occlusive occlusive disease (i.e. angina, claudication,, DVT, or cerebral or myocardial infaction Note: Patient with ANY history of thrombotic or vaso-occlusive disease were excluded midway through the trial due to safety concerns
34 Results of rfviia IIB Outcome at 24 h 40 µg/kg 80 µg/kg 160 µg/kg Combined Placebo Lesion Volume of ICH (ml) Difference in Mean Volume Increase from Baseline (98.3% CI) 3.3 (1.9 to 8.5) 4.5 (0.8 to 9.9) 5.8 (0.6 to 11) 4.5 (0.2 to 8.8) P value Reduction in hematoma volume was only significant at the highest dose
35 Results of rfviia IIB P = Percent P = 0.01 P = 0.02 P = 0.12 Placebo rfviia 0 Hematoma Growth Mortality Poor Outcome TE Events Note: Study was not adequately powered to detect difference of TE events

36 Clinical Outcomes All scales show more favourable outcome with rfviia in dose-response trend. Results significant for all doses in modified Rankin and NIH Stroke Scales.
37 Clinical Outcomes Outcome at 90 d rfviia (Combined Doses) Placebo RRR (98.3% CI) NNT (98.3% CI) Death 18% 29% 37% (6 to 57) 10 (5 to 82) Unfavourable Outcome (Death or Severe Disability) 53% 69% 23% (8 to 35) 7 (4 to 22)
38 Safety of rfviia Serious Thrombo- embolic Adverse Events 40 µg/kg 80 µg/kg 160 µg/kg Combined Placebo Total 7 (6%) 4 (4%) 10 (10%) 21 (7%) 2 (2%) Arterial 6 (6%) 2 (2%) 8 (8%) 16 (5%) 0 (0%) Venous 1 (1%) 2 (2%) 2 (2%) 5 (2%) 2 (2%)
39 Safety of rfviia Apparent 3x increase in thromboembolic events in the combined rfviia group RR 3.33, 95% CI 0.79 to Reduction or increase? Underestimation of risks of using rfviia? Recall exclusion of patients with recent history of thrombotic or vaso-occlusive occlusive disease

40 Do These Results Apply?
41 Strengths of rfviia IIB Reduction in hematoma growth is appropriate surrogate outcome Well-established established relationship between ICH volume and clinical outcome Volume is independent of hemorrhage location Intention-to to-treat treat analysis was performed
42 Limitations of rfviia IIB Were baseline characteristics similar? GCS, location of ICH, baseline volume, BP Benefit was only significant in patients treated 3 h after onset At >3 h, mean volume increase was 14% vs. 16% in favour of placebo (p=0.86) Subgroup was underpowered to detect difference Reduction in hematoma growth was only statistically significant at 160 µg/kg
43 Limitations of rfviia IIB Study was not powered to detect the magnitude of the study s difference in AEs Exclusion criteria were changed midway due to safety concerns 49% of patients had already been enrolled
44 Application to Mr. ICH rfviia may not be suitable due to several unanswered questions Acceptable safety profile? prothrombotic risk factors (recent history of DVT) Optimal therapeutic window? treatment after 3 h of ICH onset Fits the study population? African descent
45 Conclusions Early hemostatic therapy with rfviia given within 4 hours of primary spontaneous ICH onset reduces: Hematoma growth Unfavourable outcome at 90 days Mortality at 90 days Data is promising, but not clinically directive More evidence is needed to address Safety and prothrombotic risk Optimal treatment window Influence of other prognostic factors Use in other ICH subtypes
46 Conclusions Results cannot be generalized to all ICH patients Inclusions? Elderly caucasian males who can be treated within 3 h Exclusions? ICH due to secondary cause eg.. anticoagulant use, aneurysm, AVM, etc. History of thrombotic or vaso-occlusive occlusive disease Ischemic stroke Myocardial infarction DVT / PE Claudication
47 Ongoing Phase III Trial rfviia in Acute Hemorrhagic Stroke Treatment (FAST) trial Desired sample size 675 patients Intervention rfviia (20 µg/kg or 80 µg/kg) vs. placebo Primary endpoint death or severe disability at day 90 Study likely will not have power to detect differences in serious thromboembolic AEs
48 Discussion & Questions
Review of the TICH-2 Trial
 Review of the TICH-2 Trial Mikaela Hofer, PharmD PGY-1 Pharmacy Resident Pharmacy Grand Rounds September 18, 2018 2018 MFMER slide-1 Objectives Review the pharmacologic options to limit hematoma expansion
Review of the TICH-2 Trial Mikaela Hofer, PharmD PGY-1 Pharmacy Resident Pharmacy Grand Rounds September 18, 2018 2018 MFMER slide-1 Objectives Review the pharmacologic options to limit hematoma expansion
Modern Management of ICH
 Modern Management of ICH Bradley A. Gross, MD Assistant Professor, Dept of Neurosurgery, University of Pittsburgh October 2018 ICH Background Assessment & Diagnosis Medical Management Surgical Management
Modern Management of ICH Bradley A. Gross, MD Assistant Professor, Dept of Neurosurgery, University of Pittsburgh October 2018 ICH Background Assessment & Diagnosis Medical Management Surgical Management
Hypertensive Haemorrhagic Stroke. Dr Philip Lam Thuon Mine
 Hypertensive Haemorrhagic Stroke Dr Philip Lam Thuon Mine Intracerebral Haemorrhage Primary ICH Spontaneous rupture of small vessels damaged by HBP Basal ganglia, thalamus, pons and cerebellum Amyloid
Hypertensive Haemorrhagic Stroke Dr Philip Lam Thuon Mine Intracerebral Haemorrhage Primary ICH Spontaneous rupture of small vessels damaged by HBP Basal ganglia, thalamus, pons and cerebellum Amyloid
Stroke: What did we learn in the last year?
