Erosion of Woven Polyester Pubovaginal Sling. The Dalkon Shield. William Stewart Halsted, M.D
|
|
|
- Claire Collins
- 5 years ago
- Views:
Transcription


1 Who Are We and Who Should We Be As 21 st Century Pelvic Reconstructive Surgeons? Daniel K. Roberts Lecture June 14, 2013 Wichita, KS Bob L. Shull, M.D. Professor of Obstetrics and Gynecology Scott & White Clinic and Hospital Texas A&M University Health Sciences Center Temple, Texas USA Learning objectives My wife and I have no financial disclosures to make At then end of the presentation you will: 1. Know you have at least 2 roles you serve 2. Know there is legitimate t concern regarding the use of mesh kits for reconstructive vaginal surgery 3. Know how to identify specific anatomic pelvic support defects Pretest Are you a: a) Gynecologic surgeon b) Learned intermediary c) Fiduciary for your patient d) Thought leader e) Plaintiff s lawyer f) Teacher g) Mentor Why Does It Matter? 1




2 We Are In The Middle of A Perfect Storm: Surgeons who want to be on the leading edge Patients who are willing to be alpha test subjects Industry who wants to sell products Poor regulatory oversight Potent Medico-Legal system Timeless Qualities of a Surgeon Timeless Qualities of a Surgeon Diligence 2





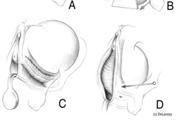
3 William Stewart Halsted, M.D Surgeon-in-chief Johns Hopkins Hospital Professor of Surgery Johns Hopkins University School of Medicine The past: That which will not tell us what we ought to do what we ought to avoid. -José Ortega y Gossett Ignaz Simmelweis Savior of Mothers Childbed fever Wash your hands in chlorinated lime solutions The Dalkon Shield Erosion of Woven Polyester Pubovaginal Sling Purpose: Use of synthetic materials provides a theoretical advantage in that no graft harvesting is necessary. Major risks of synthetic material use are erosion and infection of the sling. We report on erosion of woven polyester slings treated with pressure injected bovine collagen (ProteGen*) which required removal. Results: A total of 34 women required removal of the polyester sling secondary to erosion, infection or pain. Kobashi KC, Dmochowski R, Mee SL, et.al. The Journal of Urology, 1999 Dec; 162,
4 Total Pelvic Mesh Repair: A Ten-Year Experience Results: From January 1990 to December 1999, 236 females had total pelvic mesh repair, and 205 (87 percent) were available for follow-up. Reoperation rate because of complications of the total pelvic mesh repair procedure was 10 percent. Additional surgical procedures at various intervals subsequent to total pelvic mesh repair have been performed in 36 percent of patients to further improve bladder function and have been performed in 28 percent of patients to improve anorectal function. Timeless Qualities of a Surgeon Diligence Doing the Right Thing Sullivan ES, Longaker CJ, Lee PY Dis Colon Rectum 2001 Jun;44(6): Timeless Qualities of a Surgeon Diligence Doing the Right Thing First Do No Harm Hippocratic Oath Timeless Qualities of a Surgeon Diligence Doing the Right Thing First Do No Harm Harm Hippocratic Oath Ingenuity Thomas Hepburn Retropubic Urethropexy Ulf Ulmsten Tension Free Vaginal Tape Societal issues which presently effect and will continue to influence the surgeon s behavior. 4

5 Societal issues which presently effect and will continue to influence the surgeon s behavior. Communication Connectivity Societal issues which presently effect and will continue to influence the surgeon s behavior. Communication Connectivity Medico-Legal Systems Societal issues which presently effect and will continue to influence the surgeon s behavior. Physician Industry Relationships Communication Connectivity Medico-Legal Systems Physician-Industry Relationships Reports: Data on Vioxx was misused Corporate and government documents from Vioxx lawsuits indicate that the drug's maker, Merck & Co., apparently downplayed evidence showing the painkiller tripled the risk of death in Alzheimer's-prone patients, researchers report today. Reports: Data on Vioxx was misused "The drug industry appears to treat scientific data as if they were a marketing tool," says the University of Washington's Bruce Pasty, a co-author of one of the JAMA articles. "That's not appropriate." USA Today:Wednesday, April 16, 2008 USA Today:Wednesday, April 16,
6 Reports: Data on Vioxx was misused The Vioxx disclosures are "just the tip of the iceberg," JAMA editor Catherine DeAngelis says. "I've been sitting in this office for eight years, watching physicians and clinical researchers be used by pharmaceutical companies in ways that can end up with patients being hurt. Physicians have allowed it to happen, and it's time to stop." USA Today:Wednesday, April 16, 2008 Information on Surgical Mesh for Pelvic Organ Prolapse and Stress Urinary Incontinence FDA U.S. Food and Drug Administration 10/21/2008 What to Advise Patients About Hernias Commentary by Edward H. Livingston, MD What advice should primary care clinicians give to patients regarding repair of abdominal wall hernia? Do all hernias need repair? If the hernia is repaired, should mesh be used? If so, why, and what are the risks? Is the operation best performed laparoscopically? JAMA, September 1, 2010 Vol 304, No 9 Following diagnosis of a hernia, patients are referred to surgeons for repair to reduce hernia-related related symptoms and to avoid complications. It was assumed, but never proven, that the risks of hernia surgery were less than those posed by the risk for complications that might be attributable to hernias. This study showed that the commonly accepted approach that all hernias require repair is no longer valid. JAMA, September 1, 2010 Vol 304, No 9 Mesh is not risk free and can cause chronic pain or become infected. The pendulum has swung too far in favor of mesh implantation, and it is commonly placed to reinforce congenital umbilical hernias or other abdominal wall hernias that are surrounded by healthy, durable fascia in which reinforcement of the defect is not necessary. Placement of mesh on the inside of the abdominal wall adds risk because it might contact the bowel, which tends to attach to mesh and may result in bowel obstruction, mesh infection, and fistula formation. JAMA, September 1, 2010 Vol 304, No 9 Major complications were more frequent in the laparoscopic group compared with the open surgery group (4.4% vs 1.4%, respectively), and were mostly attributable to bowel injuries. There was no statistical difference at 2 years for hernia recurrence rates (12.5% for the laparoscopic group vs 8.2% for the open surgery group). Similarly, quality-of of-life and pain scores were similar between groups in the long term. In another well-executed executed randomized controlled trial comparing laparoscopic with open groin hernia operations, Neumayer et al reported similar results for hernia outcomes, with somewhat better results for open operations. JAMA, September 1, 2010 Vol 304, No 9 6
7 Clinical Opinion -Urogynecology Use of vaginal mesh in the face of recent FDA warnings and litigation Use of vaginal mesh in the face of recent FDA warnings and litigation Many gynecologists may be hesitant to continue offering vaginal mesh procedures secondary to recent FDA warnings and the many advertisements from plaintiff attorneys seeking patients who have experienced complications from their mesh placements. Mucowski SJ, MD; Jurnalow C, MD; Phelps JY. Use of vaginal mesh in the face of recent FDA warnings and litigation. Am J Obstet Gynecol 2010;203:103 e1-4. Mucowski SJ, MD; Jurnalow C, MD; Phelps JY. Use of vaginal mesh in the face of recent FDA warnings and litigation. Am J Obstet Gynecol 2010;203:103 e1-4. Use of vaginal mesh in the face of recent FDA warnings and litigation Learned intermediary doctrine and preemption The learned intermediary doctrine shifts the liability of harm caused by a medication or medical device away from the manufacturer and onto the physician prescribing or using the product. Overall, under learned intermediary doctrine, if a manufacturer adequately warns a physician of a product s potential complications and risks, then they do not possess the legal duty to warn patients of possible dangers associated with their product. Instead, the duty to warn falls on the physician prescribing the product. Use of vaginal mesh in the face of recent FDA warnings and litigation Learned intermediary doctrine and preemption For example, in Linsley v C.R. Bard Inc,, the manufacturer of Marlex mesh used the learned intermediary doctrine to shift liability of the duty to warn patients of potential complications onto physicians. This suit stated that mesh was and is a prescription medical device, which requires that it be used only upon order of a qualified physician, thus the warning required is not to the general public or to the patient, but to the prescribing physician. Mucowski SJ, MD; Jurnalow C, MD; Phelps JY. Use of vaginal mesh in the face of recent FDA warnings and litigation. Am J Obstet Gynecol 2010;203:103 e1-4. Mucowski SJ, MD; Jurnalow C, MD; Phelps JY. Use of vaginal mesh in the face of recent FDA warnings and litigation. Am J Obstet Gynecol 2010;203:103 e1-4. Use of vaginal mesh in the face of recent FDA warnings and litigation Learned intermediary doctrine and preemption Johnson & Johnson (New Brunswick, NJ), the parent company of Ethicon (Somerville, NJ), a manufacturer of mesh used in tension-free midurethral tape procedures, has used the learned intermediary doctrine to shift liability away from itself in suits involving its pharmaceutical product, the Ortho Evra Patch. If the learned intermediary doctrine is used by a company in suits involving transvaginal mesh, gynecologists can attempt to redirect responsibility to the manufacturer by showing that they did not receive adequate warning of risks associated with the use of their product. However, with the recent FDA warnings, it will be difficult for gynecologists to successfully argue they were not aware of the potential complications involving the use of mesh in vaginal reconstructive surgery. Use of vaginal mesh in the face of recent FDA warnings and litigation Learned intermediary doctrine and preemption Alternatively, a better choice for gynecologists defending themselves from liability is to assure there is documentation in the medical record that the patient was properly informed of the potential complications that may be encountered with mesh use in vaginal reconstructive surgery. Another recent development that significantly impacts existing and deters future lawsuits against manufacturers of medical devices is the 2008 US Supreme Court case Riegel v Medtronic Inc. In this case, the US Supreme Court held that the preemption clause enacted in the Medical Device Amendments, 21 USC 360k (1976), bars claims challenging the safety and effectiveness of a medical device given premarket approval by the FDA. Mucowski SJ, MD; Jurnalow C, MD; Phelps JY. Use of vaginal mesh in the face of recent FDA warnings and litigation. Am J Obstet Gynecol 2010;203:103 e1-4. Mucowski SJ, MD; Jurnalow C, MD; Phelps JY. Use of vaginal mesh in the face of recent FDA warnings and litigation. Am J Obstet Gynecol 2010;203:103 e1-4. 7
