Cardio Renal Disease. Dr. Rajasekara Chakravarthi Head, Dept of Nephrology CARE Hospitals Hyderabad
|
|
|
- Wesley Holland
- 5 years ago
- Views:
Transcription
1 Cardio Renal Disease Dr. Rajasekara Chakravarthi Head, Dept of Nephrology CARE Hospitals Hyderabad
2 PREVALENCE OF CVD IS HIGH CAD LVH CHF (CLINICAL) (ECHO) (CLINICAL) GENERAL POPULATION 5-12% 20% 5% CKD NA 25-50% NA HEMODIALYSIS 40% 75% 40% PERITONIAL DIALYSIS 40% 75% 40% RENAL TRANSPLANT 15% 50% NA SARNAK AND LEVEY AJKD 2000, 35:
3 Def: _ Cardio renal syndrome - a relatively normal kidney is dysfunctional because of a diseased heart, with the assumption that in the presence of a healthy heart same kidney performs normally.
4 DEF: _ Cardiorenal syndrome, general definition: a pathophysiological disorder of the heart and kidneys in which acute or chronic dysfunction in one organ may induce acute or chronic dysfunction in the other organ
5 CRS type 1 (acute CRS). _ Type 1 CRS is characterized by a rapid worsening of cardiac function, leading to acute kidney injury (AKI)
6 _ Acute heart failure (HF) may be divided into 4 subtypes: _ hypertensive pulmonary edema with preserved left ventricular (LV) systolic function _ acutely decompensated chronic HF _ cardiogenic shock, and _ predominant right ventricular failure

7
8 Type II: chronic cardiorenal syndrome. _ Chronic abnormalities in cardiac function (e.g. chronic congestive heart failure) causing progressive and potentially permanent chronic kidney disease

9
10 Type III: acute renocardiac syndrome _. Abrupt worsening of renal function (e.g. acute kidney ischaemia or glomerulonephritis) causing acute cardiac disorder (e.g. heart failure, arrhythmia, ischaemia)
11
12 Type IV: chronic renocardiac syndrome _. Chronic kidney disease (e.g. chronic glomerular or interstitial disease) contributing to decreased cardiac function, cardiac hypertrophy and/or increased risk of adverse cardiovascular events


13
14 Type V: Secondary cardiorenal syndrome _ Systemic condition (e.g. diabetes mellitus, sepsis) causing both cardiac and renal dysfunction

15
16 Current Approaches to managing Cardiorenal Dysfunction Neurohormonal antagonists Other vasoactive therapies - Positive ionotropes - Natriuretic peptides Agents that target the kidney - Vasopressin - Adenosine antagonists Renal replacement therapy (Ultrafiltration) Mechanical circulatory support
17 Current Options May Have Undesirable Clinical Impacts _ Favorable aspects of diuretic therapy Increases urine output; reduces total body volume in majority of patients 4 _ Adverse aspects of diuretic therapy Direct activation of renin-angiotensin-aldosterone system 3,10 Enhanced myocardial aldosterone uptake 12 Loss of K, Mg, Ca, secondary myocyte Ca loading 12 Indirect reduction of cardiac output 10,11 Increased total systemic vascular resistance 11 Reduced natriuresis 8 and GFR 7,9 Associated with increased morbidity and mortality 2,5,6
18 Furosemide Monotherapy Causes Significant Decline in Renal Function (GFR) Change in GFR after IV furosemide 80 mg in CHF GFR (% Change) Placebo IV furosemide Urine Output (ml) 0 8 h Gottlieb et al. Circulation. 2002;105:1348.
19 Relief for Acutely Fluid Overloaded Patients With Decompensated Congestive Heart Failure The RAPID-CHF Trial Bart et al. J Am Coll Cardiol. 2005;46:
20 Early Ultrafiltration in Patients With Decompensated HF and Observed Resistance to Intervention With Diuretic Agents The EUPHORIA Trial
21 Ultrafiltration versus IV Diuretics for Patients Hospitalized ized for f Acute Decompensated Congestive HF: A Prospective Randomized Clinical Trial UNLOAD Trial Costanzo MR et al. J Am Coll Cardiol. 2007;49:
22 Conclusions Early ultrafiltration produces greater weight loss than IV diuretics, without changes in renal function An early ultrafiltration strategy reduces 90-day Percentage of patients requiring rehospitalization for HF Number of HF rehospitalizations Days of rehospitalization for HF Emergency department and unscheduled office visits Costanzo MR et al. J Am Coll Cardiol. 2007;49:
23 WHY ULTRAFILTRATION? _ PATIENT effective control of symptoms - early control of symptoms - short hospital stay - no requirement for ICU - diuretic side effects HOSPITAL - faster turnaround time - less requirement ICU bed - day heart failure clinic (like CRF)
24 Pathophysiology IL 1 IL 6 ANP MDF (Myocardial depressant factors) Removed by UF
25 Renal function and survival in CHF _ Most powerful predictor mortality in CHF _ 1906 pts Crcl.. < 44 ml/min (CG equation) mortality risk 2.85 (P= <0.001) _ RF stronger predictor factor than Na, K, Mg, EF or NYHA Class _ N terminal ANP - Hillage et al Circulation 102: ; 2000
26 Evolution of CRRT SLOW IHD 1993 CVVHDF 1988 IHD 1960 Cytokine control SCUF CAVH CAVHD CAVHDF SCUF 1977 CAVH 1978 CVVHD 1986 CAVH D 1984 Uraemic control All of the above CVVH 1985 CAVHDF 1984 CHF Control SCUF CAVH CVVH Paganini et al Seminars in dialysis vol9, No.2 (Mar-Apr)1996;
27 AIM OF THE STUDY _ Role of CAPD in refractory congestive heart failure at our centre during the period _ Prospective study continued till date
28 Inclusion Criteria _ Refractory heart failure _ Severe systolic dysfunction (EF<35%) _ No possibility of surgical treatment _ No response to the best medical therapy available (fluid decongestive therapy) _ Adequate socio financial support
29 MATERIALS & METHODS _ 21 patients with severe congestive heart failure refractory to optimal pharmacological therapy _ All patients had NYHA class IV with varying stages of CKD III-IV _ CAPD prescription is based on the amount of UF needs to be achieved _ The total follow up ranged between 6 months to 2 years _ Statistical analysis : paired student t test
30 Clinical and technical Data Pt. Gend er Age Diagnosis PD Prescription Ultra-filtration PD Follow- up (months) Peritonitis episodes 1 M 63 Ischaemic CMP One Icodextrin nocturnal exchange F 54 RHD+MVR One Icodextrin nocturnal exchange + 1.5% one exchange F 60 Ischaemic CMP One Icodextrin nocturnal exchange + 1.5% one exchange F 57 Ischaemic CMP One Icodextrin nocturnal exchange + 2.5% one exchange M 63 Ischaemic CMP One Icodextrin nocturnal exchange M 58 Ischaemic CMP One 2.5% exchange per day M 57 Ischemic CMP Three 2.5% exchange per day M 59 Ischemic CMP One 2.5% exchange per day M 70 Ischemic CMP Two 2.5%exchnage per day M 63 Ischemic CMP Three 2.5% exchange
31 RESULTS _ Of the 21 patients studied 17 were males and 4 were females _ The mean age was yrs _ There was a significant improvement in NYHA class IV to II in 4 patients and NYHA class IV to III in 1 patient NYHA class IV to I in 1 patient (p=0.0006) _ We have observed significant improvement in quality of life, reduction in morbidity and decreased hospitalization rates (p=0.0010) _ Only one patient had an episode of peritonitis during the follow up
32 Table summarizing our experience at Care Hospitals Pt. Gende r Age Diagnosis Ejection Fraction % Before After Renal egfr CKDstages Hospitalisation days (before) Hospitalisatio n days (after) 1 M 63 Ischaemic CMP F 54 RHD+MVR F 60 Ischaemic CMP F 57 Ischaemic CMP M 63 Ischaemic CMP M 58 Ischaemic CMP M 57 Dilated cardio myopathy M 59 RHD M 70 Dilated cadio myopathy M 63 Dilated cadio myopathy
33 Change in the functional class NYHA Grade NYHA(before) NYHA(after) p= Patients
34 Number of Hospitalisation Days Number of Days Hospitalisation days(before) Hospitalisation days(after) p= Patients
35 Improvement in LV Ejection fraction Ejection Fraction % Ejectiuon fraction(before) Ejection fraction(after) Patients
36 CONCLUSION _ Independent of the renal functions peritoneal dialysis appears to be a promising therapeutic option for patients with refractory CHF _ Peritoneal Dialysis offers significant improvement in quality of life, reduction in morbidity and decreased hospitalization rates in patients with refractory CHF _ One exchange (Dextrose/ Icodextrin) is sufficient enough for achieving fluid balance
37 Definition of CIN _ CIN is most commonly defined as: an acute impairment of renal function following the use of CM with an increase in serum creatinine (SCr) of 44.2 µmol/l (0.5 mg/dl), or as an increase of 25% from baseline within 72 h after Intravascular CM administration In the absence of an alternative etiology ESUR, European Society of Urogenital Radiology Thomsen HS. Curr Opin Urol. 2007;17:70-76.