 Stroke: What did we learn in the last year? J. Claude Hemphill III, MD, MAS Associate Professor of Clinical Neurology and Neurological Surgery University of California, San Francisco Director, Neurocritical
Stroke: What did we learn in the last year? J. Claude Hemphill III, MD, MAS Associate Professor of Clinical Neurology and Neurological Surgery University of California, San Francisco Director, Neurocritical
Starting or Resuming Anticoagulation or Antiplatelet Therapy after ICH: A Neurology Perspective
 Starting or Resuming Anticoagulation or Antiplatelet Therapy after ICH: A Neurology Perspective Cathy Sila MD George M Humphrey II Professor and Vice Chair of Neurology Director, Comprehensive Stroke Center
Starting or Resuming Anticoagulation or Antiplatelet Therapy after ICH: A Neurology Perspective Cathy Sila MD George M Humphrey II Professor and Vice Chair of Neurology Director, Comprehensive Stroke Center
ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist
 ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist Pharmacy Grand Rounds 26 July 2016 2015 MFMER slide-1 Learning
ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist Pharmacy Grand Rounds 26 July 2016 2015 MFMER slide-1 Learning
GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE
 2018 UPDATE QUICK SHEET 2018 American Heart Association GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE A Summary for Healthcare Professionals from the American Heart Association/American
2018 UPDATE QUICK SHEET 2018 American Heart Association GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE A Summary for Healthcare Professionals from the American Heart Association/American
How Low Should You Go? Management of Blood Pressure in Intracranial Hemorrhage
 How Low Should You Go? Management of Blood Pressure in Intracranial Hemorrhage Rachael Scott, Pharm.D. PGY2 Critical Care Pharmacy Resident Pharmacy Grand Rounds August 21, 2018 2018 MFMER slide-1 Patient
How Low Should You Go? Management of Blood Pressure in Intracranial Hemorrhage Rachael Scott, Pharm.D. PGY2 Critical Care Pharmacy Resident Pharmacy Grand Rounds August 21, 2018 2018 MFMER slide-1 Patient
THROMBOTIC DISORDERS: The Final Frontier
 THROMBOTIC DISORDERS: The Final Frontier Jeffrey I. Weitz, MD, FRCP(C), FACP Professor of Medicine and Biochemistry McMaster University Canada Research Chair in Thrombosis Heart & Stroke Foundation/ J.F.
THROMBOTIC DISORDERS: The Final Frontier Jeffrey I. Weitz, MD, FRCP(C), FACP Professor of Medicine and Biochemistry McMaster University Canada Research Chair in Thrombosis Heart & Stroke Foundation/ J.F.
FVIIa for Acute Hemorrhagic Stroke Administered at Earliest Time (FASTEST) Trial. Joseph P. Broderick, MD James Grotta, MD Jordan Elm, PhD
 Trial. Joseph P. Broderick, MD James Grotta, MD Jordan Elm, PhD") FVIIa for Acute Hemorrhagic Stroke Administered at Earliest Time (FASTEST) Trial Joseph P. Broderick, MD James Grotta, MD Jordan Elm, PhD Background Intracerebral hemorrhage (ICH) accounts for more than
FVIIa for Acute Hemorrhagic Stroke Administered at Earliest Time (FASTEST) Trial Joseph P. Broderick, MD James Grotta, MD Jordan Elm, PhD Background Intracerebral hemorrhage (ICH) accounts for more than
11/27/2017. Stroke Management in the Neurocritical Care Unit. Conflict of interest. Karel Fuentes MD Medical Director of Neurocritical Care
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Neurosurgical Management of Stroke
 Overview Hemorrhagic Stroke Ischemic Stroke Aneurysmal Subarachnoid hemorrhage Neurosurgical Management of Stroke Jesse Liu, MD Instructor, Neurological Surgery Initial management In hospital management
Overview Hemorrhagic Stroke Ischemic Stroke Aneurysmal Subarachnoid hemorrhage Neurosurgical Management of Stroke Jesse Liu, MD Instructor, Neurological Surgery Initial management In hospital management
Neurosurgical decision making in structural lesions causing stroke. Dr Rakesh Ranjan MS, MCh, Dip NB (Neurosurgery)
") Neurosurgical decision making in structural lesions causing stroke Dr Rakesh Ranjan MS, MCh, Dip NB (Neurosurgery) Subarachnoid Hemorrhage Every year, an estimated 30,000 people in the United States experience
Neurosurgical decision making in structural lesions causing stroke Dr Rakesh Ranjan MS, MCh, Dip NB (Neurosurgery) Subarachnoid Hemorrhage Every year, an estimated 30,000 people in the United States experience
Online Supplementary Data. Country Number of centers Number of patients randomized
 A Randomized, Double-Blind, -Controlled, Phase-2B Study to Evaluate the Safety and Efficacy of Recombinant Human Soluble Thrombomodulin, ART-123, in Patients with Sepsis and Suspected Disseminated Intravascular
A Randomized, Double-Blind, -Controlled, Phase-2B Study to Evaluate the Safety and Efficacy of Recombinant Human Soluble Thrombomodulin, ART-123, in Patients with Sepsis and Suspected Disseminated Intravascular
Controversies in Hemorrhagic Stroke Management. Sarah L. Livesay, DNP, RN, ACNP-BC, ACNS-BC Associate Professor Rush University
 Controversies in Hemorrhagic Stroke Management Sarah L. Livesay, DNP, RN, ACNP-BC, ACNS-BC Associate Professor Rush University Disclosures AHA/ASA Outline Blood pressure VTE Coagulopathy Early mobilization
Controversies in Hemorrhagic Stroke Management Sarah L. Livesay, DNP, RN, ACNP-BC, ACNS-BC Associate Professor Rush University Disclosures AHA/ASA Outline Blood pressure VTE Coagulopathy Early mobilization
Index. C Capillary telangiectasia, intracerebral hemorrhage in, 295 Carbon monoxide, formation of, in intracerebral hemorrhage, edema due to,
 Neurosurg Clin N Am 13 (2002) 395 399 Index Note: Page numbers of article titles are in boldface type. A Age factors, in intracerebral hemorrhage outcome, 344 Albumin, for intracerebral hemorrhage, 336
Neurosurg Clin N Am 13 (2002) 395 399 Index Note: Page numbers of article titles are in boldface type. A Age factors, in intracerebral hemorrhage outcome, 344 Albumin, for intracerebral hemorrhage, 336
Stroke - Intracranial hemorrhage. Dr. Amitesh Aggarwal Associate Professor Department of Medicine
 Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
Intracranial Hemorrhage. Objectives. What Do Need to Know?