8 Use of vaginal mesh in the face of recent FDA warnings and litigation Learned intermediary doctrine and preemption As a result, patients injured by a medical device previously approved by the FDA have little recourse other than to sue their physicians. Use of vaginal mesh in the face of recent FDA warnings and litigation Fiduciary responsibility The relationship between the physician and the patient is one of fiduciary i responsibility, meaning that t the patient t seeks out a physician, trusting that the physician possesses a level of knowledge necessary to inform the patient. This is essential when providing informed consent of surgical procedures. Mucowski SJ, MD; Jurnalow C, MD; Phelps JY. Use of vaginal mesh in the face of recent FDA warnings and litigation. Am J Obstet Gynecol 2010;203:103 e1-4. Mucowski SJ, MD; Jurnalow C, MD; Phelps JY. Use of vaginal mesh in the face of recent FDA warnings and litigation. Am J Obstet Gynecol 2010;203:103 e1-4. Use of vaginal mesh in the face of recent FDA warnings and litigation Potential causes of action against physicians Overall, there are 2 major potential instances where physicians may find themselves liable in a lawsuit surrounding the use of transvaginal mesh. The first is basic medical negligence in using mesh that is knowingly harmful to the patient, and the second is failure to obtain adequate informed consent for the procedure. Letters to the Editor - AJOG Informed consent cannot be obtained for use of vaginal mesh Mucowski SJ, MD; Jurnalow C, MD; Phelps JY. Use of vaginal mesh in the face of recent FDA warnings and litigation. Am J Obstet Gynecol 2010;203:103 e1-4. Anne M. Weber, MD, MS, American Journal of Obstetrics & Gynecology March 2011 e6 The New England Journal of Medicine Original Article Anterior Colporrhaphy versus Transvaginal Mesh for Pelvic-Organ Prolapse Daniel Altman, M.D., Ph.D., Tapio Väyrynen, M.D., Maria Ellström Engh, M.D., Ph.D., Susanne Axelsen, M.D., Ph.D., and Christian Falconer, M.D., Ph.D., for the Nordic Transvaginal Mesh Group N Engl J Med 364;19 NEJM.ORG May 12, 2011 Anterior Colporrhaphy versus Transvaginal Mesh for Pelvic-Organ Prolapse Background The use of standardized mesh kits for repair of pelvic-organ prolapse has spread rapidly in recent years, but it is unclear whether this approach results in better outcomes than traditional colporrhaphy. N Engl J Med 364;19 NEJM.ORG May 12,
9 Anterior Colporrhaphy versus Transvaginal Mesh for Pelvic-Organ Prolapse Conclusions As compared with anterior colporrhaphy, use of a standardized, trocar-guided mesh kit for cystocele repair resulted in higher short-term term rates of successful treatment but also in higher rates of surgical complications and postoperative adverse events. (Funded by the Karolinska Institutet and Ethicon; ClinicalTrials.gov number, NCT ) N Engl J Med 364;19 NEJM.ORG May 12, 2011 Urogynecologic Surgical Mesh: Update on the Safety and Effectiveness Of Transvaginal Placement for Pelvic Organ Prolapse July 2011 Executive Summary In October 2008, the FDA issued a Public Health Notification (PHN) to inform clinicians and patients of adverse events related to urogynecologic use of surgical mesh, and to provide recommendations on how to mitigate risks and how to counsel patients. Following the PHN, the FDA continued to monitor the outcomes of urogynecologic use of surgical mesh. A search of the FDA s Manufacturer and User Device Experience (MAUDE) database from the last 3 years (January 1, 2008-December 31, 2010), identified 2,874 Medical Device Reports (MDRs) for urogynecologic surgical meshes, including reports of injury, death, and malfunctions. Among the 2,874 reports, 1,503 were associated with pelvic organ prolapse (POP) repairs, and 1,371 were associated with stress urinary incontinence (SUI) repairs. Overview In 1996, the FDA cleared the first surgical mesh product specifically for use in SUI, and in 2002, the FDA cleared the first surgical mesh product specifically for use in POP. Over the next few years, surgical mesh products for transvaginal POP repair became incorporated into kits that included tools to aid in the delivery and insertion of the mesh. Surgical mesh kits continue to evolve, adding new insertion tools, tissue fixation anchors, surgical techniques, and absorbable and biologic materials. Clinical performance data typically has not been used to support clearance for POP or SUI urogynecologic mesh products. Safety The literature review identified the following safety concerns with transvaginally placed surgical mesh for POP repair: Patients who undergo POP repair with mesh are subject to mesh-related complications that are not experienced by patients who undergo traditional surgery without mesh. Adverse events associated with transvaginally placed mesh can be life-altering for some women. Sequelae (e.g., pain) may continue despite mesh removal. Safety cont d Mesh-associated complications are not rare. The most common mesh-related complication experienced by patients undergoing transvaginal POP repair with mesh is vaginal mesh erosion. Based on data from 110 studies including 11,785 women, approximately 10 percent of women undergoing transvaginal POP repair with mesh experienced mesh erosion within 12 months of surgery. More than half of the women who experienced erosion from non-absorbable synthetic mesh required surgical excision in the operating room. Some women required two to three additional surgeries. 9
10 Safety cont d Mesh contraction, causing vaginal shortening, tightening, and/or vaginal pain in association with transvaginal POP repair with mesh, is increasingly reported in the literature. New onset SUI has been reported to occur more frequently following mesh augmented anterior repair compared to traditional anterior repair without mesh. Safety cont d Transvaginal surgery with mesh to correct vaginal apical prolapse is associated with a higher rate of complication requiring reoperation and reoperation for any reason compared to traditional vaginal surgery or sacral colpopexy. Abdominal POP surgery using mesh (sacral colpopexy) appears to result in lower rates of mesh complications compared to transvaginal POP surgery with mesh, with the median vaginal mesh erosion rate reported at 4 percent within 23 months of surgery. Effectiveness The literature review found that while transvaginal POP repair with mesh often restores anatomy, it has not been shown to improve clinical benefit over traditional non-mesh repair, as evidenced by the following key findings: Transvaginal apical or posterior repair with mesh does not appear to provide any added benefit compared to traditional surgery without mesh. Effectiveness cont d There does appear to be an anatomic benefit to anterior repair with mesh augmentation. This anatomic benefit may not result in superior symptomatic outcomes or lower rates of repeat surgery for recurrent prolapse compared to traditional POP repair without mesh. Patients who undergo traditional POP repair without mesh have equivalent improvement in quality of life when compared to patients who undergo transvaginal POP repair with mesh. Effectiveness cont d Compared to traditional vaginal surgery without mesh, abdominal apical prolapse repair with mesh (sacral colpopexy) results in less recurrent prolapse, p although it has not been shown to reduce the rate of repeat surgery for recurrent prolapse. Recommendations for Health Care Providers The FDA encourages health care providers to: Recognize that in most cases, POP can be treated successfully without mesh thus avoiding the risk of mesh-related complications. Choose mesh surgery only after weighing the risks ik and db benefits of surgery with mesh versus all surgery and non-surgical alternatives. 10


11 Recommendations for Health Care Providers cont d Consider these factors before placing surgical mesh: Surgical mesh is a permanent implant that may make future surgical repair more challenging. A mesh procedure may put the patient at risk for requiring additional surgery or for the development of new complications Removal of mesh due to mesh complications may involve multiple surgeries and significantly impair the patient s quality of life. Complete removal of mesh may not be possible and may not result in complete resolution of complications, including pain. Mesh placed abdominally for POP repair may result in lower rates of mesh complications compared to transvaginal POP surgery with mesh. The past: That which will not tell us what we ought to do what we ought to avoid. -José Ortega y Gossett Lesson 1 PARATUS SEMPER DISCERE ALWAYS PREPARED TO LEARN! Learning is by nature curiosity prying into everything, reluctant to leave anything, material or immaterial unexplained. Philo of Alexandria 11









12 I am glad of all the details, whether they seem to you to be relevant or not. By a man s finger-nails, nails, by his coat- sleeve, by his boots, by his trouser- knees, by the callosities of his forefinger and thumb, by his expression, by his shirt-cuffs by each of these things a man s calling is plainly revealed. ea ed That all united should fail to enlighten the competent inquirer in any case is almost inconceivable. -From A Study in Scarlet Lesson 2 The fundamentals of surgical repair of any hernia are to reduce it and maintain its reduction by supporting structures. Williams GA, Richardson AC. Am J Obst & Gynec, September, 1952; Vol 64, Number 3, pages Lesson 3 The eyes can t see what the mind don t (sic) know! 12






