Modern Management of ICH
|
|
|
- Cleopatra Bates
- 5 years ago
- Views:
Transcription


1 Modern Management of ICH Bradley A. Gross, MD Assistant Professor, Dept of Neurosurgery, University of Pittsburgh October 2018


2 ICH Background Assessment & Diagnosis Medical Management Surgical Management 2/37

3 Background ICH accounts for 20% of all stroke Most common form of hemorrhagic stroke Meta Analysis of 36 Studies Incidence of 24.6/100,000 person-years No Sex Predilection Incidence Increases With Age Median 1 Month Fatality 40.4% ( %)
4 Primary IPH HTN CAA Secondary IPH AVM davf Cav Mal Mycotic Aneurysm Venous Sinus Thrombosis Moyamoya Vasculitis Hemorrhagic Tumor Hemorrhagic Ischemic Stroke
5 Case-Control Study in 22 Countries 3000 Cases (663 ICH) with 3000 controls Risk Factor OR of ICH Self-reported history of HTN or SBP > 160/ (99% CI ) Current Smoker 1.45 (99% CI ) 1-30 Drinks Per Month > 30 Drinks Per Month or Binge Drinker Non-HDL Cholesterol (Third vs First Tertile) HDL Cholesterol (Third vs First Tertile) 1.52 (99% CI ) 2.01 (99% CI ) 0.50 (99% CI ) 1.91 (99% CI )




6
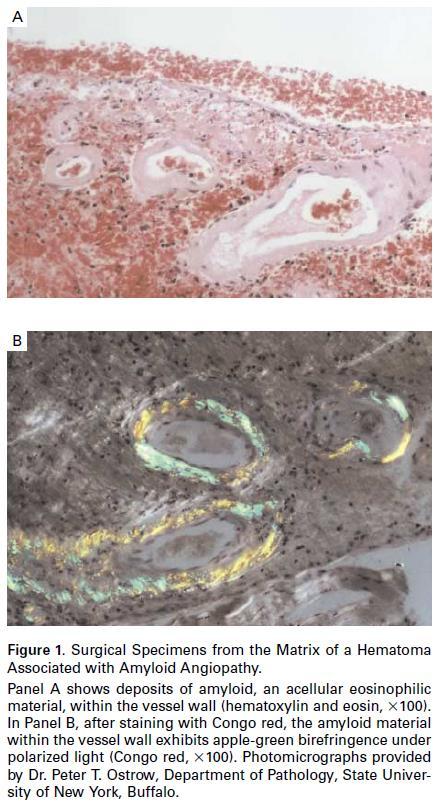
7


8 110 patients all undergoing autopsy with ICH
9 ICH Background Assessment & Diagnosis Medical Management Surgical Management 9/37
10 22% Deteriorate in Transport Crit Care Med 2008; 36: Presentation 23% GCS in ED deteriorate at least 2 points in ED Predictors: Antiplatelet use, ictus to ED arrival < 3 hours, Temp at least 37.5C, IVH, 2 mm or more MLS Acad Emerg Med 2012; 19: ED Evaluation: Time of Onset, PMH (HTN, Anticoagulant), Exam Ischemic/Hemorrhagic Stroke Acute Onset Focal Deficit HTN / Blood Pressure Lability Hemorrhagic Stroke Headache Nausea/Vomiting Depressed Mental Status
11
 CTA Positive Predictors (JNS 2012; 117: 761-766): Age < 65 (OR")
 No HTN (OR 515.")
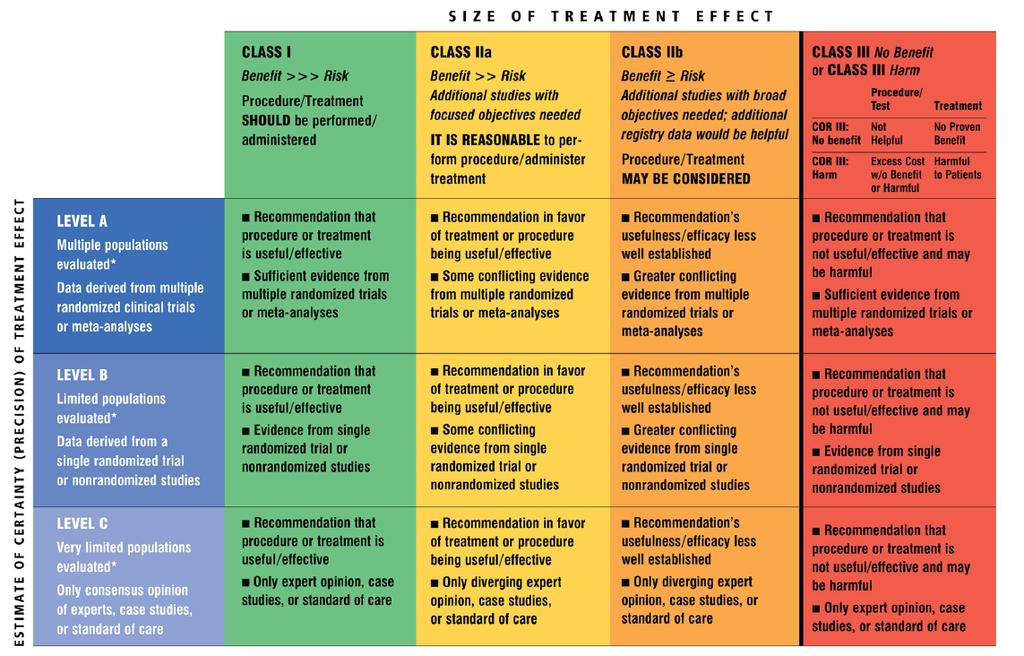
12 Diagnosis Rapid Imaging (Class I, Level A) Advanced Imaging For Underlying Lesion (Class IIa, Level B) CTA Positive Predictors (JNS 2012; 117: ): Age < 65 (OR 16.36) Female Sex (OR 14.9) Nonsmoker (OR 103.8) IVH Presence (OR 9.42) No HTN (OR ) HTN, older than 65 with basal ganglia / cerebellar bleed > negative CTA MRI DSA




13 63yo F HTN, HL, DM, smoker
14 Assessment Baseline Severity Score Should Be Performed Class I, Level of Evidence B ICH Score Factors Mortality GCS Score (3-4, 2 points; 5-12, 1 point) 0 points = 0% Age at least 80 (1 point) 1 point = 13% Infratentorial Hemorrhage Origin (1 point) 2 points = 26% Volume of at least 30 cc (1 point) 3 points = 72% Intraventricular Blood (1 point) 4 points = 97% 5 points = 100% Hemphill JC, et al. The ICH Score: a simple, reliable grading scale for intracerebral hemorrhage. Stroke 2001; 32:
15 ICH Background Assessment & Diagnosis Medical Management Surgical Management 15/37
 Coagulopathy Management ICU / Stroke Unit Admission (Class I, Level B) No: Prophylactic AED, rviia, Tranexamic Acid, Steroids GOAL: Mitigate Hematoma Growth, Improve")
16 Initial / Medical Management Secure Airway As Indicated Avoid Hyper/Hypoglycemia (Class I, Level C) AED if Seizure (Class I, Level A) Screening EKG and Tn (Class IIa, Level C) BP Control (< 140) Coagulopathy Management ICU / Stroke Unit Admission (Class I, Level B) No: Prophylactic AED, rviia, Tranexamic Acid, Steroids GOAL: Mitigate Hematoma Growth, Improve Outcome


17 What s the Deal with Blood Pressure?


18 INTEnsive blood pressure Reduction in Acute Cerebral Hemorrhage (INTERACT2) INTERACT-1 RCT in Lancet Neurol 2008 of 500 patients with less hematoma growth with SBP < 140 Spontaneous nonmassive ICH, GCS Patients SBP vs 1412 Patients SBP Initiated within 6 hours after bleed for next 7 days mrs 3-6 in 52.0% vs 55.6% at 3 months (p = 0.06); meets significance in ordinal analysis Serious Adverse Events 23.3% vs 23.6%.