 Intracranial Hemorrhage What Do Need to Know? Kerry Brega, MD Associate Professor of Neurosurgery University of Colorado Objectives Know the common types of ICH. Know how they can be differentiated. Know
Intracranial Hemorrhage What Do Need to Know? Kerry Brega, MD Associate Professor of Neurosurgery University of Colorado Objectives Know the common types of ICH. Know how they can be differentiated. Know
ADVANCES IN ANTICOAGULATION
 ADVANCES IN ANTICOAGULATION The Clinicians Perspective Claudine M. Lewis Cardiologist OUTLINE Indications for anticoagulants Review - Physiology of Hemostasis Types of anticoagulants New anticoagulants
ADVANCES IN ANTICOAGULATION The Clinicians Perspective Claudine M. Lewis Cardiologist OUTLINE Indications for anticoagulants Review - Physiology of Hemostasis Types of anticoagulants New anticoagulants
Blood Pressure Management in Acute Ischemic Stroke
 Blood Pressure Management in Acute Ischemic Stroke Kimberly Clark, PharmD, BCCCP Clinical Pharmacy Specialist Critical Care, Greenville Health System Adjunct Assistant Professor, South Carolina College
Blood Pressure Management in Acute Ischemic Stroke Kimberly Clark, PharmD, BCCCP Clinical Pharmacy Specialist Critical Care, Greenville Health System Adjunct Assistant Professor, South Carolina College
Patients with intracerebral hemorrhage (ICH) have an
 have an") Thromboembolic Events With Recombinant Activated Factor VII in Spontaneous Intracerebral Hemorrhage Results From the Factor Seven for Acute Hemorrhagic Stroke (FAST) Trial Michael N. Diringer, MD; Brett
Thromboembolic Events With Recombinant Activated Factor VII in Spontaneous Intracerebral Hemorrhage Results From the Factor Seven for Acute Hemorrhagic Stroke (FAST) Trial Michael N. Diringer, MD; Brett
Clopidogrel and ASA after CABG for NSTEMI
 Clopidogrel and ASA after CABG for NSTEMI May 17, 2007 Justin Lee Pharmacy Resident University Health Network Objectives At the end of this session, you should be able to: Explain the rationale for antiplatelet
Clopidogrel and ASA after CABG for NSTEMI May 17, 2007 Justin Lee Pharmacy Resident University Health Network Objectives At the end of this session, you should be able to: Explain the rationale for antiplatelet
5/15/2018. Reduced Platelet Activity
 ASSOCIATION OF DESMOPRESSIN ACETATE ON OUTCOMES IN ACUTE INTRACRANIAL HEMORRHAGE IN PATIENTS ON ANTIPLATELET THERAPY Jessica McManus, Pharm. D. PGY2 Critical Care Pharmacy Resident UF Health Jacksonville
ASSOCIATION OF DESMOPRESSIN ACETATE ON OUTCOMES IN ACUTE INTRACRANIAL HEMORRHAGE IN PATIENTS ON ANTIPLATELET THERAPY Jessica McManus, Pharm. D. PGY2 Critical Care Pharmacy Resident UF Health Jacksonville
Angel J. Lacerda MD PhD, Daisy Abreu MD, Julio A. Díaz MD, Sandro Perez MD, Julio C Martin MD, Daiyan Martin MD.
 Angel J. Lacerda MD PhD, Daisy Abreu MD, Julio A. Díaz MD, Sandro Perez MD, Julio C Martin MD, Daiyan Martin MD. Introduction: Spontaneous intracerebral haemorrhage (SICH) represents one of the most severe
Angel J. Lacerda MD PhD, Daisy Abreu MD, Julio A. Díaz MD, Sandro Perez MD, Julio C Martin MD, Daiyan Martin MD. Introduction: Spontaneous intracerebral haemorrhage (SICH) represents one of the most severe
Blood Thinner Agent. Done by: Meznah Al-mutairi Pharm.D Candidate PNU Collage of Pharmacy
 Blood Thinner Agent Done by: Meznah Al-mutairi Pharm.D Candidate PNU Collage of Pharmacy Outline: Blood thinner agent definition. anticoagulants drugs. Thrombolytics. Blood thinner agent Therapeutic interference
Blood Thinner Agent Done by: Meznah Al-mutairi Pharm.D Candidate PNU Collage of Pharmacy Outline: Blood thinner agent definition. anticoagulants drugs. Thrombolytics. Blood thinner agent Therapeutic interference
NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS. ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS
 FOR THROMBOLYSIS") NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS I. Purpose : A. To reduce morbidity and mortality associated
NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS I. Purpose : A. To reduce morbidity and mortality associated
UPSTATE Comprehensive Stroke Center. Neurosurgical Interventions Satish Krishnamurthy MD, MCh
 UPSTATE Comprehensive Stroke Center Neurosurgical Interventions Satish Krishnamurthy MD, MCh Regional cerebral blood flow is important Some essential facts Neurons are obligatory glucose users Under anerobic
UPSTATE Comprehensive Stroke Center Neurosurgical Interventions Satish Krishnamurthy MD, MCh Regional cerebral blood flow is important Some essential facts Neurons are obligatory glucose users Under anerobic
SCCEP 2013 LLSA Course Article 10 AHA/ASA Guidelines for the Management of Spontaneous ICH
 SCCEP 2013 LLSA Course Article 10 AHA/ASA Guidelines for the Management of Spontaneous ICH Morgenstern LB, Hemphill JC. Stroke July 2010;41:2108-2129. Article: This article presents guidelines whose "aim
SCCEP 2013 LLSA Course Article 10 AHA/ASA Guidelines for the Management of Spontaneous ICH Morgenstern LB, Hemphill JC. Stroke July 2010;41:2108-2129. Article: This article presents guidelines whose "aim
Intracerebral Hemorrhage
 Review of Primary Intracerebral Hemorrhage Réza Behrouz, DO Assistant Professor of Neurology University of South Florida College of Medicine STROKE 85% ISCHEMIC 15% HEMORRHAGIC HEMORRHAGIC STROKE 1/3 Subarachnoid
Review of Primary Intracerebral Hemorrhage Réza Behrouz, DO Assistant Professor of Neurology University of South Florida College of Medicine STROKE 85% ISCHEMIC 15% HEMORRHAGIC HEMORRHAGIC STROKE 1/3 Subarachnoid
HAEMORRHAGIA Bleeding
 HAEMORRHAGIA Bleeding Cassification Size Location pathomechanism Hematoma: external or may be enclosed within a tissue petechial rash (spot) : 1-2 mm hemorrhages into skin, mucous membranes, or serosal
HAEMORRHAGIA Bleeding Cassification Size Location pathomechanism Hematoma: external or may be enclosed within a tissue petechial rash (spot) : 1-2 mm hemorrhages into skin, mucous membranes, or serosal
Recombinant Activated Factor VII: Useful. Department of Surgery Grand Rounds 11/8/10 David Mauchley MD
 Recombinant Activated Factor VII: Useful Department of Surgery Grand Rounds 11/8/10 David Mauchley MD Hemostasis and Coagulation Traditional cascade model Two convergent pathways Series of proteolytic
Recombinant Activated Factor VII: Useful Department of Surgery Grand Rounds 11/8/10 David Mauchley MD Hemostasis and Coagulation Traditional cascade model Two convergent pathways Series of proteolytic
Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข
 Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข Emergency start at community level: Prehospital care Acute stroke
Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข Emergency start at community level: Prehospital care Acute stroke
Primary Stroke Center Acute Stroke Transfer Guidelines When to Consider a Transfer:
 When to Consider a Transfer: Hemorrhagic Stroke Large volume intracerebral hematoma greater than 5cm on CT Concern for expanding hematoma Rapidly declining mental status, especially requiring intubation
When to Consider a Transfer: Hemorrhagic Stroke Large volume intracerebral hematoma greater than 5cm on CT Concern for expanding hematoma Rapidly declining mental status, especially requiring intubation
Using DOACs in CAD Patients in Sinus Ryhthm Results of the ATLAS ACS 2, COMPASS and COMMANDER-HF Trials