13 Lesson 4 Careful examination and evaluation of patients prior to operative procedures cannot be too strongly gy stressed. Define Normal Lesson 5 Sites to be described Conditions of examination Williams GA, Richardson AC. Am J Obst & Gynec, September, 1952; Vol 64, Number 3, pages Requirements for Improvement Define Normal Sites to be described Conditions of examination 13








14 Goals Assessment of specific sites Description of support loss with maximum stress Anatomic abnormalities contributing to support loss Reproducible Understandable Usable Improves patient care Staging Oncology Clinical Surgical Infertility Surgical 14







15 Normal Physical Exam Genital hiatus Closed Urethral meatus parallel to the floor no evidence of urethral prolapse/caruncle Anterior compartment Cervix/Cuff Posterior compartment Neuromuscular assessment of pelvic floor Gynecologic pelvimetry Normal Pelvic Exam 15









16 Cuff and uterosacral ligaments Gynecologic pelvimetry Abnormal Pelvic Exam At Rest Straining Open genital hiatus Lesson 6 Anterior Compartment Defects Transverse Cystocele Am J Obstet Gynecol 2002, 187:
17 Anterior Compartment & Apical Defect Post Hysterectomy Cuff Prolapse Posterior Compartment Defects Posterior Compartment and Apical Defects Perineal Descent Rectal Prolapse 17







18 Lesson 7 The treatment of prolapse of the vagina following a hysterectomy is demanding of the resourcefulness of the surgeon. Lesson 8 In spite of careful preoperative examination and meticulous surgery there will be a certain number of failures. Williams GA, Richardson AC. Am J Obst & Gynec, September, 1952; Vol 64, Number 3, pages Williams GA, Richardson AC. Am J Obst & Gynec, September, 1952; Vol 64, Number 3, pages It is one of those instances where the reasoner can produce an effect which seems remarkable to his neighbor because the latter has missed the one little point which is the basis for the deduction. 18

 e t) Marshall-Marchetti-Krantz a Marchettia a t")
 (Retropubic or vaginal reattachment) Superior Reattachment to cervix or cuff Defect: Midline Posterior Segment Repair: Posterior colporrhaphy")

19 Superior Segment (Supra vaginal defects) Cardinal- Uterosacral Ligament Complex Defect: Repair: Uterosacral Ligament U-S ligament plication/suspension Sacral fixation U-S Cardinal Ligament Shortening U/S-cardinal ligaments Complex Sacrospinous fixation Sacrocolpopexy Cul-de-sac Excision sac and cerclage Uterosacral ligament plication Puborectalis plication/ interposition Anterior Segment - Urethra, Bladder Defects Defect: Repair: Midline Anterior colporrhaphy Excision urethral diverticulum Para urethral Retropubic suspensions (Lateral a detachment) e t) Marshall-Marchetti-Krantz a Marchettia a t Burch Paravaginal (Lateral Vaginal Wall) Combined Needle suspensions (Pereyra, Stamey, Raz) Sling procedures Para vesicle Paravaginal repair (Lateral detachment) (Retropubic or vaginal reattachment) Superior Reattachment to cervix or cuff Defect: Midline Posterior Segment Repair: Posterior colporrhaphy Lateral detachment t Pararectal reattachment t Superior PERINEAL DEFECTS: Anal sphincter laceration Reattachment to cuff Perineorrhaphy Sphincteroplasty Lesson 9 Surgical Techniques for Pelvic Support Defects Must be Individualized Depending on the Patient s Expectations Support defects Functional status of urethra, bladder, bowel, and vagina 19





20 Lesson 10 Surgical techniques for pelvic support defects must be individualized depending on the surgeon s skills PARATUS SEMPER DOCERE ALWAYS PREPARED TO TEACH! Lesson 11 Personalized care of the surgical patient by nurse and doctor Richardson AC, Graham EE Am J Obstet Gynecol, Vol 115, Issue 7, pp 962-5, 1973 Lesson 12 Lesson 13 Patients are eager to find a friendly face when they enter the operating room. Richardson AC, Graham EE Am J Obstet Gynecol, Vol 115, Issue 7, pp 962-5, 1973 Mentor and Friend 20
Traditional Anterior, Posterior, and Apical Compartment Repairs A Technique Based Review
 Traditional Anterior, Posterior, and Apical Compartment Repairs A Technique Based Review Sandip Vasavada, MD Center for Female Urology and Pelvic Reconstructive Surgery The Glickman Urological and Kidney
Traditional Anterior, Posterior, and Apical Compartment Repairs A Technique Based Review Sandip Vasavada, MD Center for Female Urology and Pelvic Reconstructive Surgery The Glickman Urological and Kidney
Surgical repair of vaginal wall prolapse using mesh
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Interventional procedure consultation document Surgical repair of vaginal wall prolapse using mesh Vaginal wall prolapse happens when the normal support
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Interventional procedure consultation document Surgical repair of vaginal wall prolapse using mesh Vaginal wall prolapse happens when the normal support
International Federation of Gynecology and Obstetrics
 International Federation of Gynecology and Obstetrics COMMITTEE FOR UROGYNAECOLOGY AND PELVIC FLOOR MEMBER: TSUNG-HSIEN (CHARLES) SU, CHAIR (TAIWAN) DAVID RICHMOND, CO-CHAIR (UK) CHITTARANJAN PURANDARE,
International Federation of Gynecology and Obstetrics COMMITTEE FOR UROGYNAECOLOGY AND PELVIC FLOOR MEMBER: TSUNG-HSIEN (CHARLES) SU, CHAIR (TAIWAN) DAVID RICHMOND, CO-CHAIR (UK) CHITTARANJAN PURANDARE,
LAPAROSCOPIC REPAIR OF PELVIC FLOOR
 LAPAROSCOPIC REPAIR OF PELVIC FLOOR Dr. R. K. Mishra Elements comprising the Pelvis Bones Ilium, ischium and pubis fusion Ligaments Muscles Obturator internis muscle Arcus tendineus levator ani or white
LAPAROSCOPIC REPAIR OF PELVIC FLOOR Dr. R. K. Mishra Elements comprising the Pelvis Bones Ilium, ischium and pubis fusion Ligaments Muscles Obturator internis muscle Arcus tendineus levator ani or white
FDA & Transvaginal Mesh: What Happened? What s Next?
 FDA & Transvaginal Mesh: What Happened? What s Next? Matthew D. Barber, MD MHS Professor & Vice Chair for Clinical Research Obstetrics Gynecology & Women s Health Institute Disclosures I receive no grants,
FDA & Transvaginal Mesh: What Happened? What s Next? Matthew D. Barber, MD MHS Professor & Vice Chair for Clinical Research Obstetrics Gynecology & Women s Health Institute Disclosures I receive no grants,
What are we talking about? Symptoms. Prolapse Risk Factors. Vaginal bulge 1 Splinting. ?? Pelvic pressure Back pain 1 Urinary complaints 2
 Options for Vaginal Prolapse What are we talking about? Michelle Y. Morrill, M.D. Director of Urogynecology The Permanente Medical Group Kaiser, San Francisco Assistant Professor, Volunteer Faculty Department
Options for Vaginal Prolapse What are we talking about? Michelle Y. Morrill, M.D. Director of Urogynecology The Permanente Medical Group Kaiser, San Francisco Assistant Professor, Volunteer Faculty Department
Karanvir Virk M.D. Minimally Invasive & Pelvic Reconstructive Surgery 01/28/2015
 Karanvir Virk M.D. Minimally Invasive & Pelvic Reconstructive Surgery 01/28/2015 Disclosures I have none Objectives Identify the basic Anatomy and causes of Pelvic Organ Prolapse Examine office diagnosis
Karanvir Virk M.D. Minimally Invasive & Pelvic Reconstructive Surgery 01/28/2015 Disclosures I have none Objectives Identify the basic Anatomy and causes of Pelvic Organ Prolapse Examine office diagnosis
PRACTICE BULLETIN Female Pelvic Medicine & Reconstructive Surgery Volume 23, Number 4, July/August 2017
 PRACTICE BULLETIN Number 176, April 2017 (Replaces Committee Opinion Number 513, December 2011) Pelvic Organ Prolapse Pelvic organ prolapse (POP) is a common, benign condition in women. For many women
PRACTICE BULLETIN Number 176, April 2017 (Replaces Committee Opinion Number 513, December 2011) Pelvic Organ Prolapse Pelvic organ prolapse (POP) is a common, benign condition in women. For many women
Stephen T Jeffery. University of Cape Town, South Africa
 Stephen T Jeffery University of Cape Town, South Africa I still think there s a role for mesh in Prolapse surgery Examples of my most recent mesh cases Case 1 62 yr old Sacrocolpopexy for vault prolapse
Stephen T Jeffery University of Cape Town, South Africa I still think there s a role for mesh in Prolapse surgery Examples of my most recent mesh cases Case 1 62 yr old Sacrocolpopexy for vault prolapse
Current status in pelvic organ prolapse surgery: an evidence based review
 Current status in pelvic organ prolapse surgery: an evidence based review Christian Falconer, MD, PhD Department of Obstetrics and Gynecology Danderyd University Hospital Stockholm, Sweden Finnish Society
Current status in pelvic organ prolapse surgery: an evidence based review Christian Falconer, MD, PhD Department of Obstetrics and Gynecology Danderyd University Hospital Stockholm, Sweden Finnish Society
Interventional procedures guidance Published: 28 June 2017 nice.org.uk/guidance/ipg583
 Sacrocolpopexy using mesh to repair vaginal vault prolapse Interventional procedures guidance Published: 28 June 2017 nice.org.uk/guidance/ipg583 Your responsibility This guidance represents the view of
Sacrocolpopexy using mesh to repair vaginal vault prolapse Interventional procedures guidance Published: 28 June 2017 nice.org.uk/guidance/ipg583 Your responsibility This guidance represents the view of
Gynecology Dr. Sallama Lecture 3 Genital Prolapse
 Gynecology Dr. Sallama Lecture 3 Genital Prolapse Genital(utero-vaginal )prolapse is extremely common, with an estimated 11% of women undergoing at least one operation for this condition. Definition: A
Gynecology Dr. Sallama Lecture 3 Genital Prolapse Genital(utero-vaginal )prolapse is extremely common, with an estimated 11% of women undergoing at least one operation for this condition. Definition: A
Recent advances in POP. Dr. Bernhard Uhl Department for Obstetrics and Gynecology St. Vinzenz-Hospital Dinslaken Germany
 Recent advances in POP Dr. Bernhard Uhl Department for Obstetrics and Gynecology St. Vinzenz-Hospital Dinslaken Germany Level of pelvic floor support Level I apical Level II transverse/ horizontal Level
Recent advances in POP Dr. Bernhard Uhl Department for Obstetrics and Gynecology St. Vinzenz-Hospital Dinslaken Germany Level of pelvic floor support Level I apical Level II transverse/ horizontal Level
