Genitourinary Tract Trauma. Wen-xuan Chen Department of urology Tianjin medical university General hospital
|
|
|
- Marjory Black
- 5 years ago
- Views:
Transcription
1 Genitourinary Tract Trauma Wen-xuan Chen Department of urology Tianjin medical university General hospital
2 Introduction About 10% of all injuries in the emergency room are genitourinary injuries. The most commonly injured organ is the kidney; the second is the urethra and the third is the bladder.
3 Renal Trauma
4 Introduction Renal trauma is not common and occurs in approximately 1-5% of all traumas. Although the majority of renal traumas are mild,sometimes renal trauma can also be acutely life-threatening.
5 Introduction Renal trauma is often accompanied by injury to other organs or structures,such as rib fracture, spleen injury or liver injury. Kidneys with existing pathologic conditions such as hydronephrosis or malignant tumors are more readily ruptured from mild trauma.
6 Etiology Blunt Trauma: Blunt trauma directly to the abdomen,flank,or back is the most common mechanism,accounting for 80~85% of all renal injuries. Trauma may result from motor vehicle accidents, fights,falls,and contact sports.
7 Etiology Penetrating Trauma: Gunshot and knife wounds cause most penetrating injuries to the kidney. Any such wound in the flank area should be regarded as a cause of renal injury until proved otherwise. Renal injuries from penetrating trauma tend to be more severe and less predictable.
8 Pathologic Classification Minor renal trauma (85% of cases) Renal contusion of the parenchyma is the most common lesion. Subcapsular hematoma and superficial cortical lacerations are also considered minor trauma. These injuries rarely require surgical exploration.
9 Pathologic Classification Major renal trauma (15% of cases) Deep corticomedullary lacerations may extend into the collecting system,resulting in extravasation of urine into the perirenal space. Large retroperitoneal and perinephric hematomas often accompany these deep lacerations. Multiple lacerations may cause complete destruction of the kidney which may be called shattered kidney
10 Pathologic Classification Vascular injury(1% of all blunt trauma cases) Vascular injury of the renal pedicle is rare but may occur,usually from blunt trauma. There may be total avulsion of the artery and vein or partial avulsion of the segmental branches of these vessels. Vascular injuries are difficult to diagnose and result in total destruction of the kidney.
11 AAST renal-injury scaling system The Committee on Organ Injury Scaling of the American Association for the Surgery of Trauma (AAST) has developed a new renal-injury scaling system which is now widely used. This scaling system is the most important variable predicting the need for kidney repair or removal. Renal injuries are classified as grade 1 to grade 5.
12 Description of injury Grade 1: contusion or non-expanding subcapsular haematoma no laceration

13 Description of injury Grade 2: non-expanding perirenal haematoma cortical laceration < 1cm deep without extravasation

14 Description of injury Grade 3: cortical laceration>1cm without urinary extravasation
15 Description of injury Grade 4: Parenchymal laceration extending through the corticomedullary junction and into the collecting system

16 Description of injury Grade 4: segmental renal artery or vein injury with contained haematoma

17 Description of injury Grade 5: multiple major lacerations, resulting in a shattered kidney

18 Description of injury Grade 5: avulsion of the main renal artery and/or vein

19 Which grade?
20 Which grade?
21 Which grade?

22
23 Clinical Findings Microscopic or gross hematuria following trauma to the abdomen indicates injury to the urinary tract. It bears repeating that stab or gunshot wounds to the flank area should alert the physician to possible renal injury whether or not hematuria is present.
24 Clinical Findings The degree of renal injury does not correspond to the degree of hematuria,since gross hematuria may occur in minor renal trauma and only mild hematuria in major trauma. Patients with gross hematuria or microscopic hematuria with shock should undergo radiographic assessment;patients with microscopic hematuria without shock need not.
25 Clinical Findings If physical examination or associated injuries prompt reasonable suspicion of renal injury, renal imaging should be undertaken. This is especially true of patients with rapid deceleration trauma,who may have renal injury without the presence of hematuria.
26 Clinical Findings A. Symptoms: Pain may be localized to one flank area or over the abdomen. Catheterization usually reveals hematuria. Retroperitoneal bleeding may cause abdominal distention,ileus,and nausea and vomiting.
27 Clinical Findings B. Signs: Initially,shock or signs of a large loss of blood from heavy retroperitoneal bleeding may be noted. Ecchymosis in the flank or upper quadrants of the abdomen is often noted. Diffuse abdominal tenderness may be found on palpation.
28 Clinical Findings B. Signs: A palpable mass in the flank or abdomen may represent a large retroperitoneal hematoma or perhaps urinary extravasation. The abdomen may be distended and bowel sounds absent.
29 Clinical Findings C. laboratory evaluation: Haematuria (microscopic or gross) is a hallmark sign of renal injury. But haematuria is neither sensitive nor specific for differentiating minor and major injuries and it does not correlate with the degree of injury. In case of disruption of the ureteropelvic junction,renal pedicle injuries,and segmental arterial thrombosis,no haematuria is present.
30 Clinical Findings C. laboratory evaluation: The hematocrit may be normal initially,but a drop may be found when serial studies are done. This findings represents persistent retroperitoneal bleeding and development of a large retroperitoneal hematoma. Persistent bleeding may necessitate operation.
31 Clinical Findings D. Staging and Imaging : Adequate imaging studies help define the extent of injury and dictate appropriate management. Imaging studies include Ultrasonography, Intravenous Pyelography(IVP), Computed Tomography (CT), Magnetic Resonance Imaging(MRI), and Angiography.
32 Clinical Findings D. Staging and Imaging : Ultrasonography is a quick,non-invasive,lowcost imaging modality and is popularly used in the primary evaluation of polytrauma patients. Ultrasound scans can detect renal lacerations but can not definitely assess their depth and extent and do not provide functional information about renal excretion.
33 Clinical Findings D. Staging and Imaging : A CT scan with enhancement is the best imaging study for diagnosing and staging renal injuries in haemodynamically stable patients. This non-invasive technique clearly defines parenchymal lacerations and urinary extravasation,shows the extent of the retroperitoneal hematoma,and outlines injuries to surrounding organs such as the pancreas,spleens,liver,et al.
34 Clinical Findings D. Staging and Imaging : IVP,MRI are reliable alternative methods of imaging renal trauma when CT is not available. IVP may show extensive extravasation of radiopaque material if the kidney is lacerated. Nonvisualization of the kidney requires immediate arteriography or CT scan to determine whether renal vascular injury exists.
35 Clinical Findings D. Staging and Imaging : Angiography can be used for diagnosis and simutaneous selective embolization of bleeding vessels.