38 CIN adversely affects survival for many years after the episode Brown JR et al. Circulation 2007; 116: Abs 1689.
39 Are We Failing to Identify Patients With Renal Impairment Because of How We Screen for Them? Age, y Normal SCr Patients with Abnormal egfr Yes 1.2% Yes 12.6% 70 Yes 47.3% Duncan L et al. Nephrol Dial Transplant 2001; 16:
40
41 Estimating Kidney Function Cockcroft Gault: estimates creatinine clearance (ml/min) (140-age) x weight (kg) 72 x SCr (mg/dl dl) x 0.85 (if female) 4-variable MDRD: estimates GFR (ml/min/1.73 m 2 ) x SCr x age x (0.742 if female) x (1.21 if black) 6-variable MDRD: estimates GFR (ml/min/1.73 m 2 ) 170 x (SCr x 0.011) x (age) x (SUN x 2.801) x (SAlb x 0.1) x (if African-American) x (if female) Coritsidis GN. Available at: Lamb EJ et al. J Am Geriatr Soc 2003;51: ;Grubb A et al. Clin Chem 2005;51 (8):

42 Stages of CKD Adapted from the National Kidney Foundation K/DOQI Clinical Practice Guidelines for Chronic Kidney Disease; Evaluation, Classification, and Stratification.
43 The CIN Risk Index CIN Risk Factors and Scores Risk Factors Hypotension Presence of an intra-aortic balloon pump Congestive heart failure Age >75 years Anemia Diabetes Chronic kidney disease Volume of contrast agent used Integer Score (SCr( >1.5 mg/dl dl) 2 (GFR 40 60) 4 (GFR 20 40) 6 (GFR <20) 1 per each 100 cc 3 Reference: Mehran R et al. J Am Coll Cardiol. 2004;44:
44
45 Algorithm for Management of Patients Receiving Iodinated CM Calculate egfr Assess CIN risk egfr <30 ml/min egfr ml/min Discontinue NSAIDs, other nephrotoxic drugs, metformin egfr 60 ml/min Discontinue metformin Hospital admission Nephrology consultation Dialysis planning* Other strategies as for egfr ml Serial SCr and electrolytes Intravenous volume expansion Consider choice of contrast medium Limit contrast volume (<100 ml) Consider pharmacological treatment SCr before discharge or within h Good clinical practice * Plans should be made in case CIN occurs and dialysis is required IV isotonic crystalloid ml/kg/h for 3 12 h before and 6 24 h after the procedure Consider potentially beneficial agents (theophylline, statins, ascorbic acid, PGE 1 ); 45 none Adapted from McCullough PA, et al. Am J Cardiol. 2006;98[Suppl]:2K-4K. approved for this indication
46 Fluids What? _ 0.9% saline significantly reduced contrast nephropathy compared to 0.45% saline (0.7% vs. 2% ; P =0.04) USE ISOTONIC CRYSTALLOIDS Mueller C et al: Arch Intern Med 2002; 162: _ Hydration with isotonic sodium bicarbonate decreased the incidence of contrast nephropathy compared to 0.9% saline (1.7% vs. 13.6%; P = 0.02) Merten GJ et al: JAMA 2004; 291:
47 _ Check e GFR _ Stop ACEI /ARB/ ARB s /DRI s _ Stop Metformin _ Stop diuretics _ No NSAID S _ IV hydration NS 1 ml /kg/hr/12-24 hrs (pre & post) If HF _ ml/kg/hr/12-24 hrs (pre & post) - Maintain I/O check - IV Na HCo 3? - NAC mg 3 doses (Vol( of contrast, type of contrast) - Check S. Creatinine 48 hrs
48 Society Society Recommendations: Type of CM for High-risk Patients Isosmol ar Low- osmolar ACC/AHA/SCAI 2007 (PCI) ACC/AHA 2007 (UA/NSTEMI) Hungarian Society of Nephrology 2007 National Kidney Foundation (K/DOQI) 2005 Norwegian Society of Nephrology 2004 German Cardiac Society 2004 ESUR 2005 French Radiologic Society 2004


49

50
51 As medicine is practised in the 1990s the pt with heart disease and renal disease are frequently managed by physicians who are interested in only one of the two organ systems. In circumstances when the pt is visited by both, the physicians frequently take opposite points of view and make therapeutic recommendations that are principally designed to preserve a single organ system. Packer M Cardio Renal Disease (II Ed) 1992 PP III - VI
52
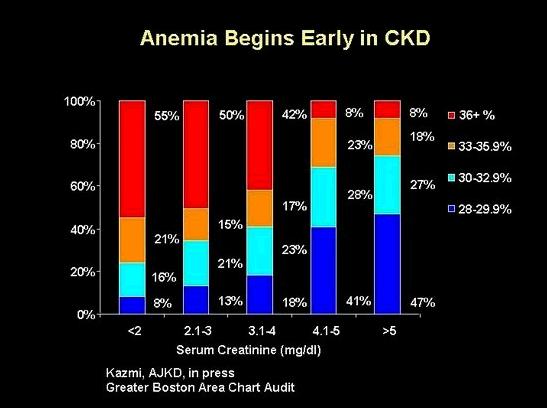
53 ANEMIA MANAGEMENT IN CKD Critical links : CKD CVD Anemia Adverse consequences of anemia Anemia and clinical outcomes 1) observational studies 2) Interventional trials Challenges of targeting higher hb Trends in anemia management Epoetin vs. Darbepoetin
54 Heart Failure after MI- Benefit beyond Hemoglobolin from Erythropoetin _ Erythropoetin Induces Neovascularization and Improves Cardiac Function in Rats with Heart Failure after Myocardial Infarction. - Van der Meer et al. J Am Coll Cardiol 46: , 2005 _ Editorial Eberhard Ritz J Am Soc Nephrol 5: 2-7, 2006 _ High dose Epo - A Limitation
55 Volume overload Primary stimulus Pressure overload Increased diastolic pressure - Increased diastolic stress Increased systolic pressure + - Increased systolic stress Series addition of new sarcomeres Parallel addition of new myofibrils Chamber enlargement Wall thickening Eccentric hypertrophy Concentric hypertrophy
56 Initial insult Hypoxia Oxidative stress GLOMERULAR INJURY proteinuria INTERSTITIAL FIBROSIS Glomerular hypertension/ hypertrophy GLOMERULO- SCLEROSIS Hypoxia Oxidative stress Tubular dysfunction REDUCED NEPHRON NUMBER Destruction of capillaries Hypoxia Oxidative stress Epoetin? Tubular destruction
57 CKD-MBD Ca X P > 55 PTH Phosphate binders Calcinimetics Vit D analogues Ca containing Non Ca containing Sevelamer Lanthanum
58
Contrast Induced Nephropathy
 Contrast Induced Nephropathy O CIAKI refers to an abrupt deterioration in renal function associated with the administration of iodinated contrast media O CIAKI is characterized by an acute (within 48 hours)
Contrast Induced Nephropathy O CIAKI refers to an abrupt deterioration in renal function associated with the administration of iodinated contrast media O CIAKI is characterized by an acute (within 48 hours)
Minimizing the Renal Toxicity of Iodinated Contrast
 Minimizing the Renal Toxicity of Iodinated Contrast Peter A. McCullough, MD, MPH, FACC, FACP, FAHA, FCCP Chief Academic and Scientific Officer St. John Providence Health System Detroit, MI USA Outline
Minimizing the Renal Toxicity of Iodinated Contrast Peter A. McCullough, MD, MPH, FACC, FACP, FAHA, FCCP Chief Academic and Scientific Officer St. John Providence Health System Detroit, MI USA Outline
Pivotal Role of Renal Function in Acute Heart failure
 Pivotal Role of Renal Function in Acute Heart failure Doron Aronson MD, FESC Department of Cardiology RAMBAM Health Care Campus Haifa, Israel Classification and definitions of cardiorenal syndromes CRS
Pivotal Role of Renal Function in Acute Heart failure Doron Aronson MD, FESC Department of Cardiology RAMBAM Health Care Campus Haifa, Israel Classification and definitions of cardiorenal syndromes CRS
The Cardiorenal Syndrome in Heart Failure
 The Cardiorenal Syndrome in Heart Failure Van N Selby, MD Assistant Professor of Medicine Advanced Heart Failure Program, UCSF October 9, 2015 Disclosures None 1 Cardiorenal Syndrome (CRS) A pathophysiologic
The Cardiorenal Syndrome in Heart Failure Van N Selby, MD Assistant Professor of Medicine Advanced Heart Failure Program, UCSF October 9, 2015 Disclosures None 1 Cardiorenal Syndrome (CRS) A pathophysiologic
Heart Failure and Renal Failure. Gerasimos Filippatos, MD, FESC, FHFA President HFA
 Heart Failure and Renal Failure Gerasimos Filippatos, MD, FESC, FHFA President HFA Definition Epidemiology Pathophysiology Management (?) Recommendations for NHLBI in cardiorenal interactions related to
Heart Failure and Renal Failure Gerasimos Filippatos, MD, FESC, FHFA President HFA Definition Epidemiology Pathophysiology Management (?) Recommendations for NHLBI in cardiorenal interactions related to
Heart Failure and Renal Disease Cardiorenal Syndrome
 Advanced Heart Failure: Clinical Challenges Heart Failure and Renal Disease Cardiorenal Syndrome 17 th Apr 2015 Ju-Hee Lee, M.D Cardiovascular Center, Chungbuk National University Hospital Chungbuk National
Advanced Heart Failure: Clinical Challenges Heart Failure and Renal Disease Cardiorenal Syndrome 17 th Apr 2015 Ju-Hee Lee, M.D Cardiovascular Center, Chungbuk National University Hospital Chungbuk National