19 Antihypertensive Treatment of Acute Cerebral Hemorrhage II (ATACH-2) ATACH feasibility and safety of three BP tiers in 60 patients (Crit Care Med 2010) Spontaneous Supratentorial ICH < 60 cc, GCS Patients SBP vs 500 Patients SBP via cardene gtt Initiated within 4.5 hours after symptom onset for next 24 hours with SBP > 180 mrs 4-6 in 38.7% vs 37.7% at 3 months Overall Treatment-Related Serious Adverse Events 1.6% vs 1.2% Hematoma Expansion (33% or more at 24 hours) 18.9% vs 24.4% (p = 0.08) Renal Adverse Events 9% vs 4% (p = 0.002) Mean SBP vs in two hours (150 vs 164 in INTERACT2)
 Reversal of Anticoagulation If VKA: PCC (Class IIb Level B), Vit K")
?")
20 Coagulopathy Management Repletion for Coagulation Factor Deficiency/Thrombocytopenia (Class I Level C) Reversal of Anticoagulation If VKA: PCC (Class IIb Level B), Vit K (Class I Level C) Hematoma growth: 19% if PCC vs 33% FFP FFP = fluid overload, similar thromboembolic complications Protamine Sulfate for Heparin (Class IIb Level C)? Reversal of Antiplatelet

 mrs 3-6 at 3 months 78% vs 82% (OR 1.75, 95% CI 0.77-3.97) Median ICH growth at 24 hours 2.01 vs 1.16 (p = 0.")
21 Spontaneous supratentorial ICH within 6 hrs of Sx Used antiplatelet for at least 7 days prior 78% Cox-I, 16% Cox-I + Dipyridamole, 3% ADP-I, 2% Cox-I + ADP-I GCS at least 8 97 transfusion vs 93 standard care Alive at 3 months 68% vs 77% (OR 0.62, 95% CI ) mrs 4-6 at 3 months 72% vs 56% (OR 2.04, 95% CI ) mrs 3-6 at 3 months 78% vs 82% (OR 1.75, 95% CI ) Median ICH growth at 24 hours 2.01 vs 1.16 (p = 0.81) Serious adverse event: 42% vs 29%.

22 ICU / Stroke Unit Admission (Class I, Level B) Greater chance of independence! Terent et al. JNNP 2009: 8206 patients in stroke unit vs 2871 on standard ward 3 month death / dependence 59% vs 75% (OR 0.59, 95% CI ) Early dysphagia screen (Class I, Level B) Intermittent Pneumatic Compression (Class I, Level A) CLOTS (Clots in Legs Or stockings after Stroke), Lancet 2013; 382: : DVT rate: 8.5% vs 12.1% (p < 0.05) SC Heparin / LMWH 1-4 days after stability (Class IIb, Level B)
 PE rate: 1.7% vs 2.9% (RR 0.")
 Mortality 16.1% vs. 20.")
23 UFH/LMWH within hr DVT rate: 3.3% vs 4.2%, (RR 0.77, 95% CI ) PE rate: 1.7% vs 2.9% (RR 0.37, 95% CI ) Hematoma Enlargement rate: 8.0% vs 4.0% (RR 1.42, 95% CI ) Mortality 16.1% vs. 20.9% (RR 0.76, 95% CI )
24 ICH Background Assessment & Diagnosis Medical Management Surgical Management 24/37
 Deteriorating Brainstem Compression/Hydrocephalus Supratentorial IPH Large Hematoma with shift (Class IIB,")
25 Neurosurgical Consultation Hydrocephalus 23% of all patients in STICH, 55% if IVH EVD Decreased LOC (Class IIa Level B) GCS < 9 (Class IIb, Level C) Surgical Evacuation > 3 cm Cerebellar IPH (Class I, Level B) Deteriorating Brainstem Compression/Hydrocephalus Supratentorial IPH Large Hematoma with shift (Class IIB, Level C)


26



27 6 mo mrs 2
 or")

28 1003 patients from 83 centres in 27 countries Minimum hematoma diameter of 2 cm, GCS at least 5 Early surgery (n = 503) or conservative treatment (n = 530) 6 month Favourable Outcome: 26% vs 24% GOS good recovery / moderate disability (OR 0.89, 95% CI )
 or conservative treatment (n = 294) 6 month Unfavourable Outcome: 59% vs 62% (p =")
29 601 patients from78 centres in 27 countries Superficial Hematoma cc (1 cm from surface), GCS 8+ Early surgery (n = 307) or conservative treatment (n = 294) 6 month Unfavourable Outcome: 59% vs 62% (p = 0.37)
30

 7 day mortality: 0% vs 1.9% (p = 0.")
 Asymptomatic Bleed: 22.2% vs 7.1% (p = 0.")
31 18-80 yo with spontaneous 20 cc + bleed MIS: Image Guided Placement of Catheter, Aspiration, rtpa rtpa 0.3 mg to 1.0 mg q8h up to 9 doses 54 MIS plus rtpa vs 42 Medical Care 30 day mortality: 9.5% vs 14.8% (p = 0.54) 7 day mortality: 0% vs 1.9% (p = 0.56) Symptomatic Bleed: 2.4% vs 9.3% (p = 0.23) Infection: 2.4% vs 0% (p = 0.43) Asymptomatic Bleed: 22.2% vs 7.1% (p = 0.051) MISTIE III: 180 day functional outcome comparison




32




33 39 cases Median GCS 10, 36 cc hematoma volume 52% mrs 2 or less, no mortality


34 ENRICH Early minimally invasive Removal of IntraCerebral Hemorrhage Age 18-80, GCS 5-14, cc IPH Brainpath vs medical management within 24 hours Primary outcome utility-weighted mrs at 180 days


35 Secondary ICH Etiology Dx Tx AVM CTA / DSA Surgery / SRS / Embolization davf CTA / DSA Embolization / Surgery Cavernous Malformation MRI Surgery Distal/Mycotic Aneurysm CTA / DSA Embolization/ Surgery Venous Sinus Thrombosis CTV Thrombectomy/Anticoagulation Moyamoya CTA / DSA Revascularization Vasculitis CTA / DSA Rx Tumor MRI / Surgery Surgery / SRS
36 Summary ICH accounts for 20% of all Stroke Median 1 month fatality 40% ICH Risk Factors: HTN, Smoking, EtOH, HDL Cholesterol CAA recurrent ICH rate: 7.4% / yr vs 1.1% / yr CAA Factors: SAH, Finger projections, Apoe4 Hemphill Score: GCS, Age > 80, Infratentorial, IVH, > 30 cc SBP < 140, Coagulopathy Management, ICU Admission EVD for hydrocephalus, Evacuate/Decompress if Cerebellar > 3 cm / Herniation Minimally Invasive Trials for Supratentorial Bleeds