Clinical Curriculum: Urogynecology
 Updated July 201 Clinical Curriculum: Urogynecology GOAL: The primary goal of the Urogynecology rotation at the University of Alabama at Birmingham (UAB) is to train physicians to have a broad knowledge
Updated July 201 Clinical Curriculum: Urogynecology GOAL: The primary goal of the Urogynecology rotation at the University of Alabama at Birmingham (UAB) is to train physicians to have a broad knowledge
Stop Coping. Start Living. Talk to your doctor about pelvic organ prolapse and sacrocolpopexy
 Stop Coping. Start Living Talk to your doctor about pelvic organ prolapse and sacrocolpopexy Did you know? One in three women will suffer from a pelvic health condition in her lifetime. Four of the most
Stop Coping. Start Living Talk to your doctor about pelvic organ prolapse and sacrocolpopexy Did you know? One in three women will suffer from a pelvic health condition in her lifetime. Four of the most
Introduction. Regarding the Section of the UPDATE Entitled Purpose
 Time to Rethink: an Evidence-Based Response from Pelvic Surgeons to the FDA Safety Communication: UPDATE on Serious Complications Associated with Transvaginal Placement of Surgical Mesh for Pelvic Organ
Time to Rethink: an Evidence-Based Response from Pelvic Surgeons to the FDA Safety Communication: UPDATE on Serious Complications Associated with Transvaginal Placement of Surgical Mesh for Pelvic Organ
Polypropylene vaginal mesh implants for vaginal prolapse
 Polypropylene vaginal mesh implants for vaginal prolapse This statement has been developed and reviewed by the Women s Health Committee and approved by the RANZCOG Board and Council. A list of Women s
Polypropylene vaginal mesh implants for vaginal prolapse This statement has been developed and reviewed by the Women s Health Committee and approved by the RANZCOG Board and Council. A list of Women s
FDA and Mesh Complications in Vaginal Surgery
 FDA and Mesh Complications in Vaginal Surgery Response to FDA Safety Communication dated July 13, 2011 To Our Patients and Women of the Community: As many of you are aware, on July 13, 2011, the FDA released
FDA and Mesh Complications in Vaginal Surgery Response to FDA Safety Communication dated July 13, 2011 To Our Patients and Women of the Community: As many of you are aware, on July 13, 2011, the FDA released
Prolapse & Stress Incontinence
 Advanced Pelvic Floor Course Prolapse & Stress Incontinence OVERVIEW Day One and morning of Day Two- Pelvic Organ Prolapse The Prolapse component covers the detailed anatomy of POP including the DeLancey
Advanced Pelvic Floor Course Prolapse & Stress Incontinence OVERVIEW Day One and morning of Day Two- Pelvic Organ Prolapse The Prolapse component covers the detailed anatomy of POP including the DeLancey
Surgery for stress incontinence:
 Surgery for stress incontinence: information for you aashara Published February 2005 by the RCOG Contents Key points About this information What is stress incontinence? Do I need an operation? What operation
Surgery for stress incontinence: information for you aashara Published February 2005 by the RCOG Contents Key points About this information What is stress incontinence? Do I need an operation? What operation
Avoiding Mesh Disasters: Tips and Tricks for Success and Handling Complications
 Avoiding Mesh Disasters: Tips and Tricks for Success and Handling Complications Karyn S. Eilber, M.D. Cedars-Sinai FPMRS Associate Professor, Cedars-Sinai Dept of Surgery Associate Director, Urology Residency
Avoiding Mesh Disasters: Tips and Tricks for Success and Handling Complications Karyn S. Eilber, M.D. Cedars-Sinai FPMRS Associate Professor, Cedars-Sinai Dept of Surgery Associate Director, Urology Residency
By:Dr:ISHRAQ MOHAMMED
 By:Dr:ISHRAQ MOHAMMED Protrusion of an organ or structure beyond its normal confines. Prolapses are classified according to their location and the organs contained within them. 1-Anterior vaginal wall
By:Dr:ISHRAQ MOHAMMED Protrusion of an organ or structure beyond its normal confines. Prolapses are classified according to their location and the organs contained within them. 1-Anterior vaginal wall
Bard: Continence Therapy. Stress Urinary Incontinence. Regaining Control. Restoring Your Lifestyle.
 Bard: Continence Therapy Stress Urinary Incontinence Regaining Control. Restoring Your Lifestyle. Stress Urinary Incontinence Urinary incontinence is a common problem and one that can be resolved by working
Bard: Continence Therapy Stress Urinary Incontinence Regaining Control. Restoring Your Lifestyle. Stress Urinary Incontinence Urinary incontinence is a common problem and one that can be resolved by working
Pelvic Prolapse. A Patient Guide to Pelvic Floor Reconstruction
 Pelvic Prolapse A Patient Guide to Pelvic Floor Reconstruction Pelvic Prolapse When an organ becomes displaced, or slips down in the body, it is referred to as a prolapse. Your physician has diagnosed
Pelvic Prolapse A Patient Guide to Pelvic Floor Reconstruction Pelvic Prolapse When an organ becomes displaced, or slips down in the body, it is referred to as a prolapse. Your physician has diagnosed
Dr John Short. Obstetrician and Gynaecologist Christchurch Women s Hospital, Oxford Women's Health, Christchurch
 Dr John Short Obstetrician and Gynaecologist Christchurch Women s Hospital, Oxford Women's Health, Christchurch 8:30-9:25 WS #142: Peeling Back the Layers - The Pelvic Floor Uncovered 9:35-10:30 WS #152:
Dr John Short Obstetrician and Gynaecologist Christchurch Women s Hospital, Oxford Women's Health, Christchurch 8:30-9:25 WS #142: Peeling Back the Layers - The Pelvic Floor Uncovered 9:35-10:30 WS #152:
12/1/13. What are Pelvic Floor Disorders? What is the Pelvic Floor? Facts. Prevalence of Urinary InconOnence. What s New in Pelvic Floor Disorders?
 What are Pelvic Floor Disorders? Urinary Control Problems - InconOnence or leakage of urine Prolapse of pelvic organs - Vagina, bladder, rectum What s New in Pelvic Floor Disorders? Kimberly Kenton MD,
What are Pelvic Floor Disorders? Urinary Control Problems - InconOnence or leakage of urine Prolapse of pelvic organs - Vagina, bladder, rectum What s New in Pelvic Floor Disorders? Kimberly Kenton MD,
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal mesh background of, 84 85 Age as factor in PFDs, 8 Anal plugs in FI management in women, 107 Anterior compartment native tissue
Index Note: Page numbers of article titles are in boldface type. A Abdominal mesh background of, 84 85 Age as factor in PFDs, 8 Anal plugs in FI management in women, 107 Anterior compartment native tissue
Does trocar-guided tension-free vaginal mesh (Prolift ) repair provoke prolapse of the unaffected compartments?
 repair provoke prolapse of the unaffected compartments?") Int Urogynecol J (2010) 21:271 278 DOI 10.1007/s00192-009-1028-1 ORIGINAL ARTICLE Does trocar-guided tension-free vaginal mesh (Prolift ) repair provoke prolapse of the unaffected compartments? Mariëlla
Int Urogynecol J (2010) 21:271 278 DOI 10.1007/s00192-009-1028-1 ORIGINAL ARTICLE Does trocar-guided tension-free vaginal mesh (Prolift ) repair provoke prolapse of the unaffected compartments? Mariëlla
MIDLAND MEMORIAL HOSPITAL Delineation of Privileges FEMALE PELVIC MEDICINE AND RECONSTRUCTIVE SURGERY (UROGYNECOLOGY)
") MIDLAND MEMORIAL HOSPITAL Delineation of Privileges FEMALE PELVIC MEDICINE AND RECONSTRUCTIVE SURGERY (UROGYNECOLOGY) Physician Name: Your home for healthcare Female Pelvic Medicine and Reconstructive
MIDLAND MEMORIAL HOSPITAL Delineation of Privileges FEMALE PELVIC MEDICINE AND RECONSTRUCTIVE SURGERY (UROGYNECOLOGY) Physician Name: Your home for healthcare Female Pelvic Medicine and Reconstructive
A PATIENT GUIDE TO Understanding Stress Urinary Incontinence
 A PATIENT GUIDE TO Understanding Stress Urinary Incontinence Q: What is SUI? A: Stress urinary incontinence is defined as the involuntary leakage of urine. The problem afflicts approximately 18 million
A PATIENT GUIDE TO Understanding Stress Urinary Incontinence Q: What is SUI? A: Stress urinary incontinence is defined as the involuntary leakage of urine. The problem afflicts approximately 18 million
Understanding Pelvic Organ Prolapse. Stephanie Pickett, MD, MS Female Pelvic Medicine and Reconstructive Surgery
 Understanding Pelvic Organ Prolapse Stephanie Pickett, MD, MS Female Pelvic Medicine and Reconstructive Surgery Disclosures None I am the daughter of a physician assistant. Objectives List types of pelvic
Understanding Pelvic Organ Prolapse Stephanie Pickett, MD, MS Female Pelvic Medicine and Reconstructive Surgery Disclosures None I am the daughter of a physician assistant. Objectives List types of pelvic
Infracoccygeal sacropexy using mesh for uterine prolapse repair
 Infracoccygeal sacropexy using mesh for uterine Issued: January 2009 www.nice.org.uk/ipg280 NHS Evidence has accredited the process used by the NICE Interventional Procedures Programme to produce interventional
Infracoccygeal sacropexy using mesh for uterine Issued: January 2009 www.nice.org.uk/ipg280 NHS Evidence has accredited the process used by the NICE Interventional Procedures Programme to produce interventional
Pelvic Floor. Reimbursement & Coding Guide
 Pelvic Floor Reimbursement & Coding Guide Pelvic Floor Reimbursement and Coding Guide ACell Pelvic Floor Matrix products are biologically-derived devices comprised of porcine Urinary Bladder Matrix (UBM),
Pelvic Floor Reimbursement & Coding Guide Pelvic Floor Reimbursement and Coding Guide ACell Pelvic Floor Matrix products are biologically-derived devices comprised of porcine Urinary Bladder Matrix (UBM),
Robotic-Assisted Surgery in Urogynecology: Beyond Sacrocolpopexy
 Robotic-Assisted Surgery in Urogynecology: Beyond Sacrocolpopexy Marie Fidela R. Paraiso, M.D. Professor of Surgery Section Head, Urogynecology and Reconstructive Pelvic Surgery Cleveland, OH Disclosures
Robotic-Assisted Surgery in Urogynecology: Beyond Sacrocolpopexy Marie Fidela R. Paraiso, M.D. Professor of Surgery Section Head, Urogynecology and Reconstructive Pelvic Surgery Cleveland, OH Disclosures
Prediction and prevention of stress urinary incontinence after prolapse surgery van der Ploeg, J.M.