Contrast-Induced Nephropathy: Evidenced Based Prevention
 Contrast-Induced Nephropathy: Evidenced Based Prevention Michael J Cowley, MD, FSCAI Nothing to disclose Contrast-Induced Nephropathy (CIN) Definitions New onset or worsening of renal function after contrast
Contrast-Induced Nephropathy: Evidenced Based Prevention Michael J Cowley, MD, FSCAI Nothing to disclose Contrast-Induced Nephropathy (CIN) Definitions New onset or worsening of renal function after contrast
SAFETY IN THE CATH LAB How to Minimise Contrast Toxicity
 SAFETY IN THE CATH LAB How to Minimise Contrast Toxicity Dr. Vijay Kunadian MBBS, MD, MRCP Senior Lecturer and Consultant Interventional Cardiologist Institute of Cellular Medicine, Faculty of Medical
SAFETY IN THE CATH LAB How to Minimise Contrast Toxicity Dr. Vijay Kunadian MBBS, MD, MRCP Senior Lecturer and Consultant Interventional Cardiologist Institute of Cellular Medicine, Faculty of Medical
Cardiovascular Disease in CKD. Parham Eftekhari, D.O., M.Sc. Assistant Clinical Professor Medicine NSUCOM / Broward General Medical Center
 Cardiovascular Disease in CKD Parham Eftekhari, D.O., M.Sc. Assistant Clinical Professor Medicine NSUCOM / Broward General Medical Center Objectives Describe prevalence for cardiovascular disease in CKD
Cardiovascular Disease in CKD Parham Eftekhari, D.O., M.Sc. Assistant Clinical Professor Medicine NSUCOM / Broward General Medical Center Objectives Describe prevalence for cardiovascular disease in CKD
Cardiorenal Syndrome
 Cardiorenal Syndrome Peenida Skulratanasak, M.D. Division of Nephrology, Department of Medicine, Faculty of Medicine, Siriraj Hospital, Mahidol University Definition of Cardiorenal syndrome (CRS) Structural
Cardiorenal Syndrome Peenida Skulratanasak, M.D. Division of Nephrology, Department of Medicine, Faculty of Medicine, Siriraj Hospital, Mahidol University Definition of Cardiorenal syndrome (CRS) Structural
Objectives 6/14/2016. Cardiorenal Syndrome: Critical Link Between Heart and Kidney
 Cardiorenal Syndrome: Critical Link Between Heart and Kidney Chris M. Bell, ACNP Cardiology Associates of North Mississippi Objectives Review the 5 Subtypes of the Cardiorenal Syndrome (CRS) Discuss the
Cardiorenal Syndrome: Critical Link Between Heart and Kidney Chris M. Bell, ACNP Cardiology Associates of North Mississippi Objectives Review the 5 Subtypes of the Cardiorenal Syndrome (CRS) Discuss the
Dr.Nahid Osman Ahmed 1
 1 ILOS By the end of the lecture you should be able to Identify : Functions of the kidney and nephrons Signs and symptoms of AKI Risk factors to AKI Treatment alternatives 2 Acute kidney injury (AKI),
1 ILOS By the end of the lecture you should be able to Identify : Functions of the kidney and nephrons Signs and symptoms of AKI Risk factors to AKI Treatment alternatives 2 Acute kidney injury (AKI),
The Triple Threat. Cardiac Care in the NT Annual Workshop 2017 is proudly supported by:
 The Triple Threat DR KELUM PRIYADARSHANA FRACP CONSULTANT NEPHROLOGIST ROYAL DARWIN HOSPITAL Cardiac Care in the NT Annual Workshop 2017 is proudly supported by: Pathogenesis Diabetes CKD CVD Diabetic
The Triple Threat DR KELUM PRIYADARSHANA FRACP CONSULTANT NEPHROLOGIST ROYAL DARWIN HOSPITAL Cardiac Care in the NT Annual Workshop 2017 is proudly supported by: Pathogenesis Diabetes CKD CVD Diabetic
Overcoming the Cardiorenal Syndrome
 Overcoming the Cardiorenal Syndrome October 29, 2016 Randall C Starling MD MPH FACC FESC FHFSA FHFA Professor of Medicine Heart & Vascular Institute Cleveland Clinic Lerner College of Medicine Cleveland
Overcoming the Cardiorenal Syndrome October 29, 2016 Randall C Starling MD MPH FACC FESC FHFSA FHFA Professor of Medicine Heart & Vascular Institute Cleveland Clinic Lerner College of Medicine Cleveland
 www.usrds.org www.usrds.org 1 1,749 + (2,032) 1,563 to
www.usrds.org www.usrds.org 1 1,749 + (2,032) 1,563 to Doreen P. Foley MS RN ANP-C Doctor of Nursing Practice Program Chamberlain College of Nursing
 Doreen P. Foley MS RN ANP-C Doctor of Nursing Practice Program Chamberlain College of Nursing This program has been developed solely for the purposes of describing the level of nurse practitioner (NP)
Doreen P. Foley MS RN ANP-C Doctor of Nursing Practice Program Chamberlain College of Nursing This program has been developed solely for the purposes of describing the level of nurse practitioner (NP)
CATH LAB SYMPOSIUM 2010
 CATH LAB SYMPOSIUM 2010 Low resistance system High Pressure in Capillaries to filter plasma RBF: 1.2-1.3 L/min (25% of C.O.) Low AV difference ( shunt ) Kidney: 14 ml O2/L blood Brain: 62 ml O2/L blood
CATH LAB SYMPOSIUM 2010 Low resistance system High Pressure in Capillaries to filter plasma RBF: 1.2-1.3 L/min (25% of C.O.) Low AV difference ( shunt ) Kidney: 14 ml O2/L blood Brain: 62 ml O2/L blood
Medical Management of Acute Heart Failure
 Critical Care Medicine and Trauma Medical Management of Acute Heart Failure Mary O. Gray, MD, FAHA Associate Professor of Medicine University of California, San Francisco Staff Cardiologist and Training
Critical Care Medicine and Trauma Medical Management of Acute Heart Failure Mary O. Gray, MD, FAHA Associate Professor of Medicine University of California, San Francisco Staff Cardiologist and Training
Biomarkers for optimal management of heart failure. Cardiorenal syndrome. Veli-Pekka Harjola Helsinki University Central Hospital Helsinki, Finland
 Biomarkers for optimal management of heart failure Cardiorenal syndrome Veli-Pekka Harjola Helsinki University Central Hospital Helsinki, Finland Presenter Disclosure Information V-P Harjola The following
Biomarkers for optimal management of heart failure Cardiorenal syndrome Veli-Pekka Harjola Helsinki University Central Hospital Helsinki, Finland Presenter Disclosure Information V-P Harjola The following
Heart Failure and Cardio-Renal Syndrome 1: Pathophysiology. Biomarkers of Renal Injury and Dysfunction
 CRRT 2011 San Diego, CA 22-25 February 2011 Heart Failure and Cardio-Renal Syndrome 1: Pathophysiology Biomarkers of Renal Injury and Dysfunction Dinna Cruz, M.D., M.P.H. Department of Nephrology San Bortolo
CRRT 2011 San Diego, CA 22-25 February 2011 Heart Failure and Cardio-Renal Syndrome 1: Pathophysiology Biomarkers of Renal Injury and Dysfunction Dinna Cruz, M.D., M.P.H. Department of Nephrology San Bortolo
Cardiorenal Syndrome Prof. Dr. Bülent ALTUN Hacettepe University Faculty of Medicine Department of Internal Medicine Division of Nephrology
 Cardiorenal Syndrome Prof. Dr. Bülent ALTUN Hacettepe University Faculty of Medicine Department of Internal Medicine Division of Nephrology Heart and Kidney The kidney yin dominates water, The heart yang
Cardiorenal Syndrome Prof. Dr. Bülent ALTUN Hacettepe University Faculty of Medicine Department of Internal Medicine Division of Nephrology Heart and Kidney The kidney yin dominates water, The heart yang
Cardiorenal and Renocardiac Syndrome
 And Renocardiac Syndrome A Vicious Cycle Cardiorenal and Renocardiac Syndrome Type 1 (acute) Acute HF results in acute kidney injury Type 2 Chronic cardiac dysfunction (eg, chronic HF) causes progressive
And Renocardiac Syndrome A Vicious Cycle Cardiorenal and Renocardiac Syndrome Type 1 (acute) Acute HF results in acute kidney injury Type 2 Chronic cardiac dysfunction (eg, chronic HF) causes progressive
Novel Approaches for Recognition and Management of Life Threatening Complications of AKI and CKD: Focus on Acute Cardiorenal Syndromes
 Novel Approaches for Recognition and Management of Life Threatening Complications of AKI and CKD: Focus on Acute Cardiorenal Syndromes Peter A. McCullough, MD, MPH Baylor University Medical Center, Dallas
Novel Approaches for Recognition and Management of Life Threatening Complications of AKI and CKD: Focus on Acute Cardiorenal Syndromes Peter A. McCullough, MD, MPH Baylor University Medical Center, Dallas
THE KIDNEY IN HYPOTENSIVE STATES. Benita S. Padilla, M.D.