37 Acknowledgments
SCCEP 2013 LLSA Course Article 10 AHA/ASA Guidelines for the Management of Spontaneous ICH
 SCCEP 2013 LLSA Course Article 10 AHA/ASA Guidelines for the Management of Spontaneous ICH Morgenstern LB, Hemphill JC. Stroke July 2010;41:2108-2129. Article: This article presents guidelines whose "aim
SCCEP 2013 LLSA Course Article 10 AHA/ASA Guidelines for the Management of Spontaneous ICH Morgenstern LB, Hemphill JC. Stroke July 2010;41:2108-2129. Article: This article presents guidelines whose "aim
Recombinant Factor VIIa for Intracerebral Hemorrhage
 Recombinant Factor VIIa for Intracerebral Hemorrhage January 24, 2006 Justin Lee Pharmacy Resident University Health Network Outline 1. Introduction to patient case 2. Overview of intracerebral hemorrhage
Recombinant Factor VIIa for Intracerebral Hemorrhage January 24, 2006 Justin Lee Pharmacy Resident University Health Network Outline 1. Introduction to patient case 2. Overview of intracerebral hemorrhage
Treatment of Acute Hemorrhagic Stroke 5th QSVS Neurovascular Conference Dar Dowlatshahi MD PhD FRCPC Sept 14, 2012
 Treatment of Acute Hemorrhagic Stroke 5th QSVS Neurovascular Conference Dar Dowlatshahi MD PhD FRCPC Sept 14, 2012 Disclosure of potential conflicts of interest Quebec Society of Vascular Sciences presents
Treatment of Acute Hemorrhagic Stroke 5th QSVS Neurovascular Conference Dar Dowlatshahi MD PhD FRCPC Sept 14, 2012 Disclosure of potential conflicts of interest Quebec Society of Vascular Sciences presents
Controversies in Hemorrhagic Stroke Management. Sarah L. Livesay, DNP, RN, ACNP-BC, ACNS-BC Associate Professor Rush University
 Controversies in Hemorrhagic Stroke Management Sarah L. Livesay, DNP, RN, ACNP-BC, ACNS-BC Associate Professor Rush University Disclosures AHA/ASA Outline Blood pressure VTE Coagulopathy Early mobilization
Controversies in Hemorrhagic Stroke Management Sarah L. Livesay, DNP, RN, ACNP-BC, ACNS-BC Associate Professor Rush University Disclosures AHA/ASA Outline Blood pressure VTE Coagulopathy Early mobilization
Benjamin Anyanwu,MD Medical Director In-patient Neurology and Neuroscience ICU Novant Health Forsyth Medical Center, Winston-Salem NC
 Benjamin Anyanwu,MD Medical Director In-patient Neurology and Neuroscience ICU Novant Health Forsyth Medical Center, Winston-Salem NC Emergency Treatment of Hemorrhagic Stroke Objectives Discuss the etiology
Benjamin Anyanwu,MD Medical Director In-patient Neurology and Neuroscience ICU Novant Health Forsyth Medical Center, Winston-Salem NC Emergency Treatment of Hemorrhagic Stroke Objectives Discuss the etiology
Neurosurgical Management of Stroke
 Overview Hemorrhagic Stroke Ischemic Stroke Aneurysmal Subarachnoid hemorrhage Neurosurgical Management of Stroke Jesse Liu, MD Instructor, Neurological Surgery Initial management In hospital management
Overview Hemorrhagic Stroke Ischemic Stroke Aneurysmal Subarachnoid hemorrhage Neurosurgical Management of Stroke Jesse Liu, MD Instructor, Neurological Surgery Initial management In hospital management
North Oaks Trauma Symposium Friday, November 3, 2017
 Traumatic Intracranial Hemorrhage Aaron C. Sigler, DO, MS Neurosurgery Tulane Neurosciences None Disclosures Overview Anatomy Epidural hematoma Subdural hematoma Cerebral contusions Outline Traumatic ICH
Traumatic Intracranial Hemorrhage Aaron C. Sigler, DO, MS Neurosurgery Tulane Neurosciences None Disclosures Overview Anatomy Epidural hematoma Subdural hematoma Cerebral contusions Outline Traumatic ICH
Starting or Resuming Anticoagulation or Antiplatelet Therapy after ICH: A Neurology Perspective
 Starting or Resuming Anticoagulation or Antiplatelet Therapy after ICH: A Neurology Perspective Cathy Sila MD George M Humphrey II Professor and Vice Chair of Neurology Director, Comprehensive Stroke Center
Starting or Resuming Anticoagulation or Antiplatelet Therapy after ICH: A Neurology Perspective Cathy Sila MD George M Humphrey II Professor and Vice Chair of Neurology Director, Comprehensive Stroke Center
The Worst Headache of My Life Hemorrhagic Stroke
 The Worst Headache of My Life Hemorrhagic Stroke Lindsay Trantum ACNP-BC Neurocritical Care Nurse Practitioner Assistant in Anesthesiology, Division of Critical Care Objectives Identify the risk factors
The Worst Headache of My Life Hemorrhagic Stroke Lindsay Trantum ACNP-BC Neurocritical Care Nurse Practitioner Assistant in Anesthesiology, Division of Critical Care Objectives Identify the risk factors
UPSTATE Comprehensive Stroke Center. Neurosurgical Interventions Satish Krishnamurthy MD, MCh
 UPSTATE Comprehensive Stroke Center Neurosurgical Interventions Satish Krishnamurthy MD, MCh Regional cerebral blood flow is important Some essential facts Neurons are obligatory glucose users Under anerobic
UPSTATE Comprehensive Stroke Center Neurosurgical Interventions Satish Krishnamurthy MD, MCh Regional cerebral blood flow is important Some essential facts Neurons are obligatory glucose users Under anerobic
Hypertensive Haemorrhagic Stroke. Dr Philip Lam Thuon Mine
 Hypertensive Haemorrhagic Stroke Dr Philip Lam Thuon Mine Intracerebral Haemorrhage Primary ICH Spontaneous rupture of small vessels damaged by HBP Basal ganglia, thalamus, pons and cerebellum Amyloid
Hypertensive Haemorrhagic Stroke Dr Philip Lam Thuon Mine Intracerebral Haemorrhage Primary ICH Spontaneous rupture of small vessels damaged by HBP Basal ganglia, thalamus, pons and cerebellum Amyloid
Intracerebral Hemorrhage
 Review of Primary Intracerebral Hemorrhage Réza Behrouz, DO Assistant Professor of Neurology University of South Florida College of Medicine STROKE 85% ISCHEMIC 15% HEMORRHAGIC HEMORRHAGIC STROKE 1/3 Subarachnoid
Review of Primary Intracerebral Hemorrhage Réza Behrouz, DO Assistant Professor of Neurology University of South Florida College of Medicine STROKE 85% ISCHEMIC 15% HEMORRHAGIC HEMORRHAGIC STROKE 1/3 Subarachnoid
Management of Intracerebral Haemorrhage
 Management of Intracerebral Haemorrhage It s the worst type of stroke. Least treatable form of stroke Evidence-base limited most Overall mortality 35-50% Half of these would die within first 24 hours
Management of Intracerebral Haemorrhage It s the worst type of stroke. Least treatable form of stroke Evidence-base limited most Overall mortality 35-50% Half of these would die within first 24 hours
Intracerebral Hemorrhage
 Update on Intracerebral Hemorrhage November 8, 2013 Anne E. O Duffy, MD Assistant Professor of Neurology Stroke Division Intracerebral Hemorrhage Traumatic Spontaneous Primary (80-88%): due to spontaneous
Update on Intracerebral Hemorrhage November 8, 2013 Anne E. O Duffy, MD Assistant Professor of Neurology Stroke Division Intracerebral Hemorrhage Traumatic Spontaneous Primary (80-88%): due to spontaneous
How Low Should You Go? Management of Blood Pressure in Intracranial Hemorrhage
 How Low Should You Go? Management of Blood Pressure in Intracranial Hemorrhage Rachael Scott, Pharm.D. PGY2 Critical Care Pharmacy Resident Pharmacy Grand Rounds August 21, 2018 2018 MFMER slide-1 Patient
How Low Should You Go? Management of Blood Pressure in Intracranial Hemorrhage Rachael Scott, Pharm.D. PGY2 Critical Care Pharmacy Resident Pharmacy Grand Rounds August 21, 2018 2018 MFMER slide-1 Patient
CLEAR III TRIAL : UPDATE ON SURGICAL MATTERS THAT MATTER
 CLEAR III TRIAL : UPDATE ON SURGICAL MATTERS THAT MATTER CLEAR Surgical Center Team July 2011 Trial Enrollment Status Updates Insert latest enrollment update chart from most recent CLEAR newsletter Imaging
CLEAR III TRIAL : UPDATE ON SURGICAL MATTERS THAT MATTER CLEAR Surgical Center Team July 2011 Trial Enrollment Status Updates Insert latest enrollment update chart from most recent CLEAR newsletter Imaging