 Using DOACs in CAD Patients in Sinus Ryhthm Results of the ATLAS ACS 2, COMPASS and COMMANDER-HF Trials 19 th Annual San Diego Heart Failure Symposium for Primary Care Physicians January 11-12, 2019 La
Using DOACs in CAD Patients in Sinus Ryhthm Results of the ATLAS ACS 2, COMPASS and COMMANDER-HF Trials 19 th Annual San Diego Heart Failure Symposium for Primary Care Physicians January 11-12, 2019 La
CEREBRO VASCULAR ACCIDENTS
 CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
Benjamin Anyanwu,MD Medical Director In-patient Neurology and Neuroscience ICU Novant Health Forsyth Medical Center, Winston-Salem NC
 Benjamin Anyanwu,MD Medical Director In-patient Neurology and Neuroscience ICU Novant Health Forsyth Medical Center, Winston-Salem NC Emergency Treatment of Hemorrhagic Stroke Objectives Discuss the etiology
Benjamin Anyanwu,MD Medical Director In-patient Neurology and Neuroscience ICU Novant Health Forsyth Medical Center, Winston-Salem NC Emergency Treatment of Hemorrhagic Stroke Objectives Discuss the etiology
Chapter 1 Introduction
 Chapter 1 Introduction There are several disorders which carry an increased risk of thrombosis, clots that interfere with normal circulation, including: venous thromboembolism (VTE), comprising both deep
Chapter 1 Introduction There are several disorders which carry an increased risk of thrombosis, clots that interfere with normal circulation, including: venous thromboembolism (VTE), comprising both deep
Klinikum Frankfurt Höchst
 Blood pressure management in hemorrhagic stroke Blood pressure in acute ICH Do we need additional trials after INTERACT2 and ATTACH-II? Focus.de Department of Neurology,, Germany Department of Neurology,
Blood pressure management in hemorrhagic stroke Blood pressure in acute ICH Do we need additional trials after INTERACT2 and ATTACH-II? Focus.de Department of Neurology,, Germany Department of Neurology,
Anticoagulants. Pathological formation of a haemostatic plug Arterial associated with atherosclerosis Venous blood stasis e.g. DVT
 Haemostasis Thrombosis Phases Endogenous anticoagulants Stopping blood loss Pathological formation of a haemostatic plug Arterial associated with atherosclerosis Venous blood stasis e.g. DVT Vascular Platelet
Haemostasis Thrombosis Phases Endogenous anticoagulants Stopping blood loss Pathological formation of a haemostatic plug Arterial associated with atherosclerosis Venous blood stasis e.g. DVT Vascular Platelet
Stroke 101. Maine Cardiovascular Health Summit. Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013
 Stroke 101 Maine Cardiovascular Health Summit Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013 Stroke Statistics Definition of stroke Risk factors Warning signs Treatment
Stroke 101 Maine Cardiovascular Health Summit Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013 Stroke Statistics Definition of stroke Risk factors Warning signs Treatment
Thrombolysis for acute ischaemic stroke Rapid Assessment Protocol NORTHERN IRELAND Regional Protocol (Version 002 July 08)
") Thrombolysis for acute ischaemic stroke Rapid Assessment Protocol NORTHERN IRELAND Regional Protocol (Version 002 July 08) Patient Details Time of onset? Capillary Blood glucose 2.8-22.2 mmol/l? Blood
Thrombolysis for acute ischaemic stroke Rapid Assessment Protocol NORTHERN IRELAND Regional Protocol (Version 002 July 08) Patient Details Time of onset? Capillary Blood glucose 2.8-22.2 mmol/l? Blood
Treatment of Acute Hemorrhagic Stroke 5th QSVS Neurovascular Conference Dar Dowlatshahi MD PhD FRCPC Sept 14, 2012
 Treatment of Acute Hemorrhagic Stroke 5th QSVS Neurovascular Conference Dar Dowlatshahi MD PhD FRCPC Sept 14, 2012 Disclosure of potential conflicts of interest Quebec Society of Vascular Sciences presents
Treatment of Acute Hemorrhagic Stroke 5th QSVS Neurovascular Conference Dar Dowlatshahi MD PhD FRCPC Sept 14, 2012 Disclosure of potential conflicts of interest Quebec Society of Vascular Sciences presents
Update in Management of Acute Spontaneous Intracerebral Haemorrhage
 Update in Management of Acute Spontaneous Intracerebral Haemorrhage Aldy S. Rambe Neurology Department, School of Medicine EPIDEMIOLOGY Although ICH represents only about 9% of all stroke, it accounts
Update in Management of Acute Spontaneous Intracerebral Haemorrhage Aldy S. Rambe Neurology Department, School of Medicine EPIDEMIOLOGY Although ICH represents only about 9% of all stroke, it accounts
Cerebrovascular Disorders. Blood, Brain, and Energy. Blood Supply to the Brain 2/14/11
 Cerebrovascular Disorders Blood, Brain, and Energy 20% of body s oxygen usage No oxygen/glucose reserves Hypoxia - reduced oxygen Anoxia - Absence of oxygen supply Cell death can occur in as little as
Cerebrovascular Disorders Blood, Brain, and Energy 20% of body s oxygen usage No oxygen/glucose reserves Hypoxia - reduced oxygen Anoxia - Absence of oxygen supply Cell death can occur in as little as
Intracranial spontaneous hemorrhage mechanisms, imaging and management
 Intracranial spontaneous hemorrhage mechanisms, imaging and management Dora Zlatareva Department of Diagnostic Imaging Medical University, Sofia, Bulgaria Intracranial hemorrhage (ICH) ICH 15% of strokes
Intracranial spontaneous hemorrhage mechanisms, imaging and management Dora Zlatareva Department of Diagnostic Imaging Medical University, Sofia, Bulgaria Intracranial hemorrhage (ICH) ICH 15% of strokes
The Multi arm Optimization of Stroke Thrombolysis (MOST) Trial
 Trial") The Multi arm Optimization of Stroke Thrombolysis (MOST) Trial Study Team Principal Investigators: Opeolu Adeoye, University of Cincinnati (Lead) Andrew Barreto, University of Texas Houston Jim Grotta,
The Multi arm Optimization of Stroke Thrombolysis (MOST) Trial Study Team Principal Investigators: Opeolu Adeoye, University of Cincinnati (Lead) Andrew Barreto, University of Texas Houston Jim Grotta,
Hit head, on blood thinner-wife wants CT. Will Davies June 2014
 Hit head, on blood thinner-wife wants CT Will Davies June 2014 Selection of Adults with Head Injury for CT Scan Early management of head injury: summary of updated NICE guidance. Hodgkinson S, Pollit V,
Hit head, on blood thinner-wife wants CT Will Davies June 2014 Selection of Adults with Head Injury for CT Scan Early management of head injury: summary of updated NICE guidance. Hodgkinson S, Pollit V,
Introduction. Blood Pressure
 Introduction Spontaneous intracerebral hemorrhage (ICH) is a major cause of morbidity and mortality worldwide [1]. Of a number of factors that have been linked to ICH (e.g., higher rates in Asians and
Introduction Spontaneous intracerebral hemorrhage (ICH) is a major cause of morbidity and mortality worldwide [1]. Of a number of factors that have been linked to ICH (e.g., higher rates in Asians and
Prothrombin Complex Concentrate- Octaplex. Octaplex
 Prothrombin Complex Concentrate- Concentrated Factors Prothrombin Complex Concentrate (PCC) 3- factor (factor II, IX, X) 4-factor (factors II, VII, IX, X) Activated 4-factor (factors II, VIIa, IX, X) Coagulation
Prothrombin Complex Concentrate- Concentrated Factors Prothrombin Complex Concentrate (PCC) 3- factor (factor II, IX, X) 4-factor (factors II, VII, IX, X) Activated 4-factor (factors II, VIIa, IX, X) Coagulation
 www.yassermetwally.com MANAGEMENT OF CEREBRAL HAEMORRHAGE (ICH): A QUICK GUIDE Overview 10% of strokes is caused by ICH. Main Causes: Less than 40 years old: vascular malformations and illicit drug use.