 UvA-DARE (Digital Academic Repository) Prediction and prevention of stress urinary incontinence after prolapse surgery van der Ploeg, J.M. Link to publication Citation for published version (APA): van
UvA-DARE (Digital Academic Repository) Prediction and prevention of stress urinary incontinence after prolapse surgery van der Ploeg, J.M. Link to publication Citation for published version (APA): van
We welcome comments and corrections which will be used to improve the system annually.
 ACGME Case Log Instructions: Female Pelvic Medicine and Reconstructive Surgery (FPMRS) Review Committees for Obstetrics and Gynecology, and Urology Updated July 2013 BACKGROUND The ACGME Case Log System
ACGME Case Log Instructions: Female Pelvic Medicine and Reconstructive Surgery (FPMRS) Review Committees for Obstetrics and Gynecology, and Urology Updated July 2013 BACKGROUND The ACGME Case Log System
This information is intended as an overview only
 This information is intended as an overview only Please refer to the INSTRUCTIONS FOR USE included with this device for indications, contraindications, warnings, precautions and other important information
This information is intended as an overview only Please refer to the INSTRUCTIONS FOR USE included with this device for indications, contraindications, warnings, precautions and other important information
T h e C o m p l e t e Tr e a t m e n t o f P e l v i c F l o o r P r o l a p s e by Laparoscopy Technique, Tips and Tricks
 T h e C o m p l e t e Tr e a t m e n t o f P e l v i c F l o o r P r o l a p s e by Laparoscopy Technique, Tips and Tricks R Botchorishvili, A Wattiez, G Mage, M Canis, B Rabischong, K Jardon, C Rivoire,
T h e C o m p l e t e Tr e a t m e n t o f P e l v i c F l o o r P r o l a p s e by Laparoscopy Technique, Tips and Tricks R Botchorishvili, A Wattiez, G Mage, M Canis, B Rabischong, K Jardon, C Rivoire,
PL Narducci Department of Obstetrics and Gynecology General Hospital San Giovanni Battista Foligno, ITALY
 NESA DAYS 2018 New European Surgical Academy Perugia, April 19-21, 2018 EXCELLENCE IN FEMALE SURGERY PROLAPSE RECONSTRUCTIVE SURGERY IN SEXUALLY ACTIVE WOMEN LAPAROSCOPIC ANTERIOR ABDOMINAL WALL COLPOPEXY
NESA DAYS 2018 New European Surgical Academy Perugia, April 19-21, 2018 EXCELLENCE IN FEMALE SURGERY PROLAPSE RECONSTRUCTIVE SURGERY IN SEXUALLY ACTIVE WOMEN LAPAROSCOPIC ANTERIOR ABDOMINAL WALL COLPOPEXY
Imaging of Pelvic Floor Weakness. Dr Susan Kouloyan-Ilic Radiologist Epworth Medical Imaging The Women s, Melbourne
 Imaging of Pelvic Floor Weakness Dr Susan Kouloyan-Ilic Radiologist Epworth Medical Imaging The Women s, Melbourne Outline Overview and Epidemiology Risk Factors, Causes and Results Review of Relevant
Imaging of Pelvic Floor Weakness Dr Susan Kouloyan-Ilic Radiologist Epworth Medical Imaging The Women s, Melbourne Outline Overview and Epidemiology Risk Factors, Causes and Results Review of Relevant
Desara TV and Desara Blue TV
 Desara TV and Desara Blue TV Sling for Female Stress Urinary Incontinence Instructions For Use D I Prescription Use only Do not reuse Sterilized using ethylene oxide Available Electronically M Manufactured
Desara TV and Desara Blue TV Sling for Female Stress Urinary Incontinence Instructions For Use D I Prescription Use only Do not reuse Sterilized using ethylene oxide Available Electronically M Manufactured
INTERNATIONAL UROGYNAECOLOGICAL ASSOCIATION (IUGA) JOINT REPORT ON THE TERMINOLOGY FOR SURGICAL PROCEDURES TO
 JOINT REPORT ON THE TERMINOLOGY FOR SURGICAL PROCEDURES TO") AN AMERICAN UROGYNECOLOGIC SOCIETY (AUGS) / INTERNATIONAL UROGYNAECOLOGICAL ASSOCIATION (IUGA) JOINT REPORT ON THE TERMINOLOGY FOR SURGICAL PROCEDURES TO TREAT PELVIC ORGAN PROLAPSE NEED FOR A WORKING
AN AMERICAN UROGYNECOLOGIC SOCIETY (AUGS) / INTERNATIONAL UROGYNAECOLOGICAL ASSOCIATION (IUGA) JOINT REPORT ON THE TERMINOLOGY FOR SURGICAL PROCEDURES TO TREAT PELVIC ORGAN PROLAPSE NEED FOR A WORKING
q7:480499_P0 6/5/09 10:23 AM Page 1 WHAT YOU SHOULD KNOW ABOUT YOUR DIAGNOSIS OF STRESS URINARY INCONTINENCE
 493495.q7:480499_P0 6/5/09 10:23 AM Page 1 WHAT YOU SHOULD KNOW ABOUT YOUR DIAGNOSIS OF STRESS URINARY INCONTINENCE 493495.q7:480499_P0 6/5/09 10:23 AM Page 2 What is Stress Urinary Incontinence? Urinary
493495.q7:480499_P0 6/5/09 10:23 AM Page 1 WHAT YOU SHOULD KNOW ABOUT YOUR DIAGNOSIS OF STRESS URINARY INCONTINENCE 493495.q7:480499_P0 6/5/09 10:23 AM Page 2 What is Stress Urinary Incontinence? Urinary
Pelvic Health Coding & Payment Quick Reference
 Payer policies will vary and should be verified prior to treatment for limitations on diagnosis, coding or site of service requirements. The coding options listed within this guide are commonly used codes
Payer policies will vary and should be verified prior to treatment for limitations on diagnosis, coding or site of service requirements. The coding options listed within this guide are commonly used codes
Long-Term Effectiveness of Uterosacral Colpopexy and Minimally Invasive Sacral Colpopexy for Treatment of Pelvic Organ Prolapse
 ORIGINAL ARTICLE Long-Term Effectiveness of Uterosacral Colpopexy and Minimally Invasive Sacral Colpopexy for Treatment of Pelvic Organ Prolapse Cecile A. Unger, MD, MPH, Matthew D. Barber, MD, MHS, Mark
ORIGINAL ARTICLE Long-Term Effectiveness of Uterosacral Colpopexy and Minimally Invasive Sacral Colpopexy for Treatment of Pelvic Organ Prolapse Cecile A. Unger, MD, MPH, Matthew D. Barber, MD, MHS, Mark
Options for Vaginal Prolapse. What is prolapse? What is prolapse? Disclosures 10/23/2013. Michelle Y. Morrill, M.D. None
 Options for Vaginal Prolapse Disclosures None Michelle Y. Morrill, M.D. Director of Urogynecology Kaiser, San Francisco Assistant Professor, Volunteer Faculty Department of Ob/Gyn, UCSF What is prolapse?
Options for Vaginal Prolapse Disclosures None Michelle Y. Morrill, M.D. Director of Urogynecology Kaiser, San Francisco Assistant Professor, Volunteer Faculty Department of Ob/Gyn, UCSF What is prolapse?