Outlook for intracerebral haemorrhage after a MISTIE spell
 Outlook for intracerebral haemorrhage after a MISTIE spell David J Werring PhD FRCP Stroke Research Centre, Department of Brain Repair and Rehabilitation, UCL Institute of Neurology, National Hospital
Outlook for intracerebral haemorrhage after a MISTIE spell David J Werring PhD FRCP Stroke Research Centre, Department of Brain Repair and Rehabilitation, UCL Institute of Neurology, National Hospital
4/10/2018. The Surgical Treatment of Cerebral Aneurysms. Aneurysm Locations. Aneurysmal Subarachnoid Hemorrhage. Jerone Kennedy, M.D.
 The Surgical Treatment of Cerebral Aneurysms Aneurysmal Subarachnoid Hemorrhage Jerone Kennedy, M.D. Medical Director, Vascular Neurosurgery CentraCare Health-Neurosciences St. Cloud Hospital Aneurysm
The Surgical Treatment of Cerebral Aneurysms Aneurysmal Subarachnoid Hemorrhage Jerone Kennedy, M.D. Medical Director, Vascular Neurosurgery CentraCare Health-Neurosciences St. Cloud Hospital Aneurysm
Tyler Carson D.O., Vladamir Cortez D.O., Dan E. Miulli D.O.
 Bedside Intracranial Hematoma Evacuation and Intraparenchymal Drain Placement for Spontaneous Intracranial Hematoma Larger than 30 cc in Volume: Institutional Experience and Patient Outcomes Tyler Carson
Bedside Intracranial Hematoma Evacuation and Intraparenchymal Drain Placement for Spontaneous Intracranial Hematoma Larger than 30 cc in Volume: Institutional Experience and Patient Outcomes Tyler Carson
Intracranial spontaneous hemorrhage mechanisms, imaging and management
 Intracranial spontaneous hemorrhage mechanisms, imaging and management Dora Zlatareva Department of Diagnostic Imaging Medical University, Sofia, Bulgaria Intracranial hemorrhage (ICH) ICH 15% of strokes
Intracranial spontaneous hemorrhage mechanisms, imaging and management Dora Zlatareva Department of Diagnostic Imaging Medical University, Sofia, Bulgaria Intracranial hemorrhage (ICH) ICH 15% of strokes
Stroke - Intracranial hemorrhage. Dr. Amitesh Aggarwal Associate Professor Department of Medicine
 Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
Intracerebral Hemorrhage
 Intracerebral Hemorrhage J. Claude Hemphill III, MD, MAS Kenneth Rainin Chair in Neurocritical Care Professor of Clinical Neurology and Neurological Surgery University of California, San Francisco Director,
Intracerebral Hemorrhage J. Claude Hemphill III, MD, MAS Kenneth Rainin Chair in Neurocritical Care Professor of Clinical Neurology and Neurological Surgery University of California, San Francisco Director,
Surgical Management of Stroke Brandon Evans, MD Department of Neurosurgery
 Surgical Management of Stroke Brandon Evans, MD Department of Neurosurgery 2 Stroke Stroke kills almost 130,000 Americans each year. - Third cause of all deaths in Arkansas. - Death Rate is highest in
Surgical Management of Stroke Brandon Evans, MD Department of Neurosurgery 2 Stroke Stroke kills almost 130,000 Americans each year. - Third cause of all deaths in Arkansas. - Death Rate is highest in
[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]
![[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]](/thumbs/89/98619893.jpg "[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]") 2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
The management of ICH when to operate when not to?
 The management of ICH when to operate when not to? Intracranial Hemorrhage High Incidence o Accounts for 10-15% of all strokes 1,2,5 o 80,000 cases in US; 2 million WW 2,5 o Incidence doubles for African-
The management of ICH when to operate when not to? Intracranial Hemorrhage High Incidence o Accounts for 10-15% of all strokes 1,2,5 o 80,000 cases in US; 2 million WW 2,5 o Incidence doubles for African-
Klinikum Frankfurt Höchst
 Blood pressure management in hemorrhagic stroke Blood pressure in acute ICH Do we need additional trials after INTERACT2 and ATTACH-II? Focus.de Department of Neurology,, Germany Department of Neurology,
Blood pressure management in hemorrhagic stroke Blood pressure in acute ICH Do we need additional trials after INTERACT2 and ATTACH-II? Focus.de Department of Neurology,, Germany Department of Neurology,
A few Neurosurgical Emergencies. Cathrin Parsch Lyell Mc Ewin Hospital SA Ambulance Service SAAS medstar Spring Seminar on Emergency Medicine 2015
 A few Neurosurgical Emergencies Cathrin Parsch Lyell Mc Ewin Hospital SA Ambulance Service SAAS medstar Spring Seminar on Emergency Medicine 2015 Outline Neuroanatomy and physiology (85 slides ) Raised
A few Neurosurgical Emergencies Cathrin Parsch Lyell Mc Ewin Hospital SA Ambulance Service SAAS medstar Spring Seminar on Emergency Medicine 2015 Outline Neuroanatomy and physiology (85 slides ) Raised
SPONTANEOUS INTRACEREBRAL HEMORRHAGE: MEDICAL MANAGEMENT. Neeraj Naval, MD Baptist Neurological Institute
 SPONTANEOUS INTRACEREBRAL HEMORRHAGE: MEDICAL MANAGEMENT Neeraj Naval, MD Baptist Neurological Institute Disclosures/ COI Nothing to disclose (what happens in Vegas stays in Vegas) No Conflict of interest
SPONTANEOUS INTRACEREBRAL HEMORRHAGE: MEDICAL MANAGEMENT Neeraj Naval, MD Baptist Neurological Institute Disclosures/ COI Nothing to disclose (what happens in Vegas stays in Vegas) No Conflict of interest
Hemorrhagic Stroke. Team Members: Nawaf Aldarwish, Rawan Alqahtani, Talal AlTukhaim, Fatima Altassan.
 Hemorrhagic Stroke Objectives: Introduction Etiology Pathophysiology Clinical presentation Diagnosis and Imaging Treatment Team Members: Nawaf Aldarwish, Rawan Alqahtani, Talal AlTukhaim, Fatima Altassan.
Hemorrhagic Stroke Objectives: Introduction Etiology Pathophysiology Clinical presentation Diagnosis and Imaging Treatment Team Members: Nawaf Aldarwish, Rawan Alqahtani, Talal AlTukhaim, Fatima Altassan.
Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข
 Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข Emergency start at community level: Prehospital care Acute stroke
Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข Emergency start at community level: Prehospital care Acute stroke
Review of the TICH-2 Trial
 Review of the TICH-2 Trial Mikaela Hofer, PharmD PGY-1 Pharmacy Resident Pharmacy Grand Rounds September 18, 2018 2018 MFMER slide-1 Objectives Review the pharmacologic options to limit hematoma expansion
Review of the TICH-2 Trial Mikaela Hofer, PharmD PGY-1 Pharmacy Resident Pharmacy Grand Rounds September 18, 2018 2018 MFMER slide-1 Objectives Review the pharmacologic options to limit hematoma expansion
Jan 5, Coma 8 years. Jan 11, 2014
 Jan 5, 2006 Coma 8 years Jan 11, 2014 CT Scan of Head showing large right frontal ICH The Intracerebral Hemorrhage: Team Approach Rodney Leacock MD Introduction Intracerebral hemorrhage (ICH) is a very
Jan 5, 2006 Coma 8 years Jan 11, 2014 CT Scan of Head showing large right frontal ICH The Intracerebral Hemorrhage: Team Approach Rodney Leacock MD Introduction Intracerebral hemorrhage (ICH) is a very
Overview. Introduction. New Interventions for Acute Stroke. New Approaches to hemorrhagic Strokes
 Overview New Interventions for Acute Stroke Paula Eboli, MD Department of Neurosurgery Rockwood Clinic, Deaconess Hospital Introduction New Approaches to hemorrhagic Strokes New Approaches to Ischemic
Overview New Interventions for Acute Stroke Paula Eboli, MD Department of Neurosurgery Rockwood Clinic, Deaconess Hospital Introduction New Approaches to hemorrhagic Strokes New Approaches to Ischemic
Welcome to our Quarterly MISTIE III Safety Forum April 6, 2016
 Welcome to our Quarterly MISTIE III Safety Forum April 6, 2016 Agenda: Update from our Surgical Centers: Where we stand surgically Issam Awad, MD, University of Chicago Vascular Defect Screening in MISTIE