 THE KIDNEY IN HYPOTENSIVE STATES Benita S. Padilla, M.D. Objectives To discuss what happens when the kidney encounters low perfusion To discuss new developments and clinical application points in two scenarios
THE KIDNEY IN HYPOTENSIVE STATES Benita S. Padilla, M.D. Objectives To discuss what happens when the kidney encounters low perfusion To discuss new developments and clinical application points in two scenarios
Rationale for renal replacement therapy in ICU: indications, approaches and outcomes. Richard Beale
 Rationale for renal replacement therapy in ICU: indications, approaches and outcomes Richard Beale RIFLE classification (ADQI group) 2004 Outcome AKIN classification Definition: Abrupt (within 48 hrs)
Rationale for renal replacement therapy in ICU: indications, approaches and outcomes Richard Beale RIFLE classification (ADQI group) 2004 Outcome AKIN classification Definition: Abrupt (within 48 hrs)
ECMO & Renal Failure Epidemeology Renal failure & effect on out come
 ECMO Induced Renal Issues Transient renal dysfunction Improvement in renal function ECMO & Renal Failure Epidemeology Renal failure & effect on out come With or Without RRT Renal replacement Therapy Utilizes
ECMO Induced Renal Issues Transient renal dysfunction Improvement in renal function ECMO & Renal Failure Epidemeology Renal failure & effect on out come With or Without RRT Renal replacement Therapy Utilizes
Medical Management of Acutely Decompensated Heart Failure. William T. Abraham, MD Director, Division of Cardiovascular Medicine
 Medical Management of Acutely Decompensated Heart Failure William T. Abraham, MD Director, Division of Cardiovascular Medicine Orlando, Florida October 7-9, 2011 Goals of Acute Heart Failure Therapy Alleviate
Medical Management of Acutely Decompensated Heart Failure William T. Abraham, MD Director, Division of Cardiovascular Medicine Orlando, Florida October 7-9, 2011 Goals of Acute Heart Failure Therapy Alleviate
Recognizing and Treating Patients with the Cardio-Renal Syndrome
 Recognizing and Treating Patients with the Cardio-Renal Syndrome Joachim H. Ix, MD, MAS, FASN Professor of Medicine Chief; Division of Nephrology-Hypertension University of California San Diego 1 Conflicts
Recognizing and Treating Patients with the Cardio-Renal Syndrome Joachim H. Ix, MD, MAS, FASN Professor of Medicine Chief; Division of Nephrology-Hypertension University of California San Diego 1 Conflicts
Cardiorenal syndrome. Sofie Gevaert. Ghent University Hospital, Belgium
 Cardiorenal syndrome Sofie Gevaert Ghent University Hospital, Belgium Disclosures Consultancy Astra Zeneca Boegringer MSD Novartis 68 y old man, ADHF ICMP, ejection fraction 35 %: progressive dyspnea,
Cardiorenal syndrome Sofie Gevaert Ghent University Hospital, Belgium Disclosures Consultancy Astra Zeneca Boegringer MSD Novartis 68 y old man, ADHF ICMP, ejection fraction 35 %: progressive dyspnea,
Left ventricular hypertrophy: why does it happen?
 Nephrol Dial Transplant (2003) 18 [Suppl 8]: viii2 viii6 DOI: 10.1093/ndt/gfg1083 Left ventricular hypertrophy: why does it happen? Gerard M. London Department of Nephrology and Dialysis, Manhes Hospital,
Nephrol Dial Transplant (2003) 18 [Suppl 8]: viii2 viii6 DOI: 10.1093/ndt/gfg1083 Left ventricular hypertrophy: why does it happen? Gerard M. London Department of Nephrology and Dialysis, Manhes Hospital,
The pathophysiology of contrast medium induced nephropathy
 The pathophysiology of contrast medium induced nephropathy Peter Aspelin Professor of Radiology Karolinska Institutet 5th Nordic Course in Emergency Radiology, Oslo 2015 Background Contrast medium-induced
The pathophysiology of contrast medium induced nephropathy Peter Aspelin Professor of Radiology Karolinska Institutet 5th Nordic Course in Emergency Radiology, Oslo 2015 Background Contrast medium-induced
Antialdosterone treatment in heart failure
 Update on the Treatment of Chronic Heart Failure 2012 Antialdosterone treatment in heart failure 전남의대윤현주 Chronic Heart Failure Prognosis of Heart failure Cecil, Text book of Internal Medicine, 22 th edition
Update on the Treatment of Chronic Heart Failure 2012 Antialdosterone treatment in heart failure 전남의대윤현주 Chronic Heart Failure Prognosis of Heart failure Cecil, Text book of Internal Medicine, 22 th edition
Definition of Congestive Heart Failure
 Heart Failure Definition of Congestive Heart Failure A clinical syndrome of signs & symptoms resulting from the heart s inability to supply adequate tissue perfusion. CHF Epidemiology Affects 4.7 million
Heart Failure Definition of Congestive Heart Failure A clinical syndrome of signs & symptoms resulting from the heart s inability to supply adequate tissue perfusion. CHF Epidemiology Affects 4.7 million
Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease
 / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease") Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease Investigator Meeting 12 th September 2017 - Sheffield Prof Sunil Bhandari Consultant
Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease Investigator Meeting 12 th September 2017 - Sheffield Prof Sunil Bhandari Consultant
WEEK. MPharm Programme. Acute Kidney Injury. Alan M. Green MPHM13: Acute Kidney Injury. Slide 1 of 47
 MPharm Programme Acute Kidney Injury Alan M. Green 2017 Slide 1 of 47 Overview Renal Function What is it? Why does it matter? What causes it? Who is at risk? What can we (Pharmacists) do? How do you recognise
MPharm Programme Acute Kidney Injury Alan M. Green 2017 Slide 1 of 47 Overview Renal Function What is it? Why does it matter? What causes it? Who is at risk? What can we (Pharmacists) do? How do you recognise
Cardio-Renal Syndrome in Acute Heart Failure:
 Cardio-Renal Syndrome in Acute Heart Failure: Target for Therapy Marvin A. Konstam, M.D. Research support and/or consulting relevant to this lecture: Merck, Otsuka, Johnson & Johnson; Amgen; Cardiokine
Cardio-Renal Syndrome in Acute Heart Failure: Target for Therapy Marvin A. Konstam, M.D. Research support and/or consulting relevant to this lecture: Merck, Otsuka, Johnson & Johnson; Amgen; Cardiokine
Cardiorenal Syndrome: What the Clinician Needs to Know. William T. Abraham, MD Director, Division of Cardiovascular Medicine
 Cardiorenal Syndrome: What the Clinician Needs to Know William T. Abraham, MD Director, Division of Cardiovascular Medicine Orlando, Florida October 7-9, 2011 Renal Hemodynamics in Heart Failure Glomerular
Cardiorenal Syndrome: What the Clinician Needs to Know William T. Abraham, MD Director, Division of Cardiovascular Medicine Orlando, Florida October 7-9, 2011 Renal Hemodynamics in Heart Failure Glomerular
Pathophysiology: Heart Failure
 Pathophysiology: Heart Failure Mat Maurer, MD Irving Assistant Professor of Medicine Outline Definitions and Classifications Epidemiology Muscle and Chamber Function Pathophysiology Heart Failure: Definitions