36

37

38

39
40 Management A. Emergency measures: The objectives of early management are prompt treatment of shock and haemorrhage,complete resuscitation,and evaluation of associated injuries.
41 Management B. Conservative measures: Stable patients,following grade 1-4 blunt renal trauma,should be managed conservatively with bed-rest for 2 weeks,prophylactic antibiotics,and continuous monitoring of vital signs until haematuria resolves.
42 Management B. Conservative measures: Stable patients,following grade 1-3 stab and low-velocity gunshot wounds after complete staging,should be selected for expectant management.
43 Management C. Indications for surgical measures: 1. haemodynamic instability 2. exploration for associated injuries 3. expanding or pulsatile perirenal haematoma identified during laparotomy 4. a grade V injury 5. incidental finding of pre-existing renal pathology requiring surgical therapy
44 Complications A. Early complications: Early complications occur within the first month after injury which include bleeding,infection, perinephric abscess,sepsis,and urinary extravasation and urinoma. Hemorrhage is perhaps the most important immediate complication of renal injury.
45 Complications A. Early complications: Patients must be observed closely,with careful monitoring of blood pressure,pulse and serial hematocrit. Evidence of an enlarging mass in the flank implies persistent bleeding. Bleeding may stop spontaneously in 80~85% of cases.
46 Complications A. Early complications: Urinary extravasation from renal fracture may show as an expanding mass (urinoma) in the retroperitoneum. These collections are prone to abscess formation and sepsis. A resolving retroperitoneal hematoma may cause slight fever,but higher temperatures suggest infection.
47 Complications B. Late complications: Hypertension,hydronephrosis,calculus formation, pyelonephritis,and arteriovenous fistula are important late complications. At 3-6 months,a follow-up excretory urogram or CT scan should be obtained to be certain that perinephric scarring has not caused hydronephrosis or vascular compromise.
48 Complications B. Late complications: Vascular compromise may result renal atrophy. The blood pressure should be carefully checked for several months because hypertension may be presented due to renal ischemia.
49 Prognosis Most renal injureis have an excellent prognosis. Follow up should involve physical exmination, urinalysis, excretory urography, serial blood presure measurement and serum determination of renal function.
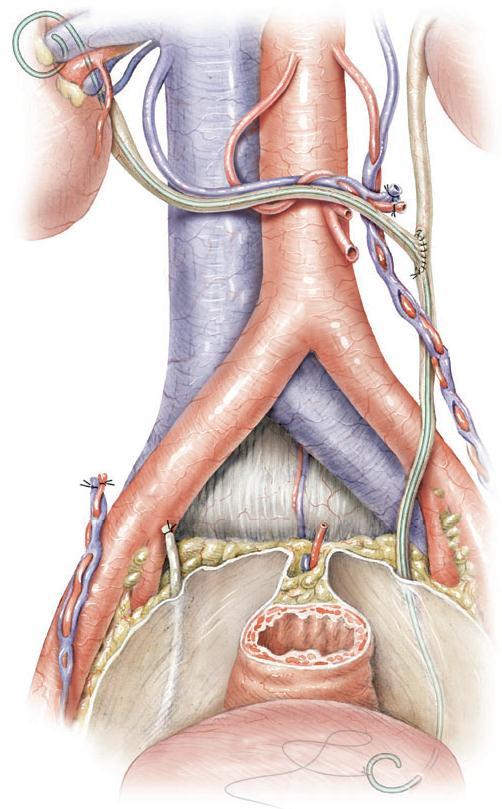
50 Injuries to the ureter
51 Introduction Ureteral injury is rare but may occur,usually during the course of a difficult pelvic surgical procedure or as a result of gunshot wounds. Endoscopic basket manipulation of ureteral calculi may also result in injury.
52 Clinical Findings A. Symptoms and signs: If the ureter has been injured during operation, the patient may complain of flank and lower abdominal pain on the injured side. Fever,nausea and vomiting are often present. Anuria following pelvic surgery means bilateral ureteral ligation until proved otherwise.
53 Clinical Findings A. Symptoms and signs: If ureterovaginal or cutaneous fistula develops,it usually does so within the first 10 postoperative days. Signs and symptoms of acute peritonitis may be present if there is urinary extravasation into the peritoneal cavity.
54 Clinical Findings B. Laboratory Findings: Microscopic hematuria is usually found. Tests of renal function will be normal unless both ureters are occluded.
55 Clinical Findings C. X-Ray Findings: Excretory urograms may show evidence of ureteral occlusion. Extravasation of radiopaque fluid may be seen in the region of the ureter. Retrograde urography will depict the site and nature of the injury.
 in the ureter below the site of injury, indicating complete ureteral")
56 Excretory urography demonstrating extravasation in the upper right ureter consequent to stab wound. Note lack of contrast (arrow) in the ureter below the site of injury, indicating complete ureteral transection.
57 Clinical Findings D. Ultrasonography: Ultrasonography outlines hydroureter or urinary extravasation as it develops into a urinoma and it perhaps the best means of ruling out ureteral injury in the early postoperative period. It has the advantages of being noninvasive and rapid.
58 Clinical Findings E. Radionuclide Scanning: This technique will show delayed excretion,with an accumulation of counts in the pelvis and renal parenchyma resulting from ureteral obstruction. It is useful postoperatively to assess the result of corrective surgery.
59 AAST s classification Grade 1 haematoma only Grade 2 laceration < 50% of circumference Grade 3 laceration > 50% of circumference Grade 4 complete tear<2cm of devascularization Grade 5 complete tear>2cm of devascularization
60 Management Prompt treatment of ureteral injuries is required. The best opportunity for successful repair is in the operating room when the injury occurs. If the injury is not recognized until 7-10 days after the event and no infection,abscess,or other complications exist,immediate reexploration and repair are indicated.
61 Management If the injury is recognized late or if the patient has significant complications that make immediate reconstruction unsatisfactory,proximal urinary drainage by percutaneous nephrostomy or formal nephrostomy should be considered.
62 Management A. Partial injuries: These can be defined as grade 1 to grade 2 lesions. Once recognized,they can be managed with ureteral stenting or by placement of a nephrostomy tube to divert urine. If this technique is utilized,a bladder catheter should be left in place for 2 days to limit stent reflux during voiding.
63 Management A. Partial injuries: The ureteral stent should be left in place for at least 3 weeks. If a grade 2 or 3 injury is encountered during immediate surgical exploration,primary closure of the ureteral ends over a stent may be recommended,with placement of an external drain adjacent to the injury.

64 Double J tube an indwelling stent Management
65 Management B. Complete injuries: These are grade 3 to 4 injuries. Successful repair should utilize the principles described in below.
66 Management Principles of repair of complete injury: Debridement of ureteral ends to fresh tissue Spatulation of ureteral ends Placement of internal stent Watertight closure of reconstructed ureter with absorbable suture Placement of external,non suction drain Isolation of injury with peritoneum or omentum
67 Management Uretero- ureterostomy
68 The type of reconstructive repair procedure chosen by the surgeon depends on the nature and site of the injury Management
69 Injuries to the upper third of the ureter are best managed by primary ureteroureterostomy. Management
70 Midureteral injuries usually result from external violence and are best repaired by primary ureteroureterostomy or transureteroureterostomy Management

71 Transureteroureterostomy may be used in lower-third injuries if extensive urinoma and pelvic infection have developed. This procedure allows anastomosis and reconstruction in area away from the pathologic processes. Management
72 Management
73 Prognosis The prognosis for ureteral injury is excellent if the diagnosis is made early and prompt corrective surgery is done. Delay in diagnosis worsens the prognosis because of infection,hydronephrosis,abscess, and fistula formation.
74 Injuries to the bladder
75 Introduction Bladder injuries occur most often from external force and are often associated with pelvic fractures. When the bladder is filled to near capacity,a direct blow to the lower abdomen may also result in bladder rupture.
76 Mechanism Blunt trauma accounts for 67~86% of bladder ruptures,while penetrating trauma for 14~33%. The most common cause (90%) of bladder rupture by blunt trauma is motor vehicle accidents. About 70~97% of patients with bladder injuries from blunt trauma have associated pelvic fractures.

77 A direct blow over the full bladder causes increased intravesical pressure. If the bladder ruptures,it will usually rupture into the peritoneal cavity. Mechanism
78 Classification Type Description 1 Bladder contusion 2 Intraperitoneal rupture 3 Interstitial bladder injury 4 Extraperitoneal rupture 5 Combined injury
79 Clinical Findings A. Symptom and signs: The two most common sign and symptoms are gross haematuria (82%) and abdominal tenderness (62%)in patients with major bladder injuries. Other findings may include the inability to void, bruises over the suprapubic region and abdominal distension. Extravasation of urine may result in swelling in the perineum,scrotum and thighs.
80 Clinical Findings B. Laboratory Findings: Catheterization usually is required in patients with pelvic trauma but not if bloody urethral discharge is noted. Bloody urethral discharge indicates urethral injury,and a urethrogram is necessary before catheterization. When catheterization is done,gross or,less commonly,microscopic hematuria is usually present.
81 Clinical Findings C. X-Ray Findings: A plain abdominal film generally demonstrates pelvic fractures. An intravenous urogram should be obtained to establish whether kidney and ureteral injuries are present.
82 Clinical Findings D. Cystography: Retrograde cystography is the standard and the most accurate radiological study for diagnosing bladder rupture.when adequate bladder filling and post-void images are obtained,it has an accuracy rate of %. Immediate cystography is required in the presence of haematuria and pelvic fracture.
83 Clinical Findings D. Cystography: Diagnosis should be made with retrograde cystography with a minimum of 350 ml of gravity filled contrast medium. For cystography,the minimum requirement includes a plain film, filled film, and postdrainage film. Half-filled film and obliques are optional.

84

85 Plain film

86 cystogram

87

88
89 Management The first priority in the treatment of bladder injuries is stabilization of the patient and treatment of associated life-threatening injuries. Extraperitoneal bladder ruptures caused by blunt trauma are managed by catheter drainage only. Intraperitoneal bladder ruptures by blunt trauma and any type of bladder injury by penetrating trauma must be managed by emergency surgical exploration and repair.
90 Prognosis With appropriate treatment,the prognosis is excellent. Early diagnosis and treatment lead to low rate complications and death.
91 Injuries to the urethra
92 Introduction Urethral injuries are uncommon and occur most often in men. The urethra can be separated into 2 broad anatomic divisions: 1. the anterior urethra, consisting of the bulbous and pendulous portions; 2. the posterior urethra, consisting of the prostatic and membranous portions.

93
94 Injuries to the anterior urethra Anterior urethral injury is more ofen than posterior urethral injury. The majority of anterior urethral injury occurs in bulbous urethra. The most common cause is straddle-type injuries caused by blows of blunt objects against the perineum.

95 Injury to the bulbous urethra Mechanism: Usually a perineal blow or fall astride an object; crushing of urethra against inferior edge of pubic symphysis
96 Classification Contusion: blood at the urethral meatus; no extravasation on urethrography Partial disruption: extravasation of contrast at injury site with contrast visualized in the proximal urethra or bladder Complete disruption: extravasation of contrast at injury site without visualization of proximal urethra or bladder
97 Clinical Findings A. Symptoms and Signs: There is usually a history of a fall,and in some cases a history of instrumentation. Bleeding from the urethra is usually present. There is local pain into the perineum and sometimes massive perineal hematoma.
98 Clinical Findings A. Symptoms and Signs: The patient may complain of pain on urination or inability to void. If voiding has occurred and extravasation is noted,sudden swelling in the area will be present. If diagnosis has been delayed,sepsis and severe infection may be present.
99 Clinical Findings A. Symptoms and Signs: The perineum is very tender,and a mass may be found. Rectal examination reveals a normal prostate. The patient usually has a desire to void,but voiding should not be allowed until assessment of the urethra is complete. No attempt should be made to pass a urethral catheter.
100 Clinical Findings B. Laboratory Findings: The amount of urethral bleeding correlates poorly with the severity of injury. A contusion or partial disruption may be accompanied by plenty of bleeding while total disruption may result in little bleeding.
101 Clinical Findings C. X-Ray Findings: Retrograde urethrography is considered the gold standard for evaluating urethral injury. A urethrogram,with instillation of 15-20ml of water soluble contrast material,demonstrates extravasation and the location of injury. A contused urethra shows no evidence of extravasation.
102 Clinical Findings D. Instrumental Examination: If there is no evidence of extravasation on the urethrogram,a urethral catheter may be passed into the bladder. Extravasation is a contraindication to further instrumentation at this time.
103 Management General Measures: Major blood loss usually does not occur from straddle injury. If heavy bleeding does occur,local pressure for control,followed by resuscitation,is required.
104 Management A. Urethral Contusion: The patient with urethral contusion shows no evidence of extravasation,and the urethra remains intact. After urethrography,the patient is allowed to void;and if the voiding occurs normally,without pain or bleeding,no additional treatment is necessary.if bleeding persists,urethral catheter drainage can be done.
105 Management B. Urethral disruptions: A suprapubic cystostomy tube should be placed and maintained for approximately 4 weeks. Voiding cystourethrography is then performed and if normal voiding can be re-established and no contrast extravasation nor subsequent stricture is present,then the tube can be safely removed.
106 Management B. Urethral disruptions: Immediate repair of urethral lacerations can be performed,but the procedure is difficult and the incidence of associated stricture is high.
107 Complications The potential early complications of acute urethral injuries include stricture and infections. Drainage of extensive urinary extravasation and large hematoma may be required.
108 Complications Prompt urinary diversion coupled with the appropriate administration of antibiotics decreases the incidence of these complications. Urethral stricture may be managed with optical urethrotomy,anastomotic urethroplasty or flap urethroplasty.
109 Injuries to the posterior urethra Posterior urethral injury commonly occur from blunt trauma and pelvic fractures. When pelvic fractures occur from blunt trauma, the membranous urethra is sheared from the prostatic apex at the prostatomembranous junction. Urinary extravasation and bleeding are periprostatic and perivesical.