Welcome to our Quarterly MISTIE III Safety Forum April 6, 2016 Agenda: Update from our Surgical Centers: Where we stand surgically Issam Awad, MD, University of Chicago Vascular Defect Screening in MISTIE
SPONTANEOUS INTRACEREBRAL HEMORRHAGE
 SPONTANEOUS INTRACEREBRAL HEMORRHAGE Intracerebral hemorrhageis an acute and spontaneous extravasationof blood into the brain parenchyma that may extend into the ventricles and subarachnoid space. It is
SPONTANEOUS INTRACEREBRAL HEMORRHAGE Intracerebral hemorrhageis an acute and spontaneous extravasationof blood into the brain parenchyma that may extend into the ventricles and subarachnoid space. It is
Stroke Guidelines. November 19, 2011
 Stroke Guidelines November 19, 2011 Clinical Practice Guidelines American Stroke Association Guidelines are comprehensive statements that provide the highest level of scientific evidence for clinical practice.
Stroke Guidelines November 19, 2011 Clinical Practice Guidelines American Stroke Association Guidelines are comprehensive statements that provide the highest level of scientific evidence for clinical practice.
Giuseppe Micieli Dipartimento di Neurologia d Urgenza IRCCS Fondazione Istituto Neurologico Nazionale C Mondino, Pavia
 Giuseppe Micieli Dipartimento di Neurologia d Urgenza IRCCS Fondazione Istituto Neurologico Nazionale C Mondino, Pavia Charidimou et al, 2012 Pathogenesis of spontaneous and anticoagulationassociated
Giuseppe Micieli Dipartimento di Neurologia d Urgenza IRCCS Fondazione Istituto Neurologico Nazionale C Mondino, Pavia Charidimou et al, 2012 Pathogenesis of spontaneous and anticoagulationassociated
CEREBRO VASCULAR ACCIDENTS
 CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
Life after ARUBA: Management of Unruptured Brain Arteriovenous Malformations (AVMs)
") Life after ARUBA: Management of Unruptured Brain Arteriovenous Malformations (AVMs) Eric L. Zager, MD University of Pennsylvania Department of Neurosurgery No Disclosures Brain AVMs Incidence ~1 in 100,000
Life after ARUBA: Management of Unruptured Brain Arteriovenous Malformations (AVMs) Eric L. Zager, MD University of Pennsylvania Department of Neurosurgery No Disclosures Brain AVMs Incidence ~1 in 100,000
Update on Guidelines for Traumatic Brain Injury
 Update on Guidelines for Traumatic Brain Injury Current TBI Guidelines Shirley I. Stiver MD, PhD Department of Neurosurgery Guidelines for the management of traumatic brain injury Journal of Neurotrauma
Update on Guidelines for Traumatic Brain Injury Current TBI Guidelines Shirley I. Stiver MD, PhD Department of Neurosurgery Guidelines for the management of traumatic brain injury Journal of Neurotrauma
Objectives. Definition 3/21/2017. Spontaneous, Nontraumatic Intracerebral Hemorrhage
 Management of Spontaneous Intracerebral Hemorrhage (ICH) Mindy Mason, MSN, RN, ACNP-BC University of New Mexico Academic Medical Center Level I Trauma Center 24 bed Neuroscience ICU Albuquerque, NM Objectives
Management of Spontaneous Intracerebral Hemorrhage (ICH) Mindy Mason, MSN, RN, ACNP-BC University of New Mexico Academic Medical Center Level I Trauma Center 24 bed Neuroscience ICU Albuquerque, NM Objectives
New Frontiers in Intracerebral Hemorrhage
 New Frontiers in Intracerebral Hemorrhage Ryan Hakimi, DO, MS Director, Neuro ICU Director, Inpatient Neurology Services Greenville Health System Clinical Associate Professor Department of Medicine (Neurology)
New Frontiers in Intracerebral Hemorrhage Ryan Hakimi, DO, MS Director, Neuro ICU Director, Inpatient Neurology Services Greenville Health System Clinical Associate Professor Department of Medicine (Neurology)
Angel J. Lacerda MD PhD, Daisy Abreu MD, Julio A. Díaz MD, Sandro Perez MD, Julio C Martin MD, Daiyan Martin MD.
 Angel J. Lacerda MD PhD, Daisy Abreu MD, Julio A. Díaz MD, Sandro Perez MD, Julio C Martin MD, Daiyan Martin MD. Introduction: Spontaneous intracerebral haemorrhage (SICH) represents one of the most severe
Angel J. Lacerda MD PhD, Daisy Abreu MD, Julio A. Díaz MD, Sandro Perez MD, Julio C Martin MD, Daiyan Martin MD. Introduction: Spontaneous intracerebral haemorrhage (SICH) represents one of the most severe
Symptoms of small vessel strokes. Small Vessel stroke. What is this? Treatment. Large Vessel stroke 6/1/2018
 Stroke Stroke Megan Stevens MD Vascular Neurology SUDDEN Maximal at onset Lateralized weakness, lateralized numbness, vision loss (one eye or portion of field in both eyes), double vision, slurred speech,
Stroke Stroke Megan Stevens MD Vascular Neurology SUDDEN Maximal at onset Lateralized weakness, lateralized numbness, vision loss (one eye or portion of field in both eyes), double vision, slurred speech,
Intracranial Hemorrhage. Objectives. What Do Need to Know?
 Intracranial Hemorrhage What Do Need to Know? Kerry Brega, MD Associate Professor of Neurosurgery University of Colorado Objectives Know the common types of ICH. Know how they can be differentiated. Know
Intracranial Hemorrhage What Do Need to Know? Kerry Brega, MD Associate Professor of Neurosurgery University of Colorado Objectives Know the common types of ICH. Know how they can be differentiated. Know
AHA/ASA Guideline. by guest on September 29, 2016
 AHA/ASA Guideline Guidelines for the Management of Spontaneous Intracerebral Hemorrhage A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association The American
AHA/ASA Guideline Guidelines for the Management of Spontaneous Intracerebral Hemorrhage A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association The American
DVT PROPHYLAXIS IN HOSPITALIZED MEDICAL PATIENTS SAURABH MAJI SR (PULMONARY,MEDICINE)
") DVT PROPHYLAXIS IN HOSPITALIZED MEDICAL PATIENTS SAURABH MAJI SR (PULMONARY,MEDICINE) Introduction VTE (DVT/PE) is an important complication in hospitalized patients Hospitalization for acute medical illness
DVT PROPHYLAXIS IN HOSPITALIZED MEDICAL PATIENTS SAURABH MAJI SR (PULMONARY,MEDICINE) Introduction VTE (DVT/PE) is an important complication in hospitalized patients Hospitalization for acute medical illness
Developing, implementing and scaling up an acute care bundle for intracerebral haemorrhage in Greater Manchester
 Developing, implementing and scaling up an acute care bundle for intracerebral haemorrhage in Greater Manchester Adrian Parry-Jones NIHR Clinician Scientist & Honorary Consultant Neurologist Manchester
Developing, implementing and scaling up an acute care bundle for intracerebral haemorrhage in Greater Manchester Adrian Parry-Jones NIHR Clinician Scientist & Honorary Consultant Neurologist Manchester
Stroke: What did we learn in the last year?
 Stroke: What did we learn in the last year? J. Claude Hemphill III, MD, MAS Associate Professor of Clinical Neurology and Neurological Surgery University of California, San Francisco Director, Neurocritical
Stroke: What did we learn in the last year? J. Claude Hemphill III, MD, MAS Associate Professor of Clinical Neurology and Neurological Surgery University of California, San Francisco Director, Neurocritical
Lothian Audit of the Treatment of Cerebral Haemorrhage (LATCH)
") 1. INTRODUCTION Stroke physicians, emergency department doctors, and neurologists are often unsure about which patients they should refer for neurosurgical intervention. Early neurosurgical evacuation
1. INTRODUCTION Stroke physicians, emergency department doctors, and neurologists are often unsure about which patients they should refer for neurosurgical intervention. Early neurosurgical evacuation
Patients presenting with acute stroke while on DOACs