EndoFast Reliant System vs. Tension- free Mesh in a Sheep Model; three arm Comparative Study Assessing the Mechanical Pullout Force of Mesh Over Time
 EndoFast Reliant System vs. Tension- free Mesh in a Sheep Model; three arm Comparative Study Assessing the Mechanical Pullout Force of Mesh Over Time Menachem Alcalay,M.D, Urogynecology unit, Sheba Medical
EndoFast Reliant System vs. Tension- free Mesh in a Sheep Model; three arm Comparative Study Assessing the Mechanical Pullout Force of Mesh Over Time Menachem Alcalay,M.D, Urogynecology unit, Sheba Medical
Gökmen Sukgen, 1 Esra SaygJlJ YJlmaz, 2 and Eralp BaGer Introduction. 2. Case Presentation
 Case Reports in Obstetrics and Gynecology Volume 2016, Article ID 2906596, 4 pages http://dx.doi.org/10.1155/2016/2906596 Case Report Vaginal Hysterectomy with Anterior Four-Arm Mesh Implant Technique
Case Reports in Obstetrics and Gynecology Volume 2016, Article ID 2906596, 4 pages http://dx.doi.org/10.1155/2016/2906596 Case Report Vaginal Hysterectomy with Anterior Four-Arm Mesh Implant Technique
SURGICAL. How to manage the cuff at vaginal hysterectomy. For personal use only. Copyright Dowden Health Media TECHNIQUES
 For mass reproduction, content licensing and permissions contact Dowden Health Media. How to manage the cuff at vaginal hysterectomy The high McCall culdoplasty and its modifications can prevent apical
For mass reproduction, content licensing and permissions contact Dowden Health Media. How to manage the cuff at vaginal hysterectomy The high McCall culdoplasty and its modifications can prevent apical
Female Urology. The Results of Grade IV Cystocele Repair Using Mesh. Introduction ZARGAR MA, EMAMI M*, ZARGAR K, JAMSHIDI M
 Urology Journal UNRC/IUA Vol. 1, No. 4, 263-267 Autumn 2004 Printed in IRAN Female Urology The Results of Grade IV Cystocele Repair Using Mesh ZARGAR MA, EMAMI M*, ZARGAR K, JAMSHIDI M Department of Urology,
Urology Journal UNRC/IUA Vol. 1, No. 4, 263-267 Autumn 2004 Printed in IRAN Female Urology The Results of Grade IV Cystocele Repair Using Mesh ZARGAR MA, EMAMI M*, ZARGAR K, JAMSHIDI M Department of Urology,
Consultation Guide: Specialised gynaecology surgery and complex urogynaecology conditions service specifications
 Consultation Guide: Specialised gynaecology surgery and complex urogynaecology conditions service specifications Consultation guide: Specialised gynaecology surgery and complex urogynaecology conditions
Consultation Guide: Specialised gynaecology surgery and complex urogynaecology conditions service specifications Consultation guide: Specialised gynaecology surgery and complex urogynaecology conditions
2012/13 NHS STANDARD CONTRACT FOR ACUTE, AMBULANCE, COMMUNITY AND MENTAL HEALTH AND LEARNING DISABILITY SERVICES (MULTILATERAL)
") E10d 2012/13 NHS STANDARD CONTRACT FOR ACUTE, AMBULANCE, COMMUNITY AND MENTAL HEALTH AND LEARNING DISABILITY SERVICES (MULTILATERAL) SECTION B PART 1 - SERVICE SPECIFICATIONS Service Specification No.
E10d 2012/13 NHS STANDARD CONTRACT FOR ACUTE, AMBULANCE, COMMUNITY AND MENTAL HEALTH AND LEARNING DISABILITY SERVICES (MULTILATERAL) SECTION B PART 1 - SERVICE SPECIFICATIONS Service Specification No.
1) What conditions is vaginal mesh used to commonly treat? Vaginal mesh is used to treat two different health issues in women:
 What conditions is vaginal mesh used to commonly treat? Vaginal mesh is used to treat two different health issues in women:") Vaginal Mesh Frequently Asked Questions 1) What conditions is vaginal mesh used to commonly treat? Vaginal mesh is used to treat two different health issues in women: a) stress urinary incontinence (SUI)
Vaginal Mesh Frequently Asked Questions 1) What conditions is vaginal mesh used to commonly treat? Vaginal mesh is used to treat two different health issues in women: a) stress urinary incontinence (SUI)
The UK National Prolapse Survey: 10 years on
 Int Urogynecol J (2018) 29:795 801 DOI 10.1007/s00192-017-3476-3 ORIGINAL ARTICLE The UK National Prolapse Survey: 10 years on Swati Jha 1 & Alfred Cutner 2 & Paul Moran 3 Received: 28 June 2017 /Accepted:
Int Urogynecol J (2018) 29:795 801 DOI 10.1007/s00192-017-3476-3 ORIGINAL ARTICLE The UK National Prolapse Survey: 10 years on Swati Jha 1 & Alfred Cutner 2 & Paul Moran 3 Received: 28 June 2017 /Accepted:
9/24/2015. Pelvic Floor Disorders. Agenda. What is the Pelvic Floor? Pelvic Floor Problems
 Management of Pelvic Floor Disorders Doctor, I don t want THAT mesh! Agenda What are pelvic floor disorders (PFDs)? What are the treatment options? Expectant. Conservative. Surgical. How and when are grafts
Management of Pelvic Floor Disorders Doctor, I don t want THAT mesh! Agenda What are pelvic floor disorders (PFDs)? What are the treatment options? Expectant. Conservative. Surgical. How and when are grafts
Women s Health. Product innovation. Commitment. We are committed to you... and advancing the quality of your patient care.
 II Commitment We are committed to you... and advancing the quality of your patient care. Boston Scientific is always there for you, your physicians and your patients. We are anchored in our guiding principle
II Commitment We are committed to you... and advancing the quality of your patient care. Boston Scientific is always there for you, your physicians and your patients. We are anchored in our guiding principle
Innovations in mesh kit technology for vaginal wall prolapse
 Available at www.obgmanagement.com s u p p l e m e n t t o This supplement is supported by American Medical Systems, Inc., and has been peer reviewed by the editors of OBG Management. J a n u a r y 2 0
Available at www.obgmanagement.com s u p p l e m e n t t o This supplement is supported by American Medical Systems, Inc., and has been peer reviewed by the editors of OBG Management. J a n u a r y 2 0
Protective effect of suburethral slings on postoperative cystocele recurrence after reconstructive pelvic operation
 Protective effect of suburethral slings on postoperative cystocele recurrence after reconstructive pelvic operation Roger P. Goldberg, MD, MPH, Sumana Koduri, MD, Robert W. Lobel, MD, Patrick J. Culligan,
Protective effect of suburethral slings on postoperative cystocele recurrence after reconstructive pelvic operation Roger P. Goldberg, MD, MPH, Sumana Koduri, MD, Robert W. Lobel, MD, Patrick J. Culligan,
CHAU KHAC TU M.D., Ph.D.
 CHAU KHAC TU M.D., Ph.D. Hue Central Hospital Vietnam LAPAROSCOPIC PROMONTOFIXATION FOR THE GENITAL PROLAPSE TREATMENT Chau Khac Tu MD.PhD. Hue central hospital CONTENT 3 1 INTRODUCTION 2 OBJECTIVE AND
CHAU KHAC TU M.D., Ph.D. Hue Central Hospital Vietnam LAPAROSCOPIC PROMONTOFIXATION FOR THE GENITAL PROLAPSE TREATMENT Chau Khac Tu MD.PhD. Hue central hospital CONTENT 3 1 INTRODUCTION 2 OBJECTIVE AND
Medical Review Criteria Invasive Treatment for Urinary Incontinence
 Medical Review Criteria Invasive Treatment for Urinary Incontinence Effective Date: December 21, 2016 Subject: Invasive Treatment for Urinary Incontinence Background: Urinary incontinence (the involuntary
Medical Review Criteria Invasive Treatment for Urinary Incontinence Effective Date: December 21, 2016 Subject: Invasive Treatment for Urinary Incontinence Background: Urinary incontinence (the involuntary
Randomized trial of fascia lata and polypropylene mesh for abdominal sacrocolpopexy: 5-year follow-up
 DOI 10.1007/s00192-010-1249-3 ORIGINAL ARTICLE Randomized trial of fascia lata and polypropylene mesh for abdominal sacrocolpopexy: 5-year follow-up Susan B. Tate & Linda Blackwell & Douglas J. Lorenz
DOI 10.1007/s00192-010-1249-3 ORIGINAL ARTICLE Randomized trial of fascia lata and polypropylene mesh for abdominal sacrocolpopexy: 5-year follow-up Susan B. Tate & Linda Blackwell & Douglas J. Lorenz
Scottish Clinical Coding Standards
 Scottish Clinical Coding Standards Number 16 October 2017 Scottish Clinical Coding Standards ICD-10 Sepsis Sepsis is a serious condition which must always be coded when documented in the medical record.
Scottish Clinical Coding Standards Number 16 October 2017 Scottish Clinical Coding Standards ICD-10 Sepsis Sepsis is a serious condition which must always be coded when documented in the medical record.
DENOMINATOR: All patients undergoing anterior or apical pelvic organ prolapse (POP) surgery
 surgery") Measure #428: Pelvic Organ Prolapse: Preoperative Assessment of Occult Stress Urinary Incontinence National Quality Strategy Domain: Effective Clinical Care 2016 PQRS OPTIONS FOR INDIVIDUAL MEASURES: REGISTY
Measure #428: Pelvic Organ Prolapse: Preoperative Assessment of Occult Stress Urinary Incontinence National Quality Strategy Domain: Effective Clinical Care 2016 PQRS OPTIONS FOR INDIVIDUAL MEASURES: REGISTY
Vaginal McCall culdoplasty versus laparoscopic uterosacral plication to prophylactically address vaginal vault prolapse
 Vaginal McCall culdoplasty versus laparoscopic uterosacral to prophylactically address vaginal vault prolapse Niblock, K., Bailie, E., McCracken, G., & Johnston, K. (2017). Vaginal McCall culdoplasty versus
Vaginal McCall culdoplasty versus laparoscopic uterosacral to prophylactically address vaginal vault prolapse Niblock, K., Bailie, E., McCracken, G., & Johnston, K. (2017). Vaginal McCall culdoplasty versus
DENOMINATOR: All patients undergoing anterior or apical pelvic organ prolapse (POP) surgery
 surgery") Quality ID #428: Pelvic Organ Prolapse: Preoperative Assessment of Occult Stress Urinary Incontinence National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY
Quality ID #428: Pelvic Organ Prolapse: Preoperative Assessment of Occult Stress Urinary Incontinence National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY
ig. 2. The organs and their outlet tubes.