110 Injuries to the posterior urethra The prostate has been avulsed from the membranous urethra secondary to fracture of the pelvis. Extravasation occurs above the triangular ligament and is periprostatic and perivesical
111 Clinical Findings A. Symptoms: A history of crushing injury to the pelvis is usually obtained. Patients usually complain of lower abdominal pain and inability to urinate.
112 Clinical Findings B. Signs: Blood at the urethral meatus is the single most important sign of urethral injury.the importance of this finding can not be overemphasized, because an attempt to pass a urethral catheter may result in infection of the periprostatic and perivesical hematoma and conversion of an incomplete laceration to a complete one.
113 Clinical Findings B. Signs: The presence of blood at the meatus indicates that immediate urethrogram is necessary to establish the diagnosis. Suprapubic tenderness and the presence of pelvic fracture are noted on physical examination.
114 Clinical Findings B. Signs: A large developing pelvic hematoma may be palpated perineal or suprapubic contusions are often noted. Rectal examination may reveal a large pelvic hematoma with the prostate displaced superiorly.
115 Clinical Findings C. Laboratory Findings: Anemia due to hemorrhage may be noted. Urine usually can not be obtained initially,since the patient should not void and catheterization should not be attempted.
116 Clinical Findings D. X-Ray Findings: Pelvic fractures are usually present. A urethrogram (using ml of water-soluble contrast material) shows the site of extravasation at the prostatomembranous junction. Ordinarily,there is free extravasation of contrast material into the perivesical space.
117 Clinical Findings D. X-Ray Findings: Incomplete prostatomembranous disruption is seen as minor extravasation,with a portion of contrast material passing into the prostatic urethra and bladder.
118 Clinical Findings E. Instrumental Examination: The only instrumentation involved should be for urethrography. Catheterization or urethroscopy should not be done,because these procedures pose an increased risk of hematoma,infection,and further damage to partial urethral disruptions.

119 Retrograde urethrogram demonstrating complete posterior urethral disruption.
120 Management A. Emergency measures: Shock and hemorrhage should be treated.
121 Management B. Surgical measures: Initial management should consist of suprapubic cystostomy to provide urinary drainage. The suprapubic cystostomy is maintained in place for about 3 months.this allows resolution of the pelvic hematoma,and the prostate and bladder will slowly return to their anatomic positions.
122 Management B. Surgical measures: Incomplete laceration of the posterior urethra heals spontaneously,and the suprapubic cystostomy can be removed within 2-3 weeks. The cystostomy tube should not be removed before voiding cystourethrography shows that no extravasation persists.
123 Management B. Surgical measures: Urethral reconstruction can be undertaken within 3 months,assuming there is no pelvic abscess or other evidence of persistent pelvic infection. Before reconstruction,a combined cystogram and urethrogram should be done to determine the exact length of the resulting urethral stricture.