 Patients presenting with acute stroke while on DOACs Vemmos Kostas, MD, PhD Stroke Medicine Hellenic Cardiovascular Research Society Conflicts of interest Honoraria and speaker fees from: BAYER, SANOFI,
Patients presenting with acute stroke while on DOACs Vemmos Kostas, MD, PhD Stroke Medicine Hellenic Cardiovascular Research Society Conflicts of interest Honoraria and speaker fees from: BAYER, SANOFI,
Definition พ.ญ.ส ธ ดา เย นจ นทร. Epidemiology. Definition 5/25/2016. Seizures after stroke Can we predict? Poststroke seizure
 Seizures after stroke Can we predict? พ.ญ.ส ธ ดา เย นจ นทร PMK Epilepsy Annual Meeting 2016 Definition Poststroke seizure : single or multiple convulsive episode(s) after stroke and thought to be related
Seizures after stroke Can we predict? พ.ญ.ส ธ ดา เย นจ นทร PMK Epilepsy Annual Meeting 2016 Definition Poststroke seizure : single or multiple convulsive episode(s) after stroke and thought to be related
Protocol for IV rtpa Treatment of Acute Ischemic Stroke
 Protocol for IV rtpa Treatment of Acute Ischemic Stroke Acute stroke management is progressing very rapidly. Our team offers several options for acute stroke therapy, including endovascular therapy and
Protocol for IV rtpa Treatment of Acute Ischemic Stroke Acute stroke management is progressing very rapidly. Our team offers several options for acute stroke therapy, including endovascular therapy and
Use of Anticoagulant Reversal Agents
 Use of Anticoagulant Reversal Agents Lori Shutter, MD shutterla@upmc.edu Vice Chair of Education Director, Neurocritical Care Program Professor, Critical Care Medicine, Neurology & Neurosurgery University
Use of Anticoagulant Reversal Agents Lori Shutter, MD shutterla@upmc.edu Vice Chair of Education Director, Neurocritical Care Program Professor, Critical Care Medicine, Neurology & Neurosurgery University
2018 Early Management of Acute Ischemic Stroke Guidelines Update
 2018 Early Management of Acute Ischemic Stroke Guidelines Update Brandi Bowman, PhC, Pharm.D. April 17, 2018 Pharmacist Objectives Describe the recommendations for emergency medical services and hospital
2018 Early Management of Acute Ischemic Stroke Guidelines Update Brandi Bowman, PhC, Pharm.D. April 17, 2018 Pharmacist Objectives Describe the recommendations for emergency medical services and hospital
ENDOVASCULAR TREATMENT OF CEREBRAL ANEURYSMS AND MANAGEMENT OF RUPTURED ANEURYSM. Vikram Jadhav MD, PhD. 04/12/2018 CentraCare Health St.
 ENDOVASCULAR TREATMENT OF CEREBRAL ANEURYSMS AND MANAGEMENT OF RUPTURED ANEURYSM Vikram Jadhav MD, PhD 04/12/2018 CentraCare Health St. Cloud, MN OBJECTIVES Understand epidemiology and risk factors for
ENDOVASCULAR TREATMENT OF CEREBRAL ANEURYSMS AND MANAGEMENT OF RUPTURED ANEURYSM Vikram Jadhav MD, PhD 04/12/2018 CentraCare Health St. Cloud, MN OBJECTIVES Understand epidemiology and risk factors for
TIA: Updates and Management 2008
 TIA: Updates and Management 2008 S. Andrew Josephson, MD Department of Neurology, Neurovascular Division University of California San Francisco Commonly Held TIA Misconceptions TIA is easy to diagnose
TIA: Updates and Management 2008 S. Andrew Josephson, MD Department of Neurology, Neurovascular Division University of California San Francisco Commonly Held TIA Misconceptions TIA is easy to diagnose
Stroke ESO.org. Csiba László.
 Stroke ESO.org Csiba László csiba@dote.hu Global mortality Cause of death Dept. of Neurology? 1938-1950 1990-2002 Tumor Stroke Tumor Infect. Stroke Normal lifestyle After MI 70-80% After stroke 10% Differential
Stroke ESO.org Csiba László csiba@dote.hu Global mortality Cause of death Dept. of Neurology? 1938-1950 1990-2002 Tumor Stroke Tumor Infect. Stroke Normal lifestyle After MI 70-80% After stroke 10% Differential
Pelvic Inflammatory Disease
 The Articles Pelvic Inflammatory Disease Brunham RC, Gottlieb SL, Paavonen J. Pelvic inflammatory disease. N Engl J Med 2015 May;372(21):2039-48. 2018 LLSA Article Review Shared Decision-making Hess EP,
The Articles Pelvic Inflammatory Disease Brunham RC, Gottlieb SL, Paavonen J. Pelvic inflammatory disease. N Engl J Med 2015 May;372(21):2039-48. 2018 LLSA Article Review Shared Decision-making Hess EP,
Vascular Malformations of the Brain: A Review of Imaging Features and Risks
 Vascular Malformations of the Brain: A Review of Imaging Features and Risks Comprehensive Neuroradiology: Best Practices October 27-30, 2016 Sudhakar R. Satti, MD Associate Director Neurointerventional
Vascular Malformations of the Brain: A Review of Imaging Features and Risks Comprehensive Neuroradiology: Best Practices October 27-30, 2016 Sudhakar R. Satti, MD Associate Director Neurointerventional
Stroke Case Studies. Dr Stuti Joshi Neurology Advanced Trainee Telestroke fellow
 Stroke Case Studies Dr Stuti Joshi Neurology Advanced Trainee Telestroke fellow Case 1 64 year old female with dysphasia and right arm weakness 3 hours prior CT head: dense M1 sign. No established ischaemia
Stroke Case Studies Dr Stuti Joshi Neurology Advanced Trainee Telestroke fellow Case 1 64 year old female with dysphasia and right arm weakness 3 hours prior CT head: dense M1 sign. No established ischaemia
Diagnosis of Subarachnoid Hemorrhage (SAH) and Non- Aneurysmal Causes
 and Non- Aneurysmal Causes") Diagnosis of Subarachnoid Hemorrhage (SAH) and Non- Aneurysmal Causes By Sheila Smith, MD Swedish Medical Center 1 Disclosures I have no disclosures 2 Course Objectives Review significance and differential
Diagnosis of Subarachnoid Hemorrhage (SAH) and Non- Aneurysmal Causes By Sheila Smith, MD Swedish Medical Center 1 Disclosures I have no disclosures 2 Course Objectives Review significance and differential
Sinus Venous Thrombosis
 Sinus Venous Thrombosis Joseph J Gemmete, MD FACR, FSIR, FAHA Professor Departments of Radiology and Neurosurgery University of Michigan Hospitals Ann Arbor, MI Outline Introduction Medical Treatment Options
Sinus Venous Thrombosis Joseph J Gemmete, MD FACR, FSIR, FAHA Professor Departments of Radiology and Neurosurgery University of Michigan Hospitals Ann Arbor, MI Outline Introduction Medical Treatment Options
The management of ICH when to operate when not to?
 The management of ICH when to operate when not to? ICH is a Bad Disease High Incidence o Accounts for 10-15% of all strokes 1,2,5 o 80,000 cases in US; 2 million WW 2,5 o Incidence doubles for African-
The management of ICH when to operate when not to? ICH is a Bad Disease High Incidence o Accounts for 10-15% of all strokes 1,2,5 o 80,000 cases in US; 2 million WW 2,5 o Incidence doubles for African-
Perioperative Management Of Extra-Ventricular Drains (EVD)
") Perioperative Management Of Extra-Ventricular Drains (EVD) Dr. Vijay Tarnal MBBS, FRCA Clinical Assistant Professor Division of Neuroanesthesiology Division of Head & Neck Anesthesiology Michigan Medicine
Perioperative Management Of Extra-Ventricular Drains (EVD) Dr. Vijay Tarnal MBBS, FRCA Clinical Assistant Professor Division of Neuroanesthesiology Division of Head & Neck Anesthesiology Michigan Medicine
Welcome to our MISTIE III Safety Forum September 12, 2016
 Welcome to our MISTIE III Safety Forum September 12, 2016 Agenda: Update from our Surgical Centers: Where we stand surgically Mario Zuccarello, MD, University of Cincinnati Revisiting the Importance of
Welcome to our MISTIE III Safety Forum September 12, 2016 Agenda: Update from our Surgical Centers: Where we stand surgically Mario Zuccarello, MD, University of Cincinnati Revisiting the Importance of
Stroke in the ED. Dr. William Whiteley. Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian
 Stroke in the ED Dr. William Whiteley Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian 2016 RCP Guideline for Stroke RCP guidelines for acute ischaemic stroke