Pathophysiology: Heart Failure Mat Maurer, MD Irving Assistant Professor of Medicine Outline Definitions and Classifications Epidemiology Muscle and Chamber Function Pathophysiology Heart Failure: Definitions
egfr 34 ml/min egfr 130 ml/min Am J Kidney Dis 2002;39(suppl 1):S17-S31
:S17-S31") Update on Renal Therapeutics Caroline Ashley Lead Pharmacist Renal Services UCL Centre for Nephrology, Royal Free Hospital, London Kongress für Arzneimittelinformation January 2011 What are we going to
Update on Renal Therapeutics Caroline Ashley Lead Pharmacist Renal Services UCL Centre for Nephrology, Royal Free Hospital, London Kongress für Arzneimittelinformation January 2011 What are we going to
CKD and CVD. Jamal Salameh, MD, FACP, FASN First Coast Nephrology
 CKD and CVD Jamal Salameh, MD, FACP, FASN First Coast Nephrology An Epidemic of Kidney Disease Prevalence CKD stages 1-4 10% 1988-94 13% 1999-2004 Coresh, JAMA 298:2038, 2007 Stage 5: GFR
CKD and CVD Jamal Salameh, MD, FACP, FASN First Coast Nephrology An Epidemic of Kidney Disease Prevalence CKD stages 1-4 10% 1988-94 13% 1999-2004 Coresh, JAMA 298:2038, 2007 Stage 5: GFR
Acute Coronary Syndrome (ACS) Patients with Chronic Kidney Disease being considered for Cardiac Catheterization. PROVINCIAL PROTOCOL March 2015
 Patients with Chronic Kidney Disease being considered for Cardiac Catheterization. PROVINCIAL PROTOCOL March 2015") Acute Coronary Syndrome (ACS) Patients with Chronic Kidney Disease being considered for Cardiac Catheterization PROVINCIAL PROTOCOL March 2015 Contents Introduction.......................1 Assessing kidney
Acute Coronary Syndrome (ACS) Patients with Chronic Kidney Disease being considered for Cardiac Catheterization PROVINCIAL PROTOCOL March 2015 Contents Introduction.......................1 Assessing kidney
The ACC Heart Failure Guidelines
 The ACC Heart Failure Guidelines Fakhr Alayoubi, Msc,R Ph President of SCCP Cardiology Clinical Pharmacist Assistant Professor At King Saud University King Khalid University Hospital Riyadh-KSA 2017 ACC/AHA/HFSA
The ACC Heart Failure Guidelines Fakhr Alayoubi, Msc,R Ph President of SCCP Cardiology Clinical Pharmacist Assistant Professor At King Saud University King Khalid University Hospital Riyadh-KSA 2017 ACC/AHA/HFSA
Acute kidney injury and outcomes in acute decompensated heart failure in Korea
 Acute kidney injury and outcomes in acute decompensated heart failure in Korea Mi-Seung Shin 1, Seong Woo Han 2, Dong-Ju Choi 3, Eun Seok Jeon 4, Jae-Joong Kim 5, Myeong-Chan Cho 6, Shung Chull Chae 7,
Acute kidney injury and outcomes in acute decompensated heart failure in Korea Mi-Seung Shin 1, Seong Woo Han 2, Dong-Ju Choi 3, Eun Seok Jeon 4, Jae-Joong Kim 5, Myeong-Chan Cho 6, Shung Chull Chae 7,
CKD FOR INTERNISTS. Dr Ahmed Hossain Associate professor Medicine Sir Salimullah Medical College
 CKD FOR INTERNISTS Dr Ahmed Hossain Associate professor Medicine Sir Salimullah Medical College INTRODUCTION In 2002, the National Kidney Foundation s Kidney Disease Outcomes Quality Initiative(KDOQI)
CKD FOR INTERNISTS Dr Ahmed Hossain Associate professor Medicine Sir Salimullah Medical College INTRODUCTION In 2002, the National Kidney Foundation s Kidney Disease Outcomes Quality Initiative(KDOQI)
QUICK REFERENCE FOR HEALTHCARE PROVIDERS
 KEY MESSAGES 1 SCREENING CRITERIA Screen: Patients with DM and/or hypertension at least yearly. Consider screening patients with: Age >65 years old Family history of stage 5 CKD or hereditary kidney disease
KEY MESSAGES 1 SCREENING CRITERIA Screen: Patients with DM and/or hypertension at least yearly. Consider screening patients with: Age >65 years old Family history of stage 5 CKD or hereditary kidney disease
Section 3: Prevention and Treatment of AKI
 http://www.kidney-international.org & 2012 KDIGO Summary of ommendation Statements Kidney International Supplements (2012) 2, 8 12; doi:10.1038/kisup.2012.7 Section 2: AKI Definition 2.1.1: AKI is defined
http://www.kidney-international.org & 2012 KDIGO Summary of ommendation Statements Kidney International Supplements (2012) 2, 8 12; doi:10.1038/kisup.2012.7 Section 2: AKI Definition 2.1.1: AKI is defined
LXIV: DRUGS: 4. RAS BLOCKADE
 LXIV: DRUGS: 4. RAS BLOCKADE ACE Inhibitors Components of RAS Actions of Angiotensin i II Indications for ACEIs Contraindications RAS blockade in hypertension RAS blockade in CAD RAS blockade in HF Limitations
LXIV: DRUGS: 4. RAS BLOCKADE ACE Inhibitors Components of RAS Actions of Angiotensin i II Indications for ACEIs Contraindications RAS blockade in hypertension RAS blockade in CAD RAS blockade in HF Limitations
Learning Objectives. How big is the problem? ACUTE KIDNEY INJURY
 ACUTE KIDNEY INJURY Karen Innocent, DNP, RN, CRNP, ANP-BC, CMSRN Executive Director, Continuing Education Wolters Kluwer Health, Inc May 2016 Orlando FL Learning Objectives Identify the risk factors and
ACUTE KIDNEY INJURY Karen Innocent, DNP, RN, CRNP, ANP-BC, CMSRN Executive Director, Continuing Education Wolters Kluwer Health, Inc May 2016 Orlando FL Learning Objectives Identify the risk factors and
Outline. Pathophysiology: Heart Failure. Heart Failure. Heart Failure: Definitions. Etiologies. Etiologies
 Outline Pathophysiology: Mat Maurer, MD Irving Assistant Professor of Medicine Definitions and Classifications Epidemiology Muscle and Chamber Function Pathophysiology : Definitions An inability of the
Outline Pathophysiology: Mat Maurer, MD Irving Assistant Professor of Medicine Definitions and Classifications Epidemiology Muscle and Chamber Function Pathophysiology : Definitions An inability of the
Acute Kidney Injury in the Hospitalized Patient
 Acute Kidney Injury in the Hospitalized Patient Biff F. Palmer, M.D. Professor of Internal Medicine University of Texas Southwestern Medical Center, Dallas Texas Classification of Acute Kidney Injury 1
Acute Kidney Injury in the Hospitalized Patient Biff F. Palmer, M.D. Professor of Internal Medicine University of Texas Southwestern Medical Center, Dallas Texas Classification of Acute Kidney Injury 1
From PARADIGM-HF to Clinical Practice. Waleed AlHabeeb, MD, MHA Associate Professor of Medicine President of the Saudi Heart Failure Group
 From PARADIGM-HF to Clinical Practice Waleed AlHabeeb, MD, MHA Associate Professor of Medicine President of the Saudi Heart Failure Group PARADIGM-HF: Inclusion Criteria Chronic HF NYHA FC II IV with LVEF
From PARADIGM-HF to Clinical Practice Waleed AlHabeeb, MD, MHA Associate Professor of Medicine President of the Saudi Heart Failure Group PARADIGM-HF: Inclusion Criteria Chronic HF NYHA FC II IV with LVEF
ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure
 Patients t with acute heart failure frequently develop chronic heart failure Patients with chronic heart failure frequently decompensate acutely ESC Guidelines for the Diagnosis and A clinical response
Patients t with acute heart failure frequently develop chronic heart failure Patients with chronic heart failure frequently decompensate acutely ESC Guidelines for the Diagnosis and A clinical response