124 Combination urethrogram and cystogram demonstrating a 2-cm urethral rupture defect (arrow).
125 Management B. Surgical measures: If the stricture is <2cm long,the preferred approach is a single-stage reconstruction with direct excision of the strictured area and anastomosis of the bulbous urethra directly to the apex of the prostate.
126 Complications Late complications include urethral stricture at the site of healing. Impotence as a result of damage to local nerves or blood vessels,is permanent in about 10% of patients. Urinary incontinence seldom follows transpubic or perineal reconstruction.if present,it usually resolves slowly.
Canadian Undergraduate Urology Curriculum (CanUUC): Genitourinary Trauma. Last reviewed June 2014
: Genitourinary Trauma. Last reviewed June 2014") Canadian Undergraduate Urology Curriculum (CanUUC): Genitourinary Trauma Last reviewed June 2014 Session Objectives 1. Recognize hematuria as the cardinal symptom of urinary tract trauma. 1. Outline the
Canadian Undergraduate Urology Curriculum (CanUUC): Genitourinary Trauma Last reviewed June 2014 Session Objectives 1. Recognize hematuria as the cardinal symptom of urinary tract trauma. 1. Outline the
UROLOGIC TRAUMA. Urology Division, Surgery Department Medical Faculty, University of Sumatera Utara
 UROLOGIC TRAUMA Urology Division, Surgery Department Medical Faculty, University of Sumatera Utara UROLOGIC TRAUMA Renal trauma Ureteral injury Bladder injury Urethral injury Injury to external genitalia
UROLOGIC TRAUMA Urology Division, Surgery Department Medical Faculty, University of Sumatera Utara UROLOGIC TRAUMA Renal trauma Ureteral injury Bladder injury Urethral injury Injury to external genitalia
Clinical aspects in urogenital injuries
 Clinical aspects in urogenital injuries Rolf Wahlqvist Oslo Urological University Clinic Aker University Hospital Nordic Rad.2008 1 Urogenital injuries in trauma patients Renal injury Ureteral injury (infrequent/iatrogenic)
Clinical aspects in urogenital injuries Rolf Wahlqvist Oslo Urological University Clinic Aker University Hospital Nordic Rad.2008 1 Urogenital injuries in trauma patients Renal injury Ureteral injury (infrequent/iatrogenic)
Genitourinary Tract Injuries
 Genitourinary Tract Injuries Chapter 18 Genitourinary Tract Injuries Introduction Genitourinary injuries constitute approximately 5% of the total injuries encountered in combat. Their treatment adheres
Genitourinary Tract Injuries Chapter 18 Genitourinary Tract Injuries Introduction Genitourinary injuries constitute approximately 5% of the total injuries encountered in combat. Their treatment adheres
Genitourinary Trauma Introduction GU Trauma overlooked
 Genitourinary Trauma Introduction GU Trauma overlooked 10-20% of all injured patients Long term morbidity Impotence Incontinence Life-threatening injuries first Urethral Injury Plan Bladder Injury Kidney
Genitourinary Trauma Introduction GU Trauma overlooked 10-20% of all injured patients Long term morbidity Impotence Incontinence Life-threatening injuries first Urethral Injury Plan Bladder Injury Kidney
UBC Department of Urologic Sciences Lecture Series. Urological Trauma
 UBC Department of Urologic Sciences Lecture Series Urological Trauma Disclaimer: This is a lot of information to cover and we are unlikely to cover it all today These slides are to be utilized for your
UBC Department of Urologic Sciences Lecture Series Urological Trauma Disclaimer: This is a lot of information to cover and we are unlikely to cover it all today These slides are to be utilized for your
Diagnosis & Management of Kidney Trauma. LAU - Urology Residency Program LOP Urology Residents Meeting
 Diagnosis & Management of Kidney Trauma LAU - Urology Residency Program LOP Urology Residents Meeting Outline Introduction Investigation Staging Treatment Introduction The kidneys are the most common genitourinary
Diagnosis & Management of Kidney Trauma LAU - Urology Residency Program LOP Urology Residents Meeting Outline Introduction Investigation Staging Treatment Introduction The kidneys are the most common genitourinary
Bladder Trauma Data Collection Sheet
 Bladder Trauma Data Collection Sheet If there was no traumatic injury with PENETRATION of the bladder DO NOT proceed Date of injury: / / Time of injury: Date of hospital arrival: / / Time of hospital arrival:
Bladder Trauma Data Collection Sheet If there was no traumatic injury with PENETRATION of the bladder DO NOT proceed Date of injury: / / Time of injury: Date of hospital arrival: / / Time of hospital arrival:
Role of imaging in evaluation of genitourinary i trauma Spectrum of GU injuries Relevance of imaging findings in determining management Focus on MDCT
 Genitourinary Tract Injuries 6 th Nordic Course Scott D. Steenburg, MD Assistant Professor University of Maryland Department of Radiology Division of Trauma and Emergency Radiology R Adams Cowley Shock
Genitourinary Tract Injuries 6 th Nordic Course Scott D. Steenburg, MD Assistant Professor University of Maryland Department of Radiology Division of Trauma and Emergency Radiology R Adams Cowley Shock
Renal Trauma: Management Options
 Renal Trauma: Management Options Immediate surgical repair Nephrectomy Conservative management Alonso RC et al. Kidney in Danger: CT Findings of Blunt and Penetrating Renal Trauma. RadioGraphics 2009;
Renal Trauma: Management Options Immediate surgical repair Nephrectomy Conservative management Alonso RC et al. Kidney in Danger: CT Findings of Blunt and Penetrating Renal Trauma. RadioGraphics 2009;
Urogenital Injuries The role of radiology
 Urogenital Injuries The role of radiology NORDTER 7 th Nordic Trauma Radiology Course Helsinki, Finland May 21-24, 2012 Johann Baptist Dormagen, MD, PhD Oslo University Hospital, Norway Kidney injuries
Urogenital Injuries The role of radiology NORDTER 7 th Nordic Trauma Radiology Course Helsinki, Finland May 21-24, 2012 Johann Baptist Dormagen, MD, PhD Oslo University Hospital, Norway Kidney injuries
EAU GUIDELINES POCKET EDITION 4
 EAU GUIDELINES POCKET EDITION 4 CONTENTS: UROLOGICAL TRAUMA PAIN MANAGEMENT IN UROLOGY UROGENERIC LUTS RENAL TRANSPLANTATION 2 EAU POCKET GUIDELINES POCKET EDITION 4 Introduction 3 Introduction This is
EAU GUIDELINES POCKET EDITION 4 CONTENTS: UROLOGICAL TRAUMA PAIN MANAGEMENT IN UROLOGY UROGENERIC LUTS RENAL TRANSPLANTATION 2 EAU POCKET GUIDELINES POCKET EDITION 4 Introduction 3 Introduction This is
West Yorkshire Major Trauma Network Clinical Guidelines 2015
 WYMTN: Pelvic fracture with urogenital trauma KEY RECOMMENDATIONS 1. During the initial exploratory survey / secondary survey, a. The external urethral meatus and the transurethral bladder catheter (if
WYMTN: Pelvic fracture with urogenital trauma KEY RECOMMENDATIONS 1. During the initial exploratory survey / secondary survey, a. The external urethral meatus and the transurethral bladder catheter (if
Uroradiology For Medical Students
 Uroradiology For Medical Students Lesson 4: Cystography & Urethrography - Part 2 American Urological Association Review Cystography is useful in evaluating the bladder, the urethra and the competence of
Uroradiology For Medical Students Lesson 4: Cystography & Urethrography - Part 2 American Urological Association Review Cystography is useful in evaluating the bladder, the urethra and the competence of
Guidelines on Urological Trauma
 Guidelines on Urological Trauma D. Lynch, L. Martinez-Piñeiro, E. Plas, E. Serafetinidis, L. Turkeri, R. Santucci, M. Hohenfellner European Association of Urology 2006 TABLE OF CONTENTS PAGE 1. RENAL TRAUMA
Guidelines on Urological Trauma D. Lynch, L. Martinez-Piñeiro, E. Plas, E. Serafetinidis, L. Turkeri, R. Santucci, M. Hohenfellner European Association of Urology 2006 TABLE OF CONTENTS PAGE 1. RENAL TRAUMA
GUIDELINEs ON UROLOGICAL TRAUMA
 GUIDELINEs ON UROLOGICAL TRAUMA (Text update March 2009) N. Djakovic, Th. Lynch, L. Martínez-Piñeiro, Y. Mor, E. Plas, E. Serafetinides, L. Turkeri, R.A. Santucci, M. Hohenfellner Eur Urol 2005;47(1):1-15
GUIDELINEs ON UROLOGICAL TRAUMA (Text update March 2009) N. Djakovic, Th. Lynch, L. Martínez-Piñeiro, Y. Mor, E. Plas, E. Serafetinides, L. Turkeri, R.A. Santucci, M. Hohenfellner Eur Urol 2005;47(1):1-15
GUIDELINEs ON UROLOGICAL TRAUMA
 GUIDELINEs ON UROLOGICAL TRAUMA (Text update March 2009) N. Djakovic, Th. Lynch, L. Martínez-Piñeiro, Y. Mor, E. Plas, E. Serafetinides, L. Turkeri, R.A. Santucci, M. Hohenfellner Eur Urol 2005;47(1):1-15
GUIDELINEs ON UROLOGICAL TRAUMA (Text update March 2009) N. Djakovic, Th. Lynch, L. Martínez-Piñeiro, Y. Mor, E. Plas, E. Serafetinides, L. Turkeri, R.A. Santucci, M. Hohenfellner Eur Urol 2005;47(1):1-15
Excretory urography (EU) or IVP US CT & radionuclide imaging
 or IVP US CT & radionuclide imaging") Excretory urography (EU) or IVP US CT & radionuclide imaging MRI arteriography studies requiring catherization or direct puncture of collecting system EU & to a lesser extent CT provide both functional
Excretory urography (EU) or IVP US CT & radionuclide imaging MRI arteriography studies requiring catherization or direct puncture of collecting system EU & to a lesser extent CT provide both functional
PROFESSIONAL SKILLS 1 3RD YEAR SEMESTER 6 RADIOGRAPHY. THE URINARY SYSTEM Uz. Fatema shmus aldeen Tel
 PROFESSIONAL SKILLS 1 3RD YEAR SEMESTER 6 RADIOGRAPHY THE URINARY SYSTEM Uz. Fatema shmus aldeen Tel. 0925111552 Professional skills-2 THE URINARY SYSTEM The urinary system (review anatomy and physiology)