Stroke in the ED Dr. William Whiteley Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian 2016 RCP Guideline for Stroke RCP guidelines for acute ischaemic stroke
Acute stroke imaging
 Acute stroke imaging Aims Imaging modalities and differences Why image acute stroke Clinical correlation to imaging appearance What is stroke Classic definition: acute focal injury to the central nervous
Acute stroke imaging Aims Imaging modalities and differences Why image acute stroke Clinical correlation to imaging appearance What is stroke Classic definition: acute focal injury to the central nervous
Management of Spontaneous Intracerebral Hemorrhage (ICH)
") Management of Spontaneous Intracerebral Hemorrhage (ICH) Mindy Mason, MSN, RN, ACNP BC University of New Mexico Academic Medical Center Level I Trauma Center 24 bed Neuroscience ICU Albuquerque, NM 1 Objectives
Management of Spontaneous Intracerebral Hemorrhage (ICH) Mindy Mason, MSN, RN, ACNP BC University of New Mexico Academic Medical Center Level I Trauma Center 24 bed Neuroscience ICU Albuquerque, NM 1 Objectives
Endovascular Treatment of Cerebral Arteriovenous Malformations. Bs. Nguyễn Ngọc Pi Doanh- Bs Đặng Ngọc Dũng Khoa Ngoại Thần Kinh
 Endovascular Treatment of Cerebral Arteriovenous Malformations Bs. Nguyễn Ngọc Pi Doanh- Bs Đặng Ngọc Dũng Khoa Ngoại Thần Kinh Stroke Vascular Malformations of the Brain Epidemiology: - Incidence: 0.1%,
Endovascular Treatment of Cerebral Arteriovenous Malformations Bs. Nguyễn Ngọc Pi Doanh- Bs Đặng Ngọc Dũng Khoa Ngoại Thần Kinh Stroke Vascular Malformations of the Brain Epidemiology: - Incidence: 0.1%,
Antithrombotic therapy in patients with transient ischemic attack / stroke (acute phase <48h)
") Antithrombotic therapy in patients with transient ischemic attack / stroke (acute phase
Antithrombotic therapy in patients with transient ischemic attack / stroke (acute phase
Complicated issues in GI bleeding for internists? Nonthalee Pausawasdi, M.D. Faculty of Medicine Siriraj Hospital
 Complicated issues in GI bleeding for internists? Nonthalee Pausawasdi, M.D. Faculty of Medicine Siriraj Hospital Complicated issues in GI bleeding; Survey results from internists Optimal resuscitation
Complicated issues in GI bleeding for internists? Nonthalee Pausawasdi, M.D. Faculty of Medicine Siriraj Hospital Complicated issues in GI bleeding; Survey results from internists Optimal resuscitation
Update in Management of Acute Spontaneous Intracerebral Haemorrhage
 Update in Management of Acute Spontaneous Intracerebral Haemorrhage Aldy S. Rambe Neurology Department, School of Medicine EPIDEMIOLOGY Although ICH represents only about 9% of all stroke, it accounts
Update in Management of Acute Spontaneous Intracerebral Haemorrhage Aldy S. Rambe Neurology Department, School of Medicine EPIDEMIOLOGY Although ICH represents only about 9% of all stroke, it accounts
Incidence and Impact of Antithrombotic-related Intracerebral Hemorrhage
 Incidence and Impact of Antithrombotic-related Intracerebral Hemorrhage John J. Lewin III, PharmD, MBA, BCCCP, FASHP, FCCM, FNCS Division Director, Critical Care & Surgery Pharmacy Services, The Johns
Incidence and Impact of Antithrombotic-related Intracerebral Hemorrhage John J. Lewin III, PharmD, MBA, BCCCP, FASHP, FCCM, FNCS Division Director, Critical Care & Surgery Pharmacy Services, The Johns
Stroke secondary prevention. Gill Cluckie Stroke Nurse Consultant St. George s Hospital
 Stroke secondary prevention Gill Cluckie Stroke Nurse Consultant St. George s Hospital Stroke recurrence The risk of recurrent stroke is greatest after first stroke 2 3% of survivors of a first stroke
Stroke secondary prevention Gill Cluckie Stroke Nurse Consultant St. George s Hospital Stroke recurrence The risk of recurrent stroke is greatest after first stroke 2 3% of survivors of a first stroke
Acute Management of Anticoagulation-Associated Intracerebral Hemorrhage
 Acute Management of Anticoagulation-Associated Intracerebral Hemorrhage Authors Joji B. Kuramatsu, Stefan T. Gerner, Hagen B. Huttner, Stefan Schwab Affiliation University Hospital Erlangen Department
Acute Management of Anticoagulation-Associated Intracerebral Hemorrhage Authors Joji B. Kuramatsu, Stefan T. Gerner, Hagen B. Huttner, Stefan Schwab Affiliation University Hospital Erlangen Department
11/27/2017. Stroke Management in the Neurocritical Care Unit. Conflict of interest. Karel Fuentes MD Medical Director of Neurocritical Care
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Neurologic Emergency: Intracranial Hemorrhage Stabilization, and Effective Communication for the Non-Neurologist
 Neurologic Emergency: Intracranial Hemorrhage Stabilization, and Effective Communication for the Non-Neurologist Giuseppe Ciccotto MD, MPH Dept. of Neurosurgical Critical Care Ochsner Health System, New
Neurologic Emergency: Intracranial Hemorrhage Stabilization, and Effective Communication for the Non-Neurologist Giuseppe Ciccotto MD, MPH Dept. of Neurosurgical Critical Care Ochsner Health System, New
Stroke: The First Critical Hour. Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP
 Stroke: The First Critical Hour Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP Disclosures We have no actual or potential conflicts of interest in relation to this presentation. Objectives Discuss
Stroke: The First Critical Hour Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP Disclosures We have no actual or potential conflicts of interest in relation to this presentation. Objectives Discuss
Traumatic Brain Injury:
 Traumatic Brain Injury: Changes in Management Across the Spectrum of Age and Time Omaha 2018 Trauma Symposium June 15, 2018 Gail T. Tominaga, M.D., F.A.C.S. Scripps Memorial Hospital La Jolla Outline Background
Traumatic Brain Injury: Changes in Management Across the Spectrum of Age and Time Omaha 2018 Trauma Symposium June 15, 2018 Gail T. Tominaga, M.D., F.A.C.S. Scripps Memorial Hospital La Jolla Outline Background
INTRACEREBRAL HAEMORRHAGE:
 INTRACEREBRAL HAEMORRHAGE: WHAT IS THE CAUSE? Prof. Charlotte Cordonnier Head, Department of neurology & stroke centre Director, Lille haemorrhagic stroke research program Lille University Hospital France
INTRACEREBRAL HAEMORRHAGE: WHAT IS THE CAUSE? Prof. Charlotte Cordonnier Head, Department of neurology & stroke centre Director, Lille haemorrhagic stroke research program Lille University Hospital France
Supratentorial cerebral arteriovenous malformations : a clinical analysis
 Original article: Supratentorial cerebral arteriovenous malformations : a clinical analysis Dr. Rajneesh Gour 1, Dr. S. N. Ghosh 2, Dr. Sumit Deb 3 1Dept.Of Surgery,Chirayu Medical College & Research Centre,
Original article: Supratentorial cerebral arteriovenous malformations : a clinical analysis Dr. Rajneesh Gour 1, Dr. S. N. Ghosh 2, Dr. Sumit Deb 3 1Dept.Of Surgery,Chirayu Medical College & Research Centre,
5/2/2016. Outpatient Stroke Management Sheila Smith MD May 5, 2016
 Outpatient Stroke Management Sheila Smith MD May 5, 2016 1 Management of Outpatient Stroke Objectives Review blood pressure management post stroke Review antithrombotic therapy Review statin therapy Discuss
Outpatient Stroke Management Sheila Smith MD May 5, 2016 1 Management of Outpatient Stroke Objectives Review blood pressure management post stroke Review antithrombotic therapy Review statin therapy Discuss
Understanding Best Practices in Anticoagulation Therapy in Patients with Venous Thromboembolism. Rajat Deo, MD, MTR