Summary/Key Points Introduction
 Summary/Key Points Introduction Scope of Heart Failure (HF) o 6.5 million Americans 20 years of age have HF o 960,000 new cases of HF diagnosed annually o 5-year survival rate for HF is ~50% Classification
Summary/Key Points Introduction Scope of Heart Failure (HF) o 6.5 million Americans 20 years of age have HF o 960,000 new cases of HF diagnosed annually o 5-year survival rate for HF is ~50% Classification
Renal Replacement Therapy - Indication and Follow up
 Renal Replacement Therapy - Indication and Follow up Prof Brigadier General Mamun Mostafi FCPS, FRCP Chief Physician Combined Military Hospital Dhaka Bangladesh Primary Functions of the Kidney Removal
Renal Replacement Therapy - Indication and Follow up Prof Brigadier General Mamun Mostafi FCPS, FRCP Chief Physician Combined Military Hospital Dhaka Bangladesh Primary Functions of the Kidney Removal
ACUTE KIDNEY INJURY. Stuart Linas U. Colorado SOM
 ACUTE KIDNEY INJURY Stuart Linas U. Colorado SOM Marked increases in incidence of dialysis-requiring AKI in last decade JASN 24 37 2013 Question 1 Of patients who recover from an episode of AKI, what percentage
ACUTE KIDNEY INJURY Stuart Linas U. Colorado SOM Marked increases in incidence of dialysis-requiring AKI in last decade JASN 24 37 2013 Question 1 Of patients who recover from an episode of AKI, what percentage
Heart Failure. Subjective SOB (shortness of breath) Peripheral edema. Orthopnea (2-3 pillows) PND (paroxysmal nocturnal dyspnea)
 Peripheral edema. Orthopnea (2-3 pillows) PND (paroxysmal nocturnal dyspnea)") Pharmacology I. Definitions A. Heart Failure (HF) Heart Failure Ezra Levy, Pharm.D. HF Results when one or both ventricles are unable to pump sufficient blood to meet the body s needs There are 2 types
Pharmacology I. Definitions A. Heart Failure (HF) Heart Failure Ezra Levy, Pharm.D. HF Results when one or both ventricles are unable to pump sufficient blood to meet the body s needs There are 2 types
Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes
 Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes Seung-Jae Joo and other KAMIR-NIH investigators Department of Cardiology, Jeju National
Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes Seung-Jae Joo and other KAMIR-NIH investigators Department of Cardiology, Jeju National
Cardiorenal Syndrome
 SOCIEDAD ARGENTINA DE CARDIOLOGIA Cardiorenal Syndrome Joint session ESC-SAC ESC Congress 2012, Munich César A. Belziti Hospital Italiano de Buenos Aires I have no conflicts of interest to declare Cardiorenal
SOCIEDAD ARGENTINA DE CARDIOLOGIA Cardiorenal Syndrome Joint session ESC-SAC ESC Congress 2012, Munich César A. Belziti Hospital Italiano de Buenos Aires I have no conflicts of interest to declare Cardiorenal
Special Challenges and Co-Morbidities
 Special Challenges and Co-Morbidities Renal Disease/ Hypertension/ Diabetes in African-Americans M. Keith Rawlings, MD Medical Director Peabody Health Center AIDS Arms, Inc Dallas, TX Chair, Internal Medicine
Special Challenges and Co-Morbidities Renal Disease/ Hypertension/ Diabetes in African-Americans M. Keith Rawlings, MD Medical Director Peabody Health Center AIDS Arms, Inc Dallas, TX Chair, Internal Medicine
16/05/2018 NEFROPATIA DA MEZZO DI CONTRASTO: ANCORA UNA VECCHIA NEMICA?
 16/05/2018 NEFROPATIA DA MEZZO DI CONTRASTO: ANCORA UNA VECCHIA NEMICA? Dott. Andrea Boccatonda Università degli Studi G. d Annunzio Chieti Chi di voi non ha mai discusso con un radiologo per eseguire
16/05/2018 NEFROPATIA DA MEZZO DI CONTRASTO: ANCORA UNA VECCHIA NEMICA? Dott. Andrea Boccatonda Università degli Studi G. d Annunzio Chieti Chi di voi non ha mai discusso con un radiologo per eseguire
Renal replacement therapy in Pediatric Acute Kidney Injury
 Renal replacement therapy in Pediatric Acute Kidney Injury ASCIM 2014 Dr Adrian Plunkett Consultant Paediatric Intensivist Birmingham Children s Hospital, UK Aims of the presentation Important topic: AKI
Renal replacement therapy in Pediatric Acute Kidney Injury ASCIM 2014 Dr Adrian Plunkett Consultant Paediatric Intensivist Birmingham Children s Hospital, UK Aims of the presentation Important topic: AKI
Heart-failure or Kidney Failure?
 Heart-failure or Kidney Failure? Dr Ajith James Consultant Nephrologist Barts Health and BHRUT Mr AR 65 yrs Case Type 2 DM, IHD-MI 1998, 2003. PCI x 3. CABG 2008, HT CCF with LVEF 30% 2014. NYHA Class
Heart-failure or Kidney Failure? Dr Ajith James Consultant Nephrologist Barts Health and BHRUT Mr AR 65 yrs Case Type 2 DM, IHD-MI 1998, 2003. PCI x 3. CABG 2008, HT CCF with LVEF 30% 2014. NYHA Class
Office Management of Reduced GFR Practical advice for the management of CKD
 Office Management of Reduced GFR Practical advice for the management of CKD CKD Online Education CME for Primary Care April 27, 2016 Monica Beaulieu, MD FRCPC MHA CHAIR PROVINCIAL KIDNEY CARE COMMITTEE
Office Management of Reduced GFR Practical advice for the management of CKD CKD Online Education CME for Primary Care April 27, 2016 Monica Beaulieu, MD FRCPC MHA CHAIR PROVINCIAL KIDNEY CARE COMMITTEE
Metabolic Syndrome and Chronic Kidney Disease
 Metabolic Syndrome and Chronic Kidney Disease Definition of Metabolic Syndrome National Cholesterol Education Program (NCEP) Adult Treatment Panel (ATP) III Abdominal obesity, defined as a waist circumference
Metabolic Syndrome and Chronic Kidney Disease Definition of Metabolic Syndrome National Cholesterol Education Program (NCEP) Adult Treatment Panel (ATP) III Abdominal obesity, defined as a waist circumference
Congestive Heart Failure: Outpatient Management
 The Chattanooga Heart Institute Cardiovascular Symposium Congestive Heart Failure: Outpatient Management E. Philip Lehman MD, MPP Disclosure No financial disclosures. Objectives Evidence-based therapy
The Chattanooga Heart Institute Cardiovascular Symposium Congestive Heart Failure: Outpatient Management E. Philip Lehman MD, MPP Disclosure No financial disclosures. Objectives Evidence-based therapy
Cardiorenal Syndrome: Clinical Outcome Study
 Journal of The Association of Physicians of India Vol. 64 December 2016 41 Original Article Cardiorenal Syndrome: Clinical Outcome Study HR Shah 1, NP Singh 2, NP Aggarwal 3, D Singhania 4, LK Jha 3, A
Journal of The Association of Physicians of India Vol. 64 December 2016 41 Original Article Cardiorenal Syndrome: Clinical Outcome Study HR Shah 1, NP Singh 2, NP Aggarwal 3, D Singhania 4, LK Jha 3, A
Protocol Identifier Subject Identifier Visit Description. [Y] Yes [N] No. [Y] Yes [N] N. If Yes, admission date and time: Day Month Year
![Protocol Identifier Subject Identifier Visit Description. [Y] Yes [N] No. [Y] Yes [N] N. If Yes, admission date and time: Day Month Year](/thumbs/76/74263761.jpg "Protocol Identifier Subject Identifier Visit Description. [Y] Yes [N] No. [Y] Yes [N] N. If Yes, admission date and time: Day Month Year") PAST MEDICAL HISTORY Has the subject had a prior episode of heart failure? o Does the subject have a prior history of exposure to cardiotoxins, such as anthracyclines? URGENT HEART FAILURE VISIT Did heart