PROFESSIONAL SKILLS 1 3RD YEAR SEMESTER 6 RADIOGRAPHY THE URINARY SYSTEM Uz. Fatema shmus aldeen Tel. 0925111552 Professional skills-2 THE URINARY SYSTEM The urinary system (review anatomy and physiology)
Traumatic Renocaval Fistula With Pseudoaneurysm Leading To Renal Atrophy
 ISPUB.COM The Internet Journal of Radiology Volume 6 Number 2 Traumatic Renocaval Fistula With Pseudoaneurysm Leading To Renal Atrophy M Kukkady, A Deena, S Raj, Ramachandra Citation M Kukkady, A Deena,
ISPUB.COM The Internet Journal of Radiology Volume 6 Number 2 Traumatic Renocaval Fistula With Pseudoaneurysm Leading To Renal Atrophy M Kukkady, A Deena, S Raj, Ramachandra Citation M Kukkady, A Deena,
Guidelines on Urological Trauma
 Guidelines on Urological Trauma N. Djakovic, E. Plas, L. Martínez-Piñeiro, Th. Lynch, Y. Mor, R.A. Santucci, E. Serafetinidis, L.N. Turkeri, M. Hohenfellner European Association of Urology 2012 TABLE OF
Guidelines on Urological Trauma N. Djakovic, E. Plas, L. Martínez-Piñeiro, Th. Lynch, Y. Mor, R.A. Santucci, E. Serafetinidis, L.N. Turkeri, M. Hohenfellner European Association of Urology 2012 TABLE OF
EAU GUIDELINES ON UROLOGICAL TRAUMA
 EAU GUIDELINES ON UROLOGICAL TRAUMA (Limited text update March 2016) N.D. Kitrey (Chair), N. Djakovic, M. Gonsalves, F.E. Kuehhas, N. Lumen, E. Serafetinidis, D.M. Sharma, D.J. Summerton Guidelines Associates:
EAU GUIDELINES ON UROLOGICAL TRAUMA (Limited text update March 2016) N.D. Kitrey (Chair), N. Djakovic, M. Gonsalves, F.E. Kuehhas, N. Lumen, E. Serafetinidis, D.M. Sharma, D.J. Summerton Guidelines Associates:
The number following the procedure code is the TRICARE payment group. KIDNEY
 TRICARE/CHAMPUS POLICY MANUAL 6010.47-M JUNE 25, 1999 S POLICY CHAPTER 13 SECTION 9.1 ADDENDUM 1, SECTION 8 TRICARE-APPROVED AMBULATORY SURGERY S - URINARY SYSTEM The number following the procedure code
TRICARE/CHAMPUS POLICY MANUAL 6010.47-M JUNE 25, 1999 S POLICY CHAPTER 13 SECTION 9.1 ADDENDUM 1, SECTION 8 TRICARE-APPROVED AMBULATORY SURGERY S - URINARY SYSTEM The number following the procedure code
Center for Reconstructive Urethral Surgery Guido Barbagli Center for Reconstructive Urethral Surgery Arezzo - Italy
 Guido Barbagli Arezzo - Italy E-mail: guido@rdn.it Website: www.urethralcenter.it 23 rd ANNUAL EAU CONGRESS Sub-plenary Session on Male urinary incontinence 26 29 March 2008 Milan Italy Incontinence following
Guido Barbagli Arezzo - Italy E-mail: guido@rdn.it Website: www.urethralcenter.it 23 rd ANNUAL EAU CONGRESS Sub-plenary Session on Male urinary incontinence 26 29 March 2008 Milan Italy Incontinence following
GUIDELINES ON UROLOGICAL TRAUMA
 GUIDELINES ON UROLOGICAL TRAUMA (Limited text update March 2015) D.J. Summerton (Chair), N. Djakovic, N.D. Kitrey, F.E. Kuehhas, N. Lumen, E. Serafetinides, D.M. Sharma Eur Urol 2010 May;57(5):791-803
GUIDELINES ON UROLOGICAL TRAUMA (Limited text update March 2015) D.J. Summerton (Chair), N. Djakovic, N.D. Kitrey, F.E. Kuehhas, N. Lumen, E. Serafetinides, D.M. Sharma Eur Urol 2010 May;57(5):791-803
Hydronephrosis. What is hydronephrosis?
 What is hydronephrosis? Hydronephrosis Hydronephrosis describes the situation where the urine collecting system of the kidney is dilated. This may be a normal variant or it may be due to an underlying
What is hydronephrosis? Hydronephrosis Hydronephrosis describes the situation where the urine collecting system of the kidney is dilated. This may be a normal variant or it may be due to an underlying
Question 2. What percentage of abdominal trauma involve the kidney? a) 5 % b) 10% c) 15 % d) 20 %
 5 % b) 10% c) 15 % d) 20 %") Quiz Question 1 After injecting 2ml/kg of contrast for a patient needing a single-shot IVP before kidney exploration, What is the best turnaround time to take the X-ray? a) 3 minutes b) 5 minutes c) 10
Quiz Question 1 After injecting 2ml/kg of contrast for a patient needing a single-shot IVP before kidney exploration, What is the best turnaround time to take the X-ray? a) 3 minutes b) 5 minutes c) 10
Urethral Injuries: Realignment vs. Delayed Reconstruction
 Urethral Injuries: Realignment vs. Delayed Reconstruction E. Charles Osterberg, MD Assistant Professor of Surgery (Urology) Dell Medical School Chief of Urology and Genitourinary Reconstruction None Disclosures
Urethral Injuries: Realignment vs. Delayed Reconstruction E. Charles Osterberg, MD Assistant Professor of Surgery (Urology) Dell Medical School Chief of Urology and Genitourinary Reconstruction None Disclosures
Guido Barbagli. Center for Reconstructive ti Urethral lsurgery
 Guido Barbagli Center for Reconstructive ti Urethral lsurgery Arezzo - Italy E-mail: guido@rdn.it Website: www.urethralcenter.it Dedicated to Ruggero Lenzi, teacher and friend. His passing was a great
Guido Barbagli Center for Reconstructive ti Urethral lsurgery Arezzo - Italy E-mail: guido@rdn.it Website: www.urethralcenter.it Dedicated to Ruggero Lenzi, teacher and friend. His passing was a great
2. Blunt abdominal Trauma
 Abdominal Trauma 1. Evaluation and management depends on: a. Mechanism (Blunt versus Penetrating) b. Injury complex in addition to abdomen c. Haemodynamic stability assessment: i. Classically patient s
Abdominal Trauma 1. Evaluation and management depends on: a. Mechanism (Blunt versus Penetrating) b. Injury complex in addition to abdomen c. Haemodynamic stability assessment: i. Classically patient s
LIVER INJURIES PROFF. S.FLORET
 LIVER INJURIES PROFF. S.FLORET Abdominal injuries For anatomical consideration: Abdomen can be divided in four areas Intra thoracic abdomen True abdomen Pelvic abdomen Retroperitoneal abdomen ETIOLOGY
LIVER INJURIES PROFF. S.FLORET Abdominal injuries For anatomical consideration: Abdomen can be divided in four areas Intra thoracic abdomen True abdomen Pelvic abdomen Retroperitoneal abdomen ETIOLOGY
Urinary tract embolization
 Beograd, 14.10.2012 Urinary tract embolization asist. Peter Popovič, MD, MSc Head of abdominal radiology department, Institute of Radiology, UMC Ljubljana Embolization Who and when procedure: local/general
Beograd, 14.10.2012 Urinary tract embolization asist. Peter Popovič, MD, MSc Head of abdominal radiology department, Institute of Radiology, UMC Ljubljana Embolization Who and when procedure: local/general
A Z OF ABDOMINAL RADIOLOGY
 Z OF BDOMINL RDIOLOGY bdominal trauma to Z of bdominal Radiology Clinical characteristics general discussion, followed by organ-specific summaries, is given below. bdominal trauma is managed as part of
Z OF BDOMINL RDIOLOGY bdominal trauma to Z of bdominal Radiology Clinical characteristics general discussion, followed by organ-specific summaries, is given below. bdominal trauma is managed as part of
Muscle spasm Diminished bowel sounds Nausea/vomiting
 3 4 5 6 7 8 9 0 Chapter 8: Abdomen and Genitalia Injuries Abdominal Injuries Abdomen is major body cavity extending from to pelvis. Contains organs that make up digestive, urinary, and genitourinary systems.
3 4 5 6 7 8 9 0 Chapter 8: Abdomen and Genitalia Injuries Abdominal Injuries Abdomen is major body cavity extending from to pelvis. Contains organs that make up digestive, urinary, and genitourinary systems.
THE operation of reimplantation of the ureter into the bladder has undergone
 REIMPLANTATION OF THE URETER INTO THE BLADDER J. G. WARDEN, M.D., and C. C. HIGGINS, M.D. Department of Urology THE operation of reimplantation of the ureter into the bladder has undergone a stormy course
REIMPLANTATION OF THE URETER INTO THE BLADDER J. G. WARDEN, M.D., and C. C. HIGGINS, M.D. Department of Urology THE operation of reimplantation of the ureter into the bladder has undergone a stormy course
Lec-8 جراحة بولية د.نعمان
 4th stage Lec-8 جراحة بولية د.نعمان 11/10/2015 بسم هللا الرحمن الرحيم Ureteric, Vesical, & urethral stones Ureteric Calculus Epidemiology like renal stones Etiology like renal stones Risk factors like
4th stage Lec-8 جراحة بولية د.نعمان 11/10/2015 بسم هللا الرحمن الرحيم Ureteric, Vesical, & urethral stones Ureteric Calculus Epidemiology like renal stones Etiology like renal stones Risk factors like
A Giant Hydronephrotic Kidney with Ureteropelvic Junction Obstruction with Blunt Renal Trauma in a Boy
 A Giant Hydronephrotic Kidney with Ureteropelvic Junction Obstruction with Blunt Renal Trauma in a Boy BY JUNYA TSURUKIRI, HIDEFUMI SANO, YOSUKE TANAKA, TAKAO SATO, HIROKAZU TAGUCHI Abstract An 18-year-old
A Giant Hydronephrotic Kidney with Ureteropelvic Junction Obstruction with Blunt Renal Trauma in a Boy BY JUNYA TSURUKIRI, HIDEFUMI SANO, YOSUKE TANAKA, TAKAO SATO, HIROKAZU TAGUCHI Abstract An 18-year-old
Abdomen and Genitalia Injuries. Chapter 28
 Abdomen and Genitalia Injuries Chapter 28 Hollow Organs in the Abdominal Cavity Signs of Peritonitis Abdominal pain Tenderness Muscle spasm Diminished bowel sounds Nausea/vomiting Distention Solid Organs
Abdomen and Genitalia Injuries Chapter 28 Hollow Organs in the Abdominal Cavity Signs of Peritonitis Abdominal pain Tenderness Muscle spasm Diminished bowel sounds Nausea/vomiting Distention Solid Organs
Trauma of the lower urinary tract. Shady Saikali PGY 3 Urology LAUMCRH
 Trauma of the lower urinary tract Shady Saikali PGY 3 Urology LAUMCRH IntroducBon Urologic trauma occurs in 10-20% of pabents who experience major trauma Series of 31,380 trauma pabents, bladder injury
Trauma of the lower urinary tract Shady Saikali PGY 3 Urology LAUMCRH IntroducBon Urologic trauma occurs in 10-20% of pabents who experience major trauma Series of 31,380 trauma pabents, bladder injury
Genitourinary. Common Clinical Scenarios Protocoling Module. Patty Ojeda & Mariam Shehata