www.yassermetwally.com MANAGEMENT OF CEREBRAL HAEMORRHAGE (ICH): A QUICK GUIDE Overview 10% of strokes is caused by ICH. Main Causes: Less than 40 years old: vascular malformations and illicit drug use.
3/19/2012. What is the indication for anticoagulation? Has the patient previously been on warfarin? If so, what % of the time was the INR therapeutic?
 Abigail E. Miller, PharmD, BCPS Clinical Specialist, Cardiology University of North Carolina Hospitals I have no personal financial relationships with the manufacturers of the products to disclose. Boehringer
Abigail E. Miller, PharmD, BCPS Clinical Specialist, Cardiology University of North Carolina Hospitals I have no personal financial relationships with the manufacturers of the products to disclose. Boehringer
DVT Pathophysiology and Prophylaxis in Medically Hospitalized Patients. David Liff MD Oklahoma Heart Institute Vascular Center
 DVT Pathophysiology and Prophylaxis in Medically Hospitalized Patients David Liff MD Oklahoma Heart Institute Vascular Center Overview Pathophysiology of DVT Epidemiology and risk factors for DVT in the
DVT Pathophysiology and Prophylaxis in Medically Hospitalized Patients David Liff MD Oklahoma Heart Institute Vascular Center Overview Pathophysiology of DVT Epidemiology and risk factors for DVT in the
William Barr, M.D. January 28, 2017
 William Barr, M.D. January 28, 2017 Types of Stroke Ischemic Stroke Small vessel (20%) Large vessel (31%) Embolic (32%) Hemorrhagic Intracerebral Hemorrhage (10%) Subarachnoid Hemorrhage (7%) The Majority
William Barr, M.D. January 28, 2017 Types of Stroke Ischemic Stroke Small vessel (20%) Large vessel (31%) Embolic (32%) Hemorrhagic Intracerebral Hemorrhage (10%) Subarachnoid Hemorrhage (7%) The Majority
New Frontiers in Intracerebral Hemorrhage
 New Frontiers in Intracerebral Hemorrhage Ryan Hakimi, DO, MS Director, Neuro ICU Director, Inpatient Neurology Services Greenville Health System Clinical Associate Professor Department of Medicine (Neurology)
New Frontiers in Intracerebral Hemorrhage Ryan Hakimi, DO, MS Director, Neuro ICU Director, Inpatient Neurology Services Greenville Health System Clinical Associate Professor Department of Medicine (Neurology)
HAEMORRHAGIA Bleeding
 HAEMORRHAGIA Bleeding Cassification Size Location pathomechanism Hematoma: external or may be enclosed within a tissue petechiae : 1-2 mm hemorrhages into skin, mucous membranes, or serosal surfaces increased
HAEMORRHAGIA Bleeding Cassification Size Location pathomechanism Hematoma: external or may be enclosed within a tissue petechiae : 1-2 mm hemorrhages into skin, mucous membranes, or serosal surfaces increased
Thrombolytic therapy should be the first line treatment in acute ishchemic stroke. We are against it!!
 Thrombolytic therapy should be the first line treatment in acute ishchemic stroke We are against it!! 85% of strokes are ischaemic, and related to blockage of an artery by a blood clot, so potential treatments
Thrombolytic therapy should be the first line treatment in acute ishchemic stroke We are against it!! 85% of strokes are ischaemic, and related to blockage of an artery by a blood clot, so potential treatments
Comparison of Five Major Recent Endovascular Treatment Trials
 Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
La gestione dell ictus ischemico o emorragico nel paziente sotto NAO
 La gestione dell ictus ischemico o emorragico nel paziente sotto NAO Antonio Carolei e Cindy Tiseo Clinica Neurologica e Stroke Unit Avezzano - Sulmona Università degli Studi dell Aquila Abano Terme, 10
La gestione dell ictus ischemico o emorragico nel paziente sotto NAO Antonio Carolei e Cindy Tiseo Clinica Neurologica e Stroke Unit Avezzano - Sulmona Università degli Studi dell Aquila Abano Terme, 10
Journal Club. 1. Develop a PICO (Population, Intervention, Comparison, Outcome) question for this study
 question for this study") Journal Club Articles for Discussion Tissue plasminogen activator for acute ischemic stroke. The National Institute of Neurological Disorders and Stroke rt-pa Stroke Study Group. N Engl J Med. 1995 Dec
Journal Club Articles for Discussion Tissue plasminogen activator for acute ischemic stroke. The National Institute of Neurological Disorders and Stroke rt-pa Stroke Study Group. N Engl J Med. 1995 Dec
Patients presenting with acute stroke while on DOACs
 Patients presenting with acute stroke while on DOACs Vemmos Kostas, MD, PhD Stroke Medicine Hellenic Cardiovascular Research Society Conflicts of interest Honoraria and speaker fees from: BAYER, SANOFI,
Patients presenting with acute stroke while on DOACs Vemmos Kostas, MD, PhD Stroke Medicine Hellenic Cardiovascular Research Society Conflicts of interest Honoraria and speaker fees from: BAYER, SANOFI,
An Overview of Non Vitamin-K Antagonist Oral Anticoagulants. Helen Williams Consultant Pharmacist for CV Disease South London
 An Overview of Non Vitamin-K Antagonist Oral Anticoagulants Helen Williams Consultant Pharmacist for CV Disease South London Contents Drugs and drug classes Licensed indications and NICE recommendations
An Overview of Non Vitamin-K Antagonist Oral Anticoagulants Helen Williams Consultant Pharmacist for CV Disease South London Contents Drugs and drug classes Licensed indications and NICE recommendations
Boehringer-Ingelheim satellite symposium Ligue cardiologique belge 13/05/2017
 Boehringer-Ingelheim satellite symposium Ligue cardiologique belge 13/05/2017 Dr André Peeters Service de Neurologie Cliniques Universitaires Saint-Luc / U.C.L. 1200 BRUXELLES Introduction 1. Aim NOACS
Boehringer-Ingelheim satellite symposium Ligue cardiologique belge 13/05/2017 Dr André Peeters Service de Neurologie Cliniques Universitaires Saint-Luc / U.C.L. 1200 BRUXELLES Introduction 1. Aim NOACS
FACTOR Xa AND PAR-1 BLOCKER : ATLAS-2, APPRAISE-2 & TRACER TRIALS
 New Horizons In Atherothrombosis Treatment 2012 순환기춘계학술대회 FACTOR Xa AND PAR-1 BLOCKER : ATLAS-2, APPRAISE-2 & TRACER TRIALS Division of Cardiology, Jeonbuk National University Medical School Jei Keon Chae,
New Horizons In Atherothrombosis Treatment 2012 순환기춘계학술대회 FACTOR Xa AND PAR-1 BLOCKER : ATLAS-2, APPRAISE-2 & TRACER TRIALS Division of Cardiology, Jeonbuk National University Medical School Jei Keon Chae,