PAST MEDICAL HISTORY Has the subject had a prior episode of heart failure? o Does the subject have a prior history of exposure to cardiotoxins, such as anthracyclines? URGENT HEART FAILURE VISIT Did heart
Doppler ultrasound, see Ultrasonography. Magnetic resonance imaging (MRI), kidney oxygenation assessment 75
, kidney oxygenation assessment 75") Subject Index Acidemia, cardiorenal syndrome type 3 146 Acute Dialysis Quality Initiative (ADQI) acute kidney injury biomarkers, see Acute kidney injury; specific biomarkers cardiorenal syndrome, see specific
Subject Index Acidemia, cardiorenal syndrome type 3 146 Acute Dialysis Quality Initiative (ADQI) acute kidney injury biomarkers, see Acute kidney injury; specific biomarkers cardiorenal syndrome, see specific
The Art and Science of Diuretic therapy
 The Art and Science of Diuretic therapy Dr. Fayez EL Shaer Associate Professour of cardiology Consultant cardiologist MD, MSc, PhD, CBNC, NBE FESC, ACCP, FASNC,HFA KKUH, KFCC Heart failure: fluid overload
The Art and Science of Diuretic therapy Dr. Fayez EL Shaer Associate Professour of cardiology Consultant cardiologist MD, MSc, PhD, CBNC, NBE FESC, ACCP, FASNC,HFA KKUH, KFCC Heart failure: fluid overload
Screening and early recognition of CKD. John Ngigi (FISN) Kidney specialist
 Kidney specialist") Screening and early recognition of CKD John Ngigi (FISN) Kidney specialist screening Why? Who? When? How? Primary diagnosis for patients who start dialysis Other 10% Glomerulonephritis 13% No. of dialysis
Screening and early recognition of CKD John Ngigi (FISN) Kidney specialist screening Why? Who? When? How? Primary diagnosis for patients who start dialysis Other 10% Glomerulonephritis 13% No. of dialysis
HFpEF. April 26, 2018
 HFpEF April 26, 2018 (J Am Coll Cardiol 2017;70:2476 86) HFpEF 50% or more (40-71%) of patients with CHF have preserved LV systolic function. HFpEF is an increasingly frequent hospital discharge. Outcomes
HFpEF April 26, 2018 (J Am Coll Cardiol 2017;70:2476 86) HFpEF 50% or more (40-71%) of patients with CHF have preserved LV systolic function. HFpEF is an increasingly frequent hospital discharge. Outcomes
LCZ696 A First-in-Class Angiotensin Receptor Neprilysin Inhibitor
 The Angiotensin Receptor Neprilysin Inhibitor LCZ696 in Heart Failure with Preserved Ejection Fraction The Prospective comparison of ARNI with ARB on Management Of heart failure with preserved ejection
The Angiotensin Receptor Neprilysin Inhibitor LCZ696 in Heart Failure with Preserved Ejection Fraction The Prospective comparison of ARNI with ARB on Management Of heart failure with preserved ejection
Fluid Resuscitation in Critically Ill Patients with Acute Kidney Injury (AKI)
") Fluid Resuscitation in Critically Ill Patients with Acute Kidney Injury (AKI) Robert W. Schrier, MD University of Colorado School of Medicine Denver, Colorado USA Prevalence of acute renal failure in Intensive
Fluid Resuscitation in Critically Ill Patients with Acute Kidney Injury (AKI) Robert W. Schrier, MD University of Colorado School of Medicine Denver, Colorado USA Prevalence of acute renal failure in Intensive
Clinical efficacy of ultrafiltration in the treatment of acute decompensated heart failure with diuretic resistance.
 Biomedical Research 2017; 28 (14): 6155-6159 ISSN 0970-938X www.biomedres.info Clinical efficacy of ultrafiltration in the of acute decompensated heart failure with diuretic resistance. Jian Zhang, Qi
Biomedical Research 2017; 28 (14): 6155-6159 ISSN 0970-938X www.biomedres.info Clinical efficacy of ultrafiltration in the of acute decompensated heart failure with diuretic resistance. Jian Zhang, Qi
Chronic Kidney Disease The 6 Pillars. Dr. Tiina Podymow Associate Professor Division of Nephrology McGill University Health Centre
 Chronic Kidney Disease The 6 Pillars Dr. Tiina Podymow Associate Professor Division of Nephrology McGill University Health Centre None Disclosures Objectives 1. Describe evidence-based measures to slow
Chronic Kidney Disease The 6 Pillars Dr. Tiina Podymow Associate Professor Division of Nephrology McGill University Health Centre None Disclosures Objectives 1. Describe evidence-based measures to slow
ALLHAT RENAL DISEASE OUTCOMES IN HYPERTENSIVE PATIENTS STRATIFIED INTO 4 GROUPS BY BASELINE GLOMERULAR FILTRATION RATE (GFR)
") 1 RENAL DISEASE OUTCOMES IN HYPERTENSIVE PATIENTS STRATIFIED INTO 4 GROUPS BY BASELINE GLOMERULAR FILTRATION RATE (GFR) 6 / 5 / 1006-1 2 Introduction Hypertension is the second most common cause of end-stage
1 RENAL DISEASE OUTCOMES IN HYPERTENSIVE PATIENTS STRATIFIED INTO 4 GROUPS BY BASELINE GLOMERULAR FILTRATION RATE (GFR) 6 / 5 / 1006-1 2 Introduction Hypertension is the second most common cause of end-stage
Trial to Reduce. Aranesp* Therapy. Cardiovascular Events with
 Trial to Reduce Cardiovascular Events with Aranesp* Therapy John J.V. McMurray, Hajime Uno, Petr Jarolim, Akshay S. Desai, Dick de Zeeuw, Kai-Uwe Eckardt, Peter Ivanovich, Andrew S. Levey, Eldrin F. Lewis,
Trial to Reduce Cardiovascular Events with Aranesp* Therapy John J.V. McMurray, Hajime Uno, Petr Jarolim, Akshay S. Desai, Dick de Zeeuw, Kai-Uwe Eckardt, Peter Ivanovich, Andrew S. Levey, Eldrin F. Lewis,
Chronic Kidney Disease for the Primary Care Physician in What do the Kidneys do? CKD in the US
 1:25-2:25pm Managing Chronic Kidney Disease in 2019 SPEAKERS Adriana Dejman, MD Chronic Kidney Disease for the Primary Care Physician in 2019 Adriana Dejman, MD Assistant Professor of Clinical Medicine
1:25-2:25pm Managing Chronic Kidney Disease in 2019 SPEAKERS Adriana Dejman, MD Chronic Kidney Disease for the Primary Care Physician in 2019 Adriana Dejman, MD Assistant Professor of Clinical Medicine
CKD and risk management : NICE guideline
 CKD and risk management : NICE guideline 2008-2014 Shahed Ahmed Consultant Nephrologist shahed.ahmed@rlbuht.nhs.uk Key points : Changing parameters of CKD and NICE guidance CKD and age related change of
CKD and risk management : NICE guideline 2008-2014 Shahed Ahmed Consultant Nephrologist shahed.ahmed@rlbuht.nhs.uk Key points : Changing parameters of CKD and NICE guidance CKD and age related change of
Prevalence of anemia and cardiovascular diseases in chronic kidney disease patients: a single tertiary care centre study
 International Journal of Advances in Medicine Sathyan S et al. Int J Adv Med. 2017 Feb;4(1):247-251 http://www.ijmedicine.com pissn 2349-3925 eissn 2349-3933 Original Research Article DOI: http://dx.doi.org/10.18203/2349-3933.ijam20170120
International Journal of Advances in Medicine Sathyan S et al. Int J Adv Med. 2017 Feb;4(1):247-251 http://www.ijmedicine.com pissn 2349-3925 eissn 2349-3933 Original Research Article DOI: http://dx.doi.org/10.18203/2349-3933.ijam20170120
Acute Kidney Injury- What Is It and How Do I Treat It?