 Understanding Best Practices in Anticoagulation Therapy in Patients with Venous Thromboembolism Rajat Deo, MD, MTR Director of Translational Research in Cardiac Arrhythmias Division of Cardiovascular Medicine
Understanding Best Practices in Anticoagulation Therapy in Patients with Venous Thromboembolism Rajat Deo, MD, MTR Director of Translational Research in Cardiac Arrhythmias Division of Cardiovascular Medicine
Advances in Acute stroke Management
 Advances in Acute stroke Management Sandra Ripper-Brown, DNP Neuroscience Nurse Practitioner St. Mary s Medical Center WPB, FL Palm Beach County Nurse Practitioner Council Annual Conference APRNs: Agents
Advances in Acute stroke Management Sandra Ripper-Brown, DNP Neuroscience Nurse Practitioner St. Mary s Medical Center WPB, FL Palm Beach County Nurse Practitioner Council Annual Conference APRNs: Agents
Stroke Update. Lacunar 19% Thromboembolic 6% SAH 13% ICH 13% Unknown 32% Hemorrhagic 26% Ischemic 71% Other 3% Cardioembolic 14%
 Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
The surgical strategy of hypertensive thalamus hemorrhage. Lu Ma, Chao You Dept. of Neurosurgery, West China Hospital
 The surgical strategy of hypertensive thalamus hemorrhage Lu Ma, Chao You Dept. of Neurosurgery, West China Hospital Preface Spontaneous Intracranial hemorrhage (SICH) Spontaneous thalamus hemorrhage---hypertensive
The surgical strategy of hypertensive thalamus hemorrhage Lu Ma, Chao You Dept. of Neurosurgery, West China Hospital Preface Spontaneous Intracranial hemorrhage (SICH) Spontaneous thalamus hemorrhage---hypertensive
Challenges in Anticoagulation Bridging and Emerging Therapies. Disclosures and Relationships. Objectives. Dr. Cumbler has no conflicts of interest
 Challenges in Anticoagulation Bridging and Emerging Therapies Ethan Cumbler MD FACP Associate Professor of Medicine Hospitalist Medicine Section University of Colorado Denver 2011 Disclosures and Relationships
Challenges in Anticoagulation Bridging and Emerging Therapies Ethan Cumbler MD FACP Associate Professor of Medicine Hospitalist Medicine Section University of Colorado Denver 2011 Disclosures and Relationships
Classification of Stroke. CNA Neuroscience Nursing Course: Cerebrovascular Disorders. Stroke in Canada
 CNA Neuroscience Nursing Course: Cerebrovascular Disorders Breeda O Farrell RN(EC), MScN, CNN(C) Nurse Practitioner Neurology University Hospital, London Health Science Centre London, ON Deb Bisnaire RN(EC),
CNA Neuroscience Nursing Course: Cerebrovascular Disorders Breeda O Farrell RN(EC), MScN, CNN(C) Nurse Practitioner Neurology University Hospital, London Health Science Centre London, ON Deb Bisnaire RN(EC),
GLYCEMIC CONTROL IN NEUROCRITICAL CARE PATIENTS
 GLYCEMIC CONTROL IN NEUROCRITICAL CARE PATIENTS David Zygun MD MSc FRCPC Professor and Director Division of Critical Care Medicine University of Alberta Zone Clinical Department Head Critical Care Medicine,
GLYCEMIC CONTROL IN NEUROCRITICAL CARE PATIENTS David Zygun MD MSc FRCPC Professor and Director Division of Critical Care Medicine University of Alberta Zone Clinical Department Head Critical Care Medicine,
M. Edip Gurol, MD, MSc Stroke Service/Neurology, Massachusetts General Hospital, Harvard Medical School
 High Risk of Thromboembolism and ICH: Problems with Medical Management M. Edip Gurol, MD, MSc Stroke Service/Neurology, Massachusetts General Hospital, Harvard Medical School Disclosures Funding from NIH
High Risk of Thromboembolism and ICH: Problems with Medical Management M. Edip Gurol, MD, MSc Stroke Service/Neurology, Massachusetts General Hospital, Harvard Medical School Disclosures Funding from NIH
Acute Medical Management. Bogachan Sahin, M.D., Ph.D. Department of Neurology
 Acute Medical Management Bogachan Sahin, M.D., Ph.D. Department of Neurology Outline Head-of-bed position Blood pressure management Antiplatelet therapy Anticoagulation Statin therapy Rehabilitation and
Acute Medical Management Bogachan Sahin, M.D., Ph.D. Department of Neurology Outline Head-of-bed position Blood pressure management Antiplatelet therapy Anticoagulation Statin therapy Rehabilitation and
Aneurysmal Subarachnoid Hemorrhage Presentation and Complications
 Aneurysmal Subarachnoid Hemorrhage Presentation and Complications Sherry H-Y. Chou MD MMSc FNCS Department of Critical Care Medicine, Neurology and Neurosurgery University of Pittsburgh School of Medicine
Aneurysmal Subarachnoid Hemorrhage Presentation and Complications Sherry H-Y. Chou MD MMSc FNCS Department of Critical Care Medicine, Neurology and Neurosurgery University of Pittsburgh School of Medicine
Content 1. Relevance 2. Principles 3. Manangement
 Intracranial haemorrhage and anticoagulation Department of Neurology,, Germany Department of Neurology, Heidelberg University Hospital, Germany Department of Clinical Medicine Copenhagen University, Denmark
Intracranial haemorrhage and anticoagulation Department of Neurology,, Germany Department of Neurology, Heidelberg University Hospital, Germany Department of Clinical Medicine Copenhagen University, Denmark
11/23/2015. Disclosures. Stroke Management in the Neurocritical Care Unit. Karel Fuentes MD Medical Director of Neurocritical Care.
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Identifying Cerebrovascular Disorders. Wengui Yu, MD, PhD Department of Neurology, University of California, Irvine
 Identifying Cerebrovascular Disorders Wengui Yu, MD, PhD Department of Neurology, University of California, Irvine Objectives Review different types of cerebrovascular disorders. Briefly discuss etiology,
Identifying Cerebrovascular Disorders Wengui Yu, MD, PhD Department of Neurology, University of California, Irvine Objectives Review different types of cerebrovascular disorders. Briefly discuss etiology,
Thrombolysis for acute ischaemic stroke Rapid Assessment Protocol NORTHERN IRELAND Regional Protocol (Version 002 July 08)
") Thrombolysis for acute ischaemic stroke Rapid Assessment Protocol NORTHERN IRELAND Regional Protocol (Version 002 July 08) Patient Details Time of onset? Capillary Blood glucose 2.8-22.2 mmol/l? Blood
Thrombolysis for acute ischaemic stroke Rapid Assessment Protocol NORTHERN IRELAND Regional Protocol (Version 002 July 08) Patient Details Time of onset? Capillary Blood glucose 2.8-22.2 mmol/l? Blood
CHAPTER 2 VENOUS THROMBOEMBOLISM
 CHAPTER 2 VENOUS THROMBOEMBOLISM Objectives Venous Thromboembolism (VTE) Prevalence Patho-physiology Risk Factors Diagnosis Pulmonary Embolism (PE) Management of DVT/PE Prevention VTE Patho-physiology
CHAPTER 2 VENOUS THROMBOEMBOLISM Objectives Venous Thromboembolism (VTE) Prevalence Patho-physiology Risk Factors Diagnosis Pulmonary Embolism (PE) Management of DVT/PE Prevention VTE Patho-physiology
Canadian Best Practice Recommendations for Stroke Care 3.7 Acute Intracerebral Hemorrhage
 Last Updated: May 21st, 2013 Canadian Best Practice Recommendations for Stroke Care 3.7 Acute Intracerebral Hemorrhage Canadian Best Practice Recommendations for Stroke Care 2012-2013 Update Contents Search
Last Updated: May 21st, 2013 Canadian Best Practice Recommendations for Stroke Care 3.7 Acute Intracerebral Hemorrhage Canadian Best Practice Recommendations for Stroke Care 2012-2013 Update Contents Search
INDICATIONS FOR THROMBO-PROPHYLAXIS AND WHEN TO STOP ANTICOAGULATION BEFORE ELECTIVE SURGERY
 INDICATIONS FOR THROMBO-PROPHYLAXIS AND WHEN TO STOP ANTICOAGULATION BEFORE ELECTIVE SURGERY N.E. Pearce INTRODUCTION Preventable death Cause of morbidity and mortality Risk factors Pulmonary embolism
INDICATIONS FOR THROMBO-PROPHYLAXIS AND WHEN TO STOP ANTICOAGULATION BEFORE ELECTIVE SURGERY N.E. Pearce INTRODUCTION Preventable death Cause of morbidity and mortality Risk factors Pulmonary embolism