Thrombolysis-WAKE UP Intra-arterial interventions DEFUSE 3 Haemorrhagic Stroke - TICH 2 Secondary Prevention CROMIS 2 Secondary Prevention NAVIGATE
 Thrombolysis-WAKE UP Intra-arterial interventions DEFUSE 3 Haemorrhagic Stroke - TICH 2 Secondary Prevention CROMIS 2 Secondary Prevention NAVIGATE ESUS Progression of haematoma Anticoagulation Large ICH
Thrombolysis-WAKE UP Intra-arterial interventions DEFUSE 3 Haemorrhagic Stroke - TICH 2 Secondary Prevention CROMIS 2 Secondary Prevention NAVIGATE ESUS Progression of haematoma Anticoagulation Large ICH
Overview of Stroke: Etiologies, Demographics, Syndromes, and Outcomes. Alex Abou-Chebl, MD, FSVIN Medical Director, Stroke Baptist Health Louisville
 Overview of Stroke: Etiologies, Demographics, Syndromes, and Outcomes Alex Abou-Chebl, MD, FSVIN Medical Director, Stroke Baptist Health Louisville Disclosure Statement of Financial Interest Within the
Overview of Stroke: Etiologies, Demographics, Syndromes, and Outcomes Alex Abou-Chebl, MD, FSVIN Medical Director, Stroke Baptist Health Louisville Disclosure Statement of Financial Interest Within the
The Worst Headache of My Life Hemorrhagic Stroke
 The Worst Headache of My Life Hemorrhagic Stroke Lindsay Trantum ACNP-BC Neurocritical Care Nurse Practitioner Assistant in Anesthesiology, Division of Critical Care Objectives Identify the risk factors
The Worst Headache of My Life Hemorrhagic Stroke Lindsay Trantum ACNP-BC Neurocritical Care Nurse Practitioner Assistant in Anesthesiology, Division of Critical Care Objectives Identify the risk factors
Emergency Department Management of Acute Ischemic Stroke
 Emergency Department Management of Acute Ischemic Stroke R. Jason Thurman, MD Associate Professor of Emergency Medicine and Neurosurgery Associate Director, Vanderbilt Stroke Center Vanderbilt University,
Emergency Department Management of Acute Ischemic Stroke R. Jason Thurman, MD Associate Professor of Emergency Medicine and Neurosurgery Associate Director, Vanderbilt Stroke Center Vanderbilt University,
Drug Class Review Newer Oral Anticoagulant Drugs
 Drug Class Review Newer Oral Anticoagulant Drugs Final Original Report May 2016 The purpose of reports is to make available information regarding the comparative clinical effectiveness and harms of different
Drug Class Review Newer Oral Anticoagulant Drugs Final Original Report May 2016 The purpose of reports is to make available information regarding the comparative clinical effectiveness and harms of different
Disclosures. Outline. Updated Recommendations for Using Alteplase (TPA) in Acute Ischemic Stroke
 in Acute Ischemic Stroke") Updated Recommendations for Using Alteplase (TPA) in Acute Ischemic Stroke Mark J. Alberts, MD, FAHA Chief of Neurology Hartford Hospital Hartford, CT Disclosures Dr. Alberts is a speaker and consultant
Updated Recommendations for Using Alteplase (TPA) in Acute Ischemic Stroke Mark J. Alberts, MD, FAHA Chief of Neurology Hartford Hospital Hartford, CT Disclosures Dr. Alberts is a speaker and consultant
Which drug do you prefer for stable CAD? - P2Y12 inhibitor
 Which drug do you prefer for stable CAD? - P2Y12 inhibitor Jung Rae Cho, MD, PhD Cardiovascular Division, Department of Internal Medicine Kangnam Sacred Heart Hospital, Hallym University Medical Center,
Which drug do you prefer for stable CAD? - P2Y12 inhibitor Jung Rae Cho, MD, PhD Cardiovascular Division, Department of Internal Medicine Kangnam Sacred Heart Hospital, Hallym University Medical Center,
Cerebrovascular Disease
 Neuropathology lecture series Cerebrovascular Disease Physiology of cerebral blood flow Brain makes up only 2% of body weight Percentage of cardiac output: 15-20% Percentage of O 2 consumption (resting):
Neuropathology lecture series Cerebrovascular Disease Physiology of cerebral blood flow Brain makes up only 2% of body weight Percentage of cardiac output: 15-20% Percentage of O 2 consumption (resting):
Coagulation Disorders. Dr. Muhammad Shamim Assistant Professor, BMU
 Coagulation Disorders Dr. Muhammad Shamim Assistant Professor, BMU 1 Introduction Local Vs. General Hematoma & Joint bleed Coagulation Skin/Mucosal Petechiae & Purpura PLT wound / surgical bleeding Immediate
Coagulation Disorders Dr. Muhammad Shamim Assistant Professor, BMU 1 Introduction Local Vs. General Hematoma & Joint bleed Coagulation Skin/Mucosal Petechiae & Purpura PLT wound / surgical bleeding Immediate
Reversal of Novel Oral Anticoagulants. Angelina The, MD March 22, 2016
 Reversal of Novel Oral Anticoagulants Angelina The, MD March 22, 2016 Argatroban Bivalirudin Enoxaparin Lepirudin Heparin Dabigatran Apixaban 1939 1954 1998 2000 1999 2001 10/2010 7/2011 12/2012 1/2015
Reversal of Novel Oral Anticoagulants Angelina The, MD March 22, 2016 Argatroban Bivalirudin Enoxaparin Lepirudin Heparin Dabigatran Apixaban 1939 1954 1998 2000 1999 2001 10/2010 7/2011 12/2012 1/2015
Thromboembolic Adverse Events After Use of Recombinant Human Coagulation Factor VIIa
 ORIGINAL CONTRIBUTION Thromboembolic Adverse Events After Use of Recombinant Human Coagulation Factor VIIa Kathryn A. O Connell, MD, PhD Jennifer J. Wood, PhD, MPH Robert P. Wise, MD, MPH Jay N. Lozier,
ORIGINAL CONTRIBUTION Thromboembolic Adverse Events After Use of Recombinant Human Coagulation Factor VIIa Kathryn A. O Connell, MD, PhD Jennifer J. Wood, PhD, MPH Robert P. Wise, MD, MPH Jay N. Lozier,
Debate: New Generation Anti-Coagulation Agents are a Better Choice than Warfarin in the Management of AF
 Debate: New Generation Anti-Coagulation Agents are a Better Choice than Warfarin in the Management of AF Bradley P. Knight, MD Director of Cardiac Electrophysiology Bluhm Cardiovascular Institute Northwestern
Debate: New Generation Anti-Coagulation Agents are a Better Choice than Warfarin in the Management of AF Bradley P. Knight, MD Director of Cardiac Electrophysiology Bluhm Cardiovascular Institute Northwestern
Neuropathology lecture series. III. Neuropathology of Cerebrovascular Disease. Physiology of cerebral blood flow