 The following training module was developed as a quality improvement project to serve as an educational tool for junior radiology residents. The following diagnostic radiology protocoling modules were
The following training module was developed as a quality improvement project to serve as an educational tool for junior radiology residents. The following diagnostic radiology protocoling modules were
Radiological Investigations of Abdominal Trauma
 76 77 Investigations of Abdominal Trauma Introduction: Trauma to abdominal organs is a common cause of patient morbidity and mortality among trauma patients. Causes of abdominal trauma include blunt injuries,
76 77 Investigations of Abdominal Trauma Introduction: Trauma to abdominal organs is a common cause of patient morbidity and mortality among trauma patients. Causes of abdominal trauma include blunt injuries,
ISPUB.COM. Traumatic Uretero-Pelvic Junction Disruption. G Kraushaar, S Harder, K Visvanathan INTRODUCTION CASE REPORT
 ISPUB.COM The Internet Journal of Radiology Volume 4 Number 1 Traumatic Uretero-Pelvic Junction Disruption G Kraushaar, S Harder, K Visvanathan Citation G Kraushaar, S Harder, K Visvanathan. Traumatic
ISPUB.COM The Internet Journal of Radiology Volume 4 Number 1 Traumatic Uretero-Pelvic Junction Disruption G Kraushaar, S Harder, K Visvanathan Citation G Kraushaar, S Harder, K Visvanathan. Traumatic
Find Medical Solutions to Your Problems HYDRONEPHROSIS. (Distension of Renal Calyces & Pelvis)
") HYDRONEPHROSIS (Distension of Renal Calyces & Pelvis) Hydronephrosis is the distension of the renal calyces and pelvis due to accumulation of the urine as a result of the obstruction to the outflow of
HYDRONEPHROSIS (Distension of Renal Calyces & Pelvis) Hydronephrosis is the distension of the renal calyces and pelvis due to accumulation of the urine as a result of the obstruction to the outflow of
SURGICAL PROCEDURES OPERATIONS ON THE UROGENITAL SYSTEM
 KIDNEYS AND PERINEPHRUM 1. No additional claim should be made for nephroscopy when done at the time of pyelolithotomy or nephrolithotomy. 2. In a routine surgical approach to the kidney and related procedures,
KIDNEYS AND PERINEPHRUM 1. No additional claim should be made for nephroscopy when done at the time of pyelolithotomy or nephrolithotomy. 2. In a routine surgical approach to the kidney and related procedures,
TitleRadiographic evaluation of blunt re. TSUJI, Akira; MATSUZAKI, Shouji; TA. Citation 泌尿器科紀要 (1989), 35(7):
, 35(7):") TitleRadiographic evaluation of blunt re TSUJI, Akira; MATSUZAKI, Shouji; TA Author(s) NAGAKURA, Kazuhiko; MURAI, Masaru; Hiroshi Citation 泌尿器科紀要 (1989), 35(7): 1119-1123 Issue Date 1989-07 URL http://hdl.handle.net/2433/116611
TitleRadiographic evaluation of blunt re TSUJI, Akira; MATSUZAKI, Shouji; TA Author(s) NAGAKURA, Kazuhiko; MURAI, Masaru; Hiroshi Citation 泌尿器科紀要 (1989), 35(7): 1119-1123 Issue Date 1989-07 URL http://hdl.handle.net/2433/116611
11 Genitourinary Trauma and Emergencies
 Página 1 de 26 11 Genitourinary Trauma and Emergencies Meir Daller Gennaro Carpinito A urologic emergency arises when a condition requires rapid diagnosis and immediate treatment. This chapter focuses
Página 1 de 26 11 Genitourinary Trauma and Emergencies Meir Daller Gennaro Carpinito A urologic emergency arises when a condition requires rapid diagnosis and immediate treatment. This chapter focuses
Case Report Delayed Presentation of Traumatic Intraperitoneal Rupture of Urinary Bladder
 Case Reports in Urology Volume 2012, Article ID 430746, 4 pages doi:10.1155/2012/430746 Case Report Delayed Presentation of Traumatic Intraperitoneal Rupture of Urinary Bladder Hazim H. Alhamzawi, 1 Husham
Case Reports in Urology Volume 2012, Article ID 430746, 4 pages doi:10.1155/2012/430746 Case Report Delayed Presentation of Traumatic Intraperitoneal Rupture of Urinary Bladder Hazim H. Alhamzawi, 1 Husham
Uroradiology Tutorial For Medical Students
 Uroradiology Tutorial For Medical Students Lesson 3: Cystography & Urethrography Part 1 American Urological Association Introduction Conventional radiography of the urinary tract includes several diagnostic
Uroradiology Tutorial For Medical Students Lesson 3: Cystography & Urethrography Part 1 American Urological Association Introduction Conventional radiography of the urinary tract includes several diagnostic
Surgery of urogenital trauma in condition of war or precarity
 Surgery of urogenital trauma in condition of war or precarity C. H. Rochat Multi-disciplinary Center for Robotic Surgery, Geneva (www.beaulieu.ch) Geneva Foundation for Medical Education and Research (www.gfmer.ch)
Surgery of urogenital trauma in condition of war or precarity C. H. Rochat Multi-disciplinary Center for Robotic Surgery, Geneva (www.beaulieu.ch) Geneva Foundation for Medical Education and Research (www.gfmer.ch)
Lecture 56 Kidney and Urinary System
 Lecture 56 Kidney and Urinary System The adrenal glands are located on the superomedial aspect of the kidney The right diagram shows a picture of the kidney with the abdominal walls and organs removed
Lecture 56 Kidney and Urinary System The adrenal glands are located on the superomedial aspect of the kidney The right diagram shows a picture of the kidney with the abdominal walls and organs removed
ABDOMINAL TRAUMA Lecture Prof. Zbigniew Wlodarczyk
 ABDOMINAL TRAUMA Lecture Prof. Zbigniew Wlodarczyk Epidemiology 2% of all traumas (4% amongst hospitalized patients) 75% M 25% F Average age 35 years 80% close 20% penetrating 40% liver and spleen, 10%
ABDOMINAL TRAUMA Lecture Prof. Zbigniew Wlodarczyk Epidemiology 2% of all traumas (4% amongst hospitalized patients) 75% M 25% F Average age 35 years 80% close 20% penetrating 40% liver and spleen, 10%
already in the operating room.(0 Ultrasonography (US) has also been found to be very useful in the early evaluation
 has also been found to be very useful in the early evaluation") Pictorial Essay Singapore Med J 2010, 51(6) 68 CME Article Computed tomography of blunt renal trauma Razali M R, Azian A A, Am ran A R, Azlin S ABSTRACT Renal injury is observed in 10 percent of cases
Pictorial Essay Singapore Med J 2010, 51(6) 68 CME Article Computed tomography of blunt renal trauma Razali M R, Azian A A, Am ran A R, Azlin S ABSTRACT Renal injury is observed in 10 percent of cases
SciFed Journal of Public Health. Endoscopic Management of Obstetrical Uretero-Uterine Fistula. Case Report and Review of Literature
 SciFed Journal of Public Health Case Report Open Access Endoscopic Management of Obstetrical Uretero-Uterine Fistula. Case Report and Review of Literature * Yasin Idweini * Chairperson of Urology Department
SciFed Journal of Public Health Case Report Open Access Endoscopic Management of Obstetrical Uretero-Uterine Fistula. Case Report and Review of Literature * Yasin Idweini * Chairperson of Urology Department
Delayed Presentation of Traumatic Bladder Injury: A case report and review of current treatment trends
 ISPUB.COM The Internet Journal of Urology Volume 5 Number 1 Delayed Presentation of Traumatic Bladder Injury: A case report and review of current treatment trends S Deem, C Lavender, S Agarwal Citation
ISPUB.COM The Internet Journal of Urology Volume 5 Number 1 Delayed Presentation of Traumatic Bladder Injury: A case report and review of current treatment trends S Deem, C Lavender, S Agarwal Citation
Pelvic fractures. Dr Raymond Yean, MBBS Surgical SRMO
 Pelvic fractures Dr Raymond Yean, MBBS Surgical SRMO PELVIC FRACTURES Pelvic fracture account for 2-8% all skeletal injuries Associated with High energy trauma Soft tissue injuries and blood loss. Shock,
Pelvic fractures Dr Raymond Yean, MBBS Surgical SRMO PELVIC FRACTURES Pelvic fracture account for 2-8% all skeletal injuries Associated with High energy trauma Soft tissue injuries and blood loss. Shock,
PARA107 Summary. Page 1-3: Page 4-6: Page 7-10: Page 11-13: Page 14-17: Page 18-21: Page 22-25: Page 26-28: Page 29-33: Page 34-36: Page 37-38:
 PARA107 Summary Page 1-3: Page 4-6: Page 7-10: Page 11-13: Page 14-17: Page 18-21: Page 22-25: Page 26-28: Page 29-33: Page 34-36: Page 37-38: Injury, Mechanisms of Injury, Time Critical Guidelines Musculoskeletal
PARA107 Summary Page 1-3: Page 4-6: Page 7-10: Page 11-13: Page 14-17: Page 18-21: Page 22-25: Page 26-28: Page 29-33: Page 34-36: Page 37-38: Injury, Mechanisms of Injury, Time Critical Guidelines Musculoskeletal
Role of Imaging in the evaluation of Renal Trauma
 Role of Imaging in the evaluation of Renal Trauma M. H. Ather,M.A. Noor ( Department of Surgery, The Aga Khan University, Karachi. ) Trauma is the leading cause of morbidity and mortality among young adults
Role of Imaging in the evaluation of Renal Trauma M. H. Ather,M.A. Noor ( Department of Surgery, The Aga Khan University, Karachi. ) Trauma is the leading cause of morbidity and mortality among young adults
Conservative Management of Renal Trauma: Ten Years Experience Reem Al-Bareeq MRCSI, CABU* Kadem Zabar CABS** Mohammed Al-Tantawi CABS***
 Bahrain Medical Bulletin, Vol. 28, No. 3, September 2006 Conservative Management of Renal Trauma: Ten Years Experience Reem Al-Bareeq MRCSI, CABU* Kadem Zabar CABS** Mohammed Al-Tantawi CABS*** Objective:
Bahrain Medical Bulletin, Vol. 28, No. 3, September 2006 Conservative Management of Renal Trauma: Ten Years Experience Reem Al-Bareeq MRCSI, CABU* Kadem Zabar CABS** Mohammed Al-Tantawi CABS*** Objective:
FIG The inferior and posterior peritoneal reflection is easily