 Fig. 1. Birth-related laxity. The diagram shows the baby s head severely stretching ligaments and other tissues in and outside the vagina. This may cause various degrees of looseness, prolapse of the bladder
Fig. 1. Birth-related laxity. The diagram shows the baby s head severely stretching ligaments and other tissues in and outside the vagina. This may cause various degrees of looseness, prolapse of the bladder
Tian-Ni Kuo 1, Ming-Ping Wu 1,2 *
 RESEARCH LETTER THE USE OF A CONCOMITANT TENSION-FREE VAGINAL MESH TECHNIQUE AND A TENSION-FREE MIDURETHRAL SLING IN TREATING PELVIC ORGAN PROLAPSE AND OCCULT STRESS URINARY INCONTINENCE Tian-Ni Kuo 1,
RESEARCH LETTER THE USE OF A CONCOMITANT TENSION-FREE VAGINAL MESH TECHNIQUE AND A TENSION-FREE MIDURETHRAL SLING IN TREATING PELVIC ORGAN PROLAPSE AND OCCULT STRESS URINARY INCONTINENCE Tian-Ni Kuo 1,
Interventional procedures guidance Published: 12 October 2016 nice.org.uk/guidance/ipg566
 Single-incision short sling mesh insertion for stress urinary incontinence in women Interventional procedures guidance Published: 12 October 2016 nice.org.uk/guidance/ipg566 Your responsibility This guidance
Single-incision short sling mesh insertion for stress urinary incontinence in women Interventional procedures guidance Published: 12 October 2016 nice.org.uk/guidance/ipg566 Your responsibility This guidance
Female Pelvic Medicine & Reconstructive Surgery
 Female Pelvic Medicine & Reconstructive Surgery APPLICATION FOR NEW FELLOWSHIP Name of Institution: McGill University Location: Royal Victoria Hospital (Glen Site), St Mary s Hospital Centre Type of Fellowship:
Female Pelvic Medicine & Reconstructive Surgery APPLICATION FOR NEW FELLOWSHIP Name of Institution: McGill University Location: Royal Victoria Hospital (Glen Site), St Mary s Hospital Centre Type of Fellowship:
Urethrolysis; When, Why & How. M Karram Professor of Ob/Gyn & Urology University of Cincinnati
 Urethrolysis; When, Why & How M Karram Professor of Ob/Gyn & Urology University of Cincinnati Anatomy Urethra may be fixed to the pubic bone with dense scar tissue Goal of urethrolysis is to completely
Urethrolysis; When, Why & How M Karram Professor of Ob/Gyn & Urology University of Cincinnati Anatomy Urethra may be fixed to the pubic bone with dense scar tissue Goal of urethrolysis is to completely
Complications from permanent synthetic mesh
 Original Research Symptom Resolution After Operative Management of Complications From Transvaginal Mesh Erin C. Crosby, MD, Melinda Abernethy, MD, MPH, Mitchell B. Berger, MD, PhD, John O. DeLancey, MD,
Original Research Symptom Resolution After Operative Management of Complications From Transvaginal Mesh Erin C. Crosby, MD, Melinda Abernethy, MD, MPH, Mitchell B. Berger, MD, PhD, John O. DeLancey, MD,
AGENDA. 8:00 AM 8:30 AM Pelvic Anatomy of the Lower Urinary Tract and the Anatomy and Physiology of Continence/Incontinence Mickey M.
 Thursday, June 12, 2014 Juniper Ballroom 1: Exhibits AGENDA 6:30 AM 8:00 AM Breakfast and Exhibits EVALUATION AND MANAGEMENT OF LOWER URINARY TRACT SYMPTOMS 8:00 AM 8:30 AM Pelvic Anatomy of the Lower
Thursday, June 12, 2014 Juniper Ballroom 1: Exhibits AGENDA 6:30 AM 8:00 AM Breakfast and Exhibits EVALUATION AND MANAGEMENT OF LOWER URINARY TRACT SYMPTOMS 8:00 AM 8:30 AM Pelvic Anatomy of the Lower
2017 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY. MEASURE TYPE: Process
 Measure #428: Pelvic Organ Prolapse: Preoperative Assessment of Occult Stress Urinary Incontinence National Quality Strategy Domain: Effective Clinical Care 2017 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY
Measure #428: Pelvic Organ Prolapse: Preoperative Assessment of Occult Stress Urinary Incontinence National Quality Strategy Domain: Effective Clinical Care 2017 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY
SACROSPINOUS LIGAMENT FIXATION, A SAFE AND EFFECTIVE WAY TO MANAGE VAGINAL VAULT PROLAPSE.A 10-YEAR OBSERVATIONAL STUDY OF CLINICAL PRACTICE
 Original Article, A SAFE AND EFFECTIVE WAY TO MANAGE VAGINAL VAULT PROLAPSE.A 10-YEAR OBSERVATIONAL STUDY OF CLINICAL PRACTICE * ** Fauzia Rasool Memon, Mohamed Matar * Consultant Obstetrician and Gynecologist
Original Article, A SAFE AND EFFECTIVE WAY TO MANAGE VAGINAL VAULT PROLAPSE.A 10-YEAR OBSERVATIONAL STUDY OF CLINICAL PRACTICE * ** Fauzia Rasool Memon, Mohamed Matar * Consultant Obstetrician and Gynecologist
ARTIFICIAL MESH REPAIR FOR TREATMENT OF PELVIC ORGAN PROLAPSE
 Pelvic Floor Unit / Department of Gynaecology Ward 17, Singleton Hospital, Sketty, Swansea, SA2 8QA 01792 205666 Secretary Direct Line: 01792 285688. Fax: 01792 285874 ARTIFICIAL MESH REPAIR FOR TREATMENT
Pelvic Floor Unit / Department of Gynaecology Ward 17, Singleton Hospital, Sketty, Swansea, SA2 8QA 01792 205666 Secretary Direct Line: 01792 285688. Fax: 01792 285874 ARTIFICIAL MESH REPAIR FOR TREATMENT
New Insights in the Surgical Management of Stress Urinary Incontinence in Women
 New Insights in the Surgical Management of Stress Urinary Incontinence in Women Gabriel Gillon MD Dept. of Urology Rabin Med. Cent. /Beilinson Incontinence and LUTS 25/6/2009 Symposium Ramat Aviv New Insights
New Insights in the Surgical Management of Stress Urinary Incontinence in Women Gabriel Gillon MD Dept. of Urology Rabin Med. Cent. /Beilinson Incontinence and LUTS 25/6/2009 Symposium Ramat Aviv New Insights
Site-specific fascial defects in the diagnosis and surgical management of enterocele
 Site-specific fascial defects in the diagnosis and surgical management of enterocele John R. Miklos, MD,a Neeraj Kohli, MD,b Vincent Lucente, MD,c and William B. Safe, MDd Atlanta and Marietta, GeO1gia,
Site-specific fascial defects in the diagnosis and surgical management of enterocele John R. Miklos, MD,a Neeraj Kohli, MD,b Vincent Lucente, MD,c and William B. Safe, MDd Atlanta and Marietta, GeO1gia,
Medium-term follow-up on use of freeze-dried, irradiated donor fascia for sacrocolpopexy and sling procedures
 Int Urogynecol J (2004) 15: 238 242 DOI 10.1007/s00192-004-1146-8 ORIGINAL ARTICLE Mary Pat FitzGerald Æ S. Renee Edwards Æ Dee Fenner Medium-term follow-up on use of freeze-dried, irradiated donor fascia
Int Urogynecol J (2004) 15: 238 242 DOI 10.1007/s00192-004-1146-8 ORIGINAL ARTICLE Mary Pat FitzGerald Æ S. Renee Edwards Æ Dee Fenner Medium-term follow-up on use of freeze-dried, irradiated donor fascia
Paravaginal Repair: A Laparoscopic Approach
 44 Paravaginal Repair: A Laparoscopic Approach John R. Miklos and Robert Moore Atlanta Urogynecology Associates, Atlanta, Georgia, U.S.A. Neeraj Kohli Harvard University, Boston, Massachusetts, U.S.A.
44 Paravaginal Repair: A Laparoscopic Approach John R. Miklos and Robert Moore Atlanta Urogynecology Associates, Atlanta, Georgia, U.S.A. Neeraj Kohli Harvard University, Boston, Massachusetts, U.S.A.