 Neuropathology lecture series III. Neuropathology of Cerebrovascular Disease Physiology of cerebral blood flow Brain makes up only 2% of body weight Percentage of cardiac output: 15-20% Percentage of O
Neuropathology lecture series III. Neuropathology of Cerebrovascular Disease Physiology of cerebral blood flow Brain makes up only 2% of body weight Percentage of cardiac output: 15-20% Percentage of O
Anticoagulation Therapy in LTC
 Anticoagulation Therapy in LTC By: Cynthia Leung, RPh, BScPhm, PharmD. Clinical Consultant Pharmacist MediSystem Pharmacy Jun 11, 2013 Agenda Stroke and Bleeding Risk Assessment Review of Oral Anticoagulation
Anticoagulation Therapy in LTC By: Cynthia Leung, RPh, BScPhm, PharmD. Clinical Consultant Pharmacist MediSystem Pharmacy Jun 11, 2013 Agenda Stroke and Bleeding Risk Assessment Review of Oral Anticoagulation
Disseminated intravascular coagulation (DIC) Dr. Klara Vezendi Szeged University Transfusiology Department
 Dr. Klara Vezendi Szeged University Transfusiology Department") Disseminated intravascular coagulation (DIC) Dr. Klara Vezendi Szeged University Transfusiology Department Disseminated intravascular coagulation (DIC, consumptive coagulopathy) is a clinicopathologic
Disseminated intravascular coagulation (DIC) Dr. Klara Vezendi Szeged University Transfusiology Department Disseminated intravascular coagulation (DIC, consumptive coagulopathy) is a clinicopathologic
WHITE PAPER: A GUIDE TO UNDERSTANDING SUBARACHNOID HEMORRHAGE
 WHITE PAPER: A GUIDE TO UNDERSTANDING SUBARACHNOID HEMORRHAGE Subarachnoid Hemorrhage is a serious, life-threatening type of hemorrhagic stroke caused by bleeding into the space surrounding the brain,
WHITE PAPER: A GUIDE TO UNDERSTANDING SUBARACHNOID HEMORRHAGE Subarachnoid Hemorrhage is a serious, life-threatening type of hemorrhagic stroke caused by bleeding into the space surrounding the brain,
DEPARTMENT OF HEALTH & HUMAN SERVICES Public Health Service
 M AY. 6. 2011 10:37 A M F D A - C D R H - O D E - P M O N O. 4147 P. 1 DEPARTMENT OF HEALTH & HUMAN SERVICES Public Health Service Food and Drug Administration 10903 New Hampshire Avenue Document Control
M AY. 6. 2011 10:37 A M F D A - C D R H - O D E - P M O N O. 4147 P. 1 DEPARTMENT OF HEALTH & HUMAN SERVICES Public Health Service Food and Drug Administration 10903 New Hampshire Avenue Document Control
11/23/2015. Disclosures. Stroke Management in the Neurocritical Care Unit. Karel Fuentes MD Medical Director of Neurocritical Care.
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination pulse 80/min reg, BP 160/95
Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination pulse 80/min reg, BP 160/95
5/2/2016. Outpatient Stroke Management Sheila Smith MD May 5, 2016
 Outpatient Stroke Management Sheila Smith MD May 5, 2016 1 Management of Outpatient Stroke Objectives Review blood pressure management post stroke Review antithrombotic therapy Review statin therapy Discuss
Outpatient Stroke Management Sheila Smith MD May 5, 2016 1 Management of Outpatient Stroke Objectives Review blood pressure management post stroke Review antithrombotic therapy Review statin therapy Discuss
Low Dose Rivaroxaban Versus Aspirin, in Addition to P2Y12 Inhibition, in Acute Coronary Syndromes (GEMINI-ACS-1)
") Low Dose Rivaroxaban Versus Aspirin, in Addition to P2Y12 Inhibition, in Acute Coronary Syndromes (GEMINI-ACS-1) Caitlin C. Akerman, PharmD PGY2 Cardiology Resident WakeMed Health & Hospitals Raleigh,
Low Dose Rivaroxaban Versus Aspirin, in Addition to P2Y12 Inhibition, in Acute Coronary Syndromes (GEMINI-ACS-1) Caitlin C. Akerman, PharmD PGY2 Cardiology Resident WakeMed Health & Hospitals Raleigh,
What s new with DOACs? Defining place in therapy for edoxaban &
 What s new with DOACs? Defining place in therapy for edoxaban & Use of DOACs in cardioversion Caitlin M. Gibson, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy University of North Texas
What s new with DOACs? Defining place in therapy for edoxaban & Use of DOACs in cardioversion Caitlin M. Gibson, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy University of North Texas
4/23/2009. September 15, 2008
 The Current Treatment of Deep Venous Thrombosis: Are We Doing Enough? George H. Meier, MD Professor and Chief Division of Vascular Surgery University of Cincinnati College of Medicine Cincinnati, Ohio
The Current Treatment of Deep Venous Thrombosis: Are We Doing Enough? George H. Meier, MD Professor and Chief Division of Vascular Surgery University of Cincinnati College of Medicine Cincinnati, Ohio
Thrombolysis administration
 Thrombolysis administration Liz Mackey Stroke Nurse Practitioner Western Health Sunshine & Footscray Hospital, Melbourne Thanks ASNEN committee members Skye Coote, Acute Stroke Nurse, Eastern Health (slide
Thrombolysis administration Liz Mackey Stroke Nurse Practitioner Western Health Sunshine & Footscray Hospital, Melbourne Thanks ASNEN committee members Skye Coote, Acute Stroke Nurse, Eastern Health (slide
Study design: Multicenter, randomized, controlled, cross-over, blinded PK comparison
 Brand Name 1, 2 : Rixubis Generic Name 1, 2 : Coagulation factor IX recombinant Manufacturer 5 : Baxter Drug Class 1, 2, 3 : Antihemophilic agent Labeled Uses 1, 2 : Hemophilia B hemorrhage, routine prophylaxis,
Brand Name 1, 2 : Rixubis Generic Name 1, 2 : Coagulation factor IX recombinant Manufacturer 5 : Baxter Drug Class 1, 2, 3 : Antihemophilic agent Labeled Uses 1, 2 : Hemophilia B hemorrhage, routine prophylaxis,
Definition พ.ญ.ส ธ ดา เย นจ นทร. Epidemiology. Definition 5/25/2016. Seizures after stroke Can we predict? Poststroke seizure
 Seizures after stroke Can we predict? พ.ญ.ส ธ ดา เย นจ นทร PMK Epilepsy Annual Meeting 2016 Definition Poststroke seizure : single or multiple convulsive episode(s) after stroke and thought to be related
Seizures after stroke Can we predict? พ.ญ.ส ธ ดา เย นจ นทร PMK Epilepsy Annual Meeting 2016 Definition Poststroke seizure : single or multiple convulsive episode(s) after stroke and thought to be related
Stroke Guidelines. November 19, 2011
 Stroke Guidelines November 19, 2011 Clinical Practice Guidelines American Stroke Association Guidelines are comprehensive statements that provide the highest level of scientific evidence for clinical practice.