 PSOAS HITCH, BOARI FLAP, AND COMBINATION OF PSOAS 7 HITCH AND BOARI FLAP The psoas hitch procedure, Boari flap, and transureteroureterostomy are useful operative procedures for reestablishing continuity
PSOAS HITCH, BOARI FLAP, AND COMBINATION OF PSOAS 7 HITCH AND BOARI FLAP The psoas hitch procedure, Boari flap, and transureteroureterostomy are useful operative procedures for reestablishing continuity
Medical - Clinical Research & Reviews
 Research Article Research Article Medical - Clinical Research & Reviews ISSN 2575-6087 Management of Kidney in Saiful Anwar General Hospital Malang Indonesia Besut Daryanto, I Made Udiyana Indradiputra,
Research Article Research Article Medical - Clinical Research & Reviews ISSN 2575-6087 Management of Kidney in Saiful Anwar General Hospital Malang Indonesia Besut Daryanto, I Made Udiyana Indradiputra,
Contents. Review anatomy of the urinary tract Imaging modalities
 Contents Review anatomy of the urinary tract Imaging modalities The Urinary Tract Kidneys ตาแหน งไต (position) อย ใน retroperitoneum ระด บ T12-L3 โดยไต ขวาจะม ระด บตากว าไตซ ายเล กน อย ร ปร าง (shape)
Contents Review anatomy of the urinary tract Imaging modalities The Urinary Tract Kidneys ตาแหน งไต (position) อย ใน retroperitoneum ระด บ T12-L3 โดยไต ขวาจะม ระด บตากว าไตซ ายเล กน อย ร ปร าง (shape)
MDCT Findings of Renal Trauma
 MDT of Renal Trauma Genitourinary Imaging Pictorial Essay Downloaded from www.ajronline.org by 148.251.232.83 on 04/06/18 from IP address 148.251.232.83. opyright RRS. For personal use only; all rights
MDT of Renal Trauma Genitourinary Imaging Pictorial Essay Downloaded from www.ajronline.org by 148.251.232.83 on 04/06/18 from IP address 148.251.232.83. opyright RRS. For personal use only; all rights
Contributors. COL James Jezoir, MC, USA MAJ Steve Hudak, MC, USA LTC Jack Walters, MC, USA CAPT Zsolt Stockinger, MC, USN
 JOINT TRAUMA SYS TEM CLINICAL PRACTIC E GUIDELINE (JTS CPG ) Genitourinary (GU) Injury Trauma Management (CPG ID: 42) This CPG provides indications for and the procedures associated with the initial management
JOINT TRAUMA SYS TEM CLINICAL PRACTIC E GUIDELINE (JTS CPG ) Genitourinary (GU) Injury Trauma Management (CPG ID: 42) This CPG provides indications for and the procedures associated with the initial management
Urologic Surgical Complications In Renal Transplantation
 Urologic Surgical Complications In Renal Transplantation Chris Freise, MD Professor of Surgery UCSF Transplant Division Urologic Complications Review of Bladder Anastomosis Complications and Management
Urologic Surgical Complications In Renal Transplantation Chris Freise, MD Professor of Surgery UCSF Transplant Division Urologic Complications Review of Bladder Anastomosis Complications and Management
Contributors T A B L E O F C O N T E N T S
 JOINT TRAUMA SYS TEM CLINICAL PRACTIC E GUIDELINE (JTS CPG ) Urologic Trauma Management (CPG ID: 42) Provides indications for and the procedures associated with the initial management of genitourinary
JOINT TRAUMA SYS TEM CLINICAL PRACTIC E GUIDELINE (JTS CPG ) Urologic Trauma Management (CPG ID: 42) Provides indications for and the procedures associated with the initial management of genitourinary
Combined Antegrade And Retrograde Endoscopic Realignment Of Traumatic Urethral Disruption
 ISPUB.COM The Internet Journal of Urology Volume 7 Number 1 Combined Antegrade And Retrograde Endoscopic Realignment Of Traumatic Urethral Disruption I SO, O OA, E JO, B BO, A RA Citation I SO, O OA, E
ISPUB.COM The Internet Journal of Urology Volume 7 Number 1 Combined Antegrade And Retrograde Endoscopic Realignment Of Traumatic Urethral Disruption I SO, O OA, E JO, B BO, A RA Citation I SO, O OA, E
Bladder & Urethral Trauma. Bohyun Kim Professor of Radiology Mayo Clinic College of Medicine
 Bladder & Urethral Trauma Bohyun Kim Professor of Radiology Mayo Clinic College of Medicine Disclosure None Acknowledgement Akira Kawashima, Mayo Clinic Scottsdale, AZ Eric Lantz, Mayo Clinic Rochester,
Bladder & Urethral Trauma Bohyun Kim Professor of Radiology Mayo Clinic College of Medicine Disclosure None Acknowledgement Akira Kawashima, Mayo Clinic Scottsdale, AZ Eric Lantz, Mayo Clinic Rochester,
We have reviewed this material in accordance with U.S. Copyright Law and have tried to maximize your ability to
 Author(s): Patrick Carter, Daniel Wachter, Rockefeller Oteng, Carl Seger, 2009-2010. License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution
Author(s): Patrick Carter, Daniel Wachter, Rockefeller Oteng, Carl Seger, 2009-2010. License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution
Penetrating abdominal trauma clinical view. Ari Leppäniemi, MD Department of Abdominal Surgery Meilahti hospital University of Helsinki Finland
 Penetrating abdominal trauma clinical view Ari Leppäniemi, MD Department of Abdominal Surgery Meilahti hospital University of Helsinki Finland Meilahti hospital - one of Helsinki University hospitals -
Penetrating abdominal trauma clinical view Ari Leppäniemi, MD Department of Abdominal Surgery Meilahti hospital University of Helsinki Finland Meilahti hospital - one of Helsinki University hospitals -
PROTOCOLS. Lap-belt syndrome. Principal investigator. Background
 Lap-belt syndrome Principal investigator Claude Cyr, MD, Centre hospitalier universitaire de Sherbrooke, 3001 12 e Avenue Nord, Sherbrooke QC J1H 5N4; tel.: (819) 346-1110, ext. 14634; fax: (819) 564-5398;
Lap-belt syndrome Principal investigator Claude Cyr, MD, Centre hospitalier universitaire de Sherbrooke, 3001 12 e Avenue Nord, Sherbrooke QC J1H 5N4; tel.: (819) 346-1110, ext. 14634; fax: (819) 564-5398;
Pelvic Injuries. Chapter 21
 Chapter 21 Introduction Injuries of the pelvis are an uncommon, but potentially lethal, battlefield injury. Blunt injuries may be associated with major hemorrhage and early mortality. Death within the
Chapter 21 Introduction Injuries of the pelvis are an uncommon, but potentially lethal, battlefield injury. Blunt injuries may be associated with major hemorrhage and early mortality. Death within the
Algorithms for managing the common trauma patient
 ALGORITHMS Algorithms for managing the common trauma patient J John, MB ChB Department of Urology, Frere Hospital, East London Hospital Complex, East London, South Africa Corresponding author: J John (jeffveenajohn@gmail.com)
ALGORITHMS Algorithms for managing the common trauma patient J John, MB ChB Department of Urology, Frere Hospital, East London Hospital Complex, East London, South Africa Corresponding author: J John (jeffveenajohn@gmail.com)
Pancreatico-Duodenal Trauma: Drain, Debride, Divert, Despair BACKGROUND EPIDEMIOLOGY 9/11/2018
 Pancreatico-Duodenal Trauma: Drain, Debride, Divert, Despair Rochelle A. Dicker, M.D. Professor of Surgery and Anesthesia UCLA BACKGROUND Lancet 1827: Travers, B Rupture of the Pancreas British Journal
Pancreatico-Duodenal Trauma: Drain, Debride, Divert, Despair Rochelle A. Dicker, M.D. Professor of Surgery and Anesthesia UCLA BACKGROUND Lancet 1827: Travers, B Rupture of the Pancreas British Journal
An Unexpected Cause Of Spontaneous Perinephric Urinoma: A Case Report. L Chandrasekharan, T Abdl Ghaffar, M Venkatramana, K Mammigatty
 ISPUB.COM The Internet Journal of Radiology Volume 4 Number 1 An Unexpected Cause Of Spontaneous Perinephric Urinoma: A Case Report L Chandrasekharan, T Abdl Ghaffar, M Venkatramana, K Mammigatty Citation
ISPUB.COM The Internet Journal of Radiology Volume 4 Number 1 An Unexpected Cause Of Spontaneous Perinephric Urinoma: A Case Report L Chandrasekharan, T Abdl Ghaffar, M Venkatramana, K Mammigatty Citation
Pelvic Prolapse. A Patient Guide to Pelvic Floor Reconstruction
 Pelvic Prolapse A Patient Guide to Pelvic Floor Reconstruction Pelvic Prolapse When an organ becomes displaced, or slips down in the body, it is referred to as a prolapse. Your physician has diagnosed
Pelvic Prolapse A Patient Guide to Pelvic Floor Reconstruction Pelvic Prolapse When an organ becomes displaced, or slips down in the body, it is referred to as a prolapse. Your physician has diagnosed
Nursing Care for Children with Genitourinary Dysfunction I
 Nursing Care for Children with Genitourinary Dysfunction I 1 Assessment of renal function Clinical manifestations Laboratory tests Urinalysis Urine culture and sensitivity Renal/bladder ultrasound Testicular
Nursing Care for Children with Genitourinary Dysfunction I 1 Assessment of renal function Clinical manifestations Laboratory tests Urinalysis Urine culture and sensitivity Renal/bladder ultrasound Testicular
Coding Companion for Urology/Nephrology. A comprehensive illustrated guide to coding and reimbursement
 Coding Companion for Urology/Nephrology A comprehensive illustrated guide to coding and reimbursement 2014 Contents Getting Started with Coding Companion...i Integumentary...1 Arteries and Veins...15 Lymph
Coding Companion for Urology/Nephrology A comprehensive illustrated guide to coding and reimbursement 2014 Contents Getting Started with Coding Companion...i Integumentary...1 Arteries and Veins...15 Lymph
Sara Schaenzer Grand Rounds January 24 th, 2018
 Sara Schaenzer Grand Rounds January 24 th, 2018 Bladder Anatomy Ureter Anatomy Areas of Injury Bladder: Posterior bladder wall above trigone Ureter Crosses beneath uterine vessels At pelvic brim when ligating
Sara Schaenzer Grand Rounds January 24 th, 2018 Bladder Anatomy Ureter Anatomy Areas of Injury Bladder: Posterior bladder wall above trigone Ureter Crosses beneath uterine vessels At pelvic brim when ligating
EAU Guidelines on Urological Trauma