Childbirth after pelvic floor surgery: analysis of Hospital Episode Statistics in England,
 DOI: 10.1111/1471-0528.12076 www.bjog.org Urogynaecology Childbirth after pelvic floor surgery: analysis of Hospital Episode Statistics in England, 2002 2008 A Pradhan, a DG Tincello, b R Kearney a a Department
DOI: 10.1111/1471-0528.12076 www.bjog.org Urogynaecology Childbirth after pelvic floor surgery: analysis of Hospital Episode Statistics in England, 2002 2008 A Pradhan, a DG Tincello, b R Kearney a a Department
Subspecialty Procedural Volume Guidelines
 Subspecialty Review Committee for Obstetrics and Gynecology In response to requests from program directors, and in an effort to be transparent, the Review Committee for Obstetrics and Gynecology has elected
Subspecialty Review Committee for Obstetrics and Gynecology In response to requests from program directors, and in an effort to be transparent, the Review Committee for Obstetrics and Gynecology has elected
Sep \8958 Appell Dmochowski.ppt LMF 1
 Surgical Outcomes (How did we get ourselves into this mess?) Roger R. Dmochowski, MD, FACS Department of Urologic Surgery Vanderbilt University School of Medicine Nashville, Tennessee Considerations Evaluation
Surgical Outcomes (How did we get ourselves into this mess?) Roger R. Dmochowski, MD, FACS Department of Urologic Surgery Vanderbilt University School of Medicine Nashville, Tennessee Considerations Evaluation
Introduction to GYN Specialties
 Outline Introduction to GYN Specialties Gynecologic Oncology* Female Pelvic Medicine and Reconstructive Surgery* Reproductive Endocrinology and Infertility* Pediatric and Adolescent Gynecology** Family
Outline Introduction to GYN Specialties Gynecologic Oncology* Female Pelvic Medicine and Reconstructive Surgery* Reproductive Endocrinology and Infertility* Pediatric and Adolescent Gynecology** Family
Pelvic Floor Reconstruction
 3.9 Curriculum in Urology Trauma and Reconstruction Pelvic Floor Reconstruction W. Artibani a, Stuart L. Stanton b, D. Kumar c, R. Villet d a University of Verona, Italy; b Saint George Hospital Medical
3.9 Curriculum in Urology Trauma and Reconstruction Pelvic Floor Reconstruction W. Artibani a, Stuart L. Stanton b, D. Kumar c, R. Villet d a University of Verona, Italy; b Saint George Hospital Medical
Ina S. Irabon, MD, FPOGS, FPSRM, FPSGE Obstetrics and Gynecology Reproductive Endocrinology and Infertility Laparoscopy and Hysteroscopy
 Ina S. Irabon, MD, FPOGS, FPSRM, FPSGE Obstetrics and Gynecology Reproductive Endocrinology and Infertility Laparoscopy and Hysteroscopy Comprehensive Gynecology 7 th edition, 2017 (Lobo RA, Gershenson
Ina S. Irabon, MD, FPOGS, FPSRM, FPSGE Obstetrics and Gynecology Reproductive Endocrinology and Infertility Laparoscopy and Hysteroscopy Comprehensive Gynecology 7 th edition, 2017 (Lobo RA, Gershenson
Anatomical and Functional Results of Pelvic Organ Prolapse Mesh Repair: A Prospective Study of 105 Cases
 International Journal of Clinical Urology 2018; 2(1): 20-24 http://www.sciencepublishinggroup.com/j/ijcu doi: 10.11648/j.ijcu.20180201.14 Anatomical and Functional Results of Pelvic Organ Prolapse Mesh
International Journal of Clinical Urology 2018; 2(1): 20-24 http://www.sciencepublishinggroup.com/j/ijcu doi: 10.11648/j.ijcu.20180201.14 Anatomical and Functional Results of Pelvic Organ Prolapse Mesh
Urogynecology: Evidence-Based Clinical Practice
 Urogynecology: Evidence-Based Clinical Practice Kate H. Moore Urogynecology: Evidence-Based Clinical Practice Second Edition Kate H. Moore, MBBS, FRCOG, FRANZCOG, MD, CU Department Obstetrics & Gynaecology
Urogynecology: Evidence-Based Clinical Practice Kate H. Moore Urogynecology: Evidence-Based Clinical Practice Second Edition Kate H. Moore, MBBS, FRCOG, FRANZCOG, MD, CU Department Obstetrics & Gynaecology
WORKING TOGETHER FOR THE NHS 20/07/2018
 20/07/2018 NHS Improvement and NHS England Wellington House 133-155 Waterloo Road London SE1 8UG 020 3747 0000 www.england.nhs.uk www.improvement.nhs.uk To: Regional Directors, Trust Medical Directors,
20/07/2018 NHS Improvement and NHS England Wellington House 133-155 Waterloo Road London SE1 8UG 020 3747 0000 www.england.nhs.uk www.improvement.nhs.uk To: Regional Directors, Trust Medical Directors,
Urogynecology Curriculum for the PGY III and IV Resident
 Urogynecology Curriculum for the PGY III and IV Resident Sinai Hospital of Baltimore Maryland Department of Obstetrics and Gynecology I. Educational Purpose: The dedicated Urogynecology rotation is intended
Urogynecology Curriculum for the PGY III and IV Resident Sinai Hospital of Baltimore Maryland Department of Obstetrics and Gynecology I. Educational Purpose: The dedicated Urogynecology rotation is intended
Operative Approach to Stress Incontinence. Goals of presentation. Preoperative evaluation: Urodynamic Testing? Michelle Y. Morrill, M.D.
 Operative Approach to Stress Incontinence Goals of presentation Michelle Y. Morrill, M.D. Director of Urogynecology The Permanente Medical Group Kaiser, San Francisco Review preoperative care & evaluation
Operative Approach to Stress Incontinence Goals of presentation Michelle Y. Morrill, M.D. Director of Urogynecology The Permanente Medical Group Kaiser, San Francisco Review preoperative care & evaluation
Appendix 1. Canadian Classification of Health Intervention Codes Used to Identify
 1 2 3 Appendix 1. Canadian Classification of Health Intervention Codes Used to Identify any Vaginal Mesh (Synthetic) Implantation Procedure(s) for Pelvic Organ Prolapse 4 Canadian Classification of health
1 2 3 Appendix 1. Canadian Classification of Health Intervention Codes Used to Identify any Vaginal Mesh (Synthetic) Implantation Procedure(s) for Pelvic Organ Prolapse 4 Canadian Classification of health
Uphold LITE Vaginal Support System 2015 Coding & Quick Reference Guide
 Hospital Outpatient Coding Scenarios This guide contains specific information for two (2) common coding/reimbursement scenarios related to the use of the Uphold LITE Vaginal Support System when performed
Hospital Outpatient Coding Scenarios This guide contains specific information for two (2) common coding/reimbursement scenarios related to the use of the Uphold LITE Vaginal Support System when performed
Guide to Pelvic Floor Multicompartment Scanning
 Guide to Pelvic Floor Multicompartment Scanning These guidelines have been prepared by Giulio A. Santoro, MD, PhD, Head Pelvic Floor Unit, Section of Anal Physiology and Ultrasound, Coloproctology Service,
Guide to Pelvic Floor Multicompartment Scanning These guidelines have been prepared by Giulio A. Santoro, MD, PhD, Head Pelvic Floor Unit, Section of Anal Physiology and Ultrasound, Coloproctology Service,
John Laughlin 4 th year Cardiff University Medical Student
 John Laughlin 4 th year Cardiff University Medical Student Prolapse/incontinence You need to know: Pelvic floor anatomy in relation to uterovaginal support and continence The classification of uterovaginal
John Laughlin 4 th year Cardiff University Medical Student Prolapse/incontinence You need to know: Pelvic floor anatomy in relation to uterovaginal support and continence The classification of uterovaginal
Content. Terminology Anatomy Aetiology Presentation Classification Management
 Prolapse Content Terminology Anatomy Aetiology Presentation Classification Management Terminology Prolapse Descent of pelvic organs into the vagina Cystocele ant. vaginal wall involving bladder Uterine
Prolapse Content Terminology Anatomy Aetiology Presentation Classification Management Terminology Prolapse Descent of pelvic organs into the vagina Cystocele ant. vaginal wall involving bladder Uterine
Management of Vaginal Prolapse
 Information for Patients Saint Mary s Hospital/Trafford General Hospital Uro-gynaecology Service Management of Vaginal Prolapse Before reading this leaflet you should read What is vaginal prolapse? If
Information for Patients Saint Mary s Hospital/Trafford General Hospital Uro-gynaecology Service Management of Vaginal Prolapse Before reading this leaflet you should read What is vaginal prolapse? If
The incidence of mesh extrusion after vaginal incontinence and pelvic floor prolapse surgery
 ORIGINAL ARTICLE The incidence of mesh extrusion after vaginal incontinence and pelvic floor prolapse surgery Seth Cohen, Elizabeth Kavaler Department of Urology, Lenox Hill Hospital, USA Correspondence:
ORIGINAL ARTICLE The incidence of mesh extrusion after vaginal incontinence and pelvic floor prolapse surgery Seth Cohen, Elizabeth Kavaler Department of Urology, Lenox Hill Hospital, USA Correspondence:
HYSTERECTOMY FOR BENIGN CONDITIONS
 UnitedHealthcare Commercial Medical Policy HYSTERECTOMY FOR BENIGN CONDITIONS Policy Number: 2018T0572G Effective Date: September 1, 2018 Table of Contents Page INSTRUCTIONS FOR USE... 1 BENEFIT CONSIDERATIONS...
UnitedHealthcare Commercial Medical Policy HYSTERECTOMY FOR BENIGN CONDITIONS Policy Number: 2018T0572G Effective Date: September 1, 2018 Table of Contents Page INSTRUCTIONS FOR USE... 1 BENEFIT CONSIDERATIONS...
Pelvic Support Problems
 AP012, April 2010 ACOG publications are protected by copyright and all rights are reserved. ACOG publications may not be reproduced in any form or by any means without written permission from the copyright
AP012, April 2010 ACOG publications are protected by copyright and all rights are reserved. ACOG publications may not be reproduced in any form or by any means without written permission from the copyright
Registry Protocol Research Registry (PFDR-R) Version 1.3. (August 2016)
 Version 1.3. (August 2016)") Registry Protocol Research Registry (PFDR-R) Version 1.3 (August 2016) Table of Contents List of Abbreviations... 4 1. Background... 5 2. Rationale... 7 3. Objectives... 8 4. Registry Design... 9 4.1 Registry
Registry Protocol Research Registry (PFDR-R) Version 1.3 (August 2016) Table of Contents List of Abbreviations... 4 1. Background... 5 2. Rationale... 7 3. Objectives... 8 4. Registry Design... 9 4.1 Registry