Stroke Guidelines November 19, 2011 Clinical Practice Guidelines American Stroke Association Guidelines are comprehensive statements that provide the highest level of scientific evidence for clinical practice.
Management of Intracerebral Haemorrhage
 Management of Intracerebral Haemorrhage It s the worst type of stroke. Least treatable form of stroke Evidence-base limited most Overall mortality 35-50% Half of these would die within first 24 hours
Management of Intracerebral Haemorrhage It s the worst type of stroke. Least treatable form of stroke Evidence-base limited most Overall mortality 35-50% Half of these would die within first 24 hours
HEME 10 Bleeding Disorders
 HEME 10 Bleeding Disorders When injury occurs, three mechanisms occur Blood vessels Primary hemostasis Secondary hemostasis Diseases of the blood vessels Platelet disorders Thrombocytopenia Functional
HEME 10 Bleeding Disorders When injury occurs, three mechanisms occur Blood vessels Primary hemostasis Secondary hemostasis Diseases of the blood vessels Platelet disorders Thrombocytopenia Functional
ACUTE STROKE TREATMENT IN LARGE NIHSS PATIENTS. Justin Nolte, MD Assistant Profession Marshall University School of Medicine
 ACUTE STROKE TREATMENT IN LARGE NIHSS PATIENTS Justin Nolte, MD Assistant Profession Marshall University School of Medicine History of Presenting Illness 64 yo wf with PMHx of COPD, HTN, HLP who was in
ACUTE STROKE TREATMENT IN LARGE NIHSS PATIENTS Justin Nolte, MD Assistant Profession Marshall University School of Medicine History of Presenting Illness 64 yo wf with PMHx of COPD, HTN, HLP who was in
Adult Reversal of Anticoagulation and Anti-platelet Agents for Life- Threatening Bleeding or Emergency Surgery Protocol
 Adult Reversal of Anticoagulation and Anti-platelet Agents for Life- Threatening Bleeding or Emergency Surgery Protocol Page Platelet Inhibitors 2 Aspirin, Clopidogrel (Plavix), Prasugrel (Effient) & Ticagrelor
Adult Reversal of Anticoagulation and Anti-platelet Agents for Life- Threatening Bleeding or Emergency Surgery Protocol Page Platelet Inhibitors 2 Aspirin, Clopidogrel (Plavix), Prasugrel (Effient) & Ticagrelor
Guideline scope Subarachnoid haemorrhage caused by a ruptured aneurysm: diagnosis and management
 0 0 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Subarachnoid haemorrhage caused by a ruptured aneurysm: diagnosis and management The Department of Health and Social Care in England
0 0 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Subarachnoid haemorrhage caused by a ruptured aneurysm: diagnosis and management The Department of Health and Social Care in England
Clinical issues which drug for which patient
 Anticoagulants - a matter of heart! Towards a bright future? Clinical issues which drug for which patient Sabine Eichinger Dept. of Medicine I Medical University of Vienna/Austria Conflicts of interest
Anticoagulants - a matter of heart! Towards a bright future? Clinical issues which drug for which patient Sabine Eichinger Dept. of Medicine I Medical University of Vienna/Austria Conflicts of interest
Acute Stroke Care: the Nuts and Bolts of it. ECASS I and II ATLANTIS. Chris V. Fanale, MD Colorado Neurological Institute Swedish Medical Center
 Acute Stroke Care: the Nuts and Bolts of it Chris V. Fanale, MD Colorado Neurological Institute Swedish Medical Center ECASS I and II tpa for patients presenting
Acute Stroke Care: the Nuts and Bolts of it Chris V. Fanale, MD Colorado Neurological Institute Swedish Medical Center ECASS I and II tpa for patients presenting
Prevention of bleeding in surgical interventions or invasive procedures in congenital FVII deficiency (1.4)
") HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use NovoSeven RT safely and effectively. See full prescribing information for NovoSeven RT. NovoSeven
HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use NovoSeven RT safely and effectively. See full prescribing information for NovoSeven RT. NovoSeven
C. Michael Gibson, M.S., M.D. Professor of Medicine Harvard Medical School
 Novel Strategies to Prevent Pulmonary Embolism and DVT: APEX Trial and Substudies C. Michael Gibson, M.S., M.D. Professor of Medicine Harvard Medical School Conflict of Interest Statement 2 Present Research/Grant
Novel Strategies to Prevent Pulmonary Embolism and DVT: APEX Trial and Substudies C. Michael Gibson, M.S., M.D. Professor of Medicine Harvard Medical School Conflict of Interest Statement 2 Present Research/Grant
Disclosure Statement: Dr. Knoefel has nothing to disclose
 Stroke Janice E. Knoefel, MD, MPH Professor of Medicine & Neurology University of New Mexico Geriatrics/Extended Care (retired) New Mexico VA Healthcare System Albuquerque, NM Disclosure Statement: Dr.
Stroke Janice E. Knoefel, MD, MPH Professor of Medicine & Neurology University of New Mexico Geriatrics/Extended Care (retired) New Mexico VA Healthcare System Albuquerque, NM Disclosure Statement: Dr.