 Acute Kidney Injury- What Is It and How Do I Treat It? Jayant Kumar, MD Renal Medicine Assoc., Albuquerque, NM Incidence of ARF in ICU Causes of ARF Non -ICU ICU 1 KDIGO criteria for AKI Increase in serum
Acute Kidney Injury- What Is It and How Do I Treat It? Jayant Kumar, MD Renal Medicine Assoc., Albuquerque, NM Incidence of ARF in ICU Causes of ARF Non -ICU ICU 1 KDIGO criteria for AKI Increase in serum
The Diabetes Kidney Disease Connection Missouri Foundation for Health February 26, 2009
 The Diabetes Kidney Disease Connection Missouri Foundation for Health February 26, 2009 Teresa Northcutt, RN BSN Primaris Program Manager, Prevention - CKD MO-09-01-CKD This material was prepared by Primaris,
The Diabetes Kidney Disease Connection Missouri Foundation for Health February 26, 2009 Teresa Northcutt, RN BSN Primaris Program Manager, Prevention - CKD MO-09-01-CKD This material was prepared by Primaris,
DIASTOLIC HEART FAILURE
 DIASTOLIC HEART FAILURE M Mohsen Ibrahim, MD Alexandria, Proposed Criteria for Diastolic Heart Failure ESC Working Group (EHJ 1998) CHF signs/symptoms EF 45% Hemodynamic or echo evidence of diastolic dysfunction
DIASTOLIC HEART FAILURE M Mohsen Ibrahim, MD Alexandria, Proposed Criteria for Diastolic Heart Failure ESC Working Group (EHJ 1998) CHF signs/symptoms EF 45% Hemodynamic or echo evidence of diastolic dysfunction
Pathophysiology: Heart Failure. Objectives
 Pathophysiology: Heart Failure Mat Maurer, MD Irving Assistant Professor of Clinical Medicine Objectives At the conclusion of this seminar, learner will be able to: 1. Define heart failure as a clinical
Pathophysiology: Heart Failure Mat Maurer, MD Irving Assistant Professor of Clinical Medicine Objectives At the conclusion of this seminar, learner will be able to: 1. Define heart failure as a clinical
Volume Management 2/25/2017. Disclosures statement: Objectives. To discuss evaluation of hypervolemia in peritoneal dialysis patients
 Volume Management Sagar Nigwekar MD, MMSc Massachusetts General Hospital E-mail: snigwekar@mgh.harvard.edu March 14, 2017 Disclosures statement: Consultant: Allena, Becker Professional Education Grant
Volume Management Sagar Nigwekar MD, MMSc Massachusetts General Hospital E-mail: snigwekar@mgh.harvard.edu March 14, 2017 Disclosures statement: Consultant: Allena, Becker Professional Education Grant
Renal Disease and PK/PD. Anjay Rastogi MD PhD Division of Nephrology
 Renal Disease and PK/PD Anjay Rastogi MD PhD Division of Nephrology Drugs and Kidneys Kidney is one of the major organ of drug elimination from the human body Renal disease and dialysis alters the pharmacokinetics
Renal Disease and PK/PD Anjay Rastogi MD PhD Division of Nephrology Drugs and Kidneys Kidney is one of the major organ of drug elimination from the human body Renal disease and dialysis alters the pharmacokinetics
A patient with acute heart failure and renal impairment ACCA Masterclass 2017
 A patient with acute heart failure and renal impairment Dr Sofie Gevaert Mister P. J.M., 67-years-old Cardiac risk factors: Ex-smoker, AHT, Type 2 diabetes, BMI 43, Hyperlipidaemia Medical history: 2009:
A patient with acute heart failure and renal impairment Dr Sofie Gevaert Mister P. J.M., 67-years-old Cardiac risk factors: Ex-smoker, AHT, Type 2 diabetes, BMI 43, Hyperlipidaemia Medical history: 2009:
Drug Use in Dialysis
 (Last Updated: 08/22/2018) Created by: Socco, Samantha Drug Use in Dialysis Drambarean, B. (2017). Drug Use in Dialysis. Lecture presented at PHAR 503 Lecture in UIC College of Pharmacy, Chicago. DIALYSIS
(Last Updated: 08/22/2018) Created by: Socco, Samantha Drug Use in Dialysis Drambarean, B. (2017). Drug Use in Dialysis. Lecture presented at PHAR 503 Lecture in UIC College of Pharmacy, Chicago. DIALYSIS
Chronic Kidney Disease
 Chronic Kidney Disease Chronic Kidney Disease (CKD) Educational Objectives Outline Demographics Propose Strategies to slow progression and improve outcomes Plan for treatment of CKD Chronic Kidney Disease
Chronic Kidney Disease Chronic Kidney Disease (CKD) Educational Objectives Outline Demographics Propose Strategies to slow progression and improve outcomes Plan for treatment of CKD Chronic Kidney Disease
HEART FAILURE. Heart Failure in the US. Heart Failure (HF) 3/2/2014
 3/2/2014") HEART FAILURE Martina Frost, PA-C Desert Cardiology of Tucson Northwest Medical Center March 2014 Heart Failure in the US Prevalence - ~5 million 650,000 new cases annually 300,000 deaths annually Leading
HEART FAILURE Martina Frost, PA-C Desert Cardiology of Tucson Northwest Medical Center March 2014 Heart Failure in the US Prevalence - ~5 million 650,000 new cases annually 300,000 deaths annually Leading
UPDATES IN MANAGEMENT OF HF
 UPDATES IN MANAGEMENT OF HF Jennifer R Brown MD, MS Heart Failure Specialist Medstar Cardiology Associates DC ACP Meeting Fall 2017 Disclosures: speaker bureau for novartis speaker bureau for actelion
UPDATES IN MANAGEMENT OF HF Jennifer R Brown MD, MS Heart Failure Specialist Medstar Cardiology Associates DC ACP Meeting Fall 2017 Disclosures: speaker bureau for novartis speaker bureau for actelion
changes that occur in kidney with aging is THE MOST DRAMATIC ANY ORGAN SYSTEM.
 The Kidney in Aging The the OF OF changes that occur in kidney with aging is THE MOST DRAMATIC ANY ORGAN SYSTEM. Age related charges in kidney structure and function At age 2 GFR at adult level. Reamins
The Kidney in Aging The the OF OF changes that occur in kidney with aging is THE MOST DRAMATIC ANY ORGAN SYSTEM. Age related charges in kidney structure and function At age 2 GFR at adult level. Reamins
Acute Kidney Injury (AKI) How Wise is Early Dialysis in Critically Ill Patients? Modalities of Dialysis
 How Wise is Early Dialysis in Critically Ill Patients? Modalities of Dialysis") Acute Kidney Injury (AKI) How Wise is Early Dialysis in Critically Ill Patients? A common condition in ICU patients Associated with high mortality and morbidity Renal Replacement Therapy (RRT) is the cornerstone
Acute Kidney Injury (AKI) How Wise is Early Dialysis in Critically Ill Patients? A common condition in ICU patients Associated with high mortality and morbidity Renal Replacement Therapy (RRT) is the cornerstone
Prevention of Contrast induced Nephropathy
 55 th Annual Scientific Meeting of The Korean Society of Cardiology 11:50 12:10 Message from Nephrologists Dec 03, 2011 Prevention of Contrast induced Nephropathy Soo Wan Kim, MD, PhD Department of Internal
55 th Annual Scientific Meeting of The Korean Society of Cardiology 11:50 12:10 Message from Nephrologists Dec 03, 2011 Prevention of Contrast induced Nephropathy Soo Wan Kim, MD, PhD Department of Internal
Optimal blockade of the Renin- Angiotensin-Aldosterone. in chronic heart failure
 Optimal blockade of the Renin- Angiotensin-Aldosterone Aldosterone- (RAA)-System in chronic heart failure Jan Östergren Department of Medicine Karolinska University Hospital Stockholm, Sweden Key Issues
Optimal blockade of the Renin- Angiotensin-Aldosterone Aldosterone- (RAA)-System in chronic heart failure Jan Östergren Department of Medicine Karolinska University Hospital Stockholm, Sweden Key Issues
Protecting the heart and kidney: implications from the SHARP trial
 Cardiology Update, Davos, 2013: Satellite Symposium Protecting the heart and kidney: implications from the SHARP trial Colin Baigent Professor of Epidemiology CTSU, University of Oxford S1 First CTT cycle:
Cardiology Update, Davos, 2013: Satellite Symposium Protecting the heart and kidney: implications from the SHARP trial Colin Baigent Professor of Epidemiology CTSU, University of Oxford S1 First CTT cycle:
Aldosterone Antagonism in Heart Failure: Now for all Patients?
 Aldosterone Antagonism in Heart Failure: Now for all Patients? Inder Anand, MD, FRCP, D Phil (Oxon.) Professor of Medicine, University of Minnesota, Director Heart Failure Program, VA Medical Center 111C
Aldosterone Antagonism in Heart Failure: Now for all Patients? Inder Anand, MD, FRCP, D Phil (Oxon.) Professor of Medicine, University of Minnesota, Director Heart Failure Program, VA Medical Center 111C
Editorial Staying in the Pink of Health for Patients with Cardiorenal Anemia Requires a Multidisciplinary Approach
 Editorial Staying in the Pink of Health for Patients with Cardiorenal Anemia Requires a Multidisciplinary Approach Anemia and Heart Failure Ragavendra R. Baliga, MD, MBA James B. Young, MD Consulting Editors
Editorial Staying in the Pink of Health for Patients with Cardiorenal Anemia Requires a Multidisciplinary Approach Anemia and Heart Failure Ragavendra R. Baliga, MD, MBA James B. Young, MD Consulting Editors
Update on Cardiorenal Syndrome: A Clinical Conundrum
 Advances in Peritoneal Dialysis, Vol. 27, 2011 Eric J. Chan, 1 Kevin C. Dellsperger 1 3 Update on Cardiorenal Syndrome: A Clinical Conundrum Our understanding of the cardiorenal syndrome continues to progress.
Advances in Peritoneal Dialysis, Vol. 27, 2011 Eric J. Chan, 1 Kevin C. Dellsperger 1 3 Update on Cardiorenal Syndrome: A Clinical Conundrum Our understanding of the cardiorenal syndrome continues to progress.
Outline. Outline CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW. Question 1: Which of these patients has CKD?
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,