 EAU Guidelines on Urological Trauma N.D. Kitrey (Chair), N. Djakovic, M. Gonsalves, F.E. Kuehhas, N. Lumen, E. Serafetinidis, D.M. Sharma, D.J. Summerton Guidelines Associates: P-J. Elshout, A. Sujenthiran,
EAU Guidelines on Urological Trauma N.D. Kitrey (Chair), N. Djakovic, M. Gonsalves, F.E. Kuehhas, N. Lumen, E. Serafetinidis, D.M. Sharma, D.J. Summerton Guidelines Associates: P-J. Elshout, A. Sujenthiran,
CLINICAL PRESENTATION AND RADIOLOGY QUIZ QUESTION
 Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 6/23/2012 Radiology Quiz of the Week # 78 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 6/23/2012 Radiology Quiz of the Week # 78 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
Radiographic Procedures III (RAD 228)
") Radiographic Procedures III (RAD 228) Urinary System RADIOGRAPHIC EXAMINATIONS Urinary System Antegrade Exam IVU Functional test Hypertensive evaluation as per protocol Retrograde Exams Retrograde Urography
Radiographic Procedures III (RAD 228) Urinary System RADIOGRAPHIC EXAMINATIONS Urinary System Antegrade Exam IVU Functional test Hypertensive evaluation as per protocol Retrograde Exams Retrograde Urography
Trauma. Neck trauma zones. Neck Injuries 1/3/2018. Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure
 Trauma 45 minutes highest points Ahmed Mahmoud, MD Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure Neck trauma zones Airway ;Rapid sequence intubation Breathing ;Needle
Trauma 45 minutes highest points Ahmed Mahmoud, MD Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure Neck trauma zones Airway ;Rapid sequence intubation Breathing ;Needle
Joint Theater Trauma System Clinical Practice Guideline
 Page 1 of 10 UROLOGIC TRAUMA MANAGEMENT Original Release/Approval 18 Dec 2004 Note: This CPG requires an annual review. Reviewed: Mar 2012 Approved: 2 Apr 2012 Supersedes:, 30 June 2010 Minor Changes (or)
Page 1 of 10 UROLOGIC TRAUMA MANAGEMENT Original Release/Approval 18 Dec 2004 Note: This CPG requires an annual review. Reviewed: Mar 2012 Approved: 2 Apr 2012 Supersedes:, 30 June 2010 Minor Changes (or)
Pediatric Ure-Radiology*
 Pediatric Ure-Radiology* HERMAN GROSSMAN, M.D. Professor of Radiology and Pediatrics, Duke University Medical Center, Durham, North Carolina "Routine" radiologic studies do not, often enough, concentrate
Pediatric Ure-Radiology* HERMAN GROSSMAN, M.D. Professor of Radiology and Pediatrics, Duke University Medical Center, Durham, North Carolina "Routine" radiologic studies do not, often enough, concentrate
Jerne Kaz Niels B. Paber, MD* and Michael U. Abutazil, MD**
 Case Report Case Report: Page Kidney Secondary to Severe Ureterohydronephrosis and Perinephric Urinoma with Rupture of Renal Fornix Secondary to a Rare Complication of Ureteral Calculi Jerne Kaz Niels
Case Report Case Report: Page Kidney Secondary to Severe Ureterohydronephrosis and Perinephric Urinoma with Rupture of Renal Fornix Secondary to a Rare Complication of Ureteral Calculi Jerne Kaz Niels
Evaluation and management of renal injuries: consensus statement of the renal trauma subcommittee
 Miscellaneous RENAL TRAUMA CONSENSUS STATEMENT R.A. SANTUCCI ET AL. The first in this series of five papers concerns the evaluation and management of renal injuries. The authors of this paper come from
Miscellaneous RENAL TRAUMA CONSENSUS STATEMENT R.A. SANTUCCI ET AL. The first in this series of five papers concerns the evaluation and management of renal injuries. The authors of this paper come from
Interventional Radiology in Trauma. Vikash Prasad, MD, FRCPC Vascular and Interventional Radiology The Moncton Hospital
 Interventional Radiology in Trauma Vikash Prasad, MD, FRCPC Vascular and Interventional Radiology The Moncton Hospital Disclosures None relevant to this presentation Shareholder Johnson and Johnson Goal
Interventional Radiology in Trauma Vikash Prasad, MD, FRCPC Vascular and Interventional Radiology The Moncton Hospital Disclosures None relevant to this presentation Shareholder Johnson and Johnson Goal
Renal trauma: What the radiologist needs to know
 Renal trauma: What the radiologist needs to know Poster No.: C-1519 Congress: ECR 2016 Type: Educational Exhibit Authors: D. Roriz, I. Abreu, P. Belo Soares, F. Caseiro Alves ; 1 1 2 2 3 3 4 4 Guimarães/PT,
Renal trauma: What the radiologist needs to know Poster No.: C-1519 Congress: ECR 2016 Type: Educational Exhibit Authors: D. Roriz, I. Abreu, P. Belo Soares, F. Caseiro Alves ; 1 1 2 2 3 3 4 4 Guimarães/PT,
Forms: Etiology ureter-occlusion! Ureter-occlusion
 Surgical anatomy Surgery of the Kidney Dr. T. Németh, DVM, Ph.D Surgical Diseases of the Kidney Hydronephrosis Renal injuries Surgical Diseases of the Kidney Hydronephrosis Renal injuries Hydronephrosis
Surgical anatomy Surgery of the Kidney Dr. T. Németh, DVM, Ph.D Surgical Diseases of the Kidney Hydronephrosis Renal injuries Surgical Diseases of the Kidney Hydronephrosis Renal injuries Hydronephrosis
ORIGINAL ARTICLE. Complications Following Renal Trauma
 ORIGINAL ARTICLE Complications Following Renal Trauma Margaret Starnes, MD; Demetrios Demetriades, MD, PhD; Pantelis Hadjizacharia, MD; Kenji Inaba, MD; Charles Best, MD; Linda Chan, PhD Objectives: To
ORIGINAL ARTICLE Complications Following Renal Trauma Margaret Starnes, MD; Demetrios Demetriades, MD, PhD; Pantelis Hadjizacharia, MD; Kenji Inaba, MD; Charles Best, MD; Linda Chan, PhD Objectives: To
Approach to imaging in urological injuries secondary to trauma
 Approach to imaging in urological injuries secondary to trauma Poster No.: C-1470 Congress: ECR 2015 Type: Educational Exhibit Authors: M. Pérez Rubiralta, R. Mast Vilaseca, A. Pons, M. de Albert, R. Barranco
Approach to imaging in urological injuries secondary to trauma Poster No.: C-1470 Congress: ECR 2015 Type: Educational Exhibit Authors: M. Pérez Rubiralta, R. Mast Vilaseca, A. Pons, M. de Albert, R. Barranco
URINARY SYSTEM. MEDICAL TERMINOLOGY Chapter Six HIT #141. Anatomy
 URINARY SYSTEM MEDICAL TERMINOLOGY Chapter Six HIT #141 Anatomy Kidneys = bean-shaped organs, located on each side of the spinal column, removal of waste from the blood. Nephron = microscopic located in
URINARY SYSTEM MEDICAL TERMINOLOGY Chapter Six HIT #141 Anatomy Kidneys = bean-shaped organs, located on each side of the spinal column, removal of waste from the blood. Nephron = microscopic located in
List of Core and Specialised Procedures for Urology
 List of Core and Specialised Procedures for Urology Appendix 5 The list below of privileges for core and specialised procedures is subject to periodic review by Farrer Park Hospital and/or Farrer Park
List of Core and Specialised Procedures for Urology Appendix 5 The list below of privileges for core and specialised procedures is subject to periodic review by Farrer Park Hospital and/or Farrer Park
How I Do It - Evaluation of the Urethra
 How I Do It - Evaluation of the Urethra Parvati Ramchandani, MD Professor, Radiology and Surgery University of Pennsylvania Medical Center Philadelphia, PA, USA Disclosure of Commercial Interest Neither
How I Do It - Evaluation of the Urethra Parvati Ramchandani, MD Professor, Radiology and Surgery University of Pennsylvania Medical Center Philadelphia, PA, USA Disclosure of Commercial Interest Neither
Proceedings of the 34th World Small Animal Veterinary Congress WSAVA 2009
 www.ivis.org Proceedings of the 34th World Small Animal Veterinary Congress WSAVA 2009 São Paulo, Brazil - 2009 Next WSAVA Congress : Reprinted in IVIS with the permission of the Congress Organizers IMAGING
www.ivis.org Proceedings of the 34th World Small Animal Veterinary Congress WSAVA 2009 São Paulo, Brazil - 2009 Next WSAVA Congress : Reprinted in IVIS with the permission of the Congress Organizers IMAGING
Pediatric Abdomen Trauma
 Pediatric Abdomen Trauma Susan D. John, MD, FACR Pediatric Trauma Trauma is leading cause of death and disability in children and adolescents Causes and effects vary between age groups Blunt trauma predominates
Pediatric Abdomen Trauma Susan D. John, MD, FACR Pediatric Trauma Trauma is leading cause of death and disability in children and adolescents Causes and effects vary between age groups Blunt trauma predominates
IMAGING OF BLUNT ABDOMINAL TRAUMA, PART I
 IMAGING OF BLUNT ABDOMINAL TRAUMA, PART I QuickTime and a TIFF (Uncompressed) decompressor are needed to see this picture. Ruedi F. Thoeni, M. D. D University of California, San Francisco SCBT-MR Summer
IMAGING OF BLUNT ABDOMINAL TRAUMA, PART I QuickTime and a TIFF (Uncompressed) decompressor are needed to see this picture. Ruedi F. Thoeni, M. D. D University of California, San Francisco SCBT-MR Summer
University of Cape Town
 The copyright of this thesis vests in the author. No quotation from it or information derived from it is to be published without full acknowledgement of the source. The thesis is to be used for private
The copyright of this thesis vests in the author. No quotation from it or information derived from it is to be published without full acknowledgement of the source. The thesis is to be used for private
URETHRAL injuries are rarely lifethreatening. Cases Theresa M. Campo, DNP, RN, NP-C. Scrotal Pain After a Fall
 Cases O F N O T E Theresa M. Campo, DNP, RN, NP-C Advanced Emergency Nursing Journal Vol. 31, No. 3, pp. 214 220 Copyright c 2009 Wolters Kluwer Health Lippincott Williams & Wilkins Scrotal Pain After
Cases O F N O T E Theresa M. Campo, DNP, RN, NP-C Advanced Emergency Nursing Journal Vol. 31, No. 3, pp. 214 220 Copyright c 2009 Wolters Kluwer Health Lippincott Williams & Wilkins Scrotal Pain After